71
Presented by: Dr. Md. Zareer Tafadar Post Graduate Student Deptt. Of Anaesthesiology &Critical Care Silchar Medical College & Hospital.
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | zareer-tafadar |
| View: | 308 times |
| Download: | 0 times |
Presented by:
Dr. Md. Zareer Tafadar
Post Graduate Student
Deptt. Of Anaesthesiology &Critical Care
Silchar Medical College & Hospital.
Opioids have been the mainstay of pain treatment for thousandsof years, and they remain so today.
The word opium is derived from the Greek word for juice “opios”.
Opium is a dark brown, resinous material obtained from thecapsule of the poppy plant (Papaver somniferum).
There are 20 natural alkaloids derived from the juice of poppyplant.
The term “opioid” is used to denote all exogenous substancesnatural and synthetic, that bind to any of the several sub-populations of opioid receptors and produce at least some agonisteffects.
Opiate is the term used for drugs derived from opium.
Opioids are among the world's oldest known drugs and thetherapeutic use of the opium predates recorded history.
Hippocrates and Galen, two of the most prominent Greekphysicians, employed opium to battle headaches, coughing,asthma and melancholy
1805- German chemist Friedrich Serturner isolated the pure activeingredient in opium. He named this chemical “morphine”, afterMorpheus, the Greek god of dreams
1874: German chemists invented heroin by adding two acetyl groups to morphine .
1939: Meperidine the first opiate with a structure altogether different from that of morphine.

1942: Weijlard and Erikson produced nalorphine (N-allylnormorphine), the first opiate antagonist.
1959:Fentanyl was first synthesized by Paul Janssen
1973: Candace Pert and Solomon Snyder discovered that opioidsact by attaching to specific receptors within the brain. These receptors were called the opiate receptors.
1975: Scottish neuroscientists John Hughes and Hans Kosterlitzdiscovered two neurotransmitters that activate the opiate receptors.- “endorphins”.
1974 to 1976: Other fentanyl congeners like alfentanyl, sufentanylwere synthesized.

On the basis of source
Naturally occuring
Phenanthrene :Morphine, Codeine ,Thebaine
Benzylisoquinoline: Papaverine ,Noscapine ,Narcine
Semisynthetic
Heroin
Dihydromorphone/morphinone
Thebaine derivatives: Etorphine, Buprenorphine.
Synthetic
Phenylpiperidines: Meperidine, Fentanyl, Sufentanil, Alfentanil, Remifentanil.
Morphinan compounds:Levorphanol, Butorphanol.
Phenyl-heptylmines: Methadone, Propoxyphene,Dextropropoxyphene Diphenylpropylamine.
Benzomorphans: Pentazocine

On the basis of action
Opioid Agonists
Morphine Meperidine Fentanyl Sufentanyl Remifentanyl Alfentanyl Codeine Hydromorphone Oxymorphone Oxycodone Propoxyphene Methadone Tramadol Heroin
Opiod Agonist- Antagonist
Pentazocine Butorphanol Nalbuphine Buprenorphine Nalorphene Bremazocine Dezocine
Opiod Antagonist
Naloxone Naltrexone Nalmefene
Endorphins:
Derived from POMC
ß-endorphins: 2 Types - ß-endorphin1 and ß-endorphin-2
Primarily μ agonist and also has δ action
Enkephalins:
Derive from Proenkephalin
Met-ENK and leu-ENK
Met-ENK - Primarily μ and δ agonist and leu-ENK – δ agonist
Dynorphins:
Derive from Prodynorphin: DYN-A and DYN-B
Potent κ agonist and also have μ and δ action
Endomorphins:
Binds to the µ-receptor with high affinity and high selectivity.

