36
HOAG ORTHOPEDIC INSTITUTE 2012 OUTCOMES REPORT
HOAG
ORTHOPEDIC I N S T I T U T E
2012 O U T C O M E S R E P O R T

TABLE OF CONTENTSINTRODUCTION 4
COMMUNITY SERVICE 5
CHARITY CARE 5
RESEARCH AND EDUCATION 6
OUTCOMES 8
VALUE-BASED PURCHASING 8
SURGICAL CASE VOLUME 10
READMISSION RATE 13
INFECTION PREVENTION 14
METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS (MRSA) 14
CATHETER ASSOCIATED URINARY TRACT INFECTIONS (CAUTI) 16
SURGICAL SITE INFECTIONS 16
SURGICAL CARE IMPROVEMENT PROJECT (SCIP) 18
LENGTH OF STAY 20
RAPID MOBILIZATION 20
iCAREPASSPORT™ – PATIENT EDUCATION 20
PATIENT EXPERIENCE 21
HOSPITAL CONSUMER ASSESSMENT OF HEALTH PROVIDERS 21 AND SYSTEMS SURVEY (HCAHPS)
iCAREPASSPORT™ – PATIENT ENGAGEMENT 23
PERFORMANCE IMPROVEMENT 26
DISTINCTIONS & INNOVATIONS 28
FACILITY INNOVATION 29
“GREEN MEASURES” INITIATIVE 29
BEST PRACTICE STERILIZATION 29
TRAVEL PROGRAM FOR OUT-OF-AREA PATIENTS 30
LEADERSHIP & MEDICAL STAFF 31
CONTACT INFORMATION & RESOURCES 33
DISCLOSURE OF OWNERSHIP 34
2012 O U T C O M E S R E P O RT | 3
PRESENTING THE 2012 OUTCOMES REPORTAt Hoag Orthopedic Institute (HOI), raising the quality of orthopedic care while simultaneously lowering costs calls for a deliberate, thorough and ongoing evaluation of outcomes, trends, and quality improvement interventions. Performance measurement provides a vital tool for our delivery of best-practice medical care.
HOI has committed to transparency in reporting outcomes data. By providing timely and accurate information about our patient care practices, referring physicians and patients can be well informed and thus make better healthcare decisions.
HOI’s quality tracking mechanisms enable us to participate in the following public reporting initiatives:
• Joint Commission Performance Measurement Initiative (www.qualitycheck.org)
• California Department of Health (www.calhospitalcompare.org)
• U.S. Department of Health and Human Services (www.hospitalcompare.hhs.gov)
As a forerunner in outcomes measurement and reporting, HOI has been selected by the California Joint Replacement Registry to develop a statewide registry database for tracking long-term outcomes in patients undergoing joint replacement surgery.
In this report, along with clinical outcomes, we have provided some concrete examples regarding our pursuit of excellence in quality of care and patient safety, community partnerships and leadership in future healthcare delivery. To augment the information in this Outcomes Report, we have included additional data on our website at www.hoagorthopedicinstitute.com.
We are proud to present our inaugural Outcomes Report and welcome your comments and feedback.
Sincerely,
Robert S. Gorab, MD Dereesa Reid, MBA Chief Medical Officer Chief Operating Officer
OUR MISSION
TO RESTORE, IMPROVE AND ENHANCE THE HEALTH AND MOBILITY OF
INDIVIDUALS WITH MUSCULOSKELETAL CONDITIONS AND DISEASES
THROUGH EXCELLENCE IN CARE AND OUTCOMES, CLINICAL INNOVATION,
RESEARCH AND ADVOCACY.

4 | H O A G O RT H O P E D I C I N S T I T U T E
INTRODUCTIONWhen Hoag Orthopedic Institute opened in November 2010, it brought together many of Southern California’s most respected orthopedic surgeons in a partnership with the leading healthcare system in Orange County, Hoag Memorial Hospital Presbyterian.
Through this unique alliance, a number of highly regarded orthopedic specialists joined forces to offer patients unprecedented access to comprehensive orthopedic diagnostics and treatment in state-of-the-art facilities.
Hoag Orthopedic Institute and its 320 medical specialists and 80 board-certified orthopedic surgeons operate one of the highest volume specialty hospitals in the United States. Care is exclusively for orthopedic patients requiring inpatient and outpatient surgical care for conditions related to:
The facility was fully renovated prior to its opening in late 2010. For the interior architecture, designers used the nearby Mountains to Sea Trail, a popular 26-mile hiking and biking trail, as inspiration. A photo contest soliciting community images of the trail helped add to the local personality of the hospital. The physical surroundings are designed to foster healing, incorporating feng shui elements and focusing attention on keeping the noise level at a minimum.
Nurse navigators foster HOI’s patient-centered environment. Each inpatient has a nurse navigator as a personal guide from the moment the patient decides to pursue surgery, through the surgery itself, physical therapy, discharge and ongoing care.
The HOI enterprise also includes Orthopedic Surgery Center of Orange County (OSCOC) in Newport Beach and Main Street Specialty Surgery Center in Orange–two well-respected outpatient surgical facilities dedicated to the care of orthopedic patients. Data in this publication reflects statistics for patients treated at all three centers, with a more specific emphasis on care exclusively at Hoag Orthopedic Institute’s hospital.
• Arthritis
• Ankle & Foot
• Fracture Care
• Hand & Wrist
• Knee & Hip
• Pain Management
• Shoulder & Elbow
• Spinal Disorders
• Sports Medicine
Located at 16250 Sand Canyon Avenue between the 5 and 405 freeways in Irvine, California, HOI’s hospital has 70 beds and nine operating rooms designed and equipped specifically for orthopedic surgical procedures.
2012 O U T C O M E S R E P O RT | 5
COMMUNITY SERVICEHoag Orthopedic Institute surgeons and staff have long been committed to the communities where they work and live. This commitment is furthered by contributing one percent of HOI’s gross charges to fund charity orthopedic care; and through a partnership with El Sol Community Clinic.
In addition, Hoag Orthopedic Institute surgeons have supported regional athletic programs for more than two decades, acting as physicians for the following Orange County and national teams:
Corona Del Mar High School Crean Lutheran High School El Modena High School Irvine High School Mater Dei High School Newport Harbor High School Sage Hill High School Servite High School St. Margaret’s Episcopal School University High School Villa Park High School
California State University, Fullerton Chapman University Santa Ana College University of California, Irvine Vanguard University
USA Diving USA Gymnastics USA Volleyball
CHARITY CAREIn Fiscal Year (FY) 2012, HOI physicians and staff provided charity care to the underserved in our communities worth more than $800,000. HOI staff members are also engaged as volunteers in numerous community-strengthening capacities. Activities ranged from the chief operating officer’s volunteer work at Taller San Jose, which provides unemployed, unskilled young adults who have gotten off track in life with the job training and life skills necessary to support themselves and their families; to staff members involved in neighborhood watch, senior centers and youth organizations. HOI personnel have served as staff for a summer camp for teens at risk; traveled to Haiti and Kenya to provide medical care; gone to New Orleans for rebuilding projects; and organized Arthritis Foundation fundraising.
On September 28, 2012, HOI celebrated another first when HOI CEO Carlos Prietto, MD, provided the first orthopedic eConsult to the Share Our Selves (SOS) Wellness Center in Santa Ana. The clinic reaches the underserved community that has few to no options for affordable health care. The clinic focuses on improving access to care, eliminating health disparities, and reducing the number of emergency department visits for primary care needs. Care is free and includes health screenings for uninsured students and their families at the charter school El Sol Science and Arts Academy in Santa Ana. The eConsult marked the beginning of our commitment to providing orthopedic services to the SOS-El Sol Wellness Center’s families.
HOI medical and administrative leaders intend to broaden inroads they have made into improving the health of Orange County’s most vulnerable populations.
“HOAG ORTHOPEDIC INSTITUTE HAS EMBRACED THE CHANGES RESHAPING
THE HEALTHCARE INDUSTRY. WE HAVE ASSEMBLED SOME OF THE NATION’S
BEST ORTHOPEDIC SURGEONS TO WORK IN A COLLEGIAL ENVIRONMENT,
GUIDED BY A COHESIVE LEADERSHIP TEAM WITH A SHARED VISION TO BE
ONE OF THE NATION’S LEADING PROVIDERS OF SPECIALTY ORTHOPEDIC CARE.”
CARLOS A. PRIETTO, MD, CHIEF EXECUTIVE OFFICER, HOAG ORTHOPEDIC INSTITUTE

