_____________________________ Anca Maria Raducanu et al 91 CASE REPORTS abstract Received for publication: Feb. 22, 2008. Revised: May 19, 2008. rEZUMat Department of Pediatric Dentistry, Faculty of Dental Medicine, Carol Davila University of Medicine and Pharmacy, Bucharest Correspondence to: Anca Maria Raducanu, 12 Ionel Perlea Str., Bucuresti, Tel. +40-21-314.20.80 Email: [email protected]INtrODUctION The cerebral palsy (CP) is a term that describes a constellation of neuro-muscular non-contagious and non-evolutionary disturbances, caused by a brain lesion in the early stages of its development (in the first 5 years of life). Spastic tetraparesis represents the most severe form of spastic cerebral palsy. The CP produces handicapping changes of movement and posture. 1-8 OraL MaNIFEstatIONs OF cErEbraL PaLsY - tHE sPastIc tEtraParEsIs tYPE: a LItEratUrE rEVIEW aND cLINIcaL casEs Anca Maria Raducanu, Irina Cristea, Victor I. Feraru Introduction: The cerebral palsy (CP) is a term describing a constellation of neuro-muscular disturbances, non-contagious and non-progressive, that are determined by brain damage in its early stages of development. Spastic tetraparesis represents the most severe form of spastic cerebral palsy. Compared to normal children, those with cerebral palsy are more susceptible to oro-dental diseases such as caries, gingivitis, malocclusion, bruxism, deglutition, mastication and speaking disorders, etc. Aim: To review the literature regarding the general and oral manifestations of cerebral palsy with tetraparesis and to present two clinical cases. Method: Two clinical cases with spastic tetraparesis, of different severity and etiology are presented. Discussions and conclusions: Both cases with spastic tetraparesis present typical CP general and oral features. The most important therapeutic goals were the control of the oral bacterial plaque with a consecutive reduction of dental disease and the change of the negative behavior pattern in both cases. Dental treatment could be performed without sedation or general anesthesia in both cases. Physical and mechanical restraint may me necessary at times, when serious problems in the safe maneuvering of the instruments appear. Dental treatment in patients with CP can be performed, in certain situations, even in a dental office with average conditions and equipment. Key Words: spastic tetraparesis, cerebral palsy, muscular spasticity and tonicity Introducere: Paralizia cerebral\ este un termen care descrie o constela]ie de deregl\ri neuro-musculare, necontagioase [i neevolutive, provocate de lezarea creierului n stadiile precoce ale dezvolt\rii sale. Tetrapareza spastic\ reprezint\ forma cea mai grav\ a paraliziei cerebrale spastice. Copiii cu paralizie cerebral\ sunt mai susceptibili la unele boli buco-dentare fa]\ de copiii normali. Scop: Sistematizarea informa]iilor din literatura de specialitate cu privire la manifest\rile generale [i orale ale paraliziei cerebrale - forma cu tetraparez\, urmat\ de prezentarea a dou\ cazuri. Metod\: Sunt prezentate dou\ cazuri clinice cu tetraparez\ spastic\, ale c\ror semne [i simptome generale [i orale se nscriu n tabloul clasic al paraliziei cerebrale spastice, descris n literatura de specialitate. Primul caz este al unei feti]e de 6 ani, cu tetraparez\ spastic\ provocat\ de hipoxia la na[tere, cazul al doilea fiind o feti]\ de 11 ani, cu acela[i diagnostic, dar la care nu s-au putut depista factorii etiologici ai bolii. Pentru prezentarea acestor cazuri au fost folosite date din: anamnez\, copia fi[ei generale de s\n\tate ntocmit\ de medicul curant neurolog, date din examenul clinic precum [i rezultatele investiga]iilor complementare generale [i orale efectuate. Rezultate [i concluzii: Conduita terapeutic\ aplicat\ celor dou\ paciente atrage aten]ia, pe de o parte, asupra dificult\]ilor ntmpinate iar, pe de alt\ parte, asupra faptului c\ aceste greut\]i pot fi dep\[ite chiar [i n condi]iile unui cabinet stomatologic obi[nuit care nu este dotat pentru practicarea anesteziei generale sau a inhalosed\rii. Cuvinte cheie: tetraparez\ spastic\, paralizie cerebral\, spasticitate [i tonicitate muscular\ The prevalence of CP ranges from 1 to 4 children /1000 alive new-born. 3,6,8 The etiology of CP is multifactorial and includes prenatal causes (genetic diseases, embryonic anomalies), perinatal (hypoxia, Rh incompatibility, premature birth, underweight at birth, etc.) and postnatal (infections, trauma, etc.). In 30% of the cases, the risk factors can be traced. The frequency is 10 times higher in premature children and 25 times higher in small-for-birth children. 1,2,6,8 The CP classification includes four types: spastic, dyskinetic, hypotonic, and mixed, the spastic type being the most common one. Spastic tetraparesis represents the most severe form of spastic cerebral palsy in which the motor disturbance affects the whole body: face, trunk, legs, arms, which usually puts the patient in a wheelchair. 4,9 General manifestations of the CP are diverse, ranging from minimal limitations of the movement, that don’t call for treatment, to severe alteration of
Transcript
_____________________________Anca Maria Raducanu et al 91
CASE REPORTS
abstract
Received for publication: Feb. 22, 2008. Revised: May 19, 2008.
