66
ORBITAL PATHOLOGIES Dr. Mohit Goel JRIII
| Date post: | 17-Aug-2015 |
| Category: |
Education |
| Upload: | dr-mohit-goel |
| View: | 72 times |
| Download: | 0 times |

ORBITAL PATHOLOGIES
Dr. Mohit GoelJRIII

TRAUMA
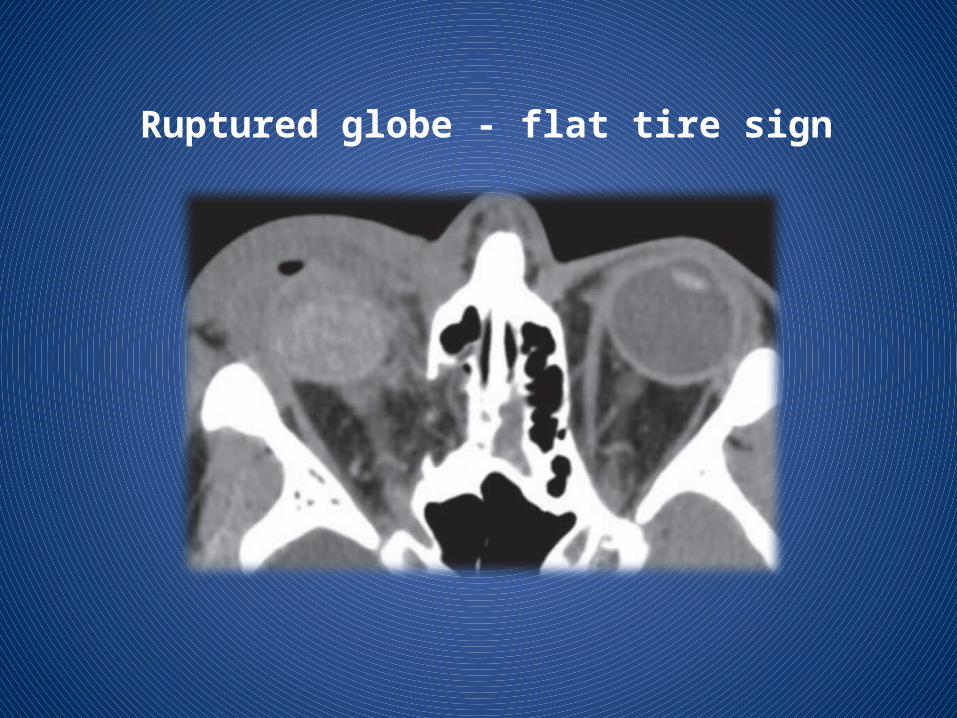
Ruptured globe - flat tire sign
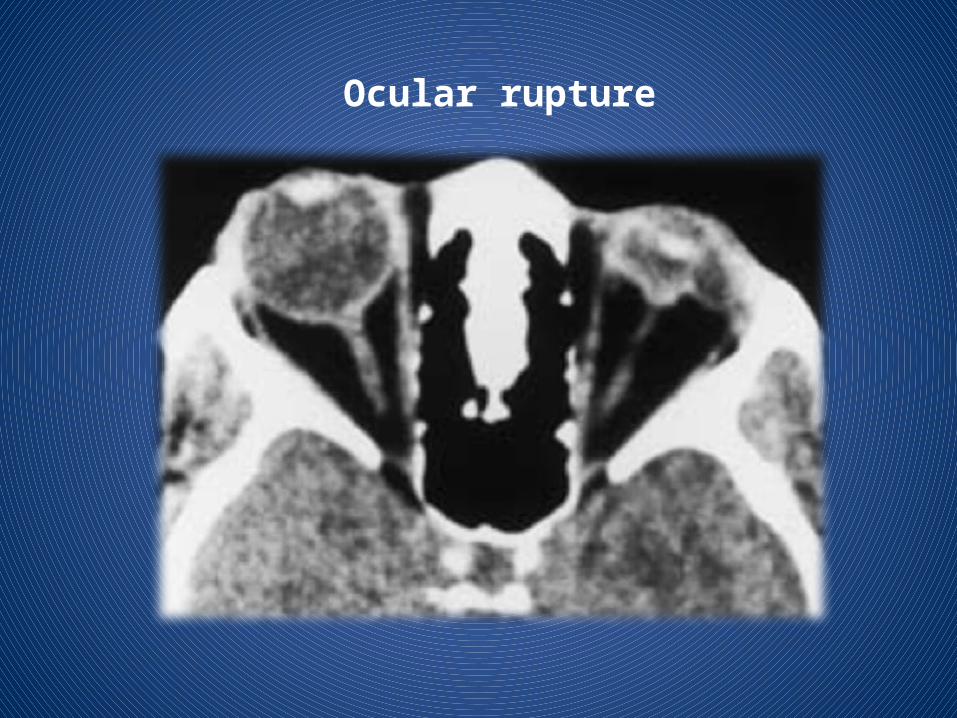
Ocular rupture
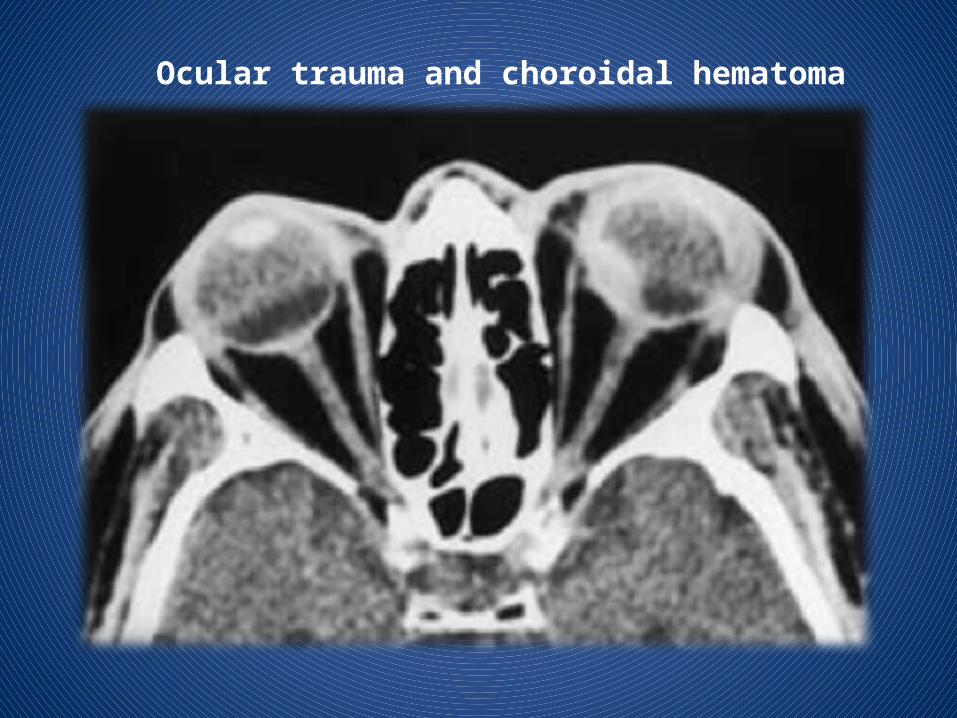
Ocular trauma and choroidal hematoma

