Original Research Spinal Cord Stimulation (SCS) with Anatomically Guided (3D) Neural Targeting Shows Superior Chronic Axial Low Back Pain Relief Compared to Traditional SCS—LUMINA Study Elias Veizi, MD, PhD,* ,† Salim M. Hayek, MD, PhD,* ,‡ James North, MD, § T. Brent Chafin, MD, ¶ Thomas L. Yearwood, MD, PhD, k Louis Raso, MD, ˆ Robert Frey, MD,** Kevin Cairns, MD, †† Anthony Berg, MD, ‡‡ John Brendel, MD, §§ Nameer Haider, MD, ¶¶ Matthew McCarty, MD, ˆ Henry Vucetic, MD, ˆ Alden Sherman, BA,*** Lilly Chen, PhD,*** and Nitzan Mekel-Bobrov, PhD*** *Case Western Reserve Medical Center, Cleveland, Ohio; † Louis Stokes VA Medical Center, Cleveland, Ohio; ‡ University Hospitals Case Medical Center, Cleveland, Ohio; § Carolinas Pain Institute, Winston- Salem, North Carolina; ¶ Roanoke-Chowan Hospital, Roanoke, North Carolina; k Comprehensive Pain and Rehabilitation, Pascagoula, Mississippi; ˆ Jupiter Pain Clinic, Jupiter, Florida; **Pacific Pain Management, Ventura, California; †† Florida Spine Specialists, Fort Lauderdale, Florida; ‡‡ Spine Team Texas, Southlake, Texas; §§ Interventional Pain Specialists of Wisconsin, Rice Lake, Wisconsin; ¶¶ Spinal and Skeletal Pain Medicine, Utica, New York; ˆ Balcones Pain Consultants, Austin, Texas; ˆ Spine and Pain Institute, Akron, Ohio; ***Boston Scientific Corporation, Valencia, California, USA Correspondence to: Elias Veizi MD, MD, Assistant Professor, Department of Anesthesiology, Case Western Reserve University, Pain Medicine Service, Louis Stokes, Cleveland VA, Medical Center, 10701 East Blvd Cleveland, Ohio 44106, Email: [email protected]. Funding sources: Funding for this study was provided by Boston Scientific Neuromodulation Corporation. Disclosure: Data collected from the participating center were provided to the sponsor. The sponsor of the study had full control of the data and performed analysis. Based on the disclosures, the study was sponsored by Boston Scientific Neuromodulation Corporation. Conflicts of interest: All the authors received no funding for manuscript preparation. Dr. Veizi has nothing to dis- close and no conflicts of interest to report. Dr. Hayek is a consultant for Boston Scientific and serves as a mem- ber of the scientific advisory board. Dr. Yearwood is currently a consultant to St. Jude Medical, Nevro, Flownix, Meghan Medical, and Neuronano and was previously a consultant for Boston Scientific. Drs. North, Raso, Haider, Cairns, Berg, Brendel, and Vucetic are consultants for Boston Scientific. Drs. Chafin and McCarty have nothing to disclose and no conflicts of interest to report. Mr. Sherman and Drs. Chen and Mekel-Bobrov are employees of Boston Scientific. Abstract Background. The aim of this study was to deter- mine whether spinal cord stimulation (SCS) using 3D neural targeting provided sustained overall and low back pain relief in a broad routine clinical prac- tice population. Study Design and Methods. This was a multicenter, open-label observational study with an observa- tional arm and retrospective analysis of a matched cohort. After IPG implantation, programming was done using a patient-specific, model-based algo- rithm to adjust for lead position (3D neural target- ing) or previous generation software (traditional). Demographics, medical histories, SCS parameters, pain locations, pain intensities, disabilities, and safety data were collected for all patients. Results. A total of 213 patients using 3D neural tar- geting were included, with a trial-to-implant ratio of 86%. Patients used seven different lead configur- ations, with 62% receiving 24 to 32 contacts, and a broad range of stimulation parameters utilizing a mean of 14.3 (66.1) contacts. At 24 months V C 2017 American Academy of Pain Medicine. All rights reserved. For permissions, please e-mail: [email protected]1 Pain Medicine 2017; 0: 1–15 doi: 10.1093/pm/pnw286
Transcript
Original Research
Spinal Cord Stimulation (SCS) with AnatomicallyGuided (3D) Neural Targeting Shows SuperiorChronic Axial Low Back Pain Relief Comparedto Traditional SCS—LUMINA Study
Elias Veizi, MD, PhD,*, † Salim M. Hayek, MD, PhD,*, ‡
James North, MD,§ T. Brent Chafin, MD,¶
Thomas L. Yearwood, MD, PhD,k Louis Raso, MD,ˆ
Robert Frey, MD,** Kevin Cairns, MD,††
Anthony Berg, MD,‡‡ John Brendel, MD,§§
Nameer Haider, MD,¶¶ Matthew McCarty, MD,ˆ̂
Henry Vucetic, MD,ˆ̂̂ Alden Sherman, BA,***Lilly Chen, PhD,*** and Nitzan Mekel-Bobrov, PhD***
*Case Western Reserve Medical Center, Cleveland,
Ohio; †Louis Stokes VA Medical Center, Cleveland,
Ohio; ‡University Hospitals Case Medical Center,
Cleveland, Ohio; §Carolinas Pain Institute, Winston-
Funding sources: Funding for this study was provided
by Boston Scientific Neuromodulation Corporation.
Disclosure: Data collected from the participating center
were provided to the sponsor. The sponsor of the study
had full control of the data and performed analysis.
Based on the disclosures, the study was sponsored by
Boston Scientific Neuromodulation Corporation.
Conflicts of interest: All the authors received no funding
for manuscript preparation. Dr. Veizi has nothing to dis-
close and no conflicts of interest to report. Dr. Hayek is
a consultant for Boston Scientific and serves as a mem-
ber of the scientific advisory board. Dr. Yearwood is
currently a consultant to St. Jude Medical, Nevro,
Flownix, Meghan Medical, and Neuronano and was
previously a consultant for Boston Scientific. Drs. North,
Raso, Haider, Cairns, Berg, Brendel, and Vucetic are
consultants for Boston Scientific. Drs. Chafin and
McCarty have nothing to disclose and no conflicts of
interest to report. Mr. Sherman and Drs. Chen and
Mekel-Bobrov are employees of Boston Scientific.
Abstract
Background. The aim of this study was to deter-mine whether spinal cord stimulation (SCS) using3D neural targeting provided sustained overall andlow back pain relief in a broad routine clinical prac-tice population.
Study Design and Methods. This was a multicenter,open-label observational study with an observa-tional arm and retrospective analysis of a matchedcohort. After IPG implantation, programming wasdone using a patient-specific, model-based algo-rithm to adjust for lead position (3D neural target-ing) or previous generation software (traditional).Demographics, medical histories, SCS parameters,pain locations, pain intensities, disabilities, andsafety data were collected for all patients.