rEZUMat
Department of Pediatric Dentistry, Faculty of Dental Medicine, Carol Davila University of Medicine and Pharmacy, Bucharest
The cerebral palsy (CP) is a term that describes a constellation of neuro-muscular non-contagious and non-evolutionary disturbances, caused by a brain lesion in the early stages of its development (in the first 5 years of life). Spastic tetraparesis represents the most severe form of spastic cerebral palsy. The CP produces handicapping changes of movement and posture.1-8
OraL MaNIFEstatIONs OF cErEbraL PaLsY - tHE sPastIc tEtraParEsIs tYPE: a LItEratUrE rEVIEW aND cLINIcaL casEs
Anca Maria Raducanu, Irina Cristea, Victor I. Feraru
Introduction: The cerebral palsy (CP) is a term describing a constellation of neuro-muscular disturbances, non-contagious and non-progressive, that are determined by brain damage in its early stages of development. Spastic tetraparesis represents the most severe form of spastic cerebral palsy. Compared to normal children, those with cerebral palsy are more susceptible to oro-dental diseases such as caries, gingivitis, malocclusion, bruxism, deglutition, mastication and speaking disorders, etc. Aim: To review the literature regarding the general and oral manifestations of cerebral palsy with tetraparesis and to present two clinical cases. Method: Two clinical cases with spastic tetraparesis, of different severity and etiology are presented. Discussions and conclusions: Both cases with spastic tetraparesis present typical CP general and oral features. The most important therapeutic goals were the control of the oral bacterial plaque with a consecutive reduction of dental disease and the change of the negative behavior pattern in both cases. Dental treatment could be performed without sedation or general anesthesia in both cases. Physical and mechanical restraint may me necessary at times, when serious problems in the safe maneuvering of the instruments appear. Dental treatment in patients with CP can be performed, in certain situations, even in a dental office with average conditions and equipment.Key Words: spastic tetraparesis, cerebral palsy, muscular spasticity and tonicity
Introducere: Paralizia cerebral\ este un termen care descrie o constela]ie de deregl\ri neuro-musculare, necontagioase [i neevolutive, provocate de lezarea creierului n stadiile precoce ale dezvolt\rii sale. Tetrapareza spastic\ reprezint\ forma cea mai grav\ a paraliziei cerebrale spastice. Copiii cu paralizie cerebral\ sunt mai susceptibili la unele boli buco-dentare fa]\ de copiii normali. Scop: Sistematizarea informa]iilor din literatura de specialitate cu privire la manifest\rile generale [i orale ale paraliziei cerebrale - forma cu tetraparez\, urmat\ de prezentarea a dou\ cazuri. Metod\: Sunt prezentate dou\ cazuri clinice cu tetraparez\ spastic\, ale c\ror semne [i simptome generale [i orale se nscriu n tabloul clasic al paraliziei cerebrale spastice, descris n literatura de specialitate. Primul caz este al unei feti]e de 6 ani, cu tetraparez\ spastic\ provocat\ de hipoxia la na[tere, cazul al doilea fiind o feti]\ de 11 ani, cu acela[i diagnostic, dar la care nu s-au putut depista factorii etiologici ai bolii. Pentru prezentarea acestor cazuri au fost folosite date din: anamnez\, copia fi[ei generale de s\n\tate ntocmit\ de medicul curant neurolog, date din examenul clinic precum [i rezultatele investiga]iilor complementare generale [i orale efectuate. Rezultate [i concluzii: Conduita terapeutic\ aplicat\ celor dou\ paciente atrage aten]ia, pe de o parte, asupra dificult\]ilor ntmpinate iar, pe de alt\ parte, asupra faptului c\ aceste greut\]i pot fi dep\[ite chiar [i n condi]iile unui cabinet stomatologic obi[nuit care nu este dotat pentru practicarea anesteziei generale sau a inhalosed\rii.Cuvinte cheie: tetraparez\ spastic\, paralizie cerebral\, spasticitate [i tonicitate muscular\
The prevalence of CP ranges from 1 to 4 children /1000 alive new-born.3,6,8 The etiology of CP is multifactorial and includes prenatal causes (genetic diseases, embryonic anomalies), perinatal (hypoxia, Rh incompatibility, premature birth, underweight at birth, etc.) and postnatal (infections, trauma, etc.). In 30% of the cases, the risk factors can be traced. The frequency is 10 times higher in premature children and 25 times higher in small-for-birth children.1,2,6,8
The CP classification includes four types: spastic, dyskinetic, hypotonic, and mixed, the spastic type being the most common one. Spastic tetraparesis represents the most severe form of spastic cerebral palsy in which the motor disturbance affects the whole body: face, trunk, legs, arms, which usually puts the patient in a wheelchair.4,9
General manifestations of the CP are diverse, ranging from minimal limitations of the movement, that don’t call for treatment, to severe alteration of
the motor function, necessitating complex, long term, multidisciplinary treatment and permanent home care. Depending on which areas of the brain have been damaged, one or more of the following symptoms may occur: muscular rigidity or spasms, involuntary movements, difficulties of the “gross motor skills” (walking, running), difficulties of the “fine motor skills” (writing or doing up buttons, brushing the teeth ertc.). These may cause associated problems such as difficulties in feeding, poor bladder and bowel control, breathing problems etc.1-3,5,6,8
The patients with cerebral dysfunction may also display mental retardation, epilepsy, sensorial deficiencies (sight and hearing impairment), persistent primitive reflexes, attention-, memory-, learning- and emotional problems, language and speaking disturbances.8
OraL MaNIFEstatIONs
Children with CP display the same oral pathology as healthy persons. However, they present a higher susceptibility to several oro-dental diseases (dental caries, periodontal disease, dental trauma, malocclusion, bruxism, temporomandibular joint disorders, enamel hypoplasia, abnormal oral habits - tongue thrust, mouth breathing, drooling etc.) due to the abnormal neuromuscular coordination of the tongue, lips, and cheeks and to the low level and the reduced quality of the oral care.1,7
The treatment of CP is complex and multidisciplinary, consisting in general (kinetotherapy, surgical interventions, myorelaxants medication) and oral treatment (behavior management, prophylactic, curative).
