80
ERAS Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic

ERAS
Presented by
Timothy L. Beard MD, FACS, CPI
Bend Memorial Clinic

Outline
• Definition
• Justification
• Ileus
• Pain
Outline
• Specifics
• Data
• BMC Data
• Worldwide Data
• Implementation

What is ERAS?
• AKA Fast-track or ERP
• Developed by Kehlet in Denmark in colonic
surgery
• Gradually has gained world-wide acceptance
• Originally described in Open Surgery but same
advantages seem to apply for Laparoscopy
• Gustafsson/Scott



Goal of ERAS
Implement a standardized, patient centered protocol.
Integrate the pre-operative, intra-operative, post-operative and
post-discharges phases of care to reduce LOS.
Improve patient experience and satisfaction and decrease
variability.

Getting Popular
Why Me?

Studies as PI
A Multicenter, Randomized, Double-Blind,
Placebo-Controlled Study to Evaluate the
Efficacy and Safety of IV Ulimorelin Administered
Post-Operatively to Accelerate GI Motility in
Subjects Who Have Undergone a Partial Bowel
Resection. 2010

Studies as PI
Phase IIA Multicenter, Randomized, Double-Blind,
Placebo-Controlled, Parallel-Group study of
Intravenous Methylnaltrexone (MOA-728) for the
Treatment of Post-Operative Ileus after Bowel
Resections and Ventral Hernia Repairs 2007

Studies as PI
Phase III Protocol #14CL314, Multicenter, Double-
Blind, Placebo-Controlled, Parallel Study of
Alvimopan for the Management of Post-
Operative Ileus 2005
Studies as PI
A Phase 4, Multicenter, Double-Blind,
Placebo-Controlled, Parallel Study of
Alvimopan for the Management of
Postoperative Ileus in Subjects Undergoing
a Radical Cystectomy 2010



