239
| Date post: | 16-Oct-2014 |
| Category: |
Documents |
| Upload: | mafaldayguille |
| View: | 673 times |
| Download: | 3 times |

Essentials in Ophthalmology Oculoplastics and Orbit
R. F. Guthoff J. A. Katowitz
Editors
Essentials in Ophthalmology
G. K. Krieglstein R. N. Weinreb
Series Editors
Glaucoma
Cataract and Refractive Surgery
Uveitis and Immunological Disorders
Vitreo-retinal Surgery
Medical Retina
Oculoplastics and Orbit
Pediatric Ophthalmology,Neuro-Ophthalmology, Genetics
Cornea and External Eye Disease
Editors Rudolf F. Guthoff James A. Katowitz
Oculoplastics and Orbit
Aesthetic and Functional Oculofacial PlasticProblem-Solvingin the 21st Century
With 181 Figures, Mostly in Colourand 18 Tables

Th e Essentials in Ophthalmology series represents an unique updating publication on the progress in all sub-specialties of ophthalmology.
In a quarterly rhythm, eight issues are published cov-ering clinically relevant achievements in the whole fi eld of ophthalmology. Th is timely transfer of advancements for the best possible care of our eye patients has proven to be eff ective. Th e initial working hypothesis of providing new knowledge immediately following publication in the peer-reviewed journal and not waiting for the textbook appears to be highly workable.
We are now in the third cycle of the Essentials in Ophthalmology series, having been encouraged by read-
ership acceptance of the fi rst two series, each of eight volumes. Th is is a success that was made possible pre-dominantly by the numerous opinion-leading authors and the outstanding section editors, as well as with the constructive support of the publisher. Th ere are many good reasons to continue andstill improve the dissemina-tion of this didactic and clinically relevant information.
G.K. KrieglsteinR.N. Weinreb Series Editors
Foreword

Preface
Th is third volume of Oculoplastic and Orbital Surgery promises to challenge the reader with stimulating new concepts at the cutting edge of this subspecialty. A variety of innovative techniques is described in this volume, cov-ering both cosmetic and functional aspects of oculoplas-tic and orbital surgery.
Pearls in cosmetic and oculofacialplastic surgery are presented in great detail, based on extensive experience. Rather than presenting merely anecdotal solutions, spe-cifi c steps are outlined for problem solving in this rapidly evolving fi eld.
Th e latest therapies in the management of capillary hemangiomas, periorbital infections, and orbital and periorbital malignancies using specifi c targeted therapies demonstrate the increasingly important interaction between ophthalmic plastic surgery and the broad fi eld of modern oncology.
Appearance issues are also discussed in relation to managing ophthalmic anomalies in congenital ano-phthalmic and microphthalmic patients. Controversies in enucleation techniques, implant selection, and implant preparation are presented, and the role of pegging an implant to ultimately improve prosthesis motility is criti-cally evaluated.
It is our hope, as with the previous two volumes, that this presentation of the latest concepts and management techniques for a variety of problem areas in the fi eld of oculoplastic surgery will be of value for both comprehen-sive ophthalmologists and subspecialists with a particular interest in this fi eld.
Rudolf F. Guthoff James A. Katowitz
Contents
Chapter 1Ocular Adnexal Lymphoproliferative Disease
Timothy J. Sullivan
1.1 Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . 21.2 Chronic Antigen Stimulation . . . . . . . . . . . 31.3 Immunosuppression . . . . . . . . . . . . . . . . . . . 31.4 Pathology. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41.5 Cytogenetics . . . . . . . . . . . . . . . . . . . . . . . . . . . 41.6 Clinical Features. . . . . . . . . . . . . . . . . . . . . . . . 71.7 Imaging Findings . . . . . . . . . . . . . . . . . . . . . . 81.8 Staging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91.9 Positron Emission Tomography . . . . . . . . . 91.10 Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91.11 Follicular Lymphoma . . . . . . . . . . . . . . . . . . . 111.12 Mantle Cell Lymphoma . . . . . . . . . . . . . . . . . 111.13 Radiotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . 111.14 Chemotherapy . . . . . . . . . . . . . . . . . . . . . . . . . 121.15 Immunotherapy. . . . . . . . . . . . . . . . . . . . . . . . 121.16 Radioimmunotherapy . . . . . . . . . . . . . . . . . . 131.17 Outcome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.18 The Future . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Chapter 2Pearls in Cosmetic Oculofacial Plastic Surgery
Jonathan A. Hoenig
2.1 General Introduction . . . . . . . . . . . . . . . . . . . 212.2 The Aging Process and Facial Analysis. . . 222.3 Endoscopic Brow Lift . . . . . . . . . . . . . . . . . . . 232.3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 232.3.2 Endoscopic Browlift Anesthesia Pearls . . . . 262.3.3 Endoscopic Browlift Surgical
Procedure Pearls . . . . . . . . . . . . . . . . . . . . . . . 262.3.4 Endoscopic Browlift Postoperative
Care Pearls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 272.4 Upper Blepharoplasty . . . . . . . . . . . . . . . . . . 292.4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 292.4.2 Patient Evaluation . . . . . . . . . . . . . . . . . . . . . . 292.4.3 Upper Blepharoplasty
Anesthesia Pearls . . . . . . . . . . . . . . . . . . . . . . 30
2.4.4 Upper Blepharoplasty Surgical Procedure Pearls . . . . . . . . . . . . . . . . . . . . . . . 30
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation . . . . . . . . . . . . 33
2.5.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 332.5.2 Patient Evaluation . . . . . . . . . . . . . . . . . . . . . . 332.5.3 Lower Blepharoplasty
Anesthesia Pearls . . . . . . . . . . . . . . . . . . . . . . 372.5.4 Lower Blepharoplasty Surgical
Procedure Pearls . . . . . . . . . . . . . . . . . . . . . . . 38 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Chapter 3Current Concepts in the Management of Idiopathic Orbital Infl ammation
Katherine A. Lane and Jurij R. Bilyk
3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 473.2 What Is the Diagnosis? . . . . . . . . . . . . . . . . . 473.2.1 Pitfalls of Diagnosis. . . . . . . . . . . . . . . . . . . . . 483.2.2 A Diagnostic Corticosteroid Trial? . . . . . . . 543.2.3 The Question of Biopsy . . . . . . . . . . . . . . . . . 563.3 Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 563.3.1 Corticosteroids. . . . . . . . . . . . . . . . . . . . . . . . . 573.3.2 Radiation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 583.3.3 Other Agents . . . . . . . . . . . . . . . . . . . . . . . . . . 583.4 Special Circumstances. . . . . . . . . . . . . . . . . . 603.4.1 Pediatric IOIS. . . . . . . . . . . . . . . . . . . . . . . . . . . 603.4.2 Sclerosing Pseudotumor . . . . . . . . . . . . . . . 603.4.3 Tolosa–Hunt Syndrome. . . . . . . . . . . . . . . . . 62 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
Chapter 4Lacrimal Canalicular Infl ammation and Occlusion: Diagnosis and Management
David H. Verity and Geoff rey E. Rose
4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 674.2 Embryology, Anatomy, Physiology,
and Pathophysiology of the Canalicular System. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
4.3 Infective Causes . . . . . . . . . . . . . . . . . . . . . . . . 69
x Contents
4.3.1 Periocular Herpes Simplex Infection . . . . 694.3.2 Bacterial Canaliculitis . . . . . . . . . . . . . . . . . . . 704.4 Systemic Infl ammatory Disease . . . . . . . . . 704.4.1 Lichen Planus . . . . . . . . . . . . . . . . . . . . . . . . . . 704.4.2 Ocular Cicatricial Pemphigoid . . . . . . . . . . 704.4.3 Drug Eruptions (Stevens–Johnson
Syndrome) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 714.5 Iatrogenic Causes . . . . . . . . . . . . . . . . . . . . . . 714.5.1 Systemic Drugs . . . . . . . . . . . . . . . . . . . . . . . . 714.5.1.1 5-Fluorouracil (5-FU) . . . . . . . . . . . . . . . . . . . 714.5.1.2 Docetaxel (Taxotere) . . . . . . . . . . . . . . . . . . . 724.5.2 Radiotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . 724.5.3 Topical Ophthalmic Treatments . . . . . . . . . 734.5.3.1 Preservative-Related Chronic
Conjunctivitis . . . . . . . . . . . . . . . . . . . . . . . . . . 734.5.3.2 Mitomycin C Therapy. . . . . . . . . . . . . . . . . . . 734.5.4 Lacrimal Stents and Plugs . . . . . . . . . . . . . . 734.6 The Surgical Approach to Managing
Canalicular Disease. . . . . . . . . . . . . . . . . . . . . 744.6.1 Surgical Technique for
Dacryocystorhinostomy with Retrograde Canaliculostomy. . . . . . . . . . . . 74
4.6.2 Placement of a Jones Canalicular Bypass Tube. . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
Chapter 5Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
William R. Katowitz and James A. Katowitz
5.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 795.2 Nomenclature. . . . . . . . . . . . . . . . . . . . . . . . . . 795.3 Clinical Manifestations of NF1 . . . . . . . . . . 795.4 Orbitofacial Tumors in NF1 . . . . . . . . . . . . . 805.4.1 Neurofi bromas . . . . . . . . . . . . . . . . . . . . . . . . . 805.4.2 Malignant Peripheral Nerve
Sheath Tumors . . . . . . . . . . . . . . . . . . . . . . . . . 815.4.3 Optic Pathway Gliomas . . . . . . . . . . . . . . . . . 815.5 Genetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 835.5.1 The NF1 Gene . . . . . . . . . . . . . . . . . . . . . . . . . . 835.5.2 Overlapping NF1-Like Phenotype
(SPRED1). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 835.6 Management of Neurofi bromatosis
Type 1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 845.6.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 845.6.2 Medical Management of
Neurofi bromas . . . . . . . . . . . . . . . . . . . . . . . . . 845.7 Surgical Management of Orbitofacial
Tumors in NF1 . . . . . . . . . . . . . . . . . . . . . . . . . 845.7.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 845.7.2 Timing of Surgery . . . . . . . . . . . . . . . . . . . . . . 845.7.3 Periorbital Involvement . . . . . . . . . . . . . . . . 85
5.7.3.1 The Upper Eyelid . . . . . . . . . . . . . . . . . . . . . . . 855.7.3.2 The Lower Eyelid and Midface . . . . . . . . . . 855.7.4 Orbital Involvement . . . . . . . . . . . . . . . . . . . . 865.7.4.1 Proptosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 865.7.4.2 Proptosis Due to Orbital
Neurofi bromas . . . . . . . . . . . . . . . . . . . . . . . . . 875.7.4.3 Proptosis Due to Optic Nerve Glioma . . . 875.7.4.4 Orbital Enlargement with Dystopia
and Hypoglobus . . . . . . . . . . . . . . . . . . . . . . . 875.8 The Natural History of NF1 Tumor
Growth from Birth to Senescence . . . . . . . 90 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
Chapter 6Clinicopathologic Features of Lesions Aff ecting the Lacrimal Drainage System in External Dacryocystorhinostomy
Ludwig M. Heindl, Anselm G. M. Jünemann, and Leonard M. Holbach
6.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 956.2 Surgical Anatomy of the Lacrimal
Drainage System . . . . . . . . . . . . . . . . . . . . . . . 966.3 Basic Diagnostics for Disorders
of the Lacrimal Drainage System. . . . . . . . 976.4 Selective Lacrimal Sac Biopsy
in External Dacryocystorhinostomy . . . . . 976.5 Defi nitive Treatment and Prognosis
of Lesions Aff ecting the Lacrimal Drainage System . . . . . . . . . . . . . . . . . . . . . . . 99
6.5.1 Case A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 996.5.2 Case B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 996.5.3 Case C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1006.5.4 Case D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1006.5.5 Case E . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1016.5.6 Case F . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1016.5.7 Case G . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
Chapter 7Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic Patients
Michael P. Schittkowski and Rudolf F. Guthoff
7.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 1057.2 Patients and Methods . . . . . . . . . . . . . . . . . . 1067.2.1 Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1067.2.2 Examination . . . . . . . . . . . . . . . . . . . . . . . . . . . 1067.3 Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1067.3.1 Patient Data. . . . . . . . . . . . . . . . . . . . . . . . . . . . 1067.3.2 Age. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1067.3.3 Family History. . . . . . . . . . . . . . . . . . . . . . . . . . 1067.3.4 Pregnancy History. . . . . . . . . . . . . . . . . . . . . . 107
Contents xi
7.3.5 Birth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1077.3.6 Associated Systemic and
Ocular Diseases . . . . . . . . . . . . . . . . . . . . . . . . 1077.3.7 Developmental Anomaly and
Potential Visual Capacity of the Fellow Eye in Unilateral Disease. . . . . . . . . 110
7.3.8 Neuroradiological Findings (Brain MRI). . 1117.3.9 Nasolacrimal System Findings . . . . . . . . . . 1117.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1127.4.1 Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1127.4.2 Obstetric and Family History. . . . . . . . . . . . 1127.4.3 Associated Pathologies . . . . . . . . . . . . . . . . . 1137.4.3.1 Ophthalmological Findings
in Unilateral Disease. . . . . . . . . . . . . . . . . . . . 1137.4.3.2 Neuroradiological Findings . . . . . . . . . . . . . 1137.4.3.3 Systemic Diseases . . . . . . . . . . . . . . . . . . . . . . 1147.4.3.4 Nasolacrimal Duct Findings. . . . . . . . . . . . . 1147.5 Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . 115 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116
Chapter 8Brow Suspension in Complicated Unilateral Ptosis: Frontalis Muscle Stimulation via Contralateral Levator Recession
Markus F. Pfeiff er
8.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 1178.2 Evaluation of Complicated Ptosis . . . . . . . 1178.2.1 Compensatory Eyebrow Elevation . . . . . . 1178.2.2 Examples of Complicated Unilateral
Ptosis with Insuffi cient Compensatory Brow Elevation . . . . . . . . . . . . . . . . . . . . . . . . . 118
8.2.3 Innervation Patterns of the Frontalis Muscle. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
8.2.4 Checklist of Preoperative Evaluation of Complicated Ptosis . . . . . . . . . . . . . . . . . . 118
8.2.5 Planning Partial or Total Levator Muscle Recession Combined with Unilateral or Bilateral Brow Suspension . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
8.3 Surgical Technique of Levator Muscle Recession . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119
8.3.1 Principle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1198.3.2 Approach to the Levator. . . . . . . . . . . . . . . . 1198.3.3 Partial Levator Recession . . . . . . . . . . . . . . . 1198.3.4 Total Levator Recession. . . . . . . . . . . . . . . . . 1198.3.5 The Lid-Lowering Eff ect and Eyelid
Symmetry: Evolution of the Eyelid Level After Levator Recession . . . . . . . . . . . 121
8.3.6 Undercorrection and Overcorrection. . . . 1218.4 Surgical Technique of Brow
Suspension . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1218.4.1 Materials for Brow Suspension . . . . . . . . . . 121
8.4.1.1 Nonautogenous Materials . . . . . . . . . . . . . . 1218.4.1.2 Autogenous Fascia Lata . . . . . . . . . . . . . . . . 1218.4.2 Our Technique of Harvesting
Autogenous Fascia Lata . . . . . . . . . . . . . . . . 1218.4.3 Mechanical Principals of Brow
Suspension . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1228.4.4 Upper Lid Approach. . . . . . . . . . . . . . . . . . . . 1228.4.5 Fascia Implantation . . . . . . . . . . . . . . . . . . . . 122 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123
Chapter 9Modern Concepts in Orbital Imaging
Jonathan J. Dutton
9.1 Computerized Tomography . . . . . . . . . . . . 1259.2 Three-Dimensional Imaging . . . . . . . . . . . . 1299.3 Magnetic Resonance Imaging . . . . . . . . . . 1299.3.1 The T1 Constant. . . . . . . . . . . . . . . . . . . . . . . . 1309.3.2 The T2 Constant. . . . . . . . . . . . . . . . . . . . . . . . 1319.3.3 Creating the MR Image . . . . . . . . . . . . . . . . . 1319.4 Imaging of Common Orbital
Lesions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1349.4.1 Adenoid Cystic Carcinoma. . . . . . . . . . . . . . 1349.4.2 Cavernous Hemangioma . . . . . . . . . . . . . . . 1349.4.3 Dermoid Cyst . . . . . . . . . . . . . . . . . . . . . . . . . . 1349.4.4 Fibrous Dysplasia . . . . . . . . . . . . . . . . . . . . . . 1359.4.5 Lymphangioma . . . . . . . . . . . . . . . . . . . . . . . . 1369.4.6 Lymphoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1369.4.7 Myositis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1369.4.8 Optic Nerve Glioma . . . . . . . . . . . . . . . . . . . . 1389.4.9 Pseudotumor . . . . . . . . . . . . . . . . . . . . . . . . . . 1399.4.10 Rhabdomyosarcoma . . . . . . . . . . . . . . . . . . . 1399.5 Diff usion MRI (Diff usion-Weighted
Imaging) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1409.6 Positron Emission Tomography . . . . . . . . . 1419.7 Orbital Ultrasound . . . . . . . . . . . . . . . . . . . . . 1429.7.1 Physics and Instrumentation. . . . . . . . . . . . 1429.7.1.1 Topographic Echography . . . . . . . . . . . . . . . 1439.7.1.2 Quantitative Echography . . . . . . . . . . . . . . . 1439.7.1.3 Kinetic Echography. . . . . . . . . . . . . . . . . . . . . 1439.7.2 Extraocular Muscles . . . . . . . . . . . . . . . . . . . . 1459.7.3 Optic Nerves . . . . . . . . . . . . . . . . . . . . . . . . . . . 146 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 146
Chapter 10Management of Periorbital Cellulitis in the 21st Century
Michael P. Rabinowitz and Scott M. Goldstein
10.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 14910.2 The Infection: Stages, Symptoms,
and Eff ects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14910.3 Etiology. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15110.4 Microbiology. . . . . . . . . . . . . . . . . . . . . . . . . . . 151
xii Contents
10.5 Changing Pathogens and Resistance. . . . 15210.5.1 CA-MRSA Versus Hospital-Acquired
MRSA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15210.5.2 Orbital MRSA. . . . . . . . . . . . . . . . . . . . . . . . . . . 15310.6 Evaluation of Orbital Cellulitis . . . . . . . . . . 15410.7 Medical Treatment of Orbital Cellulitis . . 15510.8 Surgical Treatment of Orbital Cellulitis . . 15610.9 Prevention of Orbital Cellulitis
after Orbital Fracture . . . . . . . . . . . . . . . . . . . 158 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159
Chapter 11Current Concepts in the Management of Capillary Hemangiomas: Steroids, Beta-Blockers, or Surgery
François Codère and Julie Powell
11.1 Clinical Picture . . . . . . . . . . . . . . . . . . . . . . . . . 16111.1.1 Clinical Phases . . . . . . . . . . . . . . . . . . . . . . . . . 16111.1.2 Etiology, Histology, and Classifi cation . . . 16111.1.3 Diff erential Diagnosis of Infantile
Hemangioma . . . . . . . . . . . . . . . . . . . . . . . . . . 16211.2 Ocular Complications . . . . . . . . . . . . . . . . . . 16311.3 Investigation. . . . . . . . . . . . . . . . . . . . . . . . . . . 16311.3.1 Angiography. . . . . . . . . . . . . . . . . . . . . . . . . . . 16411.4 Management . . . . . . . . . . . . . . . . . . . . . . . . . . 16511.4.1 Active Nonintervention. . . . . . . . . . . . . . . . . 16511.4.2 Indications for Treatment . . . . . . . . . . . . . . . 16511.5 Modalities of Treatment . . . . . . . . . . . . . . . . 16511.5.1 Steroids. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16511.5.1.1 Topical Steroids . . . . . . . . . . . . . . . . . . . . . . . . 16511.5.1.2 Intralesional Corticosteroid Injection. . . . 16511.5.1.3 Oral Corticosteroids . . . . . . . . . . . . . . . . . . . . 16611.5.2 Interferon-Alfa . . . . . . . . . . . . . . . . . . . . . . . . . 16611.5.3 Vincristine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16711.5.4 Laser. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16711.5.5 Embolization. . . . . . . . . . . . . . . . . . . . . . . . . . . 16711.5.6 Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16711.5.7 Beta-Blockers: A New Promising
Modality of Treatment . . . . . . . . . . . . . . . . . . 168 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170
Chapter 12Evaluation and Management of Metastatic Orbital Tumors
Alejandra A. Valenzuela and Alan A. McNab
12.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 17312.2 Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . 17312.3 Biological Behavior and Timing
of Metastasis . . . . . . . . . . . . . . . . . . . . . . . . . . . 17412.4 Lateralization . . . . . . . . . . . . . . . . . . . . . . . . . . 174
12.5 Localization . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17412.6 Clinical Features. . . . . . . . . . . . . . . . . . . . . . . . 17512.7 Imaging and Patterns of Orbital
Metastatic Disease . . . . . . . . . . . . . . . . . . . . . 17612.8 Biopsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17712.9 Common Types of Orbital Metastases . . . 17812.9.1 Breast Carcinoma . . . . . . . . . . . . . . . . . . . . . . 17812.9.2 Lung Carcinoma . . . . . . . . . . . . . . . . . . . . . . . 17812.9.3 Prostatic Cancer . . . . . . . . . . . . . . . . . . . . . . . . 17912.9.4 Melanoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17912.9.5 Carcinoid Tumor . . . . . . . . . . . . . . . . . . . . . . . 17912.10 Diff erential Diagnosis . . . . . . . . . . . . . . . . . . 18012.11 Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18012.11.1 Radiotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . 18012.11.2 Chemotherapy . . . . . . . . . . . . . . . . . . . . . . . . . 18012.11.3 Hormonal Therapy . . . . . . . . . . . . . . . . . . . . . 18012.11.4 Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18112.12 Prognosis and Survival . . . . . . . . . . . . . . . . . 181 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 181
Chapter 13Targeted Therapy in the Treatment of Orbital and Periorbital Malignancies
Aaron Savar and Bita Esmaeli
13.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 18713.2 Rituximab. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18813.3 Yttrium-90-Labeled Ibritumomab
Tiuxetan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18913.4 Imatinib Mesylate . . . . . . . . . . . . . . . . . . . . . . 19013.5 Cetuximab . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192
Chapter 14Controversies in Enucleation Technique and Implant Selection: Whether to Wrap, Attach Muscles, and Peg?
David R. Jordan and Stephen R. Klapper
14.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 19514.2 Porous Orbital Implants . . . . . . . . . . . . . . . . 19614.3 Orbital Implant Selection in Adults. . . . . . 19914.4 Orbital Implant Selection
in Children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20014.5 Volume Considerations
in Orbital Implant Selection . . . . . . . . . . . . 20114.6 Orbital Implant Wrapping
and Attaching Extraocular Muscles . . . . . 20214.7 Which Wrap to Use . . . . . . . . . . . . . . . . . . . . . 20314.8 To Peg or Not to Peg Porous Implants . . . 20414.9 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 206 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 206
Contents xiii
Chapter 15Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues: Cosmetic and Functional Considerations
Ana M. Susana Morley and Raman Malhotra
15.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 21315.2 Etiology and Presentation . . . . . . . . . . . . . . 21315.2.1 Etiology of Orbital Volume Loss . . . . . . . . . 21315.2.2 Etiology of Periorbital Volume Loss . . . . . 21315.2.3 Features of Orbital Volume Loss. . . . . . . . . 21415.2.4 Features of PeriOorbital Volume Loss. . . . 21515.3 Background to Injectable
Soft-Tissue Fillers . . . . . . . . . . . . . . . . . . . . . . . 21515.3.1 Historical Perspective on Volume
Replacement. . . . . . . . . . . . . . . . . . . . . . . . . . . 21515.3.2 Advantages of Injectable
Soft-Tissue Fillers . . . . . . . . . . . . . . . . . . . . . . . 21515.3.3 Complications of Injectable
Soft-Tissue Fillers . . . . . . . . . . . . . . . . . . . . . . . 215
15.4 Types of Injectable Soft-Tissue Filler. . . . . 21615.4.1 Collagen Fillers. . . . . . . . . . . . . . . . . . . . . . . . . 21615.4.2 Hyaluronic acid Fillers . . . . . . . . . . . . . . . . . . 21615.4.3 Semipermanent Injectable
Soft-Tissue Fillers . . . . . . . . . . . . . . . . . . . . . . . 21615.5 Treatment Areas . . . . . . . . . . . . . . . . . . . . . . . 21715.5.1 Orbit. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21715.5.2 Upper Eyelid and Brow . . . . . . . . . . . . . . . . . 22015.5.3 Tear Trough . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22015.5.4 Temple and Brow . . . . . . . . . . . . . . . . . . . . . . 22315.6 Other Periorbital Uses
of Injectable Soft-Tissue Fillers . . . . . . . . . . 22515.6.1 Upper Eyelid Loading . . . . . . . . . . . . . . . . . . 22615.6.2 Lower Eyelid Elevation. . . . . . . . . . . . . . . . . . 22615.6.3 Treatment of Cicatricial Ectropion. . . . . . . 22615.7 Future Developments . . . . . . . . . . . . . . . . . . 226 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231
Contributors
Jurij R. BilykOculoplastic and Orbital Surgery Service, Wills Eye Institute, 840 Walnut St., Philadelphia, PA 19107, USA
François CodèreDepartment of Ophthalmology, Hôpital Ste-Justine, Université de Montréal, 3175 Côte Ste-Catherine, Montreal, Quebec, Canada, H3T 1C5
Jonathan J. DuttonDepartment of Ophthalmology, University of North Carolina, Chapel Hill, NC 27599-7040, USA
Bita EsmaeliSection of Ophthalmology, Department of Head and Neck Surgery, Th e University of Texas M.D. Anderson Cancer Center, 1515 Holcombe Blvd., Unit 1445, Houston, Texas 77030, USA
Scott M. GoldsteinOculoplastic Service, Wills Eye Institute, Th omas Jeff erson University, Philadelphia, PA, USA
Rudolf F. Guthoff Department of Opthalmology, Rostock University, Doberaner Straβe 140, 18055 Rostock, Germany
Ludwig M. HeindlDepartment of Ophthalmology and Eye Hospital, University Erlangen-Nürnberg, Schwabachanlage 6, 91054 Erlangen, Germany
Jonathan A. Hoenig9735 Wilshire Blvd. #308, Beverly Hills, CA 90212, USA
Leonard M. HolbachDepartment of Ophthalmology and Eye Hospital, University Erlangen-Nürnberg, Schwabachanlage 6, 91054 Erlangen, Germany
David R. JordanUniversity of Ottawa Eye Institute, 301 O’Connor Street, Ottawa, Ontario, Canada, K2P 1V6
Anselm G.M. JünemannDepartment of Ophthalmology and Eye Hospital, University Erlangen-Nürnberg, Schwabachanlage 6, 91054 Erlangen, Germany
James A. KatowitzChildren’s Hospital of Philadelphia,Division of Ophthalmology,R.D. Wood Ambulatory Care Building34th Street Civic Center Blvd.Philadelphia, PA 19104,USA
William R. KatowitzOculoplastic Surgery, Children’s Hospital of PhiladelphiaDivision of Ophthalmology, 34th Street Civic Center Blvd.Philadelphia, PA 19104, USA
Stephen R. KlapperKlapper Eyelid and Facial Plastic Surgery, 11900 North Pennsylvania Street, Suite 104, Carmel, IN 46032, USA
Katherine A. LaneDepartment of Ophthalmology, Th e Children’s Hospital of Philadelphia, 34th and Civic Center Blvd., Philadelphia, PA 19104, USA
Raman MalhotraQueen Victoria Hospital, Corneoplastic Unit, Holtye Road, East Grinstead, RH19 3DZ, West Sussex, UK
Alan A. McNabRoyal Victorian Eye and Ear Hospital, Orbital, Lacrimal and Plastic Clinic, Suite 216, 100 Victoria Parade, East Melbourne 3002, Victoria, Australia
Ana M. Susana MorleyQueen Victoria Hospital, Corneoplastic Unit, East Grinstead, West Sussex, UKSt. Th omas’ Hospital, Department of Ophthalmology, Westminster Bridge Rd., London SE1 7EH, UK
xvi Contributors
Markus J. Pfeiff erAugenklinik Herzog Carl Th eodor,Nymphenburger Str.43,80335 München, Germany
Julie PowellDivision of Pediatric Dermatology, Hôpital Ste-Justine, Université de Montréal,3175 Côte Ste-Catherine, Montreal, Quebec,Canada, H3T 1C5
Michael P. RabinowitzWills Eye Institute, Oculoplastic Service, Th omas Jeff erson University, Philadelphia, PA, USA
Geoff rey E. RoseMoorfi elds Eye Hospital, Adnexal Service, City Road, London EC1V 2PD
Aaron SavarDepartment of Head and Neck Surgery, Section of Ophthalmology, Th e University of Texas M.D. Anderson Cancer Center, Houston, Texas, USA
Michael P. SchittkowskiGeorg-August University,University Medical Center Goettingen, Department of Ophthalmology, Section for Strabismus,Neuroophthalmology and Oculoplastic SurgeryR.-Koch-Str. 40D 37075 Goettingen, Germany
Timothy J. SullivanUniversity of Queensland, Eyelid, Lacrimal and Orbital Clinic, Royal Brisbane and Women’s Hospital, Butterfi eld Street, Herston, Brisbane, Queensland, 4029, Australia
Alejandra A. ValenzuelaOrbital, Lacrimal and Oculoplastic Clinic, Department of Ophthalmology and Visual Sciences, Division of Neurosurgery, QEII Health Sciences Centre, Dalhousie University, Room 2035, 2W Victoria Building, 1276 South Park Street, Halifax, NS, B3H 2Y9, Canada
David H. VerityMoorfi elds Eye Hospital, City Road, London EC1V 2PD, UKLacrimal Clinic, Moorfi elds Eye Hospital, City Road, London EC1V 2PD, UK
Ocular Adnexal Lymphoproliferative DiseaseTimothy J. Sullivan
Chapter 1
Malignant lymphomas represent neoplastic proliferation of cells predominantly located in lymphoid tissues. Lymphoma can be broadly divided into non-Hodgkin lymphoma (NHL; 70%) and Hodgkin disease (30%) [145]. Th ere are 65,000 new cases of NHL annually as well as 19,000 deaths each year in the United States [83].
Th e annual incidence for mature B-cell neoplasms, which form the largest subgroup of lymphoma, ranges from 15/100,000 in the United States, Europe, and Australia to only 1.2/100,000 in China [61].
While the overall incidence of lymphoma has been increasing annually by 3–4% per year for many decades [22, 48], the rate of extranodal disease has been increas-ing at a greater rate [36, 50]. Within the extranodal sub-group, OALD has shown the greatest increase in incidence at a rate of up to 6.3% per year [106, 116, 137]. OALD represents a spectrum, ranging from benign reactive lym-phoid hyperplasia (RLH) to malignant ocular adnexal lymphomas (OALs). Almost all OALs are B-cell NHLs.
OALD disease has provided many challenges for the clinician and pathologist. Because of limitations in patho-logical techniques and understanding, previous workers were unable to correlate clinical behavior with pathologi-cal diagnosis in between 20% and 50% of cases [77, 114, 115]. Th is mismatch applied to both benign-appearing
1
Core Messages
Lymphoma is the most common orbital malig- ■
nancy, usually presenting clinically with a short history of painless swelling, proptosis, or a salmon patch. Th e incidence of ocular adnexal lymphop-roliferative disease Ocular adnexal lymphoprolif-erative disease (OALD) is increasing at 6% per year. Th e majority of adnexal lymphomas are extranodal marginal zone lymphoma (EMZL) or mucosa-associated lymphoid tissue (MALT).Chronic antigen stimulation and immunosup- ■
pression, including ultraviolet (UV) irradia-tion, contribute to pathogenesis. Improvements in molecular genetic techniques have led to more accurate diagnosis. Advances in imag-ing mean our ability to stage the presence and extent of systemic involvement has increased.
Computed tomographic (CT) images usually ■
show homogeneous, well-circumscribed lesions, molding to the globe, of greater than brain den-sity with moderate enhancement. Magnetic reso-nance imaging (MRI) lesions are isointense to extraocular muscles on T1- and T2-weighted images and show moderate enhancement with gadolinium. Positron emission tomography (PET) scanning provides improved detection of the presence and extent of systemic involvement.While radiotherapy remains the mainstay of ■
treatment, management approaches are undergo-ing major changes. Treatments directed to reduce chronic antigen stimulation or to use immuno-therapy or radioimmunotherapy result in greater response to treatment as well as improved quality of life and survival.
Summary for the Clinician
MALT lymphoma is the most common OALD. ■
MALT arises in response to chronic antigen ■
stimulation, and increasing genetic aberrations lead to malignancy.Molecular genetic testing with polymerase chain ■
reaction (PCR) and fl uorescent in situ hybridiza-tion (FISH) is being routinely performed to com-plement morphological fi ndings to allow more rapid accurate diagnosis of OALD.

2 1 Ocular Adnexal Lymphoproliferative Disease
1
lesions, which followed an aggressive course, and frankly malignant orbital lesions on histology, which failed to dis-seminate [94, 96]. With the discovery in the early 1970’s [74, 75, 155], that separate B- and T- lymphocyte subsets existed and also through insights gained with electron microscopy [78], pathologists began to understand that lymphoma comprised many distinct entities. Unfortunately, however, despite these advances, they were still unable to correlate clinical behavior with morphological appear-ance. Th is only came with an appreciation of immunophe-notype and the use of the cluster of diff erentiation (CD) nomenclature [37, 54, 74, 77, 94–97]. Th e fi rst CD discov-ered was B1, now known as CD20, a pan B-cell marker and target for monoclonal antibody therapy. Th e applica-tion of molecular genetics to pathological specimens [76, 80, 98, 108–110] has fi nally given pathologists the ability to precisely defi ne the genetic aberrations underlying these lesions.
Shortly aft er extranodal lymphomas of MALT were described elsewhere in the body [62, 68, 71, 72], similar lesions were recognized in the orbit [76, 79] but had prob-ably been described in the orbit prior to the systemic rec-ognition of this entity [78]. Since the early descriptions of MALT lymphoma, a greater appreciation of the impor-tance of this entity in the ocular adnexa has developed, where it constitutes the majority of primary OALs [8, 15, 26, 84, 104, 113, 117, 153, 154]. Th ere were also problems of applicability of existing classifi cation schemes to OALD because of an inability to incorporate extranodal lesions. Fortunately, the classifi cation in current use, the World Health Organization (WHO) modifi cation of the Revised European American Lymphoma Classifi cation, recog-nizes both extranodal disease and marginal zone MALT lymphomas and is designed to accommodate new entities as further diagnostic progress elucidates additional sub-types [69, 73].
OAL may be a primary process, arising within adnexal structures, but it may also be secondary from primary lesions elsewhere in the body. Less commonly, the adnexa may be involved by direct extension from primary lesions in adjacent structures such as the sinuses.
OAL is usually subdivided into orbital, eyelid, con-junctival, and lacrimal sac lesions. Most large series con-fi rmed that EMZL of MALT comprise one half to two thirds of OALs in Western countries and up to 90% in Asian communities, where the incidence of follicular lymphoma (FL) is very low. Other common indolent lesions include follicular (FL) and lymphoplasmacytic lymphoma, while the two more common aggressive lesions are the diff use large B-cell lymphoma (DLBCL) and Mantle cell lymphoma (MCL). Less commonly, other non-Hodgkin B-cell lesions (e.g., small cell lymphoma)
may occur, and T- and NK (natural killer) cell lympho-mas also occur rarely [27, 149, 156].
1.1 Pathogenesis
Lymphomas represent a malignant, clonal proliferation of lymphocytes, although clonality does not always consti-tute malignancy. Th e various lymphoma subtypes largely correspond to clonal proliferations of cells arrested at specifi c stages of lymphocyte development. Th is process begins in the marrow with precursor B lymphoblasts, which undergo immunoglobulin VDJ recombination to become surface immunoglobulin-positive naïve B cells [99]. Th ese recirculating naïve B cells are found in blood, primary lymphoid follicles, and follicle mantle zones. Exposure to antigen leads to transformation to blast cells, which migrate into the center of the primary follicle, establishing the germinal center by fi lling the follicular dendritic cell meshwork, where they are now known as centroblasts. BCL-6 is necessary for germinal center for-mation, and then its downregulation is important for fur-ther lymphocyte development [21]. Here, the cells undergo somatic mutations of the immunoglobulin vari-able region gene and BCL-6 as part of the normal immune response, eventually becoming centrocytes. Centrocytes interact with surface molecules to diff erentiate into mem-ory B cells or plasma cells. Th e memory B cells are found in the marginal zone of the lymph follicle, whereas plasma cells home to marrow [61].
Th ere is site specifi city for the homing of postgerminal center B cells, orchestrated by adhesion molecules and cytokines [122, 130]. Th us, MALT-derived B cells home to their specifi c MALT and nodal B cells to specifi c lymph nodes. Corresponding to these stages of development, EMZL and lymphoplasmacytic lymphoma arise from memory B cells and FLs and DLBCLs from the germinal center, whereas MCL arises from mature naïve B cells, found in the mantle region of the lymph node. A range of chromosomal translocations, deletions, and mutations occurs during the diff erent phases of lymphocyte devel-opment, eventually establishing a clone of malignant cells. Th e clinical behavior of the tumor usually refl ects the behavior of the normal cell counterpart. Th is corresponds to the lymphocyte stage at which the abnormal cell has accumulated suffi cient genetic abnormalities to prolifer-ate without control or avoid programmed cell death, con-stituting malignancy. Malignant cell clones that have low turnover produce indolent lymphomas such as MALT and FL, whereas cell stages that are more active will give rise to more aggressive lesions such as MCL or DLBCL. A small percentage of the low-grade lymphomas will
1.3 Immunosuppression 3
undergo transformation to a higher-grade lesion, for example, follicular and MALT lesions can transform into DLBCL.
Th e most common OAL is the MALT lymphoma. Although the orbit itself has no lymph nodes or true lym-phatic drainage system, studies have confi rmed the pres-ence of small lymphatic channels associated with the optic nerve [55, 56]. Th ere is also a well-established ocu-lar MALT system extending from the lacrimal gland, encompassing the conjunctival tissues, and including the lacrimal drainage apparatus. Th is can be broken down into the conjunctiva-associated lymphoid tissue and lac-rimal drainage-associated lymphoid tissue (CALT and LDALT, respectively) with an overall designation of eye-associated lymphoid tissue (EALT) [92, 93]. Lymphoid follicles from these tissues participate in the normal immune response to antigens with production of anti-bodies and eff ector plasma cells. While most OAL is MALT derived, presumably arising from these tissues, lymphocytes destined to reside in the EALT system pass through the normal lymphocyte development cycle, and this may explain why we see other primary B-cell lym-phomas in the ocular adnexal region. Lymphomas origi-nating in ocular adnexal tissues can have systemic lymphoid involvement of the marrow and other tissues. Conversely, systemic lymphomas may involve adnexal tissue secondarily.
Primary ocular adnexal T- and NK cell lymphomas may also be seen, but are less common, possibly refl ecting the fewer gene rearrangements that occur in their normal development compared to B lymphocytes [89].
1.2 Chronic Antigen Stimulation
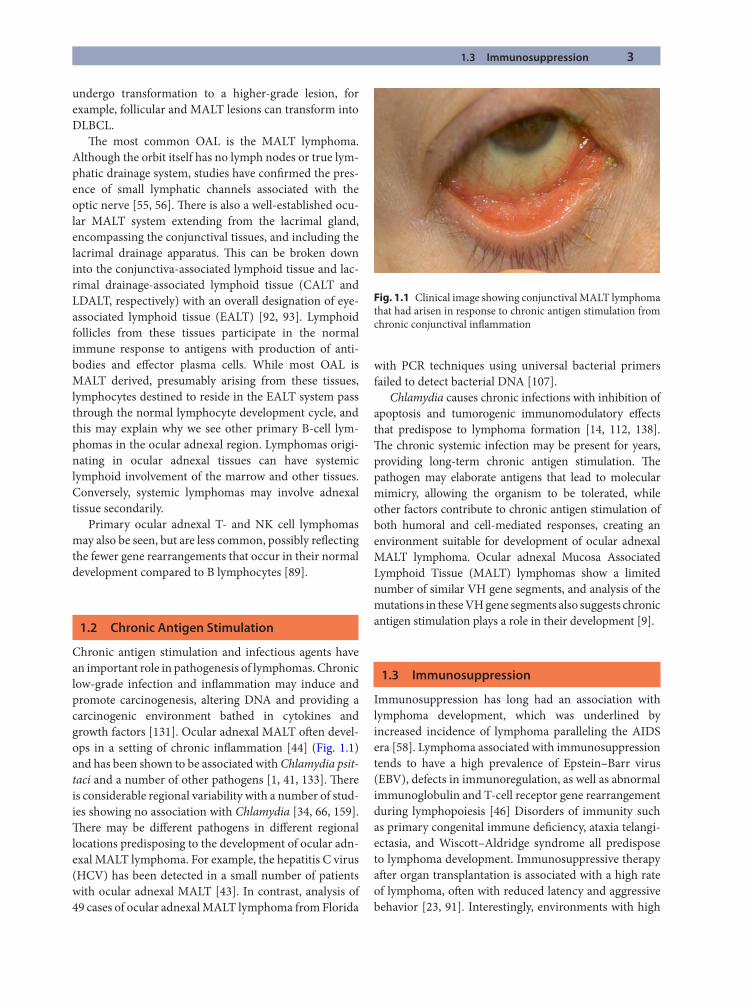
Chronic antigen stimulation and infectious agents have an important role in pathogenesis of lymphomas. Chronic low-grade infection and infl ammation may induce and promote carcinogenesis, altering DNA and providing a carcinogenic environment bathed in cytokines and growth factors [131]. Ocular adnexal MALT oft en devel-ops in a setting of chronic infl ammation [44] (Fig. 1.1) and has been shown to be associated with Chlamydia psit-taci and a number of other pathogens [1, 41, 133]. Th ere is considerable regional variability with a number of stud-ies showing no association with Chlamydia [34, 66, 159]. Th ere may be diff erent pathogens in diff erent regional locations predisposing to the development of ocular adn-exal MALT lymphoma. For example, the hepatitis C virus (HCV) has been detected in a small number of patients with ocular adnexal MALT [43]. In contrast, analysis of 49 cases of ocular adnexal MALT lymphoma from Florida
with PCR techniques using universal bacterial primers failed to detect bacterial DNA [107].
Chlamydia causes chronic infections with inhibition of apoptosis and tumorogenic immunomodulatory eff ects that predispose to lymphoma formation [14, 112, 138]. Th e chronic systemic infection may be present for years, providing long-term chronic antigen stimulation. Th e pathogen may elaborate antigens that lead to molecular mimicry, allowing the organism to be tolerated, while other factors contribute to chronic antigen stimulation of both humoral and cell-mediated responses, creating an environment suitable for development of ocular adnexal MALT lymphoma. Ocular adnexal Mucosa Associated Lymphoid Tissue (MALT) lymphomas show a limited number of similar VH gene segments, and analysis of the mutations in these VH gene segments also suggests chronic antigen stimulation plays a role in their development [9].
1.3 Immunosuppression
Immunosuppression has long had an association with lymphoma development, which was underlined by increased incidence of lymphoma paralleling the AIDS era [58]. Lymphoma associated with immunosuppression tends to have a high prevalence of Epstein–Barr virus (EBV), defects in immunoregulation, as well as abnormal immunoglobulin and T-cell receptor gene rearrangement during lymphopoiesis [46] Disorders of immunity such as primary congenital immune defi ciency, ataxia telangi-ectasia, and Wiscott–Aldridge syndrome all predispose to lymphoma development. Immunosuppressive therapy aft er organ transplantation is associated with a high rate of lymphoma, oft en with reduced latency and aggressive behavior [23, 91]. Interestingly, environments with high
Fig. 1.1 Clinical image showing conjunctival MALT lymphoma that had arisen in response to chronic antigen stimulation from chronic conjunctival infl ammation
4 1 Ocular Adnexal Lymphoproliferative Disease
1
UV light exposure such as Australia and Florida have high rates of both nonmelanoma skin cancer and lym-phoma, suggesting a common role in immunosuppres-sion from UV light in these tumors [7, 106]. Th ere is good epidemiological support for this hypothesis, but mecha-nisms remain unclear [2, 65, 86, 129].
1.4 Pathology
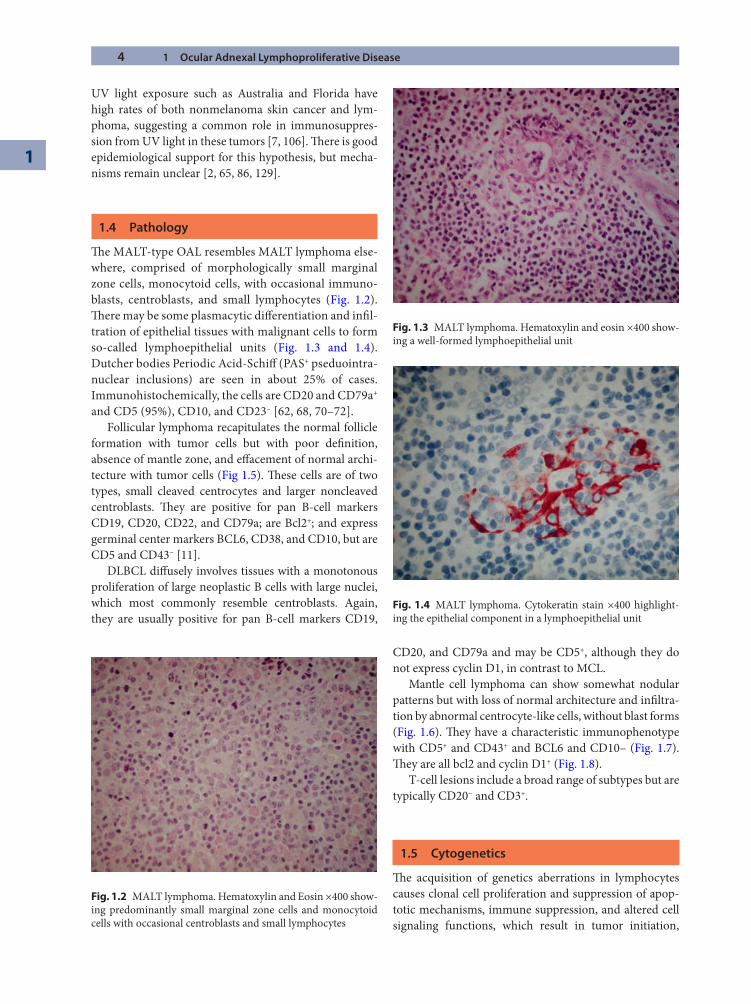
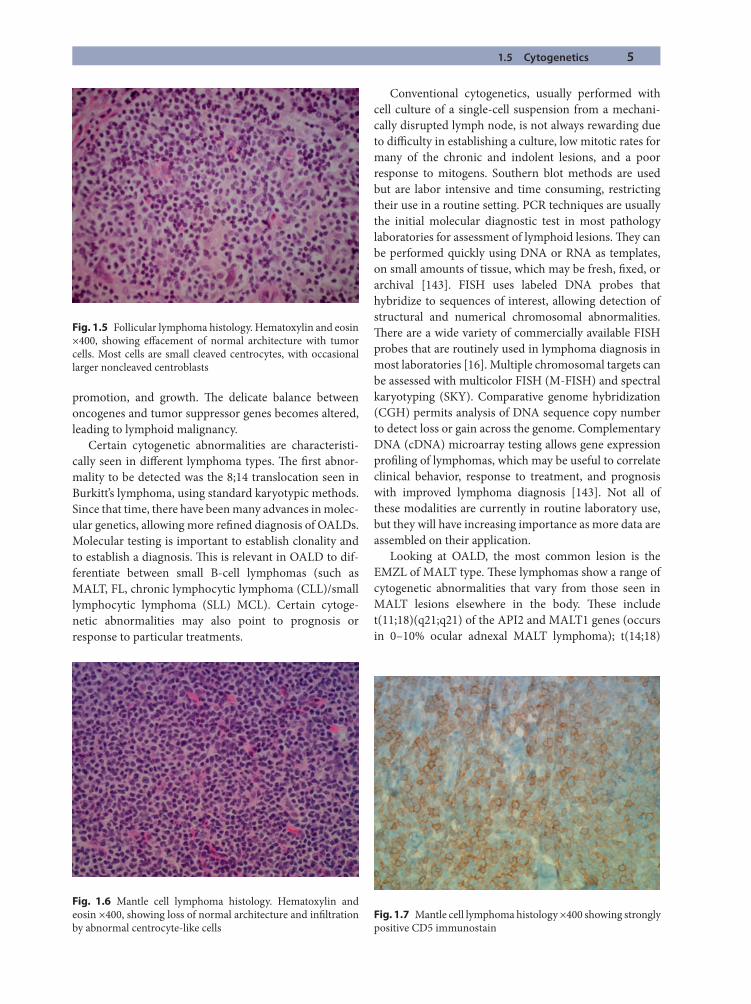
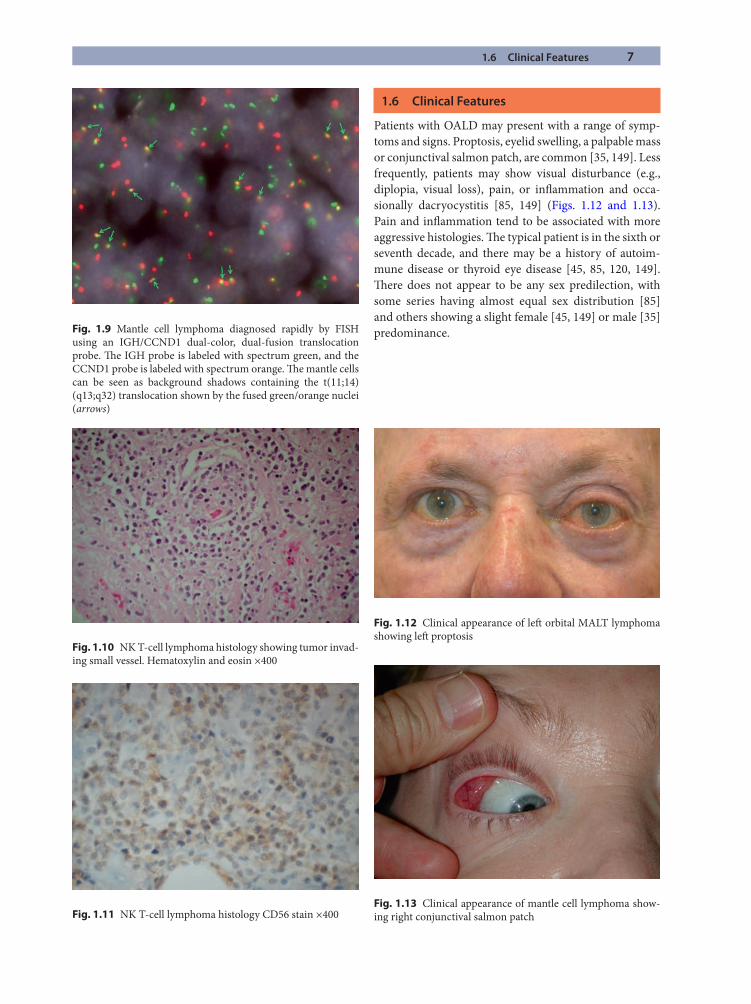
Th e MALT-type OAL resembles MALT lymphoma else-where, comprised of morphologically small marginal zone cells, monocytoid cells, with occasional immuno-blasts, centroblasts, and small lymphocytes (Fig. 1.2). Th ere may be some plasmacytic diff erentiation and infi l-tration of epithelial tissues with malignant cells to form so-called lymphoepithelial units (Fig. 1.3 and 1.4). Dutcher bodies Periodic Acid-Schiff (PAS+ pseduointra-nuclear inclusions) are seen in about 25% of cases. Immunohistochemically, the cells are CD20 and CD79a+ and CD5 (95%), CD10, and CD23– [62, 68, 70–72].
Follicular lymphoma recapitulates the normal follicle formation with tumor cells but with poor defi nition, absence of mantle zone, and eff acement of normal archi-tecture with tumor cells (Fig 1.5). Th ese cells are of two types, small cleaved centrocytes and larger noncleaved centroblasts. Th ey are positive for pan B-cell markers CD19, CD20, CD22, and CD79a; are Bcl2+; and express germinal center markers BCL6, CD38, and CD10, but are CD5 and CD43− [11].
DLBCL diff usely involves tissues with a monotonous proliferation of large neoplastic B cells with large nuclei, which most commonly resemble centroblasts. Again, they are usually positive for pan B-cell markers CD19,
CD20, and CD79a and may be CD5+, although they do not express cyclin D1, in contrast to MCL.
Mantle cell lymphoma can show somewhat nodular patterns but with loss of normal architecture and infi ltra-tion by abnormal centrocyte-like cells, without blast forms (Fig. 1.6). Th ey have a characteristic immunophenotype with CD5+ and CD43+ and BCL6 and CD10– (Fig. 1.7). Th ey are all bcl2 and cyclin D1+ (Fig. 1.8).
T-cell lesions include a broad range of subtypes but are typically CD20− and CD3+.
1.5 Cytogenetics
Th e acquisition of genetics aberrations in lymphocytes causes clonal cell proliferation and suppression of apop-totic mechanisms, immune suppression, and altered cell signaling functions, which result in tumor initiation,
Fig. 1.3 MALT lymphoma. Hematoxylin and eosin ×400 show-ing a well-formed lymphoepithelial unit
Fig. 1.2 MALT lymphoma. Hematoxylin and Eosin ×400 show-ing predominantly small marginal zone cells and monocytoid cells with occasional centroblasts and small lymphocytes
Fig. 1.4 MALT lymphoma. Cytokeratin stain ×400 highlight-ing the epithelial component in a lymphoepithelial unit
1.5 Cytogenetics 5
promotion, and growth. Th e delicate balance between oncogenes and tumor suppressor genes becomes altered, leading to lymphoid malignancy.
Certain cytogenetic abnormalities are characteristi-cally seen in diff erent lymphoma types. Th e fi rst abnor-mality to be detected was the 8;14 translocation seen in Burkitt’s lymphoma, using standard karyotypic methods. Since that time, there have been many advances in molec-ular genetics, allowing more refi ned diagnosis of OALDs. Molecular testing is important to establish clonality and to establish a diagnosis. Th is is relevant in OALD to dif-ferentiate between small B-cell lymphomas (such as MALT, FL, chronic lymphocytic lymphoma (CLL)/small lymphocytic lymphoma (SLL) MCL). Certain cytoge-netic abnormalities may also point to prognosis or response to particular treatments.
Conventional cytogenetics, usually performed with cell culture of a single-cell suspension from a mechani-cally disrupted lymph node, is not always rewarding due to diffi culty in establishing a culture, low mitotic rates for many of the chronic and indolent lesions, and a poor response to mitogens. Southern blot methods are used but are labor intensive and time consuming, restricting their use in a routine setting. PCR techniques are usually the initial molecular diagnostic test in most pathology laboratories for assessment of lymphoid lesions. Th ey can be performed quickly using DNA or RNA as templates, on small amounts of tissue, which may be fresh, fi xed, or archival [143]. FISH uses labeled DNA probes that hybridize to sequences of interest, allowing detection of structural and numerical chromosomal abnormalities. Th ere are a wide variety of commercially available FISH probes that are routinely used in lymphoma diagnosis in most laboratories [16]. Multiple chromosomal targets can be assessed with multicolor FISH (M-FISH) and spectral karyotyping (SKY). Comparative genome hybridization (CGH) permits analysis of DNA sequence copy number to detect loss or gain across the genome. Complementary DNA (cDNA) microarray testing allows gene expression profi ling of lymphomas, which may be useful to correlate clinical behavior, response to treatment, and prognosis with improved lymphoma diagnosis [143]. Not all of these modalities are currently in routine laboratory use, but they will have increasing importance as more data are assembled on their application.
Looking at OALD, the most common lesion is the EMZL of MALT type. Th ese lymphomas show a range of cytogenetic abnormalities that vary from those seen in MALT lesions elsewhere in the body. Th ese include t(11;18)(q21;q21) of the API2 and MALT1 genes (occurs in 0–10% ocular adnexal MALT lymphoma); t(14;18)
Fig. 1.5 Follicular lymphoma histology. Hematoxylin and eosin ×400, showing eff acement of normal architecture with tumor cells. Most cells are small cleaved centrocytes, with occasional larger noncleaved centroblasts
Fig. 1.6 Mantle cell lymphoma histology. Hematoxylin and eosin ×400, showing loss of normal architecture and infi ltration by abnormal centrocyte-like cells
Fig. 1.7 Mantle cell lymphoma histology ×400 showing strongly positive CD5 immunostain

6 1 Ocular Adnexal Lymphoproliferative Disease
1
(q32;q21) of the IGH and MALT1 genes (occurs in 7–11% ocular adnexal MALT lymphoma); t(1;14)(p22;q32) of the Bcl-10 and IGH genes (not reported to occur in ocu-lar adnexal MALT lymphoma); and t(3;14)(p14;q32) of the FOXP1 and IGH genes (not reported to occur in ocu-lar adnexal MALT lymphoma) [136]. Th ese diff erent abnormalities result in activation of the transcription fac-tor NF-κB (nuclear factor kappa B), which upregulates various proliferation genes in B cells [87]. Other abnor-malities seen include trisomy 3 (occurs in 40–60% of ocular adnexal MALT lymphoma) and trisomy18 (occurs in 14–50% of ocular adnexal MALT lymphoma) [146]. Th e incidence of these cytogenetic abnormalities varies greatly, with MALT lymphomas derived from diff erent tissues (e.g., gastric, lung, skin, and ocular adnexa [101]. Interestingly, given the low percentage of ocular adnexal MALT lymphomas showing the aberrations common in other MALT lymphomas, there may be other as-yet-undiscovered abnormalities associated with this entity.
Follicular lymphoma develops from centrocytes and centroblasts of the germinal centers that fail to undergo apoptosis because BCL2 expression is preserved as a result of the initial t(14;18) chromosomal rearrangement [61]. Additional genetic alterations occur, leading to FL, which may have a better or worse prognosis, depending on which secondary alterations take place [11].
We have already learned that BCL6 plays an important role in germinal center formation and subsequent lym-phocyte development. Failure to downregulate BCL6 aft er affi nity maturation may be lymphomagenic [21, 81]. BCL6 is necessary for survival of human DLBCL cells. DLBCL commonly shows alterations of the BCL6 gene at the 3q27 locus, but other complex karyotypes may be seen [51]. Th ese diff erent abnormalities may explain the
morphologically and immunohistochemically diff erent centroblastic and immunoblastic subtypes of DLBCL [51]. Th ere are at least three distinct entities grouped together under the DLBCL banner based on distinct chromosomal imbalances. Th ese are germinal center B-cell-like (best prognosis), activated B-cell-like (intermediate-to-poor prognosis), and a poor prognosis non-germinal center B-cell-like (non-GCB-like) non-ABC-like subgroup [32].
Mantle cell lymphoma develops from a combination of dysregulation of cell proliferation and survival path-ways with a high level of chromosome instability. Th e genetic hallmark of MCL is the t(11;14)(q13;q32) translo-cation that juxtaposes CCND1, at chromosome 11q13, to the immunoglobulin (Ig) heavy chain gene at chromo-some 14q32 [82]. CCND1 is a proto-oncogene that encodes cyclin D1, resulting in cyclin D1 overexpression. Th is translocation occurs in the bone marrow in an early B cell at the pre-B stage of diff erentiation when the cell is initiating the Ig gene rearrangement with the recombina-tion of the VDJ segments. Th e cell of origin is a mature B cell found in the mantle region of normal lymphoid fol-licles. Although the initial translocation occurs in imma-ture B cells in the marrow, the oncogenic advantage is realized only when additional genetic aberrations occur as the cell matures into a naïve pregerminal center B cell [82, 139]. Diagnosis of this small cell lymphoma can be confi rmed by immunohistochemical staining for cyclin D1 and with FISH techniques (Fig. 1.9) [24].
T-cell malignancies comprise two main groups: pre-cursor T-cell lymphoblastic neoplasms, derived from maturing thymocytes, and peripheral T-cell lymphomas (PTCLs), arising from mature postthymic T cells (Figs. 1.10 and 1.11). Physiological T-cell development is regu-lated by numerous oncogenes and oncogenic pathways, suggesting a balance between normal diff erentiation and malignant transformation [4]. Th e molecular pathogene-sis of T-cell lymphomas is still poorly understood, but it is recognized that there are oft en complex karyotypic abnormalities present [3].
Fig. 1.8 Mantle cell lymphoma histology ×400 showing strongly positive cyclin D1immunostain
Summary for the Clinician
OAL usually presents with a short history (5–7 ■
months) of painless proptosis or a salmon patch.MRI and CT are both useful, with MRI showing ■
soft tissue involvement better and CT showing bone changes better.PET scanning has an important role in the sys- ■
temic staging of OAL, but CT and MRI show the orbital disease better.
1.6 Clinical Features 7
1.6 Clinical Features
Patients with OALD may present with a range of symp-toms and signs. Proptosis, eyelid swelling, a palpable mass or conjunctival salmon patch, are common [35, 149]. Less frequently, patients may show visual disturbance (e.g., diplopia, visual loss), pain, or infl ammation and occa-sionally dacryocystitis [85, 149] (Figs. 1.12 and 1.13). Pain and infl ammation tend to be associated with more aggressive histologies. Th e typical patient is in the sixth or seventh decade, and there may be a history of autoim-mune disease or thyroid eye disease [45, 85, 120, 149]. Th ere does not appear to be any sex predilection, with some series having almost equal sex distribution [85] and others showing a slight female [45, 149] or male [35] predominance.Fig. 1.9 Mantle cell lymphoma diagnosed rapidly by FISH
using an IGH/CCND1 dual-color, dual-fusion translocation probe. Th e IGH probe is labeled with spectrum green, and the CCND1 probe is labeled with spectrum orange. Th e mantle cells can be seen as background shadows containing the t(11;14)(q13;q32) translocation shown by the fused green/orange nuclei (arrows)
Fig. 1.10 NK T-cell lymphoma histology showing tumor invad-ing small vessel. Hematoxylin and eosin ×400
Fig. 1.11 NK T-cell lymphoma histology CD56 stain ×400
Fig. 1.12 Clinical appearance of left orbital MALT lymphoma showing left proptosis
Fig. 1.13 Clinical appearance of mantle cell lymphoma show-ing right conjunctival salmon patch
8 1 Ocular Adnexal Lymphoproliferative Disease
1
1.7 Imaging Findings
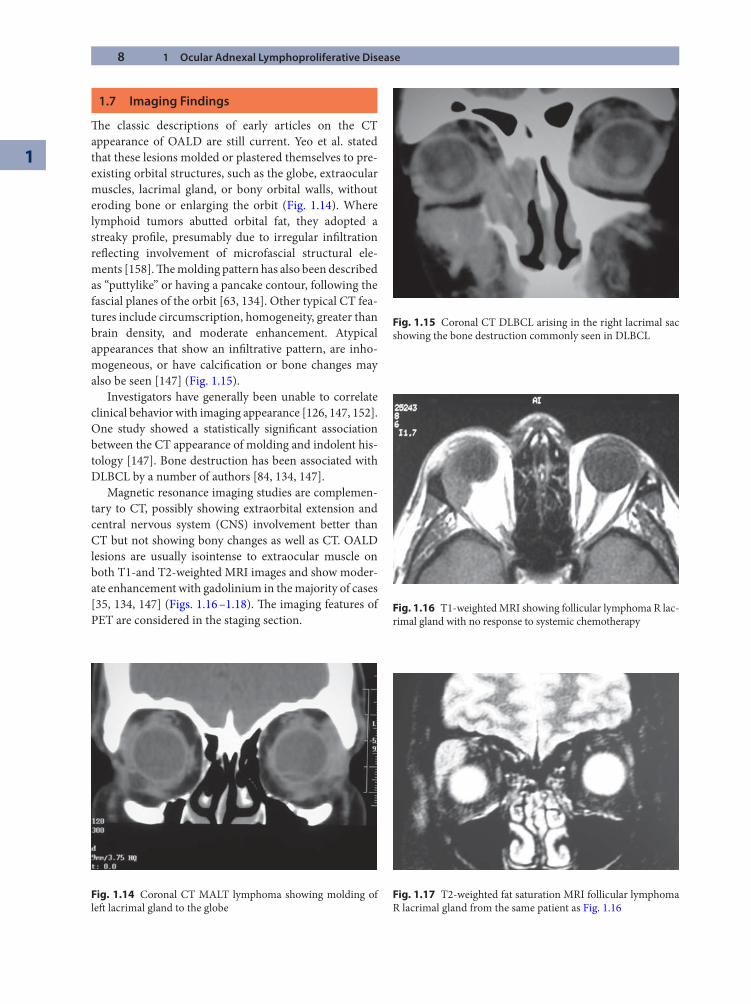
Th e classic descriptions of early articles on the CT appearance of OALD are still current. Yeo et al. stated that these lesions molded or plastered themselves to pre-existing orbital structures, such as the globe, extraocular muscles, lacrimal gland, or bony orbital walls, without eroding bone or enlarging the orbit (Fig. 1.14). Where lymphoid tumors abutted orbital fat, they adopted a streaky profi le, presumably due to irregular infi ltration refl ecting involvement of microfascial structural ele-ments [158]. Th e molding pattern has also been described as “puttylike” or having a pancake contour, following the fascial planes of the orbit [63, 134]. Other typical CT fea-tures include circumscription, homogeneity, greater than brain density, and moderate enhancement. Atypical appearances that show an infi ltrative pattern, are inho-mogeneous, or have calcifi cation or bone changes may also be seen [147] (Fig. 1.15).
Investigators have generally been unable to correlate clinical behavior with imaging appearance [126, 147, 152]. One study showed a statistically signifi cant association between the CT appearance of molding and indolent his-tology [147]. Bone destruction has been associated with DLBCL by a number of authors [84, 134, 147].
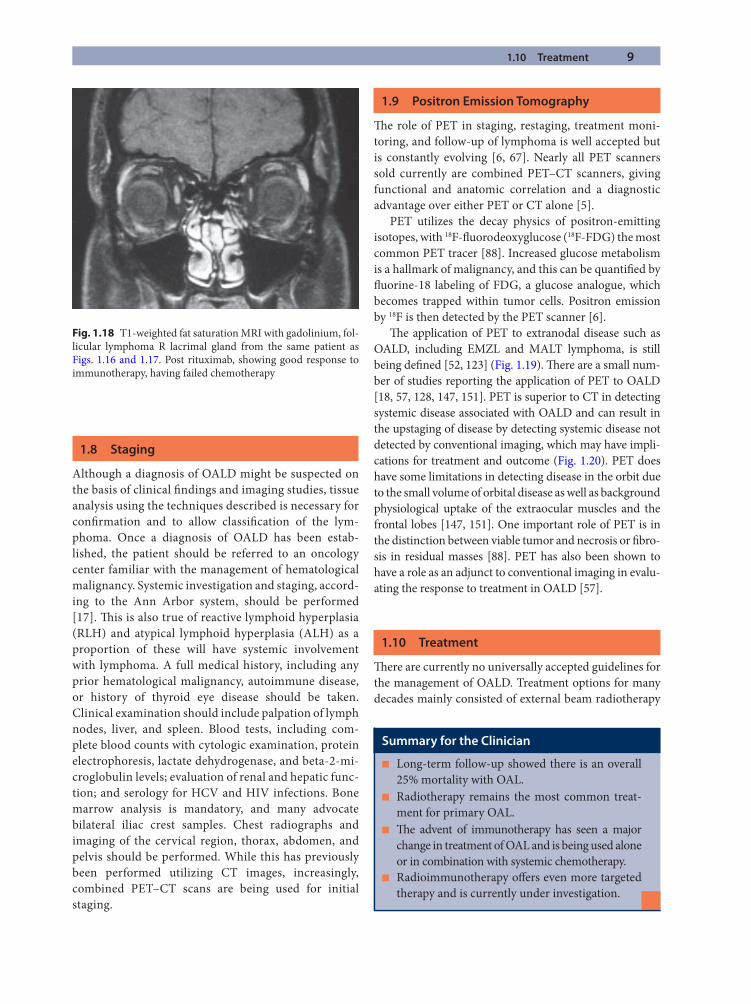
Magnetic resonance imaging studies are complemen-tary to CT, possibly showing extraorbital extension and central nervous system (CNS) involvement better than CT but not showing bony changes as well as CT. OALD lesions are usually isointense to extraocular muscle on both T1-and T2-weighted MRI images and show moder-ate enhancement with gadolinium in the majority of cases [35, 134, 147] (Figs. 1.16 –1.18). Th e imaging features of PET are considered in the staging section.
Fig. 1.14 Coronal CT MALT lymphoma showing molding of left lacrimal gland to the globe
Fig. 1.15 Coronal CT DLBCL arising in the right lacrimal sac showing the bone destruction commonly seen in DLBCL
Fig. 1.16 T1-weighted MRI showing follicular lymphoma R lac-rimal gland with no response to systemic chemotherapy
Fig. 1.17 T2-weighted fat saturation MRI follicular lymphoma R lacrimal gland from the same patient as Fig. 1.16
1.10 Treatment 9
1.8 Staging
Although a diagnosis of OALD might be suspected on the basis of clinical fi ndings and imaging studies, tissue analysis using the techniques described is necessary for confi rmation and to allow classifi cation of the lym-phoma. Once a diagnosis of OALD has been estab-lished, the patient should be referred to an oncology center familiar with the management of hematological malignancy. Systemic investigation and staging, accord-ing to the Ann Arbor system, should be performed [17]. Th is is also true of reactive lymphoid hyperplasia (RLH) and atypical lymphoid hyperplasia (ALH) as a proportion of these will have systemic involvement with lymphoma. A full medical history, including any prior hematological malignancy, autoimmune disease, or history of thyroid eye disease should be taken. Clinical examination should include palpation of lymph nodes, liver, and spleen. Blood tests, including com-plete blood counts with cytologic examination, protein electrophoresis, lactate dehydrogenase, and beta-2-mi-croglobulin levels; evaluation of renal and hepatic func-tion; and serology for HCV and HIV infections. Bone marrow analysis is mandatory, and many advocate bilateral iliac crest samples. Chest radiographs and imaging of the cervical region, thorax, abdomen, and pelvis should be performed. While this has previously been performed utilizing CT images, increasingly, combined PET–CT scans are being used for initial staging.
1.9 Positron Emission Tomography
Th e role of PET in staging, restaging, treatment moni-toring, and follow-up of lymphoma is well accepted but is constantly evolving [6, 67]. Nearly all PET scanners sold currently are combined PET–CT scanners, giving functional and anatomic correlation and a diagnostic advantage over either PET or CT alone [5].
PET utilizes the decay physics of positron-emitting isotopes, with 18F-fl uorodeoxyglucose (18F-FDG) the most common PET tracer [88]. Increased glucose metabolism is a hallmark of malignancy, and this can be quantifi ed by fl uorine-18 labeling of FDG, a glucose analogue, which becomes trapped within tumor cells. Positron emission by 18F is then detected by the PET scanner [6].
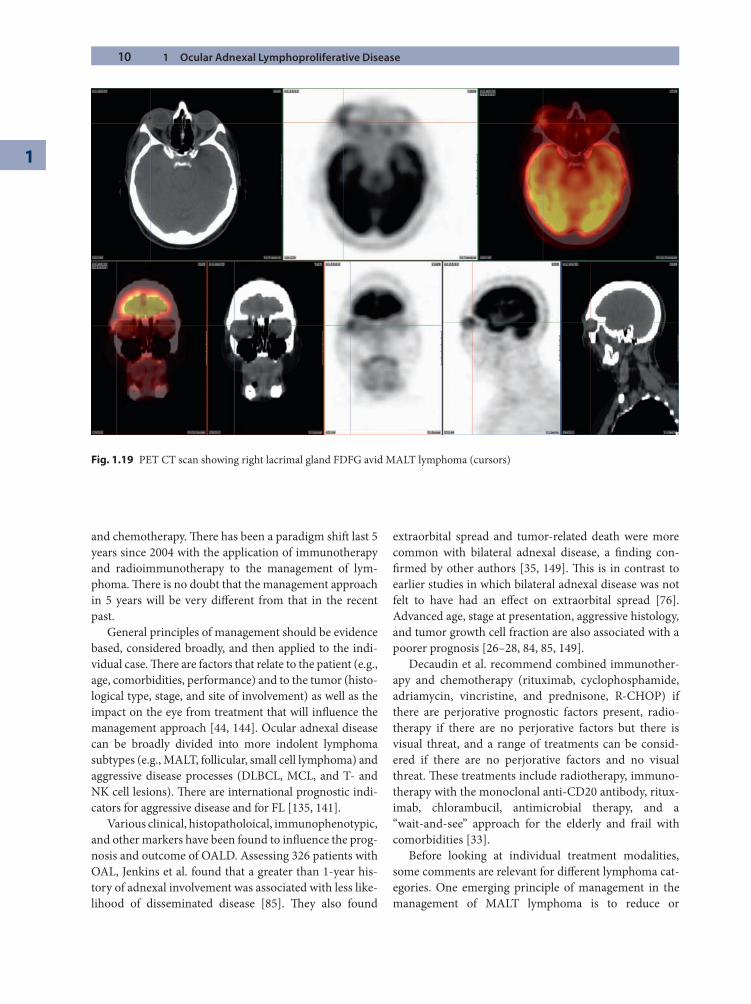
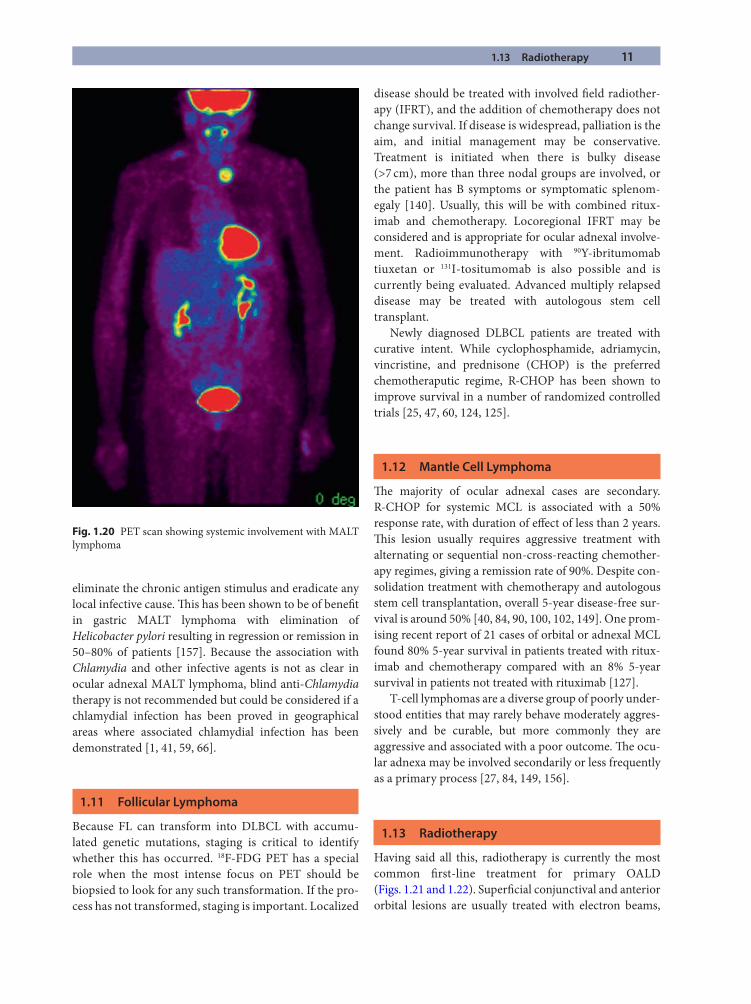
Th e application of PET to extranodal disease such as OALD, including EMZL and MALT lymphoma, is still being defi ned [52, 123] (Fig. 1.19). Th ere are a small num-ber of studies reporting the application of PET to OALD [18, 57, 128, 147, 151]. PET is superior to CT in detecting systemic disease associated with OALD and can result in the upstaging of disease by detecting systemic disease not detected by conventional imaging, which may have impli-cations for treatment and outcome (Fig. 1.20). PET does have some limitations in detecting disease in the orbit due to the small volume of orbital disease as well as background physiological uptake of the extraocular muscles and the frontal lobes [147, 151]. One important role of PET is in the distinction between viable tumor and necrosis or fi bro-sis in residual masses [88]. PET has also been shown to have a role as an adjunct to conventional imaging in evalu-ating the response to treatment in OALD [57].
1.10 Treatment
Th ere are currently no universally accepted guidelines for the management of OALD. Treatment options for many decades mainly consisted of external beam radiotherapy
Fig. 1.18 T1-weighted fat saturation MRI with gadolinium, fol-licular lymphoma R lacrimal gland from the same patient as Figs. 1.16 and 1.17. Post rituximab, showing good response to immunotherapy, having failed chemotherapy
Summary for the Clinician
Long-term follow-up showed there is an overall ■
25% mortality with OAL.Radiotherapy remains the most common treat- ■
ment for primary OAL.Th e advent of immunotherapy has seen a major ■
change in treatment of OAL and is being used alone or in combination with systemic chemotherapy.Radioimmunotherapy off ers even more targeted ■
therapy and is currently under investigation.
10 1 Ocular Adnexal Lymphoproliferative Disease
1
and chemotherapy. Th ere has been a paradigm shift last 5 years since 2004 with the application of immunotherapy and radioimmunotherapy to the management of lym-phoma. Th ere is no doubt that the management approach in 5 years will be very diff erent from that in the recent past.
General principles of management should be evidence based, considered broadly, and then applied to the indi-vidual case. Th ere are factors that relate to the patient (e.g., age, comorbidities, performance) and to the tumor (histo-logical type, stage, and site of involvement) as well as the impact on the eye from treatment that will infl uence the management approach [44, 144]. Ocular adnexal disease can be broadly divided into more indolent lymphoma subtypes (e.g., MALT, follicular, small cell lymphoma) and aggressive disease processes (DLBCL, MCL, and T- and NK cell lesions). Th ere are international prognostic indi-cators for aggressive disease and for FL [135, 141].
Various clinical, histopatholoical, immunophenotypic, and other markers have been found to infl uence the prog-nosis and outcome of OALD. Assessing 326 patients with OAL, Jenkins et al. found that a greater than 1-year his-tory of adnexal involvement was associated with less like-lihood of disseminated disease [85]. Th ey also found
extraorbital spread and tumor-related death were more common with bilateral adnexal disease, a fi nding con-fi rmed by other authors [35, 149]. Th is is in contrast to earlier studies in which bilateral adnexal disease was not felt to have had an eff ect on extraorbital spread [76]. Advanced age, stage at presentation, aggressive histology, and tumor growth cell fraction are also associated with a poorer prognosis [26–28, 84, 85, 149].
Decaudin et al. recommend combined immunother-apy and chemotherapy (rituximab, cyclophosphamide, adriamycin, vincristine, and prednisone, R-CHOP) if there are perjorative prognostic factors present, radio-therapy if there are no perjorative factors but there is visual threat, and a range of treatments can be consid-ered if there are no perjorative factors and no visual threat. Th ese treatments include radiotherapy, immuno-therapy with the monoclonal anti-CD20 antibody, ritux-imab, chlorambucil, antimicrobial therapy, and a “wait-and-see” approach for the elderly and frail with comorbidities [33].
Before looking at individual treatment modalities, some comments are relevant for diff erent lymphoma cat-egories. One emerging principle of management in the management of MALT lymphoma is to reduce or
Fig. 1.19 PET CT scan showing right lacrimal gland FDFG avid MALT lymphoma (cursors)
1.13 Radiotherapy 11
eliminate the chronic antigen stimulus and eradicate any local infective cause. Th is has been shown to be of benefi t in gastric MALT lymphoma with elimination of Helicobacter pylori resulting in regression or remission in 50–80% of patients [157]. Because the association with Chlamydia and other infective agents is not as clear in ocular adnexal MALT lymphoma, blind anti-Chlamydia therapy is not recommended but could be considered if a chlamydial infection has been proved in geographical areas where associated chlamydial infection has been demonstrated [1, 41, 59, 66].
1.11 Follicular Lymphoma
Because FL can transform into DLBCL with accumu-lated genetic mutations, staging is critical to identify whether this has occurred. 18F-FDG PET has a special role when the most intense focus on PET should be biopsied to look for any such transformation. If the pro-cess has not transformed, staging is important. Localized
disease should be treated with involved fi eld radiother-apy (IFRT), and the addition of chemotherapy does not change survival. If disease is widespread, palliation is the aim, and initial management may be conservative. Treatment is initiated when there is bulky disease (>7 cm), more than three nodal groups are involved, or the patient has B symptoms or symptomatic splenom-egaly [140]. Usually, this will be with combined ritux-imab and chemotherapy. Locoregional IFRT may be considered and is appropriate for ocular adnexal involve-ment. Radioimmunotherapy with 90Y-ibritumomab tiuxetan or 131I-tositumomab is also possible and is currently being evaluated. Advanced multiply relapsed disease may be treated with autologous stem cell transplant.
Newly diagnosed DLBCL patients are treated with curative intent. While cyclophosphamide, adriamycin, vincristine, and prednisone (CHOP) is the preferred chemotheraputic regime, R-CHOP has been shown to improve survival in a number of randomized controlled trials [25, 47, 60, 124, 125].
1.12 Mantle Cell Lymphoma
Th e majority of ocular adnexal cases are secondary. R-CHOP for systemic MCL is associated with a 50% response rate, with duration of eff ect of less than 2 years. Th is lesion usually requires aggressive treatment with alternating or sequential non-cross-reacting chemother-apy regimes, giving a remission rate of 90%. Despite con-solidation treatment with chemotherapy and autologous stem cell transplantation, overall 5-year disease-free sur-vival is around 50% [40, 84, 90, 100, 102, 149]. One prom-ising recent report of 21 cases of orbital or adnexal MCL found 80% 5-year survival in patients treated with ritux-imab and chemotherapy compared with an 8% 5-year survival in patients not treated with rituximab [127].
T-cell lymphomas are a diverse group of poorly under-stood entities that may rarely behave moderately aggres-sively and be curable, but more commonly they are aggressive and associated with a poor outcome. Th e ocu-lar adnexa may be involved secondarily or less frequently as a primary process [27, 84, 149, 156].
1.13 Radiotherapy
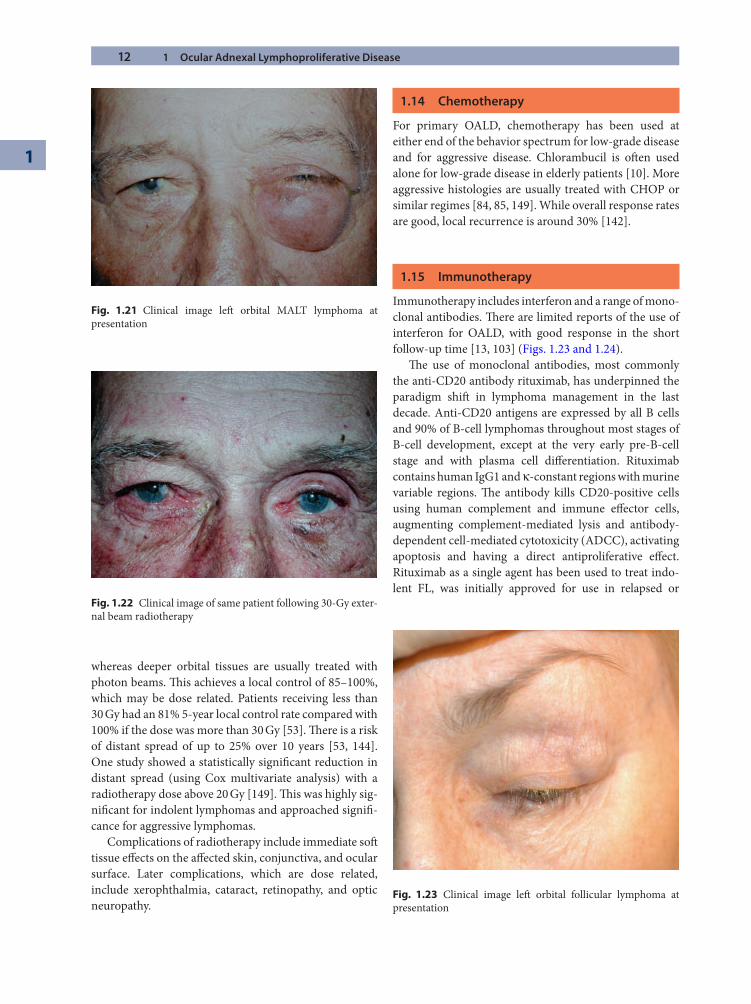
Having said all this, radiotherapy is currently the most common fi rst-line treatment for primary OALD (Figs. 1.21 and 1.22). Superfi cial conjunctival and anterior orbital lesions are usually treated with electron beams,
Fig. 1.20 PET scan showing systemic involvement with MALT lymphoma
12 1 Ocular Adnexal Lymphoproliferative Disease
1
whereas deeper orbital tissues are usually treated with photon beams. Th is achieves a local control of 85–100%, which may be dose related. Patients receiving less than 30 Gy had an 81% 5-year local control rate compared with 100% if the dose was more than 30 Gy [53]. Th ere is a risk of distant spread of up to 25% over 10 years [53, 144]. One study showed a statistically signifi cant reduction in distant spread (using Cox multivariate analysis) with a radiotherapy dose above 20 Gy [149]. Th is was highly sig-nifi cant for indolent lymphomas and approached signifi -cance for aggressive lymphomas.
Complications of radiotherapy include immediate soft tissue eff ects on the aff ected skin, conjunctiva, and ocular surface. Later complications, which are dose related, include xerophthalmia, cataract, retinopathy, and optic neuropathy.
1.14 Chemotherapy
For primary OALD, chemotherapy has been used at either end of the behavior spectrum for low-grade disease and for aggressive disease. Chlorambucil is oft en used alone for low-grade disease in elderly patients [10]. More aggressive histologies are usually treated with CHOP or similar regimes [84, 85, 149]. While overall response rates are good, local recurrence is around 30% [142].
1.15 Immunotherapy
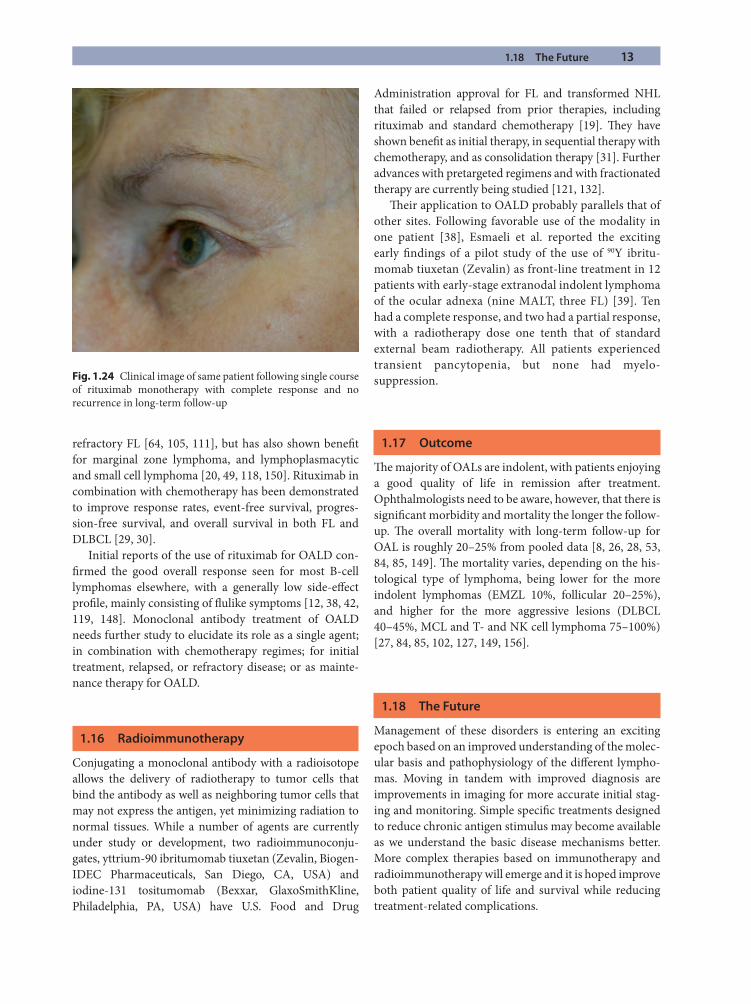
Immunotherapy includes interferon and a range of mono-clonal antibodies. Th ere are limited reports of the use of interferon for OALD, with good response in the short follow-up time [13, 103] (Figs. 1.23 and 1.24).
Th e use of monoclonal antibodies, most commonly the anti-CD20 antibody rituximab, has underpinned the paradigm shift in lymphoma management in the last decade. Anti-CD20 antigens are expressed by all B cells and 90% of B-cell lymphomas throughout most stages of B-cell development, except at the very early pre-B-cell stage and with plasma cell diff erentiation. Rituximab contains human IgG1 and κ-constant regions with murine variable regions. Th e antibody kills CD20-positive cells using human complement and immune eff ector cells, augmenting complement-mediated lysis and antibody-dependent cell-mediated cytotoxicity (ADCC), activating apoptosis and having a direct antiproliferative eff ect. Rituximab as a single agent has been used to treat indo-lent FL, was initially approved for use in relapsed or
Fig. 1.21 Clinical image left orbital MALT lymphoma at presentation
Fig. 1.22 Clinical image of same patient following 30-Gy exter-nal beam radiotherapy
Fig. 1.23 Clinical image left orbital follicular lymphoma at presentation
1.18 The Future 13
refractory FL [64, 105, 111], but has also shown benefi t for marginal zone lymphoma, and lymphoplasmacytic and small cell lymphoma [20, 49, 118, 150]. Rituximab in combination with chemotherapy has been demonstrated to improve response rates, event-free survival, progres-sion-free survival, and overall survival in both FL and DLBCL [29, 30].
Initial reports of the use of rituximab for OALD con-fi rmed the good overall response seen for most B-cell lymphomas elsewhere, with a generally low side-eff ect profi le, mainly consisting of fl ulike symptoms [12, 38, 42, 119, 148]. Monoclonal antibody treatment of OALD needs further study to elucidate its role as a single agent; in combination with chemotherapy regimes; for initial treatment, relapsed, or refractory disease; or as mainte-nance therapy for OALD.
1.16 Radioimmunotherapy
Conjugating a monoclonal antibody with a radioisotope allows the delivery of radiotherapy to tumor cells that bind the antibody as well as neighboring tumor cells that may not express the antigen, yet minimizing radiation to normal tissues. While a number of agents are currently under study or development, two radioimmunoconju-gates, yttrium-90 ibritumomab tiuxetan (Zevalin, Biogen-IDEC Pharmaceuticals, San Diego, CA, USA) and iodine-131 tositumomab (Bexxar, GlaxoSmithKline, Philadelphia, PA, USA) have U.S. Food and Drug
Administration approval for FL and transformed NHL that failed or relapsed from prior therapies, including rituximab and standard chemotherapy [19]. Th ey have shown benefi t as initial therapy, in sequential therapy with chemotherapy, and as consolidation therapy [31]. Further advances with pretargeted regimens and with fractionated therapy are currently being studied [121, 132].
Th eir application to OALD probably parallels that of other sites. Following favorable use of the modality in one patient [38], Esmaeli et al. reported the exciting early fi ndings of a pilot study of the use of 90Y ibritu-momab tiuxetan (Zevalin) as front-line treatment in 12 patients with early-stage extranodal indolent lymphoma of the ocular adnexa (nine MALT, three FL) [39]. Ten had a complete response, and two had a partial response, with a radiotherapy dose one tenth that of standard external beam radiotherapy. All patients experienced transient pancytopenia, but none had myelo-suppression.
1.17 Outcome
Th e majority of OALs are indolent, with patients enjoying a good quality of life in remission aft er treatment. Ophthalmologists need to be aware, however, that there is signifi cant morbidity and mortality the longer the follow-up. Th e overall mortality with long-term follow-up for OAL is roughly 20–25% from pooled data [8, 26, 28, 53, 84, 85, 149]. Th e mortality varies, depending on the his-tological type of lymphoma, being lower for the more indolent lymphomas (EMZL 10%, follicular 20–25%), and higher for the more aggressive lesions (DLBCL 40–45%, MCL and T- and NK cell lymphoma 75–100%) [27, 84, 85, 102, 127, 149, 156].
1.18 The Future
Management of these disorders is entering an exciting epoch based on an improved understanding of the molec-ular basis and pathophysiology of the diff erent lympho-mas. Moving in tandem with improved diagnosis are improvements in imaging for more accurate initial stag-ing and monitoring. Simple specifi c treatments designed to reduce chronic antigen stimulus may become available as we understand the basic disease mechanisms better. More complex therapies based on immunotherapy and radioimmunotherapy will emerge and it is hoped improve both patient quality of life and survival while reducing treatment-related complications.
Fig. 1.24 Clinical image of same patient following single course of rituximab monotherapy with complete response and no recurrence in long-term follow-up
14 1 Ocular Adnexal Lymphoproliferative Disease
1
References
1. Abramson DH, Rollins I, Coleman M (2005) Periocular mucosa-associated lymphoid/low grade lymphomas: treat-ment with antibiotics. Am J Ophthalmol 140:729–730
2. Adami J, Frisch M, Yuen J, et al (1995) Evidence of an asso-ciation between non-Hodgkin’s lymphoma and skin can-cer. BMJ 310:1491–1495
3. Agostinelli C, Piccaluga P, Went P (2008) Peripheral T cell lymphoma, not otherwise specifi ed: the stuff of genes, dreams and therapies. J Clin Pathol 61:1160–1167
4. Aifantis I, Raetz E, Buonamici S (2008) Molecular patho-genesis of T-cell leukaemia and lymphoma. Nat Rev Immunol 8:380–390
5. Allen-Auerbach M, Quon A, Weber WA, et al (2004) Comparison between 2-deoxy-2-[18F]fl uoro-D-glucose positron emission tomography and positron emission tomography/computed tomography hardware fusion for staging of patients with lymphoma. Mol Imaging Biol 6:411–416
6. Allen-Auerbach M, de Vos S, Czernin J (2008) Th e impact of fl uorodeoxyglucose-positron emission tomography in primary staging and patient management in lymphoma patients. Radiol Clin N Am 46:199–121
7. Australian Cancer Network Diagnosis and Management of Lymphoma Guidelines Working Party. Guidelines for the diagnosis and management of lymphoma. Th e Cancer Council Australia and Australian Cancer Network, Sydney 2005
8. Auw-Haedrich C, Coupland SE, Kapp A, et al (2001) Long term outcome of ocular adnexal lymphoma subtyped according to the REAL classifi cation. Br J Ophthalmol 85:63–69
9. Bahler D, Szankasi P, Kulkarni S (2009) Use of similar immunoglobulin VH gene segments by MALT lymphomas of the ocular adnexa. Mod Pathol. doi:10.1038/modpathol. 2009.42
10. Ben Simon GJ, Cheung N, McKelvie P, et al (2006) Oral chlorambucil for extranodal, marginal zone, B-cell lym-phoma of mucosa associated lymphoid tissue of the orbit. Ophthalmology 113:1209–1213
11. Bende R, Smit L, van Noesel C (2007) Molecular pathways in follicular lymphoma. Leukemia 2:18–29
12. Benetatos L, Alymara V, Asproudis I, et al (2006) Rituximab as fi rst line treatment for MALT lymphoma of extraocular muscles. Ann Hematol 85:625–626
13. Blasi MA, Gherlinzoni F, Calvisi G, et al (2001) Local che-motherapy with interferon-alpha for conjunctival mucosa-associated lymphoid tissue lymphoma: a preliminary report. Ophthalmology 108:559–562
14. Byrne GI, Ojcius DM (2004) Chlamydia and apoptosis: life and death decisions of an intracellular pathogen. Nat Rev Microbiol 2:802–808
15. Cahill M, Barnes C, Moriarty P, et al (1999) Ocular adnexal lymphoma–a comparison of MALT lymphoma with other histological types. Br J Ophthalmol 83:742–747
16. Campbell L (2005) Cytogenetics of lymphomas. Pathology 37:493–507
17. Carbonne PP, Kaplan HS, Mushoff HS, et al (1971) Report of the nomenclature committee on Hodgkin’s disease stag-ing. Cancer Res 311:860–861
18. Chan-Kai B, Yen M (2005) Combined PET/CT imaging of orbital lymphoma. Am J Ophthalmol 140:531–533
19. Cheson BD (2003) Radioimmunotherapy of non-Hodgkin’s lymphomas. Blood 101:391–398
20. Cheson BD, Leonard JP (2008) Monoclonal antibody ther-apy for B-cell non-Hodgkin’s lymphoma. N Engl J Med 359: 613–626
21. Ci W, Polo J, Melnick A (2008) B-cell lymphoma 6 and the molecular pathogenesis of diff use large B-cell lymphoma. Curr Opin Hematol 15:381–390
22. Clarke CA, Glaser SL (2002) Changing incidence of non-Hodgkin lymphomas in the United States. Cancer 94: 2015–2023
23. Cleary ML, Sklar J (1984) Lymphoproliferative disorders in cardiac transplant recipients are multiclonal lymphomas. Lancet ii 8401:489–493
24. Coff ee R, Lazarchick J, Chévez-Barios P, et al (2005) Rapid diagnosis of orbital mantle cell lymphoma utilizing fl uo-rescent in situ hybridization technology. Am J Ophthalmol 140:554–555
25. Coiffi er B, Lepage E, Briere J, et al (2002) CHOP chemo-therapy plus rituximab compared with CHOP alone in elderly patients with diff use large-B-cell lymphoma. N Engl J Med 346:235–242
26. Coupland SE, Krause L, Delecluse HJ, et al (1998) Lymphoproliferative lesions of the ocular adnexa. Analysis of 112 cases. Ophthalmology 105:1430–1441
27. Coupland SE, Foss H-D, Assaf C, et al (1999) T-cell and T/natural killer-cell lymphomas involving ocular and ocular adnexal tissues. Ophthalmology 106:2109–2120
28. Coupland SE, Hellmich M, Auw-Haedrich C, et al (2004) Prognostic value of cell-cycle markers in ocular adnexal lymphoma: an assessment of 230 cases Graefe’s. Arch Clin Exp Ophthalmol 242:130–145
29. Czuczman MS, Weaver R, Alkuzweny B, et al (2004) Prolonged clinical and molecular remission in patients with low-grade or follicular non-Hodgkin’s lymphoma treated with rituximab plus CHOP chemotherapy: 9-year follow-up. J Clin Oncol 22:4711–6 [Erratum (2005) J Clin Oncol 23 248]
30. Czuczman MS, Koryzna A, Mohr A, et al (2005) Rituximab in combination with fl udarabine chemotherapy in low-grade or follicular lymphoma. J Clin Oncol 23:694–704
31. Davies AJ (2007) Radioimmunotherapy for B-cell lym-phoma: Y90 ibritumomab tiuxetan and I131 tositumomab. Oncogene 26:3614–3628
References 15
32. De Paepe P, de Wolf-Peeters C (2007) Diff use large B-cell lymphoma: a heterogeneous group of non-Hodgkin lym-phomas comprising several distinct clinicopathological entities. Leukemia 21:37–43
33. Decaudin D, Dendale R, Lumbroso-Le R (2008) Treatment of mucosa-associated lymphoid tissue-type ocular adnexal lymphoma. Anticancer Drugs 19:673–680
34. Decaudin D, Dolcetti R, deCremoux P, et al (2008) Variable association between Chlamydia psittaci infection and ocu-lar adnexal lymphomas: methodological biases or true geographical variation? Anticancer Drugs 19:761–765
35. Demirci H, Shields CL, Karatza EC, et al (2008) Orbital lymphoproliferative tumors analysis of clinical features and systemic involvement in 160 cases. Ophthalmology 115:1626–1631
36. Devesa SS, Fears T (1992) Non-Hodgkin’s lymphoma time trends: United States and international data. Cancer Res 52(19 Suppl):5432s–54340s
37. Ellis JH, Banks PM, Campbell RJ, et al (1985) Lymphoid tumors of the ocular adnexa. Clinical correlation with the working formulation classifi cation and immunoperoxidase staining of paraffi n sections. Ophthalmol 92:1311–1324
38. Esmaeli B, Murray JL, Ahmadi MA, et al (2002) Immuno-therapy for low-grade non-Hodgkin secondary lymphoma of the orbit. Arch Ophthalmol 120:1225–1227
39. Esmaeli B, McLaughlin P, Pro B, et al (2009) Prospective trial of targeted radioimmunotherapy with Y-90 ibritu-momab tiuxetan (Zevalin) for front-line treatment of early-stage extranodal indolent ocular adnexal lymphoma. Ann Oncol 20:709–714
40. Evens AM, Winter JN, Hou N, et al (2008) A phase II clinical trial of intensive chemotherapy followed by consolidative stem cell transplant: long-term follow-up in newly diagnosed mantle cell lymphoma. Br J Haematol 140: 385–393
41. Ferreri AJ, Guidoboni M, De Conciliis C, et al (2004) Evidence for an association between Chlamydia psittaci and ocular adnexal lymphomas. J Natl Cancer Inst 96:586–594
42. Ferreri AJ, Ponzoni M, Martinelli G, et al (2005) Rituximab in patients with mucosal-associated lymphoid tissue-type lymphoma of the ocular adnexa. Haematologica 90: 1578–1579
43. Ferreri AJ, Viale E, Guidoboni M, et al (2006) Clinical implications of hepatitis C virus infection in MALT-type lymphoma of the ocular adnexa. Ann Oncol 17:769–772
44. Ferreri AJ, Dolcetti R, Du M-Q, et al (2008) Ocular adnexal MALT lymphoma: an intriguing model for antigen-driven lymphomagenesis and microbial-targeted therapy. Ann Oncol 19:835–846
45. Ferry JA, Fung CY, Zukerberg L, et al (2007) Lymphoma of the ocular adnexa: a study of 353 cases. Am J Surg Pathol 31:170–184
46. Filipovich AH, Mathur A, Karmat D, et al (1992) Primary immunodefi ciencies: genetic risk factors for lymphoma. Cancer Res 52(19 Suppl):5465s–5467s
47. Fisher RI, Gaynor ER, Dahlberg S, et al (1993) Comparison of a standard regimen (CHOP) with three intensive che-motherapy regimens for advanced non-Hodgkin’s lym-phoma. N Engl J Med 328:1002–1006
48. Fisher S, Fisher R (2004) Th e epidemiology of non-Hodgkin’s lymphoma. Oncogene 23:6524–6534
49. Foran JM, Rohatiner AZ, Cunningham D, et al (2000) European phase II study of rituximab (chimeric anti-CD20 monoclonal antibody) for patients with newly diagnosed mantle-cell lymphoma and previously treated mantle-cell lymphoma, immunocytoma, and small B-cell lymphocytic lymphoma. J Clin Oncol 18:317–324 [Erratum (2000) J Clin Oncol 18:2006]
50. Freeman C, Berg JW, Cutler SJ (1972) Occurrence and prognosis of extranodal lymphomas. Cancer 29:252–260
51. Freidberg J, Fisher R (2008) Diff use large B-cell lymphoma. Hematol Oncol Clin N Am 22:941–952.
52. Fueger B, Yeom K, Czernin J, et al (2009) Comparison of CT, PET, and PET/CT for staging of patients with indolent non-Hodgkin’s lymphoma. Mol Imaging Biol. (Epub 20 Mar 2009)
53. Fung CY, Tarbell NJ, Lacarelli MJ, et al (2003) Ocular adn-exal lymphoma: clinical behaviour of distinct World Health Organization classifi cation subtypes. Int J Radiat Oncol Biol Phys 57:1382–1391
54. Garner A, Rai AH, Wright JE (1983) Lymphoproliferative disorders of the orbit: an immunological approach to diag-nosis and pathogenesis. Br J Ophthalmol 67:561–569
55. Gausas RE, Gonnering RS, Lemke B, et al (1999) Identifi cation of human orbital lymphatics. Ophthal Plast Reconstr Surg 15:252–259
56. Gausas RE, Daly T, Fogt F (2007) D2-40 expression demon-strates lymphatic vessel characteristics in the dural portion of the optic nerve sheath. Ophthal Plast Reconstr Surg 23:32–36
57. Gayed I, Eskandari F, McLaughlin P, et al (2007) Value of positron emission tomography in staging ocular adnexal lymphomas and evaluating their response to therapy oph-thalmic. Surg Lasers Imaging 38:319–325
58. Goedert JJ (2000). Th e epidemiology of acquired immu-nodefi ciency syndrome malignancies. Semin Oncol 27: 390–401
59. Grünberger B, Hauff W, Lukas J, et al (2006) “Blind” antibi-otic treatment targeting Chlamydia is not eff ective in patients with MALT lymphoma of the ocular adnexa. Ann Oncol 17:484–487
60. Habermann TM, Weller EA, Morrison VA, et al (2006) Rituximab-CHOP versus CHOP alone or with mainte-nance rituximab in older patients with diff use large B-cell lymphoma. J Clin Oncol 24:3121–3127
16 1 Ocular Adnexal Lymphoproliferative Disease
1
61. Harris NL (2001) Mature B-cell neoplasms: introduction. In: Jaff e ES, Harris NL, Stein H, Vardiman JW (eds) Pathology and genetics of tumours of haematopoietic and lymphoid tissue. IARC Press, Lyon, pp 121–126
62. Harris NL, Isaacson PG (1999) What are the criteria for dis-tinguishing MALT from non-MALT lymphoma at extran-odal sites? Am J Clin Pathol 111(Suppl 1): S126–S1332
63. Henderson JW (1994) Hemotopoietic tumors. In: Henderson JW (ed) Orbital tumors, 3rd ed. Raven, New York, pp 279–307
64. Hiddemann W, Kneba M, Dreyling M, et al (2005) Frontline therapy with rituximab added to the combina-tion of cylophosphamide, doxorubicin, vincristine, and prednisone (CHOP) signifi cantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: results of a pro-spective randomized study of the German Low-Grade Lymphoma Study Group. Blood 106:3725–3732
65. Hu S, Federman D, Ma F, et al (2005) Skin cancer and non-Hodgkin’s lymphoma: examining the link. Dermatol Surg 31:76–82
66. Husain A, Roberts D, Pro B, et al (2007) Meta-analyses of the association between Chlamydia psittaci and ocular adnexal lymphoma and the response of ocular adnexal lymphoma to antibiotics. Cancer 110:809–815
67. Hutchings M, Specht L (2008) PET/CT in the management of haematological malignancies. J Haematol 80:369–380
68. Isaacson PG (1999) Mucosa-associated lymphoid tissue lymphoma. Semin Hematol 36:139–147
69. Isaacson PG (2000) Th e current status of lymphoma clas-sifi cation. Br J Haematol 109:258–266
70. Isaacson PG, Wright DH (1983) Malignant lymphoma of mucosa-associated lymphoid tissue. Cancer 52:1410–1416
71. Isaacson PG, Wright DH (1984) Extranodal malignant lymphoma arising from mucosa-associated lymphoid tis-sue. Cancer 53:2515–2524
72. Isaacson PG, Muler-Hermelink HK, Piris MA, et al (2001) Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma). In: Jaff e ES, Harris NL, Stein H, Vardiman JW (eds) Pathology and genetics of tumors of haematopoietic and lymphoid tissue. IARC Press, Lyon, pp 157–160
73. Jaff e ES, Harris NL, Diebold J, et al (1999) World health organisation classifi cation of neoplastic disease of the hematopoietic and lymphoid tissues. Am J Clin Pathol 111(Suppl):S8–S12
74. Jakobiec FA (1982) Orbital infl ammations and lymphoid tumours. Trans New Orleans Acad Ophthalmol 30:52–85
75. Jakobiec FA (1983) Ocular infl ammatory disease: the lym-phocyte redivivus. Am J Ophthalmol 96:384–391
76. Jakobiec FA, Knowles DM (1989) An overview of ocular adnexal lymphoid tumors. Trans Am Ophthalmol Soc 87: 420–442
77. Jakobiec FA, McLean I, Font RL (1979) Clinicopathologic characteristics of orbital lymphoid hyperplasia. Ophthal-mology 86:948–966
78. Jakobiec FA, Iwamoto T, Knowles DM (1982) Ocular adnexal lymphoid tumors. Correlative ultrastructural and immunologic marker studies. Arch Ophthalmol 100:84–98
79. Jakobiec FA, Iwamoto T, Patell M, et al (1986) Ocular adn-exal monoclonal lymphoid tumors with a favourable prog-nosis. Ophthalmology 93:1547–1557
80. Jakobiec FA, Neri A, Knowles DM (1987) Genotypic monoclonality in immunophenotypically polyclonal orbital lymphoid tumors. A model of tumor progression in the lymphoid system. Ophthalmology 94:980–994
81. Jardin F, Ruminy P, Bastard C, et al (2007) Th e BCL6 proto-oncogene: a leading role during germinal center develop-ment and lymphomagenesis. Pathol Biologie 55:73–83
82. Jares P, Colomer D, Campo E (2007) Genetic and molecu-lar pathogenesis of mantle cell lymphoma: perspectives for new targeted therapeutics. Nat Rev Cancer 7:750–762
83. Jemal A, Siegel R, Ward E, et al (2008) Cancer statistics. CA Cancer J Clin 58:71–96. (Epub 20 Feb 2008)
84. Jenkins C, Rose GE, Bunce C, et al (2000) Histological fea-tures of ocular adnexal lymphoma (REAL classifi cation) and their association with patient morbidity and survival. Br J Ophthalmol 84:907–913
85. Jenkins C, Rose GE, Bunce C, et al (2003) Clinical features associated with survival of patients with lymphoma of the ocular adnexa. Eye 17:809–820
86. Jensen A, Olesen A, Dethlefsen C, et al (2008) Chronic dis-eases requiring hospitalization and risk of non-melanoma skin cancers—a population based study from Denmark. J Invest Dermatol 128:926–931
87. Jost PJ, Ruland J (2007) Aberrant NFkappaB signaling in lymphoma: mechanisms, consequences, and therapeutic implications. Blood 109: 2700–2707
88. Juweid M, Cheson B (2006) Positron-emission tomogra-phy and assessment of cancer therapy. N Engl J Med 354: 496–507
89. Kadin M (2003) Genetic and molecular genetic studies in the diagnosis of T-cell malignancies. Hum Pathol 34: 322–329
90. Khouri IF, Romaguera J, Kantarjian H, et al (1998) Hyper-CVAD and high-dose methotrexate/cytarabine followed by stem-cell transplantation: an active regimen for aggres-sive mantle-cell lymphoma. J Clin Oncol 16:3803–3809
91. Kinlen L (1992) Immunosuppressive therapy and acquired immunological disorders. Cancer Res 52(19 Suppl): 5474s–5476s
92. Knop E, Knop N (2001) Lacrimal drainage—associated lymphoid tissue (LDALT): a part of the human mucosal immune system. Invest Ophthalmol Vis Sci 42:566–574
93. Knop E, Knop N 2005 Th e role of eye-associated lymphoid tissue in corneal immune protection. J Anat 206: 271–285
References 17
94. Knowles DM, Jakobiec FA (1980) Orbital lymphoid neo-plasms: a clinicopathologic study of 60 patients. Cancer 46: 576–589
95. Knowles DM, Jakobiec FA (1982) Ocular adnexal lymphoid neoplasms: clinical, histopathologic, electron microscopic, and immunologic characteristics. Hum Pathol 13:148–162
96. Knowles DM, Jakobiec FA, Halper JP (1979) Immunologic characterization of ocular adnexal lymphoid neoplasms. Am J Ophthalmol 87:603–619
97. Knowles DM, Halper JP, Jakobiec FA (1982) Th e immu-nologic characterization of 40 extranodal lymphoid infi l-trates: in distinguishing between benign pseudolymphoma and malignant lymphoma. Cancer 49:2321–2335
98. Knowles DM, Jakobiec FA, McNally L (1990) Lymphoid hyperplasia and malignant lymphoma occurring in the ocular adnexa (orbit, conjunctiva, and eyelids): a pro-spective multiparametric analysis of 108 cases during 1977 to 1987. Hum Pathol 21:959–973
99. Küppers R, Klein U, Hansmann M-L, et al (1999) Cellular origin of human B-cell lymphomas. N Engl J Med 341(20):1520–1529
100. Lenz G, Dreyling M, Hoster E, et al (2005) Immuno-chemotherapy with rituximab and cyclophosphamide, doxorubicin, vincristine, and prednisone signifi cantly improves response and time to treatment failure, but not long-term outcome in patients with previously untreated mantle cell lymphoma: results of a prospective random-ized trial of the German Low Grade Lymphoma Study Group (GLSG). J Clin Oncol 23:1984–1992
101. Li BZ, Lu HF, Zhou XY, et al (2008) Frequency of genetic aberrations of mucosa-associated lymphoid tissue lym-phoma of diff erent sites. Zhonghua Bing Li Xue Za Zhi 37:604–608
102. Looi A, Gascoyne RD, Chaanabhai M, et al (2005) Mantle cell lymphoma in the ocular adnexal region. Ophthalmology 112:114–119
103. Lucas RS, Mortimore R, Sullivan TJ, et al (2003) Interferon treatment of childhood conjunctival lymphoma. Br J Ophthalmol 87:1191
104. Mannami T, Yoshino T, Oshima K, et al (2001) Clinical, histopathological, and immunogenetic analysis of ocular adnexal lymphoproliferative disorders: characterization of MALT lymphoma and reactive lymphoid hyperplasia. Mod Pathol 14:641–649
105. Marcus R, Imrie K, Solal-Celigny P, et al (2008) A phase III study of rituximab plus CVP versus CVP alone in patients with previously untreated advanced follicular lymphoma: updated results with 53 months’ median follow-up and analysis of outcomes according to baseline prognostic fac-tors. J Clin Oncol 26(28):4579–86.
106. Margo CE, Mulla ZD (1998) Malignant tumors of the orbit. Analysis of the Florida Cancer Registry. Ophthal-mology 105:185–190
107. Matthews JM, Moreno LI, Dennis J, et al (2008) Ocular adnexal lymphoma: no evidence for bacterial DNA asso-ciated with lymphoma pathogenesis. Br J Haematol. (Epub ahead of print 19 May 2008)
108. Medeiros LJ, Harris NL (1989) Lymphoid infi ltrates of the orbit and conjunctiva. A morphologic and immunophe-notypic study of 99 cases. Am J Surg Pathol 13:459–471
109. Medeiros LJ, Harris NL (1990) Immunohistologic analy-sis of small lymphocytic infi ltrates of the orbit and con-junctiva. Hum Pathol 21:1126–1131
110. Medeiros LJ, Harmon DC, Linggood RM, et al (1989) Immunohistologic features predict clinical behaviour of orbital and conjunctival lymphoid infi ltrates. Blood 74: 2121–2129
111. McLaughlin P, Grillo-López AJ, Link BK, et al (1998) Rituximab chimeric anti-CD20 monoclonal antibody therapy of relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. J Clin Oncol 16:2825–2833
112. Miyairi I, Byrne GI (2006) Chlamydia and programmed cell death. Curr Opin Microbiol 9:102–108
113. McKelvie PA, McNab AA, Francis IC, et al (2001) Ocular adnexal lymphoproliferative disease: a series of 73 cases. Clin Exp Ophthalmol 29:387–393
114. Morgan G (1975) Lymphocytic tumours of the orbit. Mod Probl Ophthalmol 14:355–360
115. Morgan G, Harry J (1978) Lymphocytic tumours of inde-terminate nature: a 5-year follow-up of 98 conjunctival and orbital lesions. Br J Ophthalmol 62:381–383
116. Moslehi R, Devesa SS, Schairer C, et al (2006) Rapidly increasing incidence of ocular non-Hodgkin lymphoma. J Natl Cancer Inst 98:936–939
117. Nakata M, Matsuno Y, Katsumata N, et al (1999) Histology according to the revised European-American lymphoma classifi cation signifi cantly predicts the prognosis of ocu-lar adnexal lymphoma. Leuk Lymphoma 32:533–543
118. Nguyen DT, Amess JA, Doughty H, et al (1999) IDEC-C2B8 anti-CD20 (rituximab) immunotherapy in patients with low-grade non-Hodgkin’s lymphoma and lymphop-roliferative disorders: evaluation of response on 48 patients. Eur J Haematol 62:76–82
119. Nuckel H, Meller D, Steuhl KP, et al (2004) Anti-CD20 monoclonal antibody therapy in relapsed MALT lym-phoma of the conjunctiva. Eur J Haematol 73:258–262
120. Nutting CM, Shah-Desai S, Rose GE, et al (2006) Th yroid orbitopathy possibly predisposes to late-onset of periocu-lar lymphoma. Eye 20:645–648
121. Otte A, van de Wiele C, Dierckx RA (2009) Radiolabeled immunotherapy in non-Hodgkin’s lymphoma treatment: the next step. Nucl Med Commun 30:5–15
122. Pals ST, De Gorter DJ Spaargaren M (2007) Lymphoma dissemination: the other face of lymphocyte homing. Blood 110:3102–3111
18 1 Ocular Adnexal Lymphoproliferative Disease
1
123. Perry C, Herishanu Y, Metzer U, et al (2007) Diagnostic accuracy of PET/CT in patients with extranodal marginal zone MALT lymphoma. Eur J Haematol 79:205–209
124. Pfreundschuh M, Trumper L, Osterborg A, et al (2006) CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diff use large-B-cell lymphoma: a randomised controlled trial by the Mab-Th era International Trial (MInT) Group. Lancet Oncol 7:379–391
125. Pfreundschuh M, Schubert J, Ziepert M, et al (2008) Six versus eight cycles of bi-weekly CHOP-14 with or without rituximab in elderly patients with aggressive CD20 B-cell lymphomas: a randomised controlled trial (RICOVER-60). Lancet Oncol 9:105–116
126. Polito E, Galieni P, Leccisotti A (1996) Clinical and radio-logical presentation of 95 orbital lymphoid tumors. Graefes Arch Clin Exp Ophthalmol 234:504–509
127. Rasmussen P, Sjo LD, Prause JU (2009) Mantle cell lym-phoma in the orbital and adnexal region. Br J Ophthalmol. (Epub ahead of print 7 May 2009)
128. Roe R, Finger PT, Kurli M, et al (2006) Whole-body posi-tron emission tomography/computed tomography imag-ing and staging of orbital lymphoma. Ophthalmology 113: 1854–1858
129. Romagosa Y, Hu S, Kirsner R (2008) Chronic diseases and non-Melanoma skin cancer: is there an association? J Invest Dermatol 128:768
130. Roos E (1991) Adhesion molecules in lymphoma metas-tasis. Cancer Metastasis Rev 10:33–48
131. Schotterfi eld D, Beebe-Dimmer J (2006) Chronic infl am-mation: a common and important factor in the pathogen-esis of neoplasia. CA Cancer J Clin 56:69–83
132. Sharkey RM, Press OW, Goldenberg DM (2009) A re-examination of radioimmunotherapy in the treatment of non-Hodgkins lymphoma: prospects for dual-targeted antibody/radioantibody therapy. Blood 113:3891–3895
133. Shen D, Yuen HKL (2006) Detection of chlamydia pneu-monia in a bilateral orbital mucosa-associated lymphoid tissue lymphoma. Am J Ophthalmol 141:1162–1163
134. Shields JA (1989) Lymphoid tumors and leukemias. In: Shileds JA, Saunders WB (eds). Diagnosis and manage-ment of orbital tumors. Lippincott, Philadelphia, pp 316–340
135. Shipp MA, Harrington DP, Anderson JR, et al (1993) International Non-Hodgkin’s Lymphoma Prognostic Factors Project. N Engl J Med 329(14):987–994
136. Sjo LD (2009) Ophthalmic lymphoma: epidemiology and pathogenesis. Acta Ophthalmol 87 Th esis 1:1–20
137. Sjo LD, Ralfk iaer E, Prause JU, et al (2008) Increasing incidence of ophthalmic lymphoma in Denmark from 1980 to 2005. Invest Ophthalmol Vis Sci 49:3283–3288
138. Smith JS, Munoz N, Herrero R, et al (2002) Evidence for Chlamydia trachomatis as a human papillomavirus cofac-
tor in the etiology of invasive cervical cancer in Brazil and the Philippines. J Infect Dis 185:324–331
139. Smith M (2008) Mantle cell lymphoma: advances in biol-ogy and therapy. Curr Opin Hematol 15:415–421
140. Solal-Celigny P, Lepage E, Brousse N, et al (1993) Recombinant interferon alfa-2b combined with a regi-men containing doxorubicin in patients with advanced follicular lymphoma. Groupe d’Etude des Lymphomes de l’Adulte. N Engl J Med 329:1608–1614
141. Solal-Seligny P, Roy P, Colombat P, et al (2004) Follicular lymphoma international prognostic index. Blood 104:1258–1265
142. Song EK, Kim SY, Kim TM et al (2008) Effi cacy of chemo-therapy as a fi rst-line treatment in ocular adnexal extran-odal marginal zone B-cell lymphoma. Ann Oncol 19: 242–246
143. Spagnolo DV, Ellis DW, Juneja S, et al (2004) Th e role of molecular studies in lymphoma diagnosis: a review. Pathology 36:19–44
144. Stefanovic A, Lossos I (2009) Extranodal marginal zone lymphoma of the ocular adnexa. Blood. (Prepublished online 16 April 2009)
145. Stein H (2001) Hodgkin lymphomas: introduction. In: Jaff e ES, Harris NL, Stein H, Vardiman JW (eds) Pathology and genetics of tumours of haematopoietic and lymphoid tissue. IARC Press, Lyon, p 239
146. Streubel B, Simonitsch-Klupp I, Mullauer L, et al (2004) Variable frequencies of MALT lymphoma-associated genetic aberrations in MALT lymphomas of diff erent sites. Leukemia 18:1722–1726
147. Sullivan TJ, Valenzuela AA (2006) Imaging features of ocular adnexal lymphoproliferative disease. Eye 20: 1189–1195
148. Sullivan TJ, Grimes D, Bunce I (2004) Monoclonal anti-body treatment of orbital lymphoma. Ophthal Plast Reconstr Surg 20:103–106
149. Sullivan TJ, Whitehead K, Williamson R, et al (2005) Lymphoproliferative disease of the ocular adnexa: a clini-cal and pathologic study with statistical analysis of 69 patients. Ophthal Plast Reconstr Surg 21:177–188
150. Treon SP, Agus DB, Link B, et al (2001) CD20-directed antibody-mediated immunotherapy induces responses and facilitates hematologic recovery in patients with Waldenstrom’s macroglobulinemia. J Immunother 24: 272–279
151. Valenzuela AA, Allen C, Grimes D, et al (2006) Positron emission tomography in the detection and staging of ocu-lar adnexal lymphoproliferative disease. Ophthalmology 113:2331–2337
152. Westacott S, Garner A, Moseley IF, et al (1991) Orbital lymphoma vs reactive lymphoid hyperplasia: an analysis of the use of computed tomography in diff erential diag-nosis. Br J Ophthalmol 75:722–725
References 19
153. White VA, Gascoyne RD, McNeil BK, et al (1996) Histopathologic fi ndings and frequency of clonality detected by the polymerase chain reaction in ocular adn-exal lymphoproliferative lesions. Mod Pathol 9: 1052–1061
154. White WL, Ferry JA, Harris NL, et al (1995) Ocular adn-exal lymphoma. A clinicopathologic study with identifi -cation of lymphomas of mucosa-associated lymphoid tissue type. Ophthalmology 102:1994–2006
155. Whiteside TL, Rowlands DT Jr (1977) T-cell and B-cell identifi cation in the diagnosis of lymphoproliferative dis-ease. A review. Am J Pathol 88:754–792
156. Woog JJ, Kim YK, Yeatts RP, et al (2006) Natural killer/T-cell lymphoma with ocular and adnexal involvement. Ophthalmology 113:140–145
157. Wündisch T, Th iede C, Morgner A, et al (2005) Long-term follow-up of gastric MALT lymphoma aft er Helicobacter pylori eradication. J Clin Oncol 23: 8018–8024
158. Yeo JH, Jakobiec FA, Abbott GF, et al (1982) Combined clinical and computed tomographic diagnosis of orbital lymphoid tumors. Am J Ophthalmol 94:235–245
159. Zhang G, Winter J, Variakojis D (2007) Lack of an asso-ciation between Chlamydia psittaci and ocular adnexal lymphoma. Leuk Lymphoma 48:577–583

