7 Osteoporosis: strategies for prevention and management Richard Keen * BSc, PhD, MRCP Consultant Rheumatologist and Honorary Senior Lecturer in Metabolic Bone Disease Institute of Orthopaedics and Musculoskeletal Sciences, The Royal National Orthopaedic Hospital, Brockley Hill, Stanmore, Middlesex HA7 4LP, UK Osteoporosis is a serious public health issue, affecting up to 1 in 2 women and 1 in 5 men over the age of 50 years. The common osteoporotic fractures occur at the spine, wrist and hip. For the patient affected by osteoporosis, these fractures are associated with significant morbidity and, in the case of hip and spine fractures, an excess mortality. The treatment of osteoporotic fractures is also associated with a significant healthcare cost for society. Currently, measurement of bone mineral density using dual energy X-ray absorptiometry is the gold standard for the diagnosis of osteoporosis. In the future, however, assessment of frac- ture risk will be based on algorithms incorporating clinical risk factors and bone density mea- surements, where appropriate. The goal of treatment is to reduce the risk of future fracture. Patients at high risk for fracture should be assessed and screened to exclude secondary causes for osteoporosis. Bisphosphonates (alendronate, etidronate, ibandronate, risedronate) are the first-line ther- apy for the majority of patients and these treatments can be given either orally or intravenously. Alternative treatment options include strontium ranelate and raloxifene. Anabolic therapy with parathyroid hormone can be considered for patients with severe disease. These patients will of- ten require referral for specialist assessment and monitoring. All patients at risk of developing osteoporosis should be given lifestyle advice regarding dietary intake of calcium and vitamin D and regular weight-bearing exercise. Key words: osteoporosis; management; fracture; bisphosphonates. Osteoporosis is a skeletal disease characterised by low bone mass and microarchitec- tural deterioration, with a resulting increase in bone fragility and hence susceptibility to fracture. 1 Fractures of the hip, vertebral body and distal forearm have long been regarded as the classical osteoporotic fractures. Osteoporosis is, however, a systemic * Tel.: þ44 20 8090 5289; Fax: þ44 20 8420 7487. E-mail address: [email protected]1521-6942/$ - see front matter ª 2006 Elsevier Ltd. All rights reserved. Best Practice & Research Clinical Rheumatology Vol. 21, No. 1, pp. 109e122, 2007 doi:10.1016/j.berh.2006.10.004 available online at http://www.sciencedirect.com
Transcript
Best Practice & Research Clinical RheumatologyVol. 21, No. 1, pp. 109e122, 2007
doi:10.1016/j.berh.2006.10.004available online at http://www.sciencedirect.com
7
Osteoporosis: strategies for prevention
and management
Richard Keen* BSc, PhD, MRCP
Consultant Rheumatologist and Honorary Senior Lecturer in Metabolic Bone Disease
Institute of Orthopaedics and Musculoskeletal Sciences, The Royal National Orthopaedic Hospital,
Brockley Hill, Stanmore, Middlesex HA7 4LP, UK
Osteoporosis is a serious public health issue, affecting up to 1 in 2 women and 1 in 5 men overthe age of 50 years. The common osteoporotic fractures occur at the spine, wrist and hip. Forthe patient affected by osteoporosis, these fractures are associated with significant morbidityand, in the case of hip and spine fractures, an excess mortality. The treatment of osteoporoticfractures is also associated with a significant healthcare cost for society.
Currently, measurement of bone mineral density using dual energy X-ray absorptiometry isthe gold standard for the diagnosis of osteoporosis. In the future, however, assessment of frac-ture risk will be based on algorithms incorporating clinical risk factors and bone density mea-surements, where appropriate. The goal of treatment is to reduce the risk of future fracture.Patients at high risk for fracture should be assessed and screened to exclude secondary causesfor osteoporosis.
Bisphosphonates (alendronate, etidronate, ibandronate, risedronate) are the first-line ther-apy for the majority of patients and these treatments can be given either orally or intravenously.Alternative treatment options include strontium ranelate and raloxifene. Anabolic therapy withparathyroid hormone can be considered for patients with severe disease. These patients will of-ten require referral for specialist assessment and monitoring. All patients at risk of developingosteoporosis should be given lifestyle advice regarding dietary intake of calcium and vitamin Dand regular weight-bearing exercise.