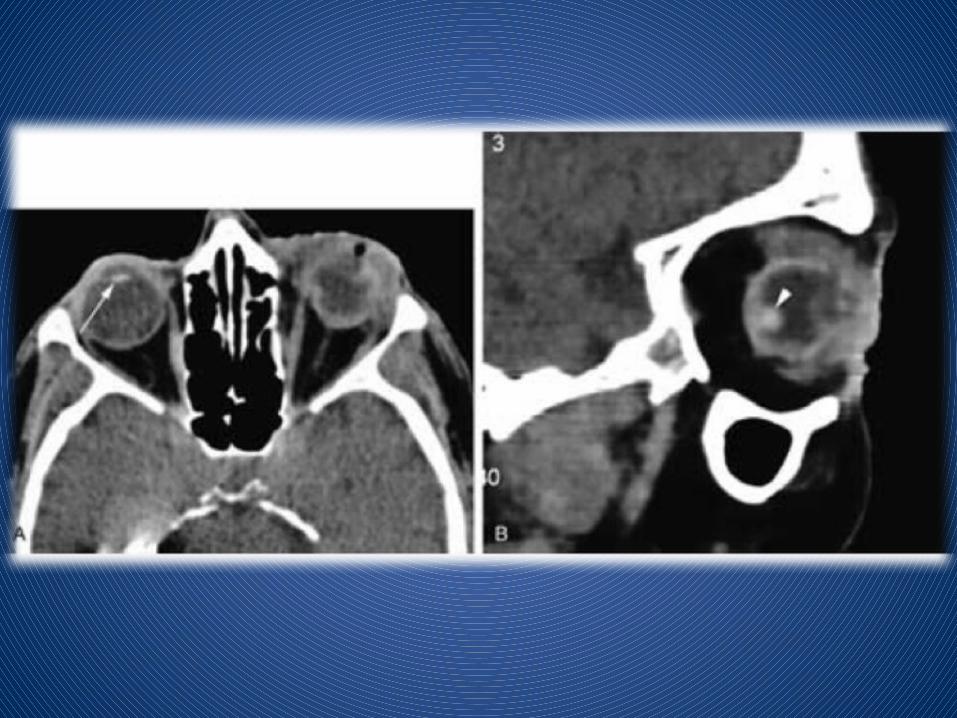
Choroidal hematoma following ocular surgery

Perforation and collapse of the globe



Partially dislocated lens

Perforation of the cornea

Corneal laceration
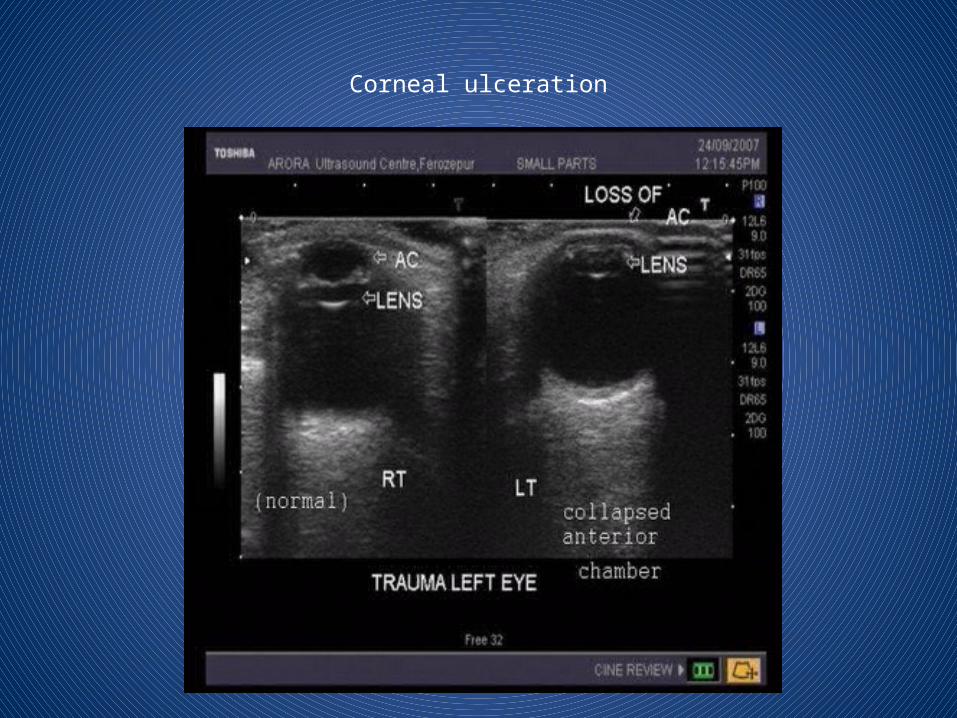
Corneal ulceration

Acute perforation of the lens capsule
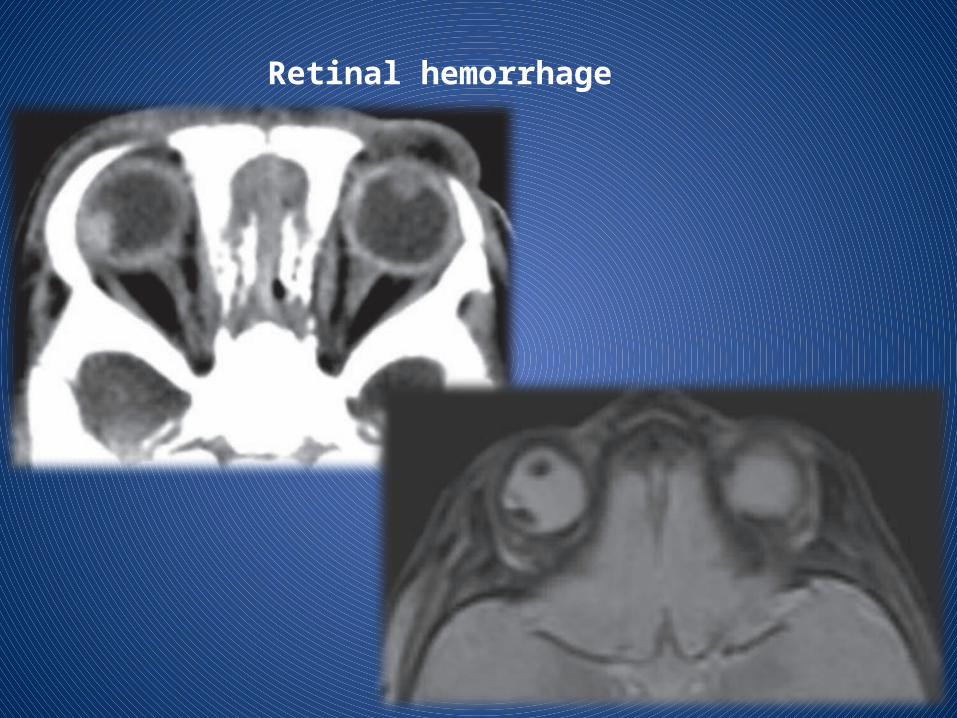
Retinal hemorrhage

