57
The Mouth – Body Connection: Oral Health and Systemic Health Connections

The Mouth – Body Connection: Oral Health and Systemic Health Connections
The Mouth: An Open Pathway into the Body

A Window for Disease Manifestations
Medication Induced Hyperplasia

Learning Objectives
By the end of this seminar, participants will be able to:
• Discuss the prevalence and sequelae
of oral disease
• Recognize the inter‐relationships between oral and systemic disease

5
The Big Picture“You are not healthy without
good oral health…” C. Everett Koop, MD
• Dental care: the most common unmet health need• Oral disease can severely affect systemic health• Profound disparities in oral health and access to
care exist at all ages• Much oral disease is preventable (or at least
controllable)

6
Prevalence• Dental caries is the most
common chronic disease of childhood
5 times more common than
asthma
Affects 50% of low income children
Affects up to 70% of Native
American children
• Periodontitis
affects 19% of adults aged 25‐44

7
Prevalence• 30,000 oral cancers
diagnosed annually
8000 die
Diagnosis is often late

Prevalence of Geriatric Oral Health Issues
• 50% of the elderly (age >65) perceive their dental health as poor or very poor
• 33% of the elderly had untreated cavities
• Low income elderly suffer more severe tooth loss than their wealthy counterparts

Prevalence of Geriatric Oral Health Issues
• Edentulism: – affects 1/3 of those over age 65; – 50% of those in nursing homes
• Periodontitis in 41% of the elderly

Photos: Donald Greiner DDS MS, ICOHP
10
Physical, Economic and Social Consequences
• Mounting evidence of aggravating
effects on systemic conditions
• Oral pain– Poor school performance in children
– Work loss in adults
– Poor chewing and poor nutrition– Costly emergency department visits
• Dental decay and tooth loss– Aesthetics and self‐image
– Speech and language development
– Costly restoration

11
The Disconnect…
• Children are 2.5 times more likely to lack dental coverage than medical coverage
• Only 43% of elderly visit the dentist
• Dentists per capita appear to be declining, especially those that accept Medicaid and see
infants

12
The Disconnect…
• More than 90% of physicians think oral health should be addressed at well visits, yet greater than
50% have little or no oral health training.
• Little communication and cooperation between medical and dental providers

So who should take care of a patient’s oral health?
Who is responsible for
the patient’s oral health?

