248
ORAL BIOLOGY
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | atousa-chd |
| View: | 429 times |
| Download: | 2 times |

ORAL BIOLOGY

Sensory root : Afferents Somatic / Special
Motor root : Efferents Motor / Secretion

Sensation ( Somatosensory system )
• Special senses : smell, sight, taste, hearing and balance
• General senses : touch - position - pain- temperature
• There are two basic types of general sensation:
• touch/position pain/temperature
• touch/position information is carried by myelinated (fast-conducting) nerve fibers,
• pain/temperature information is carried by unmyelinated (slow-conducting) nerve fibers.

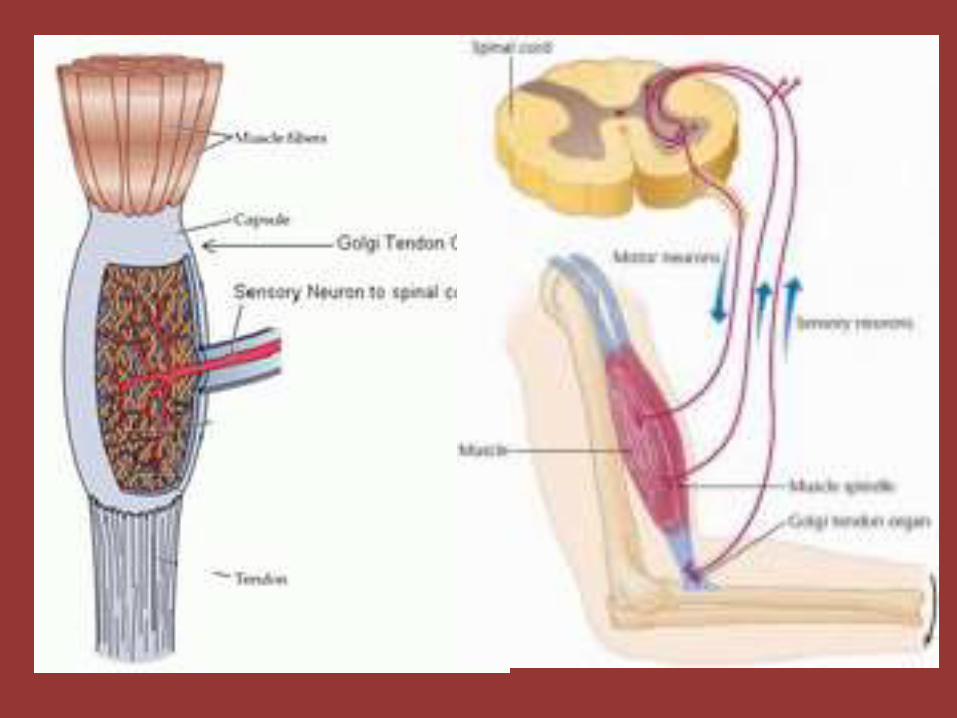
The primary sensory receptors for touch/position :Meissner’s corpuscles,Merkel's receptors,Pacinian corpuscles,Ruffini’s corpuscles,hair receptors,muscle spindle organs, Golgi tendon organs
The primitive receptors for pain/temperature: bare nerve endings.
Proprioceptors (muscle spindle organs and Golgi tendon organs) provide information about joint position and muscle movement. Much of this information is processed at an unconscious level (mainly by the cerebellum and the vestibular nuclei).

Sensory fiber types
TypeErlanger-Gasser
ClassificationDiameter Myelin
Conduction
velocity
Associated sensory
receptors
Ia Aα 13-20 µm Yes 80-120 m/sPrimary receptors of muscle
spindle
Ib Aα 13-20 µm Yes 80-120 m/s Golgi tendon organ
II Aβ 6-12 µm Yes 33-75 m/s
Secondary receptors of
muscle spindle
All cutaneous
mechanoreceptors
III Aδ 1-5 µm Thin 3-30 m/s
Free nerve endings of touch
and pressure
Nociceptors of
neospinothalamic tract
Cold thermoreceptors
IV C0.2-1.5
µmNo 0.5-2.0 m/s
Nociceptors of
paleospinothalamic tract
Warmth receptors

Sensory pathwaysThe two types of sensation in humans, touch/position and pain/temperature, are
processed by different pathways in the central nervous system. The distinction is hard-wired, and it is maintained all the way to the cerebral cortex.




• 1 Olfactory (CN I)• 2 Oculomotor (CN III)• 3 Abducens (CN VI)• 4 Facial (CN VII)• 5 Hypoglossal (CN XII)• 6 Accessory (CN XI)• 7 Vagus (CN X)• 8 Glossopharyngeal (CN IX)• 9 Vestibulocochlear (CN VIII)• 10 Trigerminal (CN V)• 11 Trochlear (CN IV)• 12 Optic chiasma• 13 Optic nerve (CN II)
Cranial Nerves

Cranial nerves
Sensory –Motor –Parasympathetic
•Trigeminal nerves(V)
•Facial nerve (VII)
•Glossopharyngeal nerve (IX)
•Vagus nerve (X)
•Hypoglossal nerve(XII)

Oral Sensation
The trigeminal nerve is the largest cranial nerve

It emerges from the side of the pons.The trigeminal nerve is a mixed nerve.
Function
•It is the great sensory nerve of the head and face.The sensory function of the trigeminal nerve is to provide the tactile, proprioceptive, and nociceptive afferent of the face and mouth.(The posterior scalp and the neck are
innervated by C2-C3, not by the trigeminal nerve.)
•The motor function activates the muscles of mastication(biting, chewing, and swallowing).

It has three major branches:
the ophthalmic nerve(V1), the maxillary nerve (V2),
the mandibular nerve (V3).

• The three branches converge on the trigeminal ganglion( semilunarganglion or gasserian ganglion) .This location can be found along the temporal bone and contains the cell bodies of incoming sensory nerve fibers.
• From the trigeminal ganglion, a single large sensory root enters the brainstem at the level of the pons.
• Adjacent to the sensory root, a smaller motor root emerges from the pons.Their cell bodies are located in the motor nucleus of the fifth nerve.
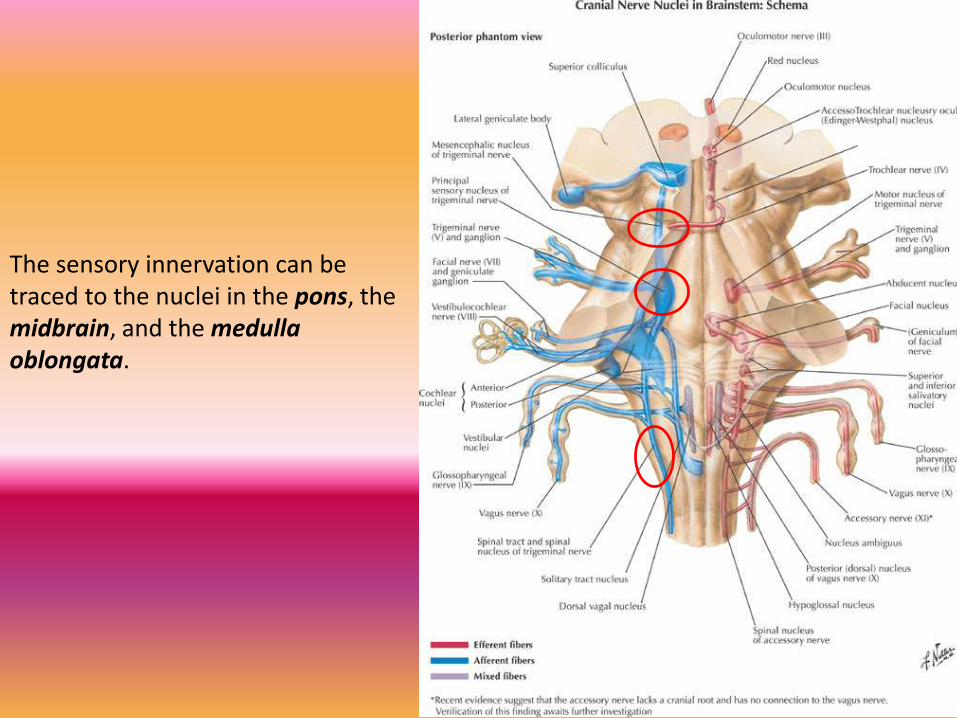
The sensory innervation can be traced to the nuclei in the pons, the midbrain, and the medulla oblongata.

The ophthalmic, maxillary and mandibular branches leave the skull through three separate foramina: the superior orbital fissure, the foramen rotundumand the foramen ovale.
•The ophthalmic nerve :the scalp and forehead, the upper eyelid,the conjunctiva and cornea of the eye, the nose(including the tip of the nose)
, the nasal mucosa, the frontal sinuses.
•The maxillary nerve :the lower eyelid and cheek, upper lip, the upper teeth and gums, the nasal mucosa, the palate and roof of the pharynx, the maxillary,ethmoid and sphenoid sinuses, and parts of the meninges.
•The mandibular nerve carries sensory information from the lower lip, the lower teeth and gums, the chin and, parts of the external ear. the mandibular is joined outside the cranium by the motor root.
•The mandibular nerve carries touch/position and pain/temperature sensation from the mouth. It does not carry taste sensation,but one of its branches, the lingual nerve carries multiple types of nerve fibers that
do not originate in the mandibular nerve.

Motor branches of the trigeminal nerve• Motor branches of the trigeminal nerve are distributed in the mandibular nerve.
These fibers originate in the motor nucleus of the fifth nerve, which is located near the main trigeminal nucleus in the pons.
• The motor branches of the trigeminal nerve control the movement of eight muscles, including the four muscles of mastication.
Muscles of mastication
• masseter
• temporalis
• medial pterygoid
• lateral pterygoid
Other
• tensor veli palatini
• mylohyoid
• anterior belly of digastric
• tensor tympani
• With the exception of tensor tympani, all of these muscles are involved in biting, chewing and swallowing. All have bilateral cortical representation.

Touch/position information from the body is carried to the thalamus by the medial lemniscus;touch/position information from the face is carried to the thalamus by the trigeminal
lemniscus.
Pain/temperature information from the body is carried to the thalamus by the spinothalamic tract;pain/temperature information from the face is carried to the thalamus by the
trigeminothalamic tract .


Pathways for touch/position sensation from the face and body merge together in the brainstem. A single touch/position sensory map of the entire body is projected onto the thalamus. Likewise, pathways for pain/temperature sensation from the face and body merge together in the brainstem. A single pain/temperature sensory map of the entire body is projected onto the thalamus.

Cerebral Cortex


The facial nerve is mixed nerve containing both sensory and motor components.
The nerve emanates from the brain stem at the ventral part of the pontomedullary junction.
facial nerve

All of the muscles of facial expression and some of the muscles of mastication are innervated by the facial nerve.
The facial nerve also carries some parasympathetic fibers to the salivary glands.
It also carries the sensation of taste.

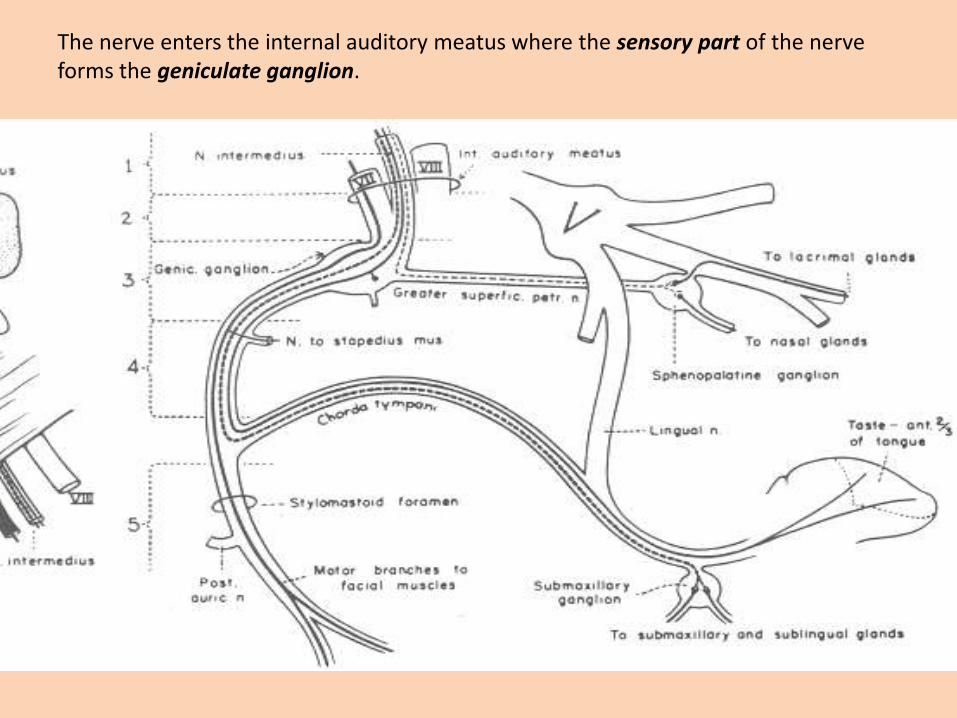
The nerve enters the internal auditory meatus where the sensory part of the nerve forms the geniculate ganglion.

In the internal auditory meatus is where the greater petrosal nerve branches
from the facial nerve. The facial nerve continues in the facial canal where the chorda tympani branches from it. The main body of the facial nerve is somatomotor and supplies the muscles of facial expression. The somatomotor component originates from neurons in the facial motor nucleuslocated in the ventral pons.

The visceral motor (parasympathetic) components of the facial nerve originate in the lacrimal or superior salivatory nucleus.The visceral motor part of the facial nerve is carried by the greater petrosal nerve.The greater petrosalnerve synapses in the pterygopalatine ganglion. The ganglion then gives of nerve branches which supply the lacrimal gland and the mucous secreting glands of the nasal and oral cavities.
The other parasympathetic part of the facial nerve travel with the chorda tympani.They travel with lingual nerve prior to synapsing in the submandibular ganglion which is located in the lateral floor of the oral cavity. The submandibular ganglion originates nerve fibers that innervate the submandibular and sublingual glands.

There are two sensory (special and general) components of facial nerve both of which originate from cell bodies in the geniculate ganglion.
The special sensory component carries information from the taste buds in the tongue and travel in the chorda tympani.
The general sensory component conducts sensation from skin in the external auditory meatus, a small area behind the ear, and external surface of the tympanic membrane. The general sensory component enters the brainstem and eventually synapses in the spinal part of trigeminal nucleus.
The special sensory or taste fibers enter the brainstem and terminate in the gustatory nucleus which is a rostral part of the nucleus of the solitary tract.

The ninth cranial nerve exits the brain stem between the olive and inferior cerebellarpeduncle.
Glossopharyngeal nerve

FunctionsThere are a number of functions of the glossopharyngeal nerve:
• It receives general sensory fibers (ventral trigeminothalamic tract) from the tonsils, the pharynx, the middle ear and the posterior 1/3 of the tongue
Spinal nucleus of the trigeminal nerve
• It receives special sensory fibers (taste)
from the posterior one-third of the tongue
Solitary nucleus
Inferior salivatory nucleus
It supplies parasympathetic fibers to
the parotid gland via the otic ganglion
Nucleus ambiguus It supplies motor fibers to stylopharyngeus muscle, the only motor component of this cranial nerve.

The glossopharyngeal nerve:The IXth nerve has no real nucleus to itself. Instead it shares nuclei with VII and X. The sensory information in IX goes to the solitary nucleus, a nucleus it shares with VII and X. All motor information, essentially the innervation of the stylopharyngeus muscle, comes from the nucleus ambiguus, also shared with X. Finally, like VII, there are some parasympathetic fibers in IX that innervate the salivary glands.

The tympanic nerve is a branch that is occurs prior to exit the skull

CN XII. Hypoglossal Nerve
The hypoglossal nerve can be found below the tongue.It is a somatomotor nerve that innervates all the intrinsic and all but one of the
extrinsic muscles of the tongue.The neuronal cell bodies that originate the hypoglossal nerve are found in the dorsal
medulla of the brain stem in the hypoglossal nucleus.

(general sensation-taste-motor-parasympathetic)Pharyngeal nerve( Superior, middle and inferior pharyngeal constrictors) Superior laryngeal nerve : Muscles of the larynx(speech).
(X)Vagus nerve

When you think vagus, you tend to think parasympathetic .However, the vagus has dozens of functions. They can be grouped into about four categories, and each category is associated with a medullary nucleus.
• Nucleus ambiguus is a motor nucleus. Cells in the nucleus ambiguus are very difficult to see (hence the name), and innervate striated muscle throughout the neck and thorax. This includes some muscles of the palate and pharynx, muscles of the larynx, and the parasympathetic innervation of the heart.
• The second is the dorsal nucleus of the vagus, which is the secretomotorparasympathetic nucleus. Secretomotor primarily means that it stimulates glands -including mucus glands of the pharynx, lungs, and gut, as well as gastric glands in the stomach. (Incidentally, it is fair-inks, not far-nicks).
• The third is the sensory nucleus of the vagus, the solitary nucleus. It receives taste information, sensation from the back of the throat, and also visceral sensation. Visceral sensation includes blood pressure receptors, blood-oxygen receptors, sensation in the larynx and trachea, and stretch receptors in the gut.
• The general sensory components of the tenth cranial nerve conduct sensation from the larynx, pharynx, skin the external ear and external auditory canal, external surface of the tympanic membrane, and the meninges of the posterior cranial fossa. The central processes from both ganglia enter the medulla and terminate in the nucleus of the spinal trigeminal tract.

nucleus ambiguus :The pharyngeal branch travels between the internal and external carotid arteries and enters the pharynx at the upper border of the middle constrictor muscle. It supplies the all the muscles of the pharynx and soft palate except the stylopharyngeas and tensor palati. These include the three constrictor muscles, levatorveli palatini, salpingopharyngeus, palatopharyngeus and palatoglossal muscles.
The superior laryngeal nerve branches distal to the pharyngeal branch and descends lateral to the pharynx. It divides into an internal and external branch. The internal branch is purely sensory and will be discussed later. The external branch travel to the cricothyroidmuscle which it supplies.
The visceromotor or parasympathetic component of the vagus nerve originates from the dorsal motor nucleus of the vagus in the dorsal medulla. These cells give rise to axons that travel in the vagus nerve. The visceromotor part of the vagus innervates ganglionicneurons which are located in or adjacent to each target organ. The target organs in the head-neck include glands of the pharynx and larynx (via the pharyngeal and internal branches).
The general sensory components of the tenth cranial nerve conduct sensation from the larynx, pharynx, skin the external ear and external auditory canal, external surface of the tympanic membrane, and the meninges of the posterior cranial fossa. Sensation from the larynx travels via the recurrent laryngeal and internal branches of the vagus to reach the inferior vagal ganglion. Sensory nerve fibers from the skin and tympanic membrane travel with auricular branch of the vagus to reach the superior vagal ganglion. The central processes from both ganglia enter the medulla and terminate in the nucleus of the spinal trigeminal tract.

Stimulation of a nociceptor, due to a chemical, thermal, or mechanical event that has the potential to damage body tissue, may cause nociceptive pain.
pain
All nociceptors are free nerve endingsthat are widely distributed throughoutthe body. They innervate the skin, bone,
muscle, most internal organs,blood vessels, and the heart.
They are generally absent from the brain substance itself, although they are in the meninges.
fast-conducting myelinated A delta fibers : fast, localized, sharp pain slow-conducting unmyelinated C fibers : slow, poorly-localized, dull pain. They are called
polymodal because of their ability to respond to a mechanical, thermal or chemical stimulus,(dental pain).
Glutamate and substance p
(>45o C or <5o C)
H+,K+,PG,polypepyides,Histamin,serotonin,bradykinin


Central pain control mechanisms
1-(Medulla) spinal cord : The gate control theory
2- Direct desending pathways from the brain
3-Opioids induced analegsia

• Gate control theory :activation of nerves which do not transmit pain signals, called nonnociceptive fibers, can interfere with signals from pain fibers, thereby inhibiting pain.
• The nonnociceptive fibers indirectly inhibit the effects of the pain fibers, 'closing a gate' to the transmission of their stimuli. In other parts of the laminae, pain fibersalso inhibit the effects of nonnociceptive fibers, 'opening the gate‘.
• An inhibitory connection may exist with Aβ and C fibers, which may form a synapse on the same projection neuron. The same neurons may also form synapses with an inhibitory interneuron that also synapses on the projection neuron, reducing the chance that the latter will fire and transmit pain stimuli to the brain .
• Thus, depending on the relative rates of firing of C and Aβ fibers, the firing of the nonnociceptive fiber may inhibit the firing of the projection neuron and the transmission of pain stimuli.
Ι

One area of the brain involved in reduction of pain sensation is the periaqueductalgray matter that surrounds the third ventricle and the cerebral aqueduct of the ventricular system. Stimulation of this area produces analgesia by activating descending pathways that directly and indirectly inhibit nociceptors in the laminae of the spinal cord.

