86
Dr. Mohit Goel JR III 3/07/2014
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | anish-choudhary |
| View: | 162 times |
| Download: | 0 times |
Dr. Mohit Goel
JR III
3/07/2014

1. Congenital anomalies
2. Infection / Inflammation
3. Tumors
4. Trauma
5. Neoplasm
Congenital anomalies
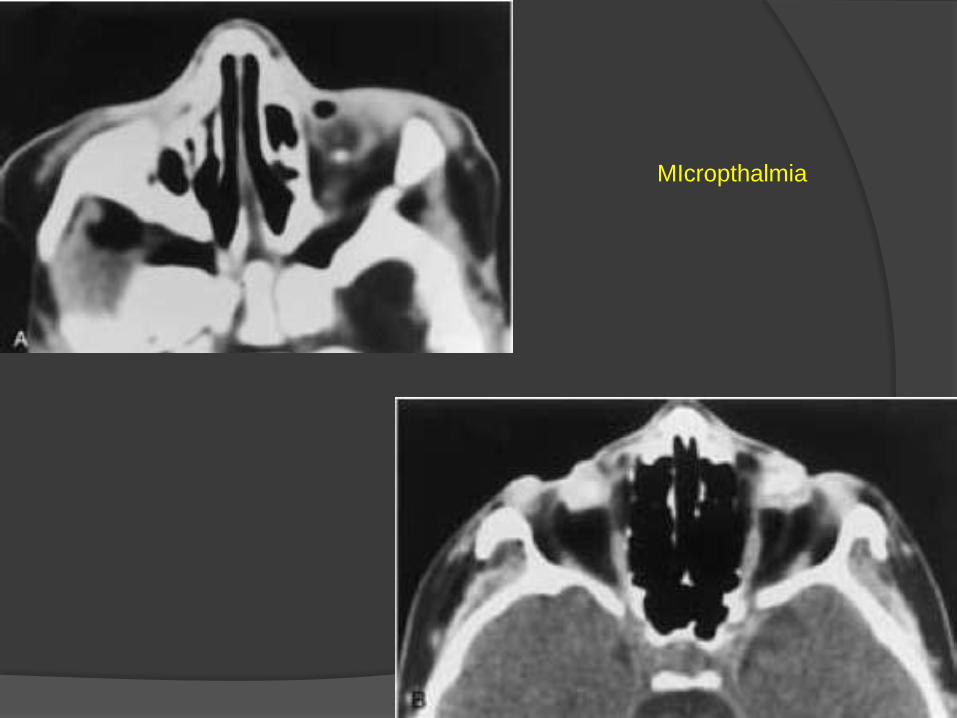
MIcropthalmia
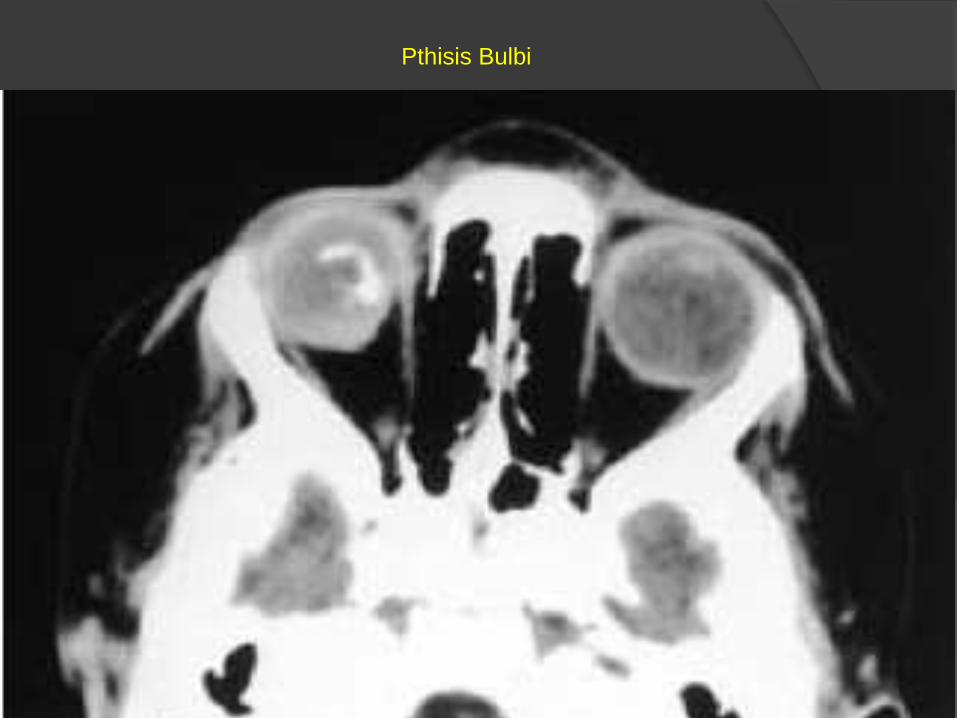
Pthisis Bulbi

Coloboma

Colobomatous cyst


Ocular detachments

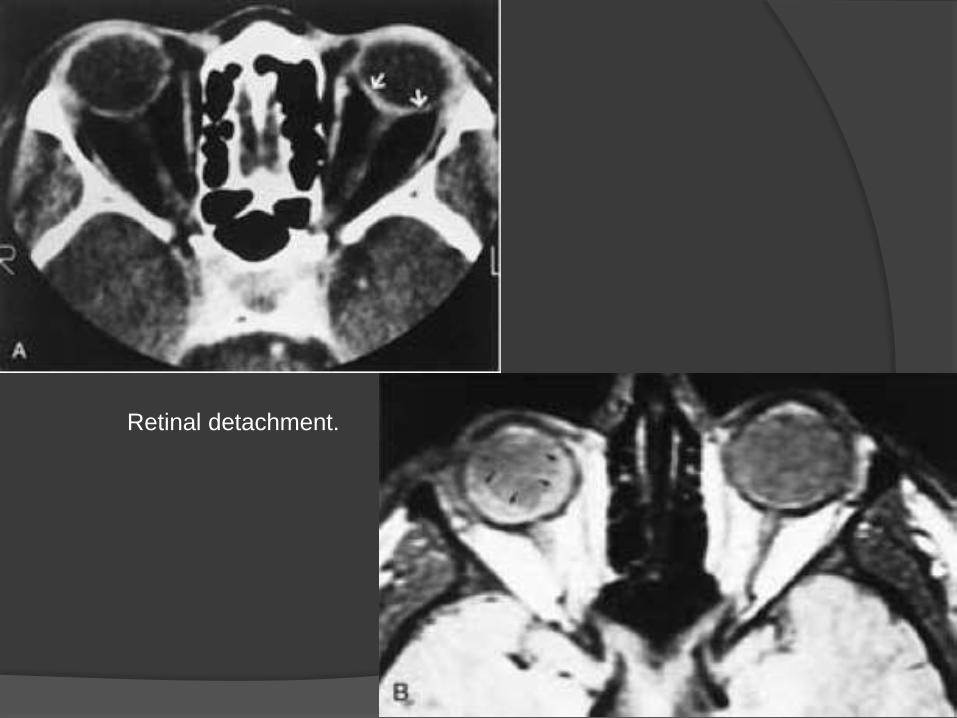
Retinal detachment.