casE rEPOrts
Two cases that present typical oral and general features for the spastic tetraparesis with uncontrolled extrapyramidal movements are described. The two cases present many general and oral similarities but also some differences.
The general common features are: - Neither of the patients displays hearing problems
or epilepsy;- The motor functions and the posture are
deteriorated at both patients but in different degrees, therefore they are unable to perform simple current activities, like washing, dressing, hair doing, feeding, teeth brushing etc., and necessitate permanent caretaking;
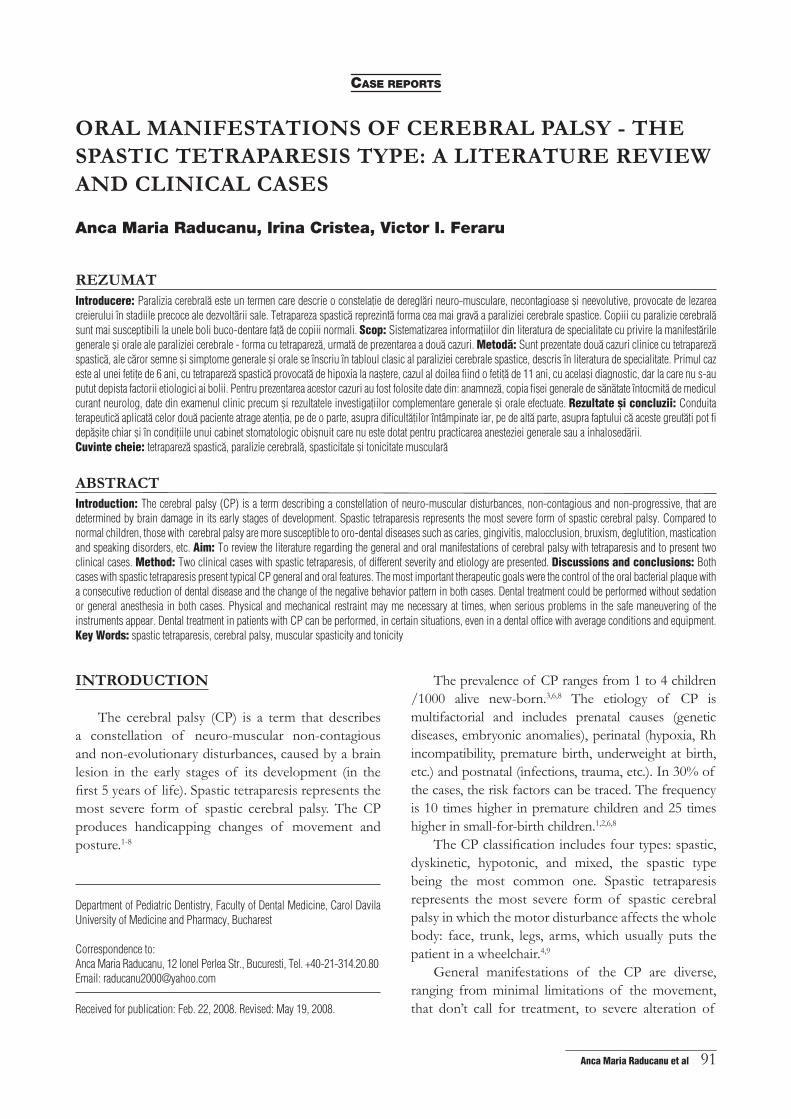
- Both patients presented tensed position of the head, spastic facial muscles, opened mouth and oral breathing. (Fig. 1)
Figure 1. Case 1. Opened mouth, protruded tongue position.