6 | H O A G O RT H O P E D I C I N S T I T U T E
RESEARCH AND EDUCATION
Orthopaedics Education and Research Institute (OERI)
In late 2012 Hoag Orthopedic Institute established an affiliation agreement with the Orthopaedics Education and Research Institute (OERI), a non-profit organization (501c3) to improve the quality of life for patients with musculoskeletal disease. OERI is actively involved in medical research, teaming with innovators to develop new orthopedic treatment modalities. Monthly OERI educational conferences on joint replacements are now held at HOI. Through OERI, Michael J. Patzakis, MD, former chair of the Department of Orthopaedic Surgery at the University of Southern California (USC) Keck School of Medicine, serves as HOI’s Medical Director of Research and Education.
Fellowship Program
As surgical techniques and procedures have become more complex, orthopedic surgeons have benefitted from more advanced training than what most orthopedic surgical residency training programs can cover in a finite amount of time. And because orthopedics is such a diverse specialty, many surgeons seek to complete specialized, sub-specialty fellowship training after residency training.
Responding to this need, HOI initiated an Orthopedic Surgery Fellowship Program in 2012. Several of HOI’s orthopedic surgeons direct the annual fellowship in joint replacement and arthritis surgery. The fellows experience a high volume of surgical procedures, including new techniques in primary hip and knee replacement as well as complex revision and reconstructive procedures. Fellowships in other orthopedic specialties, including orthopedic research, spinal reconstruction and sports medicine, are anticipated in the near future. In addition, a clinical research fellow will join HOI in 2013.
INTRODUCTION CONTINUED
“THE ORTHOPAEDICS EDUCATION AND RESEARCH INSTITUTE HEIGHTENS THE LEVEL OF CARE AT HOI AND IN ORTHOPEDICS AT LARGE. HOI WILL BE TRAINING THE NEXT GENERATION OF SURGEONS, EVALUATING CLINICAL PATHWAYS AND OUTCOMES, INCREASING OUR UNDERSTANDING OF ANATOMY, IMPROVING HEALTH, AND TAKING A LEADERSHIP POSITION IN EMERGING TECHNOLOGIES AND TREATMENT MODALITIES.”
MICHAEL J. PATZAKIS, MD, EMERITUS PROFESSOR, DEPARTMENT OF ORTHOPAEDICS, KECK SCHOOL OF MEDICINE OF USC, HOI MEDICAL DIRECTOR OF RESEARCH AND EDUCATION

2012 O U T C O M E S R E P O RT | 7
Annual Orthopedic Nursing Symposiums
HOI’s nursing education team, physicians, marketing team, audio-visual department, various supporting departments and volunteers collaborate on this event annually. It is for the educational benefit of orthopedic nurses, certified nursing assistants, physical therapists, occupational therapists, rehabilitation staff, orthopedic technicians/cast technicians, peri-operative staff and clinicians working in an orthopedic setting and interested in learning more about topics related to musculoskeletal issues. This symposium offers specialty continuing education credit that supports the Orthopedic Rehabilitation Education efforts as well as contact hours designated by the Orthopaedic Nurse Certification Board. This year, HOI medical staff and other leading physicians from the region gave attendees in-depth insight into musculoskeletal conditions and cutting edge orthopedic care in the following presentations:
• Fundamentals of an Orthopedic/Musculoskeletal Nursing Assessment
• Minimally Invasive Total Knee Arthroplasty (live from OR)
• Femoral Nerve Block
• Total Shoulder Arthroplasty
• Effective Treatment Options for Osteoporosis
• Treatment Options for Spine-based Pain
The live, narrated total knee replacement surgery streamed to HOI’s auditorium. The presentation was interactive, with questions taken from the moderator. In December 2011, 133 healthcare professionals participated in the third annual symposium and in December 2012, 127 healthcare professionals from numerous areas hospitals attended the fourth annual symposium.
Student Rotations
HOI supports the growth and development of the medical community. In 2012, HOI provided clinical experience for a variety of healthcare students rotating through HOI:
• Surgical tech students from Western University and CNI Vocational College
• Physician assistants from Loma Linda University and Midwestern University
• Masters of nursing students from California State University Long Beach (CSULB) and Vanguard University
• Nursing students from Cypress and Saddleback Colleges
• Physical therapy students from Loma Linda University, CSULB and Azusa Pacific University
“AT HOI, WE BELIEVE CLINICAL EXPERIENCE UTILIZING EVIDENCE-
BASED PRACTICE IS A VITAL PART OF A CLINICIAN’S EDUCATION.
WE ENJOY PROVIDING A SUPPORTIVE ENVIRONMENT FOR CLINICAL
ROTATIONS THAT WILL BUILD COMPETENCE AND CONFIDENCE.”KANOE ALLEN, RN, MSN-CNS, PHN, ONC, CHIEF NURSING OFFICER

8 | H O A G O RT H O P E D I C I N S T I T U T E
A national movement toward more accountable care has led to the standardization of key performance measures. As an early adopter of these measures, HOI has tracked its outcomes against national benchmark data since opening its doors in November 2010. In this report, fiscal year 2012 data (October 2011 to September 2012) is presented along with fiscal year 2011 data (annualized from November 2010 to September 2011.)
HOI has invested in rigorous outcomes tracking systems and reporting to foster excellence in care, optimize outcomes and validate quality. Thus, Hoag Orthopedic Institute patients and payers have gained an unprecedented level of insight into
the community’s orthopedic care. Physicians and staff stay abreast of what has been accomplished, and what remains to be done, via distribution of performance dashboards.
The institute continues to expand its data collection efforts. As the field of outcomes assessments and national benchmarks continues to mature, HOI is well positioned to collect patients’ data and reap the benefits from this knowledge.
VALUE-BASED PURCHASINGUnder Medicare’s Hospital Value-Based Purchasing (VBP) “pay for performance” approach which began in October 2012, hospitals receive incentive payments based on how well they perform on
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Role in Value-Based Purchasing FY 2013
OUTCOMES
Lowest HCAHPS Score Additional 6%*
Discharge Information 3%
Overall Rating 3%
Pain Management 3%
Clean/Quiet 3%
Responsiveness 3%
Communication RE: Meds 3%
RN Communication 3%
MD Communication 3%
Source: American Hospital Association
Clinical Measures 70%
* The hospital’s lowest HCAHPS score has a disproportionate weight to the others—30 of the 100 HCAHPS value-based-purchasing points are based on that one measure.
Seventy percent of these scores are based upon the process of care, such as the Centers for Medicare & Medicaid Services (CMS) Surgical Care Improvement Project (SCIP) measures. The remaining 30 percent focus on patient experience metrics from HCAHPS. The pie chart below illustrates what is weighted for VBP.

2012 O U T C O M E S R E P O RT | 9
100
90
80
70
60
50
40
30
20
10
0
Source: QualityNet.org (CMS-approved website for secure communications and healthcare quality data exchange) for performance period of 07/1/2011 to 03/31/12
Hoag Orthopedic Institute
State of CA
National
73%
53% 55%
HOI Hospital’s Value-Based Purchasing Score 2013Percent (Higher is Better)
“SPECIALTY ORTHOPEDIC HOSPITALS
HAVE BETTER PATIENT OUTCOMES, AS
MEASURED BY MEDICARE ADMINISTRATIVE
DATA, THAN GENERAL HOSPITALS.”
12 Clinical Process of Care Measures and 8 Patient Experience of Care Measures, or on how much their performance improves relative to a baseline performance.
In October 2012 through the Patient Protection and Affordable Care Act, Medicare began rewarding hospitals that provide high-quality care for their patients using its new Hospital Value-Based Purchasing Program. The concept of value-based healthcare purchasing is that buyers should hold providers of health care accountable for both cost and quality of care.
VBP brings together statistics on the quality of health care, including patient outcomes and health status, with data on the dollar outlays going towards health. It focuses on managing the use of the healthcare system to reduce inappropriate care and to identify and reward the best-performing providers. This strategy contrasts with more limited efforts to negotiate price discounts, which reduce costs but do little to ensure that quality of care is improved.
In a value-based purchasing system, employers and other purchasers contract selectively with plans or provider organizations based on demonstrated performance. In this manner, the best performing plans and providers are rewarded with a greater volume of patients.
Source: Journal of Bone and Joint Surgery August 2007
In October 2012 all hospitals began receiving their first VBP scores. HOI was well above the state and national scores.
1 0 | H O A G O RT H O P E D I C I N S T I T U T E
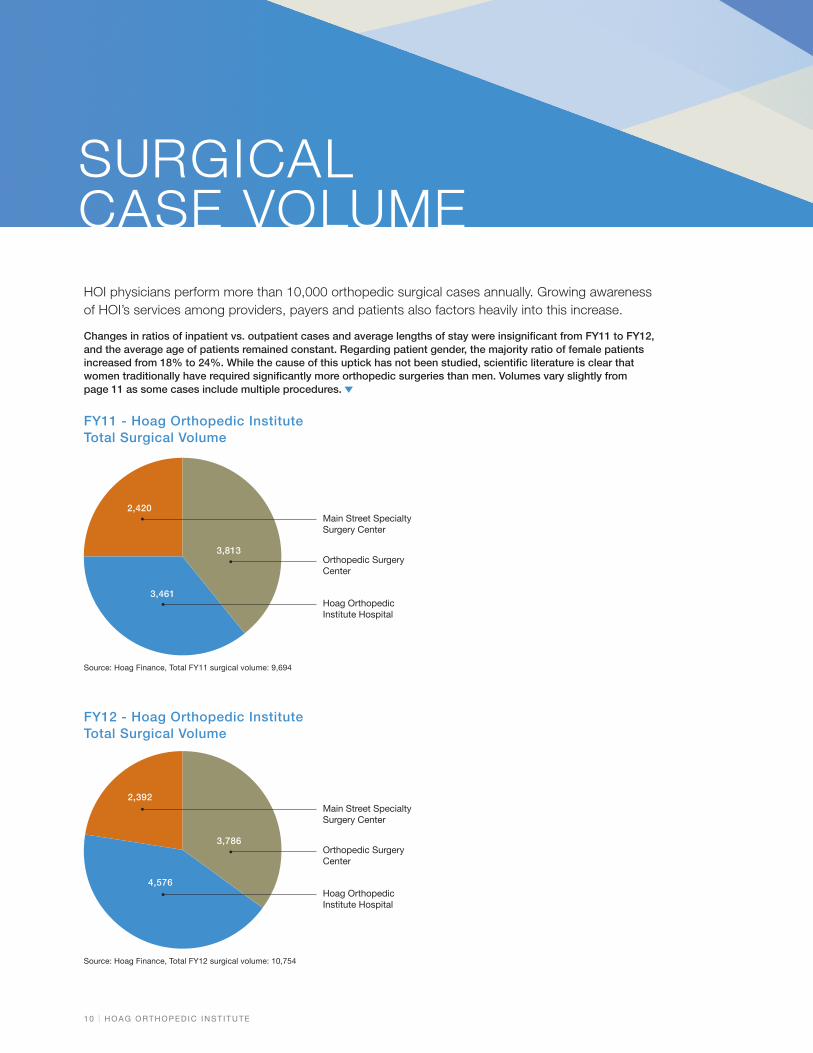
HOI physicians perform more than 10,000 orthopedic surgical cases annually. Growing awareness of HOI’s services among providers, payers and patients also factors heavily into this increase.
Changes in ratios of inpatient vs. outpatient cases and average lengths of stay were insignificant from FY11 to FY12, and the average age of patients remained constant. Regarding patient gender, the majority ratio of female patients increased from 18% to 24%. While the cause of this uptick has not been studied, scientific literature is clear that women traditionally have required significantly more orthopedic surgeries than men. Volumes vary slightly from page 11 as some cases include multiple procedures.
SURGICAL CASE VOLUME
Source: Hoag Finance, Total FY11 surgical volume: 9,694
FY11 - Hoag Orthopedic Institute Total Surgical Volume
2,420
3,813
3,461
Main Street Specialty Surgery Center
Orthopedic Surgery Center
Hoag Orthopedic Institute Hospital
Source: Hoag Finance, Total FY12 surgical volume: 10,754
FY12 - Hoag Orthopedic Institute Total Surgical Volume
2,392
4,576
3,786
Main Street Specialty Surgery Center
Orthopedic Surgery Center
Hoag Orthopedic Institute Hospital