μ receptor κ receptor δ receptor
Location μ1 – supraspinal
µ2 - spinal
κ1 – spinal
κ3 –supraspinal
Spinal
Supra-spinal
Effects Analgesia
Respiratory depression
Sedation
Euphoria
Miosis
Bradycardia,
Hypothermia
Physical dependence
Spinal analgesia
Dysphoria
Sedation
Psychomimetic
Spinal analgesia
Affective behaviour
(Supraspinal)
Respiratory depression
Agonists Morphine, Codeine,
Fentanyl
Pentazocine(weak)
Endorphins
Pentazocine,
Dynorphins
Enkephalins
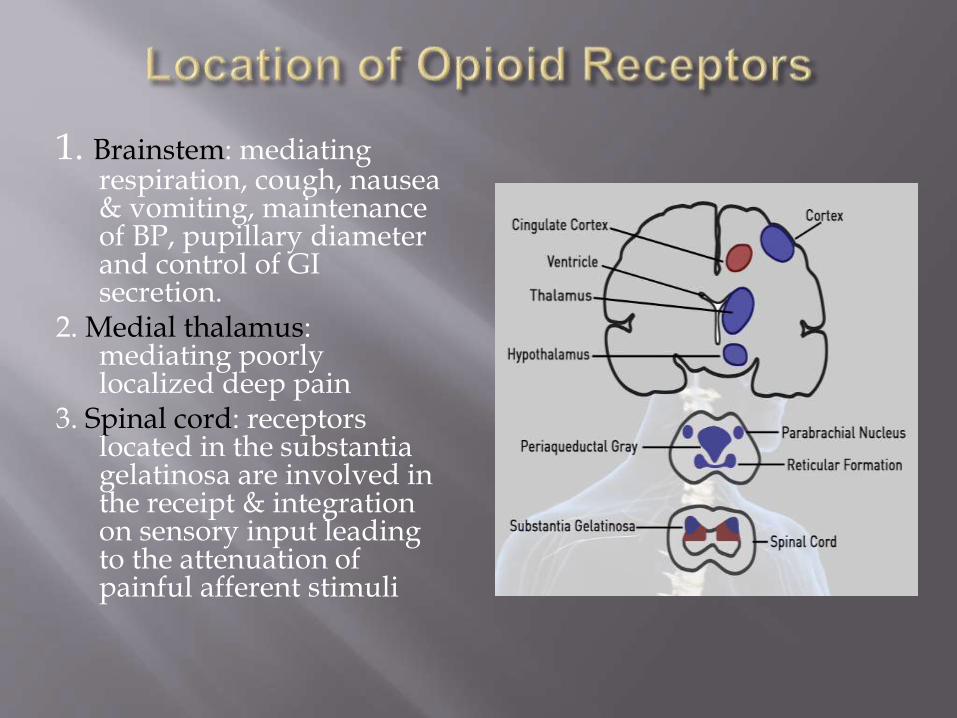
1. Brainstem: mediating respiration, cough, nausea & vomiting, maintenance of BP, pupillary diameter and control of GI secretion.
2. Medial thalamus: mediating poorly localized deep pain
3. Spinal cord: receptors located in the substantiagelatinosa are involved in the receipt & integration on sensory input leading to the attenuation of painful afferent stimuli
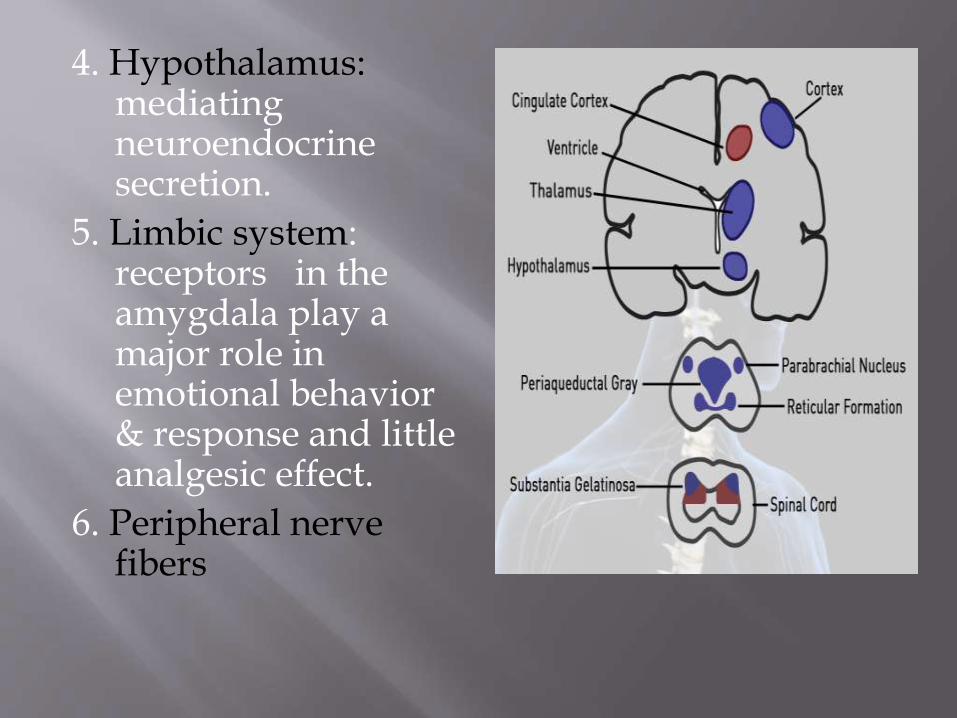
4. Hypothalamus: mediating neuroendocrinesecretion.
5. Limbic system: receptors in the amygdala play a major role in emotional behavior & response and little analgesic effect.
6. Peripheral nerve fibers
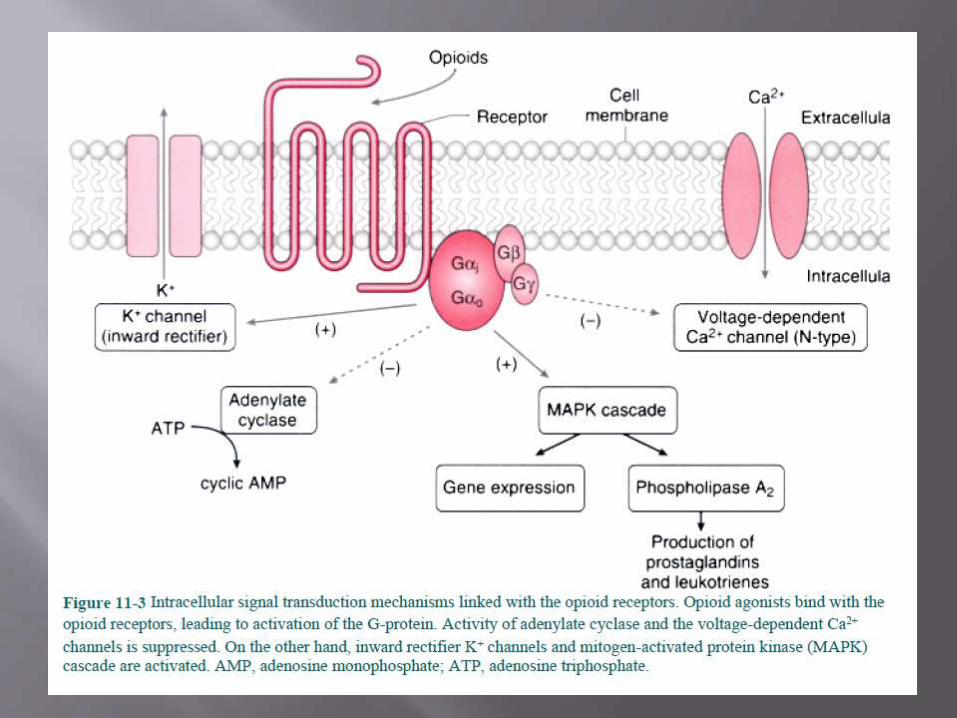
Opioid receptors belong to a super family of G-protein coupled receptors.
All three opioid receptor classes couple to G-proteins and inhibit adenyl-cyclase. The subsequent reduction of intracellular cAMPresults in opening of K+ channels and supression of N type of Ca2+
channels.
The resultant hyperpolarization prevents excitation and propagation of action potential.
The reduced intracellular Ca2+ leads to suppression of neurotransmitter release – NA, DA, 5-HT, GABA and Glutamate.
Opioid receptors may regulate the function of other ion channels including excitatory post synaptic currents evoked by NMDA receptors.

