42
Orientation to ICU care Dr. Sameer Jahagirdar & Dr. Lakshmimani

Orientation to ICU care Dr. Sameer Jahagirdar & Dr. Lakshmimani

The presentation deals with….
• How critical care started…
• Types of ICUs
• Overview of ICU admission & progress
• Principles of ICU care:
• Bedside evaluation of critical care
• Therapeutic supportive interventions
Introduction
• ICUs are areas specialized in care of critically ill patients
• The concept evolved from the historical recognition that the needs of patients with acute, life-threatening illness or injury could be better treated if they were grouped into specific areas of the hospital

Historical perspective…
• Florence Nightingale era
In Crimean War (1853) she contributed and introduced Intensive care Protocols in caring severely injured and critically ill war patients.

Historical perspective…
• Dandy era:
Walter Edward Dandy
Neurosurgeon at Johns Hopkins University School of Medicine
Created the first ICU in world, 3 beds in Boston in 1926 for neurocare.

Historical perspective… • Ibsen era
Bjørn Aage Ibsen (1915–2007)
Trained in anaesthesiology (1949 to 1950) at the Massachusetts General Hospital, Boston
He became involved in the 1952 poliomyelitis outbreak in Denmark; changed negative pressure ventilation protocol to intubation & IPPV with help of 200 medical students

Historical perspective…
• Safar era
Peter Safar, the first Intensivist doctor in the USA
Anesthesiologist by profession
Introduced concepts of ABC (airway, breathing, circulation )protocols in resuscitation to ICU care
The first surgical ICU was established in Baltimore, and, in 1962, in the University of Pittsburgh
Types of ICUs… Specialties directed:
General (medical/surgical/combined) Specialized (cardiothoracic/neuro/burns/neonatal/coronary)
OPEN/CLOSED ICU: based on admission & management policy:
Closed ICU: Intensivist is responsible for day to day management of the patients, including all admissions & discharges, orders & clinical mgt. Open ICU: Daily mgt decisions taken by primary physician Primary physician determines need for admission & discharge Intensivist involved in patient care at discretion of primary physician Shared ICU: combined responsibilities with defined domains

Types of ICUs… • High intensity vs Low intensity ICU:
High intensity ICU:
Intensivist responsible for all patient care in a closed ICU
mandatory Intensivist consultation though ICU is open
Low intensity ICU:
Elective Intensivist consultation: ICU is open
No Intensivist available
• Choice vs no-choice ICU:
Choice: Open ICU where Intensivist at discretion of primary physician
No Choice: Closed ICU, Intensivist consultation mandatory or no intensivist
Types of ICUs & Outcome • Variable results depends on involvement of intensivist,
adherence to guidelines
• Closed ICUs have lower morbidity & mortality
• Closed unit may result into “blind period” (primary physician not aware of what happened in ICU after transferring patient back in ward)
• Open ICU: multiple policies by diff physicians creat confusion to junior staff
• Shared mode: dual responsibility

Overview of ICU admission & progress
• No ideal method of “triaging” for admission
• ‘Triage model’ adopted must be within ‘ethical framework’: two key issues
• What criteria or guidelines to be applied
• Who should decide on the allocation of places
• ‘Triage model’ aims at maximum consistency & less psychological impact of decision making on individuals
• Patients admitted to ICU should generally have reversible problem.
• Acute insults causing organ dysfunction: organ support & specific therapy given to hasten recovery

General flow diagram of ICU Process
EXOGENOUS CAUSES
ENDOGENOUS CAUSES INSULT TO THE SYSTEM
ACUTE DETERIORATION & ORGAN DYSFUNCTION
INTENSIVE CARE
DEATH
CARDIORESPIRATORY BRAIN
ORGAN DONATION
RECOVERY
PARTIAL
REHABILITATION
COMPLETE

Principles of ICU care • THERAPEUTIC PERSPECTIVES IN BEDSIDE EVLUATION:
• The term intensive care implies the potential for rapid changes in clinical status. Therefore, patient must be monitored carefully, and lines of communication among caregivers must be kept open.
• A knowledgeable and responsive physician must be continuously accessible and committed to re-evaluating the patient as often and as long as required
• “Feedback loop” approach linking intervention, result, and midcourse correction
• Use of modern gadgets/ PDAs/Internet/telecommunication
• Trends in data stream evaluation
• ICU practitioner’s intervention: quick & decisive action
• Clinician's prime objective should not be to reestablish “normal physiology”, but rather to encourage smooth resolution or adaptation to the pathophysiologic insult
ELEMENTS OF BEDSIDE EVALUATION Verbal communication: Caregivers/ Patient / Family / Referring physician or institution Written communication: Chart record / Nursing notes / Current orders / Medication/therapy lists / Data board Laboratory record: Imaging studies Physical examination: Vital signs Systems review Directed examination Monitored information: Ventilator Hemodynamics Electrocardiogram Other apparatus

