69
Oral Anticoagulant and Antiplatelet agents An update for the gastroenterologist Nadeem Kazi, MD April 2nd, 2016 Barcelona, Spain

Oral Anticoagulant and Antiplatelet agents An update for the gastroenterologist
Nadeem Kazi, MD April 2nd, 2016
Barcelona, Spain

Antithrombotic agents
• Anticoagulant agents – Atrial fibrillation (Afib) – Mechanical heart valves – Deep vein thrombosis (DVT) – Pulmonary embolus (PE)
• Antiplatelet agents – Acute coronary syndromes (ACS) – unstable angina, non-
ST elevation myocardial infarction (NSTEMI), ST elevation myocardial infarction (STEMI)
– Coronary (and vascular) stents

Antithrombotic agents
• Oral anticoagulant agents – Warfarin (Coumadin) – Dabigatran (Pradaxa) – Rivaroxaban (Xarelto) – Apixaban (Eliquis)
• Oral antiplatelet agents – Clopidogrel (Plavix) – Prasugrel (Effient) – Ticagrelor (Brilinta)

Venous clotting
• Underlying vascular damage absent
• Venous stasis
• Activation of coagulation cascade
• “Red thrombi” – RBCs enmeshed in fibrin
• Heparin, Lovenox, Coumadin

Venous clotting
*https://www.med.unc.edu/wolberglab/scientific-images/venous%20thrombosis.jpg

Coagulation cascade
Abraham NS, Castillo DL. Curr Opin Gastroenterol 2013.

Warfarin (Coumadin)
• Only oral anticoagulant in U.S. for over 50 years
• Slow onset, offset
• Narrow therapeutic window
• Frequent laboratory monitoring
• Multiple food and drug interactions

Warfarin (Coumadin)
• Predictable
• Widespread familiarity
• Proven track record
• Quickly and easily reversed with fresh frozen plasma (FFP) and vitamin K
Prothrombin complex concentrates (PCCs)
• Clotting factors from concentrated human plasma
• 3-factor PCCs – Factors II, IX, X – Bebulin VH
– Profilnine SD
• 4-factor PCCs – Factors II, VII, IX, X, proteins C and S, antithrombin – Kcentra
– Factor VIII inhibitor bypass activity (FEIBA NF)

Kcentra
• Nonactivated 4-factor PCC
• Urgent reversal in severe Coumadin-related bleeding
• Slightly increased risk of thrombosis
NovoSeven
• Recombinant factor VIIa
• Combines with tissue factor
• Extrinsic pathway
• Approved for treatment of hemophilia
• Used off-label for refractory GI bleeding
Dabigatran (Pradaxa)
• Direct thrombin inhibitor
• FDA-approved in 2010
• 150 mg and 75 mg tablets
• Twice daily dosing