The body possesses an additional mechanism to control pain: the release of endogenous opioids, especially at the level of the PAG,ventral medulla and spinal dorsal horn . There are neurons that release enkephalins, endorphins, and dynorphins at the PAG, and in this way modulate its ability to modulate pain perception. Other neurons can release their endogenous opioids at the source of the pain.Synapse between nociceptive afferent & projections neurons:1- presynaptic inhibition( inhibit ca2+ entry)2- postsynaptic inhibition (increase K+ conductance)

• Allodynia is a pain due to a stimulus which does not normally provoke pain .The cell types involved in nociception and mechanical sensation are the cells responsible for allodynia. injury to the spinal cord might lead to loss and re-organization of the nociceptrors, mechanoreceptors and interneurons, leading to the transmission of pain information by mechanoreceptors.
• Hyperalgesia is induced by platelet-activating factor (PAF) which comes about in an inflammation or an allergic response. This seems to occur via immune cells interacting with the peripheral nervous system and releasing pain-producing chemicals (cytokines and chemokines).
• Referred pain : pain perceived at a site adjacent to or at a distance from the site of an injury's origin. One of the best examples of this is during ischemia brought on by a myocardial infarction(heart attack) where
pain is often felt in the neck, shoulders,
and back rather than in the chest, the site
of the injury.

• Skin, joints, or muscles that have been damaged or inflamed are unusually sensitive to further stimuli. This phenomenon is called hyperalgesia.
• Hyperalgesia seems to involve processes near peripheral receptors , as well as mechanisms in the CNS(spinal dorsal horn).
• Damaged skin releases a variety of chemical substances from itself, blood cells, and nerve endings : bradykinin, prostaglandins, serotonin, substance P, K+, H+
they trigger the set of local responses that we know as inflammation. As a result, blood vessels become more leaky and cause tissue swelling (or edema) and redness . Nearby mast cells release the chemical histamine, which directly excites nociceptors. Finally, the spreading axon branches of the nociceptors themselves may release substances that sensitize nociceptive terminals and make them responsive to previously nonpainful stimuli. Such "silent" nociceptors among our small Aδ and C fibers are normally unresponsive to stimuli-even destructive ones. Only after sensitization do they become responsive to mechanical or chemical stimuli and contribute greatly to hyperalgesia.
• Aspirin suppresses the synthesis of prostaglandins.


Taste:Taste fibers, from the taste buds, are predominantly (from the front 2/3 of the tongue, anyway) carried by the facial nerve. (Keep in mind that touch and pain sensation from the tongue is V, and motor to the tongue is XII.) Taste from the back of the tongue and palate is carried by the glossopharyngeal nerve. Regardless of their origin, the taste fibers enter the solitary tract of the medulla, and synapse in the surrounding solitary nucleus.

Taste is a form of direct chemoreception and is one of the traditional five senses. In the West, experts traditionally identified four taste sensations: sweet, salty, sour, and bitter. Eastern experts traditionally identified a fifth, called umami (savory).
Taste
diagrams of the tongue showing levels of sensitivity to different tastes in different regions. In fact, taste qualities are found in all areas of the tongue. the different sorts of tastes our tongue can identify are between 4000-10000 chemicals.
Discrimination of different taste:proportion of different primary taste quality, smell,mouthmechanoreceptors(capsaicin)

Taste buds are small structures on the upper surface of the tongue, soft palate, upper esophagus and epiglottis that provide information about the taste of food being eaten.
These structures are involved in detecting the five elements of taste perception: salty, sour, bitter, sweet, and umami (or savory). Via small openings in the tongue epithelium, called taste pores, parts of the food dissolved in saliva come into contact with the taste receptors. These are located on top of the taste receptor cells that constitute the taste buds. The taste receptor cells send informationdetected by clusters of various receptorsand ion channels to the gustatory areas ofthe brain via the seventh, ninth and tenth
cranial nerves.
the human tongue has 2,000–8,000 taste buds.
The receptor cells for taste "taste buds" in humans are found on the surface of the tongue, along the soft palate, and in the epithelium of the pharynx and epiglottis. A single taste bud contains 50–100 taste cells representing all 5 taste sensations .

Types of papillae
The majority of taste buds on the tongue sit on raised protrusions of the tongue surface called papillae. There are four types of papillae present in the human tongue:
Fungiform papillae - these are slightly mushroom-shaped . These are present mostly at the apex (tip) of the tongue, as well as at the sides. Innervated by facial nerve.

• Filiform papillae - these are thin, long papillae "V"-shaped cones that don't contain taste buds but are the most numerous. These papillae are mechanical and not involved in gustation. Characterized increased keratinization.
Foliate papillae - these are ridges and grooves towards the posterior part of the tongue found on lateral margins. Innervated by facial nerve (anterior papillae) and glossopharyngeal nerve (posterior papillae).

• Circumvallate papillae - there are only about 3-14 of these papillae on most people, and they are present at the back of the oral part of the tongue. They are arranged in a circular-shaped row just in front of the sulcus terminalis of the tongue. Innervated by the glossopharyngeal nerve.

• Sweet, Bitter, and Umam work with a signal through a G protein-coupled receptor.
• Salty and Sour, which work with ion channels.
More than 90%of receptor cells respond to 2 or more of the basic taste and many respond to all. There is different sensitivity of taste cells to basic tastes.One taste cells may have all kind of transduction pathway.




• Cellular basis of taste transduction. A, Salty taste is mediated by an epithelial Na+
channel (ENaC) that is sensitive to amiloride. Sour is mediated by H+ entering through the same ENaC channel or by the effect of low pH inhibiting a K+ channel. The resulting depolarization opens voltage-gated Ca2+ channels, increasing [Ca2+]i
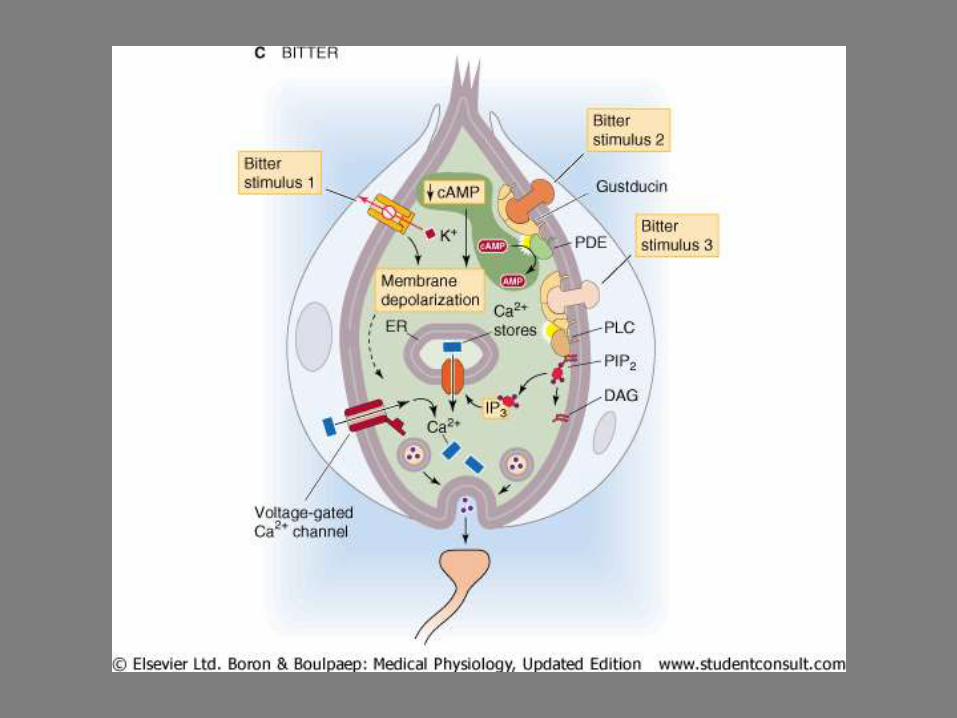
and leading to transmitter release. B, Sugar binds to a 7-transmembrane receptor that activates heterotrimeric G protein, stimulating AC, increasing cAMP, and activating PKA, which then closes a K+ channel. The resulting depolarization opens voltage-gated Ca2+ channels, increasing [Ca2+]i and leading to transmitter release. Bitter substances can act via any of three pathways. (1) A bitter compound directly inhibits K+ channels. The resulting depolarization opens voltage-gated Ca2+
channels, increasing [Ca2+]i and leading to transmitter release. (2) A ligand binds to a 7-transmembrane receptor and activates a G protein called gustducin that stimulates phosphodiesterase. The resultant decrease in [cAMP]i somehow leads to depolarization. (3) Ligand binds to a receptor that is linked to a G protein, which activates phospholipase C. The resultant increase in [IP3] releases Ca2+ from stores, raises [Ca2+]i, and leads to transmitter release. D, Glutamate binds to a glutamate-gated, nonselective cation channel and opens it. The resultant depolarization opens voltage-gated Ca2+ channels, increases [Ca2+]i, and leads to transmitter release.
• AC, adenylyl cyclase; AMP, adenosine monophosphate; cAMP, cyclic adenosine monophosphate; DAG, diacylglycerol; ER, endoplasmic reticulum; IP3, inositol 1,4,5-triphosphate; PDE, phosphodiesterase; PIP2, phosphatidyl inositol 4,5-biphosphate; PLC, phospholipase C.



Mastication
Mastication or chewing is the process by which food is crushed and ground by teeth. It is the first step of digestion and it increases the surface area of foods to allow more efficient break down by enzymes. As chewing continues, the food is made softer and warmer, and the enzymes in saliva begin to break down carbohydrates in the food. After chewing, the food (bolus) is swallowed. It enters the esophagus and continues on to the stomach, where the next step of digestion occurs.

The chewing cycleMastication is a repetitive sequence of jaw opening and closing with a profile in the vertical plane called the chewing cycle. Mastication consists of a number of chewing cycles. Opening phase: the mouth is opened and the mandible is depressed Closing phase: the mandible is raised towards the maxillaOcclusal or intercuspal phase: the mandible is stationary and the teeth from both upper and lower arches approximate

Mastication motor program
• Mastication is primarily an unconscious act, but can be mediated by higher conscious input. The motor program for mastication is a hypothesized central nervous system function by which the complex patterns governing mastication are created and controlled.
• The presence of food in the mouth causes a reflex inhibition of the muscles of the lower jaw. Those muscles relax and the lower jaw drops, causing a stretch reflex which causes muscle contraction and closure of the mouth. During mastication, the tongue and, to a lesser extent, the lips and cheeks acts to keep food between the grinding surfaces of the teeth.
• It is thought that feedback from proprioceptive nerves in teeth and the temporomandibular joints govern the creation of neural pathways, which in turn determine duration and force of individual muscle activation.
• The motor program continuously adapts to changes in food type or occlusion.

• Mastication is accomplished through the activity of the four muscles of mastication:
• The masseter
• The temporalis
• The medial pterygoid
• The lateral pterygoid
Each of these primary muscles of mastication is paired, with each side of the mandible possessing one of the four.

The muscles of mastication are all innervated by the trigeminal nerve, they are innervated by the mandibular branch or V3 and to lesser extend by fascial nerve.
the mandible is connected to the temporal bone of the skull via the temporomandibularjoint, an extremely complex joint which permits movement in all planes. The muscles of mastication originate on the skull and insert into the mandible, thereby allowing for jaw movements during contraction.
The mandible is the only bone that moves during mastication and other activities, such as talking.While these four muscles are the primary participants in mastication, other muscles are usually if not always helping the process, such as those of the tongue and the cheeks.

• Mammalian mastication results from the interaction of an intrinsic rhythmical neural pattern and sensory feedback generated by the interaction of the effecter system (muscles, bones, joints, teeth, soft tissues) with food.
• The main variables that explain variation in the pattern of human mastication are the subjects themselves, their age, the type of food being eaten, and time during a sequence of movements.
• The intrinsic pattern of mastication is generated by a central pattern generator (CPG) located in the pons and medulla. The output of the CPG is modified by inputs that descend from higher centers of the brain and by feedback from sensory receptors.
• Intraoral touch receptors, muscle spindles in the jaw-closing muscles, and specialized mechanoreceptors in the periodontal ligament have especially powerful effects on movement parameters.

• The CPG receives inputs from higher centers of the brain, especially from the inferio-lateral region of the sensorimotor cortex and from sensory receptors. Mechanoreceptors in the lips and oral mucosa, in muscles, and in the periodontal ligaments around the roots of the teeth have particularly powerful effects on movement parameters. The central pattern generator includes a core group of neurons with intrinsic bursting properties, as well as a variety of other neurons that receive inputs from oral and muscle spindle afferents. Reorganization of subpopulations of neurons within the CPG underlies changes in movement pattern.
• In addition to controlling motoneurons supplying the jaw, tongue, and facial muscles, the CPG also modulates reflex circuits. It is proposed that these brainstem circuits also participate in the control of human speech.

swallowing is a complex neuromuscular activity consisting essentially of three phases:oral, pharyngeal and esophageal phase.
Each phase is controlled by a different neurological mechanism.
•The oral phase, a bolus of food is pressed backward into the pharynx by the tongue, which is entirely voluntary, is mainly controlled by the medial temporal lobes and limbic system of the cerebral cortex with contributions from the motor cortex and other cortical areas.

– The pharyngeal swallow is started by the oral phase and subsequently is co-ordinated by the swallowing centre in the medulla oblongata and pons. The reflex is initiated by touch receptors in the pharynx. which basically involve shunting the bolus into the esophagus while at the same time closing alternative routes of escape.
– The soft palate and uvula fold upward and cover the nasopharynx to prevent the passage of food up and into the nasal cavity.
– The lumen of the larynx is squeezed shut and the epiglottis swings backward to cover the larynx. The larynx is also pulled forward and down making the opening to the esophagus larger.

• Swallowing is a complex mechanism using both
skeletal muscle (tongue) and smooth muscles of thepharynx and esophagus. The ANS coordinates thisprocess in the pharyngeal and esophageal phases.
•The upper esophageal sphincter relaxes to let food pass, after which various striated constrictor muscles of the pharynx as well as peristalsis and relaxation of the lower esophageal sphincter sequentially push the bolus of food through the esophagus into the stomach.The esophageal phase occurs involuntarily in the esophagus.The esophageal sphincter, normally closed,opens to allow food to pass when the larynx rises during
swallowing. When food reaches the lower end of the esophagus, the cardia sphincter opensto allow the food to enter the stomach.


Mucosal Membrane
Its role1- Protection•Mecanical•Microorganisms
2- Sensation
3- Secretion
Structure1- Epitelium2- Lamina Propia

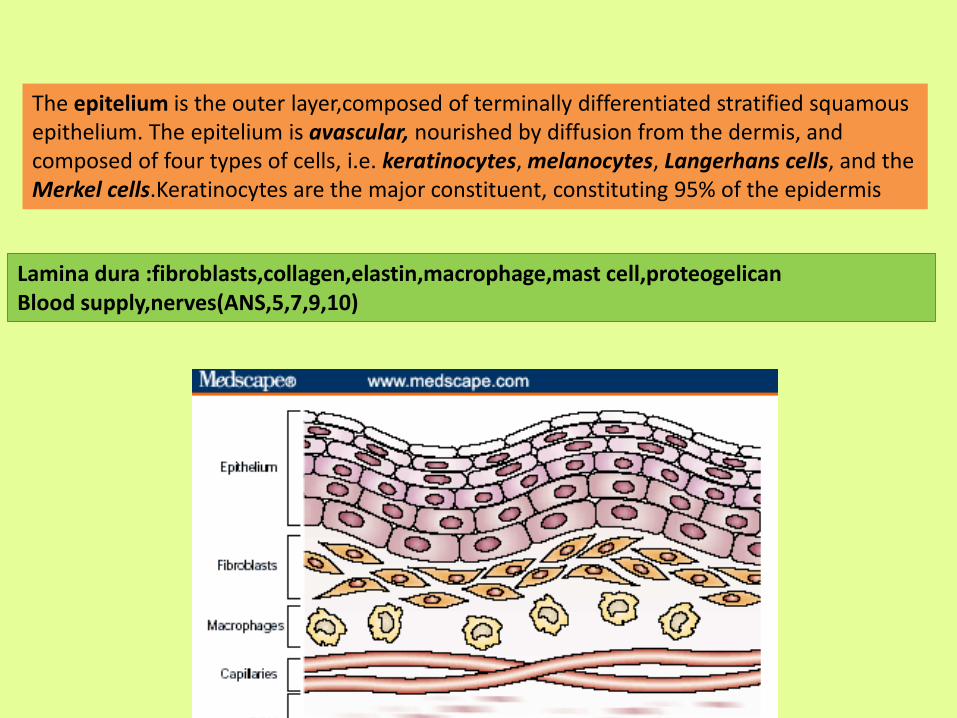
The epitelium is the outer layer,composed of terminally differentiated stratified squamousepithelium. The epitelium is avascular, nourished by diffusion from the dermis, and composed of four types of cells, i.e. keratinocytes, melanocytes, Langerhans cells, and the Merkel cells.Keratinocytes are the major constituent, constituting 95% of the epidermis
Lamina dura :fibroblasts,collagen,elastin,macrophage,mast cell,proteogelicanBlood supply,nerves(ANS,5,7,9,10)

Oral mucosa
The oral mucosa is the mucous membrane epithelium of the mouth. It can be
divided into three categories:
•Masticatory mucosa - keratinized stratified squamous epithelium, found on the
dorsum of the tongue, hard palate and attached gingiva.
•Lining mucosa - non-keratinized stratified squamous epithelium, found almost
everywhere else in the oral cavity.
•Specialized mucosa - specifically in the regions of the taste buds on the
dorsum of the tongue.

A stratified squamous epithelium consists of squamous (flattened) epithelial cellsarranged in layers upon a basement membrane. Only one layer is in contact with the basement membrane; the other layers adhere to one another to maintain structural integrity. Although this epithelium is referred to as squamous, many cells within the layers may not be flattened; this is due to the convention of naming epithelia according to the cell type at the surface.This type of epithelium is well suited to areas in the body subject to constant abrasion, as the layers can be sequentially sloughed off and replaced before the basement membrane is exposed.Stratified squamous epithelium is further classified by the presence or absence of keratinat the apical surface. Non-keratinized surfaces must be kept moist by bodily secretions to prevent them drying out and dying, whereas keratinized surfaces are kept hydrated and protected by keratin.Non-keratinized stratified squamous epithelium: cornea (see also corneal epithelium), oral cavity, esophagus, rectum, vagina, and the internal portion of the lipsKeratinized stratified squamous epithelium: skin, tongue (partially keratinized), and the external portion of the lips
Keratinization is the process of making the top layer(s) of a stratified squamous sheet hardened and dead. It's an adaptation to wear and tear found on abraded surfaces. Not all stratified squamous epithelial sheets are keratinized, but most are. This example is from the footpad of a dog.


