Osteoporosis in Men Osteoporosis in Men Update Ohio State: November 2011 Update Ohio State: November 2011 Robert A. Adler, MD Robert A. Adler, MD McGuire Veterans Affairs Med Ctr McGuire Veterans Affairs Med Ctr Virginia Commonwealth University Virginia Commonwealth University Richmond, Virginia, USA Richmond, Virginia, USA
Transcript
Osteoporosis in MenOsteoporosis in MenUpdate Ohio State: November 2011Update Ohio State: November 2011
Robert A. Adler, MDRobert A. Adler, MD
McGuire Veterans Affairs Med CtrMcGuire Veterans Affairs Med CtrVirginia Commonwealth UniversityVirginia Commonwealth University
Richmond, Virginia, USARichmond, Virginia, USA
DisclosuresDisclosures
Research SupportResearch Support NovartisNovartis GenentechGenentech Eli LillyEli Lilly AmgenAmgen MerckMerck
ObjectivesObjectives-- Participants should be able to:Participants should be able to:
Outline the etiology and risk factors Outline the etiology and risk factors Discuss use of fracture risk calculators Discuss use of fracture risk calculators
and other means to identify men at riskand other means to identify men at risk Describe current Rx and the challenges of Describe current Rx and the challenges of
using surrogates for patient outcomes in using surrogates for patient outcomes in chronic disease studieschronic disease studies
OP in Men EvaluationOP in Men Evaluation
Pathophysiology and ClassificationPathophysiology and Classification Primary osteoporosisPrimary osteoporosis Secondary osteoporosisSecondary osteoporosis
Choosing men for evaluationChoosing men for evaluation Laboratory EvaluationLaboratory Evaluation DXA DXA
Riggs and Melton NEJM Riggs and Melton NEJM 314:1676, 1986314:1676, 1986
Primary Osteoporosis: Type IPrimary Osteoporosis: Type I
Ages 51Ages 51--7575Women >> Men (6:1)Women >> Men (6:1) Trabecular bone lostTrabecular bone lost Vertebral and distal radius fracturesVertebral and distal radius fractures Associated with menopause in womenAssociated with menopause in women ?Cause in men?Cause in men
Type I OP in Men:Type I OP in Men:Potential CausesPotential Causes
Increased urinary calcium excretionIncreased urinary calcium excretion Long term negative calcium balanceLong term negative calcium balance Often have a history of kidney stonesOften have a history of kidney stones
Decreased IGFDecreased IGF--I with normal GHI with normal GH Low free estradiolLow free estradiol ?Low free 25 (OH) Vitamin D?Low free 25 (OH) Vitamin D Mastocytosis in marrow onlyMastocytosis in marrow only Cryptic secondary causesCryptic secondary causes
Riggs and Melton NEJM Riggs and Melton NEJM 314:1676, 1986314:1676, 1986
Primary Osteoporosis: Type II Primary Osteoporosis: Type II
Age > 70Age > 70Women > Men (2:1)Women > Men (2:1) Trabecular and Cortical BoneTrabecular and Cortical Bone Hip and vertebral fracturesHip and vertebral fractures AgeAge--related, other factorsrelated, other factors
HypogonadismHypogonadism Primary and secondary (organic)Primary and secondary (organic) Cancer chemotherapy (cyclophosphamide)Cancer chemotherapy (cyclophosphamide) Androgen withdrawal for prostate cancerAndrogen withdrawal for prostate cancer ?Testosterone decline with aging?Testosterone decline with aging
Organic hypogonadism causes OPOrganic hypogonadism causes OP Testosterone replacement increases bmdTestosterone replacement increases bmd No Fracture dataNo Fracture data Does the milder decline in testosterone Does the milder decline in testosterone
with aging lead to osteoporosis?with aging lead to osteoporosis?
Declining Testosterone in AgingDeclining Testosterone in Aging
Common but mild decreaseCommon but mild decrease Total T not correlated with bone densityTotal T not correlated with bone density Better correlation of bioavail EBetter correlation of bioavail E22 & BMD& BMD Newer studies find some relation with T: Newer studies find some relation with T:
data from MrOS suggest men with lower data from MrOS suggest men with lower bioavail T may at higher risk for fracture bioavail T may at higher risk for fracture (but were also the men with lowest (but were also the men with lowest bioavail Ebioavail E22 and highest SHBG)and highest SHBG)
Secondary Factors in 1571 Secondary Factors in 1571 Older Men (MrOS)Older Men (MrOS)
HA Fink, ASBMR 2011HA Fink, ASBMR 2011
Comparative Effects: T & EComparative Effects: T & E
Healthy men ages 20Healthy men ages 20--5050 All received GnRH analogAll received GnRH analog→→ hypogonadismhypogonadism
Group A: Different doses of T gelGroup A: Different doses of T gel
Group B: T gel doses + anastrozoleGroup B: T gel doses + anastrozole
J Finkelstein et al, ASBMR 2011J Finkelstein et al, ASBMR 2011
Effect of T/E vs T onlyEffect of T/E vs T only
T/E (i.e. T gel) T/E (i.e. T gel) →→ ↓↓CTX with CTX with ↑↑ T gel doseT gel dose
T only (i.e. T gel + anastrozole) T only (i.e. T gel + anastrozole) →→ slight slight ↓↓ CTX CTX (but dose response present)(but dose response present)
Conclusions:Conclusions: T & E both affect bone turnover in menT & E both affect bone turnover in men
E more importantE more important
J Finkelstein et al, ASBMR 2011J Finkelstein et al, ASBMR 2011
EE22 may be important, butmay be important, but……
Assays for estradiol are problematic in the Assays for estradiol are problematic in the low male rangelow male range
What is the reference range?What is the reference range? Treat men with ETreat men with E22?? Treat men with SERMs?Treat men with SERMs? Testosterone Rx as a proTestosterone Rx as a pro--hormone and hormone and
hormone?hormone?