Inflammatory conditions




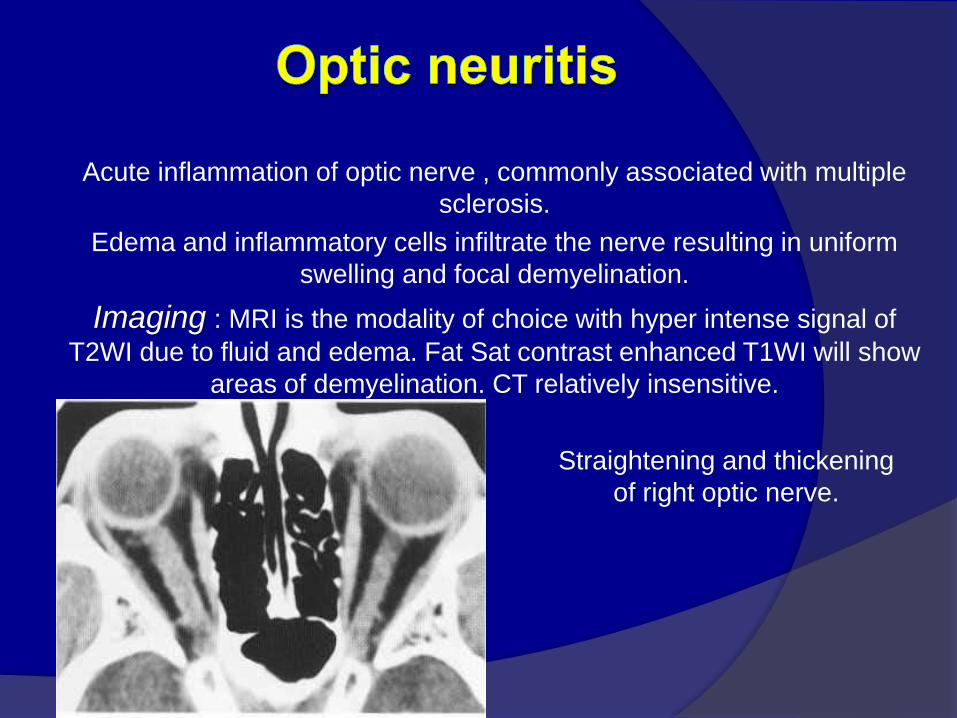
Acute inflammation of optic nerve , commonly associated with multiple
sclerosis.
Edema and inflammatory cells infiltrate the nerve resulting in uniform
swelling and focal demyelination.
Imaging : MRI is the modality of choice with hyper intense signal of
T2WI due to fluid and edema. Fat Sat contrast enhanced T1WI will show
areas of demyelination. CT relatively insensitive.
Straightening and thickening
of right optic nerve.

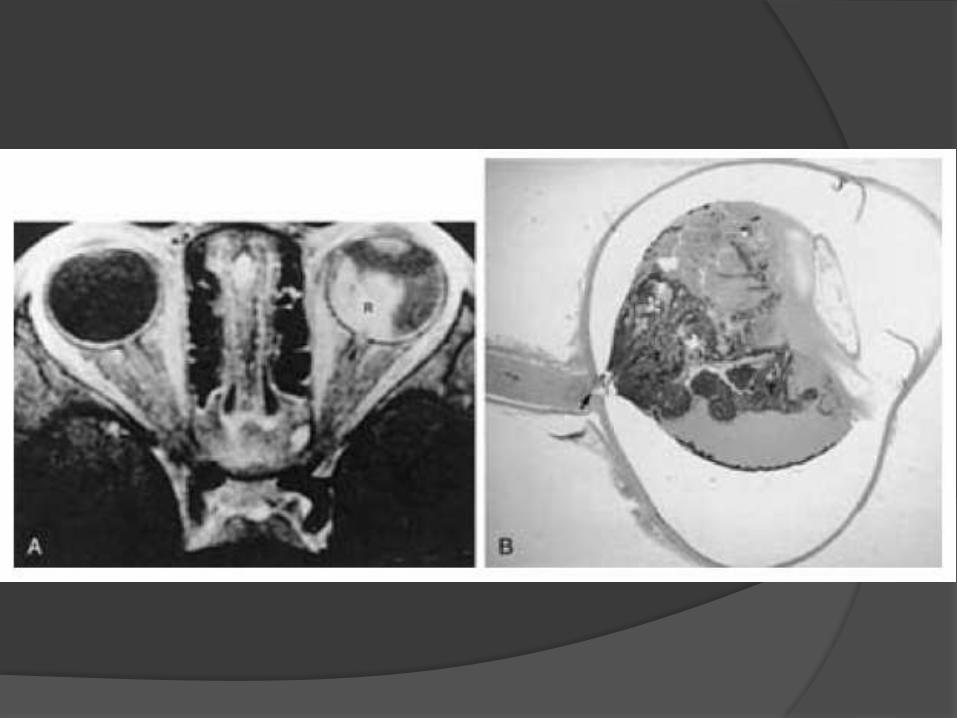
Optic Neuritis. CE Fat Sat T1W axial
(B) MR images demonstrate subtle enlargement and enhancement of the left
optic nerve (curved arrow).
T 2 WI (C) demonstrates corresponding increased signal intensity (straight
arrow).