The oral features are:- Multiple dental caries (complicated and
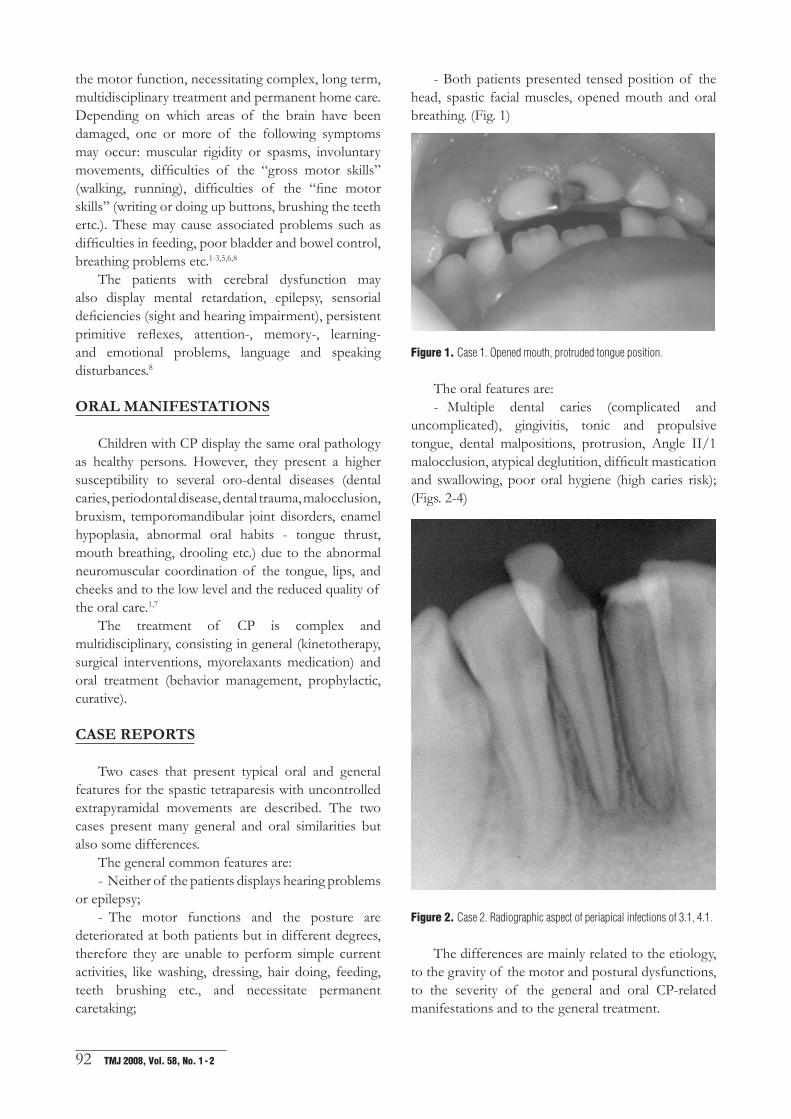
Figure 2. Case 2. Radiographic aspect of periapical infections of 3.1, 4.1.
The differences are mainly related to the etiology, to the gravity of the motor and postural dysfunctions, to the severity of the general and oral CP-related manifestations and to the general treatment.
_____________________________Anca Maria Raducanu et al 93
Figure 3. Case 1. Malocclusion, extensive caries on 5.1, 6.1.
Figure 4. Case 1. Opened mouth, Angle class II/1 malocclusion.
1. Patient I.N., 6 years and 4 months old, from Bucharest presenting at our Pediatric Dentistry Department at the initiative of her mother who has noticed the progressive destruction of several teeth.
- Etiology: perinatal causes (premature birth, low birth weight, natal hypoxia) and many risk factors. During pregnancy her mother had vaginal bleeding from 2.5 months up to 4 months, abnormal insertion of the placenta, risk of placenta detachment and abortion impendence. The birth was premature (at 31 weeks), in pelvian presentation, and the labor was long. At birth the girl had 2000 g and the Apgar score was initially 1, reaching 3 after 3 minutes. The neonatal jaundice was persistent, and associated with the fact that the girl did not gain weight and presented with nosocomial Klebsiella infection, blood transfusions were necessary.