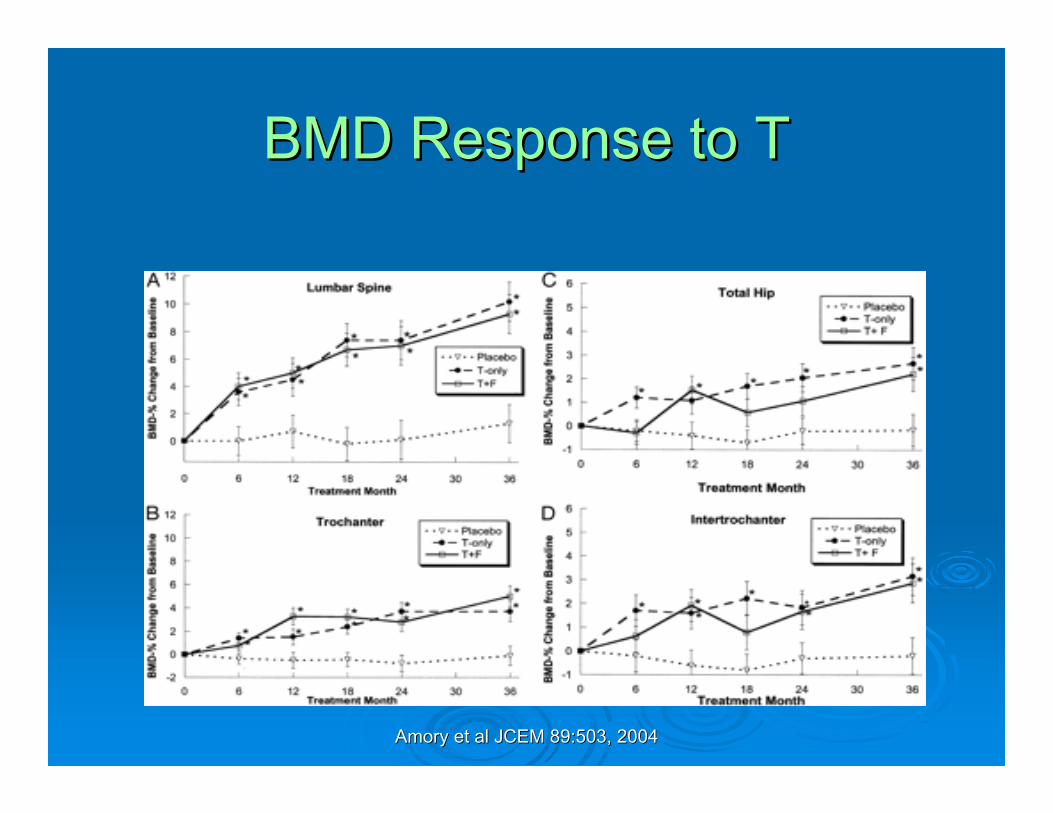
JK Amory et al. JCEM 89:503, JK Amory et al. JCEM 89:503, 20042004
T Rx in men w/ mildly T Rx in men w/ mildly [T][T]
75 men with mildly low T (ages 6475 men with mildly low T (ages 64--83)83) Received T or placebo for 3 yearsReceived T or placebo for 3 years One group received T + finasterideOne group received T + finasteride
Amory et al JCEM 89:503, 2004Amory et al JCEM 89:503, 2004
BMD Response to TBMD Response to T
JK Amory et al, JCEM 89:503, JK Amory et al, JCEM 89:503, 20042004
TT--Rx: 3 Year StudyRx: 3 Year Study
Improvement in BMD, muscle massImprovement in BMD, muscle mass Decreased LDL cholesterolDecreased LDL cholesterol No change in HDL cholesterolNo change in HDL cholesterol No change in No change in PSA or prostate volumePSA or prostate volume
Effects of Testosterone and Effects of Testosterone and Metabolites in MenMetabolites in Men
Facial & Body HairAcne
Scalp Hair LossProstrate Growth
Dihydrotestosterone Muscle MassSkeletal Growth
SpermatogenesisSexual Function
Bone FormationBreast Tissue
Estradiol
Testosterone
OP in men: Etiology SummaryOP in men: Etiology Summary
Idiopathic OP in middle aged men: SpineIdiopathic OP in middle aged men: Spine AgingAging--associated OP: associated OP: ““old oldold old”” : Hip: Hip Secondary causes important in menSecondary causes important in men Testosterone for organic hypogonadismTestosterone for organic hypogonadism ?T for men with the mildly ?T for men with the mildly T of agingT of agingMost older men with osteoporosis have Most older men with osteoporosis have
normal testosterone level for age normal testosterone level for age –– Rx Rx other than T probably indicatedother than T probably indicated
Evaluation other than DXAEvaluation other than DXA
History and physical examHistory and physical examModest laboratory evaluationModest laboratory evaluation
C Ryan, Osteoporos Int 22:1845, C Ryan, Osteoporos Int 22:1845, 20112011