2012 O U T C O M E S R E P O RT | 1 1
PATIENTS UNDERGOING ELECTIVE ORTHOPEDIC
SURGERIES AT HIGH-VOLUME, REGIONAL
HOSPITALS HAVE BETTER SURGICAL OUTCOMES
AND FEWER COMPLICATIONS THAN THOSE
HAVING SURGERIES AT LOCAL HOSPITALS.
CASES AVERAGE AGE 2011 2012 2011 2012
PROCEDURES 2011
2012
2011
2012
MA
LES
FEM
ALE
S
MA
LES
FEM
ALE
S
INPA
TIE
NT
S
OU
TPA
TIE
NT
S
INPA
TIE
NT
S
OU
TPA
TIE
NT
S
HIP
Hip Replacement 839 1,088 66.3 66.3 385 454 475 613 837 2 1,088 ...
Hip Revision 112 112 66.0 67.8 46 66 41 71 110 2 112 ...
KNEE
Knee Replacement 1,160 1,488 67.7 67.6 494 666 624 864 1,160 ... 1,488 ...
Knee Revision 79 105 66.7 66.1 46 33 42 63 77 2 104 1
SPINE
Cervical Fusion 141 186 55.0 53.2 79 62 93 93 141 ... 186 ...
Thoracic Fusion 11 10 60.1 74.4 5 6 4 6 11 ... 10 ...
Lumbosacral Fusion 178 296 62.4 62.8 84 94 142 154 174 4 293 3
Disc Excision 153 217 48.2 49.0 96 57 136 81 29 124 46 171
Kyphoplasty 85 120 77.7 76.8 27 58 30 90 85 120
Other 64 80 64.5 62.3 41 23 44 36 42 22 41 39
FRACTURE CARE
Hip 61 140 76.2 77.9 16 45 44 96 61 ... 139 1
Knee 12 14 70.2 71.4 2 10 5 9 10 2 12 2
Foot Ankle 29 53 51.0 49.7 9 20 20 33 14 15 22 31
Hand Upper Extremity 44 38 54.2 57.2 19 25 16 22 8 36 11 27
Shoulder 29 50 56.3 60.6 12 17 20 30 13 16 18 32
Other 28 51 54.0 48.5 9 19 28 23 25 3 39 12
OTHER SURGICAL
Foot Ankle 39 41 55.1 56.6 14 25 18 23 6 33 10 31
Hand Upper Extremity 20 28 56.7 62.0 9 11 15 13 2 18 4 24
Hip 31 30 43.7 55.6 19 12 15 15 10 21 10 20
Knee 74 113 54.6 51.6 36 38 69 44 27 47 28 85
Other 104 132 55.5 56.7 52 52 74 58 55 49 51 81
Shoulder 135 143 64.3 63.8 70 65 75 68 90 45 88 55
Other Medical 72 103 64.0 63.6 33 39 39 64 38 34 49 54
GRAND TOTAL 3,500 4,638 64.2 64.3 1,603 1,897 2,069 2,569 2,940 560 3,849 789
Hoag Orthopedic Institute Hospital Procedural Volume Overview
Source: FY12 Hoag Finance
Source: 2011 Annual Meeting of the American Academy of Orthopaedic Surgeons (AAOS).
1 2 | H O A G O RT H O P E D I C I N S T I T U T E
Source: Hoag Finance
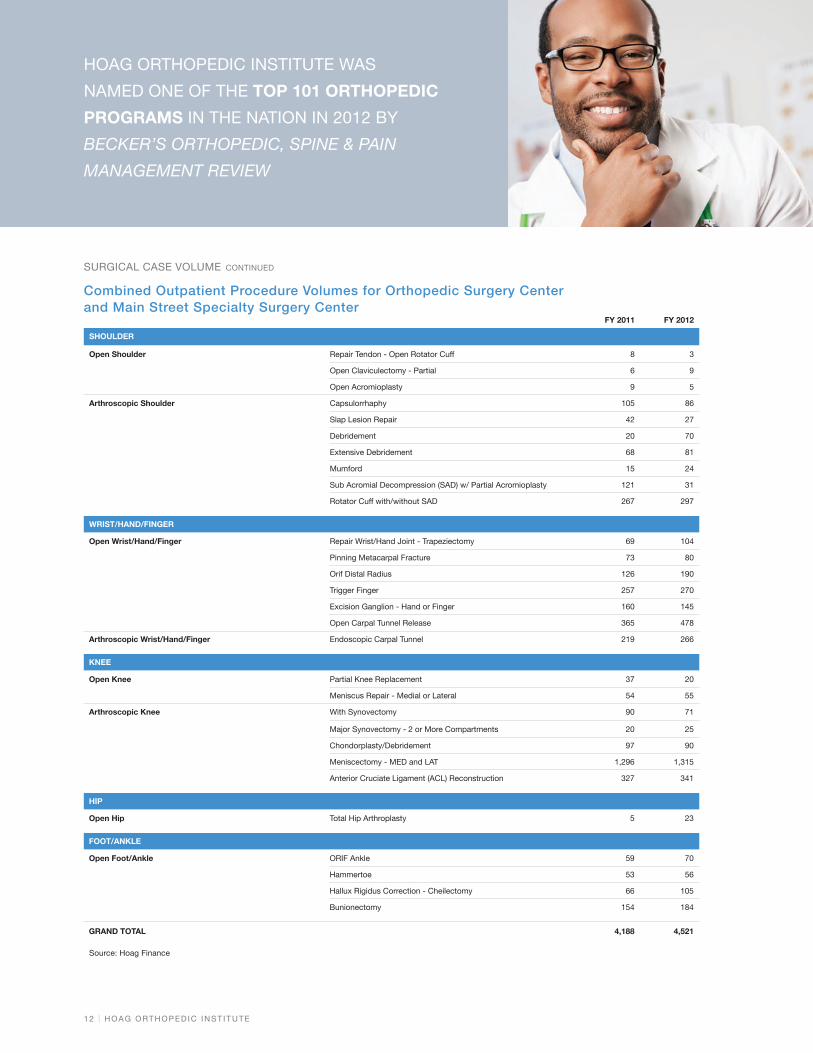
SURGICAL CASE VOLUME CONTINUED
HOAG ORTHOPEDIC INSTITUTE WAS
NAMED ONE OF THE TOP 101 ORTHOPEDIC
PROGRAMS IN THE NATION IN 2012 BY
BECKER’S ORTHOPEDIC, SPINE & PAIN
MANAGEMENT REVIEW
Combined Outpatient Procedure Volumes for Orthopedic Surgery Center and Main Street Specialty Surgery Center
FY 2011 FY 2012
SHOULDER
Open Shoulder Repair Tendon - Open Rotator Cuff 8 3
Open Claviculectomy - Partial 6 9
Open Acromioplasty 9 5
Arthroscopic Shoulder Capsulorrhaphy 105 86
Slap Lesion Repair 42 27
Debridement 20 70
Extensive Debridement 68 81
Mumford 15 24
Sub Acromial Decompression (SAD) w/ Partial Acromioplasty 121 31
Rotator Cuff with/without SAD 267 297
WRIST/HAND/FINGER
Open Wrist/Hand/Finger Repair Wrist/Hand Joint - Trapeziectomy 69 104
Pinning Metacarpal Fracture 73 80
Orif Distal Radius 126 190
Trigger Finger 257 270
Excision Ganglion - Hand or Finger 160 145
Open Carpal Tunnel Release 365 478
Arthroscopic Wrist/Hand/Finger Endoscopic Carpal Tunnel 219 266
KNEE
Open Knee Partial Knee Replacement 37 20
Meniscus Repair - Medial or Lateral 54 55
Arthroscopic Knee With Synovectomy 90 71
Major Synovectomy - 2 or More Compartments 20 25
Chondorplasty/Debridement 97 90
Meniscectomy - MED and LAT 1,296 1,315
Anterior Cruciate Ligament (ACL) Reconstruction 327 341
HIP
Open Hip Total Hip Arthroplasty 5 23
FOOT/ANKLE
Open Foot/Ankle ORIF Ankle 59 70
Hammertoe 53 56
Hallux Rigidus Correction - Cheilectomy 66 105
Bunionectomy 154 184
GRAND TOTAL 4,188 4,521