Pearls in Cosmetic Oculofacial Plastic SurgeryJonathan A. Hoenig
Chapter 2
2.1 General Introduction
Twenty years ago, life for the oculoplastic surgeon was relatively simple. If a patient presented with a problem, there were limited options to address the problem. As surgeons, we were good at removing tissue: fat, muscle, and skin. For example, if a patient presented with lower eyelid “bags,” the fat was always removed, while the skin would either be removed or be resurfaced. Most patients were treated in a similar manner despite signifi cant ana-tomic diff erences. Most surgeons and patients were rela-tively happy with the surgical results. Th e reality is that we did not know any better. Th en came the Internet.
Th e Internet allowed patients and physicians to share and gather information. We all became more sophisti-cated. A variety of injectable fi llers came on the market. Our whole philosophy of the aging process suddenly changed.
Today, we are blessed with an array of options to reju-venate the periocular region. Th ere are multiple surgical and nonsurgical options. However, with all the various options, confusion ensues. What technique do we use to rejuvenate the lower eyelids? Do we use fi ller or fat? Who needs a transcutaneous blepharoplasty, and who is a bet-ter candidate for a transconjunctival incision? I oft en hear, “What about a midface lift , doctor?” “My friend read on the Internet that to fi x lower eyelid bags you need to put in an orbital rim implant.” “How about a laser or a peel?” Th e combination of solutions can get dizzying.
Th is chapter summarizes my personal experience and philosophy on what techniques seem to be the most eff ec-tive. Many of these ideas are based on work described by others. Th e purpose of this chapter is to show the reader and surgeon my path through the mountain of options that are now available. Th e chapter is organized into sec-tions for brow lift s, upper blepharoplasty, and lower
2
Core Messages
Analyze the Face in Layers: Aging occurs in the ■
skin, muscle, fat, and bony layers. Th e key for suc-cessful and consistent results is to defi ne the ana-tomic problem and select procedures that address these problems.Do not sacrifi ce function for beauty. It is impera- ■
tive that the patient and surgeon come to an under-standing that function always supersedes beauty. Th e eyelids are unique in that they serve a vital function: to protect the eye. It is sometimes diffi -cult for the patient to understand that, for example, the wrinkles that are still present aft er surgery are in actuality the skin necessary for eyelid closure.Endoscopic Brow Lift : Th e goal of a brow lift is ■
less about lift ing and more about contouring the shape of the brow. In women, the brow is elevated in a superior/medial vector. In men, the brow is elevated superiorly so that the brow becomes
straight and forms a T confi guration with the nose.Upper Blepharoplasty: An upper blepharoplasty ■
procedure cannot cure brow ptosis. If the brow is ptotic, correct the brow. Th e goal of upper bleph-aroplasty is defi nition and subbrow fullness. Blepharoplasty is not about how much skin and fat you take out but how much tissue you leave in. Preserving the pretarsal and preseptal orbicularis is necessary for proper eyelid function.Lower Blepharoplasty: Th e goal of lower bleph- ■
aroplasty is restoration of the youthful contour of the eyelid and midface. Th is consists of a verti-cally short lower eyelid and a full, convex midface. Analysis of the lower eyelid involves the relation-ship between the globe and inferior orbital rim projection, orbital fat protrusion, and midfacial fat loss and skin elasticity versus excess.
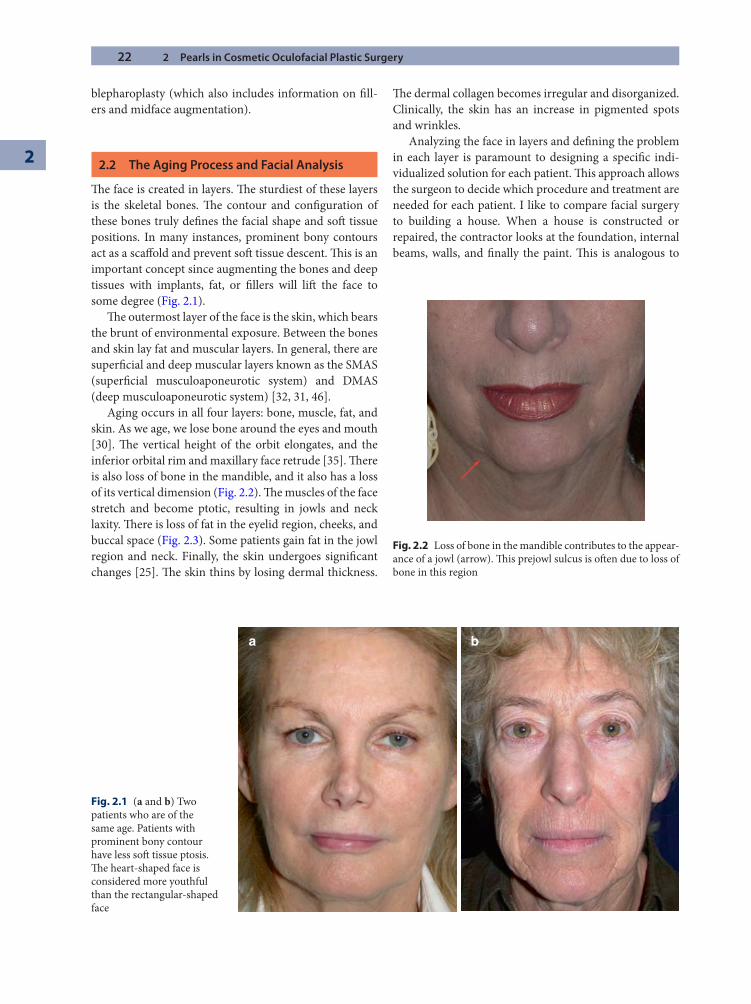
22 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
blepharoplasty (which also includes information on fi ll-ers and midface augmentation).
2.2 The Aging Process and Facial Analysis
Th e face is created in layers. Th e sturdiest of these layers is the skeletal bones. Th e contour and confi guration of these bones truly defi nes the facial shape and soft tissue positions. In many instances, prominent bony contours act as a scaff old and prevent soft tissue descent. Th is is an important concept since augmenting the bones and deep tissues with implants, fat, or fi llers will lift the face to some degree (Fig. 2.1).
Th e outermost layer of the face is the skin, which bears the brunt of environmental exposure. Between the bones and skin lay fat and muscular layers. In general, there are superfi cial and deep muscular layers known as the SMAS (superfi cial musculoaponeurotic system) and DMAS (deep musculoaponeurotic system) [32, 31, 46].
Aging occurs in all four layers: bone, muscle, fat, and skin. As we age, we lose bone around the eyes and mouth [30]. Th e vertical height of the orbit elongates, and the inferior orbital rim and maxillary face retrude [35]. Th ere is also loss of bone in the mandible, and it also has a loss of its vertical dimension (Fig. 2.2). Th e muscles of the face stretch and become ptotic, resulting in jowls and neck laxity. Th ere is loss of fat in the eyelid region, cheeks, and buccal space (Fig. 2.3). Some patients gain fat in the jowl region and neck. Finally, the skin undergoes signifi cant changes [25]. Th e skin thins by losing dermal thickness.
Th e dermal collagen becomes irregular and disorganized. Clinically, the skin has an increase in pigmented spots and wrinkles.
Analyzing the face in layers and defi ning the problem in each layer is paramount to designing a specifi c indi-vidualized solution for each patient. Th is approach allows the surgeon to decide which procedure and treatment are needed for each patient. I like to compare facial surgery to building a house. When a house is constructed or repaired, the contractor looks at the foundation, internal beams, walls, and fi nally the paint. Th is is analogous to
a b
Fig. 2.1 (a and b) Two patients who are of the same age. Patients with prominent bony contour have less soft tissue ptosis. Th e heart-shaped face is considered more youthful than the rectangular-shaped face
Fig. 2.2 Loss of bone in the mandible contributes to the appear-ance of a jowl (arrow). Th is prejowl sulcus is oft en due to loss of bone in this region
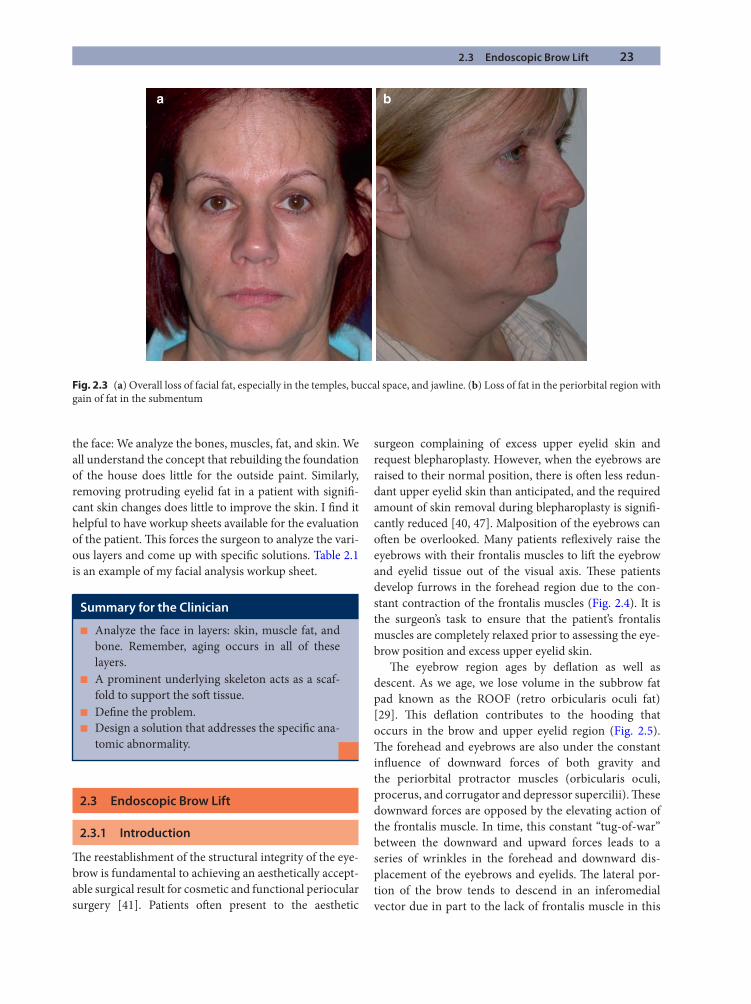
2.3 Endoscopic Brow Lift 23
the face: We analyze the bones, muscles, fat, and skin. We all understand the concept that rebuilding the foundation of the house does little for the outside paint. Similarly, removing protruding eyelid fat in a patient with signifi -cant skin changes does little to improve the skin. I fi nd it helpful to have workup sheets available for the evaluation of the patient. Th is forces the surgeon to analyze the vari-ous layers and come up with specifi c solutions. Table 2.1 is an example of my facial analysis workup sheet.
2.3 Endoscopic Brow Lift
2.3.1 Introduction
Th e reestablishment of the structural integrity of the eye-brow is fundamental to achieving an aesthetically accept-able surgical result for cosmetic and functional periocular surgery [41]. Patients oft en present to the aesthetic
surgeon complaining of excess upper eyelid skin and request blepharoplasty. However, when the eyebrows are raised to their normal position, there is oft en less redun-dant upper eyelid skin than anticipated, and the required amount of skin removal during blepharoplasty is signifi -cantly reduced [40, 47]. Malposition of the eyebrows can oft en be overlooked. Many patients refl exively raise the eyebrows with their frontalis muscles to lift the eyebrow and eyelid tissue out of the visual axis. Th ese patients develop furrows in the forehead region due to the con-stant contraction of the frontalis muscles (Fig. 2.4). It is the surgeon’s task to ensure that the patient’s frontalis muscles are completely relaxed prior to assessing the eye-brow position and excess upper eyelid skin.
Th e eyebrow region ages by defl ation as well as descent. As we age, we lose volume in the subbrow fat pad known as the ROOF (retro orbicularis oculi fat) [29]. Th is defl ation contributes to the hooding that occurs in the brow and upper eyelid region (Fig. 2.5). Th e forehead and eyebrows are also under the constant infl uence of downward forces of both gravity and the periorbital protractor muscles (orbicularis oculi, procerus, and corrugator and depressor supercilii). Th ese downward forces are opposed by the elevating action of the frontalis muscle. In time, this constant “tug-of-war” between the downward and upward forces leads to a series of wrinkles in the forehead and downward dis-placement of the eyebrows and eyelids. Th e lateral por-tion of the brow tends to descend in an inferomedial vector due in part to the lack of frontalis muscle in this
a b
Fig. 2.3 (a) Overall loss of facial fat, especially in the temples, buccal space, and jawline. (b) Loss of fat in the periorbital region with gain of fat in the submentum
Summary for the Clinician
Analyze the face in layers: skin, muscle fat, and ■
bone. Remember, aging occurs in all of these layers.A prominent underlying skeleton acts as a scaf- ■
fold to support the soft tissue.Defi ne the problem. ■
Design a solution that addresses the specifi c ana- ■
tomic abnormality.
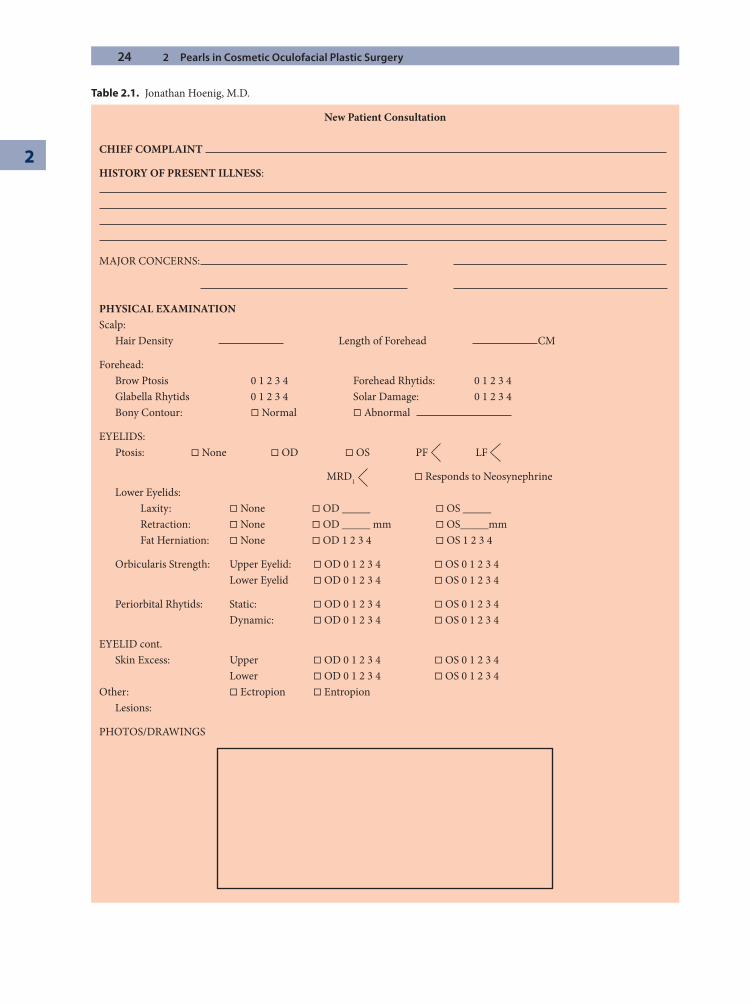
24 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
Table 2.1. Jonathan Hoenig, M.D.
New Patient Consultation
CHIEF COMPLAINT
HISTORY OF PRESENT ILLNESS:
MAJOR CONCERNS:
PHYSICAL EXAMINATIONScalp: Hair Density Length of Forehead CM
Forehead: Brow Ptosis 0 1 2 3 4 Forehead Rhytids: 0 1 2 3 4 Glabella Rhytids 0 1 2 3 4 Solar Damage: 0 1 2 3 4 Bony Contour: � Normal � Abnormal
EYELIDS: Ptosis: � None � OD � OS PF LF
MRD1 � Responds to Neosynephrine Lower Eyelids: Laxity: � None � OD _____ � OS _____ Retraction: � None � OD _____ mm � OS_____mm Fat Herniation: � None � OD 1 2 3 4 � OS 1 2 3 4
Orbicularis Strength: Upper Eyelid: � OD 0 1 2 3 4 � OS 0 1 2 3 4 Lower Eyelid � OD 0 1 2 3 4 � OS 0 1 2 3 4
Periorbital Rhytids: Static: � OD 0 1 2 3 4 � OS 0 1 2 3 4 Dynamic: � OD 0 1 2 3 4 � OS 0 1 2 3 4
EYELID cont. Skin Excess: Upper � OD 0 1 2 3 4 � OS 0 1 2 3 4 Lower � OD 0 1 2 3 4 � OS 0 1 2 3 4Other: � Ectropion � Entropion Lesions:
PHOTOS/DRAWINGS
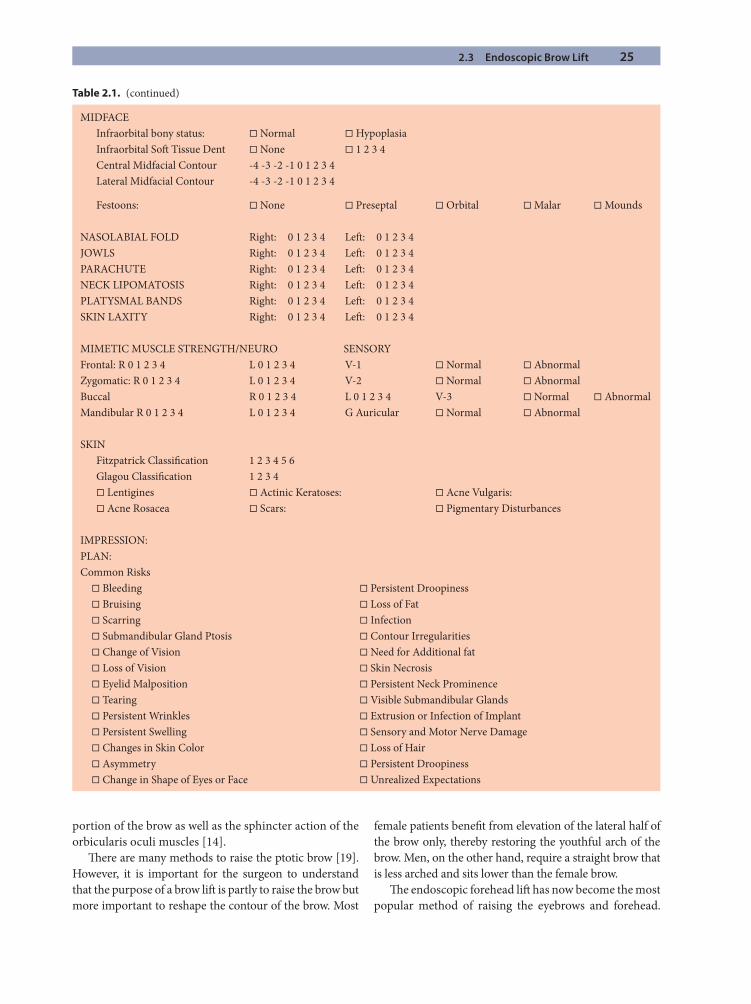
2.3 Endoscopic Brow Lift 25
MIDFACE Infraorbital bony status: � Normal � Hypoplasia Infraorbital Soft Tissue Dent � None � 1 2 3 4 Central Midfacial Contour -4 -3 -2 -1 0 1 2 3 4 Lateral Midfacial Contour -4 -3 -2 -1 0 1 2 3 4
Festoons: � None � Preseptal � Orbital � Malar � Mounds
NASOLABIAL FOLD Right: 0 1 2 3 4 Left : 0 1 2 3 4JOWLS Right: 0 1 2 3 4 Left : 0 1 2 3 4PARACHUTE Right: 0 1 2 3 4 Left : 0 1 2 3 4NECK LIPOMATOSIS Right: 0 1 2 3 4 Left : 0 1 2 3 4PLATYSMAL BANDS Right: 0 1 2 3 4 Left : 0 1 2 3 4SKIN LAXITY Right: 0 1 2 3 4 Left : 0 1 2 3 4
MIMETIC MUSCLE STRENGTH/NEURO SENSORYFrontal: R 0 1 2 3 4 L 0 1 2 3 4 V-1 � Normal � AbnormalZygomatic: R 0 1 2 3 4 L 0 1 2 3 4 V-2 � Normal � AbnormalBuccal R 0 1 2 3 4 L 0 1 2 3 4 V-3 � Normal � AbnormalMandibular R 0 1 2 3 4 L 0 1 2 3 4 G Auricular � Normal � Abnormal
SKIN Fitzpatrick Classifi cation 1 2 3 4 5 6 Glagou Classifi cation 1 2 3 4 � Lentigines � Actinic Keratoses: � Acne Vulgaris: � Acne Rosacea � Scars: � Pigmentary Disturbances
IMPRESSION:PLAN:Common Risks � Bleeding � Persistent Droopiness � Bruising � Loss of Fat � Scarring � Infection � Submandibular Gland Ptosis � Contour Irregularities � Change of Vision � Need for Additional fat � Loss of Vision � Skin Necrosis � Eyelid Malposition � Persistent Neck Prominence � Tearing � Visible Submandibular Glands � Persistent Wrinkles � Extrusion or Infection of Implant � Persistent Swelling � Sensory and Motor Nerve Damage � Changes in Skin Color � Loss of Hair � Asymmetry � Persistent Droopiness � Change in Shape of Eyes or Face � Unrealized Expectations
Table 2.1. (continued)
portion of the brow as well as the sphincter action of the orbicularis oculi muscles [14].
Th ere are many methods to raise the ptotic brow [19]. However, it is important for the surgeon to understand that the purpose of a brow lift is partly to raise the brow but more important to reshape the contour of the brow. Most
female patients benefi t from elevation of the lateral half of the brow only, thereby restoring the youthful arch of the brow. Men, on the other hand, require a straight brow that is less arched and sits lower than the female brow.
Th e endoscopic forehead lift has now become the most popular method of raising the eyebrows and forehead.
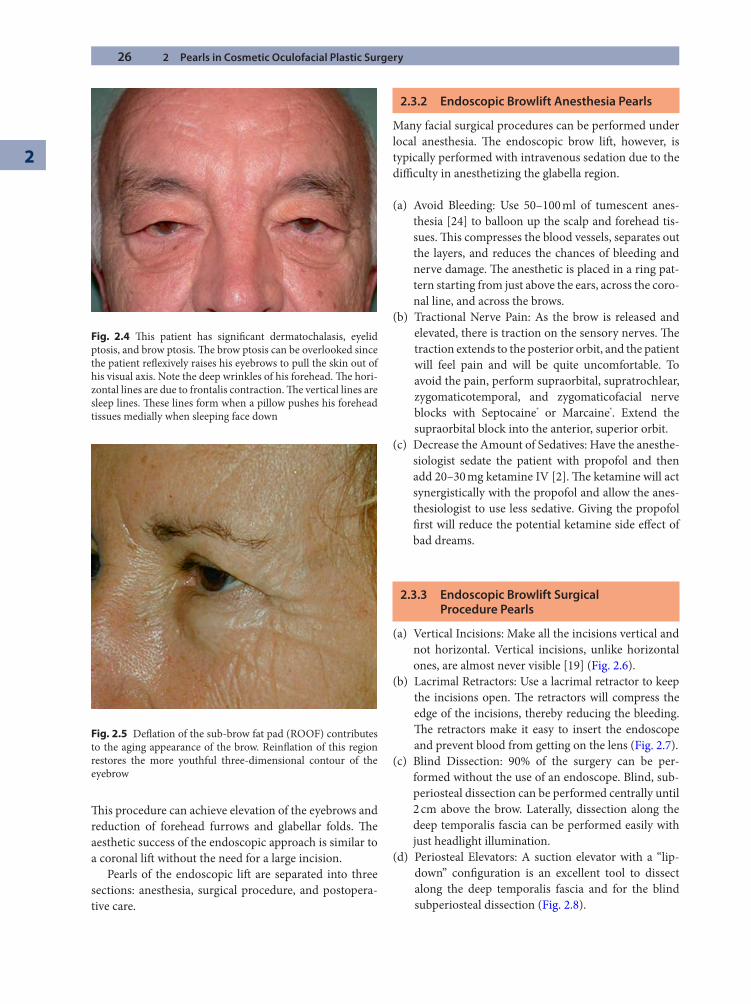
26 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
Th is procedure can achieve elevation of the eyebrows and reduction of forehead furrows and glabellar folds. Th e aesthetic success of the endoscopic approach is similar to a coronal lift without the need for a large incision.
Pearls of the endoscopic lift are separated into three sections: anesthesia, surgical procedure, and postopera-tive care.
2.3.2 Endoscopic Browlift Anesthesia Pearls
Many facial surgical procedures can be performed under local anesthesia. Th e endoscopic brow lift , however, is typically performed with intravenous sedation due to the diffi culty in anesthetizing the glabella region.
(a) Avoid Bleeding: Use 50–100 ml of tumescent anes-thesia [24] to balloon up the scalp and forehead tis-sues. Th is compresses the blood vessels, separates out the layers, and reduces the chances of bleeding and nerve damage. Th e anesthetic is placed in a ring pat-tern starting from just above the ears, across the coro-nal line, and across the brows.
(b) Tractional Nerve Pain: As the brow is released and elevated, there is traction on the sensory nerves. Th e traction extends to the posterior orbit, and the patient will feel pain and will be quite uncomfortable. To avoid the pain, perform supraorbital, supratrochlear, zygomaticotemporal, and zygomaticofacial nerve blocks with Septocaine® or Marcaine®. Extend the supraorbital block into the anterior, superior orbit.
(c) Decrease the Amount of Sedatives: Have the anesthe-siologist sedate the patient with propofol and then add 20–30 mg ketamine IV [2]. Th e ketamine will act synergistically with the propofol and allow the anes-thesiologist to use less sedative. Giving the propofol fi rst will reduce the potential ketamine side eff ect of bad dreams.
2.3.3 Endoscopic Browlift Surgical Procedure Pearls
(a) Vertical Incisions: Make all the incisions vertical and not horizontal. Vertical incisions, unlike horizontal ones, are almost never visible [19] (Fig. 2.6).
(b) Lacrimal Retractors: Use a lacrimal retractor to keep the incisions open. Th e retractors will compress the edge of the incisions, thereby reducing the bleeding. Th e retractors make it easy to insert the endoscope and prevent blood from getting on the lens (Fig. 2.7).
(c) Blind Dissection: 90% of the surgery can be per-formed without the use of an endoscope. Blind, sub-periosteal dissection can be performed centrally until 2 cm above the brow. Laterally, dissection along the deep temporalis fascia can be performed easily with just headlight illumination.
(d) Periosteal Elevators: A suction elevator with a “lip-down” confi guration is an excellent tool to dissect along the deep temporalis fascia and for the blind subperiosteal dissection (Fig. 2.8).
Fig. 2.4 Th is patient has signifi cant dermatochalasis, eyelid ptosis, and brow ptosis. Th e brow ptosis can be overlooked since the patient refl exively raises his eyebrows to pull the skin out of his visual axis. Note the deep wrinkles of his forehead. Th e hori-zontal lines are due to frontalis contraction. Th e vertical lines are sleep lines. Th ese lines form when a pillow pushes his forehead tissues medially when sleeping face down
Fig. 2.5 Defl ation of the sub-brow fat pad (ROOF) contributes to the aging appearance of the brow. Reinfl ation of this region restores the more youthful three-dimensional contour of the eyebrow
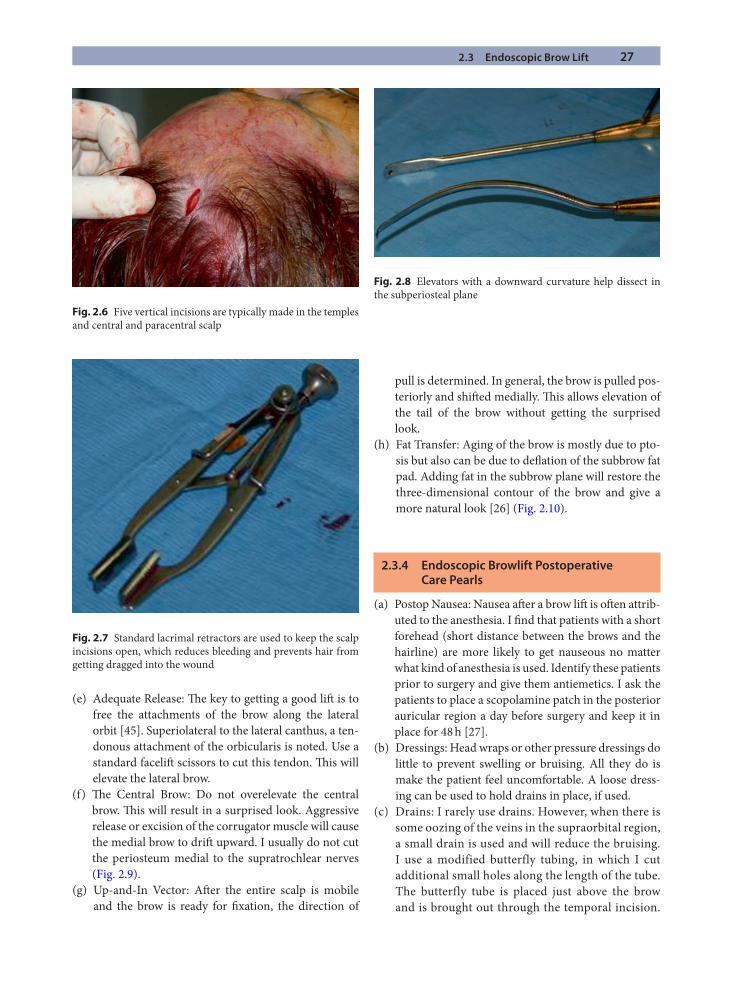
2.3 Endoscopic Brow Lift 27
(e) Adequate Release: Th e key to getting a good lift is to free the attachments of the brow along the lateral orbit [45]. Superiolateral to the lateral canthus, a ten-donous attachment of the orbicularis is noted. Use a standard facelift scissors to cut this tendon. Th is will elevate the lateral brow.
(f) Th e Central Brow: Do not overelevate the central brow. Th is will result in a surprised look. Aggressive release or excision of the corrugator muscle will cause the medial brow to drift upward. I usually do not cut the periosteum medial to the supratrochlear nerves (Fig. 2.9).
(g) Up-and-In Vector: Aft er the entire scalp is mobile and the brow is ready for fi xation, the direction of
pull is determined. In general, the brow is pulled pos-teriorly and shift ed medially. Th is allows elevation of the tail of the brow without getting the surprised look.
(h) Fat Transfer: Aging of the brow is mostly due to pto-sis but also can be due to defl ation of the subbrow fat pad. Adding fat in the subbrow plane will restore the three-dimensional contour of the brow and give a more natural look [26] (Fig. 2.10).
2.3.4 Endoscopic Browlift Postoperative Care Pearls
(a) Postop Nausea: Nausea aft er a brow lift is oft en attrib-uted to the anesthesia. I fi nd that patients with a short forehead (short distance between the brows and the hairline) are more likely to get nauseous no matter what kind of anesthesia is used. Identify these patients prior to surgery and give them antiemetics. I ask the patients to place a scopolamine patch in the posterior auricular region a day before surgery and keep it in place for 48 h [27].
(b) Dressings: Head wraps or other pressure dressings do little to prevent swelling or bruising. All they do is make the patient feel uncomfortable. A loose dress-ing can be used to hold drains in place, if used.
(c) Drains: I rarely use drains. However, when there is some oozing of the veins in the supraorbital region, a small drain is used and will reduce the bruising. I use a modified butterfly tubing, in which I cut additional small holes along the length of the tube. The butterfly tube is placed just above the brow and is brought out through the temporal incision.
Fig. 2.6 Five vertical incisions are typically made in the temples and central and paracentral scalp
Fig. 2.7 Standard lacrimal retractors are used to keep the scalp incisions open, which reduces bleeding and prevents hair from getting dragged into the wound
Fig. 2.8 Elevators with a downward curvature help dissect in the subperiosteal plane
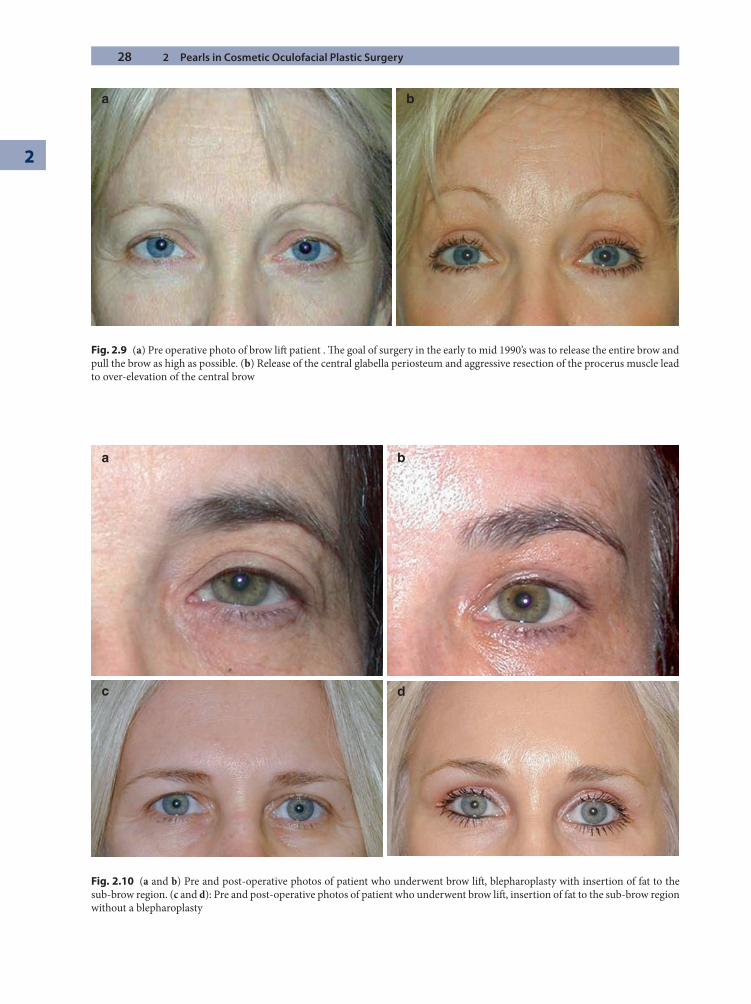
28 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
a b
Fig. 2.9 (a) Pre operative photo of brow lift patient . Th e goal of surgery in the early to mid 1990’s was to release the entire brow and pull the brow as high as possible. (b) Release of the central glabella periosteum and aggressive resection of the procerus muscle lead to over-elevation of the central brow
c d
a b
Fig. 2.10 (a and b) Pre and post-operative photos of patient who underwent brow lift , blepharoplasty with insertion of fat to the sub-brow region. (c and d): Pre and post-operative photos of patient who underwent brow lift , insertion of fat to the sub-brow region without a blepharoplasty
2.4 Upper Blepharoplasty 29
It is then attached to a red-top blood collection tube.
(d) Showering: Have patients shower and wash their hair on postop day 2. Th is will get the incisions clean and make the patients feel much better.
(e) Strict Salt Avoidance: Canned foods, Asian food, and Mexican food all have high sodium content. Eating these in the early postop period will result in a lot of swelling.
(f) Sleeping Pattern: Have patients sleep on the back for the fi rst 2 weeks aft er surgery. Sleeping on the side or on the stomach will cause the edema to settle in the eye region. A cervical pillow, available at most back stores, will help the patients unaccustomed to sleep-ing on the back.
(g) Botox®: Inject Botox in the glabella region within the fi rst week of surgery. Th is will weaken the brow depressors and prevent the brow from getting pulled down during the fi rst 3 months aft er surgery. Th is will increase the longevity of the browlift results [4]. During the fi rst postoperative week, the brow and forehead region is typically numb, and the patients do not mind the injections.
2.4 Upper Blepharoplasty
2.4.1 Introduction
Th e upper eyelid forms the lowest portion of the fore-head/eyebrow/eyelid continuum. As noted, it is extremely important to take into account brow position before deciding on the degree of “laxity” of the upper eyelids. Th e eyelids are unique in that they are regarded in both their aesthetic and functional sense. It is imperative that the surgeon prioritize function over beauty.
2.4.2 Patient Evaluation
Patients presenting for blepharoplasty are evaluated in a similar manner to those patients presenting for brow lift . Th e eyelids are evaluated in layers: skin, muscle, fat, and bone. Th e skin of the eyelid is extremely thin and stretches over time. When considering the amount of skin that is “redundant,” it is important to keep in mind that there is a minimal amount of skin that is necessary to ensure proper eyelid function [39]. Patients with prominent eyes will require more skin since the eyelid has to cover a greater convex surface. It is also imperative that the sur-geon keep in mind that the degree of dermatochalasis is based on brow position. Due to gravitational eff ects, the position of the eyebrow will be lower when the patient is upright. When the patient is supine, the brow will be in a higher position, thus requiring more skin for the eyelids to close properly. Th is is the reason why many patients who seem to have enough eyelid skin when we evaluate them in our offi ce actually have nocturnal lagophthal-mus. Th e most important concept in blepharoplasty is not about how much skin you take out but how much you leave. Remember also that a blepharoplasty cannot cure brow ptosis.
Th e orbicularis oculi is separated into three portions: pretarsal, preseptal, and orbital. Th e pretarsal and presep-tal portions of the eyelid are needed for proper eyelid clo-sure [36]. Removal of too much orbicularis oculi muscle will aff ect blinking and lead to dry eyes. For this reason, currently we remove less muscle during blepharoplasty than we did in the past.
Th e upper eyelid fat pockets contribute to the fullness of the upper eyelids [34]. In decades past, a hollow upper lid with a high lid crease was considered aesthetically pleasing. Fullness is now in vogue and considered a sign of youth. It is the role of the surgeon to decide how much upper eyelid fat to remove. In general, I remove a moder-ate amount of the medial fat pad while removing little to none of the central eyelid fat pad.
Th e sub-brow fat pad known as the ROOF is evalu-ated. As we age, there is defl ation of this fat, which con-tributes to the apparent redundancy of the eyebrow and eyelid skin. Reinfl ating this fat pad improves the three-dimensional contours of the brow and eyelids. Hyaluronic acid fi llers and fat are oft en used as substrates [10].
Th e bones of the orbit consist of the zygoma and the frontal bone. It is important to carefully evaluate the bony contour of the superior orbit. Asymmetries are noted as well as convexities and concavities of the bone. Th e larger the bone is, the greater the foundational eff ects the bone exerts on the overlying soft tissue. Th us, it is common to
Summary for the Clinician: Endoscopic Brow Lift
Tumesce the incisions and supraorbital region. ■
Use ■ Septocaine for nerve blocks, propofol and ketamine intravenously.Make short, vertical incisions. ■
Add volume: Learn how to inject fat. ■
Shift the forehead up and in. ■
Botox ■ the brow depressors postop.Identify the short-forehead patients; have them ■
use scopolamine.
30 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
see one brow higher than another due to more prominent bone on the side with the higher eyebrow. Th ese asym-metries are diffi cult to correct by manipulating the soft tissue. Th e only long-standing solution is to correct the bony asymmetry.
Upper blepharoplasty is a technically simple surgery. Th ere are only a handful of upper blepharoplasty tech-niques that are utilized [8]. However, blepharoplasty is oft en combined with other procedures, such as volume enhancement of the subbrow, brow-lift ing and brow-sta-bilizing techniques, ptosis repair, lacrimal gland reposi-tioning [23], and upper eyelid crease formation. Knowing when these adjunct procedures are necessary is the key to achieving great results. Th e pearls of upper blepharo-plasty are separated into those for anesthesia and procedures.
2.4.3 Upper Blepharoplasty Anesthesia Pearls
Upper blepharoplasty can easily be performed under local anesthesia. For patients who are anxious, 10 mg of diazepam is given orally 45 min prior to surgery [18]. I fi nd it helpful for the patients to cooperate during surgery by opening and closing their eyes.
(a) Topical Anesthesia: Use a topical anesthetic to blunt the pain of the local injection [33]. A combination of tetracaine, lidocaine, and prilocaine cream is placed on the eyelid for 30 min prior to the procedure.
(b) Local Anesthetic Choice: I prefer to use articaine (Septocaine) to inject the upper eyelids. Articaine is a dental anesthetic that is pH balanced and stings much less than lidocaine. It gives a dense block and is longer lasting than lidocaine. However, it takes sev-eral minutes to take eff ect.
(c) Timing of Local Anesthetic Injection: I prefer to inject the local anesthetic prior to marking the upper eyelid. Th is puts the skin on stretch and gives me an accurate idea of the amount of eyelid skin. Since the pretarsal skin is on stretch, the location of the antici-pated lid crease becomes more accurate.
2.4.4 Upper Blepharoplasty Surgical Procedure Pearls
(a) Marking: Th e proposed new lid crease height is marked with a thin marking pen. Th e proposed skin incision is an ellipse that is greater in vertical dimen-sion laterally. Typically in women, the inferior por-tion of the incision is marked at 9–10 mm. In a man,
it is marked at 8 mm. In an Asian, depending on the tarsal height, it is 6–7 mm [6]. Th e inferior border of the eyebrow skin is marked. Th e eyebrow skin is thicker than the eyelid skin, and the junction between the eyebrow and eyelid skin can be easily determined. Do not use the inferior brow cilia as a guide since many women pluck these hairs. Measure 13–15 mm inferior to the eyebrow/eyelid junction. Th is point will be the superior portion of the incision. Th is will guarantee that a minimum of 23–25 mm of eyelid skin will be left in the eyelid aft er the blepharoplasty. In a more prominent eye, more skin is left than a deeper-set eye.
(b) Skin/Muscle Excision: Traditionally, blepharoplasty involved removing the same amount of skin and muscle, usually in an en bloc fashion. Currently, none or a minimal amount of orbicularis oculi is removed. Th us, the skin is fi rst excised and dissected off of the underlying muscle. If the goal of surgery is to volu-mize the region inferior to the superior orbital rim, no muscle is removed [8]. Fat can also be injected in the subbrow region. If a more sculpted look is desired, a small portion of the preseptal orbicularis is removed across the eyelid, usually more in the lateral portion of the lid.
(c) Crease Formation in the Lateral Th ird of the Lid: Defi ning the contour of the lateral portion of the lid is key to achieving aesthetically acceptable results in blepharoplasty. In patients with brow ptosis, elevat-ing the lateral portion of the brow will improve the contour of the lateral portion of the lid. In patients with minimal brow ptosis or those who refuse a brow lift , redefi ning the contour of the orbital rim will mit-igate the illusion of hooding. Th is can be achieved by suturing the superior cut edge of the orbicularis to the arcus marginalis in the lateral third of the lid [50]. Th ese sutures support the subbrow fat pad and invagi-nate the skin and orbicularis so that they follow the contour of the orbital rim (Fig. 2.11).
(d) Management of Excess Lateral Skin: Oft en, there is excess skin in the lateral portion of the lid. To address this “dog-ear,” many surgeons extend the incision laterally toward the thicker lateral canthal skin. However, dissection and skin excision in the thick lateral orbital region oft en result in a visible scar. To manage the extra skin an “M-”plasty is used that reduces the length of the extended scar by 50% [1, 7, 47] (Fig. 2.12).
(e) Volumizing the Brow: Increasing the volume of the brow results in a more aesthetically pleasing contour of the upper eyelid. Th e defl ation of the subbrow fat pad contributes to the dermatochalasis of the upper
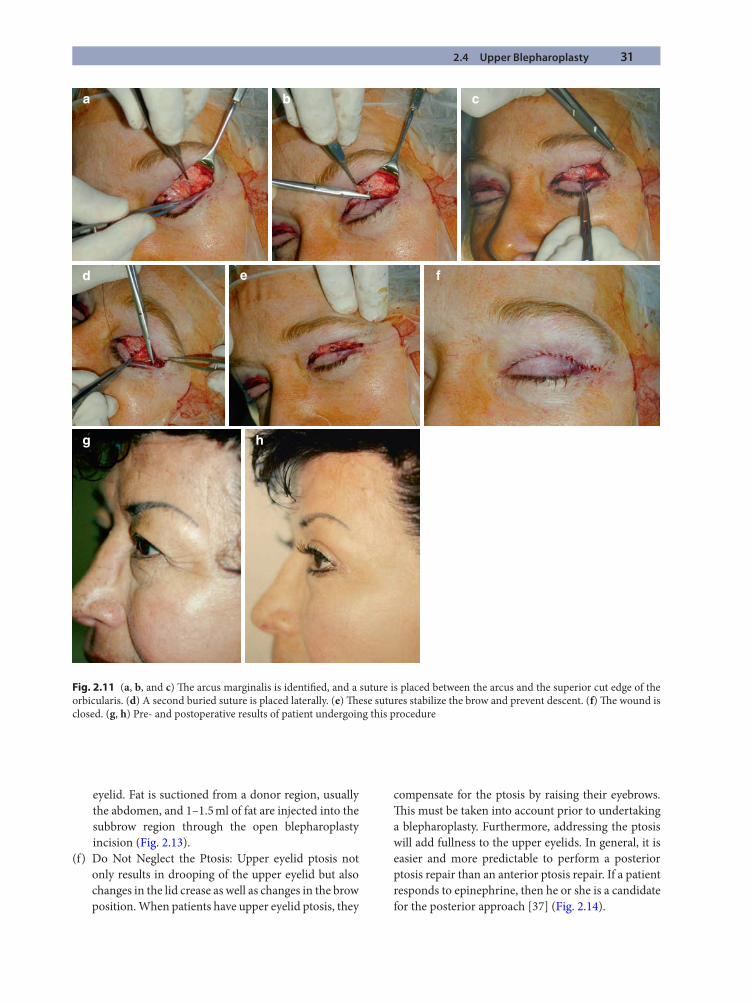
2.4 Upper Blepharoplasty 31
a b
e
g h
f
c
d
Fig. 2.11 (a, b, and c) Th e arcus marginalis is identifi ed, and a suture is placed between the arcus and the superior cut edge of the orbicularis. (d) A second buried suture is placed laterally. (e) Th ese sutures stabilize the brow and prevent descent. (f) Th e wound is closed. (g, h) Pre- and postoperative results of patient undergoing this procedure
eyelid. Fat is suctioned from a donor region, usually the abdomen, and 1–1.5 ml of fat are injected into the subbrow region through the open blepharoplasty incision (Fig. 2.13).
(f) Do Not Neglect the Ptosis: Upper eyelid ptosis not only results in drooping of the upper eyelid but also changes in the lid crease as well as changes in the brow position. When patients have upper eyelid ptosis, they
compensate for the ptosis by raising their eyebrows. Th is must be taken into account prior to undertaking a blepharoplasty. Furthermore, addressing the ptosis will add fullness to the upper eyelids. In general, it is easier and more predictable to perform a posterior ptosis repair than an anterior ptosis repair. If a patient responds to epinephrine, then he or she is a candidate for the posterior approach [37] (Fig. 2.14).

32 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
“M” Plasty Ellipsea
c d
b
Fig. 2.12 (a) Upper blepharoplasty incision closed with lateral M plasty. (b) Th e M plasty reduces the scar length by 50% compared to a standard ellipse. (c and d) Pre- and postoperative patient who underwent upper blepharoplasty. Th e patient has excess lateral skin, which would force the incision to extend lateral to the canthus. Th e M plasty keeps the scar within the orbital region
a b c
Fig. 2.13 (a) Fat is transferred to the suborbicularis region of the subbrow with multiple passes using a cannula. (b and c) Pre- and postoperative results of blepharoplasty and fat transfer
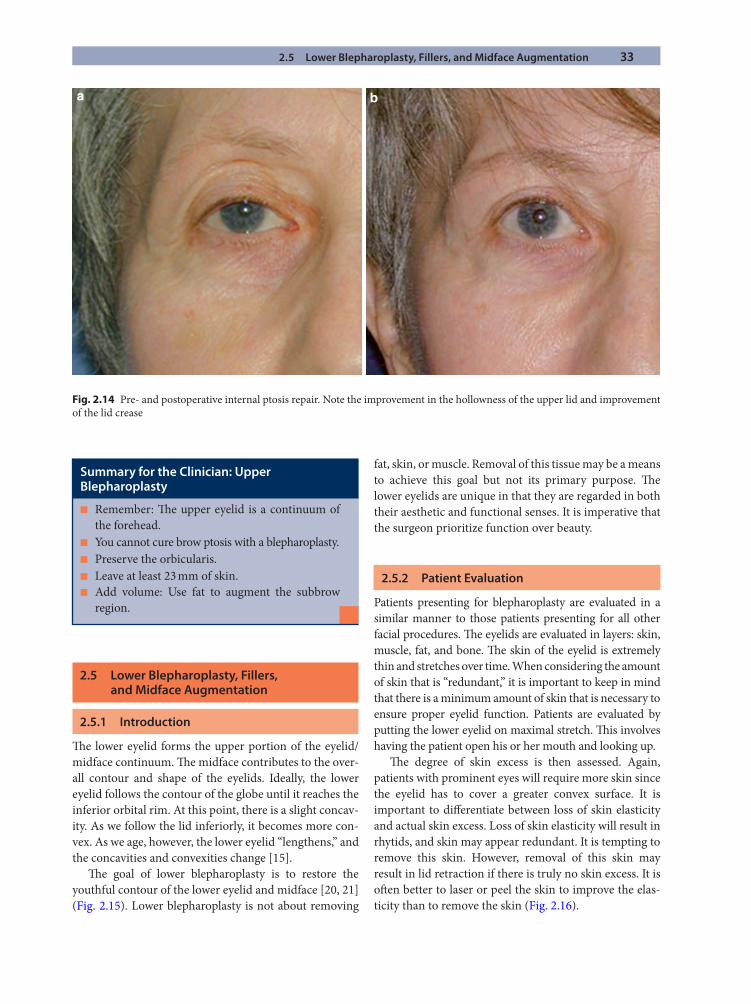
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation 33
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation
2.5.1 Introduction
Th e lower eyelid forms the upper portion of the eyelid/midface continuum. Th e midface contributes to the over-all contour and shape of the eyelids. Ideally, the lower eyelid follows the contour of the globe until it reaches the inferior orbital rim. At this point, there is a slight concav-ity. As we follow the lid inferiorly, it becomes more con-vex. As we age, however, the lower eyelid “lengthens,” and the concavities and convexities change [15].
Th e goal of lower blepharoplasty is to restore the youthful contour of the lower eyelid and midface [20, 21] (Fig. 2.15). Lower blepharoplasty is not about removing
fat, skin, or muscle. Removal of this tissue may be a means to achieve this goal but not its primary purpose. Th e lower eyelids are unique in that they are regarded in both their aesthetic and functional senses. It is imperative that the surgeon prioritize function over beauty.
2.5.2 Patient Evaluation
Patients presenting for blepharoplasty are evaluated in a similar manner to those patients presenting for all other facial procedures. Th e eyelids are evaluated in layers: skin, muscle, fat, and bone. Th e skin of the eyelid is extremely thin and stretches over time. When considering the amount of skin that is “redundant,” it is important to keep in mind that there is a minimum amount of skin that is necessary to ensure proper eyelid function. Patients are evaluated by putting the lower eyelid on maximal stretch. Th is involves having the patient open his or her mouth and looking up.
Th e degree of skin excess is then assessed. Again, patients with prominent eyes will require more skin since the eyelid has to cover a greater convex surface. It is important to diff erentiate between loss of skin elasticity and actual skin excess. Loss of skin elasticity will result in rhytids, and skin may appear redundant. It is tempting to remove this skin. However, removal of this skin may result in lid retraction if there is truly no skin excess. It is oft en better to laser or peel the skin to improve the elas-ticity than to remove the skin (Fig. 2.16).
a b
Fig. 2.14 Pre- and postoperative internal ptosis repair. Note the improvement in the hollowness of the upper lid and improvement of the lid crease
Summary for the Clinician: Upper Blepharoplasty
Remember: Th e upper eyelid is a continuum of ■
the forehead.You cannot cure brow ptosis with a blepharoplasty. ■
Preserve the orbicularis. ■
Leave at least 23 mm of skin. ■
Add volume: Use fat to augment the subbrow ■
region.
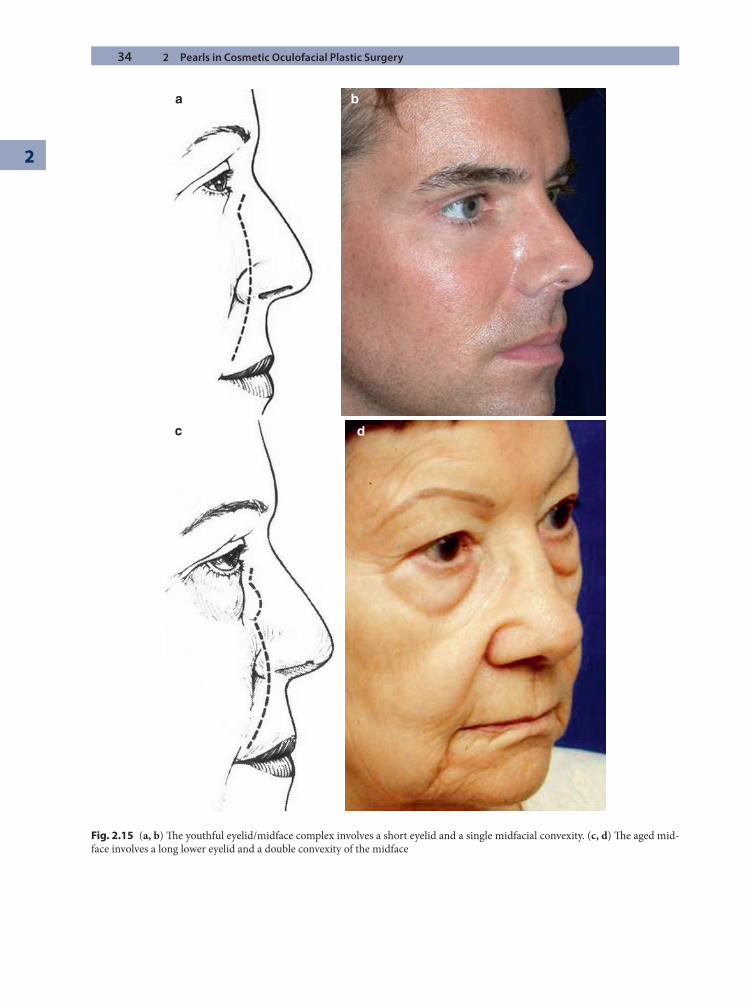
34 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
Fig. 2.15 (a, b) Th e youthful eyelid/midface complex involves a short eyelid and a single midfacial convexity. (c, d) Th e aged mid-face involves a long lower eyelid and a double convexity of the midface
c
b
d
a
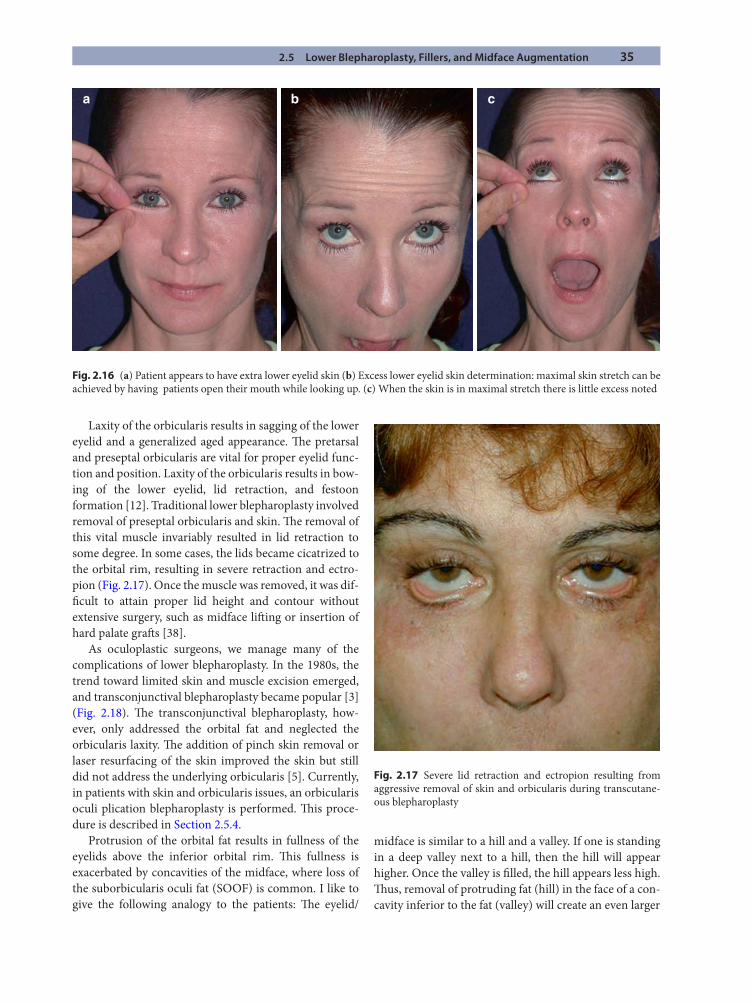
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation 35
a b c
Fig. 2.16 (a) Patient appears to have extra lower eyelid skin (b) Excess lower eyelid skin determination: maximal skin stretch can be achieved by having patients open their mouth while looking up. (c) When the skin is in maximal stretch there is little excess noted
Laxity of the orbicularis results in sagging of the lower eyelid and a generalized aged appearance. Th e pretarsal and preseptal orbicularis are vital for proper eyelid func-tion and position. Laxity of the orbicularis results in bow-ing of the lower eyelid, lid retraction, and festoon formation [12]. Traditional lower blepharoplasty involved removal of preseptal orbicularis and skin. Th e removal of this vital muscle invariably resulted in lid retraction to some degree. In some cases, the lids became cicatrized to the orbital rim, resulting in severe retraction and ectro-pion (Fig. 2.17). Once the muscle was removed, it was dif-fi cult to attain proper lid height and contour without extensive surgery, such as midface lift ing or insertion of hard palate graft s [38].
As oculoplastic surgeons, we manage many of the complications of lower blepharoplasty. In the 1980s, the trend toward limited skin and muscle excision emerged, and transconjunctival blepharoplasty became popular [3] (Fig. 2.18). Th e transconjunctival blepharoplasty, how-ever, only addressed the orbital fat and neglected the orbicularis laxity. Th e addition of pinch skin removal or laser resurfacing of the skin improved the skin but still did not address the underlying orbicularis [5]. Currently, in patients with skin and orbicularis issues, an orbicularis oculi plication blepharoplasty is performed. Th is proce-dure is described in Section 2.5.4.
Protrusion of the orbital fat results in fullness of the eyelids above the inferior orbital rim. Th is fullness is exacerbated by concavities of the midface, where loss of the suborbicularis oculi fat (SOOF) is common. I like to give the following analogy to the patients: Th e eyelid/
midface is similar to a hill and a valley. If one is standing in a deep valley next to a hill, then the hill will appear higher. Once the valley is fi lled, the hill appears less high. Th us, removal of protruding fat (hill) in the face of a con-cavity inferior to the fat (valley) will create an even larger
Fig. 2.17 Severe lid retraction and ectropion resulting from aggressive removal of skin and orbicularis during transcutane-ous blepharoplasty

36 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
concavity (greater valley). It is imperative that the bleph-aroplasty surgeon evaluate the contours of the lower eye-lid and decide if fat removal, fat addition, or fat repositioning is indicated (Fig. 2.19).
Th e inferior orbital rim and bony midface are evalu-ated. Th e contours of these bones signifi cantly contribute to eyelid position [13]. Th e relationship between the ante-rior corneal surface and the inferior orbital rim is evalu-ated in the sagittal plane. Patients are grouped into three categories: negative vector (the globe projects anterior to the rim), neutral vector (the globe is in line with the infe-rior rim), and positive vector (the globe projects poste-rior to the rim) [11] (Fig. 2.20).
Patients with a negative vector confi guration have less midfacial support and are more at risk for lid malposi-tions and contour irregularities aft er transconjunctival fat removal or transcutaneous blepharoplasty. Patients with prominent eyes and severe negative vector confi guration may benefi t from midface implants and a midface lift (Fig. 2.21).
Th e question of fat removal versus fat preservation and repositioning is daunting [17]. I have abided by the
following general principals and have managed to get consistent results: In patients with a prominent eye, nega-tive vector, and orbital fat protrusion, a fat-repositioning procedure is performed [42]. In patients with a deeper-set eye, positive vector, and orbital fat protrusion, fat removal is acceptable (Table 2.2).
Th e lower eyelids are probably the most diffi cult region of the face to rejuvenate. Attaining excellent and consistent results in lower eyelid surgery is dependent on proper evaluation of the anatomic problems and proper solutions to address these problems. Since there are so many anatomic variations among patients, there are multiple procedures that are available for lower eye-lid rejuvenation. Oft en, a patient may require multiple procedures within the context of “blepharoplasty” to address each anatomic abnormality. For example, lower lid fat repositioning may be combined with orbicularis suspension and skin excision. Transconjunctival bleph-aroplasty may be combined with hyaluronic fi llers and a chemical peel [22].
Th e pearls of lower blepharoplasty are separated into anesthesia and procedure sections.
Fig. 2.19 Th is patient has mild fat protrusion and signifi cant infraorbital hollowness. Th e concavity extends from the medial to lateralmost portion of the eyelid. Removal of protruding orbital fat in this patient will make the hollowness worse
Fig. 2.18 (a and b) Transconjunctival blepharoplasty combined with laser resurfacing: Pre and Postoperative photos
a
b
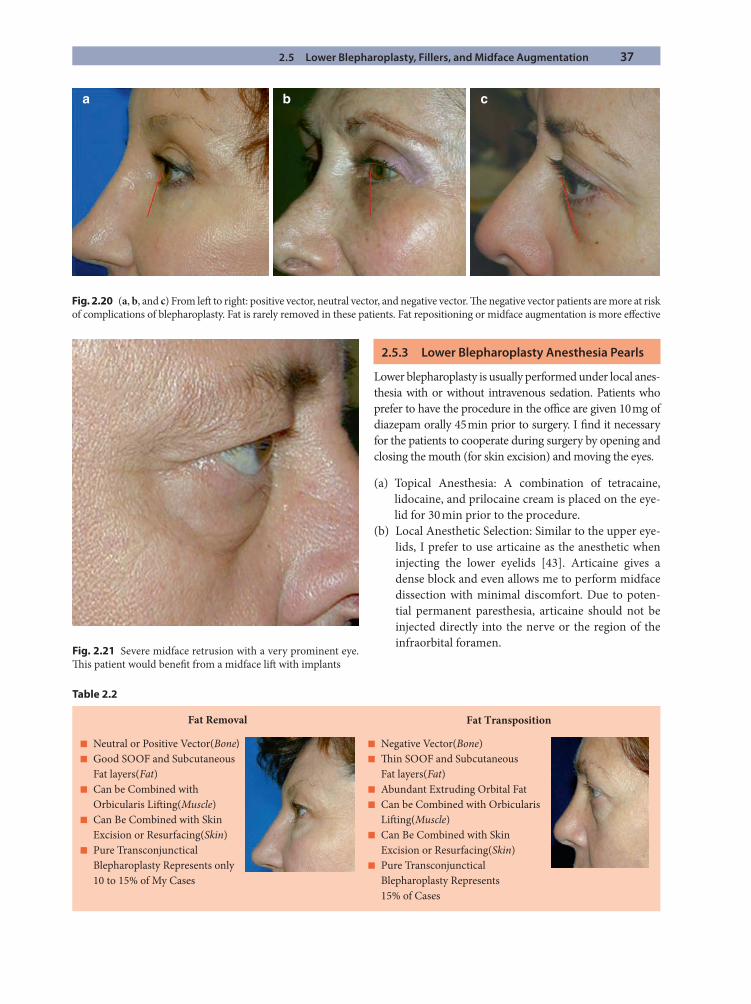
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation 37
a b c
Fig. 2.20 (a, b, and c) From left to right: positive vector, neutral vector, and negative vector. Th e negative vector patients are more at risk of complications of blepharoplasty. Fat is rarely removed in these patients. Fat repositioning or midface augmentation is more eff ective
Table 2.2
Fat Removal Fat Transposition
■ Neutral or Positive Vector(Bone)■ Good SOOF and Subcutaneous Fat layers(Fat)■ Can be Combined with Orbicularis Lifting(Muscle)■ Can Be Combined with Skin Excision or Resurfacing(Skin)■ Pure Transconjunctical Blepharoplasty Represents only 10 to 15% of My Cases
■ Negative Vector(Bone)■ Thin SOOF and Subcutaneous Fat layers(Fat)■ Abundant Extruding Orbital Fat■ Can be Combined with Orbicularis Lifting(Muscle)■ Can Be Combined with Skin Excision or Resurfacing(Skin)■ Pure Transconjunctical Blepharoplasty Represents 15% of Cases
Fig. 2.21 Severe midface retrusion with a very prominent eye. Th is patient would benefi t from a midface lift with implants
2.5.3 Lower Blepharoplasty Anesthesia Pearls
Lower blepharoplasty is usually performed under local anes-thesia with or without intravenous sedation. Patients who prefer to have the procedure in the offi ce are given 10 mg of diazepam orally 45 min prior to surgery. I fi nd it necessary for the patients to cooperate during surgery by opening and closing the mouth (for skin excision) and moving the eyes.
(a) Topical Anesthesia: A combination of tetracaine, lidocaine, and prilocaine cream is placed on the eye-lid for 30 min prior to the procedure.
(b) Local Anesthetic Selection: Similar to the upper eye-lids, I prefer to use articaine as the anesthetic when injecting the lower eyelids [43]. Articaine gives a dense block and even allows me to perform midface dissection with minimal discomfort. Due to poten-tial permanent paresthesia, articaine should not be injected directly into the nerve or the region of the infraorbital foramen.

38 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
2.5.4 Lower Blepharoplasty Surgical Procedure Pearls
(a) Infralash Muscle Plication Blepharoplasty: Th is pro-cedure is a modifi cation of that described by Fagien [9]. Patients with true excess skin and laxity of the orbicularis are candidates for this procedure. Th e procedure is also useful in the management of festoons.
Step 1: Th e lower eyelid skin and muscle are rein-jected with dilute lidocaine with epinephrine to bal-loon up the skin.
Step 2: Two traction sutures are placed through the gray line of the lower eyelid. Th e sutures are clamped to the towels on the forehead, thereby putting the lower eyelid on stretch.
Step 3: A number 15 blade is used to make an incision from medial to lateral. Laterally, the incision extends about a centimeter and is angled slightly inferiorly. It can be hidden in a rhytid in this region.
Step 4: Th e assistant places two fi ngers on the skin of the lower eyelid/cheek junction, thereby putting the eyelid on maximal stretch.
Step 5: Scissors are used to dissect the skin off the underlying muscle. Th e dissection proceeds until the inferior orbital rim is reached. It is important to stay superfi cial and not to damage the underlying muscle. Pinpoint bleeding is cauterized at this point. If fat reposition or fat excision is necessary, it is performed at this point of the procedure. A small horizontal incision is made through the orbicularis, and the sep-tum is buttonholed. Midface dissection can easily be performed through this small hole. Fat excision is also quite easy to perform through this hole. Aft er the fat manipulation is completed, the orbicularis is closed with several 6–0 buried Vicryl sutures. Th e traction sutures are now released.
Step 6: Th e degree of lower eyelid laxity is assessed. In 70% of cases, a lateral canthal plication suture is placed to tighten the lower eyelid margin. If severe laxity exists, a tarsal strip is performed. It is impera-tive that the lower eyelid hug the globe. Th e suture is replaced until the proper tension and proper position of the eyelid are achieved.
Step 7: Th e orbicularis is grasped at a point inferome-dial to the canthus. Th e muscle is then pulled supero-lateral and folded on itself. If this elevates the orbicularis in the desired manner, a buried, 5–0 PDS
suture is then placed from this portion of the orbicu-laris to the periosteum just lateral to the canthus. Multiple sutures are placed progressively laterally, thereby securing the orbicularis to the periosteum. Th e imbrication of the orbicularis adds fullness to the lateral lower eyelid, where a crescent typically forms during the aging process.
Step 8: Th e skin is pulled superiorly and laterally, and the patient is asked to open his or her mouth and look superiorly. A pilot cut is then made through the skin at the lateral canthal region. Skin is conserva-tively excised lateral to medial. Very little skin is excised medially. Th e skin is then closed in the sub-ciliary region. Th e skin lateral to the canthus is simi-larly excised. If a dog-ear is noted, an M-plasty can be performed (Fig. 2.22).
(b) Transconjunctival Fat Repositioning: Th e transcon-junctival approach for fat repositioning is utilized in patients with minimal or no skin/muscle issues. Th e techniques of fat repositioning have been described in the past [16, 17, 28]. Th e following are some tips that will make the procedure easier (Fig. 2.23):
Step 1: A transconjunctival incision is made with a fi ne-tipped cautery. Th e incision extends through the lower eyelid retractors.
Step 2: Cotton-tipped applicators are used to dissect to the inferior orbital rim. Th e arcus marginalis becomes visible. If the lateral fat pocket is prolapsing but is not large enough to reposition, it is excised at this point in the surgery.
Step 3: Th e cutting cautery is then used to cut through the arcus marginalis.
Step 4: A Senn retractor is helpful for the midface dis-section. Th e dissection plane is a combination of pre-periosteal and subperiosteal. Subperiosteal dissection proceeds for about 1.5 cm medial and lateral to the location of the infraorbital nerve. It is not necessary to disinsert the origin of the levator labii superioris muscle that overlies the infraorbital nerve. Blunt dis-section with cotton-tipped applicators is performed on the anterior surface of the muscle.
Step 5: Th e fat pockets are dissected free from their attachments to create a rectangular pedicle. Two 4–0 gut sutures are tied together. Th e suture is passed through the leading edge of the fat and locked at the medial and lateral poles (similar to what is performed in strabismus surgery).
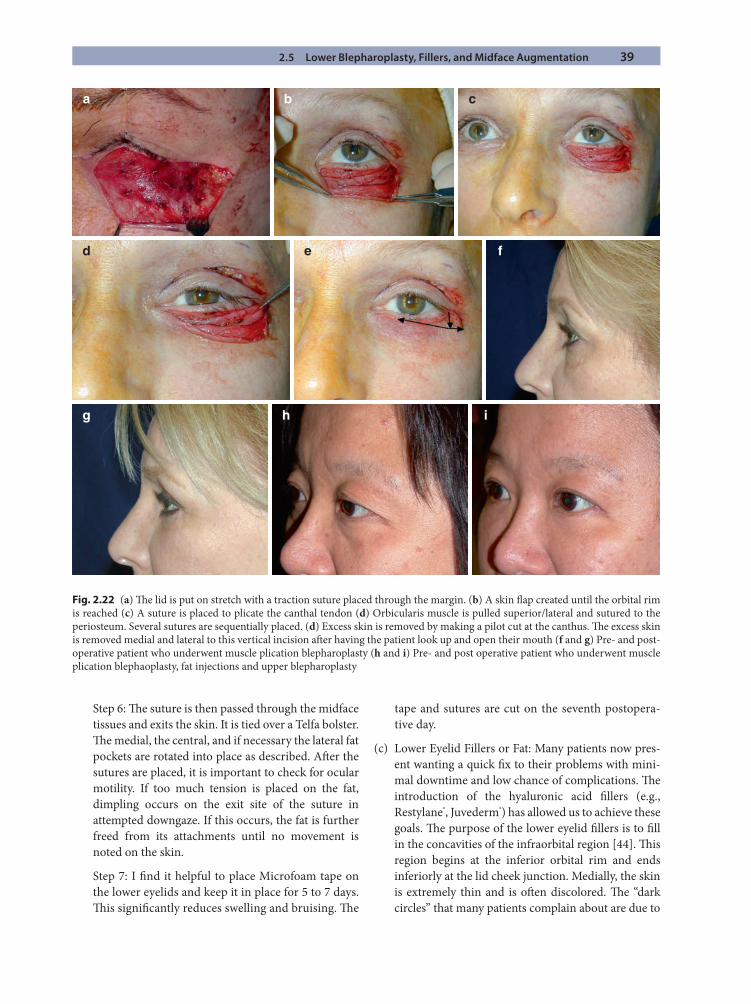
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation 39
a b c
d e f
ihg
Fig. 2.22 (a) Th e lid is put on stretch with a traction suture placed through the margin. (b) A skin fl ap created until the orbital rim is reached (c) A suture is placed to plicate the canthal tendon (d) Orbicularis muscle is pulled superior/lateral and sutured to the periosteum. Several sutures are sequentially placed. (d) Excess skin is removed by making a pilot cut at the canthus. Th e excess skin is removed medial and lateral to this vertical incision aft er having the patient look up and open their mouth (f and g) Pre- and post-operative patient who underwent muscle plication blepharoplasty (h and i) Pre- and post operative patient who underwent muscle plication blephaoplasty, fat injections and upper blepharoplasty
Step 6: Th e suture is then passed through the midface tissues and exits the skin. It is tied over a Telfa bolster. Th e medial, the central, and if necessary the lateral fat pockets are rotated into place as described. Aft er the sutures are placed, it is important to check for ocular motility. If too much tension is placed on the fat, dimpling occurs on the exit site of the suture in attempted downgaze. If this occurs, the fat is further freed from its attachments until no movement is noted on the skin.
Step 7: I fi nd it helpful to place Microfoam tape on the lower eyelids and keep it in place for 5 to 7 days. Th is signifi cantly reduces swelling and bruising. Th e
tape and sutures are cut on the seventh postopera-tive day.
(c) Lower Eyelid Fillers or Fat: Many patients now pres-ent wanting a quick fi x to their problems with mini-mal downtime and low chance of complications. Th e introduction of the hyaluronic acid fi llers (e.g., Restylane®, Juvederm®) has allowed us to achieve these goals. Th e purpose of the lower eyelid fi llers is to fi ll in the concavities of the infraorbital region [44]. Th is region begins at the inferior orbital rim and ends inferiorly at the lid cheek junction. Medially, the skin is extremely thin and is oft en discolored. Th e “dark circles” that many patients complain about are due to
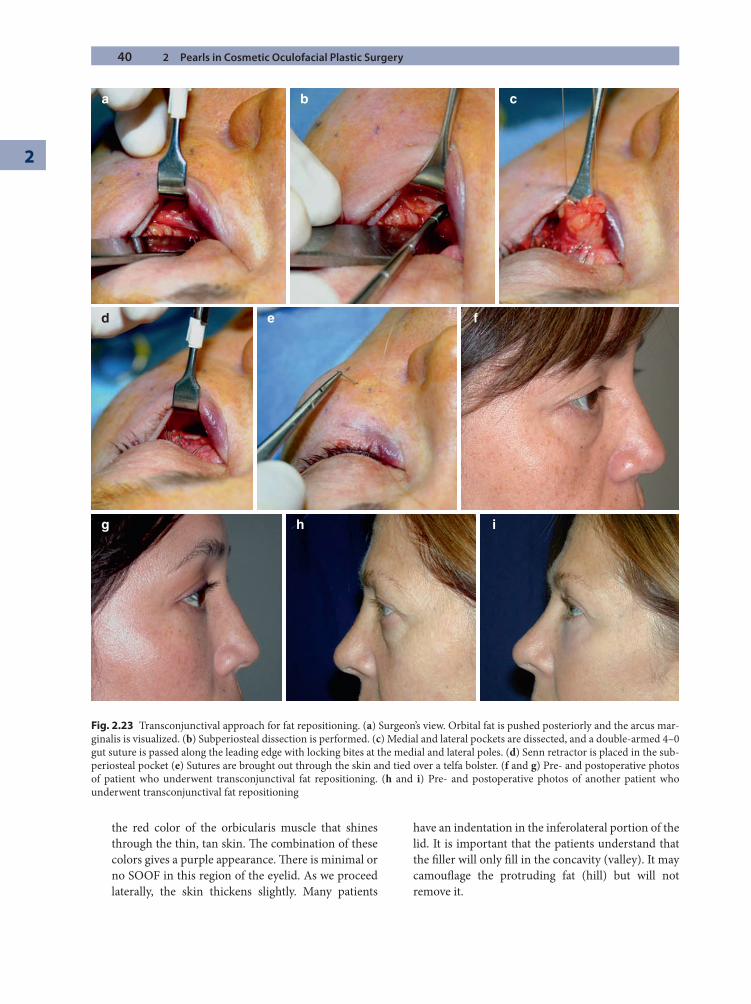
40 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
a b c
d e
g h i
f
Fig. 2.23 Transconjunctival approach for fat repositioning. (a) Surgeon’s view. Orbital fat is pushed posteriorly and the arcus mar-ginalis is visualized. (b) Subperiosteal dissection is performed. (c) Medial and lateral pockets are dissected, and a double-armed 4–0 gut suture is passed along the leading edge with locking bites at the medial and lateral poles. (d) Senn retractor is placed in the sub-periosteal pocket (e) Sutures are brought out through the skin and tied over a telfa bolster. (f and g) Pre- and postoperative photos of patient who underwent transconjunctival fat repositioning. (h and i) Pre- and postoperative photos of another patient who underwent transconjunctival fat repositioning
the red color of the orbicularis muscle that shines through the thin, tan skin. Th e combination of these colors gives a purple appearance. Th ere is minimal or no SOOF in this region of the eyelid. As we proceed laterally, the skin thickens slightly. Many patients
have an indentation in the inferolateral portion of the lid. It is important that the patients understand that the fi ller will only fi ll in the concavity (valley). It may camoufl age the protruding fat (hill) but will not remove it.
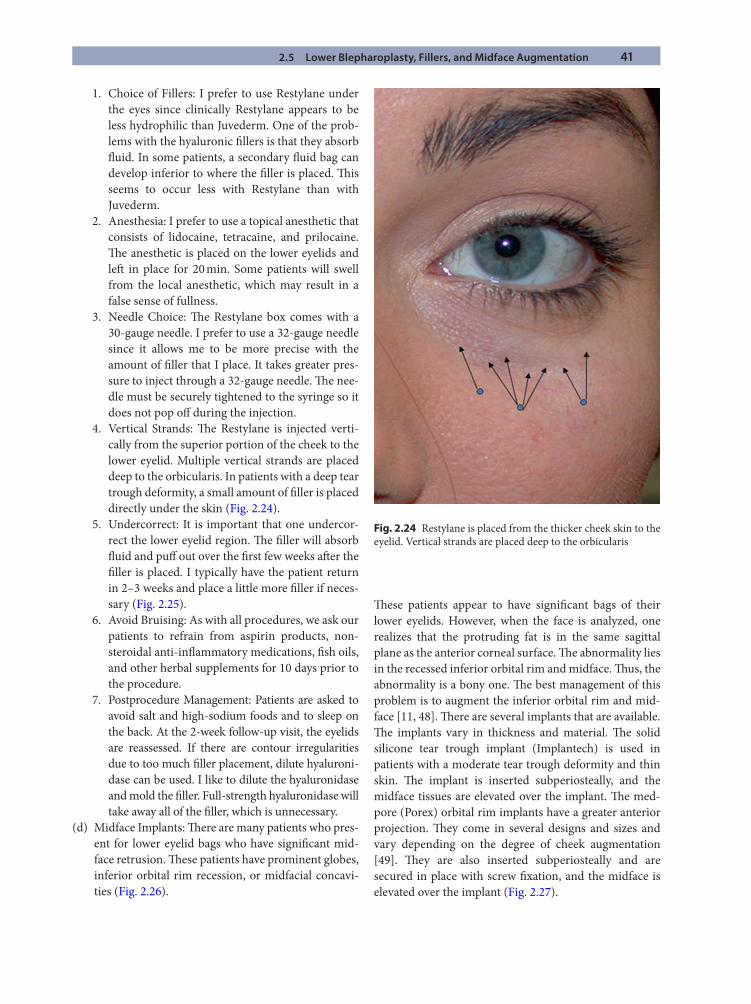
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation 41
1. Choice of Fillers: I prefer to use Restylane under the eyes since clinically Restylane appears to be less hydrophilic than Juvederm. One of the prob-lems with the hyaluronic fi llers is that they absorb fl uid. In some patients, a secondary fl uid bag can develop inferior to where the fi ller is placed. Th is seems to occur less with Restylane than with Juvederm.
2. Anesthesia: I prefer to use a topical anesthetic that consists of lidocaine, tetracaine, and prilocaine. Th e anesthetic is placed on the lower eyelids and left in place for 20 min. Some patients will swell from the local anesthetic, which may result in a false sense of fullness.
3. Needle Choice: Th e Restylane box comes with a 30-gauge needle. I prefer to use a 32-gauge needle since it allows me to be more precise with the amount of fi ller that I place. It takes greater pres-sure to inject through a 32-gauge needle. Th e nee-dle must be securely tightened to the syringe so it does not pop off during the injection.
4. Vertical Strands: Th e Restylane is injected verti-cally from the superior portion of the cheek to the lower eyelid. Multiple vertical strands are placed deep to the orbicularis. In patients with a deep tear trough deformity, a small amount of fi ller is placed directly under the skin (Fig. 2.24).
5. Undercorrect: It is important that one undercor-rect the lower eyelid region. Th e fi ller will absorb fl uid and puff out over the fi rst few weeks aft er the fi ller is placed. I typically have the patient return in 2–3 weeks and place a little more fi ller if neces-sary (Fig. 2.25).
6. Avoid Bruising: As with all procedures, we ask our patients to refrain from aspirin products, non-steroidal anti-infl ammatory medications, fi sh oils, and other herbal supplements for 10 days prior to the procedure.
7. Postprocedure Management: Patients are asked to avoid salt and high-sodium foods and to sleep on the back. At the 2-week follow-up visit, the eyelids are reassessed. If there are contour irregularities due to too much fi ller placement, dilute hyaluroni-dase can be used. I like to dilute the hyaluronidase and mold the fi ller. Full-strength hyaluronidase will take away all of the fi ller, which is unnecessary.
(d) Midface Implants: Th ere are many patients who pres-ent for lower eyelid bags who have signifi cant mid-face retrusion. Th ese patients have prominent globes, inferior orbital rim recession, or midfacial concavi-ties (Fig. 2.26).
Th ese patients appear to have signifi cant bags of their lower eyelids. However, when the face is analyzed, one realizes that the protruding fat is in the same sagittal plane as the anterior corneal surface. Th e abnormality lies in the recessed inferior orbital rim and midface. Th us, the abnormality is a bony one. Th e best management of this problem is to augment the inferior orbital rim and mid-face [11, 48]. Th ere are several implants that are available. Th e implants vary in thickness and material. Th e solid silicone tear trough implant (Implantech) is used in patients with a moderate tear trough deformity and thin skin. Th e implant is inserted subperiosteally, and the midface tissues are elevated over the implant. Th e med-pore (Porex) orbital rim implants have a greater anterior projection. Th ey come in several designs and sizes and vary depending on the degree of cheek augmentation [49]. Th ey are also inserted subperiosteally and are secured in place with screw fi xation, and the midface is elevated over the implant (Fig. 2.27).
Fig. 2.24 Restylane is placed from the thicker cheek skin to the eyelid. Vertical strands are placed deep to the orbicularis
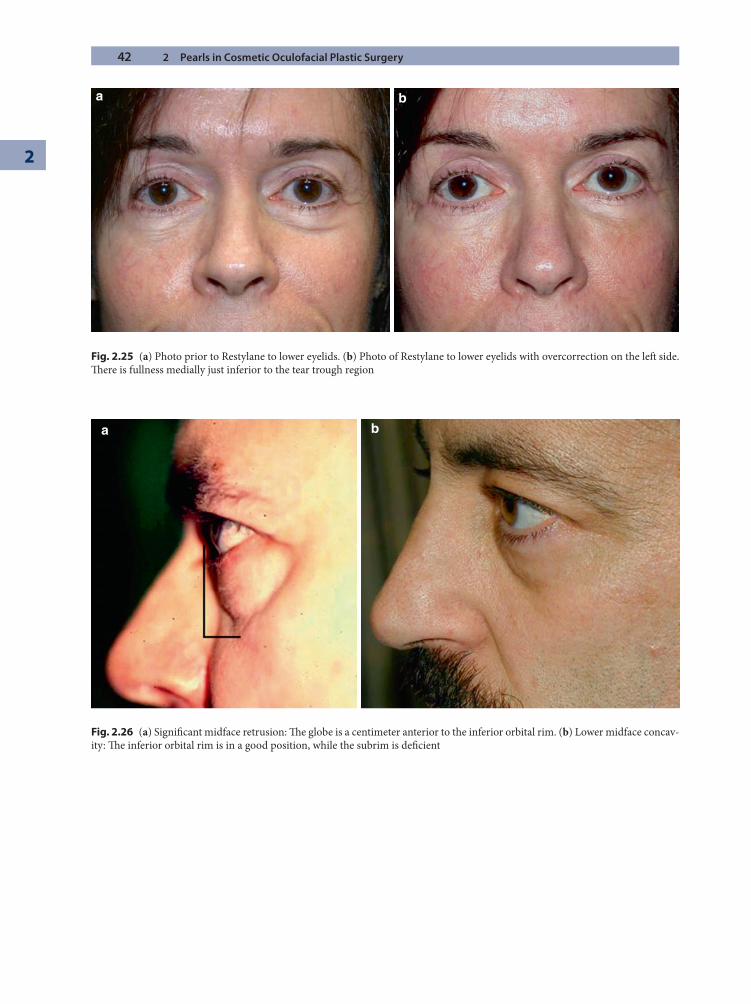
42 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
a b
Fig. 2.25 (a) Photo prior to Restylane to lower eyelids. (b) Photo of Restylane to lower eyelids with overcorrection on the left side. Th ere is fullness medially just inferior to the tear trough region
a b
Fig. 2.26 (a) Signifi cant midface retrusion: Th e globe is a centimeter anterior to the inferior orbital rim. (b) Lower midface concav-ity: Th e inferior orbital rim is in a good position, while the subrim is defi cient
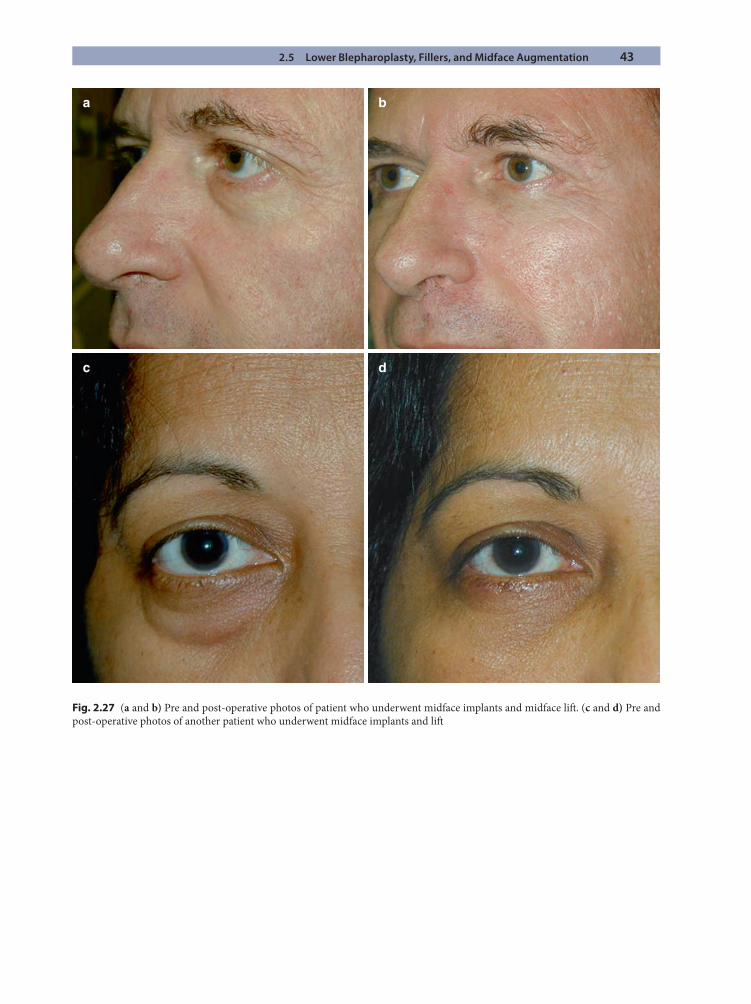
2.5 Lower Blepharoplasty, Fillers, and Midface Augmentation 43
Fig. 2.27 (a and b) Pre and post-operative photos of patient who underwent midface implants and midface lift . (c and d) Pre and post-operative photos of another patient who underwent midface implants and lift
a b
c d
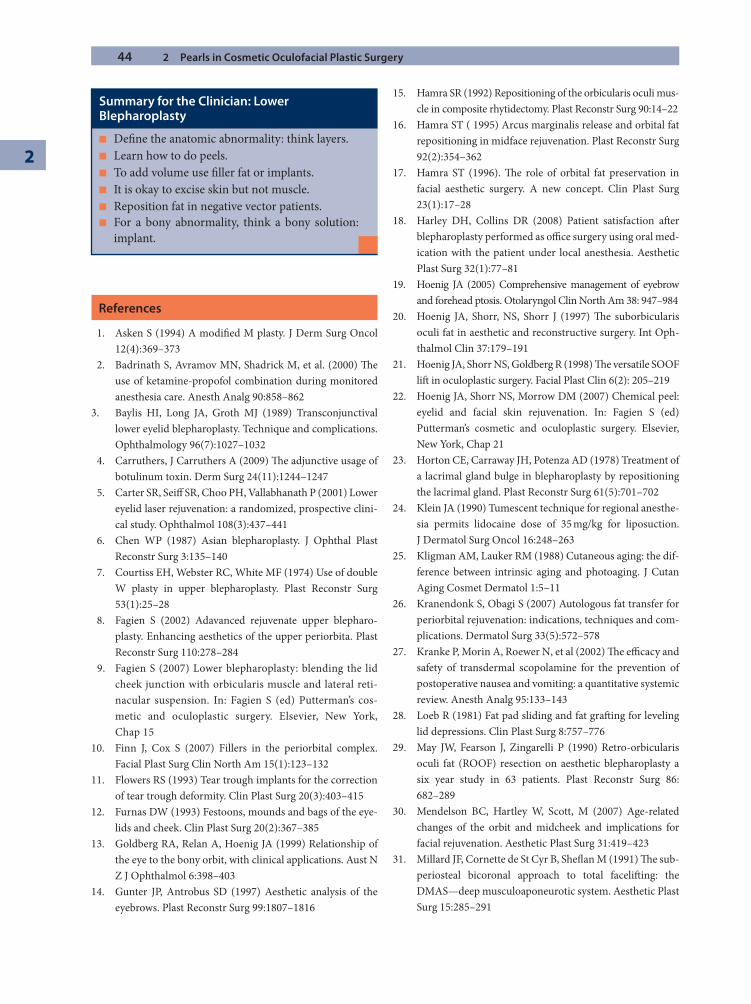
44 2 Pearls in Cosmetic Oculofacial Plastic Surgery
2
References
1. Asken S (1994) A modifi ed M plasty. J Derm Surg Oncol 12(4):369–373
2. Badrinath S, Avramov MN, Shadrick M, et al. (2000) Th e use of ketamine-propofol combination during monitored anesthesia care. Anesth Analg 90:858–862
3. Baylis HI, Long JA, Groth MJ (1989) Transconjunctival lower eyelid blepharoplasty. Technique and complications. Ophthalmology 96(7):1027–1032
4. Carruthers, J Carruthers A (2009) Th e adjunctive usage of botulinum toxin. Derm Surg 24(11):1244–1247
5. Carter SR, Seiff SR, Choo PH, Vallabhanath P (2001) Lower eyelid laser rejuvenation: a randomized, prospective clini-cal study. Ophthalmol 108(3):437–441
6. Chen WP (1987) Asian blepharoplasty. J Ophthal Plast Reconstr Surg 3:135–140
7. Courtiss EH, Webster RC, White MF (1974) Use of double W plasty in upper blepharoplasty. Plast Reconstr Surg 53(1):25–28
8. Fagien S (2002) Adavanced rejuvenate upper blepharo-plasty. Enhancing aesthetics of the upper periorbita. Plast Reconstr Surg 110:278–284
9. Fagien S (2007) Lower blepharoplasty: blending the lid cheek junction with orbicularis muscle and lateral reti-nacular suspension. In: Fagien S (ed) Putterman’s cos-metic and oculoplastic surgery. Elsevier, New York, Chap 15
10. Finn J, Cox S (2007) Fillers in the periorbital complex. Facial Plast Surg Clin North Am 15(1):123–132
11. Flowers RS (1993) Tear trough implants for the correction of tear trough deformity. Clin Plast Surg 20(3):403–415
12. Furnas DW (1993) Festoons, mounds and bags of the eye-lids and cheek. Clin Plast Surg 20(2):367–385
13. Goldberg RA, Relan A, Hoenig JA (1999) Relationship of the eye to the bony orbit, with clinical applications. Aust N Z J Ophthalmol 6:398–403
14. Gunter JP, Antrobus SD (1997) Aesthetic analysis of the eyebrows. Plast Reconstr Surg 99:1807–1816
15. Hamra SR (1992) Repositioning of the orbicularis oculi mus-cle in composite rhytidectomy. Plast Reconstr Surg 90:14–22
16. Hamra ST ( 1995) Arcus marginalis release and orbital fat repositioning in midface rejuvenation. Plast Reconstr Surg 92(2):354–362
17. Hamra ST (1996). Th e role of orbital fat preservation in facial aesthetic surgery. A new concept. Clin Plast Surg 23(1):17–28
18. Harley DH, Collins DR (2008) Patient satisfaction aft er blepharoplasty performed as offi ce surgery using oral med-ication with the patient under local anesthesia. Aesthetic Plast Surg 32(1):77–81
19. Hoenig JA (2005) Comprehensive management of eyebrow and forehead ptosis. Otolaryngol Clin North Am 38: 947–984
20. Hoenig JA, Shorr, NS, Shorr J (1997) Th e suborbicularis oculi fat in aesthetic and reconstructive surgery. Int Oph-thalmol Clin 37:179–191
21. Hoenig JA, Shorr NS, Goldberg R (1998) Th e versatile SOOF lift in oculoplastic surgery. Facial Plast Clin 6(2): 205–219
22. Hoenig JA, Shorr NS, Morrow DM (2007) Chemical peel: eyelid and facial skin rejuvenation. In: Fagien S (ed) Putterman’s cosmetic and oculoplastic surgery. Elsevier, New York, Chap 21
23. Horton CE, Carraway JH, Potenza AD (1978) Treatment of a lacrimal gland bulge in blepharoplasty by repositioning the lacrimal gland. Plast Reconstr Surg 61(5):701–702
24. Klein JA (1990) Tumescent technique for regional anesthe-sia permits lidocaine dose of 35 mg/kg for liposuction. J Dermatol Surg Oncol 16:248–263
25. Kligman AM, Lauker RM (1988) Cutaneous aging: the dif-ference between intrinsic aging and photoaging. J Cutan Aging Cosmet Dermatol 1:5–11
26. Kranendonk S, Obagi S (2007) Autologous fat transfer for periorbital rejuvenation: indications, techniques and com-plications. Dermatol Surg 33(5):572–578
27. Kranke P, Morin A, Roewer N, et al (2002) Th e effi cacy and safety of transdermal scopolamine for the prevention of postoperative nausea and vomiting: a quantitative systemic review. Anesth Analg 95:133–143
28. Loeb R (1981) Fat pad sliding and fat graft ing for leveling lid depressions. Clin Plast Surg 8:757–776
29. May JW, Fearson J, Zingarelli P (1990) Retro-orbicularis oculi fat (ROOF) resection on aesthetic blepharoplasty a six year study in 63 patients. Plast Reconstr Surg 86: 682–289
30. Mendelson BC, Hartley W, Scott, M (2007) Age-related changes of the orbit and midcheek and implications for facial rejuvenation. Aesthetic Plast Surg 31:419–423
31. Millard JF, Cornette de St Cyr B, Shefl an M (1991) Th e sub-periosteal bicoronal approach to total facelift ing: the DMAS—deep musculoaponeurotic system. Aesthetic Plast Surg 15:285–291
Summary for the Clinician: Lower Blepharoplasty
Defi ne the anatomic abnormality: think layers. ■
Learn how to do peels. ■
To add volume use fi ller fat or implants. ■
It is okay to excise skin but not muscle. ■
Reposition fat in negative vector patients. ■
For a bony abnormality, think a bony solution: ■
implant.
References 45
32. Mitz V, Peyronie M (1976) Th e superfi cial muscu-loaponeurtic system (SMAS) in the parotid and cheek area. Plast Reconstr Surg 58:80–88
33. Moody BR, Hold JB (2006) Anesthesia for offi ce-based oculoplastic surgery. Dermatol Surg 31(7):766–770
34. Persichetti P, Di Lella F, Delfi no F (2004) Adipose compart-ments of the upper eyelid: anatomy applied to blepharo-plasty. Plast Reconstr Surg 113:373–378
35. Pessa JE (2000) An algorithm of facial aging: verifi cation of Lambros’s theory by three dimensional stereolithography, with reference to the pathogenesis of midfacial aging, sclera show, and the lateral suborbital tera trough defor-mity. Plast Reconstr Surg 106:479–488
36. Porter JD, Burns LA, May PJ (1989) Morphological sub-strate for eyelid movements: Innervation and structure of primate levator palpebrae superioris and orbicularis oculi muscles. J Comp Neurol 287:64–81
37. Putterman AM, Urist MJ (1975) Muller’s muscle-conjunc-tival resection: technique for treatment of blepharoptosis. Arch Ophthalmol 93:619–623
38. Shorr NS (1997) Madame butterfl y procedure: total lower eyelid reconstruction in three layers utilizing a hard palate graft : management of the unhappy post-blepharoplasty patient with round eye and sclera show. Int J Aesthetic Restor Surg 3: 3–26
39. Shorr NS, Cohen MS (1991) Cosmetic blepharoplasty. Ophthalmol Clin North Am 4(1):17–33
40. Shorr N, Enzer Y (1992) Considerations in aesthetic sur-gery. J Dermatol Surg Oncol 18:1081–1095
41. Shorr N, Hoenig JA (1995) Brow lift . In: Levine M (ed) Manual of oculoplastic surgery. Butterworth-Heinrmann, Newton, MA
42. Shorr N, Hoenig JA, Goldberg RA (1999) Fat preservation to rejuvenate the lower eyelid. Arch Facial Plast Surg 1(1): 38–39
43. Steele EA, Ng JD, Poissant TM, et al. (2009) Comparison of injection pain of articaine and lidocaine in eyelid surgery. Ophthal Plast Reconstr Surg 25(1):13–15
44. Steinsapir KD, Steinsapir SM (2006) Deep-fi ll hyaluronic acid for the temporary treatment of the naso-jugal groove: a report of 303 consecutive treatments. Ophthal Plast Reconstr Surg 22(5):344–348
45. Steinsapir K, Shorr N, Hoenig JA, et al. (1998) Endoscopic forehead lift . Ophthal Plast Reconstr Surg 14:107–118
46. Stuzin JM, Baker TJ, Gordon HL (1992) Th e relationship of the superfi cial and deep facial fascias: the relevance to rhytidectomy and aging. Plast Reconstr Surg 89: 441–449
47. Webster RC, Fanous N, Smith RC (1979) Blepharoplasty: when to combine it with eyebrow, temple or coronal lift . J Otolaryngol 8:339–343
48. Yaremchuk MJ (2001) Infraorbital rim augmentation. Plast Reconstr Surg 107(6):1585–1592
49. Yaremchuk MJ (2005) Making the concave midface con-vex. Aesthetic Plast Surg 29(3)141–148
50. Zarem HA, Resnick JL, Carr RM, Wooton DG (1997) Browpexy: lateral orbicularis muscle fi xation as an adjunct to upper blepharoplasty. Plast Reconstr Surg 10:1258–1261
Current Concepts in the Management of Idiopathic Orbital Infl ammationKatherine A. Lane and Jurij R. Bilyk
Chapter 3
3
3.1 Introduction
Idiopathic orbital infl ammatory syndrome is also known as orbital pseudotumor and is a constellation of clinical fi ndings consistent with nonspecifi c infl ammation of orbital tissues with no identifi able local or systemic cause. It is important to note that over the past century this has been a diagnosis in transition as improving diagnostic capabilities have steadily narrowed the once broad and expansive term “idiopathic.” For example, serologic tests and immunologic markers can now distinguish sarcoido-sis, Wegener granulomatosis (WG), xanthogranulomato-sis, and lymphoid hyperplasia, among others.
Th e classic presentation of IOIS includes the abrupt onset, oft en over the course of hours, of periorbital pain associated with edema, erythema, and chemosis. Other protean features include proptosis, diplopia, and visual changes. When supported by positive fi ndings on appro-priate imaging studies and in the absence of any attribut-able cause, this clinical presentation is considered by some to be diagnostic. Th ese signs and symptoms most likely represent the clinical manifestations of a variety of autoimmune and cell-mediated processes [18] for which the triggers have yet to be determined.
IOIS is a heterogeneous disease process that can involve virtually any orbital tissue individually or in combination. Although there have been many classifi cation schemes
proposed, one of the most commonly employed is based on the anatomic location of infl ammation: myositis, dacryoadenitis, peribulbar infl ammation (posterior scleri-tis, tenonitis), and infl ammation of the orbital fat, the orbital apex, or the cavernous sinus (presumed Tolosa–Hunt syndrome, THS) [11, 57, 60] (Figs. 3.1 and 3.2).
3.2 What Is the Diagnosis?
One of the enduring controversies concerning IOIS lays in the question of what, precisely, is the diagnosis? Is “infl ammation” a valid diagnosis, or is it merely a tis-sue response due to some other process [49] not yet
Core Messages
Idiopathic orbital infl ammatory syndrome (IOIS) ■
is a nonspecifi c infl ammation of orbital tissue with no identifi able local or systemic cause.Infl ammation is oft en categorized based on its ■
anatomic location.Because there is no imaging study or laboratory ■
test that can rule in or rule out IOIS, the syn-drome remains one of exclusion.Classically, the signs and symptoms of IOIS are ■
extremely responsive to corticosteroid therapy.
Typical treatment doses are 1 mg/kg/day. Patients whose disease is “steroid resistant” are considered atypical.An orbital biopsy should be attempted in patients ■
who present in an atypical fashion, in patients who do not respond to corticosteroid treatment, and in patients with recurrent episodes of infl ammation.Patients with steroid-resistant IOIS may be ■
responsive to low-dose orbital radiation or immu-nomodulating agents.
Summary for the Clinician
IOIS is a diagnosis of exclusion. ■
Th e classic presentation of IOIS includes the ■
abrupt onset, oft en over the course of hours, of periorbital pain associated with edema, ery-thema, and chemosis and sometimes diplopia, proptosis, and vision loss.IOIS is commonly subclassifi ed by anatomic ■
location.
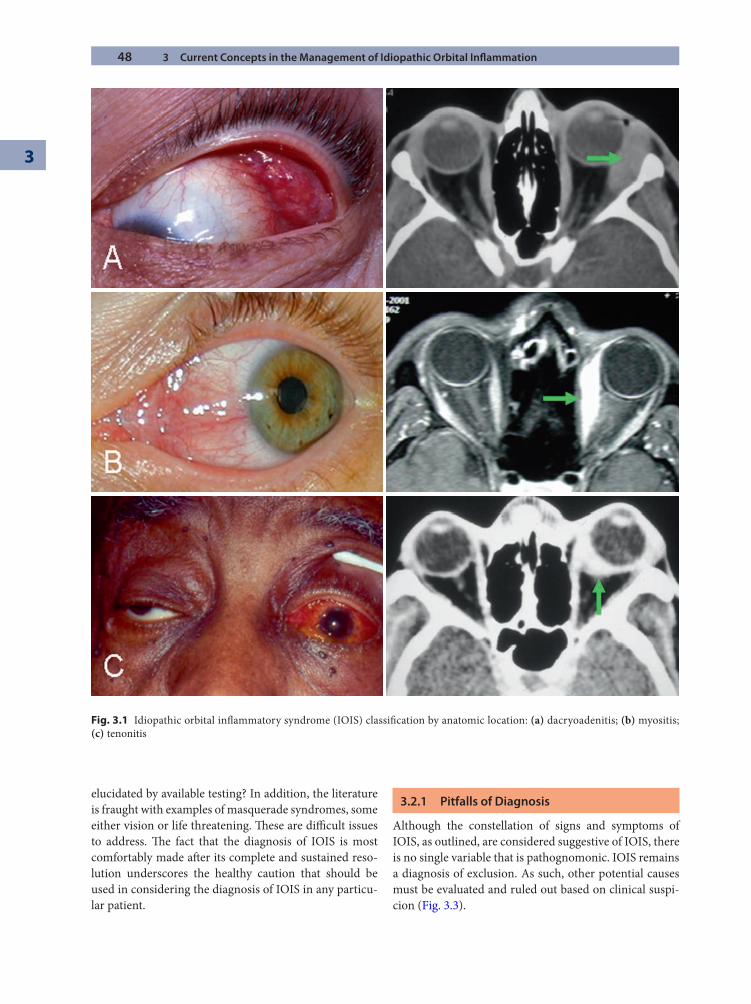
48 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
elucidated by available testing? In addition, the literature is fraught with examples of masquerade syndromes, some either vision or life threatening. Th ese are diffi cult issues to address. Th e fact that the diagnosis of IOIS is most comfortably made aft er its complete and sustained reso-lution underscores the healthy caution that should be used in considering the diagnosis of IOIS in any particu-lar patient.
3.2.1 Pitfalls of Diagnosis
Although the constellation of signs and symptoms of IOIS, as outlined, are considered suggestive of IOIS, there is no single variable that is pathognomonic. IOIS remains a diagnosis of exclusion. As such, other potential causes must be evaluated and ruled out based on clinical suspi-cion (Fig. 3.3).
Fig. 3.1 Idiopathic orbital infl ammatory syndrome (IOIS) classifi cation by anatomic location: (a) dacryoadenitis; (b) myositis; (c) tenonitis
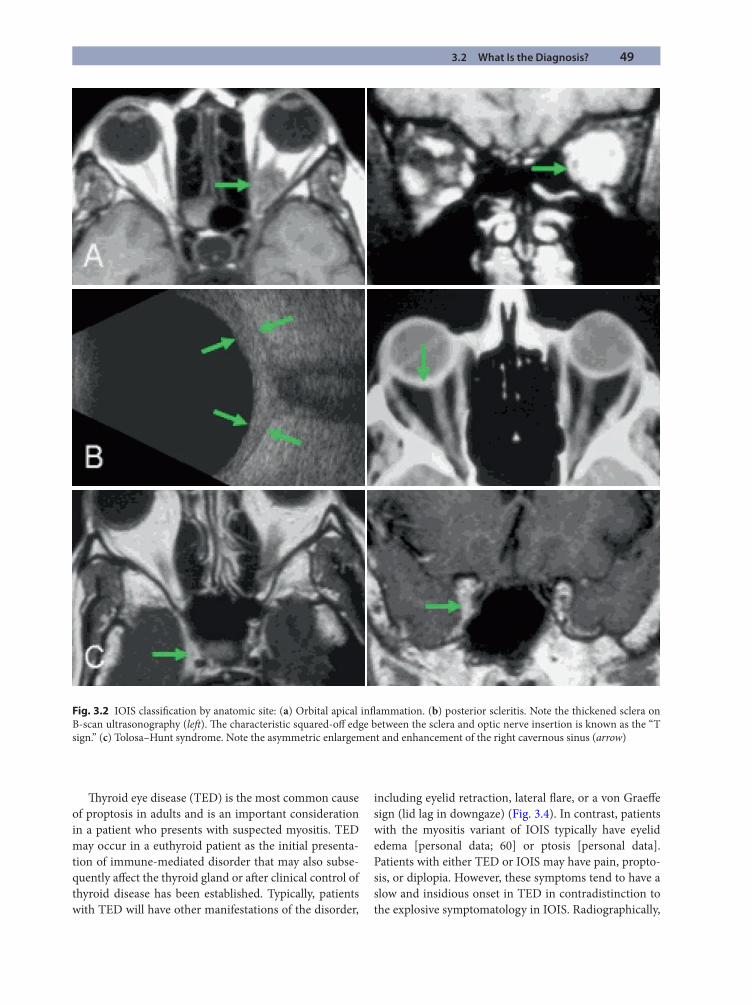
3.2 What Is the Diagnosis? 49
Th yroid eye disease (TED) is the most common cause of proptosis in adults and is an important consideration in a patient who presents with suspected myositis. TED may occur in a euthyroid patient as the initial presenta-tion of immune-mediated disorder that may also subse-quently aff ect the thyroid gland or aft er clinical control of thyroid disease has been established. Typically, patients with TED will have other manifestations of the disorder,
including eyelid retraction, lateral fl are, or a von Graeff e sign (lid lag in downgaze) (Fig. 3.4). In contrast, patients with the myositis variant of IOIS typically have eyelid edema [personal data; 60] or ptosis [personal data]. Patients with either TED or IOIS may have pain, propto-sis, or diplopia. However, these symptoms tend to have a slow and insidious onset in TED in contradistinction to the explosive symptomatology in IOIS. Radiographically,
Fig. 3.2 IOIS classifi cation by anatomic site: (a) Orbital apical infl ammation. (b) posterior scleritis. Note the thickened sclera on B-scan ultrasonography (left ). Th e characteristic squared-off edge between the sclera and optic nerve insertion is known as the “T sign.” (c) Tolosa–Hunt syndrome. Note the asymmetric enlargement and enhancement of the right cavernous sinus (arrow)
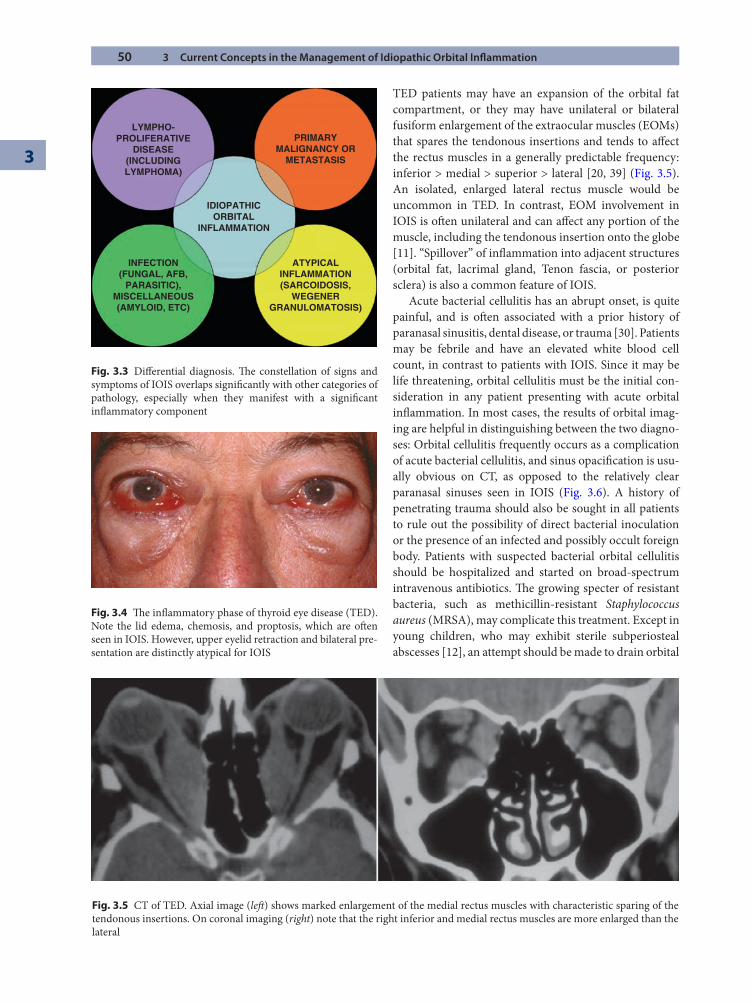
50 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
TED patients may have an expansion of the orbital fat compartment, or they may have unilateral or bilateral fusiform enlargement of the extraocular muscles (EOMs) that spares the tendonous insertions and tends to aff ect the rectus muscles in a generally predictable frequency: inferior > medial > superior > lateral [20, 39] (Fig. 3.5). An isolated, enlarged lateral rectus muscle would be uncommon in TED. In contrast, EOM involvement in IOIS is oft en unilateral and can aff ect any portion of the muscle, including the tendonous insertion onto the globe [11]. “Spillover” of infl ammation into adjacent structures (orbital fat, lacrimal gland, Tenon fascia, or posterior sclera) is also a common feature of IOIS.
Acute bacterial cellulitis has an abrupt onset, is quite painful, and is oft en associated with a prior history of paranasal sinusitis, dental disease, or trauma [30]. Patients may be febrile and have an elevated white blood cell count, in contrast to patients with IOIS. Since it may be life threatening, orbital cellulitis must be the initial con-sideration in any patient presenting with acute orbital infl ammation. In most cases, the results of orbital imag-ing are helpful in distinguishing between the two diagno-ses: Orbital cellulitis frequently occurs as a complication of acute bacterial cellulitis, and sinus opacifi cation is usu-ally obvious on CT, as opposed to the relatively clear paranasal sinuses seen in IOIS (Fig. 3.6). A history of penetrating trauma should also be sought in all patients to rule out the possibility of direct bacterial inoculation or the presence of an infected and possibly occult foreign body. Patients with suspected bacterial orbital cellulitis should be hospitalized and started on broad-spectrum intravenous antibiotics. Th e growing specter of resistant bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA), may complicate this treatment. Except in young children, who may exhibit sterile subperiosteal abscesses [12], an attempt should be made to drain orbital
LYMPHO-PROLIFERATIVE
DISEASE(INCLUDINGLYMPHOMA)
PRIMARYMALIGNANCY OR
METASTASIS
IDIOPATHICORBITAL
INFLAMMATION
INFECTION(FUNGAL, AFB,
PARASITIC),MISCELLANEOUS(AMYLOID, ETC)
ATYPICALINFLAMMATION(SARCOIDOSIS,
WEGENERGRANULOMATOSIS)
Fig. 3.3 Diff erential diagnosis. Th e constellation of signs and symptoms of IOIS overlaps signifi cantly with other categories of pathology, especially when they manifest with a signifi cant infl ammatory component
Fig. 3.4 Th e infl ammatory phase of thyroid eye disease (TED). Note the lid edema, chemosis, and proptosis, which are oft en seen in IOIS. However, upper eyelid retraction and bilateral pre-sentation are distinctly atypical for IOIS
Fig. 3.5 CT of TED. Axial image (left ) shows marked enlargement of the medial rectus muscles with characteristic sparing of the tendonous insertions. On coronal imaging (right) note that the right inferior and medial rectus muscles are more enlarged than the lateral
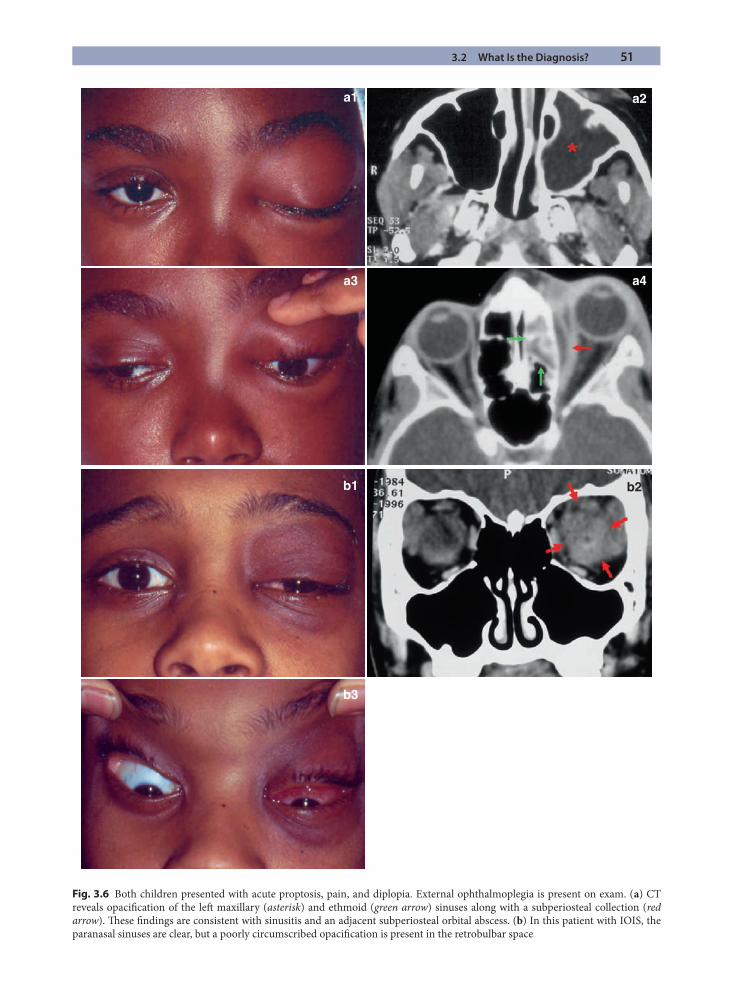
3.2 What Is the Diagnosis? 51
Fig. 3.6 Both children presented with acute proptosis, pain, and diplopia. External ophthalmoplegia is present on exam. (a) CT reveals opacifi cation of the left maxillary (asterisk) and ethmoid (green arrow) sinuses along with a subperiosteal collection (red arrow). Th ese fi ndings are consistent with sinusitis and an adjacent subperiosteal orbital abscess. (b) In this patient with IOIS, the paranasal sinuses are clear, but a poorly circumscribed opacifi cation is present in the retrobulbar space
a1 a2
a4
b3
b2b1
a3
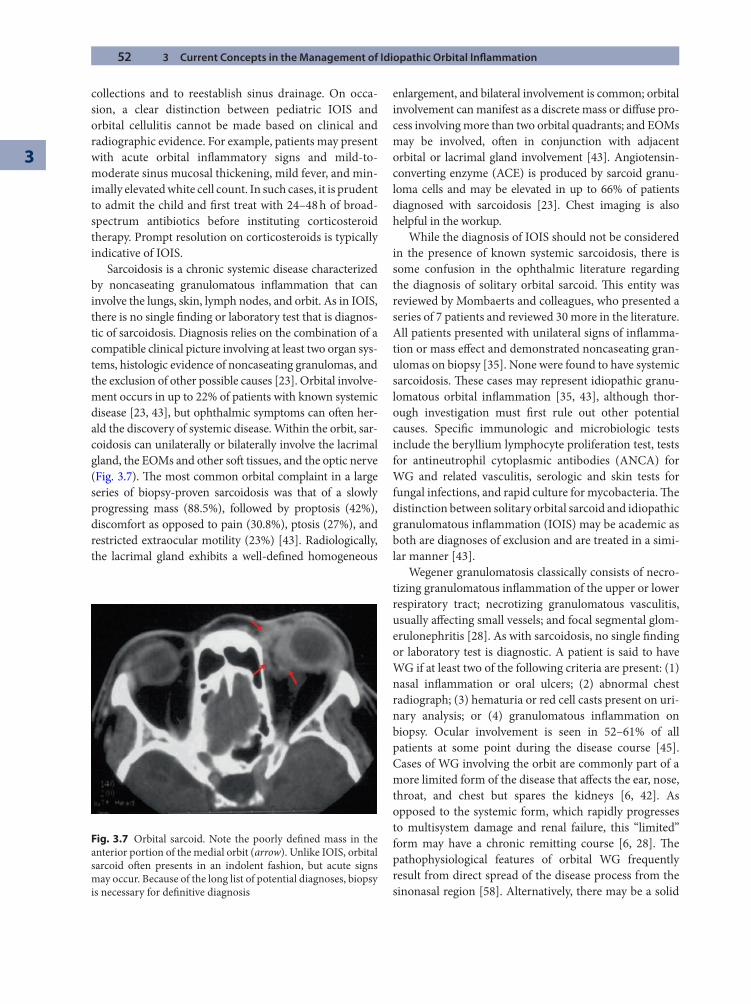
52 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
collections and to reestablish sinus drainage. On occa-sion, a clear distinction between pediatric IOIS and orbital cellulitis cannot be made based on clinical and radiographic evidence. For example, patients may present with acute orbital infl ammatory signs and mild-to- moderate sinus mucosal thickening, mild fever, and min-imally elevated white cell count. In such cases, it is prudent to admit the child and fi rst treat with 24–48 h of broad-spectrum antibiotics before instituting corticosteroid therapy. Prompt resolution on corticosteroids is typically indicative of IOIS.
Sarcoidosis is a chronic systemic disease characterized by noncaseating granulomatous infl ammation that can involve the lungs, skin, lymph nodes, and orbit. As in IOIS, there is no single fi nding or laboratory test that is diagnos-tic of sarcoidosis. Diagnosis relies on the combination of a compatible clinical picture involving at least two organ sys-tems, histologic evidence of noncaseating granulomas, and the exclusion of other possible causes [23]. Orbital involve-ment occurs in up to 22% of patients with known systemic disease [23, 43], but ophthalmic symptoms can oft en her-ald the discovery of systemic disease. Within the orbit, sar-coidosis can unilaterally or bilaterally involve the lacrimal gland, the EOMs and other soft tissues, and the optic nerve (Fig. 3.7). Th e most common orbital complaint in a large series of biopsy-proven sarcoidosis was that of a slowly progressing mass (88.5%), followed by proptosis (42%), discomfort as opposed to pain (30.8%), ptosis (27%), and restricted extraocular motility (23%) [43]. Radiologically, the lacrimal gland exhibits a well-defi ned homogeneous
enlargement, and bilateral involvement is common; orbital involvement can manifest as a discrete mass or diff use pro-cess involving more than two orbital quadrants; and EOMs may be involved, oft en in conjunction with adjacent orbital or lacrimal gland involvement [43]. Angiotensin-converting enzyme (ACE) is produced by sarcoid granu-loma cells and may be elevated in up to 66% of patients diagnosed with sarcoidosis [23]. Chest imaging is also helpful in the workup.
While the diagnosis of IOIS should not be considered in the presence of known systemic sarcoidosis, there is some confusion in the ophthalmic literature regarding the diagnosis of solitary orbital sarcoid. Th is entity was reviewed by Mombaerts and colleagues, who presented a series of 7 patients and reviewed 30 more in the literature. All patients presented with unilateral signs of infl amma-tion or mass eff ect and demonstrated noncaseating gran-ulomas on biopsy [35]. None were found to have systemic sarcoidosis. Th ese cases may represent idiopathic granu-lomatous orbital infl ammation [35, 43], although thor-ough investigation must fi rst rule out other potential causes. Specifi c immunologic and microbiologic tests include the beryllium lymphocyte proliferation test, tests for antineutrophil cytoplasmic antibodies (ANCA) for WG and related vasculitis, serologic and skin tests for fungal infections, and rapid culture for mycobacteria. Th e distinction between solitary orbital sarcoid and idiopathic granulomatous infl ammation (IOIS) may be academic as both are diagnoses of exclusion and are treated in a simi-lar manner [43].
Wegener granulomatosis classically consists of necro-tizing granulomatous infl ammation of the upper or lower respiratory tract; necrotizing granulomatous vasculitis, usually aff ecting small vessels; and focal segmental glom-erulonephritis [28]. As with sarcoidosis, no single fi nding or laboratory test is diagnostic. A patient is said to have WG if at least two of the following criteria are present: (1) nasal infl ammation or oral ulcers; (2) abnormal chest radiograph; (3) hematuria or red cell casts present on uri-nary analysis; or (4) granulomatous infl ammation on biopsy. Ocular involvement is seen in 52–61% of all patients at some point during the disease course [45]. Cases of WG involving the orbit are commonly part of a more limited form of the disease that aff ects the ear, nose, throat, and chest but spares the kidneys [6, 42]. As opposed to the systemic form, which rapidly progresses to multisystem damage and renal failure, this “limited” form may have a chronic remitting course [6, 28]. Th e pathophysiological features of orbital WG frequently result from direct spread of the disease process from the sinonasal region [58]. Alternatively, there may be a solid
Fig. 3.7 Orbital sarcoid. Note the poorly defi ned mass in the anterior portion of the medial orbit (arrow). Unlike IOIS, orbital sarcoid oft en presents in an indolent fashion, but acute signs may occur. Because of the long list of potential diagnoses, biopsy is necessary for defi nitive diagnosis
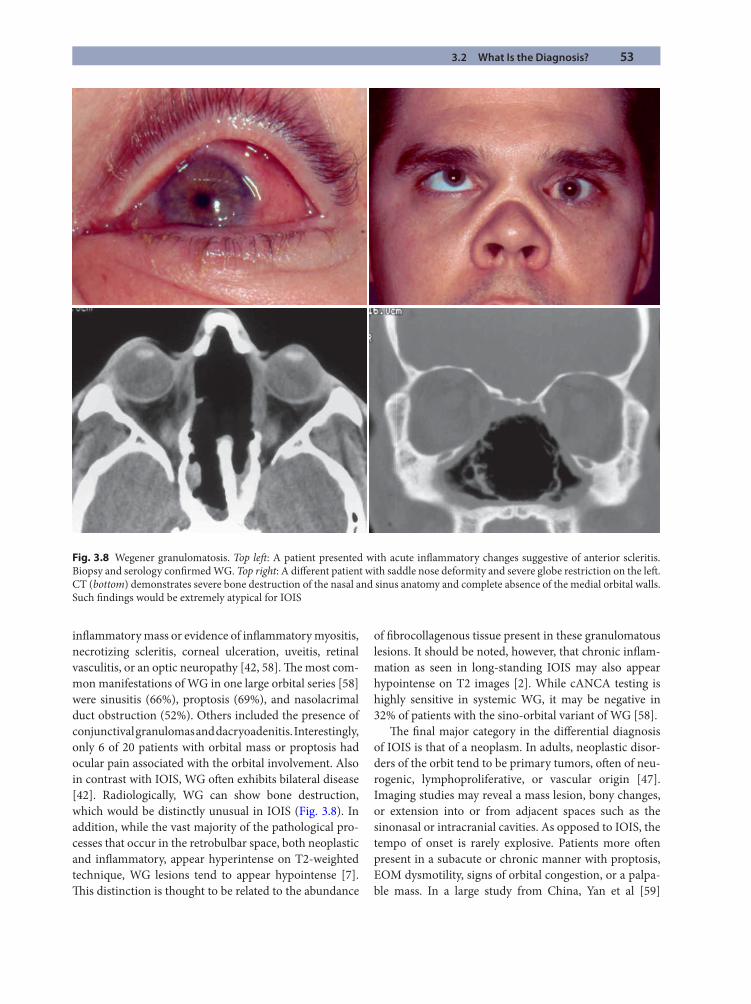
3.2 What Is the Diagnosis? 53
infl ammatory mass or evidence of infl ammatory myositis, necrotizing scleritis, corneal ulceration, uveitis, retinal vasculitis, or an optic neuropathy [42, 58]. Th e most com-mon manifestations of WG in one large orbital series [58] were sinusitis (66%), proptosis (69%), and nasolacrimal duct obstruction (52%). Others included the presence of conjunctival granulomas and dacryoadenitis. Interestingly, only 6 of 20 patients with orbital mass or proptosis had ocular pain associated with the orbital involvement. Also in contrast with IOIS, WG oft en exhibits bilateral disease [42]. Radiologically, WG can show bone destruction, which would be distinctly unusual in IOIS (Fig. 3.8). In addition, while the vast majority of the pathological pro-cesses that occur in the retrobulbar space, both neoplastic and infl ammatory, appear hyperintense on T2-weighted technique, WG lesions tend to appear hypointense [7]. Th is distinction is thought to be related to the abundance
of fi brocollagenous tissue present in these granulomatous lesions. It should be noted, however, that chronic infl am-mation as seen in long-standing IOIS may also appear hypointense on T2 images [2]. While cANCA testing is highly sensitive in systemic WG, it may be negative in 32% of patients with the sino-orbital variant of WG [58].
Th e fi nal major category in the diff erential diagnosis of IOIS is that of a neoplasm. In adults, neoplastic disor-ders of the orbit tend to be primary tumors, oft en of neu-rogenic, lymphoproliferative, or vascular origin [47]. Imaging studies may reveal a mass lesion, bony changes, or extension into or from adjacent spaces such as the sinonasal or intracranial cavities. As opposed to IOIS, the tempo of onset is rarely explosive. Patients more oft en present in a subacute or chronic manner with proptosis, EOM dysmotility, signs of orbital congestion, or a palpa-ble mass. In a large study from China, Yan et al [59]
Fig. 3.8 Wegener granulomatosis. Top left : A patient presented with acute infl ammatory changes suggestive of anterior scleritis. Biopsy and serology confi rmed WG. Top right: A diff erent patient with saddle nose deformity and severe globe restriction on the left . CT (bottom) demonstrates severe bone destruction of the nasal and sinus anatomy and complete absence of the medial orbital walls. Such fi ndings would be extremely atypical for IOIS
54 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
compared patients with IOIS to those with lymphoma and found that more patients with lymphoid tumors had a palpable mass than did patients with IOIS (90% vs. 65%, p < .0001). Th ey also noted that patients with IOIS were more likely to present with lid swelling (55% vs. 40%, p = .014); eyelid or conjunctival congestion (42% vs. 24%, p = .001); and pain (24% and 1%, p < .0001), among others. Two entities that may mimic IOIS in the pediatric popu-lation need to stressed. Rhabdomyosarcoma presents with rapidly progressive orbital signs (proptosis, globe malposition) in the absence of acute infl ammation (pain, erythema, etc.), but on occasion, infl ammation may also be present [53]. Conversely, a ruptured dermoid cyst presents with an intense infl ammatory orbital reaction that may mimic cellulitis or IOIS [53].
Tumors metastatic to the orbit are rare, representing 7–10% of all orbital neoplasms [47, 53]. Similar to IOIS, diplopia, ocular motility limitation, proptosis, or globe dystopia and the presence of a palpable mass are common signs and symptoms of metastasis to the orbit [14, 16]. However, the tempo of onset tends to be less acute than in IOIS (Fig. 3.9). Common primary sites include breast, prostate, lung, and kidney. Of note, orbital metastasis may be the presenting sign of systemic cancer in as many as 25–30% [14, 53] of patients. Certainly, in any patient with a known history of cancer, the diagnosis of IOIS should be made with extreme caution. Even if biopsy of the involved tissue may appear infl ammatory, the possi-bility of an acute or chronic infl ammatory reaction sur-rounding a metastatic lesion should also be considered.
3.2.2 A Diagnostic Corticosteroid Trial?
Despite patient age, duration of symptoms, or tissue type involved, one of the most consistent fi ndings in patients with IOIS is an exquisite sensitivity to corticosteroids. It is common to observe near-complete resolution of a patient’s signs and symptoms aft er the fi rst dose or two of oral or intravenous steroids (Fig. 3.10). Some have advocated that such a rapid and signifi cant response to corticoster-oids be considered diagnostic of IOIS [29]. Others coun-ter that any type of reactive infl ammation, be it due to tumor, infection, systemic vasculitis, or hematological malignancy, will demonstrate clinical improvement with systemic steroids, and that therefore a “steroid response” cannot be used as a diagnostic test for IOIS [34, 49]. Th ere are also numerous examples in the literature of patients with IOIS who “fail” corticosteroid therapy. Care must be taken in interpreting these steroid failures, however, as steroid resistance may be multifactorial. For example, inadequate dosage may result in incomplete resolution of
a patient’s symptoms and thus may be interpreted as treat-ment failure. Th e standard oral dose for suspected IOIS is between 1.0 and 1.5 mg/kg/day or approximately 80 mg of prednisone a day for a 70-kg adult. In addition, corticos-teroids that are tapered too rapidly may predispose a patient to signifi cant symptomatic fl ares, which may also be misconstrued as “steroid failures.”
Th e literature addressing the use of corticosteroids in the diagnosis of IOIS is limited. Mombaerts et al exam-ined the effi cacy of systemic corticosteroids in a group
Summary for the Clinician
IOIS is a diagnosis of exclusion. ■
Patients with TED may present with periorbital ■
pain, proptosis, and diplopia that is slow in onset and accompanied by characteristic eyelid fi nd-ings, such as upper eyelid retraction and lateral fl are.Acute bacterial cellulitis has an abrupt onset, is ■
painful, and is oft en associated with a prior his-tory of sinusitis, dental disease, or trauma. Patients are oft en febrile with an elevated white blood cell count. Orbital imaging usually distin-guishes infection from IOIS.Sarcoidosis is a chronic systemic disease charac- ■
terized by noncaseating granulomatous infl am-mation involving at least two organ systems. Within the orbit, sarcoidosis can involve the lac-rimal gland, the EOMs and other soft tissues, and the optic nerve. On occasion, isolated orbital sar-coid may occur with no serologic or chest abnormality.WG is a chronic systemic disease characterized by ■
necrotizing granulomatous infl ammation of the upper or lower respiratory tract; necrotizing gran-ulomatous vasculitis, usually aff ecting small ves-sels; and focal segmental glomerulonephritis. Cases involving the orbit may be part of a more limited form of the disease and may present with sinusitis, proptosis, nasolacrimal duct obstruction, conjunc-tival granulomas, or dacryoadenitis. cANCA may be negative in the limited form of WG.Primary orbital tumors oft en present with the ■
insidious onset of proptosis, orbital congestion, or diplopia.Tumors metastatic to the orbit are rare but may pres- ■
ent in a manner similar to IOIS. Orbital biopsy should be strongly considered in any patient with a known history of cancer who presents with suspected IOIS.
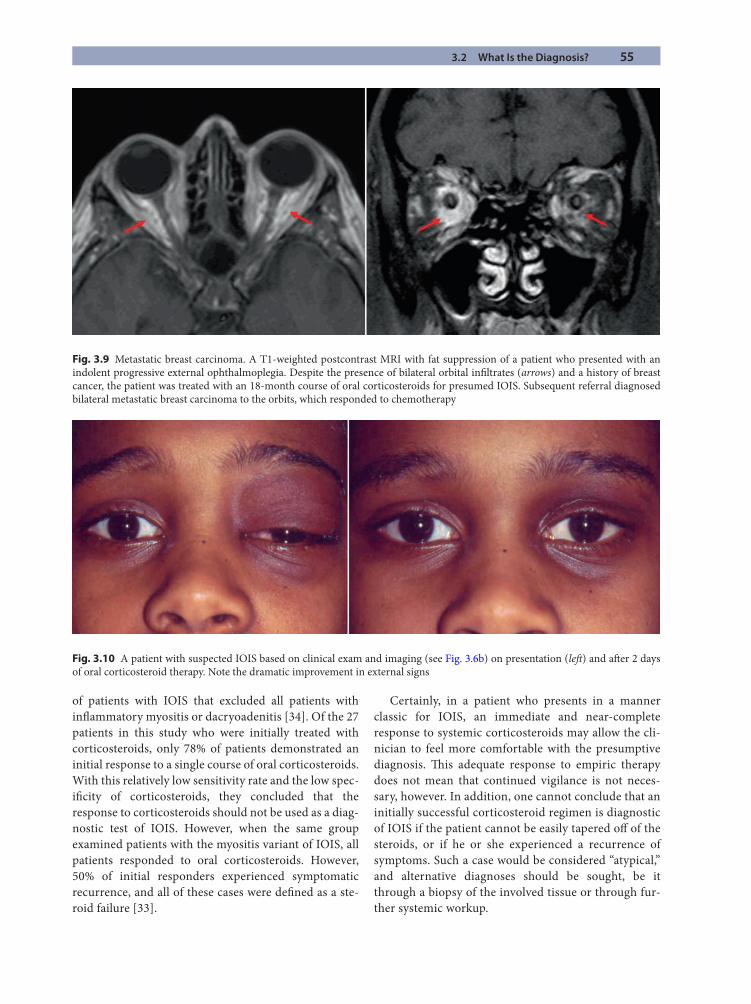
3.2 What Is the Diagnosis? 55
of patients with IOIS that excluded all patients with infl ammatory myositis or dacryoadenitis [34]. Of the 27 patients in this study who were initially treated with corticosteroids, only 78% of patients demonstrated an initial response to a single course of oral corticosteroids. With this relatively low sensitivity rate and the low spec-ifi city of corticosteroids, they concluded that the response to corticosteroids should not be used as a diag-nostic test of IOIS. However, when the same group examined patients with the myositis variant of IOIS, all patients responded to oral corticosteroids. However, 50% of initial responders experienced symptomatic recurrence, and all of these cases were defi ned as a ste-roid failure [33].
Certainly, in a patient who presents in a manner classic for IOIS, an immediate and near-complete response to systemic corticosteroids may allow the cli-nician to feel more comfortable with the presumptive diagnosis. Th is adequate response to empiric therapy does not mean that continued vigilance is not neces-sary, however. In addition, one cannot conclude that an initially successful corticosteroid regimen is diagnostic of IOIS if the patient cannot be easily tapered off of the steroids, or if he or she experienced a recurrence of symptoms. Such a case would be considered “atypical,” and alternative diagnoses should be sought, be it through a biopsy of the involved tissue or through fur-ther systemic workup.
Fig. 3.9 Metastatic breast carcinoma. A T1-weighted postcontrast MRI with fat suppression of a patient who presented with an indolent progressive external ophthalmoplegia. Despite the presence of bilateral orbital infi ltrates (arrows) and a history of breast cancer, the patient was treated with an 18-month course of oral corticosteroids for presumed IOIS. Subsequent referral diagnosed bilateral metastatic breast carcinoma to the orbits, which responded to chemotherapy
Fig. 3.10 A patient with suspected IOIS based on clinical exam and imaging (see Fig. 3.6b) on presentation (left ) and aft er 2 days of oral corticosteroid therapy. Note the dramatic improvement in external signs
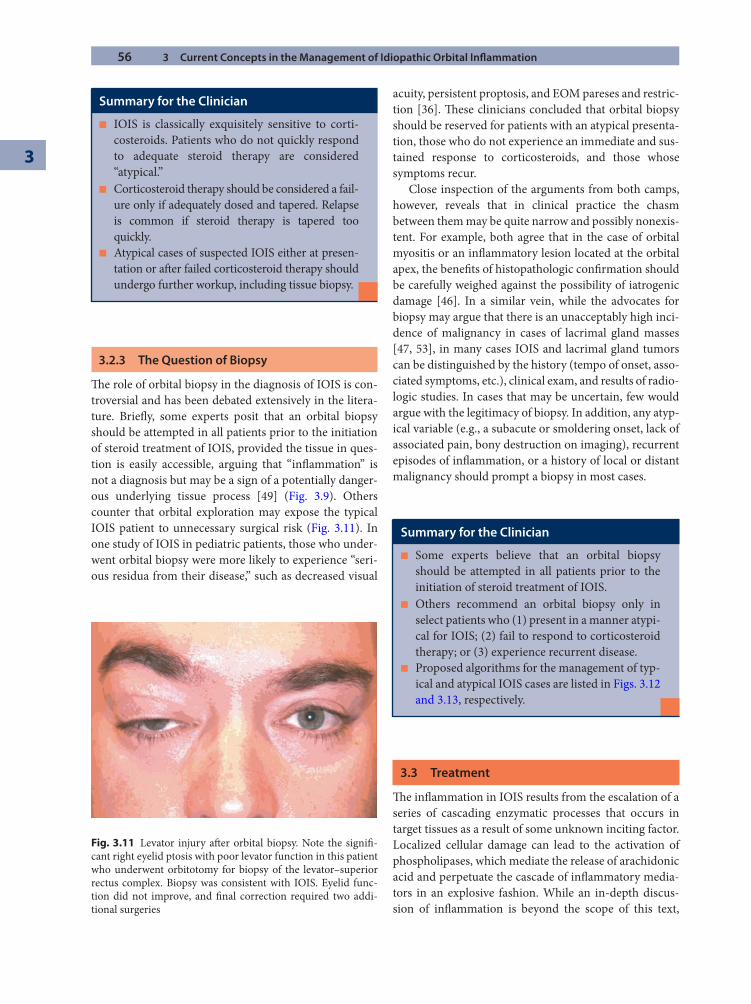
56 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
3.2.3 The Question of Biopsy
Th e role of orbital biopsy in the diagnosis of IOIS is con-troversial and has been debated extensively in the litera-ture. Briefl y, some experts posit that an orbital biopsy should be attempted in all patients prior to the initiation of steroid treatment of IOIS, provided the tissue in ques-tion is easily accessible, arguing that “infl ammation” is not a diagnosis but may be a sign of a potentially danger-ous underlying tissue process [49] (Fig. 3.9). Others counter that orbital exploration may expose the typical IOIS patient to unnecessary surgical risk (Fig. 3.11). In one study of IOIS in pediatric patients, those who under-went orbital biopsy were more likely to experience “seri-ous residua from their disease,” such as decreased visual
acuity, persistent proptosis, and EOM pareses and restric-tion [36]. Th ese clinicians concluded that orbital biopsy should be reserved for patients with an atypical presenta-tion, those who do not experience an immediate and sus-tained response to corticosteroids, and those whose symptoms recur.
Close inspection of the arguments from both camps, however, reveals that in clinical practice the chasm between them may be quite narrow and possibly nonexis-tent. For example, both agree that in the case of orbital myositis or an infl ammatory lesion located at the orbital apex, the benefi ts of histopathologic confi rmation should be carefully weighed against the possibility of iatrogenic damage [46]. In a similar vein, while the advocates for biopsy may argue that there is an unacceptably high inci-dence of malignancy in cases of lacrimal gland masses [47, 53], in many cases IOIS and lacrimal gland tumors can be distinguished by the history (tempo of onset, asso-ciated symptoms, etc.), clinical exam, and results of radio-logic studies. In cases that may be uncertain, few would argue with the legitimacy of biopsy. In addition, any atyp-ical variable (e.g., a subacute or smoldering onset, lack of associated pain, bony destruction on imaging), recurrent episodes of infl ammation, or a history of local or distant malignancy should prompt a biopsy in most cases.
3.3 Treatment
Th e infl ammation in IOIS results from the escalation of a series of cascading enzymatic processes that occurs in target tissues as a result of some unknown inciting factor. Localized cellular damage can lead to the activation of phospholipases, which mediate the release of arachidonic acid and perpetuate the cascade of infl ammatory media-tors in an explosive fashion. While an in-depth discus-sion of infl ammation is beyond the scope of this text,
Summary for the Clinician
IOIS is classically exquisitely sensitive to corti- ■
costeroids. Patients who do not quickly respond to adequate steroid therapy are considered “atypical.”Corticosteroid therapy should be considered a fail- ■
ure only if adequately dosed and tapered. Relapse is common if steroid therapy is tapered too quickly.Atypical cases of suspected IOIS either at presen- ■
tation or aft er failed corticosteroid therapy should undergo further workup, including tissue biopsy.
Fig. 3.11 Levator injury aft er orbital biopsy. Note the signifi -cant right eyelid ptosis with poor levator function in this patient who underwent orbitotomy for biopsy of the levator–superior rectus complex. Biopsy was consistent with IOIS. Eyelid func-tion did not improve, and fi nal correction required two addi-tional surgeries
Summary for the Clinician
Some experts believe that an orbital biopsy ■
should be attempted in all patients prior to the initiation of steroid treatment of IOIS.Others recommend an orbital biopsy only in ■
select patients who (1) present in a manner atypi-cal for IOIS; (2) fail to respond to corticosteroid therapy; or (3) experience recurrent disease.Proposed algorithms for the management of typ- ■
ical and atypical IOIS cases are listed in Figs. 3.12 and 3.13, respectively.
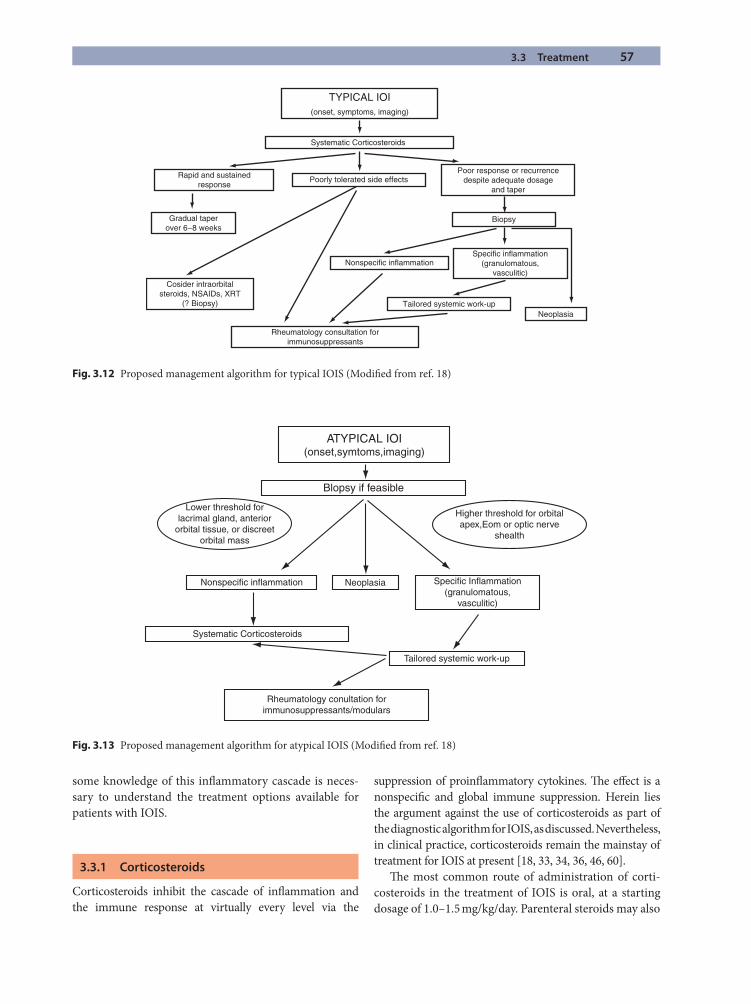
3.3 Treatment 57
some knowledge of this infl ammatory cascade is neces-sary to understand the treatment options available for patients with IOIS.
3.3.1 Corticosteroids
Corticosteroids inhibit the cascade of infl ammation and the immune response at virtually every level via the
suppression of proinfl ammatory cytokines. Th e eff ect is a nonspecifi c and global immune suppression. Herein lies the argument against the use of corticosteroids as part of the diagnostic algorithm for IOIS, as discussed. Nevertheless, in clinical practice, corticosteroids remain the mainstay of treatment for IOIS at present [18, 33, 34, 36, 46, 60].
Th e most common route of administration of corti-costeroids in the treatment of IOIS is oral, at a starting dosage of 1.0–1.5 mg/kg/day. Parenteral steroids may also
Blopsy if feasible
ATYPICAL IOI(onset,symtoms,imaging)
Lower threshold forlacrimal gland, anterior
orbital tissue, or discreetorbital mass
Higher threshold for orbitalapex,Eom or optic nerve
shealth
Specific Inflammation(granulomatous,
vasculitic)
NeoplasiaNonspecific inflammation
Systematic Corticosteroids
Tailored systemic work-up
Rheumatology conultation forimmunosuppressants/modulars
Fig. 3.13 Proposed management algorithm for atypical IOIS (Modifi ed from ref. 18)
Fig. 3.12 Proposed management algorithm for typical IOIS (Modifi ed from ref. 18)
TYPICAL IOI(onset, symptoms, imaging)
Systematic Corticosteroids
Rapid and sustainedresponse
Poorly tolerated side effectsPoor response or recurrence
despite adequate dosageand taper
Biopsy
Specific inflammation(granulomatous,
vasculitic)
NeoplasiaTailored systemic work-up
Rheumatology consultation forimmunosuppressants
Gradual taperover 6−8 weeks
Cosider intraorbitalsteroids, NSAIDs, XRT
(? Biopsy)
Nonspecific inflammation