The gingiva or gums, consists of the mucosal tissue that lies over the alveolar bone.
Gingiva are part of the soft tissue lining of the mouth. They surround the teeth and provide a seal around them. Compared with the soft tissue linings of the lips and cheeks, most of the gingiva are tightly bound to the underlying bone and are designed to resist the friction of food passing over them.
The alveolar process is the thickened ridge of bone that contains the tooth sockets on bones that bear teeth. It is also referred to as the alveolar bone. In humans, the tooth-bearing bones are the maxilla and the mandible. The mineral content of alveolar bone is mostly hydroxyapatite, which is also found in enamel as the main inorganic substance.On the maxilla, the alveolar process is a ridge on the inferior surface, and on the mandible it is a ridge on the superior surface. It makes up the thickest part of the maxilla.
Gingiva

•Free gingiva•Attached gingiva•Interdental gingiva
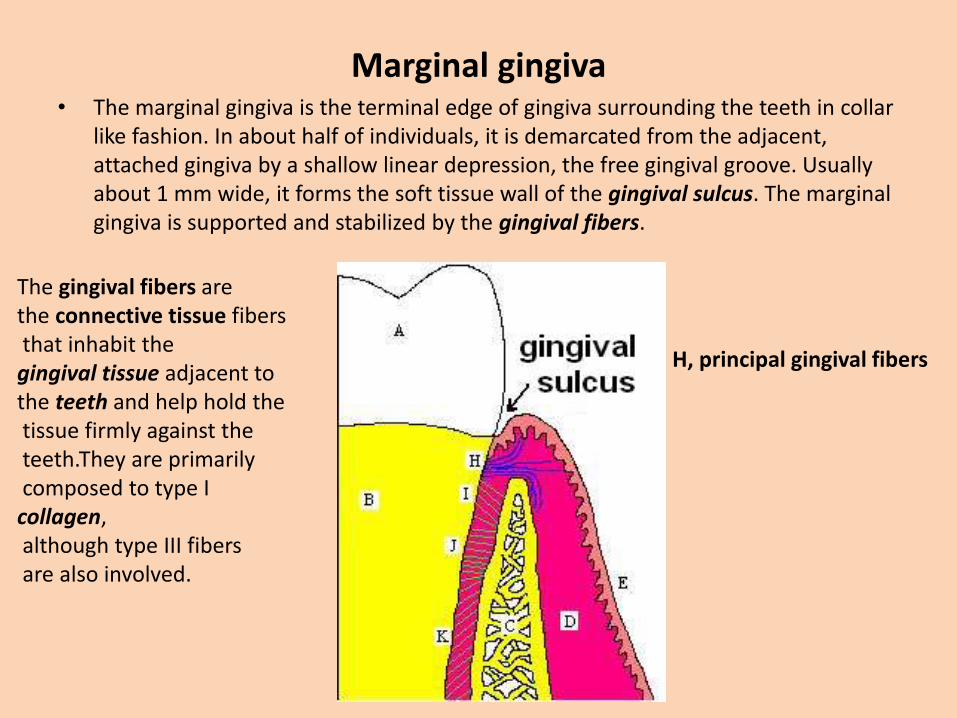
Marginal gingiva• The marginal gingiva is the terminal edge of gingiva surrounding the teeth in collar
like fashion. In about half of individuals, it is demarcated from the adjacent, attached gingiva by a shallow linear depression, the free gingival groove. Usually about 1 mm wide, it forms the soft tissue wall of the gingival sulcus. The marginal gingiva is supported and stabilized by the gingival fibers.
H, principal gingival fibers
The gingival fibers are the connective tissue fibersthat inhabit the
gingival tissue adjacent to the teeth and help hold thetissue firmly against theteeth.They are primarilycomposed to type I
collagen,although type III fibersare also involved.

Attached gingiva• The attached gingiva is continuous with the marginal gingiva. It is firm, resilient,
and tightly bound to the underlying periosteum of alveolar bone. The facial aspect of the attached gingiva extends to the relatively loose and movable alveolar mucosa, from which it is demarcated by the mucogingival junction. Attached gingiva may present with surface stippling.

Interdental gingiva• The interdental gingiva occupies the gingival embrasure, which is the interproximal
space beneath the area of tooth contact. The interdental gingiva can be pyramidal or have a col shape.

A, crown of the tooth covered by enamel. B, root of the tooth covered by cementum. C, alveolar bone.D, subepithelial connective tissue. E, oral
epithelium. F, free gingival margin. H, principal gingival fibers. I, alveolar crest fibers of the PDL. J, horizontal fibers of the PDL. K, oblique fibers of the PDL.
The periodontal ligament : PDL is a group of specialized connective tissue fibers that essentially attach a tooth to the alveolar bone within which it sits. These fibers help the tooth withstand the naturally substantial compressive forces which occur during chewing and remain embedded in the bone.Another function of the PDL is to serve as a source of proprioception, or sensory innervation, so that the brain can detect the forces being placed on the teeth and react accordingly. To achieve this end, there are pressure sensitive receptors within the PDL which allow the brain to discern the amount of force being placed on a tooth during chewing, for example. This is important because the exposed surface of the tooth, called enamel, has no such sensory receptors itself.



The salivary glands
The salivary glands in mammals are exocrine glands, glands with ducts, that produce saliva. Salivary glands produce the saliva used to moisten your mouth, initiate digestion, and help protect your teeth(enamel) from decay.
Most animals have three major pairs of salivary glands that differ in the type of secretion they produce:parotid glands produce a serous, watery secretion submaxillary (mandibular) glands produce a mixed serous and mucous secretion sublingual glands secrete a saliva that is predominantly mucous in character

The glands are enclosed in a capsule of connective tissue and internally divided into lobules. Blood vessels and nerves enter the glands at the hilum and gradually branch out into the lobules.
In the duct system, the lumens formed by intercalated ducts, which in turn join to form striated ducts. These drain into ducts situated between the lobes of the gland (called interlobar ducts or secretory ducts).
The basic secretory units of salivary glands are clusters of cells called an acini. These cells secrete a fluid that contains water, electrolytes, mucus and enzymes
(amylase that breaks down starch into glucose)all of which flow out of the acinusinto collecting ducts.

Saliva consists of mucus and serous fluid; the serous fluid contains the enzyme amylase important for the digestion of carbohydrates. Minor salivary glands of von Ebner present on the tongue secrete the amylase. The parotid gland produces purely serous saliva. The other major salivary glands produce mixed (serous and mucus) saliva.
All of the human salivary glands terminate in the mouth, where the saliva proceeds to aid in digestion. The saliva that salivary glands release is quickly inactivated in the stomach by the acid that is present there.

• Mucus is a "slimy" material that coats many epithelial surfaces and is secreted into fluids such as saliva. It is composed chiefly of mucins and inorganic salts suspended in water.
• Mucus adheres to many epithelial surfaces, where it serves as a diffusion barrieragainst contact with noxious substances (e.g. gastric acid, smoke) and as a lubricant to minimize shear stresses; such mucus coatings are particularly prominent on the epithelia of the respiratory, gastrointestinal and genital tracts. Mucus is also an abundant and important component of saliva, giving it virtually unparalleled lubricating properties.

Functions of Saliva
•Lubrication and binding: the mucus in saliva is extremely effective in binding masticated food into a slippery bolus that slides easily through the esophagus without inflicting damage to the mucosa. Saliva also coats the oral cavity and esophagus, and food basically never directly touches the epithelial cells of those tissues.
•Solubilizes dry food: in order to be tasted, the molecules in food must be solubilized.
•Oral hygiene: The oral cavity is almost constantly flushed with saliva, which floats away food debris and keeps the mouth relatively clean. Flow of saliva diminishes considerably during sleep, allow populations of bacteria to build up in the mouth -- the result is dragon breath in the morning. Saliva also contains lysozyme, an enzyme that lyses many bacteria and prevents overgrowth of oral microbial populations.
•Initiates starch digestion: in most species, the serous acinar cells secrete an alpha-amylase which can begin to digest dietary starch into maltose.
•Provides alkaline buffering and fluid: Bicarbonate secretion along with phosphate, provides a critical buffer that neutralizes acid in oral cavity.
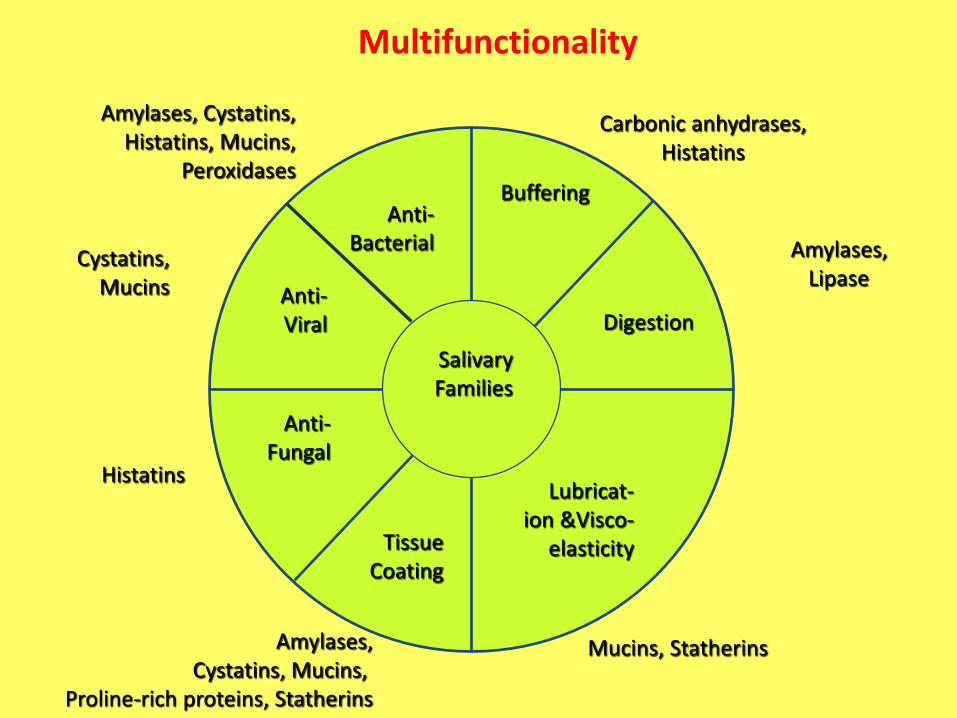
Multifunctionality
SalivaryFamilies
Anti-Bacterial
Buffering
Digestion
Lubricat-ion &Visco-
elasticityTissueCoating
Anti-Fungal
Anti-Viral
Carbonic anhydrases,Histatins
Amylases,Lipase
Mucins, StatherinsAmylases,Cystatins, Mucins,
Proline-rich proteins, Statherins
Histatins
Cystatins,Mucins
Amylases, Cystatins,Histatins, Mucins,
Peroxidases

Parotid Glands• The parotid glands are a pair of glands located in the subcutaneous tissues of the
face overlying the mandibular ramus and anterior and inferior to the external ear. The secretion produced by the parotid glands is serous in nature, and enters the oral cavity through the Stensen's duct after passing through the intercalated ducts which are prominent in the gland. Despite being the largest pair of glands, only approximately 25% of saliva is produced by the glands.Saliva contains a mixture of enzymes like salivary amylase (ptyalin), maltase(trace amounts), lysozyme (which disinfect and kills bacteria and germs which enter the mouth), salts and water. Saliva helps converting starch into maltose which is then converted patially to glucose by the maltase.

Submandibular Glands
The submandibular glands are a pair of glands located beneath lower jaws, superior to the digastric muscles. The secretion produced is a mixture of both serous and mucousand enters the oral cavity via Wharton's ducts. Approximately 70% of saliva in the oral cavity is produced by the submandibular glands, even though they are much smaller than the parotid glands.

Sublingual Gland
The sublingual glands are a pair of glands located beneath the tongue to the submandibular glands. The secretion produced is mainly mucous in nature, however it is categorized as a mixed gland. Unlike the other two major glands, the ductal system of the sublingual glands do not have striated ducts, and exit from 8-20 excretory ducts.Approximately 5% of saliva entering the oral cavity come from these glands through sublingual duct(Bartholin) .

Minor Salivary GlandsThere are over 600 minor salivary glands located throughout the oral cavity within the lamina propria of the oral mucosa. They are 1-2mm in diameter and unlike the other glands, they are not encapsulated by connective tissue only surrounded by it. The gland is usually a number of acini connected in a tiny lobule. A minor salivary gland may have a common excretory duct with another gland, or may have its own excretory duct. Their secretion is mainly mucous in nature (except for Von Ebner's glands) and have many functions such as coating the oral cavity with saliva.

Von Ebner's Glands
These glands are located around circumvallate and foliate papillae in the tongue, and they secrete lingual lipase, beginning the process of lipid hydrolysis in the mouth. These glands empty their serous secretion into the base of the moats located around the foliate and circumvallate papillae. This secretion presumably flushes material from the moat to enable the taste buds to respond rapidly to changing stimuli.

the acini and the striated ducti, participate in salivary secretion.Transport of water and electrolytes, and synthesis of enzymes, proteins, mucin and
other organic components, occur in the acini, which secrete a fluid isotonic with plasma. This fluid is then modified in the ductus system, by both reabsorption and secretion of electrolytes.
Salivary glands are effector organs in which a large amount of fluid and electrolytes is transferred from the interior of the body to the outside. The amount of fluid translocatedeach day through salivary glands approaches 750 ml, which represents approximately 20% of total plasma volume.

• Within the ducts, the composition of the secretion is altered. Much of the sodiumis actively reabsorbed, potassium is secreted, and large quantities of bicarbonateion are secreted. Small collecting ducts within salivary glands lead into larger ducts, eventually forming a single large duct that empties into the oral cavity.

Saliva is characteristically a colorless dilute fluid, Its pH is usually around 6.64
Although a variety of components is always present in saliva, the total concentration of inorganic and organic constituents is generally low when compared to serum.
Of the inorganic constituents, sodium and potassium (and perhaps calcium) are the cations of major osmotic importance in saliva; the major osmotically active anions are chloride and bicarbonate. Other organic components existing in saliva include: maltase, serum albumin, urea, uric acid, creatinine, mucine, vitamin C, several amino acids, lysozime, lactate, and some hormones such as testosterone and cortisol. Some gases (CO2, O2, and N2) are also present in saliva. Saliva contains immunoglobins such as Ig A and Ig G.

InnervationSalivary glands are innervated by the parasympathetic and sympathetic arms of the autonomic nervous system.Secretion of saliva is under control of the autonomic nervous system, which controls both the volume and type of saliva secreted.
Parasympathetic innervation to the glands is carried via cranial nerves.The parotid gland receives itsparasympathetic input from theglossopharyngeal nerve (CN IX) viaotic ganglion.
The submandibular and sublingual glands receive their parasympathetic input from the facial nerve(CN VII) via the submandibular ganglion.


Direct sympathetic innervation of the salivary glands takes place via preganglionicnerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine, which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands, increase of saliva secretion. Note that in this regard both parasympathetic and sympathetic stimuli result in an increase in salivary gland secretions.The sympathetic nervous system also affects salivary gland secretions indirectly by innervating the blood vessels that supply the glands.

Parasympathetic stimulation results in a copious flow of saliva low in organic and inorganic compounds concentrations.
Sympathetic stimulation produces a saliva low in volume. In addition, saliva evoked by action of adrenergic mediators is generally higher in organic content and its concentration of certain inorganic salts is also higher than saliva evoked by cholinergic stimulation. The higher organic content of saliva evoked by adrenergic stimulation trough the activity of adenyl-cyclase, includes elevated levels of total protein, especially the digestive enzyme alpha-amilase. The levels of inorganic compounds, i.e., Ca++, K+ and HCO3-, are usually higher with sympathetic stimulation.
The secretory cells are not the only glandular elements that respond to stimulation of the sympathetic innervation. Myoepithelial cells and blood vessels of the glands also respond to such innervation, and these responses can in turn modify the quantity and composition of the elaborated saliva. It has been shown, for example, that sympathetic stimulation to salivary glands can produce a markedly increased degree of vasoconstriction.

BoneOral rigid tissues:• Bone•Cement•Enamel•Dentin
Bones are rigid organs that form part of theendoskeleton of vertebrates.
-MechanicalProtection — Bones can serve to protect internal organs, such as the skull protecting the brain or the ribs protectingthe heart and lungs.
Shape — Bones provide a frame to keep the body supported. Movement — Bones, skeletal muscles, tendons, ligaments and joints function together to generate and transfer forces so that individual body parts or the whole body can be manipulated in three-dimensional space. Sound transduction — Bones are important in the mechanical aspect of overshadowed hearing.
-SyntheticBlood production — The marrow, located within the medullary cavity of long bones and interstices of cancellous bone, produces blood cells in a process called haematopoiesis.

-MetabolicMineral storage — Bones act as reserves of minerals important for the body, most notably calcium and phosphorus.
Growth factor storage — Mineralized bone matrix stores important growth factors such as insulin-like growth factors, transforming growth factor, bone morphogenetic proteins and others.
Fat Storage — The yellow bone marrow acts as a storage reserve of fatty acids
Acid-base balance — Bone buffers the blood against excessive pH changes by absorbing or releasing alkaline salts.
Detoxification — Bone tissues can also store heavy metals and other foreign elements, removing them from the blood and reducing their effects on other tissues. These can later be gradually released for excretion.
Endocrine organ - Bone controls phosphate metabolism by releasing fibroblast growth factor - 23 (FGF-23), which acts on kidney to reduce phosphate reabsorption

•Maxilla•Mandible•Alveolar bone

The majority of bone is made of the bone tissue.Bone tissue is a mineralized connective tissue. It has inorganic and organic parts. Inorganic
The inorganic is mainly crystalline mineral salts and calcium, which is present in the form of hydroxyapatite. OrganicThe organic part of matrix is mainly composed of Type I collagen. This is synthesised intracellularly as tropocollagen and then exported, forming fibrils.

Inorganic :60%-65%The inorganic is mainly crystalline mineral salts and calcium, which is present in the form of hydroxyapatite. The matrix is initially laid down as unmineralised osteoid(manufactured by osteoblasts). Mineralisation involves osteoblasts secreting vesicles containing alkaline phosphatase. This cleaves the phosphate groups and acts as the foci for calcium and phosphate deposition. The vesicles then rupture and act as a centre for crystals to grow on.Organic : 30%-35%The organic part of matrix is mainly composed of Type I collagen. This is synthesised intracellularly as tropocollagen and then exported, forming fibrils. The organic part is also composed of various growth factors, the functions of which are not fully known. Factors present include glycosaminoglycans, osteocalcin, osteonectin, bone sialo protein, osteopontin and Cell Attachment Factor. One of the main things that distinguishes the matrix of a bone from that of another cell is that the matrix in bone is hard.
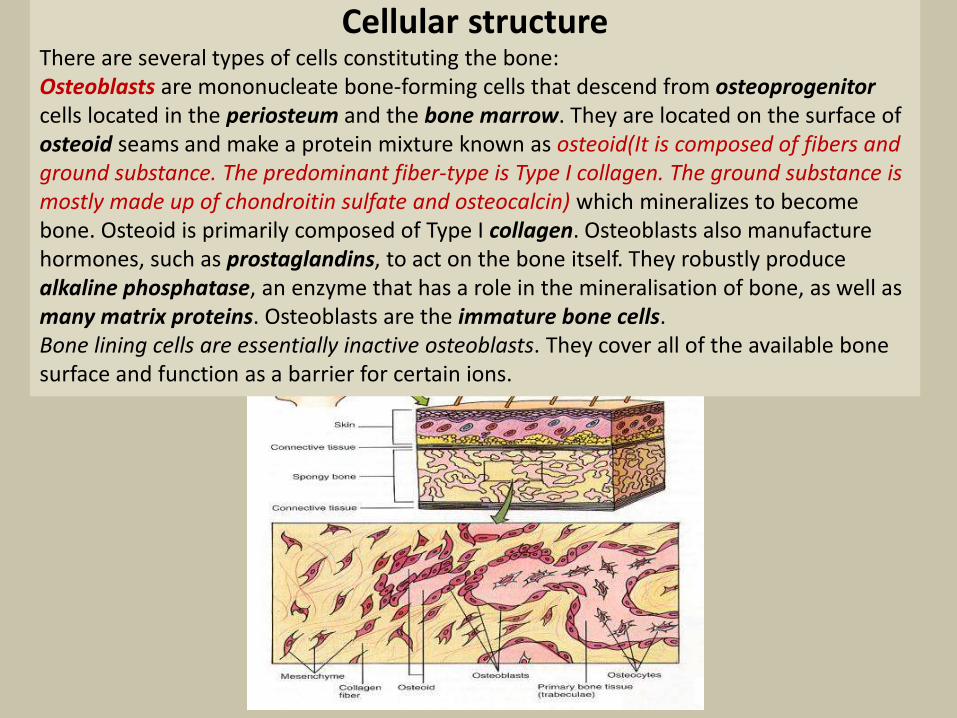
Cellular structureThere are several types of cells constituting the bone:Osteoblasts are mononucleate bone-forming cells that descend from osteoprogenitorcells located in the periosteum and the bone marrow. They are located on the surface of osteoid seams and make a protein mixture known as osteoid(It is composed of fibers and ground substance. The predominant fiber-type is Type I collagen. The ground substance is mostly made up of chondroitin sulfate and osteocalcin) which mineralizes to become bone. Osteoid is primarily composed of Type I collagen. Osteoblasts also manufacture hormones, such as prostaglandins, to act on the bone itself. They robustly produce alkaline phosphatase, an enzyme that has a role in the mineralisation of bone, as well as many matrix proteins. Osteoblasts are the immature bone cells. Bone lining cells are essentially inactive osteoblasts. They cover all of the available bone surface and function as a barrier for certain ions.