Results. A total of 213 patients using 3D neural tar-geting were included, with a trial-to-implant ratio of86%. Patients used seven different lead configur-ations, with 62% receiving 24 to 32 contacts, and abroad range of stimulation parameters utilizing amean of 14.3 (66.1) contacts. At 24 months
VC 2017 American Academy of Pain Medicine. All rights reserved. For permissions, please e-mail: [email protected] 1
postimplant, pain intensity decreased significantlyfrom baseline (DNRS 5 4.2, N 5 169, P < 0.0001) andeven more in in the severe pain subgroup(DNRS 5 5.3, N 5 91, P < 0.0001). Axial low back painalso decreased significantly from baseline to 24months (DNRS 5 4.1, N 5 70, P < 0.0001, on the over-all cohort and DNRS 5 5.6, N 5 38, on the severesubgroup). Matched cohort comparison with 213patients treated with traditional SCS at the samecenters showed overall pain responder rates of 51%(traditional SCS) and 74% (neural targeting SCS)and axial low back pain responder rates of 41% and71% in the traditional SCS and neural targeting SCScohorts, respectively. Lastly, complicationsoccurred in a total of 33 of the 213 patients, with a1.6% lead replacement rate and a 1.6% explant rate.
Conclusions. Our results suggest that 3D neuraltargeting SCS and its associated hardware flexibil-ity provide effective treatment for both chronic legand chronic axial low back pain that is significantlysuperior to traditional SCS.
Key Words. Spinal Cord Stimulation; Chronic Pain;Low Back Pain; Spectra; 3D Neural Targeting SCS
Introduction
Chronic pain, estimated to affect up to 55% of the USpopulation [1–6], has been treated using a variety ofapproaches. Spinal cord stimulation (SCS) has beenused effectively over the past decades to treat chronicneuropathic pain in the trunk and limbs. While treatmentof leg pain has been successful, treatment of axial lowback pain with traditional SCS has been challenging [7–11].Anatomical factors are considered to be significant con-tributors to the complexity in treating low back pain withSCS. In particular, in the lower thoracic spine, the pos-ition of the accessible neural fibers innervating the lowback area is believed to be in the lateral part of the dor-sal columns near the larger and more excitable dorsalroots. The excitation of the dorsal roots in these thoracicspinal regions can contribute to unwanted abdominalstimulation [12]. Further, in the midthoracic spinal re-gions where back coverage is most likely to be attained,the contacts are separated from the spinal cord by upto several millimeters of highly conductive cerebrospinalfluid [13], making it more difficult to stimulate the backfibers without generating side effects at the dorsal roots[12,14]. Studies of traditional SCS technologies haveshown that traditional SCS has difficulties overcomingthe challenges in stimulating low back fibers [9]. Recentsmall studies [15] suggest that technical advancementsdesigned to enable better control of the paresthesia lo-cation could yield improvements. Traditionally electricalstimulation of the dorsal columns is associated with par-esthesia. Optimal overlap of paresthesia with the area ofpain has been a prerequisite for good outcomes andpain-relieving stimulation. Electrical field steering for
optimal paresthesia can be challenging due to multiplefactors influencing it. Computer modeling taking into ac-count anatomy, neurophysiology, and stimulation-inducedelectrical fields’ effects on nerve fibers on a three-dimen-sional volume conductor model provides insight that canpotentially lead to improvement of SCS outcomes.Alternative SCS approaches have focused on augmentingthe temporal domain, either by increasing the rate ofstimulation to very high rates [16,17] or by altering thetemporal pattern [18]. However, there are several draw-backs to these approaches. First, these modalities de-plete the battery much more rapidly, requiring morefrequent recharging. Second, these modalities appear tohave significantly longer "wash in" times and require fewhours to a couple of days or longer before the patient ex-periences their benefit [16,17]. As a result, programmingoptimization may take longer as it is difficult to determinein the clinic whether the lead placement, contact configur-ation, and stimulation parameters have been optimallyselected.
A new method to improve SCS outcome for axial lowback pain transforms how the desired neural targets areselected. The approach, called Anatomically GuidedNeural Targeted, uses a combination of independentcurrent control with up to 32 contacts and a three-di-mensional programming algorithm that calculates pre-cisely how much current is needed at each contact.The algorithm is based on a 3D anatomical model thattakes into account the electrical conductivity of spinalcolumn structures—including dorsal CSF depth, relativelead location, and vertebral level of the leads. This sys-tem was developed to supplant an already advancedtraditional SCS system (PRECISION) that had the abilityto fractionate current by 1% increments between con-tacts. These advances have allowed specific steering tothe stimulation to target locations and, with the use ofAnatomically Guided 3D Neural Targeting, rely at theoutset on model-based calculation of how to optimallyposition the central points of stimulation. When stimula-tion is turned on, a central point of stimulation (CPS) isgenerated, enabling precise real-time targeting of thestimulation field to the nerve fibers needed to recruit. Bystimulating the right nerve fibers, the objective is toachieve consistent axial low back pain relief comparedwith traditional SCS. Unlike traditional SCS, which util-izes a trial-and-error method of turning on and off con-tact electrodes in a trial-and-error fashion in order toachieve desired paresthesia, the novel anatomicallyguided 3D neural targeting relies on a priori calculationsin order to target the "sweet spot" of stimulation.
To test the hypothesis that neural targeting can provideeffective low back pain relief, we performed a multicen-ter, long-term pragmatic clinical study of over 200 pa-tients. We examined the improvement in pain scoresobserved in real-world clinical practice, which would in-dicate the effectiveness of SCS therapy and would sup-port the decision-making process on specific chronicpain clinical phenotypes best treated by neuromodula-tion. Real world refers to the concept of "real world
Veizi et al.
2
evidence (RWE), which has been discussed extensivelyin the comparative effectiveness literature. The Instituteof Pharmacoeconomics and Outcomes Research de-fines real world evidence as a measure in understandinghealth care data collected under real life practice cir-cumstances and defines real world studies as observa-tional data from cohort studies.
This paper reports the 24-month results from a multicen-ter, open-label, observational clinical study evaluating thereal world effectiveness of 3D neural targeting in SCS forthe treatment of chronic low back and leg paincompared with traditional SCS. This is the largest chronicaxial low back pain SCS cohort published to date andone of the largest multicenter observational SCS studies.
Methods
Study Design and Patient Selection
This study had three key objectives: 1) to assess thelong-term effectiveness of a new SCS modality, termedanatomically guided 3D neural targeting SCS, under realworld clinical practice. To achieve this, we examinedchanges in pain intensity (0–10 numeric rating scale[NRS]) from baseline to 24 months, both as a continu-ous outcome and as a responder rate; 2) to assess theeffectiveness of neural targeting SCS in treating chronicaxial low back pain, which historically has had limitedsuccess with traditional SCS. To achieve this, we exam-ined the subgroup of patients with axial low back painseparately, that is, no radicular component; and 3) tocompare the effectiveness of neural targeting SCS withtraditional SCS. To achieve this, we incorporated aretrospective cohort from the same centers matched bypropensity scores.
