Orientation of the COHE Program and WA States L&I Occupational Health Best Practices __________________________________________________________ Prepared by COHE Community of Eastern Washington
Transcript
Orientation of the COHE Program and WA States L&I Occupational Health Best Practices__________________________________________________________Prepared by COHE Community of Eastern Washington
Agenda• What is COHE
• Why do providers join COHE
• What is the role of an HSC
Background of the Centers of Occupational Health &
Education
• Types of workers’ compensation claims
Introduction to Workers’ Compensation
• What are the best practices
• How to apply them
Overview of L&I Occupational Health Best Practices
• Program resources
• Final step for enrollment
Next Steps to Complete Enrollment
• Provide reliable resources to all stakeholders and reduce obstacles within the first year of opening a Washington State Labor & Industry (L&I) Worker Compensation claim.Goal
• Educate providers about the Washington State Occupational Health Best Practices.
Focus
• Deliver care coordination for improved return to work outcomes.
Foundation
Why do providers join COHE?
Incentives• COHE enrolled facilities receive up to 50%
more compensation when initiating an L&I state fund claim.
Best Practice Training
• Receive education in Occupational Health best practices.
• Preferred provider on L&I Find-A-Doc.
Health Service Coordinator
(HSC)
• Access to HSCs for care coordination for up to the first year of a claim to resolve barriers and help to prevent prolonged disability.
COHE Medical Advisors
• Access to expert consultations related to occupational health and assessment of claim barriers.
What is the Role of the Health Services Coordinator (HSC)?
Care Coordination
To provide care coordination in the 1st year of a claim.
To resolve barriers and reduce prolonged disability for improved claim outcomes.
Stakeholder Consultation
To assist Workers, Employers and Providers in navigating worker compensation systems and resources.
Continuous Education
To educate Providers and staff regarding Occupational Health Best Practices.
Call an HSC when:
Assistance is needed with a challenging claim
Have questions related to the Employer or Worker
Have questions regarding L&I Paperwork or Process
L&I State Fund Claims
U.S. Government Federal Claims
Self-Insured Claims
Types of Worker Compensation Claims
L&I State Fund Claims
COHE currently supports State Fund worker compensation
claims ONLY.
Employers and employees pay into a fund for Washington
State to manage the employees’ worker
compensation benefits.
Facility is reimbursed for services by Washington State
Department of Labor & Industries (L&I).
Several thousand employers are covered under the
centralized L&I state fund system.
Self-Insured Claims
Employers can choose to manage their own claims or
have them managed by a third-party administrator
(TPA).
When an employer partners with a Third-Party insurance company, they pay workers’
compensation benefits directly to the worker and
provider.
The claim processes are similar to State Fund
coverage.
The Office of the Ombuds serves as an independent
agent and advocate for self-insured workers.
http://ombuds.selfinsured.wa.gov/
U.S. Government Federal Claims(OWCP, Longshore, Maritime, Rail)
Employees who work for the U.S. Government or for a
Federally regulated Employer fall into this worker
compensation group.
Forms and processes are different than that of L&I State Fund or Self-Insured
patients.
Best Practices
Complete & Timely Report of Accident (ROA)
Complete & Timely Activity Prescription Form (APF)
Provider-to-Employer Phone Call
Barriers to Recovery:Functional Recovery Questionnaire (FRQ)
*Coming Soon
Best Practice 5: Prescribing
#1
Best Practices for Emergency
Department Providers
#2
#3
#4
**
*
Urgent Care providers and all non-ED providers complete 4 Best Practices.
#5
Best Practice #1 Report of Accident (ROA)
• The ROA is the 1st official notice L&I receives of an injury or illness.
• The ROA can be filed online via FileFast. ($10 additional reimbursement for online filing)
• When completing the ROA via FileFast the completed original ROA must still be faxed to L&I.
• Process the ROA as a HOT CLAIM If the injured worker is admitted into hospital or transferred to another; if a catastrophic injury occurred; or if injury resulted in death of worker.
• Fax completed ROA and APF within 2 business days to L&I: 855.222.4652 or 360.902.5126.
• Fax HOT CLAIM to 360.902.4980
Completion of each box on the ROA is not only required but is essential for claim adjudication.
Box 1: List work-related medical diagnosis. e.g., contusion, strain/sprain, abrasion.
Diagnoses such as “pain” and “tenderness” are considered subjective and will not be
allowed by L&I and will result in revision and delay of claim acceptance.
Box 2: Can be completed by support staff, ICD Codes are not required at ED.
Box 3 : Indicate the date you first saw patient for this condition.
Completion of ROA
Pain, Tenderness
Box 4 : Indicate if this condition is due to a specific incident.
