Optimal Birth Spacing: Improving Maternal and Child Health Outcomes Dr. Taroub Harb Faramand-CATALYST Consortium Dr. Issakha Diallo, Advance Africa State-of-the-Art Family Planning & Reproductive Health Services MAQ Mini-University USAID-Washington DC May 12, 2003
Transcript
Optimal Birth Spacing:Improving Maternal and Child Health
Outcomes
Dr. Taroub Harb Faramand-CATALYST Consortium
Dr. Issakha Diallo, Advance Africa
State-of-the-Art
Family Planning &
Reproductive
Health Services
MAQ Mini-UniversityUSAID-Washington DC
May 12, 2003
Session Objectives
1. Present the latest quantitative and qualitative research findings on the impact of Optimal Birth Spacing on maternal and child health outcomes
2. Present CATALYST’s approach to integrating birth spacing messages into health and non-health programs
3. Share with the participants Advance Africa’s approach of using health benefits of Optimal Birth Spacing to revitalizing FP programs in Sub-Saharan Africa
4. Discuss and share experiences on program integration of Optimal Birth Spacing messages
Source: Conde-Agudelo, 2nd Champions Meeting on Birth Spacing, CATALYST Consortium, Washington DC, May 2, 2002
The Potential Impact of OBS
If Women Spaced Births for 3 Years…
INDIA Infant mortality
would drop 29% Under age five
mortality would drop 35%
Deaths to children under age five would fall by
1,434,000 annually
EGYPT Infant mortality
would drop 35% Under age Five
mortality would drop 45%
Deaths to children under age five would fall by 109,000 annually
Fertility rate would potentially drop by 8%
Non-Health Benefits of Family Planning**
Provides economic and health benefits Can improve sexual life (satisfaction),
partner relations, and family well-being Family planning users are more likely to
take advantage of job opportunities Family planning helps women meet
practical needs and is necessary to help meet strategic need (gender equity)
** Synthesis of finding from the Women’s Studies Project, FHI 1998
Results from Focus Group Discussion on Optimal Birth SpacingOverview of the Focus Groups Conducted in 4 countries—India, Pakistan, Peru, and
Bolivia
Egypt—on-going
Close to 1000 participants in 122 focus group discussions
Audience: ▸ Spacers and non-spacers, ages 15-19, 20-30 yrs▸ Male partners, ages 15-19, 20-30 yrs▸ Health providers ▸ Mothers-in-law (India, Pakistan, Egypt)
FGD Common Findings
Reasons for Spacing
1. Economic Consideration—relief from financial burdens surfaced as a driving force for spacing births
2. The overall physical and mental well-being of the mother, new born, husband and other children living in the household was regarded as a major benefit of birth spacing
FGD Common Findings
Reasons for NOT Spacing (Barriers)1. Inaccurate information and/or misconceptions
about contraceptives
2. Gender Inequity▸ Women lack power in making decisions concerning their
reproductive choices▸ Husbands having the final say in spacing of children
3. Mothers-in-laws influence (India and Pakistan) ▸ Exert strong influence in the couple’s reproductive
behavior
Possible Programmatic Approaches Based on FGD Findings
Address Barriers and Strengthen Current Support for OBS
Improve family planning counseling▸ Provide credible and comprehensive information regarding
FP methods• Access to information• Dispel misconceptions
▸ Involve men in the counseling session Media Campaign
▸ Disseminate information on the benefits of Birth Spacing ▸ Solicit community support for Birth Spacing
Empowerment of couples to decide on their reproductive choices
Programmatic Response: Integration with Health Programs
RH/FP
IMCI/MCH
Neonatal Health
HIV/AIDS/Infectious
Diseases
PAC
BCC
Female Health Volunteers
Peer Educators
Community-Based
Distributors (CBDs)
Hea
lth P
rogr
ams Clinical
Programs
Non-clinical Programs
Programmatic Response: Integration with Non-Health Programs
Source: Population Reports, Volume XXX, Number 3, Summer 2002 (11)
African Birth Interval Preferences
Mothers in Sub-Saharan African countries would prefer longer birth intervals.
Few African mothers prefer birth intervals shorter than 36 months.