58 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
be employed, usually in cases of IOIS-related optic neu-ropathy. Th e initial dose is tapered over the course of weeks to months, as dictated by the patient’s symptoms. While too rapid a taper may predispose the patient to rebound infl ammation, a prolonged steroid taper will expose the patient to some of the more serious treatment-related side eff ects. Weight gain, gastritis, cushingoid facies, and mood swings are commonly cited eff ects. Corticosteroid treatment can also exacerbate or induce diabetes, hypertension, glaucoma, and cataract in suscep-tible patients. In light of the signifi cant side eff ects of sys-temic therapy, some authors advocate local intraorbital injection of triamcinolone acetonide in cases of infl am-matory masses or dacryoadenitis [15]. It should be noted that this is an off -label use of the medication, and it car-ries with it the inherent risk of retinal vasculature embo-lization of particulate matter.
A review of the literature reveals numerous examples of “steroid-resistant” IOIS as well as outright steroid fail-ures. Direct comparison of published studies is diffi cult, however, as inclusion criteria and treatment protocols are inconsistent at best. For example, Mombaerts et al reported a low cure rate (37%) and a high recurrence rate (52%) of IOIS treated with corticosteroids; however, patients with myositis and lacrimal gland involvement were excluded from analysis [34]. In a separate study looking only at patients with idiopathic infl ammatory myositis, the authors reported that all patients responded well to corticosteroid therapy, but symptoms recurred in 50% with prolonged follow-up [33]. In Yuen and Rubin’s study [60], 69% of patients were managed with corticos-teroids alone and a further 9% with the addition of a nonsteroidal anti-infl ammatory drug (NSAID) to man-age residual symptoms, for a total of 78%. An incom-plete resolution of symptoms was noted in approximately 30%, and these patients were designated steroid failures.
3.3.2 Radiation
Radiotherapy is eff ective treatment for IOIS, especially in patients who are steroid responsive but intolerant of ste-roid-related side eff ects. Th e studies demonstrating effi -cacy of radiation therapy are somewhat dated and, as is the problem with many studies concerning IOIS, are dif-fi cult to compare due to diff erent inclusion criteria and treatment measures. For example, Sergott et al [51] showed a response in 15 of 21 patients (72%) with a dose of 1,000–2,000 cGy over 10–15 days. Orcutt et al [40], on the other hand, showed a 75% treatment eff ect at doses of 2,500 cGy over 15 days. Gunalp et al [17] reported successful results
of radiation treatment in 9 of 14 (64%) of patients who failed to respond to corticosteroid therapy.
Fortunately, the side eff ects of low-dose orbital radia-tion in the range of 1,000–2,500 cGy are rare. Th e eyelids tolerate approximately 5,000–6,000 cGy before exhibiting signifi cant signs of radiation dermatitis and eyelid scar-ring. Similar doses induce lacrimal gland atrophy, radia-tion retinopathy, and optic neuropathy. At the lower end, punctate keratopathy and conjunctivitis are noted with dosages of between 3,000 and 4,000 cGy. A radiation cata-ract may develop at 2,000 cGy [1]. However, these radia-tion dosage associations are averages; certain patients, such as those with vasculopathic risk factors (hyperten-sion, diabetes mellitus, etc.), may be more at risk for adverse events related to radiation therapy.
3.3.3 Other Agents
Following a lead from rheumatologists and dermatolo-gists, there has been a growing interest among orbital specialists in the use of immunomodulating agents in the treatment of IOIS. Although corticosteroids remain a fi rst-line treatment, immunosuppressive agents, includ-ing antimetabolites (e.g., methotrexate [MTX], azathio-prine); alkylating agents (e.g., cyclophosphamide, chlorambucil); T-cell inhibitors (e.g., cyclosporine, tac-rolimus); and biologics (e.g., infl iximab, etanercep) it are increasingly used as steroid-sparing alternatives.
Methotrexate is an antimetabolite that interferes with intracellular folic acid metabolism during DNA and RNA synthesis. It is a cytotoxic agent that is used in combina-tion with other chemotherapeutic agents in the treatment of many types of cancers. Lower doses of MTX have been shown to be very eff ective for the management of rheuma-toid arthritis, Crohn disease, and psoriasis [24]. Several small studies have addressed the usefulness of MTX in the treatment of orbital infl ammatory disease. Both Shah et al [52] and Smith and Rosenbaum [55] showed that MXT (7.5–25 mg/week) had some benefi t in patients with non-infectious orbital infl ammatory disease, including IOIS, who had failed to respond to systemic corticosteroids or orbital irradiation. Azithroprine is also an antimetabolite that works by inhibiting purine synthesis. Like MTX, it has been used in the treatment of various rheumatologic and dermatologic conditions (i.e., rheumatoid arthritis, infl ammatory bowel disease, pemphigus, systemic lupus erythematosis), but its effi cacy in terms of orbital disease is limited to a small number of case reports [9].
Alkylating agents slow or stop cell growth by forming cross-links between DNA strands, inducing apoptosis. Examples include cyclophosphamide (Cytoxan), a mainstay
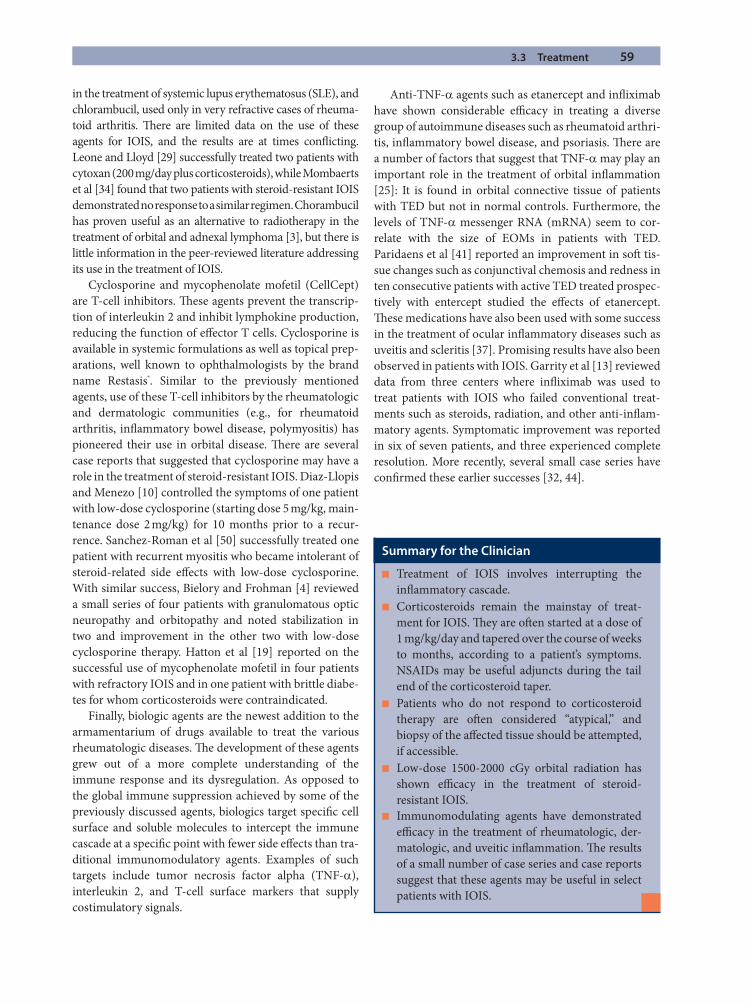
3.3 Treatment 59
in the treatment of systemic lupus erythematosus (SLE), and chlorambucil, used only in very refractive cases of rheuma-toid arthritis. Th ere are limited data on the use of these agents for IOIS, and the results are at times confl icting. Leone and Lloyd [29] successfully treated two patients with cytoxan (200 mg/day plus corticosteroids), while Mombaerts et al [34] found that two patients with steroid-resistant IOIS demonstrated no response to a similar regimen. Chorambucil has proven useful as an alternative to radiotherapy in the treatment of orbital and adnexal lymphoma [3], but there is little information in the peer-reviewed literature addressing its use in the treatment of IOIS.
Cyclosporine and mycophenolate mofetil (CellCept) are T-cell inhibitors. Th ese agents prevent the transcrip-tion of interleukin 2 and inhibit lymphokine production, reducing the function of eff ector T cells. Cyclosporine is available in systemic formulations as well as topical prep-arations, well known to ophthalmologists by the brand name Restasis®. Similar to the previously mentioned agents, use of these T-cell inhibitors by the rheumatologic and dermatologic communities (e.g., for rheumatoid arthritis, infl ammatory bowel disease, polymyositis) has pioneered their use in orbital disease. Th ere are several case reports that suggested that cyclosporine may have a role in the treatment of steroid-resistant IOIS. Diaz-Llopis and Menezo [10] controlled the symptoms of one patient with low-dose cyclosporine (starting dose 5 mg/kg, main-tenance dose 2 mg/kg) for 10 months prior to a recur-rence. Sanchez-Roman et al [50] successfully treated one patient with recurrent myositis who became intolerant of steroid-related side eff ects with low-dose cyclosporine. With similar success, Bielory and Frohman [4] reviewed a small series of four patients with granulomatous optic neuropathy and orbitopathy and noted stabilization in two and improvement in the other two with low-dose cyclosporine therapy. Hatton et al [19] reported on the successful use of mycophenolate mofetil in four patients with refractory IOIS and in one patient with brittle diabe-tes for whom corticosteroids were contraindicated.
Finally, biologic agents are the newest addition to the armamentarium of drugs available to treat the various rheumatologic diseases. Th e development of these agents grew out of a more complete understanding of the immune response and its dysregulation. As opposed to the global immune suppression achieved by some of the previously discussed agents, biologics target specifi c cell surface and soluble molecules to intercept the immune cascade at a specifi c point with fewer side eff ects than tra-ditional immunomodulatory agents. Examples of such targets include tumor necrosis factor alpha (TNF-a), interleukin 2, and T-cell surface markers that supply costimulatory signals.
Anti-TNF-a agents such as etanercept and infl iximab have shown considerable effi cacy in treating a diverse group of autoimmune diseases such as rheumatoid arthri-tis, infl ammatory bowel disease, and psoriasis. Th ere are a number of factors that suggest that TNF-a may play an important role in the treatment of orbital infl ammation [25]: It is found in orbital connective tissue of patients with TED but not in normal controls. Furthermore, the levels of TNF-a messenger RNA (mRNA) seem to cor-relate with the size of EOMs in patients with TED. Paridaens et al [41] reported an improvement in soft tis-sue changes such as conjunctival chemosis and redness in ten consecutive patients with active TED treated prospec-tively with entercept studied the eff ects of etanercept. Th ese medications have also been used with some success in the treatment of ocular infl ammatory diseases such as uveitis and scleritis [37]. Promising results have also been observed in patients with IOIS. Garrity et al [13] reviewed data from three centers where infl iximab was used to treat patients with IOIS who failed conventional treat-ments such as steroids, radiation, and other anti-infl am-matory agents. Symptomatic improvement was reported in six of seven patients, and three experienced complete resolution. More recently, several small case series have confi rmed these earlier successes [32, 44].
Summary for the Clinician
Treatment of IOIS involves interrupting the ■
infl ammatory cascade.Corticosteroids remain the mainstay of treat- ■
ment for IOIS. Th ey are oft en started at a dose of 1 mg/kg/day and tapered over the course of weeks to months, according to a patient’s symptoms. NSAIDs may be useful adjuncts during the tail end of the corticosteroid taper.Patients who do not respond to corticosteroid ■
therapy are oft en considered “atypical,” and biopsy of the aff ected tissue should be attempted, if accessible.Low-dose 1500-2000 cGy orbital radiation has ■
shown effi cacy in the treatment of steroid- resistant IOIS.Immunomodulating agents have demonstrated ■
effi cacy in the treatment of rheumatologic, der-matologic, and uveitic infl ammation. Th e results of a small number of case series and case reports suggest that these agents may be useful in select patients with IOIS.

60 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
3.4 Special Circumstances
3.4.1 Pediatric IOIS
Pediatric IOIS comprises between 6% and 16% of all IOIS in published series [5, 7, 34, 60]. While the signs and symptoms of IOIS are generally consistent across all age groups, a number of large studies have ascribed several features of pediatric IOIS that are thought to be atypical in the adult population: (1) the presence of constitutional symptoms; (2) accompanying anterior chamber reaction; and (3) the presence of bilateral disease [34, 36].
Th e diff erential diagnosis of IOIS in children includes orbital cellulitis and trauma as well as such potentially lethal entities as rhabdomyosarcoma and neuroblastoma, among others. While “classic” IOIS in a child may be approached in a manner similar to that used in adults, a high degree of suspicion should be maintained. As in the adult population, any patient with atypical presentation or recurrent disease should undergo orbital biopsy of the involved tissue.
Th e treatment algorithm for pediatric IOIS is also similar to that of the adult population. However, certain aspects deserve mention. Corticosteroids should be administered based on a weight-based formula, typically at a dosage of 1 mg/kg/day for oral prednisone. Steroid-related side eff ects, such as increased appetite, weight gain, gastritis, headache, and mood swings are common in children, and the classic cushingoid appearance may develop quickly. Corticosteroids also have an eff ect on linear growth, especially with prolonged therapy [8]. Fortunately, corticosteroids also inhibit closure of epi-physeal plates [22]. Once the steroids are tapered, chil-dren oft en experience rebound growth, allowing them to rejoin previous growth curves and attain normal adult height. Other known complications of steroid use, such as hypertension, diabetes, glaucoma, and cataract, are rare in the pediatric population [8, 22].
Th e data with regard to other treatment modalities are sparse for pediatric IOIS. Radiation therapy is generally avoided in children due to fears of inducing bony hyp-oplasia, soft tissue deformities, and secondary tumors, such as are seen in children receiving radiation for retino-blastoma and rhabdomyosarcoma. Although the dosages in the treatment are much lower (2,000 cGy vs. 5,000–6,000 cGy), there are no studies in the literature docu-menting a “safe” dosage. Anecdotally, we have treated two patients, ages 11 and 15, with orbital radiation. Both have been followed for more than 4 years, and neither has experienced any treatment-related side eff ects.
Methotrexate, cyclosporine, and etanercept have been used with much success in the treatment of pediatric
uveitis [54] and rheumatologic diseases [38]. Th ese agents may also be employed in the treatment of children with refractory IOIS or in those who become intolerant of steroid-related side eff ects, although there is very little published to support this use. Consultation and coman-agement with a pediatric rheumatologist familiar with the use of these steroid-sparing and immunomodulating agents are recommended.
3.4.2 Sclerosing Pseudotumor
Idiopathic sclerosing orbital infl ammation (ISOI) is a rare cause of orbital infl ammation that some consider a distinct clinicopathological entity [48]. It is character-ized by a chronic, slowly progressive course and lacks the acute onset frequently associated with IOIS. Common signs and symptoms of ISOI include a dull pain, propto-sis, EOM restriction with diplopia, and mild-to-moder-ate infl ammation [21, 48]. Within the orbit, the superior and lateral portions, particularly the lacrimal gland, tend to be aff ected more oft en; however, up to 50% of patients may present with an apical mass [21, 48]. Th e disease is oft en unilateral but may be bilateral and asymmetric (Fig. 3.14).
On imaging, ISOS is characterized by a homoge-neously enhancing mass with irregular margins, which may obliterate adjacent structures such as EOMs, the lac-rimal gland, or bone. Th e masses are deeply hypointense on T2-weighted sequences. Histopathologically, normal anatomic structures are replaced by broad areas of fi bro-sis with a sparse infl ammatory infi ltrate of lymphocytes, plasma cells, histiocytes, eosinophils, and neutrophils [21, 48]. Th is characteristic picture is also seen in retro-peritoneal fi brosis, a condition with which ISOI may be associated [31]. Calcifi cation may also be present [61].
Summary for the Clinician
Th e signs and symptoms of IOIS in the pediatric ■
population are similar to those of adults. Th e presence of bilateral disease, constitutional symp-toms, and an accompanying anterior chamber reaction may be more common in children. Peripheral eosinophilia may also be present.Corticosteroid dosages for treatment of IOIS ■
should be calculated based on the child’s weight (1 mg/kg/day).Th erapeutic management of pediatric IOIS should ■
be managed in conjunction with pediatricians or pediatric rheumatologists familiar with the dos-ages and side eff ects of treatment regimens.
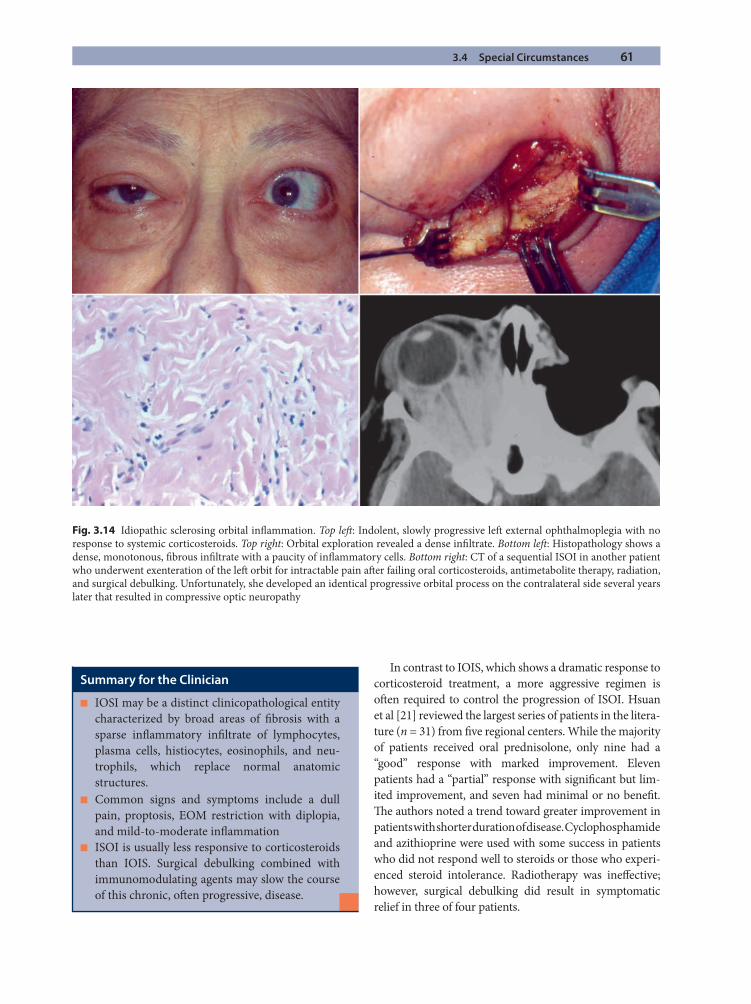
3.4 Special Circumstances 61
In contrast to IOIS, which shows a dramatic response to corticosteroid treatment, a more aggressive regimen is oft en required to control the progression of ISOI. Hsuan et al [21] reviewed the largest series of patients in the litera-ture (n = 31) from fi ve regional centers. While the majority of patients received oral prednisolone, only nine had a “good” response with marked improvement. Eleven patients had a “partial” response with signifi cant but lim-ited improvement, and seven had minimal or no benefi t. Th e authors noted a trend toward greater improvement in patients with shorter duration of disease. Cyclophosphamide and azithioprine were used with some success in patients who did not respond well to steroids or those who experi-enced steroid intolerance. Radiotherapy was ineff ective; however, surgical debulking did result in symptomatic relief in three of four patients.
Summary for the Clinician
IOSI may be a distinct clinicopathological entity ■
characterized by broad areas of fi brosis with a sparse infl ammatory infi ltrate of lymphocytes, plasma cells, histiocytes, eosinophils, and neu-trophils, which replace normal anatomic structures.Common signs and symptoms include a dull ■
pain, proptosis, EOM restriction with diplopia, and mild-to-moderate infl ammationISOI is usually less responsive to corticosteroids ■
than IOIS. Surgical debulking combined with immunomodulating agents may slow the course of this chronic, oft en progressive, disease.
Fig. 3.14 Idiopathic sclerosing orbital infl ammation. Top left : Indolent, slowly progressive left external ophthalmoplegia with no response to systemic corticosteroids. Top right: Orbital exploration revealed a dense infi ltrate. Bottom left : Histopathology shows a dense, monotonous, fi brous infi ltrate with a paucity of infl ammatory cells. Bottom right: CT of a sequential ISOI in another patient who underwent exenteration of the left orbit for intractable pain aft er failing oral corticosteroids, antimetabolite therapy, radiation, and surgical debulking. Unfortunately, she developed an identical progressive orbital process on the contralateral side several years later that resulted in compressive optic neuropathy
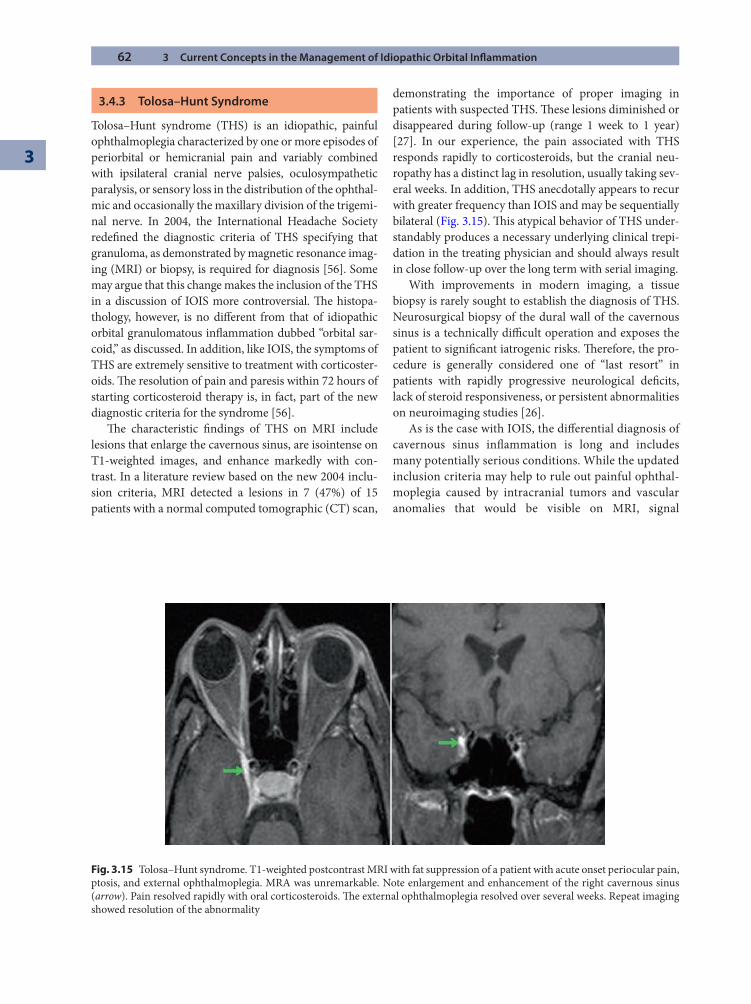
62 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
3.4.3 Tolosa–Hunt Syndrome
Tolosa–Hunt syndrome (THS) is an idiopathic, painful ophthalmoplegia characterized by one or more episodes of periorbital or hemicranial pain and variably combined with ipsilateral cranial nerve palsies, oculosympathetic paralysis, or sensory loss in the distribution of the ophthal-mic and occasionally the maxillary division of the trigemi-nal nerve. In 2004, the International Headache Society redefi ned the diagnostic criteria of THS specifying that granuloma, as demonstrated by magnetic resonance imag-ing (MRI) or biopsy, is required for diagnosis [56]. Some may argue that this change makes the inclusion of the THS in a discussion of IOIS more controversial. Th e histopa-thology, however, is no diff erent from that of idiopathic orbital granulomatous infl ammation dubbed “orbital sar-coid,” as discussed. In addition, like IOIS, the symptoms of THS are extremely sensitive to treatment with corticoster-oids. Th e resolution of pain and paresis within 72 hours of starting corticosteroid therapy is, in fact, part of the new diagnostic criteria for the syndrome [56].
Th e characteristic fi ndings of THS on MRI include lesions that enlarge the cavernous sinus, are isointense on T1-weighted images, and enhance markedly with con-trast. In a literature review based on the new 2004 inclu-sion criteria, MRI detected a lesions in 7 (47%) of 15 patients with a normal computed tomographic (CT) scan,
demonstrating the importance of proper imaging in patients with suspected THS. Th ese lesions diminished or disappeared during follow-up (range 1 week to 1 year) [27]. In our experience, the pain associated with THS responds rapidly to corticosteroids, but the cranial neu-ropathy has a distinct lag in resolution, usually taking sev-eral weeks. In addition, THS anecdotally appears to recur with greater frequency than IOIS and may be sequentially bilateral (Fig. 3.15). Th is atypical behavior of THS under-standably produces a necessary underlying clinical trepi-dation in the treating physician and should always result in close follow-up over the long term with serial imaging.
With improvements in modern imaging, a tissue biopsy is rarely sought to establish the diagnosis of THS. Neurosurgical biopsy of the dural wall of the cavernous sinus is a technically diffi cult operation and exposes the patient to signifi cant iatrogenic risks. Th erefore, the pro-cedure is generally considered one of “last resort” in patients with rapidly progressive neurological defi cits, lack of steroid responsiveness, or persistent abnormalities on neuroimaging studies [26].
As is the case with IOIS, the diff erential diagnosis of cavernous sinus infl ammation is long and includes many potentially serious conditions. While the updated inclusion criteria may help to rule out painful ophthal-moplegia caused by intracranial tumors and vascular anomalies that would be visible on MRI, signal
Fig. 3.15 Tolosa–Hunt syndrome. T1-weighted postcontrast MRI with fat suppression of a patient with acute onset periocular pain, ptosis, and external ophthalmoplegia. MRA was unremarkable. Note enlargement and enhancement of the right cavernous sinus (arrow). Pain resolved rapidly with oral corticosteroids. Th e external ophthalmoplegia resolved over several weeks. Repeat imaging showed resolution of the abnormality
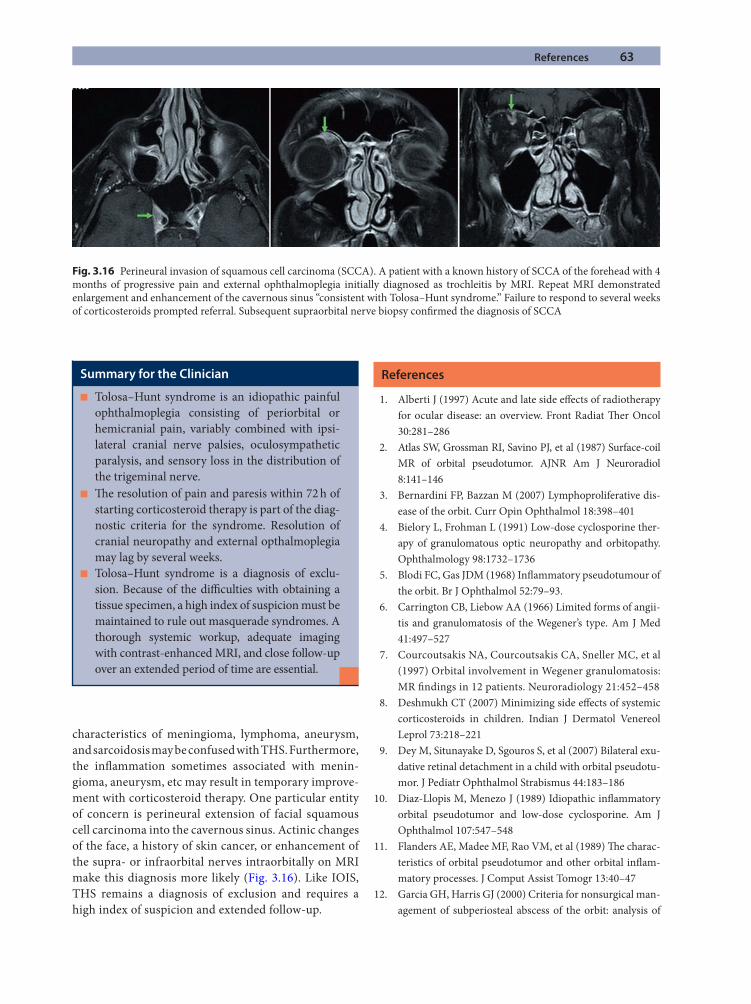
References 63
characteristics of meningioma, lymphoma, aneurysm, and sarcoidosis may be confused with THS. Furthermore, the infl ammation sometimes associated with menin-gioma, aneurysm, etc may result in temporary improve-ment with corticosteroid therapy. One particular entity of concern is perineural extension of facial squamous cell carcinoma into the cavernous sinus. Actinic changes of the face, a history of skin cancer, or enhancement of the supra- or infraorbital nerves intraorbitally on MRI make this diagnosis more likely (Fig. 3.16). Like IOIS, THS remains a diagnosis of exclusion and requires a high index of suspicion and extended follow-up.
References
1. Alberti J (1997) Acute and late side eff ects of radiotherapy for ocular disease: an overview. Front Radiat Th er Oncol 30:281–286
2. Atlas SW, Grossman RI, Savino PJ, et al (1987) Surface-coil MR of orbital pseudotumor. AJNR Am J Neuroradiol 8:141–146
3. Bernardini FP, Bazzan M (2007) Lymphoproliferative dis-ease of the orbit. Curr Opin Ophthalmol 18:398–401
4. Bielory L, Frohman L (1991) Low-dose cyclosporine ther-apy of granulomatous optic neuropathy and orbitopathy. Ophthalmology 98:1732–1736
5. Blodi FC, Gas JDM (1968) Infl ammatory pseudotumour of the orbit. Br J Ophthalmol 52:79–93.
6. Carrington CB, Liebow AA (1966) Limited forms of angii-tis and granulomatosis of the Wegener’s type. Am J Med 41:497–527
7. Courcoutsakis NA, Courcoutsakis CA, Sneller MC, et al (1997) Orbital involvement in Wegener granulomatosis: MR fi ndings in 12 patients. Neuroradiology 21:452–458
8. Deshmukh CT (2007) Minimizing side eff ects of systemic corticosteroids in children. Indian J Dermatol Venereol Leprol 73:218–221
9. Dey M, Situnayake D, Sgouros S, et al (2007) Bilateral exu-dative retinal detachment in a child with orbital pseudotu-mor. J Pediatr Ophthalmol Strabismus 44:183–186
10. Diaz-Llopis M, Menezo J (1989) Idiopathic infl ammatory orbital pseudotumor and low-dose cyclosporine. Am J Ophthalmol 107:547–548
11. Flanders AE, Madee MF, Rao VM, et al (1989) Th e charac-teristics of orbital pseudotumor and other orbital infl am-matory processes. J Comput Assist Tomogr 13:40–47
12. Garcia GH, Harris GJ (2000) Criteria for nonsurgical man-agement of subperiosteal abscess of the orbit: analysis of
Summary for the Clinician
Tolosa–Hunt syndrome is an idiopathic painful ■
ophthalmoplegia consisting of periorbital or hemicranial pain, variably combined with ipsi-lateral cranial nerve palsies, oculosympathetic paralysis, and sensory loss in the distribution of the trigeminal nerve.Th e resolution of pain and paresis within 72 h of ■
starting corticosteroid therapy is part of the diag-nostic criteria for the syndrome. Resolution of cranial neuropathy and external opthalmoplegia may lag by several weeks.Tolosa–Hunt syndrome is a diagnosis of exclu- ■
sion. Because of the diffi culties with obtaining a tissue specimen, a high index of suspicion must be maintained to rule out masquerade syndromes. A thorough systemic workup, adequate imaging with contrast-enhanced MRI, and close follow-up over an extended period of time are essential.
Fig. 3.16 Perineural invasion of squamous cell carcinoma (SCCA). A patient with a known history of SCCA of the forehead with 4 months of progressive pain and external ophthalmoplegia initially diagnosed as trochleitis by MRI. Repeat MRI demonstrated enlargement and enhancement of the cavernous sinus “consistent with Tolosa–Hunt syndrome.” Failure to respond to several weeks of corticosteroids prompted referral. Subsequent supraorbital nerve biopsy confi rmed the diagnosis of SCCA
64 3 Current Concepts in the Management of Idiopathic Orbital Infl ammation
3
outcomes 1988–1998. Ophthalmology 107:1454–1456; discussion 1457–1458
13. Garrity JA, Coleman AW, Matteson EL, et al (2004) Treatment of recalcitrant idiopathic orbital infl ammation (chronic orbital myositis) with infl iximab. Am J Ophthalmol 138:925–930
14. Goldberg RA, Rootman J (1990) Clinical characteristics of metastatic orbital tumors. Ophthalmology 97:620–624
15. Goldberg RA, McCann JD, Shorr N (2004) Idiopathic orbital infl ammatory disease. Arch Ophthalmol 122:1092–1093
16. Gunalp I, Gunduz K (1995) Metastatic orbital tumors. Jpn J Ophthalmol 39:65–70
17. Gunalp I, Gunduz K, Yazar Z (1996) Idiopathic orbital infl ammatory disease. Acta Ophthalmol Scan 74:191–193
18. Harris G (2006) Idiopathic orbital infl ammation: a patho-genetic construct and treatment strategy. Ophthalmol Plast Reconstr Surg 22:79–86
19. Hatton MP, Rubin PA, Foster CS (2005) Successful treat-ment of idiopathic orbital infl ammation with mycopheno-late mofetil. Am J Ophthalmol 140:916–918
20. Hosten N, Sander B, Cordes M, et al (1989) Graves ophthal-mopathy: MR imaging of the orbits. Radiology 172:759–762
21. Hsuan JD, Selva D, McNab AA, et al (2006) Idiopathic scleros-ing orbital infl ammation. Arch Ophthalmol 124:1244–1250
22. Hughes, IA (1987) Steroids and growth [Editorial]. BMJ (Clin Res Ed) 295:683–684
23. Johns CJ, Michele TM (1999) Th e clinical management of sarcoidosis: a 50-year experience at the Johns Hopkins Hospital. Medicine 78:65–111
24. Johnston A, Gudjonsson JE, Sigmundsdottir H, et al (2005) Th e anti-infl ammatory action of methotrexate is not mediated by lymphocyte apoptosis, but by the suppression of activation and adhesion molecules. Clin Immunol 114:154–163
25. Kapadia MK, Rubin PA (2006) Th e emerging use of TNF-alpha inhibitors in orbital infl ammatory disease. Int Ophthalmol Clin 46:165–181
26. Kline LB, Hoyt WF (2001) Nosological entities?: Th e Tolosa–Hunt syndrome. J Neurol Neurosurg Psychiatry 71:577–582
27. La Mantia L, Curone M, Rapoport AM, et al (2006) Tolosa–Hunt syndrome: critical literature review based on IHS 2004 criteria. Cephalalgia 26:772–781
28. Leavitt RY, Fauci AS, Bloch DA, et al (1990) Th e American College of Rheumatology 1990 criteria for the classifi cation of Wegener’s granulomatosis. Arthritis Rheum 33:1101–1107
29. Leone CR Jr, Lloyd WC III (1985) Treatment protocol for orbital infl ammatory disease. Ophthalmology 92:1325–1333
30. Mauriello J (1994) Acute infl ammation of the orbit. In: Margo C, Hamed L, Mames R (eds) Diagnostic problems in clinical ophthalmology. Saunders, Philadelphia
31. McCarthy JM, White VA, Harris G, et al (1993) Idiopathic sclerosing infl ammation of the orbit: immunohistologic analysis and comparison with retroperitoneal fi brosis. Mod Pathol 6:581–587
32. Miquel T, Abad S, Badelon I, et al (2008) Successful treat-ment of idiopathic orbital infl ammation with infl iximab: an alternative to conventional steroid-sparing agents. Ophthal Plast Reconstr Surg 24:415–417
33. Mombaerts I, Koornneef L (1997) Current status in the treatment of orbital myositis. Ophthalmology 104: 402–408
34. Mombaerts I, Schlingemann RO, Goldschmeding R, et al (1996) Are systemic corticosteroids useful in the management of orbital pseudotumors? Ophthalmology 103:521–528
35. Mombaerts I, Schlingemann RO, Goldschmeding R, et al (1996) Idiopathic granulomatous orbital infl ammation. Ophthalmology 103:2135–2141
36. Mottow L, Jakobiec F, Smith M (1978) Idiopathic infl am-matory orbital pseudotumor in early childhood I: Clinical characteristics. Arch Ophthalmol 96:1410–1417
37. Murphy CC, Ayliffe WH, Booth A, et al (2004) Tumor necrosis factor alpha blockade with infliximab for refractory uveitis and scleritis. Ophthalmology 111: 352–356
38. Niehues T, Lankisch P (2006) Recommendations for the use of methotrexate in juvenile idiopathic arthritis. Pediatr Drugs 8:347–356
39. Nugent RA, Belkin RI, Neigel JM, et al (1990) Graves orbi-topathy: correlation of CT and clinical fi ndings. Radiology 177:675–682
40. Orcutt J, Garner A, Henk J, et al (1983) Treatment of idio-pathic infl ammatory orbital pseudotumors by radiother-apy. Br J Ophthalmol 67:570–574
41. Paridaens D, van den Bosch WA, van der Loos TL, et al (2005) Th e eff ect of etanercept on Graves’ ophthalmopa-thy: a pilot study. Eye 19:1286–1289
42. Perry SR, Rootman J, White VA (1991) Th e clinical and pathologic constellation of Wegener granulomatosis of the orbit. Ophthalmology 104:683–1694
43. Prabhakaran VC, Saeed P, Esmaeli B, et al (2007) Orbital and adnexal sarcoidosis. Arch Ophthalmol 125:1657–1662
44. Prendiville C, O’Doherty M, Moriarty P, et al (2008) Th e use of infl iximab in ocular infl ammation. Br J Ophthalmol 92:823–825
45. Reinhold-Keller E, Beuge N, Latza U, et al (2000) An inter-disciplinary approach to the care of patients with Wegener’s granulomatosis. Long-term outcome in 155 patients. Arthritis Rheum 43:1021–1032
45. Rootman J, Nugent R (1982) Th e classifi cation and man-agement of acute orbital pseudotumors. Ophthalmology 89:1040–1048
47. Rootman J, Chang W, Jones D (2003) Distribution and dif-ferential diagnosis of orbital disease. In: Rootman J (ed) Diseases of the orbit: a multidisciplinary approach, 2nd ed. Lippincott Williams & Wilkins, Philadelphia
48. Rootman J, McCarthy M, White V, et al (1994) Idiopathic sclerosing infl ammation of the orbit: a distinct clinico-pathologic entity. Ophthalmology 101:570–584

References 65
49. Rose GE (2007) A personal view: probability in medicine, levels of (un)certainty, and the diagnosis of orbital disease (with particular reference to orbital “pseudotumor”). Arch Ophthalmol 125:1171–1172
50. Sanchez-Roman J, Varela-Aguilar JM, Bravo-Ferrer J, et al (1993) Idiopathic orbital myositis: treatment with cyclosporine. Ann Rheum Dis 52:84–85
51. Sergott R, Glaser J, Charyulu K (1981) Radiotherapy for idiopathic infl ammatory orbital pseudotumor: indications and results. Arch Ophthalmol 99:853–856
52. Shah SS, Lowder CY, Schmitt MA, et al (1992) Low-dose methotrexate therapy for ocular infl ammatory disease. Ophthalmology 99:1419–1423
53. Shields JA, Shields CL, Scartozzi R (2004) Survey of 1,264 patients with orbital tumors and simulating lesions: the 2002 Montgomery Lecture, part 1. Ophthalmology 111: 997–1008
54. Smith J (2002) Management of uveitis in pediatric patients: special considerations. Pediatr Drugs 4:183–189
55. Smith JR, Rosenbaum JT (2001) A role for methotrexate in the management of non-infectious orbital infl ammatory disease. Br J Ophthalmol 85:1220–1224
56. Th e International Classifi cation of Headache Disorders ICHD-II (2004) Cephalalgia 24(Suppl 1):131
57. Weber AL, Jakobiec FA, Sabates NR (1996) Pseudotumor of the orbit. Neuroimaging Clin North Am 6:73–91
58. Woo TL, Francis IC, Wilcsek GA, et al (2001) Australasian orbital and adnexal Wegener’s granulomatosis. Ophthal-mology 108:1535–1543
59. Yan J, Wu Z, Li Y (2004) Th e diff erentiation of idiopathic infl ammatory pseudotumor from lymphoid tumors of orbit: analysis of 319 cases. Orbit 23:245–254
60. Yuen SJ, Rubin PA (2003) Idiopathic orbital infl ammation: distributions, clinical features and treatment outcome. Arch Ophthalmol 121:491–499
61. Zakir R, Manners RM, Ellison D, et al (2000) Idiopathic sclerosing infl ammation of the orbit: a new fi nding of cal-cifi cation. Br J Ophthalmol 84:1322–1324
Lacrimal Canalicular Infl ammation and Occlusion: Diagnosis and ManagementDavid H. Verity and Geoff rey E. Rose
Chapter 4
4.1 Introduction
Canaliculitis, either epithelial or pericanalicular infl am-mation, has many underlying causes with rather charac-teristic clinical patterns. Although certain etiologies, such as herpetic canaliculitis, are rapidly progressive, others are insidious and frequently pass unrecognized until the onset of lacrimal symptoms. Infl ammation, either within the epithelium or deep to its basement membrane, leads to scarring with a reduction of both longitudinal compliance and cross-sectional area of the aff ected canaliculus; these changes result in impaired function of both the active pumping mechanism and the static drainage (Table 4.1).
Th is review considers idiopathic, infective, and iatro-genic causes of canalicular infl ammation and obstruc-tion, but canalicular trauma—comprehensively reviewed elsewhere—is excluded [24, 27].
4.2 Embryology, Anatomy, Physiology, and Pathophysiology of the Canalicular System
Th e lacrimal drainage pathway arises, at day 32, from a thickening of the ectoderm in the naso-optic fi ssure. Th is ectoderm descends into the surrounding mesoderm and forms a cord that extends from the developing eyelids to the nasal space, the cord subsequently forming a lumen by disintegration of the central ectoderm.
Th e lacrimal puncta, ampullae, and canaliculi form the proximal, high-resistance, elements of the lacrimal drainage system: Measuring 0.3 mm in diameter, the puncta lie within the lacrimal papillae and drain into the vertical ampullae, each being 1–2 mm in length and 2.5 mm in width. Th e horizontal canaliculi are about 6 mm long in the upper lid and 8 mm in the lower, have an internal diameter of about 0.4 mm, and are surrounded
4
Core Messages
Canalicular infl ammation may lead to loss of ■
compliance and stenosis, with lacrimal symptoms occurring despite anatomical patency.Microbial canaliculitis is frequently overlooked, ■
leading to a delay in diagnosis and management.Failure adequately to remove canalicular stones and ■
debris is a common cause for persistent canaliculitis.Canalicular ■ epithelial infl ammation due to pri-mary herpes simplex infection is a common cause of canalicular, or common canalicular, occlusion.Subepithelial ■ canalicular infl ammation—as seen with lichen planus (LP)—may lead to a more severe and extensive annular fi brosis and carries a poor prognosis.Systemic chemotherapeutic agents, including ■
radioiodine, 5-fl uorouracil (5-FU), mitomycin C (MMC), and docetaxel, may injure the canalicu-lar epithelium, the evidence suggesting active concentration of these agents by the lacrimal out-fl ow structures.
Th e surgical approach to canalicular occlusion ■
depends on the extent of disease.Dacryocystorhinostomy (DCR) with retrograde ■
canaliculostomy is the preferred surgery for prox-imal and midcanalicular occlusion.Th e indication for ■ primary placement of a Jones canalicular bypass tube is the total absence of all distal canalicular and common canalicular struc-tures, with this ascertained during open lacrimal surgery.Th e indication for ■ secondary Jones tube place-ment is a functional failure aft er primary DCR with retrograde canaliculostomy.A canalicular bypass tube should be sutured such ■
that the tube fl ange is held clear of the healing carunculectomy site; the function is not to pre-vent prolapse of the tube. As such, an encirclage suture is required only during primary placement of a bypass tube, when carunculectomy has just been performed.
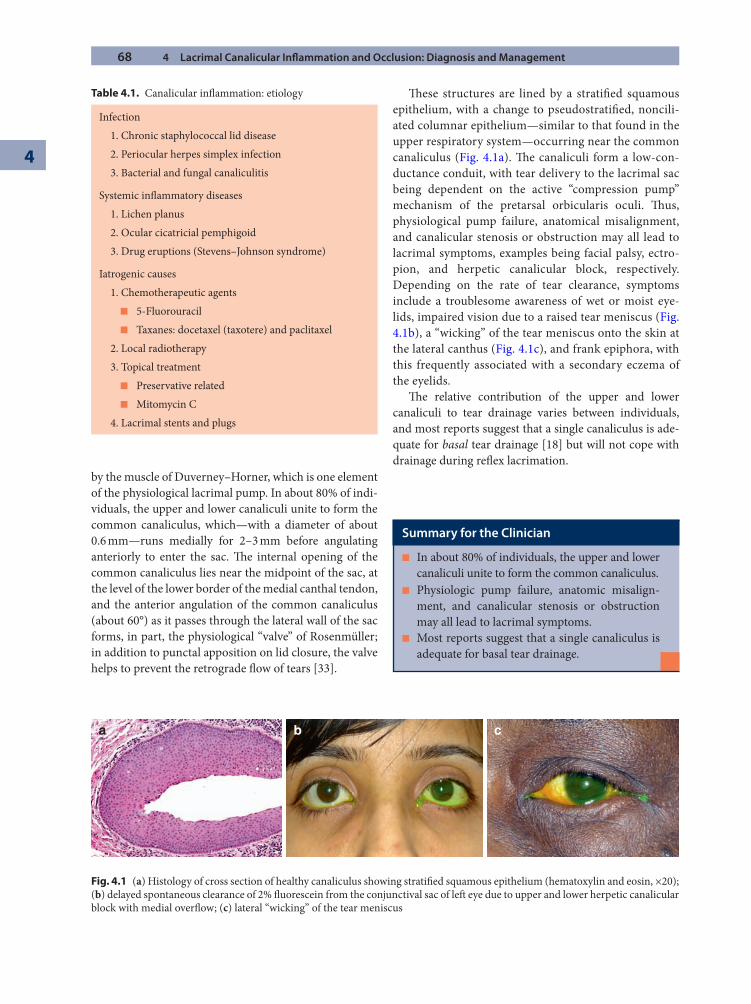
68 4 Lacrimal Canalicular Infl ammation and Occlusion: Diagnosis and Management
4
by the muscle of Duverney–Horner, which is one element of the physiological lacrimal pump. In about 80% of indi-viduals, the upper and lower canaliculi unite to form the common canaliculus, which—with a diameter of about 0.6 mm—runs medially for 2–3 mm before angulating anteriorly to enter the sac. Th e internal opening of the common canaliculus lies near the midpoint of the sac, at the level of the lower border of the medial canthal tendon, and the anterior angulation of the common canaliculus (about 60°) as it passes through the lateral wall of the sac forms, in part, the physiological “valve” of Rosenmüller; in addition to punctal apposition on lid closure, the valve helps to prevent the retrograde fl ow of tears [33].
Th ese structures are lined by a stratifi ed squamous epithelium, with a change to pseudostratifi ed, noncili-ated columnar epithelium—similar to that found in the upper respiratory system—occurring near the common canaliculus (Fig. 4.1a). Th e canaliculi form a low-con-ductance conduit, with tear delivery to the lacrimal sac being dependent on the active “compression pump” mechanism of the pretarsal orbicularis oculi. Th us, physiological pump failure, anatomical misalignment, and canalicular stenosis or obstruction may all lead to lacrimal symptoms, examples being facial palsy, ectro-pion, and herpetic canalicular block, respectively. Depending on the rate of tear clearance, symptoms include a troublesome awareness of wet or moist eye-lids, impaired vision due to a raised tear meniscus (Fig. 4.1b), a “wicking” of the tear meniscus onto the skin at the lateral canthus (Fig. 4.1c), and frank epiphora, with this frequently associated with a secondary eczema of the eyelids.
Th e relative contribution of the upper and lower canaliculi to tear drainage varies between individuals, and most reports suggest that a single canaliculus is ade-quate for basal tear drainage [18] but will not cope with drainage during refl ex lacrimation.
Summary for the Clinician
In about 80% of individuals, the upper and lower ■
canaliculi unite to form the common canaliculus.Physiologic pump failure, anatomic misalign- ■
ment, and canalicular stenosis or obstruction may all lead to lacrimal symptoms.Most reports suggest that a single canaliculus is ■
adequate for basal tear drainage.
Table 4.1. Canalicular infl ammation: etiology
Infection 1. Chronic staphylococcal lid disease 2. Periocular herpes simplex infection 3. Bacterial and fungal canaliculitis
Systemic infl ammatory diseases 1. Lichen planus 2. Ocular cicatricial pemphigoid 3. Drug eruptions (Stevens–Johnson syndrome)
Iatrogenic causes 1. Chemotherapeutic agents
5-Fluorouracil ■
Taxanes: docetaxel (taxotere) and paclitaxel ■
2. Local radiotherapy 3. Topical treatment
Preservative related ■
Mitomycin C ■
4. Lacrimal stents and plugs
Fig. 4.1 (a) Histology of cross section of healthy canaliculus showing stratifi ed squamous epithelium (hematoxylin and eosin, ×20); (b) delayed spontaneous clearance of 2% fl uorescein from the conjunctival sac of left eye due to upper and lower herpetic canalicular block with medial overfl ow; (c) lateral “wicking” of the tear meniscus
a b c
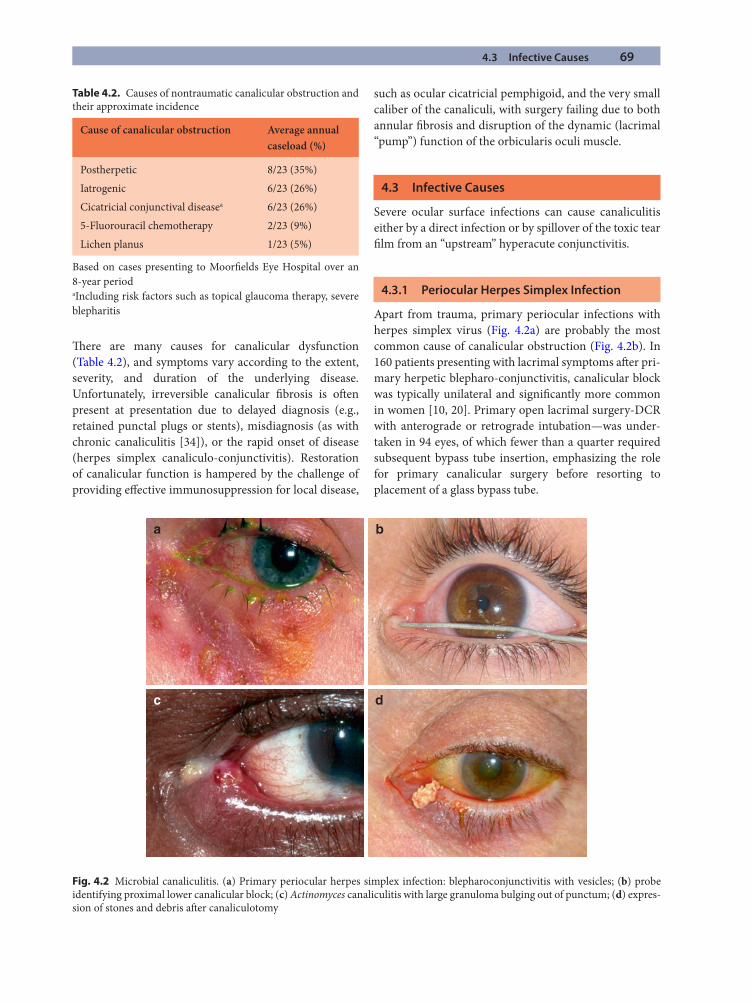
4.3 Infective Causes 69
Th ere are many causes for canalicular dysfunction (Table 4.2), and symptoms vary according to the extent, severity, and duration of the underlying disease. Unfortunately, irreversible canalicular fi brosis is oft en present at presentation due to delayed diagnosis (e.g., retained punctal plugs or stents), misdiagnosis (as with chronic canaliculitis [34]), or the rapid onset of disease (herpes simplex canaliculo-conjunctivitis). Restoration of canalicular function is hampered by the challenge of providing eff ective immunosuppression for local disease,
such as ocular cicatricial pemphigoid, and the very small caliber of the canaliculi, with surgery failing due to both annular fi brosis and disruption of the dynamic (lacrimal “pump”) function of the orbicularis oculi muscle.
4.3 Infective Causes
Severe ocular surface infections can cause canaliculitis either by a direct infection or by spillover of the toxic tear fi lm from an “upstream” hyperacute conjunctivitis.
4.3.1 Periocular Herpes Simplex Infection
Apart from trauma, primary periocular infections with herpes simplex virus (Fig. 4.2a) are probably the most common cause of canalicular obstruction (Fig. 4.2b). In 160 patients presenting with lacrimal symptoms aft er pri-mary herpetic blepharo-conjunctivitis, canalicular block was typically unilateral and signifi cantly more common in women [10, 20]. Primary open lacrimal surgery-DCR with anterograde or retrograde intubation—was under-taken in 94 eyes, of which fewer than a quarter required subsequent bypass tube insertion, emphasizing the role for primary canalicular surgery before resorting to placement of a glass bypass tube.
Table 4.2. Causes of nontraumatic canalicular obstruction and their approximate incidence
Cause of canalicular obstruction Average annual caseload (%)
Postherpetic 8/23 (35%)Iatrogenic 6/23 (26%)Cicatricial conjunctival diseasea 6/23 (26%)5-Fluorouracil chemotherapy 2/23 (9%)Lichen planus 1/23 (5%)
Based on cases presenting to Moorfi elds Eye Hospital over an 8-year periodaIncluding risk factors such as topical glaucoma therapy, severe blepharitis
a b
c d
Fig. 4.2 Microbial canaliculitis. (a) Primary periocular herpes simplex infection: blepharoconjunctivitis with vesicles; (b) probe identifying proximal lower canalicular block; (c) Actinomyces canaliculitis with large granuloma bulging out of punctum; (d) expres-sion of stones and debris aft er canaliculotomy
70 4 Lacrimal Canalicular Infl ammation and Occlusion: Diagnosis and Management
4
4.3.2 Bacterial Canaliculitis
Numerous microbes may infect the canalicular epithelial surface (Table 4.3), but the most characteristic is due to Actinomyces species. Such patients usually present aft er many months of a painless chronic discharge at the medial canthus, this typically being misdiagnosed as conjunctivitis, chalazion, or nasolacrimal duct obstruction [1, 3]. Although rare, microbial canaliculitis may also lead to chronic or recurrent nasolacrimal obstruction in children [26], and may also be a cause of blood-stained tears. Typically, there is swelling with mild infl ammation, centered on the mid-canaliculus, and the characteristically stringy yellow dis-charge at a pouting punctum (Fig. 4.2c). Pressure over the canaliculus may lead to discharge of pus or gritlike “gran-ules,” but in most cases the debris is typically not expressible (unlike that of a lacrimal sac mucocele). Actinomyces, espe-cially A. israelii, is a cast-forming gram-positive fi lamentous anaerobe that can be diffi cult to isolate, and the organism has a propensity for colonizing hollow spaces and forming “stones,” such as canaliculiths (Fig. 4.2d).
In all but the mildest cases, Actinomyces canaliculitis is resistant to topical antibiotics alone. Antibiotic syringing of the aff ected canaliculus is well described [23], but this tends to be ineff ective [35] and, more importantly, carries the risk of microbial dissemination into the lacrimal sac and nasolacrimal duct. Defi nitive treatment entails canali-culostomy with expression of all infl ammatory and infec-tive debris; a 6-mm incision is made along the conjunctival border of the aff ected canaliculus, and the canalicular con-tents are expressed with fi rm pressure on either side of its walls. Although a large chalazion spoon may be used to curette stones, this instrument is best avoided as it is liable to damage the severely infl amed canalicular mucosa and result in canalicular occlusion. Chronic infection may lead
to gross distension of the canaliculus by the large number of stones, all of which require removal. Th e canaliculo-tomy incision heals spontaneously, and the patient should be placed on a week’s course of a topical antibiotic, such as ofl oxacin; because the incision lies along, rather than across, the canaliculus, ring contracture is rare and post-operative epiphora most unusual [1]. Recurrence of symp-toms is a likely indication of persistent canalicular stones, and a further canaliculotomy should be performed if nec-essary; occasionally, such recurrent infection is centered on the lacrimal sac rather than the canaliculi.
4.4 Systemic Infl ammatory Disease
4.4.1 Lichen Planus
Lichen planus (LP), an idiopathic autoimmune disease of the skin and oral or genital mucosa, may rarely aff ect con-junctiva [15, 28] and lead to severe canalicular obstruc-tion [10, 22]. Etiological mechanisms include autoreactive T cells to keratinocytes and activated tissue matrix metal-loproteinases and mast cells. Systemic lesions show sub- and intraepithelial lymphocytic infi ltration with degeneration of basal keratinocytes, and although con-junctival disease is less well characterized, case reports describe reticular subconjunctival scarring, forniceal shortening, and symblepharon formation. Th ese features resemble those seen in ocular cicatricial pemphigoid [21, 25], but immune complex deposition within the conjunc-tival basement membrane—pathognomonic for ocular cicatricial pemphigoid—is absent in LP.
Canalicular LP leads to extensive bilateral, bicanalic-ular occlusion in three quarters of patients with symp-tomatic disease [10]; these changes probably refl ect infl ammation within the subepithelial substantia propria of the canaliculus, with consequent deep fi brosis “throt-tling” the canaliculus (Fig. 4.3a). LP patients with proxi-mal or midcanalicular block are off ered DCR with retrograde canaliculostomy [36] but are warned of the high likelihood of requiring secondary placement of a Jones bypass tube.
4.4.2 Ocular Cicatricial Pemphigoid
Distal spillover of the severe conjunctival infl ammation of ocular cicatricial pemphigoid will oft en cause proximal canalicular blockage (Figs. 4.3c, d). Retention of infl am-matory debris will, in some cases, be associated with an exacerbation of ocular surface disease, and consideration will be given to the reestablishment of tear drainage; in
Table 4.3. Microbial isolates in canaliculitis
Actinomycetes spp.Arcanobacterium haemolyticumEikenella corrodensHaemophilus aphrophilusLactococcus lactis cremorisMolluscum contagiousuma
Mycobacterium chelonaeNocardia asteroidesPropionobacterium propionicumStaphylocococcus spp.
aPrimary involvement of the conjunctiva or cornea by mollus-cum is rare and is oft en associated with HIV infection
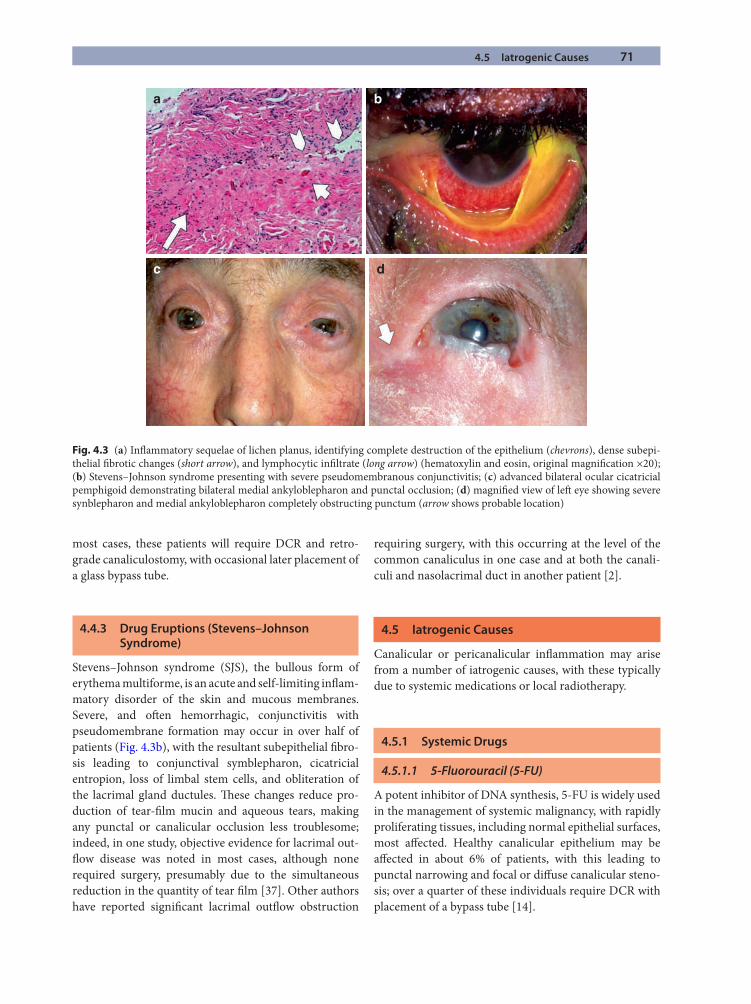
4.5 Iatrogenic Causes 71
a
d
b
c
Fig. 4.3 (a) Infl ammatory sequelae of lichen planus, identifying complete destruction of the epithelium (chevrons), dense subepi-thelial fi brotic changes (short arrow), and lymphocytic infi ltrate (long arrow) (hematoxylin and eosin, original magnifi cation ×20); (b) Stevens–Johnson syndrome presenting with severe pseudomembranous conjunctivitis; (c) advanced bilateral ocular cicatricial pemphigoid demonstrating bilateral medial ankyloblepharon and punctal occlusion; (d) magnifi ed view of left eye showing severe synblepharon and medial ankyloblepharon completely obstructing punctum (arrow shows probable location)
most cases, these patients will require DCR and retro-grade canaliculostomy, with occasional later placement of a glass bypass tube.
4.4.3 Drug Eruptions (Stevens–Johnson Syndrome)
Stevens–Johnson syndrome (SJS), the bullous form of erythema multiforme, is an acute and self-limiting infl am-matory disorder of the skin and mucous membranes. Severe, and oft en hemorrhagic, conjunctivitis with pseudomembrane formation may occur in over half of patients (Fig. 4.3b), with the resultant subepithelial fi bro-sis leading to conjunctival symblepharon, cicatricial entropion, loss of limbal stem cells, and obliteration of the lacrimal gland ductules. Th ese changes reduce pro-duction of tear-fi lm mucin and aqueous tears, making any punctal or canalicular occlusion less troublesome; indeed, in one study, objective evidence for lacrimal out-fl ow disease was noted in most cases, although none required surgery, presumably due to the simultaneous reduction in the quantity of tear fi lm [37]. Other authors have reported signifi cant lacrimal outfl ow obstruction
requiring surgery, with this occurring at the level of the common canaliculus in one case and at both the canali-culi and nasolacrimal duct in another patient [2].
4.5 Iatrogenic Causes
Canalicular or pericanalicular infl ammation may arise from a number of iatrogenic causes, with these typically due to systemic medications or local radiotherapy.
4.5.1 Systemic Drugs
4.5.1.1 5-Fluorouracil (5-FU)
A potent inhibitor of DNA synthesis, 5-FU is widely used in the management of systemic malignancy, with rapidly proliferating tissues, including normal epithelial surfaces, most aff ected. Healthy canalicular epithelium may be aff ected in about 6% of patients, with this leading to punctal narrowing and focal or diff use canalicular steno-sis; over a quarter of these individuals require DCR with placement of a bypass tube [14].
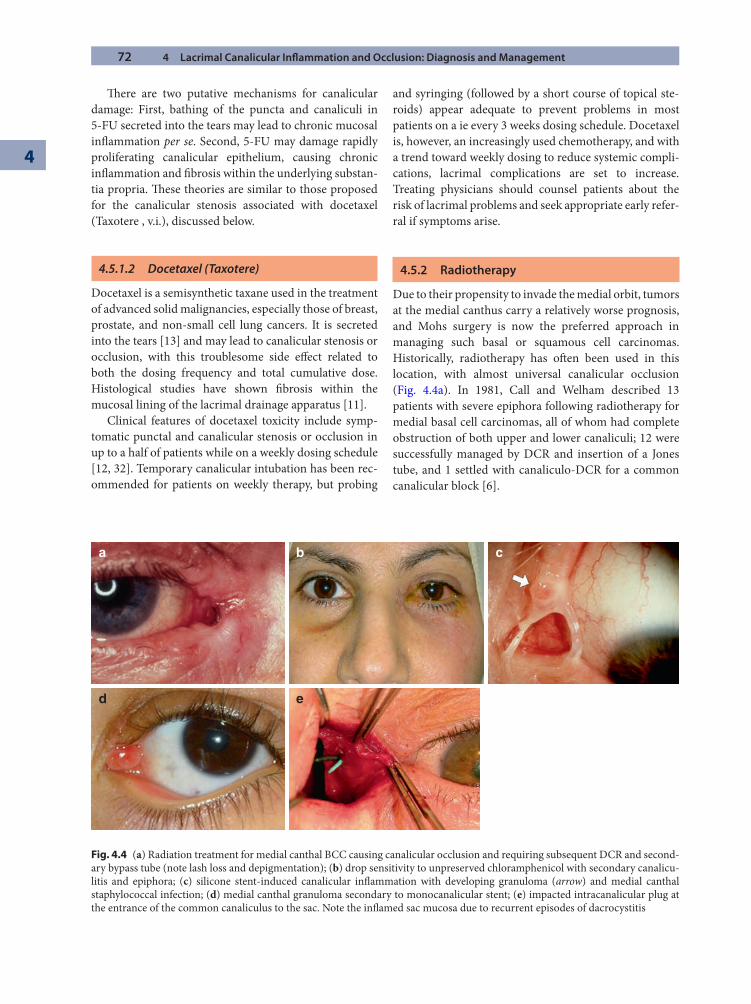
72 4 Lacrimal Canalicular Infl ammation and Occlusion: Diagnosis and Management
4
Th ere are two putative mechanisms for canalicular damage: First, bathing of the puncta and canaliculi in 5-FU secreted into the tears may lead to chronic mucosal infl ammation per se. Second, 5-FU may damage rapidly proliferating canalicular epithelium, causing chronic infl ammation and fi brosis within the underlying substan-tia propria. Th ese theories are similar to those proposed for the canalicular stenosis associated with docetaxel (Taxotere , v.i.), discussed below.
4.5.1.2 Docetaxel (Taxotere)
Docetaxel is a semisynthetic taxane used in the treatment of advanced solid malignancies, especially those of breast, prostate, and non-small cell lung cancers. It is secreted into the tears [13] and may lead to canalicular stenosis or occlusion, with this troublesome side eff ect related to both the dosing frequency and total cumulative dose. Histological studies have shown fi brosis within the mucosal lining of the lacrimal drainage apparatus [11].
Clinical features of docetaxel toxicity include symp-tomatic punctal and canalicular stenosis or occlusion in up to a half of patients while on a weekly dosing schedule [12, 32]. Temporary canalicular intubation has been rec-ommended for patients on weekly therapy, but probing
and syringing (followed by a short course of topical ste-roids) appear adequate to prevent problems in most patients on a ie every 3 weeks dosing schedule. Docetaxel is, however, an increasingly used chemotherapy, and with a trend toward weekly dosing to reduce systemic compli-cations, lacrimal complications are set to increase. Treating physicians should counsel patients about the risk of lacrimal problems and seek appropriate early refer-ral if symptoms arise.
4.5.2 Radiotherapy
Due to their propensity to invade the medial orbit, tumors at the medial canthus carry a relatively worse prognosis, and Mohs surgery is now the preferred approach in managing such basal or squamous cell carcinomas. Historically, radiotherapy has oft en been used in this location, with almost universal canalicular occlusion (Fig. 4.4a). In 1981, Call and Welham described 13 patients with severe epiphora following radiotherapy for medial basal cell carcinomas, all of whom had complete obstruction of both upper and lower canaliculi; 12 were successfully managed by DCR and insertion of a Jones tube, and 1 settled with canaliculo-DCR for a common canalicular block [6].
a
d e
b c
Fig. 4.4 (a) Radiation treatment for medial canthal BCC causing canalicular occlusion and requiring subsequent DCR and second-ary bypass tube (note lash loss and depigmentation); (b) drop sensitivity to unpreserved chloramphenicol with secondary canalicu-litis and epiphora; (c) silicone stent-induced canalicular infl ammation with developing granuloma (arrow) and medial canthal staphylococcal infection; (d) medial canthal granuloma secondary to monocanalicular stent; (e) impacted intracanalicular plug at the entrance of the common canaliculus to the sac. Note the infl amed sac mucosa due to recurrent episodes of dacrocystitis
4.5 Iatrogenic Causes 73
Systemic radioiodine (131I) is used for the manage-ment of thyroid carcinoma and has well-documented ocular side eff ects, including xerophthalmia and chronic conjunctivitis [31]. Symptomatic lacrimal outfl ow obstruction is less well recognized, occurring in at least 5% of patients, with the distal nasolacrimal duct more commonly aff ected than the canalicular systems [5]1; whether this eff ect is mediated by local toxicity from passive fl ow of 131I into the tears or is due to active uptake by the sodium–iodide symporter (known to exist in both lacrimal and thyroid gland) remains uncer-tain, although at least one report supported the latter mechanism [4].
4.5.3 Topical Ophthalmic Treatments
4.5.3.1 Preservative-Related Chronic Conjunctivitis
Lacrimal canalicular occlusion may occur aft er exposure to topical ocular medications, with one study reporting obstruction as little as a month aft er beginning treatment [21]. Outfl ow obstruction is most commonly observed 2–5 mm from the lacrimal punctum, with other associ-ated fi ndings including symblepharon, keratinization of the medial canthal tissues, and cicatricial medial entropion.
Canalicular occlusion may follow a chronic infl amma-tory response to drop preservatives and, if a patient has symptoms of dry eye, features suggestive of chronic allergy (e.g., skin changes, ocular redness or irritation, and a conjunctival papillary response) (Fig. 4.4b) should not be confused with those of aqueous insuffi ciency.
4.5.3.2 Mitomycin C (MMC) Therapy
Topical MMC is proven in the treatment of ocular sur-face malignancy, such as intraepithelial carcinoma, pri-mary acquired melanosis with atypia, superfi cial conjunctival malignant melanoma, and sebaceous carci-noma with pagetoid spread. Transient side eff ects of MMC include an allergic reaction in a third of patients in addition to kerato-conjunctivitis and punctate epithelial keratopathy.
Canalicular disease has been reported in 3/14 (21%) patients receiving topical MMC for 2 weeks [16], although another report found punctal stenosis in only 14/100 eyes of 91 patients who received the drop for 1 week (of which only 1 required lacrimal surgery), sug-gesting that symptomatic canalicular stenosis occurs only rarely and may be related to duration of topical therapy [17]. To reduce canalicular toxicity, some authors advocate temporary punctal occlusion with removable plugs while using MMC drops, which has the additional advantages of increasing drug bioavailability on the ocu-lar surface.
4.5.4 Lacrimal Stents and Plugs
All foreign bodies within the lacrimal outfl ow tract, including stones, stents, and plugs, incite a mucosal infl ammatory response. At about a month aft er lacrimal surgery, silicone stents typically cause medial canthal irri-tation and mucus production due to punctal and canalic-ular infl ammatory changes; when stent removal is delayed beyond 3 months, frank exophytic granulomas may occur (Fig. 4.4c, d). Th us, even the most inert of materials is capable of inciting mucosal infl ammation, with second-ary submucosal fi brosis and risk of canalicular stricture.
Although the vast majority of lacrimal plugs are not used appropriately, a variety of punctal and canalicular plugs are available to treat symptoms of true aqueous insuffi ciency. Self-degrading collagen plugs are eff ective for a few weeks, and silicone punctal plugs, which are rea-sonably well tolerated, are best used to identify those patients in whom permanent outfl ow occlusion would be appropriate. Other materials include a fl exible thermo-sensitive acrylic material (SmartPlug) that molds to the internal contour of the ampullae, but none is without complication, and all may cause canaliculitis [8, 9, 29, 30]. Intracanalicular plugs have been advocated for the treat-ment of dry eye for some years, but these tend to migrate into the nasolacrimal sac, be held up at the entrance to the sac (Fig. 4.4e), or become embedded through the com-mon canalicular wall. Th e presence of a chronic intrac-analicular foreign body can fuel a gross conjunctival infl ammatory response, and the retrograde discharge of purulent debris further compromises the ocular surface. Indeed, intracanalicular plugs were the cause of lacrimal outfl ow symptoms in 6% of eyes in one series, with the high prevalence possibly refl ecting practice within one particular catchment population [19]; over a quarter of eyes in this study had persistent epiphora aft er plug removal or reparative lacrimal surgery, presumably due to persistent canalicular stenosis.
1 A lower dose 131I is used in controlling hyperthyroidism (ther-apeutic activity 10–15 mCi 131I) compared to managing thyroid carcinoma (30–200 mCi 131I), which in the context of metastatic disease may require substantial cumulative activities (up to 300 mCi 131I).

74 4 Lacrimal Canalicular Infl ammation and Occlusion: Diagnosis and Management
4
4.6 The Surgical Approach to Managing Canalicular Disease
A micropunctoplasty, such as the three-snip procedure, is useful if punctal stenosis is present with a patent canalic-ulus and nasolacrimal duct or extreme punctal stenosis prevents canalicular assessment. Th e purpose is to remove the posterior wall of both the punctal ampulla and 1–2 mm proximal canaliculus, although recent evidence suggests that removal of the posterior ampullary wall alone, without disruption of the canaliculus, may be pref-erable [7].
In performing a standard punctoplasty, a punctum seeker may be required fi rst to identify and enter the lac-rimal punctum, which may then be further dilated with the wider-tipped Nettleship dilator. Th ree incisions are then made with either a pair of fi ne Westcott or Vannas scissors; a vertical incision is made through the most pos-terolateral part of the punctum and ampulla, a second along the avascular superior margin of the canaliculus, and the third removes the fl ap of tissue thus created.
For complete punctal occlusion, the tip of a 19-gauge needle is inserted bevel up and obliquely—under micro-scopic illumination—into the punctal “hill” at an angle almost in line with the (presumed) canalicular lumen. Th e cutting edge of the needle is advanced medially while slowly rotating to bevel down to open the proximal canaliculus. Failure to identify the mucosal-lined lumen signifi es a more extensive block, and the patient should be off ered open lacrimal drainage surgery with retrograde intubation (discussed in the next section).
If there is complete closure of the canaliculi, external DCR with retrograde intubation should be off ered. Although resistance to outfl ow may appear to be limited to a small segment of a canaliculus (or canaliculi), DCR is advocated for three reasons: First, the full extent of canali-cular disease is impossible to determine by probing and may be limited to only a short proximal segment. Second, bypassing the physiological resistance of the nasolacrimal duct with DCR reduces the overall resistance to tear fl ow, and this will aid drainage, even if canalicular dynamics remain impaired. Th ird, it is known that some patients will require a secondary bypass tube—even if the recon-structed anastomosis is anatomically patent—and this is best achieved aft er prior open DCR and carunculectomy.
4.6.1 Surgical Technique for Dacryocystorhinostomy with Retrograde Canaliculostomy
If canalicular occlusion occurs within the proximal 7 mm, DCR with retrograde canaliculostomy is the procedure of choice; this marsupializes the healthy distal canaliculus into the conjunctival sac. Th e extent of canalicular block is established only at surgery, and since a healthy com-mon canaliculus is required to perform retrograde canali-culostomy, the patient should be warned of the possible need for a primary glass bypass tube in the event that no common canaliculus is found. In all cases, carunculec-tomy should be performed as later placement of a bypass tube is more successful within a previously healed carun-culectomy bed.
A large osteotomy should be created as this allows versa-tility in the positioning of any subsequent Jones canalicular bypass tube. Aft er suturing of the posterior mucosal fl aps, the internal common canalicular opening is entered retro-gradely using a “1”-gauge Bowman probe that has been bent perpendicularly at about 8–9 mm from its end. Th e probe is passed as far laterally as possible along each canaliculus, and a 1- to 2-mm fenestration is created in the canalicular wall overlying the tip of the probe (Fig. 4.5a); the “pseudopuncta” are intubated, and the DCR is completed in a standard
Summary for the Clinician
Th ere are many causes for canalicular dysfunc- ■
tion, and symptoms can vary according to the severity and duration of the underlying disease.Local infective causes can include herpes sim- ■
plex and bacterial canaliculitis.Systemic infl ammatory causes include LP, ocular ■
cicatricial pemphigoid, SJS.Topical medications can be a cause of canalicular ■
obstruction.Radiation can have a secondary eff ect that causes ■
an obstruction.Systemic medications such as Taxotere can also ■
lead to canalicular scarring. Proper dosing can reduce the incidence of this.Topical ophthalmic treatments can cause canali- ■
cular scarring.Medications with preservatives can induce ■
chronic infl ammation.MMC therapy used for the treatment of ocular ■
surface malignancy can produce canalicular dis-ease in approximately 21% of patients.Lacrimal stents and plugs may sometimes incite a ■
mucosal infl ammatory response, which may lead to secondary fi brosis and the risk of canalicular stenosis.
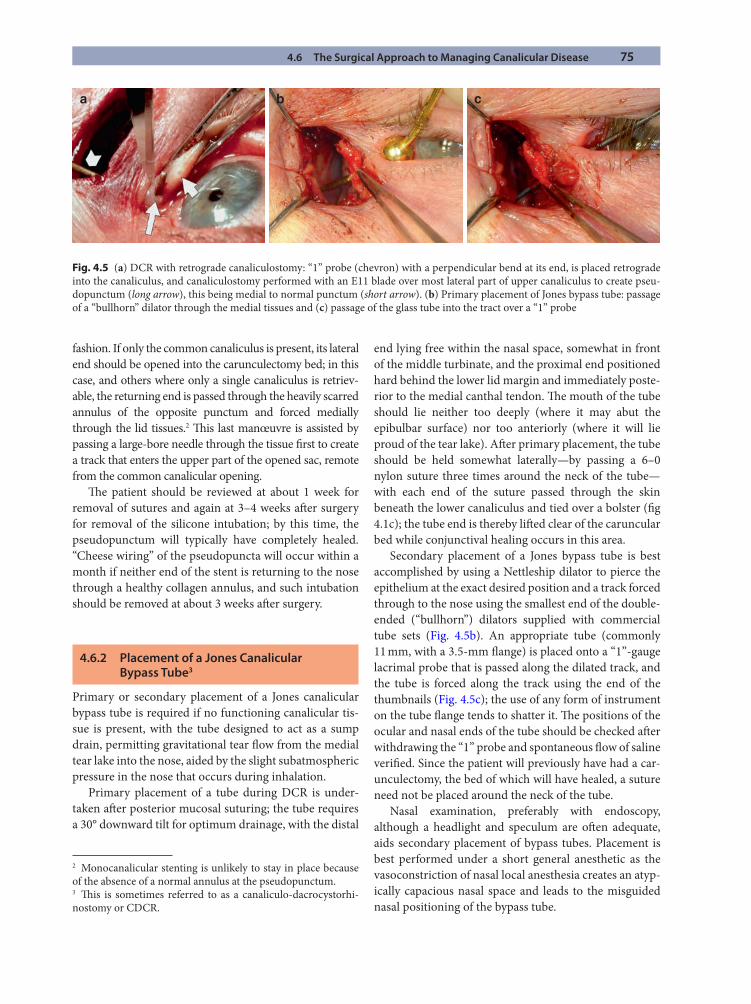
4.6 The Surgical Approach to Managing Canalicular Disease 75
fashion. If only the common canaliculus is present, its lateral end should be opened into the carunculectomy bed; in this case, and others where only a single canaliculus is retriev-able, the returning end is passed through the heavily scarred annulus of the opposite punctum and forced medially through the lid tissues.2 Th is last manœuvre is assisted by passing a large-bore needle through the tissue fi rst to create a track that enters the upper part of the opened sac, remote from the common canalicular opening.
Th e patient should be reviewed at about 1 week for removal of sutures and again at 3–4 weeks aft er surgery for removal of the silicone intubation; by this time, the pseudopunctum will typically have completely healed. “Cheese wiring” of the pseudopuncta will occur within a month if neither end of the stent is returning to the nose through a healthy collagen annulus, and such intubation should be removed at about 3 weeks aft er surgery.
4.6.2 Placement of a Jones Canalicular Bypass Tube3
Primary or secondary placement of a Jones canalicular bypass tube is required if no functioning canalicular tis-sue is present, with the tube designed to act as a sump drain, permitting gravitational tear fl ow from the medial tear lake into the nose, aided by the slight subatmospheric pressure in the nose that occurs during inhalation.
Primary placement of a tube during DCR is under-taken aft er posterior mucosal suturing; the tube requires a 30° downward tilt for optimum drainage, with the distal
end lying free within the nasal space, somewhat in front of the middle turbinate, and the proximal end positioned hard behind the lower lid margin and immediately poste-rior to the medial canthal tendon. Th e mouth of the tube should lie neither too deeply (where it may abut the epibulbar surface) nor too anteriorly (where it will lie proud of the tear lake). Aft er primary placement, the tube should be held somewhat laterally—by passing a 6–0 nylon suture three times around the neck of the tube—with each end of the suture passed through the skin beneath the lower canaliculus and tied over a bolster (fi g 4.1c); the tube end is thereby lift ed clear of the caruncular bed while conjunctival healing occurs in this area.
Secondary placement of a Jones bypass tube is best accomplished by using a Nettleship dilator to pierce the epithelium at the exact desired position and a track forced through to the nose using the smallest end of the double-ended (“bullhorn”) dilators supplied with commercial tube sets (Fig. 4.5b). An appropriate tube (commonly 11 mm, with a 3.5-mm fl ange) is placed onto a “1”-gauge lacrimal probe that is passed along the dilated track, and the tube is forced along the track using the end of the thumbnails (Fig. 4.5c); the use of any form of instrument on the tube fl ange tends to shatter it. Th e positions of the ocular and nasal ends of the tube should be checked aft er withdrawing the “1” probe and spontaneous fl ow of saline verifi ed. Since the patient will previously have had a car-unculectomy, the bed of which will have healed, a suture need not be placed around the neck of the tube.
Nasal examination, preferably with endoscopy, although a headlight and speculum are oft en adequate, aids secondary placement of bypass tubes. Placement is best performed under a short general anesthetic as the vasoconstriction of nasal local anesthesia creates an atyp-ically capacious nasal space and leads to the misguided nasal positioning of the bypass tube.
a b c
Fig. 4.5 (a) DCR with retrograde canaliculostomy: “1” probe (chevron) with a perpendicular bend at its end, is placed retrograde into the canaliculus, and canaliculostomy performed with an E11 blade over most lateral part of upper canaliculus to create pseu-dopunctum (long arrow), this being medial to normal punctum (short arrow). (b) Primary placement of Jones bypass tube: passage of a “bullhorn” dilator through the medial tissues and (c) passage of the glass tube into the tract over a “1” probe
2 Monocanalicular stenting is unlikely to stay in place because of the absence of a normal annulus at the pseudopunctum.3 Th is is sometimes referred to as a canaliculo-dacrocystorhi-nostomy or CDCR.
76 4 Lacrimal Canalicular Infl ammation and Occlusion: Diagnosis and Management
4
References
1. Anand S, Hollingworth K, Kumar V, Sandramouli S. Canaliculitis (2004) Th e incidence of long-term epiphora following canaliculotomy. Orbit 23:19–26
2. Auran J, Hornblass A, Gross ND (1990) Stevens–Johnson syndrome with associated nasolacrimal duct obstruction treated with dacrocystorhinostomy and Crawford silicone tube insertion. Ophthalmic Plast Reconstr Surg 6:60–63
3. Briscoe D, Edelstein E, Zacharopoulos I, et al (2004) Actinomyces canaliculitis: diagnosis of a masquerading disease. Graefes Arch Clin Exp Ophthalmol 242:682–686
4. Brockmann H, Wilhelm K, Joe A, Palmedo H, Biersack H-J (2005) Nasolacrimal drainage obstruction aft er radioio-dine therapy: case report and a review of the literature. Clin Nucl Med 30:543–545
5. Burns JA, Morgenstern KE, Cahill KV, Foster JA, Jhiang SM, Kloos RT (2004) Nasolacrimal obstruction secondary to I(131) therapy. Ophthal Plast Reconstr Surg 20:126–129
6. Call NB, Welham RA (1981) Epiphora aft er irradiation of medial eyelid tumors. Am J Ophthalmol 92:842–845
7. Chak M, Irvine F (2009) Rectangular 3-snip punctoplasty outcomes: preservation of the lacrimal pump in puncto-plasty surgery. Ophthal Plast Reconstr Surg 2:134–135
8. Chen SX, Lee GA (2007) SmartPlug in the management of severe dry eye syndrome. Cornea 26:534–538
9. Dutton JJ, Fowler WC, Gilligan P (2008) Mycobacterium chelonae canaliculitis associated with SmartPlug use. Ophthal Plast Reconstr Surg 24:241–243
10. Durrani OM, Verity DH, Meligonis G, Rose GE (2008) Bicanalicular obstruction in lichen planus: a characteristic pattern of disease. Ophthalmol 115:386–389
11. Esmaeli B, Burnstine MA, Ahmadi MA, Prieto VG (2003) Docetaxel-induced histologic changes in the lacrimal sac and the nasal mucosa. Ophthal Plast Reconstr Surg 19:305–308
12. Esmaeli B, Hidaji L, Adinin RB, et al (2003) Blockage of the lacrimal drainage apparatus as a side eff ect of docetaxel therapy. Cancer 98:504–507
13. Esmaeli B, Hortobagyi G, Esteva F, et al (2003) Canalicular stenosis secondary to weekly docetaxel: a potentially pre-ventable side eff ect. Ann Oncol 13:218–221
14. Fezza JP, Wesley RE, Klippenstein KA (1999) Th e treat-ment of punctal and canalicular stenosis in patients on sys-temic 5-FU. Ophthalmic Surg Lasers 30:105–108
15. Hahn JM, Meisler DM, Lowder CY, Tung RC, Camisa C (2000) Cicatrizing conjunctivitis associated with paraneo-plastic lichen planus. Am J Ophthalmol 129:98–99
16. Khong JJ, Muecke J (2006) Complications of mitomycin C therapy in 100 eyes with ocular surface neoplasia. Br J Ophthalmol 90:819–822
17. Kopp ED, Seregard S (2004) Epiphora as a side eff ect of topical mitomycin C. Br J Ophthalmol 88:1422–1424
18. Linberg JV, Moore CA (1988) Symptoms of canalicular obstruction. Ophthalmology 95:1077–1079
19. Mazow ML, McCall T, Prager TC (2007) Lodged intrac-analicular plugs as a cause of lacrimal obstruction. Ophthal Plast Reconstr Surg 23:138–142
20. McLean CJ, Rose GE (2000) Postherpetic lacrimal obstruc-tion. Ophthalmology 107:496–499
21. McNab AA (1998) Lacrimal canalicular obstruction asso-ciated with topical ocular medication. Aust N Z J Oph-thalmol 26:219–223
22. McNab AA (1998) Lacrimal canalicular obstruction in lichen planus. Orbit 17:201–202
23. Mohan ER, Kabra S, Udhay P, Madhavan HN (2008) Intracanalicular antibiotics may obviate the need for surgi-cal management of chronic suppurative canaliculitis. Indian J Ophthalmol 56:338–340
24. Naik MN, Kelapure A, Rath S, Honavar SG (2008) Management of canalicular lacerations: epidemiological aspects and experience with Mini-Monoka monocanalicu-lar stent. Am J Ophthalmol 145:375–380
25. Neumann R, Dutt CJ, Foster CS (1993) Immuno histo-pathologic features and therapy of conjunctival lichen planus. Am J Ophthalmol 115:494–500
26. Park A, Morgenstern KE, Kahwash SB, Foster JA (2004) Pediatric canaliculitis and stone formation. Ophthal Plast Reconstr Surg 20:243–246
27. Reifl er DM (1991) Management of canalicular laceration. Surv Ophthalmol 36:113–132
28. Rhee MK, Mootha VV (2004) Bilateral keratoconjunctivi-tis associated with lichen planus. Cornea 23:100–105
29. Rumelt S, Remulla H (1997) Silicone punctal plug migra-tion resulting in dacryocystitis and canaliculitis. Cornea 16:377–379
30. Scheepers M, Pearson A, Michaelides M (2007) Bilateral canaliculitis following SmartPLUG insertion for dry eye syndrome post LASIK surgery. Graefes Arch Clin Exp Ophthalmol 245:895–897
Summary for the Clinician
Th e surgical management depends on the location and the severity of canalicular obstruction, and may include:
Punctoplasty ■
DCR with retrograde canaliculostomy ■
Canalicular Pyrex bypass tubes (possibly the ■
only eff ective solution for severe canalicular obstruction)
References 77
31. Solans R, Bosch JA, Galofre P, et al (2004) Salivary and lac-rimal gland dysfunction (sicca syndrome) aft er radioio-dine therapy. J Nucl Med 42:738–743
32. Tsalic M, Gilboa M, Visel B, Miller B, Haim N (2006) Epiphora (excessive tearing) and other ocular manifesta-tions related to weekly docetaxel: underestimated dose-limiting toxicity. Med Oncol 23:57–61
33. Tucker NA, Tucker SM, Linberg JV (1996) Th e anatomy of the common canaliculus. Arch Ophthalmol 114:1231–1234
34. Varma D, Chang B, Musaad S (2005) A case series on chronic canaliculitis. Orbit 24:11–14
35. Vécsei VP, Huber-Spitzy V, Arocker-Mettinger E, Steinkogler FJ (1994) Canaliculitis: diffi culties in diagnosis, diff erential diagnosis and comparison between conservative and surgi-cal treatment. Ophthalmologica 208: 314–317
36. Wearne MJ, Beigi B, Davis G, Rose GE (1999) Retrograde intubation dacryocystorhinostomy for proximal and mid-canalicular obstruction. Ophthalmology 106:2325–2328
37. Wright P, Collin JR (1983) Th e ocular complications of erythema multiforme (Stevens Johnson syndrome) and their management. Trans Ophthalmol Soc U K 103: 338–341
5.1 Introduction
Neurofi bromatosis type 1 (NF1) is an autosomal domi-nant disorder occurring with an estimated incidence of 1 in 3,000 live births [16]. Th e propensity for tumor pro-gression and skeletal abnormalities in this disease present both functional and cosmetic challenges for both patients and the physicians treating them. Th is is most evident in patients disfi gured by NF1 involving the orbits and face. Th is chapter summarizes the clinical fi ndings, updates current clinical trials, and describes surgical techniques useful in the treatment of NF1 tumors involving the orbit and adjacent tissues.
5.2 Nomenclature
Th e fi rst published case report describing the fi ndings in NF1 was published by Von Recklinghausen in1882 [43]. Th ere have since been numerous terms used to describe
the involvement of the orbit and face. Orbitotemporal neurofi bromatosis has been the most common [12]. Other terms are orbitopalpebral neurofi bromatosis [35], orbitofacial neurofi bromatosis [46], oculofacial neurofi -bromatosis [10], and cranio-orbital-temporal neurofi bro-matosis [18]. Orbitofacial neurofi bromatosis is perhaps the most inclusive term for the oculoplastic surgeon since it highlights the potential involvement of NF1 tumors aff ecting not only the orbit, eyelids, and temporalis region but also facial structures above and below the orbits.
5.3 Clinical Manifestations of NF1
NF1 is caused by a germline-inactivating mutation in the NF1 gene on chromosome 17 that results in deregulated cell growth. Th is abnormal growth manifests in various soft tissue and bony abnormalities, oft en producing major orbitofacial deformities [50]. Th e lesions most disfi guring in orbitofacial NF1 are neurofi bromas and optic gliomas.
Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical ManagementWilliam R. Katowitz and James A. Katowitz
Chapter 5
5
Core Messages
Neurofi bromatosis type 1 (NF1) is an inherited ■
disorder that predisposes a patient to acquired neoplasms.Th ere are many challenges to the management of ■
NF1 associated orbitofacial neurofi bromas and optic pathway gliomas.New understanding of intracellular pathways, ■
specifi cally the role of neurofi bromin as a nega-tive regulator of Ras, an intracellular signaling protein, may allow future treatment to target NF1-associated tumors.While chemotherapy protocols to treat optic ■
pathway gliomas (OPGs) have been somewhat eff ective, the medical treatment of plexiform neu-rofi bromas to date has been less successful.
A multidisciplinary approach is essential for ■
treating patients with NF1 and should include genetic counseling and testing for both patients and their families.Early intervention can better control expansion ■
of soft tissues and possibly reduce bony orbital expansion.Periorbital surgical techniques for managing ■
tumors involving the orbit and adnexal structures can oft en spare more invasive neurosurgical approaches in the orbitofacial rehabilitation of NF1 patients.Orbital exenteration can be avoided in almost ■
every instance.
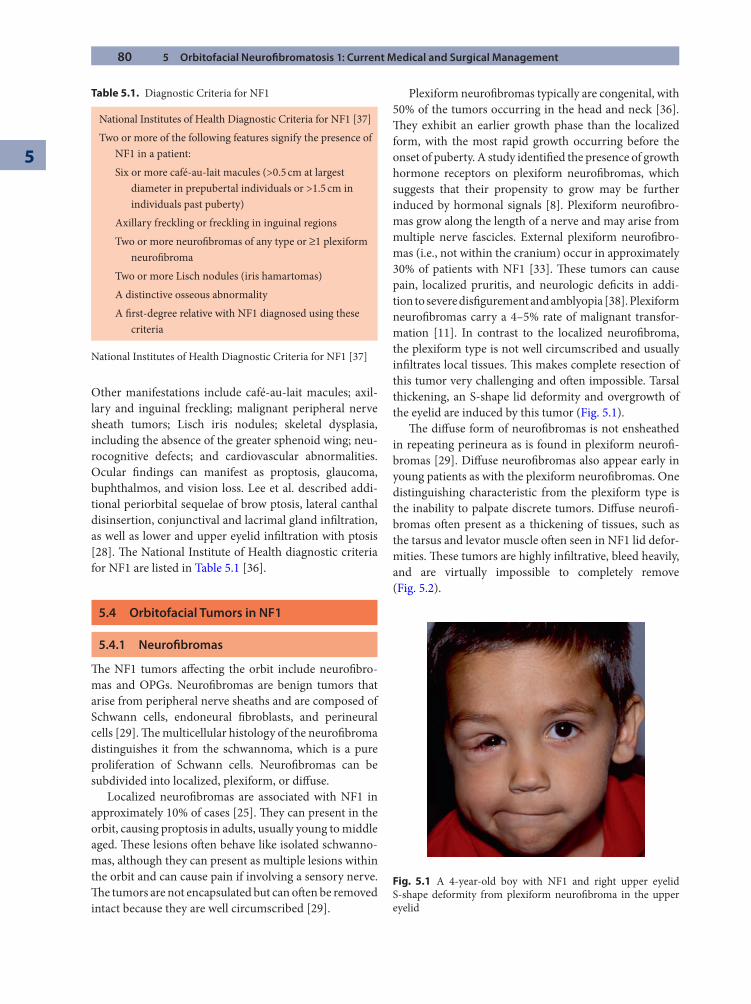
80 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
Other manifestations include café-au-lait macules; axil-lary and inguinal freckling; malignant peripheral nerve sheath tumors; Lisch iris nodules; skeletal dysplasia, including the absence of the greater sphenoid wing; neu-rocognitive defects; and cardiovascular abnormalities. Ocular fi ndings can manifest as proptosis, glaucoma, buphthalmos, and vision loss. Lee et al. described addi-tional periorbital sequelae of brow ptosis, lateral canthal disinsertion, conjunctival and lacrimal gland infi ltration, as well as lower and upper eyelid infi ltration with ptosis [28]. Th e National Institute of Health diagnostic criteria for NF1 are listed in Table 5.1 [36].
5.4 Orbitofacial Tumors in NF1
5.4.1 Neurofi bromas
Th e NF1 tumors aff ecting the orbit include neurofi bro-mas and OPGs. Neurofi bromas are benign tumors that arise from peripheral nerve sheaths and are composed of Schwann cells, endoneural fi broblasts, and perineural cells [29]. Th e multicellular histology of the neurofi broma distinguishes it from the schwannoma, which is a pure proliferation of Schwann cells. Neurofi bromas can be subdivided into localized, plexiform, or diff use.
Localized neurofi bromas are associated with NF1 in approximately 10% of cases [25]. Th ey can present in the orbit, causing proptosis in adults, usually young to middle aged. Th ese lesions oft en behave like isolated schwanno-mas, although they can present as multiple lesions within the orbit and can cause pain if involving a sensory nerve. Th e tumors are not encapsulated but can oft en be removed intact because they are well circumscribed [29].
Plexiform neurofi bromas typically are congenital, with 50% of the tumors occurring in the head and neck [36]. Th ey exhibit an earlier growth phase than the localized form, with the most rapid growth occurring before the onset of puberty. A study identifi ed the presence of growth hormone receptors on plexiform neurofi bromas, which suggests that their propensity to grow may be further induced by hormonal signals [8]. Plexiform neurofi bro-mas grow along the length of a nerve and may arise from multiple nerve fascicles. External plexiform neurofi bro-mas (i.e., not within the cranium) occur in approximately 30% of patients with NF1 [33]. Th ese tumors can cause pain, localized pruritis, and neurologic defi cits in addi-tion to severe disfi gurement and amblyopia [38]. Plexiform neurofi bromas carry a 4–5% rate of malignant transfor-mation [11]. In contrast to the localized neurofi broma, the plexiform type is not well circumscribed and usually infi ltrates local tissues. Th is makes complete resection of this tumor very challenging and oft en impossible. Tarsal thickening, an S-shape lid deformity and overgrowth of the eyelid are induced by this tumor (Fig. 5.1).
Th e diff use form of neurofi bromas is not ensheathed in repeating perineura as is found in plexiform neurofi -bromas [29]. Diff use neurofi bromas also appear early in young patients as with the plexiform neurofi bromas. One distinguishing characteristic from the plexiform type is the inability to palpate discrete tumors. Diff use neurofi -bromas oft en present as a thickening of tissues, such as the tarsus and levator muscle oft en seen in NF1 lid defor-mities. Th ese tumors are highly infi ltrative, bleed heavily, and are virtually impossible to completely remove (Fig. 5.2).
National Institutes of Health Diagnostic Criteria for NF1 [37]Two or more of the following features signify the presence of
NF1 in a patient:Six or more café-au-lait macules (>0.5 cm at largest
diameter in prepubertal individuals or >1.5 cm in individuals past puberty)
Axillary freckling or freckling in inguinal regionsTwo or more neurofi bromas of any type or ≥1 plexiform
neurofi bromaTwo or more Lisch nodules (iris hamartomas)A distinctive osseous abnormalityA fi rst-degree relative with NF1 diagnosed using these
criteria
Fig. 5.1 A 4-year-old boy with NF1 and right upper eyelid S-shape deformity from plexiform neurofi broma in the upper eyelid
National Institutes of Health Diagnostic Criteria for NF1 [37]
Table 5.1. Diagnostic Criteria for NF1
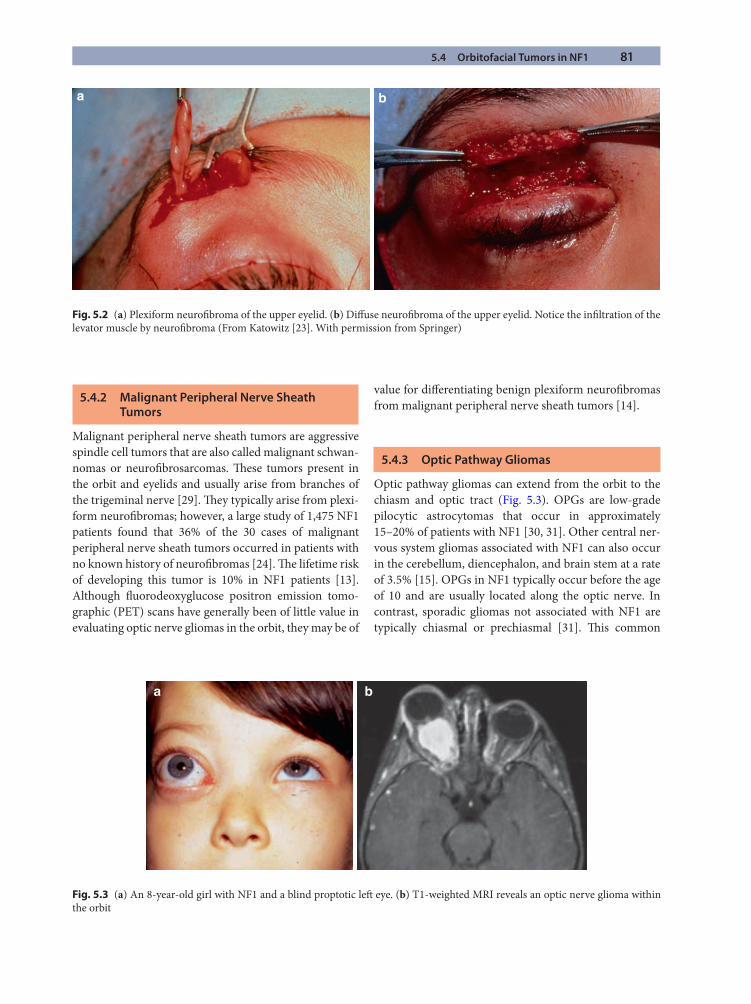
5.4 Orbitofacial Tumors in NF1 81
5.4.2 Malignant Peripheral Nerve Sheath Tumors
Malignant peripheral nerve sheath tumors are aggressive spindle cell tumors that are also called malignant schwan-nomas or neurofi brosarcomas. Th ese tumors present in the orbit and eyelids and usually arise from branches of the trigeminal nerve [29]. Th ey typically arise from plexi-form neurofi bromas; however, a large study of 1,475 NF1 patients found that 36% of the 30 cases of malignant peripheral nerve sheath tumors occurred in patients with no known history of neurofi bromas [24]. Th e lifetime risk of developing this tumor is 10% in NF1 patients [13]. Although fl uorodeoxyglucose positron emission tomo-graphic (PET) scans have generally been of little value in evaluating optic nerve gliomas in the orbit, they may be of
value for diff erentiating benign plexiform neurofi bromas from malignant peripheral nerve sheath tumors [14].
5.4.3 Optic Pathway Gliomas
Optic pathway gliomas can extend from the orbit to the chiasm and optic tract (Fig. 5.3). OPGs are low-grade pilocytic astrocytomas that occur in approximately 15–20% of patients with NF1 [30, 31]. Other central ner-vous system gliomas associated with NF1 can also occur in the cerebellum, diencephalon, and brain stem at a rate of 3.5% [15]. OPGs in NF1 typically occur before the age of 10 and are usually located along the optic nerve. In contrast, sporadic gliomas not associated with NF1 are typically chiasmal or prechiasmal [31]. Th is common
a b
Fig. 5.2 (a) Plexiform neurofi broma of the upper eyelid. (b) Diff use neurofi broma of the upper eyelid. Notice the infi ltration of the levator muscle by neurofi broma (From Katowitz [23]. With permission from Springer)
a b
Fig. 5.3 (a) An 8-year-old girl with NF1 and a blind proptotic left eye. (b) T1-weighted MRI reveals an optic nerve glioma within the orbit

82 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
belief has been challenged by Singhal et al., who found a signifi cant involvement of the chiasm in NF1-associated OPG as compared to sporadic cases (10 of 17 cases with NF1 and 6 of 17 sporadic OPGs) [44]. Symptoms can include proptosis, vision loss, and hypothalamic involve-ment, resulting in precocious puberty. Th ere are reports of progression of OPGs, although the common belief is that this occurs more frequently in sporadic cases [50].
When considering outcomes, the term progression, from an orbital surgeon’s perspective, needs clarifi cation. In this regard, it is useful to review the neurooncology perspective, particularly as it applies to NF1. Th ere are several categories that can be used to describe the clinical status of OPGs from initial diagnosis to remission or cure. Remission is most commonly used to describe a positive response to medical therapy. While spontaneous remis-sions can occur in NF1 OPGs, this is rarely, if ever, observed in sporadic OPGs [41]. Recurrence of tumor describes evidence of tumor aft er an apparent tumor-free period. Progression of tumor describes growth of an exist-ing mass. Th is can be observed either clinically (i.e., increasing proptosis), for example, or by serial imaging studies demonstrating an increase in volume or expan-sion of the lesion. For the orbital surgeon, the major con-cern has related to the possibility of “retrograde progression,” particularly regarding optic nerve gliomas growing posteriorly from the orbital apex through the bony optic canal toward the chiasm [2, 22].
Management paradigms for treating NF1 orbital tumors and particularly optic nerve glioma have been somewhat controversial. A common assumption has been that these lesions represent hamartomas with early and then static growth. Th e traditional concepts have been that (1) NF1-related gliomas act more benignly, (2) optic nerve gliomas without chiasmatic involvement do not later spread into the chiasm, and (3) surgical removal to prevent spread is unnecessary. Studies, however, indi-cated that there may be some cases when retrograde pro-gression can occur. Singhal et al. reported one case of an NF1-associated glioma that had aff ected the left optic nerve and was excised. Nine years later, the optic glioma recurred in the chiasm [44].
A report by Walrath et al. demonstrated retrograde growth in a non-NF1 patient [47]. Progression from pre-chiasmal to chiasmal to postchiasmal disease was dem-onstrated on serial magnetic resonance imaging (MRI) scans. Of signifi cance, clinically, with treatment using confocal radiation and intravenous steroids, vision was regained from no light perception (NLP) to 20/20. Because of disfi guring proptosis, however, an excisional biopsy was done. Th e histopathology confi rmed that the tumor was a benign pilocytic astrocytoma. Of major
interest, however, were the results of histochemical stud-ies, which revealed evidence of a mindbomb homolog (MIB-1 LI) [6]. Th is homolog is an antibody that recog-nizes Ki 67, a protein active during all phases of the cell cycle. Increased levels of Ki 67 have been found to be con-sistent with aggressive tumor behavior in OPGs [7, 47]. Th e normal value for Ki 67 in benign pilocytic astrocy-tomas is less than 1%. In this patient, however, the speci-men revealed an average of 2.8%, with some areas as high as 7%. Th e importance of this case is not only that active growth in the tumor was observed both clinically and his-tologically but also that the tumor responded to therapy with a dramatic improvement in vision. Th ese fi ndings do not conform with the concept of a hamartoma. An accom-panying editorial by Miller in the same journal empha-sized that it is “inaccurate to consider such lesions to be hamartomas and equally inappropriate to recommend no treatment for lesions that show evidence of clinical or imaging progression” [34]. Walrath and his coauthors further suggested that early biopsy with histochemical studies may possibly provide prognostic information regarding timing and extent of surgical resection [47].
Th is assertion is supported by the histologic fi ndings by Burstine et al. [6], who performed quantitative analy-sis of proliferative activity of 14 optic nerve gliomas using the silver nucleolar organizing region technique and found 6 of 14 gliomas positive. A similar fi nding was observed in other malignant tumors. In addition, the analysis was equivocal regardless of location or NF1 association.
First-line therapy for OPGs includes appropriate imaging and chemotherapy [39]. Although chemother-apy regimens vary depending on the institution, a new protocol (Children’s Oncology Group Chemotherapy Protocol CCG-A9952) has completed a phase III ran-domized study of carboplatin and vincristine compared to thioguanine, procarbazine, lomustine, and vincristine in children with progressive low-grade astrocytoma [4]. Although the results of this study have not yet been pub-lished, it does appear from other reports that the eff ec-tiveness of chemotherapy for chiasmal gliomas has been greatly improved, with 5-year survival rates of over 70% [44]. Radiation for chiasmal lesions has not been recom-mended for children under 5 years of age because of dam-age to the brain and hypothalamus. Because of the success rates with chemotherapy, however, the use of radiation even in older patients is no longer recommended [26]. Surgical intervention is usually reserved for gliomas that either respond poorly to chemotherapy or radiation or are associated with severe proptosis causing vision loss or a marked cosmetic deformity. Th is is discussed more fully in other sections of this chapter.
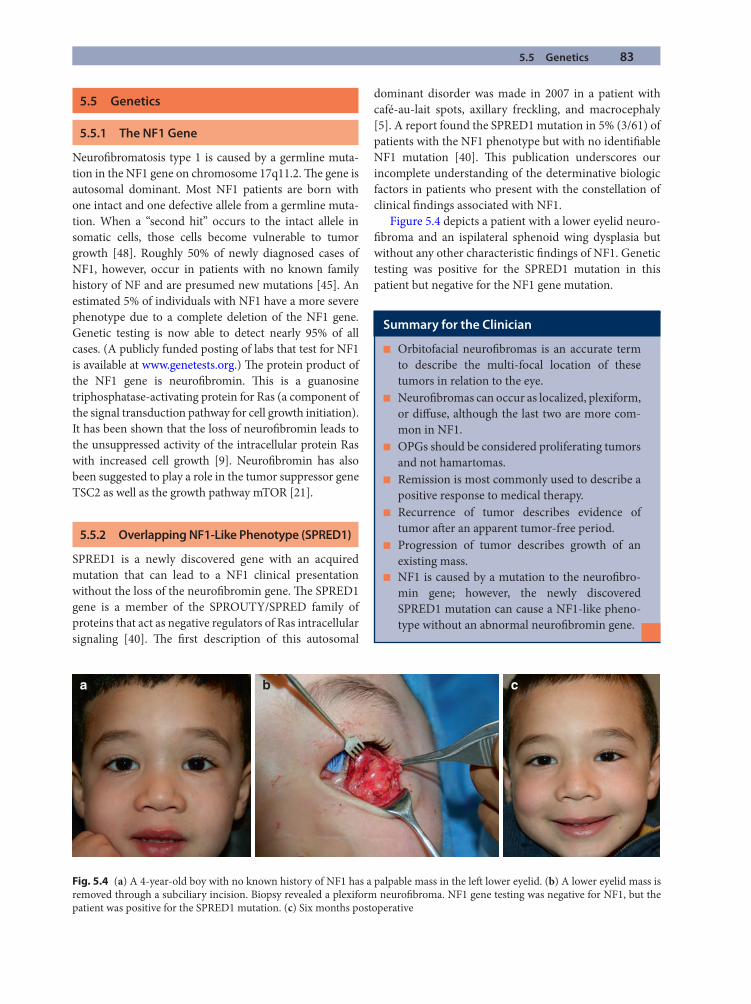
5.5 Genetics 83
5.5 Genetics
5.5.1 The NF1 Gene
Neurofi bromatosis type 1 is caused by a germline muta-tion in the NF1 gene on chromosome 17q11.2. Th e gene is autosomal dominant. Most NF1 patients are born with one intact and one defective allele from a germline muta-tion. When a “second hit” occurs to the intact allele in somatic cells, those cells become vulnerable to tumor growth [48]. Roughly 50% of newly diagnosed cases of NF1, however, occur in patients with no known family history of NF and are presumed new mutations [45]. An estimated 5% of individuals with NF1 have a more severe phenotype due to a complete deletion of the NF1 gene. Genetic testing is now able to detect nearly 95% of all cases. (A publicly funded posting of labs that test for NF1 is available at www.genetests.org.) Th e protein product of the NF1 gene is neurofi bromin. Th is is a guanosine triphosphatase-activating protein for Ras (a component of the signal transduction pathway for cell growth initiation). It has been shown that the loss of neurofi bromin leads to the unsuppressed activity of the intracellular protein Ras with increased cell growth [9]. Neurofi bromin has also been suggested to play a role in the tumor suppressor gene TSC2 as well as the growth pathway mTOR [21].
5.5.2 Overlapping NF1-Like Phenotype (SPRED1)
SPRED1 is a newly discovered gene with an acquired mutation that can lead to a NF1 clinical presentation without the loss of the neurofi bromin gene. Th e SPRED1 gene is a member of the SPROUTY/SPRED family of proteins that act as negative regulators of Ras intracellular signaling [40]. Th e fi rst description of this autosomal
dominant disorder was made in 2007 in a patient with café-au-lait spots, axillary freckling, and macrocephaly [5]. A report found the SPRED1 mutation in 5% (3/61) of patients with the NF1 phenotype but with no identifi able NF1 mutation [40]. Th is publication underscores our incomplete understanding of the determinative biologic factors in patients who present with the constellation of clinical fi ndings associated with NF1.
Figure 5.4 depicts a patient with a lower eyelid neuro-fi broma and an ispilateral sphenoid wing dysplasia but without any other characteristic fi ndings of NF1. Genetic testing was positive for the SPRED1 mutation in this patient but negative for the NF1 gene mutation.
a b c
Fig. 5.4 (a) A 4-year-old boy with no known history of NF1 has a palpable mass in the left lower eyelid. (b) A lower eyelid mass is removed through a subciliary incision. Biopsy revealed a plexiform neurofi broma. NF1 gene testing was negative for NF1, but the patient was positive for the SPRED1 mutation. (c) Six months postoperative
Summary for the Clinician
Orbitofacial neurofi bromas is an accurate term ■
to describe the multi-focal location of these tumors in relation to the eye.Neurofi bromas can occur as localized, plexiform, ■
or diff use, although the last two are more com-mon in NF1.OPGs should be considered proliferating tumors ■
and not hamartomas.Remission is most commonly used to describe a ■
positive response to medical therapy.Recurrence of tumor describes evidence of ■
tumor aft er an apparent tumor-free period.Progression of tumor describes growth of an ■
existing mass.NF1 is caused by a mutation to the neurofi bro- ■
min gene; however, the newly discovered SPRED1 mutation can cause a NF1-like pheno-type without an abnormal neurofi bromin gene.
84 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
5.6 Management of Neurofi bromatosis Type 1
5.6.1 Introduction
Due to the variable clinical manifestations of NF1, treatment must be tailored to the patient and not the disease. A multidisciplinary approach is important for optimizing patient care by incorporating the diagnostic and management skills of other medical services such as genetics, neurooncology, ophthalmology, neu-roophthalmology, plastic surgery, otolaryngology, orthopedics, general surgery, and developmental psy-chiatry/psychology.
5.6.2 Medical Management of Neurofi bromas
Although there has been some success in treating OPGs with chemotherapy or radiation, the management for optic nerve gliomas in the orbit has been primarily surgi-cal when treatment for severe proptosis has been deter-mined necessary. For plexiform neurofi bromas, however, because of their marked vascularity, numerous chemo-therapeutic agents are being tested as potential treat-ments. A clinical trial with alfa-interferon has had poor results [50]. Th alidomide has also had poor results with plexiform neurofi bromas but has shown more promise in treating malignant peripheral nerve sheath tumors [17]. AZD2171, a small molecule VEGF-like vascular endothe-lial growth factor (VEGF) receptor, is currently under phase I study [3]. Tipifarnib, a drug specifi cally targeting tumor cells, is also currently in phase II trials. Th is is a farnysyl transferase inhibitor that aff ects intracellular Ras activity and has shown some promise in phase I trials in both children and adults [49].
Th e antifi brotic agent pirifenidone (5-methyl-1-phenyl-2-[1H]-pyridone) is now in phase II trials. Th is medication attenuates cytokine release by fi broblasts thus weakening the cellular support of neurofi bromas [1]. At the Children’s Hospital of Philadelphia, the eff ectiveness of methotrexate with Velban for suppressing NF1 tumor growth is currently being evaluated as well as an NF consortium study using rapamycin. Although there is as yet no published data, anecdotally, however, it appears that there may be some slowing of growth but little evidence of regression [4].
Unfortunately, to date an eff ective “home run” medical regimen has not been found for managing plexiform neu-rofi bromas [4]. For this reason, surgical debulking and reconstruction still remain the best option for orbitofacial rejuvenation from the disfi guring tumors associated with NF1. Th e following section outlines our current approach to the surgical management of orbitofacial tumors associ-ated with NF1.
5.7 Surgical Management of Orbitofacial Tumors in NF1
5.7.1 Introduction
Surgical intervention to help restore function and improve cosmesis in patients with orbitofacial involvement of neurofi bromatosis has been well described in the litera-ture. Jackson et al., in their series of 24 patients with NF1, defi ned three treatment groups [19]:
1. Orbital soft tissue involvement with a seeing eye2. Orbital soft tissue and signifi cant bony involvement
with a seeing eye3. Orbital soft tissue and signifi cant bony involvement
with a blind or absent eye
Lee et al., in their series of 33 patients with NF1, elabo-rated on this classifi cation by describing additional fi nd-ings to these treatment groups [28]:
1. Brow ptosis2. Upper lid infi ltration with ptosis3. Lower lid infi ltration4. Lateral canthal disinsertion5. Conjunctival and lacrimal gland infi ltration
5.7.2 Timing of Surgery
It is critical to recognize the emotional stress and psycho-social implications of NF1 deformities not only on the aff ected individuals but also on their families and friends. Social withdrawal due to disfi gurement and chronic pain must be considered when evaluating the need for and tim-ing of surgical intervention. Some authors suggest delay-ing intervention if possible due to the higher rate of “recurrence” in younger patients. In the periorbital region, these tumors really do not represent recurrences, how-ever, but rather continued progression of sheath and cuta-neous tumors in particular. In our experience, most families are extremely motivated to begin treatment, including surgical intervention, even though cautioned
Summary for the Clinician
First-line therapy for OPGs is proper imaging ■
and chemotherapy.Medical therapy for neurofi bromas is currently ■
under clinical trials; however, initial data do not point to a home run therapy. and surgery should always be considered a primary treatment.