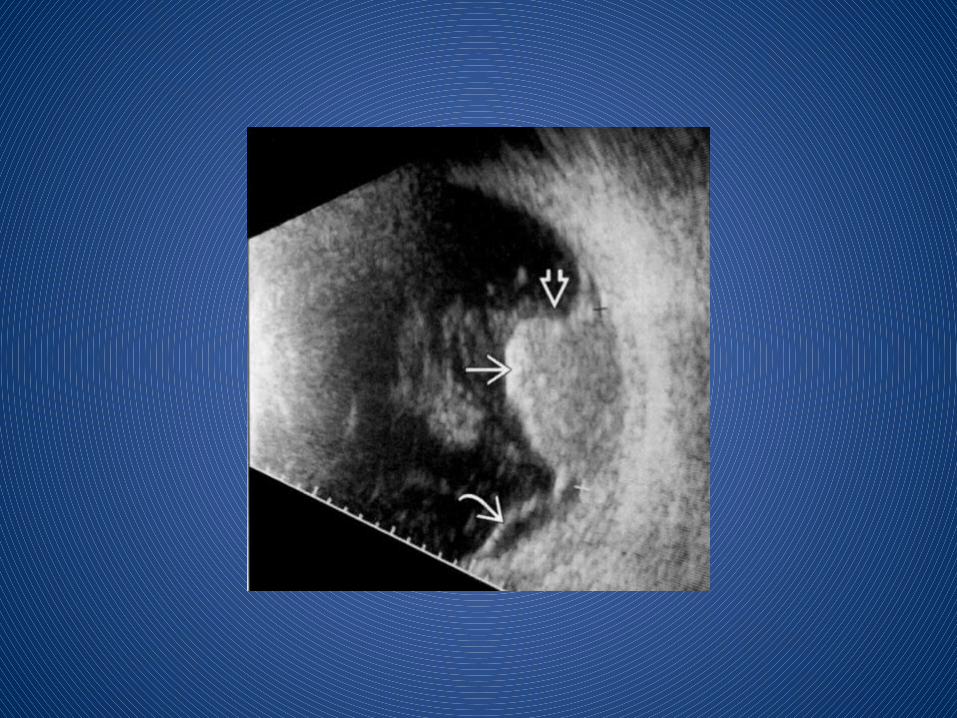
Configuration of collection is cresent shaped or V shaped on axial sections. Limbs of V represent detached leaves of retina converging towards optic disc represent the apex of V.
Collection anteriorly extend upto ora serrata represent anterior limit due to normal anterior attachment of retina.
Retinal detachment
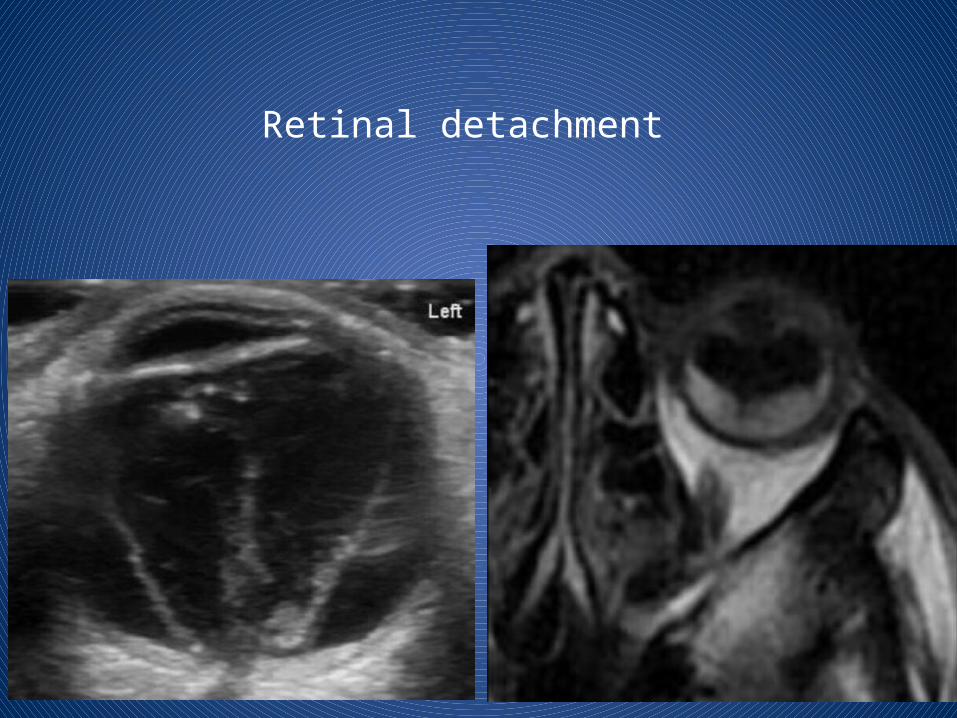
Retinal detachment

Choroidal detachmentChoroidal detachment is accumulation of blood or fluid in supra choroidal space between choroid and sclera, so collection extend circumferentially along the entire supra choroidal space , configuration is lentiform shaped along medial as well as lateral wall of globe, choroid bulging medially on either side giving so called kissing choroid sign.
Anteriorly extend upto ciliary bodies and posterior limit formed by anchoring effect of short posterior ciliary arteries and nerves preventing convergence of detached choroidal leaves to a single point.
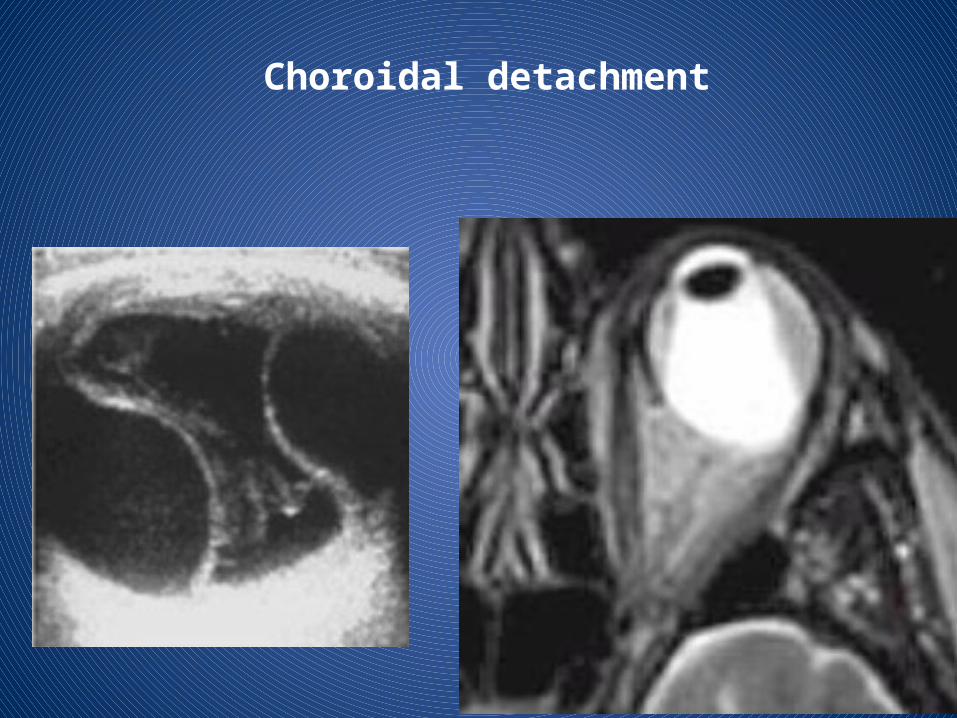
Choroidal detachment