Dabigatran (Pradaxa)
• Prevention of stroke and systemic embolism in patients with nonvalvular Afib
• Primary prevention of venous thromboembolic events (VTEs) after elective total hip or knee replacement
• Predictable pharmacokinetic profile allowing for fixed-dose regimen
• Does not require routine lab monitoring
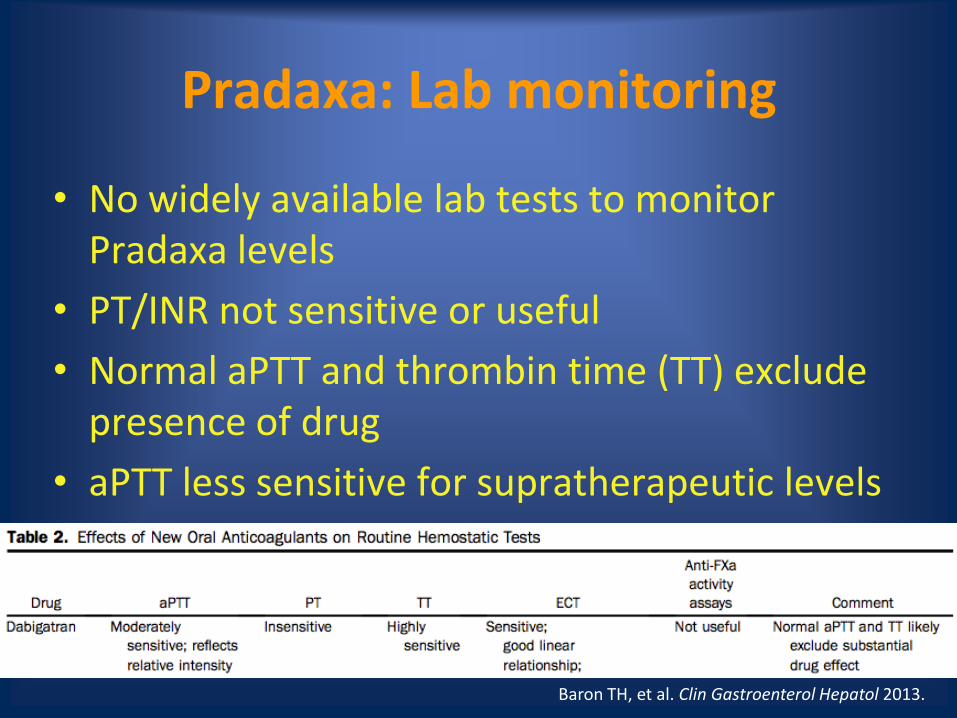
Pradaxa: Lab monitoring
• No widely available lab tests to monitor Pradaxa levels
• PT/INR not sensitive or useful
• Normal aPTT and thrombin time (TT) exclude presence of drug
• aPTT less sensitive for supratherapeutic levels
Baron TH, et al. Clin Gastroenterol Hepatol 2013.

Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY)
Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY)
• 18,113 patients with nonvalvular Afib
• Established noninferiority and superiority of Pradaxa compared to Coumadin
• Primary outcome – systemic embolism or stroke
– Coumadin: 1.69% per year
– Pradaxa 110 mg: 1.53% per year (p<0.001 for noninferiority)
– Pradaxa 150 mg: 1.11% per year (RR 0.66, p<0.001 for superiority)

Bleeding in RE-LY
• Major bleeding, any site – Coumadin: 3.36% per year
– Pradaxa 110 mg: 2.71% per year (p<0.003)
– Pradaxa 150 mg: 3.11% per year (p=0.31)
• Gastrointestinal bleeding – Coumadin: 1.02% per year
– Pradaxa 110 mg: 1.12% per year (p=0.43)
– Pradaxa 150 mg: 1.51% per year (RR 1.50, p<0.001)

GI side effects in RE-LY
• Upper GI side effects overall – 16.9% Pradaxa vs. 9.4% Coumadin (RR 1.81, p<0.001)
• GERD – 5.5% vs. 1.5% (RR 3.71, p<0.001)
• Upper abdominal pain – 4.9% vs. 2.1% (RR 2.29, p<0.001)
• Dysmotility – 6.1% vs. 4.9% (RR 1.24, p<0.001)
• Gastroduodenal injury – 3.4% vs. 2.2% (RR 1.54, p<0.001)