5.7 Surgical Management of Orbitofacial Tumors in NF1 85
regarding the continuing need for multiple surgical cor-rections in most instances [28]. We have observed signifi -cant improvements in patients’ social interactions aft er surgery that have defi nitely outweighed a more conserva-tive approach to defer intervention until postadolescent years. In addition, the preservation of vision is also an important factor since surgery can oft en help to reduce the amblyogenic infl uence on a patient’s visual develop-ment. Th e indication for a diagnostic biopsy may some-times be an important consideration as well, requiring surgical intervention in certain clinical situations. Eff orts to correct orbitofacial deformities are very challenging from both functional and aesthetic perspectives. Regarding ptosis surgery, in particular, Jackson et al. stated [19]:
Th e most unsatisfactory part of the procedure is the ptosis correction. Th is frequently requires repeat surgery, and even aft er this, there may be incomplete lid elevation.
Indeed, most patients require multiple procedures to treat tumor progression, as well as repeat procedures for the mechanical type of ptosis caused by NF1. It is important to counsel patients and families of the strong possibility that multiple procedures may be required in any eff ort to approach a normal appearance through orbitofacial reha-bilitation surgery.
Th e reality of tumor “recurrence,” specifi cally plexiform neurofi broma, is well documented. A 20-year review pub-lished by the neurofi bromatosis clinic at the Children’s Hospital of Philadelphia reviewed 121 patients who had 302 procedures. Th e overall freedom from tumor progression was 54%. Th e main risk factors for progression were (1) tumors of the head/neck/face, (2) less-extensive progres-sion, and (3) aff ected children less than10 years of age [38]. Th e risk of tumor progression, however, should not be con-sidered a deterrent to surgical intervention when one weighs the overall psychological, aesthetic, and oft en functional benefi ts of orbitofacial rehabilitation for NF1 deformities.
Some authors have actually advocated the need for exenteration in part to prevent tumor progression but also to decrease the risk of malignant transformation [12, 32]. It is our belief, however, that this permanently disfi g-uring procedure can be avoided in almost all circum-stances with acceptable results.
5.7.3 Periorbital Involvement
5.7.3.1 The Upper Eyelid
Th e classic appearance of an upper eyelid S-shape defor-mity frequently occurs in NF1 patients with neurofi -broma infi ltration of the upper eyelid (Fig. 5.1). Th is can
involve any of the eyelid tissues from the dermis, orbic-ularis, levator complex, tarsus, and conjunctiva. Sometimes, the lid may become thickened and heavy with tumor, causing ptosis of the upper eyelid. Th e term bag of worms oft en used to describe plexiform neurofi -bromas is appropriate as these tumors can be readily palpated in the upper lid. Th ey represent sheath abnor-malities occurring in multiple nerve fi bers in the upper eyelid tissues.
When approaching the management of NF1-induced ptosis in children, one must always be cognizant of the amblyogenic risk of ptosis as well as possible anisometro-pia from induced astigmatism. In our experience, we usu-ally fi nd an anterior approach for NF1-induced ptosis most useful because tumor debulking is most commonly required. In general, patients with moderate or better levator function have a good functional result with an anterior levator resection. With advancing age, as plexi-form and diff use neurofi bromas grow, the anterior lid crease approach for ptosis repair can be extended to per-mit wedge resection and re-formation of the lateral can-thal angle. A periosteal fl ap is oft en useful.
Frontalis suspension surgery is reserved for those patients with poor levator function (4 mm or worse). In patients under the age of 5, we prefer a silicone frontalis sling passed in a rhomboid fashion with two brow stab wounds (medial fi xation of sling over a silicone sleeve). In patients older than 5 years, the ideal sling material is autogenous fascia lata.
5.7.3.2 The Lower Eyelid and Midface
Some patients may present with an isolated mass of the lower eyelid with or without a known diagnosis of NF1. Figure 5.4 illustrates how a lower eyelid/upper midface mass may be removed through a subciliary incision with minimal morbidity. A patient in France underwent a lower and midface transplant for a massive plexiform neurofi broma. On 1-year follow-up, aft er two episodes of clinical rejection (at 1 month and at 2 months), the patient had acceptable sensory and motor innervation of the transplanted territory [27]. Th is treatment represents a potential new horizon for allotransplantation that cer-tainly warrants further research. While most cases of adnexal deformity due to NF1 can be managed by less-drastic measures, there may be a place for facial trans-plantation in the patient who has not had the benefi t of early debulking and reconstruction, including subsequent follow-up procedures, and presents as an adult with extraordinarily gross deformities diffi cult to manage from both a functional and aesthetic perspective using more conventional techniques.
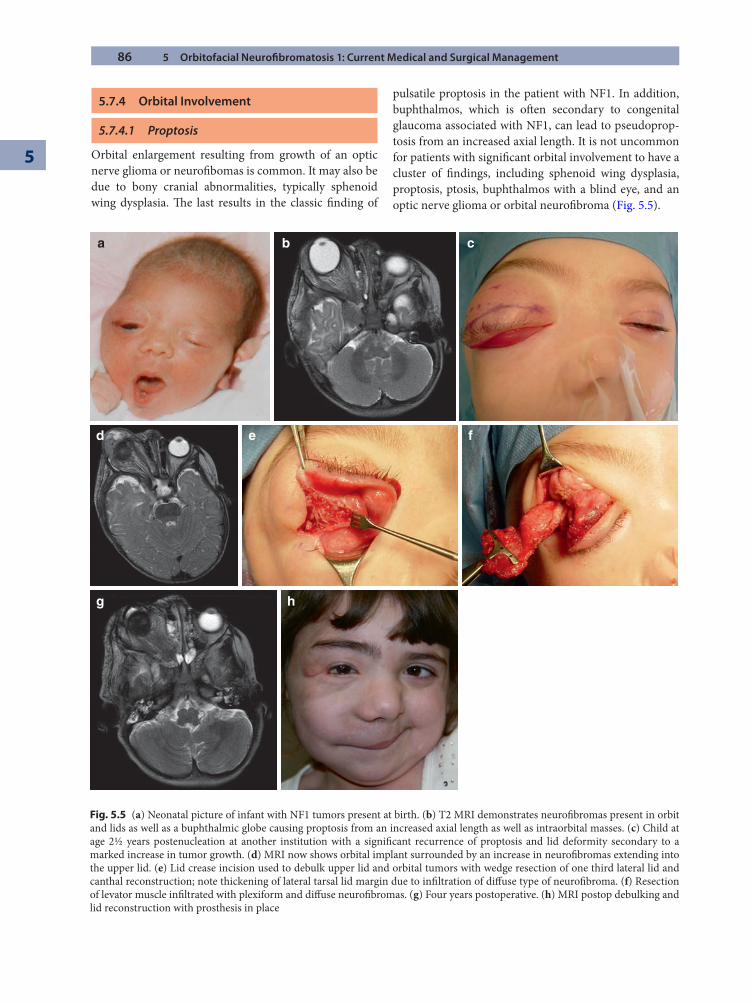
86 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
5.7.4 Orbital Involvement
5.7.4.1 Proptosis
Orbital enlargement resulting from growth of an optic nerve glioma or neurofi bomas is common. It may also be due to bony cranial abnormalities, typically sphenoid wing dysplasia. Th e last results in the classic fi nding of
pulsatile proptosis in the patient with NF1. In addition, buphthalmos, which is oft en secondary to congenital glaucoma associated with NF1, can lead to pseudoprop-tosis from an increased axial length. It is not uncommon for patients with signifi cant orbital involvement to have a cluster of fi ndings, including sphenoid wing dysplasia, proptosis, ptosis, buphthalmos with a blind eye, and an optic nerve glioma or orbital neurofi broma (Fig. 5.5).
a b c
d
g h
e f
Fig. 5.5 (a) Neonatal picture of infant with NF1 tumors present at birth. (b) T2 MRI demonstrates neurofi bromas present in orbit and lids as well as a buphthalmic globe causing proptosis from an increased axial length as well as intraorbital masses. (c) Child at age 2½ years postenucleation at another institution with a signifi cant recurrence of proptosis and lid deformity secondary to a marked increase in tumor growth. (d) MRI now shows orbital implant surrounded by an increase in neurofi bromas extending into the upper lid. (e) Lid crease incision used to debulk upper lid and orbital tumors with wedge resection of one third lateral lid and canthal reconstruction; note thickening of lateral tarsal lid margin due to infi ltration of diff use type of neurofi broma. (f) Resection of levator muscle infi ltrated with plexiform and diff use neurofi bromas. (g) Four years postoperative. (h) MRI postop debulking and lid reconstruction with prosthesis in place

5.7 Surgical Management of Orbitofacial Tumors in NF1 87
A multidisciplinary approach is best for the NF1 patient affl icted with these complicated disfi guring prob-lems. Even aft er neurooncological evaluation and treat-ment, it is oft en necessary to intervene surgically to rehabilitate a patient’s appearance. For the child with gross orbital and periorbital deformities, this may be of even greater concern to the family than the preservation of the eye on the aff ected side despite the opportunity for a reasonable visual potential. Th e surgeon must thor-oughly discuss the realistic limits to keeping a proptotic eye versus complete resection (enucleation, etc.) with subsequent socket reconstruction.
Th e approach to the proptotic patient with NF1 may require craniofacial or neurosurgical collaboration depending on the need to reach a specifi c area of the orbit. For posterior apical lesions or the repair of certain bony abnormalities of the orbit and cranium, a transcra-nial neurosurgical approach may be warranted. Other options for treating proptosis in NF1 are usually available to avoid unnecessarily aggressive intervention, such as orbital exenteration for rehabilitation. As stated, we strongly reject use of this technique except for an extremely unusual case for which malignancy is of docu-mented concern. With a carefully staged approach to multiple surgeries, reasonable results can be achieved to optimize ocular prosthesis retention with acceptable or even good cosmesis in many cases.
5.7.4.2 Proptosis Due to Orbital Neurofi bromas
Patients with orbital neurofi bromas, particularly of the plexiform type, may benefi t from possible reduction of tumor with additional chemotherapy. To this date, how-ever, no chemotherapy regimen has proven eff ective in completely reducing orbital neurofi bromas [4]. Th e main eff ect, as stated, has been possible slowed growth. At this time, for patients with signifi cant orbital involvement, surgery remains the most hopeful modality for address-ing issues of painful proptosis or disfi gurement. Patients may suff er from exposure due to proptosis and from orbital or periorbital discomfort secondary to their orb-itofacial neurofi bromas. Th e surgeon must obtain ade-quate imaging in such cases to delineate the presence of any intracranial extension as well as any additional intrac-ranial tumors or other pathology.
5.7.4.3 Proptosis Due to Optic Nerve Glioma
Th e medical management and controversies regarding tumor classifi cation of OPGs in NF1 have been addressed in this chapter. In addition to medical management,
tumor resection may be considered. Th is is both to treat disfi guring proptosis and to remove a lesion that could potentially grow posteriorly. Gliomas of the orbital optic nerve causing proptosis can oft en be removed by a lateral approach, especially in children, for whom the orbit is shallower and removal of the orbital bone can be avoided (Fig. 5.6). Gliomas directly behind the globe can some-times be removed by an anterior approach combined with enucleation (Fig. 5.7). For posterior lesions where there is severe proptosis or real concern regarding retrograde progression, a superior transcranial neurosurgical approach may be required (Fig. 5.8).
5.7.4.4 Orbital Enlargement with Dystopia and Hypoglobus
Early involvement of NF1 tumors can lead to orbital enlargement (Fig. 5.9). Th is can present a signifi cant sur-gical dilemma for reconstruction. Debulking of tumor from the orbit early in life may decrease the stimulus for asymmetric growth to some degree but is usually not suf-fi cient to control this eff ectively. Orbital bony enlarge-ment, while a problem, is oft en less noticeable than the soft tissue deformities usually associated with this. For the casual observer, the increase in orbital volume is actu-ally hidden. Th e periorbital soft tissue changes are what is noticeable, represented by a higher and oft en more prom-inent brow, a lengthened lid fi ssure with lid deformities secondary to tumor growth, as well as an associated mechanical ptosis. Bony sphenoid wing dysplasia or even aplasia permits visible pulsations transmitted from the brain through the orbital defect.
Fig. 5.6 Optic nerve glioma excision: lateral approach. Gliomas can oft en be excised via a lateral orbitotomy as demonstrated above. Glioma visible in front of retractor (see arrow). Removal of the lateral wall in children may not be necessary due to the shallow orbit in this age group (From Katowitz [23]. With per-mission from Springer)
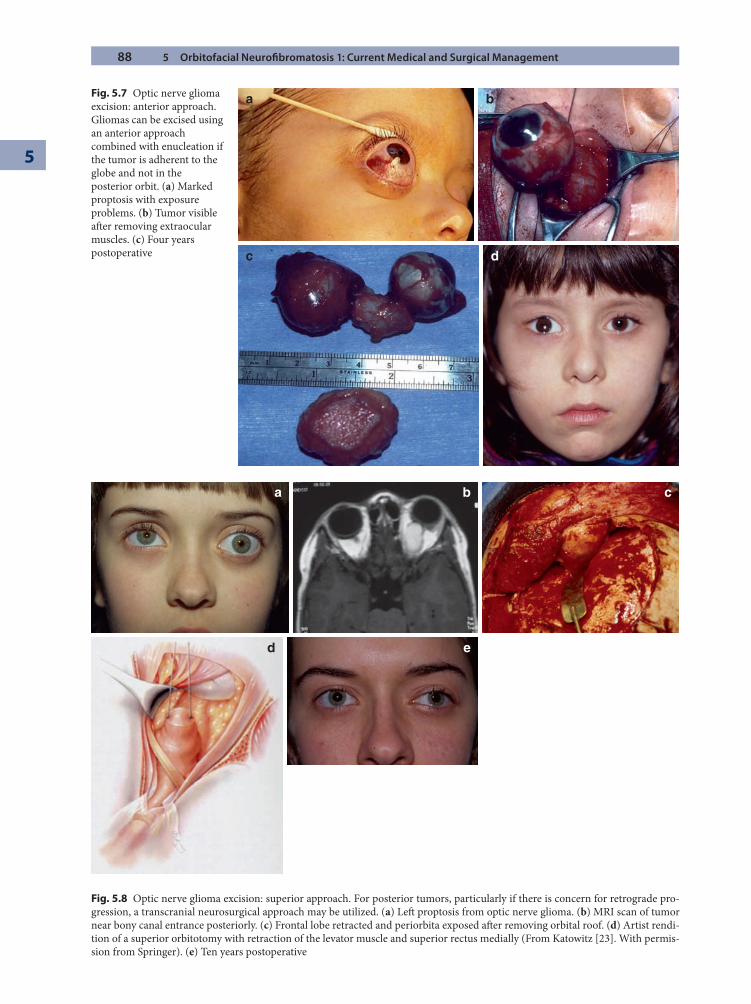
88 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
a
c d
bFig. 5.7 Optic nerve glioma excision: anterior approach. Gliomas can be excised using an anterior approach combined with enucleation if the tumor is adherent to the globe and not in the posterior orbit. (a) Marked proptosis with exposure problems. (b) Tumor visible aft er removing extraocular muscles. (c) Four years postoperative
a b
ed
c
Fig. 5.8 Optic nerve glioma excision: superior approach. For posterior tumors, particularly if there is concern for retrograde pro-gression, a transcranial neurosurgical approach may be utilized. (a) Left proptosis from optic nerve glioma. (b) MRI scan of tumor near bony canal entrance posteriorly. (c) Frontal lobe retracted and periorbita exposed aft er removing orbital roof. (d) Artist rendi-tion of a superior orbitotomy with retraction of the levator muscle and superior rectus medially (From Katowitz [23]. With permis-sion from Springer). (e) Ten years postoperative
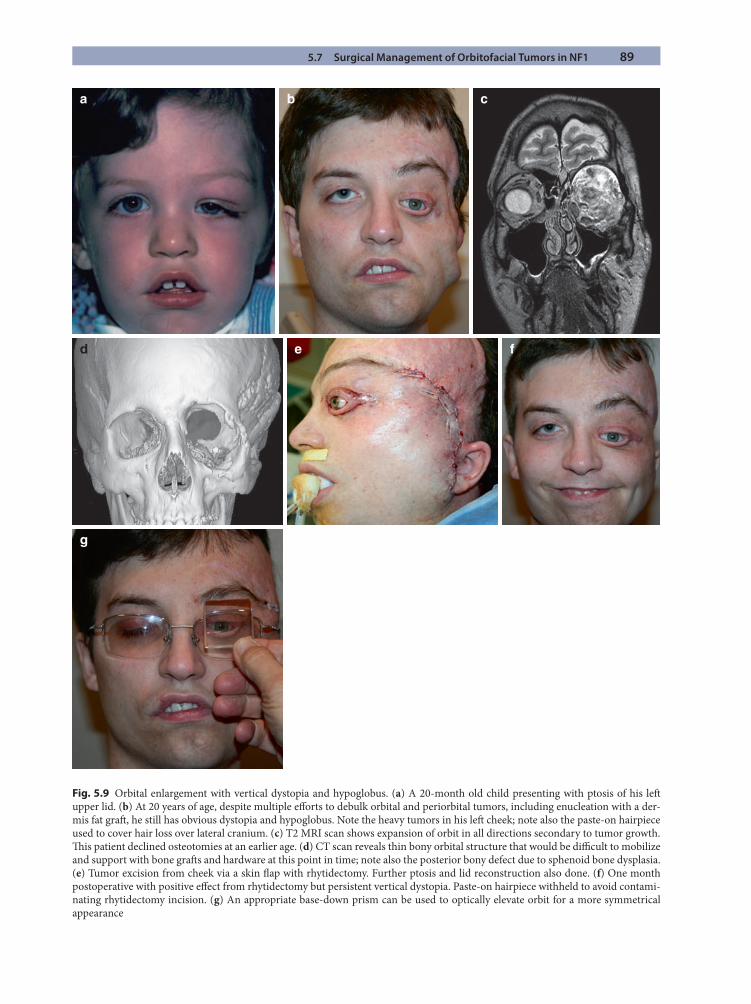
5.7 Surgical Management of Orbitofacial Tumors in NF1 89
a
e
g
fd
b c
Fig. 5.9 Orbital enlargement with vertical dystopia and hypoglobus. (a) A 20-month old child presenting with ptosis of his left upper lid. (b) At 20 years of age, despite multiple eff orts to debulk orbital and periorbital tumors, including enucleation with a der-mis fat graft , he still has obvious dystopia and hypoglobus. Note the heavy tumors in his left cheek; note also the paste-on hairpiece used to cover hair loss over lateral cranium. (c) T2 MRI scan shows expansion of orbit in all directions secondary to tumor growth. Th is patient declined osteotomies at an earlier age. (d) CT scan reveals thin bony orbital structure that would be diffi cult to mobilize and support with bone graft s and hardware at this point in time; note also the posterior bony defect due to sphenoid bone dysplasia. (e) Tumor excision from cheek via a skin fl ap with rhytidectomy. Further ptosis and lid reconstruction also done. (f) One month postoperative with positive eff ect from rhytidectomy but persistent vertical dystopia. Paste-on hairpiece withheld to avoid contami-nating rhytidectomy incision. (g) An appropriate base-down prism can be used to optically elevate orbit for a more symmetrical appearance

90 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
Surgery to decrease the diameter of the bony orbital entrance or to signifi cantly build up the orbital fl oor to reduce volume requires an experienced craniofacial sur-gical team. Because of the high vascularity of NF tumors, the risks of extensive blood loss is always a major concern. Surgery to alter the bony orbit is diffi cult but can be eff ec-tive in selected cases [20, 42]. A major problem with early osteotomies to reduce the orbital rim diameter or to shift the orbit up, however, is in determining how progressive and destructive any given orbital process will become. Th e problem with deferring orbital bone surgery to a later adult stage is that over time, with the gradual expansion of soft tissue tumor growth, the bony rims become thin and brittle. Th is adds to the surgical diffi culties given the pro-pensity for major loss of blood in the NF1 patient. Another factor is that while most adult patients and parents of aff ected children accept the concept of multiple soft tissue procedures, they are usually more reticent to undergo major orbital bony reconstruction when presented with the risk–benefi t ratios and the prolonged postoperative course of major craniofacial reconstruction.
Elevation of the canthi rather than onlay graft s to the orbital fl oor or sectioning the orbital rims to achieve a smaller diameter is an alternative that can yield a reason-able result in many instances but may require wiring of the canthi into a higher position on the bony orbit. Even with this approach, there is a tendency for a downward drift over time. Th is is compounded by the gravitational pull of tumors in the cheek and lower face that can add to this downward drift . Care must be taken to protect the lacrimal drainage system during medial canthopexy, and bicanali-cular silastic intubation may be of value for this purpose.
Further support of the lower lid and canthi with an autogenous fascia lata sling can be a useful adjunct. When there is still a noticeable vertical dystopia, use of a base-down prism in spectacles can also produce a more sym-metric appearance if the patient does not wish to proceed with craniofacial bony reconstruction for this aspect of orbitofacial rehabilitation (Fig. 5.9g).
5.8 The Natural History of NF1 Tumor Growth from Birth to Senescence
Growth or progression of NF1 tumors aff ecting the orb-itofacial region is generally considered to begin in the fi rst few years of life and then to advance more rapidly with natural growth spurts, slowing in the third decade of life. Unfortunately, there are no published studies docu-menting the long-term eff ects of NF1 in a large series of patients with multidecade follow-up. We have had a somewhat unusual opportunity, however, to observe the evolution and progression of NF1 tumors in such a patient over a period of more than 60 years (Fig. 5.10). What is evident from this case is that NF1 tumor growth does not always slow in progression aft er the second decade. Although we have photographic documentation of his appearance at 2 years of age, our direct experience with this patient began at age 37 when our surgical team fi rst had the opportunity to evaluate him and then to perform
Summary for the Clinician
It is not necessary to delay surgical intervention ■
for disfi guring NF1 tumors.Patients and families oft en seek early interven- ■
tion and are willing to tolerate the likelihood of multiple procedures.When approaching disfi guring proptosis, the sur- ■
geon must counsel the patient and family regard-ing the visual prognosis and weigh the overall benefi t of removing an eye to rehabilitate a patient’s comfort, self-perception, and appearance.Orbital exenteration can be avoided except for ■
cases of malignancy.Patients with NF1 require a lifetime of follow-up ■
due to the tendency of tumor progression, recur-rence, and involvement of other organ systems.
Fig. 5.10 NF1 tumor growth from birth to senescence. (a) Patient at age 2 with obvious NF1 tumor presentation. (b) Appearance 35 years later at age 37 aft er multiple procedures elsewhere. Th ese included a neurosurgical excision of tumor involving cranial bone on the left side. (c) Coronal CT scan shows missing left cranial bone due to infected metal plate with subsequent removal. (d) Patient at 2 months aft er combined team approach for excision of tumors in scalp, cheek, and orbit, including enucleation with a dermis fat graft implant. (e) Transposition fl ap moved from lower to upper lid with lateral canthopexy. (f) Transposition fl aps sutured into place. (g) Patient at 2 years postoperative (age 39); note that skin and cheeks are relatively free of tumor. (h) Patient now 20 years postprocedure (age 60); note the cutaneous neurofi bromas now aff ecting both sides of his face as well as the deeper left cheek tumors. (i) Severe enophthalmic appearance due to presumed atrophy of orbital soft tissues. (j) Scan actually reveals healthy dermis fat graft placed 20 years previously with signifi cant atrophy of the temporal lobe as the cause of the enophthalmos due to a direct communication of orbital contents through an aplastic sphenoid bone defect. (k) Large dermis fat graft from inguinal area has been placed in orbit to repair enophthamic appearance. (l) Patient at 2 months post-op and age 61 years. Note that despite orbital dystopia in this case, the canthi have remained in a relatively symmetrical position, possibly related to use of a fascia lata sling with canthopexy repair
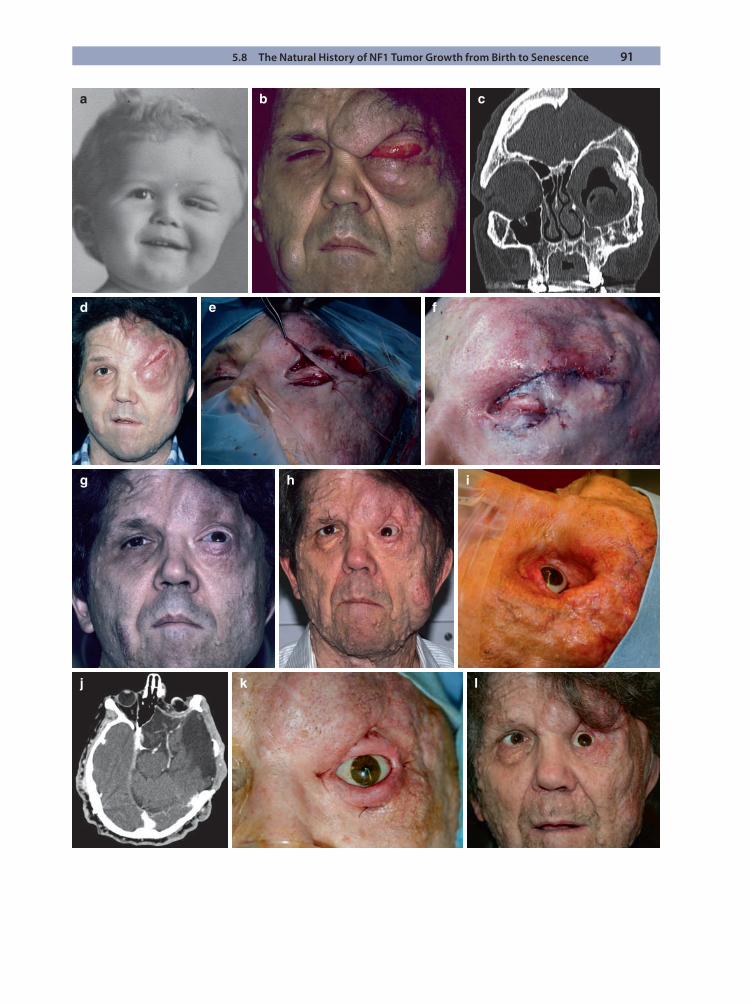
5.8 The Natural History of NF1 Tumor Growth from Birth to Senescence 91
a b c
d e f
g h i
j k l

92 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
major orbitofacial tumor resection and reconstruction. Underscoring the problems with potential blood loss in the NF1 patient, his fi rst procedure involved replacement of eight units of blood and then an additional four units postoperatively. At age 60, he presented with marked enopthalmos in his enucleated left socket, with his pros-thesis lying fl at in the socket, presumably due to orbital fat atrophy. Imaging, however, revealed this not to be due to atrophy of his dermis fat graft or orbital fat but to fur-ther atrophy of his temporal lobe, with the orbital con-tents herniating through the opening in his aplastic sphenoid bone. A large dermis fat graft from the inguinal region was placed to fi ll the upper lid sulcus and periorbit along with additional lid reconstruction to permit better positioning of his prosthesis. His appearance was further marred by the progression of cutaneous neurofi bromas on both the right side of his face and his left as compared to his facial appearance 25 years earlier.
Th is case illustrates that NF1 tumors, although they may well be benign initially, can continue to manifest in the orbit and elsewhere for decades. It must be recognized
that the risks for secondary malignancy, whether in sheath tumors, in secondary central nervous system tumors, or in other more distant locations, are of real sig-nifi cance, particularly in NF1 patients, thus mandating careful follow-up evaluations [44].
References
1. Babovic-Vuksanovic D, Ballman K, Michels V, et al (2006) Phase II trial of pirfenidone in adults with neurofi broma-tosis type 1. Neurology 67(10):1860–1862
2. Balcer LJ, Liu GT, Heller G, Bilaniuk L, Volpe NK, Galetta SL, et al (2001) Visual loss in children with neuro-fi bromatosis type 1 and optic pathway gliomas: relation to tumor location by magnetic resonance imaging. Am J Ophthalmol 131:442–445
3. Batchelor TT, Sorensen AG, di Tomaso E, et al (2007) AZD2171, a pan-VEGF receptor tyrosine kinase inhibitor, normalizes tumor vasculature and alleviates edema in glio-blastoma patients. Cancer Cell 11(1):83–95
4. Bellasco J (2009) Children’s Hospital of Philadelphia. Personal correspondence
5. Brems H, Chmara M, Sahbatou M, Denayer E, Taniguchi K, Kato R, Somers R, Messiaen L, De Schepper S, Fryns JP, Cools J, Marynen P, Th omas G, Yoshimura A, Legius E (2007) Germline loss-of-function mutations in SPRED1 cause a neurofi bromatosis 1 like phenotype. Nat Genet 39(9):11120–1126
6. Burnstine MA, Levine LA, Louis DN, et al (1993) Nucleolar organizer regions in optic gliomas. Brain 116:1465–1476
7. Cummings TJ, Provenzale JM, Hunter SB, et al (1987) Magnetic resonance imaging in the evaluation of optic nerve gliomas. Ophthalmology 94:709–717
8. Cunha KS, Barboza EP, Fonseca EC (2008) Identifi cation of growth hormone receptor in plexiform neurofi bromas of patients with neurofi bromatosis type 1. Clinics 63:39–42
9. Dasgupta B, Dugan LL, Gutmann DH (2003) Th e neurofi -bromatosis 1 gene product neurofi bromin regulates pitu-itary adenylate cyclase-activating polypeptide-mediated signaling in astrocytes. J Neurosci 23(26):8949–8954
10. Dilenge D, Saraux H, Simon J, Calabro A (1965) Bilateral oculofacial form of neurofi bromatosis. J Radiol Electrol Med Nucl 46:143–146
11. Ducatman BS, Scheithauer BW, Piepgras DG, Reiman HM, Ilstrup DM (1986) Malignant peripheral nerve sheath tumors. Cancer 57:2006–2021
12. Erb MH, Uzcategui N (2007) Orbitotemporal neurofi bro-matosis: classifi cation and treatment. Orbit 26:223–228
13. Evans DG, Baser ME, McGaughran J, Sharif S, Howard E, Moran A (2002) Malignant peripheral nerve sheath tumors in neurofi bromatosis 1. J Med Genet 39(5):311–314
Summary for the Clinician
Patients who suff er from NF1 present with a var- ■
ied course that oft en involves tumor progression.New understanding of intracellular pathways ■
and abnormal genes may allow future treatments to better target these tumors.While some authors recommend deferring ■
defi nitive reconstructive surgery until aft er puberty, we believe that early intervention can better control expansion of soft tissues and pos-sibly reduce bony orbital expansion.Of major importance, in addition to functional ■
concerns, is the need to recognize the value of orbitofacial rehabilitation from an appearance perspective. Improving appearance is usually of critical importance to both the patient and family.It is critical to counsel older patients and the par- ■
ents of young children regarding the likely neces-sity for multiple reconstructive procedures in the eff ort to approach normal orbitofacial function and appearance.It is also critical that NF1 patients be followed ■
carefully from a systemic medical perspective during the entire lifetime as there are numerous secondary problems related to NF1 that may become manifest at any time.
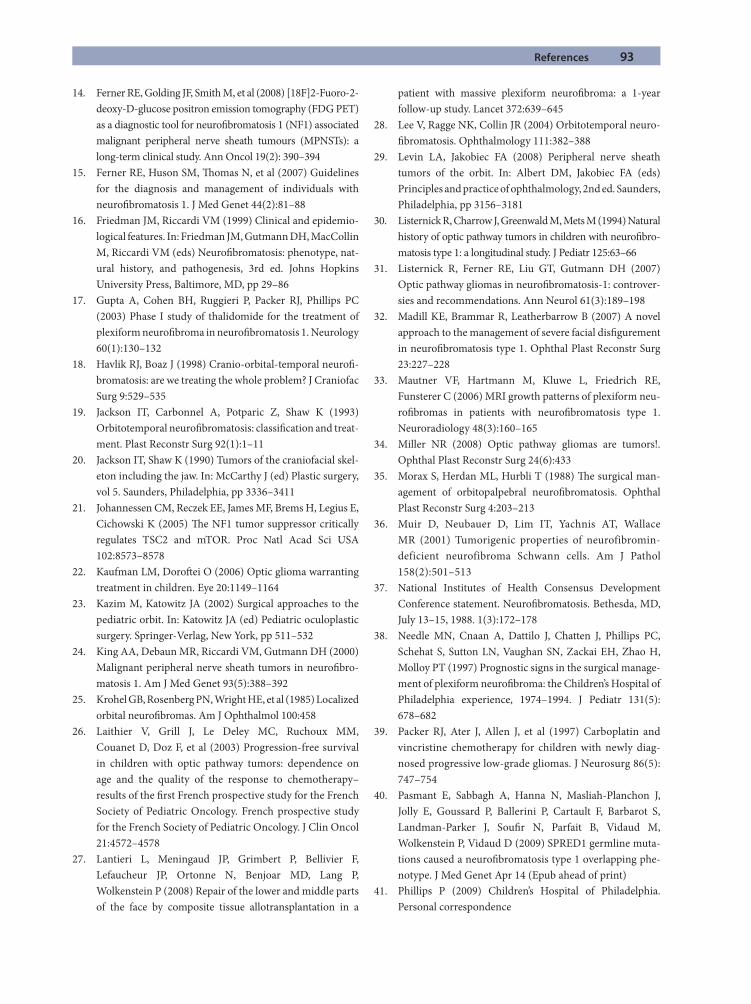
References 93
14. Ferner RE, Golding JF, Smith M, et al (2008) [18F]2-Fuoro-2-deoxy-D-glucose positron emission tomography (FDG PET) as a diagnostic tool for neurofi bromatosis 1 (NF1) associated malignant peripheral nerve sheath tumours (MPNSTs): a long-term clinical study. Ann Oncol 19(2): 390–394
15. Ferner RE, Huson SM, Th omas N, et al (2007) Guidelines for the diagnosis and management of individuals with neurofi bromatosis 1. J Med Genet 44(2):81–88
16. Friedman JM, Riccardi VM (1999) Clinical and epidemio-logical features. In: Friedman JM, Gutmann DH, MacCollin M, Riccardi VM (eds) Neurofi bromatosis: phenotype, nat-ural history, and pathogenesis, 3rd ed. Johns Hopkins University Press, Baltimore, MD, pp 29–86
17. Gupta A, Cohen BH, Ruggieri P, Packer RJ, Phillips PC (2003) Phase I study of thalidomide for the treatment of plexiform neurofi broma in neurofi bromatosis 1. Neurology 60(1):130–132
18. Havlik RJ, Boaz J (1998) Cranio-orbital-temporal neurofi -bromatosis: are we treating the whole problem? J Craniofac Surg 9:529–535
19. Jackson IT, Carbonnel A, Potparic Z, Shaw K (1993) Orbitotemporal neurofi bromatosis: classifi cation and treat-ment. Plast Reconstr Surg 92(1):1–11
20. Jackson IT, Shaw K (1990) Tumors of the craniofacial skel-eton including the jaw. In: McCarthy J (ed) Plastic surgery, vol 5. Saunders, Philadelphia, pp 3336–3411
21. Johannessen CM, Reczek EE, James MF, Brems H, Legius E, Cichowski K (2005) Th e NF1 tumor suppressor critically regulates TSC2 and mTOR. Proc Natl Acad Sci USA 102:8573–8578
22. Kaufman LM, Doroft ei O (2006) Optic glioma warranting treatment in children. Eye 20:1149–1164
23. Kazim M, Katowitz JA (2002) Surgical approaches to the pediatric orbit. In: Katowitz JA (ed) Pediatric oculoplastic surgery. Springer-Verlag, New York, pp 511–532
24. King AA, Debaun MR, Riccardi VM, Gutmann DH (2000) Malignant peripheral nerve sheath tumors in neurofi bro-matosis 1. Am J Med Genet 93(5):388–392
25. Krohel GB, Rosenberg PN, Wright HE, et al (1985) Localized orbital neurofi bromas. Am J Ophthalmol 100:458
26. Laithier V, Grill J, Le Deley MC, Ruchoux MM, Couanet D, Doz F, et al (2003) Progression-free survival in children with optic pathway tumors: dependence on age and the quality of the response to chemotherapy–results of the fi rst French prospective study for the French Society of Pediatric Oncology. French prospective study for the French Society of Pediatric Oncology. J Clin Oncol 21:4572–4578
27. Lantieri L, Meningaud JP, Grimbert P, Bellivier F, Lefaucheur JP, Ortonne N, Benjoar MD, Lang P, Wolkenstein P (2008) Repair of the lower and middle parts of the face by composite tissue allotransplantation in a
patient with massive plexiform neurofi broma: a 1-year follow-up study. Lancet 372:639–645
28. Lee V, Ragge NK, Collin JR (2004) Orbitotemporal neuro-fi bromatosis. Ophthalmology 111:382–388
29. Levin LA, Jakobiec FA (2008) Peripheral nerve sheath tumors of the orbit. In: Albert DM, Jakobiec FA (eds) Principles and practice of ophthalmology, 2nd ed. Saunders, Philadelphia, pp 3156–3181
30. Listernick R, Charrow J, Greenwald M, Mets M (1994) Natural history of optic pathway tumors in children with neurofi bro-matosis type 1: a longitudinal study. J Pediatr 125:63–66
31. Listernick R, Ferner RE, Liu GT, Gutmann DH (2007) Optic pathway gliomas in neurofi bromatosis-1: controver-sies and recommendations. Ann Neurol 61(3):189–198
32. Madill KE, Brammar R, Leatherbarrow B (2007) A novel approach to the management of severe facial disfi gurement in neurofi bromatosis type 1. Ophthal Plast Reconstr Surg 23:227–228
33. Mautner VF, Hartmann M, Kluwe L, Friedrich RE, Funsterer C (2006) MRI growth patterns of plexiform neu-rofi bromas in patients with neurofi bromatosis type 1. Neuroradiology 48(3):160–165
34. Miller NR (2008) Optic pathway gliomas are tumors!. Ophthal Plast Reconstr Surg 24(6):433
35. Morax S, Herdan ML, Hurbli T (1988) Th e surgical man-agement of orbitopalpebral neurofi bromatosis. Ophthal Plast Reconstr Surg 4:203–213
36. Muir D, Neubauer D, Lim IT, Yachnis AT, Wallace MR (2001) Tumorigenic properties of neurofibromin-deficient neurofibroma Schwann cells. Am J Pathol 158(2):501–513
37. National Institutes of Health Consensus Development Conference statement. Neurofi bromatosis. Bethesda, MD, July 13–15, 1988. 1(3):172–178
38. Needle MN, Cnaan A, Dattilo J, Chatten J, Phillips PC, Schehat S, Sutton LN, Vaughan SN, Zackai EH, Zhao H, Molloy PT (1997) Prognostic signs in the surgical manage-ment of plexiform neurofi broma: the Children’s Hospital of Philadelphia experience, 1974–1994. J Pediatr 131(5): 678–682
39. Packer RJ, Ater J, Allen J, et al (1997) Carboplatin and vincristine chemotherapy for children with newly diag-nosed progressive low-grade gliomas. J Neurosurg 86(5): 747–754
40. Pasmant E, Sabbagh A, Hanna N, Masliah-Planchon J, Jolly E, Goussard P, Ballerini P, Cartault F, Barbarot S, Landman-Parker J, Soufi r N, Parfait B, Vidaud M, Wolkenstein P, Vidaud D (2009) SPRED1 germline muta-tions caused a neurofi bromatosis type 1 overlapping phe-notype. J Med Genet Apr 14 (Epub ahead of print)
41. Phillips P (2009) Children’s Hospital of Philadelphia. Personal correspondence
94 5 Orbitofacial Neurofi bromatosis 1: Current Medical and Surgical Management
5
42. Posnick JC (2000) Other frequently seen craniofacial syn-dromes. In: Posnick JC (ed) Surgery in children and young adults. Saunders, Philadelphia, pp 503–527
43. Reynolds RM, Browning GG, Nawroz I, Campbell IW (2003) Von Recklinghausen’s neurofi bromatosis type 1. Lancet 361(9368):1552–1554
44. Singhal S, Birch JM, Kerr B, Lashford L, Evans DG (2002) Neurofi bromatosis type 1 and sporadic gliomas. Arch Dis Child 87:65–70
45. Stephens K, Kayes L, Riccardi VM, Rising M, Sybert VP, Pagon RA (1992) Preferential mutation of the neurofi bro-matosis type 1 gene in paternally derived chromosomes. Hum Genet 88(3):279–282
46. Van der Meulen JC, Moscona AR, Vaandrager M, Hirshowitz B (1982) Th e management of orbitofacial neu-rofi bromatosis. Ann Plast Surg 8:213–220
47. Walrath JD, Engelbert M, Kazim M (2008) Magnetic reso-nance imaging evidence of optic nerve glioma progression into and beyond the optic chiasm. Ophthal Plast Reconstr Surg 24:473–474
48. Ward BA, Gutmann DH (2005) Neurofi bromatosis 1: from lab bench to clinic. Pediatr Neurol 32:221–228
49. Widemann BC, Salzer WL, Arceci RJ, et al (2006) Phase I trial and pharmacokinetic study of the farnesyltransferase inhibitor tipifarnib in children with refractory solid tumors or neurofi bromatosis type I and plexiform neurofi bromas. J Clin Oncol 24(3):507–516
50. Williams VC, Lucas J, Babcock MA, Gutmann DH, Korf B, Maria BL (2009) Neurofi bromatosis type 1 revisited. Pediatrics 123:124–133
Clinicopathologic Features of Lesions Aff ecting the Lacrimal Drainage System in External DacryocystorhinostomyLudwig M. Heindl, Anselm G. M. Jünemann, and Leonard M. Holbach
Chapter 6
6.1 Introduction
Disorders of the lacrimal drainage system (Table 6.1), which cause epiphora, punctal discharge, or medial can-thal swelling, are common ophthalmic complaints com-prising approximately 3% of clinic visits in some series [8, 21]. Th e most common histopathologic fi ndings in primary acquired nasolacrimal duct obstruction include chronic infl ammation and fi brosis leading to occlusion of the lacrimal drainage system [7, 12, 13]. Secondary causes of dacryostenosis may be the result of neoplasms, systemic infl ammatory diseases, infections, or trauma [2, 19].
Neoplasms that aff ect the lacrimal drainage system are rare, but potentially life-threatening, so early diagnosis and treatment are particularly important [17, 23]. Almost 500 primary lacrimal sac tumors have been reported and were malignant in about 55% of the cases [6, 9, 10, 17–19]. Epithelial neoplasms are most common (73%), including benign (squamous cell papilloma, transitional cell papil-
loma, mixed-cell papilloma, oncocytoma) and malignant (squamous cell carcinoma, transitional cell carcinoma, adenocarcinoma, mucoepidermoid carcinoma, oncocytic adenocarcinoma) tumors [6, 9, 10, 17–19]. Mesenchymal tumors such as fi brous histiocytoma, fi broma, heman-gioma, hemangiopericytoma, angiosarcoma, or lipoma are less common (14%), and the rarer tumors include lymphomas (8%), malignant melanomas (4%), and neu-ral tumors (1%) (Table 6.2) [6, 9, 10, 17–19]. Secondary tumors originating in adjacent structures (paranasal sinuses, orbit, nose) may extend into the lacrimal sac [6, 9, 10, 17–19]. Metastatic neoplasms confi ned to the lacri-mal sac are extremely rare, and most metastases also aff ect adjacent structures, such as the eyelid, nose, sinuses, and orbit [6, 9, 10, 17–19].
Infl ammatory lesions, including nonspecifi c chronic infl ammation (“pseudotumor”) or granulomatous dis-ease, are not true neoplasms but may present as lacrimal sac masses and may be a sign of systemic diseases that require further medical treatment [6, 17–19].
6
Core Messages
Diff erential diagnostic symptoms and signs in ■
favor of a tumor of the lacrimal sac include a swell-ing above the medial canthal tendon, the presence of telangiectases in the skin overlying the mass, and the presence of serosanguinous discharge or a bloody refl ux with atraumatic irrigation.All patients should be asked for a history of pre- ■
disposing conditions, such as systemic diseases (e.g., lymphoma, Wegener granulomatosis, sar-coidosis) or neoplasms.External dacryocystorhinostomy (DCR) allows ■
detailed inspection of the lacrimal sac and ade-quate tissue biopsy.
Lacrimal sac biopsy should be considered selec- ■
tively in patients with atypical clinical or intraop-erative fi ndings or in those with a history of predisposing systemic diseases.Biopsy results may help to defi ne the degree of ■
active specifi c infl ammation requiring further chemo- or immunotherapy postoperatively.Selective lacrimal sac biopsy permits early diagno- ■
sis of potentially life-threatening malignant tumors to determine further defi nitive management.
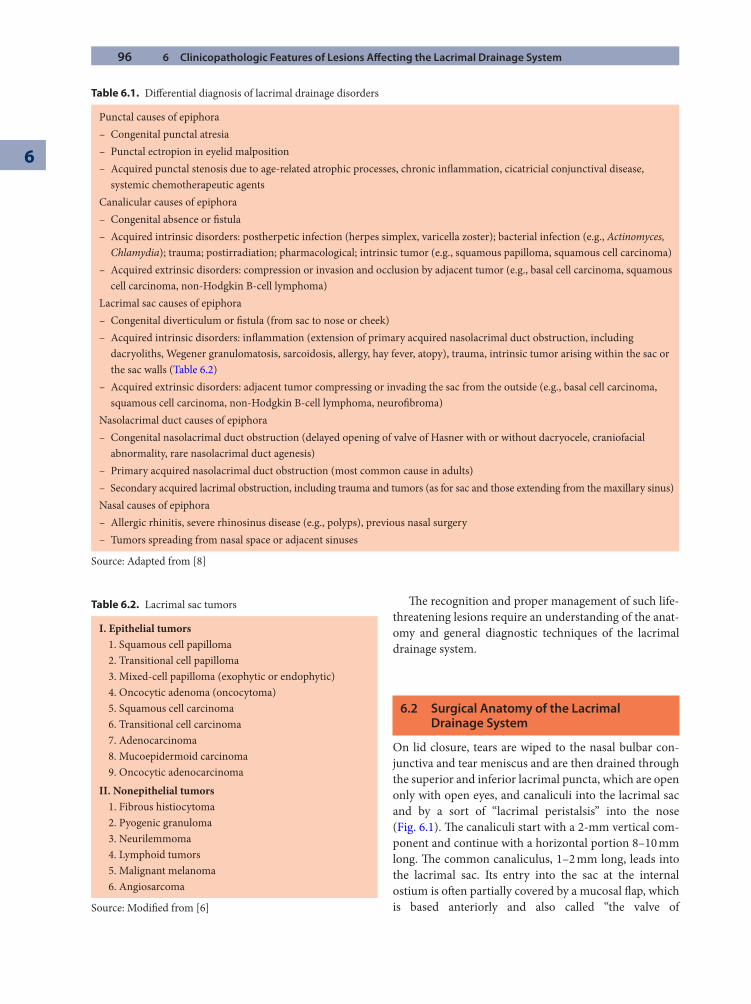
96 6 Clinicopathologic Features of Lesions Aff ecting the Lacrimal Drainage System
6
Table 6.1. Diff erential diagnosis of lacrimal drainage disorders
Punctal causes of epiphora– Congenital punctal atresia– Punctal ectropion in eyelid malposition– Acquired punctal stenosis due to age-related atrophic processes, chronic infl ammation, cicatricial conjunctival disease,
systemic chemotherapeutic agentsCanalicular causes of epiphora– Congenital absence or fi stula– Acquired intrinsic disorders: postherpetic infection (herpes simplex, varicella zoster); bacterial infection (e.g., Actinomyces,
Chlamydia); trauma; postirradiation; pharmacological; intrinsic tumor (e.g., squamous papilloma, squamous cell carcinoma)– Acquired extrinsic disorders: compression or invasion and occlusion by adjacent tumor (e.g., basal cell carcinoma, squamous
cell carcinoma, non-Hodgkin B-cell lymphoma)Lacrimal sac causes of epiphora– Congenital diverticulum or fi stula (from sac to nose or cheek)– Acquired intrinsic disorders: infl ammation (extension of primary acquired nasolacrimal duct obstruction, including
dacryoliths, Wegener granulomatosis, sarcoidosis, allergy, hay fever, atopy), trauma, intrinsic tumor arising within the sac or the sac walls (Table 6.2)
– Acquired extrinsic disorders: adjacent tumor compressing or invading the sac from the outside (e.g., basal cell carcinoma, squamous cell carcinoma, non-Hodgkin B-cell lymphoma, neurofi broma)
Nasolacrimal duct causes of epiphora– Congenital nasolacrimal duct obstruction (delayed opening of valve of Hasner with or without dacryocele, craniofacial
abnormality, rare nasolacrimal duct agenesis)– Primary acquired nasolacrimal duct obstruction (most common cause in adults)– Secondary acquired lacrimal obstruction, including trauma and tumors (as for sac and those extending from the maxillary sinus)Nasal causes of epiphora– Allergic rhinitis, severe rhinosinus disease (e.g., polyps), previous nasal surgery– Tumors spreading from nasal space or adjacent sinuses
Source: Adapted from [8]
Table 6.2. Lacrimal sac tumors
I. Epithelial tumors1. Squamous cell papilloma2. Transitional cell papilloma3. Mixed-cell papilloma (exophytic or endophytic)4. Oncocytic adenoma (oncocytoma)5. Squamous cell carcinoma6. Transitional cell carcinoma7. Adenocarcinoma8. Mucoepidermoid carcinoma9. Oncocytic adenocarcinoma
II. Nonepithelial tumors1. Fibrous histiocytoma2. Pyogenic granuloma3. Neurilemmoma4. Lymphoid tumors5. Malignant melanoma6. Angiosarcoma
Source: Modifi ed from [6]
Th e recognition and proper management of such life-threatening lesions require an understanding of the anat-omy and general diagnostic techniques of the lacrimal drainage system.
6.2 Surgical Anatomy of the Lacrimal Drainage System
On lid closure, tears are wiped to the nasal bulbar con-junctiva and tear meniscus and are then drained through the superior and inferior lacrimal puncta, which are open only with open eyes, and canaliculi into the lacrimal sac and by a sort of “lacrimal peristalsis” into the nose (Fig. 6.1). Th e canaliculi start with a 2-mm vertical com-ponent and continue with a horizontal portion 8–10 mm long. Th e common canaliculus, 1–2 mm long, leads into the lacrimal sac. Its entry into the sac at the internal ostium is oft en partially covered by a mucosal fl ap, which is based anteriorly and also called “the valve of
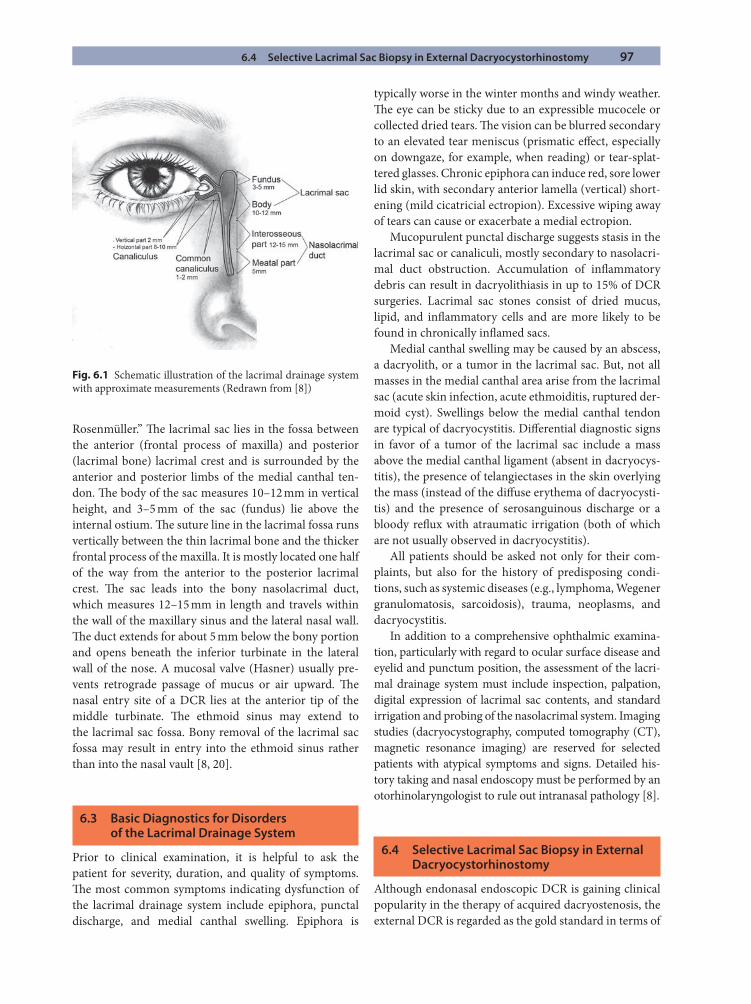
6.4 Selective Lacrimal Sac Biopsy in External Dacryocystorhinostomy 97
Rosenmüller.” Th e lacrimal sac lies in the fossa between the anterior (frontal process of maxilla) and posterior (lacrimal bone) lacrimal crest and is surrounded by the anterior and posterior limbs of the medial canthal ten-don. Th e body of the sac measures 10–12 mm in vertical height, and 3–5 mm of the sac (fundus) lie above the internal ostium. Th e suture line in the lacrimal fossa runs vertically between the thin lacrimal bone and the thicker frontal process of the maxilla. It is mostly located one half of the way from the anterior to the posterior lacrimal crest. Th e sac leads into the bony nasolacrimal duct, which measures 12–15 mm in length and travels within the wall of the maxillary sinus and the lateral nasal wall. Th e duct extends for about 5 mm below the bony portion and opens beneath the inferior turbinate in the lateral wall of the nose. A mucosal valve (Hasner) usually pre-vents retrograde passage of mucus or air upward. Th e nasal entry site of a DCR lies at the anterior tip of the middle turbinate. Th e ethmoid sinus may extend to the lacrimal sac fossa. Bony removal of the lacrimal sac fossa may result in entry into the ethmoid sinus rather than into the nasal vault [8, 20].
6.3 Basic Diagnostics for Disorders of the Lacrimal Drainage System
Prior to clinical examination, it is helpful to ask the patient for severity, duration, and quality of symptoms. Th e most common symptoms indicating dysfunction of the lacrimal drainage system include epiphora, punctal discharge, and medial canthal swelling. Epiphora is
typically worse in the winter months and windy weather. Th e eye can be sticky due to an expressible mucocele or collected dried tears. Th e vision can be blurred secondary to an elevated tear meniscus (prismatic eff ect, especially on downgaze, for example, when reading) or tear-splat-tered glasses. Chronic epiphora can induce red, sore lower lid skin, with secondary anterior lamella (vertical) short-ening (mild cicatricial ectropion). Excessive wiping away of tears can cause or exacerbate a medial ectropion.
Mucopurulent punctal discharge suggests stasis in the lacrimal sac or canaliculi, mostly secondary to nasolacri-mal duct obstruction. Accumulation of infl ammatory debris can result in dacryolithiasis in up to 15% of DCR surgeries. Lacrimal sac stones consist of dried mucus, lipid, and infl ammatory cells and are more likely to be found in chronically infl amed sacs.
Medial canthal swelling may be caused by an abscess, a dacryolith, or a tumor in the lacrimal sac. But, not all masses in the medial canthal area arise from the lacrimal sac (acute skin infection, acute ethmoiditis, ruptured der-moid cyst). Swellings below the medial canthal tendon are typical of dacryocystitis. Diff erential diagnostic signs in favor of a tumor of the lacrimal sac include a mass above the medial canthal ligament (absent in dacryocys-titis), the presence of telangiectases in the skin overlying the mass (instead of the diff use erythema of dacryocysti-tis) and the presence of serosanguinous discharge or a bloody refl ux with atraumatic irrigation (both of which are not usually observed in dacryocystitis).
All patients should be asked not only for their com-plaints, but also for the history of predisposing condi-tions, such as systemic diseases (e.g., lymphoma, Wegener granulomatosis, sarcoidosis), trauma, neoplasms, and dacryocystitis.
In addition to a comprehensive ophthalmic examina-tion, particularly with regard to ocular surface disease and eyelid and punctum position, the assessment of the lacri-mal drainage system must include inspection, palpation, digital expression of lacrimal sac contents, and standard irrigation and probing of the nasolacrimal system. Imaging studies (dacryocystography, computed tomography (CT), magnetic resonance imaging) are reserved for selected patients with atypical symptoms and signs. Detailed his-tory taking and nasal endoscopy must be performed by an otorhinolaryngologist to rule out intranasal pathology [8].
6.4 Selective Lacrimal Sac Biopsy in External Dacryocystorhinostomy
Although endonasal endoscopic DCR is gaining clinical popularity in the therapy of acquired dacryostenosis, the external DCR is regarded as the gold standard in terms of
Fig. 6.1 Schematic illustration of the lacrimal drainage system with approximate measurements (Redrawn from [8])
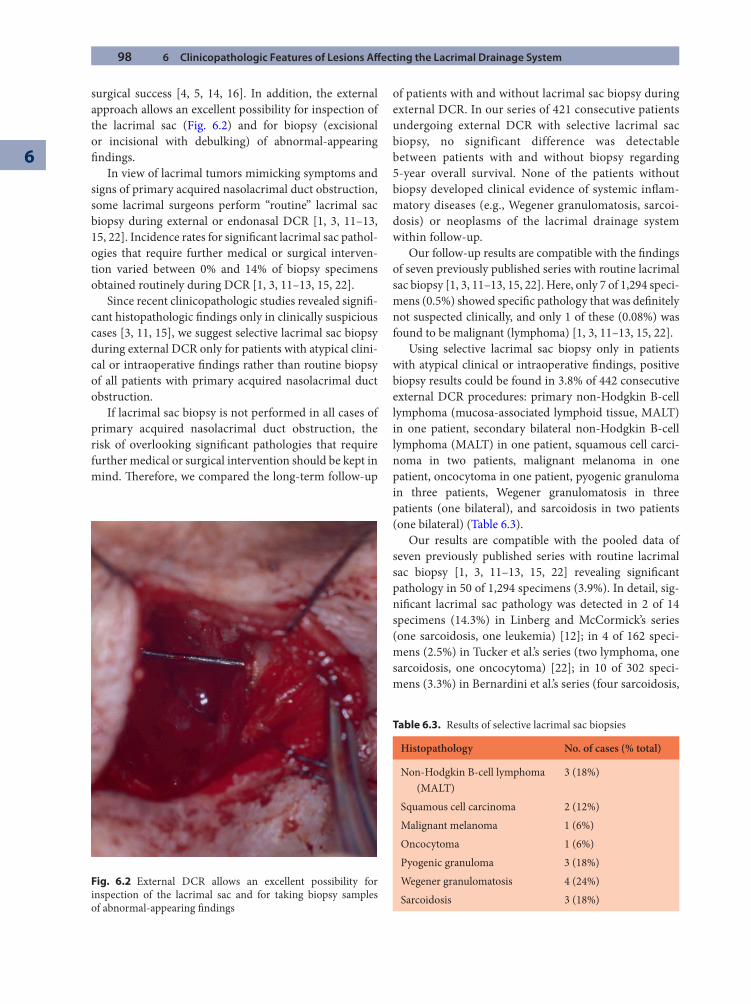
98 6 Clinicopathologic Features of Lesions Aff ecting the Lacrimal Drainage System
6
surgical success [4, 5, 14, 16]. In addition, the external approach allows an excellent possibility for inspection of the lacrimal sac (Fig. 6.2) and for biopsy (excisional or incisional with debulking) of abnormal-appearing fi ndings.
In view of lacrimal tumors mimicking symptoms and signs of primary acquired nasolacrimal duct obstruction, some lacrimal surgeons perform “routine” lacrimal sac biopsy during external or endonasal DCR [1, 3, 11–13, 15, 22]. Incidence rates for signifi cant lacrimal sac pathol-ogies that require further medical or surgical interven-tion varied between 0% and 14% of biopsy specimens obtained routinely during DCR [1, 3, 11–13, 15, 22].
Since recent clinicopathologic studies revealed signifi -cant histopathologic fi ndings only in clinically suspicious cases [3, 11, 15], we suggest selective lacrimal sac biopsy during external DCR only for patients with atypical clini-cal or intraoperative fi ndings rather than routine biopsy of all patients with primary acquired nasolacrimal duct obstruction.
If lacrimal sac biopsy is not performed in all cases of primary acquired nasolacrimal duct obstruction, the risk of overlooking signifi cant pathologies that require further medical or surgical intervention should be kept in mind. Th erefore, we compared the long-term follow-up
of patients with and without lacrimal sac biopsy during external DCR. In our series of 421 consecutive patients undergoing external DCR with selective lacrimal sac biopsy, no significant difference was detectable between patients with and without biopsy regarding 5-year overall survival. None of the patients without biopsy developed clinical evidence of systemic infl am-matory diseases (e.g., Wegener granulomatosis, sarcoi-dosis) or neoplasms of the lacrimal drainage system within follow-up.
Our follow-up results are compatible with the fi ndings of seven previously published series with routine lacrimal sac biopsy [1, 3, 11–13, 15, 22]. Here, only 7 of 1,294 speci-mens (0.5%) showed specifi c pathology that was defi nitely not suspected clinically, and only 1 of these (0.08%) was found to be malignant (lymphoma) [1, 3, 11–13, 15, 22].
Using selective lacrimal sac biopsy only in patients with atypical clinical or intraoperative fi ndings, positive biopsy results could be found in 3.8% of 442 consecutive external DCR procedures: primary non-Hodgkin B-cell lymphoma (mucosa-associated lymphoid tissue, MALT) in one patient, secondary bilateral non-Hodgkin B-cell lymphoma (MALT) in one patient, squamous cell carci-noma in two patients, malignant melanoma in one patient, oncocytoma in one patient, pyogenic granuloma in three patients, Wegener granulomatosis in three patients (one bilateral), and sarcoidosis in two patients (one bilateral) (Table 6.3).
Our results are compatible with the pooled data of seven previously published series with routine lacrimal sac biopsy [1, 3, 11–13, 15, 22] revealing signifi cant pathology in 50 of 1,294 specimens (3.9%). In detail, sig-nifi cant lacrimal sac pathology was detected in 2 of 14 specimens (14.3%) in Linberg and McCormick’s series (one sarcoidosis, one leukemia) [12]; in 4 of 162 speci-mens (2.5%) in Tucker et al.’s series (two lymphoma, one sarcoidosis, one oncocytoma) [22]; in 10 of 302 speci-mens (3.3%) in Bernardini et al.’s series (four sarcoidosis,
Fig. 6.2 External DCR allows an excellent possibility for inspection of the lacrimal sac and for taking biopsy samples of abnormal-appearing fi ndings
Table 6.3. Results of selective lacrimal sac biopsies
Histopathology No. of cases (% total)
Non-Hodgkin B-cell lymphoma (MALT)
3 (18%)
Squamous cell carcinoma 2 (12%)Malignant melanoma 1 (6%)Oncocytoma 1 (6%)Pyogenic granuloma 3 (18%)Wegener granulomatosis 4 (24%)Sarcoidosis 3 (18%)
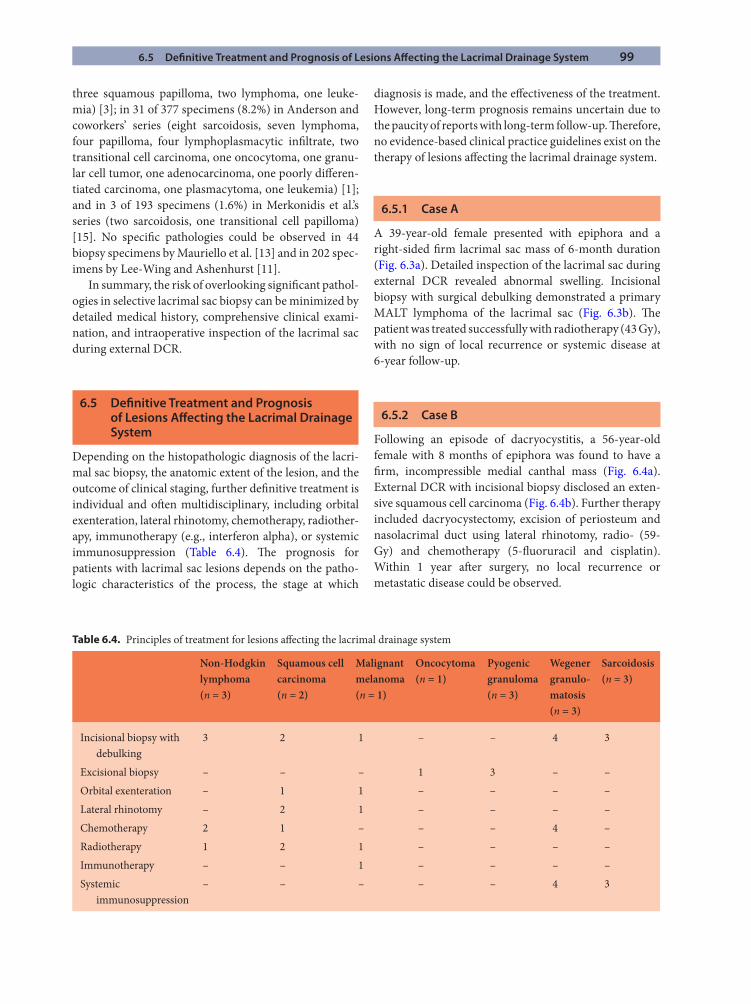
6.5 Defi nitive Treatment and Prognosis of Lesions Aff ecting the Lacrimal Drainage System 99
three squamous papilloma, two lymphoma, one leuke-mia) [3]; in 31 of 377 specimens (8.2%) in Anderson and coworkers’ series (eight sarcoidosis, seven lymphoma, four papilloma, four lymphoplasmacytic infi ltrate, two transitional cell carcinoma, one oncocytoma, one granu-lar cell tumor, one adenocarcinoma, one poorly diff eren-tiated carcinoma, one plasmacytoma, one leukemia) [1]; and in 3 of 193 specimens (1.6%) in Merkonidis et al.’s series (two sarcoidosis, one transitional cell papilloma) [15]. No specifi c pathologies could be observed in 44 biopsy specimens by Mauriello et al. [13] and in 202 spec-imens by Lee-Wing and Ashenhurst [11].
In summary, the risk of overlooking signifi cant pathol-ogies in selective lacrimal sac biopsy can be minimized by detailed medical history, comprehensive clinical exami-nation, and intraoperative inspection of the lacrimal sac during external DCR.
6.5 Defi nitive Treatment and Prognosis of Lesions Aff ecting the Lacrimal Drainage System
Depending on the histopathologic diagnosis of the lacri-mal sac biopsy, the anatomic extent of the lesion, and the outcome of clinical staging, further defi nitive treatment is individual and oft en multidisciplinary, including orbital exenteration, lateral rhinotomy, chemotherapy, radiother-apy, immunotherapy (e.g., interferon alpha), or systemic immunosuppression (Table 6.4). Th e prognosis for patients with lacrimal sac lesions depends on the patho-logic characteristics of the process, the stage at which
diagnosis is made, and the eff ectiveness of the treatment. However, long-term prognosis remains uncertain due to the paucity of reports with long-term follow-up. Th erefore, no evidence-based clinical practice guidelines exist on the therapy of lesions aff ecting the lacrimal drainage system.
6.5.1 Case A
A 39-year-old female presented with epiphora and a right-sided fi rm lacrimal sac mass of 6-month duration (Fig. 6.3a). Detailed inspection of the lacrimal sac during external DCR revealed abnormal swelling. Incisional biopsy with surgical debulking demonstrated a primary MALT lymphoma of the lacrimal sac (Fig. 6.3b). Th e patient was treated successfully with radiotherapy (43 Gy), with no sign of local recurrence or systemic disease at 6-year follow-up.
6.5.2 Case B
Following an episode of dacryocystitis, a 56-year-old female with 8 months of epiphora was found to have a fi rm, incompressible medial canthal mass (Fig. 6.4a). External DCR with incisional biopsy disclosed an exten-sive squamous cell carcinoma (Fig. 6.4b). Further therapy included dacryocystectomy, excision of periosteum and nasolacrimal duct using lateral rhinotomy, radio- (59-Gy) and chemotherapy (5-fl uoruracil and cisplatin). Within 1 year aft er surgery, no local recurrence or metastatic disease could be observed.
Table 6.4. Principles of treatment for lesions aff ecting the lacrimal drainage system
Non-Hodgkin lymphoma (n = 3)
Squamous cell carcinoma (n = 2)
Malignant melanoma (n = 1)
Oncocytoma (n = 1)
Pyogenic granuloma (n = 3)
Wegener granulo-matosis (n = 3)
Sarcoidosis (n = 3)
Incisional biopsy with debulking
3 2 1 – – 4 3
Excisional biopsy – – – 1 3 – –Orbital exenteration – 1 1 – – – –Lateral rhinotomy – 2 1 – – – –Chemotherapy 2 1 – – – 4 –Radiotherapy 1 2 1 – – – –Immunotherapy – – 1 – – – –Systemic
immunosuppression– – – – – 4 3
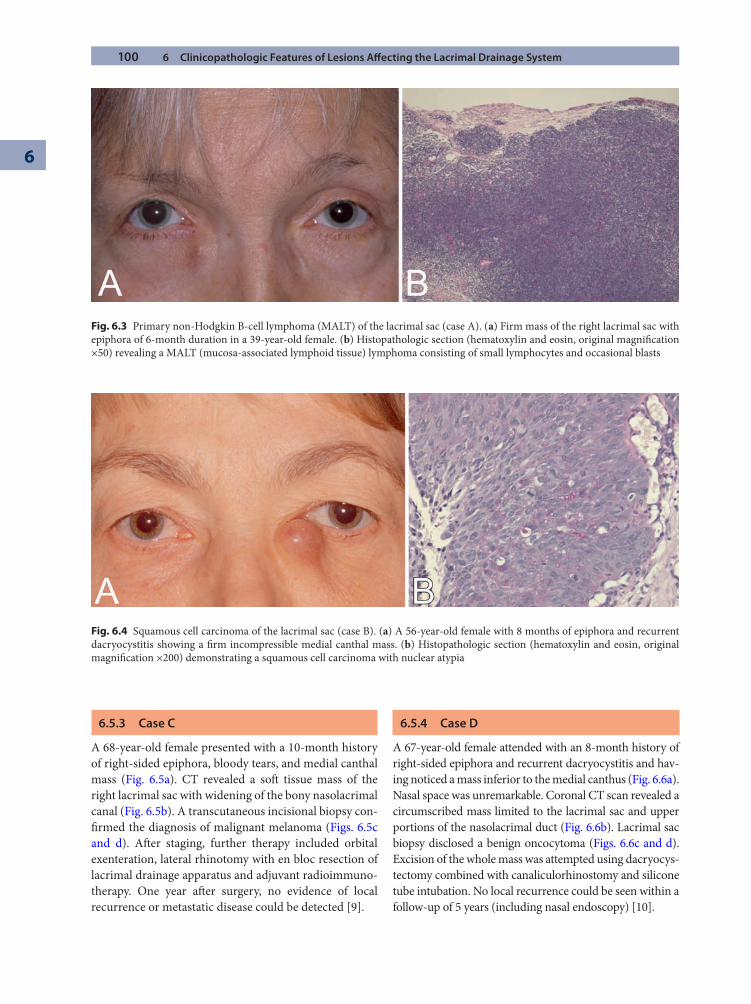
100 6 Clinicopathologic Features of Lesions Aff ecting the Lacrimal Drainage System
6
6.5.3 Case C
A 68-year-old female presented with a 10-month history of right-sided epiphora, bloody tears, and medial canthal mass (Fig. 6.5a). CT revealed a soft tissue mass of the right lacrimal sac with widening of the bony nasolacrimal canal (Fig. 6.5b). A transcutaneous incisional biopsy con-fi rmed the diagnosis of malignant melanoma (Figs. 6.5c and d). Aft er staging, further therapy included orbital exenteration, lateral rhinotomy with en bloc resection of lacrimal drainage apparatus and adjuvant radioimmuno-therapy. One year aft er surgery, no evidence of local recurrence or metastatic disease could be detected [9].
6.5.4 Case D
A 67-year-old female attended with an 8-month history of right-sided epiphora and recurrent dacryocystitis and hav-ing noticed a mass inferior to the medial canthus (Fig. 6.6a). Nasal space was unremarkable. Coronal CT scan revealed a circumscribed mass limited to the lacrimal sac and upper portions of the nasolacrimal duct (Fig. 6.6b). Lacrimal sac biopsy disclosed a benign oncocytoma (Figs. 6.6c and d). Excision of the whole mass was attempted using dacryocys-tectomy combined with canaliculorhinostomy and silicone tube intubation. No local recurrence could be seen within a follow-up of 5 years (including nasal endoscopy) [10].
Fig. 6.3 Primary non-Hodgkin B-cell lymphoma (MALT) of the lacrimal sac (case A). (a) Firm mass of the right lacrimal sac with epiphora of 6-month duration in a 39-year-old female. (b) Histopathologic section (hematoxylin and eosin, original magnifi cation ×50) revealing a MALT (mucosa-associated lymphoid tissue) lymphoma consisting of small lymphocytes and occasional blasts
Fig. 6.4 Squamous cell carcinoma of the lacrimal sac (case B). (a) A 56-year-old female with 8 months of epiphora and recurrent dacryocystitis showing a fi rm incompressible medial canthal mass. (b) Histopathologic section (hematoxylin and eosin, original magnifi cation ×200) demonstrating a squamous cell carcinoma with nuclear atypia
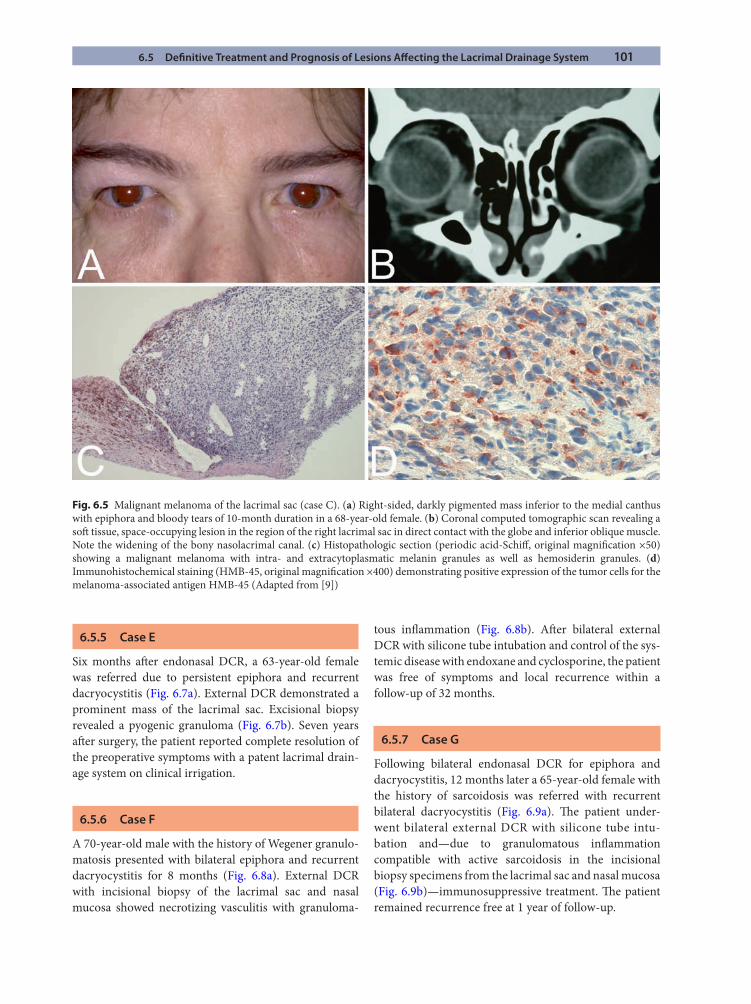
6.5 Defi nitive Treatment and Prognosis of Lesions Aff ecting the Lacrimal Drainage System 101
Fig. 6.5 Malignant melanoma of the lacrimal sac (case C). (a) Right-sided, darkly pigmented mass inferior to the medial canthus with epiphora and bloody tears of 10-month duration in a 68-year-old female. (b) Coronal computed tomographic scan revealing a soft tissue, space-occupying lesion in the region of the right lacrimal sac in direct contact with the globe and inferior oblique muscle. Note the widening of the bony nasolacrimal canal. (c) Histopathologic section (periodic acid-Schiff , original magnifi cation ×50) showing a malignant melanoma with intra- and extracytoplasmatic melanin granules as well as hemosiderin granules. (d) Immunohistochemical staining (HMB-45, original magnifi cation ×400) demonstrating positive expression of the tumor cells for the melanoma-associated antigen HMB-45 (Adapted from [9])
6.5.5 Case E
Six months aft er endonasal DCR, a 63-year-old female was referred due to persistent epiphora and recurrent dacryocystitis (Fig. 6.7a). External DCR demonstrated a prominent mass of the lacrimal sac. Excisional biopsy revealed a pyogenic granuloma (Fig. 6.7b). Seven years aft er surgery, the patient reported complete resolution of the preoperative symptoms with a patent lacrimal drain-age system on clinical irrigation.
6.5.6 Case F
A 70-year-old male with the history of Wegener granulo-matosis presented with bilateral epiphora and recurrent dacryocystitis for 8 months (Fig. 6.8a). External DCR with incisional biopsy of the lacrimal sac and nasal mucosa showed necrotizing vasculitis with granuloma-
tous infl ammation (Fig. 6.8b). Aft er bilateral external DCR with silicone tube intubation and control of the sys-temic disease with endoxane and cyclosporine, the patient was free of symptoms and local recurrence within a follow-up of 32 months.
6.5.7 Case G
Following bilateral endonasal DCR for epiphora and dacryocystitis, 12 months later a 65-year-old female with the history of sarcoidosis was referred with recurrent bilateral dacryocystitis (Fig. 6.9a). Th e patient under-went bilateral external DCR with silicone tube intu-bation and—due to granulomatous infl ammation compatible with active sarcoidosis in the incisional biopsy specimens from the lacrimal sac and nasal mucosa (Fig. 6.9b)—immunosuppressive treatment. Th e patient remained recurrence free at 1 year of follow-up.
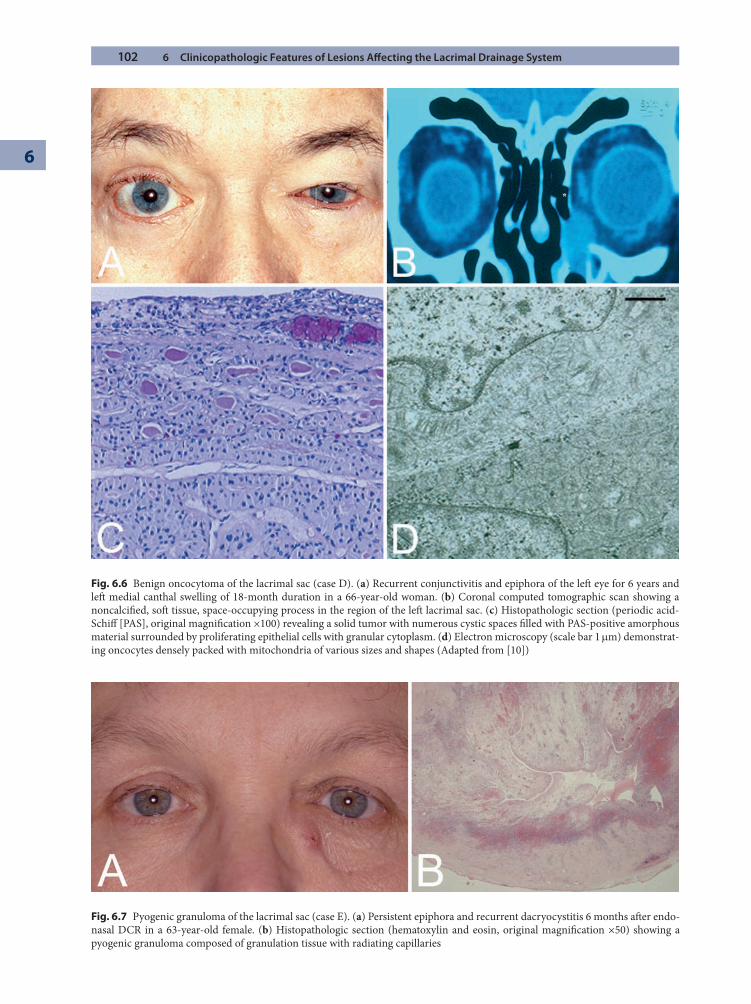
102 6 Clinicopathologic Features of Lesions Aff ecting the Lacrimal Drainage System
6
Fig. 6.6 Benign oncocytoma of the lacrimal sac (case D). (a) Recurrent conjunctivitis and epiphora of the left eye for 6 years and left medial canthal swelling of 18-month duration in a 66-year-old woman. (b) Coronal computed tomographic scan showing a noncalcifi ed, soft tissue, space-occupying process in the region of the left lacrimal sac. (c) Histopathologic section (periodic acid-Schiff [PAS], original magnifi cation ×100) revealing a solid tumor with numerous cystic spaces fi lled with PAS-positive amorphous material surrounded by proliferating epithelial cells with granular cytoplasm. (d) Electron microscopy (scale bar 1 mm) demonstrat-ing oncocytes densely packed with mitochondria of various sizes and shapes (Adapted from [10])
Fig. 6.7 Pyogenic granuloma of the lacrimal sac (case E). (a) Persistent epiphora and recurrent dacryocystitis 6 months aft er endo-nasal DCR in a 63-year-old female. (b) Histopathologic section (hematoxylin and eosin, original magnifi cation ×50) showing a pyogenic granuloma composed of granulation tissue with radiating capillaries
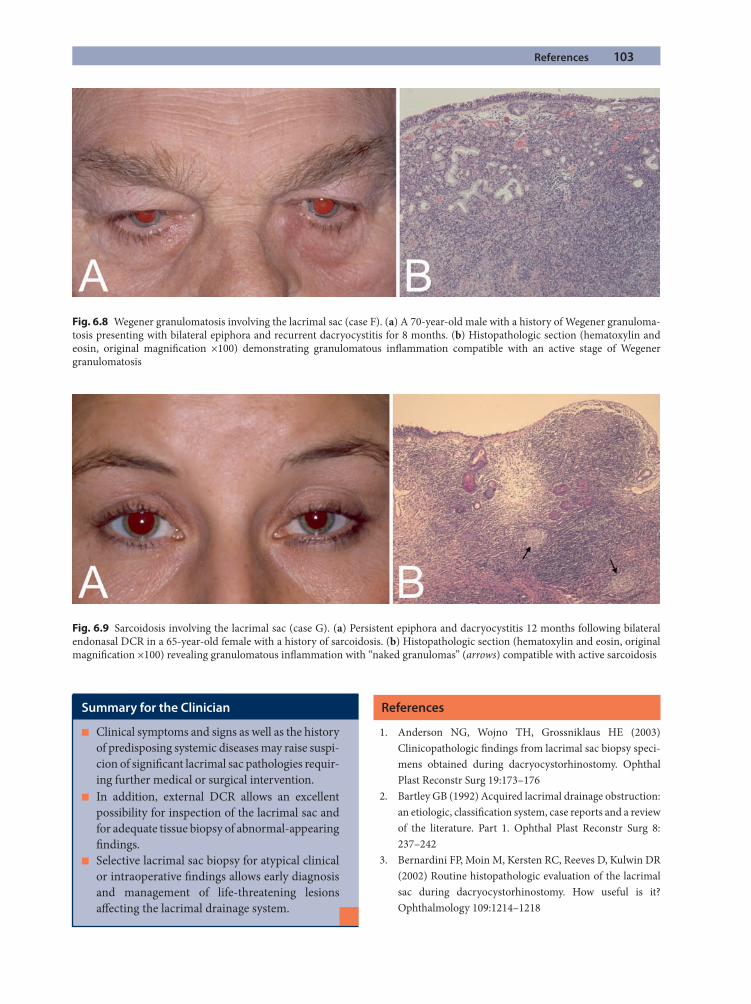
References 103
References
1. Anderson NG, Wojno TH, Grossniklaus HE (2003) Clinicopathologic fi ndings from lacrimal sac biopsy speci-mens obtained during dacryocystorhinostomy. Ophthal Plast Reconstr Surg 19:173–176
2. Bartley GB (1992) Acquired lacrimal drainage obstruction: an etiologic, classifi cation system, case reports and a review of the literature. Part 1. Ophthal Plast Reconstr Surg 8: 237–242
3. Bernardini FP, Moin M, Kersten RC, Reeves D, Kulwin DR (2002) Routine histopathologic evaluation of the lacrimal sac during dacryocystorhinostomy. How useful is it? Ophthalmology 109:1214–1218
Fig. 6.8 Wegener granulomatosis involving the lacrimal sac (case F). (a) A 70-year-old male with a history of Wegener granuloma-tosis presenting with bilateral epiphora and recurrent dacryocystitis for 8 months. (b) Histopathologic section (hematoxylin and eosin, original magnifi cation ×100) demonstrating granulomatous infl ammation compatible with an active stage of Wegener granulomatosis
Fig. 6.9 Sarcoidosis involving the lacrimal sac (case G). (a) Persistent epiphora and dacryocystitis 12 months following bilateral endonasal DCR in a 65-year-old female with a history of sarcoidosis. (b) Histopathologic section (hematoxylin and eosin, original magnifi cation ×100) revealing granulomatous infl ammation with “naked granulomas” (arrows) compatible with active sarcoidosis
Summary for the Clinician
Clinical symptoms and signs as well as the history ■
of predisposing systemic diseases may raise suspi-cion of signifi cant lacrimal sac pathologies requir-ing further medical or surgical intervention.In addition, external DCR allows an excellent ■
possibility for inspection of the lacrimal sac and for adequate tissue biopsy of abnormal-appearing fi ndings.Selective lacrimal sac biopsy for atypical clinical ■
or intraoperative fi ndings allows early diagnosis and management of life-threatening lesions aff ecting the lacrimal drainage system.

104 6 Clinicopathologic Features of Lesions Aff ecting the Lacrimal Drainage System
6
4. Boboridis KG, Bunce C, Rose GE (2005) Outcome of exter-nal dacryocystorhinostomy combined with membranectomy of a distal canalicular obstruction. Am J Ophthalmol 139: 1051–1055
5. Emmerich KH, Busse H, Meyer-Rüsenberg HW (1994) Dacryocystorhinostomia externa. Technique, indications and results [in German]. Ophthalmologe 91:395–398
6. Font RL (1996) Eyelids and lacrimal drainage system. In: Spencer WH (ed) Ophthalmic pathology, vol 4. Saunders, Philadelphia, pp 2412–2427
7. Heindl LM, Jünemann A, Holbach LM (2008) A clinico-pathologic study of nasal mucosa in 350 patients with external dacryocystorhinostomy. Orbit 27(6):462–465
8. Heindl LM, Jünemann A, Holbach LM (2008) Lacrimal drainage system. In: Naumann GOH, Holbach L, Kruse FE (eds) Applied pathology for ophthalmic microsurgeons. Springer, Berlin, pp 45–48
9. Heindl LM, Schick B, Kämpgen E, Kruse FE, Holbach LM (2008) Malignant melanoma of the lacrimal sac [in German]. Ophthalmologe 105(12):1146–1149. (Epub ahead of print)
10. Kottler UB, Schlötzer-Schrehardt U, Holbach LM (2004) Epiphora and conjunctivitis for 6 years [in German]. Ophthalmologe 101:730–732
11. Lee-Wing MW, Ashenhurst ME (2001) Clinicopathologic analysis of 166 patients with primary acquired nasolacri-mal duct obstruction. Ophthalmology 108:2038–2040
12. Linberg JV, McCormick SA (1986) Primary acquired nasolacrimal duct obstruction. A clinicopathologic report and biopsy technique. Ophthalmology 93:1055–1063
13. Mauriello JA, Palydowycz S, DeLuca J (1992) Clinicopatho-logic study of lacrimal sac and nasal mucosa in 44 patients
with complete acquired nasolacrimal duct obstruction. Ophthal Plast Reconstr Surg 8:13–21
14. McNab AA (1994) Manual of orbital and lacrimal surgery. Churchill Livingstone, Edinburgh, pp 75–86
15. Merkonidis C, Brewis C, Yung M, Nussbaumer M (2005) Is routine biopsy of the lacrimal sac wall indicated at dacryo-cystorhinostomy? A prospective study and literature review. Br J Ophthalmol 89:1589–1591
16. Olver J (2002) Colour atlas of lacrimal surgery. Butterworth Heinemann, Oxford, pp 94–114, 158–162
17. Parmar DN, Rose GE (2003) Management of lacrimal sac tumours. Eye 17:599–606
18. Pe’er JJ, Stefanyszyn M, Hidayat AA (1994) Nonepithelial tumors of the lacrimal sac. Am J Ophthalmol 118:650–865
19. Stefanyszyn MA, Hidayat AA, Pe’er JJ, Flanagan JC (1994) Lacrimal sac tumors. Ophthal Plast Reconstr Surg 10: 169–184
20. Th ale A, Paulsen E, Rochels R, Tillmann B (1998) Functional anatomy of the human eff erent tear ducts: a new theory of tear outfl ow mechanism. Graefes Arch Clin Exp Ophthalmol 236:674–678
21. Traquair HM (1941) Chronic dacryocystitis. Its causation and treatment. Arch Ophthalmol 26:165–180
22. Tucker N, Chow D, Stockl F, Codère F, Burnier M (1997). Clinically suspected primary acquired nasolacrimal duct obstruction. Clinicopathologic review of 150 patients. Ophthalmology 104:1882–1886
23. Valenzuela AA, McNab AA, Selva D, O’Donell BA, Whitehead KJ, Sullivan TJ (2006) Clinical features and management of tumors aff ecting the lacrimal drainage apparatus. Ophthal Plast Reconstr Surg 22:96–101
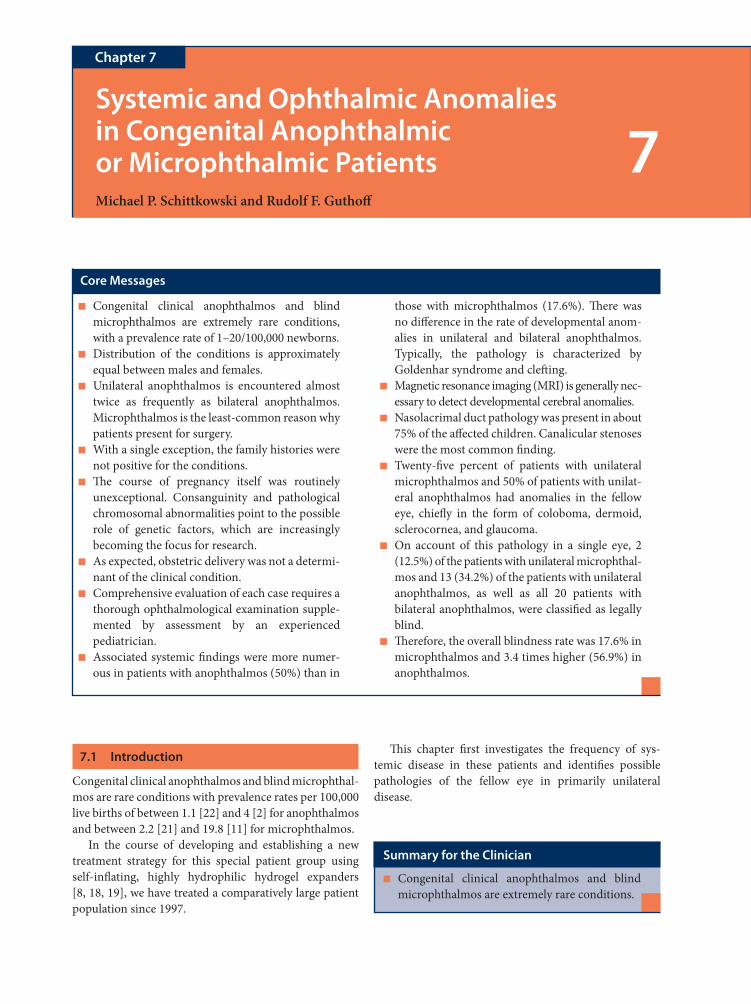
7.1 Introduction
Congenital clinical anophthalmos and blind microphthal-mos are rare conditions with prevalence rates per 100,000 live births of between 1.1 [22] and 4 [2] for anophthalmos and between 2.2 [21] and 19.8 [11] for microphthalmos.
In the course of developing and establishing a new treatment strategy for this special patient group using self-infl ating, highly hydrophilic hydrogel expanders [8, 18, 19], we have treated a comparatively large patient population since 1997.
Th is chapter fi rst investigates the frequency of sys-temic disease in these patients and identifi es possible pathologies of the fellow eye in primarily unilateral disease.
Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic PatientsMichael P. Schittkowski and Rudolf F. Guthoff
Chapter 7
7
Core Messages
Congenital clinical anophthalmos and blind ■
microphthalmos are extremely rare conditions, with a prevalence rate of 1–20/100,000 newborns.Distribution of the conditions is approximately ■
equal between males and females.Unilateral anophthalmos is encountered almost ■
twice as frequently as bilateral anophthalmos. Microphthalmos is the least-common reason why patients present for surgery.With a single exception, the family histories were ■
not positive for the conditions.Th e course of pregnancy itself was routinely ■
unexceptional. Consanguinity and pathological chromosomal abnormalities point to the possible role of genetic factors, which are increasingly becoming the focus for research.As expected, obstetric delivery was not a determi- ■
nant of the clinical condition.Comprehensive evaluation of each case requires a ■
thorough ophthalmological examination supple-mented by assessment by an experienced pediatrician.Associated systemic fi ndings were more numer- ■
ous in patients with anophthalmos (50%) than in
those with microphthalmos (17.6%). Th ere was no diff erence in the rate of developmental anom-alies in unilateral and bilateral anophthalmos. Typically, the pathology is characterized by Goldenhar syndrome and cleft ing.Magnetic resonance imaging (MRI) is generally nec- ■
essary to detect developmental cerebral anomalies.Nasolacrimal duct pathology was present in about ■
75% of the aff ected children. Canalicular stenoses were the most common fi nding.Twenty-fi ve percent of patients with unilateral ■
microphthalmos and 50% of patients with unilat-eral anophthalmos had anomalies in the fellow eye, chiefl y in the form of coloboma, dermoid, sclerocornea, and glaucoma.On account of this pathology in a single eye, 2 ■
(12.5%) of the patients with unilateral microphthal-mos and 13 (34.2%) of the patients with unilateral anophthalmos, as well as all 20 patients with bilateral anophthalmos, were classifi ed as legally blind.Th erefore, the overall blindness rate was 17.6% in ■
microphthalmos and 3.4 times higher (56.9%) in anophthalmos.
Summary for the Clinician
Congenital clinical anophthalmos and blind ■
microphthalmos are extremely rare conditions.
106 7 Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic Patients
7
7.2 Patients and Methods
7.2.1 Patients
A prospective study was conducted of all patients with congenital clinical anophthalmos and blind microphthal-mos who were treated at least once with a hydrogel expander in the Ophthalmology Department of the University of Rostock during the period aft er the fi rst introduction of hydrogel expander therapy in September 1997 until May 2008. No exclusion criteria were defi ned for this study.
7.2.2 Examination
In addition to a routine ophthalmological examination, the following specifi c patient data were collected:
Details were elicited concerning the course of preg- ■
nancy and delivery, and these were supplemented by discharge summaries from previously treating hospi-tals if available.When taking the family history, special emphasis was ■
placed on gathering information about developmental anomalies.Th e results of pediatric examinations were included to ■
rule out associated systemic changes (syndromes, organ anomalies, metabolic disorders, etc.).Magnetic resonance imaging (MRI) was generally per- ■
formed to exclude developmental cerebral anomalies.For the assessment of the nasolacrimal ducts, rou- ■
tine probing and irrigation of the nasolacrimal sys-tem was performed under anesthesia prior to fi rst-time surgery, as has been described in detail elsewhere [20].
Th e workup for genetic diagnosis is part of another ongoing study and is therefore not discussed here.
7.3 Results
7.3.1 Patient Data
To date, 75 patients (35 girls and 40 boys) have been treated.
Th e patient sample was composed as follows
Patients Orbits
Unilateral congenital clinical anophthalmos
38 38
Bilateral congenital clinical anophthalmos
20 40
Unilateral blind microphthalmos 16 16Bilateral blind microphthalmos 1 2Total 75 96
7.3.2 Age
Th e age of the patients at initial presentation was between 1 and 90 months (median 4 months).
7.3.3 Family History
Unilateral (n = 54)
Bilateral (n = 21)
Nothing of note, no siblings
39 14
Nothing of note, siblings healthy
12 7
Nothing of note, siblings unwell
2 0
One child with ■
postnatal middle cerebral artery infarction
Summary for the Clinician
Comprehensive evaluation of each case requires ■
a thorough ophthalmological examination sup-plemented by assessment by an experienced pediatrician. MRI is generally necessary to detect for developmental cerebral anomalies.
Summary for the Clinician
Distribution of the conditions was approximately ■
equal between males and females. Unilateral ano-phthalmos was encountered almost twice as fre-quently as bilateral anophthalmos. Microphthalmos was the least common condition.
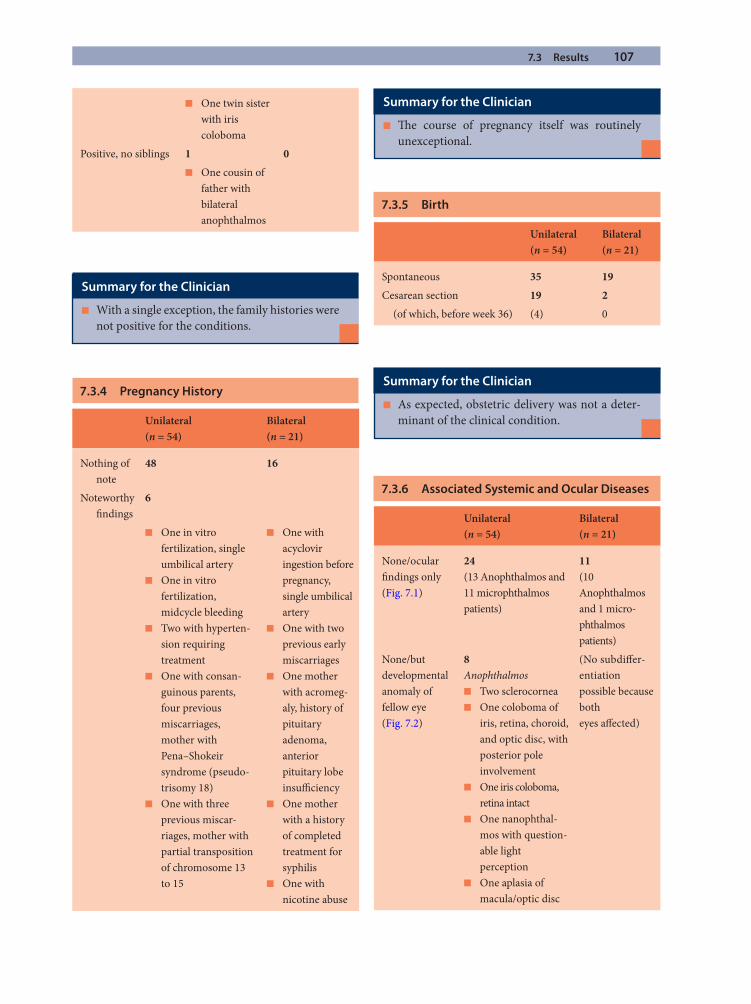
7.3 Results 107
One twin sister ■
with iris coloboma
Positive, no siblings 1 0One cousin of ■
father with bilateral anophthalmos
7.3.4 Pregnancy History
Unilateral (n = 54)
Bilateral (n = 21)
Nothing of note
48 16
Noteworthy fi ndings
6
One in vitro ■
fertilization, single umbilical arteryOne in vitro ■
fertilization, midcycle bleedingTwo with hyperten- ■
sion requiring treatmentOne with consan- ■
guinous parents, four previous miscarriages, mother with Pena–Shokeir syndrome (pseudo-trisomy 18)One with three ■
previous miscar-riages, mother with partial transposition of chromosome 13 to 15
One with ■
acyclovir ingestion before pregnancy, single umbilical arteryOne with two ■
previous early miscarriagesOne mother ■
with acromeg-aly, history of pituitary adenoma, anterior pituitary lobe insuffi ciencyOne mother ■
with a history of completed treatment for syphilisOne with ■
nicotine abuse
7.3.5 Birth
Unilateral (n = 54)
Bilateral (n = 21)
Spontaneous 35 19Cesarean section 19 2 (of which, before week 36) (4) 0
7.3.6 Associated Systemic and Ocular Diseases
Unilateral (n = 54)
Bilateral (n = 21)
None/ocular fi ndings only (Fig. 7.1)
24(13 Anophthalmos and 11 micro phthalmos patients)
11(10 Anophthalmos and 1 micro-phthalmos patients)
None/but developmental anomaly of fellow eye (Fig. 7.2)
8Anophthalmos
Two sclerocornea ■
One coloboma of ■
iris, retina, choroid, and optic disc, with posterior pole involvementOne iris coloboma, ■
retina intactOne nanophthal- ■
mos with question-able light perceptionOne aplasia of ■
macula/optic disc
(No subdiff er-entiation possible because both eyes aff ected)
Summary for the Clinician
With a single exception, the family histories were ■
not positive for the conditions.
Summary for the Clinician
Th e course of pregnancy itself was routinely ■
unexceptional.
Summary for the Clinician
As expected, obstetric delivery was not a deter- ■
minant of the clinical condition.
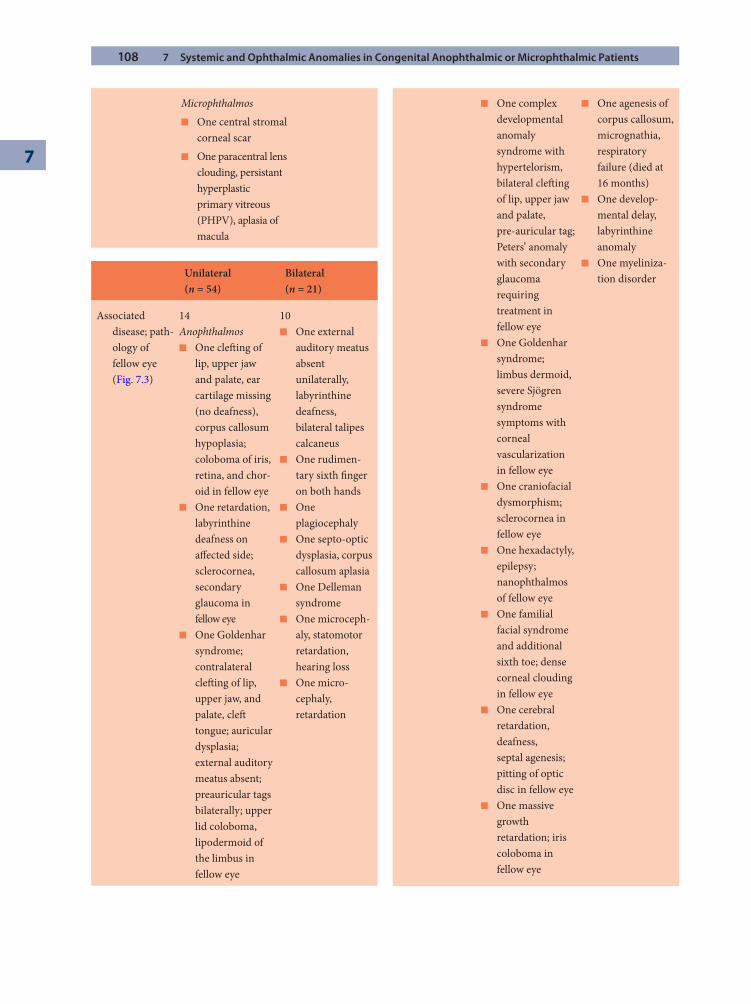
108 7 Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic Patients
7
MicrophthalmosOne central stromal ■
corneal scarOne paracentral lens ■
clouding, persistant hyperplastic primary vitreous (PHPV), aplasia of macula
Unilateral (n = 54)
Bilateral (n = 21)
Associated disease; path-ology of fellow eye (Fig. 7.3)
14Anophthalmos
One cleft ing of ■
lip, upper jaw and palate, ear cartilage missing (no deafness), corpus callosum hypoplasia; coloboma of iris, retina, and chor-oid in fellow eyeOne retardation, ■
labyrinthine deafness on aff ected side; sclerocornea, secondary glaucoma in fellow eyeOne Goldenhar ■
syndrome; contralateral cleft ing of lip, upper jaw, and palate, cleft tongue; auricular dysplasia; external auditory meatus absent; preauricular tags bilaterally; upper lid coloboma, lipodermoid of the limbus in fellow eye
10One external ■
auditory meatus absent unilaterally, labyrinthine deafness, bilateral talipes calcaneusOne rudimen- ■
tary sixth fi nger on both handsOne ■
plagiocephalyOne septo-optic ■
dysplasia, corpus callosum aplasiaOne Delleman ■
syndromeOne microceph- ■
aly, statomotor retardation, hearing lossOne micro- ■
cephaly, retardation
One complex ■
developmental anomaly syndrome with hypertelorism, bilateral cleft ing of lip, upper jaw and palate, pre-auricular tag; Peters’ anomaly with secondary glaucoma requiring treatment in fellow eyeOne Goldenhar ■
syndrome; limbus dermoid, severe Sjögren syndrome symptoms with corneal vascularization in fellow eyeOne craniofacial ■
dysmorphism; sclerocornea in fellow eyeOne hexadactyly, ■
epilepsy; nanophthalmos of fellow eyeOne familial ■
facial syndrome and additional sixth toe; dense corneal clouding in fellow eyeOne cerebral ■
retardation, deafness, septal agenesis; pitting of optic disc in fellow eyeOne massive ■
growth retardation; iris coloboma in fellow eye
One agenesis of ■
corpus callosum, micrognathia, respiratory failure (died at 16 months)One develop- ■
mental delay, labyrinthine anomalyOne myeliniza- ■
tion disorder
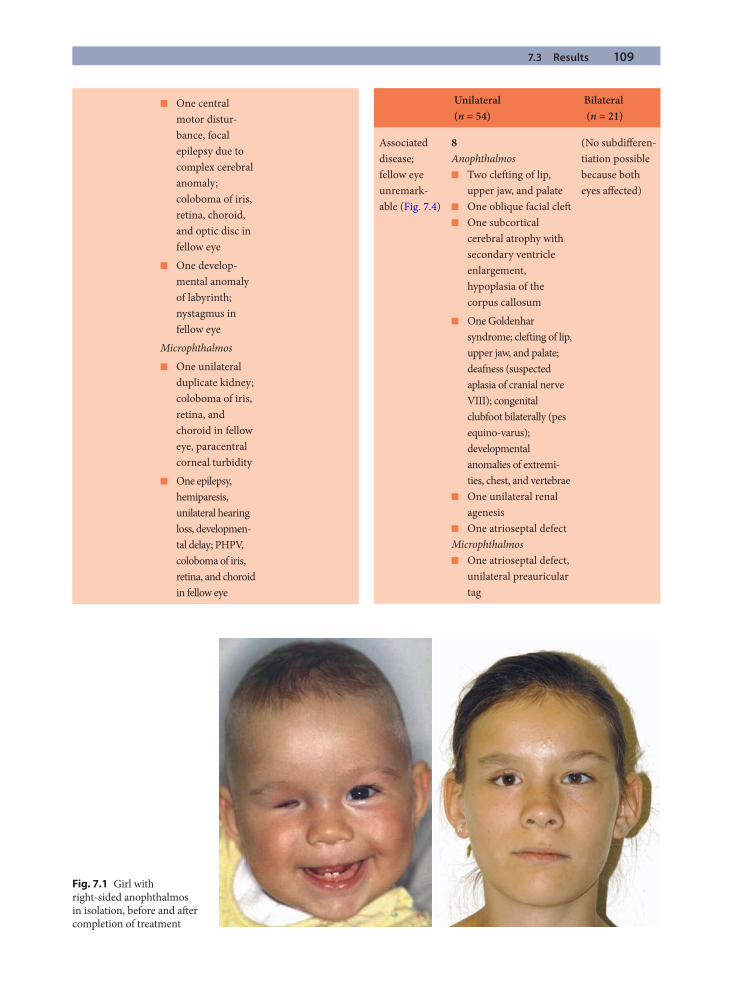
7.3 Results 109
One central ■
motor distur-bance, focal epilepsy due to complex cerebral anomaly; coloboma of iris, retina, choroid, and optic disc in fellow eyeOne develop- ■
mental anomaly of labyrinth; nystagmus in fellow eye
MicrophthalmosOne unilateral ■
duplicate kidney; coloboma of iris, retina, and choroid in fellow eye, paracentral corneal turbidityOne epilepsy, ■
hemiparesis, unilateral hearing loss, developmen-tal delay; PHPV, coloboma of iris, retina, and choroid in fellow eye
Unilateral (n = 54)
Bilateral (n = 21)
Associated disease; fellow eye unremark-able (Fig. 7.4)
8Anophthalmos
Two cleft ing of lip, ■
upper jaw, and palateOne oblique facial cleft ■
One subcortical ■
cerebral atrophy with secondary ventricle enlargement, hypoplasia of the corpus callosum
(No subdiff eren-tiation possible because both eyes aff ected)
One Goldenhar ■
syndrome; cleft ing of lip, upper jaw, and palate; deafness (suspected aplasia of cranial nerve VIII); congenital clubfoot bilaterally (pes equino-varus); developmental anomalies of extremi-ties, chest, and vertebraeOne unilateral renal ■
agenesisOne atrioseptal defect ■
MicrophthalmosOne atrioseptal defect, ■
unilateral preauricular tag
Fig. 7.1 Girl with right-sided anophthalmos in isolation, before and aft er completion of treatment
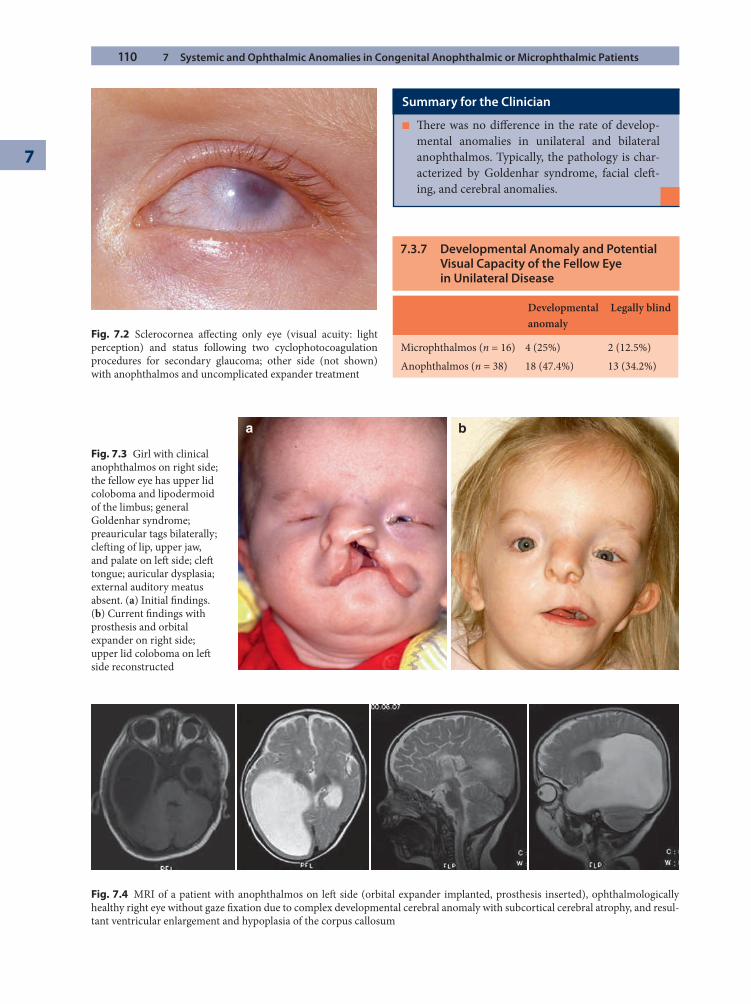
110 7 Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic Patients
7
Fig. 7.2 Sclerocornea aff ecting only eye (visual acuity: light perception) and status following two cyclophotocoagulation procedures for secondary glaucoma; other side (not shown) with anophthalmos and uncomplicated expander treatment
a b
Fig. 7.3 Girl with clinical anophthalmos on right side; the fellow eye has upper lid coloboma and lipodermoid of the limbus; general Goldenhar syndrome; preauricular tags bilaterally; cleft ing of lip, upper jaw, and palate on left side; cleft tongue; auricular dysplasia; external auditory meatus absent. (a) Initial fi ndings. (b) Current fi ndings with prosthesis and orbital expander on right side; upper lid coloboma on left side reconstructed
Fig. 7.4 MRI of a patient with anophthalmos on left side (orbital expander implanted, prosthesis inserted), ophthalmologically healthy right eye without gaze fi xation due to complex developmental cerebral anomaly with subcortical cerebral atrophy, and resul-tant ventricular enlargement and hypoplasia of the corpus callosum
Summary for the Clinician
Th ere was no diff erence in the rate of develop- ■
mental anomalies in unilateral and bilateral anophthalmos. Typically, the pathology is char-acterized by Goldenhar syndrome, facial cleft -ing, and cerebral anomalies.
7.3.7 Developmental Anomaly and Potential Visual Capacity of the Fellow Eye in Unilateral Disease
Developmental anomaly
Legally blind
Microphthalmos (n = 16) 4 (25%) 2 (12.5%)Anophthalmos (n = 38) 18 (47.4%) 13 (34.2%)
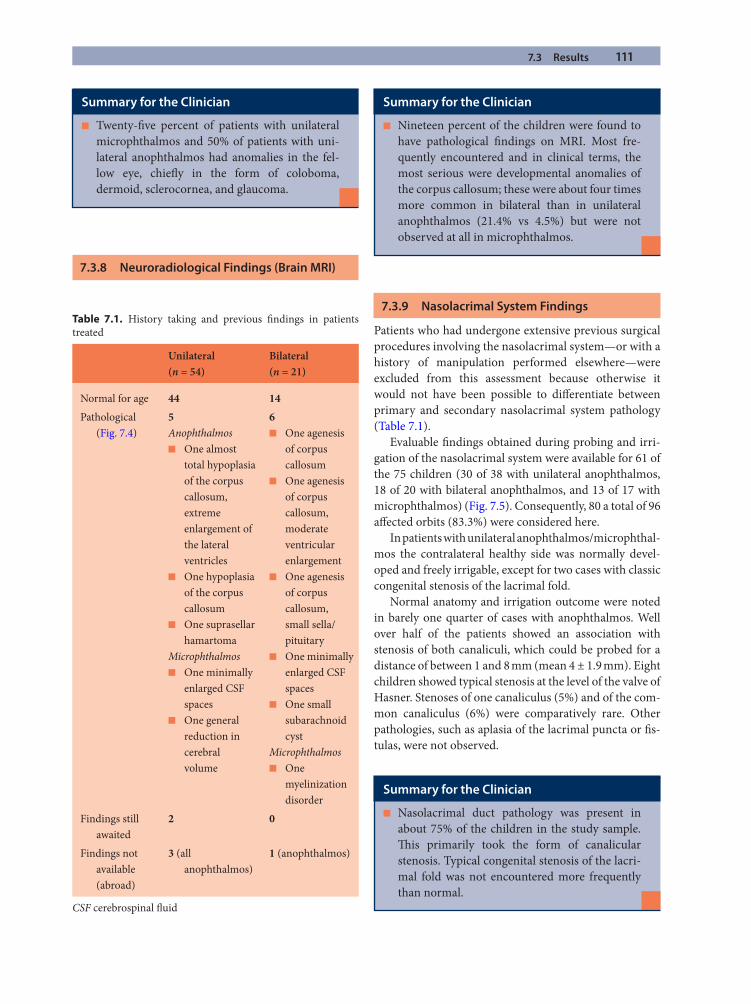
7.3 Results 111
7.3.8 Neuroradiological Findings (Brain MRI)
7.3.9 Nasolacrimal System Findings
Patients who had undergone extensive previous surgical procedures involving the nasolacrimal system—or with a history of manipulation performed elsewhere—were excluded from this assessment because otherwise it would not have been possible to diff erentiate between primary and secondary nasolacrimal system pathology (Table 7.1).
Evaluable fi ndings obtained during probing and irri-gation of the nasolacrimal system were available for 61 of the 75 children (30 of 38 with unilateral anophthalmos, 18 of 20 with bilateral anophthalmos, and 13 of 17 with microphthalmos) (Fig. 7.5). Consequently, 80 a total of 96 aff ected orbits (83.3%) were considered here.
In patients with unilateral anophthalmos/microphthal-mos the contralateral healthy side was normally devel-oped and freely irrigable, except for two cases with classic congenital stenosis of the lacrimal fold.
Normal anatomy and irrigation outcome were noted in barely one quarter of cases with anophthalmos. Well over half of the patients showed an association with stenosis of both canaliculi, which could be probed for a distance of between 1 and 8 mm (mean 4 ± 1.9 mm). Eight children showed typical stenosis at the level of the valve of Hasner. Stenoses of one canaliculus (5%) and of the com-mon canaliculus (6%) were comparatively rare. Other pathologies, such as aplasia of the lacrimal puncta or fi s-tulas, were not observed.
Summary for the Clinician
Twenty-fi ve percent of patients with unilateral ■
microphthalmos and 50% of patients with uni-lateral anophthalmos had anomalies in the fel-low eye, chiefl y in the form of coloboma, dermoid, sclerocornea, and glaucoma.
Summary for the Clinician
Nineteen percent of the children were found to ■
have pathological fi ndings on MRI. Most fre-quently encountered and in clinical terms, the most serious were developmental anomalies of the corpus callosum; these were about four times more common in bilateral than in unilateral anophthalmos (21.4% vs 4.5%) but were not observed at all in microphthalmos.
Summary for the Clinician
Nasolacrimal duct pathology was present in ■
about 75% of the children in the study sample. Th is primarily took the form of canalicular stenosis. Typical congenital stenosis of the lacri-mal fold was not encountered more frequently than normal.
Table 7.1. History taking and previous fi ndings in patients treated
Unilateral (n = 54)
Bilateral (n = 21)
Normal for age 44 14Pathological
(Fig. 7.4)5Anophthalmos
One almost ■
total hypoplasia of the corpus callosum, extreme enlargement of the lateral ventriclesOne hypoplasia ■
of the corpus callosumOne suprasellar ■
hamartomaMicrophthalmos
One minimally ■
enlarged CSF spacesOne general ■
reduction in cerebral volume
6One agenesis ■
of corpus callosumOne agenesis ■
of corpus callosum, moderate ventricular enlargementOne agenesis ■
of corpus callosum, small sella/pituitaryOne minimally ■
enlarged CSF spacesOne small ■
subarachnoid cyst
MicrophthalmosOne ■
myelinization disorder
Findings still awaited
2 0
Findings not available (abroad)
3 (all anophthalmos)
1 (anophthalmos)
CSF cerebrospinal fl uid
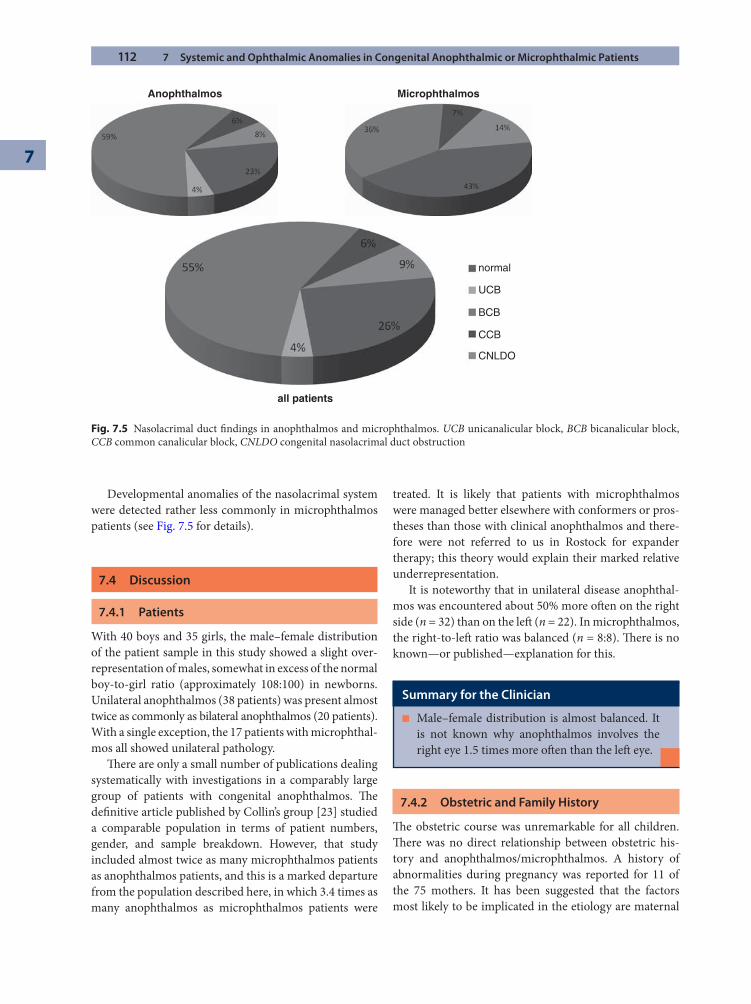
112 7 Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic Patients
7
Developmental anomalies of the nasolacrimal system were detected rather less commonly in microphthalmos patients (see Fig. 7.5 for details).
7.4 Discussion
7.4.1 Patients
With 40 boys and 35 girls, the male–female distribution of the patient sample in this study showed a slight over-representation of males, somewhat in excess of the normal boy-to-girl ratio (approximately 108:100) in newborns. Unilateral anophthalmos (38 patients) was present almost twice as commonly as bilateral anophthalmos (20 patients). With a single exception, the 17 patients with microphthal-mos all showed unilateral pathology.
Th ere are only a small number of publications dealing systematically with investigations in a comparably large group of patients with congenital anophthalmos. Th e defi nitive article published by Collin’s group [23] studied a comparable population in terms of patient numbers, gender, and sample breakdown. However, that study included almost twice as many microphthalmos patients as anophthalmos patients, and this is a marked departure from the population described here, in which 3.4 times as many anophthalmos as microphthalmos patients were
treated. It is likely that patients with microphthalmos were managed better elsewhere with conformers or pros-theses than those with clinical anophthalmos and there-fore were not referred to us in Rostock for expander therapy; this theory would explain their marked relative underrepresentation.
It is noteworthy that in unilateral disease anophthal-mos was encountered about 50% more oft en on the right side (n = 32) than on the left (n = 22). In microphthalmos, the right-to-left ratio was balanced (n = 8:8). Th ere is no known—or published—explanation for this.
7.4.2 Obstetric and Family History
Th e obstetric course was unremarkable for all children. Th ere was no direct relationship between obstetric his-tory and anophthalmos/microphthalmos. A history of abnormalities during pregnancy was reported for 11 of the 75 mothers. It has been suggested that the factors most likely to be implicated in the etiology are maternal
all patients
normal
UCB
BCB
CCB
CNLDO
Anophthalmos Microphthalmos
Fig. 7.5 Nasolacrimal duct fi ndings in anophthalmos and microphthalmos. UCB unicanalicular block, BCB bicanalicular block, CCB common canalicular block, CNLDO congenital nasolacrimal duct obstruction
Summary for the Clinician
Male–female distribution is almost balanced. It ■
is not known why anophthalmos involves the right eye 1.5 times more oft en than the left eye.
7.4 Discussion 113
vitamin A defi ciency, exposure to X-rays, and gestational-acquired infections [24]. In our own patients, for the majority of anomalies reported, there was no discernible link with the children’s anophthalmos/microphthalmos in terms of factors reported in the literature.
In an Indian population, Hornby et al. [9] reported a consanguinity rate of 64% in 24 children with microphthal-mos. In our own patients, consanguinity was established in only one child. Taken together with the described genetic fi ndings in the parents and the single case with a positive family history, however, this points to the puta-tive role of genetic factors. It seems clear that ano-phthalmos and microphthalmos have a complex and multifactorial etiology that includes chromosomal fac-tors, such as duplications, deletions, and translocations, as well as monogenic causes. Among the monogenic causes, SOX2 on chromosome 3 has been identifi ed as a principal gene that is responsible for 10–20% of (mainly bilateral) anophthalmos [6]. Other linked genes include PAX6, OTX2, CHX10, FOXE3, and RAX (for comprehensive discussion, see [24]). Th e detailed workup for genetic diagnosis in our own patients is the subject of another ongoing study and is therefore not covered in this article.
7.4.3 Associated Pathologies
7.4.3.1 Ophthalmological Findings in Unilateral Disease
In 12 (75%) of the 16 patients with unilateral microphthal-mos, the fellow eye was morphologically and functionally normal; the condition was limited to a single eye. Th e remaining four children (25%) displayed pathological changes in the fellow eye, and in two of these cases (12.5%) the changes were so severe that the children were categorized as legally blind.
Twenty (70%) of 29 microphthalmos patients had a normal fellow eye in the study conducted by Tucker et al. [23]; the remainder displayed associated developmental anomalies of the fellow eye, although no information on visual acuity was provided.
In the present study, in 20 (52.6%) of the 38 patients with unilateral anophthalmos, the fellow eye was healthy
and had normal visual function. Eighteen children (47.4%) were found to have an associated developmental anomaly of the fellow eye, such as coloboma or sclero-cornea, with the result that 13 children (34.2%) were cat-egorized as legally blind.
Th e distribution statistics are largely consistent with the details for 14 anophthalmos patients presented in the pre-viously cited study by Tucker et al. [23]. Th at publication provided no information on potential visual function.
In their group of 24 Indian children with anophthal-mos, Hornby et al. [9] did not fi nd any patients with a normal fellow eye. However, the children were recruited only from blind schools, a fact that explains the absence of children with one healthy or sighted eye and ultimately rules out any comparison with the population in the pres-ent study.
In summary, in terms of potential visual function, 46.7% of our study population were legally blind. When those children with obvious bilateral disease were left out of the calculation, the risk of blindness with presumed unilateral pathology was almost three times higher with anophthalmos than with microphthalmos. Previous pub-lications have not referred to this aspect. It is therefore necessary to examine the fellow eye at an early stage to assess the potential development of visual acuity and, if appropriate, to initiate measures for its early promotion.
7.4.3.2 Neuroradiological Findings
In technical terms, MRI is superior to computed tomog-raphy (CT) for the assessment of cerebral fi ndings [5, 7].
In our study sample, 15.9% of patients had fi ndings consistent with associated cerebral pathology. Th ese were encountered almost three times as oft en in bilateral ano-phthalmos (26.3%) as in unilateral anophthalmos (9.1%). Th e frequency of such fi ndings in unilateral microphthal-mos (12.5%) was comparable to that in unilateral
Summary for the Clinician
Consanguinity and pathological chromosome ■
fi ndings point to the involvement of genetic fac-tors, which are becoming an increasing focus of research. Summary for the Clinician
On account of this pathology in a single eye, 2 ■
(12.5%) of the patients with unilateral microphthalmos and 13 (34.2%) of the patients with unilateral anophthalmos, as well as all of the patients with bilateral anophthalmos, were classifi ed as legally blind. Th erefore, the overall blindness rate was 17.6% in microphthalmos and 3.4 times higher (56.9%) in anophthalmos.