VERBAL COMMUNICATION • ICU functions best with a team approach (physicians, nurses,
therapists) with equal commitment & mutual respect
• A well-trained nurse or therapist is often the caregiver with the best insight regarding the relation of events and medications to evolving problems, tolerance of current therapy, and the probable effects of intended interventions
• A skilful clinician seeks their active involvement and advice in the planning process
• A formal rounds with the physician to share observations and advise from nurse, physiotherapist
• “Goal directed orders” offers same advantages as protocol based care in nursing care

Family communication
Undeniable potential for miscommunication can happen during communication with family depending on physician with differing perspectives, knowledge, and attitudes
One or two physicians must be identified as the primary contact(s)
Family must be allowed to visit the patient as soon as appropriate after admission or in an unanticipated emergency
Defining the likely diagnoses and plausible alternatives, the team's approach, the strategy for action, and contingency plans helps instil confidence and trust in patient’s family

Written communication
& Records
Physician review of
chart record
Review nurses orders
Review bedside data
board
Review ventilator
sheet
Review lab records
Bedside calculations :
Anion gap, compliance, resistance,
SVR, CO
Daily weight, I/O, Infusions,
Antibiotics, ETT
secretions
LAB DATA TRENDS IN
DATA
ABGs, hemoglobin concentration, leukocyte
and platelet counts, serum glucose, blood urea
nitrogen (BUN), creatinine, electrolytes, and urinalysis
liver or cardiac enzymes, leukocyte differential,
coagulation profile, drug levels, renal function tests
Any other specific tests
PHYSICAL EXAMINATION
& MONITORING
VITAL SIGNS MENTAL STATUS &
NEUROLOGICAL
EXAMINATION
CARDIOVASCULAR
SYSTEM
RESPIRATORY SYSTEM
RENAL & ELECTROLYST
E STATUS
GASTROINTESTINAL /
NUTRITION
APPARATUS
IMAGING DATA

VITAL SIGNS
• Degree of variability
• Relationships among individual parameters (Extreme respiratory variation evident on an arterial or pulse oximetry tracing suggests relative hypovolemic and/or the paradox associated with severe airflow obstruction, severe left heart failure, or pericardial disease)

Mental status & neuromuscular system
• Glasgow coma scale (best verbal, motor, and eye opening)
• Muscle tone and strength,
• Facial appearance,
• Eye movements
• Pupillary size and reactivity
• Peripheral reflexes, and asymmetry
• Signs of fear, anxiety, depression, and delirium
Ask nursing staff “how well the patient has been sleeping?”

Cardiovascular System
• New gallop, murmur
• Rhythm disturbance
• Paradoxical pulse
• Neck vein distension
• Basilar rales
• Dryness of the mucous membranes
• Diaphoresis
• Edema
• Impaired capillary refill
• Interpreted in conjunction with ECG & arterial pressure tracings, echocardiographic and radiographic information, pulmonary artery catheter, when available
Respiratory System
• Quality, intensity, and symmetry of breath sounds
• Presence or absence of regional percussion dullness
• Breathing pattern
• Audibility and distribution of wheezes, rales, rubs, rhonchi, and bronchial breath sounds
• Vigor and effectiveness of breathing efforts
• Pulse oximetry used for adjusting inspired oxygen fraction (FiO2), positive end-expiratory pressure (PEEP), position, or ventilator settings
• Ventilator data records: minute ventilation, oxygen, and pressure requirements (peak, plateau, mean, and end-expiratory), gas exchange efficiency, patient-ventilator synchrony, integrity of the breathing circuit, and machine mode and settings

Renal and Electrolyte Status
• Urine output: serves as a useful indicator of vital organ perfusion, patients with questionable cardiovascular status, poor intravascular fluid volume status
• Color, pH, specific gravity, glucose and electrolyte concentrations, results of tests for leukocyte esterase, erythrocytes, hemoglobin, and a review of sediment characteristics and pending urine cultures
• BUN and creatinine (trends)
• Arterial blood gases and serum electrolytes: anion gap and serum osmolality

Gastrointestinal/Nutritional
• Review of nutritional intake
• Volume and character of gastric aspirates and stool output
• Evaluate gut motility: physical examination of the abdomen, auscultation

Apparatus
• Intravascular lines and pumps: inspected quickly, sites of entry should be examined for evidence of phlebitis, local cellulitis, or purulence
• Life-support equipment (balloon pump):key variables relevant to its operation and the level of support must be noted
• Enteral catheters and endotracheal tube anchoring devices inspection
• Ventilator circuit examined for collected water
• Data provided by the bedside cardiac monitor and ventilator display to be reviewed with each visit