This study includes an observational cohort of consecu-tive patients treated with neural targeting SCS and aretrospective analysis of a matched consecutive cohorttreated with traditional SCS at 13 participating centersin the United States. A total of 11 of the 13 participatingcenters enrolled patients in the study. Institutional reviewboard approval was obtained from each site, and thestudy was conducted in accordance with local regula-tions, good clinical practice guidelines (ISO 14155), andthe Declaration of Helsinki.
In order to maintain close alignment with pragmatic clin-ical outcomes consistent with the goals of this study,only two criteria were specified for inclusion in the study:1) Patients had to be 18 years or older. 2) Treatment withthe SCS device had to be on-label per the local direc-tions for use; such as, patients had to have chronic re-fractory low back and/or leg pain such as patients withfailed back surgery syndrome. In order to minimize bias,all participating centers were required to follow consecu-tive enrollment to include all patients meeting the studyinclusion criteria. Consecutive enrollment was a require-ment for screening of all subjects. The study follow-upduration was 24 months post–implant procedure.
Study Cohorts
3D Neural Targeting SCS Cohort. Two hundred thirteenpatients consecutively trialed with 3D neural targetingSCS who met the inclusion criteria were enrolled in thestudy. This cohort was treated with the PrecisionSpectra SCS System, which supports up to 32 contactsand has multiple current sources and a three-dimensionalmodel-based algorithm that takes into account multipleanatomical variables along the vertebral spine that affectSCS current delivery (Precision Spectra, Boston ScientificCorporation, Valencia, CA, USA).
Traditional SCS Cohort. All consecutive patients treatedat the participating study center with the prior gener-ation Precision SCS System (Precision, Boston ScientificCorporation, Valencia, CA, USA) were considered for in-clusion in the study. This system has been commerciallyavailable since 2004 and supports up to 16 contactswith multiple current sources, but without the model-based algorithm. Propensity score matching (PSM) wasused for inclusion of 213 patients trialed/implanted withtraditional SCS (see Data Collection and StatisticalAnalysis).
Device Description
The 3D neural targeting SCS cohort in this study wastreated with the Precision Spectra SCS System (BostonScientific Corporation, Valencia, CA, USA). The systemdelivers stimulation from an implantable pulse generator(IPG) with up to 32 contacts on leads that are implantedin the epidural space of the spinal canal. The devicecan deliver different amounts of current to each of the32 contacts assigned by the Illumina 3D programmingalgorithm. The algorithm uses a patient-specific, model-based method designed to enable particularly efficientprogramming by allowing the clinician to specify thecentral point of stimulation (CPS) in high resolution usingreal time up/down/left/right adjustment (e.g., 300 micronsin the rostral-caudal direction) with intuitive high-levelcontrols (Figure 1). The algorithm automatically assignsanode/cathode/off and percentage (%) current for eachcontact, accounting for lead positions. Current fraction-ation is possible down to 1 percentile increments.Furthermore, the algorithm allows the user to adjustanode-cathode spacing, or Focus, a parameter theor-ized to be important in adjusting the ratio of the dorsalroot threshold-to-dorsal column threshold [19,20]. Themodel employed is a finite-element model of the spinalcanal that accounts for relative lead positions, distancebetween leads, CSF thickness, and electrical conductiv-ities of several tissue domains and uses an inverse solu-tion method (minimization of squared differencesbetween the modeled desired field and the field that themodel predicts to be achievable with the physical con-tacts) (Figure 1). The algorithm relies on the system’sability to assign both polarity and percentage of totalcurrent (resolution¼ 1%) using the multiple currentsource architecture.
Spinal Cord Stimulation with Anatomically Guided Neural Targeting
3
The traditional SCS cohort was treated with thePrecision SCS System (Boston Scientific Corporation,Valencia, CA, USA). Like Precision Spectra, Precisioncan control the amount of current delivered to each and
every contact, that is, multiple independent current con-trol (MICC). It supports up to 16 contacts and two leadports. Device parameters are optimized manually, gen-erating the stimulation field by assigning individual
Figure 1 3D neural targeting programming algorithm. The programming algorithm (A) is shown with inputs and out-puts. The core of the algorithm is a well-posed least-squares matrix equation that relies on the finite element modelof spinal cord stimulation (SCS) shown in panel (B) [20]. The stimulation field model includes distinct electrical proper-ties for several tissue domains and incorporates estimates of the lead positions in three dimensions based on inputsfrom the user in a lead configuration screen (not shown). In the equation, the electrical behavior of the model isencapsulated in the transformation matrix A, and the desired stimulation field input by the user as a central point ofstimulation (CPS) is represented as u. Given the model A and the desired stimulation u, the distribution of currentsfor each electrode to best approximate u can be calculated as J. When the CPS is incrementally steered by theuser, the algorithm also modulates the amplitude to attempt to keep the stimulation intensity constant. An example isshown in panels (C) and (D). In this example, the color map in panel (C) represents a desired stimulation field (scalarpotential, u) generated by a simple bipole from two imaginary contacts (dotted white rectangles). The algorithm out-puts the polarity and percent current (integers in (D)) on each of the available physical contacts (rectangles, repre-senting two eight-contact leads that are staggered) such that the color map of panel (D) best mimics that of (C) in aleast-squares sense. Note the similarity of the color maps. Also note the complexity of the current distribution that isautomated by the algorithm. The solution afforded by the algorithm allows the clinician greater flexibility in choosingthe desired stimulation field.
Veizi et al.
4
anode and cathode locations along the leads by trialand error based on patients’ feedback regarding pares-thesia location.
Procedures
The SCS trial and permanent implantation procedureswere performed per each center’s standard practice.No lead location or lead type was mandated. Trial dur-ation was between three and seven days, based on in-dividual patient requirements. Trial success wasassessed by percent pain relief (PPR), where a success-ful trial was defined as a PPR of 50% or greater. At per-manent implant, the IPG was placed in either thebuttock or abdominal area, per the directions for use.During the implantation procedure, fluoroscopic imagingwas used to guide the leads within the epidural spaceof the spinal canal. In the 3D neural targeting group, upto four leads and 32 contacts could be used, and pro-gramming was done with the patient-specific, model-based algorithm that accounted for lead position (Table 2;Figures 3 and 4). In the control group, up to two leadsand 16 contacts could be used, and programming wasdone with previous generation (traditional) software thatdoes not have the model-based algorithm that automat-ically accounted for lead position. In both groups,reprogramming could be done as needed per standardof care.
Data Collection and Statistical Analysis
To minimize potential bias, data collection from patientswas performed directly by clinical site personnel, withoutSponsor involvement, for baseline (pre-SCS trial), trial,implant, three months, six months, 12 months, and 24months post–implant procedure. Demographic informa-tion, medical history, stimulation parameters, pain loca-tions, pain intensity, and safety data were collected forall patients. The primary outcome measure of pain in-tensity was collected on a 0–10 NRS where 0¼ no painand 10¼ the worst pain imaginable. Responder rateanalysis was performed in the 3D neural targeting SCScohort to control for the difference between a statistic-ally significant and a clinically significant change. It is ac-ceptable to define a responder to be between 30–50%[21]. In this analysis, a responder was defined as anypatient showing 50% or greater reduction from baselinein NRS score.