2012 O U T C O M E S R E P O RT | 1 3
READMISSION RATE Readmissions are often traumatic and disabling experiences for patients, as well as expensive. The Centers for Medicare & Medicaid Services (CMS) reports that readmissions cost the Medicare program $17.5 billion in inpatient spending, with nearly one in five Medicare patients returning to the hospital within a month of discharge for all types of hospitalizations.
Readmission within 30 days can be greatly influenced by hospital care and the initial transition to outpatient care. CMS has targeted readmission rates as a way to reduce the increasing cost of medical care. In September 2012, CMS announced three new outcomes measures in its Inpatient Quality Reporting (IQR) program. CMS plans to report data for the following measures on the Hospital Compare website in 2013:
• Hospital-Wide All-Cause Unplanned Readmission Measure (HWR)
• Hospital-Level 30-Day All-Cause Risk-Standardized Readmission Rate Following Elective Primary Total Hip Arthroplasty (THA) and/or Total Knee Arthroplasty (TKA) – THA/TKA Readmission
• Hospital-Level Risk-Standardized Complication Rate Following Elective Primary Total Hip Arthroplasty and/or Total Knee Arthroplasty
Hoag Orthopedic Institute has achieved readmission rates significantly below the national and regional averages.
25
20
15
10
5
0
Source: Hoag Orthopedic Institute, n= 1,553; Regional, n= 363,407; California, n= 761,100 Health Service Advisory Group, Q2, 2011-Q1, 2012.
Hoag Orthopedic Institute
State of CA
Regional
4.1%
19.1%20.4%
30 Day Readmission RatePercent (Lower is Better)

1 4 | H O A G O RT H O P E D I C I N S T I T U T E
INFECTION PREVENTIONNationally, the cost of a hospital stay for a person without an infection acquired in the hospital is, on average, $9,377, but treating an infection acquired in the hospital costs about $43,000 more than the original treatment cost. At HOI, a collaborative team aggressively pursues low infection rates through adherence to Centers for Disease Control (CDC) guidelines regarding hand hygiene, antibiotic stewardship and standard precautions that are instrumental in preventing infection and improving patients outcomes.
HOI INFECTION PREVENTION MEASURESHOI is committed to pursuing excellence in utilizing best practices and the most up-to-date evidence-based standards to prevent surgical site infections and other surgical complications. Some of the best practices utilized for surgical patients at HOI include:
• Educating patients on bathing preoperatively with chlorhexidine products that reduce bacterial colonization of the skin and have demonstrated decreasing surgical site infection risk
• Conducting preoperative screening of surgical patients for Methicillin-Resistant Staphylococcus Aureus (MRSA). MRSA carriers are identified by swabbing the nares (nostrils), providing options to the surgeon to decrease the risk of infection from MRSA. This may include adjusting the choice of antibiotics before surgery to prevent
infection, isolation protocols to decrease the opportunity for transmission, and treatment to decolonize the patient before surgery when appropriate.
• Testing urine preoperatively to identify potential kidney complications or early infections
• Tailoring choice and time of antibiotics to each patient’s surgery and needs to prevent infection
• Warming patients throughout the operative process to maintain normal temperature as studies have shown this is a significant contributor to decreasing surgical site infections
Best practices were developed based on guidelines from medical organizations such as CDC, Society of Healthcare Epidemiologists Association, Association of Professionals in Infection Control & Epidemiology, Association of Perioperative Registered Nurses, Infectious Diseases Society of America and American Hospital Association.
METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS (MRSA)All patients undergoing elective inpatient knee and hip arthroplasties and spinal surgery are screened for MRSA colonization, which portends an increased risk for Surgical Site Infections (SSIs). To prevent the transmission of MRSA among hospital patients, the following screening and treatment algorithm guides clinicians in the care of all patients scheduled for joint replacement or spinal surgery

2012 O U T C O M E S R E P O RT | 1 5
NAMED BY U.S. NEWS & WORLD REPORT AS
ONE OF THE TOP ORTHOPEDIC HOSPITALS IN
THE NATION IN 2012
Preoperative MRSA Screening Protocol for Inpatient Elective Surgery for Total Hip and Knee Replacement
Culture results Negative nasal culture (-MRSA)
Admission to hospital
Preop holding area applies Chlorhexidine Gluconate
to surgical site
Surgery
Negative cultures
Nasal culture prior to discharge
Clearance to proceed with surgery from
surgeon and/or infectious disease specialist
Night prior to surgery, apply Chlorhexidine
Gluconate cloth to body after showering
Mupiricin ointment to nasal vestibules
twice daily
Chlorhexidine Gluconate total body wash or cloth once daily for five days
Morning of surgery, apply Chlorhexidine
Gluconate cloth to body
Positive nasal culture (+MRSA)
Re-culture nares, axilla, groin and any open wounds
after 48 hours of last Mupiricin and Chlorhexidine
Gluconate wash
Recommended referral to an infectious disease
specialist for more intensive decolonization
Positive culture
Nasal culture (Within 30 days of
surgery date)
Source: U.S. News & World Report July 2012

1 6 | H O A G O RT H O P E D I C I N S T I T U T E
CATHETER ASSOCIATED URINARY TRACT INFECTIONS (CAUTI)Urinary tract infections are the most common type of healthcare-associated infections, accounting for more than 30% of healthcare-associated infections reported in acute care hospitals. Care strategies enabling HOI to prevent CAUTI and achieve zero CAUTI incidences in FY12 include:
• Insert catheters only for appropriate indications
• Leave catheters in place only as long as needed
• Following aseptic insertion, maintain a closed drainage system
• Maintain unobstructed urine flow
• Practice hand hygiene and standard (or appropriate isolation) precautions according to CDC Healthcare Infection Control Practices Advisory Committee (HICPAC) guidelines
In FY12, HOI achieved 100% success with zero CAUTIs occurring.
SURGICAL SITE INFECTIONS A surgical site infection (SSI) is defined as an infection that develops within 30 days after an operation or within one year if an implant was placed and the infection appears to be related to the surgery. National data shows that post-surgical wound infections more than double a patient’s hospital costs. A hospital-wide protocol has been implemented at HOI to prevent and monitor for SSIs.
CMS considers surgical site infections as “Never Events,” with tolerance for SSIs at 0%. HOI has embraced prevention of hospital-acquired SSIs/complications as an opportunity to improve the quality and safety of patient care. This proactive approach is reflected in HOI’s low infection rates and chronological improvement.
1.2
1.0
0.8
0.6
0.4
0.2
0
1.01%
0.42%
Overall Surgical Site Infection RatePercent (Lower is Better)
Hoag Orthopedic Institute FY11
Hoag Orthopedic Institute FY12
Source: Hoag Orthopedic Institute, Infection Prevention Dashboard Summary Report FY12
0.6
0.5
0.4
0.3
0.2
0.1
0
0.56%
0.00%
Catheter Associated Urinary Tract Infection Rates (CAUTI)Percent (Lower is Better)
Hoag Orthopedic Institute FY11
Hoag Orthopedic Institute FY12
Source: Hoag Orthopedic Institute, Infection Prevention Dashboard Summary Report FY12
INFECTION PREVENTION CONTINUED
“HAVING SURVEILLANCE METRICS TO MONITOR EVIDENCE-BASED
INFECTION PREVENTION PRACTICES TAKES PATIENT SAFETY TO
THE NEXT LEVEL.”
PHILIP ROBINSON, MD, MEDICAL DIRECTOR OF INFECTION CONTROL

2012 O U T C O M E S R E P O RT | 1 7
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0
0.38%
0.99%
0.25%
1.44%
Surgical Site Infection Rate for Joint ProsthesisPercent (Lower is Better)
Source: Hoag Orthopedic Institute, Infection Prevention Dashboard Summary Report FY12; The Association for Professionals in Infection Control and Epidemiology (APIC), Guide to the Elimination of Orthopedic Surgical Site Infections, Dec. 2009
Hoag Orthopedic Institute Knee SSI Rate FY12
CDC/NHSN Benchmark for Knee SSI
Hoag Orthopedic Institute Hip SSI Rate FY12
CDC/NHSN Benchmark for Hip SSI
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0
0.90%
1.50%
Surgical Site Infection Rate for Spine SurgeryPercent (Lower is Better)
Source: Hoag Orthopedic Institute, Infection Prevention Dashboard Summary Report FY12; The Association for Professionals in Infection Control and Epidemiology (APIC), Guide to the Elimination of Orthopedic Surgical Site Infections, Dec. 2009
Hoag Orthopedic Institute Spine SSI Rate FY12
CDC/NHSN Benchmark for Spine SSI
HOAG ORTHOPEDIC INSTITUTE IS ONE OF THE FIRST
THREE HOSPITALS SELECTED BY THE CALIFORNIA
JOINT REPLACEMENT REGISTRY TO DEVELOP
A STATEWIDE REGISTRY DATABASE TRACKING
LONG-TERM PATIENT OUTCOMES IN PATIENTS
UNDERGOING JOINT REPLACEMENT SURGERY.