Retinoblastoma


Retinopathy of Prematurity

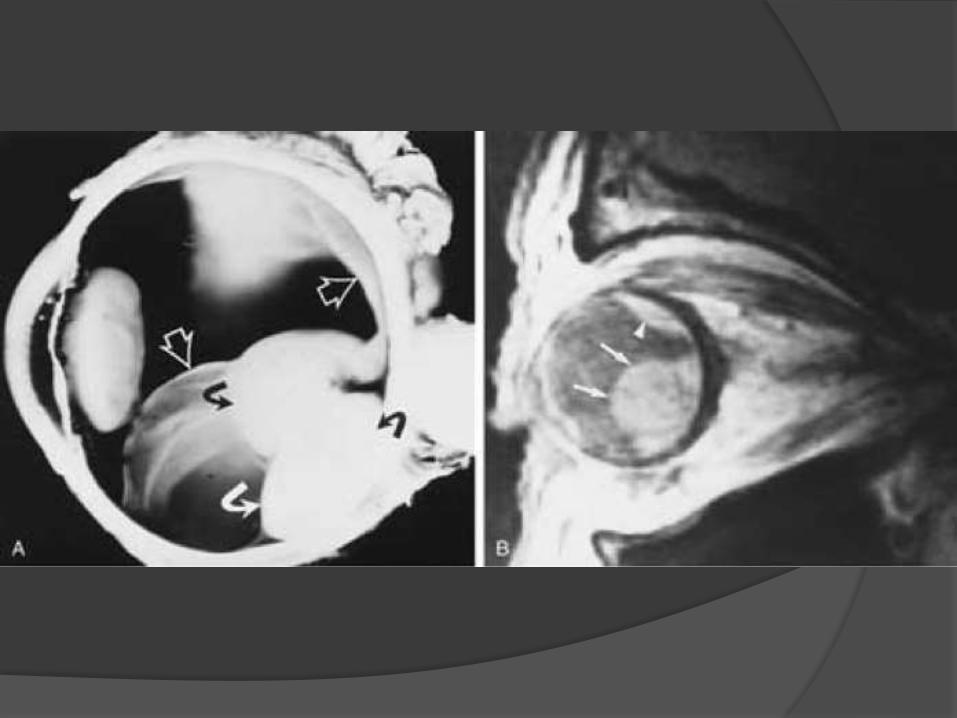
Coat’s disease
Primary retinal telengiectasis
Vascular anomaly of retina
Characterized by idiopathic retinal telengiectatic and aneurysmal retinal vessels
Progressive deposition of intraretinal and subretinal exudates
Leads to massive exudative retinal detachment


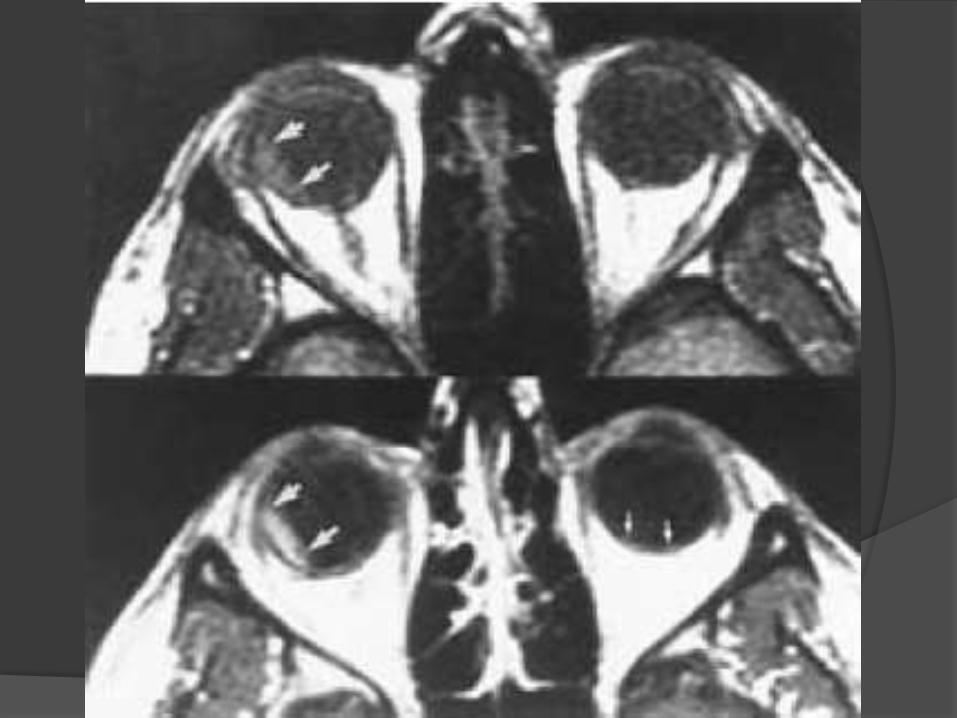
Ocular astrocytic Hamartoma

Benign yellow-white rare retinal tumor
Associated with Tuberous Sclerosis or Neurofibromatosis
Early on it may look exactly like retinoblastoma
May involve retina or optic nerve

Juvenile Xanthogranuloma

Benign cutaneous disorder
Affects eye and skin
Affects iris and ciliary body, choroid, retina and optic nerve
May present as a solitary orbital mass


Optic nerve head drusen


Tumors

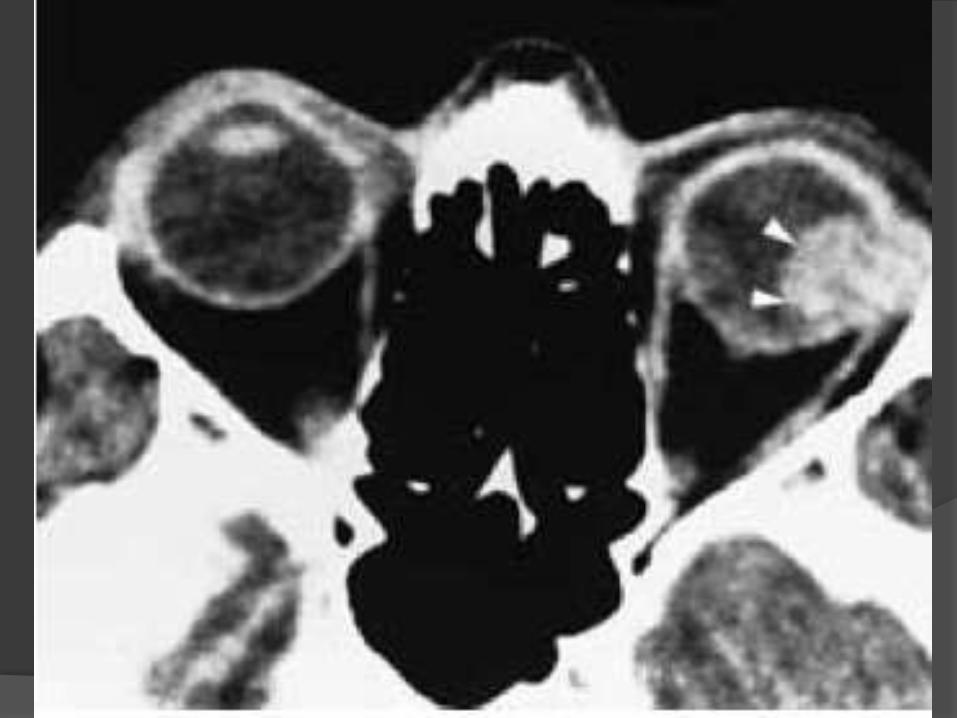
Choroidal osteoma
Benign tumor
Unilateral usually
Affects young white girls
Patients present with painless progressive loss of vision