114 7 Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic Patients
7
anophthalmos. Our study sample included only one patient with bilateral microphthalmos, and consequently no fur-ther diff erentiation was possible.
Th e most serious changes, detected in fi ve anophthal-mos patients, involved extreme hypoplasia—or complete agenesis—of the corpus callosum. Th is change aff ected 9.6% of the patients and was again far more common in bilateral (16.8%) than in unilateral (6.1%) disease. Septo-optic dysplasia was reported to be associated with an increased rate of sudden death in children [3]. Among our patients, one child with bilateral anophthalmos and corpus callosum aplasia died unexpectedly at the age of 16 months.
An association between anophthalmos and develop-mental anomalies of the corpus callosum has been described in individual case reports [1, 5].
In view of the frequent occurrence of associated cere-bral developmental anomalies, it appears justifi able to recommend MRI examination for every child with these conditions.
7.4.3.3 Systemic Diseases
In their analysis of data from the Spanish Collaborative Study of Congenital Malformations in a series of 1,124,654 consecutive births, Bermejo and Martínez-Frías [2] noted 240 cases of anophthalmos (n = 47) or microphthalmos (n = 193). Only 9.6% of these defects occurred in isola-tion. Th e 90.4% occurring in conjunction with systemic diseases were subdivided into syndromes (32.9%) and multiple congenital anomalies (57.5%). Unfortunately, those authors did not undertake any further diff erentia-tion of concomitant systemic diseases to provide a basis for comparison.
A far lower rate of systemic disease associations (39%) was reported by Mouriaux et al. [13] in their study in 7 anophthalmos and 35 microphthalmos patients; this fi g-ure is comparable to the 37.7% incidence calculated by Tucker et al. [23], who noted associated systemic diseases in 7 of 34 microphthalmos patients (20.6%) and in 22 of 43 anophthalmos patients (51.2%). Th ese published sta-tistics are consistent with our observations:
In our patient sample, 3 of 17 children with micro-phthalmos (17.6%) were found to have associated sys-temic diseases, although the pathology tended to be of a less serious nature.
Associated systemic diseases were considerably more frequent in anophthalmos patients, with 29 of 58 chil-dren aff ected (50%); most commonly, these were devel-opmental cerebral anomalies (n = 12), followed by (hemi-)facial anomalies (n = 9). Th e variable “unilateral versus bilateral” had no infl uence on absolute frequency. However, it is remarkable that the nature of the pathology is diff erent. Unilateral anophthalmos was associated most commonly with cleft ing (seven patients), which was not detected at all in the surgically managed patients with bilateral anophthalmos. (To date, bilateral cleft ing of lip, upper jaw, and palate has been noted just once in a child with bilateral anophthalmos who did not undergo sur-gery because of the underlying presence of trisomy 13; see Fig. 7.6.) In the children with bilateral anophthalmos, there was a defi nite predominance (7 of 10 aff ected chil-dren) of cerebral anomalies, which were encountered far less commonly (23%) in unilateral anophthalmos. It has been postulated that a general malformation of the fore-brain during embryological development might provide an explanation for the above-average incidence of the association between bilateral anophthalmos and devel-opmental anomalies of the optic chiasm and corpus cal-losum [1, 10]. Meanwhile unilateral anophthalmos arises mainly in association with developmental anomalies of the fi rst and second pharyngeal arches, such as Goldenhar syndrome. Th is suggests that the normal development of the mesenchyma, from which, for example, the maxilla and mandible are formed, is associated with the correct shaping of the eye and orbit, and that anomalies in this development may lead to degenerative (consecutive) anophthalmos [1].
7.4.3.4 Nasolacrimal Duct Findings
On the side aff ected by anophthalmos or microphthal-mos, 80% of patients presented with stenosis of the nasolacrimal duct system. Canalicular (62%) and presac-cal (11%) stenoses accounted for the largest proportion of
Summary for the Clinician
Th e frequent occurrence of developmental cere- ■
bral anomalies, particularly those involving the corpus callosum, warrants MRI examination for all children aff ected.
Summary for the Clinician
Associated systemic fi ndings were more numer- ■
ous and more severe in patients with anophthal-mos (50%) than in those with microphthalmos (17.6%).
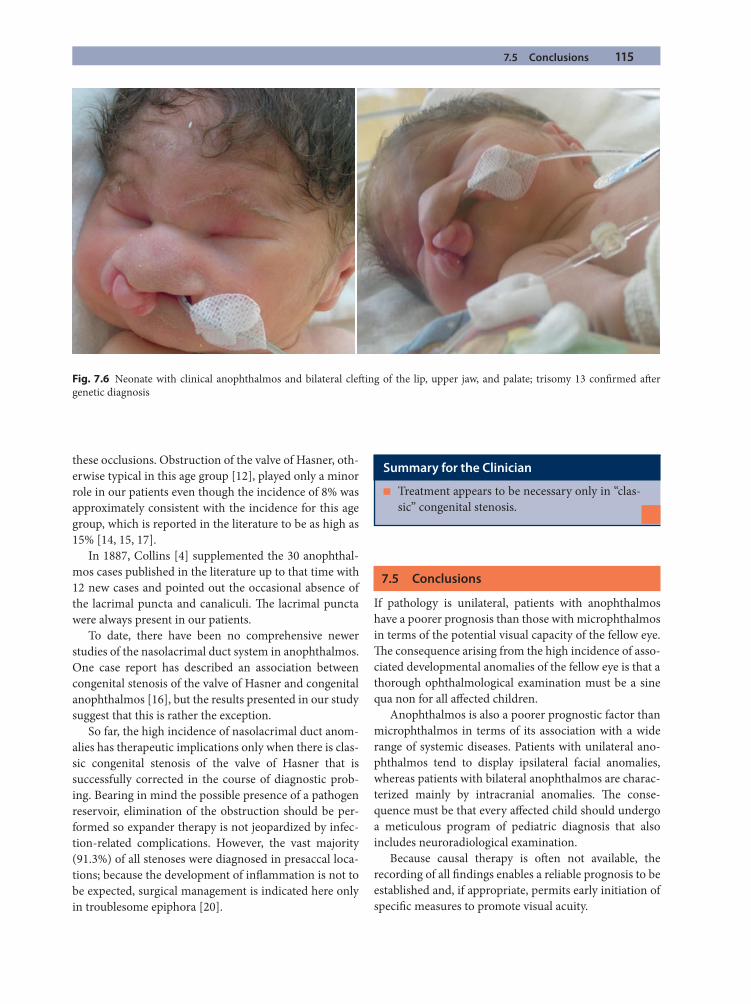
7.5 Conclusions 115
these occlusions. Obstruction of the valve of Hasner, oth-erwise typical in this age group [12], played only a minor role in our patients even though the incidence of 8% was approximately consistent with the incidence for this age group, which is reported in the literature to be as high as 15% [14, 15, 17].
In 1887, Collins [4] supplemented the 30 anophthal-mos cases published in the literature up to that time with 12 new cases and pointed out the occasional absence of the lacrimal puncta and canaliculi. Th e lacrimal puncta were always present in our patients.
To date, there have been no comprehensive newer studies of the nasolacrimal duct system in anophthalmos. One case report has described an association between congenital stenosis of the valve of Hasner and congenital anophthalmos [16], but the results presented in our study suggest that this is rather the exception.
So far, the high incidence of nasolacrimal duct anom-alies has therapeutic implications only when there is clas-sic congenital stenosis of the valve of Hasner that is successfully corrected in the course of diagnostic prob-ing. Bearing in mind the possible presence of a pathogen reservoir, elimination of the obstruction should be per-formed so expander therapy is not jeopardized by infec-tion-related complications. However, the vast majority (91.3%) of all stenoses were diagnosed in presaccal loca-tions; because the development of infl ammation is not to be expected, surgical management is indicated here only in troublesome epiphora [20].
7.5 Conclusions
If pathology is unilateral, patients with anophthalmos have a poorer prognosis than those with microphthalmos in terms of the potential visual capacity of the fellow eye. Th e consequence arising from the high incidence of asso-ciated developmental anomalies of the fellow eye is that a thorough ophthalmological examination must be a sine qua non for all aff ected children.
Anophthalmos is also a poorer prognostic factor than microphthalmos in terms of its association with a wide range of systemic diseases. Patients with unilateral ano-phthalmos tend to display ipsilateral facial anomalies, whereas patients with bilateral anophthalmos are charac-terized mainly by intracranial anomalies. Th e conse-quence must be that every aff ected child should undergo a meticulous program of pediatric diagnosis that also includes neuroradiological examination.
Because causal therapy is oft en not available, the recording of all fi ndings enables a reliable prognosis to be established and, if appropriate, permits early initiation of specifi c measures to promote visual acuity.
Summary for the Clinician
Treatment appears to be necessary only in “clas- ■
sic” congenital stenosis.
Fig. 7.6 Neonate with clinical anophthalmos and bilateral cleft ing of the lip, upper jaw, and palate; trisomy 13 confi rmed aft er genetic diagnosis
116 7 Systemic and Ophthalmic Anomalies in Congenital Anophthalmic or Microphthalmic Patients
7
References
1. Albernaz VS, Castillo M, Hudgins PA, Mukherji SK (1997) Imaging fi ndings in patients with clinical anophthalmos. Am J Neuroradiol 18(3):555–561
2. Bermejo E, Martínez-Frías ML (1998) Congenital eye mal-formations: clinical-epidemiological analysis of 1,124,654 consecutive births in Spain. Am J Med Genet 75(5): 497–504
3. Brodsky MC, Conte FA, Taylor D, Hoyt CS, Mrak RE (1997) Sudden death in septo-optic dysplasia. Report of 5 cases. Arch Ophthalmol 115(1):66–70
4. Collins ET (1887) On anophthalmos. Royal London Ophthalmic Hospital Reports. J Ophthal Med 40:429–455
5. Daxecker F, Felber S (1993) Magnetic resonance imaging features of congenital anophthalmia. Ophthalmologica 206(3):139–142
6. Fantes J, Ragge NK, Lynch SA, McGill NI, Collin JR, Howard-Peebles PN, Hayward C, Vivian AJ, Williamson K, Van Heyningen V, Fitzpatrick DR (2003) Mutations in SOX2 cause anophthalmia. Nat Genet 33(4):461–463. (Epub 3 Mar 2003)
7. Frosini R, Papini M, Campana G, Giovannucci Uzielli ML (1981) Contribution of computerized tomography to the study of severe congenital ocular dysplasias. Study of a case of clinical anophthalmos. Ophthalmologica 183(2):72–76
8. Gundlach KKH, Guthoff RF, Hingst V, Schittkowski MP, Bier UC (2005) Expansion of the socket and the orbit for congenital clinical anophthalmia. Plast Reconstr Surg 116(5):1214–1222
9. Hornby SJ, Dandona L, Foster A, Jones RB, Gilbert CE (2001) Clinical fi ndings, consanguinity, and pedigrees in children with anophthalmos in southern India. Dev Med Child Neurol 43(6):392–398
10. Jacquemin C, Mullaney PB, Bosley TM (2000) Ophthal-mological and intracranial anomalies in patients with clin-ical anophthalmos. Eye 14(1):82–87
11. Kallen B, Robert E, Harris J (1996) Th e descriptive epide-miology of anophthalmia and microphthalmia. Int J Epidemiol 25(5):1009–1016
12. Katowitz JA, Welsh MG (1987) Timing of initial probing and irrigation in congenital nasolacrimal duct obstruction. Ophthalmology 94:698–705
13. Mouriaux F, Audo I, Defoort-Dhellemmes S, Labalette P, Guilbert F, Constantinides G, Pellerin P (1997) Management of congenital microphthalmos and anophthalmos. J Fr Ophthalmol 20(8):583–591
14. Müller F (1975) Erkrankungen der Tränenorgane. In: Velhagen K (ed) Der Augenarzt, 2nd ed, vol. 3. VEB Georg Th ieme, Leipzig, pp 7–131
15. Noda S, Hayasaka S, Setogawa T (1991) Congenital nasolacrimal duct obstruction in Japanese infants: its inci-dence and treatment with massage. J Pediatr Ophthalmol Strabismus 28(1):20–22
16. Oguz H, Ozturk A, San I (2003) Congenital nasolacrimal duct occlusion with clinical anophthalmos: a possible new association. Ophthalmic Genet 24(3):181–185
17. Olver J (2001) Paediatric lacrimal surgery. In: Olver J (ed) Colour atlas of lacrimal surgery. Butterworth-Heinemann, Oxford, pp 69–90
18. Schittkowski MP, Gundlach KK, Guthoff RF (2003) Treatment of congenital clinical anophthalmos with high hydrophilic hydrogel expanders. Ophthalmologe 100(7): 525–534
19. Schittkowski MP, Guthoff RF (2006) Injectable self infl at-ing hydrogel pellet expanders for the treatment of orbital volume defi ciency in congenital microphthalmos: prelimi-nary results with a new therapeutic approach. Br J Ophthalmol 90(9):1173–1177. (Epub 17 May 2006)
20. Schittkowski MP, Guthoff RF (2007) Results of lacrimal assessment in patients with congenital clinical anophthal-mos or blind microphthalmos. Br J Ophthalmol 91(12): 1624–1626. (Epub 13 June 2007)
21. Shaw GM, Carmichael SL, Yang W, Harris JA, Finnell RH, Lammer EJ (2005) Epidemiologic characteristics of ano-phthalmia and bilateral microphthalmia among 2.5 mil-lion births in California, 1989–1997. Am J Med Genet A 137(1):36–40
22. Srsen S (1973) Congenital anophthalmos in two siblings. Acta Univ Carol Med Monogr 56:136–139
23. Tucker S, Jones B, Collin R (1996) Systemic anomalies in 77 patients with congenital anophthalmos or microphthal-mos. Eye 10(3):310–314
24. Verma AS, Fitzpatrick DR (2007 Nov) Anophthalmia and microphthalmia. Orphanet J Rare Dis 26:47–54
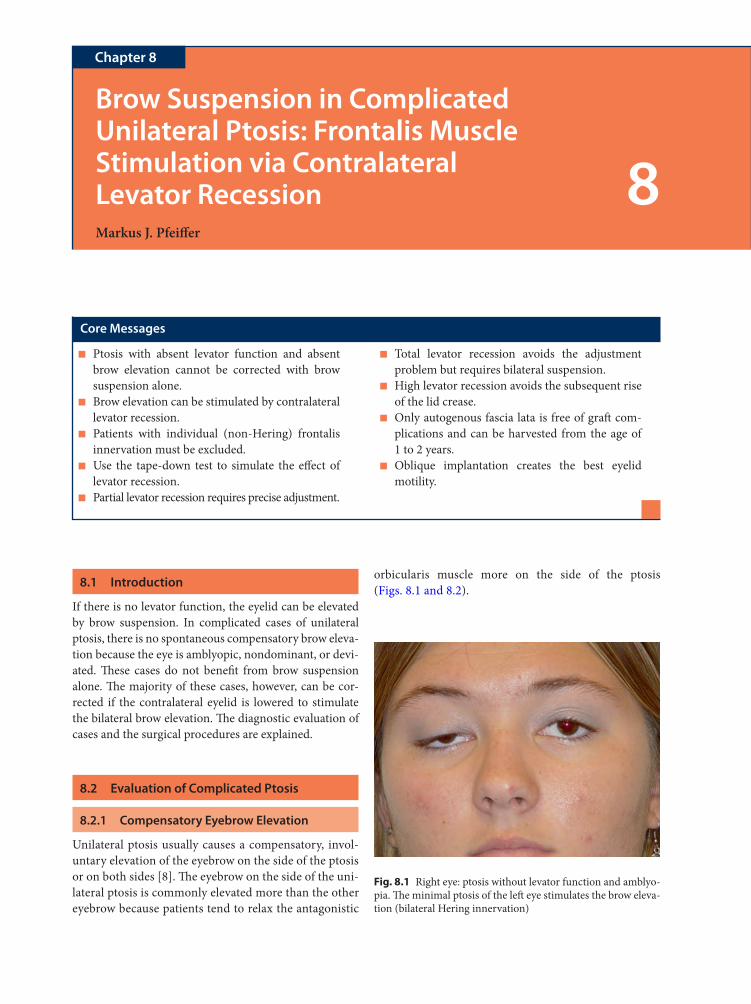
8.1 Introduction
If there is no levator function, the eyelid can be elevated by brow suspension. In complicated cases of unilateral ptosis, there is no spontaneous compensatory brow eleva-tion because the eye is amblyopic, nondominant, or devi-ated. Th ese cases do not benefi t from brow suspension alone. Th e majority of these cases, however, can be cor-rected if the contralateral eyelid is lowered to stimulate the bilateral brow elevation. Th e diagnostic evaluation of cases and the surgical procedures are explained.
8.2 Evaluation of Complicated Ptosis
8.2.1 Compensatory Eyebrow Elevation
Unilateral ptosis usually causes a compensatory, invol-untary elevation of the eyebrow on the side of the ptosis or on both sides [8]. Th e eyebrow on the side of the uni-lateral ptosis is commonly elevated more than the other eyebrow because patients tend to relax the antagonistic
orbicularis muscle more on the side of the ptosis (Figs. 8.1 and 8.2).
Brow Suspension in Complicated Unilateral Ptosis: Frontalis Muscle Stimulation via Contralateral Levator RecessionMarkus J. Pfeiff er
Chapter 8
8
Core Messages
Ptosis with absent levator function and absent ■
brow elevation cannot be corrected with brow suspension alone.Brow elevation can be stimulated by contralateral ■
levator recession.Patients with individual (non-Hering) frontalis ■
innervation must be excluded.Use the tape-down test to simulate the eff ect of ■
levator recession.Partial levator recession requires precise adjustment. ■
Total levator recession avoids the adjustment ■
problem but requires bilateral suspension.High levator recession avoids the subsequent rise ■
of the lid crease.Only autogenous fascia lata is free of graft com- ■
plications and can be harvested from the age of 1 to 2 years.Oblique implantation creates the best eyelid ■
motility.
Fig. 8.1 Right eye: ptosis without levator function and amblyo-pia. Th e minimal ptosis of the left eye stimulates the brow eleva-tion (bilateral Hering innervation)
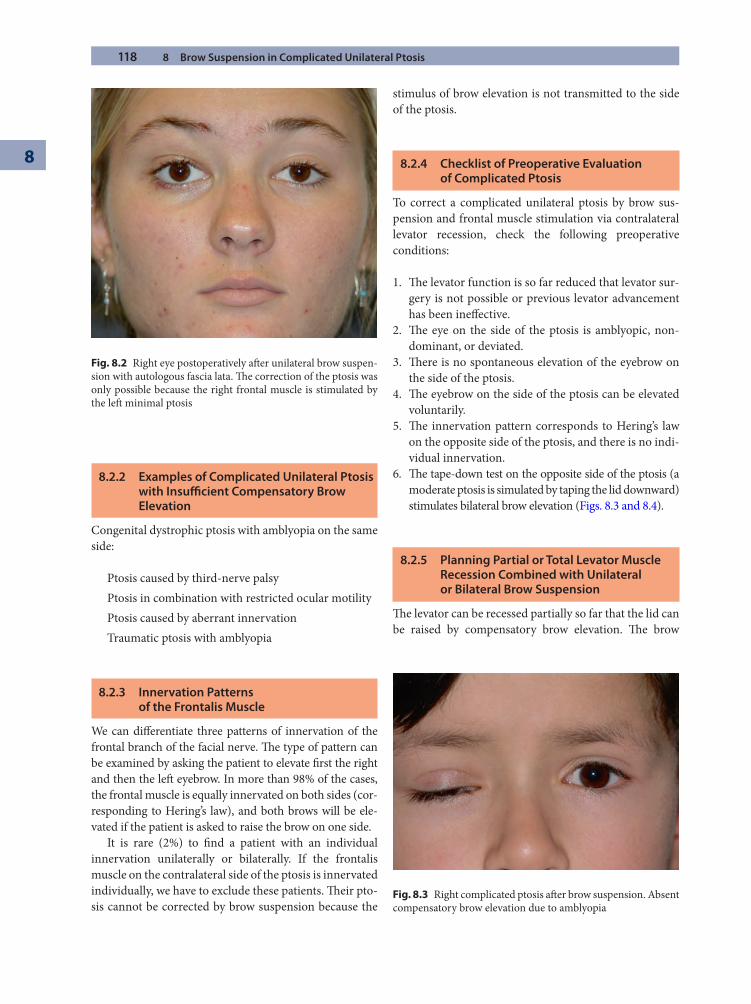
118 8 Brow Suspension in Complicated Unilateral Ptosis
8
8.2.2 Examples of Complicated Unilateral Ptosis with Insuffi cient Compensatory Brow Elevation
Congenital dystrophic ptosis with amblyopia on the same side:
Ptosis caused by third-nerve palsyPtosis in combination with restricted ocular motilityPtosis caused by aberrant innervationTraumatic ptosis with amblyopia
8.2.3 Innervation Patterns of the Frontalis Muscle
We can diff erentiate three patterns of innervation of the frontal branch of the facial nerve. Th e type of pattern can be examined by asking the patient to elevate fi rst the right and then the left eyebrow. In more than 98% of the cases, the frontal muscle is equally innervated on both sides (cor-responding to Hering’s law), and both brows will be ele-vated if the patient is asked to raise the brow on one side.
It is rare (2%) to fi nd a patient with an individual innervation unilaterally or bilaterally. If the frontalis muscle on the contralateral side of the ptosis is innervated individually, we have to exclude these patients. Th eir pto-sis cannot be corrected by brow suspension because the
stimulus of brow elevation is not transmitted to the side of the ptosis.
8.2.4 Checklist of Preoperative Evaluation of Complicated Ptosis
To correct a complicated unilateral ptosis by brow sus-pension and frontal muscle stimulation via contralateral levator recession, check the following preoperative conditions:
1. Th e levator function is so far reduced that levator sur-gery is not possible or previous levator advancement has been ineff ective.
2. Th e eye on the side of the ptosis is amblyopic, non-dominant, or deviated.
3. Th ere is no spontaneous elevation of the eyebrow on the side of the ptosis.
4. Th e eyebrow on the side of the ptosis can be elevated voluntarily.
5. Th e innervation pattern corresponds to Hering’s law on the opposite side of the ptosis, and there is no indi-vidual innervation.
6. Th e tape-down test on the opposite side of the ptosis (a moderate ptosis is simulated by taping the lid downward) stimulates bilateral brow elevation (Figs. 8.3 and 8.4).
8.2.5 Planning Partial or Total Levator Muscle Recession Combined with Unilateral or Bilateral Brow Suspension
Th e levator can be recessed partially so far that the lid can be raised by compensatory brow elevation. Th e brow
Fig. 8.2 Right eye postoperatively aft er unilateral brow suspen-sion with autologous fascia lata. Th e correction of the ptosis was only possible because the right frontal muscle is stimulated by the left minimal ptosis
Fig. 8.3 Right complicated ptosis aft er brow suspension. Absent compensatory brow elevation due to amblyopia
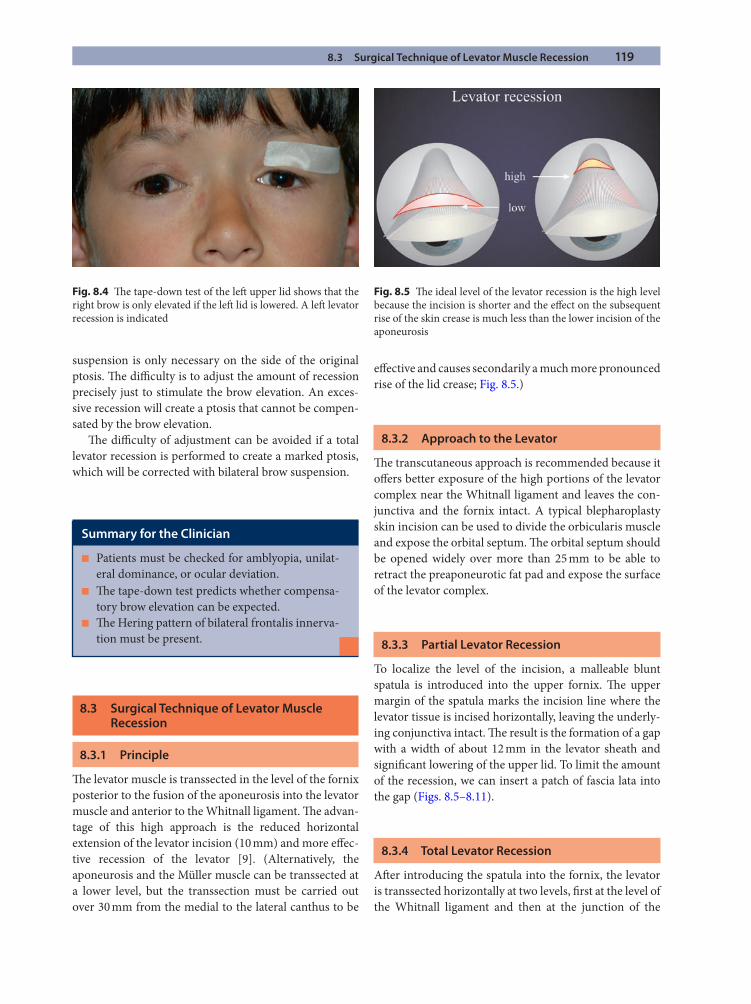
8.3 Surgical Technique of Levator Muscle Recession 119
suspension is only necessary on the side of the original ptosis. Th e diffi culty is to adjust the amount of recession precisely just to stimulate the brow elevation. An exces-sive recession will create a ptosis that cannot be compen-sated by the brow elevation.
Th e diffi culty of adjustment can be avoided if a total levator recession is performed to create a marked ptosis, which will be corrected with bilateral brow suspension.
8.3 Surgical Technique of Levator Muscle Recession
8.3.1 Principle
Th e levator muscle is transsected in the level of the fornix posterior to the fusion of the aponeurosis into the levator muscle and anterior to the Whitnall ligament. Th e advan-tage of this high approach is the reduced horizontal extension of the levator incision (10 mm) and more eff ec-tive recession of the levator [9]. (Alternatively, the aponeurosis and the Müller muscle can be transsected at a lower level, but the transsection must be carried out over 30 mm from the medial to the lateral canthus to be
eff ective and causes secondarily a much more pronounced rise of the lid crease; Fig. 8.5.)
8.3.2 Approach to the Levator
Th e transcutaneous approach is recommended because it off ers better exposure of the high portions of the levator complex near the Whitnall ligament and leaves the con-junctiva and the fornix intact. A typical blepharoplasty skin incision can be used to divide the orbicularis muscle and expose the orbital septum. Th e orbital septum should be opened widely over more than 25 mm to be able to retract the preaponeurotic fat pad and expose the surface of the levator complex.
8.3.3 Partial Levator Recession
To localize the level of the incision, a malleable blunt spatula is introduced into the upper fornix. Th e upper margin of the spatula marks the incision line where the levator tissue is incised horizontally, leaving the underly-ing conjunctiva intact. Th e result is the formation of a gap with a width of about 12 mm in the levator sheath and signifi cant lowering of the upper lid. To limit the amount of the recession, we can insert a patch of fascia lata into the gap (Figs. 8.5–8.11).
8.3.4 Total Levator Recession
Aft er introducing the spatula into the fornix, the levator is transsected horizontally at two levels, fi rst at the level of the Whitnall ligament and then at the junction of the
Fig. 8.4 Th e tape-down test of the left upper lid shows that the right brow is only elevated if the left lid is lowered. A left levator recession is indicated
Summary for the Clinician
Patients must be checked for amblyopia, unilat- ■
eral dominance, or ocular deviation.Th e tape-down test predicts whether compensa- ■
tory brow elevation can be expected.Th e Hering pattern of bilateral frontalis innerva- ■
tion must be present.
Fig. 8.5 Th e ideal level of the levator recession is the high level because the incision is shorter and the eff ect on the subsequent rise of the skin crease is much less than the lower incision of the aponeurosis
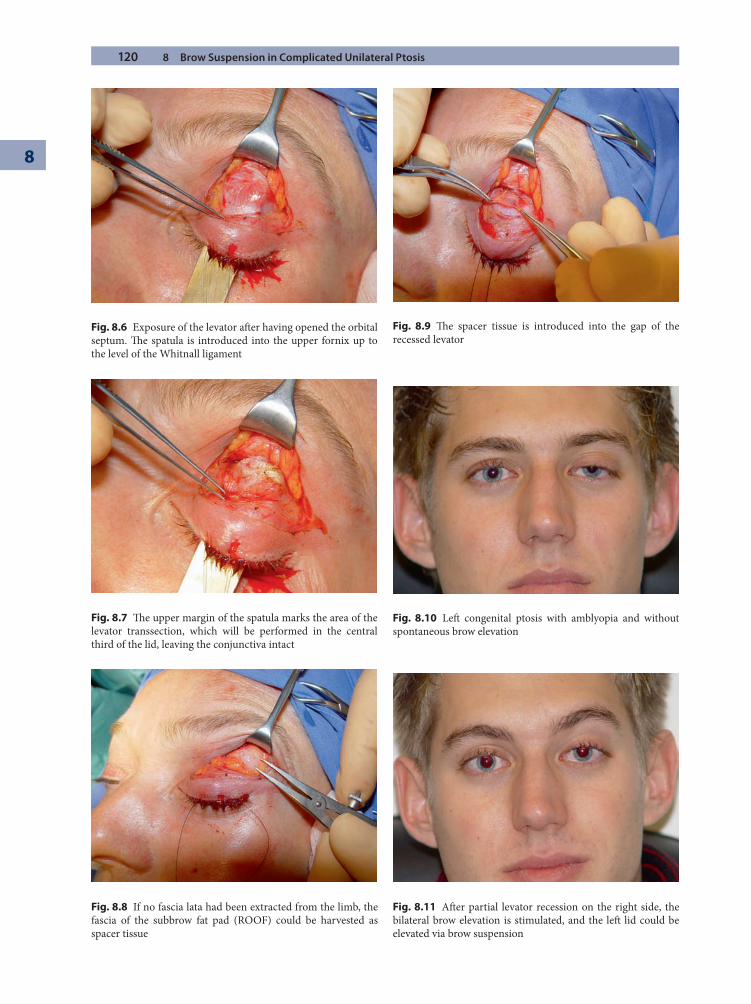
120 8 Brow Suspension in Complicated Unilateral Ptosis
8
Fig. 8.6 Exposure of the levator aft er having opened the orbital septum. Th e spatula is introduced into the upper fornix up to the level of the Whitnall ligament
Fig. 8.7 Th e upper margin of the spatula marks the area of the levator transsection, which will be performed in the central third of the lid, leaving the conjunctiva intact
Fig. 8.8 If no fascia lata had been extracted from the limb, the fascia of the subbrow fat pad (ROOF) could be harvested as spacer tissue
Fig. 8.9 Th e spacer tissue is introduced into the gap of the recessed levator
Fig. 8.10 Left congenital ptosis with amblyopia and without spontaneous brow elevation
Fig. 8.11 Aft er partial levator recession on the right side, the bilateral brow elevation is stimulated, and the left lid could be elevated via brow suspension
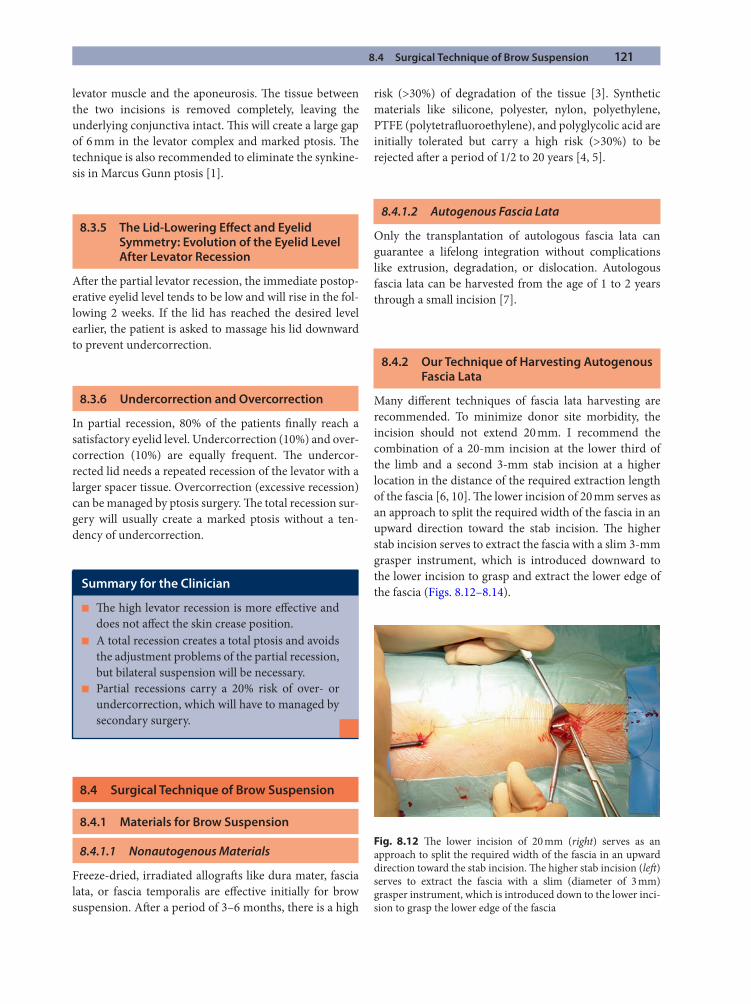
8.4 Surgical Technique of Brow Suspension 121
levator muscle and the aponeurosis. Th e tissue between the two incisions is removed completely, leaving the underlying conjunctiva intact. Th is will create a large gap of 6 mm in the levator complex and marked ptosis. Th e technique is also recommended to eliminate the synkine-sis in Marcus Gunn ptosis [1].
8.3.5 The Lid-Lowering Eff ect and Eyelid Symmetry: Evolution of the Eyelid Level After Levator Recession
Aft er the partial levator recession, the immediate postop-erative eyelid level tends to be low and will rise in the fol-lowing 2 weeks. If the lid has reached the desired level earlier, the patient is asked to massage his lid downward to prevent undercorrection.
8.3.6 Undercorrection and Overcorrection
In partial recession, 80% of the patients fi nally reach a satisfactory eyelid level. Undercorrection (10%) and over-correction (10%) are equally frequent. Th e undercor-rected lid needs a repeated recession of the levator with a larger spacer tissue. Overcorrection (excessive recession) can be managed by ptosis surgery. Th e total recession sur-gery will usually create a marked ptosis without a ten-dency of undercorrection.
8.4 Surgical Technique of Brow Suspension
8.4.1 Materials for Brow Suspension
8.4.1.1 Nonautogenous Materials
Freeze-dried, irradiated allograft s like dura mater, fascia lata, or fascia temporalis are eff ective initially for brow suspension. Aft er a period of 3–6 months, there is a high
risk (>30%) of degradation of the tissue [3]. Synthetic materials like silicone, polyester, nylon, polyethylene, PTFE (polytetrafl uoroethylene), and polyglycolic acid are initially tolerated but carry a high risk (>30%) to be rejected aft er a period of 1/2 to 20 years [4, 5].
8.4.1.2 Autogenous Fascia Lata
Only the transplantation of autologous fascia lata can guarantee a lifelong integration without complications like extrusion, degradation, or dislocation. Autologous fascia lata can be harvested from the age of 1 to 2 years through a small incision [7].
8.4.2 Our Technique of Harvesting Autogenous Fascia Lata
Many diff erent techniques of fascia lata harvesting are recommended. To minimize donor site morbidity, the incision should not extend 20 mm. I recommend the combination of a 20-mm incision at the lower third of the limb and a second 3-mm stab incision at a higher location in the distance of the required extraction length of the fascia [6, 10]. Th e lower incision of 20 mm serves as an approach to split the required width of the fascia in an upward direction toward the stab incision. Th e higher stab incision serves to extract the fascia with a slim 3-mm grasper instrument, which is introduced downward to the lower incision to grasp and extract the lower edge of the fascia (Figs. 8.12–8.14).Summary for the Clinician
Th e high levator recession is more eff ective and ■
does not aff ect the skin crease position.A total recession creates a total ptosis and avoids ■
the adjustment problems of the partial recession, but bilateral suspension will be necessary.Partial recessions carry a 20% risk of over- or ■
undercorrection, which will have to managed by secondary surgery.
Fig. 8.12 Th e lower incision of 20 mm (right) serves as an approach to split the required width of the fascia in an upward direction toward the stab incision. Th e higher stab incision (left ) serves to extract the fascia with a slim (diameter of 3 mm) grasper instrument, which is introduced down to the lower inci-sion to grasp the lower edge of the fascia
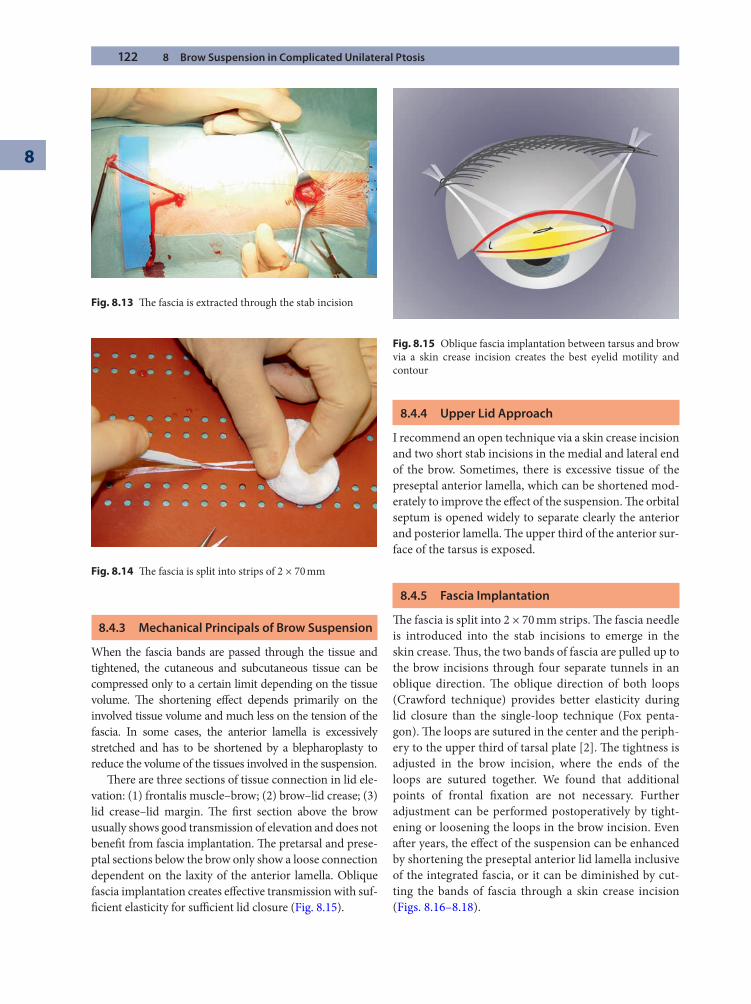
122 8 Brow Suspension in Complicated Unilateral Ptosis
8
8.4.3 Mechanical Principals of Brow Suspension
When the fascia bands are passed through the tissue and tightened, the cutaneous and subcutaneous tissue can be compressed only to a certain limit depending on the tissue volume. Th e shortening eff ect depends primarily on the involved tissue volume and much less on the tension of the fascia. In some cases, the anterior lamella is excessively stretched and has to be shortened by a blepharoplasty to reduce the volume of the tissues involved in the suspension.
Th ere are three sections of tissue connection in lid ele-vation: (1) frontalis muscle–brow; (2) brow–lid crease; (3) lid crease–lid margin. Th e fi rst section above the brow usually shows good transmission of elevation and does not benefi t from fascia implantation. Th e pretarsal and prese-ptal sections below the brow only show a loose connection dependent on the laxity of the anterior lamella. Oblique fascia implantation creates eff ective transmission with suf-fi cient elasticity for suffi cient lid closure (Fig. 8.15).
8.4.4 Upper Lid Approach
I recommend an open technique via a skin crease incision and two short stab incisions in the medial and lateral end of the brow. Sometimes, there is excessive tissue of the preseptal anterior lamella, which can be shortened mod-erately to improve the eff ect of the suspension. Th e orbital septum is opened widely to separate clearly the anterior and posterior lamella. Th e upper third of the anterior sur-face of the tarsus is exposed.
8.4.5 Fascia Implantation
Th e fascia is split into 2 × 70 mm strips. Th e fascia needle is introduced into the stab incisions to emerge in the skin crease. Th us, the two bands of fascia are pulled up to the brow incisions through four separate tunnels in an oblique direction. Th e oblique direction of both loops (Crawford technique) provides better elasticity during lid closure than the single-loop technique (Fox penta-gon). Th e loops are sutured in the center and the periph-ery to the upper third of tarsal plate [2]. Th e tightness is adjusted in the brow incision, where the ends of the loops are sutured together. We found that additional points of frontal fi xation are not necessary. Further adjustment can be performed postoperatively by tight-ening or loosening the loops in the brow incision. Even aft er years, the eff ect of the suspension can be enhanced by shortening the preseptal anterior lid lamella inclusive of the integrated fascia, or it can be diminished by cut-ting the bands of fascia through a skin crease incision (Figs. 8.16–8.18).
Fig. 8.13 Th e fascia is extracted through the stab incision
Fig. 8.14 Th e fascia is split into strips of 2 × 70 mm
Fig. 8.15 Oblique fascia implantation between tarsus and brow via a skin crease incision creates the best eyelid motility and contour
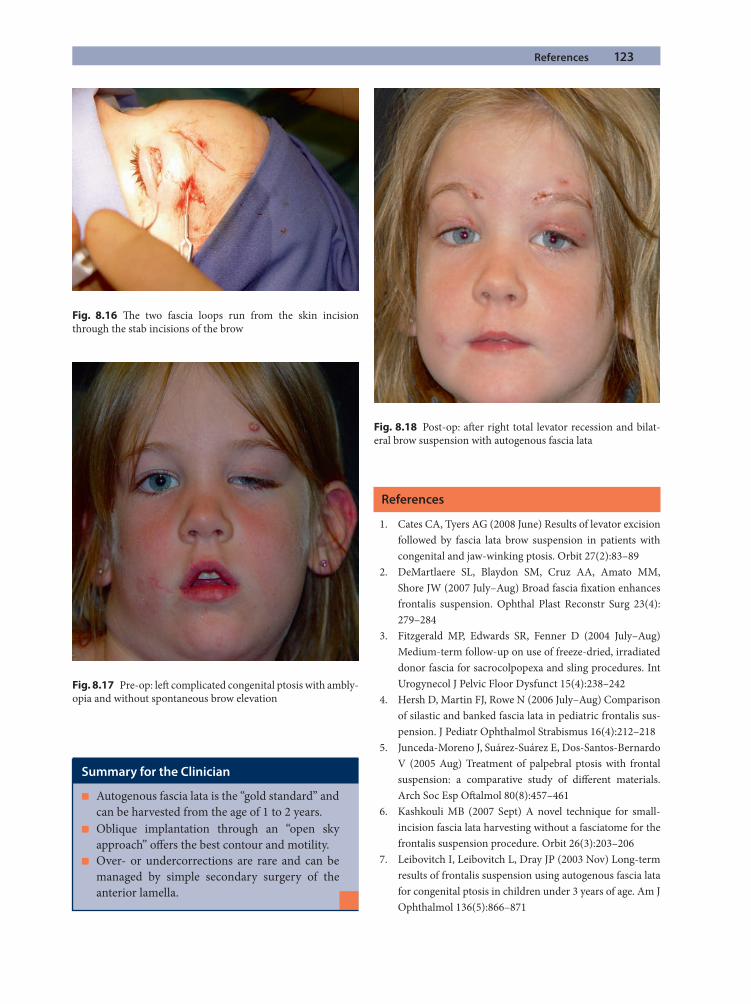
References 123
References
1. Cates CA, Tyers AG (2008 June) Results of levator excision followed by fascia lata brow suspension in patients with congenital and jaw-winking ptosis. Orbit 27(2):83–89
2. DeMartlaere SL, Blaydon SM, Cruz AA, Amato MM, Shore JW (2007 July–Aug) Broad fascia fi xation enhances frontalis suspension. Ophthal Plast Reconstr Surg 23(4): 279–284
3. Fitzgerald MP, Edwards SR, Fenner D (2004 July–Aug) Medium-term follow-up on use of freeze-dried, irradiated donor fascia for sacrocolpopexa and sling procedures. Int Urogynecol J Pelvic Floor Dysfunct 15(4):238–242
4. Hersh D, Martin FJ, Rowe N (2006 July–Aug) Comparison of silastic and banked fascia lata in pediatric frontalis sus-pension. J Pediatr Ophthalmol Strabismus 16(4):212–218
5. Junceda-Moreno J, Suárez-Suárez E, Dos-Santos-Bernardo V (2005 Aug) Treatment of palpebral ptosis with frontal suspension: a comparative study of diff erent materials. Arch Soc Esp Oft almol 80(8):457–461
6. Kashkouli MB (2007 Sept) A novel technique for small-incision fascia lata harvesting without a fasciatome for the frontalis suspension procedure. Orbit 26(3):203–206
7. Leibovitch I, Leibovitch L, Dray JP (2003 Nov) Long-term results of frontalis suspension using autogenous fascia lata for congenital ptosis in children under 3 years of age. Am J Ophthalmol 136(5):866–871
Fig. 8.16 Th e two fascia loops run from the skin incision through the stab incisions of the brow
Fig. 8.17 Pre-op: left complicated congenital ptosis with ambly-opia and without spontaneous brow elevation
Fig. 8.18 Post-op: aft er right total levator recession and bilat-eral brow suspension with autogenous fascia lata
Summary for the Clinician
Autogenous fascia lata is the “gold standard” and ■
can be harvested from the age of 1 to 2 years.Oblique implantation through an “open sky ■
approach” off ers the best contour and motility.Over- or undercorrections are rare and can be ■
managed by simple secondary surgery of the anterior lamella.
124 8 Brow Suspension in Complicated Unilateral Ptosis
8
8. Matsuo K, Yuzuriha S (2008 Jan 11) Frontalis suspension with fascia lata for severe congenital blepharoptosis using enhanced involuntary refl ex contraction of the frontals muscle. J Plast Reconstr Aesthet Surg
9. McNab AA, Galbraith JE, Friebel J, Caesar R (2004 July) Pre-Whitnall levator recession with hang-back sutures in
Graves orbitopathy. Ophthal Plast Reconstr Surg 20(4): 301–307
10. Naugle TC Jr, Fry CL, Sabatier RE, Elliot LF (1997 Sept) High leg incision fascia lata harvesting. Ophthalmology 104(9):1480–1488

Radiographic examination is an important component in the evaluation of any patient with suspected orbital disease. Such studies contribute to narrowing the diff er-ential diagnosis and oft en provide guidance in planning the most appropriate medical therapy or surgical approach. CT scanning and MRI have largely replaced older techniques, although specialized studies may still be necessary to defi ne certain lesions. Newer technolo-gies, such as PET, are adding to our repertoire of useful modalities. All of the available imaging techniques may provide some redundant information, but they each also provide some unique information not seen with other modalities. Orbital imaging should therefore never be used as a replacement for a careful and complete clinical examination and the creation of an initial diff erential diagnosis. Th is is then used to decide the most appropri-ate imaging studies that will confi rm or rule out sus-pected lesions.
9.1 Computerized Tomography
Computed tomography (CT) is an imaging technique that relies on the diff erential passage of X-rays through tissues, but unlike standard X-ray studies, CT can image soft tis-sues in addition to bone. Scans can be reconstructed in any plane through the body and contrast adjusted to max-imize visualization of specifi c tissues. CT is the imaging modality of choice for showing details of bony structures or the location of foreign bodies but is less useful for dif-ferentiating details of the optic nerve or small lesions in the orbital apex. For these, MRI is superior.
CT utilizes an array of thin, collimated X-ray beams that pass through tissue along pathways of a complex intersecting matrix (Fig. 9.1). Th e cross-sectional area defi ned by any two intersecting beams is referred to as a pixel and is analogous to a single dot in a newspaper pho-tograph. Because the X-ray beam has a certain thickness,
Modern Concepts in Orbital ImagingJonathan J. Dutton
Chapter 9
9
Core Messages
Radiologic imaging is an important adjunct to ■
the evaluation of any orbital disease and will con-tribute to establishing a likely diagnosis.Orbital imaging should not replace a careful ■
physical examination to establish a diff erential diagnosis.Each imaging modality will contribute redundant ■
data, but each also can provide unique informa-tion that may not be apparent with other imaging techniques.Computerized tomography (CT) utilizes X-rays ■
to create a two-dimensional image in any plane; this is a uniparametric modality based only on tissue transparency to the passage of X-rays.Magnetic resonance imaging (MRI) is a multi- ■
parametric modality that utilizes atomic charac-
teristics of tissue protons and their behavior in an external magnetic fi eld; the image therefore refl ects biochemical diff erences between tissues based on the molecular environment in which the proton is situated.Positron emission tomography (PET) is a newer ■
technique that images tissues based on biological activity, most specifi cally the metabolism of fl uo-ridated glucose in actively metabolizing tissues, such as tumors.Orbital ultrasound (echography) can provide ■
nonradiologic but complementary examination techniques for the detection, diff erentiation, and measurement of orbital and periorbital lesions.
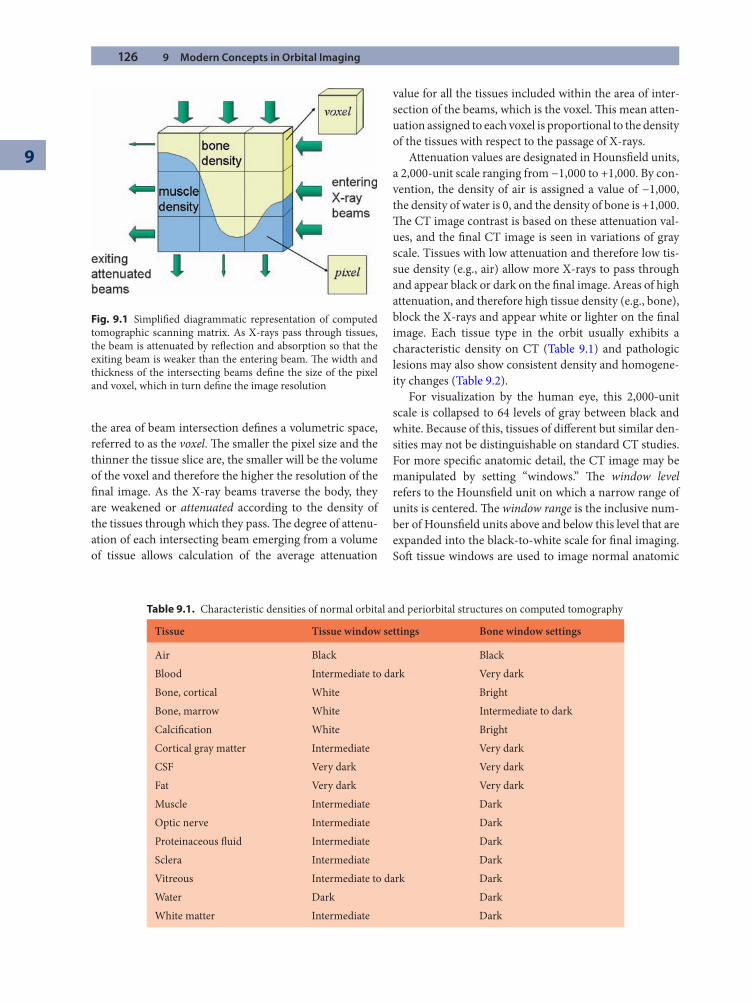
126 9 Modern Concepts in Orbital Imaging
9
the area of beam intersection defi nes a volumetric space, referred to as the voxel. Th e smaller the pixel size and the thinner the tissue slice are, the smaller will be the volume of the voxel and therefore the higher the resolution of the fi nal image. As the X-ray beams traverse the body, they are weakened or attenuated according to the density of the tissues through which they pass. Th e degree of attenu-ation of each intersecting beam emerging from a volume of tissue allows calculation of the average attenuation
value for all the tissues included within the area of inter-section of the beams, which is the voxel. Th is mean atten-uation assigned to each voxel is proportional to the density of the tissues with respect to the passage of X-rays.
Attenuation values are designated in Hounsfi eld units, a 2,000-unit scale ranging from −1,000 to +1,000. By con-vention, the density of air is assigned a value of −1,000, the density of water is 0, and the density of bone is +1,000. Th e CT image contrast is based on these attenuation val-ues, and the fi nal CT image is seen in variations of gray scale. Tissues with low attenuation and therefore low tis-sue density (e.g., air) allow more X-rays to pass through and appear black or dark on the fi nal image. Areas of high attenuation, and therefore high tissue density (e.g., bone), block the X-rays and appear white or lighter on the fi nal image. Each tissue type in the orbit usually exhibits a characteristic density on CT (Table 9.1) and pathologic lesions may also show consistent density and homogene-ity changes (Table 9.2).
For visualization by the human eye, this 2,000-unit scale is collapsed to 64 levels of gray between black and white. Because of this, tissues of diff erent but similar den-sities may not be distinguishable on standard CT studies. For more specifi c anatomic detail, the CT image may be manipulated by setting “windows.” Th e window level refers to the Hounsfi eld unit on which a narrow range of units is centered. Th e window range is the inclusive num-ber of Hounsfi eld units above and below this level that are expanded into the black-to-white scale for fi nal imaging. Soft tissue windows are used to image normal anatomic
Fig. 9.1 Simplifi ed diagrammatic representation of computed tomographic scanning matrix. As X-rays pass through tissues, the beam is attenuated by refl ection and absorption so that the exiting beam is weaker than the entering beam. Th e width and thickness of the intersecting beams defi ne the size of the pixel and voxel, which in turn defi ne the image resolution
Table 9.1. Characteristic densities of normal orbital and periorbital structures on computed tomography
Tissue Tissue window settings Bone window settings
Air Black BlackBlood Intermediate to dark Very darkBone, cortical White BrightBone, marrow White Intermediate to darkCalcifi cation White BrightCortical gray matter Intermediate Very darkCSF Very dark Very darkFat Very dark Very darkMuscle Intermediate DarkOptic nerve Intermediate DarkProteinaceous fl uid Intermediate DarkSclera Intermediate DarkVitreous Intermediate to dark DarkWater Dark DarkWhite matter Intermediate Dark
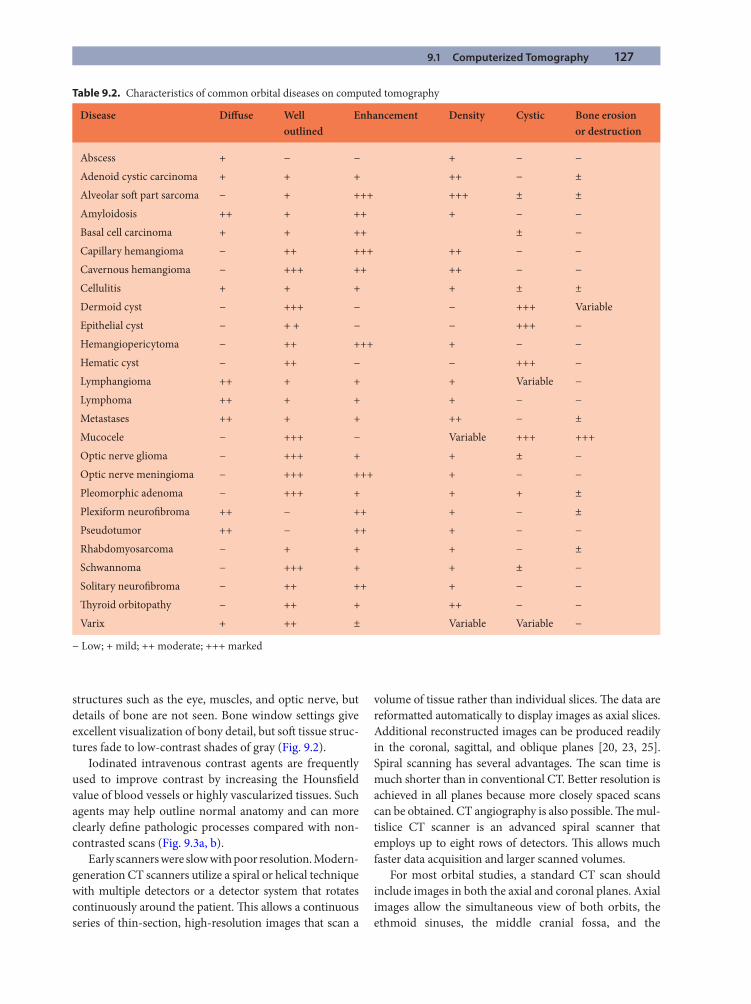
9.1 Computerized Tomography 127
structures such as the eye, muscles, and optic nerve, but details of bone are not seen. Bone window settings give excellent visualization of bony detail, but soft tissue struc-tures fade to low-contrast shades of gray (Fig. 9.2).
Iodinated intravenous contrast agents are frequently used to improve contrast by increasing the Hounsfi eld value of blood vessels or highly vascularized tissues. Such agents may help outline normal anatomy and can more clearly defi ne pathologic processes compared with non-contrasted scans (Fig. 9.3a, b).
Early scanners were slow with poor resolution. Modern-generation CT scanners utilize a spiral or helical technique with multiple detectors or a detector system that rotates continuously around the patient. Th is allows a continuous series of thin-section, high-resolution images that scan a
volume of tissue rather than individual slices. Th e data are reformatted automatically to display images as axial slices. Additional reconstructed images can be produced readily in the coronal, sagittal, and oblique planes [20, 23, 25]. Spiral scanning has several advantages. Th e scan time is much shorter than in conventional CT. Better resolution is achieved in all planes because more closely spaced scans can be obtained. CT angiography is also possible. Th e mul-tislice CT scanner is an advanced spiral scanner that employs up to eight rows of detectors. Th is allows much faster data acquisition and larger scanned volumes.
For most orbital studies, a standard CT scan should include images in both the axial and coronal planes. Axial images allow the simultaneous view of both orbits, the ethmoid sinuses, the middle cranial fossa, and the
Table 9.2. Characteristics of common orbital diseases on computed tomography
Disease Diff use Well outlined
Enhancement Density Cystic Bone erosion or destruction
Abscess + − − + − −Adenoid cystic carcinoma + + + ++ − ±Alveolar soft part sarcoma − + +++ +++ ± ±Amyloidosis ++ + ++ + − −Basal cell carcinoma + + ++ ± −Capillary hemangioma − ++ +++ ++ − −Cavernous hemangioma − +++ ++ ++ − −Cellulitis + + + + ± ±Dermoid cyst − +++ − − +++ VariableEpithelial cyst − + + − − +++ −Hemangiopericytoma − ++ +++ + − −Hematic cyst − ++ − − +++ −Lymphangioma ++ + + + Variable −Lymphoma ++ + + + − −Metastases ++ + + ++ − ±Mucocele − +++ − Variable +++ +++Optic nerve glioma − +++ + + ± −Optic nerve meningioma − +++ +++ + − −Pleomorphic adenoma − +++ + + + ±Plexiform neurofi broma ++ − ++ + − ±Pseudotumor ++ − ++ + − −Rhabdomyosarcoma − + + + − ±Schwannoma − +++ + + ± −Solitary neurofi broma − ++ ++ + − −Th yroid orbitopathy − ++ + ++ − −Varix + ++ ± Variable Variable −
− Low; + mild; ++ moderate; +++ marked
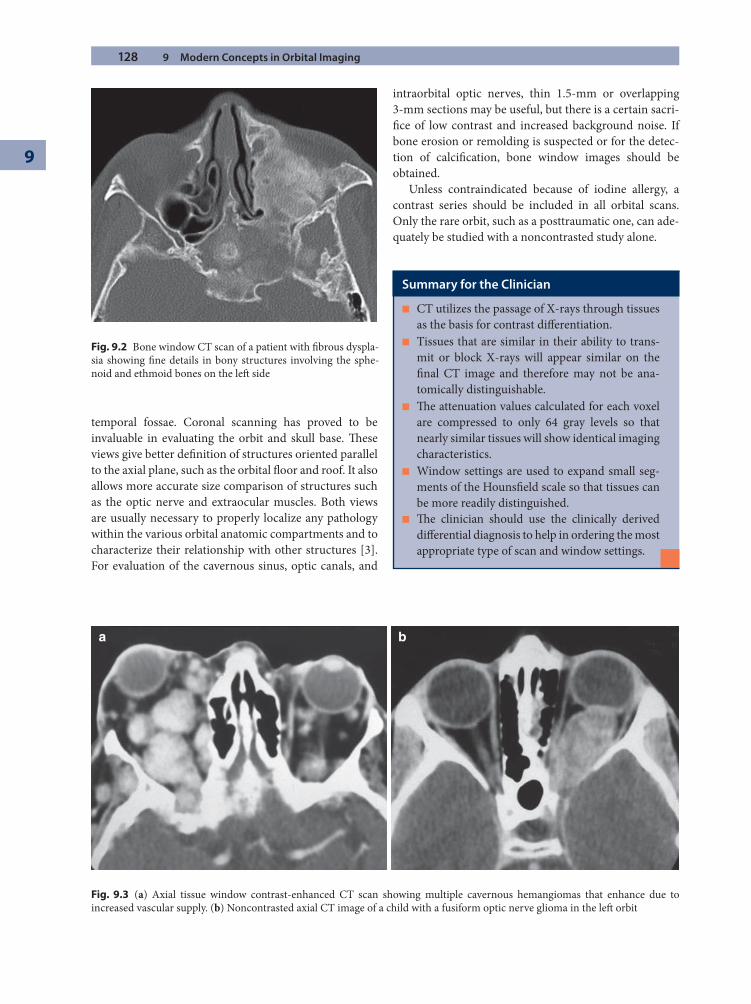
128 9 Modern Concepts in Orbital Imaging
9
temporal fossae. Coronal scanning has proved to be invaluable in evaluating the orbit and skull base. Th ese views give better defi nition of structures oriented parallel to the axial plane, such as the orbital fl oor and roof. It also allows more accurate size comparison of structures such as the optic nerve and extraocular muscles. Both views are usually necessary to properly localize any pathology within the various orbital anatomic compartments and to characterize their relationship with other structures [3]. For evaluation of the cavernous sinus, optic canals, and
intraorbital optic nerves, thin 1.5-mm or overlapping 3-mm sections may be useful, but there is a certain sacri-fi ce of low contrast and increased background noise. If bone erosion or remolding is suspected or for the detec-tion of calcifi cation, bone window images should be obtained.
Unless contraindicated because of iodine allergy, a contrast series should be included in all orbital scans. Only the rare orbit, such as a posttraumatic one, can ade-quately be studied with a noncontrasted study alone.
Fig. 9.2 Bone window CT scan of a patient with fi brous dyspla-sia showing fi ne details in bony structures involving the sphe-noid and ethmoid bones on the left side
a b
Fig. 9.3 (a) Axial tissue window contrast-enhanced CT scan showing multiple cavernous hemangiomas that enhance due to increased vascular supply. (b) Noncontrasted axial CT image of a child with a fusiform optic nerve glioma in the left orbit
Summary for the Clinician
CT utilizes the passage of X-rays through tissues ■
as the basis for contrast diff erentiation.Tissues that are similar in their ability to trans- ■
mit or block X-rays will appear similar on the fi nal CT image and therefore may not be ana-tomically distinguishable.Th e attenuation values calculated for each voxel ■
are compressed to only 64 gray levels so that nearly similar tissues will show identical imaging characteristics.Window settings are used to expand small seg- ■
ments of the Hounsfi eld scale so that tissues can be more readily distinguished.Th e clinician should use the clinically derived ■
diff erential diagnosis to help in ordering the most appropriate type of scan and window settings.
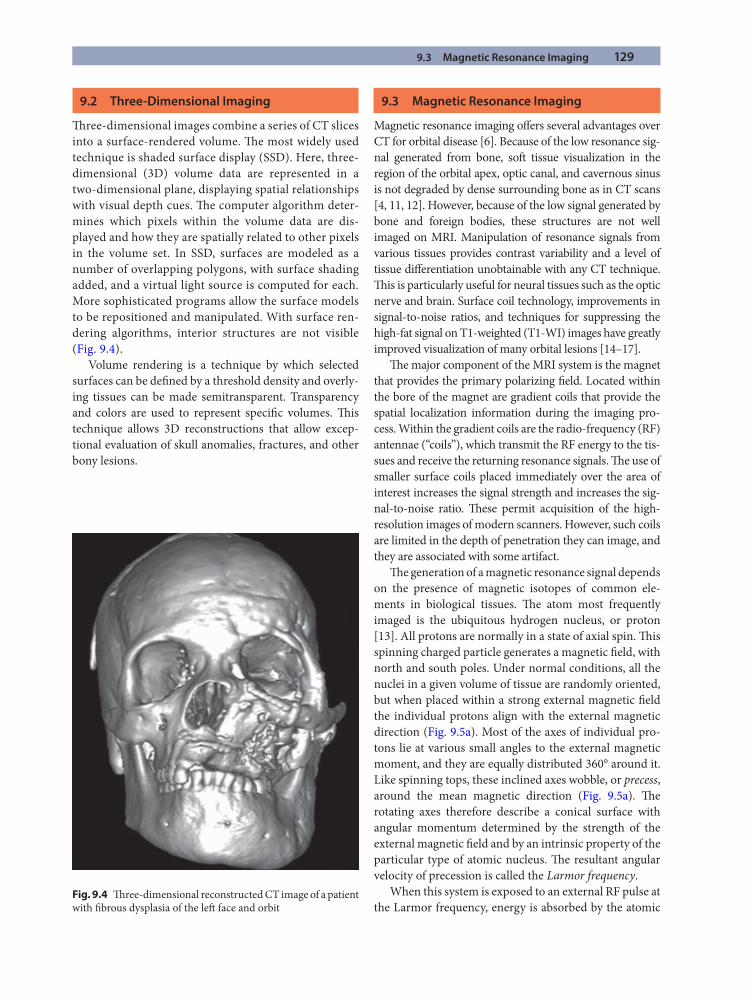
9.3 Magnetic Resonance Imaging 129
9.2 Three-Dimensional Imaging
Th ree-dimensional images combine a series of CT slices into a surface-rendered volume. Th e most widely used technique is shaded surface display (SSD). Here, three-dimensional (3D) volume data are represented in a two-dimensional plane, displaying spatial relationships with visual depth cues. Th e computer algorithm deter-mines which pixels within the volume data are dis-played and how they are spatially related to other pixels in the volume set. In SSD, surfaces are modeled as a number of overlapping polygons, with surface shading added, and a virtual light source is computed for each. More sophisticated programs allow the surface models to be repositioned and manipulated. With surface ren-dering algorithms, interior structures are not visible (Fig. 9.4).
Volume rendering is a technique by which selected surfaces can be defi ned by a threshold density and overly-ing tissues can be made semitransparent. Transparency and colors are used to represent specifi c volumes. Th is technique allows 3D reconstructions that allow excep-tional evaluation of skull anomalies, fractures, and other bony lesions.
9.3 Magnetic Resonance Imaging
Magnetic resonance imaging off ers several advantages over CT for orbital disease [6]. Because of the low resonance sig-nal generated from bone, soft tissue visualization in the region of the orbital apex, optic canal, and cavernous sinus is not degraded by dense surrounding bone as in CT scans [4, 11, 12]. However, because of the low signal generated by bone and foreign bodies, these structures are not well imaged on MRI. Manipulation of resonance signals from various tissues provides contrast variability and a level of tissue diff erentiation unobtainable with any CT technique. Th is is particularly useful for neural tissues such as the optic nerve and brain. Surface coil technology, improvements in signal-to-noise ratios, and techniques for suppressing the high-fat signal on T1-weighted (T1-WI) images have greatly improved visualization of many orbital lesions [14–17].
Th e major component of the MRI system is the magnet that provides the primary polarizing fi eld. Located within the bore of the magnet are gradient coils that provide the spatial localization information during the imaging pro-cess. Within the gradient coils are the radio-frequency (RF) antennae (“coils”), which transmit the RF energy to the tis-sues and receive the returning resonance signals. Th e use of smaller surface coils placed immediately over the area of interest increases the signal strength and increases the sig-nal-to-noise ratio. Th ese permit acquisition of the high-resolution images of modern scanners. However, such coils are limited in the depth of penetration they can image, and they are associated with some artifact.
Th e generation of a magnetic resonance signal depends on the presence of magnetic isotopes of common ele-ments in biological tissues. Th e atom most frequently imaged is the ubiquitous hydrogen nucleus, or proton [13]. All protons are normally in a state of axial spin. Th is spinning charged particle generates a magnetic fi eld, with north and south poles. Under normal conditions, all the nuclei in a given volume of tissue are randomly oriented, but when placed within a strong external magnetic fi eld the individual protons align with the external magnetic direction (Fig. 9.5a). Most of the axes of individual pro-tons lie at various small angles to the external magnetic moment, and they are equally distributed 360° around it. Like spinning tops, these inclined axes wobble, or precess, around the mean magnetic direction (Fig. 9.5a). Th e rotating axes therefore describe a conical surface with angular momentum determined by the strength of the external magnetic fi eld and by an intrinsic property of the particular type of atomic nucleus. Th e resultant angular velocity of precession is called the Larmor frequency.
When this system is exposed to an external RF pulse at the Larmor frequency, energy is absorbed by the atomic
Fig. 9.4 Th ree-dimensional reconstructed CT image of a patient with fi brous dysplasia of the left face and orbit
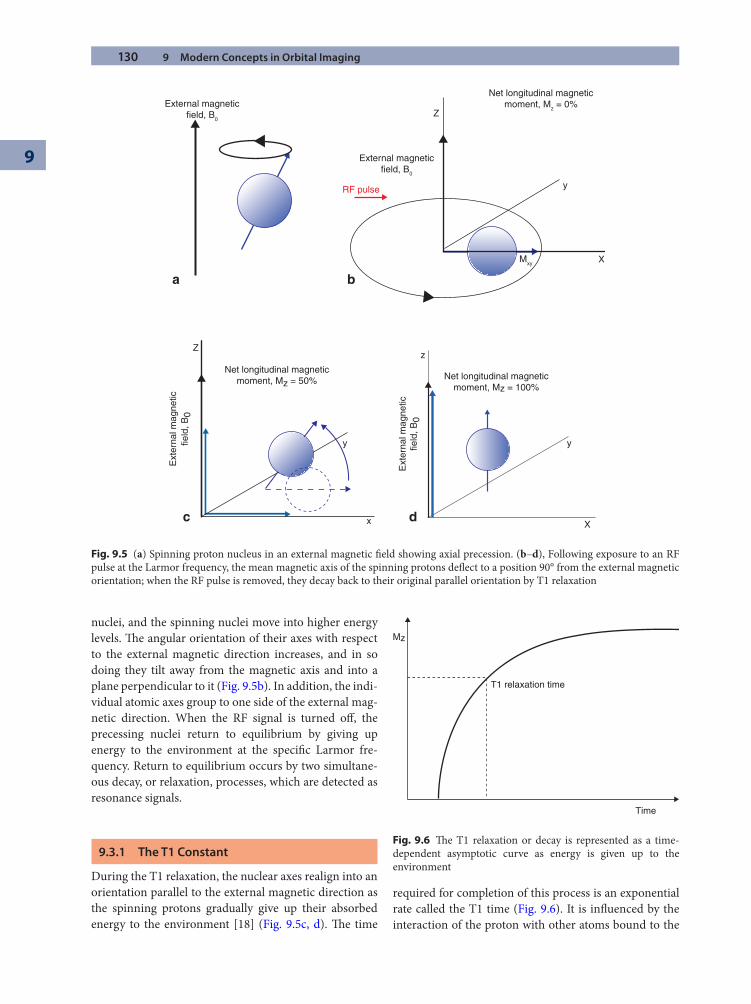
130 9 Modern Concepts in Orbital Imaging
9
nuclei, and the spinning nuclei move into higher energy levels. Th e angular orientation of their axes with respect to the external magnetic direction increases, and in so doing they tilt away from the magnetic axis and into a plane perpendicular to it (Fig. 9.5b). In addition, the indi-vidual atomic axes group to one side of the external mag-netic direction. When the RF signal is turned off , the precessing nuclei return to equilibrium by giving up energy to the environment at the specifi c Larmor fre-quency. Return to equilibrium occurs by two simultane-ous decay, or relaxation, processes, which are detected as resonance signals.
9.3.1 The T1 Constant
During the T1 relaxation, the nuclear axes realign into an orientation parallel to the external magnetic direction as the spinning protons gradually give up their absorbed energy to the environment [18] (Fig. 9.5c, d). Th e time
required for completion of this process is an exponential rate called the T1 time (Fig. 9.6). It is infl uenced by the interaction of the proton with other atoms bound to the
External magneticfield, B0
External magneticfield, B0
RF pulse
Z
y
XMxy
Net longitudinal magneticmoment, Mz = 0%
Net longitudinal magneticmoment, Mz = 50%
Z
Ext
erna
l mag
netic
field
, B0
x
y
Ext
erna
l mag
netic
field
, B0
Net longitudinal magneticmoment, Mz = 100%
z
X
y
a
c d
b
Fig. 9.5 (a) Spinning proton nucleus in an external magnetic fi eld showing axial precession. (b–d), Following exposure to an RF pulse at the Larmor frequency, the mean magnetic axis of the spinning protons defl ect to a position 90° from the external magnetic orientation; when the RF pulse is removed, they decay back to their original parallel orientation by T1 relaxation
T1 relaxation time
Time
Mz
Fig. 9.6 Th e T1 relaxation or decay is represented as a time-dependent asymptotic curve as energy is given up to the environment

9.3 Magnetic Resonance Imaging 131
molecular lattice, by temperature, and by viscosity of the tissue. At any specifi c time following the RF pulse, the total amount of energy given up by the spinning protons depends on the rate at which the T1 relaxation occurs. Tissues with a short T1 constant, such as fat, give up more resonant energy per unit time and therefore appear brighter on the fi nal MR (magnetic resonance) image than tissues with longer T1 constants, such as muscle. Th is is the basis for contrast intensity, and specifi c orbital tissues will demonstrate characteristic T1 signal intensi-ties (see Table 9.3).
9.3.2 The T2 Constant
Immediately following the RF pulse, the atomic nuclei are grouped on one side of the mean magnetic axis (Fig. 9.7a). As they rotate, they generate an RF signal as they cut across the external magnetic fi eld and thus generate a small alternating current voltage. During the T2 relax-ation, the atomic nuclei redistribute themselves evenly 360° around the external magnetic fi eld direction (Fig. 9.7b). As they do so, the strength of this induced signal decreases because of the increasing canceling vectors. Th e time for complete decay of this signal (i.e., even distribution of magnetic moments) is the T2, or spin–spin relaxation
time, and is infl uenced by the tiny magnetic fi elds gener-ated around adjacent spinning nuclei (Fig. 9.8). As with T1 constants, biochemical diff erences between tissues confer slightly diff erent T2 relaxation times to their pro-tons. At any specifi c time following the RF pulse, tissues with long T2 constants, such as vitreous, maintain a greater transverse vector component than tissues with short T2 constants, such as muscle. Th is greater trans-verse vector produces a higher signal and is therefore brighter on the fi nal MR image.
9.3.3 Creating the MR Image
Th e signals generated by the T1 relaxation and the T2 decay are measured by RF detectors. Th ey will detect in mass fashion all similar signals at the Larmor frequency, regardless of their specifi c location within the tissue. Spatial encoding of resonant signals from particular small volumes of tissue is necessary for the creation of a mean-ingful two-dimensional image. Th is is achieved by defor-mation of the external magnetic fi eld using gradient coils, such that the protons in every small volume of examined tissue (voxel) has a unique magnetic fi eld strength and therefore a unique Larmor frequency. Th e detected Larmor frequency therefore will identify the precise
Table 9.3. Characteristic signal intensities of normal orbital and periorbital structures on magnetic resonance imaging
Tissue T1-WI T2-WI
Air Very dark Very darkBlood, acute Dark to intermediate DarkBlood, chronic Dark rim with variable center Dark rim with variable centerBlood, hyperacute Intermediate IntermediateBlood, subacute Bright rim BrightBone, cortical Very dark Very darkBone, marrow Bright IntermediateCortical gray matter Dark BrightCSF Very dark Very brightFat Very bright Intermediate to darkMuscle Dark DarkOptic nerve Dark to intermediate IntermediateProteinaceous fl uid Intermediate to bright Very brightSclera Dark to intermediate IntermediateVitreous Dark BrightWater Very dark Very brightWhite matter Bright Dark
T1-WI T1 weighted image, T2-WI T2 weighted image
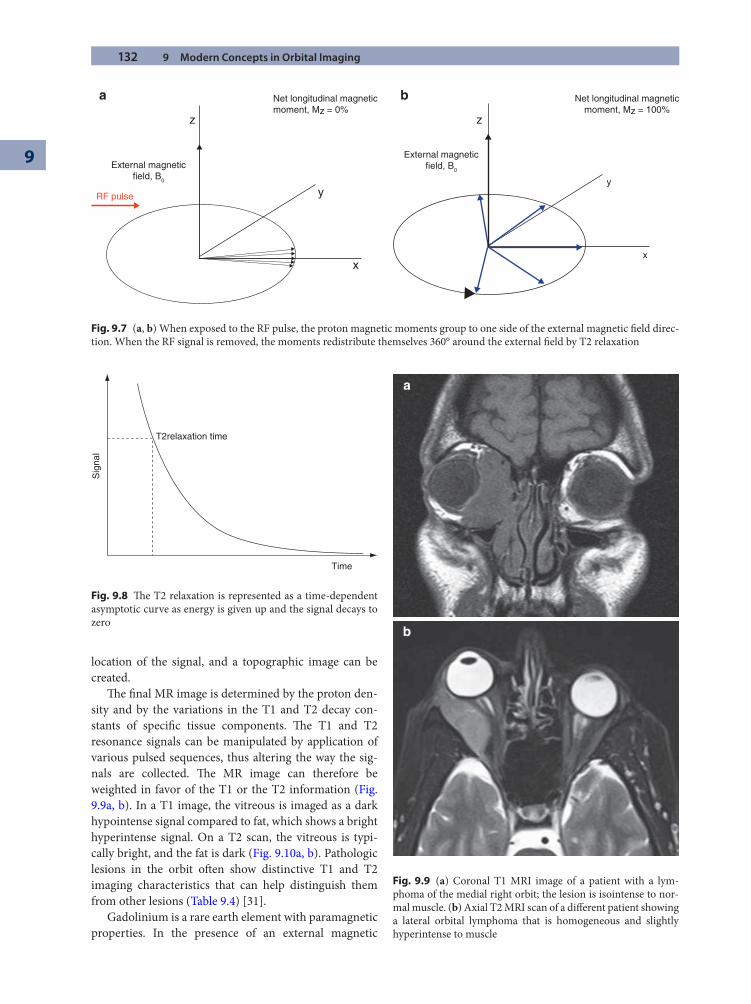
132 9 Modern Concepts in Orbital Imaging
9
location of the signal, and a topographic image can be created.
Th e fi nal MR image is determined by the proton den-sity and by the variations in the T1 and T2 decay con-stants of specifi c tissue components. Th e T1 and T2 resonance signals can be manipulated by application of various pulsed sequences, thus altering the way the sig-nals are collected. Th e MR image can therefore be weighted in favor of the T1 or the T2 information (Fig. 9.9a, b). In a T1 image, the vitreous is imaged as a dark hypointense signal compared to fat, which shows a bright hyperintense signal. On a T2 scan, the vitreous is typi-cally bright, and the fat is dark (Fig. 9.10a, b). Pathologic lesions in the orbit oft en show distinctive T1 and T2 imaging characteristics that can help distinguish them from other lesions (Table 9.4) [31].
Gadolinium is a rare earth element with paramagnetic properties. In the presence of an external magnetic
y
x
External magneticfield, B0
RF pulse
Net longitudinal magneticmoment, Mz = 0%
z z
Net longitudinal magneticmoment, Mz = 100%
External magneticfield, B0
y
x
a b
Fig. 9.7 (a, b) When exposed to the RF pulse, the proton magnetic moments group to one side of the external magnetic fi eld direc-tion. When the RF signal is removed, the moments redistribute themselves 360° around the external fi eld by T2 relaxation
T2relaxation time
Sig
nal
Time
Fig. 9.8 Th e T2 relaxation is represented as a time-dependent asymptotic curve as energy is given up and the signal decays to zero
a
b
Fig. 9.9 (a) Coronal T1 MRI image of a patient with a lym-phoma of the medial right orbit; the lesion is isointense to nor-mal muscle. (b) Axial T2 MRI scan of a diff erent patient showing a lateral orbital lymphoma that is homogeneous and slightly hyperintense to muscle
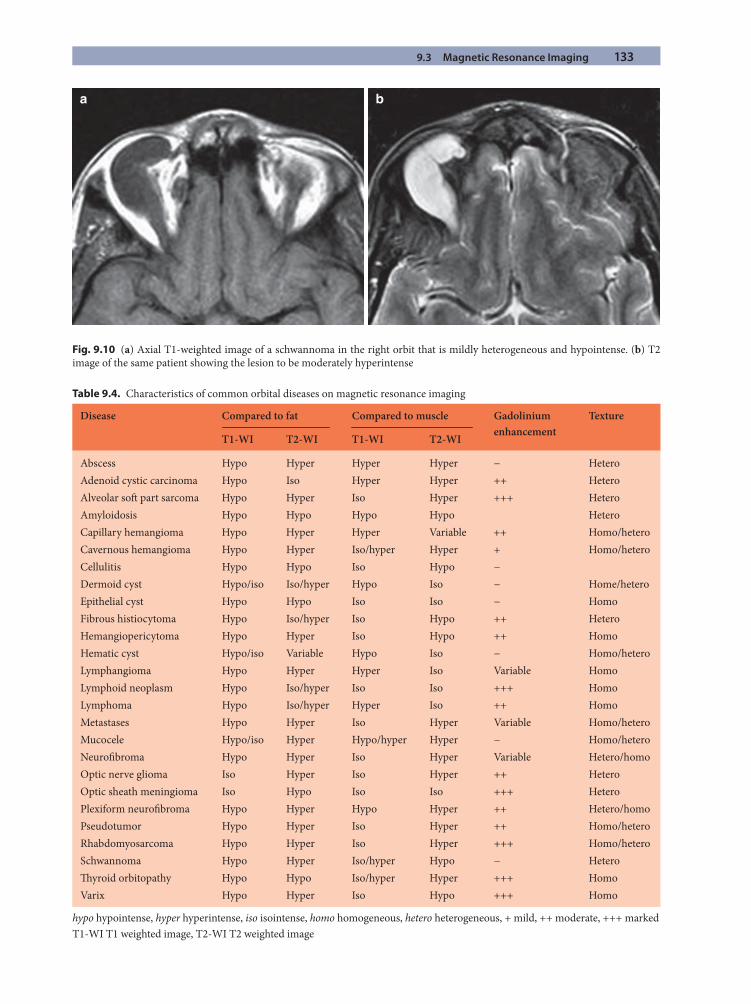
9.3 Magnetic Resonance Imaging 133
Table 9.4. Characteristics of common orbital diseases on magnetic resonance imaging
Disease Compared to fat Compared to muscle Gadolinium enhancement
Texture
T1-WI T2-WI T1-WI T2-WI
Abscess Hypo Hyper Hyper Hyper − HeteroAdenoid cystic carcinoma Hypo Iso Hyper Hyper ++ HeteroAlveolar soft part sarcoma Hypo Hyper Iso Hyper +++ HeteroAmyloidosis Hypo Hypo Hypo Hypo HeteroCapillary hemangioma Hypo Hyper Hyper Variable ++ Homo/heteroCavernous hemangioma Hypo Hyper Iso/hyper Hyper + Homo/heteroCellulitis Hypo Hypo Iso Hypo −Dermoid cyst Hypo/iso Iso/hyper Hypo Iso − Home/heteroEpithelial cyst Hypo Hypo Iso Iso − HomoFibrous histiocytoma Hypo Iso/hyper Iso Hypo ++ HeteroHemangiopericytoma Hypo Hyper Iso Hypo ++ HomoHematic cyst Hypo/iso Variable Hypo Iso − Homo/heteroLymphangioma Hypo Hyper Hyper Iso Variable HomoLymphoid neoplasm Hypo Iso/hyper Iso Iso +++ HomoLymphoma Hypo Iso/hyper Hyper Iso ++ HomoMetastases Hypo Hyper Iso Hyper Variable Homo/heteroMucocele Hypo/iso Hyper Hypo/hyper Hyper − Homo/heteroNeurofi broma Hypo Hyper Iso Hyper Variable Hetero/homoOptic nerve glioma Iso Hyper Iso Hyper ++ HeteroOptic sheath meningioma Iso Hypo Iso Iso +++ HeteroPlexiform neurofi broma Hypo Hyper Hypo Hyper ++ Hetero/homoPseudotumor Hypo Hyper Iso Hyper ++ Homo/heteroRhabdomyosarcoma Hypo Hyper Iso Hyper +++ Homo/heteroSchwannoma Hypo Hyper Iso/hyper Hypo − HeteroTh yroid orbitopathy Hypo Hypo Iso/hyper Hyper +++ HomoVarix Hypo Hyper Iso Hypo +++ Homo
hypo hypointense, hyper hyperintense, iso isointense, homo homogeneous, hetero heterogeneous, + mild, ++ moderate, +++ markedT1-WI T1 weighted image, T2-WI T2 weighted image
a b
Fig. 9.10 (a) Axial T1-weighted image of a schwannoma in the right orbit that is mildly heterogeneous and hypointense. (b) T2 image of the same patient showing the lesion to be moderately hyperintense
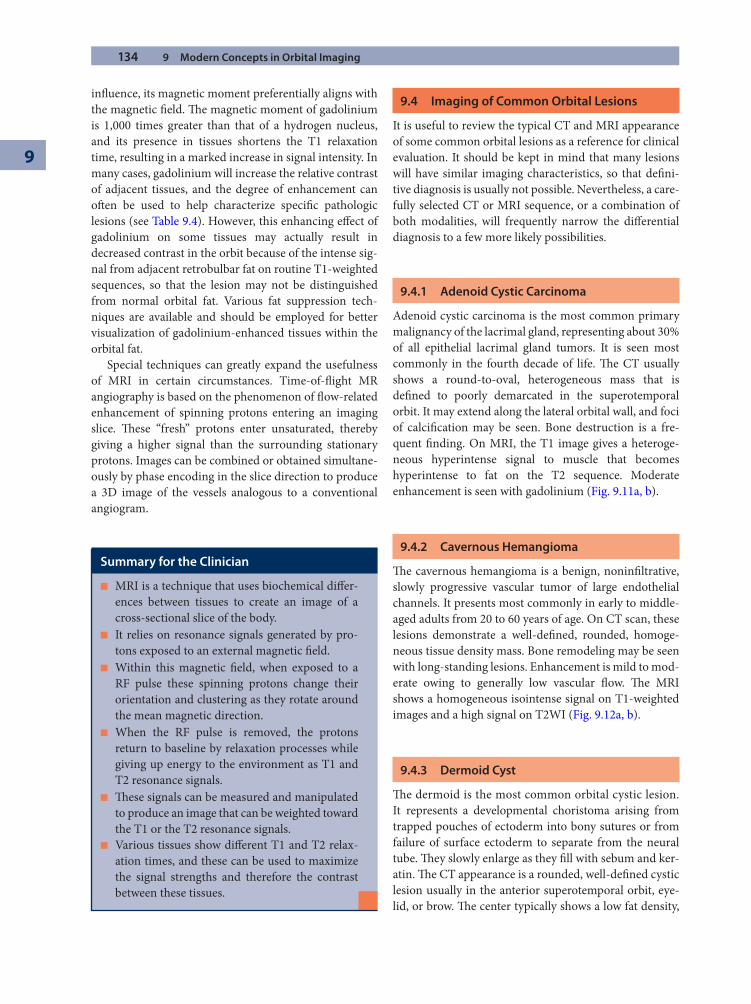
134 9 Modern Concepts in Orbital Imaging
9
infl uence, its magnetic moment preferentially aligns with the magnetic fi eld. Th e magnetic moment of gadolinium is 1,000 times greater than that of a hydrogen nucleus, and its presence in tissues shortens the T1 relaxation time, resulting in a marked increase in signal intensity. In many cases, gadolinium will increase the relative contrast of adjacent tissues, and the degree of enhancement can oft en be used to help characterize specifi c pathologic lesions (see Table 9.4). However, this enhancing eff ect of gadolinium on some tissues may actually result in decreased contrast in the orbit because of the intense sig-nal from adjacent retrobulbar fat on routine T1-weighted sequences, so that the lesion may not be distinguished from normal orbital fat. Various fat suppression tech-niques are available and should be employed for better visualization of gadolinium-enhanced tissues within the orbital fat.
Special techniques can greatly expand the usefulness of MRI in certain circumstances. Time-of-fl ight MR angiography is based on the phenomenon of fl ow-related enhancement of spinning protons entering an imaging slice. Th ese “fresh” protons enter unsaturated, thereby giving a higher signal than the surrounding stationary protons. Images can be combined or obtained simultane-ously by phase encoding in the slice direction to produce a 3D image of the vessels analogous to a conventional angiogram.
9.4 Imaging of Common Orbital Lesions
It is useful to review the typical CT and MRI appearance of some common orbital lesions as a reference for clinical evaluation. It should be kept in mind that many lesions will have similar imaging characteristics, so that defi ni-tive diagnosis is usually not possible. Nevertheless, a care-fully selected CT or MRI sequence, or a combination of both modalities, will frequently narrow the diff erential diagnosis to a few more likely possibilities.
9.4.1 Adenoid Cystic Carcinoma
Adenoid cystic carcinoma is the most common primary malignancy of the lacrimal gland, representing about 30% of all epithelial lacrimal gland tumors. It is seen most commonly in the fourth decade of life. Th e CT usually shows a round-to-oval, heterogeneous mass that is defi ned to poorly demarcated in the superotemporal orbit. It may extend along the lateral orbital wall, and foci of calcifi cation may be seen. Bone destruction is a fre-quent fi nding. On MRI, the T1 image gives a heteroge-neous hyperintense signal to muscle that becomes hyperintense to fat on the T2 sequence. Moderate enhancement is seen with gadolinium (Fig. 9.11a, b).
9.4.2 Cavernous Hemangioma
Th e cavernous hemangioma is a benign, noninfi ltrative, slowly progressive vascular tumor of large endothelial channels. It presents most commonly in early to middle-aged adults from 20 to 60 years of age. On CT scan, these lesions demonstrate a well-defi ned, rounded, homoge-neous tissue density mass. Bone remodeling may be seen with long-standing lesions. Enhancement is mild to mod-erate owing to generally low vascular fl ow. Th e MRI shows a homogeneous isointense signal on T1-weighted images and a high signal on T2WI (Fig. 9.12a, b).
9.4.3 Dermoid Cyst
Th e dermoid is the most common orbital cystic lesion. It represents a developmental choristoma arising from trapped pouches of ectoderm into bony sutures or from failure of surface ectoderm to separate from the neural tube. Th ey slowly enlarge as they fi ll with sebum and ker-atin. Th e CT appearance is a rounded, well-defi ned cystic lesion usually in the anterior superotemporal orbit, eye-lid, or brow. Th e center typically shows a low fat density,
Summary for the Clinician
MRI is a technique that uses biochemical diff er- ■
ences between tissues to create an image of a cross-sectional slice of the body.It relies on resonance signals generated by pro- ■
tons exposed to an external magnetic fi eld.Within this magnetic fi eld, when exposed to a ■
RF pulse these spinning protons change their orientation and clustering as they rotate around the mean magnetic direction.When the RF pulse is removed, the protons ■
return to baseline by relaxation processes while giving up energy to the environment as T1 and T2 resonance signals.Th ese signals can be measured and manipulated ■
to produce an image that can be weighted toward the T1 or the T2 resonance signals.Various tissues show diff erent T1 and T2 relax- ■
ation times, and these can be used to maximize the signal strengths and therefore the contrast between these tissues.
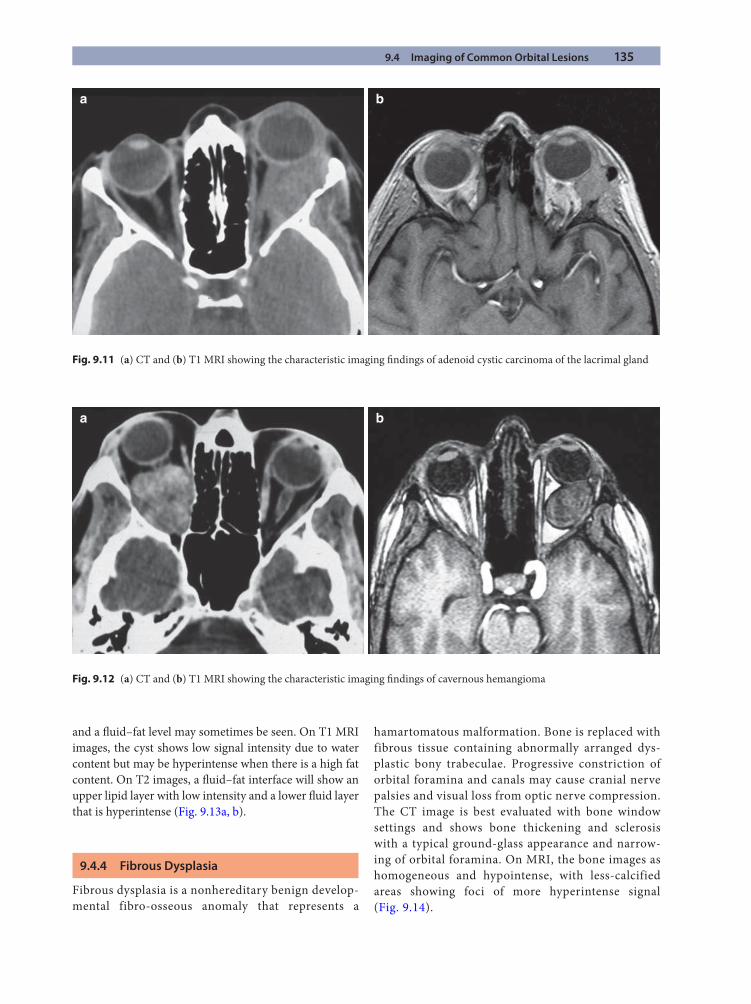
9.4 Imaging of Common Orbital Lesions 135
and a fl uid–fat level may sometimes be seen. On T1 MRI images, the cyst shows low signal intensity due to water content but may be hyperintense when there is a high fat content. On T2 images, a fl uid–fat interface will show an upper lipid layer with low intensity and a lower fl uid layer that is hyperintense (Fig. 9.13a, b).
9.4.4 Fibrous Dysplasia
Fibrous dysplasia is a nonhereditary benign develop-mental fibro-osseous anomaly that represents a
hamartomatous malformation. Bone is replaced with fibrous tissue containing abnormally arranged dys-plastic bony trabeculae. Progressive constriction of orbital foramina and canals may cause cranial nerve palsies and visual loss from optic nerve compression. The CT image is best evaluated with bone window settings and shows bone thickening and sclerosis with a typical ground-glass appearance and narrow-ing of orbital foramina. On MRI, the bone images as homogeneous and hypointense, with less-calcified areas showing foci of more hyperintense signal (Fig. 9.14).
a b
Fig. 9.11 (a) CT and (b) T1 MRI showing the characteristic imaging fi ndings of adenoid cystic carcinoma of the lacrimal gland
a b
Fig. 9.12 (a) CT and (b) T1 MRI showing the characteristic imaging fi ndings of cavernous hemangioma
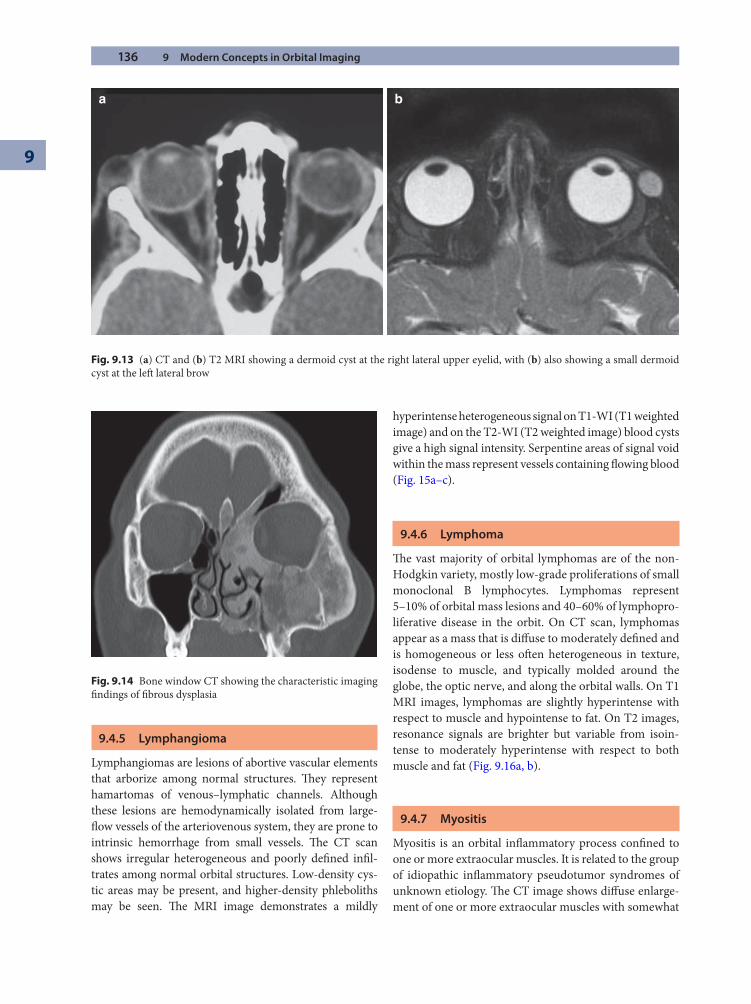
136 9 Modern Concepts in Orbital Imaging
9
9.4.5 Lymphangioma
Lymphangiomas are lesions of abortive vascular elements that arborize among normal structures. Th ey represent hamartomas of venous–lymphatic channels. Although these lesions are hemodynamically isolated from large-fl ow vessels of the arteriovenous system, they are prone to intrinsic hemorrhage from small vessels. Th e CT scan shows irregular heterogeneous and poorly defi ned infi l-trates among normal orbital structures. Low-density cys-tic areas may be present, and higher-density phleboliths may be seen. Th e MRI image demonstrates a mildly
hyperintense heterogeneous signal on T1-WI (T1 weighted image) and on the T2-WI (T2 weighted image) blood cysts give a high signal intensity. Serpentine areas of signal void within the mass represent vessels containing fl owing blood (Fig. 15a–c).
9.4.6 Lymphoma
Th e vast majority of orbital lymphomas are of the non-Hodgkin variety, mostly low-grade proliferations of small monoclonal B lymphocytes. Lymphomas represent 5–10% of orbital mass lesions and 40–60% of lymphopro-liferative disease in the orbit. On CT scan, lymphomas appear as a mass that is diff use to moderately defi ned and is homogeneous or less oft en heterogeneous in texture, isodense to muscle, and typically molded around the globe, the optic nerve, and along the orbital walls. On T1 MRI images, lymphomas are slightly hyperintense with respect to muscle and hypointense to fat. On T2 images, resonance signals are brighter but variable from isoin-tense to moderately hyperintense with respect to both muscle and fat (Fig. 9.16a, b).
9.4.7 Myositis
Myositis is an orbital infl ammatory process confi ned to one or more extraocular muscles. It is related to the group of idiopathic infl ammatory pseudotumor syndromes of unknown etiology. Th e CT image shows diff use enlarge-ment of one or more extraocular muscles with somewhat
a b
Fig. 9.13 (a) CT and (b) T2 MRI showing a dermoid cyst at the right lateral upper eyelid, with (b) also showing a small dermoid cyst at the left lateral brow
Fig. 9.14 Bone window CT showing the characteristic imaging fi ndings of fi brous dysplasia
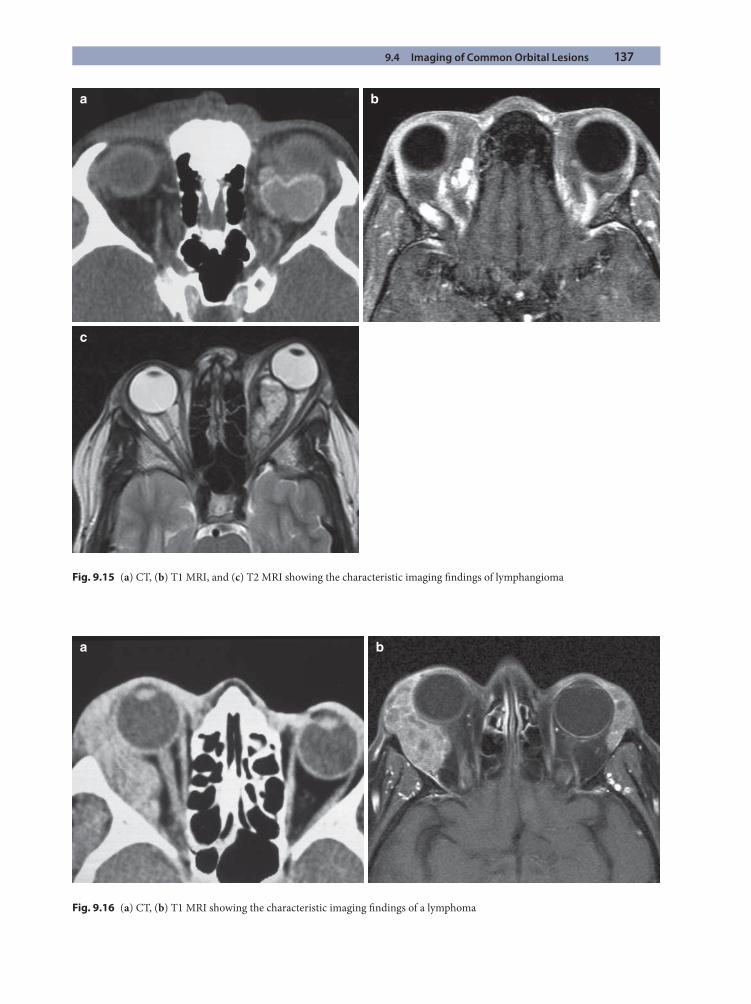
9.4 Imaging of Common Orbital Lesions 137
Fig. 9.15 (a) CT, (b) T1 MRI, and (c) T2 MRI showing the characteristic imaging fi ndings of lymphangioma
a b
c
a b
Fig. 9.16 (a) CT, (b) T1 MRI showing the characteristic imaging fi ndings of a lymphoma
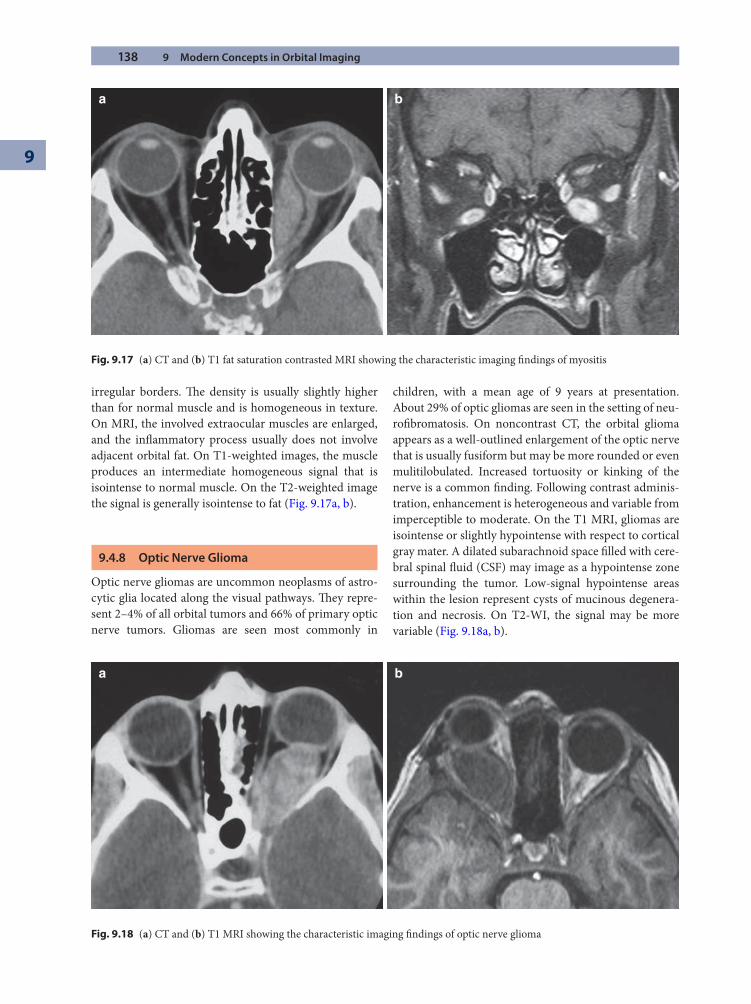
138 9 Modern Concepts in Orbital Imaging
9
irregular borders. Th e density is usually slightly higher than for normal muscle and is homogeneous in texture. On MRI, the involved extraocular muscles are enlarged, and the infl ammatory process usually does not involve adjacent orbital fat. On T1-weighted images, the muscle produces an intermediate homogeneous signal that is isointense to normal muscle. On the T2-weighted image the signal is generally isointense to fat (Fig. 9.17a, b).
9.4.8 Optic Nerve Glioma
Optic nerve gliomas are uncommon neoplasms of astro-cytic glia located along the visual pathways. Th ey repre-sent 2–4% of all orbital tumors and 66% of primary optic nerve tumors. Gliomas are seen most commonly in
children, with a mean age of 9 years at presentation. About 29% of optic gliomas are seen in the setting of neu-rofi bromatosis. On noncontrast CT, the orbital glioma appears as a well-outlined enlargement of the optic nerve that is usually fusiform but may be more rounded or even mulitilobulated. Increased tortuosity or kinking of the nerve is a common fi nding. Following contrast adminis-tration, enhancement is heterogeneous and variable from imperceptible to moderate. On the T1 MRI, gliomas are isointense or slightly hypointense with respect to cortical gray mater. A dilated subarachnoid space fi lled with cere-bral spinal fl uid (CSF) may image as a hypointense zone surrounding the tumor. Low-signal hypointense areas within the lesion represent cysts of mucinous degenera-tion and necrosis. On T2-WI, the signal may be more variable (Fig. 9.18a, b).
a b
Fig. 9.17 (a) CT and (b) T1 fat saturation contrasted MRI showing the characteristic imaging fi ndings of myositis
a b
Fig. 9.18 (a) CT and (b) T1 MRI showing the characteristic imaging fi ndings of optic nerve glioma
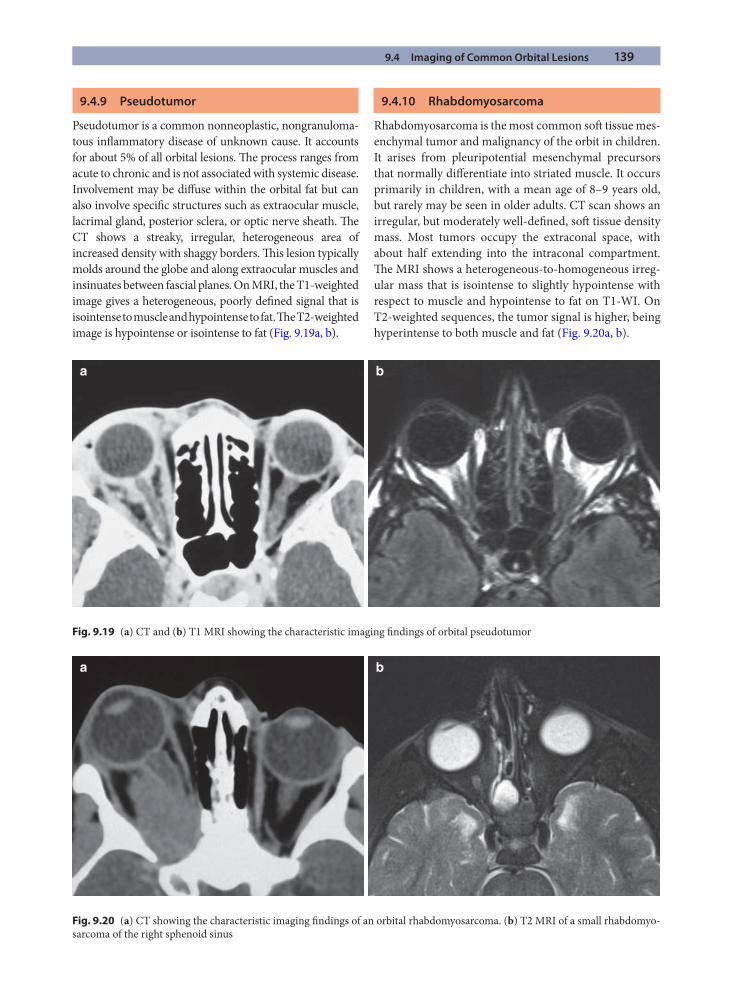
9.4 Imaging of Common Orbital Lesions 139
9.4.9 Pseudotumor
Pseudotumor is a common nonneoplastic, nongranuloma-tous infl ammatory disease of unknown cause. It accounts for about 5% of all orbital lesions. Th e process ranges from acute to chronic and is not associated with systemic disease. Involvement may be diff use within the orbital fat but can also involve specifi c structures such as extraocular muscle, lacrimal gland, posterior sclera, or optic nerve sheath. Th e CT shows a streaky, irregular, heterogeneous area of increased density with shaggy borders. Th is lesion typically molds around the globe and along extraocular muscles and insinuates between fascial planes. On MRI, the T1-weighted image gives a heterogeneous, poorly defi ned signal that is isointense to muscle and hypointense to fat. Th e T2-weighted image is hypointense or isointense to fat (Fig. 9.19a, b).
9.4.10 Rhabdomyosarcoma
Rhabdomyosarcoma is the most common soft tissue mes-enchymal tumor and malignancy of the orbit in children. It arises from pleuripotential mesenchymal precursors that normally diff erentiate into striated muscle. It occurs primarily in children, with a mean age of 8–9 years old, but rarely may be seen in older adults. CT scan shows an irregular, but moderately well-defi ned, soft tissue density mass. Most tumors occupy the extraconal space, with about half extending into the intraconal compartment. Th e MRI shows a heterogeneous-to-homogeneous irreg-ular mass that is isointense to slightly hypointense with respect to muscle and hypointense to fat on T1-WI. On T2-weighted sequences, the tumor signal is higher, being hyperintense to both muscle and fat (Fig. 9.20a, b).
a b
Fig. 9.19 (a) CT and (b) T1 MRI showing the characteristic imaging fi ndings of orbital pseudotumor
a b
Fig. 9.20 (a) CT showing the characteristic imaging fi ndings of an orbital rhabdomyosarcoma. (b) T2 MRI of a small rhabdomyo-sarcoma of the right sphenoid sinus
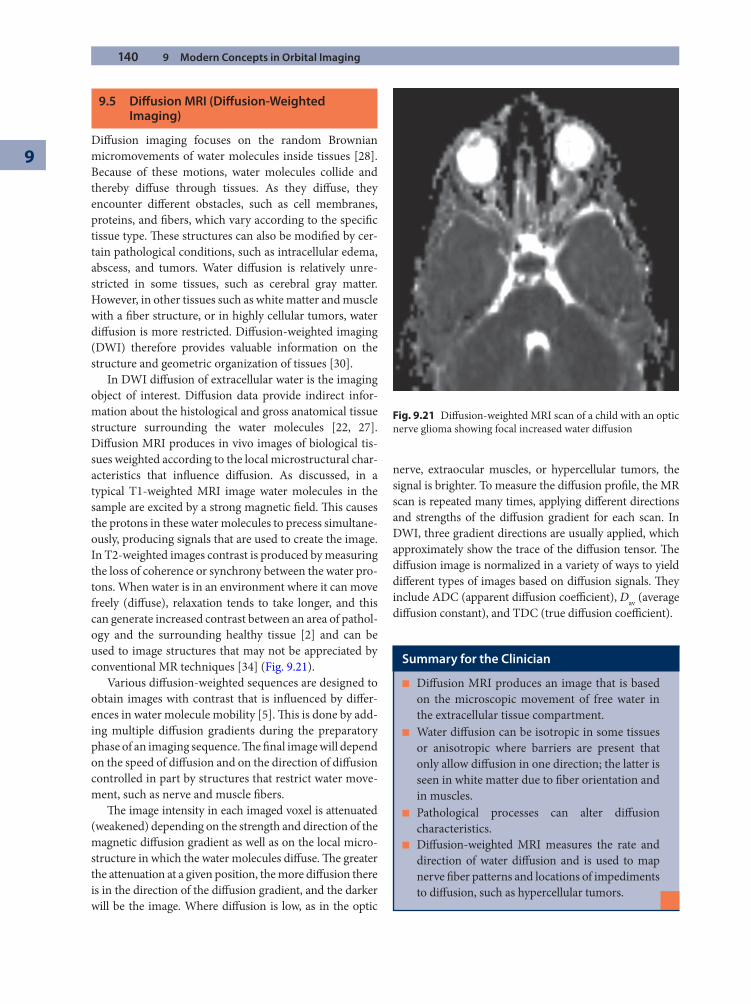
140 9 Modern Concepts in Orbital Imaging
9
9.5 Diff usion MRI (Diff usion-Weighted Imaging)
Diff usion imaging focuses on the random Brownian micromovements of water molecules inside tissues [28]. Because of these motions, water molecules collide and thereby diff use through tissues. As they diff use, they encounter diff erent obstacles, such as cell membranes, proteins, and fi bers, which vary according to the specifi c tissue type. Th ese structures can also be modifi ed by cer-tain pathological conditions, such as intracellular edema, abscess, and tumors. Water diff usion is relatively unre-stricted in some tissues, such as cerebral gray matter. However, in other tissues such as white matter and muscle with a fi ber structure, or in highly cellular tumors, water diff usion is more restricted. Diff usion-weighted imaging (DWI) therefore provides valuable information on the structure and geometric organization of tissues [30].
In DWI diff usion of extracellular water is the imaging object of interest. Diff usion data provide indirect infor-mation about the histological and gross anatomical tissue structure surrounding the water molecules [22, 27]. Diff usion MRI produces in vivo images of biological tis-sues weighted according to the local microstructural char-acteristics that infl uence diff usion. As discussed, in a typical T1-weighted MRI image water molecules in the sample are excited by a strong magnetic fi eld. Th is causes the protons in these water molecules to precess simultane-ously, producing signals that are used to create the image. In T2-weighted images contrast is produced by measuring the loss of coherence or synchrony between the water pro-tons. When water is in an environment where it can move freely (diff use), relaxation tends to take longer, and this can generate increased contrast between an area of pathol-ogy and the surrounding healthy tissue [2] and can be used to image structures that may not be appreciated by conventional MR techniques [34] (Fig. 9.21).
Various diff usion-weighted sequences are designed to obtain images with contrast that is infl uenced by diff er-ences in water molecule mobility [5]. Th is is done by add-ing multiple diff usion gradients during the preparatory phase of an imaging sequence. Th e fi nal image will depend on the speed of diff usion and on the direction of diff usion controlled in part by structures that restrict water move-ment, such as nerve and muscle fi bers.
Th e image intensity in each imaged voxel is attenuated (weakened) depending on the strength and direction of the magnetic diff usion gradient as well as on the local micro-structure in which the water molecules diff use. Th e greater the attenuation at a given position, the more diff usion there is in the direction of the diff usion gradient, and the darker will be the image. Where diff usion is low, as in the optic
nerve, extraocular muscles, or hypercellular tumors, the signal is brighter. To measure the diff usion profi le, the MR scan is repeated many times, applying diff erent directions and strengths of the diff usion gradient for each scan. In DWI, three gradient directions are usually applied, which approximately show the trace of the diff usion tensor. Th e diff usion image is normalized in a variety of ways to yield diff erent types of images based on diff usion signals. Th ey include ADC (apparent diff usion coeffi cient), Dav (average diff usion constant), and TDC (true diff usion coeffi cient).
Fig. 9.21 Diff usion-weighted MRI scan of a child with an optic nerve glioma showing focal increased water diff usion
Summary for the Clinician
Diff usion MRI produces an image that is based ■
on the microscopic movement of free water in the extracellular tissue compartment.Water diff usion can be isotropic in some tissues ■
or anisotropic where barriers are present that only allow diff usion in one direction; the latter is seen in white matter due to fi ber orientation and in muscles.Pathological processes can alter diff usion ■
characteristics.Diff usion-weighted MRI measures the rate and ■
direction of water diff usion and is used to map nerve fi ber patterns and locations of impediments to diff usion, such as hypercellular tumors.
9.6 Positron Emission Tomography 141
Diff usion tensor imaging enables the in vivo evalua-tion of tissue microstructure. It provides data that can help in the diagnosis of microscopic features, such as nerve fi ber anomalies in white matter, which may not be visible with standard imaging techniques [38]. DWI has become useful for the detection of tumors, infections, infl ammations, trauma, and degenerative diseases. It can distinguish a solid tumor from areas of cystic degenera-tion and necrosis and between benign and malignant neoplasms because of its ability to distinguish hypercel-lular from paucicellular tumors.
9.6 Positron Emission Tomography
Positron emission tomography is an imaging technique that has become useful in medicine. Unlike the CT, which images the transparency of tissues to the passage of X-rays, PET scanning measures the emission of positrons (photons) from a radiotracer that is injected intrave-nously [1]. Th e technique makes use of the concept of positron annihilation.
In a PET scan, the patient is injected with the radioac-tive substance and placed on a table that moves through a circular shaped housing. Th is housing contains the gamma ray detector array, which has a series of scintilla-tion crystals. Each detector is connected to a photomulti-plier tube that converts the gamma rays emitted from the patient to photons of light. Th e photomultiplier tubes convert and amplify the photons to electrical signals. Th ese signals are then processed by a computer to gener-ate a clinical image. As the table and patient incremen-
tally move forward, the process is repeated, giving a series of thin-slice images of the body. Th ese images are then assembled into a 3D representation [32, 37, 40]. Th e com-bined use of PET and CT is proving to be even more valu-able by demonstrating metabolic activity along with anatomical detail and localization [36].
Th e most commonly used positron-emitting nuclides are carbon-11 and fl uorine-18. Th ese replace the normal atoms in tissue compounds, and the labeled compounds are taken up by certain tissues. Th us, fl uorine-18 replaces fl uorine-19 in fl uorinated glucose to produce [2-18F]fl uoro-2-deoxy-D-glucose (FDG). Th e radioactive atom decays by positron emission. When a positron is emitted by a nucleus, it immediately collides with an electron, and the pair annihilates, converting all the mass energy of the two particles into two gamma rays. Th e two gamma ray pho-tons possess momentum, and the conservation of momentum requires that they travel in opposite direc-tions. Th e simultaneous detection of these gamma ray photons in two detectors situated 180° apart in the scan-ner allows location of the source on a line directly between those two detectors.
FDG PET scanning exploits the increased glycolytic activity associated with neoplastic diseases and has proven to be superior to other imaging modalities for some tumors, such as head and neck squamous cell carcinoma and lymphoma [24, 26, 41, 42]. PET scan imaging is of particular value for imaging of the brain (Fig. 9.22a, b). Th e fl uorine isotope 18F-labeled glucose can pass through the blood–brain barrier, where the concentration of the tracer is a measure of the level of metabolic activity at that location in the brain. In the brain and elsewhere in the
a b
Fig. 9.22 (a, b) Coronal and axial PET scans showing normal metabolic activity of the brain
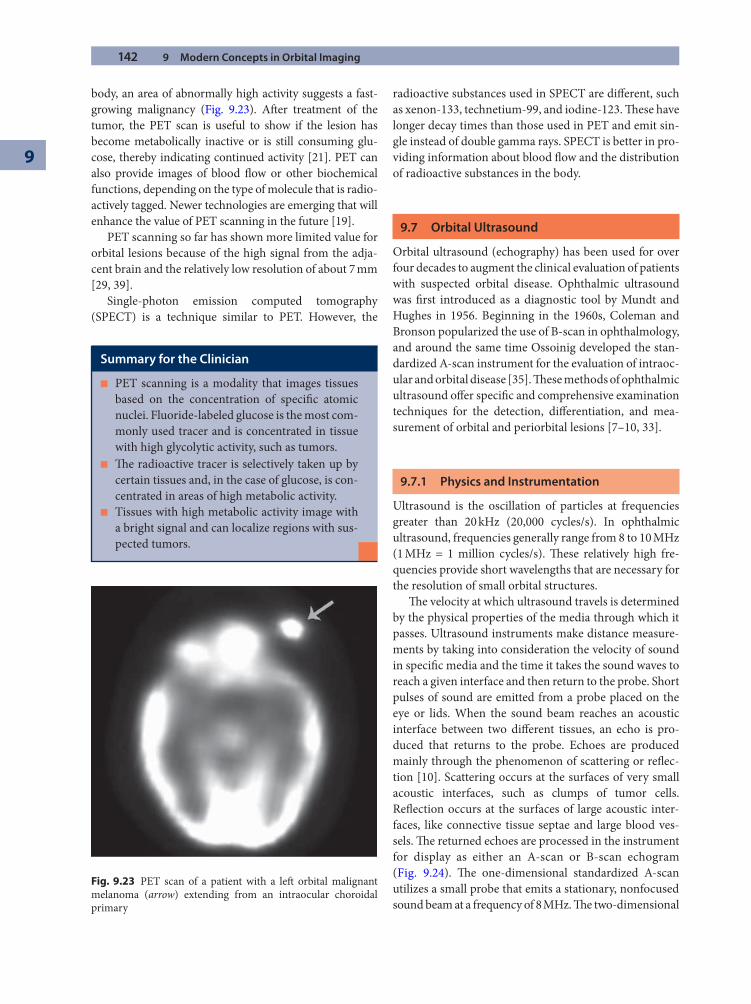
142 9 Modern Concepts in Orbital Imaging
9
body, an area of abnormally high activity suggests a fast-growing malignancy (Fig. 9.23). Aft er treatment of the tumor, the PET scan is useful to show if the lesion has become metabolically inactive or is still consuming glu-cose, thereby indicating continued activity [21]. PET can also provide images of blood fl ow or other biochemical functions, depending on the type of molecule that is radio-actively tagged. Newer technologies are emerging that will enhance the value of PET scanning in the future [19].
PET scanning so far has shown more limited value for orbital lesions because of the high signal from the adja-cent brain and the relatively low resolution of about 7 mm [29, 39].
Single-photon emission computed tomography (SPECT) is a technique similar to PET. However, the
radioactive substances used in SPECT are diff erent, such as xenon-133, technetium-99, and iodine-123. Th ese have longer decay times than those used in PET and emit sin-gle instead of double gamma rays. SPECT is better in pro-viding information about blood fl ow and the distribution of radioactive substances in the body.
9.7 Orbital Ultrasound
Orbital ultrasound (echography) has been used for over four decades to augment the clinical evaluation of patients with suspected orbital disease. Ophthalmic ultrasound was fi rst introduced as a diagnostic tool by Mundt and Hughes in 1956. Beginning in the 1960s, Coleman and Bronson popularized the use of B-scan in ophthalmology, and around the same time Ossoinig developed the stan-dardized A-scan instrument for the evaluation of intraoc-ular and orbital disease [35]. Th ese methods of ophthalmic ultrasound off er specifi c and comprehensive examination techniques for the detection, diff erentiation, and mea-surement of orbital and periorbital lesions [7–10, 33].
9.7.1 Physics and Instrumentation
Ultrasound is the oscillation of particles at frequencies greater than 20 kHz (20,000 cycles/s). In ophthalmic ultrasound, frequencies generally range from 8 to 10 MHz (1 MHz = 1 million cycles/s). Th ese relatively high fre-quencies provide short wavelengths that are necessary for the resolution of small orbital structures.
Th e velocity at which ultrasound travels is determined by the physical properties of the media through which it passes. Ultrasound instruments make distance measure-ments by taking into consideration the velocity of sound in specifi c media and the time it takes the sound waves to reach a given interface and then return to the probe. Short pulses of sound are emitted from a probe placed on the eye or lids. When the sound beam reaches an acoustic interface between two diff erent tissues, an echo is pro-duced that returns to the probe. Echoes are produced mainly through the phenomenon of scattering or refl ec-tion [10]. Scattering occurs at the surfaces of very small acoustic interfaces, such as clumps of tumor cells. Refl ection occurs at the surfaces of large acoustic inter-faces, like connective tissue septae and large blood ves-sels. Th e returned echoes are processed in the instrument for display as either an A-scan or B-scan echogram (Fig. 9.24). Th e one-dimensional standardized A-scan utilizes a small probe that emits a stationary, nonfocused sound beam at a frequency of 8 MHz. Th e two-dimensional
Summary for the Clinician
PET scanning is a modality that images tissues ■
based on the concentration of specifi c atomic nuclei. Fluoride-labeled glucose is the most com-monly used tracer and is concentrated in tissue with high glycolytic activity, such as tumors.Th e radioactive tracer is selectively taken up by ■
certain tissues and, in the case of glucose, is con-centrated in areas of high metabolic activity.Tissues with high metabolic activity image with ■
a bright signal and can localize regions with sus-pected tumors.
Fig. 9.23 PET scan of a patient with a left orbital malignant melanoma (arrow) extending from an intraocular choroidal primary
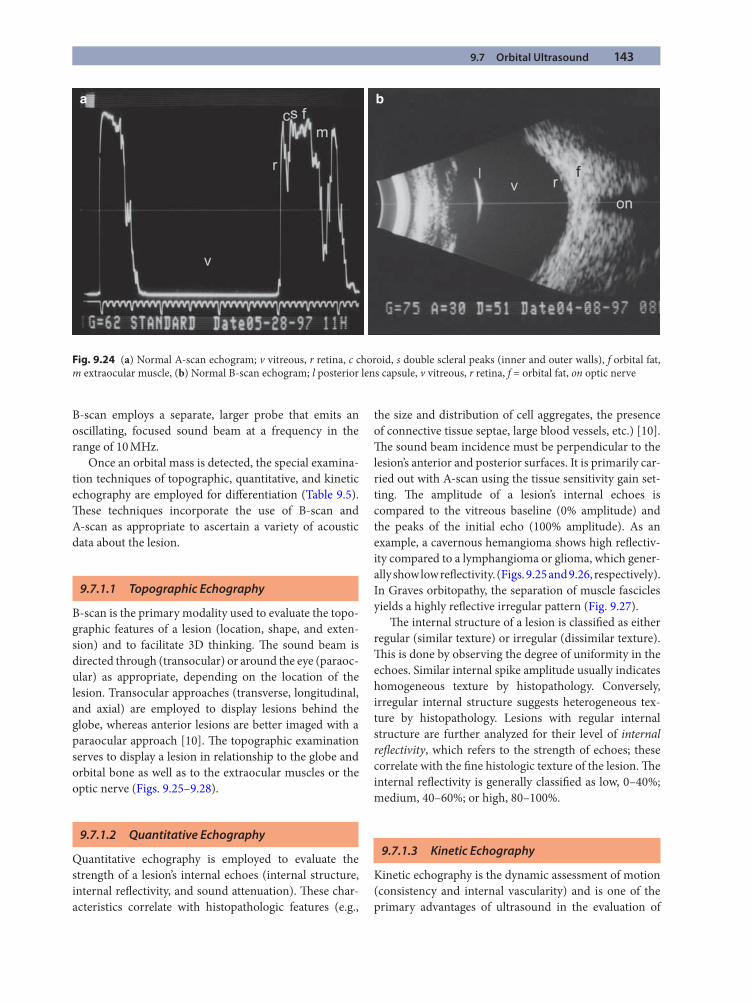
9.7 Orbital Ultrasound 143
B-scan employs a separate, larger probe that emits an oscillating, focused sound beam at a frequency in the range of 10 MHz.
Once an orbital mass is detected, the special examina-tion techniques of topographic, quantitative, and kinetic echography are employed for diff erentiation (Table 9.5). Th ese techniques incorporate the use of B-scan and A-scan as appropriate to ascertain a variety of acoustic data about the lesion.
9.7.1.1 Topographic Echography
B-scan is the primary modality used to evaluate the topo-graphic features of a lesion (location, shape, and exten-sion) and to facilitate 3D thinking. Th e sound beam is directed through (transocular) or around the eye (paraoc-ular) as appropriate, depending on the location of the lesion. Transocular approaches (transverse, longitudinal, and axial) are employed to display lesions behind the globe, whereas anterior lesions are better imaged with a paraocular approach [10]. Th e topographic examination serves to display a lesion in relationship to the globe and orbital bone as well as to the extraocular muscles or the optic nerve (Figs. 9.25–9.28).
9.7.1.2 Quantitative Echography
Quantitative echography is employed to evaluate the strength of a lesion’s internal echoes (internal structure, internal refl ectivity, and sound attenuation). Th ese char-acteristics correlate with histopathologic features (e.g.,
the size and distribution of cell aggregates, the presence of connective tissue septae, large blood vessels, etc.) [10]. Th e sound beam incidence must be perpendicular to the lesion’s anterior and posterior surfaces. It is primarily car-ried out with A-scan using the tissue sensitivity gain set-ting. Th e amplitude of a lesion’s internal echoes is compared to the vitreous baseline (0% amplitude) and the peaks of the initial echo (100% amplitude). As an example, a cavernous hemangioma shows high refl ectiv-ity compared to a lymphangioma or glioma, which gener-ally show low refl ectivity. (Figs. 9.25 and 9.26, respectively). In Graves orbitopathy, the separation of muscle fascicles yields a highly refl ective irregular pattern (Fig. 9.27).
Th e internal structure of a lesion is classifi ed as either regular (similar texture) or irregular (dissimilar texture). Th is is done by observing the degree of uniformity in the echoes. Similar internal spike amplitude usually indicates homogeneous texture by histopathology. Conversely, irregular internal structure suggests heterogeneous tex-ture by histopathology. Lesions with regular internal structure are further analyzed for their level of internal refl ectivity, which refers to the strength of echoes; these correlate with the fi ne histologic texture of the lesion. Th e internal refl ectivity is generally classifi ed as low, 0–40%; medium, 40–60%; or high, 80–100%.
9.7.1.3 Kinetic Echography
Kinetic echography is the dynamic assessment of motion (consistency and internal vascularity) and is one of the primary advantages of ultrasound in the evaluation of
a b
Fig. 9.24 (a) Normal A-scan echogram; v vitreous, r retina, c choroid, s double scleral peaks (inner and outer walls), f orbital fat, m extraocular muscle, (b) Normal B-scan echogram; l posterior lens capsule, v vitreous, r retina, f = orbital fat, on optic nerve
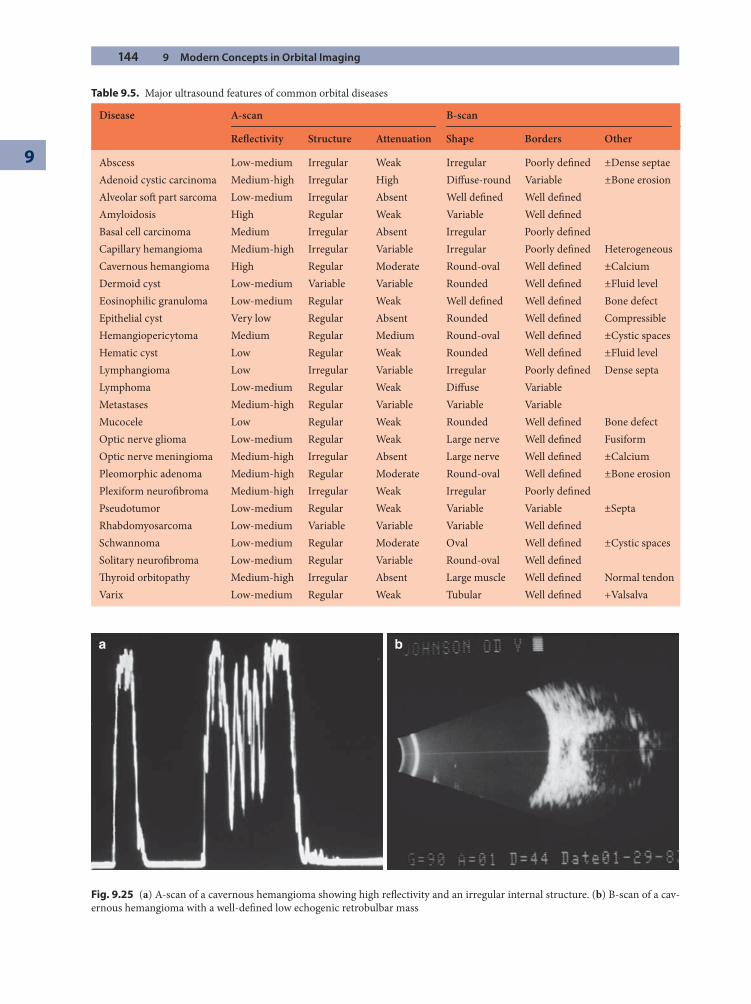
144 9 Modern Concepts in Orbital Imaging
9
a b
Fig. 9.25 (a) A-scan of a cavernous hemangioma showing high refl ectivity and an irregular internal structure. (b) B-scan of a cav-ernous hemangioma with a well-defi ned low echogenic retrobulbar mass
Table 9.5. Major ultrasound features of common orbital diseases
Disease A-scan B-scan
Refl ectivity Structure Attenuation Shape Borders Other
Abscess Low-medium Irregular Weak Irregular Poorly defi ned ±Dense septaeAdenoid cystic carcinoma Medium-high Irregular High Diff use-round Variable ±Bone erosionAlveolar soft part sarcoma Low-medium Irregular Absent Well defi ned Well defi nedAmyloidosis High Regular Weak Variable Well defi nedBasal cell carcinoma Medium Irregular Absent Irregular Poorly defi nedCapillary hemangioma Medium-high Irregular Variable Irregular Poorly defi ned HeterogeneousCavernous hemangioma High Regular Moderate Round-oval Well defi ned ±CalciumDermoid cyst Low-medium Variable Variable Rounded Well defi ned ±Fluid levelEosinophilic granuloma Low-medium Regular Weak Well defi ned Well defi ned Bone defectEpithelial cyst Very low Regular Absent Rounded Well defi ned CompressibleHemangiopericytoma Medium Regular Medium Round-oval Well defi ned ±Cystic spacesHematic cyst Low Regular Weak Rounded Well defi ned ±Fluid levelLymphangioma Low Irregular Variable Irregular Poorly defi ned Dense septaLymphoma Low-medium Regular Weak Diff use VariableMetastases Medium-high Regular Variable Variable VariableMucocele Low Regular Weak Rounded Well defi ned Bone defectOptic nerve glioma Low-medium Regular Weak Large nerve Well defi ned FusiformOptic nerve meningioma Medium-high Irregular Absent Large nerve Well defi ned ±CalciumPleomorphic adenoma Medium-high Regular Moderate Round-oval Well defi ned ±Bone erosionPlexiform neurofi broma Medium-high Irregular Weak Irregular Poorly defi nedPseudotumor Low-medium Regular Weak Variable Variable ±SeptaRhabdomyosarcoma Low-medium Variable Variable Variable Well defi nedSchwannoma Low-medium Regular Moderate Oval Well defi ned ±Cystic spacesSolitary neurofi broma Low-medium Regular Variable Round-oval Well defi nedTh yroid orbitopathy Medium-high Irregular Absent Large muscle Well defi ned Normal tendonVarix Low-medium Regular Weak Tubular Well defi ned +Valsalva
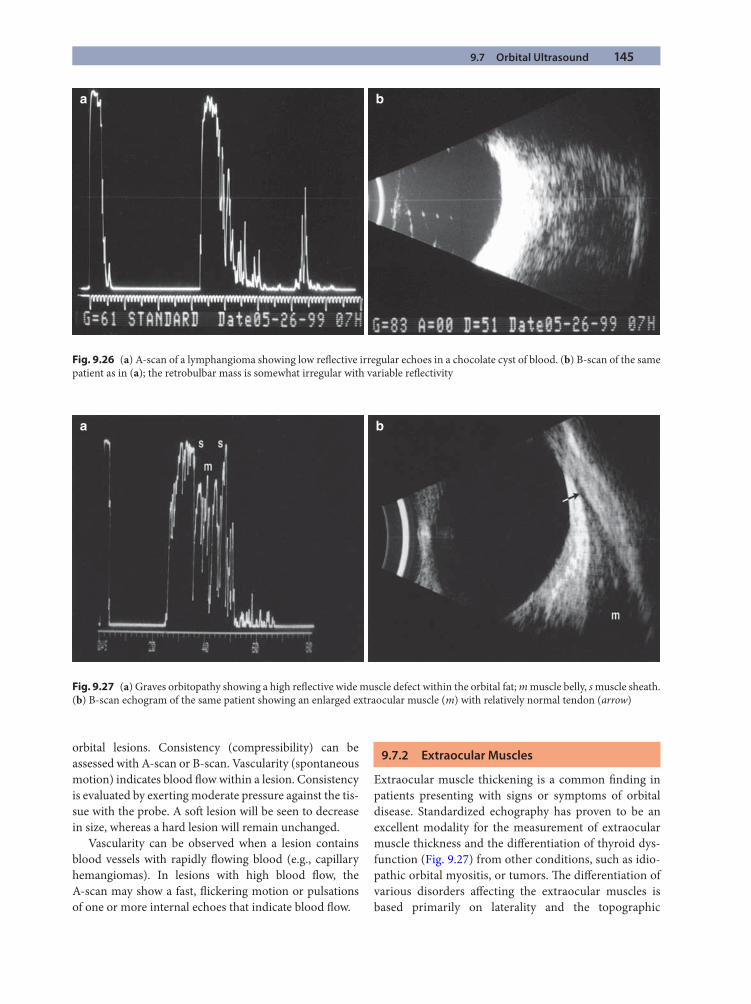
9.7 Orbital Ultrasound 145
a b
Fig. 9.26 (a) A-scan of a lymphangioma showing low refl ective irregular echoes in a chocolate cyst of blood. (b) B-scan of the same patient as in (a); the retrobulbar mass is somewhat irregular with variable refl ectivity
a b
Fig. 9.27 (a) Graves orbitopathy showing a high refl ective wide muscle defect within the orbital fat; m muscle belly, s muscle sheath. (b) B-scan echogram of the same patient showing an enlarged extraocular muscle (m) with relatively normal tendon (arrow)
orbital lesions. Consistency (compressibility) can be assessed with A-scan or B-scan. Vascularity (spontaneous motion) indicates blood fl ow within a lesion. Consistency is evaluated by exerting moderate pressure against the tis-sue with the probe. A soft lesion will be seen to decrease in size, whereas a hard lesion will remain unchanged.
Vascularity can be observed when a lesion contains blood vessels with rapidly fl owing blood (e.g., capillary hemangiomas). In lesions with high blood fl ow, the A-scan may show a fast, fl ickering motion or pulsations of one or more internal echoes that indicate blood fl ow.
9.7.2 Extraocular Muscles
Extraocular muscle thickening is a common fi nding in patients presenting with signs or symptoms of orbital disease. Standardized echography has proven to be an excellent modality for the measurement of extraocular muscle thickness and the diff erentiation of thyroid dys-function (Fig. 9.27) from other conditions, such as idio-pathic orbital myositis, or tumors. Th e diff erentiation of various disorders aff ecting the extraocular muscles is based primarily on laterality and the topographic
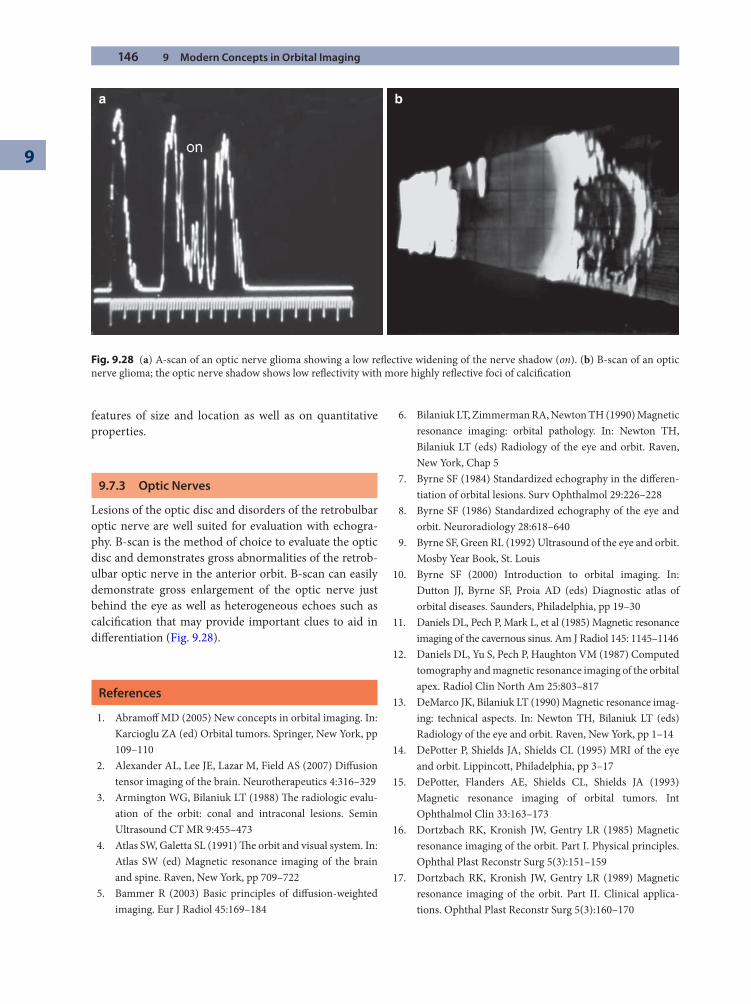
146 9 Modern Concepts in Orbital Imaging
9
features of size and location as well as on quantitative properties.
9.7.3 Optic Nerves
Lesions of the optic disc and disorders of the retrobulbar optic nerve are well suited for evaluation with echogra-phy. B-scan is the method of choice to evaluate the optic disc and demonstrates gross abnormalities of the retrob-ulbar optic nerve in the anterior orbit. B-scan can easily demonstrate gross enlargement of the optic nerve just behind the eye as well as heterogeneous echoes such as calcifi cation that may provide important clues to aid in diff erentiation (Fig. 9.28).
References
1. Abramoff MD (2005) New concepts in orbital imaging. In: Karcioglu ZA (ed) Orbital tumors. Springer, New York, pp 109–110
2. Alexander AL, Lee JE, Lazar M, Field AS (2007) Diff usion tensor imaging of the brain. Neurotherapeutics 4:316–329
3. Armington WG, Bilaniuk LT (1988) Th e radiologic evalu-ation of the orbit: conal and intraconal lesions. Semin Ultrasound CT MR 9:455–473
4. Atlas SW, Galetta SL (1991) Th e orbit and visual system. In: Atlas SW (ed) Magnetic resonance imaging of the brain and spine. Raven, New York, pp 709–722
5. Bammer R (2003) Basic principles of diff usion-weighted imaging. Eur J Radiol 45:169–184
6. Bilaniuk LT, Zimmerman RA, Newton TH (1990) Magnetic resonance imaging: orbital pathology. In: Newton TH, Bilaniuk LT (eds) Radiology of the eye and orbit. Raven, New York, Chap 5
7. Byrne SF (1984) Standardized echography in the diff eren-tiation of orbital lesions. Surv Ophthalmol 29:226–228
8. Byrne SF (1986) Standardized echography of the eye and orbit. Neuroradiology 28:618–640
9. Byrne SF, Green RL (1992) Ultrasound of the eye and orbit. Mosby Year Book, St. Louis
10. Byrne SF (2000) Introduction to orbital imaging. In: Dutton JJ, Byrne SF, Proia AD (eds) Diagnostic atlas of orbital diseases. Saunders, Philadelphia, pp 19–30
11. Daniels DL, Pech P, Mark L, et al (1985) Magnetic resonance imaging of the cavernous sinus. Am J Radiol 145: 1145–1146
12. Daniels DL, Yu S, Pech P, Haughton VM (1987) Computed tomography and magnetic resonance imaging of the orbital apex. Radiol Clin North Am 25:803–817
13. DeMarco JK, Bilaniuk LT (1990) Magnetic resonance imag-ing: technical aspects. In: Newton TH, Bilaniuk LT (eds) Radiology of the eye and orbit. Raven, New York, pp 1–14
14. DePotter P, Shields JA, Shields CL (1995) MRI of the eye and orbit. Lippincott, Philadelphia, pp 3–17
15. DePotter, Flanders AE, Shields CL, Shields JA (1993) Magnetic resonance imaging of orbital tumors. Int Ophthalmol Clin 33:163–173
16. Dortzbach RK, Kronish JW, Gentry LR (1985) Magnetic resonance imaging of the orbit. Part I. Physical principles. Ophthal Plast Reconstr Surg 5(3):151–159
17. Dortzbach RK, Kronish JW, Gentry LR (1989) Magnetic resonance imaging of the orbit. Part II. Clinical applica-tions. Ophthal Plast Reconstr Surg 5(3):160–170
a b
Fig. 9.28 (a) A-scan of an optic nerve glioma showing a low refl ective widening of the nerve shadow (on). (b) B-scan of an optic nerve glioma; the optic nerve shadow shows low refl ectivity with more highly refl ective foci of calcifi cation
References 147
18. Dutton JJ (2000) Introduction to orbital imaging. In: Dutton JJ, Byrne SF, Proia AD (eds) Diagnostic atlas of orbital diseases. Saunders, Philadelphia, pp 31–41
19. Frangiomi JV (2008) New technologies for human cancer imaging. J Clin Oncol 26:4012–4021
20. Garvey CJ (2002) Computed tomography in clinical prac-tice. BMJ 324:1077–1080
21. Gayed I, Eskandari MF, McLaughlin P, et al (2007) Value of positron emission tomography in staging ocular adnexal lymphomas and evaluating their response to therapy. Ophthal Surg Lasers Imaging 38:319–325
22. Habes C (2004) Basic principles of diff usion tensor MR technology. J Radiol 85:281–286
23. Hu H, He HD, Foley WD, Fox SH (2000) Row helical CT: image quality and volume coverage speed. Radiology 215: 55–62
24. Jabour BA, Choi Y, Hoh CK, et al (1993) Extracranial head and neck PET imaging with 2-[F-18]fl uoro-2-deoxy-D-glucose and MR imaging correlation. Radiology 186: 27–35
25. Jones R, Kaplan RT, Lane B, et al (2001) Single versus multi-detector row CT of the brain: quality assessment. Radiology 219:750–755
26. King AD, MA BB, Yau YY, et al (2008) Th e impact of 18-F-FDG PET/CT on assessment of nasopharyngeal carcinoma at diagnosis. Br J Radiol 81:291–298
27. Koh DM, Collins DJ (2007) Diff usion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol 188:1622–1635
28. Koyama T, Tamai K, Togashi K (2006) Current status of body MRI imaging: fast MR imaging and diff usion-weighted imaging. Int J Clin Oncol 11:278–285
29. Lane KA, Bilyk JR (2006) Preliminary study of positron emis-sion tomography in the detection and management of orbital malignancy. Ophthal Plast Reconstr Surg 22: 361–365
30. Le Bihan D (2006) From Brownian motion to mind imag-ing: diff usion MRI. Bull Acad Natl Med 190:605–627
31. Mafee MF, Putterman A, Valvassori GE, et al (1987) Orbital space-occupying lesions: role of computed tomography and magnetic resonance imaging. Radiol Clin North Am 25:529–559
32. Mandelkern M, Raines J (2002) Positron emission tomog-raphy in cancer research and treatment. Technol Cancer Res Treat 1:423–439
33. Mundt GH, Hughes WF (1956) Ultrasonics in ocular diag-nosis. Am J Ophthalmol 41:488–492
34. Nagae-Poetscher LM, Jiang H, Wakana S, et al (2004) High-resolution diff usion imaging of the brain stem at 3 T. AJNR Am J Neuroradiol 25:1325–1330
35. Ossoinig KC (1991) Echographic diff erentiation of vascular lesions in the orbit. In: Th ijssen JM, Verbeek AM (eds) Ultrasonography in ophthalmology. Junk, Dordrecht, p 283
36. Pan T, Mawlawi O (2008) PET/CT in radiation oncology. Med Phys 35:4955–4966
37. Reader AJ (2008) Th e promise of new PET image recon-struction. Phys Med 24:49–56
38. Rovaris M, Gass A, Bammer R, et al (2005) Diff usion MRI in multiple sclerosis. Neurology 65:1526–1532
39. Spraul CW, Lang GE, Lang GK (2001) Value of positron emission tomography in the diagnosis of malignant ocular tumors. Ophthalmologica 215:163–168
40. Townsend DW (2004) Physical principles and technology of clinical PET imaging. Ann Acad Med Singapore 33: 133–145
41. Valenzuela AA, Allen C, Grimes D, et al (2006) Positron emission tomography in the detection and staging of ocu-lar adnexal lymphoproliferative disease. Ophthalmology 113:2331–2337
42. Wirth A, Seymour JF, Hicks RJ, et al (2002) Fluorine-18 fl uorodeoxyglucose positron emission tomography, gal-lium-67 scintigraphy, and conventional staging for Hodgkin’s disease and non-Hodgkin’s lymphoma. Am J Med 112:262–268