Posttraumatic hemorrhagic choroidal detachment

Vitreous hemorrhage

MR imaging may be of value, particularly for detecting nonmetallic foreign bodies.
However, a metallic foreign body must be definitively ruled out before MR imaging is performed.
Failure to detect a metallic foreign body before performing MR imaging may result in blindness.
Fortunately, CT is a very sensitive imaging modality that can demonstrate metal fragments less than 1 mm in size.
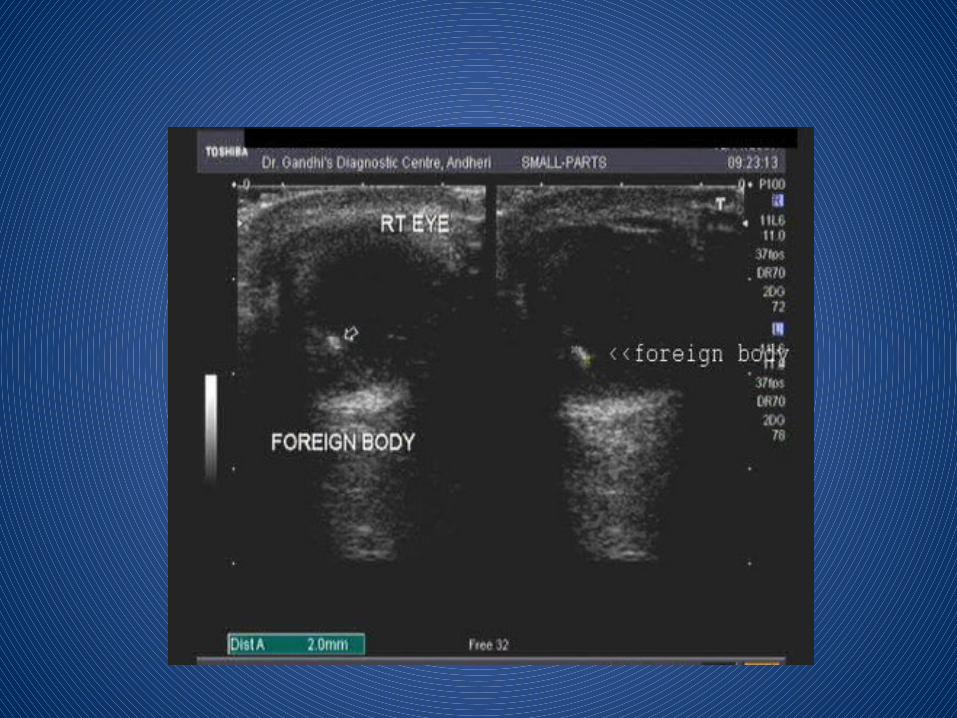
FOREIGN BODY
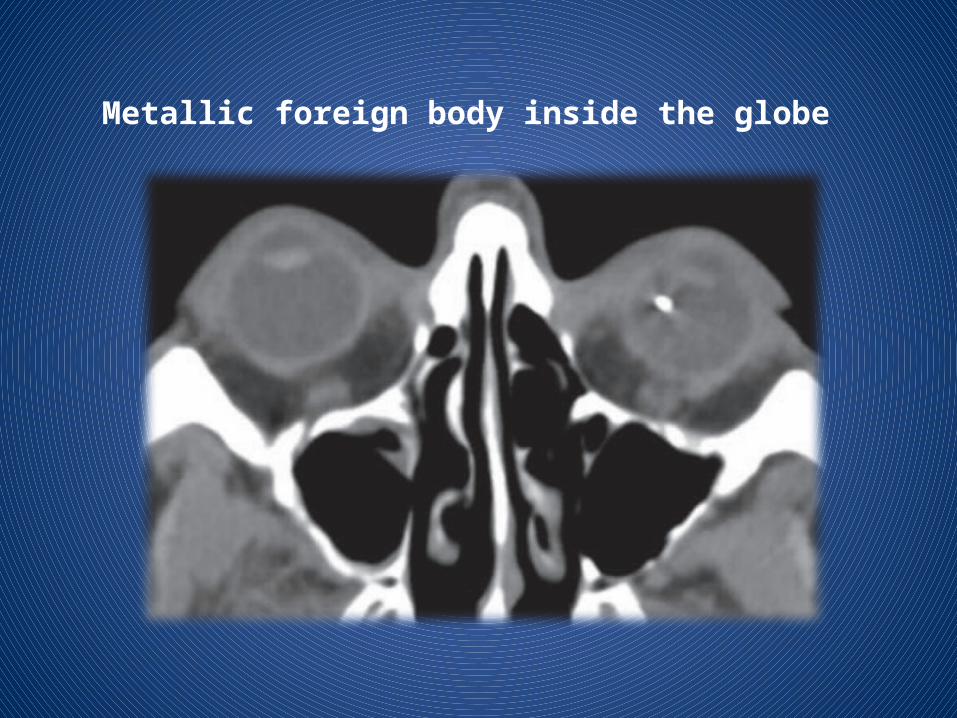
Metallic foreign body inside the globe
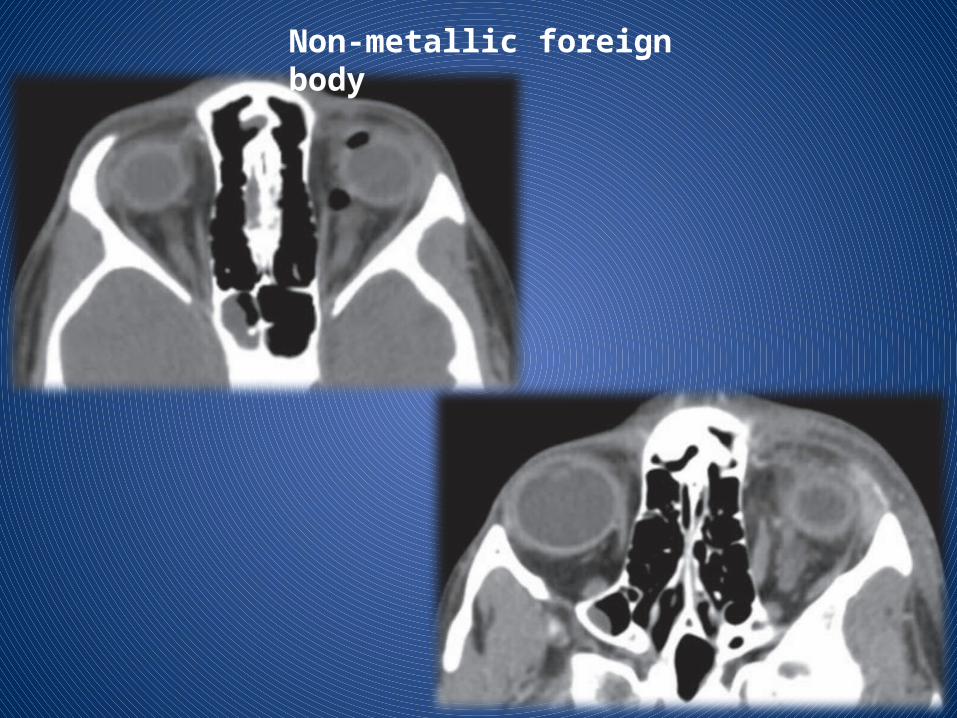
Non-metallic foreign body