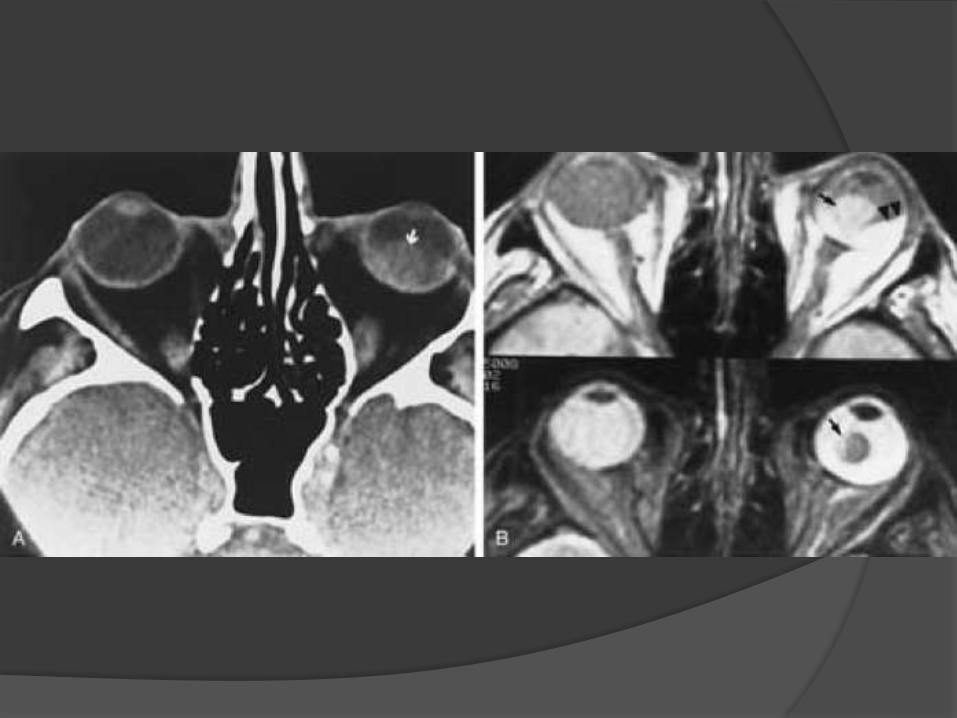

Malignant uveal melanoma
More common in whites
May arise from pre-existing nevi
Metastasizes hematogeneously to liver




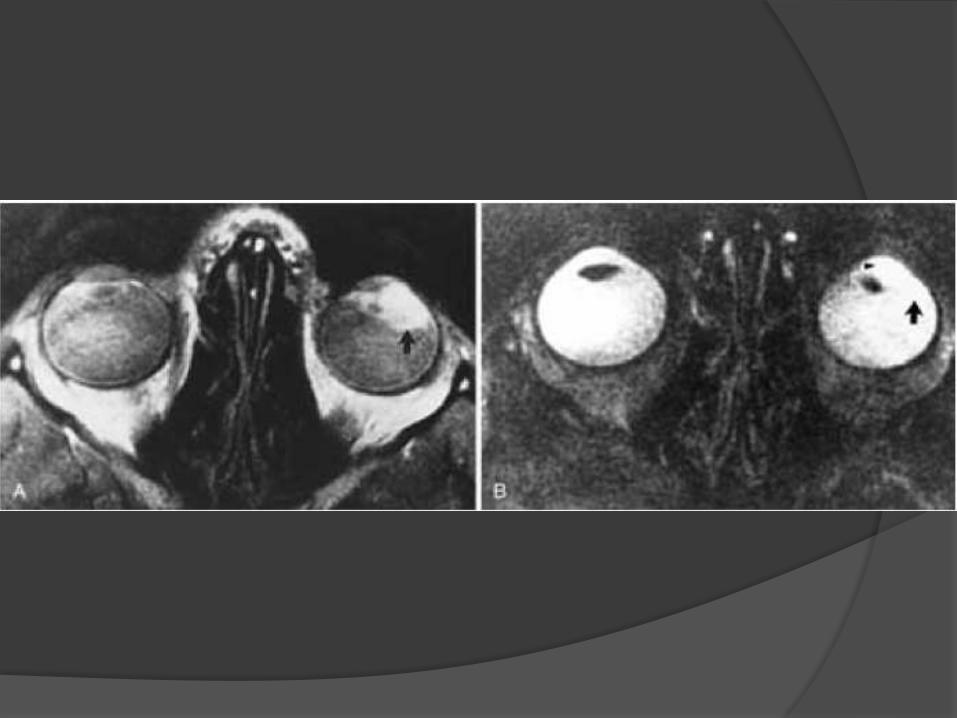

Orbital Pseudotumor
• The most common cause of orbital mass in adults.
• Acute form presents with pain, proptosis and
diminished ocular mobility, with histological changes
similar to vasculitis.
• Chronic form may mimic infection or lymphoma both
clinically and histologically. Unilateral presentation is
most common, but findings can be bilateral. All
compartments of the orbit may be affected.

