1 Optimizing Trauma Quality Improvement Harborview/ALNW EMS & Trauma Conference Gregory J Jurkovich, MD FACS Donant Professor of Trauma Surgery Vice-Chair for Clinical Affairs and Quality Department of Surgery UC Davis Health, Sacramento, CA William Stewart Halsted • “Safe Surgery” – Antisepsis – Rubber gloves – Hemostasis – Re-establish tissue planes – Tissue handling – Silk sutures • Hospital Chart Ernest Amory Codman • Ernest Codman born the year that Stanley went to find Dr. Livingston (1869) and died as Hitler was overrunning much of Europe (1940). • During his lifetime, X- rays were discovered and anesthesia became a reality, and he died just as the antibiotic era was born. Ernest Amory Codman • Graduate of Harvard Medical School • 1895 (age 25): Surgeon at the MGH • Developed X-ray imaging techniques • Wrote first English language textbook on x-ray imaging • Passion was in hospital reform Ernest Amory Codman • 5 x 8 cards on each patient • Advocated year follow-up • “End Result Program” • Advocated publicizing results • Developed the M & M conference
year that Stanley went to find Dr. Livingston (1869) and died as Hitler was overrunning much of Europe (1940).
• During his lifetime, X-rays were discovered and anesthesia became a reality, and he died just as the antibiotic era was born.
Ernest Amory Codman
• Graduate of Harvard Medical School
• 1895 (age 25): Surgeon at the MGH
• Developed X-ray imaging techniques
• Wrote first English language textbook on x-ray imaging
• Passion was in hospital reform
Ernest Amory Codman• 5 x 8 cards on each
patient• Advocated year follow-up• “End Result Program”• Advocated publicizing
results• Developed the M & M
conference
2
Codman’s “End Result” concept
• The common sense notion that every hospital should follow every patient it treats, long enough to determine whether or not the treatment has been successful, and then to inquire, “If not, why not?”with a view to preventing similar failures in the future.
• 1918: Founded ACS “Hospital Standardization Program”
• 1951: Joint Commission on Accreditation of Healthcare Organizations
Codman’s “End Result” --• 1911 Resigned his full-
time position• Opened a competing
hospital of 12 beds on Beacon Hill
• Reported a complication rate of 1 in 3
• 1915 displayed this cartoon at Suffolk District Surgical Society
• Fired from MGH
The American College of Surgeons has advocated for patient safety since its establishment in 1913.
“…all hospitals are accountable to the public for their degree of success…If the initiative is not taken by the medical profession, it will be taken by the lay public.”
• 1918 American College of Surgeons
The worst doctors will point out the errors of their
colleagues; the best will tell you about their own. Thus
you can differentiate them.
Tweeted: 03:16 AM - 12 Mar 14@medicalaxioms from Mark Reed
Fast forward→…88 years after the establishment of the ACS
• The Nature of Adverse Events in Hospitalized Patients. Results of the Harvard Medical Practice Study II– Lucian L. Leape, et al – NEJM 1991; 324– 30,000 patients; 1,131 (3.7%) disabling
medical complications, 27% due to errors– Suggested our health care system design
accounts for almost all of the problems that lead to errors, poor quality, and unsafe care.
Lucian L. Leap• Professor of Surgery Tufts
and Chief, Division of Pediatric Surgery
• Joined Harvard 1988• 1991 with TA Brennan two
NEJM articles• 1994 “Error in Medicine”• Co-author IOM report “To
Err is Human” - 1999• Father of Modern Patient
Safety movement
3
Institute of Medicine, 1999
100,000PREVENTABLEDEATHS/YEAR
MEDICAL ERRORS
Are there really 100K prentable deaths?• Prospective study of a university surgical service
(general, trauma, cardiothoracic, vascular)• Complications meticulously analyzed, including disease
related and error related.• Total complication rate of 32.1%
– Minor complications 49% avoidable– Major complications 49% avoidable
• Of the 128 deaths, 38 (30%) were felt to be avoidable• Conclusion: complication rates in surgical patients are 2-
4 times greater than those identified in the IOM report.