Traumatic Carotid cavernous fistula
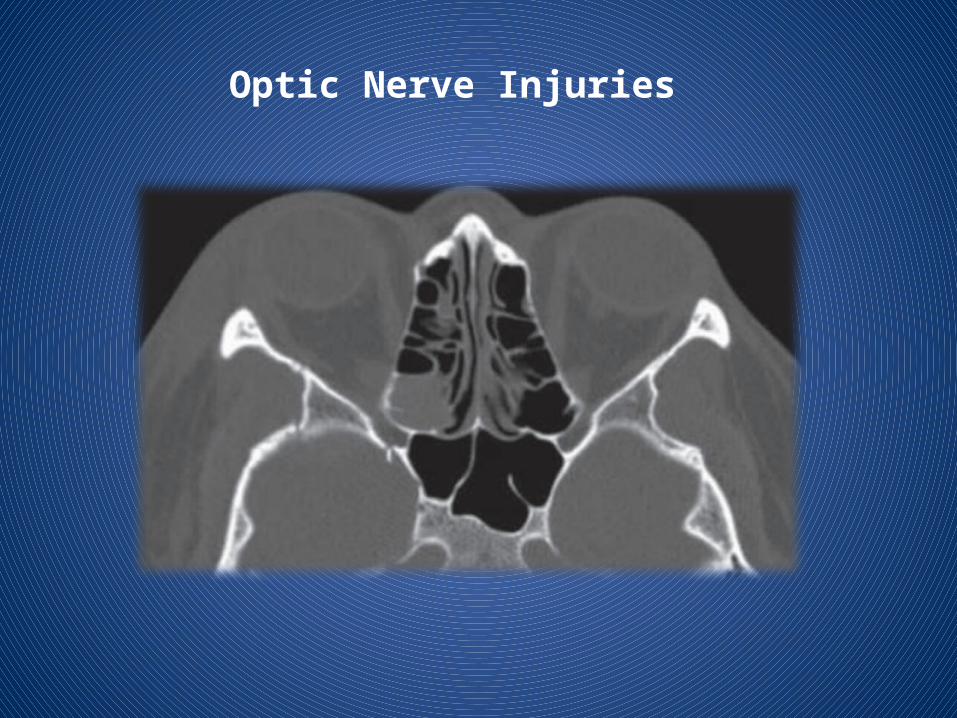
Optic Nerve Injuries
ORBITAL INFECTIONS

IDIOPATHIC ORBITAL INFLAMMATORY DISEASE
Orbital pseudotumour is an idiopathic inflammatory condition that usually involves the extraocular muscles although, in some cases there is inflammatory change involving the uvea, sclera, lacrimal gland and retrobulbar soft tissues.



Orbital and periorbital cellulitis
It is important to differentiate between orbital and periorbial cellulitis, as this has theraputic and prognostic implications:
1. peri-orbital cellulitis (pre-septal cellulitis) is limited to the soft tissues anterior to the orbital septum. This condition is often managed with oral antibiotics
2. orbital cellulitis refers to a post-septal infection (i.e. is behind or extends posterior to the orbital septum). This is a more serious condition requiring hospitalisation and parental antibiotics.
Complications such as intraorbital abscess formation may require surgical intervention