Men referred for OsteoporosisMen referred for Osteoporosis
About About ¾¾ had a secondary cause of had a secondary cause of osteoporosis osteoporosis
Many patients had multiple risk factors Many patients had multiple risk factors such as low Vitamin D, smoking, poor such as low Vitamin D, smoking, poor calcium intakecalcium intake
Even those with known secondary OP Even those with known secondary OP often had other diagnoses, risk factors often had other diagnoses, risk factors identifiedidentified
CS Ryan, Osteoporos Int 22:1845, CS Ryan, Osteoporos Int 22:1845, 20112011
Diagnosis SummaryDiagnosis Summary
Identify high risk menIdentify high risk men History & PE for secondary causesHistory & PE for secondary causes Limited lab testsLimited lab tests
Diagnosis before fracture!Diagnosis before fracture! Best test still DXA of spine, hip, and often Best test still DXA of spine, hip, and often
forearmforearm Spine DXA often not helpfulSpine DXA often not helpful Forearm BMD predicts fx well in menForearm BMD predicts fx well in men Who should get a DXA?Who should get a DXA?
What age?What age? ACP Guidelines: Men > 70 years old, ACP Guidelines: Men > 70 years old,
younger if risk factors presentyounger if risk factors present NOF: DXA at 70, earlier with risk factorsNOF: DXA at 70, earlier with risk factors USPSTF: Not enough evidence to screen USPSTF: Not enough evidence to screen
men at age 70men at age 70 Case finding: Age an important risk factorCase finding: Age an important risk factor
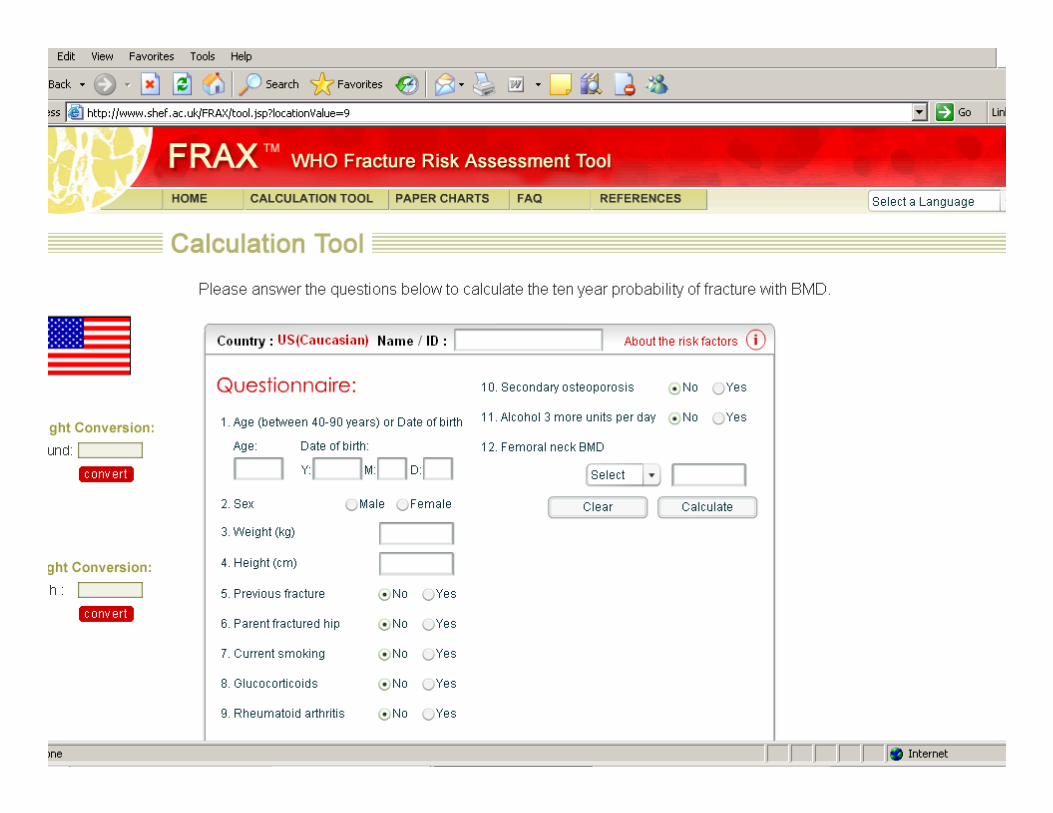
WHO: Validated Risk FactorsWHO: Validated Risk Factors BMD of femoral neckBMD of femoral neck BMI (can substitute for BMD??)BMI (can substitute for BMD??) AgeAge Prior Fragility FracturePrior Fragility Fracture Glucocorticoid ExposureGlucocorticoid Exposure Parental history of Hip FractureParental history of Hip Fracture Current SmokingCurrent Smoking Excess Alcohol IntakeExcess Alcohol Intake Secondary Causes (e.g. Rheumatoid Arthritis)Secondary Causes (e.g. Rheumatoid Arthritis) www.shef.ac.uk/FRAX/www.shef.ac.uk/FRAX/ www.fractureriskcalculator.comwww.fractureriskcalculator.com
