Page 1
Accepted Manuscript
Optical Coherence Tomography-guided Bifurcation Stenting of a Coronary ArteryDissection
Nienke S. van Ditzhuijzen, Msc Jurgen Ligthart, Bsc Shengxian Tu, PhD Marc van derLinden, MD, PhD Evelyn Regar, MD, PhD
PII: S0828-282X(14)00239-6
DOI: 10.1016/j.cjca.2014.04.009
Reference: CJCA 1185
To appear in: Canadian Journal of Cardiology
Received Date: 6 February 2014
Revised Date: 1 April 2014
Accepted Date: 6 April 2014
Please cite this article as: van Ditzhuijzen NS, Ligthart J, Tu S, van der Linden M, Regar E, OpticalCoherence Tomography-guided Bifurcation Stenting of a Coronary Artery Dissection, Canadian Journalof Cardiology (2014), doi: 10.1016/j.cjca.2014.04.009.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
Page 2
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Optical Coherence Tomography-guided Bifurcation Stenting of a Coronary Artery
Dissection
Nienke S van Ditzhuijzen, Msc1,2, Jurgen Ligthart, Bsc1, Shengxian Tu, PhD3, Marc van der Linden, MD, PhD1,
Evelyn Regar, MD, PhD1
1Department of Cardiology, Thoraxcenter, 2COEUR Cardiovascular Research school, Erasmus University
Medical Center, Rotterdam, The Netherlands
3Division of Image Processing, Department of Radiology, Leiden University Medical Centre, Leiden,
Netherlands
Corresponding author
E. Regar
Department of Cardiology, Thoraxcenter, BA-585
Erasmus University Medical Center
‘s-Gravendijkwal 230, 3015 CE Rotterdam, The Netherlands
E-mail: [email protected]
Keywords: Catheter-induced coronary artery dissection, optical coherence tomography, treatment
Word count: 1158; Figures: 2; Supplemental videos: 6
Page 3
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Abstract
Periprocedural guide-wire induced coronary artery dissection is a rare but potentially serious complication of
PCI. Immediate stenting of the entry point is one of the therapeutic options but engaging the guide-wire in the
true lumen may be challenging. We report a case of a 55-year-old woman with a guide-wire induced coronary
dissection that occurred during treatment of a bifurcation lesion. Optical coherence tomography was instrumental
to distinguish true form false lumen and thereby guide correct positioning of the guide-wire to successfully treat
the lesion using a dedicated bifurcation stent.
Summary
Guide-wire induced coronary artery dissection is a rare but potentially serious complication of PCI. Engaging the
guide-wire in the true lumen may be challenging. We report a case where OCT was instrumental to distinguish
true from false lumen and thereby guide correct guide-wire positioning and reconstruct the true lumen.
Case report
A 55-year old female was referred for PCI with stable angina (CCS class III). Coronary angiography
demonstrated a stenosis at the bifurcation of the left anterior descending artery (LAD) with the second diagonal
branch (D2) (Figure 1A). After wiring the LAD and D2 (both Hi-torque pilot 50; Abbott Vascular), the
angiogram suggested a dissection at D2 (Figure 1B) and guide-wire positioning in the false lumen. Multiple
attempts to position the guide-wire in the true lumen were unsuccessful.
As an alternative to repeated angiograms using multiple projections, and to understand the spatial
relationship between the actual guide-wire position, the true lumen and the dissection flap, a single optical
coherence tomography (OCT; C7XR) of the D2 was performed (automated pullback 20mm/sec). OCT
confirmed the dissection – demonstrating that the entry point was situated very proximally to the side-branch
ostium – , the guide-wire position in the false lumen and clearly identified the true lumen (Figure 1C;
Supplemental video S1). 3D rendering helped to understand the spatial relationship between guide-wire position
and true and false lumen (Intage realia and QAngioOCT; Medis Specials) (Figures 1D+E and supplemental
video S2). Using a parallel guide-wire technique, one wire was left in the false and a second wire (Hi-torque
Page 4
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
BMW; Abbott Vascular, USA) was placed in the true lumen of the D2 (Figure 2A; Supplemental video S3).