Box 5 : Objective Diagnosis/Findings. Be specific and detailed in your objective findings.
Objective Medical Findings (OMFs) are described as a ‘finding’ that can be seen, felt, heard,
measured, or reproduced (by provider) through examination or testing.
*L&I reviews boxes 1 & 5 against ED chart notes when making the determination for claim allowance or
Checking “YES” or "PROBABLY” means in your opinion, the condition is “more likely than not”
(≥ 51%) work-related. Checking “POSSIBLY” or “NO” means, the condition is (< 50%) work-
related, the claim will likely be rejected.
*If selecting something other than yes, indicate reason in chart note.
Box 8: Miss work. If patient is medically unable to perform any work due to the injury, estimate
how many days the patient will miss work.
*If releasing to modified duty select No and indicate restrictions on APF. Time loss begins if off
work 4 or more days.
Completion of ROA
Box 14*, & Box 15a: Shaded areas may be completed by support staff. All other fields must be
completed by health care provider.
*Box 14: For proper claim attribution and enhanced reimbursement, use your L&I Provider
Number and not your NPI. If you work at multiple locations, provider attribution maybe delayed
or made to the wrong clinic.
Box 16: Signature. Medical provider must sign & date ROA to initiate claim. If there is no
Provider signature the claim will be rejected.
Completion of ROA
L&I # is specific to practicing location and preferred
General Hospital 123 456-7890
1234 ABC Lane Port Charles WA 98123
Complete Provider Report of Accident
R Knee Sprain 1 25 20
ꭕ
ꭕ
ꭕ
ꭕ
ꭕ
ꭕ
ꭕ
ꭕOrtho
1234567
01 25 20
01 25 20AP Signature
Dr. COHE
X-ray negative, Decreased ROM, Swelling
RICE, NSAIDS, Ace Wrap, crutches
2
Reimbursement amount is based on the date the health care provider includes in box
15b of the ROA (this exam date).
If that box is blank, the payment system will use box 3 (Date you first saw patient for this
condition). If both boxes are blank, payment will automatically revert to lowest
reimbursement amount because there must be dates in order for the payment system to
calculate any incentives.
S83.91XA
Completeness of ROA includes required worker sections
• Claim ID (top box)
• Language preference (top box)
• Worker name (First-Middle-Last) (box 1)
• Worker gender (box 2)
• Worker home phone (box 4)
• Worker birth date (box 5)
• Worker address (box 6)
• Date of injury (box 14)
• Description of injury/exposure (19b)
• Job title and job duties (box 35)
• Employer Name (box 30)
• Worker signatures (box 42 and 43)
Providers verify all required worker fields are complete:
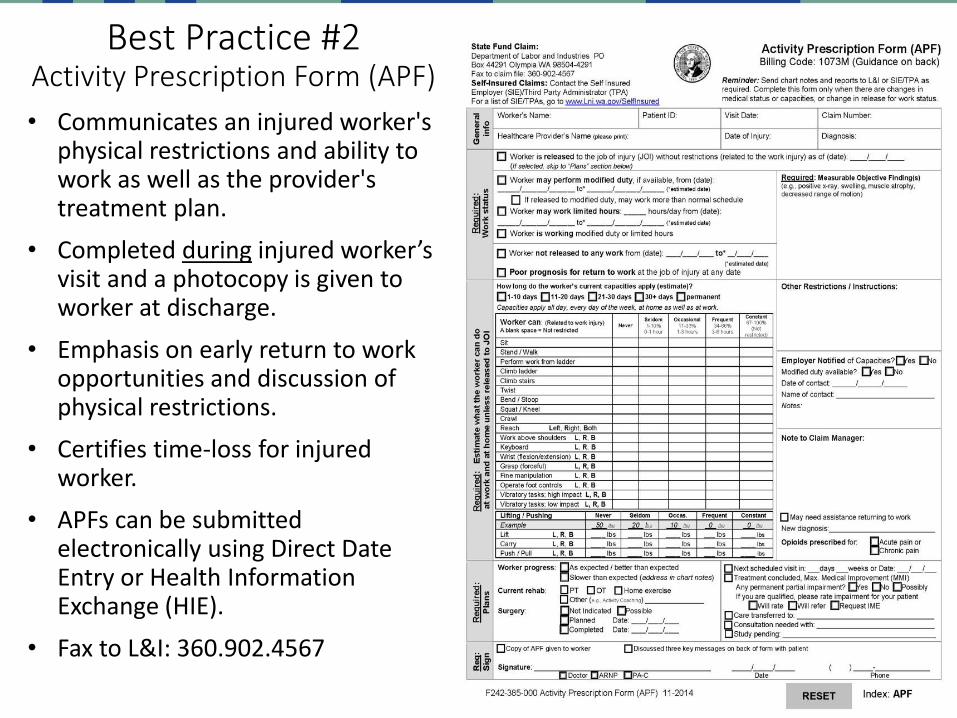
Best Practice #2Activity Prescription Form (APF)
• Communicates an injured worker's physical restrictions and ability to work as well as the provider's treatment plan.