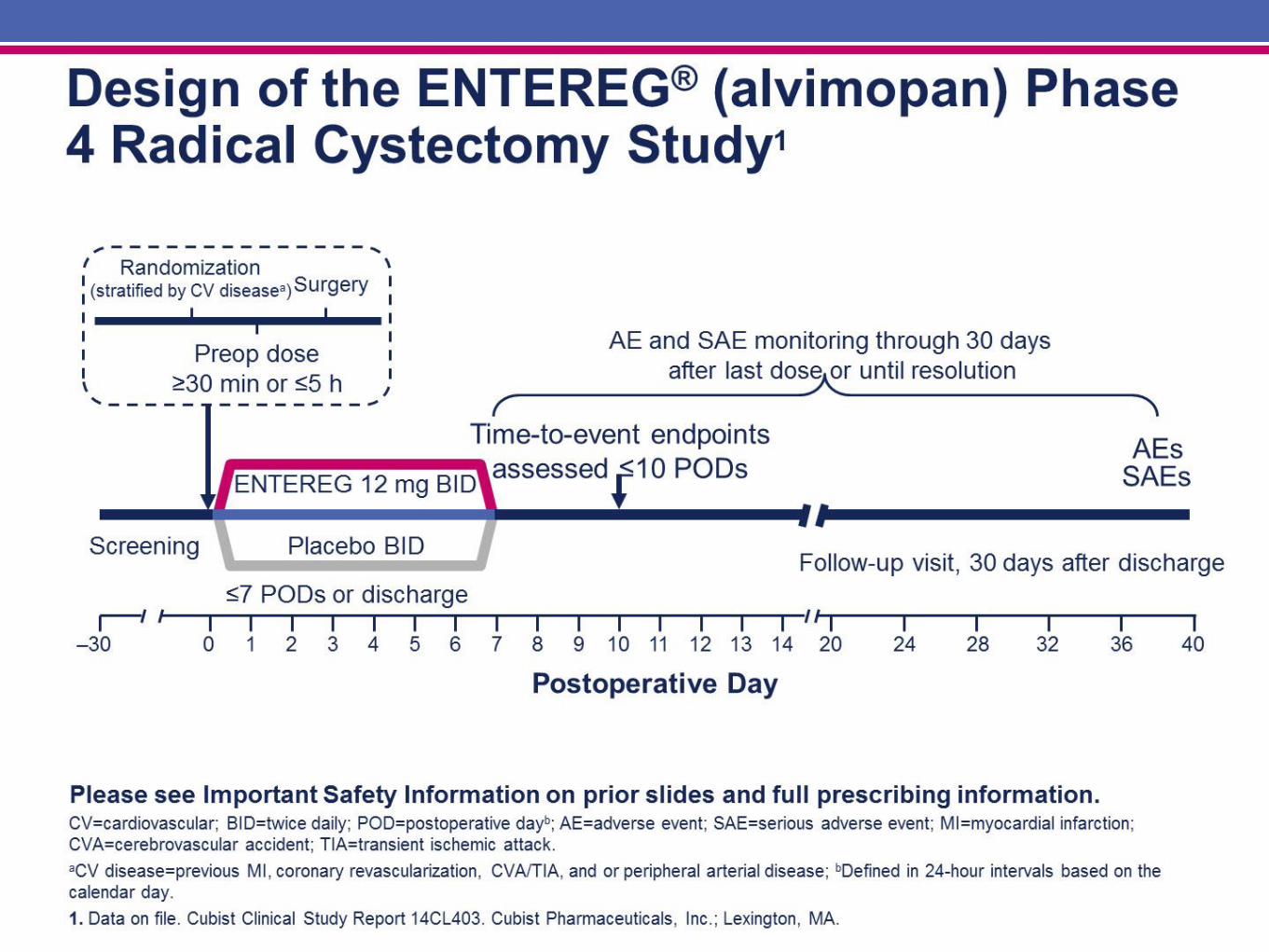


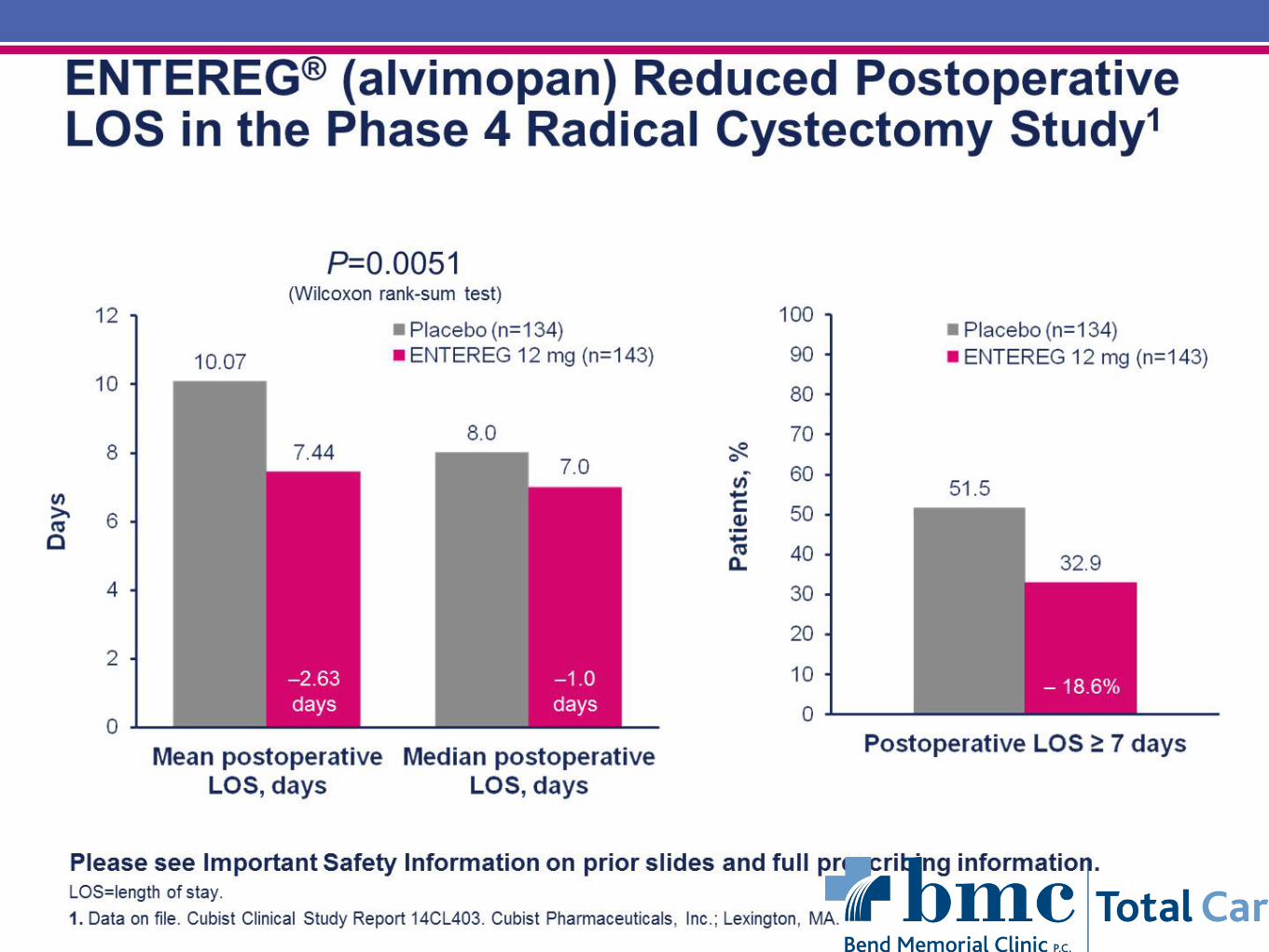

Cystectomy Trial



Great Article





Survey
Pain





Elements of ERAS
• Pre-OP
• Intra-OP
• Post-OP

Develop Clinical Specifics
and Standardization of Care
Clinic
Prep
Inpatient and ICU unit
PACU (pain control and mobilization)
Post-op pain control plan