1 8 | H O A G O RT H O P E D I C I N S T I T U T E
SURGICAL CARE IMPROVEMENT PROJECT (SCIP) SCIP measures are the result of a national quality partnership of 10 steering entities, including the Joint Commission and CMS, dedicated to saving lives and improving surgical care through complication reduction. SCIP’s process-of-care data demonstrate how consistently recommended care was provided to adult patients at participating hospitals. Only “Overall Appropriateness of Surgical Care,” summarizing whether patients received all of the recommended treatments, is not shown as a national comparison has not been available for this composite score.
SCIP protocols for orthopedic care are a major focus of HOI’s quality initiatives. To deliver the best possible care to patients undergoing procedures known to have inherent risks, HOI utilizes the SCIP “Bundle of Care.” This bundle consists of a set of evidence-based interventions in areas with potential for great harm and high cost throughout the episode of care.
SCIP MEASURES• Prophylactic antibiotic received within one hour
prior to surgical incision
• Appropriate prophylactic antibiotic selected for surgical patients
• Prophylactic antibiotic discontinued within 24 hours after surgery end time
• Surgery patients on beta blocker therapy prior to arrival who received a beta-blocker during the perioperative period
• Surgery patients with recommended venous thromboembolism prophylaxis ordered
• Surgery patients who received appropriate venous thromboembolism prophylaxis within 24 hours prior to surgery to 24 hours after surgery
• Overall appropriateness of surgical care
INFECTION PREVENTION CONTINUED
HOI HAS ACHIEVED 100% COMPLIANCE ON
THE FOLLOWING SCIP INDICATORS SINCE
DATA COLLECTION BEGAN IN JULY 2011:
• ANTIBIOTIC SELECTION
• APPROPRIATE HAIR REMOVAL
• PERIOPERATIVE TEMPERATURE MANAGEMENT
Overall Appropriateness of Surgical Care Percent (Higher is Better)
100
80
60
40
20
0
Q4 FY
11
Q1 FY
12
Q2 FY
12
Q3 FY
12
Q4 FY
12
Overa
ll FY12
93%96% 95% 97% 96% 96%
Source: HOI’s MIDAS Comparative Database

2012 O U T C O M E S R E P O RT | 1 9
Studies have demonstrated that timely antibiotic administration is best practice because the risk of infection increases progressively with greater time intervals between administration and skin incision.
Optimal use of prophylactic antibiotics involves use of appropriate agents; proper dosing, route of administration, timing, and duration; and intraoperative dosing when appropriate. HOI has had perfect performance on this measure for five consecutive quarters.
Unnecessary use of antibiotics can contribute to the spread of drug-resistant infections that are difficult to treat.
Studies have shown that abrupt discontinuation of beta blockers during the perioperative period in patients who were on chronic beta blocker therapy prior to surgery led to increased mortality during the intraoperative and postoperative periods.
Antibiotics within 1 Hour of IncisionPercent (Higher is Better)
100
80
60
40
20
0
99.6% 99% 98% 98%
Source: Hoag Orthopedic Institute Midas Reports; Comparative data from U.S. Department of Health and Human Services - HHS.gov, updated October 11, 2012
100
80
60
40
20
0
Antibiotics Discontinued within 24 HoursPercent (Higher is Better)
98% 99%96% 97%
Source: Hoag Orthopedic Institute Midas Reports; Comparative data from U.S. Department of Health and Human Services - HHS.gov, updated October 11, 2012
100
80
60
40
20
0
96%91%
96% 96%
Beta Blocker AdministrationPercent (Higher is Better)
Source: Hoag Orthopedic Institute Midas Reports; Comparative data from U.S. Department of Health and Human Services - HHS.gov, updated October 11, 2012
100
80
60
40
20
0
100% 100%95% 96%
Antibiotic SelectionPercent (Higher is Better)
Source: Hoag Orthopedic Institute Midas Reports; Comparative data from U.S. Department of Health and Human Services - HHS.gov, updated October 11, 2012
VTE is one of the most common postoperative complications and prophylaxis is the most effective strategy to reduce morbidity and mortality. Studies have shown that appropriately used thromboprophylaxis may help to prevent blood clots from forming after surgery.
100
80
60
40
20
0
Venous Thromboembolism (VTE) Prophylaxis OrderedPercent (Higher is Better)
99% 100%97%
98%
Source: Hoag Orthopedic Institute Midas Reports; Comparative data from U.S. Department of Health and Human Services - HHS.gov, updated October 11, 2012
For maximum effectiveness, VTE prophylaxis needs to be started at the right time with the right modality.
100
80
60
40
20
0
Venous Thromboembolism (VTE) TimingPercent (Higher is Better)
99% 99%96% 97%
Source: Hoag Orthopedic Institute Midas Reports; Comparative data from U.S. Department of Health and Human Services - HHS.gov, updated October 11, 2012
Hoag Orthopedic Institute FY12 Hoag Orthopedic Institute on www.calhospitalcompare.org
Average for all reporting hospitals in California
Average for all reporting hospitals in the United States

2 0 | H O A G O RT H O P E D I C I N S T I T U T E
LENGTH OF STAYReducing hospital lengths of stay (LOS) decreases the likelihood of hospital-acquired complications, thereby reducing healthcare costs. For many patients, appropriately reduced LOS means they are able to recover in the comfort of their home and recuperate in a more restful environment.
Although hospitals have lowered their average lengths of stay in the past two decades, overall LOS can be decreased for many patients through clinical best practices and discharge planning. Many delays can be traced to medical complications; others involve waiting for equipment, test results or a clinical decision, and can be rectified with coordination of resources throughout hospitalization.
HOI has taken several steps to ensure safe and expedient lengths of stay. When the decision to proceed with surgery is made, a nurse navigator contacts the patient prior to admission and addresses any issues regarding discharge planning. Pre-op patient orientation classes set patient expectations and help smooth the discharge process. Nurse navigators follow patients across the continuum of care, focusing on education, provider collaboration and development of an integrated plan of care. The navigator will work with each patient’s needs and troubleshoot problems should they arise.
Additional initiatives affecting lengths of stay include:
Impact of Rapid Mobilization on Length of Stay for Postoperative Joint Replacement Patients
Overall length of hospital stay following total joint replacement can be reduced through rapid mobilization, according to a study presented at the 2012 American Academy of Orthopaedic Surgeons. References addressing change in postoperative activity on day one date back to World War II. Furthermore, as the nursing textbook by Lewis, Heitkemper and Dirksen, 2004, Study Guide for Medical-Surgical Nursing, states, “Early ambulation is the most significant general nursing measure to prevent postoperative complications.”
Commonly accepted postoperative benefits of early ambulation implemented at HOI include a decrease in venous stasis, stimulation of circulation, prevention of deep venous thrombosis/pulmonary embolism, increases in muscle tone, coordination and independence, and improved gastrointestinal, genitourinary and pulmonary functions.
iCarePassport™ – Patient Education
HOI’s interactive patient system iCarePassport is intended to enhance the entire continuum of the patients’ experience as well as positively impact length of stay and other measurable outcomes. The iCarePassport gives patients web access to an online library of personalized health education and information around the clock, including:
• Physician and hospital organization information
• Health education based on specific procedure and disease
• Maps and directions from the patient’s home to the hospital
• Alerts and reminders (based on procedure or surgery date) for pre-admission and post-discharge events
HOI’s average lengths of stay, shown below, are significantly lower than the national average.
INFECTION PREVENTION CONTINUED
4.3
5
4
3
2
1
0
Source: Hoag Finance, Oct 2011-Aug 2012. n = 3,483; Becker’s Hospital Review, July 2012
Hoag Orthopedic Institute
National
Length of Stay Days (Lower is Better)
2.5

2012 O U T C O M E S R E P O RT | 2 1
PATIENT EXPERIENCE Achieving consistent patient-centered excellence by enhancing the clinical, physical and emotional aspects of the patients’ journey is an ongoing mandate for the entire HOI family. To that end, the institute consistently collects and closely analyzes patient feedback.
The first standardized patient experience hospital survey, the Hospital Consumer Assessment of Health Providers and Systems Survey (HCAHPS), began in 2006 with results shown at www.hospitalcompare.hhs.gov. HCAHPS provides national standards for collecting and reporting on the patient experience and enables consumers to make informed hospital comparisons on national, regional and local levels. As reported in the New England Journal of Medicine (October 30, 2008), quality of care is significantly better in hospitals that performed better on HCAHPS.
HCAHPS OVERALL ASSESSMENTMost hospitals’ HCAHPS score reflects the percentile of most favorable responses to that survey question. In these key categories measuring patients’ perspectives, Hoag Orthopedic Institute outperformed at least 98 percent of hospitals surveyed.
100
80
60
40
20
0
Source: HCAHPS and Press Ganey (surveys returned), July-September 2012. n= 1,703 hospitals
Recommend the Hospital
Overall Hospital Rating
Patient Experience Percentile (Higher is Better)
99% 98%
ENHANCING THE PATIENT EXPERIENCE THROUGH COMMUNICATIONPreoperative education empowers patients by increasing knowledge about care-related issues and lessening anxiety. HOI also views pre-admission education as an opportunity to decrease length of stay, decrease variable costs, and improve patient, staff and physician satisfaction. Each patient scheduled for orthopedic surgery is encouraged to participate in a class presented by an orthopedic specialty nurse.
Nurse navigators provide emotional and educational support to the patient throughout their care. They phone every patient prior to surgery to discuss the patient’s history, medications and expectations for their surgery. They connect the dots for the patient and provide valuable information to make sure the patient is prepared for his or her surgery and discharge.
All pre-op nurses perform chart review and four clerical coordinators communicate with the physician offices to make sure patients’ charts are complete and patients are ready for surgery. These points of communication have helped HOI to achieve a less than 1 percent day-of-surgery cancellation rate.