• Imaging -- Heterogeneous poorly marginatedincreased CT density and decreased T1 & T2 MRI signal intensity within the intraconal fat surrounding a thickened sclera or enlarged optic nerve, sometimes simulating a mass.
• The lacrimal gland may be enlarged. Enhancement occurs following contrast infusion.
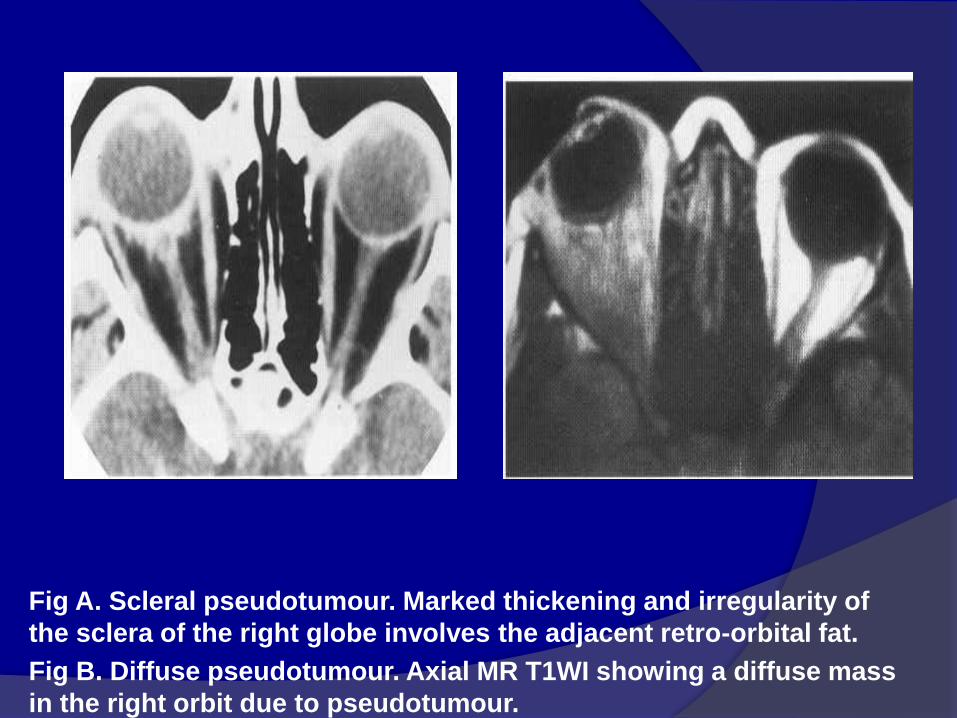
Fig A. Scleral pseudotumour. Marked thickening and irregularity of
the sclera of the right globe involves the adjacent retro-orbital fat.
Fig B. Diffuse pseudotumour. Axial MR T1WI showing a diffuse mass
in the right orbit due to pseudotumour.
Rhabdomyosarcoma
• Rhabdomyosarcoma is the most common primary
orbital malignancy in the pediatric age group. with
most patients presenting below 6 years of age.
• Patients present with rapidly progressive
exophthalmos that may mimic orbital infection.
Spread of the tumor esp. intracranially, portends
poor prognosis.

• Imaging : Both CT and MRI will typically show a mass involving an extra ocular muscle. Lesions are isodense on CT and isointense on T1WI when compared to muscle.
• There may be associated bony destruction and contiguous extra orbital spread. The tumor involves the globe less often. Marked enhancement throughout the mass is seen after contrast administration.

Rhabdomyosarcoma. CECT image
(A) Orbits demonstrates right proptosis due to large, lobular, intraorbital
mass.
(B) Image at lower level demonstrates invasion of right maxillary
sinus (asterisk) as well as extension through lateral orbital wall (arrow),
consistent with the aggressive nature of this tumor.
• Patients with abnormalities of the optic nerve and
its covering present with proptosis, visual loss and
papilloedema.
• Expansion of the tubular shaped optic nerve and
sheath is well demonstrated on CT and MRI.
• Imaging of the intracranial space is required
because the optic nerve and its coverings are
continuous with the brain and dura mater.

Occur in children
Are low grade astrocytomas.
Associated with NF-1
Imaging:- optic nerve may expand uniformly and diffusely. Plain
films will show asymmetric widening of the optic canal. Post
contrast show uniform enhancement.
Optic nerve glioma.
Enhanced coronal CT image
demonstrates homogeneous
enhancement of enlarged right
optic nerve.
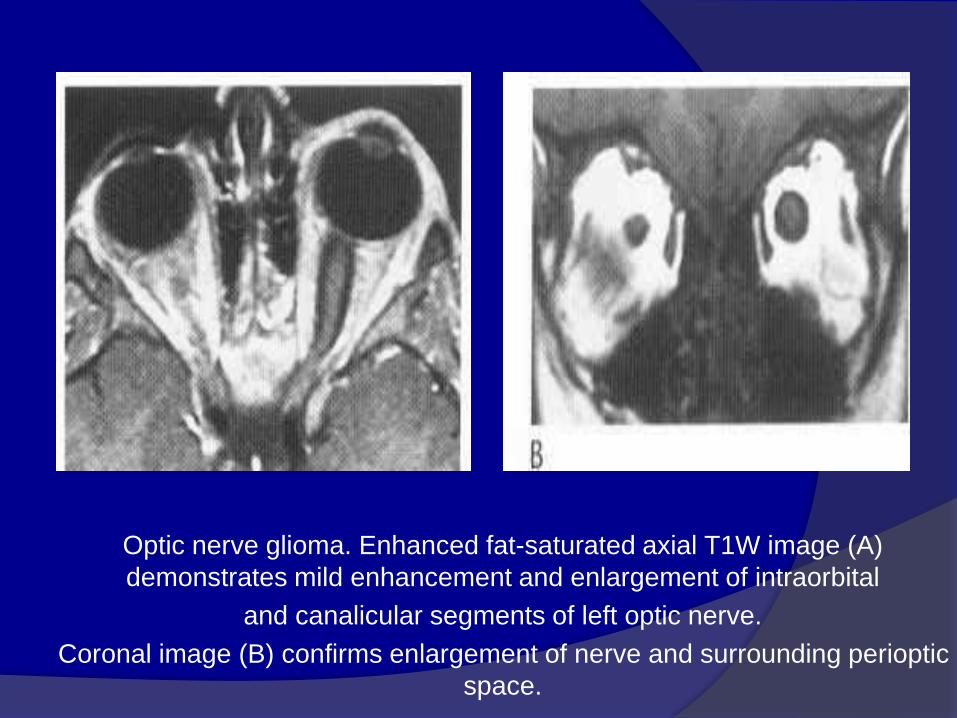
Optic nerve glioma. Enhanced fat-saturated axial T1W image (A)
demonstrates mild enhancement and enlargement of intraorbital
and canalicular segments of left optic nerve.
Coronal image (B) confirms enlargement of nerve and surrounding perioptic
space.