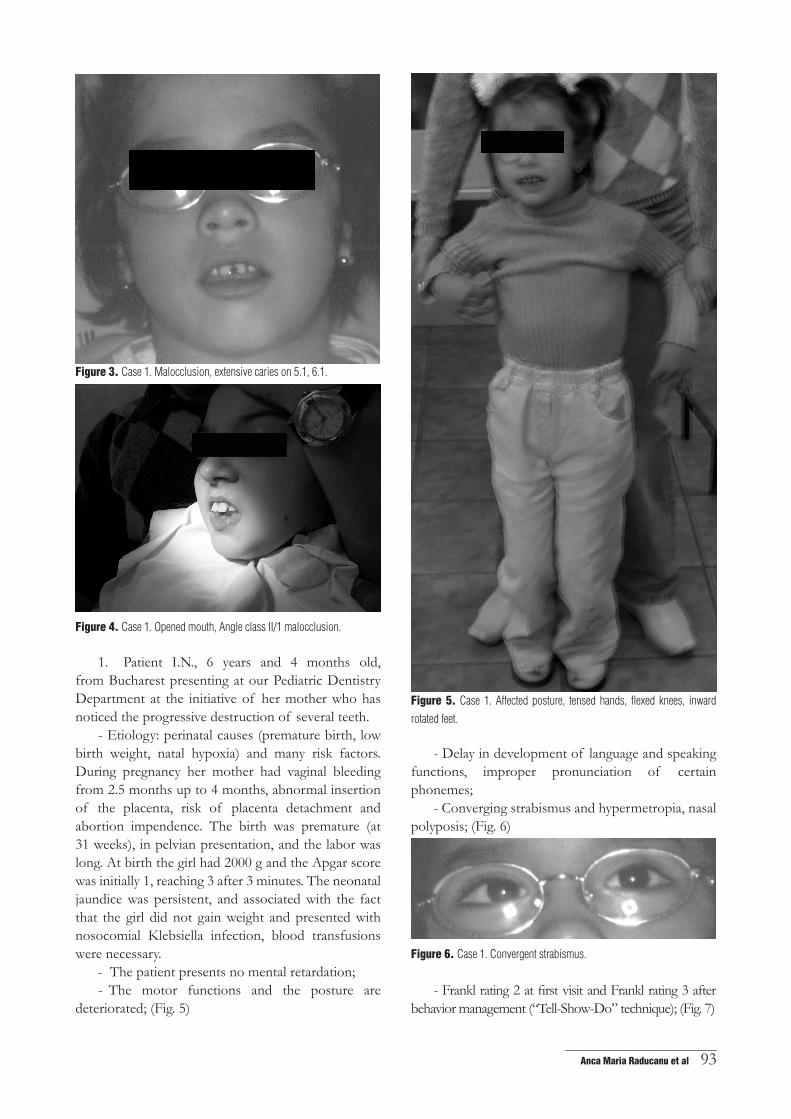
- The patient presents no mental retardation;- The motor functions and the posture are
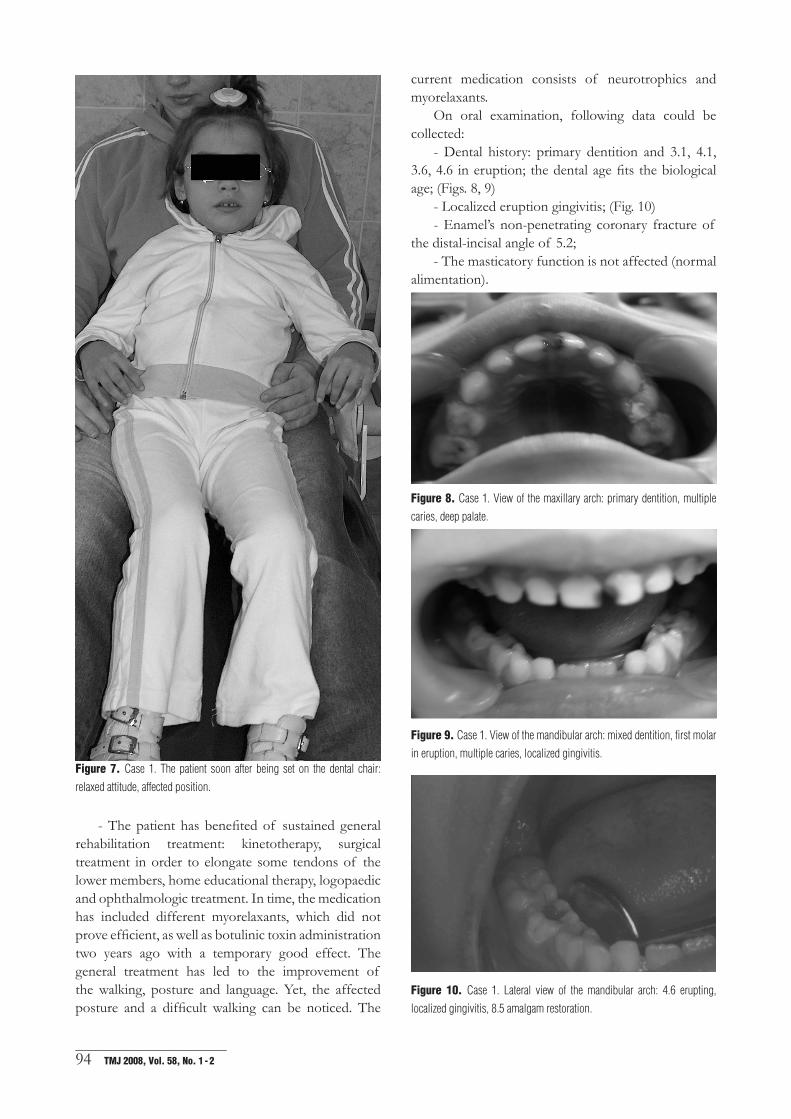
Figure 7. Case 1. The patient soon after being set on the dental chair:
relaxed attitude, affected position.
- The patient has benefited of sustained general rehabilitation treatment: kinetotherapy, surgical treatment in order to elongate some tendons of the lower members, home educational therapy, logopaedic and ophthalmologic treatment. In time, the medication has included different myorelaxants, which did not prove efficient, as well as botulinic toxin administration two years ago with a temporary good effect. The general treatment has led to the improvement of the walking, posture and language. Yet, the affected posture and a difficult walking can be noticed. The
current medication consists of neurotrophics and myorelaxants.
On oral examination, following data could be collected:
- Dental history: primary dentition and 3.1, 4.1, 3.6, 4.6 in eruption; the dental age fits the biological age; (Figs. 8, 9)
the distal-incisal angle of 5.2;- The masticatory function is not affected (normal
alimentation).