FRAX Calculation ToolFRAX Calculation Tool
FRAXFRAX®® vs. Garvan Calculatorvs. Garvan Calculator
81 yo man, 66.2Kg, 81 yo man, 66.2Kg, 168.3cm tall, no other 168.3cm tall, no other risk factorsrisk factors
BMD 0.736 g/cmBMD 0.736 g/cm22
10 yr hip fx risk: 2.4%10 yr hip fx risk: 2.4% 10 yr OP fx risk: 6.8%10 yr OP fx risk: 6.8% Generally would not Generally would not
treat (U.S.)treat (U.S.)
81 yo man, no falls or 81 yo man, no falls or fracturesfractures
BMD 0.736 g/cmBMD 0.736 g/cm22
10 yr hip fx risk: 5.1%10 yr hip fx risk: 5.1% 10 yr OP fx risk: 10 yr OP fx risk:
25.3%25.3% Treat!Treat! Based on Australian Based on Australian
populationpopulationSK Sandhu, Osteoporos Int SK Sandhu, Osteoporos Int
21:863, 201021:863, 2010
Garvan vs FRAX in WomenGarvan vs FRAX in Women% Probability of Fx% Probability of Fx
SK Sandhu OI 21:863, 2010SK Sandhu OI 21:863, 2010
Garvan vs. FRAX in MenGarvan vs. FRAX in Men% Probability of Fx% Probability of Fx
SK Sandhu, OI 21:863, 2010SK Sandhu, OI 21:863, 2010
FRAX vs. GarvanFRAX vs. Garvan
Why are there such differences?Why are there such differences?Why does Garvan identify more men?Why does Garvan identify more men?
Garvan includes falls Garvan includes falls FRAX includes glucocorticoid useFRAX includes glucocorticoid use Both rely on femoral neck BMDBoth rely on femoral neck BMD
Femoral Neck BMD Femoral Neck BMD ++ OAOA
RK Chaganti OI 21:1307, 2010RK Chaganti OI 21:1307, 2010
DXA in Older MenDXA in Older Men
Spine BMD often spuriously highSpine BMD often spuriously high Hip BMD also affected by arthritisHip BMD also affected by arthritis Forearm BMD identifies osteoporosisForearm BMD identifies osteoporosis
HyperparathyroidismHyperparathyroidism Androgen deprivation therapyAndrogen deprivation therapy ?Decrease of T/E?Decrease of T/E22 with aging?with aging?