• Meningiomas are dense fibrous tumors. Calcification is
common.
• Plain films may show widening of the optic canal, or
hyperostosis of the sphenoid wing.
• CT generally shows a dense, sharply defined tubular mass
surrounding and paralleling the course of the optic nerve, with
marked enhancement after contrast administration ('tram
track'). Kinking of the nerve may be seen.
• MRI will show a homogeneous mass of decreased T1 and T2
signal intensity, with strong enhancement, especially with the
use of fat suppression sequences.
• Coronal images are preferred, as the encased optic nerve will
be seen in relief against the densely enhanced tumor.
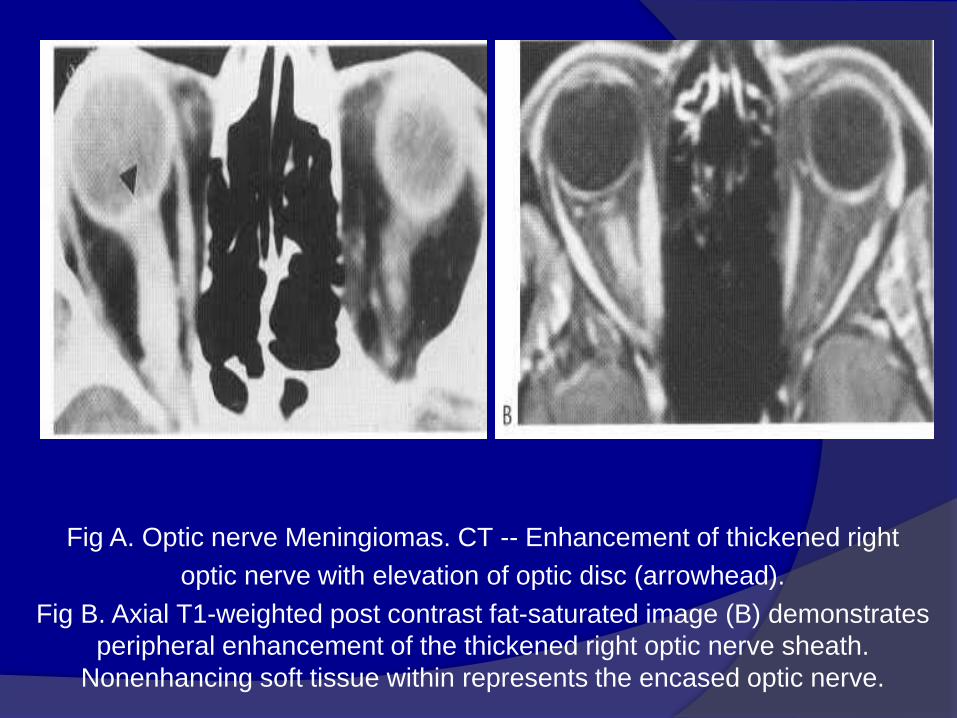
Fig A. Optic nerve Meningiomas. CT -- Enhancement of thickened right
optic nerve with elevation of optic disc (arrowhead).
Fig B. Axial T1-weighted post contrast fat-saturated image (B) demonstrates
peripheral enhancement of the thickened right optic nerve sheath.
Nonenhancing soft tissue within represents the encased optic nerve.
Trauma