Preferred birth intervals are usually longer in East and Southern Africa than in West and Middle Africa.
Source: Shea Rutstein, PhD, Measure/DHS+,Macro International, Inc.
1.0
0.80.7
0.6
0.5
0.4 0.4
0.4 0.4 0.40.3 0.3
0.3 0.30.3
0.1 0.1
0.5
0.0
0.3
0.5
0.8
1.0
Decre
ase in
Nu
mb
er
of
Ch
ild
ren
Source: Shea Rutstein, PhD, Measure/DHS+,Macro International, Inc.
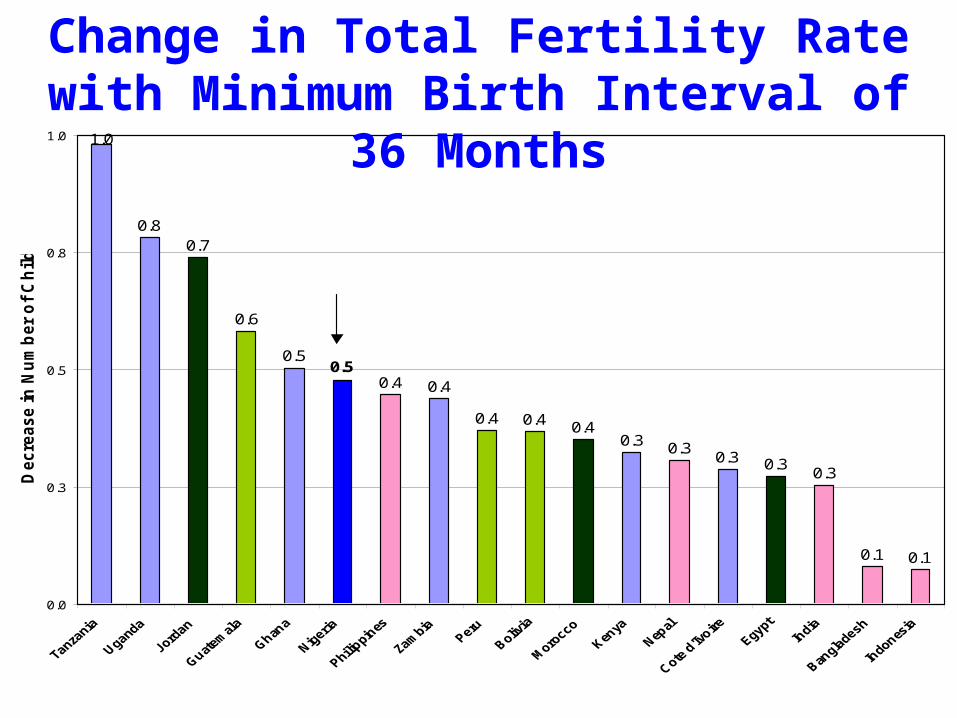
Change in Total Fertility Rate with Minimum Birth Interval of 36 Months
Analysis of DHS data from 1990 to 1997 in 27 countries has demonstrated a threshold effect in the relation between temporary method use length of birth interval.
Enabling women to realize their birth interval preferences would result in substantial decreases in both infant and child mortality and fertility.
Summary OBI research results(1)
Source: Population Reports, Volume XXX, Number 3, Summer 2002 (11)
Avoiding short birth intervals would lower both fertility and infant and child mortality by additional substantial amounts.
When children are weaned too soon, their growth suffers, they are more likely to suffer from diarrheal disease, and skins infections, and they are thus greater risk of dying
Source: Shea Rutstein, PhD, Measure/DHS+,Macro International, Inc.
Summary OBI research results(2)
Suggested Strategies to help couples space Births
Increase access to good-quality contraceptive services and full range of methods,
Encourage community campaigns that speak about needs of younger couples – and cultural norms and tradition beliefs,
Use prenatal and post natal periods as crucial times for information and counseling about birth spacing,
Discuss with mothers during well-baby and immunization visits the benefits of maintaining 3-5 years for the next child,
Support initiative that strengthen the women decision-making power in the household.
Source: Population Reports, Volume XXX, Number 3, Summer 2002 (11)