Pathology of the Mouth Pathology of the Esophagus Disease Cause Symptoms Buzzwords Other Minor Aphthous Ulcer MiRAU Immunological (Cell Mediated Immunity) Numerous Allergens Ulcer on Non-keratinized movable mucosa ~ 5 mm Heal in 2 weeks – no scarring Associated with Crohn’s, AIDS, Celiac, Behcet’s, Leukopenia & Vitamin Deficiencies Treat with topical steroids – Don’t cauterize! Major Aphthous Ulcer (Sutton’s Disease) MaRAU Immunological (Cell Mediated Immunity) Numerous Allergens Ulcer on Non-keratinized movable mucosa > 5 mm (up to~3 cm) Heal in > 2 weeks (up to 6 weeks) Scarring! Topical steroids ineffective – Treat with stronger local steroids Herpetiform Aphthous Ulcer HeRAU Immunological (Cell Mediated Immunity) Numerous Allergens Ulcer on movable or bound mucosa < 2 mm & frequently numerous No painful or erythematous gingiva Topical steroids is treatment of choice Herpangina Coxsackie Virus Ulcer on soft palate, tonsils or pharyngeal wall Sore throat, fever, headache, nausea Back of mouth Dyclonine HCl (specially prepared is DOC) Hand, Foot & Mouth Coxsackie Virus Ulcers on palate, tongue & buccal mucosa Erythematous Rash Dyclonine HCl (specially prepared is DOC) Behcet’s Syndrome Autoimmune Ulcers same as MiRAU Oral, genital & ocular lesions Eye & Genitals Herpetic Gingivostomitis Herpes Virus Painful erythematous gingival Clear fluid filled vesicles Usually unilateral recurrences keratinized, bound mucosa Gingiva Can cause herpetic whitlow (contagious infection of finger) Ulcers are the opposite of MiRAU Extremely Painful (primary occurance) Herpes Zoster Herpes Virus Unilateral White opaque ulcers resembling RAU Erythema Multiforme (Stevens-Johnson Syndrome) Unknown Preceded by viral infection or allergen exposure Involves skin & mucosal surfaces Usually movable mucosa (but not limited to) Target Lesion (Also another Eye & Genitals) Extremely Painful Stevens-Johnson = skin, eye, mouth & genitals (similar to Behcet’s?) Disease Cause Symptoms Buzzwords Other Reflux Esophagitis Reflux Esophageal Sphincter Disorder ↑ Acid & Pepsin, Bile, Lysolethicin Heartburn & Regurgitation Also dysphagia, odynophagia, hemorrhage & pulmonary symptoms (cough?) Most common esophagitis Microscope = Eosinophils, PMN’s & hyperplasia