Mechanism Of Action Of μ-Agonists In The Spinal Cord
Pre-synaptic Neuron
•Activation of opioid receptor decreases Ca2+ influx in response to incoming AP
•Decrease in level of neuroexcitatorytransmitters like Glutamate NA, DA, 5-HT.
Post-synaptic Neuron
• Increase in the K+ efflux
• Resultant hyperpolarization prevents propagation of action potential
Pharmacological Actions
Analgesia
Produces strong analgesia without
loss of consciousness.
Other sensory modalities are not
affected.
Increases the threshold of pain and modifies `
the perception of noxious stimuli.
Associated reactions to pain -apprehension, fear and autonomic effects are also relieved .
Nociceptive pain is better relieved than neuritic pain.
Visceral pain is relieved better than somatic pain.

Sedation:
Drowsiness and indifference to surroundings.
Inability to concentrate and extravagant imagination – colorful day dream.
Apparent excitement.
Larger doses produce sleep – EEG resembles normal sleep
Mood effects:
Opioids produce euphoria, tranquility, and other alterations of mood including rewarding properties.
In persons with pain & addicts sense of wellbeing, pleasurable floating feelings – euphoria.
In normal persons these sensations may be unpleasant in absence of pain – dysphoria.

Depression
Pontine and medullary ventilatory centre – Both rate and depth of respiration is diminished.
Medullary cough centre .
Temperature regulating centre.
Vasomotor centre – High doses cause fall in BP.
Stimulation
CTZ – sensitize CTZ to vestibular and other impulses.
Edinger Westphal Nucleus – miosis .
Vagal centre – Bradycardia .
Hippocampal cells – convulsions (inhibition of GABA release).

Neuro-endocrine:
GnRH and CRH are inhibited – FSH, LH and ACTH levels are lowered. Only short term tolerance develops.
Decrease in levels of Sex hormone and corticosteroids, but no infertility.
Increases ADH release – oliguria..
CVS:
No direct action on the myocardium.
Histamine release, depression of vasomotor centre and decrease in the sympathetic tone of blood vessels may cause vasodilatation leading to hypotension.
Cardiac work reduction due to consistent vasodilatation.

Pharmacokinetics
Absorption and Distribution: Well absorbed after IM administration with onset of action in 15 -30
min. Duration of action is about 4 hrs. Variable absorption orally. IV administration results in wide distribution in the visceral
circulation. However CNS penetration is poor. Readily crosses placental barrier – causing hypoxia and apnoea in
fetus. Metabolism:
The principal pathway of metabolism is conjugation with glucuronic acid in hepatic and extra hepatic sites esp. the kidneys to produce water soluble metabolites.
Morphine-3-glucuronide (70-80%): Pharmacologically inactive. Morphine-6-glucuronide (5-10%): Agonist action at µ–receptors
produces analgesia and depression of ventilation. Excretion:
Via Urine, Plasma t1/2 = 2-3 hrs Completely eliminated in 24 hrs. Elimination of morphine glucuronides may be impaired in patients
with renal failure.

all µ-receptor agonists dose dependent depression
of respiration,
• brainstem sensitivity to CO2
• slope of the CO2-ventilation response curve
• apnoeic threshold
• hypoxic drive to respiration
•carotid body chemoreception is virtually abolished
• pontine & medullary centres involved in rhythmic respiration
Signs :
Oxygen desaturation .
Obstructive apnea.
Periodic breathing resembling Cheyne- Stokes breathing.
Slow respiratory rate.
The stimulatory effect of hypercapnoea on ventilation is blunted.
Apnoeic threshold and resting EtPCO2 are increased .
However voluntary control of respiration is not lost.
Effect is increased during co-administration with other CNS
depressants like inhalational anesthetics, BZDs, and most of the
sedative-hypnotics.
Standard therapy is Naloxone.