GI side effects in RE-LY
• Pradaxa was discontinued due to upper GI side effects more commonly – 4.0% vs. 1.7% (RR 2.34, p<0.001)
• Relative risk of drug discontinuation was greatest in GERD – 1.0% vs. 0.2% (RR 5.06, p<0.001)
• Presence of upper GI side effects increased risk of major GI bleeding – 6.8% vs. 2.3 % (p<0.001)
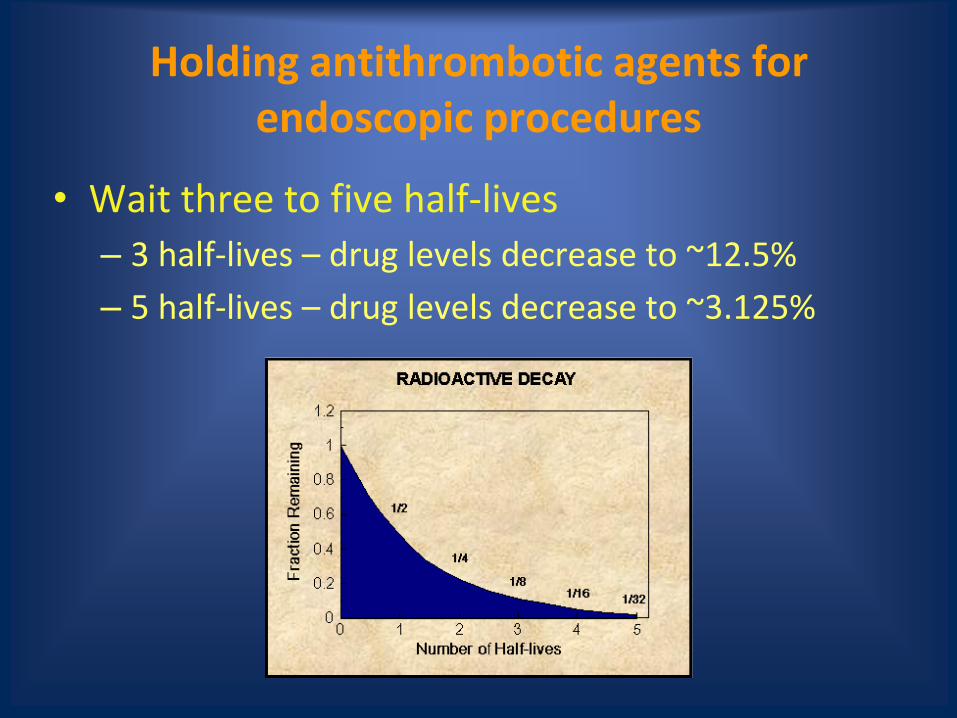
Holding antithrombotic agents for endoscopic procedures
• Wait three to five half-lives
– 3 half-lives – drug levels decrease to ~12.5%
– 5 half-lives – drug levels decrease to ~3.125%

Holding antithrombotic agents for elective endoscopic procedures
• Moderate-risk bleeding procedures (<3.3%) – Colonoscopy with polypectomy
– Diagnostic EGD, colonoscopy, (double-balloon) enteroscopy, with or without biopsy
– EUS with or without FNA
– ERCP without sphincterotomy
• High-risk bleeding procedures (up to 22%) – Endoscopic mucosal resection
– Biliary sphincterotomy
– Variceal banding
Abraham NS, Castillo DL. Curr Opin Gastroenterol 2013.

Holding Pradaxa
• Half-life is 12-17 hours
• Lengthened in patients with renal impairment
• Hold for 1-2 days before high-risk bleeding procedures in normal renal function
– CrCl 30-49 mL/min: 3 days
– CrCl < 30 mL/min: 5 days • Half-life is greater than 24 hours

Holding Pradaxa
• Recommendations vary by institution
• Some hold for 5 days in normal renal function, 7 days in those with CrCl < 50 mL/min
Van Ryn J, et al. Thromb Haemost 2010.

Rivaroxaban (Xarelto)
• Direct factor Xa inhibitor
• FDA-approved 2011
• 10 mg, 15 mg, and 20 mg tablets
• Once daily dosing

Rivaroxaban (Xarelto)
• Stroke and systemic embolism prophylaxis in patients with nonvalvular Afib
• Primary prophylaxis of VTE after hip and knee replacement surgery
• Treatment of acute DVT and PE
• Fixed dose regimen
• Avoid in patients with cirrhosis or severe renal insufficiency

Xarelto: Lab monitoring
• No widely available lab tests to monitor Xarelto levels
• PT/INR, TT, ECT are insensitive to Xarelto
• Normal PT/INR suggests no clinically relevant drug present
• aPTT is reasonable sensitive
• Anti-factor Xa levels correlate fairly well
ROCKET-AF Trial