Inter‐Relationships Between Oral and Systemic Health and Disease
Oral Systemic

15
Mechanisms• Behavioral• Nutritional• Iatrogenic• Lack of priority• Direct bacterial extension• Inflammatory

Photo: Ellen Eisenberg DMD
16
Case #155 year‐old man has a “sore”
on his tongue.
He is a 25 pack‐year smoker and drinks daily.
Photos: Brad Neville DDS, James Cecil, DMD, MPH
17
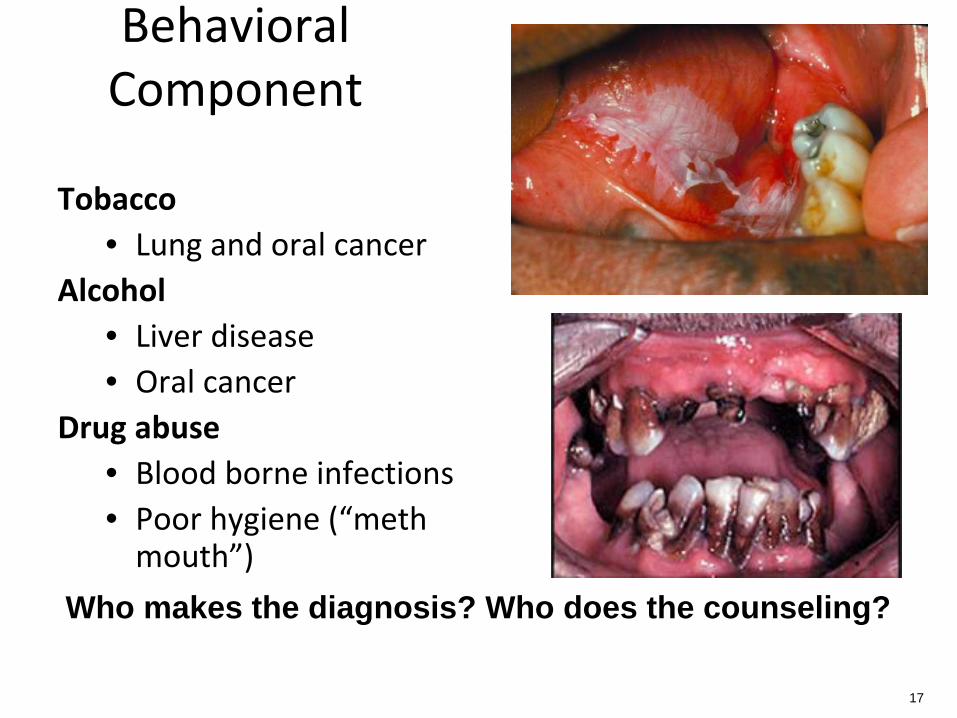
Behavioral Component
Tobacco • Lung and oral cancer
Alcohol• Liver disease• Oral cancer
Drug abuse• Blood borne infections• Poor hygiene (“meth
mouth”)
Who makes the diagnosis? Who does the counseling?

Photos: Robert Henry DMD MPH
18
Case #275 year old man is brought in by his family who are
concerned about poor appetite and progressive weight loss despite his new dentures.

19
Nutritional Component• Cariogenic diet in children and adults• Obesity• Poor dentition, mechanical issues and dental pain
interfere with eating
Children, special needs patients, and the elderly are
particularly vulnerable
Poor eating may result in malnutrition
Elderly failure‐to‐thrive: think poor fit of dentures
A lot of counseling for one office, one provider

Photo: John McDowell DDS
20
Case #3 65 year old woman on multiple medications for
depression and cardiovascular disease develops severe caries

Photo: John McDowell DDS
21
Iatrogenic Component: Xerostomia
• Decreased saliva promotes caries and periodontal disease
• Many medications reduce salivary flow
• steroids• antihistamines• diuretics• antihypertensives• anticholinergics• antidepressants
Need for dental to address medications?

Photo: Ellen Eisenberg DDS
22
Iatrogenic: Other• Gingival hyperplasia
–phenytoin• Osteonecrosis
– IV bisphosphonates• Stomatitis and mucositis
– cancer chemotherapy– radiation therapy
• Candidiasis–steroids
• Periodontal disease–immunosuppressives
Need for dental to address medications?

23
Case #5
4 year old goes to bed
with a toothache and
awakens crying and
feverish…
Photo: ICOHP

24
Direct Bacterial Extension
• Intraoral abscesses• Sinusitis• Facial cellulitis• Periorbital cellulitis• Bacteremia and its consequences
• Brain abscess• Aspiration pneumonia
Photo: ICOHP
Infections prompt medical and dental to interact!

Photo: Efthimia Ioannidou, DDS MDS
25
Case #652 year old woman with previously well‐
controlled type 2 diabetes has increasing hyperglycemia

26
The Role of Inflammation
Toxins
Neutrophils
Macrophages
Anaerobic bacteria in
plaque
Circulating inflammatory mediators

27
Diabetes• Poor glycemic control is associated with a threefold
increased risk of having periodontitis in diabetics vs controls
• Diabetics with good glycemic control have no significant increased risk of periodontal disease
• Chronic infection (like periodontal disease) worsens glucose control
• Treatment of periodontal disease results in a 10‐20% improvement in glycemic control