Figure 8. Case 1. View of the maxillary arch: primary dentition, multiple
caries, deep palate.
Figure 9. Case 1. View of the mandibular arch: mixed dentition, first molar
in eruption, multiple caries, localized gingivitis.
Figure 10. Case 1. Lateral view of the mandibular arch: 4.6 erupting,
localized gingivitis, 8.5 amalgam restoration.
_____________________________Anca Maria Raducanu et al 95
2. Patient I.R., 11 years and 4 moths old, from Bucharest, presented at our Department at the initiative of her mother who has noticed the progressive destruction of several teeth.
- Etiology: spastic tetraparesis of unknown origin;- The computer tomography performed around
the age of eight months, when the mother, after noticing the motor deficit and the severe motive aphasia, presented at the doctor, revealed the frontal cortical atrophy;
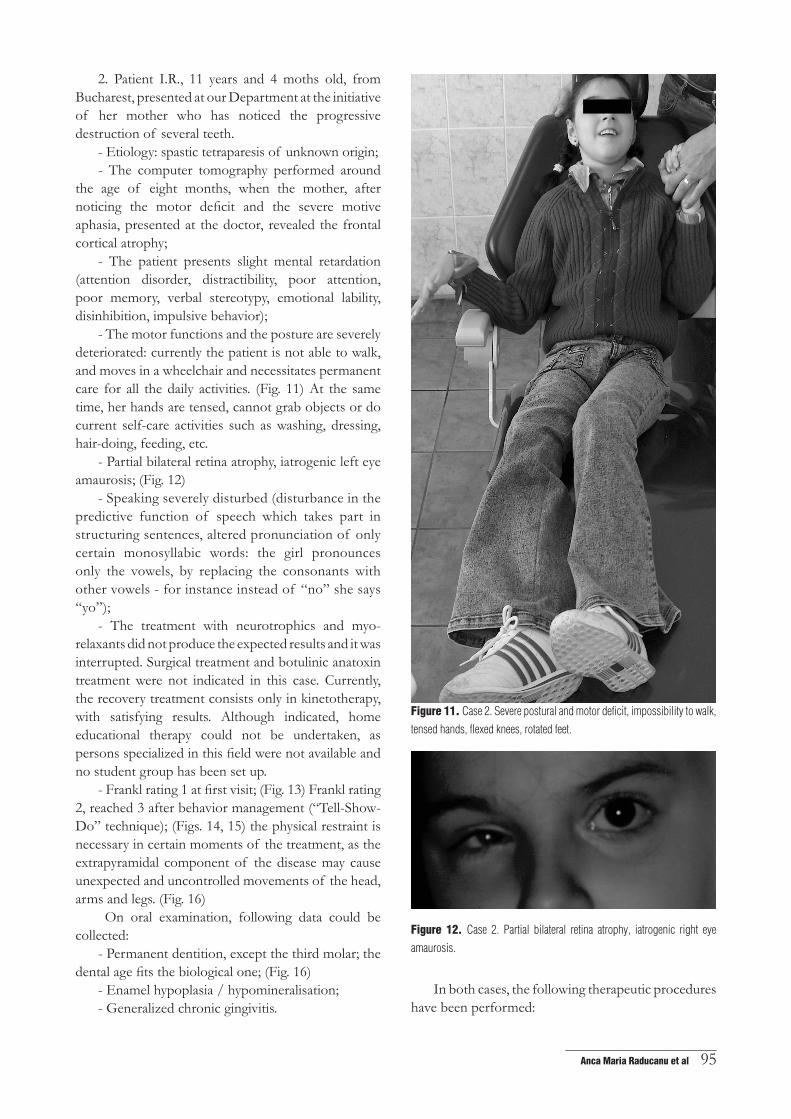
- The motor functions and the posture are severely deteriorated: currently the patient is not able to walk, and moves in a wheelchair and necessitates permanent care for all the daily activities. (Fig. 11) At the same time, her hands are tensed, cannot grab objects or do current self-care activities such as washing, dressing, hair-doing, feeding, etc.
- Speaking severely disturbed (disturbance in the predictive function of speech which takes part in structuring sentences, altered pronunciation of only certain monosyllabic words: the girl pronounces only the vowels, by replacing the consonants with other vowels - for instance instead of “no” she says “yo”);
- The treatment with neurotrophics and myo-relaxants did not produce the expected results and it was interrupted. Surgical treatment and botulinic anatoxin treatment were not indicated in this case. Currently, the recovery treatment consists only in kinetotherapy, with satisfying results. Although indicated, home educational therapy could not be undertaken, as persons specialized in this field were not available and no student group has been set up.