10.1 Introduction
Infection in the periorbital area is an acute problem that must be astutely recognized and treated. Even though these infections have been around for centuries, the spec-trum of bacteria involved continues to evolve with the ever-changing landscape of antibiotics and vaccines. Th ese bacterial infections can be superfi cial in the prese-ptal tissue, involve the orbital space, or encompass both. Th ey are a common cause for ophthalmic emergency vis-its and need to be treated promptly. When the orbit is infected, severe sequelae can result, including death, and thus must be managed aggressively. Th e goal of this chap-ter is to review the mechanisms and organisms responsi-ble for cellulitis given that the spectrum of bacteria causing cellulitis is constantly in fl ux. Current treatment regimens based on current bacteria and antibiotic sensi-tivity are addressed along with the increasing incidence of MRSA and other antibiotic resistance.
10.2 The Infection: Stages, Symptoms, and Eff ects
Most cellulitis involves the preseptal eyelid tissue. Orbital cellulitis represents an acute infection with infl ammation
of orbital contents, oft en including the pre- and postsep-tal eyelids [2, 6, 20, 44]. Periorbital cellulitis can be classi-fi ed into fi ve stages. Th e fi rst stage is preseptal cellulitis, in which infl ammatory edema remains anterior to the orbital septum. Th e second stage is posterior spread of this infl ammation, behind the arcus marginalis, to a true orbital cellulitis (infl ammation of the orbital contents without abscess formation). Th ird, subperiosteal abscesses may form, in which pus collects between the orbit and the periosteum of the involved sinus. Th e fourth stage is an orbital abscess, and the fi ft h involves cavernous sinus thrombosis [6, 24]. Th e course of treatment varies based on several factors, including the stage of the infection, the source of the infection, the health of the patient, and the underlying organism involved.
By and large, symptomatology and presentation of cel-lulitis vary with stage of disease. Th erefore, a patient with a swollen eyelid can present a challenge but may be read-ily diagnosed by careful clinical history, examination, and potentially necessary imaging modalities. Stage 1 disease, or preseptal cellulitis, typically presents as tender ery-thema of the upper or lower eyelids, with no orbital involvement (Fig. 10.1). Since this infl ammation is not restricted by the arcus marginalis, it may spread around the eye to involve both the upper and lower lids as well as the cheek and forehead. Th e history oft en includes a
Management of Periorbital Cellulitis in the 21st CenturyMichael P. Rabinowitz and Scott M. Goldstein
Chapter 10
10
Core Messages
Periorbital cellulitis can be a serious infection and ■
must be promptly recognized and treated.Due to vaccines and antibiotic use in the twenti- ■
eth century, the microbiologic spectrum of bacte-ria causing infections in the periorbital area in the twenty-fi rst century is diff erent from 10–15 years ago.Methicillin-resistant ■ Staphylococcal aureus (MRSA) infections are now a common entity and are aggres-sive.
Clinical examination and computed tomographic ■
(CT) scans are the two important aspects of prop-erly evaluating patients with infections.A combination of medical antibiotic therapy and ■
surgical intervention is oft en needed to appropri-ately treat these infections, especially in teenagers and adults.
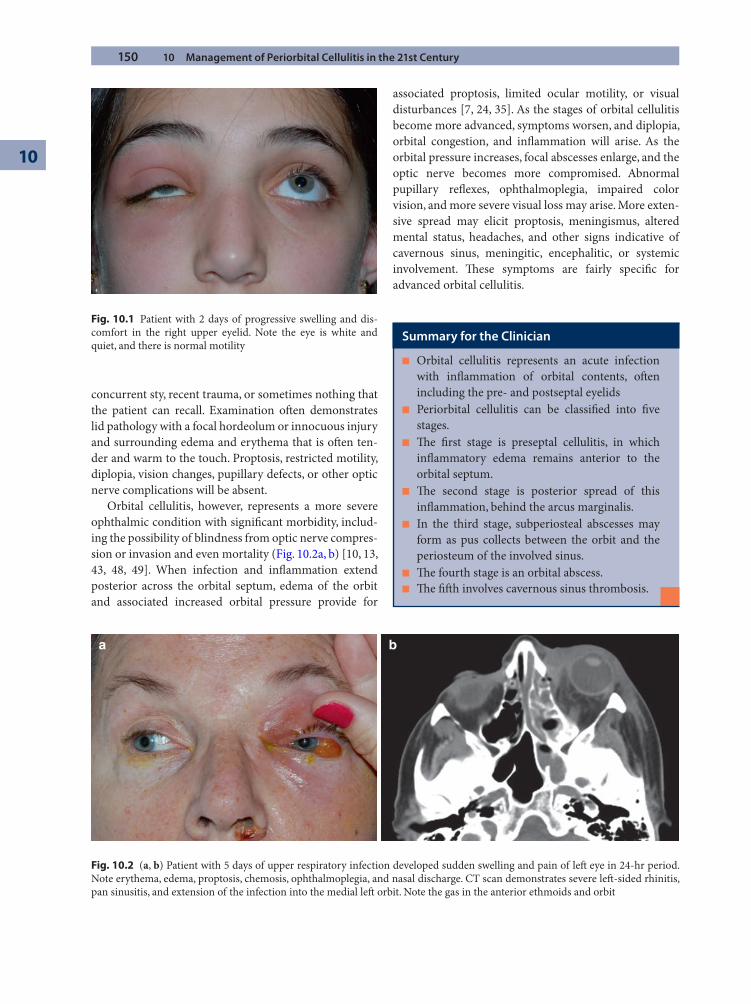
150 10 Management of Periorbital Cellulitis in the 21st Century
10
concurrent sty, recent trauma, or sometimes nothing that the patient can recall. Examination oft en demonstrates lid pathology with a focal hordeolum or innocuous injury and surrounding edema and erythema that is oft en ten-der and warm to the touch. Proptosis, restricted motility, diplopia, vision changes, pupillary defects, or other optic nerve complications will be absent.
Orbital cellulitis, however, represents a more severe ophthalmic condition with signifi cant morbidity, includ-ing the possibility of blindness from optic nerve compres-sion or invasion and even mortality (Fig. 10.2a, b) [10, 13, 43, 48, 49]. When infection and infl ammation extend posterior across the orbital septum, edema of the orbit and associated increased orbital pressure provide for
associated proptosis, limited ocular motility, or visual disturbances [7, 24, 35]. As the stages of orbital cellulitis become more advanced, symptoms worsen, and diplopia, orbital congestion, and infl ammation will arise. As the orbital pressure increases, focal abscesses enlarge, and the optic nerve becomes more compromised. Abnormal pupillary refl exes, ophthalmoplegia, impaired color vision, and more severe visual loss may arise. More exten-sive spread may elicit proptosis, meningismus, altered mental status, headaches, and other signs indicative of cavernous sinus, meningitic, encephalitic, or systemic involvement. Th ese symptoms are fairly specifi c for advanced orbital cellulitis.
Fig. 10.1 Patient with 2 days of progressive swelling and dis-comfort in the right upper eyelid. Note the eye is white and quiet, and there is normal motility
a b
Fig. 10.2 (a, b) Patient with 5 days of upper respiratory infection developed sudden swelling and pain of left eye in 24-hr period. Note erythema, edema, proptosis, chemosis, ophthalmoplegia, and nasal discharge. CT scan demonstrates severe left -sided rhinitis, pan sinusitis, and extension of the infection into the medial left orbit. Note the gas in the anterior ethmoids and orbit
Summary for the Clinician
Orbital cellulitis represents an acute infection ■
with infl ammation of orbital contents, oft en including the pre- and postseptal eyelidsPeriorbital cellulitis can be classifi ed into fi ve ■
stages.Th e fi rst stage is preseptal cellulitis, in which ■
infl ammatory edema remains anterior to the orbital septum.Th e second stage is posterior spread of this ■
infl ammation, behind the arcus marginalis.In the third stage, subperiosteal abscesses may ■
form as pus collects between the orbit and the periosteum of the involved sinus.Th e fourth stage is an orbital abscess. ■
Th e fi ft h involves cavernous sinus thrombosis. ■
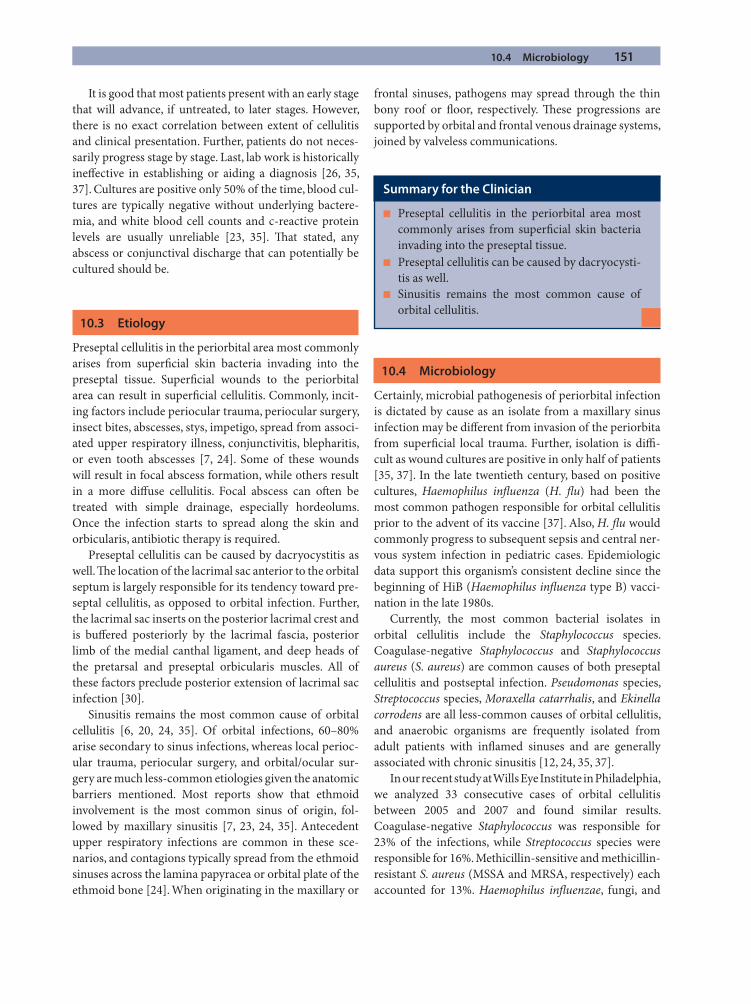
10.4 Microbiology 151
It is good that most patients present with an early stage that will advance, if untreated, to later stages. However, there is no exact correlation between extent of cellulitis and clinical presentation. Further, patients do not neces-sarily progress stage by stage. Last, lab work is historically ineff ective in establishing or aiding a diagnosis [26, 35, 37]. Cultures are positive only 50% of the time, blood cul-tures are typically negative without underlying bactere-mia, and white blood cell counts and c-reactive protein levels are usually unreliable [23, 35]. Th at stated, any abscess or conjunctival discharge that can potentially be cultured should be.
10.3 Etiology
Preseptal cellulitis in the periorbital area most commonly arises from superfi cial skin bacteria invading into the preseptal tissue. Superfi cial wounds to the periorbital area can result in superfi cial cellulitis. Commonly, incit-ing factors include periocular trauma, periocular surgery, insect bites, abscesses, stys, impetigo, spread from associ-ated upper respiratory illness, conjunctivitis, blepharitis, or even tooth abscesses [7, 24]. Some of these wounds will result in focal abscess formation, while others result in a more diff use cellulitis. Focal abscess can oft en be treated with simple drainage, especially hordeolums. Once the infection starts to spread along the skin and orbicularis, antibiotic therapy is required.
Preseptal cellulitis can be caused by dacryocystitis as well. Th e location of the lacrimal sac anterior to the orbital septum is largely responsible for its tendency toward pre-septal cellulitis, as opposed to orbital infection. Further, the lacrimal sac inserts on the posterior lacrimal crest and is buff ered posteriorly by the lacrimal fascia, posterior limb of the medial canthal ligament, and deep heads of the pretarsal and preseptal orbicularis muscles. All of these factors preclude posterior extension of lacrimal sac infection [30].
Sinusitis remains the most common cause of orbital cellulitis [6, 20, 24, 35]. Of orbital infections, 60–80% arise secondary to sinus infections, whereas local perioc-ular trauma, periocular surgery, and orbital/ocular sur-gery are much less-common etiologies given the anatomic barriers mentioned. Most reports show that ethmoid involvement is the most common sinus of origin, fol-lowed by maxillary sinusitis [7, 23, 24, 35]. Antecedent upper respiratory infections are common in these sce-narios, and contagions typically spread from the ethmoid sinuses across the lamina papyracea or orbital plate of the ethmoid bone [24]. When originating in the maxillary or
frontal sinuses, pathogens may spread through the thin bony roof or fl oor, respectively. Th ese progressions are supported by orbital and frontal venous drainage systems, joined by valveless communications.
10.4 Microbiology
Certainly, microbial pathogenesis of periorbital infection is dictated by cause as an isolate from a maxillary sinus infection may be diff erent from invasion of the periorbita from superfi cial local trauma. Further, isolation is diffi -cult as wound cultures are positive in only half of patients [35, 37]. In the late twentieth century, based on positive cultures, Haemophilus infl uenza (H. fl u) had been the most common pathogen responsible for orbital cellulitis prior to the advent of its vaccine [37]. Also, H. fl u would commonly progress to subsequent sepsis and central ner-vous system infection in pediatric cases. Epidemiologic data support this organism’s consistent decline since the beginning of HiB (Haemophilus infl uenza type B) vacci-nation in the late 1980s.
Currently, the most common bacterial isolates in orbital cellulitis include the Staphylococcus species. Coagulase-negative Staphylococcus and Staphylococcus aureus (S. aureus) are common causes of both preseptal cellulitis and postseptal infection. Pseudomonas species, Streptococcus species, Moraxella catarrhalis, and Ekinella corrodens are all less-common causes of orbital cellulitis, and anaerobic organisms are frequently isolated from adult patients with infl amed sinuses and are generally associated with chronic sinusitis [12, 24, 35, 37].
In our recent study at Wills Eye Institute in Philadelphia, we analyzed 33 consecutive cases of orbital cellulitis between 2005 and 2007 and found similar results. Coagulase-negative Staphylococcus was responsible for 23% of the infections, while Streptococcus species were responsible for 16%. Methicillin-sensitive and methicillin-resistant S. aureus (MSSA and MRSA, respectively) each accounted for 13%. Haemophilus infl uenzae, fungi, and
Summary for the Clinician
Preseptal cellulitis in the periorbital area most ■
commonly arises from superfi cial skin bacteria invading into the preseptal tissue.Preseptal cellulitis can be caused by dacryocysti- ■
tis as well.Sinusitis remains the most common cause of ■
orbital cellulitis.

152 10 Management of Periorbital Cellulitis in the 21st Century
10
other microbes contributed to the remaining cases. As other studies have found, underlying sinusitis was by far the most common cause of orbital cellulitis, accounting for 72% of the infections. Extension from endophthalmi-tis, preseptal cellulitis, and dacryocystitis accounted for 10%, 6%, and 6% of the cases, respectively.
Pathogenesis also varies by age group; Staphylococcus and Streptococcus species inoculate the vast majority of children, especially under the age of 9, whereas those teenagers over 14 years old and adults commonly suff er from polymicrobial, mixed aerobic, and anaerobic infec-tions [26, 35]. Between these age groups lies a transition zone in which infections transition from those caused by a single organism to those as a result of a combination of aerobic and anaerobic bacteria [13, 21, 26, 43].
10.5 Changing Pathogens and Resistance
Over the last century, common pathogens in orbital cel-lulitis have changed. Human activity has played the pre-dominant role in changing the microbiology of infections. From vaccines to antibiotics, there has been a profound change in the organisms responsible for causing human morbidity. Measles, mumps, rubella, smallpox, and chicken pox are many of the scourges no longer readily seen by physicians. As mentioned, H. infl uenza as of 20 years ago was a prominent, and oft en devastating, organ-ism involved in a variety of head and neck infections, periorbital cellulitis included. All of these passed to the footnotes of history due to vaccinations.
In addition, the introduction of antibiotics has changed the behavior of bacteria as they evolve in the ongoing battle with humankind. Th e most prevalent problem in the early twenty-fi rst century is MRSA [5, 38, 48]. Th e changing epidemiology of MRSA in both the hospitalized and community populations mirrors the emergence of penicillin-resistant strains of S. aureus
decades ago. Penicillin was fi rst introduced in 1941, and soon thereaft er penicillin resistance among hospitalized patients was being reported. By the end of World War II, most hospital-acquired strains of S. aureus were resistant to penicillin. Th is is largely attributed to previ-ous fi rst-line treatment with beta-lactam antibiotics in these patient populations [55]. Over several decades, most S. aureus infections in the hospitals fi rst and then later in the community became equally resistant to pen-icillin [5].
In a similar manner, methicillin was introduced as a treatment for S. aureus in 1961, and in less than 1 year, resistance to methicillin was reported in the hospital set-ting [38]. Initially, large urban tertiary care centers suf-fered MRSA rates of 10% or less, while smaller community-based institutions were largely unaff ected. Within 25–30 years, over 20% of S. aureus strains in these smaller, nonreferral centers were resistant to methicillin, as were over 40% in larger urban institutions. By 1998, resistance reached 50% in hospital settings, and soon aft er, rates of resistance in the community-based population quickly rose. Currently, rates of hospital-acquired MRSA are well over 80%, with recent exponential rises in several epidemiologic studies from around the United States.
Infections due to community-acquired MRSA (CA-MRSA) have been reported all over the world and have been exponentially growing in incidence [10, 14, 22, 49, 55]. Based on the aforementioned epidemiology of penicillin resistance, the CA-MRSA should exponentially continue to increase over the next decade. Studies between 1995 and 2006 showed CA-MRSA rates increasing from about 20% to about 60% in patients presenting with soft tissue infections [22, 33, 38]. A study found 68% of staph-ylococcal isolates from periorbital cellulitis were methi-cillin resistant [23].
10.5.1 CA-MRSA Versus Hospital-Acquired MRSA
Th e most likely mechanism of methicillin resistance in S. aureus comes secondary to the presence of the mecA gene complex, which transcribes a penicillin-binding protein that has multiple insertion sequences within its targeted DNA fragment [11, 22]. Th is mechanism accounts for the resistance of hospital-acquired MRSA to many antibiotics. Although it has variations of these genes, CA-MRSA is comparably susceptible to many non-beta-lactam antibiot-ics and can typically be successfully treated with a variety of available antibiotics, including tetracyclines, vancomy-cin, clindamycin, and sulfa-based drugs [22, 48, 49]. Th is
Summary for the Clinician
Th e most common bacterial isolates in orbital ■
cellulitis include the Staphylococcus species.Coagulase-negative ■ Staphylococcus and S. aureus are common causes of both preseptal cellulitis and postseptal infection.Pseudomonas ■ species, Streptococcus species, Moraxella catarrhalis, and Ekinella corrodens are all less-common causes of orbital cellulitis.
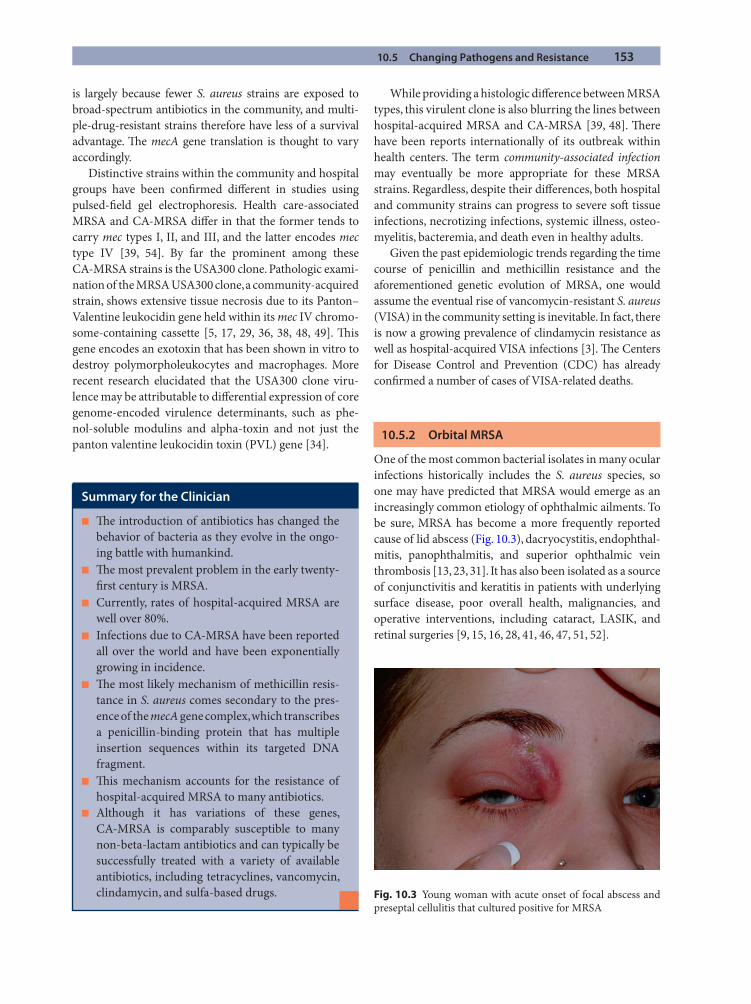
10.5 Changing Pathogens and Resistance 153
is largely because fewer S. aureus strains are exposed to broad-spectrum antibiotics in the community, and multi-ple-drug-resistant strains therefore have less of a survival advantage. Th e mecA gene translation is thought to vary accordingly.
Distinctive strains within the community and hospital groups have been confi rmed diff erent in studies using pulsed-fi eld gel electrophoresis. Health care-associated MRSA and CA-MRSA diff er in that the former tends to carry mec types I, II, and III, and the latter encodes mec type IV [39, 54]. By far the prominent among these CA-MRSA strains is the USA300 clone. Pathologic exami-nation of the MRSA USA300 clone, a community-acquired strain, shows extensive tissue necrosis due to its Panton–Valentine leukocidin gene held within its mec IV chromo-some-containing cassette [5, 17, 29, 36, 38, 48, 49]. Th is gene encodes an exotoxin that has been shown in vitro to destroy polymorpholeukocytes and macrophages. More recent research elucidated that the USA300 clone viru-lence may be attributable to diff erential expression of core genome-encoded virulence determinants, such as phe-nol-soluble modulins and alpha-toxin and not just the panton valentine leukocidin toxin (PVL) gene [34].
While providing a histologic diff erence between MRSA types, this virulent clone is also blurring the lines between hospital-acquired MRSA and CA-MRSA [39, 48]. Th ere have been reports internationally of its outbreak within health centers. Th e term community-associated infection may eventually be more appropriate for these MRSA strains. Regardless, despite their diff erences, both hospital and community strains can progress to severe soft tissue infections, necrotizing infections, systemic illness, osteo-myelitis, bacteremia, and death even in healthy adults.
Given the past epidemiologic trends regarding the time course of penicillin and methicillin resistance and the aforementioned genetic evolution of MRSA, one would assume the eventual rise of vancomycin-resistant S. aureus (VISA) in the community setting is inevitable. In fact, there is now a growing prevalence of clindamycin resistance as well as hospital-acquired VISA infections [3]. Th e Centers for Disease Control and Prevention (CDC) has already confi rmed a number of cases of VISA-related deaths.
10.5.2 Orbital MRSA
One of the most common bacterial isolates in many ocular infections historically includes the S. aureus species, so one may have predicted that MRSA would emerge as an increasingly common etiology of ophthalmic ailments. To be sure, MRSA has become a more frequently reported cause of lid abscess (Fig. 10.3), dacryocystitis, endophthal-mitis, panophthalmitis, and superior ophthalmic vein thrombosis [13, 23, 31]. It has also been isolated as a source of conjunctivitis and keratitis in patients with underlying surface disease, poor overall health, malignancies, and operative interventions, including cataract, LASIK, and retinal surgeries [9, 15, 16, 28, 41, 46, 47, 51, 52].
Summary for the Clinician
Th e introduction of antibiotics has changed the ■
behavior of bacteria as they evolve in the ongo-ing battle with humankind.Th e most prevalent problem in the early twenty- ■
fi rst century is MRSA.Currently, rates of hospital-acquired MRSA are ■
well over 80%.Infections due to CA-MRSA have been reported ■
all over the world and have been exponentially growing in incidence.Th e most likely mechanism of methicillin resis- ■
tance in S. aureus comes secondary to the pres-ence of the mecA gene complex, which transcribes a penicillin-binding protein that has multiple insertion sequences within its targeted DNA fragment.Th is mechanism accounts for the resistance of ■
hospital-acquired MRSA to many antibiotics.Although it has variations of these genes, ■
CA-MRSA is comparably susceptible to many non-beta-lactam antibiotics and can typically be successfully treated with a variety of available antibiotics, including tetracyclines, vancomycin, clindamycin, and sulfa-based drugs. Fig. 10.3 Young woman with acute onset of focal abscess and
preseptal cellulitis that cultured positive for MRSA
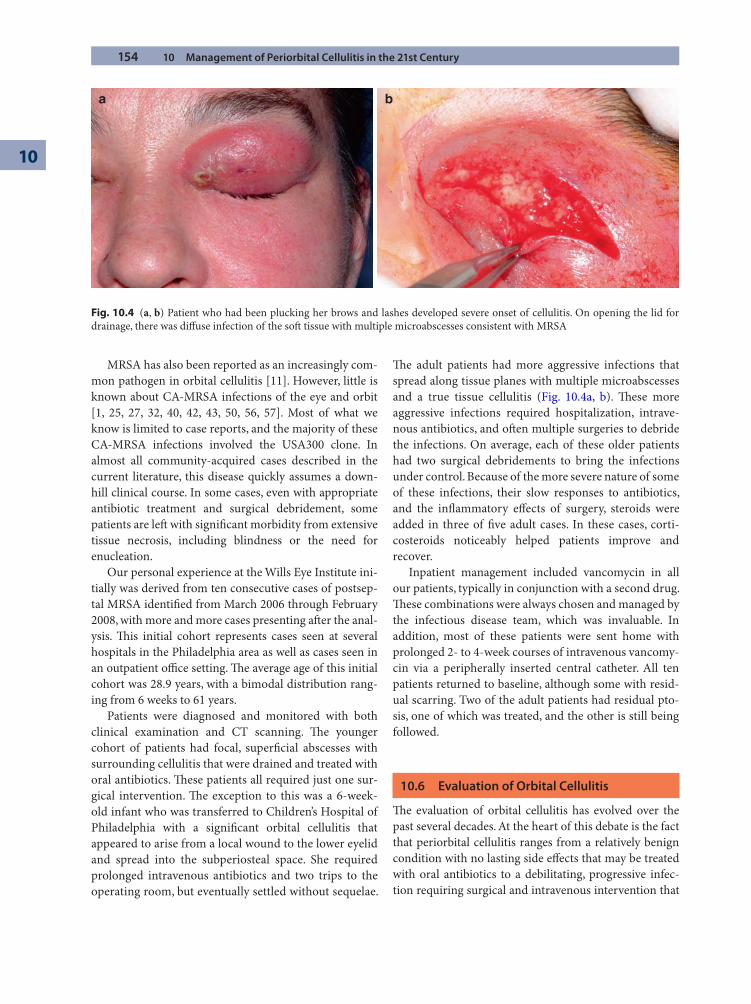
154 10 Management of Periorbital Cellulitis in the 21st Century
10
MRSA has also been reported as an increasingly com-mon pathogen in orbital cellulitis [11]. However, little is known about CA-MRSA infections of the eye and orbit [1, 25, 27, 32, 40, 42, 43, 50, 56, 57]. Most of what we know is limited to case reports, and the majority of these CA-MRSA infections involved the USA300 clone. In almost all community-acquired cases described in the current literature, this disease quickly assumes a down-hill clinical course. In some cases, even with appropriate antibiotic treatment and surgical debridement, some patients are left with signifi cant morbidity from extensive tissue necrosis, including blindness or the need for enucleation.
Our personal experience at the Wills Eye Institute ini-tially was derived from ten consecutive cases of postsep-tal MRSA identifi ed from March 2006 through February 2008, with more and more cases presenting aft er the anal-ysis. Th is initial cohort represents cases seen at several hospitals in the Philadelphia area as well as cases seen in an outpatient offi ce setting. Th e average age of this initial cohort was 28.9 years, with a bimodal distribution rang-ing from 6 weeks to 61 years.
Patients were diagnosed and monitored with both clinical examination and CT scanning. Th e younger cohort of patients had focal, superfi cial abscesses with surrounding cellulitis that were drained and treated with oral antibiotics. Th ese patients all required just one sur-gical intervention. Th e exception to this was a 6-week-old infant who was transferred to Children’s Hospital of Philadelphia with a signifi cant orbital cellulitis that appeared to arise from a local wound to the lower eyelid and spread into the subperiosteal space. She required prolonged intravenous antibiotics and two trips to the operating room, but eventually settled without sequelae.
Th e adult patients had more aggressive infections that spread along tissue planes with multiple microabscesses and a true tissue cellulitis (Fig. 10.4a, b). Th ese more aggressive infections required hospitalization, intrave-nous antibiotics, and oft en multiple surgeries to debride the infections. On average, each of these older patients had two surgical debridements to bring the infections under control. Because of the more severe nature of some of these infections, their slow responses to antibiotics, and the infl ammatory eff ects of surgery, steroids were added in three of fi ve adult cases. In these cases, corti-costeroids noticeably helped patients improve and recover.
Inpatient management included vancomycin in all our patients, typically in conjunction with a second drug. Th ese combinations were always chosen and managed by the infectious disease team, which was invaluable. In addition, most of these patients were sent home with prolonged 2- to 4-week courses of intravenous vancomy-cin via a peripherally inserted central catheter. All ten patients returned to baseline, although some with resid-ual scarring. Two of the adult patients had residual pto-sis, one of which was treated, and the other is still being followed.
10.6 Evaluation of Orbital Cellulitis
Th e evaluation of orbital cellulitis has evolved over the past several decades. At the heart of this debate is the fact that periorbital cellulitis ranges from a relatively benign condition with no lasting side eff ects that may be treated with oral antibiotics to a debilitating, progressive infec-tion requiring surgical and intravenous intervention that
a b
Fig. 10.4 (a, b) Patient who had been plucking her brows and lashes developed severe onset of cellulitis. On opening the lid for drainage, there was diff use infection of the soft tissue with multiple microabscesses consistent with MRSA

10.7 Medical Treatment of Orbital Cellulitis 155
potentially leads to optic nerve dysfunction, central ner-vous system damage, and even death. Complicating this devastating range of infectious manifestations is the potentially rapid rate of orbital expansion that can occur, leading to the aforementioned consequences.
Aft er completing a thorough physical exam, dedicated orbital CT scan is the investigation of choice for preseptal and orbital cellulitis [8, 24]. However, not every patient warrants radiological evaluation. On initial presentation, CT can assess the sinuses and extent of periorbital infec-tion if edema is excessive and the clinician is unsure that the infection is solely preseptal. Patients with clear clini-cal pictures and no signs of postseptal or optic nerve involvement do not need CT evaluation. On the other hand, patients with worsening clinical presentation, prop-tosis, ophthalmoplegia, worsening visual acuity, declin-ing color vision, bilateral symptomotology, or signs of central nervous system complications require immediate CT scan, especially if surgery is planned because of orbital compression or if there is no clinical response to treat-ment aft er 48 h [8, 24, 43, 53].
Th e use of CT must be tempered with the knowledge that radiologic improvement will lag behind the clinical picture by a number of days [24]. CT scans are helpful in aiding the initial evaluation of orbital cellulitis, the loca-tion of the primary infection, and the risk of spread to surrounding areas. Yet, the clinical examination and fol-low-up, not CT scans, should drive therapy, and CT scans should not be repeated regularly once obtained. Once orbital cellulitis is diagnosed, the clinical exam and cul-ture results will dictate appropriate management with specifi c antibiotics and possible surgery. If rapid visual decline occurs on clinical exam, operative intervention will take place well before a follow-up CT scan docu-ments progression. Repeat CT scan may be useful in fol-low-up to rule out frontal lobe abscesses if the clinical exam dictates.
10.7 Medical Treatment of Orbital Cellulitis
Medical therapy of periorbital cellulitis obviously requires the use of antibiotics, but which one is the typical ques-tion. Preseptal infection is typically treated with oral anti-biotics. Orbital infections require immediate intravenous antibiotic therapy, targeting the most likely pathogens. In the early twenty-fi rst century, broad-spectrum antibiotics that cover gram-positive organisms, including MRSA, are the best place to start for preseptal infections. Choices of oral antibiotics may include doxycycline, trimethoprim-sulfamethoxazole, clindamycin, or fl uoroquiolones.
In orbital cellulitis, anaerobes will potentially be involved, in addition to gram-positive cocci and MRSA. In these typically polymicrobial infections, the use of two agents with broad coverage is oft en required until culture results are obtained. Intravenous antibiotic choices would include vancomycin, clindamycin, ampicillin sulbactam, second- or third-generation cephalosporins, aminoglyco-sides, and fl uoroquinolones. Transition to oral antibiotics may occur once improvement is documented and sus-tained [4, 45, 53]. Interestingly, data showed that oral cip-rofl oxacin and clindamycin may be equally eff ective and safe as initial intravenous therapy for advanced cases [4]. Th is is not standard of care, however.
Targeting specifi c pathogens initially may be diffi cult as most studies agreed that routine local culture or blood cultures are typically negative and thus unhelpful. Th e yield is quite low on all pathogenic studies. Further, what data do exist in favor of culture are oft en biased; histori-cally, the treatment-refractory and most severe cases are those that have been cultured surgically, yielding poorly universal data pointing toward highly aggressive polymi-crobial etiologies of infection [37].
If surgery is performed and microbiology obtained, antibiotics can be changed pending sensitivities. If speci-mens are not obtained, clinical suspicion and broad-spectrum antibiotics geared toward the aforementioned common pathogens remain the gold standard. Further, one must remember the changing spectrum of orbital cel-lulitis pathogens and the currently growing level of resistance. If suspicion for MRSA is high or broad-spectrum treat-ment ineff ective, appropriate therapy must be redirected.
Fortunately, there are still multiple antibiotics that work against CA-MRSA. Th ese include sulfonamides such as trimethoprim-sulfamethoxazole, quinolones, aminoglycosides, tetracyclines, clindamycin, and rifampin; all off er potential aid in curing the infection. Clindamycin or trimethoprim-sulfamethoxazole should be used in children with MRSA as fl uoroquinolones and tetracy-clines cannot be utilized in this age group. Vancomycin,
Summary for the Clinician
MRSA has also been reported as an increasingly ■
common pathogen in orbital cellulitis.Th e evaluation of orbital cellulitis has evolved ■
over the past several decades.Dedicated orbital CT scan is the investigation of ■
choice for preseptal and orbital cellulitis.Th e use of CT must be tempered with the knowl- ■
edge that radiologic improvement will lag behind the clinical picture by a number of days.
156 10 Management of Periorbital Cellulitis in the 21st Century
10
linezolid, and amikacin are eff ective as well, although usually reserved for aggressive infections and multiresis-tant hospital-acquired MRSA [17, 49, 55].
Many infectious disease doctors rightfully worry about Clostridium diffi cile from prolonged clindamycin use. Th is should be taken into consideration when pre-scribing antibiotics, especially since drug-resistant C. diffi cile is now being reported. In addition, more clin-damycin-resistant cases of MRSA continue to occur, and it is becoming less of a fi rst-line agent.
Nasal decongestants used in the short term will open sinus passages and may augment antibiotic treatment by reducing sinus swelling and improving drainage [24]. Also, the use of corticosteroids in the setting of infection is certainly controversial [58]. Many otolaryngologists manage acute sinusitis with the combination of antibiot-ics and steroids since steroids diminish the mucosal edema that prevents the sinuses from opening and drain-ing. Th is is true even in cases that have secondary orbital cellulitis. No doubt, the orbit is a small space, and its
structures are at risk for compression during an acute process like orbital cellulitis. If bactericidal antibiotics are utilized to destroy the bacteria, then reducing the infl am-mation within the orbit may reduce the risk for a com-partment syndrome. In our anecdotal experience, steroids do seem to help these patients and are typically started with antibiotic therapy if signifi cant swelling and com-pression are present.
10.8 Surgical Treatment of Orbital Cellulitis
While the advent of CT in the evaluation of orbital cellu-litis has become critical for diagnostic purposes, debates regarding antibiotic regimen, use of corticosteroids, and surgical drainage have persisted ever since. Management is therefore another point of contention within the recent literature. Fundamentally, when progressing and extend-ing below the periosteum, orbital cellulitis subsists in a largely avascular area with relatively decreased mucosal blood fl ow. Th is, coupled with the fact that increasing age usually coincides with mixed infections and microbial synergy, may augment antibiotic resistance [21]. Th us, intravenous antibiotics that are eff ective against orbital pathogens in vitro may be ineff ective in the clinical treat-ment of advanced orbital cellulitis. Management of orbital cellulitis may therefore be quite diffi cult.
Treatment regimens and management styles have, and oft en remain, largely driven by individual experiences and physician preferences. Many doctors treat with only antibiotics, having positive personal experiences with such regimens. Th ese physicians are oft en of the mindset that surgery may seed adjacent areas and reserve such invasive interventions for antibiotic-refractory cases as a result [53]. Further, some reports have shown that early drainage actually prolongs hospitalization. Contradicting this, other cases portend that early surgical intervention may shorten hospital courses; to wait too long for surgical drainage may lead to infection that does not sterilize even with abscess drainage [21].
Harris revolutionized this argument in 1994 by mak-ing age a large factor in the management of orbital cellu-litis [21]. His review confi rmed the tendency to culture-negative or single-isolate infections in children younger than 9 years that responded to antibiotic therapy alone. Ten of his 12 patients younger than 9 years old required no surgical intervention; the remaining 2 cleared their infection promptly aft er intervention. Four of the 16 patients between 9 and 14 years of age cleared without drainage, while a diff erent 25% in this transitional age range had refractory and multiorganism infections. Polymicrobial illnesses were the norm in the nine adults,
Summary for the Clinician
Preseptal infection is typically treated with oral ■
antibiotics.Orbital infections require immediate intrave- ■
nous antibiotic therapy.Choices of oral antibiotics may include doxycy- ■
cline, trimethoprim-sulfamethoxazole, clindamy-cin, or fl uoroquiolones.In orbital cellulitis, anaerobes will potentially be ■
involved in addition to gram-positive cocci and MRSA.Th e use of two agents with broad coverage is ■
oft en required until culture results are obtained.Intravenous antibiotic choices include vancomycin, ■
clindamycin, ampicillin sulbactam, second- or third-generation cephalosporins, aminoglycosides, and fl uoroquinolones.Transition to oral antibiotics may occur once ■
improvement is documented and sustained.Nasal decongestants used in the short term will ■
open sinus passages and may augment antibiotic treatment by reducing sinus swelling and improv-ing drainage.Many otolaryngologists manage acute sinusitis ■
with the combination of antibiotics and steroids since steroids diminish the mucosal edema that prevents the sinuses from opening and draining.

10.8 Surgical Treatment of Orbital Cellulitis 157
and on average they had fi ve diff erent bacteria isolated from each culture.
Experience gleaned from these studies divided need for surgical intervention into emergent, urgent, and expectant groups. Keep in mind that most cases of orbital cellulitis arise primarily from acute sinusitis. Th us, sinus surgery is the key component in the surgical treatment of orbital cellulitis arising from the sinus infection. As a result, otolaryngology involvement up front is a very important part of managing these patients. Emergency drainage was deemed appropriate for cases of optic nerve or retinal compromise secondary to induced mass eff ect. Th is is true for all ages. Urgent drainage is described in this review as drainage within 24 h of presentation. Categorized therein are large subperiosteal abscesses and abscesses that have extended away from the sinuses of origin or atypical infections not arising from the sinus (Fig. 10.5a,b). Frontal sinusitis should be urgently drained for pathogen identifi cation and evaluation as central ner-vous system penetration of the infection is more likely and can be quite devastating. Also, since virtually all patients older than 14 years will have a complex, polymi-crobial infection, these infections should be drained more urgently as antibiotics are less likely to be eff ective.
Patients younger than 9 years may be observed, given the predilection toward simple infections in this popula-tion and the typical response to antibiotics alone. Expectant management may also be used for patients with no visual compromise, small medial subperiosteal abscesses and eff usions, and cases with no frontal sinus or intracranial involvement. However, while hospitalized and on intravenous antibiotics, these patients must be clinically monitored on a regular basis for progression
and development of an aff erent pupillary defect, visual decline, fevers that do not defervesce within 36 h, or 3 days without clinical improvement.
In a more recent publication, Harris further summa-rized criteria necessary for the initiation of nonsurgical intervention [18]. Th e following needed to be absent: age of 9 years or older, frontal sinusitis, nonmedial or large subperiosteal abscess, gas within abscess on CT or other suspicion of anaerobic infection, recurrence aft er prior surgical intervention, radiologic evidence of chronic sinusitis, acute optic nerve or retinal compromise, or dental etiology of infection predisposing to anaerobic infi ltration. Importantly, it was noted that clinical judg-ment is of utmost importance in all cases. Patients even without these signs may warrant surgery if clinically dete-riorating, so these patients should have clinical exams regularly. Conversely, even patients with these signs may be treated medically if clinically stable.
Most studies agreed that surgery is warranted in the circumstances mentioned. However, several more recent studies supported that surgical drainage is justifi ed in all abscesses obvious on CT scan, regardless of patient age or clinical presentation [24]. Still, other reports in the twenty-fi rst century argued that immediate intravenous antibiot-ics are the treatment of choice for subperiosteal abscesses as well as retrobulbar loculations [4, 45, 53]. Certain pedi-atric textbooks written in the last 10–12 years argue those very facts, some of which entertain immediate surgical drainage and watch-and-wait protocols in the same chap-ter [53]. It seems that the only universal rule within the current literature is that the decision to treat must rest on the physician’s opinion, clinical judgment, and knowledge of the potential course of orbital cellulitis.
a b
Fig. 10.5 (a, b) Th is gentleman presented 12 h aft er trying to rinse a foreign body out of his right eye; he had severe orbital cellulitis, decreased vision, and ophthalmoplegia. CT scan revealed an atypical lateral orbital infection; thus, he was started on antibiotics and taken to the operating room. Th ere was no abscess, just diff use soft tissue infection and a superior fornix conjunctival abscess. MRI obtained a few days later (as he was not improving) demonstrated lateral orbital cellulitis and infection of the lateral rectus muscle. His fi nal cultures were positive for MRSA
158 10 Management of Periorbital Cellulitis in the 21st Century
10
10.9 Prevention of Orbital Cellulitis After Orbital Fracture
Orbital cellulitis is a rare side eff ect of an orbital fracture [2]. When cellulitis does result from orbital blowout frac-ture, one mechanism is thought to be the formation of anatomical communications between the fractured sinuses and orbit [19]. However, the sinus is a sterile space. Th ese new anatomical communications between the orbit and sinus exist for the life of the patient. As a
result, cellulitis may arise from several days to over 20 years aft er initial orbital injury. In addition, orbital decompression is a common procedure, representing a controlled fracture of the sinus, and has a very low inci-dence of postoperative orbital infection. Further, sinuses are protected by lymphocytes, interferons, and alkaline mucus that circulates every 10 min. Logically, sinusitis in these fracture patients has been associated with the devel-opment of subsequent orbital cellulitis, albeit rarely, espe-cially in the early healing phases weeks to months aft er the injury. Th e role for prophylactic antibiotics has never been established. Th e potential orbital cellulitis following fracture should hold no clinical importance in patients not suff ering from sinusitis.
Given the very low incidence of cellulitis attributable to blowout fractures, the prolonged healing of sinus mucosa compared to the short nature of antibiotic treat-ment, the possibility of a long lag period between injury and orbital cellulitis, and previous case reports showing no obvious benefi t from the prophylaxis of orbital celluli-tis following blowout fracture, physicians should consider not prescribing antibiotics for orbital fractures. Th e prac-tice thereof may be unnecessarily costly, time consuming, and potentially harmful to the patients in this era of anti-biotic resistance. Patients with active sinus disease at the time of their fracture should still be treated with oral anti-biotics, even though studies show they do not always pre-vent infection.
Summary for the Clinician
Intravenous antibiotics eff ective against orbital ■
pathogens in vitro may be ineff ective in the clini-cal treatment of advanced orbital cellulitis.Harris confi rmed the tendency toward culture- ■
negative or single-isolate infections in children younger than 9 years that responded to antibi-otic therapy alone.Experience gleaned from these studies has clas- ■
sifi ed the need for surgical intervention into emergent, urgent, and expectant groups.Emergency drainage was deemed appropriate ■
for cases of optic nerve or retinal compromise secondary to induced mass eff ect.Virtually all patients older than 14 years will ■
have a complex, polymicrobial infection, which should be drained more urgently as antibiotics are less likely to be eff ective.Patients younger than 9 years can usually be ■
observed given the predilection to simple infec-tions in this population and the typical response to antibiotics alone.For observation, the following need to be ■ absent: age of 9 years or older, frontal sinusitis, nonme-dial or large subperiosteal abscess, gas within abscess on CT or other suspicion of anaerobic infection, recurrence aft er prior surgical inter-vention, radiologic evidence of chronic sinusitis, acute optic nerve or retinal compromise, or den-tal etiology of infection predisposing to anaero-bic infi ltration.Th e only universal rule in the current literature ■
is that the decision to intervene surgically must rest on the physician’s opinion, clinical judg-ment, and knowledge of the potential course of orbital cellulitis.
Summary for the Clinician
It is important to consider MRSA as a cause of ■
infection when choosing appropriate antibiotic therapy.CT scan of the orbit and sinus is a very helpful ■
tool when determining the best course of treatment.Antibiotics are most eff ective as single therapy in ■
young children, whereas antibiotics and surgery are more oft en needed in teenagers and adults.MRSA infections of the orbit require aggressive ■
management with appropriate antibiotics and early surgery when indicated.Atypical infections like orbital cellulitis not aris- ■
ing from the sinus or infections that potentially may spread to adjacent areas (like frontal sinus-itis with orbital involvement and possible intrac-ranial spread) should be treated surgically in a more urgent matter.

References 159
References
1. Anari S, Karagama YG, Fulton B, Wilson JA (2005 Jan) Neonatal disseminated methicillin-resistant Staphylococcus aureus presenting as orbital cellulitis. J Laryngol Otol 119(1):64–67
2. Ben Simon GJ, Bush S, Selva D, McNab AA (2005 Nov) Orbital cellulitis: a rare complication aft er orbital blowout fracture. Ophthalmology 112:2030–2034
3. Braun L, Craft D, Williams R, et al (2005) Increasing clin-damycin resistance among methicillin-resistant Staphy-lococcus aureus in 57 northeast United States military treatment facilities. Pediatr Infect Dis J 24:622–626
4. Cannon PS, Keag DM, Radford R (2008 Feb 29) Our expe-rience using primary oral antibiotics in the management of orbital cellulitis in a tertiary referral centre. Eye (Epub ahead of print)
5. Chambers HR (2001) Th e changing epidemiology of Staphylococcus aureus? Emerging Infect Dis 7(2):178–182
6. Chandler JR, Langenbrunner DJ, Stevens ER (1970) Th e pathogenesis of orbital complications in acute sinusitis. Laryngoscope 80:1414–1428
7. Chaudhry IA, Shamsi FA, Elzaridi E, Al-Rashed W, Al-Amri A, Arat YO (2008) Inpatient preseptal cellulitis: experience from a tertiary eye care centre. Br J Ophthalmol 92(10):1337–1341
8. Ho CF, Huang YC, Wang CJ, et al (2007) Clinical analysis of computed tomography-staged orbital cellulitis in chil-dren. J Microbiol Immunol Infect 40
9. Chiang RK, Rapuano CJ (2002) Recurrent methicillin-resistant Staphylococcus aureus wound ulcer aft er clear-cornea cataract surgery. CLAO J 28:109–110
10. Connell B, Kamal Z, McNab AA (2001) Fulminant orbital cellulitis with complete loss of vision. Clin Exp Ophthalmol 29:260–261
11. Deurenberg RH, Stobberingh EE (2009 Mar) Th e molecu-lar evolution of hospital- and community-associated methicillin-resistant Staphylococcus aureus. Curr Mol Med 9(2):100–115
12. Devrim I, Kanra G, Kara A, et al (2008 May–Jun) Preseptal and orbital cellulitis: 15-year experience with sulbactam ampicillin treatment. Turk J Pediatr 50(3):214–218
13. Dhariwal DK, Kittur MA, Farrier JN, Sugar AW, Aird DW, Laws DE (2003) Post-traumatic orbital cellulitis. Br J Oral Maxillofacial Surg 41:21–28
14. Diep BA, Chambers HF, Graber CJ, et al (2008) Emergence of multidrug-resistant, community-associated, methicil-lin-resistant Staphylococcus aureus clone USA300 in men who have sex with men. Ann Intern Med 148(4):249–257
15. Donnenfeld ED, O’Brien TP, Solomon R, et al (2003) Infectious keratitis aft er photorefractive keratectomy. Ophthalmology 110:743–747
16. Forster W, Becker K, Hungermann D, Busse H (2002) Methicillin-resistant Staphylococcus aureus keratitis aft er excimer laser photorefractive keratectomy. J Cataract Refract Surg 28:722–724
17. Frazee BW, Lynn J, Charlebois ED, Lambert L, Lowery D, Perdreau-Remington F (2005) High prevalence of methicil-lin-resistant Staphylococcus aureus in emergency department skin and soft tissue infections. Ann Emerg Med 45:311–320
18. Garcia GH, Harris GJ (2000) Criteria for nonsurgical man-agement of subperiosteal abscess of orbit: analysis of out-comes 1988–1998. Ophthalmol 107:1454–1456
19. Goldfarb MS, Hoff man DS, Rosenberg S (1987) Orbital cellulitis and orbital fractures. Ann Ophthalmol 19:97–99
20. Goodyear PWA, Firth AL, Strachan DR, Dudley M (2004) Periorbital swelling: the important distinction between allergy and infection. Emerg Med J 21:240–242
21. Harris GJ (1994) Subperiosteal abscess of the orbit. Age as a factor in the bacteriology and response to treatment. Ophthalmology 101(3):585–595
22. Herold BC, Immergluck LC, Maranan MC, et al (1998) Community-acquired methicillin-resistant Staphylococcus aureus in children with no identifi ed predisposing risk. JAMA 279:593–598
23. Ho CF, Huang YC, Wang CJ, et al (2007) Clinical analysis of computed tomography-staged orbital cellulitis in chil-dren. J Microbiol Immunol Infect 40:518–524
24. Howe L, Jones NS (2004) Guidelines for the management of periorbital cellulitis/abscess. Clin Otolaryngol 29:725–728
25. Ingraham HJ, Ryan ME, Burns JT, Shuhart D, Tenedios G, Malone W, et al (1995 Aug) Streptococcal preseptal celluli-tis complicated by the toxic Streptococcus syndrome. Ophthalmology 102(8):1223–1226
26. Jakobiec FA, Bilyk JR, Font RL (1990) Orbit. In: Spencer WH (ed) Ophthalmic pathology, Vol 4, 4th ed. Saunders, Philadelphia, pp. 2861–2872
27. Kannoth S, Iyer R, Th omas SV, Furtado SV, Rajesh BJ, Kesavadas C, et al (2007 May 15) Intracranial infectious aneurysm: presentation, management and outcome. J Neurol Sci 256(1–2):3–9. (Epub 23 Mar 2007)
28. Kato T, Hayasaka S (1998) Methicillin-resistant Staph-ylococcus aureus and methicillin-resistant coagulase-negative staphylococci from conjunctivas of preoperative patients. Jpn J Ophthalmol 42:461–465
29. Kazakova SV, Hageman JC, Matava M, et al (2005) A clone of methicillin-resistant Staphylococcus aureus among pro-fessional football players. N Engl J Med 352:468–475
30. Kikkawa DO, Heinz GW, Martin RT (2002) Orbital celluli-tis and abscess secondary to dacryocystitis. Arch Oph-thalmol 120:1096–1099
31. Kotlus BS, Rodgers IR, Udell IJ (2005) Dacryocystitis caused by community-onset methicillin-resistant Staphylococcus aureus. Ophthal Plast Reconstr Surg 25:371–375

160 10 Management of Periorbital Cellulitis in the 21st Century
10
32. Kronish JW, Johnson TE, Gilberg SM, Corrent GF, McLeish WM, Scott KR (1996 Sep) Orbital infections in patients with human immunodefi ciency virus infection. Ophthal mology 103(9):1483–1492
33. Layton MC, Hierholzer WJ, Jr, Patterson JE (1995) Th e evolving epidemiology of methicillin-resistant Staphy-lococcus aureus at a university hospital. Infect Control Hosp Epidemiol 16:12–17
34. Li M, Diep BA, Villaruz AE, Braughton KR, Jiang X, DeLeo FR, Chambers HF, Lu Y, Otto M (2009) Evolution of viru-lence in epidemic community-associated methicillin-resis-tant Staphylococcus aureus. Proc Natl Acad Sci USA 106(14):5883–5888
35. Liu IT, Kao SC, Wang AG, et al (2006) Preseptal and orbital cellulitis: a 10-year review of hospitalized patients. J Chin Med Assoc 69(9):415–422
36. McDougal LK, Steward CD, Killgore GE, Chaitram JM, McAllister SK, Tenover FC (2003) Pulsed-fi eld gel electro-phoresis typing of oxacillin-resistant Staphylococcus aureus isolates from the United States: establishing a national database. J Clin Microbiol 41:5113–5120
37. McKinley SH, Yen MT, Miller AM, et al (2007) Micro-biology of pediatric orbital Ccllulitis. Am J Opthalmol 144: 497–501
38. Moran GJ, Krishnadasan A, Gorwitz RJ, Fosheim GE, McDougal LK, Carey RB, et al (2006; Aug) Methicillin-resistant S. aureus infections among patients in the emer-gency department. N Engl J Med 355:666–674
39. Moroney SM, Heller LC, Arbuckle J, Talavera M, Widen RH (2007) Staphylococcal cassette chromosome mec and Panton–Valentine leukocidin characterization of methicil-lin-resistant Staphylococcus aureus clones. J Clin Microbiol 45(3):1019–1021
40. Orekoya AM, McMoli TE (1987 Mar) Morbidity and mor-tality from orbital cellulitis. East Afr Med J 64(3):190–193
41. Oshima Y, Ohji M, Inoue Y, et al (1999) Scleral buckling: methicillin-resistant Staphylococcus aureus infections aft er scleral buckling procedures for retinal detachments associ-ated with atopic dermatitis. Ophthalmol 106:142–147
42. Oshitari K, Hirakata A, Okada AA, Hida T, Oda H, Miki D, et al (2003 Oct) Vitrectomy for endophthalmitis aft er cata-ract surgery [in Japanese]. Nippon Ganka Gakkai Zasshi 107(10):590–596.
43. Osmoti AE, Ogbedo E (2007 Mar) Ophthalmic mortality in a tertiary centre in Nigeria. Niger Postgrad Med J 14(1): 54–56
44. Paterson AW, Barnard NA, Irvine GH (1994) Naso-orbital fracture leading to orbital cellulitis and visual loss as a complication of chronic sinusitis. Br J Oral Maxillofacial Surg 30:80–82
45. Pereira KD, Mitchell RB, Younis RT, Lazar RH (1997) Management of medial subperiosteal abscess of the orbit in children—a 5 year experience. Int J Pediatr Otorhinol 38:247–254
46. Rubinfeld RS, Negvesky GJ (2001) Methicillin-resistant Staphylococcus aureus ulcerative keratitis aft er laser in situ keratomilieusis. J Cataract Refract Surg 27:1523–1525
47. Rudd JC, Morshifar M (2001) Methicillin-resistant Staphy-lococcus aureus keratitis aft er laser in situ keratomileusis. J Cataract Refract Surg 27:471–473
48. Rutar T, Chambers HF, Crawford JB, Perdreau-Remington F, Zwick OM, Karr M, et al (2006) Ophthalmic manifesta-tions of infections caused by the USA300 clone of commu-nity-associated methicillin-resistant Staphylococcus aureus. Ophthalmology 113(8):1455–1462
49. Rutar T, Zwick OM, Cockerham KP, Horton JC (2005) Bilateral blindness from orbital cellulitis caused by com-munity-acquired methicillin-resistant Staphylococcus aureus. Am J Ophthalmol 140(4):740–742
50. Shanmuganathan VA, Armstrong M, Buller A, Tullo AB (2005) External ocular infections due to methicillin-resis-tant Staphylococcus aureus (MRSA). Eye 19:284–291
51. Solomon R, Donnenfeld ED, Perry HD, Biser S (2003) Bilateral methicillin-resistant Staphylococcus aureus kerati-tis in a medical resident following an uneventful bilateral photorefractive keratectomy. Eye Contact Lens 29:187–189
52. Sotozono C, Inagaki K, Fujita A, et al (2002) Methicillin-resistant Staphylococcus aureus and methicillin-resistant Staphylococcus epidermidis infections in the cornea. Cornea 21:S94–S101
53. Starkey CR, Steele RW (2001 Oct) Medical management of orbital cellulitis. Pediatr Infect Dis J 20(10):1002–1005
54. Strandén AM, Frei R, Adler H, Flückiger U, Widmer AF (2009) Emergence of SCCmec Type IV as the most com-mon type of methicillin-resistant Staphylococcus aureus in a university hospital. Infection 37(1):44–48
55. Tacconelli E, De Angelis G, Cataldo MA, Pozzi E, Cauda R (2008) Does antibiotic exposure increase the risk of meth-icillin-resistant Staphylococcus aureus (MRSA) isolation? A systematic review and meta-analysis. J Antimicrob Chemother 61:26–38
56. Uy HS, Tuano PM (2007 Mar) Preseptal and orbital cellu-litis in a developing country. Orbit 26(1):33–37
57. Walker JC, Sandhu A, Pietris G (2002 Apr) Septic superior ophthalmic vein thrombosis. Clin Exp Ophthalmol 30(2): 144–146
58. Yen MT, Yen KG (2005 Sep) Eff ect of corticosteroids in the acute management of pediatric orbital cellulitis with sub-periosteal abscess. Opthal Plast Reconstr Surg 21(5):363–6; discussion 366–367
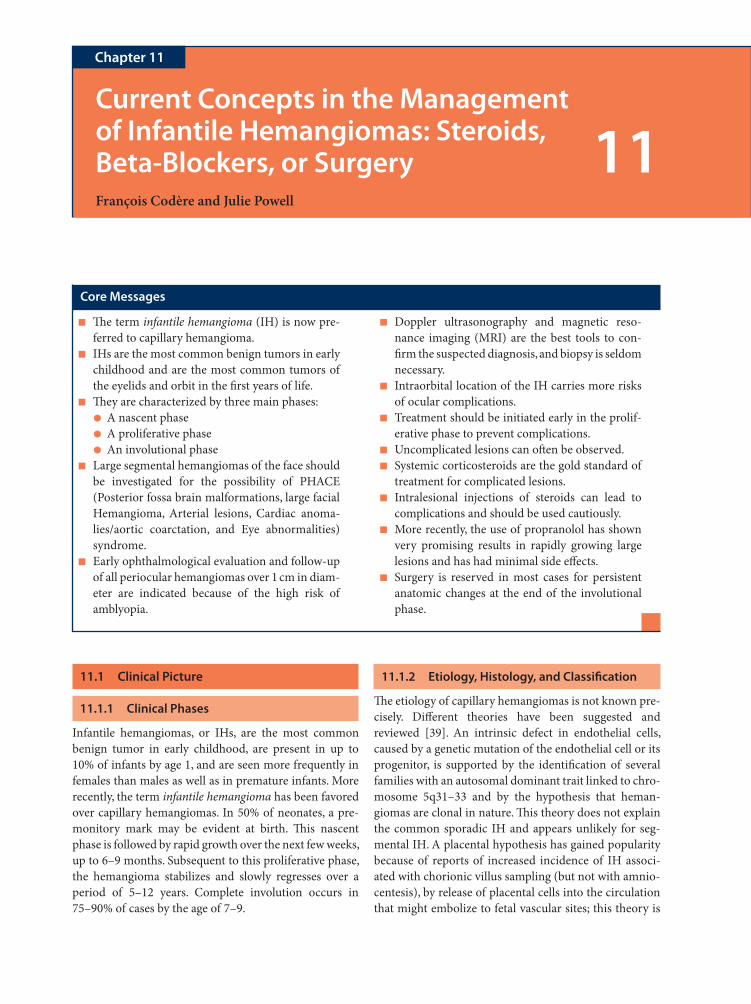
11.1 Clinical Picture
11.1.1 Clinical Phases
Infantile hemangiomas, or IHs, are the most common benign tumor in early childhood, are present in up to 10% of infants by age 1, and are seen more frequently in females than males as well as in premature infants. More recently, the term infantile hemangioma has been favored over capillary hemangiomas. In 50% of neonates, a pre-monitory mark may be evident at birth. Th is nascent phase is followed by rapid growth over the next few weeks, up to 6–9 months. Subsequent to this proliferative phase, the hemangioma stabilizes and slowly regresses over a period of 5–12 years. Complete involution occurs in 75–90% of cases by the age of 7–9.
11.1.2 Etiology, Histology, and Classifi cation
Th e etiology of capillary hemangiomas is not known pre-cisely. Diff erent theories have been suggested and reviewed [39]. An intrinsic defect in endothelial cells, caused by a genetic mutation of the endothelial cell or its progenitor, is supported by the identifi cation of several families with an autosomal dominant trait linked to chro-mosome 5q31–33 and by the hypothesis that heman-giomas are clonal in nature. Th is theory does not explain the common sporadic IH and appears unlikely for seg-mental IH. A placental hypothesis has gained popularity because of reports of increased incidence of IH associ-ated with chorionic villus sampling (but not with amnio-centesis), by release of placental cells into the circulation that might embolize to fetal vascular sites; this theory is
Current Concepts in the Management of Infantile Hemangiomas: Steroids, Beta-Blockers, or SurgeryFrançois Codère and Julie Powell
Chapter 11
11
Core Messages
Th e term ■ infantile hemangioma (IH) is now pre-ferred to capillary hemangioma.IHs are the most common benign tumors in early ■
childhood and are the most common tumors of the eyelids and orbit in the fi rst years of life.Th ey are characterized by three main phases: ■
A nascent phase ●
A proliferative phase ●
An involutional phase ●
Large segmental hemangiomas of the face should ■
be investigated for the possibility of PHACE (Posterior fossa brain malformations, large facial Hemangioma, Arterial lesions, Cardiac anoma-lies/aortic coarctation, and Eye abnormalities) syndrome.Early ophthalmological evaluation and follow-up ■
of all periocular hemangiomas over 1 cm in diam-eter are indicated because of the high risk of amblyopia.
Doppler ultrasonography and magnetic reso- ■
nance imaging (MRI) are the best tools to con-fi rm the suspected diagnosis, and biopsy is seldom necessary.Intraorbital location of the IH carries more risks ■
of ocular complications.Treatment should be initiated early in the prolif- ■
erative phase to prevent complications.Uncomplicated lesions can oft en be observed. ■
Systemic corticosteroids are the gold standard of ■
treatment for complicated lesions.Intralesional injections of steroids can lead to ■
complications and should be used cautiously.More recently, the use of propranolol has shown ■
very promising results in rapidly growing large lesions and has had minimal side eff ects.Surgery is reserved in most cases for persistent ■
anatomic changes at the end of the involutional phase.

162 11 Current Concepts in the Management of Infantile Hemangiomas
11
further supported by the demonstration that IH endothe-lium and placental vessels share expression of several surface markers (Glucon transporter 1 (GLUT1), merosin, Lewis Y, FcyRII) that are not found in other vascular tumors or malformations [39]. Evidence suggests that hypoxia has a possible role in the pathophysiology of IH via hypoxia-inducible factor 1a (HIF-1a), a major regu-lator of cellular response to hypoxia.
Histologically, in the proliferative phase, IHs are com-posed of lobules of plump, dividing endothelial cells lin-ing blood-fi lled vascular spaces; in the involutional phase, deposition of fi brofatty tissue occurs with resultant fi bro-sis and eventual involution. GLUT1, a glucose transporter also expressed by placental vessels and other blood–tissue barriers such as brain and retina but not normal skin, has been identifi ed as a specifi c marker for all stages of IH and can be useful in diff erentiating IHs from other vascu-lar tumors or malformations [34–36].
Periocular hemangiomas can be categorized accord-ing to their clinical appearance and their anatomic posi-tion. Th e reddish, classic superfi cial “strawberry lesion” or superfi cial IH involves the superfi cial dermis. Darker blue or purplish lesions correspond to a subcutaneous location, while deeper lesions without overlying skin color changes represent lesions located in the orbit oft en causing proptosis [7, 22, 40]. IHs can also be diff erenti-ated into focal versus segmental hemangiomas: A focal tumorlike IH appears to arise from a localized point, whereas segmental lesions are plaquelike and cover a ter-ritory corresponding to developmental segments [21]. Large segmental facial hemangiomas may well be the skin manifestation of PHACE syndrome, which is character-ized by posterior fossa brain malformations, large facial hemangioma, arterial lesions, cardiac anomalies/aortic coarctation, and eye abnormalities [17]. When sternal or other ventral developmental defects are present, it is referred to as PHACES syndrome. Th is represents a spec-trum of associated anomalies [31], with 70% of aff ected infants having only one extracutaneous manifestation. It is important to suspect this condition as it is associated with a high incidence of arterial and structural central nervous system anomalies with potential secondary neu-rologic sequelae. Th ese patients are at risk for progression of their neurovascular disease and should be investigated accordingly [17, 30]. Investigation for large segmental facial IHs should include MRI and magnetic resonance angiography (MRA) of the brain, echocardiogram, and ophthalmologic examination. Ocular anomalies, distinct from the visual complications of the hemangioma, asso-ciated with PHACE syndrome are microphthalmia, optic nerve hypoplasia, persistent fetal vasculature, and morn-ing glory disc anomaly.
11.1.3 Diff erential Diagnosis of Infantile Hemangioma
Th e IHs are vascular tumors characterized by a typical history of proliferative and involutional phases. Vascular malformations, such as a capillary malformation or port-wine stain, tend to remain stable and grow along with the growth of the child. Deeper orbital IHs without the char-acteristic superfi cial changes can be confused with other orbital lesions of childhood. Orbital lymphangiomas oft en have a history of acute increase in size due to intral-esional hemorrhage, followed by complete or partial res-olution over a period of days to months; recurrence of the bleeding can lead to multiple episodes of swelling, some-times resulting in fi brosis and involution. Plexiform neu-rofi bromas, if involving the superfi cial tissues, do not have the coloration changes typical of hemangiomas, and their progression, which can be rapid in childhood, is not followed by a phase of involution. Usually, other manifestations of neurofi bromatosis are present. Rhabdomyosarcoma is another lesion that has a tendency for rapid growth. It usually occurs later in childhood, with an average age of 7–8 years, but has to be ruled out when the color changes typical of hemangiomas cannot
Diff erential diagnosis of hemangioma of infancyOther vascular anomalies and tumors Capillary malformation Venous malformation Lymphatic malformation Arteriovenous malformation Non involuting congenital hemangioma (NICH) Rapidly involuting congenital hemangioma (RICH) Lobular capillary hemangioma (pyogenic granuloma) Tuft ed angioma Spindle cell hemangioendothelioma Kaposiform hemangioendotheliomaFibrosarcomaRhabdomyosarcomaMyofi bromatosis (including hemangiopericytoma)Nasal gliomaEncephaloceleLipoblastomaDermatofi brosarcoma protuberans (and giant cell
fi broblastoma)Neurofi broma
Modifi ed from Frieden IJ, Enjolras O, Esterly NB. Vascular birthmarks and other abnormalities of blood vessels and lym-phatics. In: Schachner LA, Hansen RC (eds) Pediatric dermatol-ogy, 3rd ed. Churchill Livingstone, London (in press). With permission

11.3 Investigation 163
be seen. Th e diagnosis of hemangioma can best be con-fi rmed by MRI with gadolinium contrast and Doppler ultrasound. But, in rare instances, when the diagnosis of a malignancy cannot be ruled out by imaging or when clinical evolution is atypical, a biopsy becomes manda-tory [9].
11.2 Ocular Complications
Th e most frequent ocular complications associated with IHs are related to amblyopia. Amblyopia is most oft en secondary to astigmatism but can also be due to strabis-mus or occlusion of the pupil. Risk factors for develop-ment of amblyopia are dependent on size and location. In a study of 129 patients by Schwartz et al., lesions measur-ing less than 1 cm in its greatest diameter were not associ-ated with amblyopia, while lesions of more than 1 cm induced amblyopia in 40 of 75 patients (53%). Fourteen of 18 patients (78%) with large diff use lesions had ambly-opia [12, 35].
Location of the lesion also plays a signifi cant role. In a study looking at the location of IHs, palpebral lesions induced amblyopia or astigmatism in 13 of 32 patients (40%). When the lesion was orbital with or without intra-conal involvement, these fi ndings were present in 27 of 31 patients (87%) [12]. Th e depth of the lesion also appears to be related to the length of the growth phase, with deeper lesion having a more prolonged period of growth. Lesions involving the lid, nasal location, involvement of the lid margin, or presence of a ptosis appear to have a higher incidence of amblyopia [40].
Hemangiomas can also cause strabismus either by a mass eff ect causing misalignment of the eye or by direct involvement of the extraocular muscles causing anoma-lies in the movement of the involved eye. In a series of 51 cases of hemangiomas of the eyelids, the most common complications were amblyopia (43%) and strabismus (33%). It was felt that milder forms of amblyopia in the
range of 6/12 to 6/30 were caused by anisometropia or strabismus [42]. In another study, strabismus was present in 15% of cases with eyelid or orbital lesions, but when large lesions part of PHACES syndrome were present, the strabismus incidence was much higher (71%). Visual loss can also be secondary to optic nerve involvement either by direct compression or by ischemic changes due to compression of the optic nerve supply. In rare cases, exposure and scarring of the corneal surface can also cause visual impairment and contribute to refractory amblyopia. Ulcerations are rare in the periocular areas; they typically occur in the proliferative phase and are more common in areas of mechanical trauma. Th ey can be painful and may become infected. Some degree of scarring occurs when they heal [8].
11.3 Investigation
When a periocular lesion is present and a threat for inter-ference with visual development is suspected, periodic ocular examinations are performed. Measures include visual acuity assessment, evaluation of lid fi ssures and movement, ocular alignment, and eye movements. Refraction with cycloplegia is performed. Th e lesion is measured, and photographs are taken for future compari-son. Initially, the ophthalmologic evaluation is repeated every 3–6 weeks.
Imaging is needed in cases of deep hemangiomas with normal overlying skin, cases of clinically atypical soft tis-sue masses, when the evaluation of extension of obvious hemangiomas is necessary, in cases of alarming heman-giomas, and for guiding therapy. Doppler ultrasonogra-phy is oft en the fi rst modality used to delineate and characterize vascular lesions. Its main advantages are its fl exibility, availability, cost, and ability to be repeated fre-quently over time [11]. Dubois and Garel defi ned the Doppler characteristics of hemangiomas as showing a variable echogenicity mass with increased color fl ow (Fig. 11.1).
Th e lesion displays high vessel density (>5 vessels/cm2) with a high Doppler shift (>2 kHz) and low resis-tance. Typically, there is little or no evidence of arterio-venous shunting (i.e., most veins within the lesion remain monophasic) [11]. From a previous study, they showed,
Summary for the Clinician
Knowing the three phases of the natural his- ■
tory of IH will help in the diagnosis and management.Large segmental IHs may point toward the diag- ■
nosis of PHACE(S) syndrome.In deep lesions, diagnosis must be confi rmed ■
either by imaging or more rarely by biopsy to rule out other potentially lethal lesions.
Summary for the Clinician
Amblyopia is the most important risk for the ■
patient with IH.
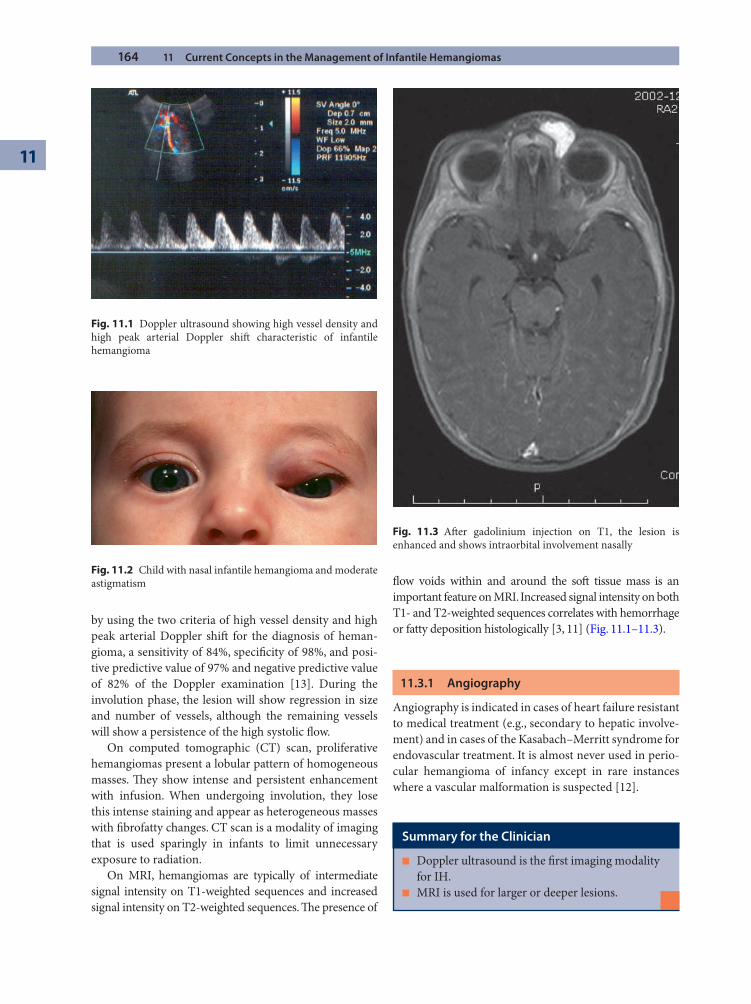
164 11 Current Concepts in the Management of Infantile Hemangiomas
11
by using the two criteria of high vessel density and high peak arterial Doppler shift for the diagnosis of heman-gioma, a sensitivity of 84%, specifi city of 98%, and posi-tive predictive value of 97% and negative predictive value of 82% of the Doppler examination [13]. During the involution phase, the lesion will show regression in size and number of vessels, although the remaining vessels will show a persistence of the high systolic fl ow.
On computed tomographic (CT) scan, proliferative hemangiomas present a lobular pattern of homogeneous masses. Th ey show intense and persistent enhancement with infusion. When undergoing involution, they lose this intense staining and appear as heterogeneous masses with fi brofatty changes. CT scan is a modality of imaging that is used sparingly in infants to limit unnecessary exposure to radiation.
On MRI, hemangiomas are typically of intermediate signal intensity on T1-weighted sequences and increased signal intensity on T2-weighted sequences. Th e presence of
fl ow voids within and around the soft tissue mass is an important feature on MRI. Increased signal intensity on both T1- and T2-weighted sequences correlates with hemorrhage or fatty deposition histologically [3, 11] (Fig. 11.1–11.3).
11.3.1 Angiography
Angiography is indicated in cases of heart failure resistant to medical treatment (e.g., secondary to hepatic involve-ment) and in cases of the Kasabach–Merritt syndrome for endovascular treatment. It is almost never used in perio-cular hemangioma of infancy except in rare instances where a vascular malformation is suspected [12].
Fig. 11.1 Doppler ultrasound showing high vessel density and high peak arterial Doppler shift characteristic of infantile hemangioma
Summary for the Clinician
Doppler ultrasound is the fi rst imaging modality ■
for IH.MRI is used for larger or deeper lesions. ■
Fig. 11.2 Child with nasal infantile hemangioma and moderate astigmatism
Fig. 11.3 Aft er gadolinium injection on T1, the lesion is enhanced and shows intraorbital involvement nasally
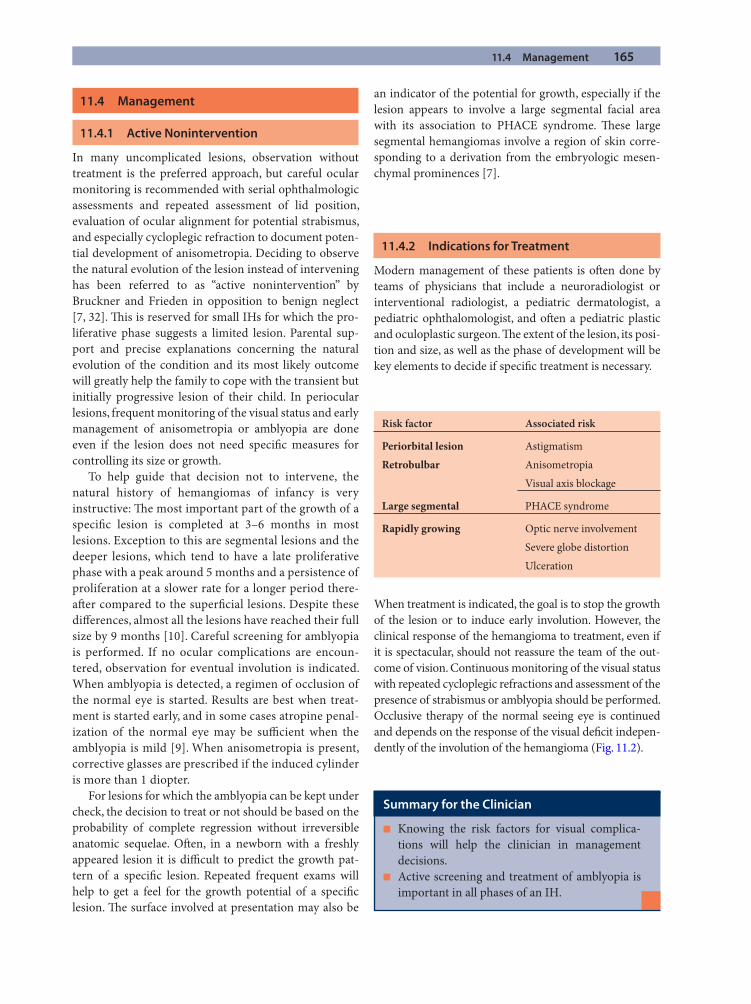
11.4 Management 165
11.4 Management
11.4.1 Active Nonintervention
In many uncomplicated lesions, observation without treatment is the preferred approach, but careful ocular monitoring is recommended with serial ophthalmologic assessments and repeated assessment of lid position, evaluation of ocular alignment for potential strabismus, and especially cycloplegic refraction to document poten-tial development of anisometropia. Deciding to observe the natural evolution of the lesion instead of intervening has been referred to as “active nonintervention” by Bruckner and Frieden in opposition to benign neglect [7, 32]. Th is is reserved for small IHs for which the pro-liferative phase suggests a limited lesion. Parental sup-port and precise explanations concerning the natural evolution of the condition and its most likely outcome will greatly help the family to cope with the transient but initially progressive lesion of their child. In periocular lesions, frequent monitoring of the visual status and early management of anisometropia or amblyopia are done even if the lesion does not need specifi c measures for controlling its size or growth.
To help guide that decision not to intervene, the natural history of hemangiomas of infancy is very instructive: Th e most important part of the growth of a specifi c lesion is completed at 3–6 months in most lesions. Exception to this are segmental lesions and the deeper lesions, which tend to have a late proliferative phase with a peak around 5 months and a persistence of proliferation at a slower rate for a longer period there-aft er compared to the superfi cial lesions. Despite these diff erences, almost all the lesions have reached their full size by 9 months [10]. Careful screening for amblyopia is performed. If no ocular complications are encoun-tered, observation for eventual involution is indicated. When amblyopia is detected, a regimen of occlusion of the normal eye is started. Results are best when treat-ment is started early, and in some cases atropine penal-ization of the normal eye may be suffi cient when the amblyopia is mild [9]. When anisometropia is present, corrective glasses are prescribed if the induced cylinder is more than 1 diopter.
For lesions for which the amblyopia can be kept under check, the decision to treat or not should be based on the probability of complete regression without irreversible anatomic sequelae. Oft en, in a newborn with a freshly appeared lesion it is diffi cult to predict the growth pat-tern of a specifi c lesion. Repeated frequent exams will help to get a feel for the growth potential of a specifi c lesion. Th e surface involved at presentation may also be
an indicator of the potential for growth, especially if the lesion appears to involve a large segmental facial area with its association to PHACE syndrome. Th ese large segmental hemangiomas involve a region of skin corre-sponding to a derivation from the embryologic mesen-chymal prominences [7].
11.4.2 Indications for Treatment
Modern management of these patients is oft en done by teams of physicians that include a neuroradiologist or interventional radiologist, a pediatric dermatologist, a pediatric ophthalomologist, and oft en a pediatric plastic and oculoplastic surgeon. Th e extent of the lesion, its posi-tion and size, as well as the phase of development will be key elements to decide if specifi c treatment is necessary.
Risk factor Associated risk
Periorbital lesion Astigmatism
Retrobulbar Anisometropia
Visual axis blockage
Large segmental PHACE syndrome
Rapidly growing Optic nerve involvement
Severe globe distortion
Ulceration
When treatment is indicated, the goal is to stop the growth of the lesion or to induce early involution. However, the clinical response of the hemangioma to treatment, even if it is spectacular, should not reassure the team of the out-come of vision. Continuous monitoring of the visual status with repeated cycloplegic refractions and assessment of the presence of strabismus or amblyopia should be performed. Occlusive therapy of the normal seeing eye is continued and depends on the response of the visual defi cit indepen-dently of the involution of the hemangioma (Fig. 11.2).
Summary for the Clinician
Knowing the risk factors for visual complica- ■
tions will help the clinician in management decisions.Active screening and treatment of amblyopia is ■
important in all phases of an IH.
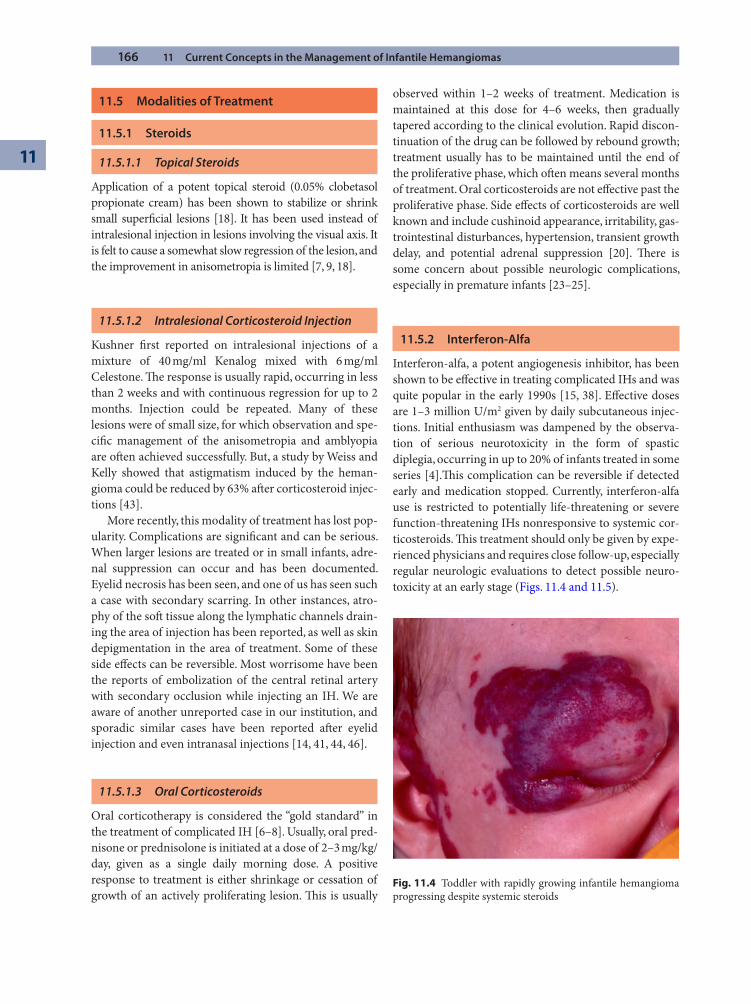
166 11 Current Concepts in the Management of Infantile Hemangiomas
11
11.5 Modalities of Treatment
11.5.1 Steroids
11.5.1.1 Topical Steroids
Application of a potent topical steroid (0.05% clobetasol propionate cream) has been shown to stabilize or shrink small superfi cial lesions [18]. It has been used instead of intralesional injection in lesions involving the visual axis. It is felt to cause a somewhat slow regression of the lesion, and the improvement in anisometropia is limited [7, 9, 18].
11.5.1.2 Intralesional Corticosteroid Injection
Kushner fi rst reported on intralesional injections of a mixture of 40 mg/ml Kenalog mixed with 6 mg/ml Celestone. Th e response is usually rapid, occurring in less than 2 weeks and with continuous regression for up to 2 months. Injection could be repeated. Many of these lesions were of small size, for which observation and spe-cifi c management of the anisometropia and amblyopia are oft en achieved successfully. But, a study by Weiss and Kelly showed that astigmatism induced by the heman-gioma could be reduced by 63% aft er corticosteroid injec-tions [43].
More recently, this modality of treatment has lost pop-ularity. Complications are signifi cant and can be serious. When larger lesions are treated or in small infants, adre-nal suppression can occur and has been documented. Eyelid necrosis has been seen, and one of us has seen such a case with secondary scarring. In other instances, atro-phy of the soft tissue along the lymphatic channels drain-ing the area of injection has been reported, as well as skin depigmentation in the area of treatment. Some of these side eff ects can be reversible. Most worrisome have been the reports of embolization of the central retinal artery with secondary occlusion while injecting an IH. We are aware of another unreported case in our institution, and sporadic similar cases have been reported aft er eyelid injection and even intranasal injections [14, 41, 44, 46].
11.5.1.3 Oral Corticosteroids
Oral corticotherapy is considered the “gold standard” in the treatment of complicated IH [6–8]. Usually, oral pred-nisone or prednisolone is initiated at a dose of 2–3 mg/kg/day, given as a single daily morning dose. A positive response to treatment is either shrinkage or cessation of growth of an actively proliferating lesion. Th is is usually
observed within 1–2 weeks of treatment. Medication is maintained at this dose for 4–6 weeks, then gradually tapered according to the clinical evolution. Rapid discon-tinuation of the drug can be followed by rebound growth; treatment usually has to be maintained until the end of the proliferative phase, which oft en means several months of treatment. Oral corticosteroids are not eff ective past the proliferative phase. Side eff ects of corticosteroids are well known and include cushinoid appearance, irritability, gas-trointestinal disturbances, hypertension, transient growth delay, and potential adrenal suppression [20]. Th ere is some concern about possible neurologic complications, especially in premature infants [23–25].
11.5.2 Interferon-Alfa
Interferon-alfa, a potent angiogenesis inhibitor, has been shown to be eff ective in treating complicated IHs and was quite popular in the early 1990s [15, 38]. Eff ective doses are 1–3 million U/m2 given by daily subcutaneous injec-tions. Initial enthusiasm was dampened by the observa-tion of serious neurotoxicity in the form of spastic diplegia, occurring in up to 20% of infants treated in some series [4].Th is complication can be reversible if detected early and medication stopped. Currently, interferon-alfa use is restricted to potentially life-threatening or severe function-threatening IHs nonresponsive to systemic cor-ticosteroids. Th is treatment should only be given by expe-rienced physicians and requires close follow-up, especially regular neurologic evaluations to detect possible neuro-toxicity at an early stage (Figs. 11.4 and 11.5).
Fig. 11.4 Toddler with rapidly growing infantile hemangioma progressing despite systemic steroids
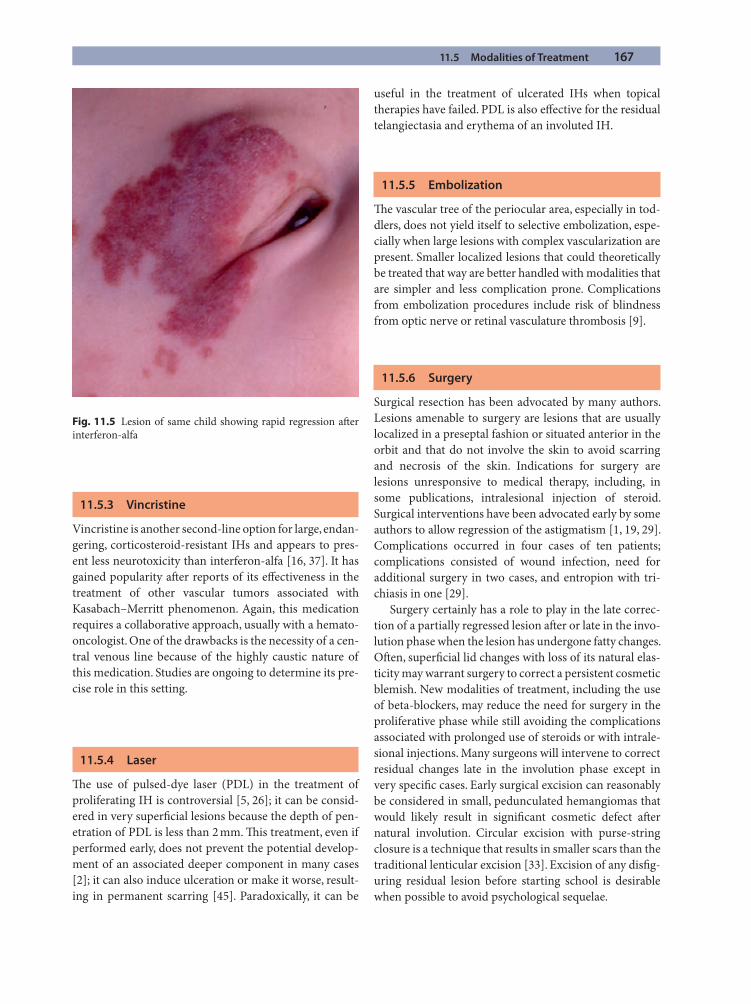
11.5 Modalities of Treatment 167
11.5.3 Vincristine
Vincristine is another second-line option for large, endan-gering, corticosteroid-resistant IHs and appears to pres-ent less neurotoxicity than interferon-alfa [16, 37]. It has gained popularity aft er reports of its eff ectiveness in the treatment of other vascular tumors associated with Kasabach–Merritt phenomenon. Again, this medication requires a collaborative approach, usually with a hemato-oncologist. One of the drawbacks is the necessity of a cen-tral venous line because of the highly caustic nature of this medication. Studies are ongoing to determine its pre-cise role in this setting.
11.5.4 Laser
Th e use of pulsed-dye laser (PDL) in the treatment of proliferating IH is controversial [5, 26]; it can be consid-ered in very superfi cial lesions because the depth of pen-etration of PDL is less than 2 mm. Th is treatment, even if performed early, does not prevent the potential develop-ment of an associated deeper component in many cases [2]; it can also induce ulceration or make it worse, result-ing in permanent scarring [45]. Paradoxically, it can be
useful in the treatment of ulcerated IHs when topical therapies have failed. PDL is also eff ective for the residual telangiectasia and erythema of an involuted IH.
11.5.5 Embolization
Th e vascular tree of the periocular area, especially in tod-dlers, does not yield itself to selective embolization, espe-cially when large lesions with complex vascularization are present. Smaller localized lesions that could theoretically be treated that way are better handled with modalities that are simpler and less complication prone. Complications from embolization procedures include risk of blindness from optic nerve or retinal vasculature thrombosis [9].
11.5.6 Surgery
Surgical resection has been advocated by many authors. Lesions amenable to surgery are lesions that are usually localized in a preseptal fashion or situated anterior in the orbit and that do not involve the skin to avoid scarring and necrosis of the skin. Indications for surgery are lesions unresponsive to medical therapy, including, in some publications, intralesional injection of steroid. Surgical interventions have been advocated early by some authors to allow regression of the astigmatism [1, 19, 29]. Complications occurred in four cases of ten patients; complications consisted of wound infection, need for additional surgery in two cases, and entropion with tri-chiasis in one [29].
Surgery certainly has a role to play in the late correc-tion of a partially regressed lesion aft er or late in the invo-lution phase when the lesion has undergone fatty changes. Oft en, superfi cial lid changes with loss of its natural elas-ticity may warrant surgery to correct a persistent cosmetic blemish. New modalities of treatment, including the use of beta-blockers, may reduce the need for surgery in the proliferative phase while still avoiding the complications associated with prolonged use of steroids or with intrale-sional injections. Many surgeons will intervene to correct residual changes late in the involution phase except in very specifi c cases. Early surgical excision can reasonably be considered in small, pedunculated hemangiomas that would likely result in signifi cant cosmetic defect aft er natural involution. Circular excision with purse-string closure is a technique that results in smaller scars than the traditional lenticular excision [33]. Excision of any disfi g-uring residual lesion before starting school is desirable when possible to avoid psychological sequelae.
Fig. 11.5 Lesion of same child showing rapid regression aft er interferon-alfa