JM Bruder, Urology 67:152, 2006JM Bruder, Urology 67:152, 2006
Men on ADT: DXA vs FRAXMen on ADT: DXA vs FRAX®®
115 Men sent from GU clinic115 Men sent from GU clinic 58% African58% African--AmericanAmerican Age 77 Age 77 ++ 8 (518 (51--91)91) BMI 28.8 BMI 28.8 ++ 4.9 (17.64.9 (17.6--42.4)42.4) Duration of ADT 3.6 Duration of ADT 3.6 ++ 3.3 (0.13.3 (0.1--11)11) DXA of spine, hip, forearmDXA of spine, hip, forearm
RA Adler, Osteoporos Int 21:647, RA Adler, Osteoporos Int 21:647, 20102010
Men on ADT: DXA vs FRAXMen on ADT: DXA vs FRAX®®
Current Smoking 14.8%Current Smoking 14.8% History of adult fracture 8.7%History of adult fracture 8.7% Parental hip fracture 0.9%Parental hip fracture 0.9% Rheumatoid Arthritis 0%Rheumatoid Arthritis 0% Prednisone use 2.6%Prednisone use 2.6%
FRAXFRAX®® vs. Tvs. T--scorescore
0 10 20 30 40 50 60 70 80
Rx by T-score < -1.5
Rx by T-score < -2.0
Rx by T-score < -2.5
Rx by FRAX w/ BMD
Rx by FRAX w/o BMD
Percent
BMD vs FRAX ScoreBMD vs FRAX Score
Adler RA, Osteoporos Int 21:647, Adler RA, Osteoporos Int 21:647, 20102010
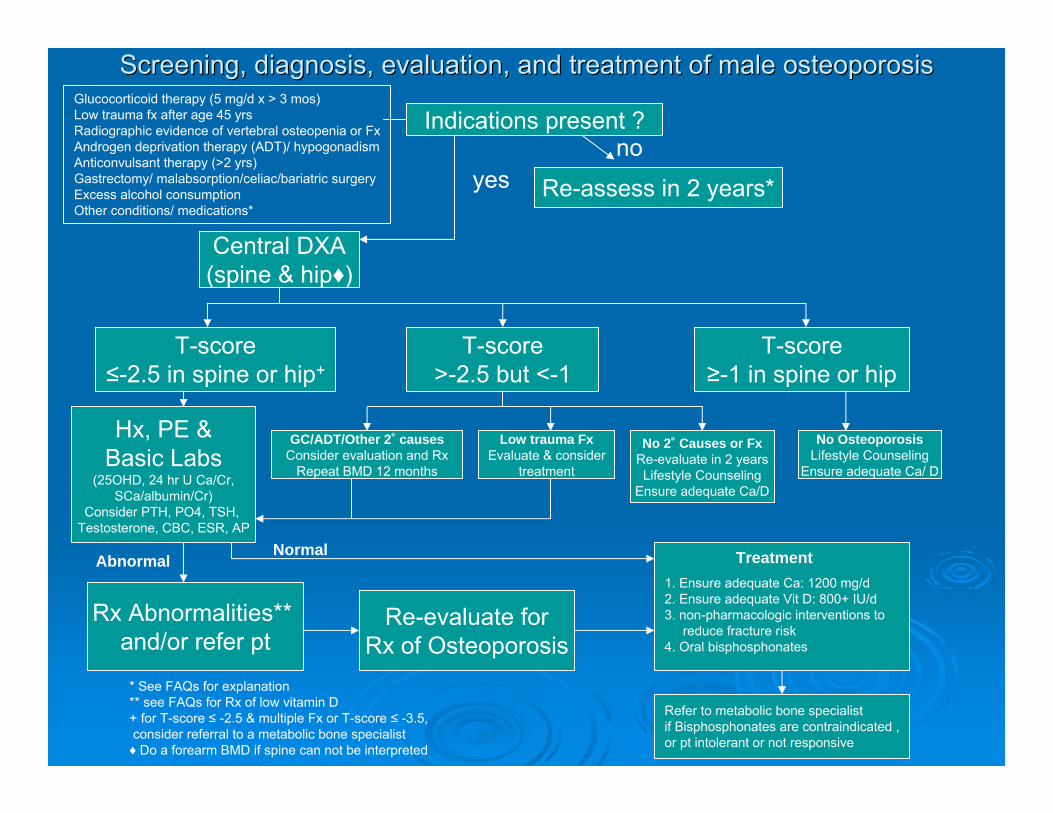
Screening, diagnosis, evaluation, and treatment of male osteoporScreening, diagnosis, evaluation, and treatment of male osteoporosisosis
Indications present ?
yes Re-assess in 2 years*
no
Central DXA(spine & hip♦)
T-score≤-2.5 in spine or hip+
T-score>-2.5 but <-1
T-score≥-1 in spine or hip
GC/ADT/Other 2˚ causesConsider evaluation and Rx
Repeat BMD 12 months
Low trauma FxEvaluate & consider
treatment
No 2˚ Causes or FxRe-evaluate in 2 yearsLifestyle Counseling
Ensure adequate Ca/D
No OsteoporosisLifestyle Counseling
Ensure adequate Ca/ D
Hx, PE &Basic Labs
(25OHD, 24 hr U Ca/Cr,SCa/albumin/Cr)
Consider PTH, PO4, TSH, Testosterone, CBC, ESR, AP
Rx Abnormalities** and/or refer pt
1. Ensure adequate Ca: 1200 mg/d2. Ensure adequate Vit D: 800+ IU/d3. non-pharmacologic interventions to