Data were summarized using descriptive statistics forcontinuous variables (e.g., mean, standard deviation, N,minimum, maximum), frequency tables or proportionsfor discrete variables, and 95% confidence intervals.Statistical significance was tested using analysis of vari-ance (ANOVA) for repeated measures. In this analysis,responder rate was based on the proportion of patientsshowing a 50% or greater reduction in their reportedNRS pain score between baseline and follow-up (it isclinically acceptable to define responder to be between
30–50% [21]). Statistical analysis was performed usingSAS version 9.3 (SAS, Cary, NC, USA).
Comparison between the 3D neural targeting and thetraditional SCS cohorts was performed using propensityscore matching (PSM). Statistical matching is an in-creasingly popular method for removing imbalance inthe empirical distribution of the pretreatment confound-ers between the treatment and control groups [22,23].PSM is a statistical matching technique for unbiasedcomparison of a treatment effect estimate between twogroups of patients in a nonrandomized study by ac-counting for the covariates that predict whether thetreatment was received instead of randomizing patientsto treatment or control. The propensity score matchingalgorithm was implemented following Dehejia andWahba 2002 [24]. Accordingly:
bsjT ¼ 1 ¼ 1
jNjX
i2N
Yi "1
jJijX
j2Ji
Yj
!;
where N is the treatment group, jNj is the number ofunits in the treatment group, Ji is the set of comparisonunits matched to treatment unit i, and jJij is the numberof comparison units in Ji. Single nearest-neighbormatching without replacement was applied to include213 propensity score–matched patients from the fullconsecutively trialed traditional SCS patients.Nearest-neighbor ties were adjudicated by the treated-first rule to replicate consecutive enrollment.Confounders in the model included site, gender, age,diagnosis, pain location, and pain severity.
Results
Patient Enrollment and Baseline Characteristics
A total of 213 patients were included in the 3D neuraltargeting SCS cohort with fully consecutive inclusion atthe 11 participating centers during the enrollmentperiod. Baseline and trial data were available for all 213patients. Table 1 displays the characteristics of thestudy population. Both cohorts appear similar in base-line characteristics. No statistically significant differencesin baseline characteristics were found between the twocohorts, indicating a successful PSM procedure. Thethree-month follow-up data were available for all pa-tients who received a permanent implant (N¼ 184).Data from the six-month, 12-month, and 24-monthfollow-up visits were available from 181, 178, and 169patients, respectively, reflecting minimal loss to follow-up or early attrition during the study period (92% datacompleteness at 24 months). At baseline, the mean(6SD) patient age was 56.8 (614.39) years and 63% ofthe patients were female. The most common primarydiagnosis for receiving SCS was failed back surgery syn-drome (36%). Patients with chronic axial low back pain (noradicular component to their pain) comprised 42% of thecohort (N¼ 89), while patients with both leg and low back
Spinal Cord Stimulation with Anatomically Guided Neural Targeting
5
pain comprised 38% (N¼ 80) and patients with only legpain comprised 21% (N¼ 44). The distribution of painscores (0–10 scale) at baseline is shown in Figure 2. Meanbaseline pain intensity score [NRS] was 7.2 6 2.06), andmedian baseline pain was 8 (N¼ 213). Nearly 90% ofpatients reported either moderate or severe pain at
baseline, with over half reporting severe pain (N¼108with baseline NRS pain scores of 8–10) (Figure 2).Apart from improving pain scores, the decision to pro-ceed with SCS was mutual between patient and clin-ician and was based on desire to improve function andsleep and reduce analgesic medication use.
*The Other category includes diagnoses found in three patients or fewer (e.g., neuropathies, spinal deformities).†Low back only pain distribution reflects axial low back pain.
Figure 2 Distribution of baseline pain intensities (3D neural targeting spinal cord stimulation [SCS] cohort). Majorityof patients reported either moderate or severe pain at baseline, with half of all patients reporting severe pain.
Veizi et al.
6
SCS Trial and Implant
A total of 213 consecutive patients underwent percutan-eous SCS epidural lead placement for SCS trial, whichlasted three to seven days. The trial success rate was94% (N¼ 200/213), with 200 patients proceeding toSCS implant. Additionally, two patients who had a 40%PPR were identified by the clinicians as appropriate forreceiving a permanent SCS implant due to marked im-provement in self-reported quality of life and a strongdesire to continue with SCS treatment. Due to insur-ance restrictions and other external constraints, the finalnumber of patients who moved on to receive permanentSCS implant was 184, corresponding to an 86.4% trial-to-perm rate. During the implantation procedure of the3D neural targeting cohort, SCS leads were placed pri-marily between the T6 and T9 vertebral levels, based onthe location of the rostral lead tip (Figure 3). The majorityof patients were implanted with leads placed at the T8vertebral level (42%), followed by T7 (30%). There was avariety of different lead configurations across the 184
implanted patients, as shown in Table 2. The predomin-ant lead configurations were two 16-contact percutan-eous leads (37%), two eight-contact percutaneousleads (35%), and four percutaneous eight-contact linearleads (12%). These configurations correspond to a vari-able number of total contacts between 16 and 32. Thisvariation is shown further in Figure 4 with the percent ofpatients implanted with one, two, three, and four leadsand the percent of patients implanted with eight, 16,24, and 32 contacts (electrodes). The predominantnumber of leads implanted was two leads (72%), andthe predominant number of contacts implanted was 32(52%), followed by 16 (37%).
Patients were treated with a wide range of stimulation par-ameters, as seen in Table 3, optimized to each patient’s re-quirements per standard clinical practice. The meanfrequency of stimulation was 59.8Hz (6109.3 Hz) at a5.64 mA (63.43 mA) mean amplitude. Notably, the meannumber of programs used per patient during the study was5.9 (64.0), using, on average, 14.3 contacts (66.1).
Figure 3 Vertebral level of spinal cord stimulation (SCS) leads during implant procedure (3D neural targeting SCScohort). Locations reflect rostral lead tip.
Table 2 SCS lead configurations (3D neural targeting SCS cohort)
Number of contacts Percent of patients
One 1 x 8 lead 8 1Two 1 X 8 leads 16 35One 1 X 16 lead 16 2Three 1 X 8 leads 24 10Four 1 X 8 leads 32 12Two 1 X 16 leads 32 37One 1 x 16 lead þ two 1 X 8 32 3
Flexibility of configurations evident from large number of lead and contact configurations.
Spinal Cord Stimulation with Anatomically Guided Neural Targeting
7
Reduction in Overall Pain (Low Back and Leg Pain)
Mean overall pain prior to treatment for the 3D neuraltargeting cohort was 7.17 6 2.06 (N¼ 213) on a 0–10scale. The pain intensity score decreased significantlyfrom implant baseline to 3.21 6 2.20 (N¼ 184), 2.92 62.07 (N¼181), and 2.94 6 2.62 (N¼ 169) at three, six,and 24 months, respectively, a statistically significantlong-term difference of 4.23 NRS points (P<0.0001,ANOVA) (Figure 5).