*Healey MA, Shackford SR, Osler TM et al. Arch Surg/Vol 137, May 2002.
Thanks to Gage Ochsner (1954-
2013)WTA 2011
• Background:– Despite advances in assessing quality and safety
surgical M&M has not changed.– Goal is to compare traditional M&M results to the data
collected using the ACS-National Surgical Quality Improvement Program(NSQIP) techniques
– How accurate is that data collected in our weekly M&M?
Hutter MH et al., J Am Coll Surg 2006;203:618-624
Morbidity and Mortality and the ACS-NSQIP
•Study Design–Retrospective study from M&M
conference at MGH. Data collected by residents and faculty over one year
–A nationally audited nurse reviewer collected the NSQIP data
Hutter MH et al., J Am Coll Surg 2006;203:618-624
Morbidity and Mortality and the ACS-NSQIP
• Results:–Mortality rates for traditional M&M were 0.9%
vs.1.9% for the NSQIP nurse reviewer
–50% of deaths were not being reported at M & M
–Complication rates in M&M were 6.4% vs. 28.9% for the NSQIP group
Hutter MH et al., J Am Coll Surg 2006;203:618-624
4
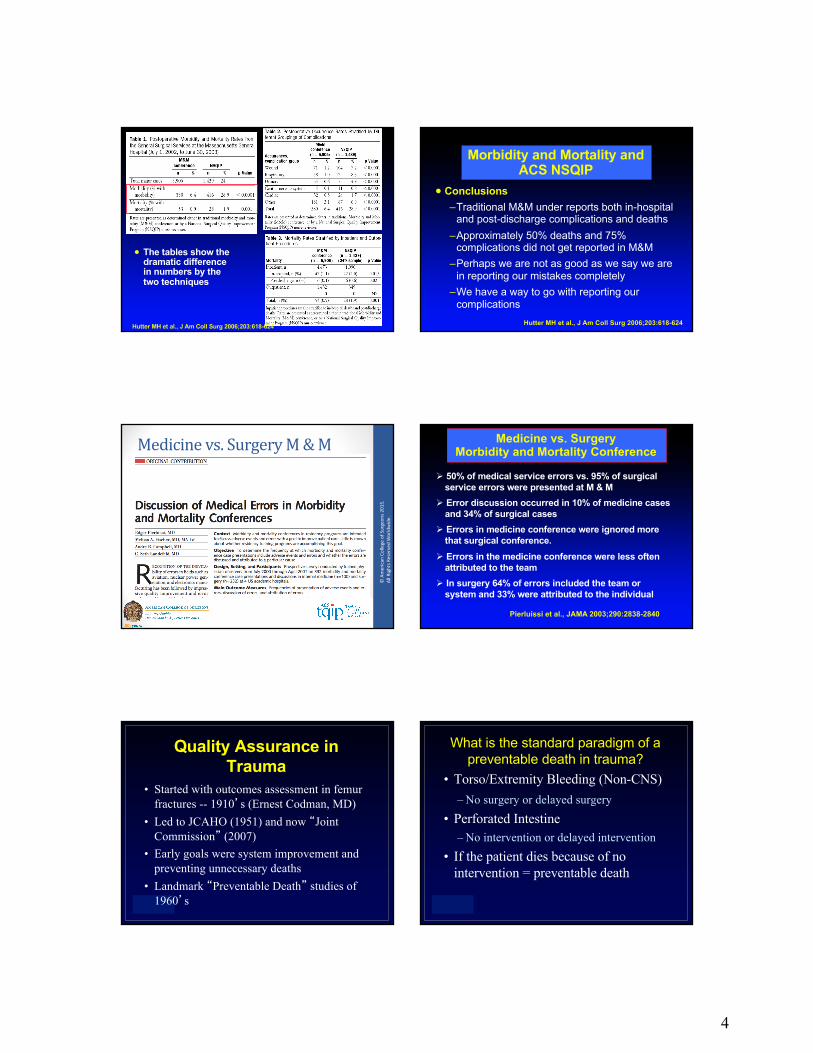