2 2 | H O A G O RT H O P E D I C I N S T I T U T E
The percentage for HOI is shown here in comparison to the average score of all Press Ganey reporting hospitals across the nation.
Source: Press Ganey surveys, May-July 2012
100
90
80
70
60
50
40
30
20
10
0
HCAHPS Survey Responses Percent (Higher is Better)
Hoag Orthopedic Institute
Press Ganey Database (1,687 Hospitals)
Rate t
he
Hos
pital
Recom
men
d
t
he H
ospita
l
Comm
unica
tion
w
ith N
urse
s
Respon
se o
f the
Hos
pital S
taff
Comm
unica
tion
with
Doc
tors
Hos
pital
Enviro
nmen
t
P
ain
Man
agem
ent
Comm
unica
tion
ab
out M
edici
nes
Discha
rge
Info
rmat
ion
PATIENT EXPERIENCE CONTINUED
HOI RANKED IN THE NATION’S TOP
1 PERCENT IN PATIENTS’ WILLINGNESS
TO RECOMMEND THE HOSPITAL, BASED
ON PRESS GANEY DATA.

2012 O U T C O M E S R E P O RT | 2 3
iCAREPASSPORT™ FOR ONGOING PATIENT ENGAGEMENTTo build relationships with patients and promote satisfaction preadmission, during hospitalization and after discharge, HOI uses iCarePassport, a breakthrough patient care and outcomes system powered by Skylight Healthcare Systems. iCarePassport’s web-based system enhances the patient experience by delivering timely and clinically relevant data.
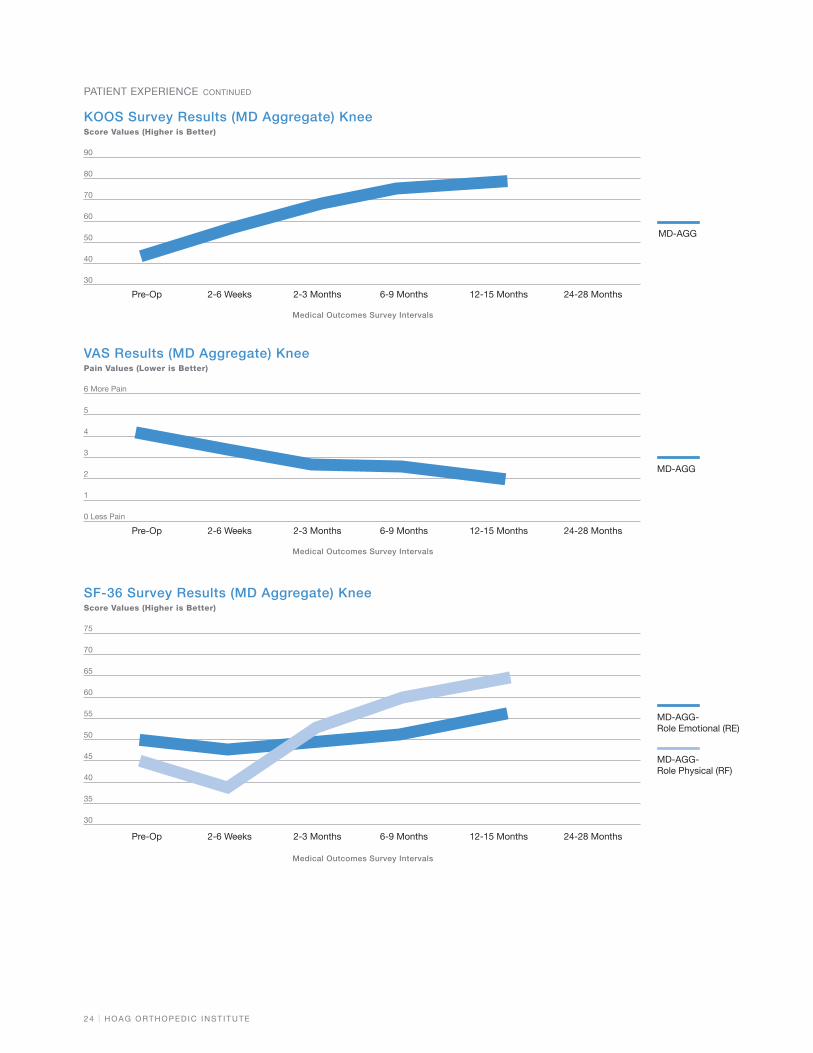
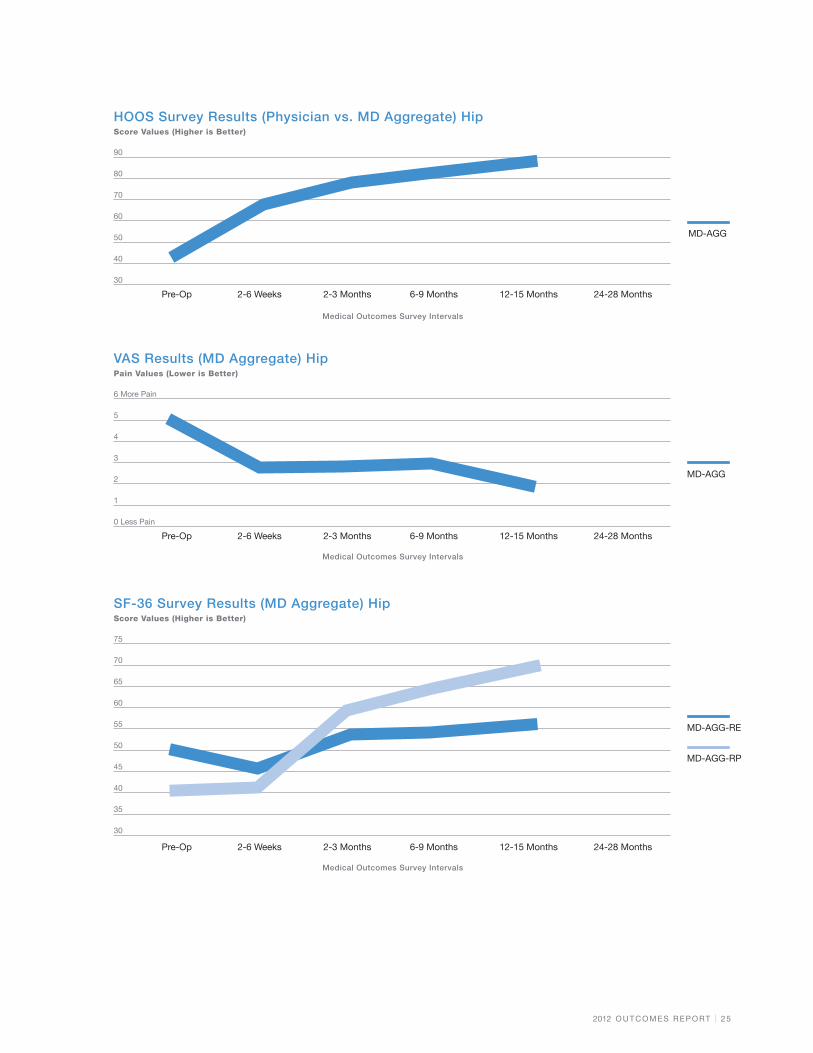
The interactive iCarePassport system allows discharged patients to report functional status securely and easily in the comfort of their homes. Since implementation, data on functional status – before surgery and then at various intervals post-surgically – has been captured as follows:
HOOS = Hip Osteoarthritis Outcome Score
The HOOS is a questionnaire used to assess the patient’s opinion about their hip and associated problems, and to evaluate symptoms and functional limitations related to the hip during a therapeutic process.
KOOS = Knee Osteoarthritis Outcome Score
The KOOS has been found reliable for the evaluation of short-term and long-term symptoms and function in subjects with knee injury and osteoarthritis. KOOS data has been validated for
several orthopedic interventions such as anterior cruciate ligament reconstruction, meniscectomy and total knee replacement. In addition, it has been used to evaluate physical therapy and nutritional supplementation.
VAS = Visual Analog Scale
The VAS is a tool widely used to measure pain intensity (from no pain to extreme pain). Each participating post-op patient is asked to indicate his/her perceived pain.
SF-36
The SF-36 is a multi-purpose, short-form, 36-question health survey. It yields a profile of functional health and well-being scores as well as psychometrically based physical and mental health summary measures and a preference-based health utility index. SF-36 has proven useful in surveys of general and specific populations, comparing the relative burden of diseases, and in differentiating the health benefits produced by a wide range of different treatments.
HOI is currently in the process of developing outcomes surveys for shoulder and spine patients.
“THE UNIQUE ADVANTAGE THAT WE GET FROM iCAREPASSPORT IS ITS
ABILITY TO DELIVER CONDITION-SPECIFIC AND TIMELY INFORMATION
TO OUR PATIENTS AND THEIR FAMILIES WHILE PROVIDING HOAG WITH
CLINICALLY RELEVANT OUTCOMES DATA.”
ALAN H. BEYER, MD, FACS, EXECUTIVE MEDICAL DIRECTOR, HOAG ORTHOPEDIC SERVICES
2 4 | H O A G O RT H O P E D I C I N S T I T U T E
6 More Pain
5
4
3
2
1
0 Less Pain
Medical Outcomes Survey Intervals
VAS Results (MD Aggregate) Knee Pain Values (Lower is Better)
Pre-Op 2-6 Weeks 2-3 Months 6-9 Months 12-15 Months
MD-AGG
24-28 Months
75
70
65
60
55
50
45
40
35
30
Medical Outcomes Survey Intervals
SF-36 Survey Results (MD Aggregate) Knee Score Values (Higher is Better)
Pre-Op 2-6 Weeks 2-3 Months 6-9 Months 12-15 Months
MD-AGG- Role Emotional (RE)
MD-AGG- Role Physical (RF)
24-28 Months
90
80
70
60
50
40
30
Medical Outcomes Survey Intervals
KOOS Survey Results (MD Aggregate) Knee Score Values (Higher is Better)
Pre-Op 2-6 Weeks 2-3 Months 6-9 Months 12-15 Months 24-28 Months
MD-AGG
PATIENT EXPERIENCE CONTINUED
2012 O U T C O M E S R E P O RT | 2 5
6 More Pain
5
4
3
2
1
0 Less Pain
Medical Outcomes Survey Intervals
VAS Results (MD Aggregate) Hip Pain Values (Lower is Better)
Pre-Op 2-6 Weeks 2-3 Months 6-9 Months 12-15 Months
MD-AGG
24-28 Months
75
70
65
60
55
50
45
40
35
30
Medical Outcomes Survey Intervals
SF-36 Survey Results (MD Aggregate) Hip Score Values (Higher is Better)
Pre-Op 2-6 Weeks 2-3 Months 6-9 Months 12-15 Months
MD-AGG-RE
MD-AGG-RP
24-28 Months
90
80
70
60
50
40
30
Medical Outcomes Survey Intervals
HOOS Survey Results (Physician vs. MD Aggregate) Hip Score Values (Higher is Better)
Pre-Op 2-6 Weeks 2-3 Months 6-9 Months 12-15 Months 24-28 Months
MD-AGG