To examine whether the clinical outcomes of 3D neuraltargeting SCS were dependent on patients’ baselinepain severity, we also analyzed pain reduction in the co-hort of severe pain patients, defined as those patientswith a baseline NRS score of 8–10 (N¼ 108). The over-all mean pain of 8.75 6 0.78 (N¼ 108) at baseline wasreduced to 3.35 6 2.38 (N¼ 98) by three months and3.03 6 2.23 (N¼ 96) by six months postimplant. This re-duction was sustained out to 24 months postimplant,with an overall mean pain of 3.41 6 2.33 (N¼ 91), astatistically significant difference of 5.34 NRS points(P< 0.0001, ANOVA).
Improvement in Axial Low Back Pain
Of the 213 total patients trialed in this study, 89 patientswere treated for chronic axial low back pain only(chronic low back pain with no radicular component).Mean low back pain prior to treatment was 7.21 6 1.96(N¼ 89). At three months postimplant, the mean lowback pain was 3.51 6 2.02 (N¼ 76), and by six monthsit reached 3.1 6 1.95 (N¼ 74) and was sustained
through 24 months with a mean NRS score of 3.1 62.6 (N¼70) (Figure 6). This corresponds to a statisticallysignificant difference of 4.1 NRS points (P< 0.0001,ANOVA). The severe axial low back pain patients startedwith a baseline mean of 8.6 6 0.7 (N¼49) and reporteda mean low back pain of 3.5 6 2.2 (N¼ 43) at threemonths postimplant. At six months postimplant, thiswas reduced to a mean of 3.1 6 2.0 (N¼ 42) and re-mained below three through 24 months postimplant at3 6 2.4 (N¼ 38), a statistically significant long-term dif-ference of 5.6 points (P< 0.0001, ANOVA).
Responder Rate Analysis
At three months postimplant, 64% of patients were re-sponders to 3D neural targeting SCS, with 50% or more
Figure 4 Percent of patients implanted with each configuration category (3D neural targeting spinal cord stimulationcohort).
Table 3 Device stimulation parameters during
24-month study period (3D neural targeting SCS
cohort)
Mean (6SD)
Stimulation amplitude 5.64 (63.43) mAPulse width 392 (6232) lsecStimulation frequency 59.8 (6109.3) HzNumber of programs per patient 5.9 (64.0)Number of anodes per patient 9.3 (65.2)Number of cathodes per patient 9.0 (65.0)Number of electrodes per patient 14.3 (66.1)
Veizi et al.
8
reduction in overall pain from baseline. By six monthspostimplant, the responder rate reached 73% and re-mained stable long-term through the entire duration of
the study, reaching 74% at 24 months post–implantprocedure (see Figure 7). Responder rate analysis of theaxial low back pain cohort showed very similar results.
Figure 5 Mean overall pain from baseline to 24 months postimplant procedure (3D neural targeting spinal cordstimulation cohort). All patients are shown in the full cohort, and severe patients refers to the patient subgroup withbaseline numeric rating scale score of 8–10. Statistical significance reflects results of repeated measures analysis ofvariance.
Figure 6 Mean axial low back pain from baseline to 24 months postimplant procedure (3D neural targeting spinalcord stimulation cohort). The graph to the left reflects full axial low back pain cohort, and severe patients in the graphto the right reflects the patient subgroup with baseline numeric rating scale score of 8–10. Statistical significance re-flects results of repeated measures analysis of variance.
Spinal Cord Stimulation with Anatomically Guided Neural Targeting
9
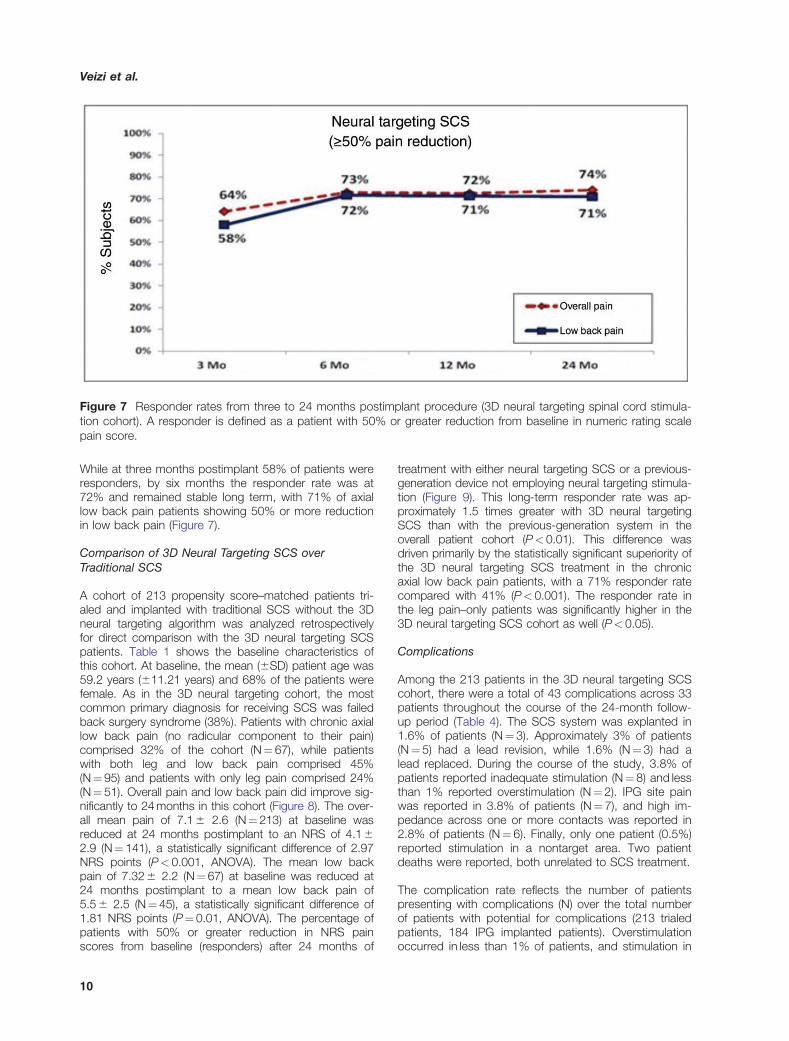
While at three months postimplant 58% of patients wereresponders, by six months the responder rate was at72% and remained stable long term, with 71% of axiallow back pain patients showing 50% or more reductionin low back pain (Figure 7).