Imaging Data
• Radiographs, computed tomograms (CT), and ultrasonic images: review

THERAPEUTIC SUPPORTIVE CARE
“Recumbent position is central to extended life support but is inherently unnatural, a working knowledge of the physiology of sustained bed rest and immobility is fundamental to understanding the rationale and consequences of ICU confinement”
Physiology of Bed Rest
Noncardiorespiratory effects
Reduced muscle bulk and strength
Altered biorhythms
Decreased glucose tolerance
Endocrine dysfunction
Fluid shifts and diuresis
Calcium, potassium, and sodium depletion
Immunologic impairment
Nasal congestion/impaired sinus drainage
Reduced gastrointestinal motility/esophageal reflux
Cardiovascular effects
Pulmonary vascular congestion
Impaired vasomotor tone and reflexes
Increased preload and stroke volume
Altered autonomic activity
Respiratory effects
Reduced functional residual capacity
Altered distribution of lung volume
Altered airway drainage

Physiology of bed rest
• Neuromuscular:
“release of the skeletal muscles from their diurnal activity for longer than 24 to 48 hours initiates metabolic processes that eventually culminate in tissue atrophy and impressive physiologic changes”
• Contraction of skeletal muscles compress veins & lymphatics – prevent edema of dependency in legs
• greatest protein losses occur in the muscle groups that normally bear the greatest postural burden—legs and dorsal trunk
• Rates of bulk and strength loss are functions of the length at which the muscle fiber is immobilized, as well as the completeness of relaxation (muscle paralysis)
• Passive manipulation of resting muscle, physical therapy
Physiology of bed rest
• Endocrine and Metabolic
• Bed rest alters circadian biorhythms
• cortisol and epinephrine: trough levels at morning
• Cholinergic (vagal) tone increases at night
• Cycles for insulin and growth hormone (and consequently glucose) often demonstrate multimodal patterns
• Activity of the pancreas gradually declines, and glucose intolerance may develop (3 days)
• Thyroid hormones tend to increase
• Androgen levels fall
• Oxygen consumption declines

Physiology of bed rest
• Fluid and Electrolyte Shifts:
• Recumbency shifts about 10% of the total blood volume (≈500 mL) cephalad, away from the legs
• 80% of shifted volume migrates to the thorax; the remainder translocate to the head and neck
• Diuresis begins on the first day of recumbency (normal subject)
• Nasal mucosal congestion
• Losses of sodium and potassium
• Loss of osteoblastic activity due to loss of standing posture – 0.5% body calcium store depletion
Physiology of bed rest
• Gastrointestinal Changes
• Anorexia and constipation
• Esophageal reflux in those with lax esophageal sphincter function
• Loss of gut mobility – lack of food

Physiology of bed rest
• Immunologic Defences:
• Normal rate of catabolizing immunoglobulin G doubles
• Neutrophilic phagocytosis slows
• Mucosal colonization rate for pathogens (staphylococcus) may increase
• Stasis, secretion pooling, and bacterial overgrowth within the maxillofacial sinuses and tracheobronchial tree – prone for infection
Physiology of bed rest
• Blood Components and Coagulation:
• Vulnerable to thrombosis—largely because of venostasis and unrelieved compression of the leg veins
• Procoagulant synthesis and fibrinolytic activity increase
• Thromboplastin time shortens
• Red cell mass decline (decreased erythropoesis)

Physiology of bed rest • Cardiovascular Effects of Recumbency:
• 1st hour of Recumbency: fluctuations in regional blood flow distribution lost
• Supine position (conscious patient): heart rate & stroke volume increased, BP, SVR & PVR reduced
• Renin angiotensin axis down-regulation: diuresis
• Baroreceptor reflexes blunted (prolonged bed rest)
• Trendelenburg (“head down”) position: • Offers no significant hemodynamic benefit over that provided by the supine
position
• No confirmed place in the management of shock (other than for central line placement)
• Increases intracranial arterial and venous pressures equally and, therefore, no change in cerebral perfusion in normal individuals
• Head injury: elevated intracranial pressures may compromise cerebral perfusion
• Esophageal reflux
• Useful for draining secretions, neck vein distention for cannulation, air embolism

Physiology of bed rest
• Respiratory System:
• Decreases functional residual capacity (FRC): upward pressure of the abdominal contents on the diaphragm and to a lesser extent to declining lung compliance
• FRC declines by approximately 30% in shifting from the sitting to the horizontal supine position and by about 50 % in the sitting to lateral decubitus transition
• Conversion from supine to prone position: increase of resting lung volume of approximately 15%, with most of this change occurring in dorsal regions