Factors Influencing Patient Recovery

Benefits
44

Example of Enhanced Recovery Elements
45
Referral from
Primary Care
Pre-
Operativ
e
Admissio
n
Intra-
Operative
Post-
Operativ
e
Follow
Up
• Optimised health /
medical condition
• Informed decision making
• Pre operative health &
risk assessment
• PT information and
expectation managed
• DX planning (EDD)
• Pre-operative therapy
instruction as appropriate
• Minimally invasive surgery
• Use of transverse incisions
(abdominal)
• No NG tube (bowel surgery)
• Use of regional / LA with
sedation
• Epidural management (inc
thoracic)
• Optimised fluid
management Individualised
goal directed fluid therapy
• Planned mobilisation
• Rapid hydration &
nourishment
• Appropriate IV therapy
• No wound drains
• No NG (bowel surgery)
• Catheters removed early
• Regular oral analgesia
• Paracetamol and NSAIDS
• Avoidance of systemic
opiate-based analgesia
where possible or
administered topically
• Admission on day
• Optimised Fluid
Hydration
• CHO Loading
• Reduced starvation
• No / reduced oral bowel
preparation ( bowel
surgery)
• DX when criteria met
• Therapy support (stoma,
physio)
• 24hr telephone follow up
• Optimising pre operative
haemoglobin levels
• Managing pre existing co
morbidities e.g. diabetes

The Bible

Pre-Op
• Preadmission counseling
• Fluid and Carbohydrate Loading
• No Prolonged Fasting
• No/Selective Bowel Prep

Pre-Op
• Antibiotic Prophylaxis
• Thromboprophylaxis
• No Pre-Meds

Intra-Op
• Short-acting anesthetic agents
• Epidural or other regional block
• PONV prophylaxis
• Limit Fluids

Intra-Op
• No NGT
• No Drains
• Lap Approach if Possible
• Normothermia
Post-Op
• Early Removal of Foley
• Early Feeding
• Early Ambulation
• Limit IVF