Miscellaneous
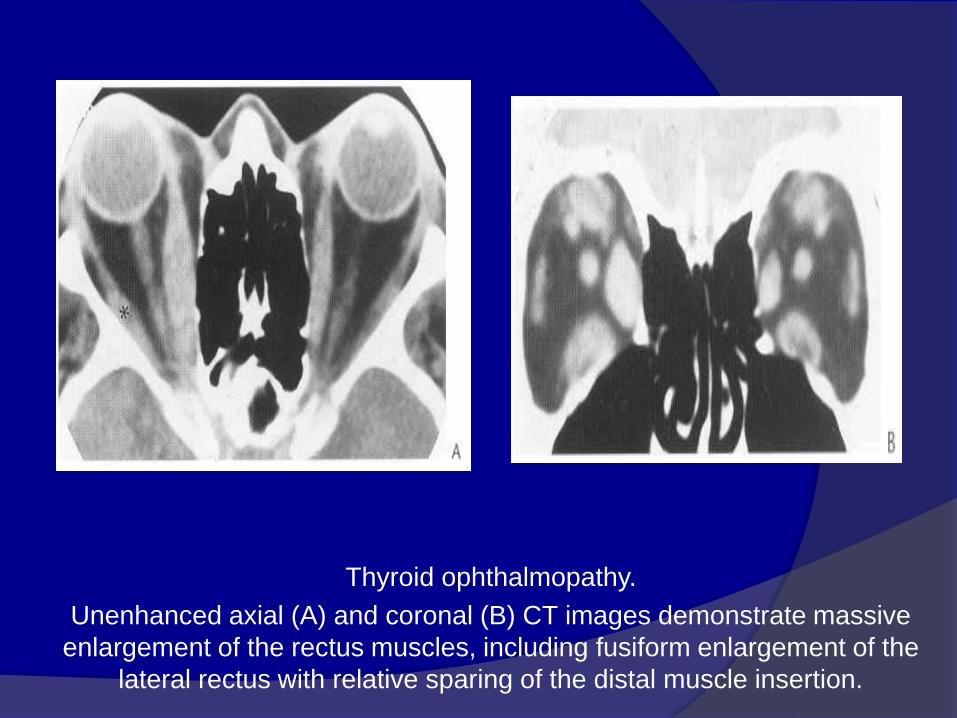
Thyroid ophthalmopathy.
Unenhanced axial (A) and coronal (B) CT images demonstrate massive
enlargement of the rectus muscles, including fusiform enlargement of the
lateral rectus with relative sparing of the distal muscle insertion.
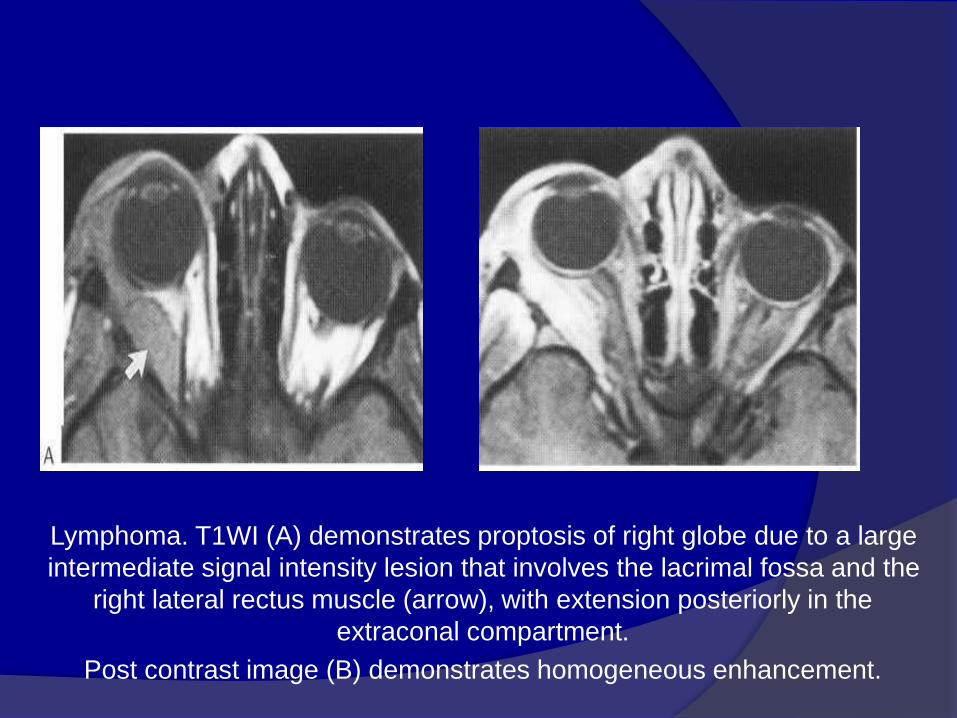
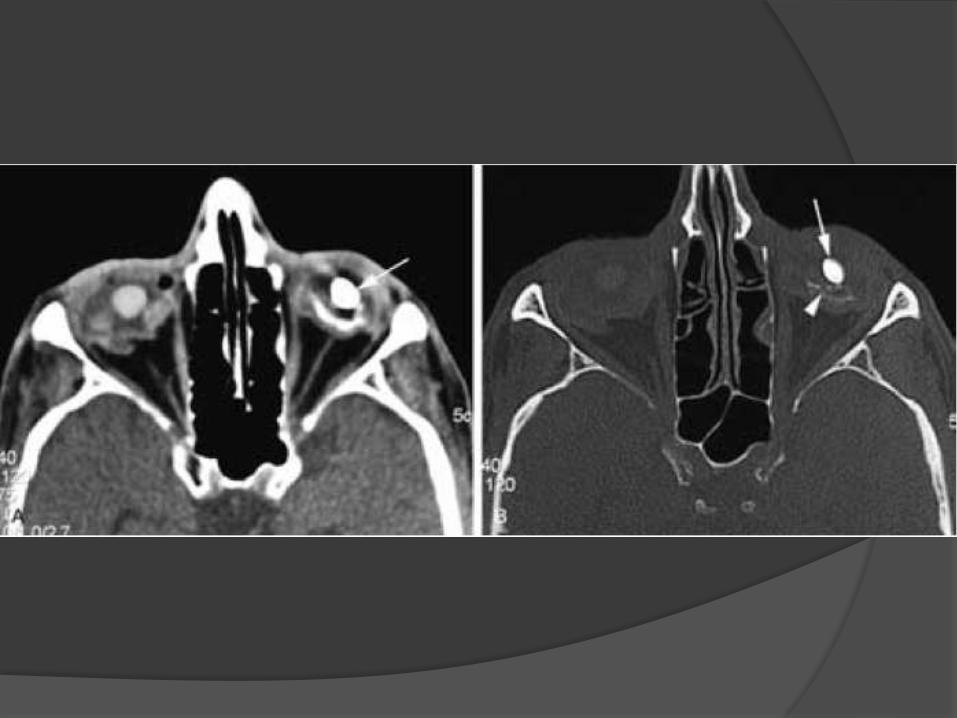
Lymphoma. T1WI (A) demonstrates proptosis of right globe due to a large
intermediate signal intensity lesion that involves the lacrimal fossa and the
right lateral rectus muscle (arrow), with extension posteriorly in the
extraconal compartment.
Post contrast image (B) demonstrates homogeneous enhancement.
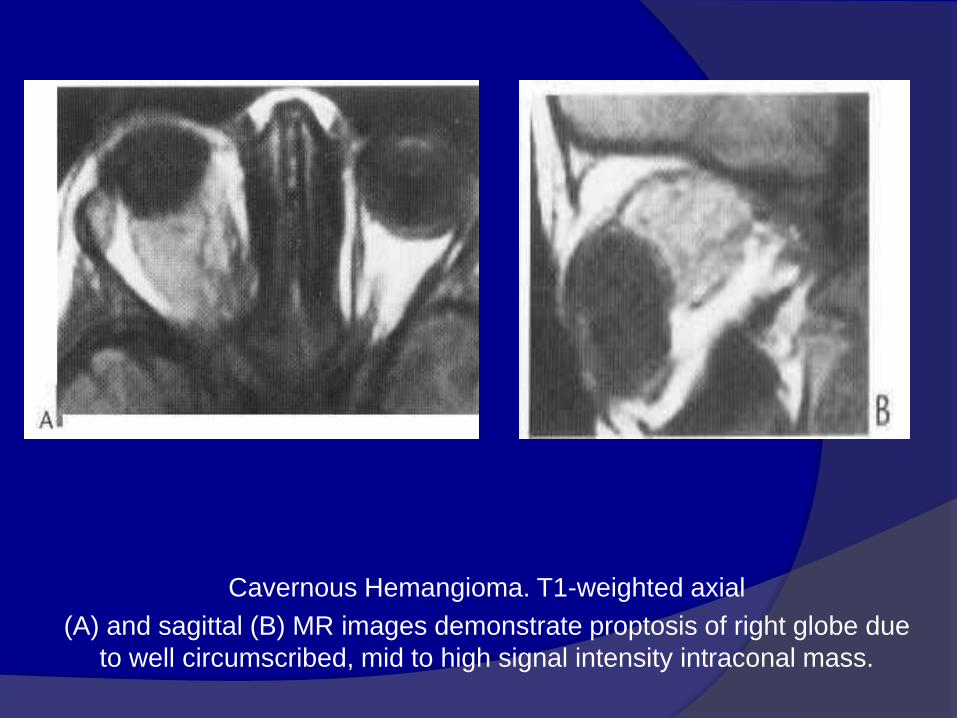
Cavernous Hemangioma. T1-weighted axial
(A) and sagittal (B) MR images demonstrate proptosis of right globe due
to well circumscribed, mid to high signal intensity intraconal mass.