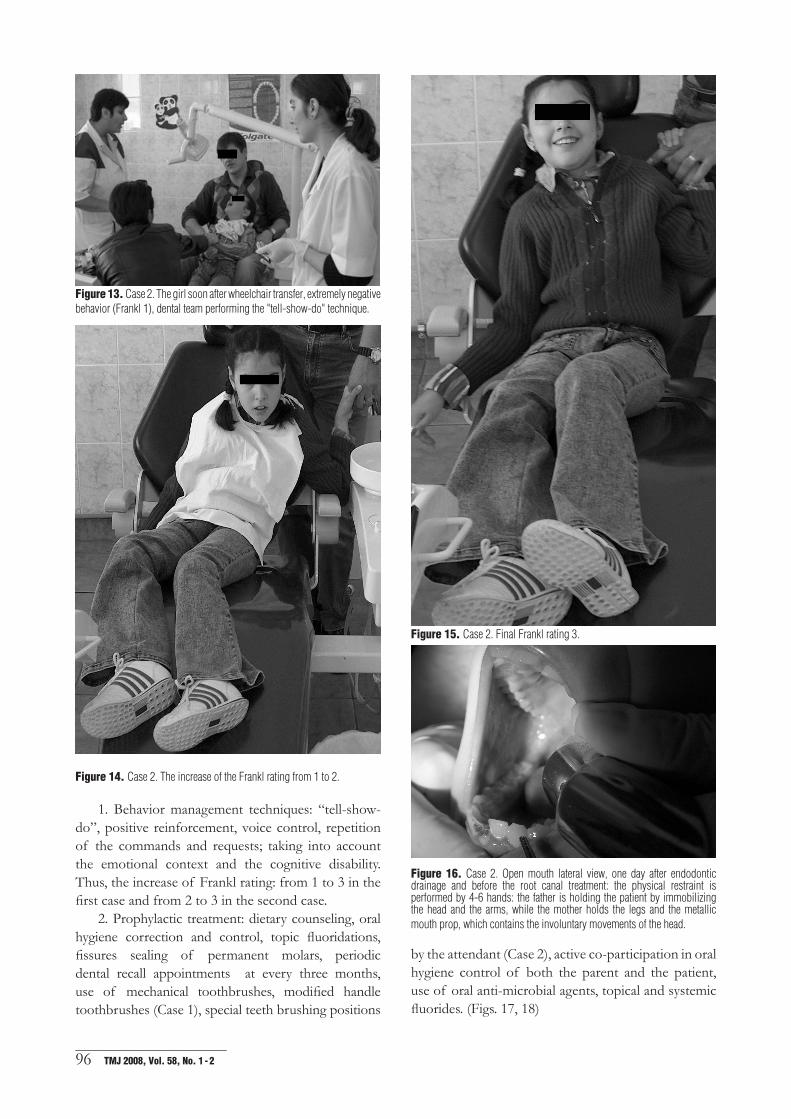
- Frankl rating 1 at first visit; (Fig. 13) Frankl rating 2, reached 3 after behavior management (“Tell-Show-Do” technique); (Figs. 14, 15) the physical restraint is necessary in certain moments of the treatment, as the extrapyramidal component of the disease may cause unexpected and uncontrolled movements of the head, arms and legs. (Fig. 16)
On oral examination, following data could be collected:
- Permanent dentition, except the third molar; the dental age fits the biological one; (Fig. 16)
Figure 13. Case 2. The girl soon after wheelchair transfer, extremely negative behavior (Frankl 1), dental team performing the "tell-show-do" technique.
Figure 14. Case 2. The increase of the Frankl rating from 1 to 2.
1. Behavior management techniques: “tell-show-do”, positive reinforcement, voice control, repetition of the commands and requests; taking into account the emotional context and the cognitive disability. Thus, the increase of Frankl rating: from 1 to 3 in the first case and from 2 to 3 in the second case.
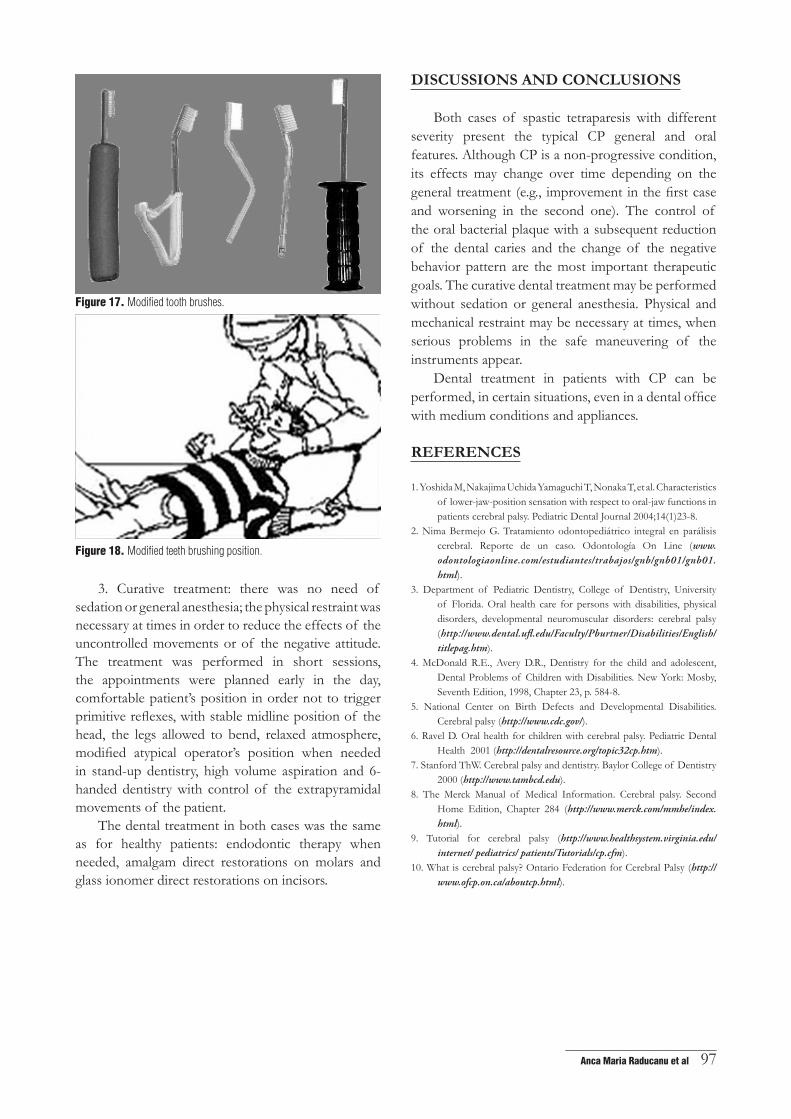
2. Prophylactic treatment: dietary counseling, oral hygiene correction and control, topic fluoridations, fissures sealing of permanent molars, periodic dental recall appointments at every three months, use of mechanical toothbrushes, modified handle toothbrushes (Case 1), special teeth brushing positions
Figure 15. Case 2. Final Frankl rating 3.