Endosteum lines the inner surface of all bones. The interface between the cancellous bone and the marrow is called the endosteum, and it is largely at this site that bone is removed in response to a need for increased calcium elsewhere in the body.
Periosteum is a membrane that lines the outer surface of all bones, except at the joints of long bones. As opposed to osseous tissue, periosteum has nociceptors nerve endings, making it very sensitive to manipulation. It also provides nourishment by providing the blood supply. Periosteum is attached to bone by strong collagenous fibers called Sharpey'sfibres, which extend to the outer circumferential and interstitial lamellae. It also provides an attachment for muscles and tendons.

Osteocyte a star-shaped cell, is the most abundant cellfound in compact bone. Cells contain a nucleus and a thinring of cytoplasm. Originate from osteoblasts that havemigrated into and become trapped and surrounded by bonematrix that they themselves produce. Osteocytes have many
processes that reach out to meet osteoblasts and otherosteocytes probably for the purposes of communication.Their functions include to varying degrees: formation of bone, matrix maintenance and
calcium homeostasis. They have also been shown to act as mechano-sensory receptors—regulating the bone's response to stress and mechanical load. They are mature bone cells.
Osteoclasts are the cells responsible for bone resorption. Osteoclasts are large, multinucleated cells located on bone surfaces in what are called Howship's lacunae or resorption pits. Because the osteoclasts are derived from a monocyte stem-cell lineage, they are equipped with phagocytic like mechanisms similar to circulating macrophages. Osteoclasts mature and/or migrate to discrete bone surfaces. Upon arrival, active enzymes, such as tartrate resistant acid phosphatase, are secreted against the mineral substrate. These bone cells can only resorb mineralized bone matrix.
Bone is a dynamic tissue that is constantly being reshaped by osteoblasts, which build bone, and osteoclasts, which resorb bone.

Bone resorption is the process by which osteoclasts break down bone and release the minerals, resulting in a transfer of calcium from bone fluid to the blood.The osteoclasts are multi-nucleated cells that contain numerous mitochondria and lysosomes. These are the cells responsible for the resorption of bone. Attachment of the osteoclast to the osteon begins the process. The osteoclast then induces an infolding of its cell membrane and secretes collagenase and other enzymes important in the resorption process. High levels of calcium, magnesium, phosphate and products of collagen will be released into the extracellular fluid as the osteoclasts tunnel into the mineralized bone. Bone resorption can be the result of disuse and the lack of stimulus for bone maintenance. Astronauts, for instance will undergo a certain amount of bone resorptiondue to the lack of gravity, providing the proper stimulus for bone maintenance.During childhood, bone formation exceeds resorption, but as the aging process occurs, resorption exceeds formation.

Regulation
Bone resorption is stimulated or inhibited by signals from other parts of the body, depending on the demand for calcium:
PTH,vit D Osteocyte Osteoclast
Calcium-sensing membrane receptors in the parathyroid gland monitor calcium levels in the extracellular fluid. Low levels of calcium stimulates the release of parathyroid hormone (PTH). In addition to its effects on kidney and intestine, PTH also increases the number and activity of osteoclasts to release calcium from bone, and thus stimulates bone resorption.High levels of calcium in the blood, on the other hand, leads to decreased PTH release from the parathyroid gland, decreasing the number and activity of osteoclasts, resulting in less bone resorption.
secretion of osteoid is stimulated by the secretion of growth hormone by the pituitary, thyroid hormone and the sex hormones (estrogens and androgens).
Osteoclast inhibitionThe rate at which osteoclasts resorb bone is inhibited by calcitonin and osteoprotegerin. Calcitonin is produced by parafollicular cells in the thyroid gland, and can bind to receptors on osteoclasts to directly inhibit osteoclast activity. Osteoprotegerin is secreted by osteoblasts and inhibiting osteoclast stimulation

Compact bone or (Cortical bone)The hard outer layer of bones is composed of compact bone tissue, so-called due to its minimal gaps and spaces. This tissue gives bones their smooth, white, and solid appearance, and accounts for 80% of the total bone mass of an adult skeleton.
Trabecular bone(cancellous or spongy bone)Filling the interior of the organ is the trabecular bone tissue which is composed of a network of rod- and plate-like elements that make the overall organ lighter and allowing room for blood vessels and marrow. Trabecular bone accounts for the remaining 20% of total bone mass but has nearly ten times the surface area of compact bone.
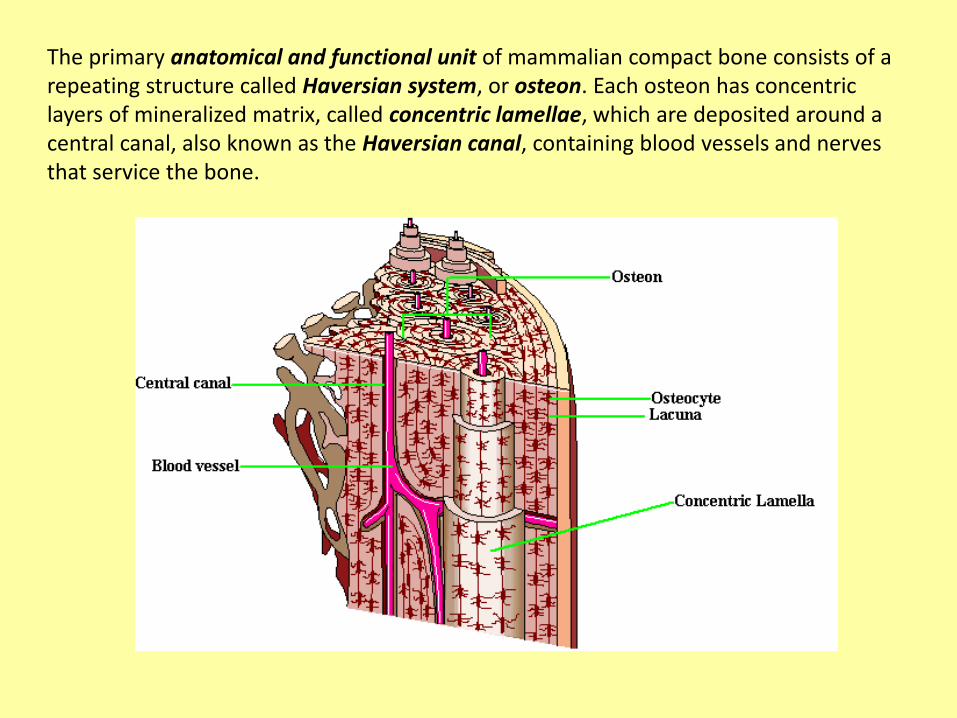
The primary anatomical and functional unit of mammalian compact bone consists of a repeating structure called Haversian system, or osteon. Each osteon has concentric layers of mineralized matrix, called concentric lamellae, which are deposited around a central canal, also known as the Haversian canal, containing blood vessels and nerves that service the bone.

Two types of bone can be identified microscopicallyaccording to the pattern of collagen forming theosteoid :
1) woven bone characterised by haphazard organisation of collagen fibers and is mechanically weak (tooth sockets )
2) lamellar bone which has a regular parallel alignment of collagen into sheets (lamellae) and is mechanically strong. Woven bone is produced when osteoblasts produce osteoid rapidly which occurs initially in all fetal bones (but is later replaced by more resilient lamellar bone). In adults woven bone is created after fractures. Woven bone is weaker, with a smaller number of randomly oriented collagen fibers, but forms quickly; it is for this appearance of the fibrous matrix that the bone is termed woven. It is soon replaced by lamellar bone, which is highly organized in concentric sheets with a much lower proportion of osteocytes to surrounding tissue. Lamellar bone is stronger and filled with many collagen fibers parallel to other fibers in the same layer (these parallel columns are called osteons).
Woven or lamellar

Bundle bone is a histologic term for the portion of the bone of the alveolar process that surrounds teeth and into which the collagen fibers of the periodontal ligament are embedded.It can also be referred to as alveolar bone proper.Bundle bone is functionally dependent in that it resorbs following tooth extraction or loss. lamina dura, a radiographic term denoting the plate of compact bone (alveolar bone) that lies adjacent to the periodontal ligament.
From arrow to PDL = alveolar bone proper
A. Haversian bone
B. Bundle bone
D. Periodontal ligament
E. Radicular dentin with contour lines of Owen
F. Radicular pulp

Primary (baby) teeth start to form between the sixth and eighth weeks, and permanent teeth begin to form in the twentieth week.If teeth do not start to develop at or near these times, they will not develop at all.
Tooth development
Histologic slide showing a tooth bud
A: enamel organ : enamel , thooth crown ,initiate dentin formationB: dental papilla : dentin , pulpC: dental follicle :supporting structure like PDL(fibroblasts),cement ( cementoblasts ),alveolar bone( osteoblasts )


Dentin
Along with enamel, cementum , and pulp is one of the four major components of teeth. It is covered by enamel on the crown and cementum on the root and surrounds the entire pulp. It serves to protect the sensitive pulp of the tooth and create a base under the enamel.The dentine contains more minerals than the bone.By weight, 70% of dentin consists of the mineral hydroxylapatite,
20% is organic material(collagen I, phosphoproteins , glycoproteins ,proteoglycans), and 10% is water.

Yellow in appearance, it greatly affects the color of a tooth due to the translucency of enamel. Dentin, which is less mineralized and less brittle than enamel, is necessary for the support of enamel. Because it is softer than enamel, it decays more rapidly and is subject to severe cavities if not properly treated, but due to its elastic properties it is a good support for enamel. Its flexibility prevents the brittle enamel fracturing. Thereby providing teeth with the ability to flex and absorb tremendous functional loads without fracturing.
The formation of dentin, dentinogenesis, begins prior to the formation of enamel and is initiated by the odontoblasts of the pulp. Unlike enamel, dentin continues to form throughout life and can be initiated in response to stimuli, such as tooth decay orattrition.

An odontoblast (differentiate from cells of the dental papilla) is part of the outer surface of the dental pulp.The odontoblasts secrete dentin throughout life (secondary dentin, once root formation is complete). Odontoblasts also secrete tertiary dentin when irritated.Odontoblasts are large columnar cells arranged in an epithelioid sheet along the junction between dentin and pulp, all the way down to the root apex. It is rich in endoplasmic reticulum and golgi apparatus, especially during primary dentin formation, to give it a high secretory capacity ,firstly collagenous matrix to form predentine, then mineral to form the complete dentine.On initial dentine formation it moves pulpally, away from the primitive amelodentinaljunction (then Inner Enamel Epithelium/dental papillary junction) leaving behind a tubular structure known as the odontoblast process. This process lies in a tubule, known simply as a dentinal tubule.
Enamel spindle
A: enamel organB: dental papillaC: dental follicle

The functions of the odontoblast process are as follows:1. Causes the secretion of hydroxyapatite crystals and mineralization of the matrix 2. General maintenance of the dentinal tubule and dentinal fluid (ion/protein content etc.)3. To secrete sclerotic dentin upon carious attack to block off dentinal tubules, slowing the progress of the attack (air space above blockage is known as a dead tract)4. To channel signals of attack to the odontoblast cell body, initiating reactionary dentin secretion5. To aid in the secretion of tubular dentin (dentin surrounding tubule)

dentin areas characterized by degenerated odontoblastic processes; may result from injury caused by caries, attrition, erosion, or cavity preparation.
Sclerotic dentin is generally caused by some insult to the dentinal tubules and is a hyper-mineralized layer of dentin intended to block dentinal fluid flow, decreasing the stimulation of the pulp. Sclerotic dentin is a protective biologic response.
sclerotic dentine a dense clear dentine formed when the dentinal tubules are filled with mineralized material.

Dentinogenesis is the formation of dentin. The formation of dentin must always occur before the formation of enamel.The different stages of dentin formation result in different types of dentin: mantle dentin, primary dentin, secondary dentin, and tertiary dentin.The unmineralized zone between the odontoblasts and mineralized dentin is called predentin.
Dentin is formed by two simultaneous processes, the formation of collagenous matrix (predentin) and the formation of mineral crystals on this matrix . Dentin formation starts with the synthesis of the extracellular matrix which is mainly formed by the fibrous web of type I collagen. In addition, type V collagen, proteoglycans and other non-collagenousproteins (serum proteins, phosphoproteins) are also secreted.Non-collagenous proteins could be involved in the nucleation of calcium- and phosphate crystals (hydroxyapatite)

They begin secreting an organic matrix around the area directly adjacent to the inner enamel epithelium, closest to the area of the future cusp of a tooth. The organic matrix contains collagen fibers with large diameters (0.1-0.2 μm in diameter). The odontoblastsbegin to move toward the center of the tooth, forming an extension called the odontoblast process. Thus, dentin formation proceeds toward the inside of the tooth. This area of mineralization is known as mantle dentin and is a layer usually about 5-30 μm thick. The outer portion of dentin bordering the enamel or cementum of the tooth. Mantle dentin is slightly less mineralized than other layers of the primary dentin.
A. Striae of Retzius
B. Reparative dentin (irregular secondary
dentin)
C. Cementum
D. Mantle dentin
E. Circumpulpal dentin

The primary dentin is formed rapidly during tooth formation. It outlines the pulp chamber and constitutes the main part of the dentin mass. The outer layer of primary dentin, which is synthesised at the onset of dentinogenesis, is called mantle dentin. The formation of primary dentin continues until the tooth becomes functional or until the root apex is closed .The larger odontoblasts cause collagen to be secreted in smaller amounts, which results in more tightly arranged, heterogeneous nucleation is used for mineralization. Other materials (such as lipids, phosphoproteins, and phospholipids) are also secreted.
Thereafter dentin formation proceeds as secondary dentinogenesis, which continues at a slower rate than the primary dentinogenesis during the life-time of the individual. The secondary dentin is considered to be more irregular in structure and sometimes less mineralized than the primary dentin.
A. Striae of Retzius
B. Reparative dentin (irregular secondary
dentin)
C. Cementum
D. Mantle dentin
E. Circumpulpal dentin

Odontoblasts also secrete tertiary dentin(reactionary dentin) when irritated. Tertiary dentin secreted by odontoblasts is often due to chemical attack, either by chemicals diffusing through the dentin and insulting the odontoblasts, or by diffusion of toxic bacterial metabolites down the dentinal tubules in the instance of a carious attack. This is an attempt to slow down the progress of the caries so that it does not reach the pulp. Reactionary dentine is secreted at varying speeds, dependant on the speed of progression of caries above. Histologically, it is easily distinguishable by its disordered tube structure, its local secretion (causing it to protrude into the pulpal cavity) and its slightly lower degree of mineralisation than normal.
In the case of an infection breaching the dentin to or very near the pulp, or in the instance of odontoblast death due to other attack (e.g. chemical or physical), Pulpal Stem Cells can differentiate into odontoblast-like cells which then secrete the other kind of tertiary dentin, reparative dentin, underneath the site of attack. This is not only to slow the progress of the attack, but also to prevent the diffusion of bacteria and their metabolites into the pulp, reducing the probability of partial pulp necrosis.

Dentin consists of microscopic channels, called dentinal tubules, which radiate outward through the dentin from the pulp to the exterior cementum or enamel border , so span the entire thickness of dentin. These tubules follow an S-shaped path. The diameter and density of the tubules are greatest near the pulp. there are branching canalicular systems that connect to each other.These tubules contain fluid(a mixture of albumin, transferrin and proteoglycans) and
cellular structures(odontoblast process). As a result, dentin has a degree of permeability which can increase the sensation of pain and the rate of tooth decay.
However, dentin also contains mineral rich fluids called dentinal fluids, which may be responsible for the mineralization of the dentin as it is secreted by the odontoblasts. Dentinal fluids contain proteins, sodium, and calcium, and are concentrated in the dentinal tubules.


A, Stria of Retzius; B, Dentino-enamel junction

The dentine may be divided into(ITD) intertubular dentine and (PTD)peritubular dentine. The former is the main product of the odontoblasts constituting the largest volume of the dentine. The intertubular dentine consists of a fibrous network of collagen with deposited mineral crystals.The peritubular dentine forms a highly mineralized sheath around the dentinal tubule
(0.5-1 micrometers thick in humans). The peritubular dentine gradually (partly or completely) fills up the dentinal tubules at some distance away from the pulp chamber.

Figure left. SEM of fractured dentin showing the open dentinal tubule (T), peritubular dentin
(P), and intertubular dentin (I).
Figure right. SEM showing on the top left the intact smear layer and a longitudinal section of
an odontoblastic process (OP) demonstrating the peritubular dentin (P) and the intertubular
dentin (I).

The term granular layer may refer to:the granular layer of Tomes, seen in dentin of the teeth.A granular layer is seen adjacent to cementum.It is believed to be caused by coalescing & looping of terminal portion of dentinal tubules.
Left to right:Tubules, granular layer of Tomes, hyaline layer, acellular cement

Incremental lines in the dentine of representatives from various dinosaur clades. The incremental lines of von Ebner run from left to right in each plate and are the smallest visible laminations. The teeth were thin sectioned longitudinally and viewed with polarized microscopy. (A) Tyrannosaurus (Tyrannosauridae); (B) Triceratops(Ceratopsidae); (C) Edmontosaurus (Hadrosauridae); (D) Edmontonia (Nodosauridae).
Incremental lines
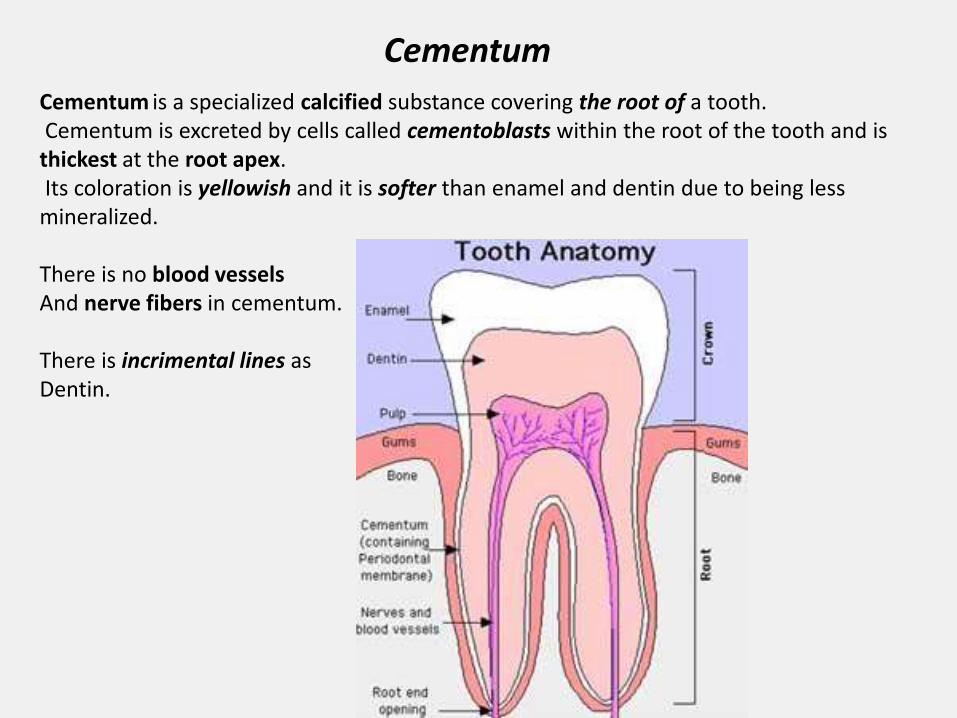
Cementum
Cementum is a specialized calcified substance covering the root of a tooth.Cementum is excreted by cells called cementoblasts within the root of the tooth and is
thickest at the root apex.Its coloration is yellowish and it is softer than enamel and dentin due to being less
mineralized.
There is no blood vesselsAnd nerve fibers in cementum.
There is incrimental lines as Dentin.