2 6 | H O A G O RT H O P E D I C I N S T I T U T E
PERFORMANCE IMPROVEMENTTo sustain performance improvement, HOI has successfully utilized the Six Sigma DMAIC model as its framework. DMAIC stands for:
HOI
ANALYZE opportunity
IMPROVE performance
CONTROL performance
DEFINE opportunity
MEASURE performance

2012 O U T C O M E S R E P O RT | 2 7
HOI is committed to an active performance improvement (PI) program for maintaining a constant state of awareness of the systems and processes that affect patient care. This awareness is critical to identifying and preventing defects, and pinpointing opportunities for improvement. PI projects incorporate LEAN techniques, pioneered by the Toyota Motor Corporation in the manufacturing sector and increasingly accepted in the healthcare industry as the gold standard for process improvement. The following grid lists HOI’s clinical PI initiatives:
DMAIC NAME DEPARTMENTS INVOLVED BRIEF DESCRIPTION
Astromorph Study Perioperative team Raw data collection from December 1 to December 29, 2011, with gradual measured decrease in the use of intrathecal Astromorph for the purpose of decreasing side effects.
Blood Bank Multidisciplinary team - anesthesiologists, Perioperative Services, Blood Bank
Decrease frequent calls to Blood Bank for verification of blood ordered, which disrupts workflow of Blood Bank personnel.
Brace and Orthotic Control Multi-Disciplinary team - Nursing, Central HHNB Missed orders for braces and other orthotic devices. Prevention of missed orders targeted.
Delirium Care Nursing Post-op mature patients often present with delirium. Help ID condition and treat, measure by decreasing restraints.
Dementia Care Nursing Help ID post-op mature patients with unknown and history of dementia. Identify condition and treat, measure by decreasing restraints.
Femoral Nerve Block (FNB) Multidisciplinary team - PACU, floor nurse, Physical Therapy
PT and floor nursing staff were not routinely informed of one-time FNB so patients had an increase risk of falls. Sticker use began in order to identify those patients.
Hand Hygiene Multidisciplinary team - hospital wide Hand hygiene is directed to infection rates. Goal is to have 100% compliance.
HCAHPS - Medication Communication
HOI Medical Surgical Units Some patients on nursing units perceived that staff did not explain side effects of new medications administered. Goal is to increase scores 5% within two quarters.
HCAHPS - Noise Reduction HOI Medical Surgical Units Improve HCAHPS score for quietness of environment on nursing units.
Lower Dose of Intrathecal Bupivicaine Usage
Perioperative team Earlier ambulation of patient on nursing unit, increase in patient satisfaction and cost savings while gradually decreasing the amounts of intrathecal Bupivicaine used for decreased time in PACU.
Patients SpecificMedication Schedule
Interdisciplinary team - perioperative team, Nursing, Pharmacy
HOI PACU, in collaboration with HOI PRE OP/PAS, Med/Surg units and Pharmacy, identified patients who need to maintain a specific medication regimen. These patients are questioned intensely regarding their medication schedule and receive their medication on their own dosing schedule to prevent complication throughout their entire stay in HOI Hospital.
PEC HOI - Coding Multidisciplinary team - orthopedic surgeons, hospitalists, anesthesiologists, coders and revenue cycle staff
Review of coding process to capture accurate patient conditions during hospitalization.
SCIP Beta-Blocker Interdisciplinary team - perioperative team, Anesthesia
Beta-blocker administration and documentation to meet SCIP guidelines and achieve 100% compliance from random audits.
SCIP - Temperature Management
Perioperative team Correct inconsistencies found when active patient warming occurs and in how temperatures are measured and recorded.
Turnover Time - OR Operating Room HOI OR must maintain room turnovers not to exceed 25 minutes. Currently, room turnovers for joint cases have been 26 minutes while spine cases have been 22 minutes.
Volume Resuscitation Project Perioperative team Review of hypovolemia and hypotension in post-op patients that resulted in new onset of renal dysfunction. New protocols implemented to ensure renal function maintenance.

2 8 | H O A G O RT H O P E D I C I N S T I T U T E
DISTINCTIONS & INNOVATIONS
In 2011, HOI became the highest volume provider of joint replacements in California, according to data from the Office of Statewide Health Planning and Development (OSHPD)
Named in 2012 by U.S. News & World Report as one of the top orthopedic hospitals in the nation
Named as one of the top 101 orthopedic programs in the nation in 2012 by Becker’s Orthopedic, Spine & Pain Management Review
Ranked in the nation’s top 2 percent in patients’ willingness to recommend the hospital, based on Press Ganey data
Designated as a Blue Distinction Center for high-quality Knee and Hip Replacement by Anthem Blue Cross and Blue Shield of California
One of three hospitals selected by the California Joint Replacement Registry to pilot a statewide registry database for patients undergoing joint replacement surgery tracking long-term patient outcomes
Collaborated with McKesson and Aetna to create the first automated implementation of Integrated Healthcare Association’s (IHA’s) bundled payment model, designed to decrease healthcare costs by improving practices and standardizing care. This model is the first of its kind in California and one of the first in the nation. The bundling system, which began in 2012 with knee replacement surgeries and now includes hip replacement surgeries, has created a new level of accountability and transparency in medical care.
Designated as an Aetna Institute of Quality® Orthopedic Care Facility for total joint replacement and spine surgery for 2011-2012
Achieved Leadership in Energy and Environment Design (LEED) Silver Certification from the United States Green Building Council for its environmentally friendly design

2012 O U T C O M E S R E P O RT | 2 9
HOI ACHIEVED LEADERSHIP IN
ENERGY AND ENVIRONMENT DESIGN
(LEED) SILVER CERTIFICATION FROM
THE UNITED STATES GREEN BUILDING
COUNCIL FOR ITS ENVIRONMENTALLY
FRIENDLY DESIGN.
FACILITY INNOVATIONThe home of Hoag Orthopedic Institute and Hoag Hospital Irvine underwent complete revitalization before opening in November 2010. A team of administrators, physicians, nurses, designers, engineers and builders spent hundreds of hours guiding an overhaul that touched every area of the 20-year old, 244,000-square-foot facility. As a result, it was transformed to support the highest quality of care – for patients, the greater Irvine community, and the environment.
With strong communication, collaboration and decision-making by the team, the completed renovation was a major, award-winning success. In 2012, the American Society for Healthcare Engineering (ASHE) of the American Hospital Association presented the hospital with the Vista Award for Renovation. The award recognizes the importance of teamwork in creating an optimal healthcare physical environment.
“GREEN MEASURES” INITIATIVEMindful of green building practices and sustainability, the revitalization team made decisions that factored in the facility’s carbon footprint. LEED Silver certification was given based on the project’s sound ecological enhancements under the U.S. Green Building Council’s Leadership in Energy & Environmental Design certification system for new construction.
Highlights of the Irvine facility’s sustainability initiatives include:
• Invested in state-of-the-art sterilizing equipment that saves one million gallons of water per year without an impact on performance
• Reduced 90 percent of construction debris on the renovation project
• Instituted green cleaning practices
• Implemented a recycling policy
• Created preferred parking incentives for staff driving fuel-efficient vehicles
• Added bicycle stalls
• Pilot-tested materials such as sustainable flooring
Specific and achievable goals were created for a variety of ongoing sustainable initiatives, including:
• 50 percent potable water reduction
• 90 percent waste reduction
• 50 percent energy cost reduction
The revitalization project came in 5 percent under budget and three months ahead of schedule. Hoag Hospital Irvine patients ranked its environment of care above national benchmarks. Moreover, patients gave HOI high marks – 97th percentile – for cleanliness.
BEST PRACTICE STERILIZATIONHaving an impeccable sterile supply contributes significantly to preventing infection and maintaining a high level of patient safety. HOI selected a state-of-the-art Belimed sterilization system to ensure maximum patient safety, minimal resource consumption and reliability. The fully automated, high-capacity Belimed system is designed to follow the relatively new disinfectant standards to kill heat-resistant spores and is considered a best practice.
HOI’s Belimed sterilization system was selected for maximum patient safety and low resource consumption. Unlike traditional models,