reduce fracture risk4. Oral bisphosphonates
AbnormalNormal
Re-evaluate forRx of Osteoporosis
Glucocorticoid therapy (5 mg/d x > 3 mos)Low trauma fx after age 45 yrsRadiographic evidence of vertebral osteopenia or FxAndrogen deprivation therapy (ADT)/ hypogonadismAnticonvulsant therapy (>2 yrs)Gastrectomy/ malabsorption/celiac/bariatric surgeryExcess alcohol consumptionOther conditions/ medications*
* See FAQs for explanation** see FAQs for Rx of low vitamin D+ for T-score ≤ -2.5 & multiple Fx or T-score ≤ -3.5,consider referral to a metabolic bone specialist♦ Do a forearm BMD if spine can not be interpreted
Refer to metabolic bone specialistif Bisphosphonates are contraindicated ,or pt intolerant or not responsive
Treatment
VA AlgorithmVA Algorithm
DXA in men with following risk factors:DXA in men with following risk factors: Oral glucocorticoid Rx (Oral glucocorticoid Rx (>> 5 mg pred X 3 mos)5 mg pred X 3 mos) Low trauma fx or fx on spine xLow trauma fx or fx on spine x--rayray ADT/hypogonadismADT/hypogonadism AntiAnti--convulsant Rxconvulsant Rx Gastrx, malabsorption, bariatric surgeryGastrx, malabsorption, bariatric surgery Current smoking, excess EtOHCurrent smoking, excess EtOH
VA prefers case finding but age is not VA prefers case finding but age is not considered an indication (yet)considered an indication (yet)
Recommendations for menRecommendations for men
Use FRAXUse FRAX®® with cautionwith caution Consider Garvan nomogram for menConsider Garvan nomogram for men Evaluate high risk men for osteoporosisEvaluate high risk men for osteoporosis Treat those with osteoporosis based on Treat those with osteoporosis based on
male databasemale database Consider treatment in men with Consider treatment in men with
osteopenia and other risk factors osteopenia and other risk factors –– clinical clinical judgment still importantjudgment still important
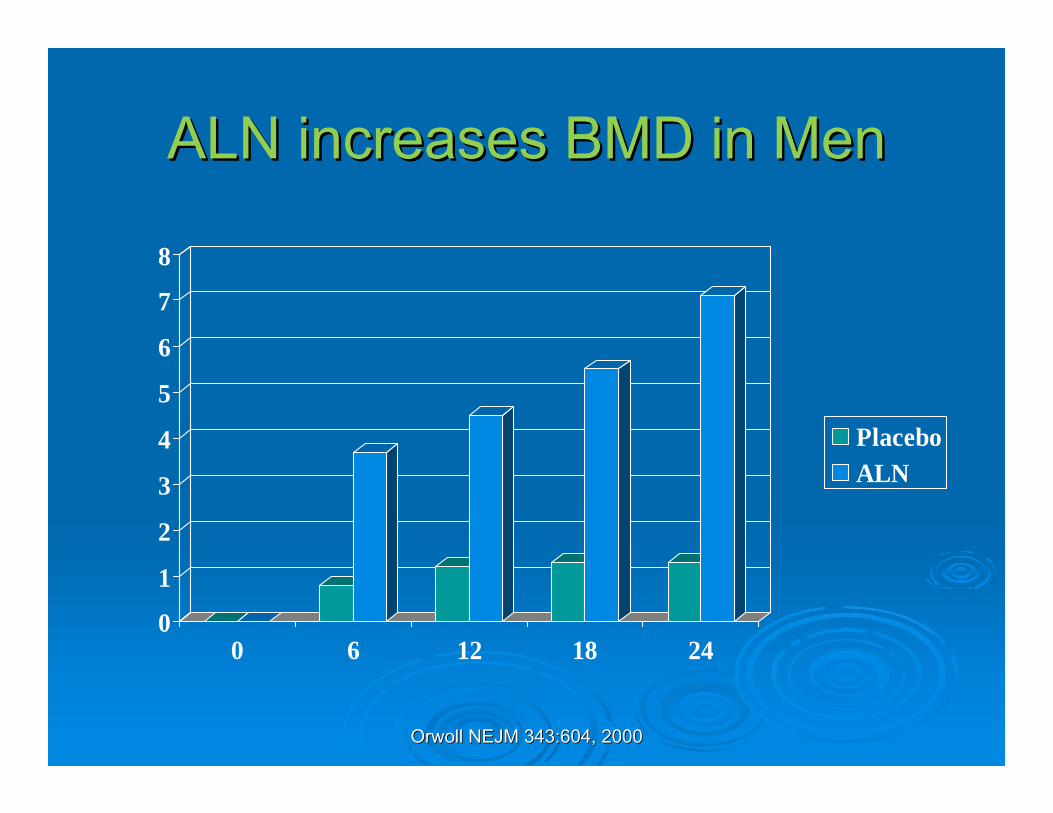