Osteoporosis is a skeletal disease characterised by low bone mass and microarchitec-tural deterioration, with a resulting increase in bone fragility and hence susceptibilityto fracture.1 Fractures of the hip, vertebral body and distal forearm have long beenregarded as the classical osteoporotic fractures. Osteoporosis is, however, a systemic
disease and prospective studies have demonstrated an increase in risk for almost allfractures in individuals with low bone mass.2
WHAT IS THE SIZE OF THE PROBLEM
The incidence of osteoporosis is best measured as the incidence of fractures that arethe consequences of osteoporosis (Figure 1).
In Western populations, hip fracture incidence rates increase exponentially withage. Above 50 years of age there is a female to male incidence ratio of approximately3:1. Overall about 98% of hip fractures occur among people aged 65 years or older and80% occur in women due to the fact that there are more elderly women than men.Worldwide, elderly people represent the fastest growing age group and with an ageingpopulation the incidence of hip fractures is likely to rise substantially. It is predictedthat the estimated number of hip fractures worldwide will rise from 1.7 million in1990 to 6.3 million in 2050.3 This estimate assumes that fracture rates remain thesame over this time period, although there is evidence that age-adjusted hip fracturerates may indeed be increasing. Under these circumstances, even assuming only a riseof 1% per year in the age-adjusted rate, the estimated number of hip fractures could beas high as 8.2 million by 2050.
Incidence rates for morphometric vertebral deformities have been obtainedthrough the European Prospective Osteoporosis study (EPOS).4 The incidence ofnew vertebral deformities was estimated from radiographs at baseline and at 4 yearfollow-up in these subjects. Overall, age and sex-adjusted incidence rates were1% per year among women and 0.6% per year among men. Only about a third of allradiographically identified fractures come to specialist attention and fewer than 10%result in hospital admission.
Distal forearm fractures display a different pattern of incidence rates. Studies fromnorthern USA around 10 years ago suggested that rates increased linearly among womenbetween the ages of 40 and 65 years; thereafter rates appeared to plateau.5 Among men,
Figure 1. Incidence of osteoporotic fractures in women.
Osteoporosis: prevention and management 111
incidence rates remained constant between the ages of 20 and 80 years. As a conse-quence, most distal forearm fractures occur in women, 50% of whom are older than65 years.
Burden of the disease
Overall, the remaining lifetime risk for a 50 year old woman sustaining an osteoporotic-related fracture is estimated at 50%.6 For a man, this lifetime risk is estimated at 20%(Table 1).
Hip fractures are the most devastating result of osteoporosis leading to emergencyhospitalisation, surgery and subsequent rehabilitation. These fractures are associatedwith an excess mortality and significant morbidity. Up to 20% of patients admittedwith an acute fracture will die within 6 months.7 Of those that survive, up to one thirdbecome totally dependent and some permanently disabled, necessitating institutional-isation.8 Vertebral fractures are also associated with excess mortality, although this ap-pears to be related to comorbid conditions rather than being directly attributable tothe fracture. Spine fractures cause significant disability due to pain and thoracic kypho-sis. This morbidity varies with the frequency and site of the fractures. Multiple frac-tures typically cause the most pain and disability and fractures in the thoracic spineappear more symptomatic and disabling than those in the lumbar spine.9 Quality oflife studies have shown an increasing impact on quality of life with an increasing num-ber of vertebral fractures.10
Although it is recognised that osteoporotic fractures represent a significant burdenof morbidity for patients, the economic burden to society is equally high. Studies invarious countries have shown that the costs of osteoporosis are very substantial. Ithas recently been estimated that the combined cost of all osteoporotic fractures is$20 billion in the USA and about $30 billion in the European Union.11 Acute care fol-lowing hip fracture contributes significantly to these costs, although substantial costsare also incurred for rehabilitation and social care. In Europe, the total costs of caringfor people in the first year after a hip fracture is estimated at V14.7 billion12 and thescale of costs is similar in the USA.13
ASSESSMENT OF FRACTURE RISK
Assessment of bone mineral density (BMD) has been critical for the diagnosis of os-teoporosis, as proposed by the World Health Organisation (WHO) in 1994. BMD is
Table 1. The lifetime and 10 year probability of a future fracture for men and women at different ages.