Cementum's main role is to anchor the tooth by attaching it via the periodontal ligaments and blockade of dentinal tubules.It meets the enamel lower on the tooth at the cemento-enamel junction.
The chemical makeup of cementum is similar to that of bone, but it lacks vascularization. Volumetrically, it is approximately 65% inorganic material (mainly hydroxyapatite), 23% organic material (mainly collagen type1) and 12% water.
Cementum is slowly formed throughout life and this allows for continual reattachment of the periodontal ligament fibres.

Intermediate cementumEpithelial root sheet is the source ofThin,amorphous,structurless and highly mineralized secretion on the surface of the root dentin.Lack of collagen and similar to enamel.More evident in the apical region of the root.
Cementum:
•Intermediate cementum•Cellular and acellular cementum
The cervical loop area: (1) dental follicle cells, (2) dental mesenchyme, (3) Odontoblasts, (4) Dentin, (5) stellate reticulum, (6) outer enamel epithelium, (7)inner enamel epithelium, (8) ameloblasts, (9) enamel.

Cellular and acellular cementum
Cells from dental follicle becomes cementoblasts and secrete cementum which covers roots.Cementogenesis is slower than dentogenesis.Cementoid(collagen,proteoglycans and glycoproteins)and mineralisation.
Acellular cementum (cervical half of the root dentin)Cellular cementum (apical half)
A: enamel organB: dental papillaC: dental follicle

The Hertwig's epithelial root sheath (frequently abbreviated as "HERS") is a proliferation of epithelial cells located at the cervical loop of the enamel organ in a developing tooth. Hertwig's epithelial root sheath initiates the formation of dentin in the root of a tooth by causing the differentiation of odontoblasts from the dental papilla. The root sheath eventually disintegrates, but residual pieces that do not completely disappear are seen as epithelial cell rests of Malassez (ERM).

After dentin formation begins, the cells of the inner enamel epithelium secrete an organic matrix against the dentin. This matrix immediately mineralizes and becomes the tooth's enamel.Outside the dentin are Ameloblasts, which are cells that continue the process of enamel
formation; therefore, enamel formation moves outwards, adding new material to the outer surface of the developing tooth.
A: enamel organB: dental papillaC: dental follicle
Tooth enamel

Tooth enamel is the hardest and most highly mineralized substance of the body.96% of enamel consists of mineral, with 4% water and organic material.The normal color of enamel varies from light yellow to grayish white. Since enamel is semitranslucent, the color of dentin and any restorative dental material underneath the enamel strongly affects the appearance of a tooth. Enamel varies in thickness over the surface of the tooth and is often thickest at the cusp, up to 2.5 mm, and thinnest at its border, which is seen clinically as the cementoenameljunction (CEJ).
Enamel's primary mineral is hydroxylapatite, which is a crystalline calcium phosphate.
Unlike dentin and bone, enamel does not contain collagen. Instead, it has two unique classes of proteins called amelogenins and enamelins.

Ameloblasts are present only during tooth development, that deposit tooth enamel.
Ameloblasts secrete the enamelin and amelogenin which will later mineralize to form enamel on teeth. The secretory end of the ameloblast ends in a six-sided pyramid-like projection known as the Tomes' process. A narrow extension of the ameloblast from which the enamel matrix is secreted.
The ameloblasts will only become fully functional after the first layer of dentine has been formed, as such dentine is a precursor to enamel.

Amelogenesis, or enamel formation, beginning at the future location of cusps, around the third or fourth month of pregnancy.The creation of enamel is complex, but can generally be divided into two stages.
The first stage, called the secretory stage, involves proteins and an organic matrix forming a partially mineralized enamel. The second stage, called the maturation stage, completes enamel mineralization.
At some point before the tooth erupts into the mouth, but after the maturation stage, the ameloblasts are broken down. Consequently, enamel, unlike many other tissues of the body, has no way to regenerate itself

The basic unit of enamel is called an enamel rod, formerly called an enamel prism, is a tightly packed mass of hydroxyapatite crystals in an organized pattern.In cross section, it is best compared to a keyhole, with the top, or head, oriented toward
the crown of the tooth, and the bottom, or tail, oriented toward the root of the tooth.
Enamel rods are found in rows along the tooth. Within each row, the long axis of the enamel rod generally is perpendicular to the underlying dentin. The arrangement of crystals within each enamel rod is highly complex.
The area around the enamel rod is known as interrod enamel. Interrod enamel has the same composition as the enamel rods. Nonetheless, a histologic distinction is made between the two because crystal orientation is different in each. The crystals lie nearly perpendicular to the enamel rod. The border where the crystals of enamel rods and crystals of interrod enamel meet is called the rod sheath.

The rod sheath is found where enamel rods meet interrod enamel. The crystals of both types of enamel meet at sharp angles and form the appearance of a space called the rod sheath. As a result of this space, the rod sheath consists of more protein (as opposed to minerals) than other areas of enamel. For this reason, the rod sheath is characterized as being hypomineralized in comparison to the rest of the highly mineralized enamel.The rod sheath is Inorganic matrix tying the enamel rods together.
Unerupted lower left canine germ of the Irhoud 3 juvenile. (A) Stereo microscope overview with position of area enlarged in B(white box) and virtual plane of section in C(dotted line). (B) Perikymata (white arrows), surface manifestations of long-period Retziuslines, were counted from the cusp tip to the cervix on the original tooth.

Striae of Retzius are stripes that appear on enamel when viewed microscopically in cross section, these stripes demonstrate the growth of enamel, similar to the annual rings on a tree.
Perikymata are shallow furrows where the striae of Retzius end.Darker than the other stripes, the neonatal line is a stripe that separates enamel formed
before and after birth.
Gnarled enamel is found at the cusps of teeth. Its twisted appearance results from the orientation of enamel rods and the rows in which they lie.

Enamel lamellae are a type of hypomineralized structure in teeth that extend either from the dentinoenamel junction (DEJ) to the surface of the enamel, or visa versa. They are prominent linear enamel defects. These structures contain proteins, proteoglycans, and lipids.
A. Enamel lamella B. Enamel tufts C. Enamel spindle

Enamel - transverse ground sectionIn a transverse section of tooth, the stria of Retzius appear as concentric bands parallel to the dentino-enamel junction (DEJ).In addition to the "hypo-mineralized" dark stria of Retzius,
there also exist hypo-mineralized areas perpendicular to the DEJ.These are enamel lamellae (that traverse the entire thickness of enamel)
and enamel tufts (that traverse the inner third of enamel adjacent to the DEJ.
Legend: A, Stria of Retzius; B, Enamel tuft; C, Enamel lamella; D, Dentino-enamel junction

Enamel tufts are frequently confused with enamel lamellae, which are also enamel defects, but which differ in two ways: lamella are linear, and not branched, and they exist primarily extending from the enamel surface, through the enamel and towards the dentinoenameljunction, whereas enamel tufts project in the opposite direction.Enamel tufts should also not be confused with the similar enamel spindles. Enamel spindles are also linear defects, similar to lamellae, but they too can be found only at the dentinoenamel junction, similar to enamel tufts. This is because they are formed by entrapment of odontoblast processes between ameloblasts prior to and during amelogenesis.
Some sources consider them to be of no clinical significance. However, they have been noted to be an important potential source of enamel fractures that arise after extended use or overloading. It appears that, although enamel easily starts to form the fracture defects of enamel tufts, they then enable enamel to resist the further progress of these fractures, ultimately preventing mechanical failure. This fracture resistance is why tooth enamel is three times stronger than its constituent hydroxyapatite crystallites that make up its enamel rods.

Dental Pulp
The dental pulp is richly vascularized and innervated part in the center of a tooth made up of living soft tissue and cells.Each person can have a total of up to 52 pulp organs, 32 in the permanent and 20 in the primary teeth.
Crowns of the teeth contain coronal pulp.The coronal pulp has six surfaces: the occlusal,the mesial, the distal, the buccal, the lingual andthe floor. Because of continuous deposition of dentin,the pulp becomes smaller with age.
Radicular pulp is that pulp extending fromthe cervical region of the crown to the root apex.
The radicular portion is continuous with the periapicaltissues through the apical foramen .
Apical foramen is the opening of the radicular pulpinto the periapical connective tissue. The averagesize is 0.3 to 0.4 mm in diameter. There can be twoor more foramina separated by a portion of dentin and cementum or by cementum only.
Accessory canals are pathways from the radicular pulp, extending laterally through the dentin to the periodontal tissue seen especially in the apical third of the root.

Dental pulp is an unmineralized oral tissue composed of soft connective tissue, vascular, lymphatic and nervous elements .
Pulp has a soft, gelatinous consistency, indicates that by either weight or volume, the majority of pulp (75-80%) is water.
Aside from the presence of pulp stones, found pathologically within the pulp cavity of aging teeth, there is no inorganic component in normal pulp.
The pulp cavities of molar teeth are approximately fourtimes larger than those of incisors.
The pulp cavity extends down throughthe root of the tooth as the root canal which opensinto the periodontium via the apical foramen.
The blood vessels, nerves etc. of dental pulp enter and leave the tooth through this foramen.
This sets up a form of communication between the pulpand surrounding tissue - clinically important in thespread of inflammation from the pulp out into thesurrounding periodontium.

Cells: fibroblasts and undifferentiated mesenchymal and odontoblasts cells as well as other cell types (macrophages, lymphocytes, etc.) required for the maintenance and defense of the tissue . undifferentiated mesenchymal cells (perivascular cells) facilitates the recruitment of newly differentiating cells to replace others when they are lost - specifically odontoblasts.
Fibrous matrix: collagen fibers, type I and II, are present in an unbundled and randomly dispersed fashion, higher in density around blood vessels and nerves. Type I collagen is thought to be produced by the odontoblasts as dentin, secreted by these cells, is composed of type I collagen. Type II is probably produced by the pulp fibroblasts as this type increases in frequency with the age of the tooth. Older pulp contains more collagen of both the bundled and diffuse types.
Ground substance: the environment that surrounds both cells and fibers of the pulp is rich in proteoglycans, glycoproteins and large amounts of water.
Pulpal component

The central region of the coronal and radicularpulp contains large nerve trunks and blood vessels.This area is lined peripherally by a specialized odontogenic area which has three layers
1. Odontoblastic layer; outermost layer which contains odontoblasts and lies next to the predentin and mature dentin.
2. Cell free zone (zone of Weil) which is rich in both capillaries and nerve networks. The nerve plexus of Rashkow is located in here
3. Cell rich zone; innermost pulp layer which contains fibroblasts and undifferentiated mesenchymal cells
Cells found in the dental pulp include fibroblasts (the principal cell), odontoblasts, defence cells like histiocytes, macrophages (macrophage), granulocytes, mast cells and plasma cells.

1 - odontoblast zone2 - cell-free zone3 - cell-rich zone4 - pulp core
A - DentinB - nerveC - blood vessel

Age-Related and Pathologic Changes in the Pulp
Specific changes occur in dental pulp with age. Cell death results in a decreased number of cells. The surviving fibroblasts respond by producing more fibrous matrix (increased type I over type II collagen) but less ground substance that contains less water. So with age the pulp becomes:a) less cellularb) more fibrousc) overall reduction in volume due to the continued deposition of dentin (secondary/reactive)

One or more small arterioles enter the pulp via the apical foramen and ascend through the radicular pulp of the root canal.Once they reach the pulp chamber in the crown they branch out peripherally to form a
dense capillary network immediately under - and sometimes extending up into - the odontoblast layer. Small venules drain the capillary bed and eventually leave as veins via the apical foramen. Blood flow is more rapid in the pulp than in most areas of the body and the blood pressure is quite high.
In recent years a number of studies have demonstrated the presence of thin-walled, irregularly shaped lymphatic vessels.They are larger than capillaries and have an incompletebasal lamina facilitating the resorption of tissue fluid
and large macromolecules of the pulp matrix.
The continued formation of cementum at the apical foramen can lead to occlusion of the opening. The walls of pulpal veins are first affected by the cemental constriction. Vascular congestion may occur. This ultimately leads to necrosis of the pulp.
Vascular Supply to the Pulp

Innervation of the Pulp
1. Autonomic Nerve Fibers. sympathetic and colinergic autonomics fibers are found in the pulp. sympathetic fibers extend from the neurons whose
cell bodies are found in the superior cervical ganglionat the base of the skull.
They are unmyelinated fibers and travel withthe blood vessels. They innervate the smooth muscle cells of the arterioles andtherefore function in regulation of blood flow
in the capillary network.
2. Afferent (Sensory) Fibers. These arise from the maxillary and mandibular branches of the 5th cranial nerve (trigeminal). They are predominantly myelinated fibers and may terminate in the central pulp. From this region some will send out small individual fibers that form the subodontoblastic plexus (of Raschkow) just under the odontoblast layer. From the plexus the fibers extend in an unmyelinated form toward the odontoblasts. The fibers terminate as "free nerve endings" near the odontoblasts, extend up between them or may even extend further up for short distances into the dentinal tubule. They function in transmitting pain stimuli from heat, cold or pressure. The subodontoblasticplexus is primarily located in the roof and lateral walls of the coronal pulp. It is less developed in the root canals.

A. Pulp B. Dentin C. PredentinD. OdontoblastsE. Subodontoblastic cell-free zone of Weil F. Cell-rich zone G. [Parietal plexus]

The most widely accepted hypothesis about how the stimuli influence nerve fibers is the hydrodynamic theory, which states that pain from exposed dentin following stimulation results from rapid fluid movement inside the dentinal tubules.
Small calcified bodies are present in up to 50% of the pulp of newly erupted teeth and in over 90% of older teeth. These calcified bodies are generally found loose within the pulp but may eventually grow large enough to encroach on adjacent dentin and become attached. These bodies are classified by either their development or histology:
1. Development
Epithelio-Mesenchymal Interactions. Small groups of epithelial cells become isolated from the epithelial root sheath during development and end up in the dental papilla. Here they interact with mesenchymal cells resulting in their differentiation into odontoblasts. They form small dentinal structures within the pulp.
Calcific Degenerations. Spontaneous calcification of pulp components (collagen fibers, ground substance, cell debris, etc.) may expand or induce pulpal cells into osteoblasts. These cells then produce concentric layers of calcifying matrix on the surface of the mass - but no cells become entrapped.
Diffuse Calcification. A variation of the above whereby seriously degenerated pulp undergoes calcification in a number of locations. These bodies resemble calcific degenerations except for their smaller size and increased number.
Calcified Bodies in the Pulp (Pulp Stones)

2. Histology
Calcified bodies in the pulp may be composed of dentin, irregularly calcified tissue, or both. A calcified body containing tubular dentin is referred to as a "true" pulp stone or denticle . True pulp stones exhibit radiating striations reminiscent of dentinal tubules. Usually those bodies formed by an epithelio- mesenchymal interaction, are true pulp stones.Irregularly calcified tissue generally does not bear much resemblance to any known tissue and as such is referred to as a "false" pulp stone or denticle . False pulp stones generally exhibit either a hyaline-like homogeneous morphology or appear to be composed of concentric lamellae.
shows both types of stones: A and B are false pulp stones, C is a true pulp stone. A is an "attached" stone (which may become embedded as secondary dentin deposition continues. B and C are "free" stones found within the pulp cavity

Functions of Dental Pulp
The primary function of dental pulp is providing vitality to the tooth. Loss of the pulp following a root canal does not mean the tooth will be lost. The tooth then functions without pain but, it has lost the protective mechanism that pulp provides.Dental pulp also has several other functions:
Nutritive: the pulp keeps the organic components of the surrounding mineralized tissue supplied with moisture and nutrients;
formative: the odontoblasts of the outer layer of the pulp organ form the dentin that surrounds and protects.
Sensory: extremes in temperature, pressure, or trauma to the dentin or pulp are perceived as pain;
protective: pulp responds to stimuli like heat, cold, pressure, operative cutting procedures of the dentin, caries, etc.. A direct response to cutting procedures, caries, extreme pressure, etc., involves the formation of reactive (secondary) dentin by the odontoblastlayer of the pulp. Formation of sclerotic dentin, in the process of obliterating the dentinal tubules, is also protective to the pulp, helping to maintain the vitality of the tooth.

Periodontium
Periodontium refers to the specialized tissues that both surround and support the teeth, maintaining them in the maxillary and mandibular bones. It consists of the Cementum, Periodontal ligaments, Gingiva and Alveolar bone.
The tissues of the periodontium combine to form an active, dynamic group of tissues. The alveolar bone (C) ,The cementum (B) is attached to the adjacent cortical surface of the alveolar bone by the alveolar crest (I), horizontal (J) and oblique (K) fibers of the periodontal ligament
Cementum is the only one that is a part of a tooth.
The gingiva , or gums, consists of the mucosal tissue that lies over the alveolar bone. the gingiva is the surrounding tissue visible in the mouth.
Alveolar bone surrounds the roots of teeth to provide support and creates what is commonly called a socket Dental alveolus.Dental alveolus are sockets in the jaws in which the roots of teeth are held in the alveolar process of maxillawith the periodontal ligament.
Periodontal ligaments connect the alveolar bone to the cementum.
The dentoalveolar fiber bundles occupy approximately two thirds of the Periodontium volume.

Cells of the Periodontium
The cellular constituents of the Periodontium include:osteoblasts, osteoclasts, Epithelial Rests of Malassez(The epithelial rests appear as small clusters of
epithelial cells which are located in the periodontal ligament adjacent to the surface of cementum. They are cellular residues of the embryonic structure known as Hertwig's epithelial root sheath.)
Fibroblasts, undifferentiated mesenchymal cells, cementoblasts and cementoclasts, neurovascular elements
The osteoblasts and osteoclasts are functionally associated with the alveolar bone,and the cementoblasts and cementoclasts are functionally associated with the
cementum. The extracellular constituents of the PDL consist of collagen fibers, oxytalan fibers, ground substance, nerves, and vessels.

The periodontal ligament, commonly abbreviated as the PDL is a group of specialized connective tissue fibers that essentially attach a tooth to the alveolar bone within which it sits. These fibers help the tooth withstand the naturally substantial compressive forces which occur during chewing and remain embedded in the bone.Another function of the PDL is to serve as a source of proprioception, or sensory innervation, so that the brain can detect the forces being placed on the teeth and react accordingly. To achieve this end, there are pressure sensitive receptors within the PDL which allow the brain to discern the amount of force being placed on a tooth during chewing.formation of the periodontal ligament begins with ligament fibroblasts from the dental follicle. These fibroblasts secrete collagen, which interacts with fibers on the surfaces of adjacent bone and cementum. This interaction leads to an attachment that develops as the tooth erupts into the mouth.
A: enamel organB: dental papillaC: dental follicle
Formation of the deciduous tooth germs occurs on the labial aspect of the dental lamina (DL). An epithelial bridge (lateral lamina, LL)is seen to connect DL with the bell-shapedtooth germ. EK: enamel knot. The free tip of DL proliferates intothe ectomesenchyme as thesuccessional lamina (SL) providing the anlage for a permanent tooth. Dental papilla (DP), dental follicle (DF).

Shortly after the beginning of root formation and the formation of the outer dentinal layer of root, the PDL is formed.
The cells of the dental follicle divide and differentiate into cementoblasts, fibroblastsand osteoblasts.
The fibroblasts (synthesis of collagen & lysis of collagen) synthesize fibers and ground substance that become the PDL. These fibers then embed themselves into the newly formed cementum laid down by cementoblasts at one end, and into the bone laid down by osteoblasts at their other end.When a tooth erupts into the oral cavity, these fibers become oriented in a particularly specific array. The fiber bundles of the periodontal ligament gradually thicken after the teeth have been in function for a while.
The periodontal ligament is one of the four supporting tissues of a tooth.Their dimensions decrease with age. The PDL fibers are composed primarily of type I collagen, although type III fibers are also involved. Compared to most other ligaments of the body, these are highly vascularized.
The PDL fibers are categorized according to their orientation and location along the tooth.