Complications = Barret Esophagus, Ulcer, Stricture Barret Esophagus Chronic Esophageal Reflux Mucosa replaced with intestinal mucosa Intestinal Metaplasia Adenocarcinoma of Esophagus Complications = risk of esophageal adenocarcinoma Squamous Cell Carcinoma 1) Drinking & Smoking Diet, Chronic injury, Genetic Dysphagia & Obstruction Aspiration pneumonia Middle 1/3 of esophagus Most frequently found in middle 1/3 of esophagus Microscope = Keratin Pearls Sliding Hiatal Hernia Herniation of cardia GE Reflux Cardia Most Common Hiatal Hernia Paraesophageal Hiatal Hernia (Rolling) Herniation of fundus Asymptomatic Strangulation & infarction possible Fundus Mallory-Weiss Lacerations Excessive Vomiting Alcoholics Vomiting Tears at the Gastroesophageal junction
Transcript
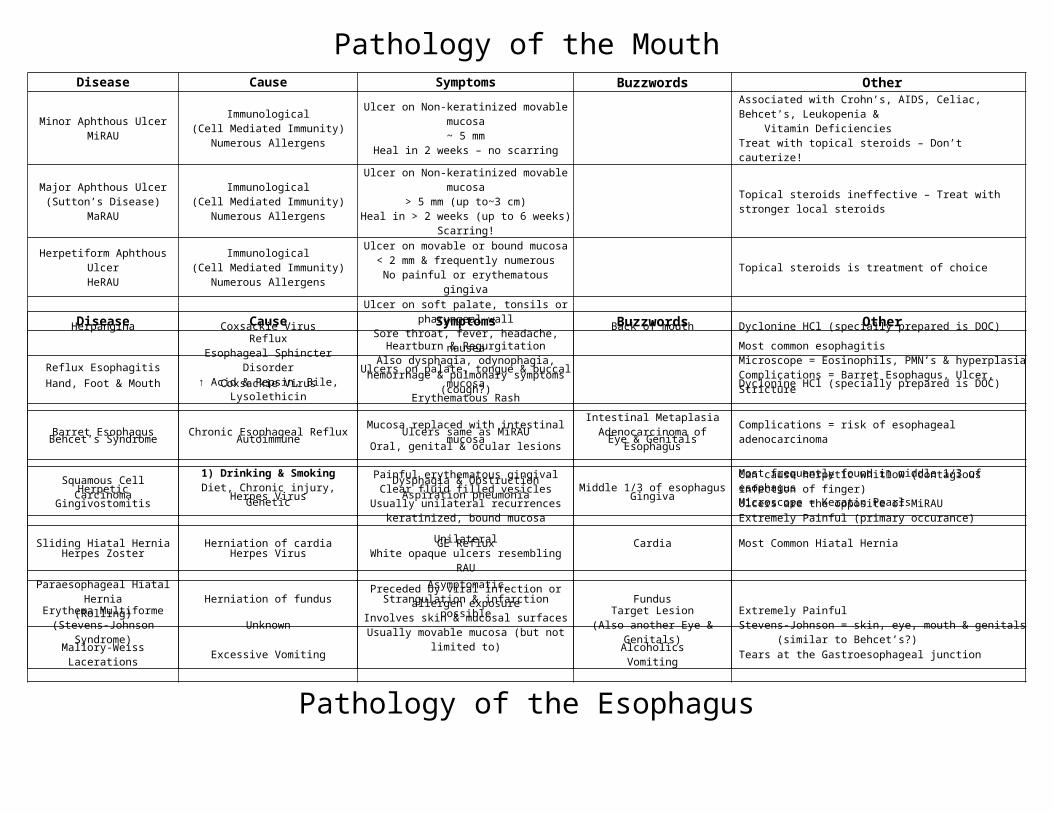
Pathology of the Mouth
Pathology of the Esophagus
Disease Cause Symptoms Buzzwords Other
Minor Aphthous UlcerMiRAU
Immunological (Cell Mediated Immunity)
Numerous Allergens
Ulcer on Non-keratinized movable mucosa~ 5 mm
Heal in 2 weeks – no scarring
Associated with Crohn’s, AIDS, Celiac, Behcet’s, Leukopenia & Vitamin DeficienciesTreat with topical steroids – Don’t cauterize!
Major Aphthous Ulcer(Sutton’s Disease)
MaRAU
Immunological (Cell Mediated Immunity)
Numerous Allergens
Ulcer on Non-keratinized movable mucosa> 5 mm (up to~3 cm)
Heal in > 2 weeks (up to 6 weeks)Scarring!
Topical steroids ineffective – Treat with stronger local steroids
Herpetiform Aphthous UlcerHeRAU
Immunological (Cell Mediated Immunity)
Numerous Allergens
Ulcer on movable or bound mucosa< 2 mm & frequently numerous
No painful or erythematous gingivaTopical steroids is treatment of choice
Herpangina Coxsackie Virus Ulcer on soft palate, tonsils or pharyngeal wallSore throat, fever, headache, nausea Back of mouth Dyclonine HCl (specially prepared is DOC)
Hand, Foot & Mouth Coxsackie Virus Ulcers on palate, tongue & buccal mucosaErythematous Rash Dyclonine HCl (specially prepared is DOC)
Behcet’s Syndrome Autoimmune Ulcers same as MiRAUOral, genital & ocular lesions Eye & Genitals
Not associated with H. pylori!Pathogenesis = Hypoperfusion, ↓ mucus production, ↑ Gastric AcidFound in 10% of hospital admissionsOutcome dependent on correction of underlying condition!