Post-Op
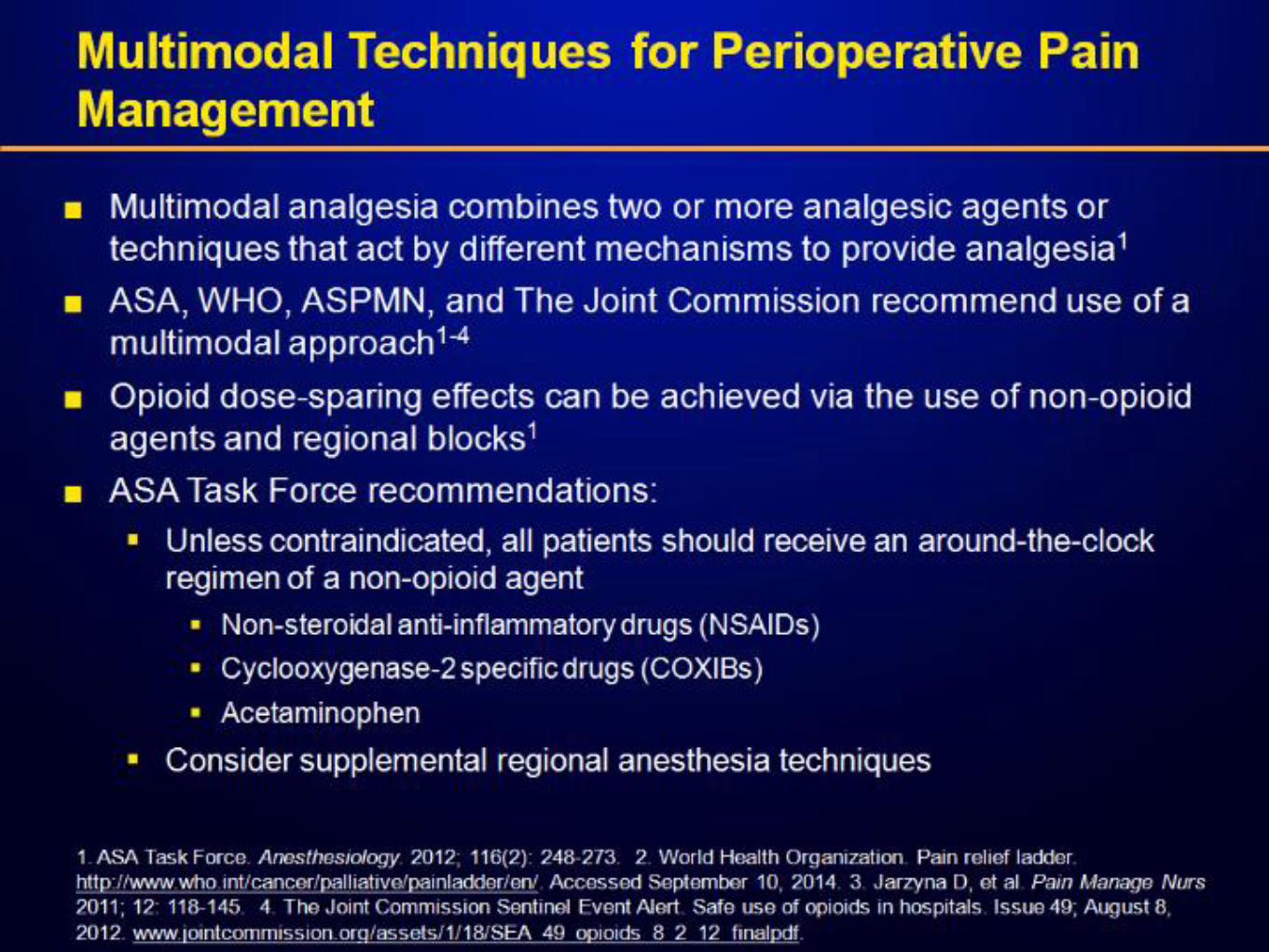
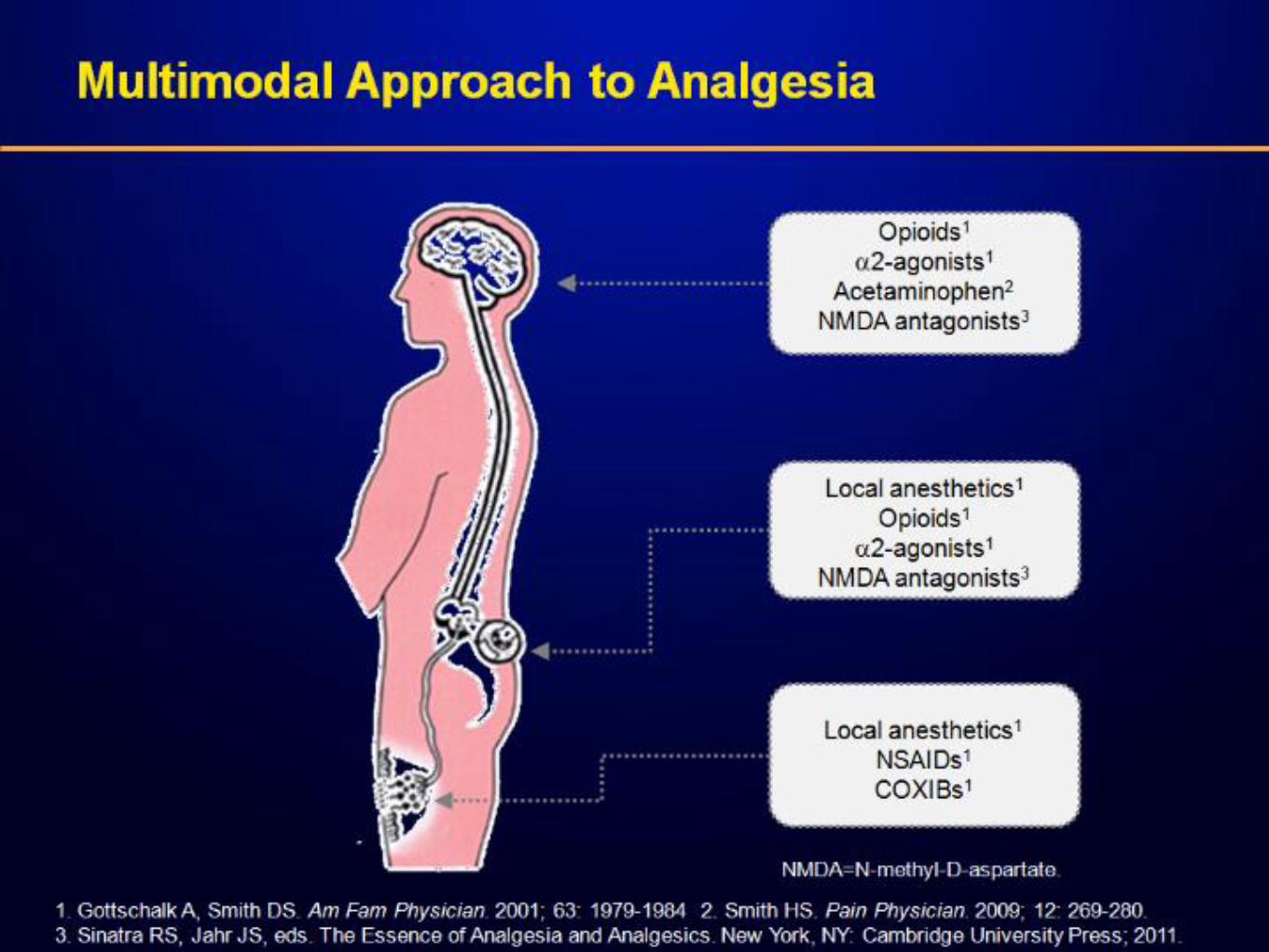
• Multi-Modal pain management
• Epidural
• Non-Opioids

Complete Guidelines

ERAS Results
Type of Operation Duration of stay
Carotid endarterectomy 1-2 days
Lung lobectomy 1-2 days
Prostatectomy 1-2 days
Colectomy 1-3 days
Aortic Aneurysm 3-4 days

Incorporation of Alvimopan (Entereg®)
as Part of Perioperative Management
of Patients Undergoing Colectomy:
1 Surgeon’s Experience
Timothy L. Beard, MD; Bob Cutter, PharmD;
Emily Meeks; Karla Lichter, RN, CCRC
Bend Memorial Clinic, Bend, Oregon