ROCKET-AF
• 14,264 patients with nonvalvular Afib
• Demonstrated noninferiority of Xarelto compared to Coumadin
• Primary outcome – systemic embolism or stroke – Coumadin – 2.2% per year
– Xarelto – 1.7% per year (HR 0.79, p<0.001)
• Intention to treat analysis – Coumadin – 2.4% per year
– Xarelto – 2.1% per year (HR 0.88, p<0.001 for noninferiority, p=0.12 for superiority)
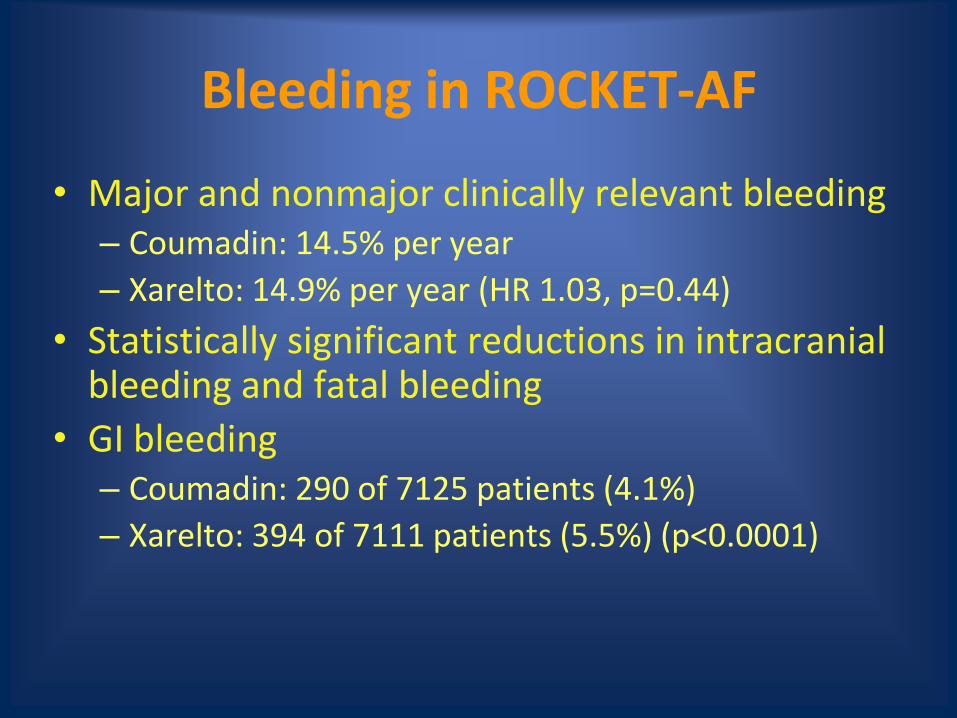
Bleeding in ROCKET-AF
• Major and nonmajor clinically relevant bleeding – Coumadin: 14.5% per year
– Xarelto: 14.9% per year (HR 1.03, p=0.44)
• Statistically significant reductions in intracranial bleeding and fatal bleeding
• GI bleeding – Coumadin: 290 of 7125 patients (4.1%)
– Xarelto: 394 of 7111 patients (5.5%) (p<0.0001)
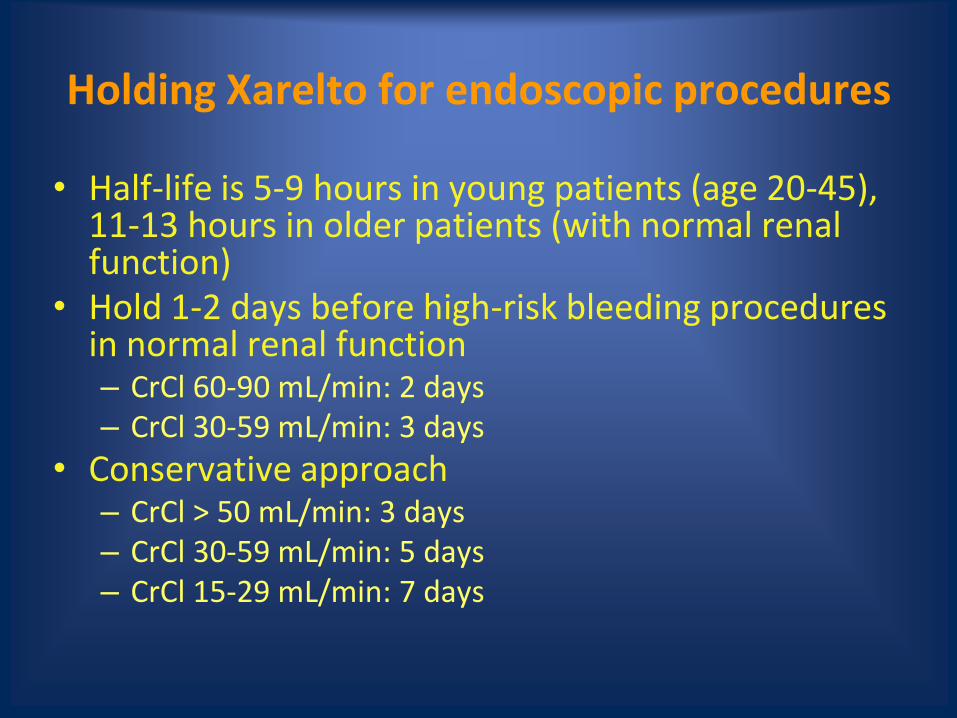
Holding Xarelto for endoscopic procedures
• Half-life is 5-9 hours in young patients (age 20-45), 11-13 hours in older patients (with normal renal function)
• Hold 1-2 days before high-risk bleeding procedures in normal renal function – CrCl 60-90 mL/min: 2 days – CrCl 30-59 mL/min: 3 days
• Conservative approach – CrCl > 50 mL/min: 3 days – CrCl 30-59 mL/min: 5 days – CrCl 15-29 mL/min: 7 days
Apixaban (Eliquis)
• Direct factor Xa inhibitor
• FDA-approved December 2012
• 5 mg and 2.5 mg tablets
• Twice daily dosing