168 11 Current Concepts in the Management of Infantile Hemangiomas
11
11.5.7 Beta-Blockers: A New Promising Modality of Treatment
A new treatment option has been proposed in the form of the nonselective beta-blocker propranolol [27]. Th is was discovered fortuitously, initially in corticosteroid-failure patients. Th e initial report of 11 infants with severe or dis-fi guring IH treated with propranolol at 2 mg/kg/day showed impressive results with minimal side eff ects. In all patients, 24 h aft er the initiation of treatment, a change in the color of the lesion was observed along with soft ening of the mass. In fi ve cases for which ultrasonography was done, an objective regression of the lesion was observed. Improvement leading to fl attening of the lesion was noted with continued treatment. Since this was published, many centers have started using this medication with various protocols, oft en initiating treatment in a hospital setting to monitor vital signs; in the outpatient setting, beginning medication at a lower dose (i.e., 0.5 mg/kg/day) and grad-ually increasing up to 2 mg/kg/day with close monitoring of blood pressure and pulse is another option. Th e optimal dosage and frequency of administration of propranolol for IH is still not well established, and additional studies
are necessary before this medication can be recommended on a widespread basis. At this time, this is still an off -label use. Contraindications include bronchospasm/asthma, congestive heart failure, bradycardia, or hypotension. Hypoglycemia can occur, especially in the very young infant. Th ere is concern that propranolol, because of its vasoconstrictive eff ect, could provoke complications in the setting of cerebrovascular anomalies in patients with PHACE syndrome; it is thus recommended to obtain an MRA in infants with facial segmental IHs to evaluate the cerebral arteries before considering this treatment option. Propranolol, however, appears to be an extremely promis-ing new treatment option with a better safety profi le than interferon-alfa or vincristine and potentially might become the fi rst-line treatment for complicated IHs. As with other systemic treatments for IHs, a multidisciplinary approach is optimal. Th e mechanism of action of propra-nolol in IHs is not well understood but may include vaso-constriction, explaining the very rapid color change and soft ening of the IH aft er initiating treatment; propranolol has also been shown to decrease the expression of VEGF and bFGF genes in vitro as well as to trigger apoptosis of capillary endothelial cells [28] (Figs. 11.6–11.11).
Fig. 11.6 Photograph of a toddler with continued growth of an IH despite systemic corticosteroids
Fig. 11.7 Necrosis of portion of the involved ear occurred despite initiation of steroids
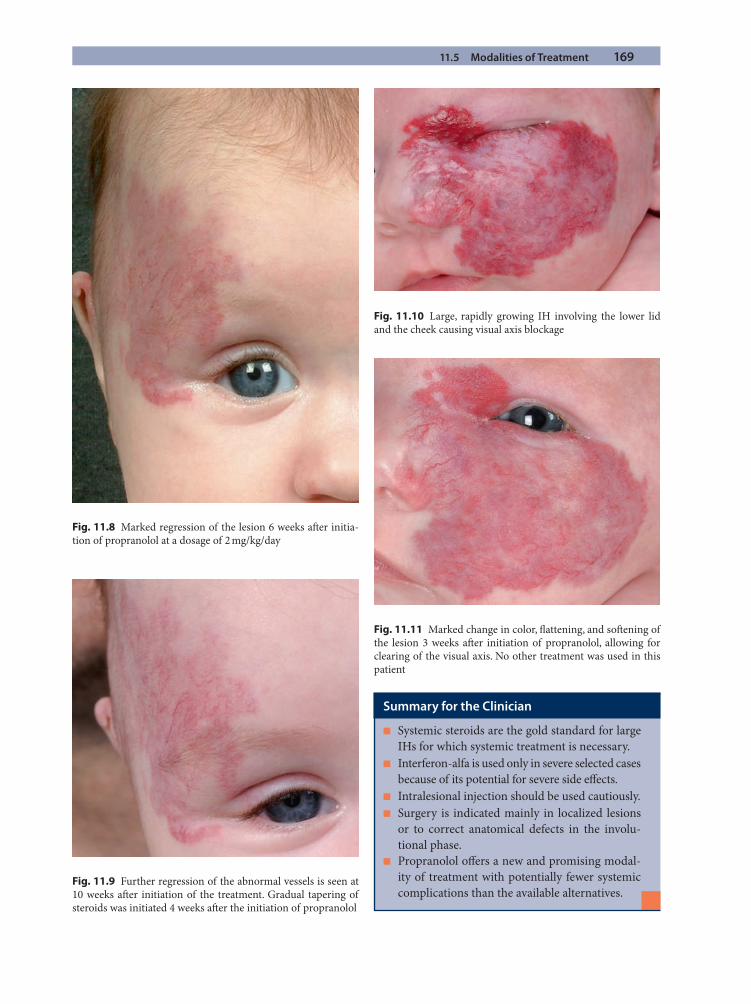
11.5 Modalities of Treatment 169
Fig. 11.8 Marked regression of the lesion 6 weeks aft er initia-tion of propranolol at a dosage of 2 mg/kg/day
Fig. 11.10 Large, rapidly growing IH involving the lower lid and the cheek causing visual axis blockage
Fig. 11.11 Marked change in color, fl attening, and soft ening of the lesion 3 weeks aft er initiation of propranolol, allowing for clearing of the visual axis. No other treatment was used in this patient
Summary for the Clinician
Systemic steroids are the gold standard for large ■
IHs for which systemic treatment is necessary.Interferon-alfa is used only in severe selected cases ■
because of its potential for severe side eff ects.Intralesional injection should be used cautiously. ■
Surgery is indicated mainly in localized lesions ■
or to correct anatomical defects in the involu-tional phase.Propranolol off ers a new and promising modal- ■
ity of treatment with potentially fewer systemic complications than the available alternatives.
Fig. 11.9 Further regression of the abnormal vessels is seen at 10 weeks aft er initiation of the treatment. Gradual tapering of steroids was initiated 4 weeks aft er the initiation of propranolol
170 11 Current Concepts in the Management of Infantile Hemangiomas
11
References
1. Aldave AJ, Shields CL, Shields JA (1999 Nov–Dec) Surgical excision of selected amblyogenic periorbital capillary hemangiomas. Ophthalmic Surg Lasers 30:754–757
2. Ashinoff R, Geronemus RG (1993 Mar) Failure of the fl ashlamp-pumped pulsed dye laser to prevent progression to deep hemangioma. Pediatr Dermatol 10:77–80
3. Baker LL, Dillon WP, Hieshima GB, Dowd CF, Frieden IJ (1993 Mar–Apr) Hemangiomas and vascular malforma-tions of the head and neck: MR characterization. AJNR Am J Neuroradiol 14:307–314
4. Barlow CF, Priebe CJ, Mulliken JB, Barnes PD, Mac Donald D, Folkman J, Ezekowitz RA (1998 Mar) Spastic diplegia as a complication of interferon alfa-2a treatment of heman-giomas of infancy. J Pediatr 132:527–530
5. Batta K, Goodyear HM, Moss C, Williams HC Hiller L, Waters R (2002 Aug 17) Randomised controlled study of early pulsed dye laser treatment of uncomplicated child-hood haemangiomas: results of a 1-year analysis. Lancet 360:521–527
6. Bennett ML, Fleischer AB, Jr., Chamlin SL, Frieden IJ (2001 Sept) Oral corticosteroid use is eff ective for cutane-ous hemangiomas: an evidence-based evaluation. Arch Dermatol 137:1208–1213
7. Bruckner AL, Frieden IJ (2003 Apr) Hemangiomas of infancy. J Am Acad Dermatol 48:477–493; quiz 494–476
8. Bruckner AL, Frieden IJ (2006 Oct) Infantile heman-giomas. J Am Acad Dermatol 55:671–682
9. Ceisler EJ, Santos L, Blei F (2004 Jan–Feb) Periocular hemangiomas: what every physician should know. Pediatr Dermatol 21:1–9
10. Chang LC, Haggstrom AN, Drolet BA, Baselga E, Chamlin SL, Garzon MC, Horii KA, Lucky AW, Mancini AJ, Metry DW, Nopper AJ, Frieden IJ (2008 Aug) Growth character-istics of infantile hemangiomas: implications for manage-ment. Pediatrics 122:360–367
11. Dubois J, Garel L (1999 Dec) Imaging and therapeutic approach of hemangiomas and vascular malformations in the pediatric age group. Pediatr Radiol 29:879–893
12. Dubois J, Milot J, Jaeger BI, McCuaig C, Rousseau E, Powell J (2006 Oct) Orbit and eyelid hemangiomas: is there a relationship between location and ocular problems?. J Am Acad Dermatol 55:614–619
13. Dubois J, Patriquin HB, Garel L, Powell J, Filiatrault D, David M, Grignon A (1998 July) Soft -tissue hemangiomas in infants and children: diagnosis using Doppler sonogra-phy. AJR Am J Roentgenol 171:247–252
14. Egbert JE, Paul S, Engel WK, Summers CG (2001 May) High injection pressure during intralesional injection of corticosteroids into capillary hemangiomas. Arch Oph-thalmol 119:677–683
15. Ezekowitz RA, Mulliken JB, Folkman J (1992 May 28) Interferon alfa-2a therapy for life-threatening heman-giomas of infancy. N Engl J Med 326:1456–1463
16. Fawcett SL, Grant I, Hall PN, Kelsall AW, Nicholson JC (2004 Mar) Vincristine as a treatment for a large haeman-gioma threatening vital functions. Br J Plast Surg 57: 168–171
17. Frieden IJ, Reese V, Cohen D (1996 Mar) PHACE syn-drome. Th e association of posterior fossa brain malforma-tions, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities. Arch Dermatol 132:307–311
18. Garzon MC, Lucky AW, Hawrot A, Frieden IJ (2006 Feb) Ultrapotent topical corticosteroid treatment of heman-giomas of infancy. J Am Acad Dermatol 52:281–286
19. Geh JL, Geh VS, Jemec B, Liasis A, Harper J, Nischal KK, Dunaway D (2007 Apr 15) Surgical treatment of periocular hemangiomas: a single-center experience. Plast Reconstr Surg 119:1553–1562
20. George ME, Sharma V, Jacobson J, Simon S, Nopper AJ (2004 Aug) Adverse eff ects of systemic glucocorticosteroid therapy in infants with hemangiomas. Arch Dermatol 140:963–969
21. Haggstrom AN, Lammer EJ, Schneider RA, Marcucio R, Frieden IJ (2006 Mar) Patterns of infantile hemangiomas: new clues to hemangioma pathogenesis and embryonic facial development. Pediatrics 117:698–703
22. Haik BG, Jakobiec FA, Ellsworth RM, Jones IS (1979 May) Capillary hemangioma of the lids and orbit: an analysis of the clinical features and therapeutic results in 101 cases. Ophthalmology 86:760–792
23. Halliday HL, Ehrenkranz RA, Doyle LW (2003) Delayed (>3 weeks) postnatal corticosteroids for chronic lung dis-ease in preterm infants. Cochrane Database Syst Rev 1:CD001145
24. Halliday HL, Ehrenkranz RA, Doyle LW (2003) Early post-natal (<96 hours) corticosteroids for preventing chronic lung disease in preterm infants. Cochrane Database Syst Rev 1:CD001146
25. Halliday HL, Ehrenkranz RA, Doyle LW (2003) Moderately early (7–14 days) postnatal corticosteroids for preventing chronic lung disease in preterm infants. Cochrane Database Syst Rev 1:CD001144
26. Kolde G (2003 Jan 25) Early pulsed-dye laser treatment of childhood haemangiomas. Lancet 361:348–349; author reply 349
27. Leaute-Labreze C, Dumas de la Roque E, Hubiche T, Boralevi F, Th ambo JB, Taieb A (2008 June 12) Propranolol for severe hemangiomas of infancy. N Engl J Med 358: 2649–2651
28. Leaute-Labreze C, Taieb A (2008 Dec) Effi cacy of beta-blockers in infantile capillary haemangiomas: the
References 171
physiopathological signifi cance and therapeutic conse-quences. Ann Dermatol Venereol 135:860–862
29. Levi M, Schwartz S, Blei F, Ceisler E, Steele M, Furlan L, Millman A, Kodsi SR (June 2007) Surgical treatment of capillary hemangiomas causing amblyopia. J AAPOS 11: 230–234
30. Metry DW, Dowd CF, Barkovich AJ, Frieden IJ (2001 July) Th e many faces of PHACE syndrome. J Pediatr 139: 117–123
31. Metry DW, Dowd CF, Barkovich AJ, Frieden IJ (2001 July) Th e many faces of PHACE syndrome. J Pediatr 139:117–123
32. Metry DW, Hebert AA (2000 July) Benign cutaneous vas-cular tumors of infancy: when to worry, what to do. Arch Dermatol 136:905–914
33. Mulliken JB, Rogers GF, Marler JJ (2002 Apr 15) Circular excision of hemangioma and purse-string closure: the smallest possible scar. Plast Reconstr Surg 109:1544–1554; discussion 1555
34. North PE, Mizeracki A, Mihm MC, Jr., Mrak RE (2000 May–June) GLUT1 immunoreaction patterns reliably dis-tinguish hemangioblastoma from metastatic renal cell car-cinoma. Clin Neuropathol 19:131–137
35. North PE, Waner M, Buckmiller L, James CA, Mihm MC Jr (2006 Nov–Dec) Vascular tumors of infancy and child-hood: beyond capillary hemangioma. Cardiovasc Pathol 15:303–317
36. North PE, Waner M, Mizeracki A, Mrak RE, Nicholas R, Kincannon J, Suen JY, Mihm MC, Jr (2001 May) A unique microvascular phenotype shared by juvenile hemangiomas and human placenta. Arch Dermatol 137:559–570
37. Perez J, Pardo J, Gomez C (2002) Vincristine—an eff ective treatment of corticoid-resistant life-threatening infantile hemangiomas. Acta Oncol 41:197–199
38. Ricketts RR, Hatley RM, Corden BJ, Sabio H, Howell CG (1994 June) Interferon-alpha-2a for the treatment of com-plex hemangiomas of infancy and childhood. Ann Surg 219:605–612; discussion 612–604
39. Ritter MR, Butschek RA, Friedlander M, Friedlander SF (2007) Pathogenesis of infantile haemangioma: new molecular and cellular insights. Expert Rev Mol Med 9:1–19
40. Schwartz SR, Blei F, Ceisler E, Steele M, Furlan L, Kodsi S (June 2006) Risk factors for amblyopia in children with capillary hemangiomas of the eyelids and orbit. J AAPOS 10:262–268
41. Shorr N, Seiff SR (1986 Apr) Central retinal artery occlu-sion associated with periocular corticosteroid injection for juvenile hemangioma. Ophthalmic Surg 17:229–231
42. Stigmar G, Crawford JS, Ward CM, Th omson HG (1978 June) Ophthalmic sequelae of infantile hemangiomas of the eyelids and orbit. Am J Ophthalmol 85:806–813
43. Weiss AH, Kelly JP (2008 Feb) Reappraisal of astigmatism induced by periocular capillary hemangioma and treat-ment with intralesional corticosteroid injection. Ophthal-mology 115:390–397.e391
44. Whiteman DW, Rosen DA, Pinkerton RM (1980 June) Retinal and choroidal microvascular embolism aft er intrana-sal corticosteroid injection. Am J Ophthalmol 89:851–853
45. Witman PM, Wagner AM, Scherer K, Waner M, Frieden IJ (2006 Feb) Complications following pulsed dye laser treat-ment of superfi cial hemangiomas. Lasers Surg Med 38: 116–123
46. Yagci A, Palamar M, Egrilmez S, Sahbazov C, Ozbek SS (2008 Jan–Feb) Anterior segment ischemia and retin-ochoroidal vascular occlusion aft er intralesional steroid injection. Ophthal Plast Reconstr Surg 24:55–57
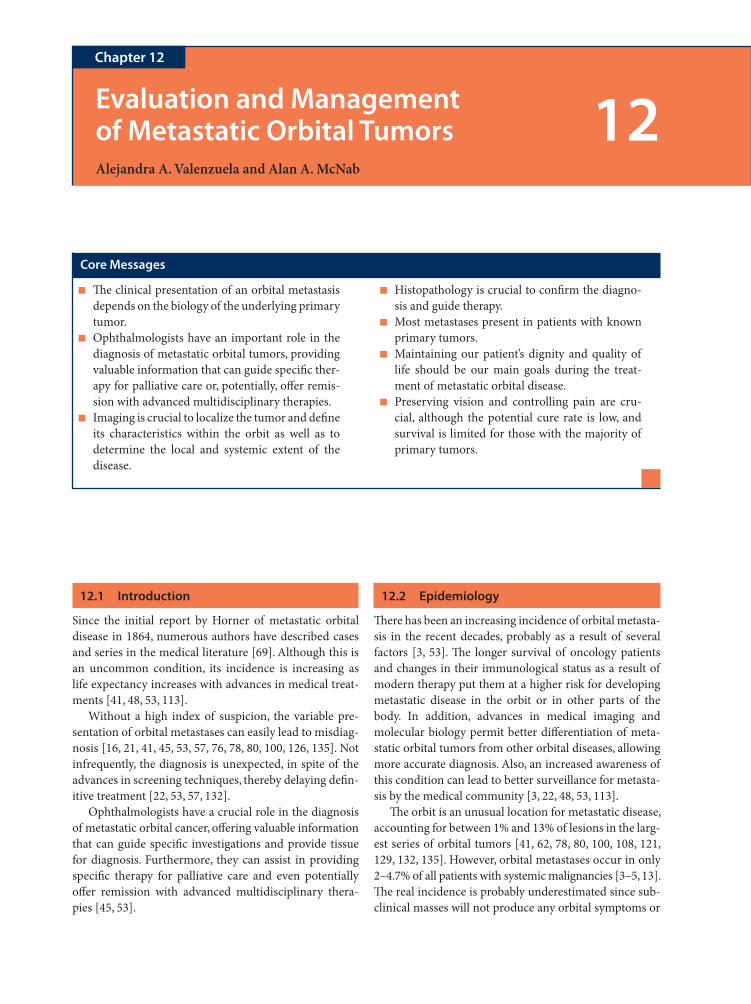
12.1 Introduction
Since the initial report by Horner of metastatic orbital disease in 1864, numerous authors have described cases and series in the medical literature [69]. Although this is an uncommon condition, its incidence is increasing as life expectancy increases with advances in medical treat-ments [41, 48, 53, 113].
Without a high index of suspicion, the variable pre-sentation of orbital metastases can easily lead to misdiag-nosis [16, 21, 41, 45, 53, 57, 76, 78, 80, 100, 126, 135]. Not infrequently, the diagnosis is unexpected, in spite of the advances in screening techniques, thereby delaying defi n-itive treatment [22, 53, 57, 132].
Ophthalmologists have a crucial role in the diagnosis of metastatic orbital cancer, off ering valuable information that can guide specifi c investigations and provide tissue for diagnosis. Furthermore, they can assist in providing specifi c therapy for palliative care and even potentially off er remission with advanced multidisciplinary thera-pies [45, 53].
12.2 Epidemiology
Th ere has been an increasing incidence of orbital metasta-sis in the recent decades, probably as a result of several factors [3, 53]. Th e longer survival of oncology patients and changes in their immunological status as a result of modern therapy put them at a higher risk for developing metastatic disease in the orbit or in other parts of the body. In addition, advances in medical imaging and molecular biology permit better diff erentiation of meta-static orbital tumors from other orbital diseases, allowing more accurate diagnosis. Also, an increased awareness of this condition can lead to better surveillance for metasta-sis by the medical community [3, 22, 48, 53, 113].
Th e orbit is an unusual location for metastatic disease, accounting for between 1% and 13% of lesions in the larg-est series of orbital tumors [41, 62, 78, 80, 100, 108, 121, 129, 132, 135]. However, orbital metastases occur in only 2–4.7% of all patients with systemic malignancies [3–5, 13]. Th e real incidence is probably underestimated since sub-clinical masses will not produce any orbital symptoms or
Evaluation and Management of Metastatic Orbital TumorsAlejandra A. Valenzuela and Alan A. McNab
Chapter 12
12
Core Messages
Th e clinical presentation of an orbital metastasis ■
depends on the biology of the underlying primary tumor.Ophthalmologists have an important role in the ■
diagnosis of metastatic orbital tumors, providing valuable information that can guide specifi c ther-apy for palliative care or, potentially, off er remis-sion with advanced multidisciplinary therapies.Imaging is crucial to localize the tumor and defi ne ■
its characteristics within the orbit as well as to determine the local and systemic extent of the disease.
Histopathology is crucial to confi rm the diagno- ■
sis and guide therapy.Most metastases present in patients with known ■
primary tumors.Maintaining our patient’s dignity and quality of ■
life should be our main goals during the treat-ment of metastatic orbital disease.Preserving vision and controlling pain are cru- ■
cial, although the potential cure rate is low, and survival is limited for those with the majority of primary tumors.
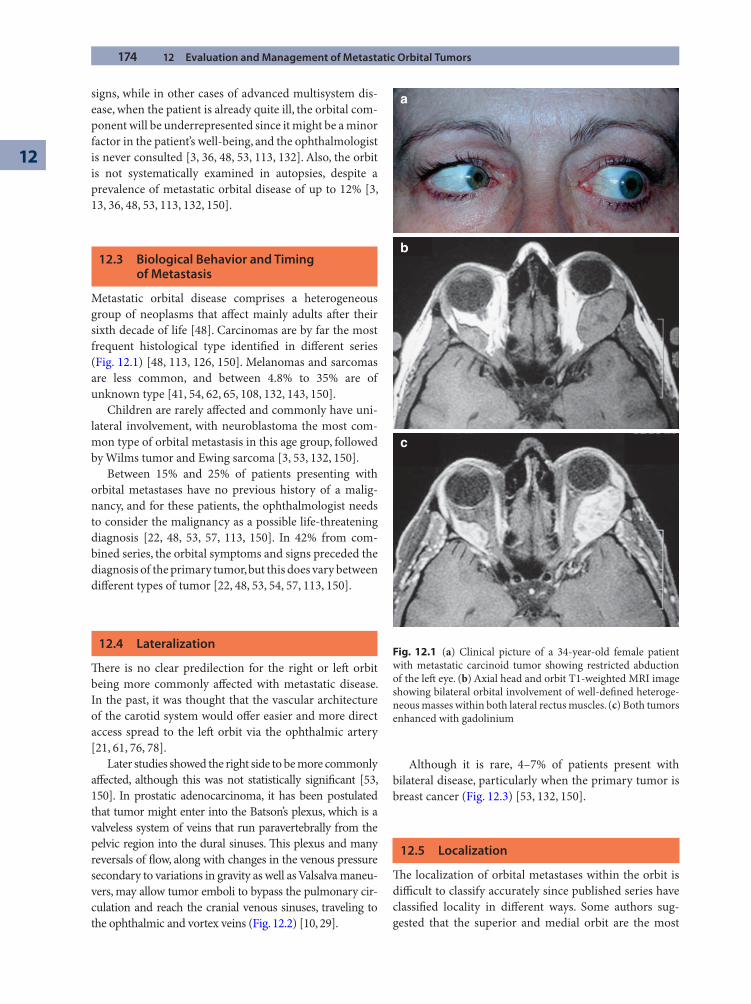
174 12 Evaluation and Management of Metastatic Orbital Tumors
12
signs, while in other cases of advanced multisystem dis-ease, when the patient is already quite ill, the orbital com-ponent will be underrepresented since it might be a minor factor in the patient’s well-being, and the ophthalmologist is never consulted [3, 36, 48, 53, 113, 132]. Also, the orbit is not systematically examined in autopsies, despite a prevalence of metastatic orbital disease of up to 12% [3, 13, 36, 48, 53, 113, 132, 150].
12.3 Biological Behavior and Timing of Metastasis
Metastatic orbital disease comprises a heterogeneous group of neoplasms that aff ect mainly adults aft er their sixth decade of life [48]. Carcinomas are by far the most frequent histological type identifi ed in diff erent series (Fig. 12.1) [48, 113, 126, 150]. Melanomas and sarcomas are less common, and between 4.8% to 35% are of unknown type [41, 54, 62, 65, 108, 132, 143, 150].
Children are rarely aff ected and commonly have uni-lateral involvement, with neuroblastoma the most com-mon type of orbital metastasis in this age group, followed by Wilms tumor and Ewing sarcoma [3, 53, 132, 150].
Between 15% and 25% of patients presenting with orbital metastases have no previous history of a malig-nancy, and for these patients, the ophthalmologist needs to consider the malignancy as a possible life-threatening diagnosis [22, 48, 53, 57, 113, 150]. In 42% from com-bined series, the orbital symptoms and signs preceded the diagnosis of the primary tumor, but this does vary between diff erent types of tumor [22, 48, 53, 54, 57, 113, 150].
12.4 Lateralization
Th ere is no clear predilection for the right or left orbit being more commonly aff ected with metastatic disease. In the past, it was thought that the vascular architecture of the carotid system would off er easier and more direct access spread to the left orbit via the ophthalmic artery [21, 61, 76, 78].
Later studies showed the right side to be more commonly aff ected, although this was not statistically signifi cant [53, 150]. In prostatic adenocarcinoma, it has been postulated that tumor might enter into the Batson’s plexus, which is a valveless system of veins that run paravertebrally from the pelvic region into the dural sinuses. Th is plexus and many reversals of fl ow, along with changes in the venous pressure secondary to variations in gravity as well as Valsalva maneu-vers, may allow tumor emboli to bypass the pulmonary cir-culation and reach the cranial venous sinuses, traveling to the ophthalmic and vortex veins (Fig. 12.2) [10, 29].
Although it is rare, 4–7% of patients present with bilateral disease, particularly when the primary tumor is breast cancer (Fig. 12.3) [53, 132, 150].
12.5 Localization
Th e localization of orbital metastases within the orbit is diffi cult to classify accurately since published series have classifi ed locality in diff erent ways. Some authors sug-gested that the superior and medial orbit are the most
a
b
c
Fig. 12.1 (a) Clinical picture of a 34-year-old female patient with metastatic carcinoid tumor showing restricted abduction of the left eye. (b) Axial head and orbit T1-weighted MRI image showing bilateral orbital involvement of well-defi ned heteroge-neous masses within both lateral rectus muscles. (c) Both tumors enhanced with gadolinium
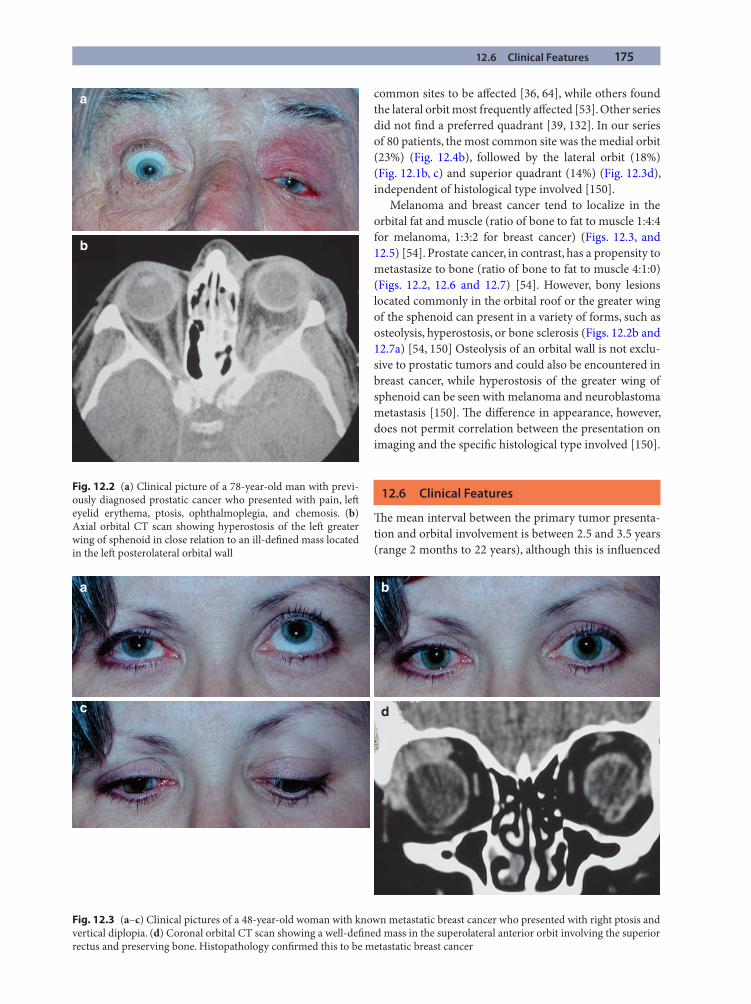
12.6 Clinical Features 175
a
b
Fig. 12.2 (a) Clinical picture of a 78-year-old man with previ-ously diagnosed prostatic cancer who presented with pain, left eyelid erythema, ptosis, ophthalmoplegia, and chemosis. (b) Axial orbital CT scan showing hyperostosis of the left greater wing of sphenoid in close relation to an ill-defi ned mass located in the left posterolateral orbital wall
a b
c d
Fig. 12.3 (a–c) Clinical pictures of a 48-year-old woman with known metastatic breast cancer who presented with right ptosis and vertical diplopia. (d) Coronal orbital CT scan showing a well-defi ned mass in the superolateral anterior orbit involving the superior rectus and preserving bone. Histopathology confi rmed this to be metastatic breast cancer
common sites to be aff ected [36, 64], while others found the lateral orbit most frequently aff ected [53]. Other series did not fi nd a preferred quadrant [39, 132]. In our series of 80 patients, the most common site was the medial orbit (23%) (Fig. 12.4b), followed by the lateral orbit (18%) (Fig. 12.1b, c) and superior quadrant (14%) (Fig. 12.3d), independent of histological type involved [150].
Melanoma and breast cancer tend to localize in the orbital fat and muscle (ratio of bone to fat to muscle 1:4:4 for melanoma, 1:3:2 for breast cancer) (Figs. 12.3, and 12.5) [54]. Prostate cancer, in contrast, has a propensity to metastasize to bone (ratio of bone to fat to muscle 4:1:0) (Figs. 12.2, 12.6 and 12.7) [54]. However, bony lesions located commonly in the orbital roof or the greater wing of the sphenoid can present in a variety of forms, such as osteolysis, hyperostosis, or bone sclerosis (Figs. 12.2b and 12.7a) [54, 150] Osteolysis of an orbital wall is not exclu-sive to prostatic tumors and could also be encountered in breast cancer, while hyperostosis of the greater wing of sphenoid can be seen with melanoma and neuroblastoma metastasis [150]. Th e diff erence in appearance, however, does not permit correlation between the presentation on imaging and the specifi c histological type involved [150].
12.6 Clinical Features
Th e mean interval between the primary tumor presenta-tion and orbital involvement is between 2.5 and 3.5 years (range 2 months to 22 years), although this is infl uenced
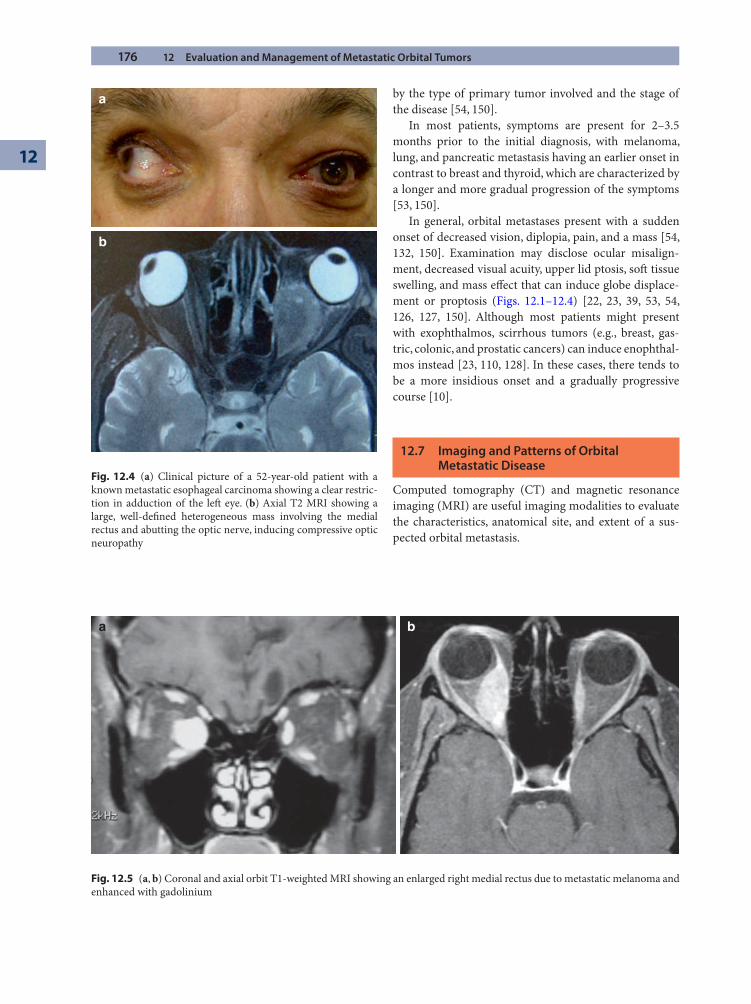
176 12 Evaluation and Management of Metastatic Orbital Tumors
12
a
b
Fig. 12.4 (a) Clinical picture of a 52-year-old patient with a known metastatic esophageal carcinoma showing a clear restric-tion in adduction of the left eye. (b) Axial T2 MRI showing a large, well-defi ned heterogeneous mass involving the medial rectus and abutting the optic nerve, inducing compressive optic neuropathy
a b
Fig. 12.5 (a, b) Coronal and axial orbit T1-weighted MRI showing an enlarged right medial rectus due to metastatic melanoma and enhanced with gadolinium
by the type of primary tumor involved and the stage of the disease [54, 150].
In most patients, symptoms are present for 2–3.5 months prior to the initial diagnosis, with melanoma, lung, and pancreatic metastasis having an earlier onset in contrast to breast and thyroid, which are characterized by a longer and more gradual progression of the symptoms [53, 150].
In general, orbital metastases present with a sudden onset of decreased vision, diplopia, pain, and a mass [54, 132, 150]. Examination may disclose ocular misalign-ment, decreased visual acuity, upper lid ptosis, soft tissue swelling, and mass eff ect that can induce globe displace-ment or proptosis (Figs. 12.1–12.4) [22, 23, 39, 53, 54, 126, 127, 150]. Although most patients might present with exophthalmos, scirrhous tumors (e.g., breast, gas-tric, colonic, and prostatic cancers) can induce enophthal-mos instead [23, 110, 128]. In these cases, there tends to be a more insidious onset and a gradually progressive course [10].
12.7 Imaging and Patterns of Orbital Metastatic Disease
Computed tomography (CT) and magnetic resonance imaging (MRI) are useful imaging modalities to evaluate the characteristics, anatomical site, and extent of a sus-pected orbital metastasis.
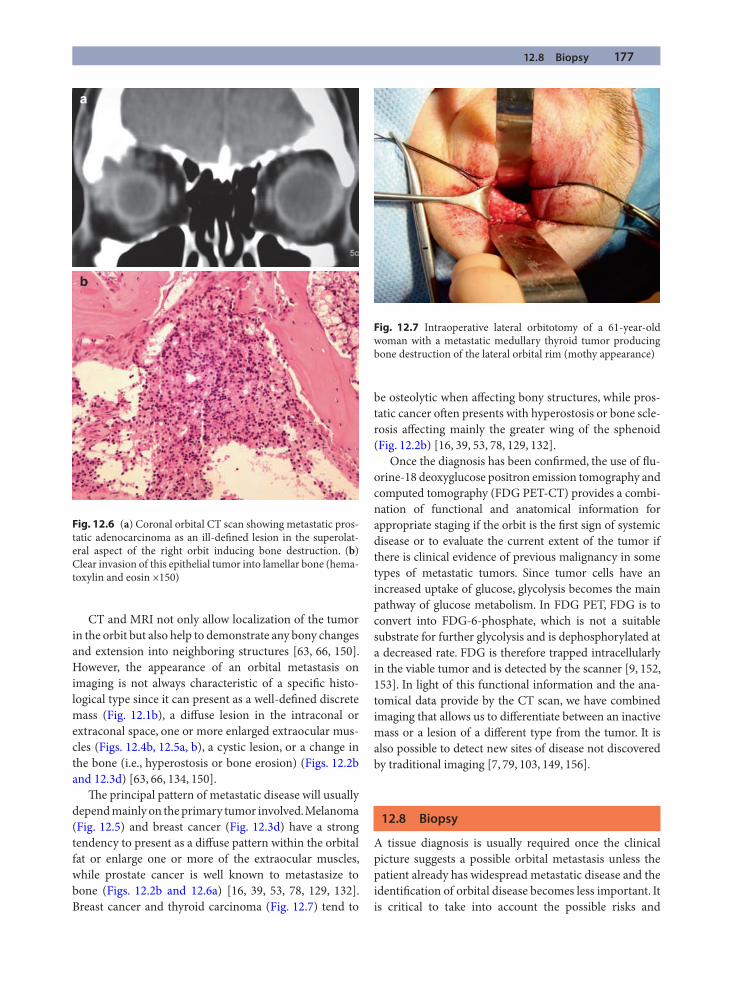
12.8 Biopsy 177
CT and MRI not only allow localization of the tumor in the orbit but also help to demonstrate any bony changes and extension into neighboring structures [63, 66, 150]. However, the appearance of an orbital metastasis on imaging is not always characteristic of a specifi c histo-logical type since it can present as a well-defi ned discrete mass (Fig. 12.1b), a diff use lesion in the intraconal or extraconal space, one or more enlarged extraocular mus-cles (Figs. 12.4b, 12.5a, b), a cystic lesion, or a change in the bone (i.e., hyperostosis or bone erosion) (Figs. 12.2b and 12.3d) [63, 66, 134, 150].
Th e principal pattern of metastatic disease will usually depend mainly on the primary tumor involved. Melanoma (Fig. 12.5) and breast cancer (Fig. 12.3d) have a strong tendency to present as a diff use pattern within the orbital fat or enlarge one or more of the extraocular muscles, while prostate cancer is well known to metastasize to bone (Figs. 12.2b and 12.6a) [16, 39, 53, 78, 129, 132]. Breast cancer and thyroid carcinoma (Fig. 12.7) tend to
be osteolytic when aff ecting bony structures, while pros-tatic cancer oft en presents with hyperostosis or bone scle-rosis aff ecting mainly the greater wing of the sphenoid (Fig. 12.2b) [16, 39, 53, 78, 129, 132].
Once the diagnosis has been confi rmed, the use of fl u-orine-18 deoxyglucose positron emission tomography and computed tomography (FDG PET-CT) provides a combi-nation of functional and anatomical information for appropriate staging if the orbit is the fi rst sign of systemic disease or to evaluate the current extent of the tumor if there is clinical evidence of previous malignancy in some types of metastatic tumors. Since tumor cells have an increased uptake of glucose, glycolysis becomes the main pathway of glucose metabolism. In FDG PET, FDG is to convert into FDG-6-phosphate, which is not a suitable substrate for further glycolysis and is dephosphorylated at a decreased rate. FDG is therefore trapped intracellularly in the viable tumor and is detected by the scanner [9, 152, 153]. In light of this functional information and the ana-tomical data provide by the CT scan, we have combined imaging that allows us to diff erentiate between an inactive mass or a lesion of a diff erent type from the tumor. It is also possible to detect new sites of disease not discovered by traditional imaging [7, 79, 103, 149, 156].
12.8 Biopsy
A tissue diagnosis is usually required once the clinical picture suggests a possible orbital metastasis unless the patient already has widespread metastatic disease and the identifi cation of orbital disease becomes less important. It is critical to take into account the possible risks and
a
b
Fig. 12.6 (a) Coronal orbital CT scan showing metastatic pros-tatic adenocarcinoma as an ill-defi ned lesion in the superolat-eral aspect of the right orbit inducing bone destruction. (b) Clear invasion of this epithelial tumor into lamellar bone (hema-toxylin and eosin ×150)
Fig. 12.7 Intraoperative lateral orbitotomy of a 61-year-old woman with a metastatic medullary thyroid tumor producing bone destruction of the lateral orbital rim (mothy appearance)
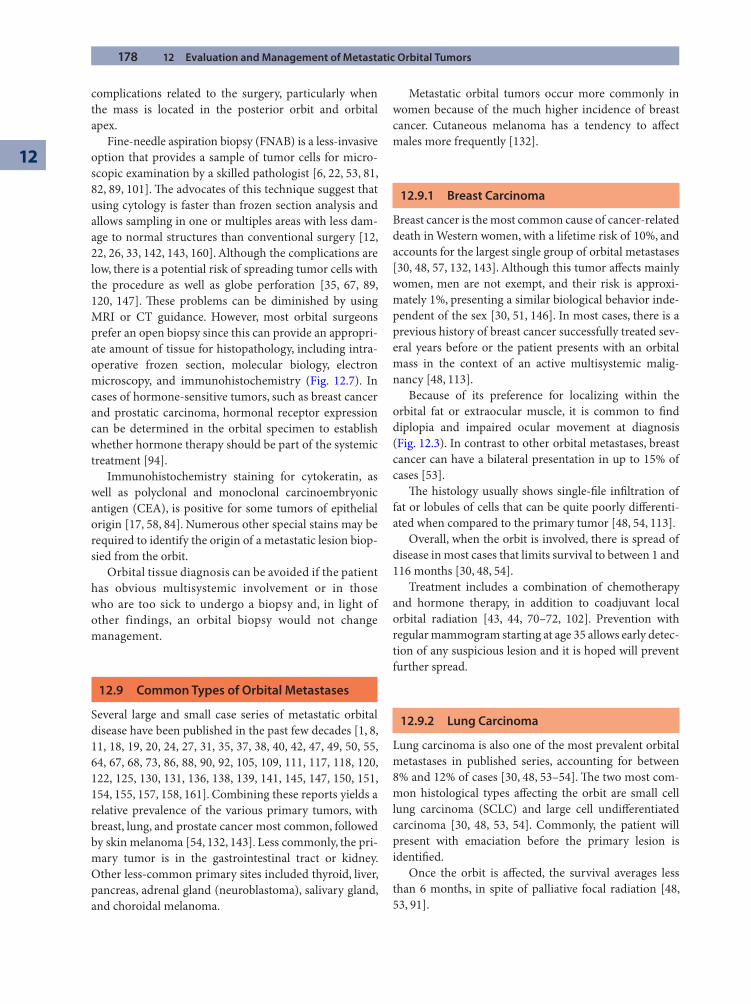
178 12 Evaluation and Management of Metastatic Orbital Tumors
12
complications related to the surgery, particularly when the mass is located in the posterior orbit and orbital apex.
Fine-needle aspiration biopsy (FNAB) is a less-invasive option that provides a sample of tumor cells for micro-scopic examination by a skilled pathologist [6, 22, 53, 81, 82, 89, 101]. Th e advocates of this technique suggest that using cytology is faster than frozen section analysis and allows sampling in one or multiples areas with less dam-age to normal structures than conventional surgery [12, 22, 26, 33, 142, 143, 160]. Although the complications are low, there is a potential risk of spreading tumor cells with the procedure as well as globe perforation [35, 67, 89, 120, 147]. Th ese problems can be diminished by using MRI or CT guidance. However, most orbital surgeons prefer an open biopsy since this can provide an appropri-ate amount of tissue for histopathology, including intra-operative frozen section, molecular biology, electron microscopy, and immunohistochemistry (Fig. 12.7). In cases of hormone-sensitive tumors, such as breast cancer and prostatic carcinoma, hormonal receptor expression can be determined in the orbital specimen to establish whether hormone therapy should be part of the systemic treatment [94].
Immunohistochemistry staining for cytokeratin, as well as polyclonal and monoclonal carcinoembryonic antigen (CEA), is positive for some tumors of epithelial origin [17, 58, 84]. Numerous other special stains may be required to identify the origin of a metastatic lesion biop-sied from the orbit.
Orbital tissue diagnosis can be avoided if the patient has obvious multisystemic involvement or in those who are too sick to undergo a biopsy and, in light of other findings, an orbital biopsy would not change management.
12.9 Common Types of Orbital Metastases
Several large and small case series of metastatic orbital disease have been published in the past few decades [1, 8, 11, 18, 19, 20, 24, 27, 31, 35, 37, 38, 40, 42, 47, 49, 50, 55, 64, 67, 68, 73, 86, 88, 90, 92, 105, 109, 111, 117, 118, 120, 122, 125, 130, 131, 136, 138, 139, 141, 145, 147, 150, 151, 154, 155, 157, 158, 161]. Combining these reports yields a relative prevalence of the various primary tumors, with breast, lung, and prostate cancer most common, followed by skin melanoma [54, 132, 143]. Less commonly, the pri-mary tumor is in the gastrointestinal tract or kidney. Other less-common primary sites included thyroid, liver, pancreas, adrenal gland (neuroblastoma), salivary gland, and choroidal melanoma.
Metastatic orbital tumors occur more commonly in women because of the much higher incidence of breast cancer. Cutaneous melanoma has a tendency to aff ect males more frequently [132].
12.9.1 Breast Carcinoma
Breast cancer is the most common cause of cancer-related death in Western women, with a lifetime risk of 10%, and accounts for the largest single group of orbital metastases [30, 48, 57, 132, 143]. Although this tumor aff ects mainly women, men are not exempt, and their risk is approxi-mately 1%, presenting a similar biological behavior inde-pendent of the sex [30, 51, 146]. In most cases, there is a previous history of breast cancer successfully treated sev-eral years before or the patient presents with an orbital mass in the context of an active multisystemic malig-nancy [48, 113].
Because of its preference for localizing within the orbital fat or extraocular muscle, it is common to fi nd diplopia and impaired ocular movement at diagnosis (Fig. 12.3). In contrast to other orbital metastases, breast cancer can have a bilateral presentation in up to 15% of cases [53].
Th e histology usually shows single-fi le infi ltration of fat or lobules of cells that can be quite poorly diff erenti-ated when compared to the primary tumor [48, 54, 113].
Overall, when the orbit is involved, there is spread of disease in most cases that limits survival to between 1 and 116 months [30, 48, 54].
Treatment includes a combination of chemotherapy and hormone therapy, in addition to coadjuvant local orbital radiation [43, 44, 70–72, 102]. Prevention with regular mammogram starting at age 35 allows early detec-tion of any suspicious lesion and it is hoped will prevent further spread.
12.9.2 Lung Carcinoma
Lung carcinoma is also one of the most prevalent orbital metastases in published series, accounting for between 8% and 12% of cases [30, 48, 53–54]. Th e two most com-mon histological types aff ecting the orbit are small cell lung carcinoma (SCLC) and large cell undiff erentiated carcinoma [30, 48, 53, 54]. Commonly, the patient will present with emaciation before the primary lesion is identifi ed.
Once the orbit is aff ected, the survival averages less than 6 months, in spite of palliative focal radiation [48, 53, 91].
12.9 Common Types of Orbital Metastases 179
Rarely, exenteration has been recommended as a last resort for pain management not responsive to medical treatment [3].
12.9.3 Prostatic Cancer
Prostatic cancer metastasizing to the orbit accounts for 3–10% of reported cases in larger series [14, 36, 48, 53, 54, 126]. Pain is a common feature encountered with this malignancy because of its tendency to involve orbital bone, most commonly inducing hyperostosis [16, 39, 53, 78, 129, 132, 150]. However, the presence of osteolytic lesions does not exclude this entity (Figs. 12.2 and 12.6) [56, 112]. Th e serum concentration of prostate-specifi c antigen (PSA) and acid phosphatase are usually high when there is metastatic disease.
Th e most common histological form is adenocarci-noma, which can show diff erent degrees of diff erentia-tion. Th e presence of neuroendocrine diff erentiation in prostatic carcinoma appears to correlate with poor prog-nosis [28].
Treatment strategies include local therapies such as external beam radiation and systemic treatments such as androgen deprivation, chemotherapy, and aminobispho-sphonates [14, 20, 53, 74]. Th e last have been shown to decrease the risk of bone metastasis in randomized clini-cal trials and prevent bone loss induced by androgen deprivation [25, 56].
12.9.4 Melanoma
Cutaneous melanoma represents 5.3–20% of all orbital metastases [53, 132, 150, 162]. Although rare, the choroid and mucous membrane can also be primary sites of dis-ease [15, 48].
As mentioned, metastatic melanoma tends to com-monly aff ect the extraocular muscles, inducing diplopia, proptosis, and globe displacement [53, 162]. Th is can also present as a multicystic mass with fl uid levels aff ecting one extraocular muscle, showing similarities to a venous–lymphatic anomaly (Figs. 12.5) [134].
Histologically, the tumor consists mainly of epithe-lioid cell types and not infrequently can be amelanotic. In these cases, immunohistochemistry and electron micros-copy help in diagnosis.
Melanoma can present with a long interval from the onset of the primary lesion to the fi rst sign of metastatic disease. However, once the orbit is aff ected, survival is limited, and the patient develops rapid progression inde-pendent of treatment [53, 115].
Th erapy is mainly palliative in cases of multisystem disease, and currently some clinical trials have been off ered to improve quality of life in those cases [2, 77, 87, 99, 107]. Surgery is not indicated except for cases of a localized orbital mass with no other site of metastasis and is done in conjunction with radiotherapy [3, 106, 133].
12.9.5 Carcinoid Tumor
Although carcinoid tumors are uncommon, they feature in all published series of orbital metastases, suggesting that the orbit is a preferential site of metastasis for this tumor. Th is malignancy arises from the Kulchitsky or enterochromaffi n cells and accounts for 4–5% of orbital metastases [53, 95, 98]. Th e majority of cases aff ecting the orbit originate in the gastrointestinal tract (ileum), but some also arise from the bronchi [95]. Females in the sixth decade are more commonly aff ected, and in most cases there is well-established systemic disease [53, 95, 98].
Th e tumor cells have the capability to secrete bioactive amines that can produce a variety of systemic symptoms and signs, including diarrhea, abdominal cramps, nausea, vomiting, paroxysmal facial fl ushing and other vasomotor disturbances, tachycardia, endocardial fi brosis, and asthma [119]. Th ese substances can be detected in the urine with elevated levels of 5-hydroxyindole acetic acid (5-HIAA). It should be remembered that a carcinoid tumor can occur with multiple endocrine neoplasia syndromes 1 and 2, von Hippel–Lindau syndrome, and neurofi bromatosis type 1. Synchronous or juxtaposed adenocarcinomas, especially colonic, may occur in 10–20% of patients with carcinoid tumors [97]. Ophthalmic manifestations of carcinoid syn-drome include conjunctival injection, lacrimation, soft tis-sue swelling, retinal artery spasm, and intravascular sludging as well as retinal pigment clumping (Figs. 12.1 and 12.7) [32].
Histologically, carcinoid tumors exhibit a characteris-tic nesting arrangement of tumor cells with abundant argentaffi n-positive granular cytoplasm [113, 124]. Immunohistochemistry frequently demonstrates reactiv-ity to chromogranin A, synaptophysin, serotonin, and serotonin markers [83, 159]. Flow cytometry has a pow-erful role, with both diagnostic and prognostic applica-tions. DNA aneuploidy has been shown to correlate with a poor clinical outcome [34, 46, 85]. Th e imaging modali-ties for staging include CT scan, PET, and indium-111–octreotide scan [95, 104, 123].
Treatment includes the surgical excision of isolated orbital metastases [39, 111]. Even in cases with wide-spread disease, the patients may also benefi t by reducing
180 12 Evaluation and Management of Metastatic Orbital Tumors
12
the amount of functioning carcinoid tumor [93]. Other authors advocate the use of systemic chemotherapy with adjuvant local radiation, and among patients with orbital metastases, carcinoid tumor patients have the highest survival rate, up to 15 years [39, 53, 93, 95, 98, 111, 114].
12.10 Diff erential Diagnosis
Th e past medical history of a cancer should be always questioned since many patients do not spontaneously disclose this information. It is important to remember that metastatic orbital disease will have a rapid onset of symptoms, and the presence of pain is helpful in diff er-entiating it from benign lesions such as nonspecifi c orbital infl ammation or lymphoproliferative ocular adn-exal disease.
Once a detailed clinical history has been obtained, with a meticulous examination and good imaging stud-ies, the possible diff erential diagnosis can be narrowed to a few possibilities.
When an orbital metastasis aff ects one extraocular muscle without other orbital involvement, the diff erential diagnosis includes thyroid-related orbitopathy, myositis, lymphoproliferative disease, arteriovenous malforma-tion, venous–lymphatic anomalies, carotid cavernous fi s-tula, amyloid deposits, and parasites [116, 137, 148].
Bone destruction can also be found in other entities, such as Langerhans cell histiocytosis, leukocytoclastic vasculitis, and lymphoproliferative disease [140].
For those patients who present with cirrhotic orbital metastases, the possibility of an early Parry-Romberg syndrome (essential facial hemiatrophy) should be ruled out since both might present with restricted ocular motil-ity, resistance to retropulsion, and enophthalmos. However, as Parry-Romberg syndrome progresses, patients will develop the characteristic regional atrophy (so-called linear scleroderma) of the diff erent facial tis-sues [110].
Some patients with metastatic deposits in the orbit may exhibit infl ammatory features due to tissue necrosis or bleeding. Th e diff erential diagnosis will therefore include nonspecifi c idiopathic orbital infl ammation, cel-lulitis, and Graves disease.
12.11 Treatment
Once the diagnosis of metastatic orbital disease has been established, a prompt referral to a medical and radiation oncologist is mandatory to decide the appropriate treat-ment in each case. Th e biological behavior of the primary
tumor, the degree of systemic involvement, and the change in survival if treatment is off ered must all be considered.
Although we have tried to highlight the diff erences between the most common orbital metastases, in general the treatment options will include chemotherapy, radio-therapy, immunotherapy, hormone therapy, surgical deb-ulking/excision, and combinations of all or some of these. Because of the wide variety of primary tumor types, the variation in extent of disease, and the treatment options available, treatment considerations for patients with orbital metastases must be individualized.
In this regard, it is particularly important to consider carefully the impact of any treatment on the patient’s quality of life and life expectancy.
12.11.1 Radiotherapy
Th e radiotherapy modality of treatment aims to deliver between 18 and 40 Gy in 10–15 fractions, combining anterior and lateral fi elds of irradiation to the orbit over a 3- to 5-week period. Reduction in mass eff ect and pain and even improvement in vision have been reported in several series [52, 59, 60, 75, 150]. In patients with orbital metastases for whom a longer survival is expected, the ophthalmologist needs to be aware of the potential long-term side eff ects related to this therapy.
12.11.2 Chemotherapy
Chemotherapy can be used alone or in combination with other treatments [150]. SCLC and neuroblastoma are particularly chemosensitive [54].
12.11.3 Hormonal Therapy
Prostatic and breast carcinoma are classical examples of tumors that may be responsive to therapeutic hormonal manipulation, particularly if they are fairly well diff eren-tiated [54].
In patients with metastatic prostate cancer, the use of diethylstilbestrol (DES), with or without orchidectomy, and specifi c luteinizing hormone-releasing hormone (LHRH) agonists, off ers excellent hormonal control in most cases [14, 20, 74, 113]. Th e latter reduce the feminiz-ing side eff ects but do not improve the survival or pallia-tion when compared to DES or orchidectomy [74]. LHRH agonists are associated with an initial testosterone surge and several weeks of tumor growth. Th is contraindicates
References 181
their use in compressive spinal cord lesions; as an anal-ogy, similarly they are not recommended for prostatic metastases located in the orbital apex [14, 20, 74, 113].
12.11.4 Surgery
Except for exceptional cases of carcinoid and renal cell tumors, surgery is mainly used for diagnostic, rather than therapeutic, purposes since the disease is usually already widespread [39, 59, 75, 111]. Surgery may also have a pal-liative benefi t in those cases in which other treatments have failed.
12.12 Prognosis and Survival
Th e overall survival of patients with orbital metastases is generally limited to less than a year [39, 45, 53, 64, 126]. A specifi c prognosis is diffi cult to obtain given the diver-sity of primary malignancies. In general, the outcome is poor, although multidisciplinary therapy can be pallia-tive, sometimes inducing remissions and even obtaining cures in some exceptional cases [3].
Metastatic breast carcinoma and carcinoid tumors are typically diagnosed long before the patient consults an oph-thalmologist, and survival is oft en measured in years [54]. Th yroid carcinoma also has a longer survival, but its initial diagnosis can be challenging [64, 68]. Isolated cases of meta-static renal cell carcinoma managed surgically have a 5-year
survival rate of up to 35%, and cures have been reported [96, 144]. Cutaneous melanoma can have a long latency, up to 46 years [115]. However, once the orbit is involved, the disease progresses rapidly, with a very short life expectancy [53]. Lung cancer has usually a fulminant course, and the survival is commonly less than 6 months [53].
In our series of 80 cases, melanoma also tended to present in a younger age group (mean 54 years) when compared with breast cancer (mean 62 years), carcinoid tumor (mean 63 years), and prostate cancer (mean 70 years) (p < .005) [150].
References
1. Abramson DH, Servodidio CA (1997) Metastatic choroi-dal melanoma to the contralateral orbit 40 years aft er enu-cleation. Arch Ophthalmol. 115(1):134
2. Agarwala SS, Kirkwood JM (1999) Melanoma: immuno-therapeutic approaches. BioDrugs 12(3):193–208
3. Ahmad SM, Esmaeli B (2007) Metastatic tumors of the orbit and ocular adnexa. Curr Opin Ophthalmol 18(5): 405–413
4. Albert DM, Rubenstein RA, Scheie HG (1967) Tumor metastasis to the eye. I. Incidence in 213 adult patients with generalized malignancy. Am J Ophthalmol 63(4):723–726
5. Albert DM, Rubenstein RA, Scheie HG (1967) Tumor metastasis to the eye. II. Clinical study in infants and chil-dren. Am J Ophthalmol 63(4):727–732
6. Arora R, Rewari R, Betharia SM (1992) Fine needle aspira-tion cytology of orbital and adnexal masses. Acta Cytol 36(4):483–491
7. Baek CH, Chung MK, Jeong HS, Son YI, Choi J, Kim YD, et al (2009) Th e clinical usefulness of (18)F-FDG PET/CT for the evaluation of lymph node metastasis in periorbital malignancies. Korean J Radiol 10(1):1–7
8. Ballinger WH Jr., Wesley RE (1984) Seminoma metastatic to the orbit. Ophthalmic Surg 15(2):120–121
9. Bar-Shalom R, Valdivia AY, Blaufox MD (2000) PET imag-ing in oncology. Semin Nucl Med 30(3):150–185
10. Baston O (1940) Th e function of the vertebral veins and their role in spread of metastasis. Ann Surg 112:138–149
11. Bernstein-Lipschitz L, Lahav M, Chen V, Gutman I, Gal R, Lipschitz M (1990) Metastatic thyroid carcinoma mas-querading as lacrimal gland tumor. Graefes Arch Clin Exp Ophthalmol 228(2):112–115
12. Berquist TH, Bailey PB, Cortese DA, Miller WE (1980) Transthoracic needle biopsy: accuracy and complications in relation to location and type of lesion. Mayo Clin Proc 55(8):475–481
13. Bloch RS, Gartner S (1971) Th e incidence of ocular meta-static carcinoma. Arch Ophthalmol 85(6):673–675
Summary for the Clinician
Metastatic orbital disease includes a heteroge- ■
neous group of neoplasms with presentation that varies depending on the extent of the disease and the biology of the primary tumor.A complete past medical history, a high index of ■
suspicion, and the rapid progression of the symptoms are key in the diagnosis.Strabismus, globe displacement, and pain are ■
common features of this entity.Investigations include appropriate orbital and ■
systemic imaging, with histologic studies on orbital tissue in most cases.A multidisciplinary approach is essential for ■
adequate management in an attempt to preserve vision, relieve pain, and improve the quality of life. Improved survival, and even cure in some cases, may be achieved.
182 12 Evaluation and Management of Metastatic Orbital Tumors
12
14. Boldt HC, Nerad JA (1988) Orbital metastases from pros-tate carcinoma. Arch Ophthalmol 106(10):1403–1408
15. Bowling BS, Damato BE, Foy PM (1994) Choroidal mela-noma metastatic to the contralateral orbit: implications for patient management. Eye 8:(Pt 1):144–145
16. Bullock JD, Yanes B (1980) Metastatic tumors of the orbit. Ann Ophthalmol 12(12):1392–1394
17. Bullock JD, Yanes B (1980) Ophthalmic manifestations of metastatic breast cancer. Ophthalmology 87(10):961–973
18. Bullock JD, Straughen WJ (1981) Carcinoma of the com-mon bile duct metastatic to the orbit. Ann Ophthalmol 13(5):619–621
19. Burch FE (1932) Orbital metastases from malignant tumors of the suprerenal gland. Arch Ophthalmol 7:418–433
20. Carriere VM, Karcioglu ZA, Apple DJ, Insler MS (1982) A case of prostate carcinoma with bilateral orbital metastases and the review of the literature. Ophthalmology 89(4): 402–406
21. Castro PA, Albert DM, Wang WJ, Ni C (1982) Tumors metastatic to the eye and adnexa. Int Ophthalmol Clin 22(3):189–223
22. Char DH, Miller T, Kroll S (1997) Orbital metastases: diag-nosis and course. Br J Ophthalmol 81(5):386–390
23. Cline RA, Rootman J (1984) Enophthalmos: a clinical review. Ophthalmology 91(3):229–237
24. Collins MJ, Wojno TH, Grossniklaus HE (1999) Metastatic esophageal carcinoma to the orbit. Am J Ophthalmol 127(2):228–229
25. Colombel M (2008) Prescription of bisphosphonates in prostate cancer. Prog Urol 18(1 Suppl FMC):F5–7
26. Czerniak B, Woyke S, Daniel B, Krzysztolik Z, Koss LG (1984) Diagnosis of orbital tumors by aspiration biopsy guided by computerized tomography. Cancer 54(11):2385–2389
27. Denby P, Harvey L, English MG (1986) Solitary metastasis from an occult renal cell carcinoma presenting as a pri-mary lacrimal gland tumor. Orbit (5):21–24
28. di Sant’Agnese PA (1992) Neuroendocrine diff erentiation in carcinoma of the prostate. Diagnostic, prognostic, and therapeutic implications. Cancer 70(1 Suppl):254–268
29. Dieckert JP, Berger BB (1982) Prostatic carcinoma meta-static to choroid. Br J Ophthalmol 66(4):234–239
30. Dieing A, Schulz CO, Schmid P, Roever AC, Lehenbauer-Dehm S, Jehn C, et al (2004) Orbital metastases in breast cancer: report of two cases and review of the literature. J Cancer Res Clin Oncol 130(12):745–748
31. Divine RD, Anderson RL, Ossoinig KC (1982) Metastatic carcinoid unresponsive to radiation therapy presenting as a lacrimal fossa mass. Ophthalmology 89(5):516–520
32. Divine RD, Anderson RL (1982) Metastatic small cell car-cinoma masquerading as orbital myositis. Ophthalmic Surg 13(6):483–487
33. Dresner SC, Kennerdell JS, Dekker A (1983) Fine needle aspiration biopsy of metastatic orbital tumors. Surv Ophthalmol 27(6):397–398
34. Ewers SB, Langstrom E, Baldetorp B, Killander D (1984) Flow-cytometric DNA analysis in primary breast carcino-mas and clinicopathological correlations. Cytometry 5(4): 408–419
35. Fan JT, Buettner H, Bartley GB, Bolling JP (1995) Clinical features and treatment of seven patients with carcinoid tumor metastatic to the eye and orbit. Am J Ophthalmol 119(2):211–218
36. Ferry AP (1978) Tumors metastatic to the eye and ocular adnexa. In: Jakobiec FA (ed) Ocular and adnexal tumors. Aesculapius, Birmingham, pp 862–892
37. Fezza J, Sinard J (1997) Metastatic liposarcoma to the orbit. Am J Ophthalmol 123(2):271–272
38. Font RL, Naumann G, Zimmerman LE (1964) Primary malignant melanoma of the skin metastatic to the eye and orbit. Am J Ophthalmol 63:738–754
39. Font RL, Ferry AP (1976) Carcinoma metastatic to the eye and orbit III. A clinicopathologic study of 28 cases meta-static to the orbit. Cancer 38(3):1326–1335
40. Font RL, Maturi RK, Small RG, Garcia-Rojas M (1998) Hepatocellular carcinoma metastatic to the orbit. Arch Ophthalmol 116(7):942–945
41. Forrest AW (1949) Intraorbital tumors. Arch Ophthal 41(2):198–232
42. Fred W, VG C (1993) Gastric carcinoma metastases to extraoculant muscles. J Comput Assist Tomogr 17:499–500
43. Frederiksen PL, Engelholm A, Mouridsen HT (1978) Treatment of drug-resistant metastasizing cancer of the breast with an antiestrogen. Ugeskr Laeger 140(43):2639–2641
44. Frederiksen PL, Joergensen ST, Roesdahl K, Th omsen J, Mouridsen HT (1978) Activity of adriamycin in metastatic breast cancer resistant to a combination regimen with cyclophosphamide, methotrexate, 5-fl uorouracil, vincris-tine, and prednisone. Cancer Treat Rep 62(3):449–450
45. Freedman MI, Folk JC (1987) Metastatic tumors to the eye and orbit. Patient survival and clinical characteristics. Arch Ophthalmol 105(9):1215–1219
46. Friedlander ML, Hedley DW, Taylor IW, Russell P, Coates AS, Tattersall MH (1984) Infl uence of cellular DNA con-tent on survival in advanced ovarian cancer. Cancer Res 44(1):397–400
47. Garcia GH, Weinberg DA, Glasgow BJ, Hunt KE, Venegas R, Goldberg RA (1998) Carcinoma of the male breast met-astatic to both orbits. Ophthal Plast Reconstr Surg 14(2):130–133
48. Garrity JA, Henderson JW, Cameron JD (2007) Metastatic carcinomas. In: Garrity JA, Henderson JW, Cameron JD, Henderson’s orbital tumors, 4th ed. Raven Press, New York, pp 313–326
49. Geetha N, Chandralekha B, Kumar A, Ittiyavirah AK, Ramadas K, Joseph F (1998) Carcinoma of the pancreas presenting as an orbital tumor: a case report. Am J Clin Oncol 21(5):532–533
References 183
50. Giordano GG (1995) Orbital metastasis from a urachal tumor. Arch Ophthalmol 113(4):413–415
51. Giordano SH, Buzdar AU, Hortobagyi GN (2002) Breast cancer in men. Ann Intern Med 137(8):678–687
52. Glassburn JR, Klionsky M, Brady LW (1984) Radiation therapy for metastatic disease involving the orbit. Am J Clin Oncol 7(2):145–148
53. Goldberg RA, Rootman J, Cline RA (1990) Tumors meta-static to the orbit: a changing picture. Surv Ophthalmol 35(1):1–24
54. Goldberg RA, Rootman J (1990) Clinical characteristics of metastatic orbital tumors. Ophthalmology 97(5):620–624
55. Goldberg SH, Kennedy RE, Metz HS, Searl SS, Rose SJ (1990) Strabismus caused by melanoma metastatic to an extraocular muscle. Ann Ophthalmol 22(12):467–471
56. Green JR (2005) Skeletal complications of prostate cancer: pathophysiology and therapeutic potential of bisphospho-nates. Acta Oncol 44(3):282–292
57. Gunalp I, Gunduz K (1995) Metastatic orbital tumors. Jpn J Ophthalmol 39(1):65–70
58. Gupta R, Honavar SG, Vemuganti GK (2005) Orbital metastasis from hepatocellular carcinoma. Surv Ophthal-mol 50(5):485–489
59. Harris AL, Montgomery A (1980) Orbital carcinoid tumor. Am J Ophthalmol 90(6):875–877
60. Harris AL, Montgomery A, Reyes RR, Gazet JC, Smith IE (1981) Carcinoid tumour presenting as an orbital metasta-sis. Clin Oncol 7(4):365–372
61. Hart W (1962) Metastatic carcinoma to the eye and orbit. Int Ophthalmol Clin 2:465–482
62. Hart W (1962) Metastatic tumors of the eye and orbit. Int Ophthalmol Clin 2:465–482
63. Healy JF (1983) Computed tomographic evaluation of metastases to the orbit. Ann Ophthalmol 15(11):1026–1029
64. Henderson J, Farrow GM (1980) Metastatic carcinoma. In: Henderson J (ed) Orbital tumors. Decker, New York, pp 451–471
65. Henderson JWCR, Farrow GM (1994) Metastatic carcino-mas. New York, Raven Press
66. Hesselink JR, Davis KR, Weber AL, Davis JM, Taveras JM (1980) Radiological evaluation of orbital metastases, with emphasis on computed tomography. Radiology 137(2): 363–366
67. Holt BAU, Holmes SAV, Kirby RS (1994) Renal cell carcinoma presenting with orbital metastasis. Br J Urol 75: 246–247
68. Hornblass A, Kass LG, Reich R (1987) Th yroid carcinoma metastatic to the orbit. Ophthalmology 94(8):1004–1007
69. Horner F (1864) Carcino der Dura mater. Klin Monatsbl Augenheilkd 2:186–190
70. Horwitz KB, Costlow ME, McGuire WL (1975) MCF-7; a human breast cancer cell line with estrogen, androgen, progesterone, and glucocorticoid receptors. Steroids 26(6): 785–795
71. Horwitz KB, McGuire WL (1975) Predicting response to endocrine therapy in human breast cancer: a hypothesis. Science 189(4204):726–727
72. Horwitz KB, McGuire WL (1975) Specifi c progesterone receptors in human breast cancer. Steroids 25(4):497–505
73. Houghton JD (1956) Solitary metastasis of renal cell carci-noma. Am J Ophthalmol (41):548–549
74. Huben RP, Murphy GP (1986) Prostate cancer: an update. CA Cancer J Clin 36(5):274–292
75. Huh SH, Nisce LZ, Simpson LD, Chu FC (1974) Proceedings: value of radiation therapy in the treatment of orbital metastasis. Am J Roentgenol Radium Th er Nucl Med 120(3):589–594
76. Hutchison DS, Smith TR (1979) Ocular and orbital meta-static carcinoma. Ann Ophthalmol 11(6):869–873
77. Ives NJ, Stowe RL, Lorigan P, Wheatley K (2007) Chemotherapy compared with biochemotherapy for the treatment of metastatic melanoma: a meta-analysis of 18 trials involving 2,621 patients. J Clin Oncol 25(34): 5426–5434
78. Jensen OA (1970) Metastatic tumours of the eye and orbit. A histopathological analysis of a Danish series. Acta Pathol Microbiol Scand 212(Suppl):201–214
79. Kawaoka T, Aikata H, Takaki S, Uka K, Azakami T Saneto H, et al (2009) FDG positron emission tomography/com-puted tomography for the detection of extrahepatic metas-tases from hepatocellular carcinoma. Hepatol Res 39(2): 134–142
80. Kennedy RE (1984) An evaluation of 820 orbital cases. Trans Am Ophthalmol Soc 82:134–157
81. Kennerdell JS, Dekker A, Johnson BL, Dubois PJ (1979) Fine-needle aspiration biopsy. Its use in orbital tumors. Arch Ophthalmol 97(7):1315–1317
82. Kennerdell JS, Maroon JC, Dekker A, Johnson BL (1979) Microsurgery and fi ne needle aspiration biopsy of orbital tumors. Trans Pa Acad Ophthalmol Otolaryngol 32(2): 147–150
83. Kimura N, Pilichowska M, Okamoto H, Kimura I, Aunis D (2000) Immunohistochemical expression of chromogra-nins A and B, prohormone convertases 2 and 3, and ami-dating enzyme in carcinoid tumors and pancreatic endocrine tumors. Mod Pathol 13(2):140–146
84. Koelma IA, Nap M, Huitema S, Krom RA, Houthoff HJ (1986) Hepatocellular carcinoma, adenoma, and focal nodular hyperplasia. Comparative histopathologic study with immunohistochemical parameters. Arch Pathol Lab Med 110(11):1035–1040
85. Kokal WA, Gardine RL, Sheibani K, Morris PL, Prager E, Zak IW, et al (1989) Tumor DNA content in resectable, pri-mary colorectal carcinoma. Ann Surg 209(2): 188–193
86. Kuzma BB, Goodman JM (1998) Slowly progressive bilat-eral enophthalmos from metastatic breast carcinoma. Surg Neurol 50(6):600–602
184 12 Evaluation and Management of Metastatic Orbital Tumors
12
87. Lacreusette A, Lartigue A, Nguyen JM, Barbieux I, Pandolfi no MC, Paris F, et al (2008) Relationship between responsiveness of cancer cells to Oncostatin M and/or IL-6 and survival of stage III melanoma patients treated with tumour-infi ltrating lymphocytes. J Pathol 216(4):451–459
88. Lee HM, Choo CT, Poh WT (1997) Orbital metastasis from carcinoma of cervix. Br J Ophthalmol 81(4): 330–331
89. Liu D (1985) Complications of fi ne needle aspiration biopsy of the orbit. Ophthalmology 92(12):1768–1771
90. Lubin JR, Grove AS Jr., Zakov ZN, Albert DM (1980) Hepatoma metastatic to the orbit. Am J Ophthalmol 89(2):268–273
91. Macedo JE, Machado M, Araujo A, Angelico V, Lopes JM (2007) Orbital metastasis as a rare form of clinical presen-tation of non-small cell lung cancer. J Th orac Oncol 2(2): 166–167
92. Margo CE, Levy MH (1993) Orbital metastasis from medullary carcinoma of the thyroid. Am J Ophthalmol 115(3): 394–395
93. Martin RG (1970) Management of carcinoid tumors. Cancer 26(3):547–551
94. McGuire WL (1975) Quantitation of estrogen receptor in mammary carcinoma. Methods Enzymol 36(00): 248–254
95. Mehta JS, Abou-Rayyah Y, Rose GE (2006) Orbital carci-noid metastases. Ophthalmology 113(3):466–472
96. Middleton RG (1967) Surgery for metastatic renal cell carcinoma. J Urol 97(6):973–977
97. Mitchell ME, Johnson JA, Wilton PB (1996) Five primary synchronous neoplasms of the gastrointestinal tract. J Clin Gastroenterol 23(4):284–288
98. Modlin IM, Lye KD, Kidd M (2003) A 5-decade analysis of 13,715 carcinoid tumors. Cancer 97(4):934–959
99. Moschos SJ, Mandic M, Kirkwood JM, Storkus WJ, Lotze MT (2008) Focus on FOCIS: interleukin 2 treat-ment associated autoimmunity. Clin Immunol 127(2): 123–129
100. Moss HM (1962) Expanding lesions of the orbit. A clini-cal study of 230 consecutive cases. Am J Ophthalmol 54: 761–770
101. Mottow-Lippa L, Jakobiec FA, Iwamoto T (1981) Pseudoinfl ammatory metastatic breast carcinoma of the orbit and lids. Ophthalmology 88(6):575–580
102. Mouridsen H, Palshof T, Patterson J, Battersby L (1978) Tamoxifen in advanced breast cancer. Cancer Treat Rev 5(3):131–141
103. Okada M, Murakami T, Kumano S, Kuwabara M, Shimono T, Hosono M, et al (2009) Integrated FDG-PET/CT compared with intravenous contrast-enhanced CT for evaluation of metastatic regional lymph nodes in patients with resectable early stage esophageal cancer. Ann Nucl Med 23(1):73–80
104. Perez-Fidalgo JA, Oltra Ferrando A, Lopez Jimenez A, Maestu Maiques I (2006) Primary carcinoid tumour of the pancreas. Clin Transl Oncol 8(1):54–56
105. Po SM, Custer PL, Smith ME (1996) Bilateral lagophthal-mos. An unusual presentation of metastatic breast carci-noma. Arch Ophthalmol 114(9):1139–1141
106. Poli T, Mora P, Reichegger V, Ricci R, Corradi D, Gandolfi SA, et al (2007) Surgical management of orbital malig-nant melanoma: our experience and a report of three cases. Klin Monatsbl Augenheilkd 224(10):794–798
107. Recchia F, Candeloro G, Necozione S, Fumagalli L, Bratta M, Rea S (2008) Multicenter phase II study of chemoim-munotherapy in the treatment of metastatic melanoma. Anticancer Drugs 19(2):201–207
108. Reese AB (1971) Expanding lesions of the orbit. Trans Ophthalmol Soc U K 91:85–104
109. Reifl er DM, Kini SR, Liu D, Littleton RH (1984) Orbital metastasis from prostatic carcinoma. Identifi cation by immunocytology. Arch Ophthalmol 102(2):292–295
110. Reifl er DM (1985) Orbital metastasis with enophthalmos: a review of the literature. Henry Ford Hosp Med J 33(4): 171–179
111. Riddle PJ, Font RL, Zimmerman LE (1982) Carcinoid tumors of the eye and orbit: a clinicopathologic study of 15 cases, with histochemical and electron microscopic observations. Hum Pathol 13(5):459–469
112. Roato I, D’Amelio P, Gorassini E, Grimaldi A, Bonello L, Fiori C, et al (2008) Osteoclasts are active in bone forming metastases of prostate cancer patients. PLoS One 3(11):e3627
113. Rootman J, Ragaz J, Cline R, Lapointe J (1988) In: Rootman J (ed) Diseases of the orbit. Lippincott, Phila-delphia, pp 405–457
114. Rosenbluth J, Laval J, Weil JV (1960) Metastasis of bron-chial adenoma to the eye. Arch Ophthalmol 63:47–50
115. Rosenkranz L, Schroeder C (1985) Recurrent malignant melanoma following a 46-year disease-free interval. N Y State J Med 85(3):95
116. Rothfus WE, Curtin HD (1984) Extraocular muscle enlargement: a CT review. Radiology 151(3):677–681
117. Rush JA, Waller RR, Campbell RJ (1980) Orbital carci-noid tumor metastatic from the colon. Am J Ophthalmol 89(5):636–640
118. Rush JA, Older JJ (1987) Testicular seminoma metastatic to the orbit. Am J Ophthalmol 104:634–640
119. Sanders RJ, Axtell HK (1964) Carcinoids of the gastroin-testinal tract. Surg Gynecol Obstet 119:369–380
120. Schwab L, Doshi H, Shields JA, Kagame K, Chana H (1994) Hepatocellular carcinoma metastatic to the orbit in an African patient. Ophthalmic Surg 25(2):105–106
121. Seregard S, Sahlin S (1999) Panorama of orbital space-occupying lesions. Th e 24-year experience of a referral centre. Acta Ophthalmol Scand 77(1):91–98
References 185
122. Seretan EL (1981) Metastatic adenocarcinoma from the stomach to the orbit. Arch Ophthalmol 99(8):1469
123. Shah NA, Urusova IA, D’Agnolo A, Colquhoun SD, Rosenbloom BE, Vener SL, et al (2007) Primary hepatic carcinoid tumor presenting as Cushing’s syndrome. J Endocrinol Invest 30(4):327–333
124. Shetlar DJ, Font RL, Ordonez N, el-Naggar A, Boniuk MA (1990) Clinicopathologic study of three carcinoid tumors metastatic to the orbit. Immunohistochemical, ultrastructural, and DNA fl ow cytometric studies. Ophthalmology 97(2):257–264
125. Shields CL, Shields JA, Eagle RC Jr., Peyster RG, Conner BE, Green HA (1987) Orbital metastasis from a carcinoid tumor. Computed tomography, magnetic resonance imaging, and electron microscopic fi ndings. Arch Ophthalmol 105(7):968–971
126. Shields CL, Shields JA, Peggs M (1988) Tumors metastatic to the orbit. Ophthal Plast Reconstr Surg 4(2):73–80
127. Shields CL, Shields JA, Mruczek AW (1989) Enophthalmos as the initial manifestation of metastasis from scirrhous carcinoma of the breast. Ophthal Practice 7:159–160
128. Shields CL, Stopyra GA, Marr BP, Moster ML, Shields JA (2004) Enophthalmos as initial manifestation of occult, mammogram-negative carcinoma of the breast. Ophthalmic Surg Lasers Imaging 35(1):56–57
129. Shields JA, Bakewell B, Augsburger JJ, Flanagan JC (1984) Classifi cation and incidence of space-occupying lesions of the orbit. A survey of 645 biopsies. Arch Ophthalmol 102(11):1606–1611
130. Shields JA, Shields CL, Shakin EP, Kobetz LE (1988) Metastasis of choroidal melanoma to the contralateral choroid, orbit, and eyelid. Br J Ophthalmol 72(6):456–460
131. Shields JA, Shields CL, Eagle RC Jr., Gunduz K, Lin B (1998) Diff use ocular metastases as an initial sign of meta-static lung cancer. Ophthalmic Surg Lasers 29(7):598–601
132. Shields JA, Shields CL, Brotman HK, Carvalho C, Perez N, Eagle RC Jr (2001) Cancer metastatic to the orbit: the 2000 Robert M. Curts Lecture. Ophthal Plast Reconstr Surg 17(5):346–354
133. Shields JA, Perez N, Shields CL, Singh AD, Eagle RC Jr (2002) Orbital melanoma metastatic from contralateral choroid: management by complete surgical resection. Ophthalmic Surg Lasers 33(5):416–420
134. Shih CY, Mirchandani G, Kazim M (2007) Atypical MRI features of intraorbital metastatic melanoma. Ophthal Plast Reconstr Surg 23(4):335–336
135. Silva D (1968) Orbital tumors. Am J Ophthalmol 65(3):318–339
136. Singer MA, Warren F, Accardi F, Sabatini M, D’Amico RA (1990) Adenocarcinoma of the stomach confi rmed by orbital biopsy in a patient seropositive for human immu-nodefi ciency virus. Am J Ophthalmol 110(6):707–709
137. Slamovits TL, Burde RM (1988) Bumpy muscles. Surv Ophthalmol 33(3):189–199
138. Stewart WB, Newman NM, Cavender JC, Spencer WH (1978) Fibrous histiocytoma metastatic to the orbit. Arch Ophthalmol 96(5):871–873
139. Stockl FA, Tucker N, Burnier MN (1997) Th ymic carci-noma metastatic to the orbit. Am J Ophthalmol 124(3):401–403
140. Sullivan TJ, Valenzuela AA (2006) Imaging features of ocular adnexal lymphoproliferative disease. Eye 20(10): 1189–1195
141. Th omas KM, Cumberworth VL, McEwan J (1995) Orbital and skin metastases in a polymorphous low grade adeno-carcinoma of the salivary gland. J Laryngol Otol 109(12):1222–1225
142. Tijl JW, Koornneef L (1991) Fine needle aspiration biopsy in orbital tumours. Br J Ophthalmol 75(8):491–4 92
143. Tijl J, Koornneef L, Eijpe A, Th omas L, Gonzalez DG, Veenhof C (1992) Metastatic tumors to the orbit—man-agement and prognosis. Graefes Arch Clin Exp Ophthalmol 230(6):527–530
144. Tolia BM, Whitmore WF Jr (1975) Solitary metastasis from renal cell carcinoma. J Urol 114(6):836–838
145. Toller KK, Gigantelli JW, Spalding MJ (1998) Bilateral orbital metastases from breast carcinoma. A case of false pseudotumor. Ophthalmology 105(10):1897–901
146. Torres JJ, Medel R, Alonso T, Morral M, Garcia-Arumi J, Myint S, et al (2007) Orbital metastases from male breast can-cer in two cases. Ophthal Plast Reconstr Surg 23(2):154–156
147. Tranfa F, Cennamo G, Rosa N, De Rosa G, Boscaino A, Bonavolonta G (1994) An unusual orbital lesion: hepa-toma metastatic to the orbit. Ophthalmologica 208(6): 329–332
148. Trokel SL, Hilal SK (1979) Recognition and diff erential diagnosis of enlarged extraocular muscles in computed tomography. Am J Ophthalmol 87(4):503–512
149. Valenzuela AA, Allen C, Grimes D, Wong D, Sullivan TJ (2006) Positron emission tomography in the detection and staging of ocular adnexal lymphoproliferative dis-ease. Ophthalmology 113:2331–2337
150. Valenzuela AA, Archibald CW, Fleming B, Ong L, O’Donnell B, Crompton J, Selva D, McNab AA, Sullivan TJ (2009) Orbital metastases: clinical features, manage-ment and outcome. Orbit 28(2):153–159
151. Walton RC, Ellis GS Jr., Haik BG (1996) Rhabdomy-osarcoma presumed metastatic to the orbit. Ophthal-mology 103(9):1512–1516
152. Warburg O (1931) Th e metabolism of tumors. Smith RR, New York
153. Weber G (1983) Biochemical strategy of cancer cells and the design of chemotherapy: G. H. A. Clowes memorial lecture. Cancer Res 43(8):3466–3492

186 12 Evaluation and Management of Metastatic Orbital Tumors
12
154. Weijerman PC, Boeve ER, Mickisch GH, Simonsz HJ, Schroder FH (1997) Orbital tumours as a fi rst indication of urological malignancies. Br J Urol 79(2):288–289
155. Whyte AM (1978) Bronchogenic carcinoma metastasiz-ing to the orbit. A case report. J Maxillofac Surg 6(4):277–280
156. Wild D, Eyrich GK, Ciernik IF, Stoeckli SJ, Schuknecht B, Goerres GW (2006) In-line (18)F-fl uorodeoxyglucose positron emission tomography with computed tomog-raphy (PET/CT) in patients with carcinoma of the sinus/nasal area and orbit. J Craniomaxillofac Surg 34(1):9–16
157. Winkler CF, Goodman GK, Eiferman RA, Yam LT (1981) Orbital metastasis from prostatic carcinoma. Identifi cation by an immunoperoxidase technique. Arch Ophthalmol 99(8):1406–1408
158. Wolin MJ (1993) Metastatic renal cell carcinoma manifest-ing as an orbital mass. Am J Ophthalmol 115(4): 542–543
159. Yang K, Ulich T, Cheng L, Lewin KJ (1983) Th e neuroen-docrine products of intestinal carcinoids. An immu-noperoxidase study of 35 carcinoid tumors stained for serotonin and eight polypeptide hormones. Cancer 51(10):1918–1926
160. Zajdela A, Vielh P, Schlienger P, Haye C (1990) Fine-needle cytology of 292 palpable orbital and eyelid tumors. Am J Clin Pathol 93(1):100–104
161. Zambarakji HJ, Simcock PR, Kinnear PE (1997) Bilateral orbital metastases in a woman with breast carcinoma. J R Soc Med 90(12):684
162. Zografos L, Ducrey N, Beati D, Schalenbourg A, Spahn B, Balmer A, et al (2003) Metastatic melanoma in the eye and orbit. Ophthalmology 110(11):2245–2256
Targeted Therapy in the Treatment of Orbital and Periorbital MalignanciesAaron Savar and Bita Esmaeli
Chapter 13
13
Core Messages
Virtually any molecule can serve as a target for ■
therapy. Th e ideal target, however, is present only on abnormal cells, allowing normal cells to be spared from the treatment eff ect.Rituximab was the fi rst monoclonal antibody ■
approved by the United States Food and Drug Administration for the treatment of cancer. It is a chimeric human/murine monoclonal anti-CD20 immunoglobulin G1 (IgG1) antibody. CD20 is a cell surface protein expressed on most B cells but not on uncommitted hematopoietic precursor cells.Rituximab is approved for the treatment of B-cell lymphoma. Rituximab has also been used suc-cessfully in the treatment of other lymphoprolif-erative disorders in the orbit, including lymphoid hyperplasiaIbritumomab is a murine IgG1 anti-CD20 anti- ■
body. It can be coupled with tiuxetan, a chelator, and ibritumomab tiuxetan can bind yttrium-90 to form yttrium-90-labeled ibritumomab tiux-etan (hereaft er referred to as ibritumomab; Zevalin) [32]. In a trial comparing rituximab to rituximab plus ibritumomab for refractory or relapsed follicular or low-grade non-Hodgkin lymphoma, response rates were 56% for ritux-imab alone and 80% for the combination. In a prospective trial, 12 patients underwent com-bined treatment with rituximab and ibritumomab as front-line treatment for stage I-E ocular adn-exal lymphoma. Ten patients had a complete response, and two had a partial response. Th ere
was one local recurrence during the follow-up period; there were no distant relapses[14].Imatinib mesylate (imatinib; Gleevec) is a selec- ■
tive tyrosine kinase inhibitor used in the treat-ment of chronic myeloid leukemia (CML) and gastrointestinal stromal tumors. Edema is the most commonly seen adverse eff ect associated with imatinib mesylate, and the periorbital region is the most common site for edema. In a phase I trial of imatinib for the treatment of gastrointesti-nal stromal tumor, edema of the periorbital region or eyelids was seen in 55.1% of the 174 patients treated. Rarely, the edema can be so severe that surgical treatment is required.Cetuximab is a monoclonal antibody directed ■
against epidermal growth factor receptor (EGFR), a member of the ErbB family of tyrosine kinase receptors. Cetuximab is used in the treatment of colon cancer and head and neck squamous cell car-cinoma (SCC). Although SCC in the head and neck can involve the orbit, we found no published reports of cetuximab used in the treatment of periorbital SCC at the time of preparation of this chapter. However, there have been reports of EGFR expres-sion in conjunctival SCC as well as in both ocular and extraocular sebaceous gland carcinomas, sug-gesting a potential role for EGFR inhibitors in treatment of conjunctival SCC, and sebaceous gland carcinoma of the eyelid. A common ocular side eff ect of cetuximab and other EGFR inhibitors is trichomegaly.
13.1 Introduction
All cells have molecules on the cell surface and within the cell that are potential targets for targeted therapy. Targeted therapies take advantage of diff erences in molecular char-
acteristics between diff erent cell types to direct treatment to specifi c cells [2, 5]. Targeted therapies are currently being used in the treatment of a variety of disease pro-cesses, including infl ammatory, infectious, and neoplas-tic processes. Table 13.1 lists many of the targeted
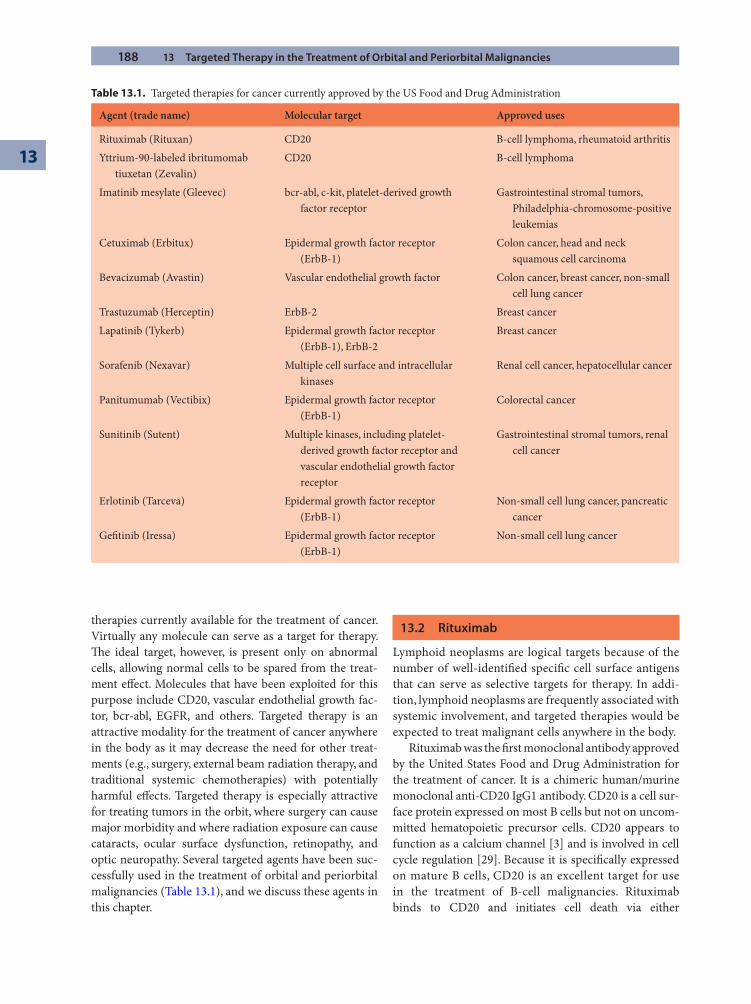
188 13 Targeted Therapy in the Treatment of Orbital and Periorbital Malignancies
13
therapies currently available for the treatment of cancer. Virtually any molecule can serve as a target for therapy. Th e ideal target, however, is present only on abnormal cells, allowing normal cells to be spared from the treat-ment eff ect. Molecules that have been exploited for this purpose include CD20, vascular endothelial growth fac-tor, bcr-abl, EGFR, and others. Targeted therapy is an attractive modality for the treatment of cancer anywhere in the body as it may decrease the need for other treat-ments (e.g., surgery, external beam radiation therapy, and traditional systemic chemotherapies) with potentially harmful eff ects. Targeted therapy is especially attractive for treating tumors in the orbit, where surgery can cause major morbidity and where radiation exposure can cause cataracts, ocular surface dysfunction, retinopathy, and optic neuropathy. Several targeted agents have been suc-cessfully used in the treatment of orbital and periorbital malignancies (Table 13.1), and we discuss these agents in this chapter.
13.2 Rituximab
Lymphoid neoplasms are logical targets because of the number of well-identifi ed specifi c cell surface antigens that can serve as selective targets for therapy. In addi-tion, lymphoid neoplasms are frequently associated with systemic involvement, and targeted therapies would be expected to treat malignant cells anywhere in the body.
Rituximab was the fi rst monoclonal antibody approved by the United States Food and Drug Administration for the treatment of cancer. It is a chimeric human/murine monoclonal anti-CD20 IgG1 antibody. CD20 is a cell sur-face protein expressed on most B cells but not on uncom-mitted hematopoietic precursor cells. CD20 appears to function as a calcium channel [3] and is involved in cell cycle regulation [29]. Because it is specifi cally expressed on mature B cells, CD20 is an excellent target for use in the treatment of B-cell malignancies. Rituximab binds to CD20 and initiates cell death via either
Table 13.1. Targeted therapies for cancer currently approved by the US Food and Drug Administration
Agent (trade name) Molecular target Approved uses
Rituximab (Rituxan) CD20 B-cell lymphoma, rheumatoid arthritis
Yttrium-90-labeled ibritumomab tiuxetan (Zevalin)
CD20 B-cell lymphoma
Imatinib mesylate (Gleevec) bcr-abl, c-kit, platelet-derived growth factor receptor
Gastrointestinal stromal tumors, Philadelphia-chromosome-positive leukemias
Cetuximab (Erbitux) Epidermal growth factor receptor (ErbB-1)
Colon cancer, head and neck squamous cell carcinoma
Bevacizumab (Avastin) Vascular endothelial growth factor Colon cancer, breast cancer, non-small cell lung cancer
Trastuzumab (Herceptin) ErbB-2 Breast cancer
Lapatinib (Tykerb) Epidermal growth factor receptor (ErbB-1), ErbB-2
Breast cancer
Sorafenib (Nexavar) Multiple cell surface and intracellular kinases
Renal cell cancer, hepatocellular cancer
Panitumumab (Vectibix) Epidermal growth factor receptor (ErbB-1)
Colorectal cancer
Sunitinib (Sutent) Multiple kinases, including platelet-derived growth factor receptor and vascular endothelial growth factor receptor
Gastrointestinal stromal tumors, renal cell cancer
Erlotinib (Tarceva) Epidermal growth factor receptor (ErbB-1)
Non-small cell lung cancer, pancreatic cancer
Gefi tinib (Iressa) Epidermal growth factor receptor (ErbB-1)
Non-small cell lung cancer
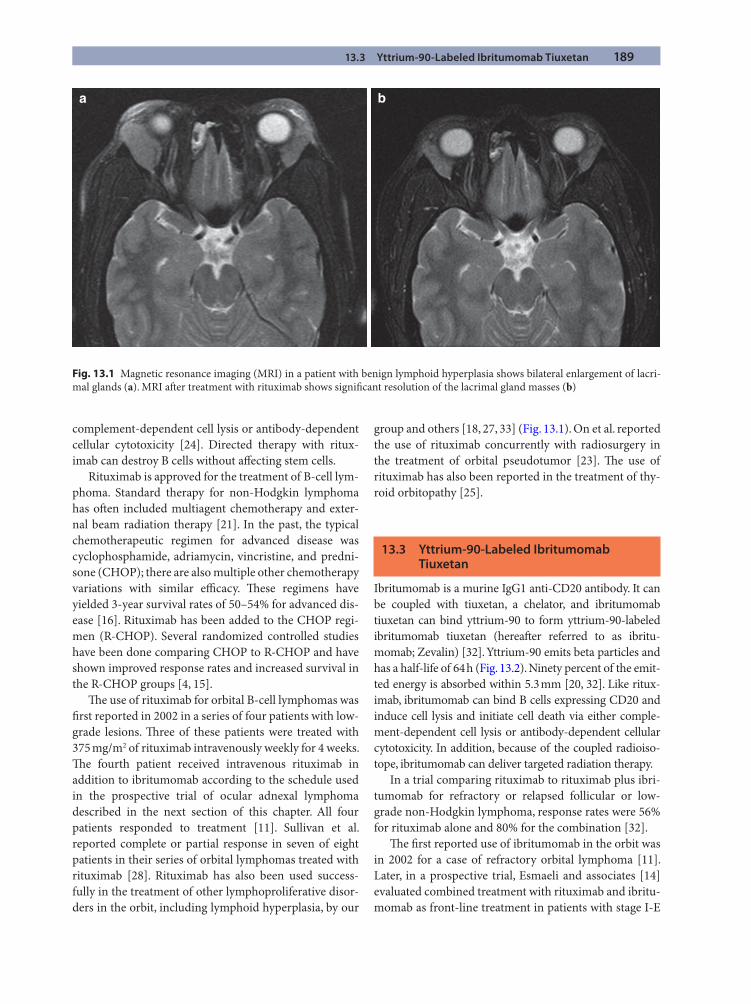
13.3 Yttrium-90-Labeled Ibritumomab Tiuxetan 189
complement-dependent cell lysis or antibody-dependent cellular cytotoxicity [24]. Directed therapy with ritux-imab can destroy B cells without aff ecting stem cells.
Rituximab is approved for the treatment of B-cell lym-phoma. Standard therapy for non-Hodgkin lymphoma has oft en included multiagent chemotherapy and exter-nal beam radiation therapy [21]. In the past, the typical chemotherapeutic regimen for advanced disease was cyclophosphamide, adriamycin, vincristine, and predni-sone (CHOP); there are also multiple other chemotherapy variations with similar effi cacy. Th ese regimens have yielded 3-year survival rates of 50–54% for advanced dis-ease [16]. Rituximab has been added to the CHOP regi-men (R-CHOP). Several randomized controlled studies have been done comparing CHOP to R-CHOP and have shown improved response rates and increased survival in the R-CHOP groups [4, 15].
Th e use of rituximab for orbital B-cell lymphomas was fi rst reported in 2002 in a series of four patients with low-grade lesions. Th ree of these patients were treated with 375 mg/m2 of rituximab intravenously weekly for 4 weeks. Th e fourth patient received intravenous rituximab in addition to ibritumomab according to the schedule used in the prospective trial of ocular adnexal lymphoma described in the next section of this chapter. All four patients responded to treatment [11]. Sullivan et al. reported complete or partial response in seven of eight patients in their series of orbital lymphomas treated with rituximab [28]. Rituximab has also been used success-fully in the treatment of other lymphoproliferative disor-ders in the orbit, including lymphoid hyperplasia, by our
group and others [18, 27, 33] (Fig. 13.1). On et al. reported the use of rituximab concurrently with radiosurgery in the treatment of orbital pseudotumor [23]. Th e use of rituximab has also been reported in the treatment of thy-roid orbitopathy [25].
13.3 Yttrium-90-Labeled Ibritumomab Tiuxetan
Ibritumomab is a murine IgG1 anti-CD20 antibody. It can be coupled with tiuxetan, a chelator, and ibritumomab tiuxetan can bind yttrium-90 to form yttrium-90-labeled ibritumomab tiuxetan (hereaft er referred to as ibritu-momab; Zevalin) [32]. Yttrium-90 emits beta particles and has a half-life of 64 h (Fig. 13.2). Ninety percent of the emit-ted energy is absorbed within 5.3 mm [20, 32]. Like ritux-imab, ibritumomab can bind B cells expressing CD20 and induce cell lysis and initiate cell death via either comple-ment-dependent cell lysis or antibody-dependent cellular cytotoxicity. In addition, because of the coupled radioiso-tope, ibritumomab can deliver targeted radiation therapy.
In a trial comparing rituximab to rituximab plus ibri-tumomab for refractory or relapsed follicular or low-grade non-Hodgkin lymphoma, response rates were 56% for rituximab alone and 80% for the combination [32].
Th e fi rst reported use of ibritumomab in the orbit was in 2002 for a case of refractory orbital lymphoma [11]. Later, in a prospective trial, Esmaeli and associates [14] evaluated combined treatment with rituximab and ibritu-momab as front-line treatment in patients with stage I-E
Fig. 13.1 Magnetic resonance imaging (MRI) in a patient with benign lymphoid hyperplasia shows bilateral enlargement of lacri-mal glands (a). MRI aft er treatment with rituximab shows signifi cant resolution of the lacrimal gland masses (b)
a b
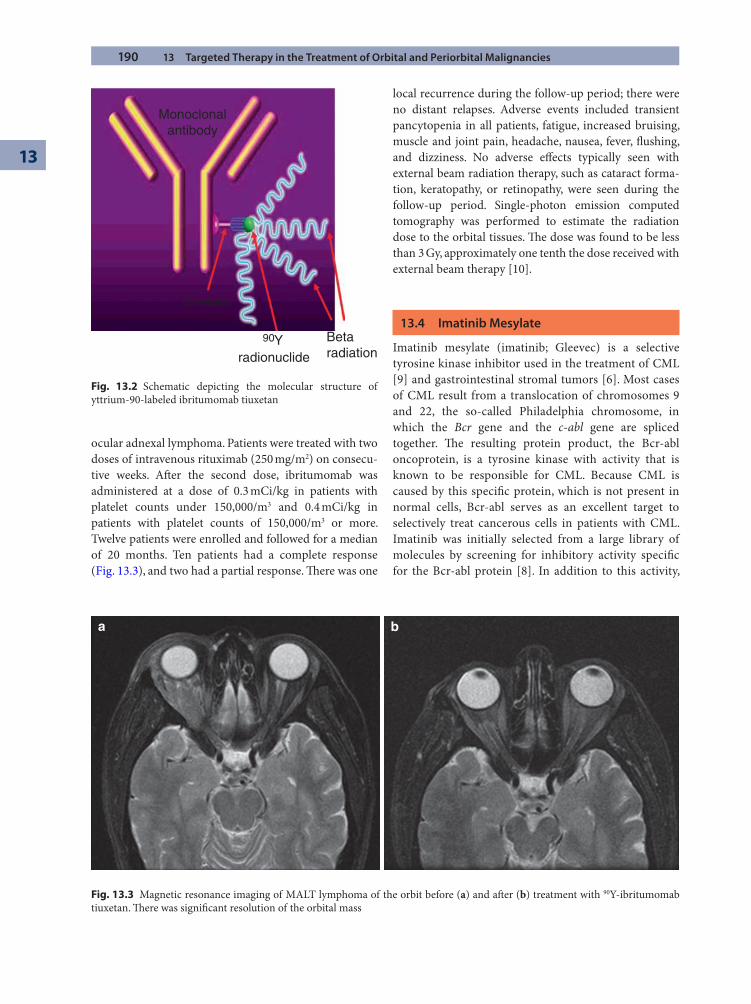
190 13 Targeted Therapy in the Treatment of Orbital and Periorbital Malignancies
13
ocular adnexal lymphoma. Patients were treated with two doses of intravenous rituximab (250 mg/m2) on consecu-tive weeks. Aft er the second dose, ibritumomab was administered at a dose of 0.3 mCi/kg in patients with platelet counts under 150,000/m3 and 0.4 mCi/kg in patients with platelet counts of 150,000/m3 or more. Twelve patients were enrolled and followed for a median of 20 months. Ten patients had a complete response (Fig. 13.3), and two had a partial response. Th ere was one
local recurrence during the follow-up period; there were no distant relapses. Adverse events included transient pancytopenia in all patients, fatigue, increased bruising, muscle and joint pain, headache, nausea, fever, fl ushing, and dizziness. No adverse eff ects typically seen with external beam radiation therapy, such as cataract forma-tion, keratopathy, or retinopathy, were seen during the follow-up period. Single-photon emission computed tomography was performed to estimate the radiation dose to the orbital tissues. Th e dose was found to be less than 3 Gy, approximately one tenth the dose received with external beam therapy [10].
13.4 Imatinib Mesylate
Imatinib mesylate (imatinib; Gleevec) is a selective tyrosine kinase inhibitor used in the treatment of CML [9] and gastrointestinal stromal tumors [6]. Most cases of CML result from a translocation of chromosomes 9 and 22, the so-called Philadelphia chromosome, in which the Bcr gene and the c-abl gene are spliced together. Th e resulting protein product, the Bcr-abl oncoprotein, is a tyrosine kinase with activity that is known to be responsible for CML. Because CML is caused by this specifi c protein, which is not present in normal cells, Bcr-abl serves as an excellent target to selectively treat cancerous cells in patients with CML. Imatinib was initially selected from a large library of molecules by screening for inhibitory activity specifi c for the Bcr-abl protein [8]. In addition to this activity,
Fig. 13.2 Schematic depicting the molecular structure of yttrium-90-labeled ibritumomab tiuxetan
Betaradiationradionuclide
Y90
Monoclonalantibody
Chelator
Fig. 13.3 Magnetic resonance imaging of MALT lymphoma of the orbit before (a) and aft er (b) treatment with 90Y-ibritumomab tiuxetan. Th ere was signifi cant resolution of the orbital mass
a b
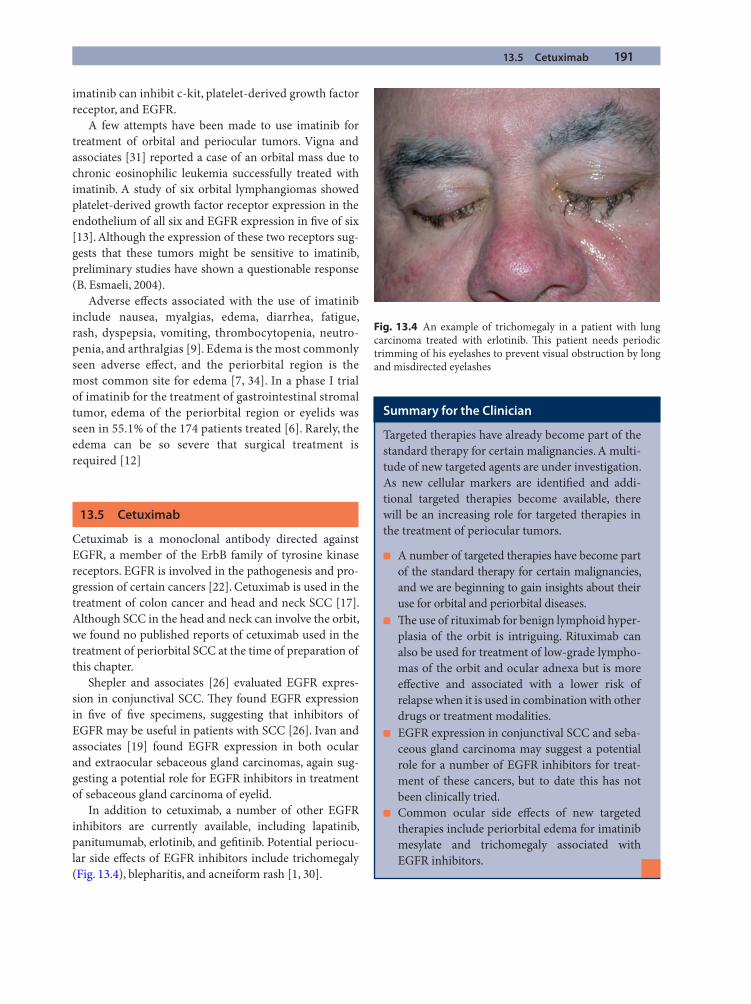
13.5 Cetuximab 191
imatinib can inhibit c-kit, platelet-derived growth factor receptor, and EGFR.
A few attempts have been made to use imatinib for treatment of orbital and periocular tumors. Vigna and associates [31] reported a case of an orbital mass due to chronic eosinophilic leukemia successfully treated with imatinib. A study of six orbital lymphangiomas showed platelet-derived growth factor receptor expression in the endothelium of all six and EGFR expression in fi ve of six [13]. Although the expression of these two receptors sug-gests that these tumors might be sensitive to imatinib, preliminary studies have shown a questionable response (B. Esmaeli, 2004).
Adverse eff ects associated with the use of imatinib include nausea, myalgias, edema, diarrhea, fatigue, rash, dyspepsia, vomiting, thrombocytopenia, neutro-penia, and arthralgias [9]. Edema is the most commonly seen adverse eff ect, and the periorbital region is the most common site for edema [7, 34]. In a phase I trial of imatinib for the treatment of gastrointestinal stromal tumor, edema of the periorbital region or eyelids was seen in 55.1% of the 174 patients treated [6]. Rarely, the edema can be so severe that surgical treatment is required [12]
13.5 Cetuximab
Cetuximab is a monoclonal antibody directed against EGFR, a member of the ErbB family of tyrosine kinase receptors. EGFR is involved in the pathogenesis and pro-gression of certain cancers [22]. Cetuximab is used in the treatment of colon cancer and head and neck SCC [17]. Although SCC in the head and neck can involve the orbit, we found no published reports of cetuximab used in the treatment of periorbital SCC at the time of preparation of this chapter.
Shepler and associates [26] evaluated EGFR expres-sion in conjunctival SCC. Th ey found EGFR expression in fi ve of fi ve specimens, suggesting that inhibitors of EGFR may be useful in patients with SCC [26]. Ivan and associates [19] found EGFR expression in both ocular and extraocular sebaceous gland carcinomas, again sug-gesting a potential role for EGFR inhibitors in treatment of sebaceous gland carcinoma of eyelid.
In addition to cetuximab, a number of other EGFR inhibitors are currently available, including lapatinib, panitumumab, erlotinib, and gefi tinib. Potential periocu-lar side eff ects of EGFR inhibitors include trichomegaly (Fig. 13.4), blepharitis, and acneiform rash [1, 30].
Fig. 13.4 An example of trichomegaly in a patient with lung carcinoma treated with erlotinib. Th is patient needs periodic trimming of his eyelashes to prevent visual obstruction by long and misdirected eyelashes
Summary for the Clinician
Targeted therapies have already become part of the standard therapy for certain malignancies. A multi-tude of new targeted agents are under investigation. As new cellular markers are identifi ed and addi-tional targeted therapies become available, there will be an increasing role for targeted therapies in the treatment of periocular tumors.
A number of targeted therapies have become part ■
of the standard therapy for certain malignancies, and we are beginning to gain insights about their use for orbital and periorbital diseases.Th e use of rituximab for benign lymphoid hyper- ■
plasia of the orbit is intriguing. Rituximab can also be used for treatment of low-grade lympho-mas of the orbit and ocular adnexa but is more eff ective and associated with a lower risk of relapse when it is used in combination with other drugs or treatment modalities.EGFR expression in conjunctival SCC and seba- ■
ceous gland carcinoma may suggest a potential role for a number of EGFR inhibitors for treat-ment of these cancers, but to date this has not been clinically tried.Common ocular side eff ects of new targeted ■
therapies include periorbital edema for imatinib mesylate and trichomegaly associated with EGFR inhibitors.
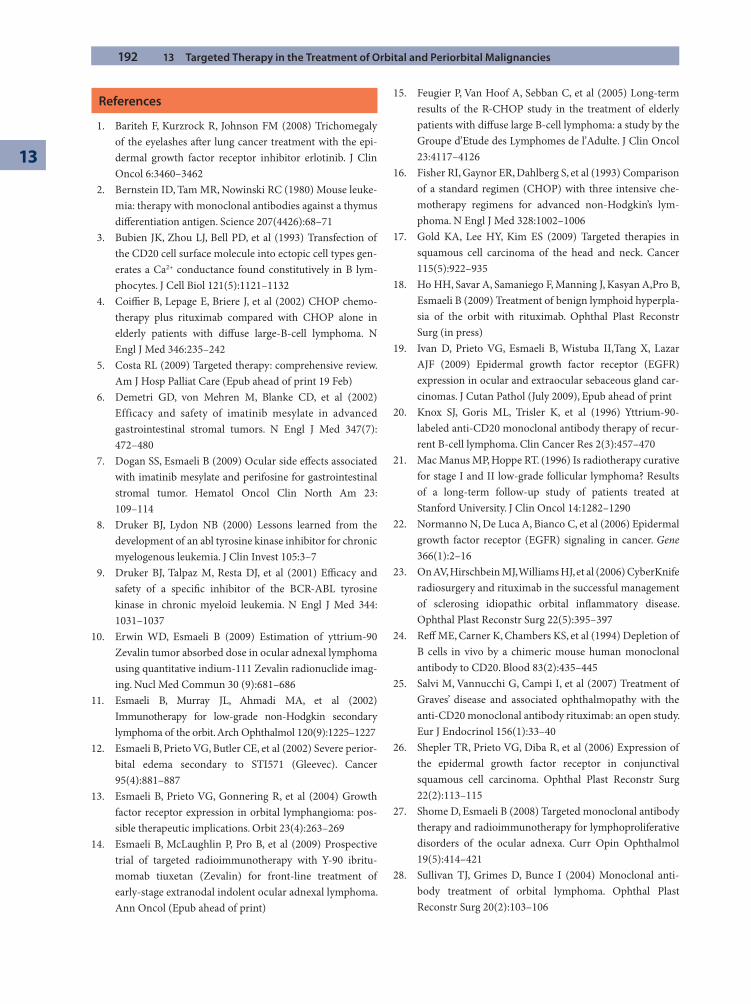
192 13 Targeted Therapy in the Treatment of Orbital and Periorbital Malignancies
13
References
1. Bariteh F, Kurzrock R, Johnson FM (2008) Trichomegaly of the eyelashes aft er lung cancer treatment with the epi-dermal growth factor receptor inhibitor erlotinib. J Clin Oncol 6:3460–3462
2. Bernstein ID, Tam MR, Nowinski RC (1980) Mouse leuke-mia: therapy with monoclonal antibodies against a thymus diff erentiation antigen. Science 207(4426):68–71
3. Bubien JK, Zhou LJ, Bell PD, et al (1993) Transfection of the CD20 cell surface molecule into ectopic cell types gen-erates a Ca2+ conductance found constitutively in B lym-phocytes. J Cell Biol 121(5):1121–1132
4. Coiffi er B, Lepage E, Briere J, et al (2002) CHOP chemo-therapy plus rituximab compared with CHOP alone in elderly patients with diff use large-B-cell lymphoma. N Engl J Med 346:235–242
5. Costa RL (2009) Targeted therapy: comprehensive review. Am J Hosp Palliat Care (Epub ahead of print 19 Feb)
6. Demetri GD, von Mehren M, Blanke CD, et al (2002) Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med 347(7): 472–480
7. Dogan SS, Esmaeli B (2009) Ocular side eff ects associated with imatinib mesylate and perifosine for gastrointestinal stromal tumor. Hematol Oncol Clin North Am 23: 109–114
8. Druker BJ, Lydon NB (2000) Lessons learned from the development of an abl tyrosine kinase inhibitor for chronic myelogenous leukemia. J Clin Invest 105:3–7
9. Druker BJ, Talpaz M, Resta DJ, et al (2001) Effi cacy and safety of a specifi c inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. N Engl J Med 344: 1031–1037
10. Erwin WD, Esmaeli B (2009) Estimation of yttrium-90 Zevalin tumor absorbed dose in ocular adnexal lymphoma using quantitative indium-111 Zevalin radionuclide imag-ing. Nucl Med Commun 30 (9):681–686
11. Esmaeli B, Murray JL, Ahmadi MA, et al (2002) Immunotherapy for low-grade non-Hodgkin secondary lymphoma of the orbit. Arch Ophthalmol 120(9):1225–1227
12. Esmaeli B, Prieto VG, Butler CE, et al (2002) Severe perior-bital edema secondary to STI571 (Gleevec). Cancer 95(4):881–887
13. Esmaeli B, Prieto VG, Gonnering R, et al (2004) Growth factor receptor expression in orbital lymphangioma: pos-sible therapeutic implications. Orbit 23(4):263–269
14. Esmaeli B, McLaughlin P, Pro B, et al (2009) Prospective trial of targeted radioimmunotherapy with Y-90 ibritu-momab tiuxetan (Zevalin) for front-line treatment of early-stage extranodal indolent ocular adnexal lymphoma. Ann Oncol (Epub ahead of print)
15. Feugier P, Van Hoof A, Sebban C, et al (2005) Long-term results of the R-CHOP study in the treatment of elderly patients with diff use large B-cell lymphoma: a study by the Groupe d’Etude des Lymphomes de l’Adulte. J Clin Oncol 23:4117–4126
16. Fisher RI, Gaynor ER, Dahlberg S, et al (1993) Comparison of a standard regimen (CHOP) with three intensive che-motherapy regimens for advanced non-Hodgkin’s lym-phoma. N Engl J Med 328:1002–1006
17. Gold KA, Lee HY, Kim ES (2009) Targeted therapies in squamous cell carcinoma of the head and neck. Cancer 115(5):922–935
18. Ho HH, Savar A, Samaniego F, Manning J, Kasyan A,Pro B, Esmaeli B (2009) Treatment of benign lymphoid hyperpla-sia of the orbit with rituximab. Ophthal Plast Reconstr Surg (in press)
19. Ivan D, Prieto VG, Esmaeli B, Wistuba II,Tang X, Lazar AJF (2009) Epidermal growth factor receptor (EGFR) expression in ocular and extraocular sebaceous gland car-cinomas. J Cutan Pathol (July 2009), Epub ahead of print
20. Knox SJ, Goris ML, Trisler K, et al (1996) Yttrium-90-labeled anti-CD20 monoclonal antibody therapy of recur-rent B-cell lymphoma. Clin Cancer Res 2(3):457–470
21. Mac Manus MP, Hoppe RT. (1996) Is radiotherapy curative for stage I and II low-grade follicular lymphoma? Results of a long-term follow-up study of patients treated at Stanford University. J Clin Oncol 14:1282–1290
22. Normanno N, De Luca A, Bianco C, et al (2006) Epidermal growth factor receptor (EGFR) signaling in cancer. Gene 366(1):2–16
23. On AV, Hirschbein MJ, Williams HJ, et al (2006) CyberKnife radiosurgery and rituximab in the successful management of sclerosing idiopathic orbital infl ammatory disease. Ophthal Plast Reconstr Surg 22(5):395–397
24. Reff ME, Carner K, Chambers KS, et al (1994) Depletion of B cells in vivo by a chimeric mouse human monoclonal antibody to CD20. Blood 83(2):435–445
25. Salvi M, Vannucchi G, Campi I, et al (2007) Treatment of Graves’ disease and associated ophthalmopathy with the anti-CD20 monoclonal antibody rituximab: an open study. Eur J Endocrinol 156(1):33–40
26. Shepler TR, Prieto VG, Diba R, et al (2006) Expression of the epidermal growth factor receptor in conjunctival squamous cell carcinoma. Ophthal Plast Reconstr Surg 22(2):113–115
27. Shome D, Esmaeli B (2008) Targeted monoclonal antibody therapy and radioimmunotherapy for lymphoproliferative disorders of the ocular adnexa. Curr Opin Ophthalmol 19(5):414–421
28. Sullivan TJ, Grimes D, Bunce I (2004) Monoclonal anti-body treatment of orbital lymphoma. Ophthal Plast Reconstr Surg 20(2):103–106

References 193
29. Tedder TF, Engel P (1994) CD20: a regulator of cell-cycle progression of B lymphocytes. Immunol Today 15(9): 450–454
30. Tullo AB, Esmaeli B, Murray PI, Bristow E, Forsythe BJ, Faulkner K (2005) Ocular findings in patients with solid tumours treated with the epidermal growth factor receptor tyrosine kinase inhibitor gefitinib (“Iressa,” ZD1839) in phase I and II clinical trials. Eye 19: 729–738
31. Vigna E, Lucia E, Gentile M, et al (2008) PDGFRalpha/FIP1L1-positive chronic eosinophilic leukemia presenting with retro-orbital localization: effi cacy of imatinib treat-ment. Cancer Chemother Pharmacol 61(4):713–716
32. Witzig TE, Gordon LI, Cabanillas F, et al (2002) Randomized controlled trial of yttrium-90-labeled ibritu-momab tiuxetan radioimmunotherapy versus rituximab immunotherapy for patients with relapsed or refractory low-grade, follicular, or transformed B-cell non-Hodgkin’s lymphoma. J Clin Oncol 20(10):2453–2463
33. Witzig TE, Inwards DJ, Habermann TM, et al (2007) Treatment of benign orbital pseudolymphomas with the monoclonal anti-CD20 antibody rituximab. Mayo Clin Proc 82(6):692–699
34. Esmaeli B, Diba R, Ahmadi MA, et al (2004) Periorbital edema and epiphora as ocular side eff ects of imatinib mesylate (Gleevec). Eye 18:760–762
Controversies in Enucleation Technique and Implant Selection: Whether to Wrap, Attach Muscles, and Peg?David R. Jordan and Stephen R. Klapper
Chapter 14
14
Core Messages
Th e advent of porous orbital implants has greatly ■
advanced the fi eld of anophthalmic surgery.Th e development of hydroxyapatite (HA) implants ■
initiated a new generation of porous implants. Porous polyethylene and aluminum oxide are now commonly used alternatives.Orbital implants are available in spherical, ■
mounded, egg, and conical shapes.Implant material selection is determined by sev- ■
eral factors, including patient age and medical history, cost, availability, and surgeon preference.A variety of techniques may be utilized to deter- ■
mine the appropriate implant size. Adults under-going enucleation surgery most frequently require a 20- to 22-mm sphere, whereas 18- to 20-mm spherical implants may be adequate for evisceration procedures.Patients younger than 5 years old typically receive ■
a nonporous implant as this facilitates replacement with a larger porous implant later in childhood or adolescence. Older pediatric patients may do well with porous implants. Appropriate implant size
selection depends on the age and development of the patient.Surgeons who use porous polyethylene as their ■
implant of choice commonly do not use an implant-wrapping material. Wrapping HA and aluminum oxide implants facilitates implant insertion and rectus muscle attachment to the implant.Several implant-wrapping materials are commer- ■
cially available. Polyglactin 910 (Vicryl®) is simple to use, is readily available, and may permit earlier implant fi brovascularization than other available materials.Porous implants can be coupled to the overlying ■
artifi cial eye with a titanium peg system. Th ese coupling systems may allow for greater prosthesis motility. Implant peg use has declined due to the high incidence of postpegging complications (increased discharge, recurrent pyogenic granu-lomas, implant exposure around the peg, implant infection, tissue overgrowth, clicking).
14.1 Introduction
Th e introduction of coralline HA orbital implants in the mid- to late 1980s following enucleation, evisceration, or as a secondary orbital implant introduced a new era of anophthalmic socket surgery. Over the past three decades, several other porous implant materials have been intro-duced as alternatives (e.g., synthetic HA, porous polyeth-ylene, aluminum oxide). A variety of orbital implant
wraps have also entered the market over this same period. Implant wraps facilitate entry of the implant (decrease tissue drag), allow extraocular muscle attachment, and may provide a barrier function over the spiculated porous implant surface. Th ere is some debate whether covering the anterior surface of the implant with an avascular material is helpful in preventing implant exposure, and some investigators have questioned whether an implant wrap is advantageous.
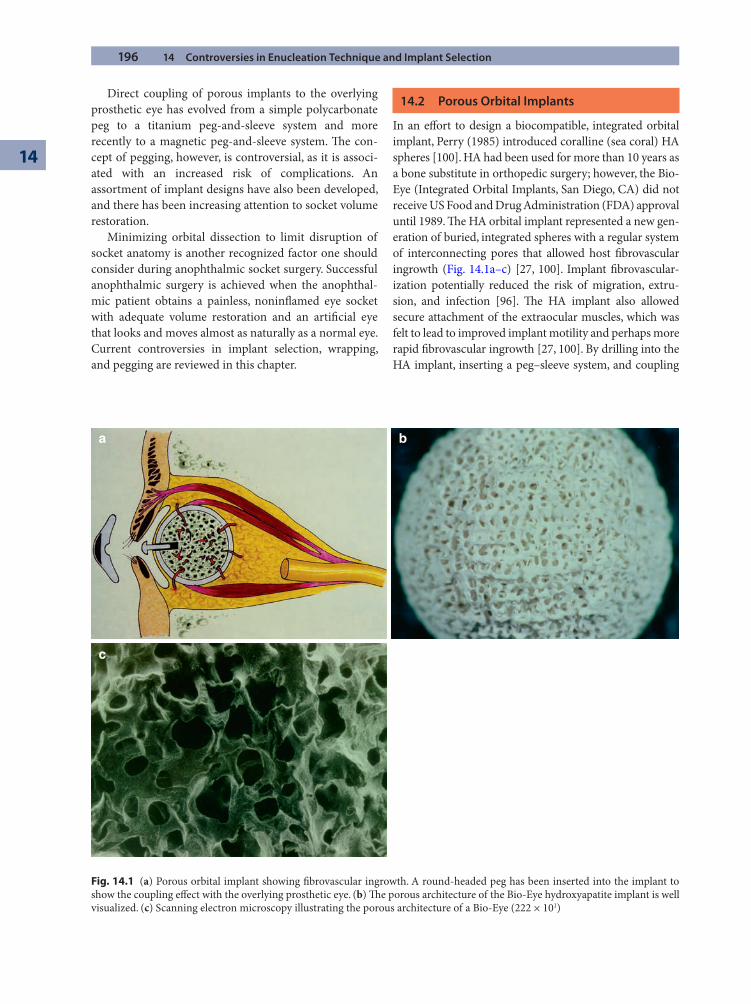
196 14 Controversies in Enucleation Technique and Implant Selection
14
Direct coupling of porous implants to the overlying prosthetic eye has evolved from a simple polycarbonate peg to a titanium peg-and-sleeve system and more recently to a magnetic peg-and-sleeve system. Th e con-cept of pegging, however, is controversial, as it is associ-ated with an increased risk of complications. An assortment of implant designs have also been developed, and there has been increasing attention to socket volume restoration.
Minimizing orbital dissection to limit disruption of socket anatomy is another recognized factor one should consider during anophthalmic socket surgery. Successful anophthalmic surgery is achieved when the anophthal-mic patient obtains a painless, noninfl amed eye socket with adequate volume restoration and an artifi cial eye that looks and moves almost as naturally as a normal eye. Current controversies in implant selection, wrapping, and pegging are reviewed in this chapter.
14.2 Porous Orbital Implants
In an eff ort to design a biocompatible, integrated orbital implant, Perry (1985) introduced coralline (sea coral) HA spheres [100]. HA had been used for more than 10 years as a bone substitute in orthopedic surgery; however, the Bio-Eye (Integrated Orbital Implants, San Diego, CA) did not receive US Food and Drug Administration (FDA) approval until 1989. Th e HA orbital implant represented a new gen-eration of buried, integrated spheres with a regular system of interconnecting pores that allowed host fi brovascular ingrowth (Fig. 14.1a–c) [27, 100]. Implant fi brovascular-ization potentially reduced the risk of migration, extru-sion, and infection [96]. Th e HA implant also allowed secure attachment of the extraocular muscles, which was felt to lead to improved implant motility and perhaps more rapid fi brovascular ingrowth [27, 100]. By drilling into the HA implant, inserting a peg–sleeve system, and coupling
a b
c
Fig. 14.1 (a) Porous orbital implant showing fi brovascular ingrowth. A round-headed peg has been inserted into the implant to show the coupling eff ect with the overlying prosthetic eye. (b) Th e porous architecture of the Bio-Eye hydroxyapatite implant is well visualized. (c) Scanning electron microscopy illustrating the porous architecture of a Bio-Eye (222 × 101)

14.2 Porous Orbital Implants 197
the peg to the overlying prosthetic eye, an improved range of prosthetic movement as well as fi ne darting eye movements (commonly seen during close conversational speech) oft en resulted. Th is allowed a more lifelike quality to the artifi cial eye. In addition, it was postulated the peg may help sup-port the weight of the prosthesis, which in turn would help decrease the risk of progressive lower lid laxity and malposi-tion associated with long-term prosthesis wear.
Although HA implants represented a signifi cant advance in anophthalmic surgery, experience with HA over the last two decades has expanded our understanding of the limita-tions of HA. Reported complications are not uncommon and include implant exposure, conjunctival thinning, socket discharge, pyogenic granuloma formation, implant infection, and persistent pain or discomfort [23, 33, 52, 74, 96, 98, 104, 108, 120]. Implant exposure problems continue to deter some surgeons from using HA implants, but this complication largely appears to be related more to surgical implantation and wound closure techniques (including implant wrap selection) and host factors than properties related to HA spherical implants [60, 96, 116, 120].
Th e introduction of HA as an orbital implant signifi -cantly raised the costs associated with enucleation, evis-ceration, and secondary orbital implant procedures. Th e Bio-Eye HA implant currently costs US $695, whereas more traditional silicone or polymethylmethacrylate (PMMA) spherical implants cost less than US $25. Additional expenses associated with HA placement may include an implant wrap material, assessment of implant vascularization with a confi rmatory magnetic resonance (MR) imaging study, a secondary drilling procedure with peg–sleeve placement, and prosthesis modifi cation. In the search for porous orbital implants with a reduced complication profi le and diminished surgical and postop-erative costs, numerous alternative implant materials have been introduced around the world.
Synthetic HA implants developed by FCI (Issy-Les-Moulineaux, Cedex, France) are currently in their third generation (FCI3). Th e FCI3 implant has an identical chem-ical composition to that of the Bio-Eye, although scanning electron microscopy (SEM) has revealed decreased pore uniformity and interconnectivity and the presence of blind pouches [87]. Central implant fi brovascularization in a rabbit model still appears to occur in a similar manner in both the Bio-Eye and FCI3 implants [63]. Th e synthetic FCI3 implant has gained in popularity in many parts of the world over the past 10 years; however, it is not yet available in the United States as a result of patent restrictions. Th e problems and complications associated with the synthetic FCI3 implant are similar to that of the Bio-Eye [49]. It is less expensive than the Bio-Eye (approximately US $450), which appears to be its only real advantage.
Other forms of HA implants in use around the world include the Chinese HA and the Brazilian HA [57, 64]. Although less expensive than the Bio-Eye, these implants have impurities or a poor porous structure that is prob-lematic. Other implant designs continue to appear, some of which seem to off er few advantages [51], while others have only been in use for a short time, and their advan-tages or disadvantages are not yet apparent [78].
Synthetic porous polyethylene (MEDPOR®, Porex Surgical, Fairburn, GA, USA) implants (a porous type of plastic) were introduced over a decade ago for use in the orbit and have been widely accepted as an alternative to the Bio-Eye HA [4, 9, 71, 92, 105]. Porous polyethylene implants, although less biocompatible than HA, are typi-cally well tolerated by orbital soft tissue [88]. Th ey have a smoother surface than HA implants, which permits easier implantation and potentially less irritation of the overlying conjunctiva following placement (Fig. 14.2a, b). Th ese implants have a high tensile strength yet are malleable, which allows sculpting of the anterior surface of the implant. Th ey may be used with or without a wrapping material, and
b
a
Fig. 14.2 (a) Th e pores within a porous polyethylene implant are more like channels than pores. (b) Scanning electron micros-copy illustrating the numerous channels within the porous poly-ethylene implant (222 × 101)

198 14 Controversies in Enucleation Technique and Implant Selection
14
the extraocular muscles can be sutured directly onto the implant, although many surgeons fi nd this challenging without predrilled holes. Porous polyethylene implants are available in spherical, egg, conical, and mounded shapes (MEDPOR Quad implant) [4, 71, 86, 92, 105]. Th e anterior surface can also be manufactured with a smooth, nonpo-rous surface to prevent abrasion of the overlying tissue (e.g., MEDPOR smooth surface tunnel implant, SST™) while retaining a larger pore size posteriorly to potentially facili-tate fi brovascular ingrowth. Despite these numerous modi-fi cations, signifi cant complications may still occur, including implant exposure and implant infection, potentially requir-ing explantation [2, 16, 92]. Th e traditional MEDPOR sphere implant costs approximately US $200 less than the Bio-Eye HA sphere. Th e newer-generation porous polyeth-ylene implant designs are more expensive. Th e MEDPOR Quad implant is US $520, and the MEDPOR SST is US $650.
Aluminum oxide (Al2O3, alumina, Bioceramic implant) is a ceramic implant biomaterial that has been used in ortho-pedic surgery and dentistry for more than 30 years. Spherical and egg-shaped Bioceramic Orbital Implants (FCI Ophthalmics, marshfi eld Hills, MA, USA) were approved for use in the United States by the FDA in April 2000 and for use in Canada by Health and Welfare Canada in February 2001. Aluminum oxide is a porous, inert sub-stance and has been suggested as a standard reference material in studies of implant biocompatibility [15, 18]. Th ese implants permit host fi brovascular ingrowth similar to the Bio-Eye [18, 62]. Human fi broblasts and osteoblasts proliferate more rapidly on aluminum oxide than HA, sug-gesting it is a more biocompatible substance than HA [15, 16, 18]. Th e Bioceramic implant is lightweight, has a uni-form pore structure, and has excellent pore interconnec-tivity (Fig. 14.3a, b) [87]. Th e microcrystalline structure is smoother than the rough-surfaced Bio-Eye (Fig. 14.3c).
a b
c
Fig. 14.3 (a) Th e porous architecture of an aluminum oxide (Bioceramic) implant is well visualized. (b) Scanning electron microscopy illustrating the more uniform porous architecture of the aluminum oxide orbital implant (222 × 101). (c) On high-power scanning electron microscopy (230 × 103), the solid component of the Bio-Eye (left half of photo) has a rough-appearing microcrystalline struc-ture compared to the smooth-appearing microcrystalline structure of the aluminum oxide (Bioceramic) implant (right half of photo)

14.3 Orbital Implant Selection in Adults 199
In our experience, anophthalmic sockets reconstructed with aluminum oxide implants appear to have less postop-erative tissue infl ammation than sockets in which HA implants have been placed [56]. Problems (e.g., exposure) encountered with its use are similar to those seen with other porous implants [9, 55, 62, 115]. Th e more inert nature of these implants is a potentially critical advantage in minimizing socket infl ammation. As with other cur-rently available porous orbital implants, aluminum oxide is less expensive than the Bio-Eye (an unwrapped Bioceramic implant is US $450, a Vicryl mesh-wrapped Bioceramic implant is US $495).
14.3 Orbital Implant Selection in Adults
Th ere continues to be little consensus regarding orbital implant material and design preference [115]. Surgeons have their own preferences regarding the use of spherical versus shaped, wrapped versus unwrapped, and pegged versus unpegged implants. Implant cost, insurance reim-bursement, and marketing pressures also have a role in implant selection. In a 2004 survey of orbital surgeons, of 1,919 primary orbital implants used following enucle-ation, porous polyethylene was used in 42.7% of cases, followed by coralline HA (27.3%), nonporous alloplastic (PMMA, silicone) implants (19.9%), dermis fat graft s (7.2%), Bioceramic (1.8%), synthetic HA (0.9%), and mammalian bone (0.2%) [110]. Th e trends reported in this survey are refl ective of a usage pattern in those responding to a nonrandom survey with a 31.4% response rate and do not suggest clinical superiority based on sci-entifi c evidence or statistical analysis [110].
When deciding which implant to use in an adult patient, we divide the various implants into three useful categories:
1. Porous spheres that may potentially be pegged (e.g., coralline or synthetic HA, porous polyethylene MEDPOR, aluminum oxide Bioceramic).
2. Quasi-integrated implants (e.g., mounded PMMA Universal implant, mounded porous polyethylene Quad MEDPOR) [3, 4, 48, 86].
3. Traditional nonporous sphere (e.g., PMMA, silicone).
If the patient is healthy and roughly between the ages of 15 and 65 years old, a porous implant (aluminum oxide, HA) that can potentially be pegged is our fi rst choice. Th e porous implant with a peg will be associated with the highest degree of movement [34, 115]. If a peg is not being considered, the advantages of using a porous spher-ical implant are diminished as the movement associated with a nonpegged porous spherical implant is equal to that of a wrapped nonporous spherical implant [17, 21, 24]. However, the advantages of fi brovascular ingrowth and the potentially diminished risk of implant migration remain substantial reasons to consider using a porous implant even when pegging is not contemplated [102]. Trichopoulos and Augsburger reported implant migra-tion in 11 of 68 nonporous implant cases (16.2%) but in only 1 of 190 porous cases (0.5%) [114]. Implant migra-tion was associated with poor prosthetic motility and suboptimal cosmesis due to enophthalmos and deep superior sulcus deformity in all cases [114].
A quasi-integrated implant such as the Universal (mounded PMMA) or MEDPOR Quad implant (mounded) is an alternative consideration to the porous spherical implants if pegging is not a consideration but potentially improved motility is desired. Th e mounded surface of the Universal or MEDPOR Quad implant off ers improved motility over a standard sphere as a result of the indirect coupling that occurs between the mounds on the implant and the posterior surface of the prosthesis. Proper placement and meticulous closure of the Tenon capsule and conjunctiva are essential when using one of these mounded implants [4, 86]. Diffi culty putting these implants into the socket and the risk of exposure deter many from using them. Th e PMMA mounded implant is signifi cantly less expensive (US $275) than HA, porous polyethylene, or aluminum oxide.
A nonporous sphere (e.g., PMMA, silicone), wrapped, centered within the muscle cone, and attached to each of the rectus muscles is another alternative if pegging is not a consideration and budgetary restraints limit the use of porous implants. Although reasonable prosthetic
Summary for the Clinician
Porous orbital implants permit fi brovascular ■
ingrowth. Implant fi brovascularization poten-tially reduces the risk of migration, extrusion, and infection.HA (Bio-Eye), porous polyethylene (MEDPOR), ■
and aluminum oxide (alumina, Bioceramic) are currently the most widely accepted porous orbital implant materials.Complications with porous orbital implants are ■
uncommon and include exposure and infection.Porous orbital implants permit direct coupling of ■
the implant to an overlying prosthesis. Peg sys-tems are the most commonly utilized coupling mechanism.

200 14 Controversies in Enucleation Technique and Implant Selection
14
movement occurs in most cases, motility of the artifi cial eye is limited compared to that oft en observed following placement of a buried, mounded implant or a porous pegged implant. Because prosthetic movement is only passively coupled to the buried sphere, the artifi cial eye may lag behind the contralateral normal eye on attempted horizontal or vertical gaze. A nonporous implant simply placed into the orbit, without a wrap and without connec-tion to the rectus muscles, is the least-desirable choice in our view as it off ers little movement, and the implants are prone to migrate over time, most commonly into the superotemporal space. A decentered implant can make fi tting of a custom artifi cial eye problematic.
Nonporous spherical implants are frequently consid-ered in maturing patients (seventh decade or beyond), debilitated or immunocompromized individuals, and patients with diabetes or a history of periorbital radiation therapy as they would not be good candidates to consider peg placement. A traditional nonporous sphere (e.g., PMMA, silicone) wrapped and centered in the muscle cone and connected to the rectus muscles is our typical approach. Maturing patients in good health and seeking to maximize potential prosthesis motility may be candi-dates for a quasi-integrated (or buried integrated) porous implant (e.g., Universal implant or MEDPOR Quad implant).
14.4 Orbital Implant Selection in Children
Adult orbital volume is achieved by 12–14 years of age [118]. It has also been shown in normal pediatric indi-viduals that 80% of adult orbital volume is reached by 5
years of age [8]. Historically, enucleation early in child-hood is believed to contribute to the underdevelopment of the involved orbital bone structure with secondary facial asymmetry [5, 73, 103, 112]. More recent studies have indicated that obvious secondary cosmetic facial asymmetries may not have always been a by-product of pediatric enucleation but rather a result of orbital irradia-tion early in life [11, 38, 40, 42]. It is recognized, however, that orbital soft tissue volume is a critical determinant of orbital bone growth, and that adequate volume replace-ment following enucleation is a critical factor in contin-ued orbital growth [11, 30, 72, 118]. Th e ocular prosthesis is also believed to be an important factor in minimizing orbital growth retardation and preventing periorbital asymmetries [36].
Our current approach in children less than 5 years of age undergoing enucleation surgery is to place a wrapped, nonporous sphere implant (e.g., PMMA, silicone), gener-ally at least 16- or 18-mm diameter centered within the muscle cone and connected to each of the rectus muscles and the inferior oblique muscle. Implant exchange, typi-cally with a larger porous orbital implant, can be consid-ered in the teenage years.
Another option for volume replacement in children (less than 5 years) is autogenous dermis fat graft s. Th ese graft s may undergo hypertrophy and perhaps contribute to orbital bone growth [36, 89, 91, 97]. Dermis fat graft s have traditionally been used most frequently aft er extru-sion of an orbital implant or removal of a migrated implant if there is some loss of conjunctival tissues and shortened furnaces. Conjunctival epithelium will migrate over the anterior surface of the dermis fat graft and potentially expand the conjunctival surface area. Disadvantages of dermis fat graft s include an unpredict-able rate of absorption with resulting superior sulcus deformity and orbital volume defi ciency. In addition, there is little or no transfer of eye socket movement to the overlying prosthesis, resulting in an artifi cial eye with little natural motility.
Formerly in children between the ages of 5 and 15 years, we have advocated nonporous implants, either a PMMA mounded implant (e.g., Universal) or a wrapped sphere (e.g., PMMA, silicone). As with younger patients, implant exchange with a porous orbital implant was then considered at a later time. Th e main reason for this was that we do not feel children younger than 15 years of age are good candidates for pegs. Regular follow-up visits and proper prosthesis care are important components for maintaining a healthy peg. In our experience, children oft en do not adequately care for their prostheses. Since the motility obtained with a mounded implant is superior to the nonpegged spherical implant, we have generally
Summary for the Clinician
Healthy patients between 15 and 65 years old are ■
generally good candidates for a porous orbital implant following enucleation or evisceration surgery.Debilitated or immunocompromized individu- ■
als and patients with diabetes or a history of periorbital radiation should receive a nonporous implant.Nonporous spherical implants (e.g., PMMA or ■
silicone) are less expensive than the newer gen-eration of porous implants. However, nonporous implants do not permit fi brovascular ingrowth or implant–prosthesis coupling and may have a greater risk of migration or extrusion.

14.5 Volume Considerations in Orbital Implant Selection 201
advocated this type of implant [4, 86]. Th ere is now an increasing trend to use porous implants in pediatric patients [26, 44, 117]. We have successfully placed porous spherical implants following childhood (5–15 years) enu-cleation and now consider the use of HA or aluminum oxide implants in many preteen and teenage patients undergoing enucleation surgery. Pegging is not a consid-eration until the child is mature enough to take care of the prosthesis and maintain follow-up visits. Importantly, the radiopaque nature of HA on imaging and potential limi-tations on postoperative external beam irradiation are no longer signifi cant concerns or strong contraindications to the use of HA following enucleation for retinoblastoma [7, 25, 26].
14.5 Volume Considerations in Orbital Implant Selection
Removal of an eye following enucleation or evisceration creates an orbital soft tissue volume defi ciency. Insuffi cient volume replacement results in a postnucleation socket syndrome that may consist of an abnormally deep supe-rior sulcus, upper eyelid ptosis, an anophthalmic appear-ance, and lower eyelid malposition and may require a larger-than-desirable prosthesis [22, 65, 67, 113]. Proper implant volume may be determined either preoperatively or intraoperatively (enucleation cases) from the axial length of the eye or by determining the volume of fl uid the enucleated eye displaces in a graduated cylinder [22, 67, 113]. Several authors have reported considerable interpatient variability of axial length and globe volume, with globe volumes varying between 6.9 and 9.0 ml [22, 67, 113]. Kaltreider and Lucarelli have shown that the axial length minus 2 mm (or A-scan minus 1 mm) approx-imates the implant diameter for optimal volume replace-
ment in emmetropic and myopic individuals [65, 67]. Custer and Trinkaus suggested a graduated cylinder be used to measure the volume of fl uid displaced by an enu-cleated eye [22].
Approximately 70–80% of the volume of an individu-al’s normal globe should be replaced with an orbital implant [22, 67]. Th is generally allows for a prosthetic volume that is ideally 2.0 to 2.5 ml [26]. While the upper limit of prosthetic volume is around 4.0 ml, larger pros-theses oft en result in progressive lower eyelid laxity and malposition due to the weight of the prostheses on the eyelid and the projection of the anterior surface of the artifi cial eye. Larger prostheses may also have limited socket excursion [65]. An 18-mm sphere has a volume of 3.1 mm, a 20-mm sphere has a volume of 4.2 ml, and a 22-mm sphere has a volume of 5.6 ml. Th eoretically, the volume of the enucleated globe minus 2.0–2.5 ml gives the ideal implant size to use [22]. Th e calculated implant size is oft en greater than 22 mm with this technique. Unfortunately, implants larger than 22 mm may have a higher exposure rate and if too large will hinder fi tting of an acceptable custom prosthesis [74, 113]. In most adults, we typically use 20- to 22-mm spherical implants follow-ing enucleation and 18- to 20-mm implants aft er evis-ceration procedures. In pediatric patients, slightly smaller implants may be required depending on the patient’s age and orbital development. Individualization of the implant size is important in optimizing orbital volume replace-ment and in achieving the best possible aesthetic result [22, 65–67, 113].
Summary for the Clinician
Approximately 80% of adult orbital volume is ■
achieved by 5 years of age.Adequate volume replacement with an appropri- ■
ately sized implant and overlying prosthesis is believed to be a critical determinant of contin-ued orbital bone development.Children under the age of 5 typically receive a ■
nonporous orbital implant that can be replaced later in life with a porous implant.Pediatric patients older than 5 may be candidates ■
for porous orbital implants.
Summary for the Clinician
Insuffi cient orbital soft tissue volume replace- ■
ment following enucleation may result in an abnormally deep superior sulcus, upper eyelid ptosis, an enophthalmic appearance, and lower eyelid malposition and may require a larger-than-desirable prosthesis.It is estimated that 80% of the volume of an indi- ■
vidual’s normal globe should be replaced with an orbital implant. Th e artifi cial eye volume is ide-ally 2.0–2.5 ml.A variety of formulas and techniques have been ■
suggested to calculate the recommended implant size. Generally, most adults should typically receive a 20- to 22-mm spherical implant follow-ing enucleation and an 18- to 20-mm implant aft er an evisceration procedure.