Occlusion or the arrangement of teeth and how teeth in opposite arches come in contact with one another, continually affects the formation of periodontal ligament. This perpetual creation of periodontal ligament leads to the formation of groups of fibers in different orientations, such as horizontal and oblique fibers.
In humans, the width of the PDL ranges from 0.15 to 0.38 mm. Occlusal loading in function affects the width of the PDL. If occlusal forces are within physiologic limits, increased function leads to an increase in width through a thickening of the fiber bundles and an increase in diameter and number of Sharpey's fibers. Forces that exceed this limit cause lesions. When function is diminished or absent, the width of the PDL decreases. The fibersare reduced in number and density.
The portion of the principal fiber that is embedded into either cementum or bone is called a Sharpey's fiber.
Principal fiber groups of the periodontal ligament. (A) Transseptal, (B) Alveolar crest, (C) Horizontal, (D) Oblique, (E) Apical, and (F) Interradicular
The fiber bundles of human PDL are arranged into networks having a complex three-dimensional overlapping arrangement. The fiber bundles follow a wavy course from the root to the bone with frequent crimping, branching, and anastomosing. The blood vessels take a primarily longitudinal course between the fiber bundles.

PDL fibersTrans-septal fibersThey extend from the cemento-enamel junction of one tooth to the cemento-enamel junction of the adjacent tooth. They serve to adhere the adjacent teeth together.Alveolar crest fibers
Alveolar crest fibers attach to the cementum just apical to the cementoenamel junction, run downward, and insert into the alveolar bone.Horizontal fibersHorizontal fibers attach to the cementum apical to the alveolar crest fibers and run perpendicularly from the root of the tooth to the alveolar bone.

Oblique fibersOblique fibers are the most numerous fibers in the periodontal ligament. They attach apical to the horizontal fibers and run diagonally toward the crown of the tooth inserting to the alveolar bone there. Because they are the most numerous, these fibers are believed to be primarily responsible in absorbing the chewing forces on the tooth. They are hence the main support of the tooth.Apical fibersApical fibers are at the apex of a root. They attach from the cementum and insert to the surrounding bone at the base of the socket. They are also the first to offer resistance to movement of the tooth in an occlusal direction (e.g. when the tooth is being extracted)Interradicular fibersInterradicular fibers are only found between the roots of multi-rooted teeth, such as a molars. They also attach from the cementum and insert to the nearby alveolar bone.

In the human PDL oxytalan fibers, which resemble immature elastin fibers, are seen among the collagen fibers. Oxytalan fibers form a network that attaches blood vessels to the cementum . Periodontal vessels are linked vertically by fibers or multiple groups of fibers forming tracts. Unique oxytalan-vascular structures consist not only of fibersassociated with the walls of individual arteries, veins, and Iymph vessels but a meshwork that surrounds the total vessel complex.Some researchers hypothesize that these fibers provide support for the blood vessels
when the PDL is under function. Others feel that these fibers may influence blood flow and thereby effect tooth support.
Oxytalan fibers. (A) Cementum, (B) Principal oxytalan fiber, (C) Oxytalan tract, and (D) Periodontal vessel

Gingiva
The connection between the gingiva and the tooth is called the dentogingival junction. This junction has three epithelial types: gingival, sulcular, and junctional epithelium. These three types form from a mass of epithelial cells known as the epithelial cuff between the tooth and the mouth.

Much about gingival formation is not fully understood, but it is known that hemidesmosomes form between the gingival epithelium and the tooth and are responsible for the primary epithelial attachment. Hemidesmosomes provide anchorage between cells through small filament-like structures provided by the remnants of ameloblasts. Once this occurs, junctional epithelium forms from reduced enamel epithelium, one of the products of the enamel organ, and divides rapidly. This results in the perpetually increasing size of the junctional epithelial layer and the isolation of the remnants of ameloblasts from any source of nutrition. As the ameloblasts degenerate, a Gingival sulcus forms.The gingival sulcus is an area of potential space between a tooth and the surrounding gingiva and is lined by sulcular epithelium.

The gingival fibers are the connective tissue fibers that inhabit the gingival tissue adjacent to the teeth and help hold the tissue firmly against the teeth.They are primarily composed to type I collagen, although type III fibers are also involved.
These fibers, unlike the fibers of the periodontalligament attach the tooth to the gingival tissue,rather than the tooth to the alveolar bone.
The gingival fibers accomplish the following tasks:•They hold the marginal gingiva against the tooth •They provide the marginal gingiva with enoughrigidity to withstand the forces of mastication
without distorting .They serve to stabilize themarginal gingiva by uniting it with both the tissueof the more rigid attached gingiva
as well as the cementum layer of the tooth.
In theory, gingival fibers are the protectors against periodontitis, as once they are breached, theycannot be regenerated. When destroyed,
the gingival sulcus increases in depth apically,allowing more debris and bacteria to remain inintimate contacts with the delicate sulcular and junctional epithelia for longer times.

Gingival fibers
dentogingival fibers (free-attached)
Alveologingival fibers
Dentinoperiosteal fibers
circular fibers - these fibers are unique in thatthey exist entirely within the gingiva and donot contact the tooth
transseptal fibers - these fibers spanning theinterproximal tissue between adjacent teeth,into which they are embedded.

Interdental view of gingival fiber groups. (A) Circular, (B) Dentogingival, (C) Dentoperiostal, and (D) Alveologingival
Frontal view of gingival fiber groups. (A) Circular, (B) Dentogingival, (C) Dentoperiostal, and (D) Alveologingival
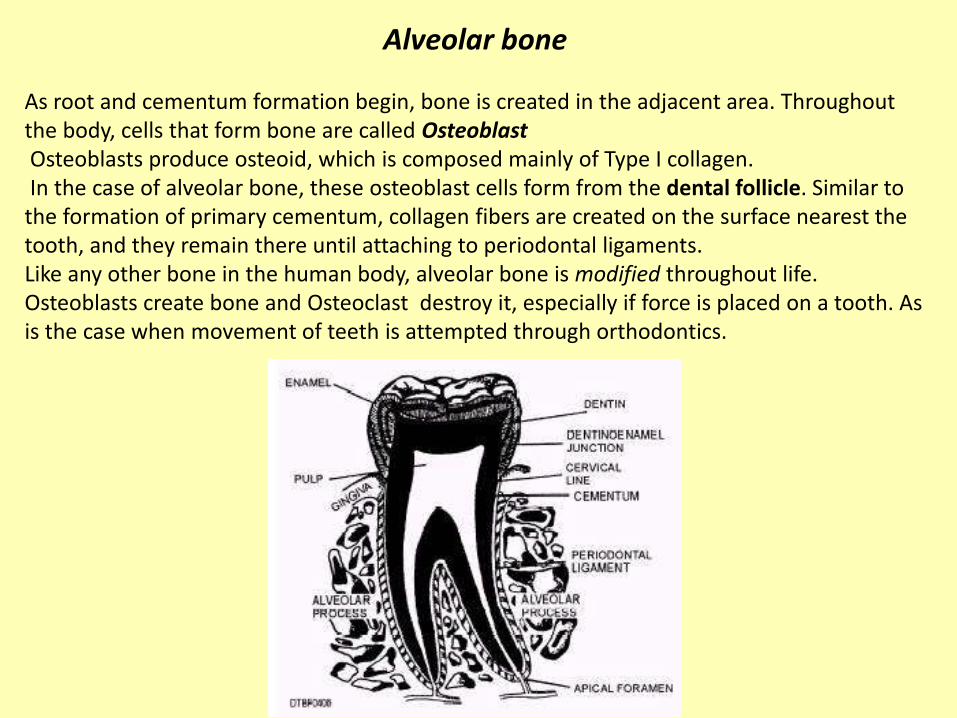
Alveolar bone
As root and cementum formation begin, bone is created in the adjacent area. Throughout the body, cells that form bone are called OsteoblastOsteoblasts produce osteoid, which is composed mainly of Type I collagen.In the case of alveolar bone, these osteoblast cells form from the dental follicle. Similar to
the formation of primary cementum, collagen fibers are created on the surface nearest the tooth, and they remain there until attaching to periodontal ligaments.Like any other bone in the human body, alveolar bone is modified throughout life. Osteoblasts create bone and Osteoclast destroy it, especially if force is placed on a tooth. As is the case when movement of teeth is attempted through orthodontics.

Nerve formationNerve fibers start to near the tooth during the cap stage of tooth development and grow toward the dental follicle. Once there, the nerves develop around the tooth bud and enter the dental papilla when dentin formation has begun. Nerves never proliferate into the enamel organ.Pain and pressure sensory organ
The PDL receives its main blood supply through vessels that enter the PDL space through the alveolar bone, but it also receives contributions from the apical and gingival vessels. The main blood vessels within the PDL course parallel to the long axis of the tooth and run between the collagen fiber bundles near the alveolar bone. These main vessels form a flat, basketlike network of capillaries that surround the root. In the cervical region of the PDL are coiled capillaries that have been described as resembling glomeruli . Axially directed veins drain into a basketlike network at the apical portion of the periodontal space as well as larger veins in the septi of the alveolar bone. These vascular elements may play a role in providing the periodontium with a hydraulic support system that acts in concert with the fiber structure, the viscoelastic ground substance, and the extracellular fluid.
Vascular formation

Periodontal blood supply. Left, buccolingual view (frontal section). Right, sagittal view of interdental bone. (A) Subepithelial capillary network of the gingiva, (B) Capillary network of the periodontal ligament, (C) Supraperiosteal arterial, and (D) Arterials penetrating the interdental alveolar bone.

Functions of periodental space
1-Supportive function
2-Sensory function
3- Nutritive function
4- Maintenance

A microbial species can help to digest food and“protect” a host in different ways:
by passively occupying a niche that could shelter pathogenic organisms or by inhibiting
the pathogen’s adhesion, vitality, growth and production of virulence factors through
metabolic antagonism or by directly inactivating them. For example, the production of
H2O2 by S.sanguis, S. uberis and A. viscosus inhibits the growth of
A.actinomycetemcomitans, thus protecting the host from the pathogenic actions of this
species .
bacteria in the human mouth play a role in creating the distinctive flavors of certain foods. These bacteria actually produce food odors from odorless components of food, allowing people to fully savor fruits and vegetables. Some fruits and vegetables release characteristic odors only after being swallowed.

Dental plaque is a general term for the diverse microbial community (predominantly bacteria) found on the tooth surface, embedded in a matrix of polymers of bacterial and salivary origin. Plaque develops naturally on teeth, and forms part of the defence systems of the host by helping to prevent colonisation of enamel by exogenous (and often pathogenic) microorganisms (colonisation resistance).
Dental plaque is a sticky, soft and colorless biofilm of bacteria that constantly builds up on the surfaces of teeth and gums. Dental plaque is comprised of colonies of bacteria and other microorganisms mixed with bacteria by-products, dead cells.
Dental Plaque

Environmental conditions on a tooth are not uniform. Differences exist in the degree of protection from oral removal forces and in the gradients of many biological and chemical factors that influence the growth of the resident microfiora. These differences will be reflected in variations in the composition of the microbial community, particularly at sites so obviously distinct as the gingival crevice, approximal regions, pits and fissures.fissure plaque will be influenced more by saliva than other sites,
whereas gingival crevicular fluid (GCF) has a greater impact on plaque in the gingival crevice. This latter is colonised by higher numbers of anaerobes, especially proteolytic species which obtain key growth factors from the catabolism of host proteins and glycoproteins in GCF.

Dental plaque formation starts almost immediately after toothbrushing.Some minutes after brushing your teeth, saliva derived glycoprotein deposits start to
cover the tooth surface with what is referred to as "pellicle". The formation of pellicle is the first step in dental plaque formation. The pellicle is then colonized by Gram-positive bacteria such as Streptococcus sanguis, Streptococcus mutans, and Actinomyces viscosus becoming what is known as dental plaque.Bacteria cells interact with pellicle components enabling plaque to firmly adhere to the
tooth surface.
the pellicle forms within seconds to minutes whenever an enamel surface is exposedto saliva. The major constituents of the pellicle arecomponents of saliva and gingival crevicular fluidsuch as proteins (albumin, lysozyme,
proline-rich proteins) , glycoproteins(lactoferrin, IgA, IgG, amylase),phosphoproteins, and lipids and bacterial-derivedglucosyltransferases .

After 1 to 3 days following the initiation of plaque formation:
1-the first bacteria colonies(Gram-positive bacteria) start to multiply and expand .
2-new bacteria species start to colonize the tooth plaque. These new species include also Gram-negative bacteria such as Fusobacterium nucleatum, Prevotella intermedia, and Capnocytophaga.
3-Substances produced by the already accumulated bacteria enrich the plaque environment making it favourable for the growth of other species of bacteria.One week after the first plaque accumulation, new Gram-negative species may be
found, such as Porphyromonas gingivalis, Campylobacter rectus, Eikenella corrodens, Actinobacillus actinomycetemcomitans, and oral spirochetes (Treponema species).
While the dental plaque formation continues Gram-negative species become dominantover the Gram-positive species.
The overgrowth of Gram-negative anaerobic bacteria is considered as one of the main causative factors of gingivitis and periodontitis.

Plaque composition
Dental plaque is composed of 80% water and 20% solid. About 50% of the plaque dry weight is bacterial and salivary protein. About 25% of the dry weight is carbohydrates and lipids,
and another 25% is inorganic component. Dental plaque is responsible for the majority of chemical activities on the tooth surface.
The carbohydrates in plaque consist of polymers synthesized by bacteria (glucans, fructans, and heteropolysaccharides). These extracellular polysaccharides are crucial for :1-bacterial attachment and cohesion,2- serve as a reservoir of fermentable substrates when other food sources become depleted. Bacteria cells contain carbohydrate in the form of intracellular glycogen-like polymers,
which are stored as granules in the cell. They also function as a reservoir when dietary substrates are depleted.
The inorganic components, especially Ca and P concentrations are several times higher than in saliva. Most of the Ca found in plaque is non-ionic. As the pH drops, plaque calcium becomes ionized and is important in determining rates of enamel dissolution and remineralization. Other ions present are, for example, K, Na, Mg, and F.

Plaque fluid: Plaque fluid is the extracellular aqueous phase of dental plaque. It provides the aqueous medium for the exchange of diffusing substances between saliva through plaque and the tooth surface. Plaque fluid can be separated from plaque by centrifugation.
Cariogenic conditions generated by plaque microorganisms can be seen by changes in the ionic composition of plaque fluid. Two types of plaque fluid reflect the metabolic activity of bacteria: resting plaque and starved plaque. Resting plaque fluid is obtained one to several hours after eating. Starved plaque fluid is obtained following overnight fasting. Resting plaque has a higher organic acid concentration (56.3 to 102.1 mmol/1) than starved
sample (31.9 to 61.5 mmol/1). pH values in rested samples (pH 5.69 to 6.54) are also lower than those found in starved samples (pH 6.78 to 7.08).
Total organic acids (mmol/L)
56.3 - 102.1
31.9 - 61.5
Among the organic acids produced by plaque bacteria, lactic acid dominates in the presence of sugar. Lactic acid is considered to be the main acid involved in caries formation. 7 min after sucrose rinse, concentration of lactic acid in plaque rose to twice the starting point and was maintained for a period of time, in this case, about 20 min.
pH
5.69 - 6.54
6.78 - 7.08
Rested plaque
Starved plaque

MICROBIAL IMBALANCES IN HEALTH AND DISEASE
Once established at a site, the plaque flora remains relatively stable with time despite regular environmental challenges.This stability (microbial homeostasis) is not due to any metabolic indifference by the
resident microflora but is due to a dynamic balance being established among the resident members of this microbial community.On occasions, homeostasis breaks down and imbalances in the microflora can occur which predispose a site to disease.For example, the repeated intake of fermentable sugar in the diet produces frequent
conditions of low pH in plaque which inhibits the growth of many of the species associated with dental health, and selects for the highly acidogenic (acid-producing) and aciduric (“acid-loving") species, such as mutans streptococci and lactobacilli, associated with dental caries.
In mature plaque, organisms have been seen in direct contact with the enamel due to enzymic attack on the pellicle.
In periodontal diseases, there is a shift in the composition of the plaque microflora to a more proteolytic Gram negative anaerobic community, which can induce damage to tissues either indirectly via the “side-effects" of an inflammatory host response or directly by the production of proteases, cytotoxins and other factors.

PATHOGENIC DETERMINANTS OF CARIOGENIC BACTERIA
•Rapid transport of dietary sugars: the sugar phosphotransferase uptake system is a high affinity process. Mutans streptococci possess more than one sugar transport system.
•Rapid rates of glycolysis (acidogenicity): can result in a terminal pH of below 4.5 in only a few minutes.
•Tolerance of, and growth at, low pH (aciduricity): the growth of many of the bacteria found on enamel (eg. Strep. sanguis is inhibited at pH <5.5, whereas this is optimal for cariogenic species.
• Extracellular polysaccharide synthesis (EPS): these polymers help make up the plaque matrix. Glucosyltransferases (GTF's) convert sucrose to soluble and insoluble glucans, that help consolidate bacterial attachment; Strep. mutans also produces a specific highly insoluble polymer (mutan). Fructosyltransferases (FTF's) convert sucrose to fructans; these polymers are labile and can be used by plaque bacteria as an energy source.
• Intracellular polysaccharide synthesis (IPS): can be used during starvation conditions and catabolised to acid when dietary sugars are not available.
A striking feature of the main cariogenic bacteria (mutans streptococci and lactobacilli) is their combined acidogenicity and aciduricity.

The relationship between plaque pH and time after sugar challenge is known as the Stephan curve. Dental plaque has the ability to produce rapid and substantial decreases in pH in vivo. The pH rapidly decreases immediately following exposure to a sugar challenge by rinsing with a glucose or sucrose solution. After reaching a minimum, the pH slowly rises until the resting pH is attained, usually in about an hour. The time course varies between individuals and the nature of the challenge. However, pH recovery can take anything between 15 and 40 minutes depending to a large extent on the acid-neutralising properties of the individual's saliva.
The period and extent of pH drop was inversely related to the caries activities of the subjects. The extent of plaque pH decrease (how low and how long) after glucose challenge is attributed to the type and amount of carbohydrateavailable, bacteria present,
other food ingested, salivary composition and flow, and thickness andage of dental plaque.
Stephan curve The principle of Stephan Curves is to assess the cariogenicity of different foods.

Type and amount of CHO available
Bacteria present
Salivary composition and flow
What contributes to the extent of pH drop after glucose challenge?
Other food ingested
Thickness and age of dental plaque

The initial rapid drop in pH is due to the speed with which plaque microbes are able to metabolise sucrose. Larger carbohydrates, such as starch, would diffuse into plaque more slowly and would need to be broken down before assimilation by the microbes. In the case of starch, salivary amylase would produce a mixture of glucose and maltose together with incompletely digested material comprising the branch points of the starch molecule (limit dextrins). The glucose and maltose would then be taken up by plaque bacteria and metabolised. The rate of starch breakdown slows up glycolysis and, therefore, acid production producing a less steep drop in pH.

Resting plaque pH:
Constant within each individual, but differences among groups.
Caries-inactive – resting pH ~ 6.5 - 7
Caries-prone – lower resting pH
Bacterial composition affects metabolic properties of plaque
Storage form of CHO energy source when diet is depleted
What contributes to the differences in resting plaque?
When the host does not ‘eat’, cariogenic bacteria still produce acids form storage carbohydrates

In addition to the pH drop, the characteristic of baseline pH value is also important. Under resting conditions, plaque pH is quite constant in each individual. But there are some differences noticeable from person to person.
Caries-inactive individual usually have a resting pH between 6.5-7, and usually remain above pH 5 following sugar exposure.
In contrast, the caries-prone group has a lower resting pH and remains below 5 for a longer period after sugar exposure. It’s probably due to bacterial composition that affects the metabolic properties of plaque. For example, the storage form of carbohydrate that allows them to ferment when external diet is depleted. Therefore cariogenic bacteria which have storage form of carbohydrate can produce acids when the host does not ‘eat’.
The critical pH is the pH below which enamel will begin to dissolve.