Apixaban (Eliquis)
• For prevention of stroke and systemic embolism in patients with nonvalvular Afib
• Primary prevention of VTE in patients who have undergone total hip or knee replacement
• Use with caution in patients with hepatic or renal impairment
• Fixed dose regimen

Eliquis: Lab monitoring
• No widely available lab tests to monitor Eliquis levels
• PT/INR, TT, ECT have poor sensitivity
• aPTT is reasonably sensitive
• Anti-factor Xa levels are fairly accurate
ARISTOTLE Trial

ARISTOTLE Trial
• 18,201 patients with nonvalvular Afib
• Demonstrated superiority of Eliquis to Coumadin
• Primary outcome was ischemic/hemorrhagic stroke or systemic embolism – Coumadin: 1.60% per year
– Eliquis: 1.27% per year (HR 0.79, p<0.001 for noninferiority, p=0.01 for superiority)
Bleeding in ARISTOTLE
• Eliquis had a 27% relative risk reduction in the rate of all-cause major bleeding compared to Coumadin (p<0.001)
• Major GI bleeding not as impressive – Coumadin: 141 of 9052 (0.93% per year)
– Eliquis: 128 of 9088 (0.83% per year) (p=0.37)
• Eliquis appeared to have lower rates of major bleeding and GI bleeding compared to Pradaxa in a recent meta-analysis
Holding Eliquis for endoscopic procedures
• Half-life is 8-15 hours
• Less dependent on renal function (~25% renally excreted) – Not studied in patients with CrCl < 25 mL/min or Cr >
2.5 mg/dL
• Hold for at least 2 days prior to moderate- to high-risk bleeding endoscopic procedures
• Eliquis may pose lower risk of GI bleeding compared to Pradaxa and Xarelto

Peri-endoscopic management of the new oral anticoagulants (NOACs)
• Currently holding NOACs before procedures is the safest option
• More studies are needed to see if NOACs can be continued for diagnostic EGD/colonoscopy, colonoscopy with polypectomy < 1 cm, ERCP without sphincterotomy, EUS without FNA

Emergent ERCP and NOACs
• Sphincterotomy should be avoided if possible
• Biliary stent placement without sphincterotomy
• Balloon sphincteroplasty – Increased risk of post-ERCP pancreatitis
• Elective sphincterotomy can be performed at a later date after holding NOAC
• If sphincterotomy must be performed, endoclips or cautery may be useful to reduce bleeding, or expectant management
Drug interactions with NOACs
• All have low potential for drug interactions
• Utilize CYP3A4 and/or P-glycoprotein transporters
• Not recommended for use in pregnant or nursing mothers