• Completed during injured worker’s visit and a photocopy is given to worker at discharge.
• Emphasis on early return to work opportunities and discussion of physical restrictions.
• Certifies time-loss for injured worker.
• APFs can be submitted electronically using Direct Date Entry or Health Information Exchange (HIE).
• Fax to L&I: 360.902.4567
General Info: Please complete all areas under General Info and list work-related
medical diagnosis. Support Staff can complete all sections except diagnosis.
*Diagnosis must be added by provider.
Work Status: If patient is medically able to return to the job of injury (JOI) without
restrictions (related to work injury), mark patient as released to JOI and note date,
then skip to “Plans” section on APF.
Completion of APF
*
Work Status: If patient is able to return to work and requires modified duty, indicate
with start and end date. If patient is medically unable to perform any work due to
the injury, estimate how many days the patient will miss work.
Make sure there are no time gaps or overlaps in any of the date ranges indicated in
the Work Status and Plans sections.
*This is an estimated date and should cover patient until follow up appointment,
which generally occurs in 3 to 7 business days from ED visit or 3 to 14 days from
Urgent Care visit.
Completion of APF
2 04 20 2 07 20*
2 01 20 2 03 20*
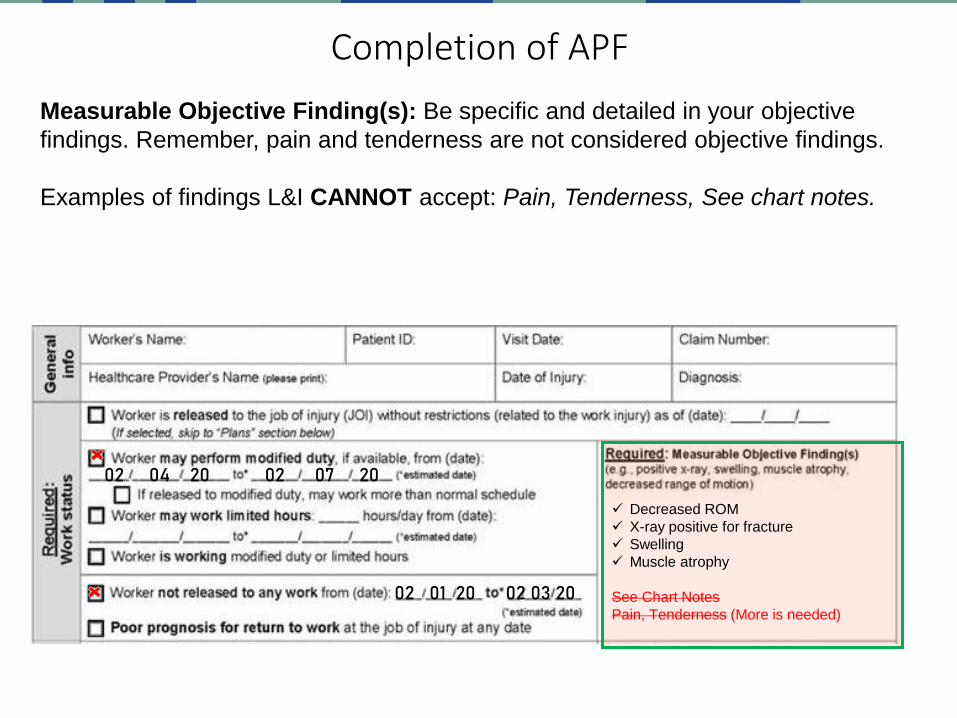
Measurable Objective Finding(s): Be specific and detailed in your objective
findings. Remember, pain and tenderness are not considered objective findings.
Examples of findings L&I CANNOT accept: Pain, Tenderness, See chart notes.