• The tables show the dramatic difference in numbers by the two techniques
Hutter MH et al., J Am Coll Surg 2006;203:618-624
Morbidity and Mortality and ACS NSQIP
• Conclusions–Traditional M&M under reports both in-hospital
and post-discharge complications and deaths–Approximately 50% deaths and 75%
complications did not get reported in M&M–Perhaps we are not as good as we say we are
in reporting our mistakes completely–We have a way to go with reporting our
complicationsHutter MH et al., J Am Coll Surg 2006;203:618-624
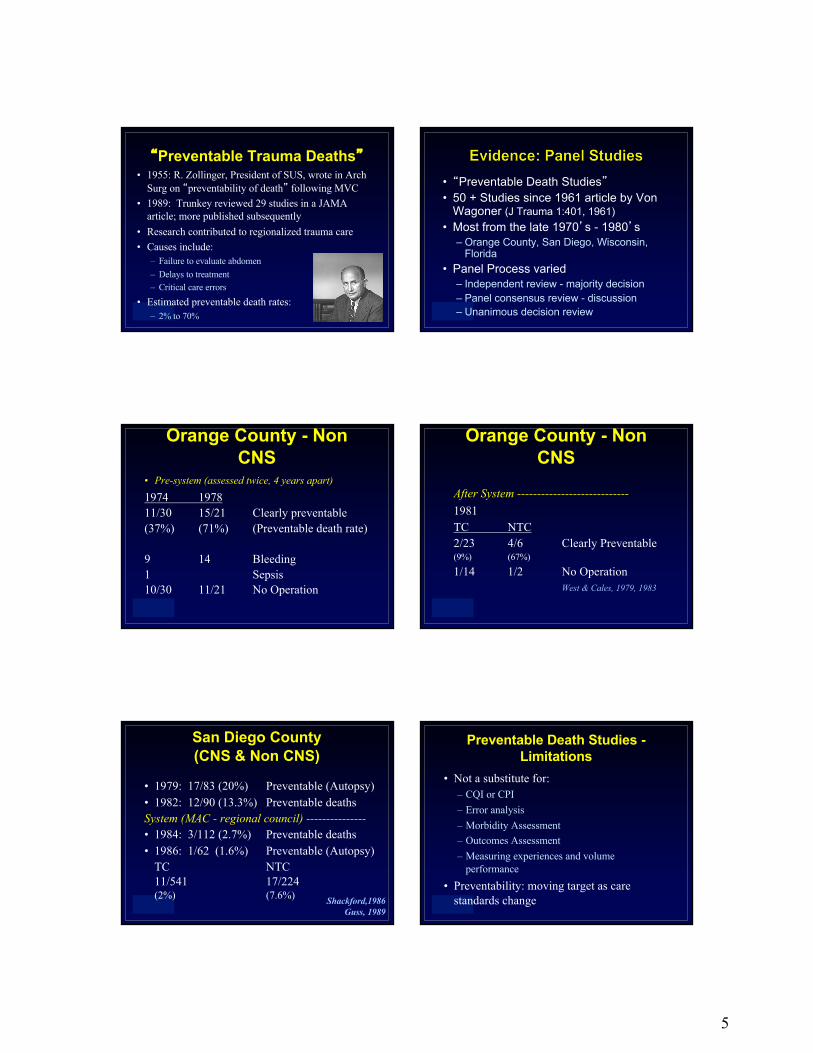
• Not a substitute for:– CQI or CPI– Error analysis– Morbidity Assessment– Outcomes Assessment– Measuring experiences and volume
performance• Preventability: moving target as care
standards change
6
Preventable death assessment struggles with:• “Potentially” preventable:
– Great variability - may assess quality not preventability
• Judging complex phase of care:– e.g.: fluid effects on respiratory function
• Attributing controversial care to preventability– e.g.: DVT prophylaxis and P.E.