28
Coronary Heart Disease• CHD and periodontitis are associated, but
causation is not clear
• Inflammatory cytokines implicated in atherogenesis are also produced in periodontitis
• Systemic antibody response to periodontitisis
associated with CHD
• Smoking is associated with both CHD and periodontitis

Pregnancy: Preterm Birth (PTB) and Low Birth Weight (LBW)
• Association between periodontitis and PTB and LBW is confirmed; however RCT studies of treatment
show no change in outcome
• Periodontal treatment is safe
in pregnancy: No bad prenatal outcomes in any studies
• Women felt better
• Need to study preconception
interventions

National Institute of Dental and Craniofacial Research
• Scientists are using an ever‐growing array of sophisticated analytical tools and imaging systems to
test and study normal function and diagnose disease through oral cells and fluids.
• New tests are constantly being developed to make oral tissues and fluids an increasingly accurate mirror
of health and sickness.

How can medical and dental providers work together:
Practical Solutions

Interdisciplinary Care• Set up in same building and conduct meetings
together (e.g. a community health center)
• Have a professional perform “visiting”
consults (e.g. hygienist in MD office once a week)
• Conduct regular in‐services for others
• Create lists for proper referrals – know who does what, what insurance they take, what patient
populations they see, etc.

Work synergistically
• Support cross pollination of ideas:
Dental supporting fluoride varnish done by
medical providers
Medical supporting dental doing oral cancer screens, blood pressure monitoring, nutrition
advice
More interprofessional health
education in schools/residencies

Take Home Messages
• Oral and systemic health are interrelated
• Oral exams must be systematic and complete
• Certain groups are at particular risk for oral problems
• Medical providers can have a major impact on the oral health of individuals and communities

Oral Health, Systemic Health and Pharmacology
Sandra Leal, PharmD, CDE
Director of Clinical Pharmacy, El Rio Health Center

Summary
• Oral health coupled with systemic health are well understood to be foundations for improved
health outcomes and quality of life for patients. This presentation will address the important
opportunity to understand the linkage between oral and systemic health, as well as the value of medication review to improve common concerns
for patients. Strategies for collaboration between dental providers, medical providers, and patients will be explored to identify and resolve common
barriers to improve both oral and systemic health.

Assessment Questions
1. The following are common ways medication affect dental health:
a.Bleeding gumsb.Dry mouthc.Bitter tasted.Metallic tastee.All of the above
2. Herbal medication is not usually associated with oral health affects.
a.Trueb.False

Objectives
At the completion of this program, participants will be able to:
•Recognize the inter‐relationships between oral and systemic disease
•Highlight the role of the primary care clinician in promoting oral health
•Describe how medication can affect oral health•Explain strategies for collaborating with the health
care team to optimize medication use with oral health

Abnormal Bleeding
• Reduced blood clotting from aspirin and anticoagulants such as warfarin
• Medications that might contribute– Aspirin
• Lessens ability for blood to clot– Warfarin (Coumadin)– Combination of anticoagulants– Chemotherapy
• Kills normal cells in mouth– Hormones
• Progesterone cause inflamed gum tissues due to the body's
exaggerated reaction to the toxins produced from plaque

Taste‐Altering Medication
• Cardiovascular agents• Chemotherapy
• Central nervous system stimulants
• NSAIDs• Respiratory inhalants• Smoking‐cessation products
• Nicotine skin patches
Taste dysfunction can be caused by damage or alteration to any part of the nerve pathway from the taste buds

Enlarged Gum Tissue
• Antiseizure medication such as phenytoin
• Immunosuppressants
• Calcium channel blockers
The exact mechanism of gingival hyperplastic reaction is unknown. Some theories includedirect stimulatory effect on fibroblast proliferation and morphologic structures, poor oral
hygiene, and direct effect on mast cells.
SING MED J. 1988; 29: 498 – 503. Source: http://smj.sma.org.sg/2905/2905smj18.pdf