Completion of APF
02 04 20 02 07 20
02 01 20 02 03 20
✓ Decreased ROM
✓ X-ray positive for fracture
✓ Swelling
✓ Muscle atrophy
See Chart Notes
Pain, Tenderness (More is needed)
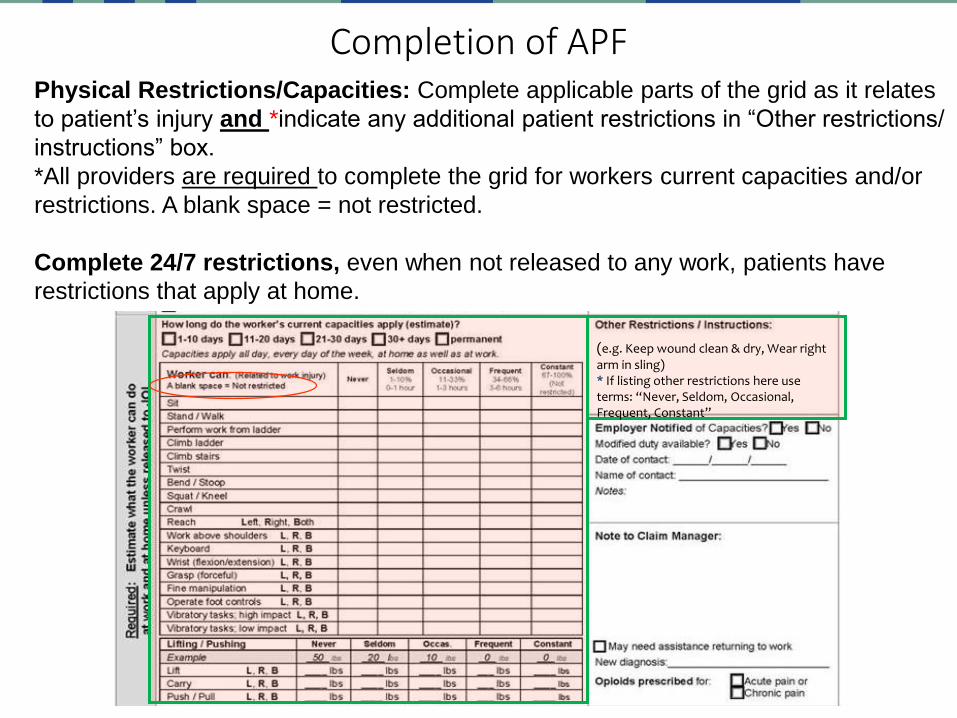
Physical Restrictions/Capacities: Complete applicable parts of the grid as it relates
to patient’s injury and *indicate any additional patient restrictions in “Other restrictions/
instructions” box.
*All providers are required to complete the grid for workers current capacities and/or
restrictions. A blank space = not restricted.
Complete 24/7 restrictions, even when not released to any work, patients have
restrictions that apply at home.
Completion of APF
(e.g. Keep wound clean & dry, Wear right arm in sling)* If listing other restrictions here use terms: “Never, Seldom, Occasional, Frequent, Constant”
Weight Reference Sheet
Produced by L&I 4/16/2007 in collaboration withHome Depot & Fred Meyer
Employer Notified: Make notation on APF when contacting the employer on first visit
or any subsequent communication; documentation must be made in SOAP-ER notes.
*The ER in SOAP-ER notes stands for E – Employment issues and R – Restrictions to
recovery.
Note to Claim Manager: Indicate any notes to claim manager, such as “I am the new
AP.”
Completion of APF
02 01 20
Examples: “I am the new Attending Provider (AP)” “Pending surgical authorization.”
Complete Plans section of APF: Please check all that apply in both columns.
Sign: Sign and date document.
Provide a copy of APF to patient at discharge. Fax a copy of all APFs to L&I.
Completion of APF
*Providers who only see patients in the ED skip to slide 27
APF Best Practice Measures: Measure 1: 80% of all claims have an APF with the ROA (1st visit).Measure 2: 80% of all time-loss claims have a second APF within 4 weeks of claim established date.Measure 3: 80% of all APFs received in 2 business days, excluding weekends and state holidays.(L&I received date subtracted from the APF visit date.)
Best Practice #3Provider-to-Employer Phone Call
Use -32 modifier for all calls or conversations to employers
99441-32Physician Brief Conversation
(1-10 min)
99442-32
Intermediate discussing/resolving RTW issues
(11-20 min)
99443-32
Complexity and/or Duration
(21-30 min)
98966-32Non-physician brief conversation
(1-10 min)
98967-32
Non-physician intermediate conversation
(11-20 min)
98968-32
Non-physician complex conversation
(21-30 min)
9918M
Physician and Non-Physician
Online Communication
(limited to once per day per claim)
Communication by the provider with the employer about restrictions, modified
work, and treatment plan is a billable service.
Make notation on APF when contacting the employer on first visit or any subsequent
communication; documentation must be made in SOAP-ER notes.
What is the FRQ? It’s six questions asked to injured workers to gauge their
chances of returning to work.