Current age (years) 50 60 70 80
Lifetime risk of any
fractures (%)
Men 20.7 14.7 11.4 9.6
Women 53.2 45.5 36.9 28.6
10 year risk of any
fractures (%)
Men 7.1 5.7 6.2 8.0
Women 9.8 13.3 17.0 21.7
Source: Adapted from van Staa et al (2001).6
112 R. Keen
able to predict fracture risk as good as, if not better, than the ability to predict heartdisease risk from blood cholesterol concentrations and to predict stroke risk fromblood pressure measurement values.14
Low bone density itself does not, however, mean that an individual will fracture andit has become clear that there are additional clinical risk factors that are able to predictfracture risk independent of BMD. The WHO has identified the following riskfactors15:
� History of fragility fracture� Use of glucocorticoids� Parental history of fracture� Associated medical diseases (i.e. rheumatoid arthritis)� Cigarette smoking� Excessive alcohol intake� Low body weight (body mass index< 19 kg/m2)
The combined use of these risk factors together with age and BMD enables theprediction of 10-year probabilities for hip and other fractures. Intervention thresholdsfor various agents can then be derived using health economic modelling.
POPULATIONS TO TARGET
When considering the individuals at whom intervention should be targeted, the fol-lowing groups can be identified within a population:
Normal: The whole population at all agesAt risk: As detailed above using WHO risk factorsOsteoporosis: Men and women with a BMD T score at the spine and/or hip of e2.5or lowerEstablished osteoporosis: Men and women with one or more fragility fractures�BMD T score below �2.5.
Most strategies will be targeted to those at risk, or to those with disease(with or without a history of fracture). Improving the skeletal health of thewhole population appears attractive from a public health perspective, althoughdata that this strategy would be effective in reducing fracture incidence is notavailable.
EVIDENCE-BASE FOR INTERVENTIONS
Non-pharmacological therapy
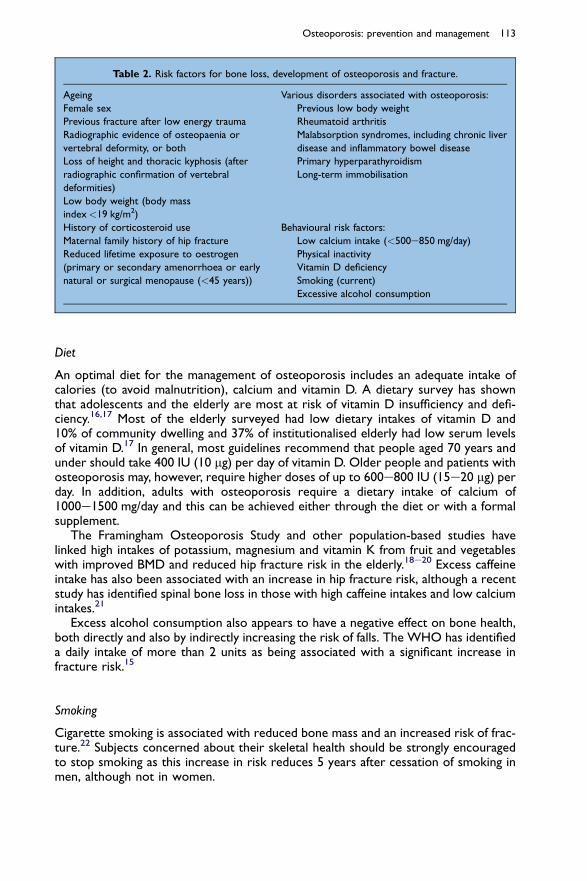
General life style measurements should be adopted in all subjects at risk ofosteoporosis. Many of these interventions are based on epidemiological data linkingeither deficiency or excess of a particular factor with an increased risk of fracture(Table 2). It is less clear, however, whether modification of the epidemiological factorswill result in a reduced fracture risk.