202 14 Controversies in Enucleation Technique and Implant Selection
14
14.6 Orbital Implant Wrapping and Attaching Extraocular Muscles
Placement of an HA implant or Bioceramic implant within the soft tissue of the eye socket is facilitated by a smooth wrapping material that diminishes tissue drag [100]. Th e wrap material facilitates precise fi xation of the extraocular muscles to the implant surface [27, 100]. Implant wraps may also provide a barrier function over the spiculated porous implant surface [27, 100], although there is some debate among ophthalmic plastic surgeons whether cov-ering the anterior surface of the implant with an avascular material is helpful in preventing implant exposure [81, 85, 101, 102, 114]. Avoiding autologous/homologous tissue donor materials eliminates the theoretical risk of immu-nologic reactions and transmission of infectious agents, and it is less expensive if the cost of wrapping tissue is avoided and operating time is diminished [114]. Another advantage of the unwrapped orbital implant is that there is no wrapping to act as a possible barrier to the fi brovascu-lar ingrowth within the porous sphere [85].
In a 2003 survey, the majority of respondents (59%) preferred not to wrap orbital implants [110]. Two previ-ous studies showed no signifi cant diff erence in exposure rates between wrapped and unwrapped porous polyethyl-ene [9, 81, 102, 114]. Trichopoulos and Augsburger [114] reported very low exposure rates (2.1%) in 190 unwrapped porous orbital implants (HA, porous polyethylene), while Perry and Tam [102] found no exposure in 21 unwrapped porous implants (HA, porous polyethylene). It has been suggested that implant wrapping may not be a protective barrier to implant exposure [114]. A potentially lower exposure rate in unwrapped implants has been attributed to more complete vascularization of the unwrapped implant as well as adherence of the rectus muscle/Tenon layer directly to the anterior surface of the implant, which may minimize wound tension [85, 111]. It may also be due to posterior implant placement and a meticulous lay-ered closure [85, 102]. Long et al. [85] demonstrated that unwrapped HA implants provide the same motility as sclera-wrapped implants. Th ey suggested a more rapid vascularization of unwrapped implants facilitated early integration of tissue in the orbit, which helped maintain the position of the extraocular muscles and ensured excellent implant motility [85]. Placement of an unwrapped implant without muscle attachment during enucleation surgery as an alternative may simplify the procedure, decrease operating room time, reduce the total cost of the procedure, avoid creating a second surgi-cal site for harvesting autogenous wraps, and eliminate the risk of disease transmission [85, 110, 111].
In contrast to some of the arguments reviewed, we advocate using an implant wrap (polyglactin 910 mesh;
Fig. 14.4a, b) material when implanting HA and alumi-num oxide spherical implants. One of the principle advan-tages of implant wraps is that they permit meticulous adherence of the rectus muscles to the implant surface. Our technique includes attachment of the rectus muscles to the implant approximately 5 mm anterior to their nor-mal anatomical position (Fig. 14.4c) [58, 60]. Th e rectus muscles end up with their insertions very close to each other. We have been advancing the medial and lateral rec-tus muscles further over the anterior implant surface so that the muscle attachment sites are nearly adjacent. It is possible that a more anterior muscle attachment helps keep the porous implant seated in good position and may facilitate fi brovascularization of the most anterior portion of the implant, which is where orbital implant exposures frequently occur. We also typically reinsert the inferior oblique muscle to the wrap just below the normal ana-tomic insertion of the lateral rectus muscle.
With secondary orbital implantation surgery (to replace a migrated or absent implant), localizing the four rectus muscles is essential to identifying the location of the mus-cle cone. Centering the implant within the muscle cone is the ideal anatomical position for a new implant. Reattaching the muscles to the wrapped implant is important as the extraocular muscles may not have been in their normal anatomic position prior to their isolation. Attachment helps keep the muscles oriented and the implant anatomi-cally centered, helping to reestablish a more natural con-junctival space and it is hoped a more comfortable and better-fi tting prosthesis. Th e centered implant with attached muscles also leads to improved prosthetic motility in most cases. A common misconception is that the extraocular muscles, once transected from the globe (in a prior enucleation procedure), retract into the orbit, pre-cluding their later localization. Fortunately, the fi brous connective tissue framework of the orbit remains intact and prevents the extraocular muscles from retracting into the posterior eye socket [46]. Th e extraocular muscles are straightforward to localize in the majority of anophthalmic sockets with or without a previously placed implant [46].
Summary for the Clinician
Advantages of orbital implant wrapping include ■
facilitating implant insertion into the socket as well as permitting simple and meticulous attachment of the rectus muscles to the implant surface.Disadvantages of orbital implant wraps include ■
additional costs and the potential barrier to implant fi brovascularization.
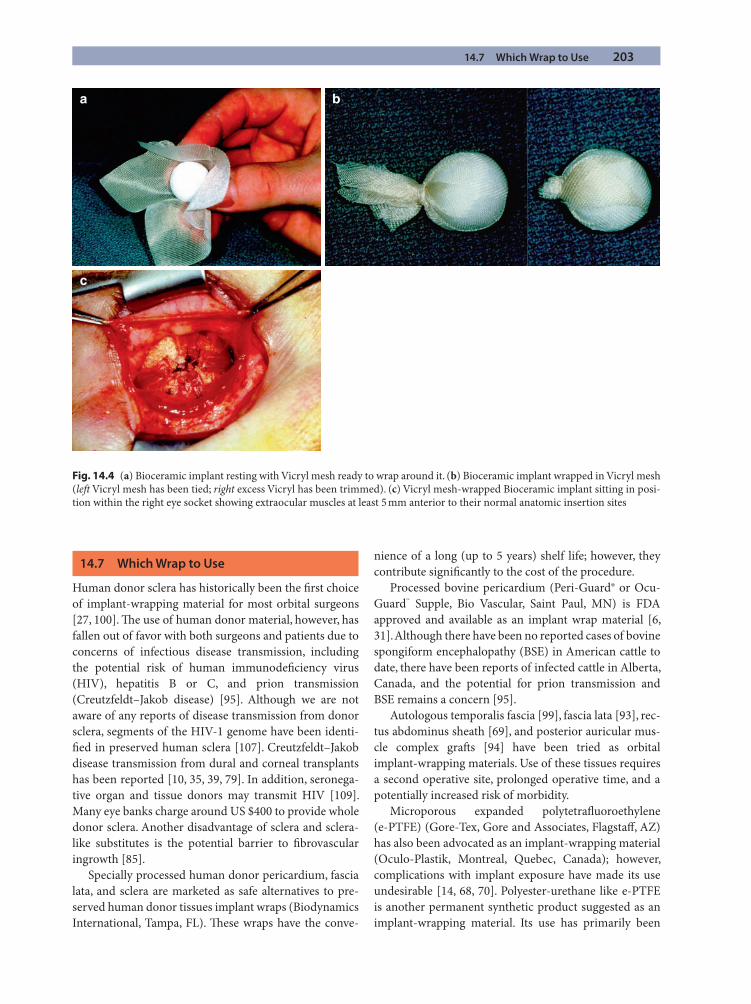
14.7 Which Wrap to Use 203
14.7 Which Wrap to Use
Human donor sclera has historically been the fi rst choice of implant-wrapping material for most orbital surgeons [27, 100]. Th e use of human donor material, however, has fallen out of favor with both surgeons and patients due to concerns of infectious disease transmission, including the potential risk of human immunodefi ciency virus (HIV), hepatitis B or C, and prion transmission (Creutzfeldt–Jakob disease) [95]. Although we are not aware of any reports of disease transmission from donor sclera, segments of the HIV-1 genome have been identi-fi ed in preserved human sclera [107]. Creutzfeldt–Jakob disease transmission from dural and corneal transplants has been reported [10, 35, 39, 79]. In addition, seronega-tive organ and tissue donors may transmit HIV [109]. Many eye banks charge around US $400 to provide whole donor sclera. Another disadvantage of sclera and sclera-like substitutes is the potential barrier to fi brovascular ingrowth [85].
Specially processed human donor pericardium, fascia lata, and sclera are marketed as safe alternatives to pre-served human donor tissues implant wraps (Biodynamics International, Tampa, FL). Th ese wraps have the conve-
nience of a long (up to 5 years) shelf life; however, they contribute signifi cantly to the cost of the procedure.
Processed bovine pericardium (Peri-Guard® or Ocu-Guard™ Supple, Bio Vascular, Saint Paul, MN) is FDA approved and available as an implant wrap material [6, 31]. Although there have been no reported cases of bovine spongiform encephalopathy (BSE) in American cattle to date, there have been reports of infected cattle in Alberta, Canada, and the potential for prion transmission and BSE remains a concern [95].
Autologous temporalis fascia [99], fascia lata [93], rec-tus abdominus sheath [69], and posterior auricular mus-cle complex graft s [94] have been tried as orbital implant-wrapping materials. Use of these tissues requires a second operative site, prolonged operative time, and a potentially increased risk of morbidity.
Microporous expanded polytetrafl uoroethylene (e-PTFE) (Gore-Tex, Gore and Associates, Flagstaff , AZ) has also been advocated as an implant-wrapping material (Oculo-Plastik, Montreal, Quebec, Canada); however, complications with implant exposure have made its use undesirable [14, 68, 70]. Polyester-urethane like e-PTFE is another permanent synthetic product suggested as an implant-wrapping material. Its use has primarily been
a b
c
Fig. 14.4 (a) Bioceramic implant resting with Vicryl mesh ready to wrap around it. (b) Bioceramic implant wrapped in Vicryl mesh (left Vicryl mesh has been tied; right excess Vicryl has been trimmed). (c) Vicryl mesh-wrapped Bioceramic implant sitting in posi-tion within the right eye socket showing extraocular muscles at least 5 mm anterior to their normal anatomic insertion sites

204 14 Controversies in Enucleation Technique and Implant Selection
14
associated with neurosurgery as a dural substitute [37]. When implanted into the orbit as a wrapping material, it was associated with a marked infl ammatory reaction with infi ltration of foreign body giant cells and a high (46%) exposure rate [37].
Undyed polyglactin 910 mesh (Vicryl mesh, Ethicon, Somerville, NJ) is a bioabsorbable synthetic material and our preference as a wrapping material for HA and Bioceramic orbital implants [47, 68] (Fig. 14.4a, b). Polyglactin mesh off ers numerous advantages over other currently available materials. Vicryl mesh eliminates the risk of infectious disease transmission, does not require a second surgical site, is readily available, and is technically simple to use. Th e cost is approximately US $290 per sheet. Polyglactin has a multiporous structure that allows fi brovascular ingrowth over the entire surface of the implant [77]. It provides a minimal barrier to vasculariza-tion as opposed to sclera or other donor tissues. In a rab-bit model, the degree of vascularization was greater in the fi rst 12 weeks in Vicryl mesh-wrapped implants than sclera-wrapped implants on both histopathologic and MR imaging studies [47, 54]. We have reported a 2.1% incidence of implant exposure in 187 consecutive patients receiving Vicryl mesh-wrapped HA orbital implants [32]. With refi nements in implant placement technique, our incidence of exposure is now less than 1% (unpublished data). Importantly, Bioceramic implants wrapped with Vicryl mesh only cost US $50 more than unwrapped implants.
Oestreicher et al. [98] reported a low exposure inci-dence using a similar bioabsorbable wrapping material composed of polyglycolic acid (Dexon mesh style no. 8, nonstretch, medium-weight closed tricot, Davis and Geck, Manati, Puerto Rico). Despite our success with polyglactin 910 mesh as an implant wrap material, some surgeons continue to believe that it is associated with a higher rate of implant exposure [19, 20, 60]. It remains our view that high exposure rates with Vicryl mesh-wrapped implants are technique related and can be sig-nifi cantly minimized with correct implant insertion and meticulous tension-free wound closure [58, 60]. In an attempt to limit the risk of implant exposure, a small 1.5 × 1.5 cm sclera patch has been added to the anterior surface of polyglactin-wrapped implants by some sur-geons [116, 117]. Wang et al. compared the exposures in Vicryl mesh-wrapped implants to Vicryl mesh-wrapped implants with an additional sclera patch graft . No expo-sures occurred in the implants capped by the sclera patch compared to 2 (11.7%) in the Vicryl mesh-only implants without a sclera patch [116]. Inkster et al. also reported using a similar technique (i.e., a sclera patch graft to cover a sclera-wrapped HA implant). Although conjunctival
dehiscence occurred in 33% of the patients, it disappeared without further intervention, and no patient developed implant exposure in their series of 110 patients [43].
14.8 To Peg or Not to Peg Porous Implants
Infrared oculography has demonstrated objective and signifi cant improvement in horizontal gaze aft er motility peg placement [34]. Despite the improved motility, many surgeons and patients still elect to avoid peg placement due to the satisfactory results without pegging and the possibility of postpegging complications (increased dis-charge, recurrent pyogenic granulomas, implant exposure around the peg, implant infection, tissue overgrowth, clicking) [12, 28, 29, 45, 53, 80, 84, 119].
Although pegging has declined dramatically over the past few years, a precise and meticulous technique under local anesthesia with intravenous sedation in the appro-priately selected patient can be a successful outpatient procedure [59]. It is important to be selective in deciding which patients are candidates for a peg system. Proper care of the artifi cial eye and regular follow-up visits with the ocularist and ophthalmic plastic surgeon are impor-tant to help ensure minimal problems with the peg sys-tem. If the patient is unlikely, unable, or unwilling to have adequate postoperative care, then pegging should be avoided. Children under 15 years of age, adults over the age of 65 years or so, or individuals of any age with a chronic illness or vasculopathy (e.g., a collagen vascular disease, sarcoidosis, diabetes mellitus, immunosuppres-sive therapy, prior orbital radiation therapy, etc.) should not be considered for pegging.
Peg and sleeve implant–prosthesis coupling systems were generally designed for peg or sleeve placement once
Summary for the Clinician
Concern over infectious disease transmission ■
has limited the continued use of sclera and other donor materials as implant-wrapping materials.Specially processed human donor tissue may con- ■
tribute substantially to the cost of the procedure.Polyglactin 910 (Vicryl) mesh is an alternative to ■
traditional implant-wrapping materials. Vicryl mesh eliminates the risk of infectious disease transmission, does not require a second surgical site, is readily available, and is technically simple to use. Aluminum oxide implants are supplied prewrapped at minimal additional cost.
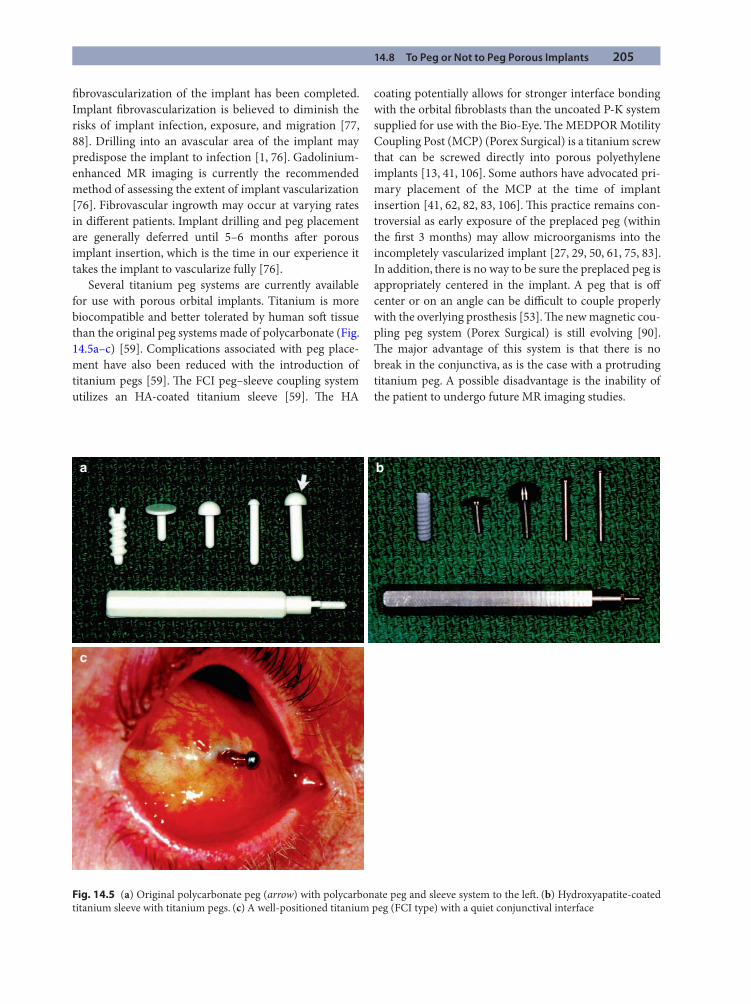
14.8 To Peg or Not to Peg Porous Implants 205
fi brovascularization of the implant has been completed. Implant fi brovascularization is believed to diminish the risks of implant infection, exposure, and migration [77, 88]. Drilling into an avascular area of the implant may predispose the implant to infection [1, 76]. Gadolinium-enhanced MR imaging is currently the recommended method of assessing the extent of implant vascularization [76]. Fibrovascular ingrowth may occur at varying rates in diff erent patients. Implant drilling and peg placement are generally deferred until 5–6 months aft er porous implant insertion, which is the time in our experience it takes the implant to vascularize fully [76].
Several titanium peg systems are currently available for use with porous orbital implants. Titanium is more biocompatible and better tolerated by human soft tissue than the original peg systems made of polycarbonate (Fig. 14.5a–c) [59]. Complications associated with peg place-ment have also been reduced with the introduction of titanium pegs [59]. Th e FCI peg–sleeve coupling system utilizes an HA-coated titanium sleeve [59]. Th e HA
coating potentially allows for stronger interface bonding with the orbital fi broblasts than the uncoated P-K system supplied for use with the Bio-Eye. Th e MEDPOR Motility Coupling Post (MCP) (Porex Surgical) is a titanium screw that can be screwed directly into porous polyethylene implants [13, 41, 106]. Some authors have advocated pri-mary placement of the MCP at the time of implant insertion [41, 62, 82, 83, 106]. Th is practice remains con-troversial as early exposure of the preplaced peg (within the fi rst 3 months) may allow microorganisms into the incompletely vascularized implant [27, 29, 50, 61, 75, 83]. In addition, there is no way to be sure the preplaced peg is appropriately centered in the implant. A peg that is off center or on an angle can be diffi cult to couple properly with the overlying prosthesis [53]. Th e new magnetic cou-pling peg system (Porex Surgical) is still evolving [90]. Th e major advantage of this system is that there is no break in the conjunctiva, as is the case with a protruding titanium peg. A possible disadvantage is the inability of the patient to undergo future MR imaging studies.
a b
c
Fig. 14.5 (a) Original polycarbonate peg (arrow) with polycarbonate peg and sleeve system to the left . (b) Hydroxyapatite-coated titanium sleeve with titanium pegs. (c) A well-positioned titanium peg (FCI type) with a quiet conjunctival interface

206 14 Controversies in Enucleation Technique and Implant Selection
14
14.9 Summary
Loss of an eye to malignancy, trauma, or end-stage ocular disease is devastating to persons of any age. Not only is there a loss of binocular vision with reduced peripheral visual fi eld and loss of depth perception with various job restrictions, but also there may be a sense of facial disfi g-urement. Since eye contact is such an essential part of human interaction, it is extremely important for the patient with an artifi cial eye to maintain a natural, normal-appearing prosthetic eye. Since 1989, there have been numerous developments and refi nements in anophthal-mic socket surgery with respect to implant material and design, implant wrapping, implant–prosthesis coupling, and socket volume considerations. Ano phthalmic surgery is no longer simply about replacing a diseased eye with an orbital implant. Ophthalmic surgeons working closely with qualifi ed ocularists must be focused on restoring a patient’s natural eye appearance with prosthetic motility as near normal as possible. We prefer implantation of a porous Bioceramic implant wrapped in polyglactin mesh. In appropriate clinical circumstances, we consider peg-ging 6–8 months aft er implant insertion. Th e technique requires a certain skill level and may not be appropriate for all implant surgeons or anophthalmic patients.
References
1. Ainbinder DJ, Haik BG, Tellado M (1994) Hydroxyapatite orbital implant abscess: histopathologic correlation of an infected implant following evisceration. Ophthal Plast Reconstr Surg 10:267–270
2. Alwitry A, West S, King J et al (2007) Long-term follow-up of porous polyethylene spherical implants aft er enucleation and evisceration. Ophthal Plast Reconstr Surg 23: 11–15
3. Anderson RL, Th iese SM, Nerad JA et al (1990) Th e uni-versal orbital implant: indications and methods. Adv Ophthalmic Plast Reconstr Surg 8:88–99
4. Anderson RL, Yen MT, Lucci LM et al (2002) Th e quasi-integrated porous polyethylene orbital implant. Ophthal Plast Reconstr Surg 18:50–55
5. Apt L, Isenberg S (1973) Changes in orbital dimensions following enucleation. Arch Ophthalmol 90:393–395
6. Arat YO, Shetlar DJ, Boniuk M (2003) Bovine pericardium versus homologous sclera as a wrapping for hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg 19:189–193
7. Arora V, Weeks K, Halperin EC et al (1992) Infl uence of coralline hydroxyapatite used as an ocular implant on the dose distribution of external beam photon radiation ther-apy. Ophthalmology 99:380–382
8. Bentley RP, Sgouros S, Natarajan K et al (2002) Normal changes in orbital volume during childhood. J Neurosurg 96:742–746
9. Blaydon SM, Shepler TR, Neuhaus RW et al (2003) Th e porous polyethylene (Medpor) spherical orbital implant: a retrospective study of 136 cases. Ophthal Plast Reconstr Surg 19:364–371
10. Brooke FJ, Boyd A, Klug GM et al (2004) Lyodura use and the risk of iatrogenic Creutzfeldt–Jakob disease in Australia. Med J Aust 180:177–181
11. Cepela MA, Nunery WR, Martin RT (1992) Stimulation of orbital growth by the use of expandable implants in the anophthalmic cat orbit. Ophthal Plast Reconstr Surg 8: 157–167
12. Cheng MS, Liao SL, Lin LL (2004) Late porous polyethyl-ene implant exposure aft er motility coupling post place-ment. Am J Ophthalmol 138:420–424
13. Choi JC, Iwamoto MA, Bstandig S et al (1999) Medpore motility coupling post: a rabbit model. Ophthal Plast Reconstr Surg 15:190–201
14. Choo PH, Carter SR, Crawford JB et al (1999) Exposure of expanded polytetrafl uoroethylene-wrapped hydroxyapa-tite orbital implant: a report of two patients. Ophthal Plast Reconstr Surg 15:77–78
15. Christel P (1992) Biocompatibility of alumina. Clin Orthop 282:10–18
16. Chuo JY, Dolman PJ, Ng TL et al (2009) Clinical and histo-pathologic review of 18 explanted porous polyethylene orbital implants. Ophthalmology 116:349–354
17. Colen TP, Paridaens DA, Lemij HG et al (2000) Com-parison of artifi cial eye amplitudes with acrylic and hydroxyapatite spherical enucleation implants. Ophthal-mology 107: 1889–1894
18. Cook S, Dalton J (1992) Biocompatibility and biofunction-ality of implanted materials. Alpha Omegan 85:41–47
Summary for the Clinician
It is generally accepted that direct coupling of an ■
orbital implant to an overlying prosthesis enhances both objective and subjective artifi cial eye motility.Titanium peg/sleeve implant–prosthesis cou- ■
pling systems are utilized with HA and alumi-num oxide implants. Th e MEDPOR MCP is a titanium screw that can be screwed directly into porous polyethylene implants.Most surgeons defer peg placement until implant ■
fi brovascular ingrowth has been completed, usually at least 6 months following implant placement.Postpegging socket complications remain a sig- ■
nifi cant obstacle to wide acceptance of current implant–prosthesis coupling systems.
References 207
19. Custer PL (2000) Enucleation: past, present, and future. Ophthal Plast Reconstr Surg 16:316–321
20. Custer PL (2001) Reply to Dr. D.R. Jordan’s letter on polyg-lactin mesh wrapping of hydroxyapatite implants. Ophthal Plast Reconstr Surg. 17:222–223
21. Custer PL, Kennedy RH, Woog JJ et al (2003) Orbital implants in enucleation surgery: a report by the American Academy of Ophthalmology. Ophthalmology 110:2054–2061
22. Custer PL, Trinkaus KM (1999) Volumetric determination of enucleation implant size. Am J Ophthalmol 128: 489–494
23. Custer PL, Trinkaus KM (2007) Porous implant exposure: incidence, management, and morbidity. Ophthal Plast Reconstr Surg 23:1–7
24. Custer PL, Trinkaus KM, Fornoff J (1999) Comparative motility of hydroxyapatite and alloplastic enucleation implants. Ophthalmology 106:513–516
25. DePotter P, Shields CL, Shields JA et al (1992) Role of mag-netic resonance imaging in the evaluation of the hydroxy-apatite orbital implant. Ophthalmology 99:824–830
26. DePotter P, Shields CL, Shields JA et al (1994) Use of the hydroxyapatite ocular implant in the pediatric population. Arch Ophthalmol 112:208–212
27. Dutton JJ (1991) Coralline hydroxyapatite as an ocular implant. Ophthalmology 98:370–377
28. Edelstein C, Shields CL, DePotter P et al (1997) Compli-cations of motility peg placement for the hydroxyapatite orbital implant. Ophthalmology 104:1616–1621
29. Fahim DK, Frueh BR, Musch DC et al (2007) Complications of pegged and non-pegged hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg 23:206–210
30. Fountain TR, Goldberger S, Murphree AL (1999) Orbital development aft er enucleation in early childhood. Ophthal Plast Reconstr Surg 15:32–36
31. Gayre GS, DeBacker CM, Lipham W et al (2001) Bovine pericardium as a wrapping for orbital implants. Ophthal Plast Reconstr Surg 17:381–387
32. Gayre GS, Lipham W, Dutton JJ (2002) A comparison of rates of fi brovascular ingrowth in wrapped versus unwrapped hydroxyapatite spheres in a rabbit model. Ophthal Plast Reconstr Surg 18:275–280
33. Goldberg RA, Holds JB, Ebrahimpour J (1992) Exposed hydroxyapatite orbital implants: report of six cases. Oph-thalmology 99:831–836
34. Guillinta P, Vasani SN, Granet DB et al (2003) Prosthetic motility in pegged versus unpegged integrated porous orbital implants. Ophthal Plast Reconstr Surg 19:119–122
35. Heckmann JG, Lang CJ, Petruch F et al (1997) Transmission of Creutzfeldt-Jakob disease via a corneal transplant. J Neurol Neurosurg Psychiatry 63:388–390
36. Heher KL, Katowitz JA, Low JE (1998) Unilateral dermis-fat graft implantation in the pediatric orbit. Ophthal Plast Reconstr Surg 14:81–88
37. Heimann H, Bechrakis NE, Zepeda LC et al (2005) Exposure of orbital implants wrapped with polyester-urethane aft er enucleation for advanced retinoblastoma. Ophthal Plast Reconstr Surg 21:123–128
38. Hintschich C, Zonneveld F, Baldeschi L et al (2001) Bony orbital development aft er early enucleation in humans. Br J Ophthalmol 85:205–208
39. Hogan RN, Brown P, Heck E et al (1999) Risk of prion dis-ease transmission from ocular donor tissue transplanta-tion. Cornea 18:2–11
40. Howard GM, Kinder RS, Macmillan AS Jr. (1965) Orbital growth aft er unilateral enucleation in childhood. Arch Ophthalmol 73:80–83
41. Hsu WC, Green JP, Spilker MH et al (2003) Primary place-ment of a titanium motility post in a porous polyethylene orbital implant. Ophthal Plast Reconstr Surg 16:370–379
42. Imhof SM, Mourits MP, Hofman P et al (1996) Quantifi -cation of orbital and mid-facial growth retardation aft er megavoltage external beam irradiation in children with retinoblastoma. Ophthalmology 103:263–268
43. Inkster CF, Ng SG, Leatherbarrow B (2002) Primary banked scleral patch graft in the prevention of exposure of hydroxy-apatite orbital implants. Ophthalmology 109:389–392
44. Iordanidou V, De PP (2004) Porous polyethylene orbital implant in the pediatric population. Am J Ophthalmol 138:425–429
45. Jordan DR (2001) Spontaneous loosening of hydroxyapa-tite peg sleeves. Ophthalmology 108:2041–2044
46. Jordan DR (2004) Localization of extraocular muscles dur-ing secondary orbital implantation surgery: the tunnel technique: experience in 100 patients. Ophthalmology 111:1048–1054
47. Jordan DR, Allen LH, Ells A et al (1995) Th e use of Vicryl mesh (polyglactin 910) for implantation of hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg 11:95–99
48. Jordan DR, Anderson RL, Nerad JA et al (1987) A prelimi-nary report on the universal implant. Arch Ophthalmol 105:1726–1731
49. Jordan DR, Bawazeer A (2001) Experience with 120 syn-thetic hydroxyapatite implants (FCI3). Ophthal Plast Reconstr Surg 17:184–190
50. Jordan DR, Brownstein S, Faraji H (2004) Clinicopathologic analysis of 15 explanted hydroxyapatite implants. Ophthal Plast Reconstr Surg 20:285–290
51. Jordan DR, Brownstein S, Gilberg S et al (2002) Investigation of a bioresorbable orbital implant. Ophthal Plast Reconstr Surg 18:342–348
52. Jordan DR, Brownstein S, Jolly SS (1996) Abscessed hydroxyapatite orbital implants: a report of two cases. Ophthalmology 103:1784–1787
53. Jordan DR, Chan S, Mawn L et al (1999) Complications associated with pegging hydroxyapatite orbital implants. Ophthalmology 106:505–512
208 14 Controversies in Enucleation Technique and Implant Selection
14
54. Jordan DR, Ells A, Brownstein S et al (1995) Vicryl-mesh wrap for the implantation of hydroxyapatite orbital implants: an animal model. Can J Ophthalmol 30:241–246
55. Jordan DR, Gilberg S, Bawazeer A (2004) Coralline hydroxyapatite orbital implant (bio-eye): experience with 158 patients. Ophthal Plast Reconstr Surg 20:69–74
56. Jordan DR, Gilberg S, Mawn LA (2003) Th e bioceramic orbital implant: experience with 107 implants. Ophthal Plast Reconstr Surg 19:128–135
57. Jordan DR, Hwang I, McEachren TM et al (2000) Brazilian hydroxyapatite implant. Ophthal Plast Reconstr Surg 16: 363–369
58. Jordan DR, Klapper SR (1999) Wrapping hydroxyapatite implants. Ophthalmic Surg Lasers 30:403–407
59. Jordan DR, Klapper SR (2000) A new titanium peg system for hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg 16:380–387
60. Jordan DR, Klapper SR, Gilberg SM (2003) Th e use of Vicryl mesh in 200 porous orbital implants. Ophthal Plast Reconstr Surg 19:53–61
61. Jordan DR, Klapper SR, Mawn L et al (1998) Abscess for-mation within a synthetic hydroxyapatite orbital implant. Can J Ophthalmol 33:329–332
62. Jordan DR, Mawn L, Brownstein S et al (2000) Th e biocer-amic orbital implant: a new generation of porous implants. Ophthal Plast Reconstr Surg 16:347–355
63. Jordan DR, Munro SM, Brownstein S et al (1998) A syn-thetic hydroxyapatite implant: the so-called counterfeit implant. Ophthal Plast Reconstr Surg 14:244–249
64. Jordan DR, Pelletier C, Gilberg S et al (1999) A new variety of hydroxyapatite: the Chinese implant. Ophthal Plast Reconstr Surg 15:420–424
65. Kaltreider SA (2000) Th e ideal ocular prosthesis: analysis of prosthetic volume. Ophthal Plast Reconstr Surg 16: 388–392
66. Kaltreider SA, Jacobs JL, Hughes MO (1999) Predicting the ideal implant size before enucleation. Ophthal Plast Reconstr Surg 15:37–43
67. Kaltreider SA, Lucarelli MJ (2002) A simple algorithm for selection of implant size for enucleation and evisceration. Ophthal Plast Reconstr Surg 18:336–341
68. Kao L (2000) Polytetrafl uoroethylene as a wrapping mate-rial for a hydroxyapatite orbital implant. Ophthal Plast Reconstr Surg 16:286–288
69. Kao SCS, Chen S (1999) Th e use of rectus abdominis sheath for wrapping of the hydroxyapatite orbital implants. Ophthalmic Surg Lasers 30:69–71
70. Karesh JW (1987) Polytetrafl uoroethylene as a graft mate-rial in ophthalmic plastic and reconstructive surgery: an experimental and clinical study. Ophthal Plast Reconstr Surg 3:179–185
71. Karesh JW, Dresner SC (1994) High-density porous poly-ethylene (Medpor) as a successful anophthalmic socket implant. Ophthalmology 101:1688–1695
72. Kaste SC, Chen G, Fontanesi J et al (1997) Orbital develop-ment in long-term survivors of retinoblastoma. J Clin Oncol 15:1183–1189
73. Kennedy RE (1964) Th e eff ect of early enucleation on the orbit in animals and humans. Trans Am Ophthalmol Soc 62:459–510
74. Kim YD, Goldberg RA, Shorr N et al (1994) Management of exposed hydroxyapatite orbital implants. Ophthalmology 101:1709–1715
75. Klapper SR, Jordan DR, Brownstein S et al (1999) Incomplete fi brovascularization of a hydroxyapatite orbital implant 3 months aft er implantation. Arch Ophthalmol 106:1640–1641
76. Klapper SR, Jordan DR, Ells A et al (2003) Hydroxyapatite orbital implant vascularization assessed by magnetic reso-nance imaging. Ophthal Plast Reconstr Surg. 19:46–52
77. Klapper SR, Jordan DR, Punja K et al (2000) Hydroxyapatite implant wrapping materials: analysis of fi brovascular ingrowth in an animal model. Ophthal Plast Reconstr Surg 16:278–285
78. Klett A, Guthoff R (2003) Muscle pedunculated scleral fl aps. A microsurgical modifi cation to improve prosthesis motility. Ophthalmologe 100:449–452
79. Lang CJ, Heckmann JG, Neundorfer B (1998) Creutzfeldt–Jakob disease via dural and corneal transplants. J Neurol Sci 160:128–139
80. Lee SY, Jang JW, Lew H et al (2002) Complications in motility PEG placement for hydroxyapatite orbital implant in anophthalmic socket. Jpn J Ophthalmol 46:103–107
81. Li T, Shen J, Duff y MT (2001) Exposure rates of wrapped and unwrapped orbital implants following enucleation. Ophthal Plast Reconstr Surg 17:431–435
82. Liao SL, Chen MS, Lin LL (2005) Primary placement of a titanium sleeve in hydroxyapatite orbital implants. Eye 19:400–405
83. Liao SL, Shih MJ, Lin LL (2005) Primary placement of a hydroxyapatite-coated sleeve in bioceramic orbital implants. Am J Ophthalmol 139:235–241
84. Lin CJ, Liao SL, Jou JR et al (2002) Complications of motil-ity peg placement for porous hydroxyapatite orbital implants. Br J Ophthalmol 86:394–396
85. Long JA, Tann TM, III, Bearden WH III et al (2003) Enucleation: is wrapping the implant necessary for optimal motility? Ophthal Plast Reconstr Surg 19:194–197
86. Marx DP, Vagefi MR, Bearden WH et al (2008) Th e quasi-integrated porous polyethylene implant in pediatric patients enucleated for retinoblastoma. Orbit 27:403–406
87. Mawn L, Jordan DR, Gilberg S (1998) Scanning electron microscopic examination of porous orbital implants. Can J Ophthalmol 33:203–209
88. Mawn LA, Jordan DR, Gilberg S (2001) Proliferation of human fi broblasts in vitro aft er exposure to orbital implants. Can J Ophthalmol 36:245–251
References 209
89. Migliori ME, Putterman AM (1991) Th e domed dermis-fat graft orbital implant. Ophthal Plast Reconstr Surg 7:23–30
90. Miller DM, Murray T, Suarez F et al (2007) Motility assessment and clinical outcomes of a magnetically inte-grated microporous implant. Ophthalmic Surg Lasers Imaging 38:339–341
91. Mitchell KT, Hollsten DA, White WL et al (2001) Th e autogenous dermis-fat orbital implant in children. J AAPOS 5:367–369
92. Naik MN, Murthy RK, Honavar SG (2007) Comparison of vascularization of Medpor and Medpor-Plus orbital implants: a prospective, randomized study. Ophthal Plast Reconstr Surg 23:463–467
93. Naugle TC Jr, Fry CL, Sabatier RE et al (1997) High leg inci-sion fascia lata harvesting. Ophthalmology 104:1480–1488
94. Naugle TC Jr, Lee AM, Haik BG et al (1999) Wrapping hydroxyapatite orbital implants with posterior auricular muscle complex graft s. Am J Ophthalmol 128:495–501
95. Nunery WR (2003) Risk of prion transmission with the use of xenograft s and allograft s in surgery. Ophthal Plast Reconstr Surg 17:389–394
96. Nunery WR, Heinz GW, Bonnin JM et al (1993) Exposure rate of hydroxyapatite spheres in the anophthalmic socket: histopathologic correlation and comparison with silicone sphere implants. Ophthal Plast Reconstr Surg 9:96–104
97. Nunery WR, Hetzler KJ (1985) Dermal-fat graft as a pri-mary enucleation technique. Ophthalmology 92:1256–1261
98. Oestreicher JH, Liu E, Berkowitz M (1997) Complications of hydroxyapatite orbital implants: a review of 100 con-secutive cases and a comparison of Dexon mesh (polygly-colic acid) with scleral wrapping. Ophthalmology 104: 324–329
99. Pelletier CR, Jordan DR, Gilberg SM (1998) Use of tem-poralis fascia for exposed hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg 14:198–203
100. Perry AC (1991) Advances in enucleation. Ophthal Plast Reconstr Surg 4:173–182
101. Perry JD (2003) Hydroxyapatite implants [letter]. Oph-thalmology 110:1281.
102. Perry JD, Tam RC (2004) Safety of unwrapped spherical orbital implants. Ophthal Plast Reconstr Surg 20:281–284
103. Pfi eff er RL (1945) Th e eff ect of enucleation on the orbit. Trans Am Acad Ophthalmol 49:236–239
104. Remulla HD, Rubin PAD, Shore JW et al (1995) Complications of porous spherical orbital implants. Oph-thalmology 102:586–593
105. Rubin PA, Popham J, Rumelt S et al (1998) Enhancement of the cosmetic and functional outcome of enucleation
with the conical orbital implant. Ophthalmology 105: 919–925
106. Rubin PAD, Fay AM, Remulla HD (1999) Primary place-ment of motility coupling post in porous polyethylene orbital implants. Arch Ophthalmol 118:826–832
107. Seiff SR, Chang JS Jr, Hurt MH et al (1994) Polymerase chain reaction identifi cation of human immunodefi -ciency virus-1 in preserved human sclera. Am J Ophthal-mol 118:528–529
108. Shoamanesh A, Pang N, Oestreicher JH (2007) Complications of orbital implants; a review of 542 patients who have undergone orbital implantation and 275 subsequent peg placements. Orbit 25:173–182
109. Simonds RJ, Holmberg SD, Hurwitz RL et al (1992) Transmission of human immunodefi ciency virus type 1 from a seronegative organ and tissue donor. N Engl J Med 326:726–732
110. Su GW, Yen MT (2004) Current trends in managing the anophthalmic socket aft er primary enucleation and evis-ceration. Ophthal Plast Reconstr Surg 20:274–280
111. Suter AJ, Molteno AC, Bevin TH et al (2002) Long term follow up of bone derived hydroxyapatite orbital implants. Br J Ophthalmol 86:1287–1292
112. Taylor W (1939) Eff ect of enucleation of one eye in child-hood upon subsequent development of the face. Trans Ophthalmol Soc U K 59:368–373
113. Th aller VT (1997) Enucleation volume measurement. Ophthal Plast Reconstr Surg 13:18–20
114. Trichopoulos N, Augsburger JJ (2005) Enucleation with unwrapped porous and nonporous orbital implants: a 15-year experience. Ophthal Plast Reconstr Surg 21: 331–336
115. Wang JK, Lai PC, Liao SL (2009) Late exposure of the bio-ceramic orbital implant. Am J Ophthalmol 147:162–170
116. Wang JK, Liao SL, Lai PC et al (2007) Prevention of expo-sure of porous orbital implants following enucleation. Am J Ophthalmol 143:61–67
117. Wang JK, Liao SL, Lin LL et al (2007) Porous orbital implants, wraps, and PEG placement in the pediatric pop-ulation aft er enucleation. Am J Ophthalmol 144:109–116
118. Yago K, Furuta M (2001) Orbital growth aft er unilateral enucleation in infancy without an orbital implant. Jpn J Ophthalmol 45:648–652
119. Yazici B, Akova B, Sanli O (2007) Complications of pri-mary placement of motility post in porous polyethylene implants during enucleation. Am J Ophthalmol 143: 828–834
120. Yoon JS, Lew H, Kim SJ et al. (2008) Exposure rate of hydroxy-apatite orbital implants. Ophthalmology 115:566–572

Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues: Cosmetic and Functional ConsiderationsAna M. Susana Morley and Raman Malhotra
Chapter 15
Core Messages
Orbital or periorbital volume loss may be due to ■
factors other than aging. Any sinister, progres-sive, or reversible etiology should be identifi ed and addressed prior to embarking upon volume replacement.Injectable soft -tissue fi llers off er titratable volume ■
augmentation, precise soft -tissue placement, the ability to be performed in the offi ce, biocompati-bility, low down-time, minimal morbidity, high safety and, in most cases, potential reversibility.Th e two main types of injectable soft -tissue fi llers ■
are collagen and stabilized hyaluronic acid. Th e latter can be instantly dissolved using hyaluroni-dase. Nonanimal stabilized hyaluronic acid fi llers are the most commonly used in orbital and peri-orbital volume augmentation.Fillers with larger particle size have increased viscos- ■
ity, reduced ease of injection and increased duration. On average, a medium viscosity hyaluronic acid gel will last a year when injected in a pre-periosteal plane in the periorbital region or in the orbit.Soft -tissue fi llers have been successfully used for ■
volume augmentation in the orbit (both sighted and anophthalmic), the tear trough, the upper eyelid/sub-brow region and in the brow and tem-ple region.
2 ml of hyaluronic acid fi ller, administered to the ■
orbit via an inferotemporal peribulbar injection and placed posterior to the equator of the globe or implant, usually reduces enophthalmos by up to 2 mm and restores the signs of periorbital vol-ume defi ciency.A serial-puncture technique, with deep pre- ■
periosteal placement of small aliquots of fi ller, followed by molding and massage of the gel, is recommended for fi lling in periorbital region.Typical side eff ects of periorbital fi ller injection ■
include bruising and mild swelling, although these usually resolve within a few days and can be concealed with make-up or glasses.Lumpiness can be a problem in a minority of ■
patients but usually settles. Persistent lumpiness can be corrected with further molding, additional fi ller or, in the case of hyaluronic acid fi llers, dis-solution with hyaluronidase.Patient satisfaction following periorbital soft - tissue ■
fi ller for rejuvenation is between 80–95%.Th e role of injectable soft -tissue fi llers in treating ■
periorbital pathology is continuing to expand, with reports of their successful use in treating paralytic lagophthalmos, lower eyelid retraction and cicatricial ectropion.
15
212 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
Summary for the Clinician
Orbital volume loss typically presents with ■
enophthalmos, a deep superior sulcus, increased upper eyelid pre-tarsal show and lower eyelid tear trough and lateral hollowness.Anophthalmic patients may also have prosthesis ■
instability and lower eyelid laxity caused by stretching of the lower eyelid from wearing a bulky prosthesis.Periorbital volume loss can give rise to a negative ■
facial vector, lagophthalmos, localized soft -tissue defects, or a generalized unmasking of the under-lying bony and ligamentous anatomy.Bony displacement must be considered in cases ■
of orbital and periorbital volume loss and where possible, corrected prior to soft -tissue volume augmentation.Occult, sinister, progressive causes of orbital and ■
periorbital volume loss include sclerosing infl am-matory disease (e.g., Wegeners granulomatosis), scirrhous carcinoma, silent –sinus syndrome and idiopathic hemifacial atrophy.More obvious causes include phthisis, facial ■
trauma, surgery, radiotherapy, neurofi bromatosis, and HIV-treatment-induced facial lipoatrophy.Soft -tissue atrophy due to aging is the most com- ■
mon cause of periorbital volume loss presenting to oculoplastic surgeons.Typical features include: ■
Unmasking of the lower eyelid fat-pads and ■
infra-orbital rim both medially (tear trough) and laterallySuperior sulcus hollowing and increased upper ■
eyelid pre-tarsal showSub-brow defl ation, brow descent and lateral ■
hoodingTemple hollowing, revealing the lateral orbital ■
rim outline and clipping the tail of the brow in the frontal viewRare but serious complications of orbital and ■
periorbital soft -tissue fi ller injections include visual loss and skin necrosis. All patients should be consented for this and sighted patients should have their visual acuity documented.Patients should be informed of the current off - ■
label status of fi llers when applied to the orbit and periorbital region.
Orbital soft -tissue fi llers are administered via a ■
peribulbar injection.In general, 2 ml of hyaluronic acid gel will reduce ■
enophthalmos by up to 2 mm.Filler should be placed just posterior to the equa- ■
tor of the globe or implant.Deliberate intraconal placement should be ■
avoided.Prior peribulbar injection with local anesthetic ■
helps to improve comfort and reduce the oculo-cardiac refl ex.Periorbital fi llers are best placed pre-periosteally ■
for the upper eyelid, lower eyelid and brow, and in the superfi cial temporalis fascia for the temple region.Vigorous molding against the underlying bony ■
orbital rim is usually necessary to achieve a smooth contour.Application is using a serial puncture technique ■
with 3–5 injection sites.Upper eyelid and sub-brow fi llers should be ■
administered from lateral to medial, avoiding the supraorbital notch, whilst tear trough fi llers are best applied from medial to lateral.Ice is a suitable anesthetic for periorbital fi ller ■
injections.Bruising is minimized by reducing the number of ■
superfi cial passes of the needle and by deep pre-periosteal placement of the fi ller. Ice also aids in producing vasoconstriction.Following periorbital soft -tissue fi ller injections, ■
patients are advised to avoid alcohol, vigorous exercise and direct pressure to the treated area for 24 hours.Most patients experience mild bruising and ■
swelling following periorbital soft -tissue fi ller injections. Th is usually settles within 1 week.One third of patients may experience mild initial ■
lumpiness which also settles.Persistent lumps or blue discoloration can be ■
treated by further molding, injection of addi-tional fi ller or, in the case of hyaluronic acid based fi llers, dissolution with hyaluronidase.Additional periorbital applications of soft -tissue ■
fi llers include upper eyelid loading, lower eyelid elevation and correction of cicatricial ectropion.

15.2 Etiology and Presentation 213
15.1 Introduction
Successful management of volume loss within the orbit and periorbital region involves accurate diagnosis of the underlying cause, treatment of any ongoing contributory factors, followed by volume replacement. Traditional sur-gical methods of volume replacement, ranging from bone graft s, orbital or periorbital implants and autogenous soft -tissue graft s (e.g., dermis-fat) have been somewhat crude and diffi cult to titrate to the exact site and degree of volume loss in any given individual. In addition, morbid-ity from these procedures has been high, with a signifi -cant risk of complications such as implant extrusion, hemorrhage, or infection. Th e development of artifi cial soft -tissue fi llers has revolutionized the management of orbitofacial volume loss, enabling a precise, titratable, reversible treatment to be applied. Th is has permitted more subtle volume defi cits to be eff ectively treated, expanding the potential role of volume replacement ther-apies from the treatment of grossly disfi guring pathology to that of subtle rejuvenation. Furthermore, the versatility of these soft -tissue fi llers has resulted in their successful application to other periocular pathologies including lagophthalmos and eyelid malposition. As newer and improved soft -tissue fi llers continue to emerge, we antici-pate wider and increased use of these products within the fi eld of oculoplastic surgery.
15.2 Etiology and Presentation
15.2.1 Etiology of Orbital Volume Loss
Orbital volume loss is caused by insuffi ciency, loss, or displacement of any of the orbital components including the bony skeleton, the globe and the intervening soft tis-sues [14]. Bony causes typically include trauma and orbital fractures, where displacement of parts of the bony skeleton causes enlargement of the orbit, leading to a relative defi ciency of orbital contents. A similar eff ect is
seen in silent-sinus syndrome where obstruction of the maxillary ostium leads to negative pressure in the maxil-lary sinus and bowing of the orbital fl oor towards the imploding sinus [8]. Other bony causes of orbital volume defi ciency include bony agenesis, such as that of the sphenoid wing seen in association with neurofi bromato-sis 1 [43], or iatrogenic bone removal, as occurs with bony orbital decompression.
Damage, loss, or absence of the globe also leads to orbital volume defi ciency. Th is includes phthisis, acquired anophthalmos from evisceration or enucleation, and con-genital microphthalmos/anophthalmos. As the latter con-dition is associated with abnormal growth of the entire orbit, it tends not to present with the same features of orbital volume loss and will not be discussed further here.
Orbital volume defi ciency can also arise due to soft -tissue changes resulting in contraction and atrophy. Contraction occurs as a result of orbital sclerosing infl am-mation which can either be specifi c, e.g., Wegeners gran-ulomatosis [60], or idiopathic. Other causes include post-infl ammatory or postsurgical fi brosis and scirrhous metastatic breast carcinoma [14]. Atrophy commonly aff ects orbital fat and can develop following orbital infl ammation, radiotherapy, surgery, trauma, or com-pression from orbital varices [14]. It can also be caused by idiopathic atrophic conditions, such as Parry-Romberg syndrome (Fig. 15.4c), a rare disorder characterized by progressive atrophy of the skin and soft -tissues over half of the face [7, 9]. Finally, orbital fat and soft -tissue atro-phy most commonly occurs with age, leading to a sec-ondary loss of orbital volume [17, 64]. Some of these causes of orbital volume loss are illustrated in Fig. 15.1.
15.2.2 Etiology of Periorbital Volume Loss
Th e causes of periorbital volume loss are similar to those responsible for orbital volume loss, with the exception of globe pathology. Both bone and soft -tissue changes contribute, through displacement, surgical removal,
Th ese require superfi cial placement of ■
fi ller using “linear-threading” or “haystack” techniques.In upper eyelid loading the filler acts as a ■
temporary weight. The filler is placed pre-tarsally and in front of the levator aponeu-rosis.
In lower eyelid elevation the fi ller acts as a tem- ■
porary spacer, supporting and stretching adja-cent tissues. Th e fi ller is placed beneath orbicularis in the pre-tarsal and pre-septal regions.In cicatricial ectropion the fi ller acts as a tempo- ■
rary lower eyelid skin expander. Th e fi ller is placed subcutaneously.
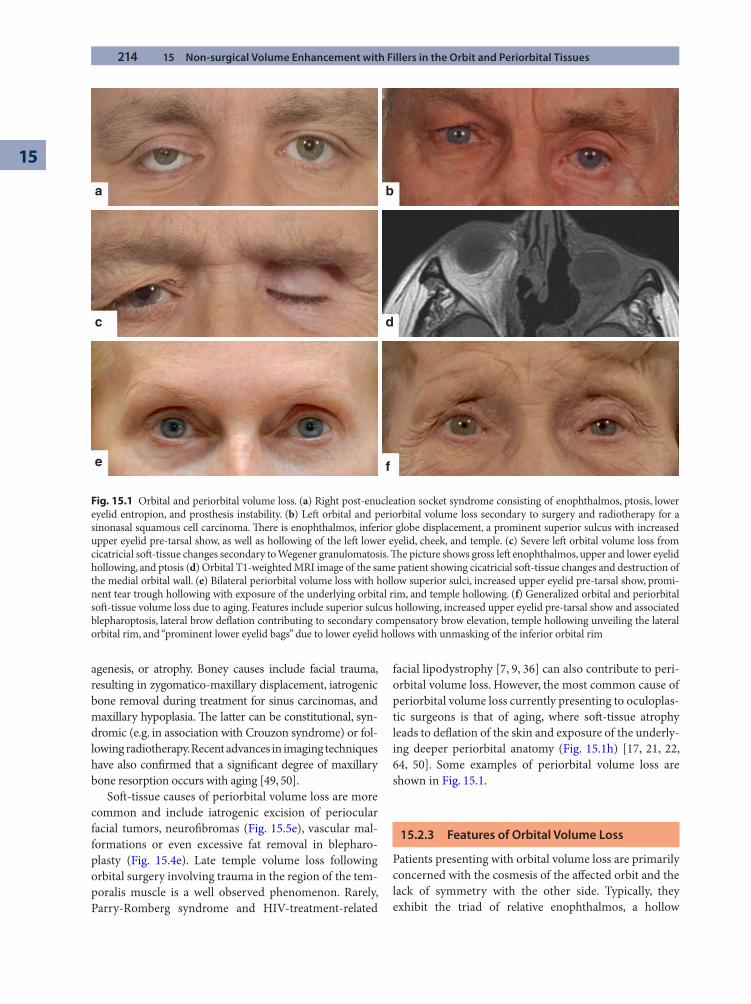
214 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
agenesis, or atrophy. Boney causes include facial trauma, resulting in zygomatico-maxillary displacement, iatrogenic bone removal during treatment for sinus carcinomas, and maxillary hypoplasia. Th e latter can be constitutional, syn-dromic (e.g. in association with Crouzon syndrome) or fol-lowing radiotherapy. Recent advances in imaging techniques have also confi rmed that a signifi cant degree of maxillary bone resorption occurs with aging [49, 50].
Soft -tissue causes of periorbital volume loss are more common and include iatrogenic excision of periocular facial tumors, neurofi bromas (Fig. 15.5e), vascular mal-formations or even excessive fat removal in blepharo-plasty (Fig. 15.4e). Late temple volume loss following orbital surgery involving trauma in the region of the tem-poralis muscle is a well observed phenomenon. Rarely, Parry-Romberg syndrome and HIV-treatment-related
facial lipodystrophy [7, 9, 36] can also contribute to peri-orbital volume loss. However, the most common cause of periorbital volume loss currently presenting to oculoplas-tic surgeons is that of aging, where soft -tissue atrophy leads to defl ation of the skin and exposure of the underly-ing deeper periorbital anatomy (Fig. 15.1h) [17, 21, 22, 64, 50]. Some examples of periorbital volume loss are shown in Fig. 15.1.
15.2.3 Features of Orbital Volume Loss
Patients presenting with orbital volume loss are primarily concerned with the cosmesis of the aff ected orbit and the lack of symmetry with the other side. Typically, they exhibit the triad of relative enophthalmos, a hollow
a
c d
fe
b
Fig. 15.1 Orbital and periorbital volume loss. (a) Right post-enucleation socket syndrome consisting of enophthalmos, ptosis, lower eyelid entropion, and prosthesis instability. (b) Left orbital and periorbital volume loss secondary to surgery and radiotherapy for a sinonasal squamous cell carcinoma. Th ere is enophthalmos, inferior globe displacement, a prominent superior sulcus with increased upper eyelid pre-tarsal show, as well as hollowing of the left lower eyelid, cheek, and temple. (c) Severe left orbital volume loss from cicatricial soft -tissue changes secondary to Wegener granulomatosis. Th e picture shows gross left enophthalmos, upper and lower eyelid hollowing, and ptosis (d) Orbital T1-weighted MRI image of the same patient showing cicatricial soft -tissue changes and destruction of the medial orbital wall. (e) Bilateral periorbital volume loss with hollow superior sulci, increased upper eyelid pre-tarsal show, promi-nent tear trough hollowing with exposure of the underlying orbital rim, and temple hollowing. (f) Generalized orbital and periorbital soft -tissue volume loss due to aging. Features include superior sulcus hollowing, increased upper eyelid pre-tarsal show and associated blepharoptosis, lateral brow defl ation contributing to secondary compensatory brow elevation, temple hollowing unveiling the lateral orbital rim, and “prominent lower eyelid bags” due to lower eyelid hollows with unmasking of the inferior orbital rim

15.3 Background to Injectable Soft-Tissue Fillers 215
superior sulcus and an increased upper eyelid pre-tarsal show. Th e hollow superior sulcus may be medially only (“A-shaped” hollow) or more generalized. Th ere can also be associated upper eyelid ptosis, with or without second-ary compensatory brow elevation. Th e lower eyelid may appear retracted, particularly laterally, and there may be hollows, both medially in the tear trough region and lat-erally, revealing the underlying inferior orbital rim. Anophthalmic patients with orbital volume loss may have additional complaints about prosthesis instability, caused by lower eyelid stretching from longstanding use of a bulky prosthesis, used to compensate for their fundamen-tal lack of orbital volume. Th is combination of relative enophthalmos, hollow superior sulcus, increased upper eyelid pre-tarsal show with ptosis and lower eyelid laxity has traditionally been termed the “post-enucleation socket syndrome” (PESS). Typical presentations of orbital volume loss are illustrated in Fig. 15.1.
15.2.4 Features of Periorbital Volume Loss
Periorbital volume loss can present in a wide range of ways refl ecting the many etiologies involved. Bony loss or hypoplasia of the maxilla results in fl at cheeks and relative globe proptosis, producing what is termed a “negative facial vector” [50]. Th is is oft en associated with lower eye-lid retraction and lagophthalmos. If signifi cant, this can cause symptoms of epiphora and refl ex tearing. Localized subcutaneous atrophy will leave a well-defi ned inferior periorbital hollow, whilst the diff use periorbital volume loss seen in facial aging leads to loose skin, lack of convex facial contours and unmasking of the underlying bony and ligamentous anatomy [17, 21, 22, 50, 64]. In the lower eyelid this results in prominence of the lower eyelid fat pad and inferior orbital rim [31]. Such “bags” and adja-cent tear trough hollows oft en cause esthetic concern.
In the upper eyelid soft -tissue atrophy leads to medial or generalized hollowing of the superior sulcus and an increased upper eyelid pre-tarsal show. A similar appearance may arise as a result of dehiscence of the leva-tor aponeurosis or aft er excessive fat removal during blepharoplasty. Associated upper eyelid dermatochalasis in this setting simply refl ects upper eyelid volume defl a-tion. In the brow region, defl ation of the sub-brow fat pad and possible supero-temporal orbital rim remodeling results in lateral brow ptosis. Th is further contributes towards upper eyelid hooding [13]. Soft -tissue atrophy in the temple region further contributes to a lack of support for the lateral brow. Temple volume loss also causes skel-etalization of the orbital rim and clipping of the tail of the brow in the frontal view (Fig. 15.1e and f).
15.3 Background to Injectable Soft-Tissue Fillers
15.3.1 Historical Perspective on Volume Replacement
Orbital and periorbital volume loss has traditionally been managed surgically by way of implants and graft s. Orbital implants include ball implants for anophthalmia, orbital fl oor implants and dermis-fat graft s, whilst those used in the periocular region include malar implants [25], dermis-fat graft s, lumbrical fat graft s [26], and “pearl fat” graft s [54, 56]. More recently, autogenous fat graft ing, using fat harvested in a manner similar to liposuction, has been successfully applied to the periocular region [4, 13, 15, 16, 40]. However, for the large part, these proce-dures require general anesthesia and carry the potential for signifi cant surgical morbidity and complications, including hemorrhage, infection, and implant extrusion. In addition, fat graft s are prone to atrophy and hypertro-phy making them somewhat unpredictable [46]. Although invaluable for large volume defects, these implants are not easy to titrate to the exact degree and location of vol-ume loss making them unsuitable for more subtle volume defi ciencies. Th is is of particular relevance to the periocu-lar region where small asymmetries in volume are very noticeable and are a concern for many patients.
15.3.2 Advantages of Injectable Soft-Tissue Fillers
Injectable soft -tissue fi llers have provided a solution to the problems of surgical volume replacement. Th eir advantages include precise soft -tissue placement, titrat-able volume augmentation, the ability to be performed in the offi ce, biocompatibility, low down-time, minimal morbidity, high safety and, in most cases, potential revers-ibility [12, 20]. Th eir principal disadvantage is a limited duration, ranging between six months and a few years depending on the product type. However, for many patients this can be an advantage as it allows volume enhancement to be altered over time depending on the desired look and changing facial structure.
15.3.3 Complications of Injectable Soft-Tissue Fillers
Overall, soft -tissue fi llers have an excellent safety record and have been extensively used for the treatment of facial rhytids and wrinkles over the last decade [42]. However,

216 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
isolated reports exist of both visual loss and skin necrosis occurring following the application of a range of soft - tissue fi llers to the face, including micronized dermal matrix, bovine collagen, autologous fat, silicone oil, and hyaluronic acid [53, 2, 58, 19, 55, 61]. Th is is thought to occur from retrograde embolization of the fi ller leading to occlusion of one of the small terminal arterioles sup-plying either the adjacent skin or the eye. Although these complications have not yet been specifi cally reported with periocular fi ller treatment, visual loss has occurred following injections into the glabella region [2]. Th e latter remains a particular concern in the periorbital region because the palpebral and anterior orbital vasculature is derived from the same source as that supplying the globe itself (i.e., the ophthalmic artery). Th e risk of emboliza-tion in general can be minimized by slow injection of the fi ller and deep pre-periosteal placement.
Orbital hemorrhage and globe trauma from injection are both additional potential causes of visual loss associ-ated with these treatments. Consequently, all sighted patients receiving orbital or periorbital volume augmen-tation with soft -tissue fi llers should have their visual acu-ity checked preoperatively and be consented for the theoretical risk of visual loss. Other signifi cant potential complications include infection and diplopia.
15.4 Types of Injectable Soft-Tissue Filler
15.4.1 Collagen Fillers
Soft -tissue fi llers composed of bovine collagen were the fi rst to be fi rst introduced, in the late 1970s, in the form of Zyderm® and Zyplast® (Allergan, Irvine, California) [38]. However, problems with allogenicity, requiring patients to undertake a pretreatment allergy test, limited their pop-ularity. Bioengineered human dermis products CosmoDerm® and CosmoPlast® (Inamed Division of Allergan, Santa Barbara, California) were approved by the US Food and Drug Administration (FDA) in March 2003 and do not require such testing before use. Other collagen products include Cymetra®, composed of micronized human cadav-eric dermis (AlloDerm, LifeCell Corporation, Palo Alto, California) and Fascian®, composed of injectable human cadaveric fascia (Biosystems, Beverly Hills, California). Th ese products, however, have reportedly had problems with inaccurate fi ller placement and lumpiness [23].
15.4.2 Hyaluronic acid Fillers
Th e second major group of soft -tissue fi llers are those composed of hyaluronic acid, derived from either animal
or bacterial sources. Hyaluronic acid was proposed for use as a soft -tissue fi ller because it is a component of skin, with structural, elastic, and hydrating properties, but was ini-tially limited by its rapid degradation in biological tissues [3]. However, cross-linking was later found to stabilize it, prolonging its tissue duration time to over six months [51].
Th e fi rst such stabilized hyaluronic acid fi ller to gain FDA approval was Restylane® (Medicis, Scottsdale, Arizona) in December 2003. Since then a wide range of other hyaluronic acid products have become available, each with slight diff erences, relating to the source derivation (animal versus bacterial), the method and amount of cross-linking, and the particle size [12, 23]. Th e latter is particularly important as a larger particle size will increase viscosity, reduce ease of injection and increase duration of the fi ller. In general, more viscous fi llers are reserved for deeper soft -tissue augmentation and require larger cannulas for injec-tion with increased associated patient discomfort. However, they have the advantage of more defi ned contouring and increased longevity. Some of the most commonly used examples of hyaluronic acid fi llers include Restylane Lipp®, Restylane Fine Line®, Restylane Touch®, Restylane Vittal®, Restylane®, Restylane Perlane® and Restylane SubQ® (Medicis and Q-med, Uppsala, Sweden); Juvederm®, Juvederm Ultra® and Juvederm Ultra Plus® (Allergan, Irvine, California); Captique® (Genzyme, Framingham, Massachusets and Allergan); HydraFill® (Allergan), Purogen® (Mentor, Santa Barbara, California) and the ani-mal derived Hylaform® and Hylaform plus® (Genzyme, and Allergan) [12, 23]. Nonanimal stabilized hyaluronic acid fi llers are commonly termed NASHA fi llers.
Hyaluronic acid fi llers have the advantage over colla-gen fi llers of instant reversibility with the application of hyaluronidase. Th e latter is a cheap, readily available product which can be easily injected into the treated area. In addition, collagen fi llers are contra-indicated in people with a known allergy to bovine collagen, pregnant or breast feeding women, or patients with connective tissue disorders. However, it has been suggested that collagen fi llers may off er superior results to hyaluronic acid fi llers when treating very superfi cial areas [23].
15.4.3 Semipermanent Injectable Soft-Tissue Fillers
In addition to the two principal categories of injectable soft -tissue fi llers outlined above, there are a few isolated, longer lasting, semipermanent products that have been approved for deep tissue augmentation [6]. Th ese include poly-L-lactic acid (Sculptra®, Dermik Labs, Bridgewater, New Jersey), which currently has approval from the FDA for use in patients with HIV-therapy-induced facial

15.5 Treatment Areas 217
lipoatrophy [11, 41, 57], and calcium hydroxylapatite (Radiesse®, BioForm Medical, San Mateo, California), which has been approved for the treatment of moderate to severe facial wrinkles [33]. Both have been reported to last years and it is suggested that this is partly due to the stimu-lation of collagen production [41, 57, 62]. A wider range of locally approved permanent fi llers are available outside of the US, including polyacrylamide gel (Aquamid®, Ferrosan A/S, Copenhagen, Denmark) [18]. A summary of the most common brands of soft -tissue fi llers is given in Table 15.1.
15.5 Treatment Areas
Soft -tissue fi llers have been successfully used for volume enhancement throughout the entire facial region by a range of practitioners. However, their use in the orbit and perior-bital area remains fairly limited. Th is is due to the concerns about visual loss and hemorrhage discussed previously, as well as concerns that the thin eyelid skin will readily reveal any underlying lumps, bruising, or discoloration, resulting in a poor cosmetic outcome. However, the oculoplastic lit-erature has seen the recent emergence of case series describing the successful use of soft -tissue fi llers for treat-ing orbital and periorbital volume loss. Th ese novel tech-niques are outlined below. In all cases it is important to remember that the fi llers are being used off -label and it is essential to convey this information to the patient.
15.5.1 Orbit
Orbital volume augmentation has been described using permanent soft -tissue fi llers, in the form of polyacrylam-ide gel (Aquamid®) [18]; semipermanent fi llers, in the form of calcium hydroxylapatite (Radiesse®) [39, 63]; and reversible ones, in the form of both collagen (Zyplast®) [10] and hyaluronic acid gel (Restylane Sub-Q®) [44]. Calcium hydroxylapatite, polyacrylamide gel and colla-gen have only been used in anophthalmic patients whilst hyaluronic acid has been used in both anophthalmic and sighted orbits. Typical features of such patients have included enophthalmos, a deep superior sulcus and an increased upper eyelid pre-tarsal show. Most treated patients have already undergone conventional surgical volume replacement.
Orbital injections can generally be administered in the offi ce under local anesthesia, although a few patients may desire concurrent sedation and are therefore best treated in an ambulatory surgery center [10, 63]. Th e patient is posi-tioned 30° supine on a couch and the skin prepared by wip-ing with alcohol. A peribulbar local anesthetic injection administered approximately 10–15 min prior to injecting
the fi ller improves comfort and limits any potential eff ects of the oculocardiac refl ex, presumably caused by rectus stretch due to intraorbital and intraconal placement of the fi ller [44]. Th e injection technique is similar to that of a standard peribulbar injection, given transcutaneously through the lateral lower eyelid into the extraconal space along the orbital fl oor [44, 63] although transcutaneous injection has also been described [10]. It is recommended that Aquamid® be given through a 22-gauge needle [18], Radiesse® through a 27-gauge one and Restylane Sub-Q® through a 25-gauge one, all on a Luer-lock attached to the prepackaged vial of fi ller. Ideally, the injection is com-menced aft er the tip of the needle is beyond the equator of the globe or implant to provide maximal correction of enophthalmos. Th e injection continues as the needle is advanced in a retrobulbar direction and also as the needle is redirected to distribute the fi ller across the orbital fl oor. Medial and lateral injections can also be performed, with similar pre-periosteal placement of fi ller within the extra-conal fat [63]. Care must be taken to avoid direct intrac-onal or excessively posterior placement of fi ller due to potential visual impairment (in sighted eyes), stimulation of the oculocardiac refl ex or cavernous sinus thrombosis.
One vial of fi ller usually suffi ces per treated orbit, except for polyacrylamide gel where two vials is recom-mended [18, 44, 63]. Th is equates to 1.3 ml of Radiesse and 2 ml of Restylane Sub-Q® or Aquamid®. Th e mean reduction in enophthalmos is 2 mm, measured using Hertel exophalmometry, for adequate placement of the fi ller, and is associated with a signifi cant esthetic improve-ment in upper eyelid sulcus volume and skin fold. Th e reported duration of eff ect from the treatment is over 1 year for Aquamid® and Radiesse® [18, 62] and 9 months for Restylane Sub-Q® [44].
Postoperatively patients may note mild orbital dis-comfort, which is controllable with oral analgesia [18]. Complications of orbital soft -tissue fi ller treatments include vasovagal attacks, peribulbar hemorrhage and anterior migration of the fi ller into the lower eyelid [18, 44, 63]. Th e latter can be readily treated by dissolution using hyaluronidase in the case of Restylane Sub-Q®. [44] No cases of visual impairment or raised intraocular pres-sure have been described in the sighted eyes that have been treated [44].
Such orbital soft -tissue fi ller injections can be cov-ered through insurance under Current Procedural Terminology code 67550, orbital implant (outside mus-cle cone) insertion. However, reimbursement for the fi ller itself may not be possible due to a lack of appropri-ate healthcare Common Procedure Coding System sup-ply code [63]. Examples of the technique and outcome of orbital volume augmentation with injectable soft -tis-sue fi ller are shown in Fig. 15.2.
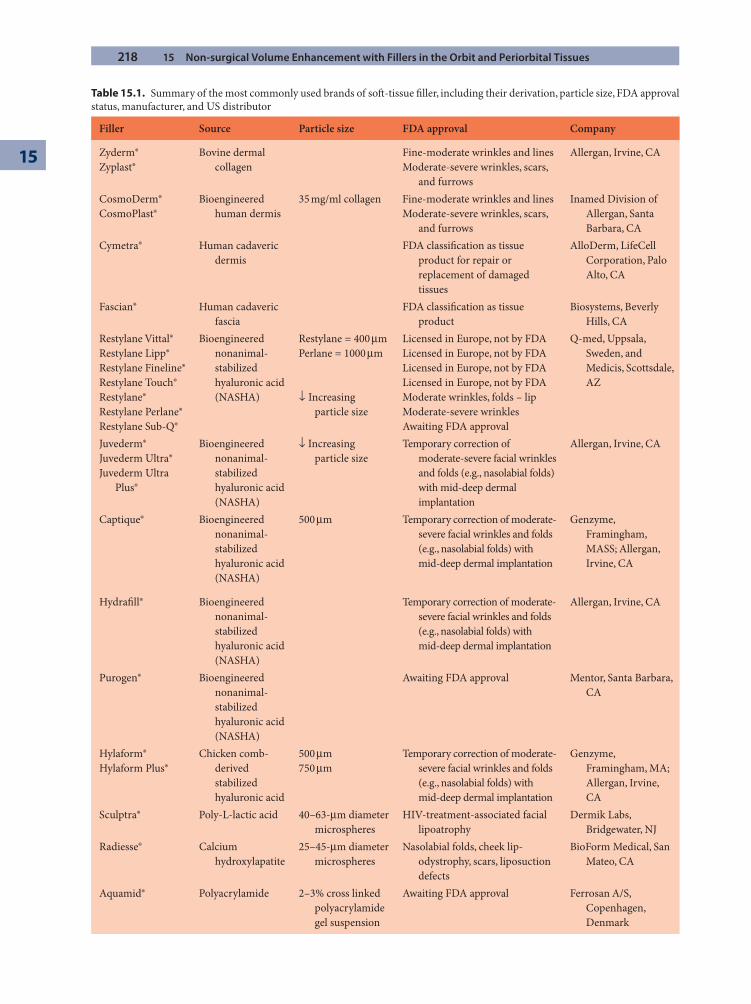
218 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
Table 15.1. Summary of the most commonly used brands of soft -tissue fi ller, including their derivation, particle size, FDA approval status, manufacturer, and US distributor
Filler Source Particle size FDA approval Company
Zyderm®Zyplast®
Bovine dermal collagen
Fine-moderate wrinkles and linesModerate-severe wrinkles, scars,
and furrows
Allergan, Irvine, CA
CosmoDerm®CosmoPlast®
Bioengineered human dermis
35 mg/ml collagen Fine-moderate wrinkles and linesModerate-severe wrinkles, scars,
and furrows
Inamed Division of Allergan, Santa Barbara, CA
Cymetra® Human cadaveric dermis
FDA classifi cation as tissue product for repair or replacement of damaged tissues
AlloDerm, LifeCell Corporation, Palo Alto, CA
Fascian® Human cadaveric fascia
FDA classifi cation as tissue product
Biosystems, Beverly Hills, CA
Restylane Vittal®Restylane Lipp®Restylane Fineline®Restylane Touch®Restylane®Restylane Perlane®Restylane Sub-Q®
Bioengineered nonanimal-stabilized hyaluronic acid (NASHA)
Restylane = 400 μmPerlane = 1000 μm
↓ Increasing particle size
Licensed in Europe, not by FDALicensed in Europe, not by FDALicensed in Europe, not by FDALicensed in Europe, not by FDAModerate wrinkles, folds – lipModerate-severe wrinklesAwaiting FDA approval
Q-med, Uppsala, Sweden, and Medicis, Scottsdale, AZ
Juvederm®Juvederm Ultra®Juvederm Ultra
Plus®
Bioengineered nonanimal-stabilized hyaluronic acid (NASHA)
↓ Increasing particle size
Temporary correction of moderate-severe facial wrinkles and folds (e.g., nasolabial folds) with mid-deep dermal implantation
Allergan, Irvine, CA
Captique® Bioengineered nonanimal-stabilized hyaluronic acid (NASHA)
500 μm Temporary correction of moderate-severe facial wrinkles and folds (e.g., nasolabial folds) with mid-deep dermal implantation
Genzyme, Framingham, MASS; Allergan, Irvine, CA
Hydrafi ll® Bioengineered nonanimal-stabilized hyaluronic acid (NASHA)
Temporary correction of moderate-severe facial wrinkles and folds (e.g., nasolabial folds) with mid-deep dermal implantation
Allergan, Irvine, CA
Purogen® Bioengineered nonanimal-stabilized hyaluronic acid (NASHA)
Awaiting FDA approval Mentor, Santa Barbara, CA
Hylaform®Hylaform Plus®
Chicken comb-derived stabilized hyaluronic acid
500 μm750 μm
Temporary correction of moderate-severe facial wrinkles and folds (e.g., nasolabial folds) with mid-deep dermal implantation
Genzyme, Framingham, MA; Allergan, Irvine, CA
Sculptra® Poly-L-lactic acid 40–63-μm diameter microspheres
HIV-treatment-associated facial lipoatrophy
Dermik Labs, Bridgewater, NJ
Radiesse® Calcium hydroxylapatite
25–45-μm diameter microspheres
Nasolabial folds, cheek lip-odystrophy, scars, liposuction defects
BioForm Medical, San Mateo, CA
Aquamid® Polyacrylamide 2–3% cross linked polyacrylamide gel suspension
Awaiting FDA approval Ferrosan A/S, Copenhagen, Denmark
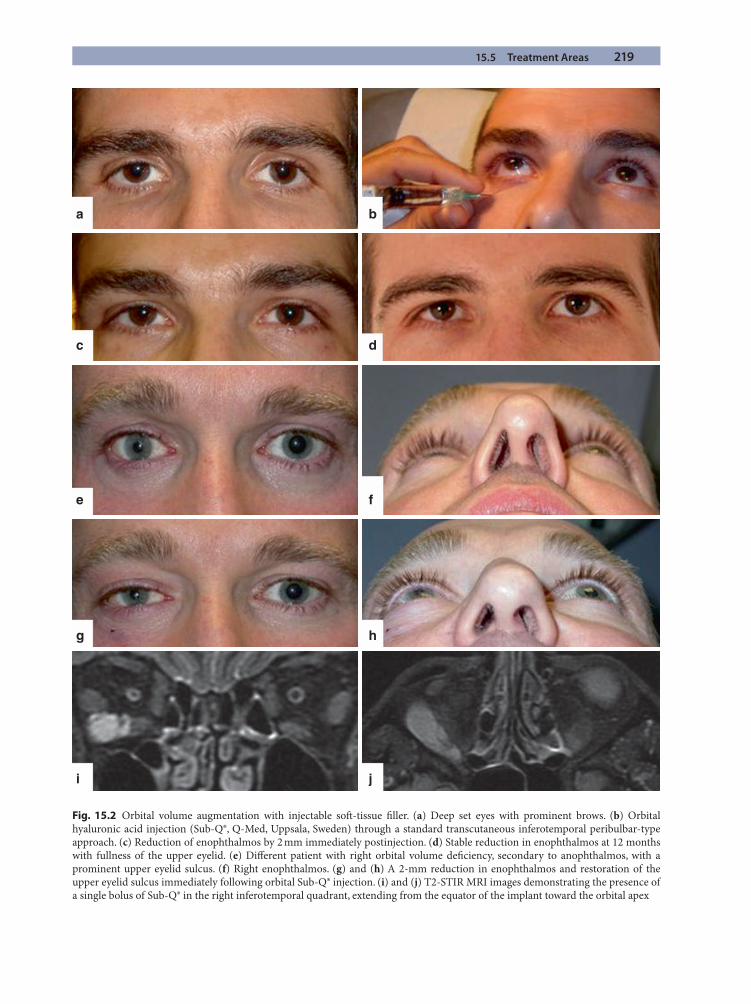
15.5 Treatment Areas 219
a b
dc
fe
hg
ji
Fig. 15.2 Orbital volume augmentation with injectable soft -tissue fi ller. (a) Deep set eyes with prominent brows. (b) Orbital hyaluronic acid injection (Sub-Q®, Q-Med, Uppsala, Sweden) through a standard transcutaneous inferotemporal peribulbar-type approach. (c) Reduction of enophthalmos by 2 mm immediately postinjection. (d) Stable reduction in enophthalmos at 12 months with fullness of the upper eyelid. (e) Diff erent patient with right orbital volume defi ciency, secondary to anophthalmos, with a prominent upper eyelid sulcus. (f) Right enophthalmos. (g) and (h) A 2-mm reduction in enophthalmos and restoration of the upper eyelid sulcus immediately following orbital Sub-Q® injection. (i) and (j) T2-STIR MRI images demonstrating the presence of a single bolus of Sub-Q® in the right inferotemporal quadrant, extending from the equator of the implant toward the orbital apex

220 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
15.5.2 Upper Eyelid and Brow
In some cases of orbital volume loss the defi ciency is pri-marily anterior, and enophthalmos is not such a concern. However, a hollow superior sulcus and an increased upper eyelid pre-tarsal show remain. Examples include patients with Parry-Romberg syndrome, patients who have undergone excessive fat excision during upper eye-lid blephroplasty, and some patients with aging and fat atrophy without concurrent dermatochalasis. In such cases, volume replacement with soft -tissue fi ller applied directly to the upper eyelid sulcus can be very eff ective in restoring facial symmetry and in improving the contour of the pre-septal skin fold. At present, this has only been reported using the NASHA fi ller Restylane® [6, 48], although a range of collagen and hyaluronic acid fi llers are theoretically suitable. However, the thin upper eyelid skin does call for the use of a medium-low viscosity com-pound to prevent visible lumpiness and permit a smooth contor. Filler placement should also be as deep as possi-ble within the pre-periosteal plane to minimize this problem.
Once again, the procedure can be carried out in the offi ce [48]. Th e skin is numbed with ice 15 minutes before injecting and wiped with an alcohol swab. Th e former pro-vides good analgesia and vasoconstriction without distort-ing the local tissue architecture. Th e patient is then positioned supine at 45° with the eyes in downgaze. Th e 30-gauge needle provided with the fi ller is usually adequate for injection. A needle puncture is created close to the junction of the lateral orbital wall and roof and the needle tip advanced in the sub-orbicularis plane until the inferior border of the superior orbital rim is reached (Fig. 15.3a). 0.1 ml of fi ller is then injected pre-periosteally and the needle is withdrawn. Th e raised bleb of fi ller is massaged and molded over the anterior aspect of the orbital rim in a medial direction to achieve a smooth contour (Fig. 15.3b). Th e needle is then passed further medially at the inferior border of the orbital rim and a further 0.1 ml of product is injected, followed by molding. Additional aliquots of fi ller can be injected as necessary using serial puncture sites, each progressively more medial. Usually three puncture sites suffi ce [48]. Injecting directly over the supraorbital notch should be avoided due to the risk of retrograde embolization of fi ller down the supraorbital vasculature. Aft er injecting, the patient is asked to raise their eyebrows and the fi ller is molded onto the anterior surface of the orbital rim. With the brows relaxed, the upper eyelid con-tour is reassessed to evaluate any residual lumpiness or irregularities. Suitable injection end points include sym-metrical fullness of the pre-septal skin fold and soft ening of any hollows [48].
In general, 0.4–0.5 ml of hyaluronic acid fi ller is suit-able for treating each upper eyelid, although the range extends from 0.1–1 ml [48]. Duration of the fi ller is less than for orbital injections due to the mobility of the eyelid and the need for a fi ller with smaller particle size and hence reduced longevity. However, despite this, eff ects persist for over six months [48].
All patients receiving upper eyelid fi ller experience some bruising and swelling which can last for up to fi ve days. However, this is readily managed with the use of concealer or sunglasses. In some patients the fi ller is also visible on marked brow elevation which can be a cosmetic concern. Additional complications of upper eyelid fi ller have not been reported [48]. Patients are advised to avoid alcohol and exercise for 24 hours following fi ller treat-ment as these activities may exacerbate bruising. Direct pressure over the treated site should also be avoided.
Reported patient satisfaction rates for such upper eye-lid contouring are extremely high, at over 95% [48]. However, careful patient selection and assessment is essential. We have found classifying patients into the fol-lowing four groups very helpful in predicting outcome and planning treatment.
(i) Medial A-shaped hollow(ii) Generalized hollow(iii) Post-blepharoplasty generalized volume loss with
no skin excess(iv) Upper eyelid hooding with sub-brow defl ation
Overall, patients from the fi rst three groups do very well with upper eyelid soft -tissue augmentation. Patients in group iv with very mild sub-brow defl ation can also ben-efi t from lateral sub-brow placement of fi ller to lift the brow slightly in this area. However, most group iv patients either require too much fi ller, resulting a prominent lat-eral brow bulge which contrasts with the adjacent temple hollowing, or else have persistent hooding or dermatoch-alasis. Consequently, these patients oft en do better with an eyelid ptosis/blepharoplasty, or brow lift procedure [48]. Comparisons should also always be made with old photographs as the degree of upper eyelid show desired by patients is very variable and oft en infl uenced by their youthful appearance. Examples of outcomes of upper eyelid contouring in patients from each of the four groups is shown in Fig. 15.4.
15.5.3 Tear Trough
Most studies describing the use of injectable soft -tissue fi llers for contouring of the tear trough relate to
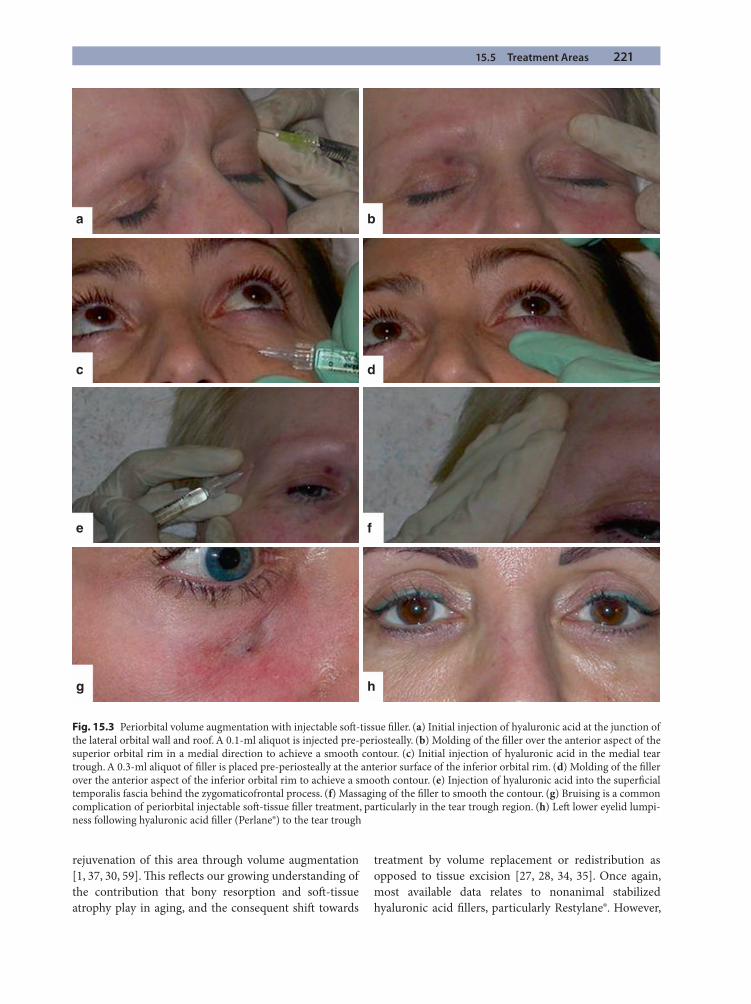
15.5 Treatment Areas 221
rejuvenation of this area through volume augmentation [1, 37, 30, 59]. Th is refl ects our growing understanding of the contribution that bony resorption and soft -tissue atrophy play in aging, and the consequent shift towards
treatment by volume replacement or redistribution as opposed to tissue excision [27, 28, 34, 35]. Once again, most available data relates to nonanimal stabilized hyaluronic acid fi llers, particularly Restylane®. However,
a b
c d
e f
g h
Fig. 15.3 Periorbital volume augmentation with injectable soft -tissue fi ller. (a) Initial injection of hyaluronic acid at the junction of the lateral orbital wall and roof. A 0.1-ml aliquot is injected pre-periosteally. (b) Molding of the fi ller over the anterior aspect of the superior orbital rim in a medial direction to achieve a smooth contour. (c) Initial injection of hyaluronic acid in the medial tear trough. A 0.3-ml aliquot of fi ller is placed pre-periosteally at the anterior surface of the inferior orbital rim. (d) Molding of the fi ller over the anterior aspect of the inferior orbital rim to achieve a smooth contour. (e) Injection of hyaluronic acid into the superfi cial temporalis fascia behind the zygomaticofrontal process. (f) Massaging of the fi ller to smooth the contour. (g) Bruising is a common complication of periorbital injectable soft -tissue fi ller treatment, particularly in the tear trough region. (h) Left lower eyelid lumpi-ness following hyaluronic acid fi ller (Perlane®) to the tear trough
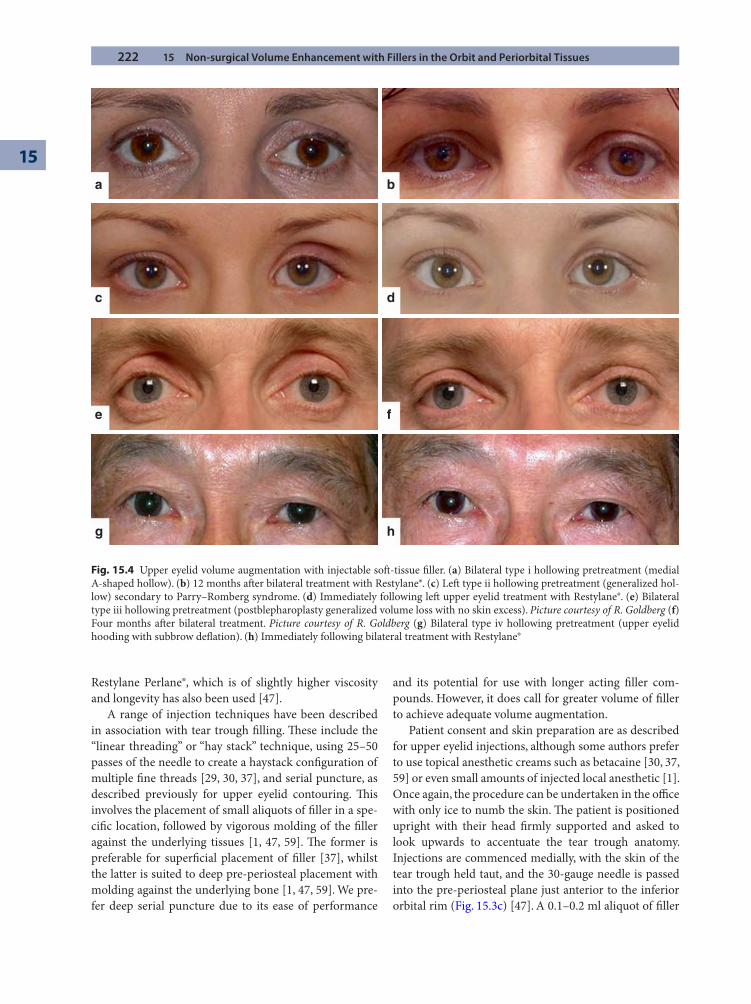
222 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
Restylane Perlane®, which is of slightly higher viscosity and longevity has also been used [47].
A range of injection techniques have been described in association with tear trough fi lling. Th ese include the “linear threading” or “hay stack” technique, using 25–50 passes of the needle to create a haystack confi guration of multiple fi ne threads [29, 30, 37], and serial puncture, as described previously for upper eyelid contouring. Th is involves the placement of small aliquots of fi ller in a spe-cifi c location, followed by vigorous molding of the fi ller against the underlying tissues [1, 47, 59]. Th e former is preferable for superfi cial placement of fi ller [37], whilst the latter is suited to deep pre-periosteal placement with molding against the underlying bone [1, 47, 59]. We pre-fer deep serial puncture due to its ease of performance
and its potential for use with longer acting fi ller com-pounds. However, it does call for greater volume of fi ller to achieve adequate volume augmentation.
Patient consent and skin preparation are as described for upper eyelid injections, although some authors prefer to use topical anesthetic creams such as betacaine [30, 37, 59] or even small amounts of injected local anesthetic [1]. Once again, the procedure can be undertaken in the offi ce with only ice to numb the skin. Th e patient is positioned upright with their head fi rmly supported and asked to look upwards to accentuate the tear trough anatomy. Injections are commenced medially, with the skin of the tear trough held taut, and the 30-gauge needle is passed into the pre-periosteal plane just anterior to the inferior orbital rim (Fig. 15.3c) [47]. A 0.1–0.2 ml aliquot of fi ller
a b
c d
e f
g h
Fig. 15.4 Upper eyelid volume augmentation with injectable soft -tissue fi ller. (a) Bilateral type i hollowing pretreatment (medial A-shaped hollow). (b) 12 months aft er bilateral treatment with Restylane®. (c) Left type ii hollowing pretreatment (generalized hol-low) secondary to Parry–Romberg syndrome. (d) Immediately following left upper eyelid treatment with Restylane®. (e) Bilateral type iii hollowing pretreatment (postblepharoplasty generalized volume loss with no skin excess). Picture courtesy of R. Goldberg (f) Four months aft er bilateral treatment. Picture courtesy of R. Goldberg (g) Bilateral type iv hollowing pretreatment (upper eyelid hooding with subbrow defl ation). (h) Immediately following bilateral treatment with Restylane®
15.5 Treatment Areas 223
is injected, the needle withdrawn and the fi ller molded and massaged against the bone to achieve the desired contour and reduce any prominent lumps (Fig. 15.3d). Th e injections are repeated in successively more lateral locations along the tear trough, by means of serial punc-ture. Usually 3–5 injections suffi ce. Care must be taken to avoid placement of more viscous gels, such as Restylane Perlane®, in the pre-septal lower eyelid location, as it is diffi cult to mold fi ller here and the very superfi cial posi-tion leads to prominent lumps or blue discoloration and consequent patient dissatisfaction. If additional contour-ing is required in this area it is best undertaken with a gel of very small particle size, such as Restylane Vittal® or Restylane Touch®, administered via the “haystack” approach. Postoperative recommendations to patients are as for upper eyelid contouring.
In general 1–1.2 ml of fi ller is suffi cient for tear trough contouring, but this can range to 3.5 mls when extending out to the malar region [47]. Th e latter helps to achieve a smoother lower lid/cheek contour and oft en gives a better esthetic fi nish. Duration of treatment ranges from 6–18 months although 8–20% of patients will request a touch-up prior to this, usually due to insuffi cient initial fi ll or patient desire for a fuller look [30, 47].
Bruising and mild swelling is common following tear-trough fi ller treatment and can last up to one week (Fig. 15.3g). However, it is readily camoufl aged with conceal-ers or glasses such that less than 20% of patients need to restrict their social engagements or work schedule fol-lowing treatment [47]. Persistent malar edema has been described with lateral fi ller placement in a few patients and has proven diffi cult to treat [30]. Mild lumpiness has been described by up to one third of patients but this usu-ally settles over the next two weeks (Fig. 15.3h). However, it may require additional treatment in up to 15% of cases [30, 47]. Th is includes further massage by the treating physician, additional fi ller to smooth out any contor irregularities or dissolution of hyaluronic acid gel. Th is can be performed in the offi ce by injecting 0.2–0.5 ml of a 1500i unit/5 ml solution of hyaluronidase in saline into the lumpy area [47]. Th e eff ects are immediate so the dose of hyaluronidase can be readily titrated against the extent of the lumpiness. Additional fi ller should not be injected into the treated area for a week to ensure that the eff ect of the hyaluronidase has ceased. Blue discoloration has also been reported by 5–10% of patients [30, 47]. It is thought to occur due to a superfi cial placement of a pool of fi ller which causes preferential scattering of blue light (Tyndall eff ect) or which becomes stained with blood. Treatment for this is also dissolution with hyaluronidase.
Patient satisfaction with lower eyelid/tear trough vol-ume augmentation using hyaluronic acid gel is reported
as being in the region of 85%, with 50% of patients express-ing “marked” satisfaction with the treatment [30, 47]. Examples of outcomes from tear trough contouring using hyaluronic acid gel (Perlane®) are given in Figs. 15.5a–d.
15.5.4 Temple and Brow
Non-surgical volume augmentation of the temple region with soft -tissue fi ller is well established for patients with HIV-treatment-associated facial lipoatrophy. In these patients, poly-L-lactic acid (Sculptra®, Dermik Labs, Bridgewater, New Jersey) has been repeatedly used with high patient satisfaction and eff ects lasting over three years [11, 41]. However, the use of fi llers to treat other causes of temple hollowing remains less well established. Reports are now emerging of the use of injectable soft -tissue fi llers in temple asymmetry following excision of orbitotemporal neurofi bromas, as well as in facial aging [52]. Hyaluronic acid fi llers have been preferred for treat-ing these causes of temple hollowing as the volume loss is more subtle and requires more careful titration of the dose of fi ller. Th e possibility of reversing the treatment, should the patients not like the esthetic result, is also use-ful. However, a viscous fi ller, such as Restylane Perlane®, should be selected as the skin overlying the temple is much thicker than the eyelid and can tolerate a fi ller with a larger particle size. Temple fi ller should also always be considered in patients receiving lateral upper eyelid/sub-brow fi ller as otherwise the latter can result in a promi-nent bulge at the lateral brow which contrasts with the adjacent hollow temple.
Patient preparation is as described previously. Injections are given behind the zygomaticofrontal pro-cess so as to soft en the bony contour of the lateral orbital rim [52]. Care must be taken to avoid the path of the superfi cial temporal artery. Th e fi ller is administered via a serial puncture technique, with 3–5 injections, each deliv-ering approximately 0.3 ml of fi ller. Placement of the fi ller is deep within the superfi cial temporal fascia (Fig. 15.3e). Aft er each aliquot is injected, the fi ller is massaged and molded against the temporal bone to achieve a smooth contour (Fig. 15.3f).
Typical treatment volumes are 1 ml per side, although this can range up to 3 ml for prominent hollowing follow-ing surgical excision (e.g., of a neurofi broma) [52]. As yet, little has been published on the longevity of hyaluronic acid fi ller in this area but the use of higher viscosity fi ller and the relative immobility of the skin in that area sug-gests that eff ects may last one year. As with most facial fi ller treatments, patient satisfaction has been high, with over 80% of patients very or moderately satisfi ed [52].
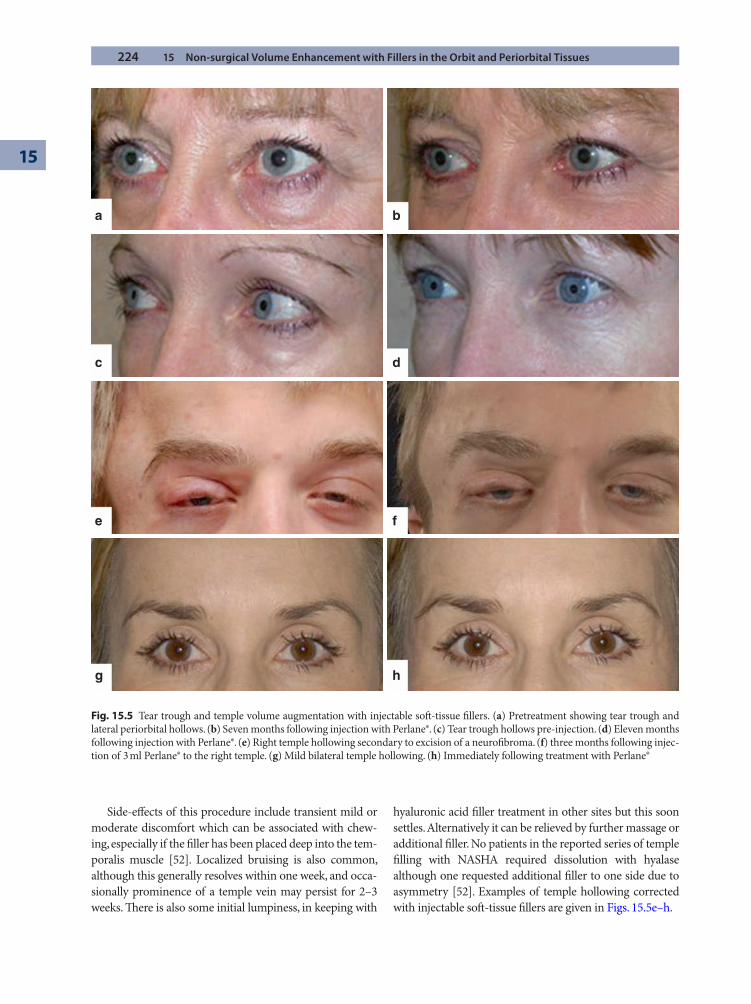
224 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
Side-eff ects of this procedure include transient mild or moderate discomfort which can be associated with chew-ing, especially if the fi ller has been placed deep into the tem-poralis muscle [52]. Localized bruising is also common, although this generally resolves within one week, and occa-sionally prominence of a temple vein may persist for 2–3 weeks. Th ere is also some initial lumpiness, in keeping with
hyaluronic acid fi ller treatment in other sites but this soon settles. Alternatively it can be relieved by further massage or additional fi ller. No patients in the reported series of temple fi lling with NASHA required dissolution with hyalase although one requested additional fi ller to one side due to asymmetry [52]. Examples of temple hollowing corrected with injectable soft -tissue fi llers are given in Figs. 15.5e–h.
a b
c d
e f
g h
Fig. 15.5 Tear trough and temple volume augmentation with injectable soft -tissue fi llers. (a) Pretreatment showing tear trough and lateral periorbital hollows. (b) Seven months following injection with Perlane®. (c) Tear trough hollows pre-injection. (d) Eleven months following injection with Perlane®. (e) Right temple hollowing secondary to excision of a neurofi broma. (f) three months following injec-tion of 3 ml Perlane® to the right temple. (g) Mild bilateral temple hollowing. (h) Immediately following treatment with Perlane®
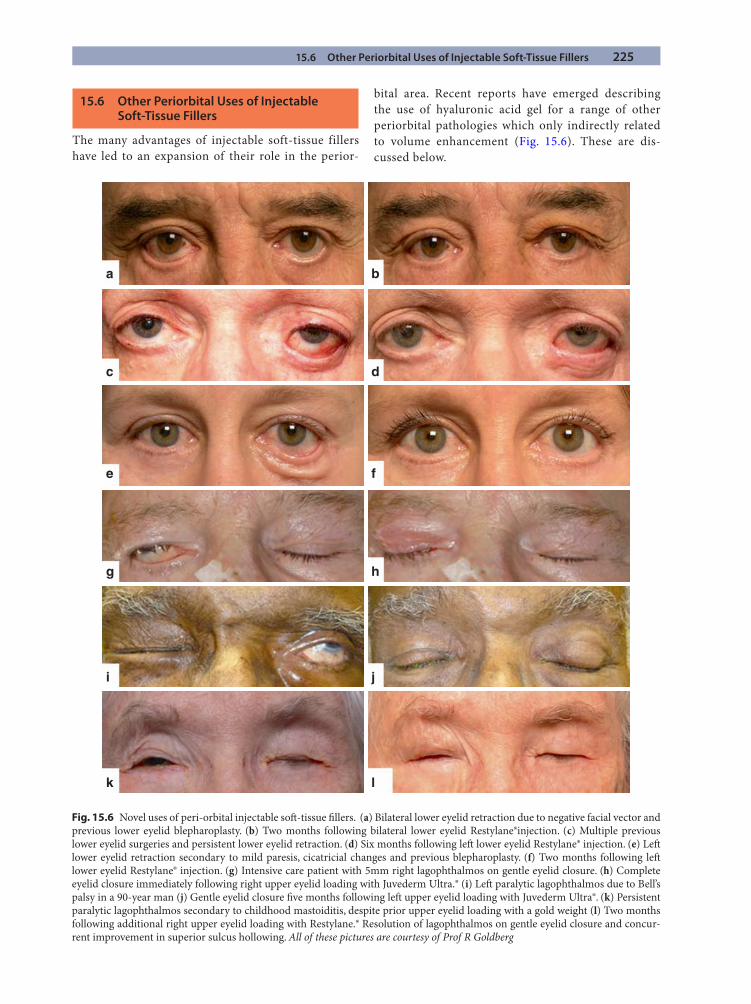
15.6 Other Periorbital Uses of Injectable Soft-Tissue Fillers 225
15.6 Other Periorbital Uses of Injectable Soft-Tissue Fillers
The many advantages of injectable soft-tissue fillers have led to an expansion of their role in the perior-
bital area. Recent reports have emerged describing the use of hyaluronic acid gel for a range of other periorbital pathologies which only indirectly related to volume enhancement (Fig. 15.6). These are dis-cussed below.
a b
c d
e f
g h
i j
k l
Fig. 15.6 Novel uses of peri-orbital injectable soft -tissue fi llers. (a) Bilateral lower eyelid retraction due to negative facial vector and previous lower eyelid blepharoplasty. (b) Two months following bilateral lower eyelid Restylane®injection. (c) Multiple previous lower eyelid surgeries and persistent lower eyelid retraction. (d) Six months following left lower eyelid Restylane® injection. (e) Left lower eyelid retraction secondary to mild paresis, cicatricial changes and previous blepharoplasty. (f) Two months following left lower eyelid Restylane® injection. (g) Intensive care patient with 5mm right lagophthalmos on gentle eyelid closure. (h) Complete eyelid closure immediately following right upper eyelid loading with Juvederm Ultra.® (i) Left paralytic lagophthalmos due to Bell’s palsy in a 90-year man (j) Gentle eyelid closure fi ve months following left upper eyelid loading with Juvederm Ultra®. (k) Persistent paralytic lagophthalmos secondary to childhood mastoiditis, despite prior upper eyelid loading with a gold weight (l) Two months following additional right upper eyelid loading with Restylane.® Resolution of lagophthalmos on gentle eyelid closure and concur-rent improvement in superior sulcus hollowing. All of these pictures are courtesy of Prof R Goldberg

226 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
15.6.1 Upper Eyelid Loading
Paralytic lagophthalmos with secondary exposure ker-atopathy is most commonly treated by upper eyelid load-ing techniques, involving implantation of either a gold or platinum weight. Complications of this procedure include extrusion of the weight, allergy, poor cosmesis, ongoing lagophthalmos, blepharoptosis, and induced astigmatism. In addition, a return of orbicularis oculi function, as in Bell’s palsy, can demand removal of the weight. Upper eyelid loading using an injection of hyaluronic acid gel off ers several advantages including immediate applica-tion in the offi ce, a titratable weight to reduce over/under correction, improved cosmesis and a duration of 6–9 months [45].
Injections are performed using a 30-gauge needle aft er application of ice or EMLA cream to anesthetize the upper eyelid. Th e fi ller is placed deep to the orbicularis oculi in the pre-tarsal and/or pre-levator aponeurosis regions by means of 3–4 injections, avoiding the area adjacent to the upper canaliculus [45]. Due to the rela-tively superfi cial placement of the fi ller and lack of an adjacent bony surface for molding, a feathered “haystack” approach is recommended with multiple passes of the needle tip to distribute the fi ller for each injection [45].
In general anything up to 1 ml of fi ller is required although the volume used will depend on severity of lagophthalmos, lid height, and desired esthetic outcome [45]. Th e mean reported improvement in lagophthalmos is 4.8 mm, (ranging from 0.9 to 11.9 mm), with 80% of cases maintaining this improvement over four months. Complications from this technique are minimal and include transient edema, erythema, pain, and tenderness that settle within a few days [45].
15.6.2 Lower Eyelid Elevation
Lagophthalmos and exposure keratopathy can also be the result of lower eyelid retraction. Causes of this are numerous and include malar volume defi ciency, globe proptosis (also causing a negative facial vector) and lower eyelid cicatrization. Defi nitive management for this has traditionally been through surgical intervention, which, as well as the usual complications of hemorrhage, infec-tion, and tissue malposition, can cause further scarring or volume depletion which exacerbates the lagophthal-mos. Once again, soft -tissue fi llers off er a less invasive, alternative treatment that eff ectively expands and rein-forces the tissues of the lower eyelid, acting as a tempo-rary spacer. Th is serves to elevate the lower eyelid reducing scleral show. To date, one study has been pub-
lished on this, using NASHA fi ller (Restylane®) adminis-tered to the lower eyelid [32].
Th e injection technique is as described above for upper eyelid loading, using the “haystack” approach and with fi ller placed in the sub-orbicularis plane in the pre-septal region and adjacent to the orbitomalar ligament [32]. For 0.9 ml of fi ller placed in this manner, to the lower eyelid inferior scleral show typically improves by 1 mm in patients whose baseline scleral show is in the order of 1.2 mm. Th e eff ects of the fi ller are temporary, with one third of patients requiring a top-up by four months. Patient satisfaction with this procedure, however, is high and reported complications are limited to mild bruising and minimal discomfort [32].
15.6.3 Treatment of Cicatricial Ectropion
Lower eyelid cicatricial ectropion, caused by shortage of the anterior lamella, has also traditionally been managed surgically. Th is has included release of scarring, recruit-ment of additional skin in the form of a fl ap, cheek lift or full-thickness skin graft , and simultaneous lid tightening. Soft -tissue fi llers off er an alternative treatment for mild cases by acting as a temporary lower eyelid tissue expander, stretching the defi cient anterior lamella in that region [24].
Th e area for injection is numbed using ice or topical anesthetic cream. In this case, the desired placement of fi ller is subcutaneous to try and stretch the defi cient skin as much as possible. Once again, a “haystack” or “linear threading” method is used to deliver the fi ller as smoothly as possible in this superfi cial location. Filler is placed along the inferior orbital rim, pre-septally, and pre-tar-sally. Posttreatment upward massage of the lower eyelid by the patient is recommended [24].
Results have been very encouraging with 70% of patients maintaining a fully corrected lower eyelid posi-tion for over twelve months. Bruising can occur in over 90% of cases and a bluish discoloration in two thirds. Th e author reports that lumpiness is rare using the linear threading method. No patients required dissolution of fi ller [24].
15.7 Future Developments
Soft -tissue fi llers are becoming key contributors to the management of orbital and periorbital volume defi ciency. Th is is due to their exemplary safety record, biocompati-bility, high tolerability, ease of administration, titratability, reversibility, and excellent results. It is likely that the

References 227
demand for such products will rise as physician and patient awareness of their potential applications increases. Th is will also refl ect the growing preference for patients to undergo minimally invasive treatments, as well as an increased demand for correction of orbital and periorbital asymmetries and contour abnormalities that may have previously been considered too minor for surgical inter-vention. Th e versatility of these products has also been shown in the ever expanding range of orbital and perior-bital pathologies that they have been successfully used for.
Future developments in this fi eld are likely to refl ect biomedical research into increased stability and longevity of hyaluronic acid products, whilst maintaining easy injectability as well as reversibility with the application of hyaluronidase. Novel compounds with longer tissue per-sistence or collagen-promoting characteristics may also emerge on the market. It is also hoped that FDA approval will be obtained for the orbital and periorbital application of existing products to remove the need for such treat-ments to occur off -label. In the meantime, increased use of soft -tissue fi llers by oculoplastic surgeons will add to the current literature and improve the documentation of existing treatment outcomes.
References
1. Airan LE, Born TM (2005) Nonsurgical lower eyelid lift . Plast Reconstr Surg 116:1785–1792
2. Apte RS, Solomon SD, Gehlbach P (2003) Acute choroidal infarction following subcutaneous injection of micronized dermal matrix in the forehead region. Retina 23:552–554
3. Balazs EA, Denlinger JL, Leshchiner E, et al (1988) Hyaluronan derivatives for soft tissue repair and augmen-tation. Biotech USA Nov:14–16, 442–445
4. Berman M (2000) Rejuvenation of the upper eyelid com-plex with autologous fat transplantation. Dermatol Surg 26: 1113–1116
5. Bosniak S, Cantisano-Zilkha M (2001) Restylane and Perlane: A six year clinical experience. Operative Techniques in Oculoplast, Orbital and Reconstr Surg 4:89–93
6. Broder KW, Cohen SR (2006) An overview of permanent and semipermanent fi llers. Plast Reconstr Surg 118 (Suppl):7S–14S
7. Buonaccorsi S, Leonardi A, Covelli E, et al (2005) Parry-Romberg stndrome. J Craniofac Surg 16:1132–1135
8. Buono LM (2004) Th e silent sinus syndrome: maxillary sinus atelectasis with enophthalmos and hypoglobus. Curr Opin Ophthalmol 15:486–489
9. Burroughs JR, Hernandez Cospin JR, Soparkar CN, Patrinley JR (2003) Misdiagnosis of silent sinus syndrome. Ophthal Plast Reconstr Surg 449–454
10. Cahil KV, Burns JA (1989) Volume augmentation of the anophthalmic orbit with cross-linked collagen (Zyplast®). Arch Ophthalmol 107:1684–1686
11. Carey DL, Baker D, Rogers GD, et al (2007) A randomized multicenter open-label study of poly-L-lactic acid for HIV-1 facial lipoatrophy. J Acquir Immune Defi c Syndr 46: 581–589
12. Carruthers A, Carruthers J (2007) Non-animal-based hyaluronic acid fi llers: scientifi c and technical consider-ations. Plast Reconstr Surg 120(6 Suppl):33S–40S
13. Ciuci PM, Obagi S (2008) Rejuvenation of the periorbital complex with autologous fat transfer: current therapy. J Oral Maxillofac Surg 66:1686–1693
14. Cline RA, Rootman J (1984) Enophthalmos:a clinical review. Ophthalmology 91:229–237
15. Coleman SR (1997) Facial recontouring with lipostructure Clin Plast Surg 24:347–367
16. Coleman SR (2004) Structural fat graft ing. Quality Medical Publishing, St Louis, MO
17. Coleman SR, Grover R (2006) Th e anatomy of the aging face: volume loss and changes on 3-dimensional topogra-phy. Aesthetic Surg J 26(1 Suppl):S4–S9
18. Da Silva AL, Bredemeier M, Gebrim ES, Moura Eda M (2008) Intraorbital polyacramide gel injection for the treat-ment of anophthalmic enophthalmos. Ophthal Plast Reconstr Surg 24:367–371
19. Danesh-Meyer HV, Savino PJ, Sergott RC (2001) Case reports and small case series: ocular and cerebral ischemia following facial injection of autologous fat. Arch Ophthalmol 119:777–778
20. DeLorenzi C, Weinberg M, Solish N, Swift A (2006) Multicenter study of the effi cacy and safety of subcutane-ous non-animal-stabilised hyaluronic acid in aesthetic facial contouring: interim report. Dermatol Surg 32:205–211
21. Donath AS, Glasgold RA, Glasgold MJ (2007) Volume loss versus gravity: new concepts in facial aging. Curr Opin Otolaryngol Head Neck Surg 15:238–243
22. Donofrio LM (2000) Fat distribution: a morphologic study of the aging face. Dermatol Surg 26:1107–1112
23. Fagien S, Klein A (2007) A brief overview and history of temporary fi llers: evolution, advantages and limitations. Plast Reconst Surg 120 (Suppl):8S
24. Fezza JP Nonsurgical treatment of cicatricial ectropion with hyaluronic acid fi ller (2008) Plast Reconstr Surg 121: 1009–1014
25. Flowers RS (1993) Tear trough implants for correction of tear trough deformity. Clin Plast Surg 20:403–415
26. Frileck SP (2002) Th e lumbrical fat graft : a replacement for lost upper eyelid fat. Plast Reconstr Surg 109:1696–1705
27. Goldberg RA (2000) Lower blepharoplasty is not about removing skin and fat. Arch Facial Plast Surg 2:22
228 15 Non-surgical Volume Enhancement with Fillers in the Orbit and Periorbital Tissues
15
28. Goldberg RA (2000) Transconjunctival orbital fat reposi-tioning: transposition of orbital fat pedicles into a subpe-riosteal pocket. Plast Reconstr Surg 105:743–748
29. Goldberg RA (2006) Periorbital Restylane®:my practice to yours. Aesth Surg J 86:69–71
30. Goldberg RA, Fiashetti D (2006) Filling the orbital hollows with hyaluronic acid gel: initial experience with 244 injec-tions. Ophthal Plast Reconstr Surg 22:335–341
31. Goldberg RA, McCann JD, Fiaschetti D, Ben Simon GJ (2005) What causes eyelid bags? Analysis of 114 consecu-tive patients. Plast Reconstr Surg 115:1395–402
32. Goldberg RA, Lee S, Jayasundera T, et al (2007) Treatment of lower eyelid retraction by expansion of the lower eyelid with hyaluronic acid gel. Ophthal Plast Reconstr Surg 23:343–348
33. Gravier MH, Bass LS, Busso M, et al (2007) Calcium hydroxlapatite (Radiesse) for correction of the mid- and lower face: concensus recommendations. Plast Reconstr Surg 120(Suppl):55S–66S
34. Hamra S (1995) Arcus marginalis release and orbital fat preservation in midface rejuvenation. Plast Reconst Surg 96:354–362
35. Hester TR, Codner MA, McCord CD, et al (1988) Transorbital lower lid and midface rejuvenation. Oper Tech Plast Reconstr Surg 5:163
36. James J, Carruthers A, Carruthers J (2002) HIV-associated facial lipoatrophy. Dermatol Surg 28:979–986
37. Kane MAC (2005) Treatment of tear trough deformity and lower lid bowing with injectable hyaluronic acid. Aesth Plast Surg 29:363–367
38. Knapp TR, Kaplan EN, Daniels JR (1977) Injectable colla-gen for soft -tissue augmentation. Plast Reconst Surg 60:389
39. Kotlus BS, Dryden RM (2007) Correction of anophthalmic enophthalmos with injectable calcium hydroxlapatitie (Radiesse). Ophthal Plast Reconstr Surg 23:313–314
40. Kranendonk S, Obagi S (2007) Autologous fat transfer for periorbital rejuvenation: indications, technique, and com-plications. Dermatol Surg 33:572–578
41. Levy RM, Redbord KP, Hanke CW (2008) Treatment of HIV lipoatrophy and lipoatrophy of aging with poly-l-lac-tic acid: a prospective 3-year follow-up study. J Am Acad Dermatol 59:923–933
42. Lowe N, Maxwell A, Patnaik R (2005) Adverse reactions to dermal fi llers: review. Dermatol Surg 31:1616–1625
43. Macfarlane R, Levin AV, Weksberg R, et al (1995) Absence of the greater sphenoid wing in neurofi bromatosis type 1: congenital or acquired: case report. Neurosurgery 37: 129–133
44. Malhotra R (2007) Deep orbital sub-Q Restylane (Nonanimal stabilized hyaluronic acid) for orbital volume enhancement in sighted and anophthalmic orbits. Arch Ophth 125:1623–1629
45. Mancici R, Taban M, Lowinger A, et al (2009) Use of hyaluronic acid gel in the management of paralytic lago-phthalmos: the hyaluronic acid gel “gold weight”. Ophthal Plast Reconstr Surg 25:23–26
46. Miller JJ, Popp JC (2002) Fat hypertrophy aft er autologous fat transfer. Ophthal Plast Reconstr Surg 18:228–231
47. Morley AM, Malhotra R (2009) Th e use of hyaluronic acid fi ller (Perlane®) for tear trough rejuvenation as an alterna-tive to lower eyelid surgery. Ophthal Plast Reconstr Surg (in press)
48. Morley AM, Taban M, Malhotra R, Goldberg RA (2009) Use of hyaluronic acid gel for upper eyelid fi lling and con-touring. Ophthal Plast Reconstr Surg (in press)
49. Pessa JE, Zadoo V, Mutimer K, et al (1998) Relative maxil-lary retrusion as a natural consequence of aging: combining skeletal and soft -tissue changes into an integrated model of midfacial aging. Plast Reconstr Surg 102:205–212
50. Pessa JE, Desvigne LD, Lambros VS, et al (1999) Changes in ocular globe-to-orbital rim position with age: implica-tions for aesthetic blepharoplasty of the lower eyelids. Aesth Plast Surg 23:337–342
51. Piacquadio D (1994) Crosslinked hyaluronic acid gel (hylan gel) as a soft tissue augmentation material: A pre-liminary assessment. In: Elson ML (ed) Evaluation and treatment of the aging face. Springer-Verlag, New York, pp 304–308
52. Ross J, Malhotra R (2009) Orbitofacial rejuvenation of temple hollowing with Restylane Perlane injectable fi ller. Presentation at the British Oculoplastic Surgery Society Annual Meeting.
53. Schanz S, Schippert W, Ulmer A, et al (2002) Arterial embolization caused by injection of hyaluronic acid (Restylane). Br J Dermatol 146:928–929
54. Seiff SR (2002) Th e fat pearl graft in ophthalmic plastic sur-gery: everyone wants to be a donor! Orbit Jun;21:105–109
55. Shin H, Lemke BN, Stevens TS, Lim MJ (1988) Posterior ciliary artery occlusion aft er subcutaneous silicone-oil injection. Ann Ophthalmol 20:342–344
56. Shorr N, Christenbury JD, Goldberg RA (1988) Free autog-enous “pearl fat” graft s to the eyelids. Ophthal Plast Reconstr Surg 4:37–40
57. Simamora P, Chern W (2006) Ploy-L-lactic acid: an over-view. J Drugs Dermatol 5:436–440
58. Stegman SJ, Chu S, Armstrong RC (1988) Adverse reac-tions to bovine collagen implant: clinical and histological features. J Dermatol Surg Oncol 14:39–48
59. Steinsapir KD, Steinsapir SM (2006) Deep-fi ll hyaluronic acid for the temporary treatment of the naso-jugal groove: a report of 303 consecutive treatments. Ophthal Plast Reconstr Surg 22:344–348
60. Talar-Williams C, Sneller MC, Langford CA, et al (2005) Orbital socket contracture: a complication of infl ammatory

References 229
orbital disease in patients with Wegener’s granulomatosis. Br J Ophthalmol 89:493–497
61. Teimourian B (1988) Blindness following fat injections. Plast Reconstr Surg 82:361
62. Tzikas TL (2008) A 52-month summary of results using calcium hydroxlapatite for facial soft tissue augmentation. Dermatol Surg 34(Suppl):S9–15
63. Vagefi MR, McMullan TF, Burroughs JR, et al (2007) Injectable calcium hydroxlapatite for orbital volume aug-mentation. Arch Facial Plast Surg 9:439–442
64. Zimbler MS, Kokoska MS, Th omas JR (2001) Anatomy and pathophysiology of facial aging. Facial Plast Surg Clin North Am 9:179–187
Index
Adenoid cystic carcinoma, 134, 135Angiography, 164Anophthalmos, congenital. See Congenital
clinical anophthalmosAzithroprine, 58
Bacterial canaliculitis, 70Beta-blockers, 169Blepharoplasty. See Lower blepharoplasty;
Upper blepharoplastyBreast carcinoma, 54, 55, 178Brow suspension, unilateral ptosis. See also
Levator muscle recessioncompensatory eyebrow elevation, 117–118congenital dystrophic ptosis, 118fascia implantation, 122–123frontalis muscle, innervation patterns, 118harvesting autogenous fascia lata, 121–122levator muscle recession, 119–121materials, 121mechanical principals, 122partial or total levator muscle recession
planning, 118–119surgical technique, 121–123upper lid approach, 122
Canalicular infl ammationanatomy, 67–68bacterial canaliculitis, 70chemotherapeutic agents, 71–72dacryocystorhinostomy and retrograde
canaliculostomy, 74–75drug eruptions, 71embryology, 67etiology, 67, 68histology, 68iatrogenic causes, 71–73infective causes, 69, 70Jones canalicular bypass tube placement, 75lacrimal stents and plugs, 73lichen planus (LP), 70microbial canaliculitis, 69ocular cicatricial pemphigoid, 70–71pathophysiology, 68–69physiology, 68radiotherapy, 72–73surgical management, 74–75systemic infl ammatory disease, 70–71
topical ophthalmic treatments, 73Carcinoid tumor, 179–180Cavernous hemangioma, 134, 135Collagen fi llers, 216Computed tomography (CT)
bone window CT scan, 126–127, 128diagrammatic representation, 125–126iodinated intravenous contrast agents, 127, 128orbital and periorbital structures, 126orbital diseases, 126, 127scanners, 127–128
Congenital clinical anophthalmosage, 106associated systemic and ocular diseases, 107–110birth, 107examination, 106family history, 106–107nasolacrimal system fi ndings, 111–112, 114–115neuroradiological fi ndings, 111, 113–114patient data, 106patients, 106pregnancy history, 107systemic diseases, 114unilateral microphthalmos, 113
Conjunctival MALT lymphoma, 3Corticosteroids, 54–55Cosmetic oculofacial plastic surgery
endoscopic brow lift , 23, 25–29facial analysis, 22–25lower blepharoplasty, 33–43upper blepharoplasty, 29–33
Dacryocystorhinostomy, 74–75Dermoid cyst, 134–135, 136Docetaxel (Taxotere), 72
Endoscopic brow lift anesthesia, 26eyebrow elevation, 25–26frontalis contraction, 23, 26postoperative care, 27–29retro orbicularis oculi fat (ROOF) defl ation, 23, 25surgical procedure, 26–27
Esophageal carcinoma, 176Etanercept, 59Eyelid blepharoplasty. See Lower blepharoplasty;
Upper blepharoplasty
232 Index
Facial analysisaging, 22facial layers, 22fat loss, 22, 23workup sheet, 23, 24–25
Fibrous dysplasia, 135, 1365-Fluorouracil (5-FU), 71–72Follicular lymphoma
cytogenesis, 6imaging fi ndings, 8incidence, 2pathogenesis, 3pathology, 5treatment, 11, 12
Hemangioma. See Infantile hemangioma (IH)Hyaluronic acid fi llers, 216Hydroxyapatite (HA) implants. See also Orbital implants
advantages, 196–197vs. aluminum oxide (Bioceramic) implant, 198, 199Bio-Eye, 197complication, 197FCI3 implants, 197vs. porous polyethylene implants, 197
Idiopathic orbital infl ammatory syndrome (IOIS), 57alkylating agents, 58–59anatomic location, 48anatomic site, 49antimetabolites, 58biologic agents, 59corticosteroids, 57–58orbital biopsy, 56diff erential diagnosis, 48, 50management algorithm, 57neoplasm, 53–54, 55orbital cellulites, 50–52pediatric IOIS, 60radiation, 58sarcoidosis, 52sclerosing pseudotumor, 60–61T-cell inhibitors, 59thyroid eye disease (TED), 49–50Tolosa–Hunt syndrome (THS), 62–63Wegener granulomatosis, 52–53
Infantile hemangioma (IH)active nonintervention, 164–165beta-blockers, 169classifi cation, 162clinical phases, 161diff erential diagnosis, 162–163embolization, 168etiology, 161–162histology, 162interferon-alfa, 166–167investigation, 163–164ocular complications, 163pulsed-dye laser (PDL), 167–168steroids, 165–166surgery, 168–169treatment indications, 165vincristine, 167
Infl iximab, 59Injectable soft -tissue fi llers
advantages, 215collagen fi llers, 216complications, 215–216hyaluronic acid fi llers, 216lower eyelid elevation, 226orbit, 217, 219preorbital volume loss (see Preorbital volume loss)semipermanent injectable soft -tissue fi llers, 216–217tear trough, 220–223, 224temple and brow, 223–224types, 216–217upper eyelid and brow, 220, 221volume replacement, 215
Interferon-alfa, 166–167Iodinated intravenous contrast agents, 127, 128
Jones canalicular bypass tube placement, 75
Lacrimal canalicular infl ammation and occlusion. See Canalicular infl ammation
Lacrimal drainage systemDCR, lacrimal sac biopsy, 97–99diagnosis, 95, 96lacrimal sac lesions, 99–103lacrimal sac tumors, 95, 96lesions, treatment and prognosis, 99–103malignant melanoma, 100, 101oncocytoma, 100, 102primary non-Hodgkin B-cell lymphoma (MALT),
99, 100pyogenic granuloma, 101, 102sarcoidosis, 101, 103squamous cell carcinoma, 99, 100surgical anatomy, 96–97Wegener granulomatosis, 101, 103
Lacrimal stents and plugs, 73Levator muscle recession
approach, 119eyelid level evolution, 121partial levator recession, 119, 120principle, 119total levator muscle recession, 119, 121undercorrection and overcorrection, 121
Lichen planus (LP), 70Lower blepharoplasty
fat protrusion and infraorbital hollowness, 35–36fat removal vs. fat preservation, 36–37inferior orbital rim and bony midface, 36, 37infralash muscle plication blepharoplasty, 38, 39lid retraction and ectropion, 35lower eyelid and midface, 33, 34lower eyelid fi llers, 39–41, 42midface implants, 41, 42–43midface retrusion, 36, 37skin excess, 33, 35transconjunctival blepharoplasty, 35, 36transconjunctival fat repositioning, 38–40
Lung carcinoma, 178–179Lymphangioma, 136, 137Lymphoma, 136, 137
Index 233
Magnetic resonance imaging (MRI)components, 129image creation, 131–134Larmor frequency, 129–130spinning tops, 129, 130T1 constant, 130–131T2 constant, 132, 133
Malignant peripheral nerve sheath tumors, 81Malignant schwannomas. See Malignant peripheral
nerve sheath tumorsMantle cell lymphoma
clinical features, 7cytogenesis, 6, 7histology, 4–6
Melanoma, 100, 101, 179Metastatic orbital tumors
biopsy, 177–178breast carcinoma, 178carcinoid tumor, 179–180chemotherapy, 180clinical features, 175–176diff erential diagnosis, 180epidemiology, 173–174hormonal therapy, 180–181imaging and patterns, 176–177lateralization, 174localization, 174–175lung carcinoma, 178–179melanoma, 179metastasis, biological behavior and timing, 174prognosis and survival, 181prostatic cancer, 179radiotherapy, 180surgery, 181
Methicillin-resistant Staphylococcal aureus (MRSA) infection, 153–154
Methotrexate, 58Microbial canaliculitis, 69Mitomycin C therapy, 73Mucosa-associated lymphoid tissue (MALT)
chronic antigen stimulation, 3clinical features, 7imaging fi ndings, 8lymphoepithelial unit, 4pathology, 4PET scan, 10, 11radiotherapy, 12
Myositis, 136, 138
Neurofi bromas, 80–81Neurofi bromatosis type 1 (NF1). See also Orbitofacial
neurofi bromatosis type 1 (NF1)clinical manifestations, 79–80diagnostic criteria, 80genetics, 83malignant peripheral nerve sheath tumors, 81medical management, 84neurofi bromas, 80–81nomenclature, 79optic pathway gliomas, 81–82surgical management, 84–90
Nonporous spherical implants, 199–200Non-surgical volume enhancement. See Injectable
soft -tissue fi llers
Ocular adnexal lymphoproliferative disease (OALD)chemotherapy, 12chronic antigen stimulation, 3classifi cation, 2clinical features, 7cluster of diff erentiation (CD), 2cytogenetics, 4–6, 7follicular lymphoma, 11imaging fi ndings, 8, 9immunosuppression, 3–4immunotherapy, 12–13incidence, 1mantle cell lymphoma, 11outcome, 13pathogenesis, 2–3pathology, 4–6positron emission tomography, 9radioimmunotherapy, 13radiotherapy, 11–12staging, 9treatment, 9–11
Ocular cicatricial pemphigoid, 70–71Oncocytoma, 100, 102Optic pathway gliomas (OPGs)
anterior approach, 88blind proptotic left eye, 81imaging and chemotherapy, 82lateral approach, 87orbital imaging, 138progression, 82proptosis, surgical intervention, 87–88remission, 82superior approach, 88
Orbital and periorbital malignanciescetuximab, 191–192imatinib mesylate, 190–191rituximab, 188–189yttrium-90-labeled ibritumomab tiuxetan, 189–190
Orbital cellulitis, 50–52evaluation, 154–155medical therapy, 155–156prevention, orbital fracture, 158surgical treatment, 156–158
Orbital imagingadenoid cystic carcinoma, 134, 135cavernous hemangioma, 134, 135computed tomography (CT) (see Computed
tomography (CT))dermoid cyst, 134–135, 136diff usion MRI (diff usion-weighted imaging), 140–141fi brous dysplasia, 135, 136lymphangioma, 136, 137lymphoma, 136, 137magnetic resonance imaging (see Magnetic
resonance imaging (MRI))myositis, 136, 138optic nerve gliomas, 138positron emission tomography, 141–142
234 Index
pseudotumor, 139rhabdomyosarcoma, 139three-dimensional images, 129ultrasound (echography) (see Ultrasound (echography))
Orbital implants. See also Hydroxyapatite (HA) implantsadults, 199–200children, 200–201extraocular muscle attachment, 202–203implant wrapping, 202peg and sleeve implants (see Peg and sleeve
implant–prosthesis coupling systems)porous orbital implants, 197–199 (see also Porous
orbital implants)volume considerations, 201wrapping materials (see Wrapping materials)
Orbital volume loss. See also Injectable soft -tissue fi llersetiology, 213, 214features, 214–215
Orbitofacial neurofi bromatosis type 1 (NF1). See also Optic pathway gliomas (OPGs)
malignant peripheral nerve sheath tumors, 81neurofi bromas, 80–81optic pathway gliomas, 81–82orbital involvement, 86–90periorbital involvement, 85progression, 90–92surgery timing, 84–85surgical management, 84–90
Parry–Romberg syndrome, 220Pediatric IOIS, 60Peg and sleeve implant–prosthesis coupling systems
FCI peg–sleeve coupling system, 205fi brovascularization, 205MEDPOR Motility Coupling Post (MCP), 205polycarbonate peg, 205titanium peg systems, 205
Periocular herpes simplex infection, 69Periorbital cellulitis
CA-MRSA vs. hospital-acquired MRSA, 152–153etiology, 151infection, 149–150microbiology, 151–152orbital MRSA, 153–154pathogens and resistance, 152–154symptomatology and presentation, 149–150
PHACE syndrome, 162, 163Plexiform neurofi broma
malignant peripheral nerve sheath tumors, 80upper eyelid, 80–81
Porous orbital implantsaluminum oxide, 198–199bio-eye implant, 197FCI3 implants, 197fi brovascular ingrowth, 196–197polyethylene implants (MEDPOR), 197–198
Porous spheres, 199Pre-and postoperative internal ptosis repair, 33Preorbital volume loss
cicatricial ectropion, 226etiology, 213–214
features, 215injectable soft -tissue fi llers, 225–226lower eyelid elevation, 226upper eyelid loading, 226volume enhancement, 225
Preservative-related chronic conjunctivitis, 73Primary non-Hodgkin B-cell lymphoma (MALT), 99, 100Proptosis
anterior approach, 88lateral approach, 87superior approach, 88
Prostatic cancer, 179Pseudotumor, 139Pulsed-dye laser (PDL), 167–168Pyogenic granuloma, 101, 102
Quasi-integrated implant, 199
Retro orbicularis oculi fat (ROOF) defl ation, 23, 25, 26Rhabdomyosarcoma, 139Rituximab
B-cell lymphomas, 189CD20, 188–189cyclophosphamide, adriamycin, vincristine, and
prednisone (CHOP), 189
Sarcoidosis, 52, 54, 101, 103Sclerosing pseudotumor, 60–61Semipermanent injectable soft -tissue fi llers, 216–217Soft -tissue fi llers. See Injectable soft -tissue fi llersSPRED1 mutation, 83Squamous cell carcinoma, 63, 99, 100Steroids
intralesional corticosteroid injection, 165–166oral corticotherapy, 166topical steroid, 165
Stevens–Johnson syndrome (SJS), 71
T-cell inhibitors, 59Th yroid eye disease (TED), 49–50Tolosa–Hunt syndrome (THS), 62–63Typical idiopathic orbital infl ammatory
syndrome (IOIS), 57
Ultrasound (echography)extraocular muscle, 145kinetic echography, 143, 145optic nerves, 146quantitative echography, 143topographic echography, 143–146
Unilateral ptosis, brow suspensioncompensatory eyebrow elevation, 117–118congenital dystrophic ptosis, 118frontalis muscle, innervation patterns, 118levator muscle recession, 119–121partial or total levator muscle recession planning,
118–119surgical technique, 121–123

Index 235
Upper blepharoplastyanesthesia, 30brow volumizing, 30–32crease formation, 30, 31excess lateral skin, management, 30, 32marking, 30patient evaluation, 29–30pre- and postoperative internal ptosis repair, 31, 33skin/muscle excision, 30
Wegener granulomatosis, 52–54, 101, 103Wrapping materials
human donor sclera, 203microporous expanded polytetrafl uoroethylene
(e-PTFE), 203polyester-urethane like e-PTFE, 203–204polyglactin 910 mesh, 204vicryl mesh-wrapped implants, 204

