CVS: Orthostatic hypotension. Bradycardia may be due to stimulation of
vagal nuclei in medulla or direct depressant effect of morphine on the SA node.
CNS: Sedation, mental clouding – sometimes dysphoria. Skeletal muscle
rigidity and myoclonus. Raised ICT
Smooth Muscle contraction: Biliary colic, urinary retention and
bronchospasm.
Nausea and vomiting.
Idiosyncrasy and allergy.
Tolerance and dependence:
Tolerance and dependence is the most common problem with morphine.
Exhibited in most actions except constipation and miosis.
It produces psychological and physical dependence.
Withdrawal may lead to drug seeking behaviour and may turn to
morphine withdrawal syndrome. It is characterized by anxiety, fear,
restlesness, diarrhoea, abdominal colic, delirium and convulsion.
Treatment is methadone

Acute Morphine Poisoning:
Occurs if >50 mg (Lethal dose – 250 mg) is administered.
Manifested as depression of ventilation which may progress to
apnoea.
The triad of miosis, hypoventilation and coma should suggest
overdose with an opioid.
Gastric lavage with KMnO4. Specific antidote: Naloxone: 0.4 to 0.8
mg IV repeatedly in 2-3 minutes till respiration picks up.
Therapeutic Uses
Analgesic:
Surgical analgesia, post operative analgesia, long bone fracture, burns.
Myocardial infarction. Palliative therapy in cancer. Visceral pains – pulmonary embolism, pleurisy, acute
pericarditis.
Other Uses
Pre-anaesthetic medication
Acute left ventricular failure – Cardiac asthma
Congeners of morphine such as loperamide and diphenoxylatemay be used in severe intractable diarrhoea.
Contraindications
Head Injury
Bronchial asthma
Respiratory insufficiency - emphysema
Shock – Hypotension
Undiagnosed acute abdomen
Renal Failure, Liver diseases and hypothyroidism
Unstable personalities
Phenylepiperidine derivativehaving structural similaritieswith that of local anaesthetics.
Pharmacokinetics
1/10th as potent as morphine, but efficacy is similar. Rapid but short duration of action (2-3 Hrs) In equal analgesic dose it produces as much sedation, euphoria
and respiratory depression as morphine. Less spasmodic action in smooth muscles – less miosis,
constipation and urinary retention Not useful in diarrhoea and is devoid of antitussive action. Less histamine release – safer in asthmatics. Better oral absorption.
Clinical Uses:
For labour analgesia and post operative analgesia. Effective for suppression of post operative shivering.
Adverse Effects:
Similar to morphine. Atropine like effects – dry mouth, blurred vision,
tachycardia. Overdose – tremors, mydriasis, delirium and
convulsion due to norpethidine accumulation. Serotonin syndrome in patients receiving MAOs

Phenylpiperidine derivative
synthetic opioid structurally
related to meperidine
Pharmacokinetics
75 to 125 times as potent as morphine.
Rapid onset and shorter duration due to greater lipid solubility.
Rapidly redistributed to inactive storage sites such as fat and skeletal muscles.
75% of the initial dose undergoes first-pass pulmonary uptake.

Clinical Uses
Analgesia: Low IV dose 1-2 µg/kg Adjuvant to anaesthetics (2-20 µg/kg) to blunt
circulatory response to Intubation of the trachea and to decrease requirement of inhalational agents.
As a component of Total Intravenous Anaesthesia(TIVA) – Dose 50-150 µg/kg.
Intrathecal fentanyl may be used to provide labouranalgesia and as an adjuvant for spinal and epidural anaesthesia.
Oral transmucosal fentanyl 5- 20 µg/kg may be used to decrease pre-operative anxiety and facilitate induction.
Transdermal fentanyl patch delivering 75 - 100 µg/hr may be used for treatment of chronic pain in cancer patients.

Adverse Effects:
Similar to morphine Persistent/ recurrent respiratory depression Carotid sinus baroreceptor reflex control is
markedly depressed- caution in neonates. Bradycardia is more prominent than in
morphine. Allergic reactions are rare. Myoclonus may produce clinical picture of
seizure activity in the absence of EEG changes
Modest increases in ICP in head injury patients inspite of an unchanged PaCO2
.

Fentanyl As a Sole Anaesthetic Agent
Advantages Lack of direct myocardial depressant effects. Absence of histamine release. Suppression of stress respone to surgery.
Disadvantages Failure to prevent sympathetic response to
surgical stimulation. Possible patient awareness. Postoperative ventilatory depression

Thienyl analogue of fentanyl.
Pharmacokinetics:
Potency is 5 to 10 times that of fentanyl..
Lipophilic nature permits rapid penetration into the BBB and onset of CNS effects.
Approx. 60% of the drug undergoes first pass pulmonary uptake.
Extensive protein binding - mainly α1 acid glycoprotein.
Enhanced effect in neonates probably due to α1 acid glycoprotein.
Metabolism :
N-dealkylation→ inactive metabolite
O-demethylation→ desmethyl sufentanyl has10% activity of sufentanyl.
Extensively metabolised by hepatic microsomal enzymes.
Hepatic clearance sensitive to hepatic blood flow.
Context-sensitive half time is shorter than that of alfentanyl for continuous infusion up to 8 hrs due to the large Vd.
Sufentanyl Vs Fentanyl:
Longer analgesia and less ventilatory depression.
More rapid induction.
Earlier emergence and earlier tracheal extubation

Fentanyl analogue with lesser potency and shorter duration of action.
Despite its lower lipid solubilty it has a more rapid onset of action due to the higher degree of non-ionisation.
It is used to provide analgesia when the noxious stimulation is acute but transient as in laryngoscopy, tracheal intubation and performance of a retrobulbar block.
Associated with a lower incidence of PONV.
Acute dystonia has been described in patients with untreated Parkinson’s disease.