OCT confirmed correct positioning of the second wire and clearly visualized the entry point of the dissection at
the side-branch ostium (Figure 2B+C; supplemental video S4). The entry point of the dissection was successfully
treated with a 3.0/2.5x18.0mm Nile Pax bifurcation stent (Minvasys). The final angiogram demonstrated good
clinical result with TIMI 3 flow (Figure 2D; Supplemental video S5). Six months after index procedure, routine
follow-up angiography demonstrated resolution of the coronary dissection with TIMI 3 flow (Supplemental
video S6).
Coronary dissections are rare but serious complications of the treatment of bifurcation lesions.1
Immediate stenting of the entry point is one of the therapeutic options but engaging the guide-wire in the true
lumen may be challenging since the relative low resolution of angiography only allows the reflection of luminal
dimensions. OCTprovides an unmatched high-resolution visualization of the coronary artery and could be
helpful in these complex situations.2 In our case, OCT demonstrated 1) guide-wire position in the false lumen
and allowed to correct the guide-wire position into the true lumen and 2) clearly demonstrated that the entry
point of the dissection was situated very proximally at the side-branch ostium, guiding stent selection. A
dedicated bifurcation stent was chosen that allowed full coverage of the entry point of the dissection at the carina
of the LAD and D2.
Alternatively, intravascular ultrasound (IVUS) could be used. IVUS employs a lower image resolution
than OCT (100µm vs. 10-15µm), but can image deeper into the tissue than OCT (penetration depth 4-10 mm vs.
1-2 mm), which could be helpful for the visualization of larger vessel dissections.3 Furthermore, IVUS can
image through blood, whereas OCT requires flushing during pullback acquisition that may increase
intracoronary pressure by approximately 10mmHg, possibly aggravating coronary dissections. 4 However, the
increased intracoronary pressure is well within a physiologic range and not considered a safety hazard. More
importantly, we did not see any signs of progression of the dissection in our patient.
In conclusion, in our case, the high resolution and sharp contrast of OCT offered advantages. The sharp
contrast between lumen and vessel wall proved to be crucial for clear visualization of the dissection membrane,
entry and exit point, true lumen, and false lumen. Furthermore, the fast image acquisition of OCT (automated
pullback 20 mm/sec versus 0.5-1.0mm/sec for IVUS), allowed for accurate three-dimensional reconstruction of
the complex anatomical situation that proved to be helpful for the operator to plan treatment strategy.
Page 5
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
Figure legends
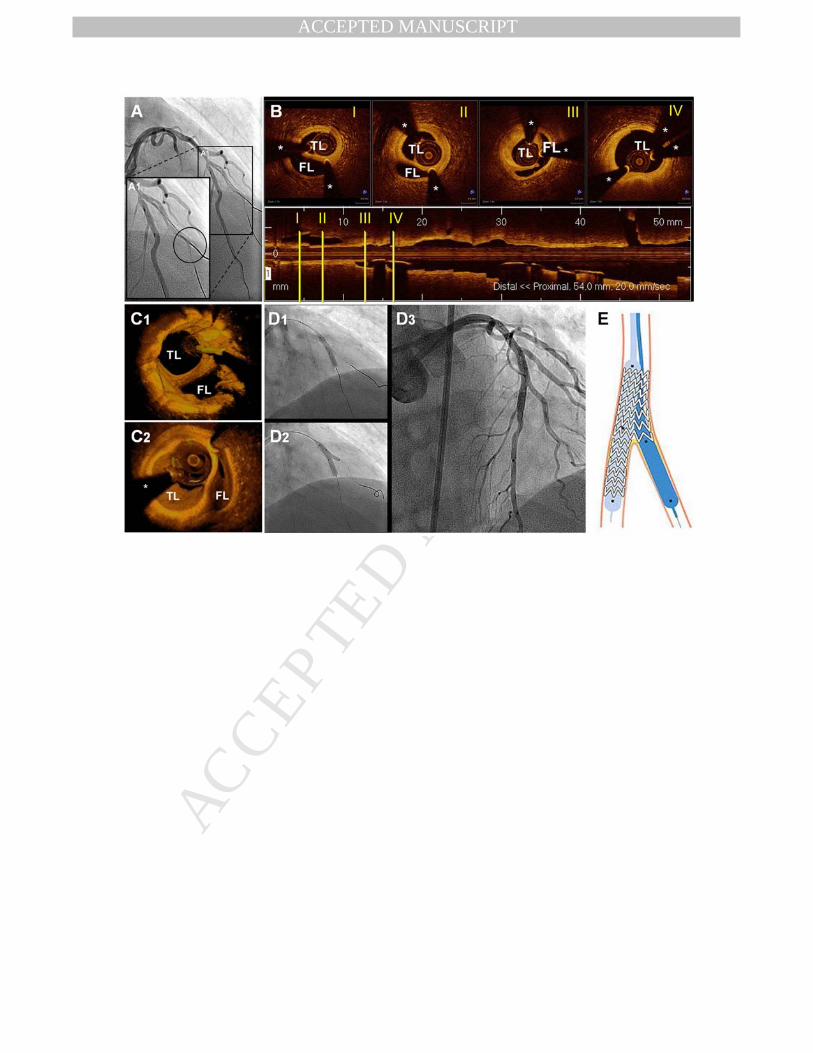
Figure 1 Pre-intervention imaging
A) Coronary angiography demonstrates a stenosis at the bifurcation of the LAD with D2. B) After wiring, the
angiogram suggested a dissection at D2. C) OCT of the D2 confirmed the dissection at the bifurcation with the