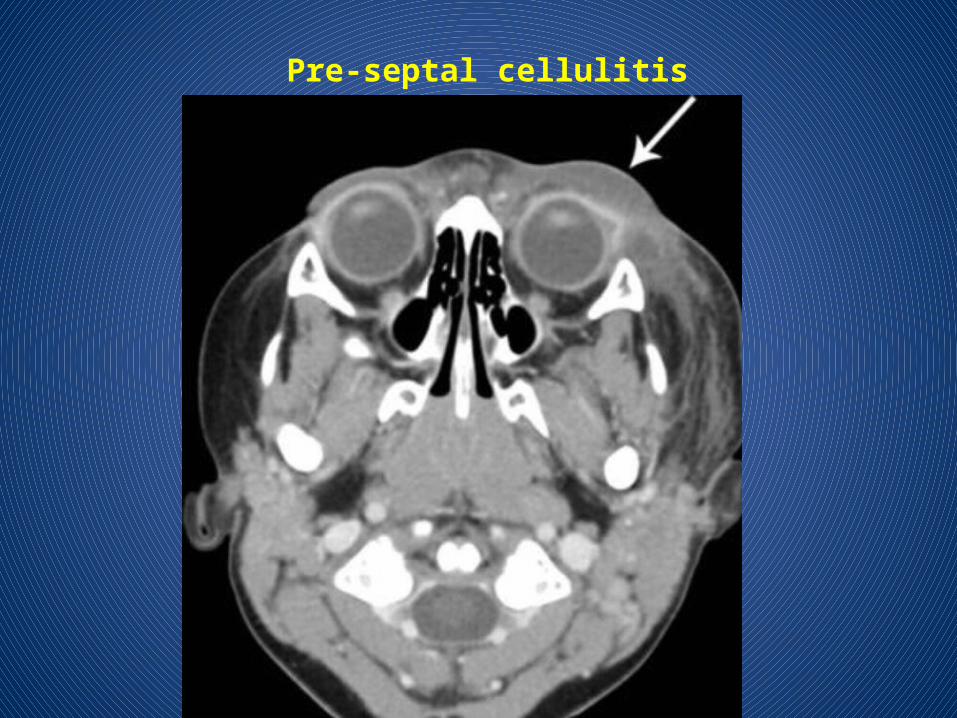
Pre-septal cellulitis

Pre-septal cellulitis
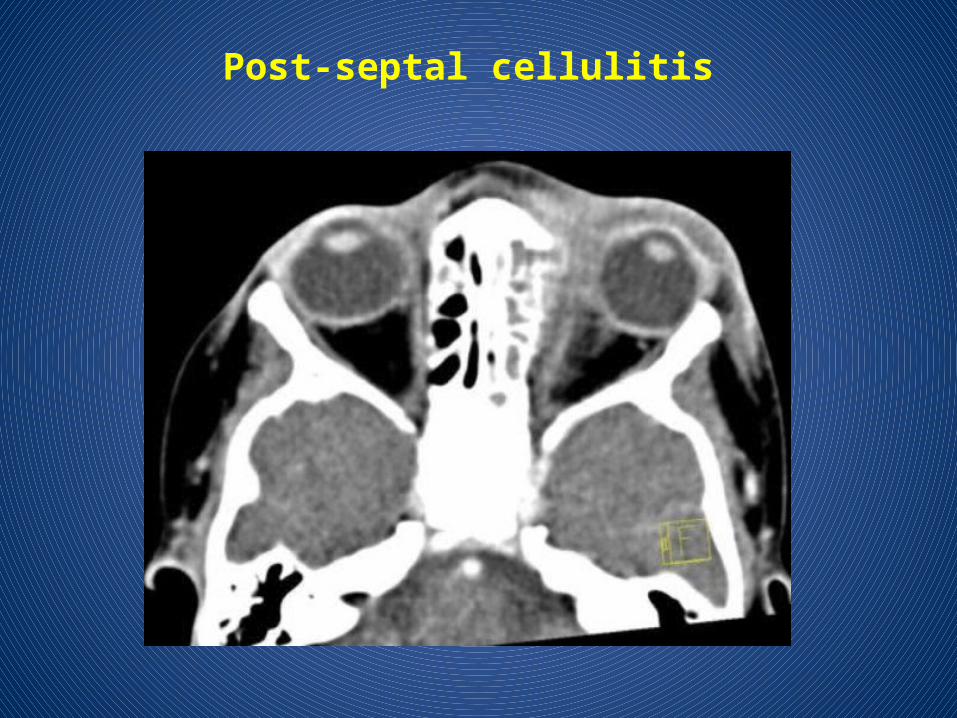
Post-septal cellulitis

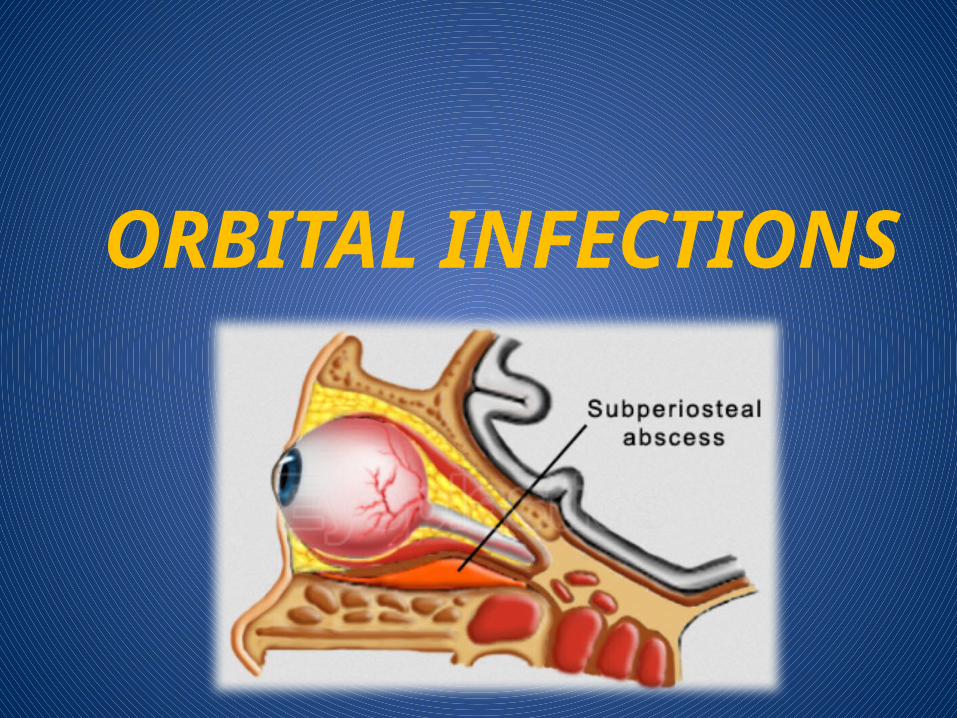
SUBPERIOSTEAL ABSCESS
Accumulation of pus between orbital wall (usually medial) and orbital periosteum.

OPTIC NEURITIS
Acute inflammation of optic nerve , commonly associated with multiple sclerosis.
Edema and inflammatory cells infiltrate the nerve resulting in uniform swelling and focal demyelination.
Imaging : MRI is the modality of choice with hyper intense signal of T2WI due to fluid and edema. Fat Sat contrast enhanced T1WI will show areas of demyelination. CT relatively insensitive.
Straightening and thickening of right optic nerve.

Optic Neuritis. CE Fat Sat T1W axial (B) MR images demonstrate subtle enlargement and enhancement of the left optic nerve (curved arrow).
T2WI (C) demonstrates corresponding increased signal intensity (straight arrow).
Thyroid associated orbitopathy
It is the most common cause of proptosis in adults, and is most frequently associated with Graves disease.
The extra-ocular muscles are involved in a predictable fashion as remembered by the I'M SLOW mnemonic.
Involvement of the rectus muscles in decreasing order of frequency:1. inferior2. medial3. superior4. lateral5. obliques