AlendronateAlendronate RisedronateRisedronate Zoledronic AcidZoledronic Acid Denosumab (Men on ADT)Denosumab (Men on ADT) TeriparatideTeriparatide Rx studies: T < Rx studies: T < --2.5 by the male database 2.5 by the male database
or T or T << --2 plus a fragility fracture2 plus a fragility fracture
ALN Decreases Vert Fx (XALN Decreases Vert Fx (X--ray)ray)
01
23
45
6
78
Fx Incidence
PlaceboALN
JD Ringe Rheumatol Int JD Ringe Rheumatol Int 26:427,200626:427,2006
Risedronate Risedronate BMD in MenBMD in Men
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
1 Year % Change in Spine BMD
Placebo
Risedronate
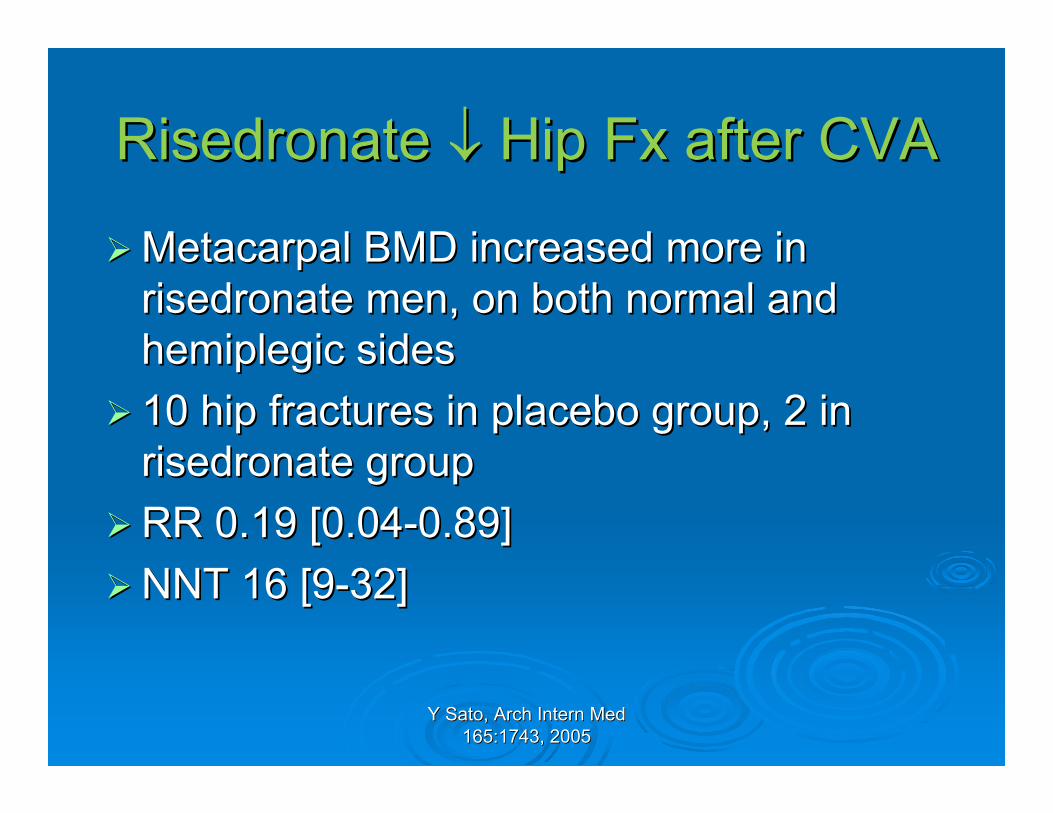
Risedronate Risedronate Hip Fx after CVAHip Fx after CVA
Metacarpal BMD increased more in Metacarpal BMD increased more in risedronate men, on both normal and risedronate men, on both normal and hemiplegic sideshemiplegic sides
10 hip fractures in placebo group, 2 in 10 hip fractures in placebo group, 2 in risedronate grouprisedronate group
Most p.o. bisphosphonate studies used Most p.o. bisphosphonate studies used daily dosingdaily dosing
Some studies: Some studies: ↓↓vertebral fx on xvertebral fx on x--rayray Same Same ∆∆ bone markers as in womenbone markers as in women No studies show No studies show ↓↓clinical fracturesclinical fractures Thus, all Rx based on Thus, all Rx based on ““bridgingbridging”” studies studies
and surrogates for fracture!and surrogates for fracture!
Choosing Rx in MenChoosing Rx in Men--11
Problems with calcium & vitamin DProblems with calcium & vitamin D Calcium Calcium ConstipationConstipation Getting enough Vitamin DGetting enough Vitamin D
Problems with bisphosphonate adherenceProblems with bisphosphonate adherence No difference in how patient feelsNo difference in how patient feels Special method of oral RxSpecial method of oral Rx
Rx based on surrogates for fractureRx based on surrogates for fracture How to choose a bisphosphonate?How to choose a bisphosphonate?