• Respiratory System:
• pulmonary hemodynamics:
• Hydrostatic pressures and blood flows tend to distribute preferentially to the dorsal regions in the supine position
• Heart tends to compress the left lower lobe bronchi and is supported partially by the lung tissue beneath – atelectasis more in left lower lobe
• Transpulmonary pressure (alveolar minus pleural pressure) reduced in recumbent position – alveolar volume more in non dependent areas - dorsal atelectasis
Physiology of bed rest
• Distribution of Ventilation:
• Mechanically ventilated patients: nondependent regions receive the most ventilation
• Dependent areas – less end expiratory lung volume – more atelectasis

Immobility: Preventative and Therapeutic Measures
• Bedridden patients must be repositioned every 2 hours unless there is an important contraindication (e.g., hemodynamic instability or spinal injury)
• Inclining the upper torso above the horizontal plane (Fowler's, reverse Trendelenburg, sitting position) helps preserve vascular reflexes, limits the risks of esophageal reflux and aspiration, and reduces the tendency for peridiaphragmatic (basilar) atelectasis.
• Lateral decubitus and prone positions effectively stretch and drain the uppermost lung regions
• Preserve skin integrity
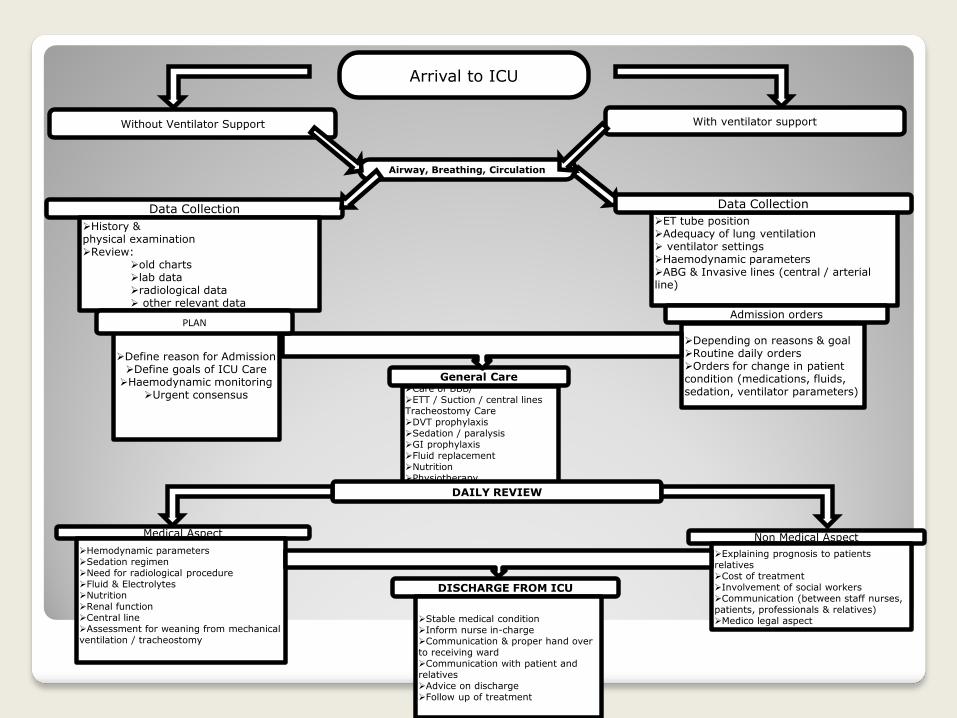
Arrival to ICU
Without Ventilator Support
Airway, Breathing, Circulation
Data Collection
History & physical examination Review:
old charts lab data radiological data other relevant data
Define reason for Admission Define goals of ICU Care Haemodynamic monitoring
Urgent consensus
With ventilator support
Check ET tube position Adequacy of lung ventilation ventilator settings Haemodynamic parameters ABG & Invasive lines (central / arterial line)
Admission orders
Depending on reasons & goal Routine daily orders Orders for change in patient condition (medications, fluids, sedation, ventilator parameters)
General Care Care of BBB/ ETT / Suction / central lines Tracheostomy Care DVT prophylaxis Sedation / paralysis GI prophylaxis Fluid replacement Nutrition Physiotherapy
DAILY REVIEW
Medical Aspect
Hemodynamic parameters Sedation regimen Need for radiological procedure Fluid & Electrolytes Nutrition Renal function Central line Assessment for weaning from mechanical ventilation / tracheostomy
Non Medical Aspect
Explaining prognosis to patients relatives Cost of treatment Involvement of social workers Communication (between staff nurses, patients, professionals & relatives) Medico legal aspect
DISCHARGE FROM ICU
Stable medical condition Inform nurse in-charge Communication & proper hand over to receiving ward Communication with patient and relatives Advice on discharge Follow up of treatment
Data Collection
PLAN