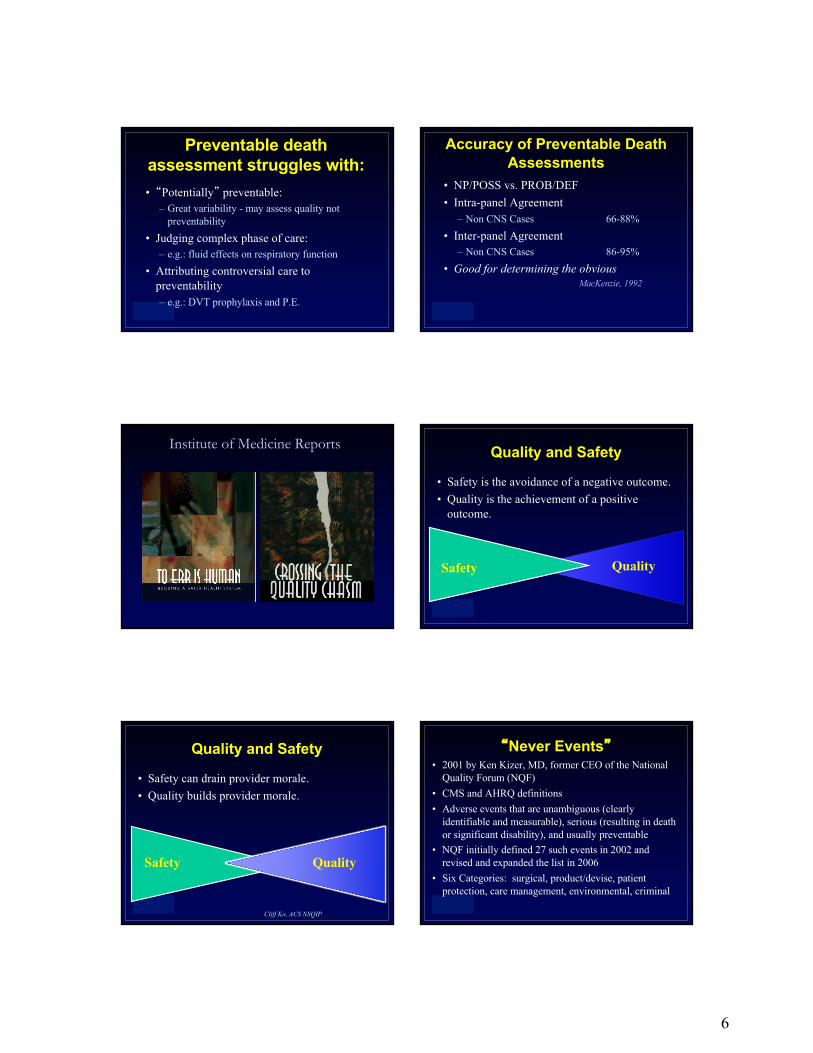
Accuracy of Preventable Death Assessments
• NP/POSS vs. PROB/DEF• Intra-panel Agreement
– Non CNS Cases 66-88%• Inter-panel Agreement
– Non CNS Cases 86-95%• Good for determining the obvious
MacKenzie, 1992
Institute of Medicine Reports Quality and Safety
• Safety is the avoidance of a negative outcome.• Quality is the achievement of a positive
outcome.
QualitySafety
Quality and Safety
• Safety can drain provider morale.• Quality builds provider morale.