Estimated Prevalence of Drug‐Associated Gingival Enlargement
According to the Most Frequently Reported Prevalence Rate
J Periodontol 2004;75:1424‐1431. Source: http://www.perio.org/resources‐products/pdf/45‐gingivalenlarge.pdf

Dry Mouth
• Antihistamines• Decongestants• Painkillers• Blood pressure medications• Muscle relaxants • Drugs for urinary incontinence• Antidepressants• Parkinson’s medication
Anticholinergic properties that generally cause decreased saliva
production




Herbs that Cause Dry Mouth
• Ephedra (ma huang): appetite suppressant
• St. Johns Wort: antidepressant
• Valerian: insomnia


Oral Fungal Infections
• Oral inhalers for asthma
• Antibiotics• Chemotherapy
• Steroids
Balance upset of microorganisms in the mouth
Treatment of Side Effects
• Reduction in dosage of the drug or changing to alternative drugs may help
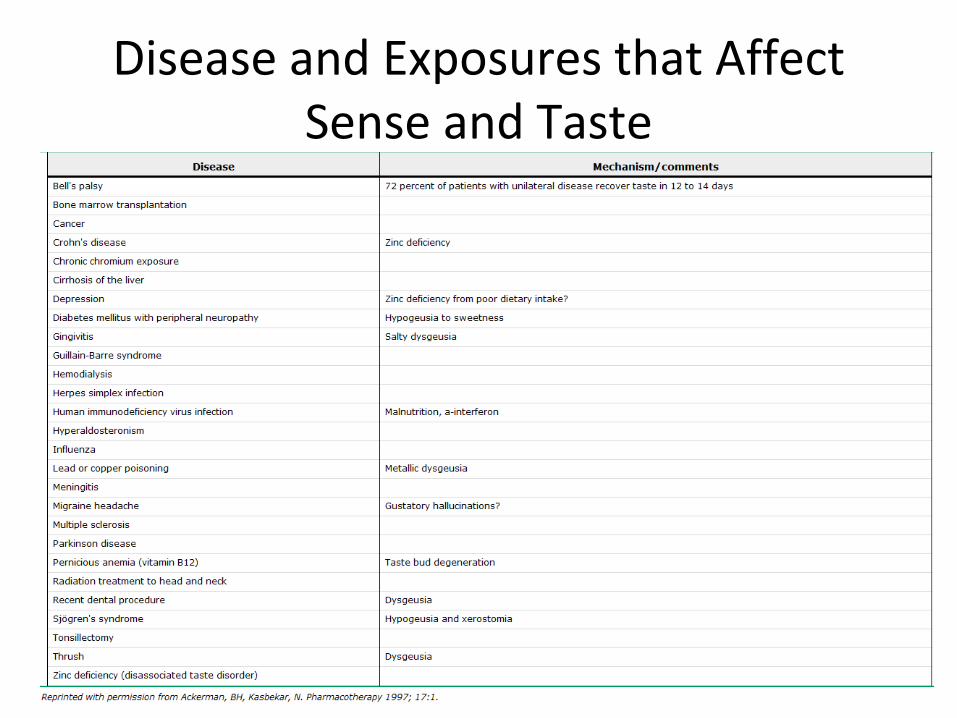
Disease and Exposures that Affect Sense and Taste

Conditions and Treatments that can Affect the Physiology of the Oral
Cavity

Impact of Medication on Oral Health
• Many medications can have negative impact on oral health
– Medication review is key to addressing problems• Include vitamins
• Minerals
• Herbal products• Over‐the‐counter preparations
Collaboration Strategies
• Communication
• Review medical conditions
• Medication review at all care transition points
• Update list of medications at all appointments
• Educate providers and patients about possibility of drug related effects

Example of Collaborative Opportunities
• Explore opportunities to create affiliations between medical and dental providers
– Research– Continuing education
• ie guideline updates– Presentations– Health promotion opportunities
– Committee work• ie P&T

Patient Centered Medical Home (PCMH)


