Selective μ agonist with potency similar to fentanyl.
Predictable onset and termination of effect because of
Rapid clearance
Smaller Vd
No significant redistribution to inactive storage sites .
Unique ester-linkage
Metabolised by non-specific plasma and tissue esterases. Safe in hepatic and renal failure.
Not a substrate of pseudo-cholinesterase.
Blood-brain equilibration time similar to alfentanil.
Clinical Uses
Short intense analgesia
Suppressing transient sympathetic response to laryngoscopy of at risk patients.
Intermittent administration as PCA during labour and delivery.
Sedation in mechanically ventilated patients.
Sedation and analgesia during monitored anaesthesia.
To attenuate haemodynamic response to electroconvulsive therapy.
Side effects:. Termination of analgesic effect on accidental stoppage of infusion.
Induce seizure like activity
Nausea and vomiting
Depression of ventillation
Decrease in B.P and H.R.
Acute opoid tolerance.
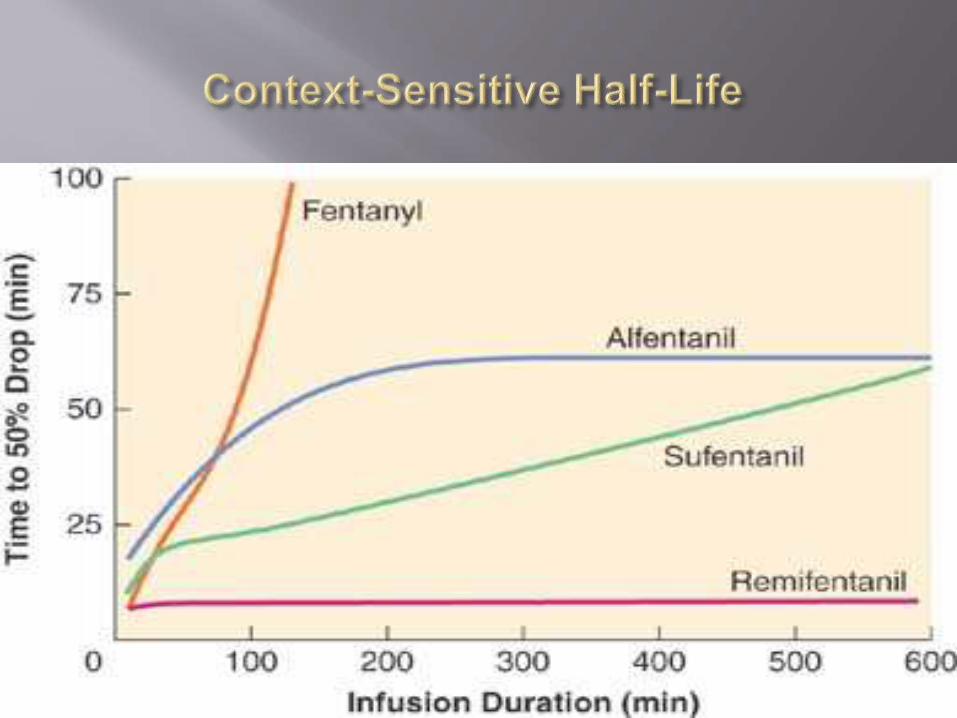
Time taken for blood plasma concentration of a drug to decline by one half after an infusion designed to maintain a steady state (i.e. a constant plasma concentration) has been stopped.
The “context” in this case is the duration of infusion.
During an infusion, the peripheral compartments begin to “fill up.” After the infusion is stopped, drug will be eliminated, but will also continue to be redistributed as long as the concentration in a peripheral compartment. This leads to a rapid drop in central compartment drug concentration.
When central compartment (plasma) concentration drops below that of the peripheral compartment(s), the direction of drug redistribution will reverse and will slow the decline in plasma concentration

Initial Phase Late Phase
Central Compartment
Peripheral compartment
Central Compartment
Peripheral compartment

Centrally acting analgesic with moderate affinity for μ receptors and weak κ and δ activity.
Dual mechanism of action Opioid agonist effect. 5-HT and NA uptake inhibition enhancing function of spinal
inhibitory pathways.
Effective both orally and IV (100mg = 10 mg Morphine).
Uses
Effective for the treatment of chronic pain. Can be used where NSAIDS are contraindicated. Short diagnostic procedures. Post-operative shivering.
Disadvantages
Seizures have been demonstrated. High incidence of nausea and vomiting.

These drugs bind to μ-receptors where they act as
partial agonist or competitive antagonist and exhibit partial
agonist actions at other receptors.
Produce analgesia with limited ventilatorydepression and low potential for producing physical dependence.
However they can attenuate the efficacy of subsequently administered opioid agonists.
Ceiling effect present.