Comparison of 3D Neural Targeting SCS overTraditional SCS
A cohort of 213 propensity score–matched patients tri-aled and implanted with traditional SCS without the 3Dneural targeting algorithm was analyzed retrospectivelyfor direct comparison with the 3D neural targeting SCSpatients. Table 1 shows the baseline characteristics ofthis cohort. At baseline, the mean (6SD) patient age was59.2 years (611.21 years) and 68% of the patients werefemale. As in the 3D neural targeting cohort, the mostcommon primary diagnosis for receiving SCS was failedback surgery syndrome (38%). Patients with chronic axiallow back pain (no radicular component to their pain)comprised 32% of the cohort (N¼ 67), while patientswith both leg and low back pain comprised 45%(N¼95) and patients with only leg pain comprised 24%(N¼51). Overall pain and low back pain did improve sig-nificantly to 24 months in this cohort (Figure 8). The over-all mean pain of 7.1 6 2.6 (N¼ 213) at baseline wasreduced at 24 months postimplant to an NRS of 4.1 62.9 (N¼ 141), a statistically significant difference of 2.97NRS points (P< 0.001, ANOVA). The mean low backpain of 7.32 6 2.2 (N¼ 67) at baseline was reduced at24 months postimplant to a mean low back pain of5.5 6 2.5 (N¼ 45), a statistically significant difference of1.81 NRS points (P¼ 0.01, ANOVA). The percentage ofpatients with 50% or greater reduction in NRS painscores from baseline (responders) after 24 months of
treatment with either neural targeting SCS or a previous-generation device not employing neural targeting stimula-tion (Figure 9). This long-term responder rate was ap-proximately 1.5 times greater with 3D neural targetingSCS than with the previous-generation system in theoverall patient cohort (P< 0.01). This difference wasdriven primarily by the statistically significant superiority ofthe 3D neural targeting SCS treatment in the chronicaxial low back pain patients, with a 71% responder ratecompared with 41% (P< 0.001). The responder rate inthe leg pain–only patients was significantly higher in the3D neural targeting SCS cohort as well (P< 0.05).
Complications
Among the 213 patients in the 3D neural targeting SCScohort, there were a total of 43 complications across 33patients throughout the course of the 24-month follow-up period (Table 4). The SCS system was explanted in1.6% of patients (N¼ 3). Approximately 3% of patients(N¼ 5) had a lead revision, while 1.6% (N¼ 3) had alead replaced. During the course of the study, 3.8% ofpatients reported inadequate stimulation (N¼8) and lessthan 1% reported overstimulation (N¼ 2). IPG site painwas reported in 3.8% of patients (N¼7), and high im-pedance across one or more contacts was reported in2.8% of patients (N¼ 6). Finally, only one patient (0.5%)reported stimulation in a nontarget area. Two patientdeaths were reported, both unrelated to SCS treatment.
The complication rate reflects the number of patientspresenting with complications (N) over the total numberof patients with potential for complications (213 trialedpatients, 184 IPG implanted patients). Overstimulationoccurred in less than 1% of patients, and stimulation in
Figure 7 Responder rates from three to 24 months postimplant procedure (3D neural targeting spinal cord stimula-tion cohort). A responder is defined as a patient with 50% or greater reduction from baseline in numeric rating scalepain score.
Veizi et al.
10
Figure 9 Long-term responder rates of 3D neural targeting spinal cord stimulation (SCS) compared with traditionalSCS with a previous generation system. At 24 months postprocedure, responder rate for SCS with 3D neural target-ing was superior to traditional SCS without 3D neural targeting for overall pain, leg pain only, and axial back pain pa-tients. In particular, the responder rate is approximately 1.5 times and 1.7 times higher for overall pain and axial backpain, respectively. (3D neural targeting cohort patients were implanted with Precision Spectra System, while previousgeneration cohort patients were implanted with Precision System.) Superiority of anatomically guided 3D neural tar-geting SCS was most statistically significant in the axial low back pain cohort.
Figure 8 Mean overall and low back pain from baseline to 24 months postimplant procedure (traditional spinal cordstimulation). Statistical significance reflects results of repeated measures analysis of variance.
Spinal Cord Stimulation with Anatomically Guided Neural Targeting
11
an unwanted region occurred in only 0.5% of patients.The two deaths in this study were not related to theSCS device or procedure.
Discussion
In this multicenter study of 213 patients, we found that3D neural targeting SCS was capable of providing long-term relief of leg pain, leg pain with low back pain, andexclusive axial low back pain for the entire 24-monthstudy period. Importantly, it provided similar amounts ofrelief to all subgroups regardless of pain location (lowback and leg or low back only) or baseline severity(mild, moderate, or severe), which has traditionally beendifficult to achieve, particularly for low back pain [9]. Inall of these subgroups, NRS pain scores dropped bymore than half at three months postimplantation andwere maintained at low levels for at least 24 monthspostimplantation. In addition, comparison between 3Dneural targeting and traditional SCS from a previous-generation system without 3D neural targeting in pa-tients treated at the same clinical sites revealed that thenew SCS paradigm was both statistically and clinicallysuperior to traditional SCS in overall pain (51% vs 74%),leg pain (63% vs 81%), and axial low back pain (41% vs71%). For overall pain, the difference between the meanbaseline and mean 24-month pain levels was 1.3 pointsgreater with neural targeting SCS. For axial low backpain, however, this difference was 2.3 points greaterwith neural targeting SCS than with traditional SCS.Thus, while superiority of neural targeting SCS isobserved for all pain areas, it is most pronounced forlow back pain. Notably, this is driven by the continuouseffectiveness in improving back pain relief at 24 months
postimplant. In traditional SCS cohort, while mean lowback pain was reduced to 3.9 6 2.2 at three months,by 24 months postimplant the mean low back pain wasback up to 5.5 6 2.5. In contrast, in the neural targetingSCS cohort, the mean low back pain at 24 monthspostimplant was maintained at 3.1 6 2.6.
Unlike traditional SCS modalities used over the past fewdecades, which optimize their stimulation parametersvia trial and error for paresthesia coverage, neural tar-geting SCS optimizes its parameters by modeling, atthe outset, the central points of the stimulation fieldwithin the patient’s unique three-dimensional anatomicalspace and lead location, and then choosing the param-eters that best target these central points to the desiredneural fibers. Thus, the differentiation from traditionalSCS seen in terms of clinical outcomes may be the re-sult of the fundamental approach neural targeting SCSuses to choose the stimulation parameters needed forrecruitment of the desired neural fibers, without recruit-ing extraneous structures.
To date, SCS studies of low back pain have focused onmixed or predominant low back pain, that is, back painthat includes a radicular component. Due to the sub-jective and dynamic nature of pain, this does not pro-vide a clean signal of the treatment effect as a patient’sability to distinguish between the effect on the low backvs radicular components of his/her pain is limited. Thisstudy, however, includes a large cohort of axial lowback pain patients (no radicular component), providing acleaner signal in determining whether this traditionallydifficult-to-treat pain area can be targeted to provide ef-fective and durable long-term relief.