Osteoporosis: prevention and management 113
Diet
An optimal diet for the management of osteoporosis includes an adequate intake ofcalories (to avoid malnutrition), calcium and vitamin D. A dietary survey has shownthat adolescents and the elderly are most at risk of vitamin D insufficiency and defi-ciency.16,17 Most of the elderly surveyed had low dietary intakes of vitamin D and10% of community dwelling and 37% of institutionalised elderly had low serum levelsof vitamin D.17 In general, most guidelines recommend that people aged 70 years andunder should take 400 IU (10 mg) per day of vitamin D. Older people and patients withosteoporosis may, however, require higher doses of up to 600e800 IU (15e20 mg) perday. In addition, adults with osteoporosis require a dietary intake of calcium of1000e1500 mg/day and this can be achieved either through the diet or with a formalsupplement.
The Framingham Osteoporosis Study and other population-based studies havelinked high intakes of potassium, magnesium and vitamin K from fruit and vegetableswith improved BMD and reduced hip fracture risk in the elderly.18e20 Excess caffeineintake has also been associated with an increase in hip fracture risk, although a recentstudy has identified spinal bone loss in those with high caffeine intakes and low calciumintakes.21
Excess alcohol consumption also appears to have a negative effect on bone health,both directly and also by indirectly increasing the risk of falls. The WHO has identifieda daily intake of more than 2 units as being associated with a significant increase infracture risk.15
Smoking
Cigarette smoking is associated with reduced bone mass and an increased risk of frac-ture.22 Subjects concerned about their skeletal health should be strongly encouragedto stop smoking as this increase in risk reduces 5 years after cessation of smoking inmen, although not in women.
Table 2. Risk factors for bone loss, development of osteoporosis and fracture.
Ageing Various disorders associated with osteoporosis:
Previous low body weight
Rheumatoid arthritis
Malabsorption syndromes, including chronic liver
disease and inflammatory bowel disease
Primary hyperparathyroidism
Long-term immobilisation
Female sex
Previous fracture after low energy trauma
Radiographic evidence of osteopaenia or
vertebral deformity, or both
Loss of height and thoracic kyphosis (after
radiographic confirmation of vertebral
deformities)
Low body weight (body mass
index<19 kg/m2)
History of corticosteroid use Behavioural risk factors:
Low calcium intake (<500e850 mg/day)
Physical inactivity
Vitamin D deficiency
Smoking (current)
Excessive alcohol consumption
Maternal family history of hip fracture
Reduced lifetime exposure to oestrogen
(primary or secondary amenorrhoea or early
natural or surgical menopause (<45 years))
114 R. Keen
Exercise
Regular weight-bearing exercise is encouraged to improve BMD. Any fracture reductionassociated with exercise is probably as a result of improved muscle strength and a lowerrisk of falling, particularly in the elderly.23 Excessive exercise in premenopausal women mayactually have detrimental effects on bone due to weight loss and secondary amenorrhoea.
Hip protectors
Controlled studies conducted in care homes have demonstrated that a structured ed-ucation programme and the provision of hip protectors can reduce the number of hipfractures.24 Compliance with hip protectors is often poor and a recent meta-analysissuggested that the beneficial effect is limited to the elderly in residential care ratherthan those living in the community.25
Pharmacological agents
Calcium and vitamin D
Adequate calcium nutrition is essential for the development and maintenance of a nor-mal skeleton. At present, calcium supplements are often administered as a combinedtherapy with other agents for the treatment of osteoporosis. Vitamin D acts to in-crease calcium absorption in the gastrointestinal tract and thereby inhibits parathyroidhormone (PTH)-mediated bone resorption. The recommended daily requirement forcalcium intake in postmenopausal women is 1000e1500 mg/day and for vitamin D it is400e800 IU/day. These values may, however, vary depending on age, ethnic group, nu-trition status and skeletal size.