Nonatrophic Chronic Gastritis H. pylori? Active gastritis & Lymphoid follicle Associated with Gastric Adenocarcinoma & MALT Lymphoma
Peptic Ulcer Disease
Gastric Acid & Pepsin, H. pyloriZollinger-Ellison Syndrome
NSAIDS & SmokingStress, alcohol & steroids
Ulcerations through muscularis mucosaPain at night, after meals, relieved with food
Bleeding (frequent complication)Pain relieved by eating
Zones = 1) Exudate 2) Necrosis 3) Granulation 4) ScarringDeath caused by perforationNot likely to cause cancer unlike nonatrophic chronic gastritisPUD is more common in duodenum than stomach
Autoimmune Atrophic Gastritis(Type A)
AutoimmuneAntibodies to parietal cell/intrinsic factor
Loss of parietal cellsHypochlorhydria, ↓ Intrinsic Factor (Low B12)
Polypoid & Well DifferentiatedIntestinal Metaplasia
Weight LossPain, Melena, Hematemesis, Anemia
MetaplasiaOccurs in older age & in males, Better outcome than diffuse typeMetastasis to lungs and liver or ovary (Krukenberg)More likely to be in antrum or pylorus (distal) than in body
Frequently involves terminal ileumNarrowed lumen, aphthoid ulcers to fissuresTransmural inf. / Noncaseating granulomas / Perianal FistualsLower risk of cancer than ulcerative colitis
Ulcerative Colitis Relapsing diarrhea associated with stressArthritis, Uveitis, Ankylosing spondylitis
Diffuse/Continuous from RectumMucosa/Submucosa
Lead PipeAbscess/Broad ulcers/pseudopolyps
Crypt abscessesNo granulomasCan cause perforation, toxic megacolon & cancerAssociated with Primary Sclerosing Cholangitis (liver)
Peptic Ulcer Disease
Gastric Acid & Pepsin, H. pyloriZollinger-Ellison Syndrome
NSAIDS & SmokingStress, alcohol & steroids
Ulcerations through muscularis mucosaPain at night, after meals, relieved with food
Bleeding (frequent complication)Pain relieved by eating
Zones = 1) Exudate 2) Necrosis 3) Granulation 4) ScarringDeath caused by perforationNot likely to cause cancer unlike nonatrophic chronic gastritisPUD is more common in duodenum than stomach
Transmural Ischemic Bowel Disease
Mechanical compromise of vesselsArterial Thrombus or Embolism
Venous ThrombosisVolvulus, Stricture, Herniation
Abrupt lower abdominal pain & bloody stool
Involves all of small bowel or splenic (watershed area) of colonAcute = coagulative necrosis & hemorrhage – No inflammation!Chronic = chronic inflammation, stricture, fibrosisHigh mortality
Mural or MucosalIschemic Bowel Disease
HypoperfusionCardiac Failure, Shock, Dehydration
RadiationVolvulus, Stricture, Herniation
Abrupt lower abdominal pain & bloody stool
Involves all of small bowel or splenic (watershed area) of colonAcute = coagulative necrosis & hemorrhage – No inflammation!Chronic = chronic inflammation, stricture, fibrosisHigh mortality
MalabsorptionDeconjugation of bile salts (poor micelle formation), Direct injury to cells, Direct utilization of nutrients by bacteriaTreat with intermittent antibiotics
Villous Atrophy caused by sensitivity to gluten in foodSymptoms disappear quickly with gluten free dietMay cause intestinal lymphomaOften found in children, whites, families
Large macrophages fill lamina propria of small intestine (PAS +)Usually a prompt recovery with antibiotics
Lactase Deficiency Lactose MalabsorptionDiarrhea & Flatulence Microscopically Normal
Lactase found in apical membrane of epithelial cells in villiLactase normally breaks lactose in glucose & galactoseMore commonly acquired, but can be congenitalMicroscope: Looks normal
Abetalipoproteinemia Genetic (AR)
AcanthocytesFailure to absorb fatty acids & Vitamin A,D,E,K