Comparison between two or more treatment groups isoften achieved by employing a randomized controlledtrial (RCT) design. The RCT design, however, has someimportant drawbacks, which have been discussed atlength in the experimental design literature. Foremostamong these is the limited generalizability of the RCTpatient population. RCTs include both restrictive patientselection criteria to minimize heterogeneity among pa-tients and highly prescriptive treatment algorithms tominimize heterogeneity among clinicians’ practices. TheInternational Society for Pharmacoeconomics andOutcomes Research (ISPOR) Real World Data TaskForce has noted that many RCTs with extensive inclu-sion and exclusion criteria may not be generalizable to areal world patient population, while a well-conductedobservational study can often provide more relevant evi-dence regarding effectiveness in a real-world setting.Consequently, the major health care policy and com-parative effectiveness research organizations stronglyrecommend greater emphasis on observational data.This is not to say that RCTs are not valuable or that ob-servational designs should replace RCT designs.Instead, the two study paradigms address differentissues—can it work vs does it work, efficacy vs effect-iveness—and should be viewed as complementary.Further, large RCTs in the SCS field have been primarily
Table 4 Complications during 24-month study
period (3D neural targeting SCS cohort)
Complication rate
Inadequate stimulation 3.8% (N¼ 8)*IPG site pain 3.8% (N¼ 7)†
High impedance 2.8% (N¼ 6)*Lead revision 2.7% (N¼ 5)†
A total of 43 complications across 33 patients. Complicationrate reflects number of patients with presenting with complica-tion (N) over total number of patients with potential for compli-cation (*¼213 trialed patients, †¼184 IPG implantedpatients). Overstimulation occurred in<1% of patients, andstimulation in an unwanted region occurred in only 0.5% ofpatients. The two deaths in this study were not related to theSCS device or procedure.
Veizi et al.
12
open-label [9,10,17] and could not control for the ex-pectation effect. In fact, previous studies have shownthat in open-label RCTs subjects have a higher likeli-hood of favoring the new treatment [25]. This confound-ing factor is particularly challenging in SCS studies giventhe subjective nature of pain and of its methods ofmeasurement.
The primary goal of the Lumina study was to examinewhether a new model-based designed algorithm(Anatomically Guided 3D Neural Targeting) when appliedclinically results in improved long-term ourcomes intreatment of back and leg pain. For that purpose, weselected an observational study design combined withunbiased enrollment of an equivalent treatment group atthe same clinical centers and statistical validation of thegroups’ comparability. Enrollment was fully consecutive,and site-level sample sizes were matched to the 3Dneural targeting treatment group, wherever possible.Selection bias, which is often raised as the key concernwith nonrandomized comparisons, was avoided here al-together in that the availability of the two systems at theparticipating centers did not co-occur. Enrollment of thetraditional SCS cohort followed consecutive enrollmentduring the 24-month period immediately preceding theenrollment of the 3D neural targeting SCS group.External bias was removed by restricting all data collec-tion from patients to clinical site personnel, with nosponsor involvement or presence. Finally, in order tominimize selection bias and ensure comparability be-tween the two treatment groups, propensity scorematching was performed for inclusion of the control co-hort from the consecutively treated comparison group.Propensity score matching (PSM) [26] is the most com-monly used matching method for causal analysis in ob-servational studies [27]. It is used or referenced in over53,600 scholarly articles [28]. The data collected reflectsthe true heterogeneity in patients’ etiologies and clin-ician’s practices that exists with any medical interven-tion. In doing so, the observed clinical outcomes arereflective of what clinicians and patients can expect inthe real world clinical setting.
Technology Considerations
Our findings are consistent with the hypothesis thatSCS with 3D neural targeting can address the historicalchallenges of traditional SCS for axial low back pain andprovide highly effective pain relief for both legs and thelow back. New technological features incorporated intothis form of SCS may contribute to these outcomes.This study is the first to use an SCS system with up tofour lead ports and 32 contacts, providing more cover-age and flexibility. The 184 patients implanted in thisstudy received seven different lead configurations, span-ning all four possible contact numbers (8–32).Theoretical studies examining leads with 20 contactshave suggested that being able to choose from manycontacts allows for more specific programming to cus-tomize the regions that are stimulated [29]. The broadselection in the stimulation parameters suggests that in
real world clinical practice different patients require awide range of parameters, including stimulation ampli-tude, frequency, pulse width, and contact configuration.Further, this study is the first to use a 3D neural target-ing algorithm incorporating lead position. The algorithmis designed to stimulate desired areas to relieve painwithout spilling over into unwanted areas (e.g., abdom-inal stimulation via dorsal root stimulation). This level ofprecision is consistent with what was observed in thisstudy, with only one patient (0.5%) reporting stimulationin an area outside the targeted pain regions (i.e., un-wanted stimulation). Additionally, the Focus feature(anode-cathode spacing) may further contribute by ad-justing the ratio of dorsal root threshold to dorsal col-umn threshold.
Limitations
While careful attention was paid to maximize the inter-pretability and generalizability of the study outcomes, aswith any study, certain limitations exist. The combinationof an observational design with statistical cohort match-ing is a powerful way of achieving valid comparisons be-tween the two treatment groups without compromisingthe pragmatic generalizability of the study results.Nonetheless, it is important to recognize that unknownconfounding variables may exist and this comparisonmethod in this study does not incorporate prospectiverandomization. Our measurement of low back painrelied only on the axial low back pain patients in ourstudy, not patients with both low back and leg pain. Wechose this approach because these patients provide thecleanest signal of low back pain improvement, withoutthe confounding matters of additional pain areas.Additionally, axial low back pain patients have historic-ally been the most challenging [11]. Consequently,measuring low back pain outcomes in these patients isconservative and may mark the minimal expected im-provement with this 3D neural targeting for low backpain. The study’s inclusion and exclusion criteria werepurposefully left almost entirely open, with the exceptionof age and on-label treatment, in order to best mirrorreal world clinical practice. While we believe that thisgeneralizability is critical to the objective of the study, itdoes inherently result in patient heterogeneity. In fact, itis precisely this heterogeneity that we sought to capture.Nonetheless, a limitation of the study is that the out-comes reflect mean improvements, some of which maybe different among different patient subgroups and etiol-ogies. Another limitation relates to the nature of chronicpain. Chronic pain may be nociceptive, neuropathic, ormixed. Our study did not attempt to differentiate thepain types and the phenotype(s) that is (are) responsiveto SCS.
Conclusions
The LUMINA Study is the largest multicenter pragmaticSCS cohort results published to date. The study dem-onstrated the long-term effectiveness of the applied 3Dneural targeting algorithm applied for SCS and even its
Spinal Cord Stimulation with Anatomically Guided Neural Targeting
13
superiority over traditional SCS in the treatment of over-all pain, leg pain, and axial low back pain. The signifi-cant improvement with 3D neural targeting SCS wasassociated with a reduction, on average, from severepain down to mild pain levels. The precise neural target-ing afforded by this new SCS paradigm was associatedwith minimal unwanted stimulation. The wide selectionin lead configuration and stimulation parameters under-scores the importance of flexibility and patient-specificcustomization to achieving these clinical outcomes. Toour knowledge, this study presents the largest multicen-ter chronic axial low back pain SCS cohort published todate, in contrast to recent studies that have excludedaxial low back pain with no radicular component[16,17,30]. In light of its overall design, large samplesize, and the steps taken to ensure unbiased compari-son between its two cohorts, the significant and super-ior leg and low back pain reduction observed in thisstudy represents evidence that may be generalizable tothe broader SCS population. These findings representan important step forward in the evidence base for SCStreatment of chronic low back pain.