Calcium appears to have little effect if given within the first 5 years of the menopausewhen bone loss is predominantly due to oestrogen withdrawal.26 Calcium supplementshave been shown to reduce ageing-associated bone loss in prospective controlled trialsby up to 50%.26,27 In the frail elderly, supplementation with 1.2 gm/day of elemental cal-cium and 800 IU/day of cholecalciferol has been shown to reduce the risk of hip fractureand other non-vertebral fractures.28 More recent studies have, however, failed to dem-onstrate any significant effect of calcium and vitamin D on fracture risk.29,30
Hormone replacement therapy (HRT)
The association between osteoporosis and oestrogen deficiency was first described byFuller Albright in 1941, when he noted that 40 out of 42 women with osteoporoticfractures were postmenopausal.31 For many years oestrogen (plus progestogen inthose with an intact uterus) replacement was considered the ‘first-line’ therapy forwomen, as both a prevention and a treatment for osteoporosis. Although HRT wasknown to reduce menopause-related bone loss, evidence for its fracture efficacywas limited. Data from meta-analyses has recently demonstrated that HRT can reducethe risk of both vertebral and non-vertebral fractures.32,33 These results have alsobeen confirmed following the publication of the Women’s Health Initiative (WHI),where treatment with HRT reduced clinical fractures in postmenopausal women.34,35
In one arm of the study 16,608 postmenopausal women with an intact uterus andaged> 50 years, were randomised to conjugated equine oestrogens (CEE) 0.625 mgdaily plus medroxyprogesterone acetate 2.5 mg daily or placebo.34 This study wasstopped 3 years early after 5.2 years because of unfavourable outcomes. In the other
Osteoporosis: prevention and management 115
arm, 10,739 postmenopausal women 50e79 years of age with hysterectomy wererandomised to CEE 0.625 mg daily or placebo and followed for an average 7.1 years.35
These studies demonstrated that HRT use was associated with a significant reductionin risk of clinical vertebral fracture and non-vertebral fractures, including hip. Despitethese beneficial effects on osteoporosis, treatment with CEE plus progestagen was as-sociated with an increased risk of breast cancer, myocardial infarction, stroke and ve-nous thromboembolic events, and CEE use alone with an increased risk of stroke.Although the risks to an individual are small, HRT is no longer recommended asa first-choice therapy in postmenopausal women for management of osteoporosis.
It is currently recommended that HRT be considered for short-term use in themanagement of menopausal symptoms and that alternative agents are consideredfor the treatment of osteoporosis. Extended use of HRT may occur where individualsfind that cessation of treatment causes a return of menopausal vasomotor symptomsand a poor quality of life. Such individuals should be counselled about the risks andbenefits of treatment and alternative options explored. They should undergo regularscreening for breast cancer and appropriate management of concurrent risk factorsfor vascular events would also be prudent.
Selective oestrogen receptor modulators (SERMs)
SERMs are designed to have tissue-specific effects, acting as either an oestrogen agonistor antagonist. Currently raloxifene is the only SERM licensed for the management of os-teoporosis, although agents such as lasofoxifene are undergoing phase III clinical trials.
Raloxifene is a benzothiophene that acts as an agonist in bone and lipid metabolismbut as an antagonist in the breast and endometrium. In the Multiple Outcome ofRaloxifene Evaluation (MORE) study, 7705 women with osteoporosis received ralox-ifene.36 There was a significant reduction in vertebral fracture risk in both those withpre-existing vertebral fractures (reduction of 50%) and in those without pre-existingvertebral fractures (reduction of 30%), although no effect was seen on non-vertebralfractures. In an extension of the phase III study for an additional 4 years in 4011women, non-vertebral fracture was a secondary endpoint, but there was still no sig-nificant difference in overall non-vertebral fracture rates.37 These data therefore sug-gest that raloxifene should not be used in patients at high risk of hip fracture. It may bemore suitable for women aged< 70 years, although in the early postmenopausal yearsthe incidence of menopausal vasomotor symptoms may be induced. The MORE studyalso demonstrated that the frequency of breast cancer was lowered by 70% and thisadditional non-skeletal benefit may be important in aiding a decision on treatment.
Bisphosphonates
Bisphosphonates are synthetic analogues of pyrophosphate that bind to hydroxyapatiteat sites of active bone remodelling. By inhibiting the action of osteoclasts they reducebone resorption. They contain a non-hydrolyzable P-C-P bond and have two sidechains, one that participates in binding to bone and one that determines the pharma-cological properties of the drug. Absorption of an oral dose is less than 5% and sub-sequent uptake by bone is 30e40%, with the remainder undergoing renal excretion.Bisphosphonates have a short plasma half-life but elimination from the skeleton isslow with a half-life in bone of several years.