Benzomorphan derivative.
Weak μ-receptor antagonist, but agonist of κ and δ receptor.
One of the commonly used agents, given orally and IM.
Ceilings in both analgesia and respiratory depression occur after 30 to 70 mg of pentazocine.
Low abuse liability. However can precipitate withdrawal symptoms in patients who have been administered opioids on a regular basis.
Uses: Moderately severe pain in injury, burns, trauma andorthopaedic manuevers .

Disadvantages
Depresses myocardial contractility.
Increases blood catecholamine levels thus increasing B.P, H.R, SVR,PAP, and LVEDP.
Inhibits gastric emptying and GIT transit.
High incidence of PONV.
Limited analgesia.
Partially antagonizes other opioids.
Produces psychotomimetic effects.

Agonist- antagonist opioid that resembles Pentazocine.
Compared to Pentazocine, its agonist action is 20 times greater and antagonist activity is 15- 30 times greater.
Rapidly and almost completely absorbed after I.M administration.
Respiratory depression is similar to morphine, higher doses reach a ceiling.
Less abuse and has less addictive potential than morphine or fentanyl.
Intra-operative use is limited like pentazocine.
Transnasal butorphanol is effective in relieving migraine and postoperative pain.

Side effects
Sedation, nausea and diaphoresis.
Ventilatory depression is similar to that produced by morphine.
In patients with cardiac disease, it causes significant increases in cardiac index,left ventricular end-diastolic pressure and pulmonary artery pressure.
Acute biliary spasm can occur but increases in biliarypressure are less than after equipotent doses of fentanyl or morphine.
Uses: Long lasting painful conditions – cancer
Postoperative pain
Myocardial infarction

Buprenorphine is a thebaine derivative,
Approximately 33 times more potent than morphine
Has 50 times higher affinity for µ- receptor than morphine.
Given Sublingually or parenterally but not orally – high 1st pass metabolism
The onset of action of is slow, peak effect takes 3 hours, and its duration of effect is prolonged (>10 hours).
Uses
Analgesic component in balanced anesthesia.
Excellent analgesic for relieving pain in the post operative period, cancer, renal colic.
Adjuvant for spinal and epidural analgesia. High lipid solubility limits cephalad spread and delayed depression of ventilation.

Adverse Effects: Hypotension,drowsiness, nausea, vomiting
Pulmonary oedema has been observed in some patients
In addicts – precipitates withdrawal syndrome.
Respiratory depression (fatal in neonates) and cannot be reversed by Naloxone
Nalbuphine is an agonist-antagonist opioid structurally related to oxymorphone and naloxone
Agonist potency is equal to that of morphine at the κ-receptor and antagonist potency at the µ-receptor is one-fourth as much as nalorphine.
Activation of supraspinal and spinal κ-receptors results in limited analgesia, respiratory depression and sedation.
Like other agonist-antagonist compounds, interferes with the analgesia produced by pure µ-agonists.
The onset of effect is rapid (5 to 10 minutes), and its duration is long (3 to 6 hours).
In contrast to pentazocine and butorphanol it causes no significant changes in systemic, pulmonary arterial, and pulmonary capillary wedge pressure. Hence can be used for sedation and analgesia in patients with heart disease.

Uses As an analgesic supplement for conscious
sedation or balanced anesthesia
Can be used to reverse the respiratory depression of opioid agonists in the postoperative period while maintaining analgesia.
Adverse Effects Sedation is the most common side effect.
Withdrawal symptoms less than that of morphine but greater than that of pentazocine.
Naloxone , naltrexone, nalmefene
Higher affinity for μ-receptors results in displacement of the opioid agonists from the receptor sites.

Non-selective antagonist of all types of opioid receptors
Uses
Treat opioid induced depression of ventilation in post-operative peiod and in neonates due to maternal opioidadministration.
Opioid overdose. Diagnostic- To confirm physical opioid dependence. In hypovolaemic and septic shock naloxone is useful to
promote myocardial contractility and inproves patient outcome.
Adverse Effects Antagonizes analgesic actions of opioids. Nausea/ vomiting . Increased sympathetic nervous system activity- tachycardia,
hypertension, pulmonary oedema and cardiac dysrhythmias.
Administration of naloxone to an opioid dependent parturient may produce acute withdrawal in the neonate.
Antagonizes the depressant effect of inhaled anaesthetics.

Highly effective orally and duration of action is as long as 24 hrs.
Nalmefene
6-methylene analogue of naltrexone.
Equipotent to naloxone.
Primary advantage is its longer duration of action as compared to naloxone – as long as 24 hrs.
Prophylactic administration decreases the need for anti-emetics and anti-pruritic medications in patients receiving opioid analgesics.
Analgesia
Sedation
Balanced Anaesthesia
Neuroleptanalgesia-Neuroleptanaesthesia
TIVA
High-Dose Opioid Anaesthesia for Cardiac Surgery
Monday, March 9, 2015 53DEPT OF ANAESTHESIA MKCG
MEDICAL COLLEGE
Intrathecal Infusion

1.Analgesia PCA using opioids is now the cornerstone of post-operative
analgesia.
Morphine remains a rational choice for PCA therapy. However it is slow in onset and does not allow rapid titration of effect.
Meperidine (50-100) mg produces variable degree of pain relief and not always effective in patients with severe pain.
IV opioids can produce potent and short-lasting analgesia.
Bolus Dose Infusion Rate
Fentanyl 1-3 µg/kg 0.01-0.05 µg/kg/min
Alfentanil 10-20 µg/kg 0.25-0.75 µg/kg/min
Sufentanil 0.1-0.3 µg/kg 0.0015-0.01µg/kg/min
Remifentanil - 0.05-0.25µg/kg/min

2.Sedation
Morphine (0.75 µg/kg/min) is the most frequently used IV agent in the ICU.
Remifentanil (0.15 µg/kg/min) allows more rapid emergence from sedation and earlier extubation while providing comparable level of sedation.
3.Balanced Anaesthesia
Opioid as a component of balanced anesthesia: Reduce post-operative pain and anxiety. Decrease the somatic and autonomic responses to airway
stimulation. Improve haemodynamic stability. Reduce the dose of sedative –hypnotic agents. Reduce the requirement of inhalational agents. Provide immediate post-operative analgesia.