Diarrhea, Steatorrhea, CNS ProblemsFailure to Thrive in Infants
AcanthocyteLipid (Fat) Vacuole
Can’t synthesize or export lipoproteins from intestinal cellsTriglycerides accumulate in epithelial cell lipid vacuolesAbsence of CM, VLDL, LDL
Pathology of the Intestines
Pathology of the Intestines (contd)Disease Cause Symptoms Buzzwords Other
Collagenous Colitis Chronic Watery Diarrhea Middle Age Women Normal colonoscopic examMarkedly thickened subepithelial layer
Hamartomatous, usually in children < 5Usually found in rectumLarge (>4 cm) with stalk, Surface erosion or ulcerationNo malignant potential in sporadic cases
Left = Napkin Ring; Right: = Cauliflower Lesion95% AdenocarcinomasCEA: reliable marker of recurrent tumorsMost important prognostic factor is staging of tumor at diagnosis
Diverticulosis Low Fiber Diet
BleedingObstruction caused by muscular hypertrophy
Pericolic abscessPerforation, Vesicocolic fistula
Pericolic abscessCommon in elderly; Typically in sigmoid colonUsually asymptomaticOutpouching of mucosa through teniae, muscular hypertrophyNot a risk for cancer
Pathology of the LiverDisease Cause Symptoms Buzzwords Other
May lead to liver failure & cirrhosisBridging necrosis with piecemeal necrosis & inflammation at limiting plateFibrosis
Hepatitis E Fecal-Oral High risk of mortality in pregnant women
Autoimmune HepatitisHLA B8, Dr3 & 4, Dr52Type I = ANA & ASMA
Type II = AKLM-1AType I = Infertility or endocrine disorder
Anti-Smooth MuscleAnti-KLM-1Plasma Cells
Macronodular (Cirrhosis)
Type I = Premenopausal women, Thyroiditis, Diabetes, Hemolytic Anemia; Hypergammaglobulinemia (anti smooth muscle)Type II = Female children; more aggressive; anti KLM-1Looks like viral, but with plasma cells in portal area
Drug Induced Liver Disease ManyTylenol, INH, Methyldopa, Halothane
Antimitochondrial AntibodiesXanthomas, ↑ Alkaline Phosphatase, Often asymptomatic, insidious onset
Pruritis, Jaundice
Antimitochondrial antibodyMiddle Aged Women
Destruction of interlobular and septal bile ducts, slow progression to cirrhosisMiddle aged women; treated with UDCA or transplantLymphoplasmacytic infiltrate, Absence of bile ducts in portal tract
Primary Sclerosing Cholangitis Unknown Radiographic diagnosis shows stenosis and dilation of biliary tree
Young MenUlcerative Colitis
Cholangiocarcinoma
Diffuse fibrosing inflammation of all segments of biliary treeYoung Men; ulcerative colitisPeriductal fibrosis, bile duct proliferationMay cause cholangiocarcinoma
Fever, chills abdominal pain, jaundice Choledocholithiasis Acute inflammation of wall of bile ducts with PMNs in lumen
Extrahepatic Biliary Atresia Obstructive type jaundiceDark urine & pale stools Kasai Procedure
50% of infants with prolonged cholestasisProgressive fibrosis and cirrhosisPeriportal ductular proliferation & fibrosis, cholestasis or no ductsTreated with Kasai procedure or transplant
Secondary Hemochromatosis
Thallassemia Major, TransfusionsAlcoholic Cirrhosis, Iron Ingestion
Sideroblastic Anemia
ThalassemiaSideroblastic Anemia
Kupffer Cells
↑ Iron causes activation of Ito (Stellate) cells to produce collagenHemosiderin deposits in Kupffer cells
Heriditary Hemochromatosis
Genetic (HFE)Upregulation of iron transport in crypt
Appears in 5th or 6th decade of life, more frequent in men↑ Iron causes activation of Ito (Stellate) cells to produce collagenHemosiderin deposits in hepatocytesHigh incidence of hepatocellular carcinoma
Pathology of the Liver (contd-2)Disease Cause Symptoms Buzzwords Other
Hepatocellular Carcinoma
CirrhosisHepatitis B & C
AflatoxinAlcohol?