3 0 | H O A G O RT H O P E D I C I N S T I T U T E
DISTINCTIONS & INNOVATIONS CONTINUED
Belimed instrument washers help conserve water. The autoclave/sterilizer system has better processing times, which allows for quicker turn around of trays. The cooling down and drying system prior to completion of the loads helps reduce cooling times and prevent the problem of “wet trays” post load (condensation in the trays) that can occur during the cooling cycle. The autoclaves are designed to take up to 30 percent more trays than traditional models. Its water chiller system facilitates using less water by as much as 90 percent (from up to 250 gallons/load to 2.5 gallons/load) by reusing condensate that is produced during the cycle and using that for the remainder of the cycle for steam and heat production.
TRAVEL PROGRAM FOR OUT-OF-AREA PATIENTSA Travel Program begun at HOI in 2011 streamlines access to knee and hip replacements and spine procedures. To date, patients from as far as Alaska, Washington, Florida and Illinois have utilized this increasingly popular program.
HOI’s Travel Program affords employers and third party payers access to care through HOI’s existing fee-for-service contracts with the major payers or a bundled, global rate that includes all providers’ services related to the procedure. It starts the day of surgery and includes post-operative rehabilitation. Reduced rates for local accommodations have been negotiated as well.
The Travel Program is attractive to patients and payers for several reasons:
• The Travel Program benefits patients from areas lacking in proven-quality providers with extensive experience in orthopedic care.
• Given that higher costs ultimately result from lower quality care, travel to a high-quality provider such as HOI Travel Program assures value.
• One bill, one check: The bundled rate covering all provider fees is easy for payers to manage. In rare instances if care is required outside of the diagnostic pathway, additional charges may apply. Knowing up front the total cost of care simplifies administrative claim work while providing cost controls.
• Because HOI contracts with all major payers, many out-of area employers can often negotiate with their insurance providers to opt to send orthopedic patients to HOI. Research demonstrates that employers are willing to adopt tactics to help improve health care while managing healthcare costs, including providing richer benefits to increase use of designated facilities, narrowing networks to feature cost-effective providers.
As a Blue Distinction Center® for Specialty Care, HOI is recognized for quality orthopedic care and among a select number of facilities nationwide approved by Blue Cross and Blue Shield to receive joint replacement Travel patients. Through the medical tourism company Healthbase, men and women from across the country insured by Blue Cross and Blue Shield receive help with travel and medical arrangements for care at HOI. Healthbase contacts HOI whenever someone who may require surgery is interested in coming to the institute. Travel expenses are reimbursed for the patient and caregiver. Covered expenses include mileage or airline tickets.
“THE BUNDLED PAYMENT TRAVEL PROGRAM HAS GROWN FROM ITS START
AT OSCOC TO HOI AND WORKS BECAUSE OF THE EXECUTIVE LEADERSHIP’S
ATTENTION TO DETAIL TO IMPROVE OVERALL OUTCOMES AND MAINTAIN
COSTS TO CREATE A PATIENT EXPERIENCE SECOND TO NONE.”
JAMES T. CAILLOUETTE, MD, SURGEON-IN-CHIEF
2012 O U T C O M E S R E P O RT | 3 1
Hoag Orthopedic Institute Leadership
Steven L. Barnett, MD Chairman, Department of Orthopedic Surgery
Alan H. Beyer, MD Medical Director
James T. Caillouette, MD Surgeon-in-Chief
Robert S. Gorab, MD Chief Medical Officer
Carlos A. Prietto, MD Chief Executive Officer
Dereesa Reid, MBA Chief Operating Officer
Terry Roth, RN, BSN, CNOR Executive Director Perioperative Services
Kanoe Allen, RN, MSN-CNS, PHN, ONC Chief Nursing Officer
Gabrielle White, RN, CASC Executive Director Ambulatory Services & Network Development
LEADERSHIP & MEDICAL STAFF
Orthopedic Surgery
Bruce M. Albert, MDGerald J. Alexander, MDLucas J. Bader, MDRobert A. Baird, MDLawrence S. Barnett, MDSteven A. Becker, MDRobert J. Bielen, MDGregory D. Carlson, MDJack Chen, MDYing Chi, MDJun Chino, MDJohn F. Cook, MDJeffrey E. Deckey, MDSteven C. Dennis, MDShaunak S. Desai, MDPaul T. Dinh, MDDavid J. Downs, MDDaniel P. Duggan, DOHerbert C. Eidt, MDPayam Farjoodi, MDScott P. Fischer, MDMichael J. Fitzpatrick, MDScott K. Forman, MDSteven H. Gausewitz, MDDavid S. Gazzaniga, MD
Andrew P. Gerken, MDTimothy W. Gibson, MDJoseph S. Gondusky, MDMichael L. Gordon, MDScott M. Graham, MDBradley S. Greenbaum, MDRobert C. Grumet, MDMark N. Halikis, MDTze C. Ip, MDJason J. Jancosko, DONimish R. Kadakia, MDJohn P. Kelly, MDZafar S. Khan, MDDavid H. Kim, MDWarren G. Kramer III, MDRyan S. Labovitch, MDRichard S. Lee, MDJoseph G. Mayo, MDStephen A. Mikulak, MDHamid R. Mir, MDAnthony R. Mork, MDRam Mudiyam, MDMark A. Newman, MDTrong B. Nguyen, MDChristopher C. Ninh, MD
Samuel W. Park, MDJay J. Patel, MDJiun-Rong Peng, MDRussell S. Petrie, MDMiguel P. Prietto, MDNicholas E. Rose, MDKasra Rowshan, MDBenjamin D. Rubin, MDMichael P. Rubinstein, MDPerry R. Secor, MDStewart L. Shanfield, MDMichael F. Shepard, MDFloyd G. Shon, MDDavid C. Smith, MDDaniel T. Stein, MDDilip H. Tapadiya, MDAlexander H. Tischler, MDShail M. Vyas, MDMichael P. Weinstein, MDJon I. White, MDKenneth J. Wilkens, MDLance J. Wrobel, MDNicholas C. Yaru, MDLincoln S. Yee, MD
On Medical Staff as of November 2012
3 2 | H O A G O RT H O P E D I C I N S T I T U T E
Physician Referral
http://orthopedichospital.com/physicians/
Patient Feedback
http://orthopedichospital.com/distinctions/feedback/
Travel Program
http://orthopedichospital.com/about-us/ travel-program/ Gabrielle White, RN, CASC Executive Director, Ambulatory Services & Network Development C: 949/257-9333 O: 949/515-0708 [email protected]
Fellowship Program
Michael J. Patzakis, MD Medical Director Orthopaedic Education and Research Institute (OERI) 949/727-1545 [email protected]
Outcomes Report Team
Robert S. Gorab, MD Chief Medical Officer
Alan H. Beyer, MD Medical Director
Dereesa Reid, MBA VP & Chief Operating Officer
Kanoe Allen, RN, MSN-CNS, PHN, ONC Chief Nursing Officer
Sopida Andronaco, RN, BSN, PHN Manager of Clinical Outcomes
Carlene Parrish Project Coordinator-Quality
Gabrielle White, RN, CASC Executive Director, Ambulatory Services & Network Development
Angela Ittu Marketing Consultant
Sheila Holliday Writing Consultant
For further information related to this report, please contact:
Sopida Andronaco, RN, BSN, PHN Manager of Clinical Outcomes 949/727-5008 [email protected]
IN 2011, HOI BECAME THE HIGHEST
VOLUME PROVIDER OF JOINT
REPLACEMENTS IN CALIFORNIA.
Source: Office of Statewide Health Planning and Development (OSHPD)
LEADERSHIP & MEDICAL STAFF CONTINUED

2012 O U T C O M E S R E P O RT | 3 3
CONTACT INFORMATION & RESOURCES
Main Street Specialty Surgery Center
280 South Main Street, Suite 100 Orange, CA 92868 714/704-1900 www.msssc.com
Orthopedic Surgery Center of Orange County
22 Corporate Plaza, Suite 150 Newport Beach, CA 92660 949/515-0708 www.oscoc.com
Hoag Orthopedic Institute
16250 Sand Canyon Avenue Irvine, CA 92618 949/517-3149 www.hoagorthopedicinstitute.com

3 4 | H O A G O RT H O P E D I C I N S T I T U T E
CONTACT INFORMATION & RESOURCES CONTINUED
DISCLOSURE OF OWNERSHIPHoag Orthopedic Institute meets the definition of a “physician-owned hospital” under 42 CFR 489.3, and is also owned in part by Hoag Memorial Hospital Presbyterian.
The hospital is owned in part by the following physicians:
Lawrence S. Barnett, MD Steven L. Barnett, MD Alan H. Beyer, MD James T. Caillouette, MD Balaji Charlu, MD Jack Chen, MD John F. Cook, Jr., MD Michael Danto, MD Jeffrey E. Deckey, MD Steven C. Dennis, MD Shaunak Desai, MD Paul Dinh, MD
Scott P. Fischer, MD Scott K. Forman, MD Steven H. Gausewitz, MD Andrew P. Gerken, MD Robert S. Gorab, MD Michael L. Gordon, MD Klane Hales, MD Mark N. Halikis, MD Tze C. Ip, MD Richard Lee, MD Stephen A. Mikulak, MD Ram Mudiyam, MD
Narendra Parson, MD Jiun-Rong Peng, MD Russell S. Petrie, MD Carlos A. Prietto, MD Miguel P. Prietto, MD Nicholas E. Rose, MD Benjamin D. Rubin, MD Kimberly Safman, MD Michael F. Shepard, MD Leighton Smith, MD Alexander H. Tischler, MD Michael P. Weinstein, MD
“WITH THOUGHTFUL AND EFFICIENT LEADERSHIP, SPECIALTY HOSPITALS
CAN BE AN INTEGRAL PART OF IMPROVING HEALTH CARE IN THE UNITED
STATES IN THE LONG TERM…”
HEALIO ORTHOPEDICS, MARCH 2012


16250 Sand Canyon Avenue Irvine, CA 92618 949/517-3149 hoagorthopedicinstitute.com
1/13
-LA
D-1
M-A
I
