Margolis HC. Enamel-plaque fluid interaction. Cariology for the Nineties, 1993
What are the differences in plaque fluid between ‘caries-free’ and caries-positive individuals?
CompositionNa+
Mg2+
K+
CalciumP
AcidLacticAcetic
Propionic
pH
DS (degree of saturation of enamel)
14.2 + 3.52.0 + 0.4
59.9 + 4.916.2 + 5.213.9 + 1.9
‘caries-free’ caries-positive
16.5 + 5.42.6 + 0.4
71.4 + 11.36.9 + 0.4
15.6 + 3.6
1.8 + 0.719.9 + 3.5
5.8 + 1.5
2.6 + 1.220.3 + 4.6
5.8 + 1.5
7.02 + 0.05
7.11 + 0.66 5.42 + 0.68
*
*
*
6.79 + 0.12

The lowest pH attained is also determined by the rates of diffusion of substrates and metabolites. Molar fissures are the most caries-prone sites because they are very sheltered from saliva flow. The deepest parts are often inaccessible to toothbrushes which means that fissures frequently contain impacted food for extended periods of time. If the food contains carbohydrate the plaque is likely to have a lower resting pH than that found at other sites in the mouth. This lower resting pH will encourage the growth of aciduricmicrobes such as S. mutans. In fact, research has shown that fissure plaque has a greater proportion of aciduric microbes including S.mutans and lactobaccilli.

The rise in pHThe pH starts to rise after a few minutes due to:1. acid by-products diffusing out of the plaque
2. salivary bicarbonate diffusing into the plaque and neutralising the acid by-products
3. In addition, the low pH produced will inhibit microbial metabolism and thereby slow the rate of acid production. This will allow the processes of diffusion and neutralisation to exert a greater effect on plaque pH. Also, as before, plaque which is less dense and fully exposed to saliva flow will show a faster rate of pH recovery. It normally takes at least 20 minutes for the plaque pH to reach its resting value but it can take considerably longer depending on the factors described above.

The lowest pH achieved depends greatly on:
Microbial composition The presence of significant numbers of aciduric, acidogenic bacteria in plaque developing in a sheltered site with a low diffusion rate coupled with a readily fermentable carbohydrate such a sucrose or glucose would produce the lowest pH. Under these conditions a pH in the region of 4.5, or even lower, might be attained.
Carbohydrate nature Conversely, a challenge with a carbohydrate which is metabolised more slowly to a plaque community with fewer aciduric, acidogenic microbes would result in less acid production and a higher terminal pH.
Rate of diffusionThe rate of diffusion of material into and out of plaque is governed by the density of the plaque and access by saliva. Thus less dense plaque fully exposed to saliva flow will more rapidly exchange metabolites with the surroundings. This will enable substrates to diffuse into the plaque rapidly and at the same time allow microbial by-products to diffuse out. The terminal pH following a challenge to the plaque will reflect the relative rates of diffusion of both substrate and metabolites.

Saliva flow rate One of the most important factors governing the overall shape of a Stephan Curve, but particularly the pH recovery, is saliva flow rate. The effect of saliva on the Stephan Curve is easily demonstrated by isolating some dental plaque using cotton wool pads. This is shown in the diagram on the right.Saliva exerts two effects. First, it dilutes and carries away metabolites diffusing out of the plaque. Second it supplies bicrabonate ions which diffuse into plaque and neutralise the by-products of fermentation (organic acids) in situ. The bicarbonate-mediated acid neutralisation effect is enhanced by the increase in salivary bicarbonate associated with increased saliva flow which co-incides with eating.
Acid neutralisation by bicarbonate isaccelerated by salivary carbonic anhydrase.
This is secreted by acinar cells of the parotid and submandibular glands and is the onlyexample of a secreted carbonic anhydrasein mammals.

The concept of critical pH
Saliva and plaque fluid are supersaturated WRT tooth enamel
Critical PH= pH at which a solution is just saturated with respect to a particular mineral
If the solution pH > critical pH supersaturated mineral precipitate
If the solution pH < critical pH undersaturated mineral dissolve
Normal condition: Our teeth do not dissolve in saliva or plaque fluid
Critical pH of carious formation in enamel ~ 4.5-5.5
Coincide with pH when plaque bacteria ferment carbohydrates
The tooth will dissolve when the pH of fluid phase is less than critical pH.
pH of saliva & plaque fluid > critical pH
Saliva & plaque fluid contain Ca, P, OH > Tooth Enamel

pH 6.5 6.0 5.5 5.0 4.5 4.0 3.5 3.0
deposit caries erosion
demineralization
remineralization
pH 6.5 6.0 5.5 5.0 4.5 4.0 3.5 3.0
Critical pH
Carious lesion forms at pH 4.5 - 5.5
Erosion lesion forms when pH < 4.5

Calculus
calculus is a form of hardened plaque and is synonymous with tartar.It is caused by the continual accumulation of minerals from saliva on plaque on the
teeth. Its rough surface provides an ideal medium for further plaque formation, threatening the health of the gingiva.
Heavy staining and calculus deposits exhibited on the lingual surface of the mandibular anterior teeth, along the gumline.

HYPOTHESES RELATING PLAQUE TO CARIES
Specific plaque hypothesis: out of the diverse collection of bacteria in plaque, only a very limited number of species are involved in disease. These species can be regarded as specific pathogens that can be targeted with specific anti-caries therapies. Non-specific plaque hypothesis: plaque is a microbial community; disease results from the outcome of the interactions among all of the component species. Prevention would be by plaque control. Ecological plaque hypothesis: disease results from shifts in the balance of the resident plaque microflora. Potentially cariogenic bacteria can be present in health, but at levels that are not clinically relevant. Disease could be controlled not only by targeting putative pathogens but also by interfering with the factors responsible for driving the deleterious shifts in the microflora.
CARIES PREVENTIONFissure sealants Fluoride (may also have some anti-glycolytic effects). Antimicrobial agents (these agents can be applied in toothpastes, mouthrinses and varnishes. Some also inhibit glycolysis and EPS production at sub-MIC levels). Sugar substitutes (prevent acid production, but xylitol may selectively inhibit Strep.
mutans)Vaccination (whole cell and sub-unit vaccines eg. surface proteins, glucosyltransferaseswith proven anti-Strep. mutans activity have been tested in animal models). Passive immunisation (anti-Strep. mutans monoclonal antibodies can prevent colonisation of teeth by Strep. mutans).

The oral cavity is a moist environment which is kept at a relatively constant temperature (34 to 36°C) and a pH close to neutrality in most areas and thus supports the growth of a wide variety of microorganisms.
The oral cavity possesses both hard (teeth) and soft (mucosa) tissues.The oral mucosa is characterized by a continuous desquamation of its surface epithelial cells, which allows rapid elimination of adhering bacteria. The mucosa that covers the cheek,tongue, gingiva, palate, and floor of the mouth varies according to the anatomical site. The epithelium may be keratinized (palate) or nonkeratinized (gingival crevice) . The tongue, with its papillary surface, provides sites of colonization that are protected from mechanical removal.
The tooth can be described as a nonshedding hard surface that offers many different sites for colonization by bacteria below (subgingival) and above (supragingival) the gingival margin.
Gingival crevice (the area between the junctional epithelium of the gingiva and teeth)provides a unique colonization site that includes both hard and soft tissues.
Dental caries is the second most common of all maladies in humans, next only to the common cold.
Microorganisms in oral cavity

More than six billion people inhabit this planet. This number is the same as the number of new microbial cells that are produced in 1h or 2h in each of our mouths . This complex oral microbiota contains more than 500 different bacterial species , as well as many species of viruses and yeast .
Multiple ecological niches maintain at least five major bacterial ecosystems :bacteria on the tongue;bacteria on the buccal mucosa;tooth-adherent bacteria that are coronal to the gingival margin (supragingival plaque);
bacteria that are apical to the gingival margins (subgingival plaque),and bacteria in the saliva.

The microbial flora of the oral cavity are rich and extremely diverse. This reflects the abundant nutrients and moisture, and hospitable temperature, and the availability of surfaces on which bacterial populations can develop.
Under normal circumstances, the microbial flora in the oral cavity reaches equilibrium, where the chemical by-products of growth of some microbes are utilized by other microbes for their growth. The metabolic activities of some bacteria can use up oxygen, creating conditions that are favorable for the growth of those bacteria that require oxygen-free conditions.
The presence of a myriad of microorganisms is a natural part of proper oral health. However, an imbalance in the microbial flora can lead to the production of acidiccompounds by some microorganisms that can damage the teeth and gums.

Physicochemical
host related
Microbial
external
FACTORS INFLUENCING THE ORAL ECOSYSTEM
Physicochemical factors:Temperature, pH, availability of water, availability of nutrients, and oxidation-reduction potential .

Temperature.The temperature in the oral cavity is relatively constant (34 to 36°C), which allows a wide range of microorganisms to grow. The temperature may be more variable on the mucosal and tooth supragingival surface. During food intake, microorganisms colonizingthese sites are exposed to hot and cold meals and probably must adapt to these extreme variations of temperature.
Water.As the mouth is constantly bathed by saliva and crevicular fluid, water is not considered to be a limiting factor.

pH.The pH of an environment affects microorganisms and microbial enzymes directly and also
influences the dissolution of many molecules that indirectly influence microorganisms.Microorganisms generally cannot tolerate extreme pH values.
In the oral cavity, the pH is maintained near neutrality (6.7 to 7.3) by saliva.The saliva contributes to maintenance of the pH by two mechanisms.First, the flow of saliva eliminates carbohydrates that could be metabolized by bacteria and
removes acids produced by bacteria. Second, acidity from drinks and foods, as well as from bacterial activity, is neutralized by the buffering activity of saliva. Bicarbonate is the major salivary buffering system of saliva, but peptides, proteins, and phosphates are also involved.
Increases in pH also result from bacteria that metabolize sialine and urea into ammonia.
Frequent sugar intake favours the growth of aciduric bacteria predisposes to caries formation. When the pH of the chemostat was controlled at 7.0, the glucose pulse had little effect on the microbial populations, suggesting that the low pH generated from carbohydrate metabolism, rather than carbohydrate availability per se, is responsible for the shift in composition of the oral microbiota in vivo.
The subgingival area is bathed by gingival fluid and is not controlled by the buffering salivary activity. The pH in the gingival crevice may vary between 7.5 and 8.5, while the crevicular fluid ranges from pH 7.5 to 7.9. An alkaline pH in gingival crevices and periodontal pockets may exert a selective force towards the colonization of periodontopathogens .
Oxidation-reduction potential.Many enzymatic reactions are oxidation-reduction reactions.
The proportion of oxidized to reduced components constitutes the oxidation-reduction potential or redox potential (Eh). The Eh is greatly influenced by the presence or absence of molecular oxygen, which is the most common electron acceptor.Anaerobic bacteria need a reducing environment (negative Eh) for growth,
Aerobic bacteria need an oxidizing environment (positive Eh).
The mouth is characterized by a wide range of oxidation-reduction potentials, allowing the growth of aerobic and anaerobic bacteria .In general, the dorsum of the tongue and the buccal and palatal mucosa are aerobicenvironments with positive Eh, thus better supporting the growth of facultative anaerobic bacteria. The gingival crevice and the approximal surfaces of the teeth (surfaces between teeth) possess the lowest Eh and the highest concentration of obligately anaerobic bacteria.
Nutrients.The levels of most bacterial populations are strongly controlled by substrate availability. Each bacterial species must be more efficient than the rest in utilizing one or a few particular substrates under certain conditions. In the oral cavity, microorganisms living in the supragingival environment have access to nutrients from both endogenous (saliva) and exogenous (diet) origin. Saliva is an important source of nutrients and can sustain normal growth of microorganisms in the absence of exogenous nutrients .Saliva contains water, carbohydrates, glycoproteins, proteins, amino acids, gases, and several ions including sodium, potassium, calcium, chloride, bicarbonate, and phosphate. Among exogenous dietary components, carbohydrates and proteins have the greatest influence on the composition of the oral microbiota .
The gingival crevice is not exposed to dietary components and saliva, and its principal source of nutrients is the gingival crevicular fluid. The crevicular fluid originates from plasma and is an excellent source of nutrients for microorganisms.
Many nutritional interrelationships also occur between microorganisms. Some microorganisms cooperate for the degradation of nutrients. Some bacteria also use nutrients and other substances produced by other microorganisms.

Physicochemical
host related
Microbial
external
Temprature,PH,Water,Nutrient,Redox potential
Defence mechanisms,Age,hormonalchange,stress,Genetic factors

Host defense mechanisms: Saliva, gingival crevicular fluid The supragingival environment of the oral cavity is controlled primarily by saliva.
The continuous flow of saliva increased by the muscular activity of the lips and tongue removes a large number of bacteria from teeth and mucosal surfaces.
Saliva contains several specific and nonspecific defense factors.
SIgA is the principal specific defense factor of saliva.
The nonspecific defense factors include mucins, nonimmune salivary glycoproteins, lactoferrin, lysozyme, peroxidase, histatins, and cystatins.
Mucins are high-molecular-weight glycoproteins produced by submandibular, sublingual, and numerous minor salivary glands. They are the principal organic constituent of mucus, the slimy viscoelastic material that envelopes all mucosal surfaces of the body. Saliva contains two forms of mucins, MG1 and MG2.They involve in tissue coating and aggregation and adherence of streptococci.
In the oral cavity, mucins provide a protective coating for both soft and hard tissues. The mucins form a viscous slime layer on oral mucosa that traps microorganisms and antigens, limiting their penetration into the tissues .Potentially harmful microorganisms are thus eliminated by the continuous renewal of the mucous layer combined with the washing action of salivary flow. Mucins are also constituents of the acquired pellicle and may protect teeth from acid demineralization.

When salivary glycoproteins are absorbed on solid surfaces, they may bind to bacteria and promote bacterial adherence. Conversely, some of these glycoproteins, when free in saliva, may prevent bacterial colonization by binding to their adhesins or by agglutinating bacteria in saliva .This type of aggregation may facilitate the removal of oral bacteria by swallowing. Saliva from subjects with low levels of mutans streptococci aggregate these bacteria more efficiently, suggesting a protective role for salivary agglutinins .
Saliva possesses defense factors with direct antimicrobial activity .A group of salivary proteins, lysozyme, lactoferrin and peroxidase, act in conjunction with
other components of saliva to limit the growth of bacteria or kill them directly.
Lysozyme is secreted by intercalated duct cells .Lysozyme can lyse some bacterial species by hydrolyzing glycosidic linkages in the cell wall.lysozyme can aggregate oral bacterial cells and inhibit their colonization on mucosalsurfaces and teeth .
Lactoferrin is an iron-binding glycoprotein produced by intercalated duct cells.It inhibits microbial growth, probably by sequestering iron in the environment.
peroxidase is an enzyme secreted by salivary gland acinar cells.Salivary peroxidase removes toxic hydrogen peroxide produced by oral microorganisms and can reduce acid production in dental plaque.

Histatins (histidine-rich peptides) are a family of small basic peptides produced by acinarcells .They inhibit the development of Candida albicans from the noninfective to the infective form .
Cystatins are a family of cysteine-containing phosphoproteins that are secreted by acinarcells .These proteins are also present in plasma and may reach the oral cavity via thegingival crevicular fluid .Cystatins act mainly as thiol protease inhibitors and can inhibit proteases produced by suspected periodontopathogens.
SIgA is the principal immunoglobulin isotype found in saliva and all other secretions. In humans, there are two IgA subclasses, IgA1 and IgA2, which occur in similar proportions in saliva and other secretions.Salivary IgA is produced by plasma cells that are located adjacent to the duct and acini of salivary glands . SIgA is considered the first line of defense against pathogens which colonize and invade surfaces bathed by secretions . The intrinsic resistance of IgA to proteolysis, preserves the biological functions of the molecule in secretions .SIgA agglutinate bacteria and neutralize toxins, enzymes, and viruses . The inhibition of bacterial adherence by SIgA is considered one of the most important defense mechanisms against mucosal bacterial invasion. SIgA may also act synergistically with innate immune factors present in secretions. by acting in synergy with other antibacterial factors such as lysozyme, lactoferrin, salivary peroxidase, and mucins.

The leukocytes in gingival crevicular fluid are composed of 90% polymorphonuclearleukocytes (PMNs) and 10% mononuclear cells( B lymphocytes, T lymphocytes, macrophages ).The cells are capable of phagocytosis and of killing microorganisms, although the
efficiency of phagocytosis is reduced compared with that of blood neutrophils .Lysozyme and peroxidase that are released from the lysosome of PMNs during phagocytosis might also control microbial growth in the gingival crevice.
Components of the complement cascade are present in the gingival crevicular fluid. Complement factors may initiate bacterial cell lysis or enhance phagocytosis of microorganisms .
Saliva does not gain access to the gingival crevice, and this area of the oral cavity is almost essentially controlled by the antimicrobial factors of plasma. Cellular and humoral componentsof blood can reach the gingival crevice of the oral cavity by the flow of gingival fluid through the junctional epithelium.Even in the healthy state, there is a continuous flow of small quantities of fluid and leukocytesfrom the gingival capillaries through the crevicular epithelium into the gingival crevice. This flow increases greatly with inflammation induced by plaque accumulation .The continuous flow of gingival fluid from the crevice to the oral cavity removes nonadherent bacterial cells. Gingivalfluid also contains antimicrobial substances including IgM, IgG, IgA, complement, and leukocytes. These factors are primarily protective against microbial invasion.

The IgG, IgM, and IgA antibodies directed against a variety of oral microorganisms have been detected in plasma and crevicular fluid even in healthy individuals .These antibodies may influence the oral microbiota by interfering with adherence or by inhibiting bacterial metabolism .The IgG antibodies may enhance phagocytosis and killing of oral microorganisms through activation of complement .
All specific and nonspecific antimicrobial factors in the oral cavity do not act in isolation. Synergistic and antagonistic interactions among antimicrobial factors may influence their actions.Mucins serve to concentrate other antimicrobial substances, including lysozyme, IgA, and cystatins, at the mucosal surface .SIgA enhances the antimicrobial activity of lactoferrin, salivary peroxidase, agglutinins, and mucins. The polycationic antimembrane effect of lysozyme may be enhanced by salivary peroxidase and histatins. In contrast, salivary peroxidase may block the bactericidal effect of lactoferrin.
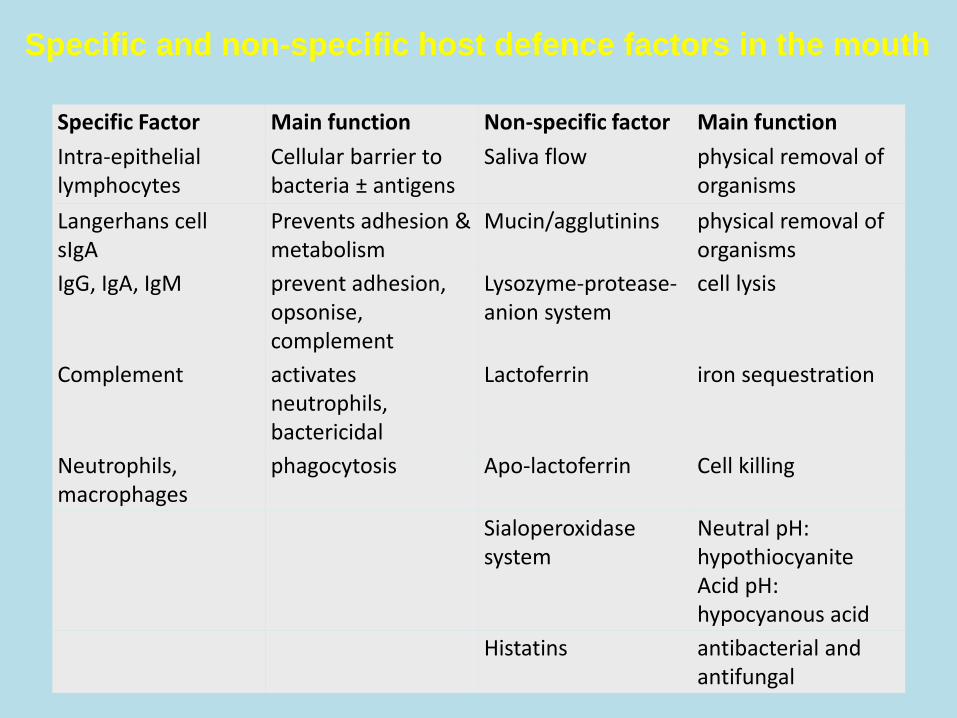
Specific Factor Main function Non-specific factor Main function
Intra-epithelial lymphocytes
Cellular barrier to bacteria ± antigens
Saliva flow physical removal of organisms
Langerhans cellsIgA
Prevents adhesion & metabolism
Mucin/agglutinins physical removal of organisms
IgG, IgA, IgM prevent adhesion, opsonise, complement
Lysozyme-protease-anion system
cell lysis
Complement activates neutrophils, bactericidal
Lactoferrin iron sequestration
Neutrophils, macrophages
phagocytosis Apo-lactoferrin Cell killing
Sialoperoxidase system
Neutral pH: hypothiocyaniteAcid pH: hypocyanous acid
Histatins antibacterial and antifungal
Specific and non-specific host defence factors in the mouth

ANTIMICROBIAL AGENTS IN HUMAN WHOLE SALIVA
1. Non-immunoglobulin, innate factorsLysozymeLactoferrinSalivary peroxidase system (enzyme – SCN (hypothiocyanite)- - H202)Myeloperoxidase system (enzyme - SCN-/halide - H202)Agglutinins (parotid saliva glycoproteins, mucins, secretary IgA,lysozyme, f2-microglobulin, fibronectin)Histidine-rich polypeptidesAnionic antimicrobial proteinsPhagocytic cells2. Immunoglobulins, acquired factorsSecretory IgAIgGIgM
Myeloperoxidase is not produced by the salivary glands ,but its oral origin is in the polymorphonuclear cells . These cells are, however, also found in substantial amounts in whole saliva of edentulous persons (Raeste, 1976), indicating passage of these cells through oral mucosa. Leukocytes are rich in myeloperoxidase, and lysed cells release active enzyme into the saliva.