Reversing NOACs
• No specific antidotes or reversal agents exist
• Drug discontinuation may be sufficient in mild bleeding – Pradaxa (80%) and Xarelto (66%) are primarily renally
excreted so give IVF
• Supportive care and endoscopic intervention when appropriate is first line – IR embolization when endoscopy unsuccessful
• FFP and Vitamin K are not effective but can be tried for severe cases

Reversing NOACs
• If dose taken < 3 hours ago, can give activated charcoal and PPI
• Charcoal hemoperfusion is under investigation
• In life-threatening cases, use of PCCs and/or recombinant factor VII can be used
– Carry increased risk of thrombosis
– Kcentra may be particularly effective for Xarelto- and Eliquis-related bleeding

Resuming NOACs
• Ideal timing after endoscopic hemostasis and high-risk bleeding procedures not known
• Weigh risk of bleeding versus risk of thromboembolic event
• Time to onset of full anticoagulation for NOACs is 1-3 hours
• Immediate/early bleeding – damage to blood vessels
• Delayed bleeding – tissue injury, vessel erosion, or delayed sloughing of hemostatic eschar

Resuming NOACs
• If risk of delayed bleeding low, consider resuming 12-24 hours after procedure
• For high-risk bleeding procedures, hold at least 48 hours after procedure
• Hold at least 72 hours after sphincterotomy – Based on a recent Coumadin study
• After EMR/ESD or other high-risk bleeding procedures, consider holding 7 days if risk of thrombosis low

Arterial clotting
• “White thrombi” – Mostly platelets, very little fibrin, RBCs
• Vessel trauma
• Atherosclerotic plaque
• Platelet adhesion, activation, aggregation
• Aspirin, clopidogrel – dual antiplatelet therapy (DAPT)

Arterial clotting
*http://www.med.unc.edu/wolberglabl/scientific-images/arterial%20thrombosis.jpg/image_view_fullscreen
Stent thrombosis
• Bare metal stents – Risk greatest in first 6 weeks
– DAPT for minimum of 1 month, ideally 1 year
• Drug eluting stents – Risk greatest in first 6 months
– DAPT for minimum 6-12 months, ideally lifelong
• Premature discontinuation before endoscopic procedures can lead to stent thrombosis and MI with mortality exceeding 50%

Clopidogrel (Plavix)
• Approved for treatment of recent ACS (UA, NSTEMI, STEMI), recent stroke, established peripheral arterial disease
• Plavix plus aspirin has been standard of care DAPT for over a decade
• Metabolized hepatically via CYP2C19 – Certain PPIs attenuate Plavix activation by inhibiting CYP2C19
• Recent meta-analysis suggested PPIs combined with Plavix did not increase incidence of major adverse cardiovascular events, while significantly reducing adverse GI events

Clopidogrel (Plavix)
• At standard dose of 75 mg/day: – 25-30% platelet inhibition in 2 days
– 50-60% platelet inhibition in 4-7 days
• With loading dose 300-600 mg: – Full antiplatelet inhibition in 2-4 hours
• 10-14% of total platelet population is restored each day when Plavix is held
• Current recommendations are to hold for at least 5 days before high-risk bleeding procedures

Limitations of Plavix
• Variable absorption and antiplatelet effects
– Polypmorphisms in genes regulating metabolic activation
• Requires loading doses to achieve early onset platelet inhibition
• Relatively delayed onset of action

Prasugrel (Effient)
• FDA-approved in 2009
• Thienopyridine irreversibly inhibits platelet P2Y12 receptor, blocking ADP-induced platelet aggregation
• Reduction of cardiovascular events and stent thrombosis in patients with ACS who are treated with percutaneous coronary intervention (PCI)