Safety Quality
Cliff Ko, ACS NSQIP
“Never Events”• 2001 by Ken Kizer, MD, former CEO of the National
Quality Forum (NQF) • CMS and AHRQ definitions• Adverse events that are unambiguous (clearly
identifiable and measurable), serious (resulting in death or significant disability), and usually preventable
• NQF initially defined 27 such events in 2002 and revised and expanded the list in 2006
• Six Categories: surgical, product/devise, patient protection, care management, environmental, criminal
7
“Sentinel Events”• Joint Commission definitions• Events that result in an unanticipated death or major
permanent loss of function, not related to the natural course of the patient’s illness or underlying condition
• Fewer (12; 2012) Sentinel Events than Never Events• Child death or abduction• Suicide, Homicide, Rape, Assault• Death, paralysis, coma, loss of function - Meds• Transfusion hemolytic reaction• Prolonged fluoroscopy/radiation exposure• Wrong site surgery
Surgical Never Events
• Surgery performed on the wrong body part• Surgery performed on the wrong patient• Wrong surgical procedure performed• Unintended retention of a foreign object• Intraoperative or immediately postoperative
death in an ASA Class I patient• Artificial insemination with the wrong sperm
or donor egg
Sentinel and Never Events
www.psnet.ahrq.gov/primer.aspx?primer
Why is the error rate so high?
• Occur relatively infrequently in individual practices and institutions, but occur simultaneously at 5000 locations. Perceived by health care workers as isolated events or “outliers”
• Most errors do no harm• Most healthcare providers have difficulty in
dealing with human error
Enabling factors
• Explosion of technological advances in the 2nd
half of the 20th century• New drugs• New operations• Specialization of healthcare providers• Healthcare is a very complex system
– The greater the complexity of the system, the greater is the propensity for chaos
– In open, interacting systems, unpredictable events will happen.
Healthcare providers have difficulty in dealing with human error
• Culture of medical practice– Error free practice
• Mistakes are unacceptable• Infallible• Error = failure of character• How can there be an error without negligence
– Sense of responsibility of the patient• Responsible for any errors that occur
– Infallibility cover up mistakes, shift blame
8
Paradox• Standard of perfection, error free practice• Errors are inevitable• Examine and learn from mistakes• Denied this by concept of infallibilty and fear
– Fear of embarrassment and censure– Fear of patient reaction– Fear of litigation
Surgical M & M Conference• Unknown origin• Codman given
credit for careful analysis of outcome (fracture healing)
• Long-standing surgical legacy and heritage
• Blame, Forgive and Remember
2003
• Or: ABC : Accuse, Blame, Confess
Forgive and Remember
“When the patient of an internist dies,the natural question his colleagues ask is,
“What happend?”When the patient of a surgeon dies, his
colleagues ask, “What did you do?”By the nature of his craft and his beliefs
about it, the surgeon is more accountable than other physicians and he also has much more to account for.” HighRiskBehavior+HighRiskSituations=AdverseEvent
HighRiskBehavior+HighRiskSituations=AdverseEvent
“One of the report’s main conclusions is that the majority of medical errors do not result from individual recklessness or the actions of a particular group--this is not a “bad apple” problem. More commonly,
errors are caused by faulty systems, processes, and conditions that lead people to make mistakes or fail to prevent them.”