Neoplastic lesions

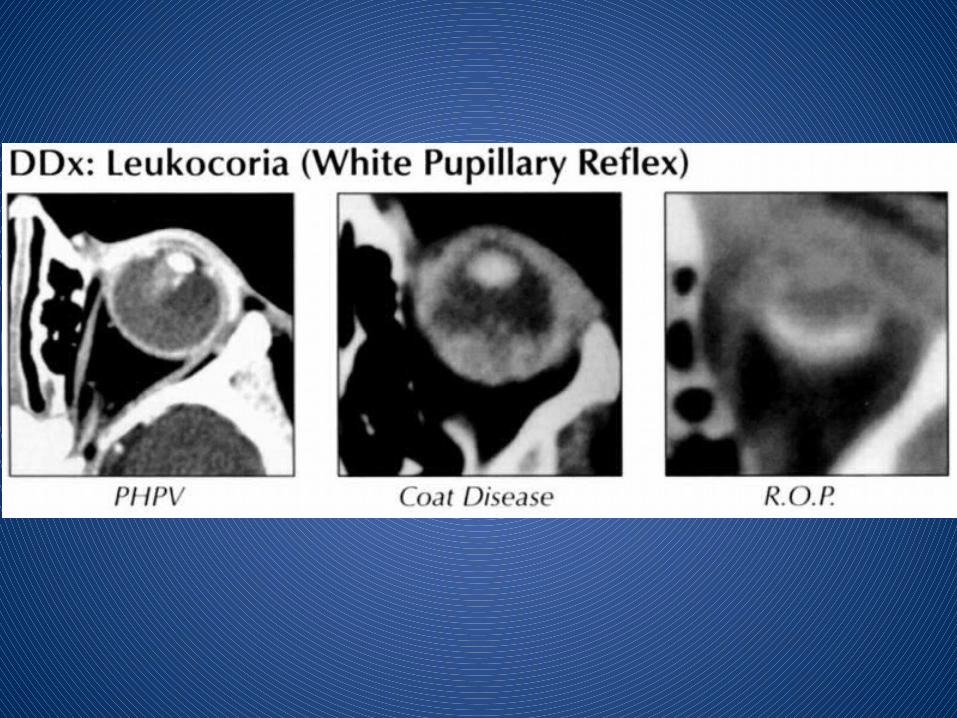
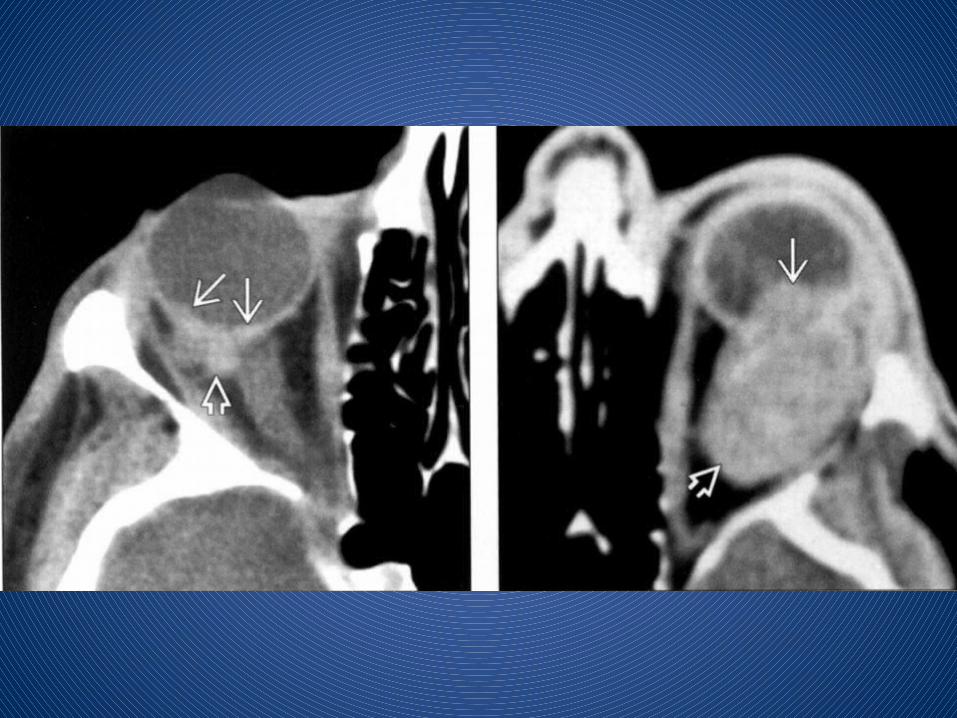
RETINOBLASTOMA


Trilateral RB: Bilateral ocular tumors plus midline intracranial neuroblastic tumor, typically pineal
Quadrilateral (tetralateral) RB: Bilateral disease plus pineal and suprasellar tumor
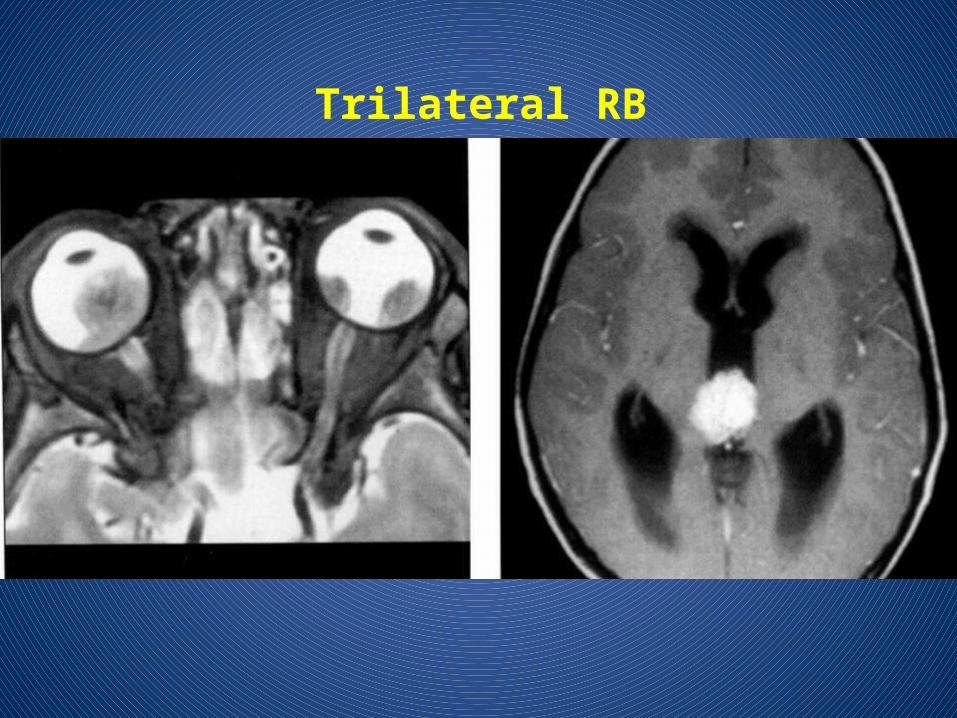
Trilateral RB
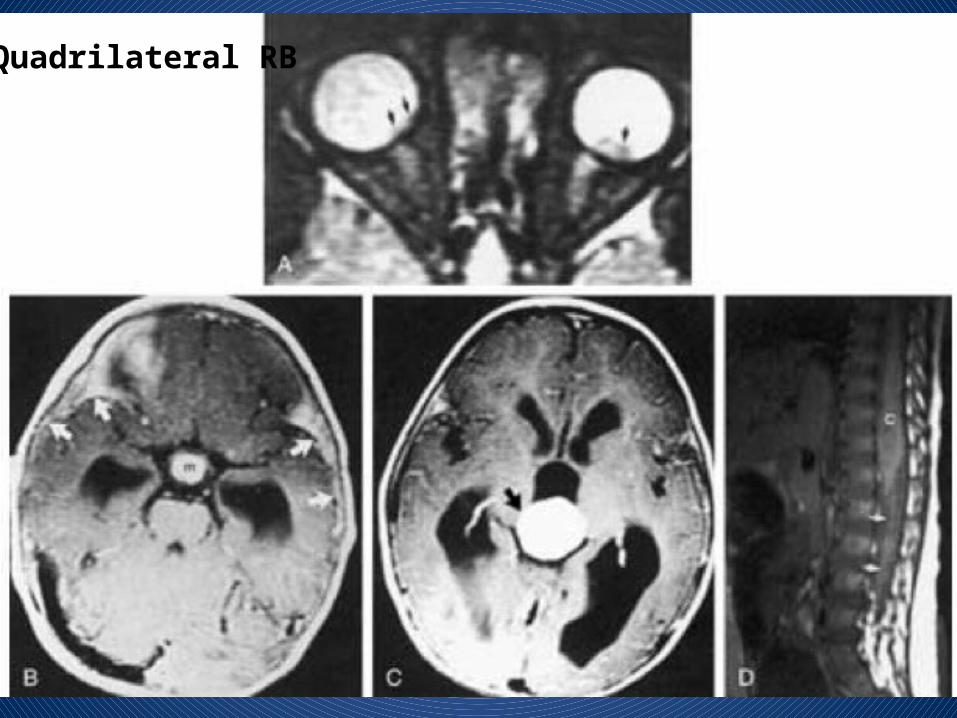
Quadrilateral RB