Study Design
Independent study of patients undergoing open colectomy • All patient data from same surgeon
Conducted at Bend Memorial Clinic • Multispecialty medical clinic with 85 physicians and
600 staff members
Patients in 2 of 3 arms received a standardized accelerated postoperative care pathway (post-pathway or alvimopan + pathway)
Based on alvimopan phase III clinical trials1-4
•Removal of NGT at the end of surgery or morning before first postoperative dose of alvimopan •Early ambulation (initiated POD 1) •Early diet advancement (liquids offered POD 1, solids offered POD 2)
Abbreviations: NGT, nasogastric tube; POD, postoperative day.
1. Wolff BG, et al. Ann Surg. 2004;240:728-734.
2. Delaney CR, et al. Dis Colon Rectum. 2005;48:1114-1125.
3. Viscusi ER, et al. Surg Endosc. 2006;20:64-70.
4. Ludwig K, et al. Arch Surg. 2008;143(11):1098-1105

Study Design
Treatment arms
Type of
analysis
Enrollment
dates
Patients
(n)
Pre-pathway Retrospective 10/04 - 10/05 19
Post-pathway Retrospective 3/07 - 9/08 26
Alvimopan +
pathway
Prospective
7/08 - 5/09
25
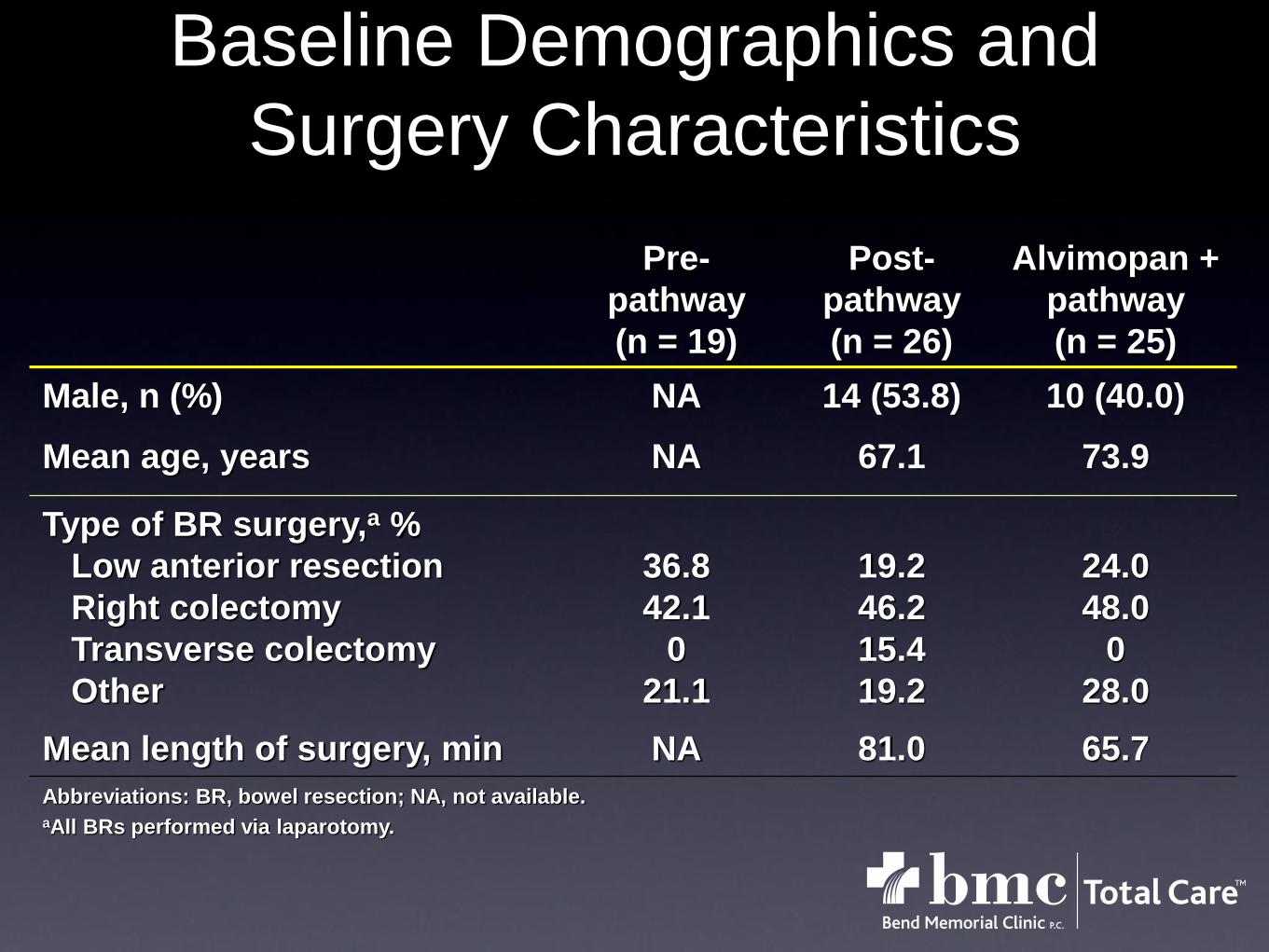
Baseline Demographics and
Surgery Characteristics
Pre-
pathway
(n = 19)
Post-
pathway
(n = 26)
Alvimopan +
pathway
(n = 25)
Male, n (%) NA 14 (53.8) 10 (40.0)
Mean age, years NA 67.1 73.9
Type of BR surgery,a %
Low anterior resection
Right colectomy
Transverse colectomy
Other
36.8
42.1
0
21.1
19.2
46.2
15.4
19.2
24.0
48.0
0
28.0
Mean length of surgery, min NA 81.0 65.7
Abbreviations: BR, bowel resection; NA, not available. aAll BRs performed via laparotomy.