Institute of Medicine “To Err is Human” 1999
9
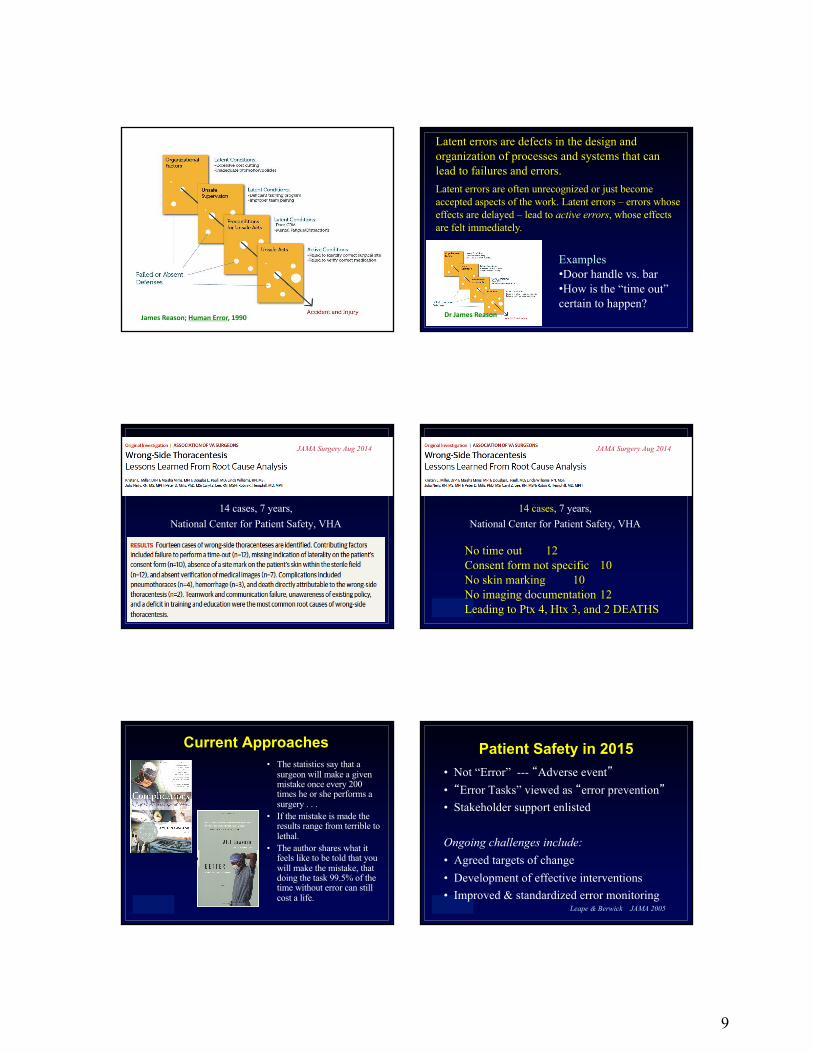
JamesReason;HumanError,1990 DrJamesReason
Latent errors are defects in the design and organization of processes and systems that can lead to failures and errors. Latent errors are often unrecognized or just become accepted aspects of the work. Latent errors – errors whose effects are delayed – lead to active errors, whose effects are felt immediately.
Examples•Door handle vs. bar•How is the “time out”certain to happen?
14 cases, 7 years, National Center for Patient Safety, VHA
JAMA Surgery Aug 2014
14 cases, 7 years, National Center for Patient Safety, VHA
JAMA Surgery Aug 2014
No time out 12Consent form not specific 10No skin marking 10No imaging documentation 12Leading to Ptx 4, Htx 3, and 2 DEATHS
Current Approaches• The statistics say that a
surgeon will make a given mistake once every 200 times he or she performs a surgery . . .
• If the mistake is made the results range from terrible to lethal.
• The author shares what it feels like to be told that you will make the mistake, that doing the task 99.5% of the time without error can still cost a life.