Loading Dose
Maintenance Dose Comments
Bolus Infusion
Fentanyl 2-6 µg/kg 25-50 µg/kg 0.5-5.0 µg/kg/hr
Risk of significant depression of spontaneous ventilation
Alfentanil 25-50 µg/kg 5-10 µg/kg 0.5-2 µg/kg/min
Propofol decreases elimination clearance and distribution
Sufentanil 0.25 -2µg/kg
0.1 - 0.25 µg/kg
0.5-1.5 µg/kg/hr
Remifentanil 1 - 2 µg/kg 0.1-1.0 µg/kg/min
During emergence and post-operatively alternative analgesia should be administered or low-dose infusion continued
4.Neuroleptanalgesia- anaesthesia
Introduced by De Castro and Mundeleer. Neuroleptanalgesia is characterized by
analgesia, absence of clinically apparent motor activity. suppression of autonomic reflexes. maintenance of cardiovascular stability. amnesia in most patients.
Neuroleptanalgesia is achieved by: Major tranquilizer ( butyrophenone /phenothiazines) and Potent opioid analgesic (fentanyl)
The addition of an inhaled agent, usually N2O, improves amnesia and has been called Neuroleptanaesthesia.

5.Total Intravenous Anaesthesia (TIVA)
Useful when delivery of inhalational agents are compromised or contraindicated.
Most commonly an opioid is combined with another drug more likely to provide hypnosis and amnesia.
Combination of alfentanil and propofol produces excellent TIVA.
Alfentanil: Provides analgesia, haemodynamic stability and blunting of responses to noxious stimuli.
Propofol: Provides hypnosis and amnesia and is anti-emetic.
Induction Maintenance
Alfentanil 25 to 50 µg/kg 0.5 - 1.5 µg/kg/min
Propofol 0.5 to 1.5 mg/kg 80 to 120 µg/kg/min

6.High-Dose Opioid Anesthesia for Cardiac Surgery
Introduced as a stress-free anesthetic method for cardiac surgery.
Opioids can be administered as the primary or sole anesthetic.
First performed with morphine. However, fentanyl and sufentanilwere recommended later.
Advantage of providing stable haemodynamics due to
Lack of myocardial depressant effect.
Absence of histamine release (fentanyl congeners)
Supression of stress response to surgery.
Several factors have diminished the popularity
Lack of evidence substantiating any significant outcome benefit
added drug costs.
Trend toward “fast-track” approaches to cardiac patients.
Possible awareness.
Postoperative depression of ventilation.
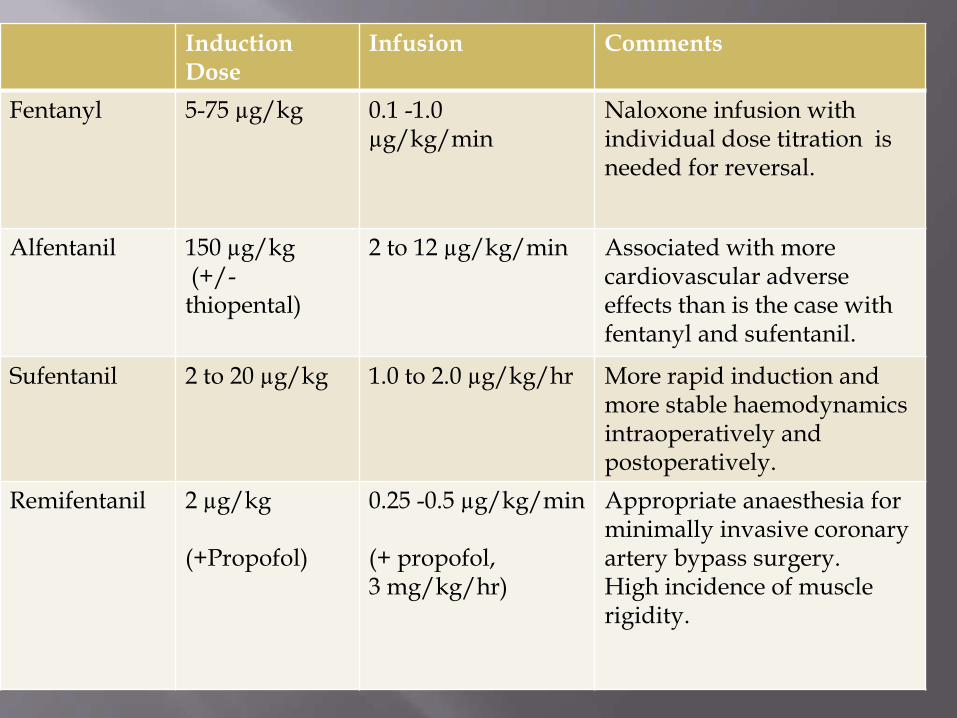
InductionDose
Infusion Comments
Fentanyl 5-75 µg/kg 0.1 -1.0µg/kg/min
Naloxone infusion with individual dose titration is needed for reversal.
Alfentanil 150 µg/kg(+/-thiopental)
2 to 12 µg/kg/min Associated with more cardiovascular adverse effects than is the case with fentanyl and sufentanil.
Sufentanil 2 to 20 µg/kg 1.0 to 2.0 µg/kg/hr More rapid induction and more stable haemodynamicsintraoperatively and postoperatively.
Remifentanil 2 µg/kg
(+Propofol)
0.25 -0.5 µg/kg/min
(+ propofol, 3 mg/kg/hr)
Appropriate anaesthesia for minimally invasive coronary artery bypass surgery.High incidence of muscle rigidity.