TRITON-TIMI 38

TRITON-TIMI 38
• Patients who took Effient following PCI 19% less likely to have death from cardiovascular causes, nonfatal MI, or nonfatal stroke compared to patients who took Plavix (p<0.001)
• Rates of all-cause life-threatening bleeding, nonfatal bleeding, and fatal bleeding were all increased
• Patients at increased risk of bleeding – History of stroke or transient ischemic attack (TIA) – Age ≥ 75 – Weight < 60 kg

Prasugrel (Effient)
• Metabolized via CYP3A4 and CYP2B6
– Not affected by PPIs
• Reaches peak antiplatelet effect within 30 minutes (no loading dose necessary)
• Half-life is 4 hours
• More consistent and complete inhibition of ADP-induced platelet aggregation compared to Plavix

Holding Effient
• Hold for 7 days prior to high-risk bleeding endoscopic procedures
• In coordination with cardiologist or PCP
• Could potentially continue for low- or moderate-risk bleeding procedures – currently no recommendations

Effient: Monitoring and reversal
• No laboratory tests available
• No reversal agents
– Supportive care
• Consider platelet transfusion in severe bleeding
– Not proven to be effective

Ticagrelor (Brilinta)
• FDA-approved in 2011
• Nonthienopyridine ADP-mediated P2Y12 platelet receptor inhibitor
• Reduction of thrombotic cardiovascular events in patients with acute coronary syndromes, with or without coronary stents

PLATO Trial
PLATO Trial
• Patients who took Brilinta following ACS 16% less likely to have death from vascular causes, MI, or stroke compared to patients who took Plavix (p<0.001)
• No significant difference in overall rates of major bleeding
• Increased rate of bleeding in patients who did not undergo coronary artery bypass graft (CABG) surgery (4.5% vs. 3.8%, p=0.03)
• Subsequent analysis suggested Brilinta may pose increased risk of bleeding

Ticagrelor (Brilinta)
• Metabolized via CYP3A4
– Does not interact with PPIs
• Reaches peak platelet inhibition in 2-4 hours (no loading dose necessary)
• Half-life of active metabolite is 9 hours
• Platelet activity should be near normal after holding 5 days
Holding Brilinta
• Hold for 5 days before high-risk bleeding endoscopic procedures
• In coordination with cardiologist or PCP
• Could potentially continue for low- or moderate-risk bleeding procedures – currently no recommendations

Brilinta: Monitoring and reversal
• No laboratory tests available
• No reversal agents
• Consider platelet transfusion in severe bleeding
– Not proven to be effective

Restarting Effient and Brilinta
• Weigh risk of post-procedure bleeding versus risk of thrombosis
• Coordinate with physician prescribing the medication
• Plavix typically can be restarted 48 hours after high-risk bleeding endoscopic procedures due to slower onset
• Effient and Brilinta have rapid onset, restart with caution
Conclusions
• Cardiologists and PCPs love these medications
• Stay up to date on risks and benefits of new antithrombotic agents – Risk of bleeding
– Risk of clotting
• Understanding mechanisms will be very important as new drugs are approved
• Unlikely that official guidelines will be published for several years

67
Management of NOAC Bleeding
•Mild Bleeding: Delay next dose- 24 hr
•Moderate- Severe Bleeding: IVF, Cause,Hemodialysis, Oral charcoal,PPI
• Life threatening Bleed; Consider rFVII or PCC
Van Ryan et al Thrombi Heamost 2010
68
A few words about ASA
• No difference in low dose and high dose ASA with respect to the risk of GI bleed
• ASA discontinuation during routine endoscopic procedures is not indicated. Becker et al; Am J Gastro; 2009
• ASA should be restarted three days after a GI bleed & not more than seven days
• NOACs and other anti platelet agents should be started ASAP after identifying and treating the cause of Acute GI Bleed
• H Pylori should be treated

69
Words about ASA
• Concomitant use of PPI’s with ASA
• Routine use of ASA without established CAD as primary prevention and GI bleed is not recommended
• In obscure GI bleed continue NOACs, ASA or other anti platelet agents and continue to identify the cause of anemia and bleed
Loraine Laine et al, Dec 2012, Am J of Gastro

Thank you!

