Saliva, the epithelial surface layers, and polymorphonuclear leukocytes (neutrophils) all contribute to maintaining the health of the oral cavity and periodontium in overlapping but independent ways . Antimicrobial peptides (AMPs) are natural antibiotics that are found in each of these compartments.AMPs are important contributors to maintaining the balance between health and disease as part of the host innate immune response. They have generally been considered to contribute to mucosal health .
antimicrobial peptides in saliva (blue), in gingival epithelium (pink), and in neutrophils(PMNs) migrating into the oral cavity via the gingival crevicular fluid

Age.The composition of the oral microbiota varies with the age of the host.
Age-related changes in the oral microflora include those due to teeth eruption, changes in dietary habits, hormones, salivary flow, the immune system, or other factors.The human oral cavity is usually sterile at birth. However, within 6 to 10 h after birth, microorganisms from the mother and those present in the environment become established in the oral cavity.
Hormonal changes. puberty and pregnancy are characterized by increased levels of steroid hormones in plasma and subsequently in the crevicular fluid and saliva .Pregnancy and puberty are associated with an increase in gingival inflammation . It has been proposed that the exacerbations in gingival inflammation may be due to hormone-induced alterations in the microbiota of the gingival crevice .Microorganisms in the subgingival area that use hormones as growth factors may be favored during the period of hormone increase associated with puberty and pregnancy.
Stress.Host stress may be associated with changes in hormones, salivary flow, dietary habits, and immune response.

Genetic factors.The genetic background appears to influence the susceptibility to caries and periodontal diseases .This could in part be because the host genetic factors select for a microbiota with varying potential for causing oral diseases. The selection of a certain microbiota by the host is dependent on inherited immune factors, physiology, metabolism, mucus composition, or receptor-ligand interactions .
Physicochemical
host related
Microbial
external
Temprature,PH,Water,Nutrient,Redox potential
Defence mechanisms,Age,hormonal change,stress,Genetic factors
Adherence, Bacterial interactions

Adherence.To get established in the oral cavity, microorganisms must first adhere to teeth or to mucosal surfaces. Adherence is essential for providing resistance to the flow of saliva. Adherence is mediated by adhesins on the surface of bacteria and by receptors on the oral surface. Microbial adhesins consist of polysaccharides, lipoteichoic acids, glucosyltransferases, and carbohydrate-binding proteins (lectins). The receptors may be salivary components (mucins, glycoproteins, amylase, lysozyme, IgA, IgG, proline-rich proteins, and statherins) or bacterial components (glucosyltransferases and glucans) that are bound to oral surfaces.
Bacterial interactions.A variety of beneficial and antagonistic interactions may help in maintaining the homeostasis
of the oral microbiota. Coaggregation is one exemple of commensalism and synergism that occurs between microbial species. Coaggregation allows the indirect adherence of some bacteria on oral surfaces. It was demonstrated that coaggregated cells were more resistant to phagocytosis and killing by neutrophils. The utilization of oxygen by facultative anaerobic. bacteria reduces the oxygen concentration that allow the colonization of anaerobic bacteria. Different bacterial species may also cooperate in the utilization of substrates that they could not metabolize alone. Competition and antagonism mechanisms among oral resident bacteria may help to maintain the ecological balance by preventing the overgrowth of some resident bacterial species . The competition for adhesion receptors, nutritional competition and the production of inhibitory substances (antagonism) are the mechanisms involved in reducing bacterial colonization and preventing bacterial overgrowth.

Physicochemical
host related
Microbial
external
Temprature,PH,Water,Nutrient,Redox potential
Defence mechanisms,Age,hormonalchange,stress,Genetic factors
Adherence, Bacterial interactions
Diet,oral hygiene,Fluoride ,Drugs and diseases

External FactorsDiet.Frequent consumption of a high-sucrose diet enhances the development of S. mutans and Lactobacillus .The fermentation of sucrose into lactate generates a low pH, favoringacidogenic and acidophilic bacteria.
Oral hygiene and antimicrobial agents.Oral hygiene is one of the most important factors in themaintenance of oral homeostasis and oral health.
The mechanical removal of plaque by tooth brushing and flossing can almost completely prevent caries and periodontaldiseases. The addition of antimicrobial agents mouthwashesincreases the effect of mechanical oral hygiene procedures.Antimicrobial agents may assist in protection by reducing bacteria adhesion to the tooth
surface, by reducing the growth of microorganisms and plaque accumulation, by selectively inhibiting only those bacteria directly associated with oral diseases, or by inhibiting the expression of virulence determinants, such as acid production or protease activity .

Fluorideis found in most toothpastes and mouth rinses and is well known for its anti-cariesproperties. The principal caries-preventive effect of fluoride is attributed to the formation of fluoroapatite and calcium fluoride, which lead to an increase in the resistance of enamel to demineralization .It can also inhibit bacterial growth by reducing the sugar transport, glycolytic activity, and acid tolerance of many gram-positive species .Fluoride can help stabilize the composition of the microflora by reducing the rate of acid production and the fall in pH during frequent carbohydrate intake .
Drugs and diseasesSalivary gland hypofunction and xerostemia may result from the intake of xerogenic
medication, irradiation treatments for head and neck cancer, and Sjøgren's syndrome. Patients with xerostomia have a decrease capacity to eliminate sugars and buffer the acids found in plaque. In addition to suffering from the reduction in saliva protection, patients with xerostomia generally consume soft, high-sucrose diets and suck sour candies to keep their mouths moist . They are also more susceptible to dental caries and candidiasis. Antibiotics that are given orally or systemically for the treatment of different infections may enter the oral cavity via saliva and gingival crevicular fluid and lead to a inbalance inthe oral microbiota .Antibiotics may suppress some resident bacterial populations which can result in overgrowth of antibiotic-resistant bacteria.

Other factors. Many other external factors may affect the oral microbiota; these include the wearing of dentures or partial dentures , smoking, oral contraceptives usage , malnutrition , host macroenvironment , and various exposures to exogenous bacterial species.

Physicochemical
host related
Microbial
external
Temprature,PH,Water,Nutrient,Redox potential
Defence mechanisms,Age,hormonalchange,stress,Genetic factors
Adherence, Bacterial interactions
Diet,oral hygiene,Fluoride ,Drugs and diseases

Due to their pathogenic potential, oral micro-organisms cause dental caries, periodontal disease, mixed anaerobic infections of oral tissues, and sometimes infections in other organs.
The oral cavity has sometimes been described as a mirror that reflects a person's health. Systemic disease such as diabetes or vitamin deficiency may be seen as alterations in the oral mucosa. A variety of external factors cause changes in the oral mucosa, thus altering mucosal structure and function, and promoting oral pathologies (most frequently bacterial, fungal and viral infections).

The indigenous microbial flora of the human oral cavity develops slowly into a complex community. When adult microhabitats (teeth and gingival crevices) are formed, as the anatomical development of the oral cavity from birth to adulthood occurs, it reaches its most complex state. The human oral cavity in utero is usually sterile. At birth, the neonate's oral cavity comes into contact with considerable numbers and kinds of microbes from a variety of external environmental sources, i.e., air,water, food, but especially with other human beings. Most of these microbes are transitory and are not found consistently with repetitive sampling. However, the establishment of an indigenous flora begins to occur within the first days of the infant's life. As weeks and months go by, an increasingly complex flora develops. The early colonizers are the Veillonella,Fusobacterium, Actinomyces, and other streptococci and a few Gram-negative rods . When the infant is six months of age (on the average),the first lower incisors erupt, offering a new and unique surface for colonization. When teeth erupt, another microhabitat, the gingival crevice, is formed. Although shallow (less than 1 mm), it provides another unique retentive area. When the infant is 6-12 months old, the oral cavity's microflora becomes increasingly complex.
tongue dorsum is the primary microhabitat and ecological niche for the majority of indigenous microbes. This appears to be the major reservoir for ongoing recolonization of the tooth surfaces and gingival crevice.
The biofilm plaque that accumulates on tooth surfaces includes over 30 categories of microorganisms from 500 bacteria, yeasts, etc. Despite this complexity, plaque formation follows a distinct sequence. It begins with colonization by a group of Gram-positive organisms, mainly streptococci, followed by further colonization by a succession of species and culminating in the arrival of Gram-negative anaerobic bacteria such as Porphyromonas gingivalis, a predominant pathogen in severe adult periodontitis .
Biofilms provide microorganisms with protected niches where they are safe from antimicrobial materials and can become a source of persistent infection.The oral cavity is also the gateway for a wide array of antigenic challenges . These are represent by the substantial bacterial colonization that exists in the oral cavity. Many species of the complex oral microbiota maintain a symbiotic relationship with the host. To maintain homeostasis within the oral cavity, the host has two distinct but interrelated immune response systems: the salivary immune system and serum immune system .The changing balance of conditions in the mouth influences the stability and integrity of
the oral mucosal tissues. The balance may be disturbed by either an increased local stress or a decreased innate immunity.

Medical pathogens, if present in the appropriate host, always produce specific disease. Caries and periodontal diseases are conditional diseases, requiring numbers of certain indigenous species at various sites, particularly the tooth surface.In the case of caries, the condition is related to sugar consumption.
Periodontal disease/s may require certain host and environmental conditions, such as local environment or nutritional factors in gingival crevicular fluids. Nonetheless, critical numbers of certain indigenous species must be present in order for these diseases to occur.

The mucosa of the oral cavity is composed of wet epithelium (mainly keratinocytes )and underlying connective tissue (lamina propria), which contains mainly fibroblasts within an extracellular matrix. The epithelium and lamina propria are linked by an acellular region, - the basement membrane. These epithelial surfaces which may be potentially colonized by bacteria are constantlyshedding and are totally renewed every 24-48 hours. That is, epithelial cells are constantly being lost at the surface and are being replaced from below. Thus, bacterial colonizationof the oral mucosal surfaces, except the tongue dorsum and its papilla, and the gingival crevice which provides more retentive areas, tends to be sparse on a per-epithelial-cell basis. Unquestionably, the most unique anatomic feature of the human oral cavity—or,for that matter, of the entire human body—is the teeth.
The major function of the oral mucosa is to protect the deeper tissues of the oral cavity .It also acts as a sensory organ and serves as a site for some glandular activities. The normal activities of seizing, biting, and chewing food expose the soft oral tissues to mechanical forces and surface abrasions. Both epithelium and connective tissues of the mucosa adapt to this trauma and to the microorganisms that normally reside within the oral cavity and would cause infection if they were to access to deeper tissues .There is no direct contact between specific immune cells in the basal epithelium and microorganisms in the upper layers of the oral mucosa. the protective immunity is conveyed through epithelial cells. These organisms produce many potentially toxic substances such as lipopolysaccharides andproteases.

Caries
Dental caries is a bacterial disease of the dental hard tissues; it is characterized by a localized, progressive, molecular disintegration of the tooth structure. The development of caries is associated with dental plaque of smooth coronal surfaces, pits, and fissures. Caries may also appear on root surfaces that are exposed to the oral environment as a result of gingival recession.The demineralization of teeth (enamel, dentine, and cementum) is caused by organic acid produced from the bacterial fermentation of dietary carbohydrates. The frequent ingestion of carbohydrates may lead to the selection of bacteria that are acidogenic (capable of producing acid from carbohydrates) and aciduric (capable oftolerating acid) and concurrently to a low-pH environment. These conditions favor the solubilization of tooth minerals. The pH at which this demineralization begins is known as the critical pH and ranges between pH 5.0 and 5.5
Periodontal diseases is a general term describing the inflammatory pathologic state of the supporting tissues of teeth. Periodontal diseases can be grouped into two major categories, gingivitis and periodontitis.
Periodontal diseases
Gingivitis is defined as an inflammation of gingival tissues which does not affect theattachment of teeth.Periodontitis involves the destruction of the connective tissue attachment and the
adjacent alveolar bone . In periodontitis, the gingival crevice is deepened to form a periodontal pocket due to the apical migration of the junctional epithelium along the root surface .The induction and progression of periodontal tissue destruction is a complex process involving plaque accumulation, release of bacterial substances, and host inflammatory response . Although bacteria rarely invade tissues, they may release substances that penetrate the gingivae and cause tissue destruction directly, by the action of enzymes and endotoxins, or indirectly, by induction of inflammation.The host inflammatory response to bacterial antigens is both protective and destructive in periodontal diseases. Tissue damage may be caused by the release of lysosomal enzymes from phagocytes and by the production of cytokines that stimulate connective tissue cells to release metalloproteinases (including collagenases) orcytokines that activate bone resorption. Among the bacteria regularly isolated from periodontal pockets, those producing such virulence factors are generally gram-negative rods.

Periodontitis
Teeth are the ideal substrate for plaque formation because of their non-exfoliating surfaces. They also link the infected “open space” of the mouth to the deep periodontal space, offering microorganisms an easy route of entry: dentinal tubules, enamel fissures orirregularities are easily colonized by microbes, but difficult to reach for the host defensemechanisms.Plaque accumulation leads to gingivitis, but the shift to periodontitis depends on both host factors and the selection of virulent bacteria.Periodontitis is not a single disease, but rather a collection of pathologies with similar
patterns and symptoms .
Aggressive Periodontitis” and “Chronic Periodontitis”.
Chronic Periodontitis is defined as an infectious pathology leading to slow or moderately slow, progressive loss of attachment and bone. It occurs mainly in adult patients in either a localized or generalized form, but can nonetheless affect children and adolescents. Predisposing factors such as cigarette smoke, stress and local (e.g., tooth-related or iatrogenic) or systemic (e.g., diabetes mellitus or HIV infection) conditions can enhance thedestructive effects of the microbiota .
Aggressive Periodontitis, on the other hand, is characterized by rapid loss of attachment and bone destruction in otherwise clinically healthy patients and presents familial aggregation.

Peri-implantitis
Peri-implantitis can be considered the “twin-sister” of periodontitis, even though some important differences between natural teeth and dental implants must clearly be borne in mind, the most important being that implants are not surrounded by a periodontal ligament and therefore present different biomechanics and defensive cell recruitment.
The destruction of supporting peri-implant tissue due to microbial infection. It is commonly believed that early failures are associated with surgical errors, while late failures are more often linked to the presence of plaque or improper prosthetic design or maintenance protocol.
Many researchers have underscored the similarity of the microorganisms found around teeth affected by periodontal disease or failing implants and fixtures placed in the same mouth: the healthy implants are colonized by the same pathogens (P.gingivalis, P.intermedia, B.forsythus, E.corrodens, F.nucleatum,C.rectus, P.micros, Spirochetes spp.), causing attachment and bone loss in the involved sites, though the bacterial count is definitely low .Such findings have relevance for the planning of immediate post-extraction implants, especially if tooth loss is determined by periodontal disease. It is suggested that waiting at least 1 month after extraction to allow for elimination of A. actinomycetemcomitans and P.gingivalis
In order to be effective, treatment must consider thebiology of the bacterial communities. Therapy may beplanned according to four different approaches withvarying underlying rationales :– Preventing biofilm formation– Disrupting existing biofilms– Preventing further biofilm growth– Killing specific organisms in the biofilm
In vitro studies of the Biofilm Inhibitory Concentration (BIC), Biofilm Eliminating Concentration (BEC) and Biofilm Killing Concentration (BKC) on single-species biofilmsdid not achieve the same success on the multi-species biofilm forming the dental plaque in vivo.
The treatment of biofilm-related disease may be classified into two main groups: resectiveand regenerative methods. Resection procedures aim to eliminate the etiological factors, while regeneration attempts to reduce the bone defect by regaining lost tissue.
Resection methods consist of scaling, root planing, decontamination of implant surfaces or the use of antimicrobial agents,while regenerative techniques include GTR and grafts.Physically checking and removing biofilms is still the most effective procedure for tackling these common disorders.

Nutrition and Oral tissues
Proteins-Collagen-Immunoproteins
Lipids-Energy supply-EFAs-vitamin absorption- lipids calsification
Carbohydrates-Energy supply

List of B vitamins
Vitamin B1 (thiamine) Vitamin B2 (riboflavin) Vitamin B3 (niacin) Vitamin B4 (adenine) Vitamin B5 (pantothenic acid) Vitamin B6 (pyridoxine) Vitamin B7 (biotin) Vitamin B9 (folic acid) Vitamin B12 (cyanocobalamin)
The B vitamins are necessary in order to:Support and increase the rate of metabolism ,Maintain healthy skin and muscle tone ,Enhance immune and nervous system function ,Promote cell growth and division—including that of the red blood cells that help prevent anemia.
All B vitamins are water soluble, and are dispersed throughout the body. Most of the B vitamins must be replenished regularly, since any excess is excreted in the urine. Vitamin B6 toxicity can damage sensory nerves, leading to numbness in the hands and feet as well as difficulty walking. Symptoms of a pyridoxine overdose may include poor coordination, staggering, numbness, decreased sensation to touch, temperature, and vibration, and tiredness .

B2 : oxidation - reduction Enzymes :FMN,FADCheilosissigns and symptoms of riboflavin deficiency include cracked and red lips, inflammation of the lining of mouth and tongue, mouth ulcers, cracks at the corners of the mouth (angular cheilitis), and a sore throat. A deficiency may also cause dry and scaling skin, fluid in the mucous membranes, and iron-deficiency anemia. The eyes may also become bloodshot, itchy, watery and sensitive to bright light.
B3
In cells, niacin is incorporated into nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP), although the pathways for nicotinamide and nicotinic acid are very similar. NAD+ and NADP+ are coenzymes in a wide variety of enzymatic oxidation-reduction reactions
B12 , folic acid megaloblastic anemia,pale mucous membranes.
Vitamin C (ascorbic acid )ascorbate is an anti-oxidant, it protects the body against oxidative stress,and is a cofactor in several vital enzymatic reactions. Vitamin C is required for the development of collagen, the ground substance between our cells that gives tissues their integrity.Vitamin C is required for the development of our immune systems.
Scurvy is an avitaminosis resulting from lack of vitamin C, since without this vitamin, the synthesised collagen is too unstable to perform its function. Scurvy leads to the formation of liver spots on the skin, spongy gums, and bleeding from all mucous membranes. The spots are most abundant on the thighs and legs, and a person with the ailment looks pale, feels depressed, and is partially immobilized. In advanced scurvy there are open, suppurating wounds and loss of teeth and, eventually, death.

Vitamin A (Retinol)the animal form of vitamin A, is a fat-soluble vitamin important in vision and bone growth.Vitamin A is essential for the correct functioning of epithelial cells. In Vitamin A deficiency, mucus-secreting cells are replaced by keratin producing cells, leading to xerosis (dry skin).Ameloblast degeneration,odontoblast and osteoclasts dysfunction.
Vitamin D is a group of fat-soluble prohormones, Calcitriol (1,25-Dihydroxycholecalciferol) is the active form of vitamin D found in the body.

Vitamin KBlood agglutination
ca2+ & phosphate
Mg2+
Fe





![[Oral Biology]Oral Histology Slides_American Corner Family [ACFF @AmCoFam]](https://static.documents.pub/doc/80x56/5571f7a349795991698bb904/oral-biologyoral-histology-slidesamerican-corner-family-acff-amcofam.jpg)