Lymphangioma.
Axial T,-weighted (A) and T2 -weighted (B) MR images demonstrate mild right
proptosis due to complex, multi loculated, cystic, extra-axial lesion in the
superomedial aspect of the right orbit.
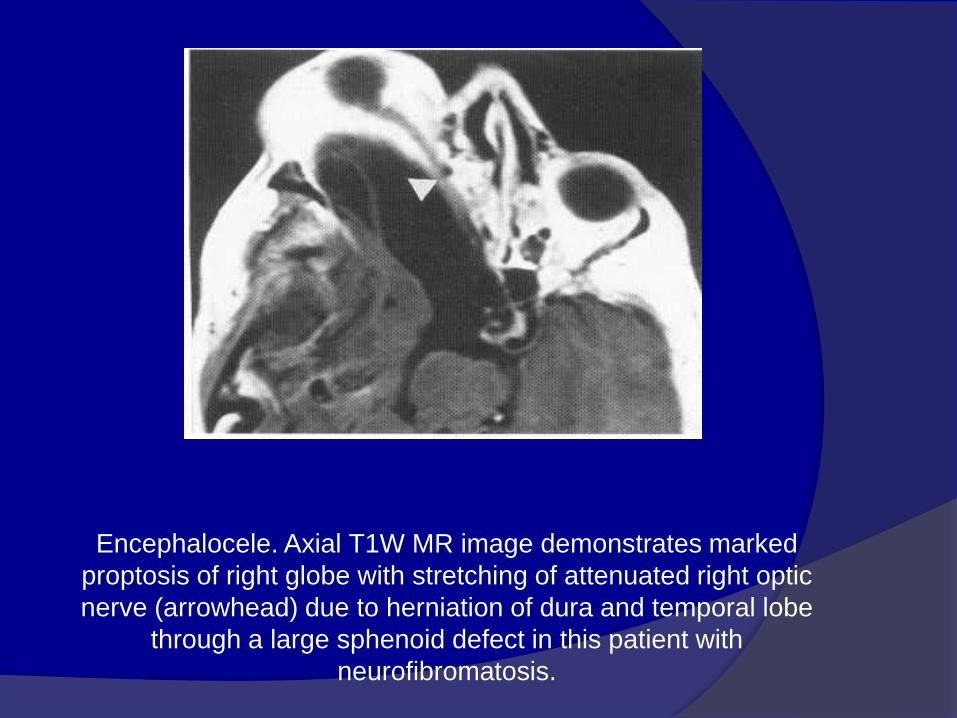
Encephalocele. Axial T1W MR image demonstrates marked
proptosis of right globe with stretching of attenuated right optic
nerve (arrowhead) due to herniation of dura and temporal lobe
through a large sphenoid defect in this patient with
neurofibromatosis.
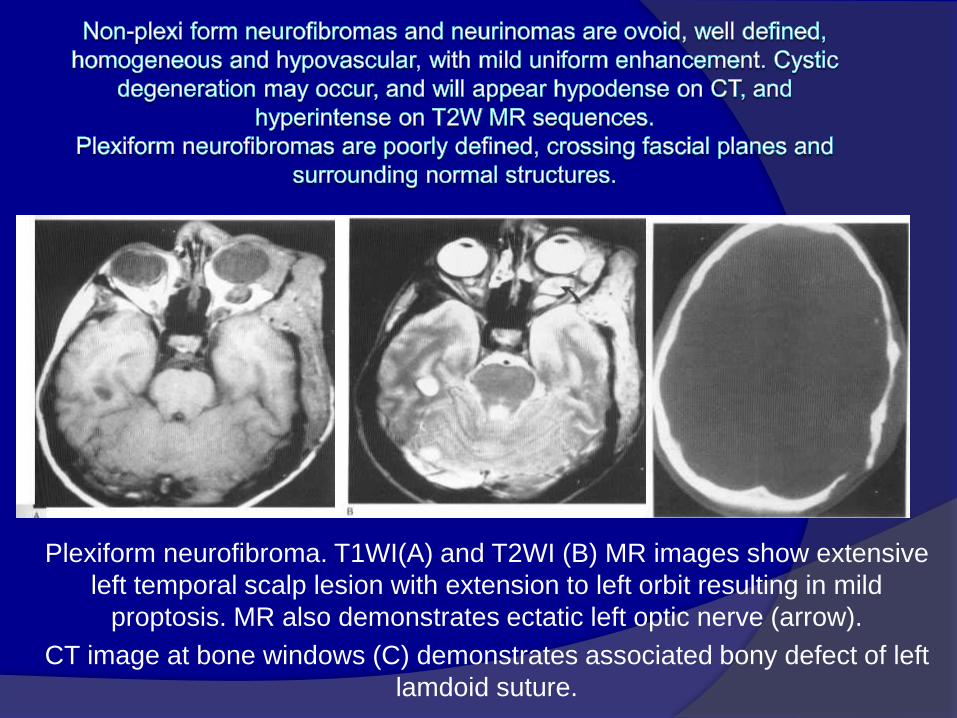
Plexiform neurofibroma. T1WI(A) and T2WI (B) MR images show extensive
left temporal scalp lesion with extension to left orbit resulting in mild
proptosis. MR also demonstrates ectatic left optic nerve (arrow).
CT image at bone windows (C) demonstrates associated bony defect of left
lamdoid suture.

Metastases to the orbit may occur from systemic primaries,
particularly neuroblastoma and leukaemias in children, and breast, lung,
prostate and stomach cancer in adults. These lesions are poorly defined,
infiltrative and demonstrate marked contrast enhancement
on CT and MRI.
Prostatic Ca: Axial CT (A) shows small lytic lesion of left lateral orbital wall.
Soft-tissue windows (B) demonstrate contiguous extension of soft tissue into
lateral extraconal compartment (asterisk) with medial displacement of the
lateral rectus muscle.

These are congenital lesions that result from sequestration of primitive
ectoderm in the region of the orbit, usually presenting during childhood as a
discrete mass, located near the lacrimal fossa or nasal bone and are
homogeneous in appearance. The presence of fat is clearly seen on CT and
MRI. They do not enhance.
Lacrimal gland dermoid.
Coronal T 1WI demonstrate a well-
circumscribed lesion located in the
upper outer quadrant of left orbit.
High signal intensity is consistent with
fat.

Thank You

