LAD and demonstrated positioning of the guide-wire in the false lumen. The red circle in the l-mode indicates
the entry point of the dissection, the red arrow indicates the LAD. D+E) 3D reconstructions clearly visualize the
true and false lumen, with a side branch in the true lumen (arrow)
Figure 2 Post-intervention results
A) Coronary angiography demonstrates one guide-wire in the LAD and two guide-wires in the D2. B+C) OCT
including 3D reconstructions confirm correct positioning of the second wire. D) Final angiography demonstrates
successful implantation of the stents and TIMI 3 flow E) Cartoon of the bifurcation stent
Page 6
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
REFERENCES
1. Carrie D, Karouny E, Chouairi S, Puel J. "T"-shaped stent placement: A technique for the treatment of
dissected bifurcation lesions. Catheterization and cardiovascular diagnosis. 1996;37:311-313
2. Prati F, Regar E, Mintz GS, et al. Expert review document on methodology, terminology, and clinical
applications of optical coherence tomography: Physical principles, methodology of image acquisition,
and clinical application for assessment of coronary arteries and atherosclerosis. European heart journal.
2010;31:401-415
3. Mintz GS, Nissen SE, Anderson WD, et al. American college of cardiology clinical expert consensus
document on standards for acquisition, measurement and reporting of intravascular ultrasound studies
(ivus). A report of the american college of cardiology task force on clinical expert consensus
documents. Journal of the American College of Cardiology. 2001;37:1478-1492
4. Gonzalo N, Serruys PW, Garcia-Garcia HM, vet al. Quantitative ex vivo and in vivo comparison of
lumen dimensions measured by optical coherence tomography and intravascular ultrasound in human
coronary arteries. Revista espanola de cardiologia. 2009;62:615-624
Page 7
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 8
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Page 9
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Supplemental video legends
Supplemental video S1
Fourier-domain optical coherence tomography (FD-OCT) of the second diagonal branch (D2) demonstrates that
the entry point of the dissection is situated very proximally to the side-branch ostium
Supplemental video S2
Three-dimensional reconstruction of the FD-OCT pullback of the D2 clearly demonstrates that the guide-wire is
positioned in the false lumen
Supplemental video S3
The coronary angiogram demonstrates one wire in the LAD and 2 wires in the D2
Supplemental video S4
FD-OCT pullback of the D2 confirms correct positioning of the second wire in the true lumen
Supplemental video S5
The final coronary angiogram demonstrates TIMI III flow
Supplemental video S6
Routine 6 month follow-up coronary angiography demonstrates resolution of the coronary artery dissection and
TIMI III flow






















![Bifurcation and Left Main Stenting[1]](https://static.documents.pub/doc/80x56/5466ba34b4af9ffd748b4bcf/bifurcation-and-left-main-stenting1.jpg)