Alvimopan Reduced Length
of Stay (LOS)
7.57.1
5.3
0
1
2
3
4
5
6
7
8
9
10
Pre-pathway Post-pathway Alvimopan +
pathway
Mean
LO
S,
days
• LOS > 5 days was observed in 84%, 77%, and 32% of patients in the pre-pathway, post-pathway, and alvimopan + pathway groups, respectively
P = 0.5724 P = 0.0040
P = 0.0005
Unpaired 2-tailed P values were calculated using a t-test.

Alvimopan Reduced Time to First
Postoperative Bowel Movement
4.6
3.6
0
1
2
3
4
5
Post-pathway Alvimopan + pathway
Mean
tim
e t
o f
irst
po
sto
pera
tive B
M,
days
Note: Time to first bowel movement (BM) was not collected for patients in the pre-pathway group.
Unpaired 2-tailed P values were calculated using a t-test.
P = 0.0084

Alvimopan Reduced the Need for
Nasogastric Tube (NGT) Reinsertion
and Readmissiona
0
19.2
0
5
10
15
20
Pa
tie
nts
re
qu
irin
g N
GT
, %
0
7.7
0
2
4
6
8
10
Pa
tie
nts
re
qu
irin
g r
ea
dm
iss
ion
, %
Post-
pathway
Alvimopan
+ pathway
Post-
pathway
Alvimopan
+ pathway
aThere was 1 death in the alvimopan + pathway group; this was attributed to sepsis.
Proportion of patients requiring NGT insertion or readmission was not collected for patients in the pre-
pathway group.
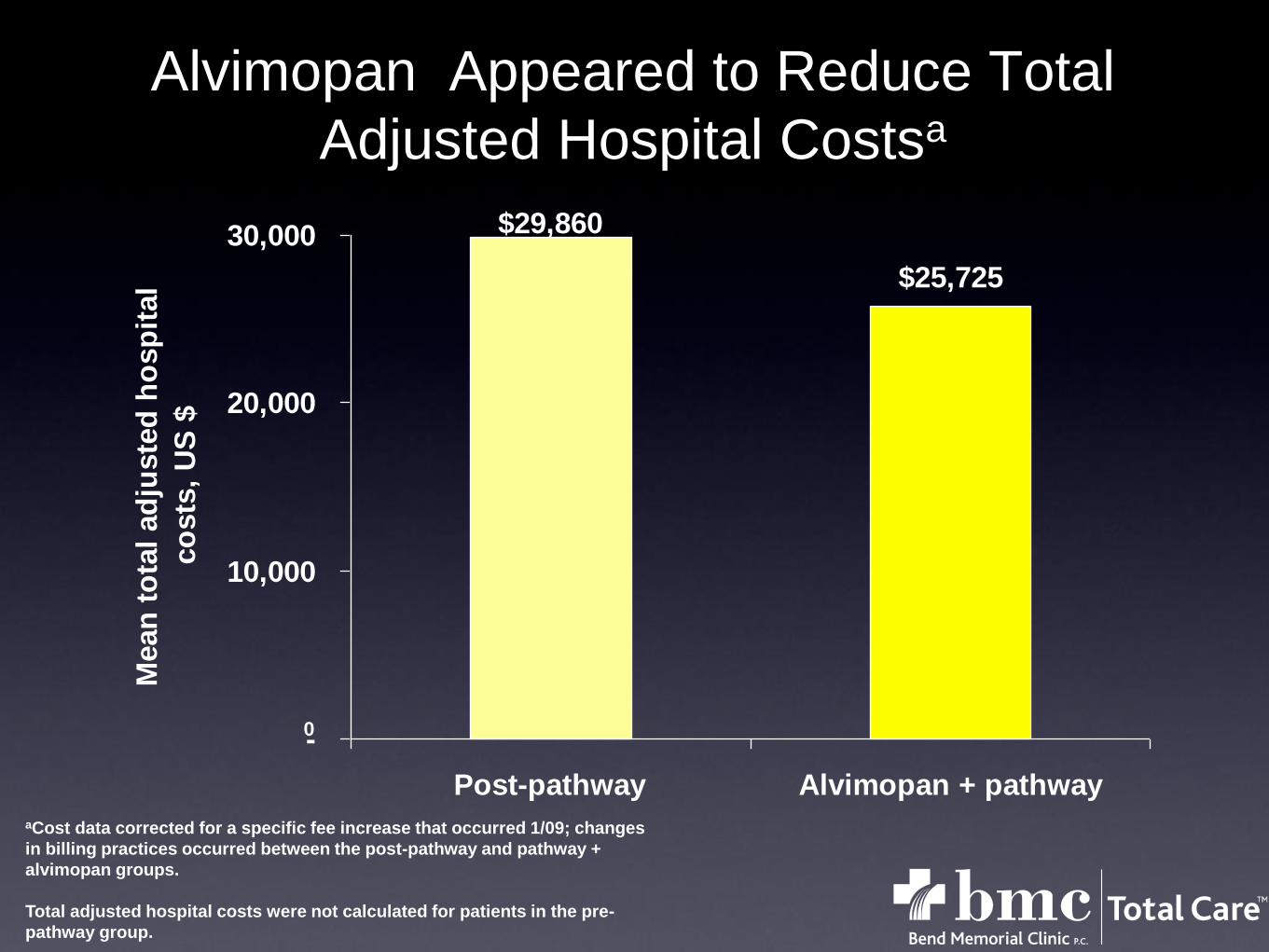
Alvimopan Appeared to Reduce Total
Adjusted Hospital Costsa
$29,860
$25,725
-
10,000
20,000
30,000
Post-pathway Alvimopan + pathway
Mean
to
tal
ad
juste
d h
osp
ital
co
sts
, U
S $
aCost data corrected for a specific fee increase that occurred 1/09; changes
in billing practices occurred between the post-pathway and pathway +
alvimopan groups.
Total adjusted hospital costs were not calculated for patients in the pre-
pathway group.
0