JS Finkelstein et al, NEJM JS Finkelstein et al, NEJM 349:1216, 2003349:1216, 2003
Choosing Rx in Men Choosing Rx in Men -- 22
Teriparatide ContraindicationsTeriparatide Contraindications H/o radiation to boneH/o radiation to bone Potential for osteoblastic metastases Potential for osteoblastic metastases –– thus thus
not for patients with prostate cancernot for patients with prostate cancer Previous/concurrent bisphosphonate Rx may Previous/concurrent bisphosphonate Rx may
blunt or delay response to PTHblunt or delay response to PTH Use PTH in drugUse PTH in drug--nanaïïve patients with ve patients with
severely low bone mass/high fracture risk severely low bone mass/high fracture risk
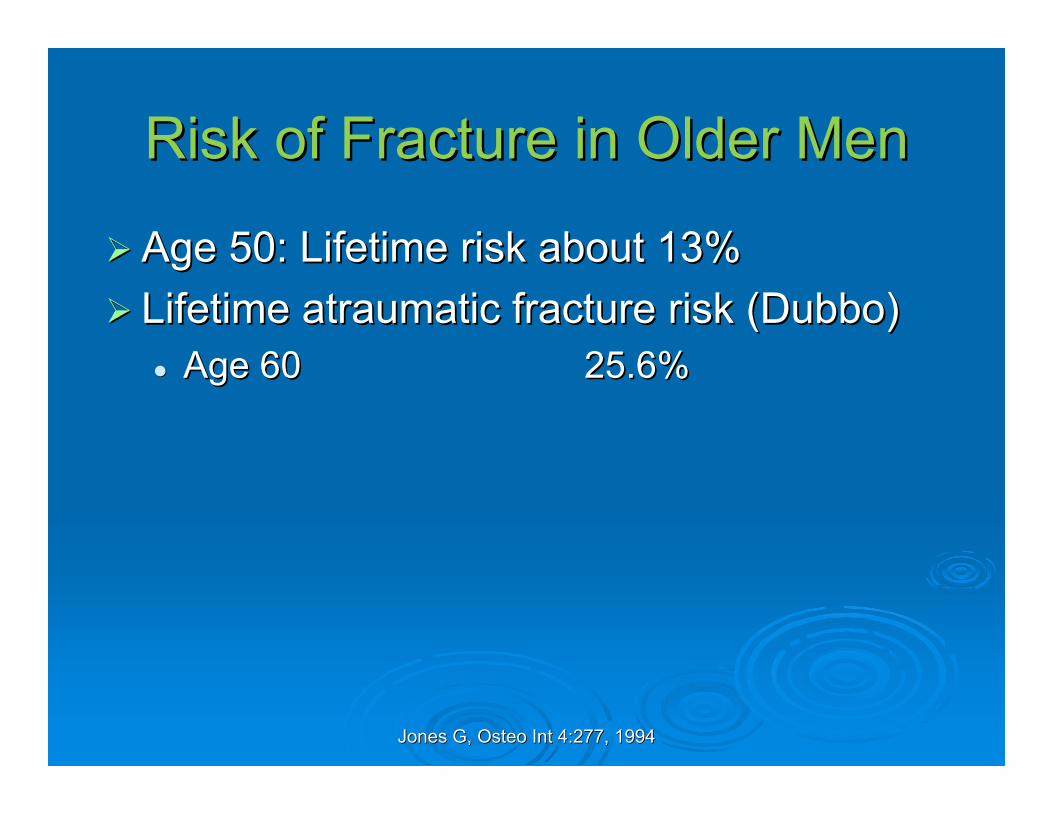
Jones G, Osteo Int 4:277, 1994Jones G, Osteo Int 4:277, 1994
Risk of Fracture in Older MenRisk of Fracture in Older Men
Age 50: Lifetime risk about 13%Age 50: Lifetime risk about 13% Lifetime atraumatic fracture risk (Dubbo)Lifetime atraumatic fracture risk (Dubbo)
Age 60Age 60 25.6%25.6%
Schuit et al Bone 34:195, 2004Schuit et al Bone 34:195, 2004
Age & Hip Fx: RotterdamAge & Hip Fx: Rotterdam
0
5
10
15
20
25
30
60-64 65-69 70-74 75-79 80-84 85+
MenWomen
Fx/100person-yr
% Patients Who Died at 1 yr % Patients Who Died at 1 yr (Age 75(Age 75--84) 84)
Block, Calcif Tissue Int 61:84, Block, Calcif Tissue Int 61:84, 19971997
Hip Fracture & MortalityHip Fracture & Mortality
Women have twice the risk of hip fractureWomen have twice the risk of hip fractureMen with hip fracture have twice the risk of Men with hip fracture have twice the risk of
dying from a hip fracturedying from a hip fracture Thus, the overall mortality rate from hip Thus, the overall mortality rate from hip
fracture is about the same in men and fracture is about the same in men and women!women!
Osteoporosis in Men Osteoporosis in Men -- SummarySummary
Secondary OP important in menSecondary OP important in menModest evaluation Modest evaluation →→ Dx, risk factorsDx, risk factors Large holes in knowledge baseLarge holes in knowledge base Role of testosterone still unclearRole of testosterone still unclear FRAXFRAX®®/Garvan nomogram may help/Garvan nomogram may help Treatment options increasingTreatment options increasing Need to find those men at highest riskNeed to find those men at highest risk
F. Borgstrom et al, Bone 34:1064, F. Borgstrom et al, Bone 34:1064, 20042004
Men Fracture Too!Men Fracture Too!ConclusionConclusion
Osteoporosis is not just a disorder of Osteoporosis is not just a disorder of postmenopausal womenpostmenopausal women
Men with osteoporosis need to be Men with osteoporosis need to be identifiedidentified This is a silent disorder with fatal This is a silent disorder with fatal
consequencesconsequences Finding cases, diagnosing and treating OP Finding cases, diagnosing and treating OP
in men will save lives and moneyin men will save lives and money