Figure 16. Case 2. Open mouth lateral view, one day after endodontic drainage and before the root canal treatment: the physical restraint is performed by 4-6 hands: the father is holding the patient by immobilizing the head and the arms, while the mother holds the legs and the metallic mouth prop, which contains the involuntary movements of the head.
by the attendant (Case 2), active co-participation in oral hygiene control of both the parent and the patient, use of oral anti-microbial agents, topical and systemic fluorides. (Figs. 17, 18)
_____________________________Anca Maria Raducanu et al 97
Figure 17. Modified tooth brushes.
Figure 18. Modified teeth brushing position.
3. Curative treatment: there was no need of sedation or general anesthesia; the physical restraint was necessary at times in order to reduce the effects of the uncontrolled movements or of the negative attitude. The treatment was performed in short sessions, the appointments were planned early in the day, comfortable patient’s position in order not to trigger primitive reflexes, with stable midline position of the head, the legs allowed to bend, relaxed atmosphere, modified atypical operator’s position when needed in stand-up dentistry, high volume aspiration and 6-handed dentistry with control of the extrapyramidal movements of the patient.
The dental treatment in both cases was the same as for healthy patients: endodontic therapy when needed, amalgam direct restorations on molars and glass ionomer direct restorations on incisors.
DIscUssIONs aND cONcLUsIONs
Both cases of spastic tetraparesis with different severity present the typical CP general and oral features. Although CP is a non-progressive condition, its effects may change over time depending on the general treatment (e.g., improvement in the first case and worsening in the second one). The control of the oral bacterial plaque with a subsequent reduction of the dental caries and the change of the negative behavior pattern are the most important therapeutic goals. The curative dental treatment may be performed without sedation or general anesthesia. Physical and mechanical restraint may be necessary at times, when serious problems in the safe maneuvering of the instruments appear.
Dental treatment in patients with CP can be performed, in certain situations, even in a dental office with medium conditions and appliances.
rEFErENcEs
1. Yoshida M, Nakajima Uchida Yamaguchi T, Nonaka T, et al. Characteristics of lower-jaw-position sensation with respect to oral-jaw functions in patients cerebral palsy. Pediatric Dental Journal 2004;14(1)23-8.
2. Nima Bermejo G. Tratamiento odontopediátrico integral en parálisis cerebral. Reporte de un caso. Odontología On Line (www.odontologiaonline.com/estudiantes/trabajos/gnb/gnb01/gnb01.html).
3. Department of Pediatric Dentistry, College of Dentistry, University of Florida. Oral health care for persons with disabilities, physical disorders, developmental neuromuscular disorders: cerebral palsy (http://www.dental.ufl.edu/Faculty/Pburtner/Disabilities/English/titlepag.htm).
4. McDonald R.E., Avery D.R., Dentistry for the child and adolescent, Dental Problems of Children with Disabilities. New York: Mosby, Seventh Edition, 1998, Chapter 23, p. 584-8.
5. National Center on Birth Defects and Developmental Disabilities.Cerebral palsy (http://www.cdc.gov/).
6. Ravel D. Oral health for children with cerebral palsy. Pediatric Dental Health 2001 (http://dentalresource.org/topic32cp.htm).
7. Stanford ThW. Cerebral palsy and dentistry. Baylor College of Dentistry 2000 (http://www.tambcd.edu).
8. The Merck Manual of Medical Information. Cerebral palsy. Second Home Edition, Chapter 284 (http://www.merck.com/mmhe/index.html).
9. Tutorial for cerebral palsy (http://www.healthsystem.virginia.edu/internet/ pediatrics/ patients/Tutorials/cp.cfm).
10. What is cerebral palsy? Ontario Federation for Cerebral Palsy (http://www.ofcp.on.ca/aboutcp.html).