Byron Holloway MS 4
WesternU/COMP
Timothy L. Beard MD, FACS
Bend Memorial Clinic
Alvimopan Use in
Laparoscopic Bowel
Resections

Retrospective Review
BMC is a multi-specialty clinic with over 80
providers and 5 general surgeons
Data collected from 2009 - early 2012
Extensive chart review
Bend Memorial Clinic Study

37 pts in Entereg group
44 pts in control group
No hand assisted cases
All done by board certified surgeons
Mix of right and left colon resections
Data

N=37
Average age 61.5 range 33-93
Ave length of stay 4.24 days range 3-6
Ave time to first BM 2.62 days range 1-5
No SAEs in this group
Alvimopan Group
N=44
Ave. age 64.02 range 33-85
Ave. length of stay 4.84 days range 3-8
Ave. time to first BM 3.57 days range 2 to 6
No SAEs in this group
One pt. excluded from this group.
Control Group

Length of stay decreased 4.81 to 4.25
P value is 0.0075
Statistically significant difference
Length of Stay

BMC Outcomes with
Laparoscopic Colon Resections

Length of hospital stay (days)
Experimental group= Enhanced Recovery After Surgery (ERAS) Control = Traditional Care (TC)
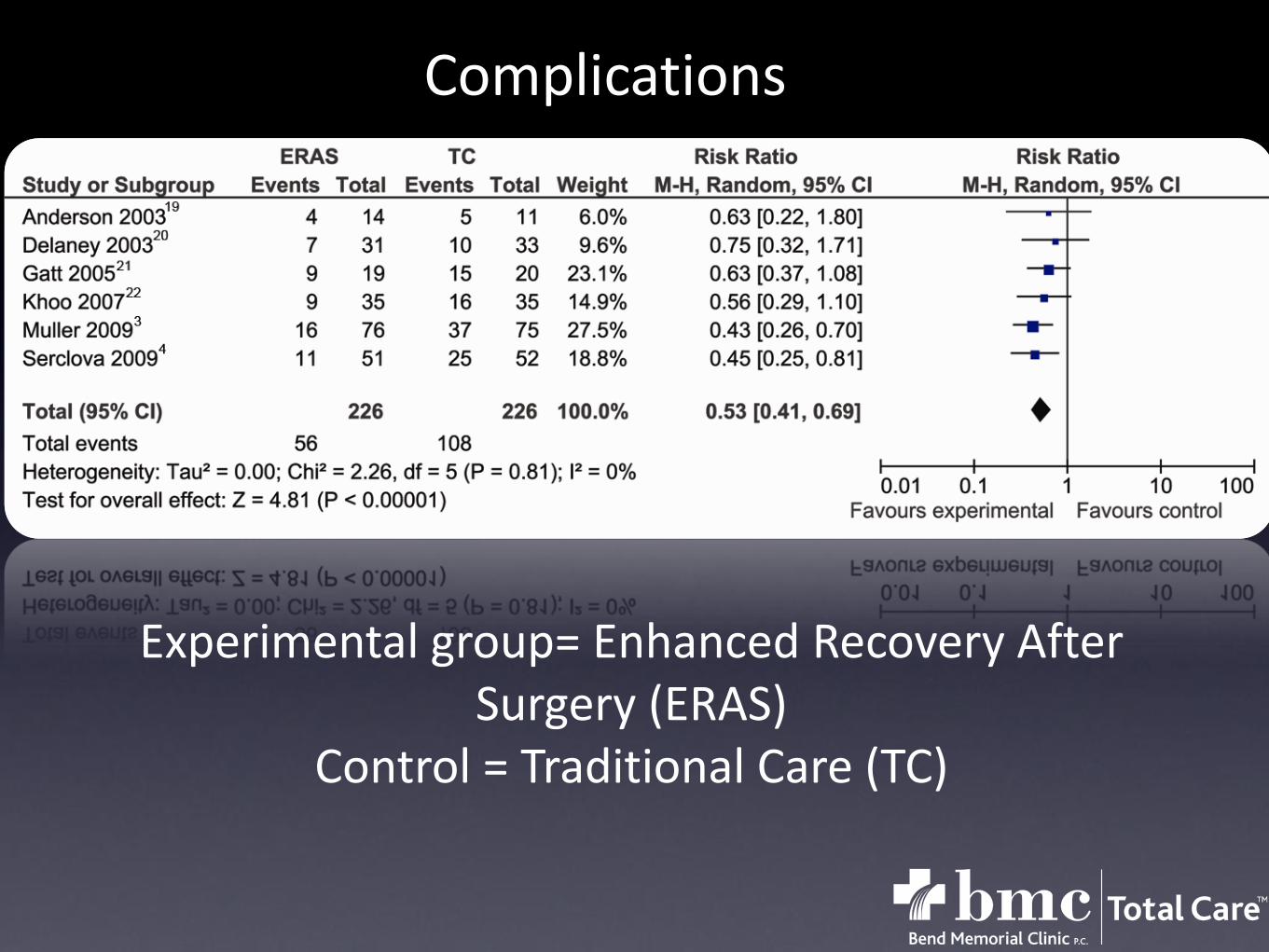
Complications
Experimental group= Enhanced Recovery After Surgery (ERAS)
Control = Traditional Care (TC)