The questionnaire is delivered by HSC between 11 days and 6 weeks after
claim initiation.
Questions 1-3: Cover time loss and pain, which determines the overall FRQ
score, positive or negative.
Questions 4-6: Cover work accommodation, recovery expectation,
and fear-avoidance, which helps identify specific worker psychosocial
issues.
If a positive FRQ is determined the HSC will review results with the Attending
Provider (AP) or designated clinic contact to help identify Functional
Recovery Interventions.
Some intervention examples are increasing activity, tracking functional improvement goals and progress, or considering referrals such as Physical
Best Practice #4Barriers to Recovery: Functional Recovery Questionnaire (FRQ)
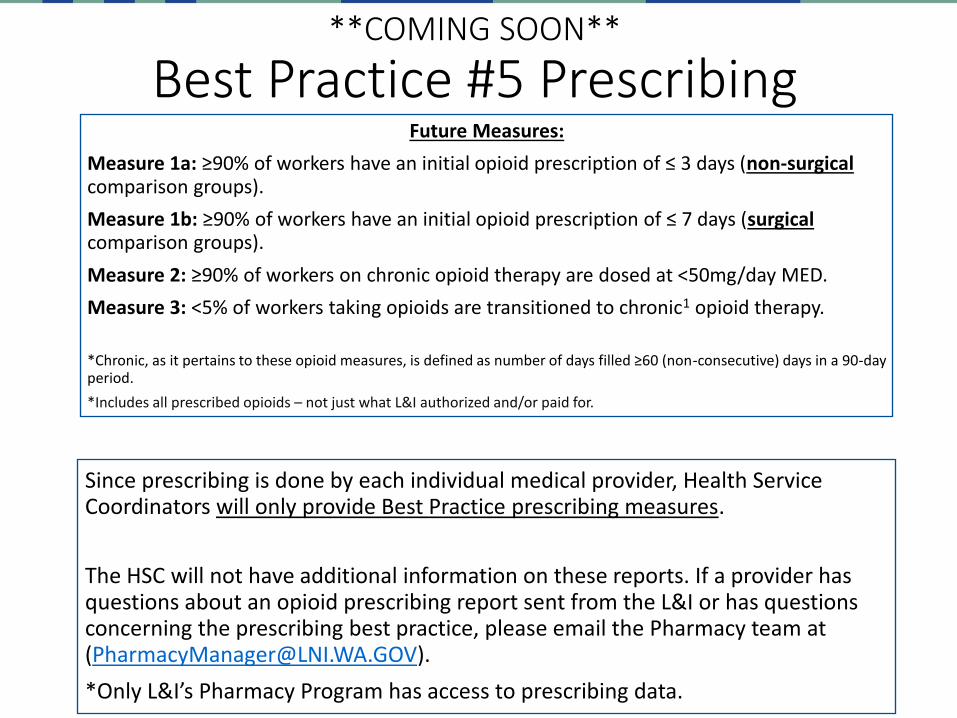
Future Measures:
Measure 1a: ≥90% of workers have an initial opioid prescription of ≤ 3 days (non-surgicalcomparison groups).
Measure 1b: ≥90% of workers have an initial opioid prescription of ≤ 7 days (surgicalcomparison groups).
Measure 2: ≥90% of workers on chronic opioid therapy are dosed at <50mg/day MED.
Measure 3: <5% of workers taking opioids are transitioned to chronic1 opioid therapy.
*Chronic, as it pertains to these opioid measures, is defined as number of days filled ≥60 (non-consecutive) days in a 90-day period.
*Includes all prescribed opioids – not just what L&I authorized and/or paid for.
Since prescribing is done by each individual medical provider, Health Service Coordinators will only provide Best Practice prescribing measures.
The HSC will not have additional information on these reports. If a provider has questions about an opioid prescribing report sent from the L&I or has questions concerning the prescribing best practice, please email the Pharmacy team at ([email protected]).
*Only L&I’s Pharmacy Program has access to prescribing data.
To complete enrollment in the COHE program, complete the quiz.
ED provider: Quiz Link Here
orUrgent Care and all Other providers:
Quiz Link Here
Once your quiz is received, your HSC will send a follow up email with contact information and confirmation of enrollment.
Once enrolled you will be required by contract to complete an annual refresher training. Your HSC will send you or your clinic contact a reminder every year.

































![[Alex] COHE LOTO [Instructor]](https://static.documents.pub/doc/80x56/56d6bed41a28ab301693c015/alex-cohe-loto-instructor.jpg)