Author Contributions
Protocol was prepared by the Boston Scientific studyteam with input from investigators. The authors wereelected based on their contributions to the study. All in-vestigators were involved in either data collection, exe-cution of the study, or preparation of the manuscriptand interpretation of the data.
Dr. Veizi and Dr. Hayek were involved in literaturesearch and preparation of the manuscript. Drs. North,Chafin, Yerwood, Raso, Cairns, Berg, Brendel, Haider,McCarty, and Vucetic were site investigators, providedreview for intellectual content, and provided final ap-proval of the manuscript. Mr. Sherman and Drs. Chenand Mekel-Bobrov were part of the sponsor’s studyteam. Dr. Mekel-Bobrov analyzed the data. The sponsorof the study had full control of the data and performedanalysis.
References1 Andersson HI, Ejlertsson G, Leden I, Rosenberg C.
Chronic pain in a geographically defined generalpopulation: Studies of differences in age, gender,social class, and pain localization. Clin J Pain 1993;9:174–82.
3 Elliott AM, Smith BH, Penny KI, Smith WC,Chambers WA. The epidemiology of chronic pain inthe community. Lancet 1999;354:1248–52.
4 Gureje O, Von Korff M, Simon GE, Gater R.Persistent pain and well-being: A World HealthOrganization Study in Primary Care. JAMA 1998;280:147–51.
5 Portenoy RK, Ugarte C, Fuller I, Haas G.Population-based survey of pain in the UnitedStates: Differences among white, African American,and Hispanic subjects. J Pain 2004;5:317–28.
6 Verhaak PF, Kerssens JJ, Dekker J, Sorbi MJ,Bensing JM. Prevalence of chronic benign pain dis-order among adults: A review of the literature. Pain1998;77:231–9.
7 Barolat G, Massaro F, He J, Zeme S, Ketcik B.Mapping of sensory responses to epidural stimula-tion of the intraspinal neural structures in man. JNeurosurg 1993;78:233–9.
8 Barolat G, Oakley JC, Law JD, et al. Epidural spinalcord stimulation with a multiple electrode paddlelead is effective in treating intractable low back pain.Neuromodulation 2001;4:59–66.
9 Kumar K, Taylor RS, Jacques L, et al. The effects ofspinal cord stimulation in neuropathic pain are sus-tained: A 24-month follow-up of the prospectiverandomized controlled multicenter trial of the effect-iveness of spinal cord stimulation. Neurosurgery2008;63:762–70; discussion 770.
10 North RB, Kidd DH, Farrokhi F, Piantadosi SA.Spinal cord stimulation versus repeated lumbosacralspine surgery for chronic pain: A randomized, con-trolled trial. Neurosurgery 2005;56:98–106. discus-sion 106-107.
11 Oakley JC, Espinosa F, Bothe H, et al. Transversetripolar spinal cord stimulation: Results of an interna-tional multicenter study. Neuromodulation 2006;9:192–203.
12 Holsheimef J, Barolat G. Spinal geometry and par-esthesia coverage in spinal cord stimulation.Neuromodulation 1998;1:129–36.
13 Holsheimer J, Barolat G, Struijk JJ, He J.Significance of the spinal cord position in spinalcord stimulation. Acta Neurochir Suppl 1995;64:119–24.
14 Oakley JC, Prager JP. Spinal cord stimulation:Mechanisms of action. Spine (Phila Pa 1976) 2002;27:2574–83.
15 Duyvendak W. Spinal cord stimulation with a dualquadripolar surgical lead placed in general
Veizi et al.
14
anesthesia is effective in treating intractable lowback and leg pain. Neuromodulation 2007;10:113–9.
16 Van Buyten JP, Al-Kaisy A, Smet I, Palmisani S,Smith T. High-frequency spinal cord stimulation forthe treatment of chronic back pain patients: Resultsof a prospective multicenter European clinical study.Neuromodulation 2013;16:59–65, discussion 65–6.
17 Kapural L, Yu C, Doust MW, et al. Novel 10-kHzHigh-frequency therapy (HF10 therapy) is superior totraditional low-frequency spinal cord stimulation forthe treatment of chronic back and leg pain: The SENZA-RCT randomized controlled trial. Anesthesiology 2015;123:851–60.
18 De Ridder D, Plazier M, Kamerling N, Menovsky T,Vanneste S. Burst spinal cord stimulation for limb andback pain. World Neurosurg 2013;80:642–9, e641.
19 Holsheimer J, Wesselink WA. Optimum electrodegeometry for spinal cord stimulation: The narrowbipole and tripole. Med Biol Eng Comput 1997;35:493–7.
20 Holsheimer J, Wesselink WA. Effect of anode-cathode configuration on paresthesia coverage inspinal cord stimulation. Neurosurgery 1997;41:654–9, discussion 659–60.
21 Farrar JT, Young JP Jr, LaMoreaux L, Werth JL,Poole RM. Clinical importance of changes in chronicpain intensity measured on an 11-point numericalpain rating scale. Pain 2001;94:149–58.
22 Ho DE, Imai K, King G, Stuart EA. Matching as non-parametric preprocessing for reducing model
dependence in parametric causal inference. PolAnal 2007;15:199–236.
23 Morgan SL, Winship C, ed. Counterfactuals andCausal Inference. 2nd edition. New York:Cambridge University Press; 2014.
24 Dehejia RH, Wahba S. Propensity score-matchingmethods for nonexperimental causal studies. RevEcon Stat 2002;84(1):151–61.
25 Colditz GA, Miller JN, Mosteller F. How study designaffects outcomes in comparisons of therapy. I:Medical. Stat Med 1989;8:441–54.
26 Rosenbaum PR, Rubin D. The central role of thepropensity score in observational studies for causaleffects. Biometrika 1983;70:41–55.
27 Pearl J. An introduction to causal inference. Int JBiostat 2010;6:Article 7.
28 King G, Neilsen R. Why propensity scores shouldnot be used for matching. 2016. https://scholar.google.com/scholar?cluster=5398301161374821142&hl=en&as_sdt=0,36.
29 Kent AR, Min X, Rosenberg SP, Fayram TA.Computational modeling analysis of a spinal cordstimulation paddle lead reveals broad, gapless der-matomal coverage. Conf Proc IEEE Eng Med BiolSoc 2014;2014:6254–7.
30 Al-Kaisy A, Palmisani S, Smith T, Harris S, Pang D.The use of 10-kilohertz spinal cord stimulation ina cohort of patients with chronic neuropathiclimb pain refractory to medical management.Neuromodulation 2015;18:18–23; discussion 23.
Spinal Cord Stimulation with Anatomically Guided Neural Targeting