Patient Safety in 2015• Not “Error” --- “Adverse event”• “Error Tasks” viewed as “error prevention”• Stakeholder support enlisted
Ongoing challenges include:• Agreed targets of change• Development of effective interventions• Improved & standardized error monitoring
rather than blame assignment• Pursuing patient safety & error reduction
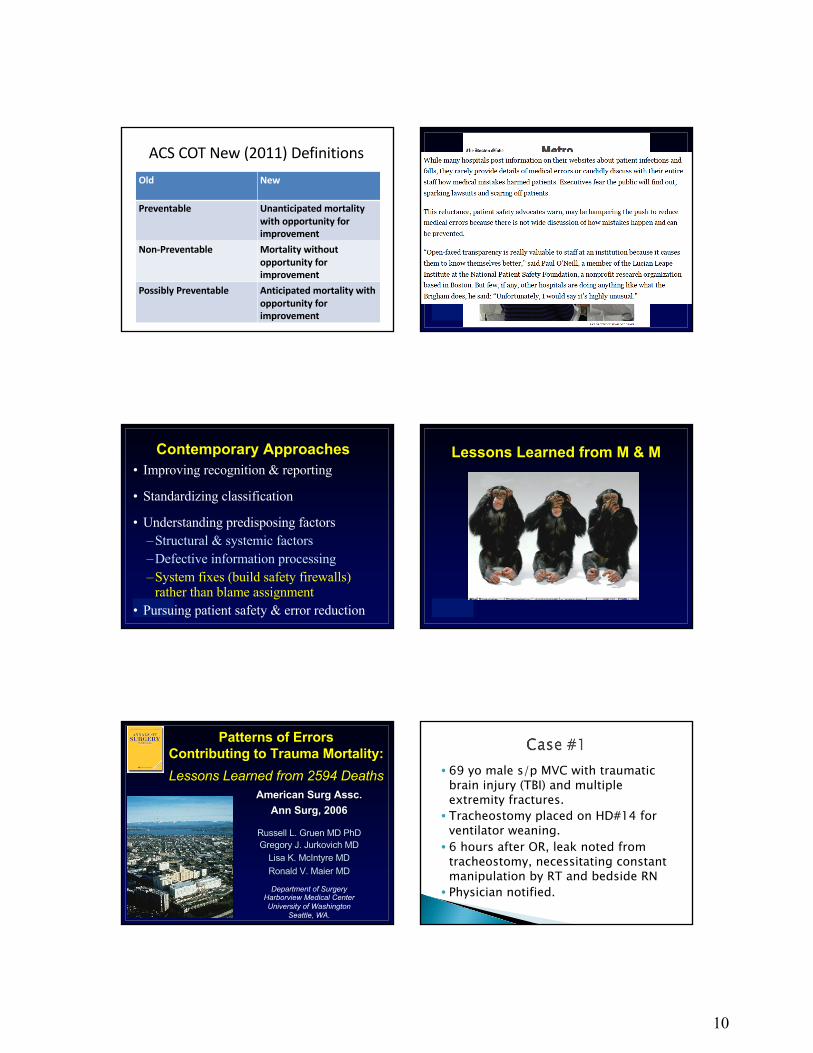
Lessons Learned from M & M
Patterns of Errors Contributing to Trauma Mortality:Lessons Learned from 2594 Deaths
American Surg Assc.Ann Surg, 2006
Russell L. Gruen MD PhDGregory J. Jurkovich MD
Lisa K. McIntyre MDRonald V. Maier MD
Department of SurgeryHarborview Medical CenterUniversity of Washington
Seattle, WA.
• 69 yo male s/p MVC with traumatic brain injury (TBI) and multiple extremity fractures. • Tracheostomy placed on HD#14 for
ventilator weaning. • 6 hours after OR, leak noted from
tracheostomy, necessitating constant manipulation by RT and bedside RN• Physician notified.
11
• See the patient; try to troubleshoot?• Call anesthesia to orally intubate and
remove tracheostomy?• If patient stable, make note to
discuss on am rounds?• Promptly notify the attending
surgeon of problem, regardless of whether the patient is stable or not?
• House physician saw patient, made note to discuss with surgeon in AM.• Just before AM rounds, patient
coughed trach out and desaturated.• Attempts made to reinsert trach in
addition to endotracheally intubating patient failed.• Patient ultimately suffered respiratory
arrest and died
• Air leaks from a fresh tracheostomy are urgent surgical problems that require attending notification.• Most require urgent revision in the
operating room.
• Identify the nurse, respiratory therapist, and house physician involved. Blame them, forgive them, hope they remember this forever.• But make a note in their record that this
occurred on their watch• Or . . . .• Write a hospital-wide policy for the
management of fresh tracheostomies. • Track problems.• Revise policy.• But . . .
• What lessons to take away from this?
• 99% of the time all is fine• What to do about that 1%?• Can surgery be perfect?• Is that a reasonable
expectation?• Can planes never crash?• Can cars never fail?• Can oil rigs never leak?• Can nuclear reactors