Readmissions (days)
Experimental group= Enhanced Recovery After Surgery (ERAS)
Control = Traditional Care (TC)
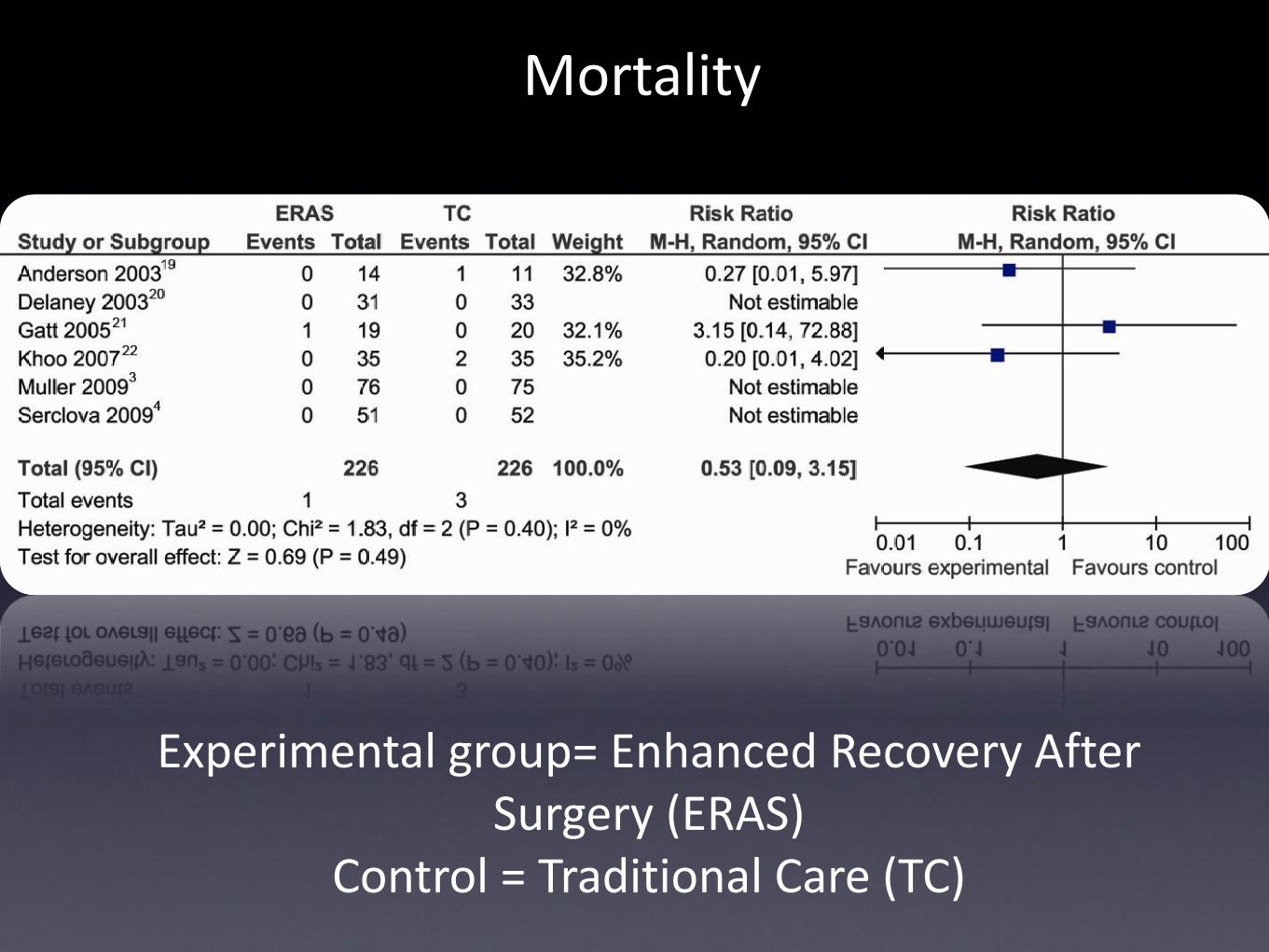
Mortality
Experimental group= Enhanced Recovery After Surgery (ERAS)
Control = Traditional Care (TC)

Results



Website
Can we do this at SCMC?
• Barriers
• Cost
• Physicians
• Admin
We Can Do IT
• ERAS website
• ERAS Society help
Well Rounded Team
Questions?

