Elevated AFP AFP
Metastatic Cancer Breast, Lung, Colon Cancer The most common cancer of the liver
CholangiosarcomaLiver Flukes
Primary Sclerosing CholangitisUlcerative Colitis
Liver Flukes Adenocarcinoma with substantial fibrosis
AngiosarcomaVinyl Chloride
ArsenicThorotrast
Vinyl ChlorideArsenic
ThorotrastVery hemorrhagic
Hepatocellular Adenoma Oral Contraceptives Abdominal Pain (hemorrhage)Rupture Oral Contraceptives Most often in young women taking oral contraceptives
No central veins or portal areas
Focal Nodular Hyperplasia Central Scar Benign hamartoma
Hemangioma Most common benign tumor of the liver
Pathology of the Pancreas
Pathology of the Gallbladder and Biliary TractDisease Cause Symptoms Buzzwords Other
Cholethiasis(Gallstones)
Cholesterol = Age & Obesity(4F’s)
Pigment = Hemolysis & Infection
Majority are assymptomaticExtremely Painful (Angel’s Sign)
Cholesterol Stone or Pigment (bilirubin) stoneComplications: cholecystitis, choledocholethisasis, ascending cholangitis, acute pancreatitis, fistula, porcelin gallbladder
Acute Calculous Cholecystitis Stones in neck or cystic ductCauses chemical irritation and ischemiaMay result in enlarged gallbladder with fibrionus exudates, gangrene, empyema, or porcelin gallbladder
Acute Acalculous Cholecystitis
Post-operative stateTrauma, Burns, Sepsis
Systemic VasculitisS. typhi
Caused by ischemic compromise
Chronic Cholesystitis GallstonesRepeated bouts of acute cholesystitis Rokitansky-Aschoff Fibrosis and variable degree of chronic inflammation
Rokitansky-Aschoff Sinuses – herniation of mucosa (diverticuli)
Cholesterolosis Strawberry Gallbladder Triglyceride & Cholesterol-laden macrophages within mucosal folds
Carcinoma of the Gallbladder CholelithiasisChronic Cholesystitis
Adenocarcinoma with marked desmoplastic reactionUncommon, but poor survival
Carcinoma of the ExtrahepaticBile Ducts
Cholecodal cystsUlcerative colitis
Chronic Biliary Parasites
JaundiceGallstones in about 1/3 of cases Adenocarcinoma with marked desmoplastic reaction
Arises from exocrine duct epitheliumPoor prognosis; Usually in adults > 60More frequent in head of pancreasDiagnosed by CA-19 marker; Treated by Whipple’s operation
Pathology of the KidneyDisease Cause Symptoms Buzzwords Other
Prerenal Acute Renal Failure
Primary Cardiac AbnormalitiesInadequate fluid volume/vascular tone
Fibrin in Bowman’s SpaceBreaks in glomerular basement membrane Crescents Rapid progression - fatal
Diabetes Mellitus(Kimmelstiel-Wilson)
Increased mesangial matrixThickened BMKW Nodules
KW Nodules
Systemic Lupus Erythematosus(SLE) Granular Deposits of all types (full house) Young Women
Full House
Chronic Glomerulonephritis
HypertensionUremia
Granular, Scattered small complexesObliteration by collagen protein
Collagen
Acute Pyelonephritis
Enteric BacteriaHematogenous (Staph & E. coli)
Ascending (E. coli, Proteus, Enterobacter)
Fever, Chills, Malaise, CVA TendernessDysuria, Frequency
Painful at end of voiding
CVA TendernessVesicoureteral Reflux
Papillary Necrosis
Usually associated with a cystitis, often undiagnosedPredisposed: Vesicoureteral Reflux, Pregnant, Females, Catheters, DiabeticsCan cause papillary necrosis, pyonephrosis & perinephric abscess
Patchy necrosis of proximal tubule & ascending limb Patchy Necrosis
ATN is most common cause of ARF & is ReversiblePoor recovery – worse if BM is lost↓ GFR, tubular back leak, tubular obstruction, altered permeability1) Injury 2) Oliguria, Acidosis, ↑ K+, BUN, etc 3) Polyruria, ↓ K+
NephrotoxicAcute Tubular Necrosis
(ATN)
Antibiotics, Anesthetics, Contrast Media, Cyclosporine, Heavy Metals
Organic Solvents, MushroomsConfluent necrosis of proximal tubule Confluent Necrosis
Great prognosisATN is most common cause of ARF & is Reversible↓ GFR, tubular back leak, tubular obstruction, altered permeability1) Injury 2) Oliguria, Acidosis, ↑ K+, BUN, etc 3) Polyruria, ↓ K+
Pathology of the Kidney (contd-2)Disease Cause Symptoms Buzzwords Other
Anion Gap Metabolic Acidosis(Renal Failure) Renal Failure
Most common renal malignancy in adults; originates in tubulesVon Hippel-Lindau Syndrome = RCA, Hemangioblastomas, cystsFrequently metastasis before symptoms appear; usually at polesClear cells most common, invades right heart