OCULAR MELANOMA

OPTIC PATHWAY GLIOMA

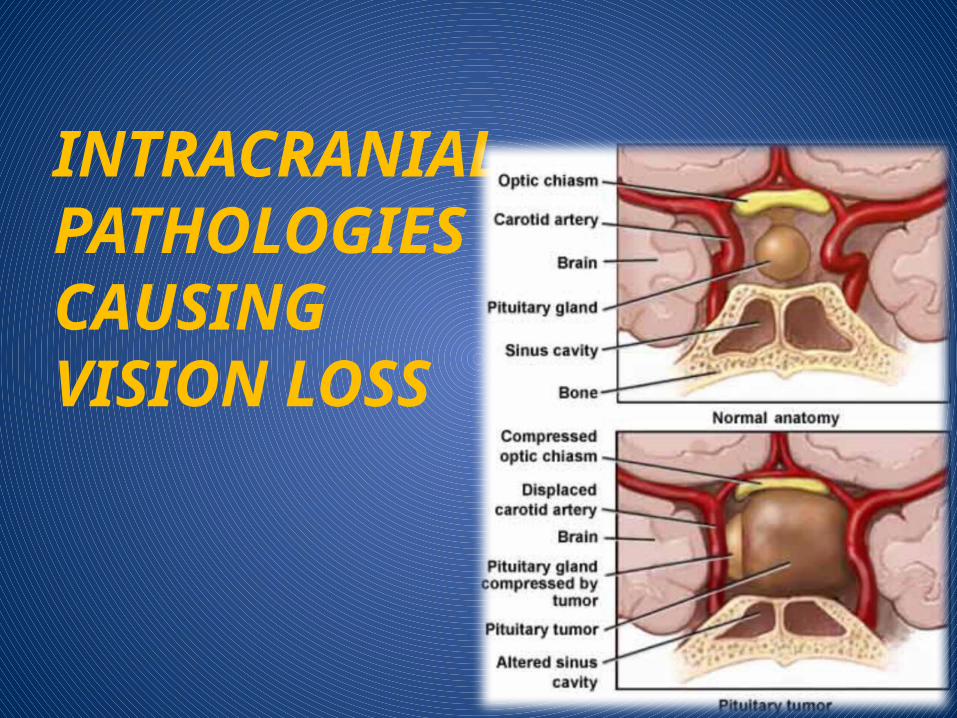
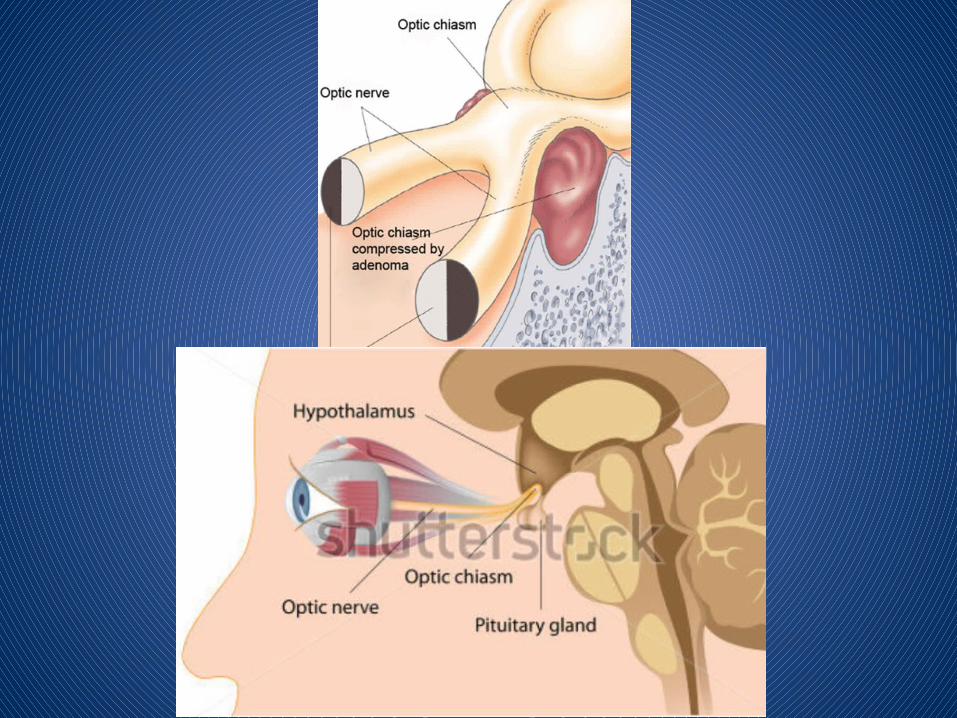
INTRACRANIAL PATHOLOGIES CAUSING VISION LOSS

Pituitary macroadenoma causing compression on optic chiasm

A variety of pathologic conditions can affect cranial nerve III. Its close association with the posterior cerebral and superior cerebellar arteries makes cranial nerve III susceptible to compression by vascular lesions such as posterior communicating artery aneurysms.

Cranial nerve IV is the only cranial nerve to exit the dorsal brainstem, and each superior oblique muscle is innervated by the contralateral cranial nerve IV nucleus.


The cisternal portion of cranial nerve VI exits the brainstem near the midline through the space between the pons and the pyramid of the medulla oblongata.
The nerve courses anteriorly in the prepontine cistern and penetrates the dura mater to enter the Dorello canal and then the cavernous sinus, where it is the only nerve to travel within the venous sinusoids of the cavernous sinus (cranial nerves III, IV, V1, and V2 all lie within the lateral dural wall of the cavernous sinus).



