7.Intrathecal Infusion
Administration of opioids into the epidural or intrathecal space provides more direct access to the substantia gelatinosa of dorsal horn of the spinal cord.
Dose is substantially lowered than those required for oral or parenteral administration.
Intraspinal narcotics often are combined with local anesthetics. This permits the use of lower concentrations of both agents.
Produce dose-dependent side effects, such as itching, nausea, vomiting, respiratory depression, and urinary retention.
Use of lipophilic opioids reduces risk of delayed respiratory depression .
Preoperative1. Evaluation: Evaluation should include early recognition andhigh index of suspicion.2. Identification: Identify factors such as total opioid doserequirement and previous surgery/trauma resulting inundermedication, inadequate analgesia, or relapse episodes.3. Consultation: Meet with addiction specialists and painspecialists with regard to perioperative planning.4. Reassurance: Discuss patient concerns related to paincontrol, anxiety, and risk of relapse.5. Medication: Calculate opioid dose requirement and modesof administration; provide anxiolytics or other medications asclinically indicated.

Intraoperative1. Maintain baseline opioids (oral, transdermal, intravenous).2. Increase intraoperative and postoperative opioid dose to
compensate for tolerance.3. Provide peripheral neural or plexus blockade; consider neuraxial
analgesic techniques when clinically indicated.
4. Use nonopioids as analgesic adjuncts.
Postoperative1. Plan preoperatively for postoperative analgesia; formulate
primary strategy as well as suitable alternatives.2. Maintain baseline opioids.3. Use multimodal analgesic techniques.4. Patient-controlled analgesia: Use as primary therapy or as
supplementation for epidural or regional techniques.5. Continue neuraxial opioids: intrathecal or epidural analgesia.6. Continue continuous neural blockade.

After discharge
7. If surgery provides complete pain relief, opioids should be slowly tapered, rather than abruptly discontinued.
8. Develop a pain management plan before hospital discharge.Provide adequate doses of opioid and nonopioid analgesics.
9. Arrange for a timely outpatient pain clinic follow-up or a visit with the patient’s addiction specialist.

Transdermal Therapeutic System
Fentanyl is available in a transdermal therapeutic system.
Advantages include no first-pass drug metabolism by the liver; improved patient compliance, convenience, and comfort; and consistent analgesia.
In cancer pain, TTS fentanyl offers an alternative to oral morphine.
Use for postoperative analgesia is not recommended due a high incidence of significant respiratory depression.
TTS fentanyl produces the same adverse effects as other opioids.

Iontophoresis: Technique by which drug
passage through the skin is augumented
with an external electric current. When in need of pain medication,patient
double clicks the button – 40 mcg offentanyl delivered over 10 minutes.
Advantages
Avoids the risk of complications from needle-related injuries and infection.
Pre-programmed electronics eliminate the potential for manual programming errors and excessive dosing.
Compact size of the system enables greater patient mobility after surgery.
Eliminates hepatic first-pass
metabolism and improves patient
comfort, convenience, and compliance.
Opioids with high lipid solubility,
such as buprenorphine, fentanyl,
and methadone are readily absorbed
from sublingual mucosal tissues.
Oral transmucosal fentanyl citrate
(OTFC) is a solid dosage form of Buccal Lozenge
fentanyl that consists of fentanyl
incorporated into a sweetened lozenge on a stick.
OTFC may be ideally suited to treat breakthrough cancer pain
In children it may be used to decrease pre op anxiety and facilitate induction.
Computer controlled infusion pumps (CCIP)
Target conc. Set instead of infusion rate
CCIP calculates infusion rate from target concentration and delivers required volume
Therapeutic pl. concfor a particular opioidfor a particular effect needs to be known
Combine the advantages
of continuous infusion with
flexibility of bolus doses
according to patient’s need.
Activating a switch –
delivers bolus dose. Disposable PCA Pump with a switch
Lockout interval:
Minimum time that would have to elapse between two activations

Administration of background infusion superimposed on patient controlled boluses.
Help to maintain plasma concentration in between boluses.

Opioids are widely used in the practice of anaesthesia for pre-anaesthetic medication, systemic and spinal analgesia and supplementation of general anaesthetic agents.
A proper understanding of the pharmacokinetic and pharmacodynamicproperties of opioids, is essential for their judicious use.
New opioid delivery systems are continually being developed. Such systems allow more flexibility in providing analgesia, both inside and outside the operating room.

