Etidronate was the first bisphosphonate to be developed and licensed for the man-agement of osteoporosis. Treatment is given intermittently (400 mg/day for 2 weeks,
116 R. Keen
repeated every 13 weeks). Etidronate has been shown to increase spinal bone densityby 4e5% during the first 2 years of treatment in two placebo-controlled studies.38,39
Despite certain limitations regarding the power of these two studies, the combinedresults suggest that this intermittent regimen of etidronate therapy is effective in re-ducing further vertebral fractures in patients with severe osteoporosis and possiblyaccelerated bone loss. Findings from a meta-analysis of controlled trials of etidronateover 1e4 years suggest a reduction in vertebral fracture risk with a relative risk (RR)of 0.63 (95% confidence interval (CI)¼ 0.44e0.92), but no effect was seen for non-vertebral fractures.40
Alendronate, ibandronate and risedronate are more potent inhibitors of bone re-sorption than etidronate. Alendronate and risedronate have been shown to reducefracture risk at all the clinically important sites, including the hip, whereas ibandronatehas only been shown to reduce the risk of vertebral fractures. In women with osteo-porosis (as defined by a BMD T-score below �2.5) and/or presence of at least onevertebral fracture, treatment with alendronate was associated with a 50% reductionin fracture risk at spine, wrist and hip when compared to placebo.41 Risedronatehas also been shown to reduce the risk of vertebral42 and non-vertebral fracture.43
Ibandronate has been shown to reduce the risk of vertebral fractures in womenwith low BMD and one or more baseline fractures.44 The optimal treatment durationis not yet known. Most clinical studies have been conducted over a 3 year duration,but data is available for alendronate up to 10 years.45 The results of further studieswith long term data on BMD, facture rates, bone turnover and bone histology areneeded to aid in management decisions. Compliance with therapy has been aided byonce weekly dosing, which is available for both risedronate (35 mg/week) and alendr-onate (70 mg/week). Monthly dosing in also available for ibandronate (150 mg/month).
Oral bisphosphonates are generally well tolerated. However, in those with gastro-intestinal intolerance or poor long term compliance intravenous treatment offers analternative. Pamidronate infused every 3 months increases BMD at the spine andhip.46 There is, however, no data on fractures with this intermittent dosing regimen.Intravenous ibandronate is licensed for the treatment of postmenopausal osteoporo-sis, given as 3 mg every 3 months. Zoledronic acid is a cyclic nitrogen containing a thirdgeneration bisphosphonate that is the most potent of the available bisphosphonates.A single 4 mg infusion of zoledronate has been shown to have effects on bone turnoverfor up to 12 months, with increases in BMD similar to those achieved with currentlyavailable oral bisphosphonates.47 Phase III studies are examining the role for zole-dronic acid in the treatment of postmenopausal osteoporosis and also in the immedi-ate post-operative period following hip fracture in the elderly.
Bisphosphonates are now regarded as the treatment of choice for postmenopausalosteoporosis due to proven efficacy and a good safety profile.48
Strontium ranelate
Strontium ranelate has been approved by the European Union for the treatment ofpostmenopausal osteoporosis. Its mode of action is unclear, although it appears tohave a modest effect on inhibiting bone resorption with no negative effect on bone for-mation. Results from a phase II trial in 1649 postmenopausal women demonstrated thatstrontium ranelate reduced the risk of vertebral fractures by 49% by 1 year and by 41%over 3 years.49 Results from a second study in older women, showed that strontiumranelate reduced the risk of non-vertebral fracture by a modest 16%50, with a reductionin the risk of hip fracture in those aged> 74 years with a low BMD (T-score below�3).
Osteoporosis: prevention and management 117
In general treatment with strontium ranelate was well tolerated apart from a low rateof gastro-intestinal side-effects and an unexplained increased risk of venous thrombosis.Strontium ranelate can be considered as an alternative to bisphosphonate therapy inthe management of postmenopausal osteoporosis.
Parathyroid hormone (PTH)
Intermittent doses of human PTH given as daily subcutaneous injections have beenshown to exert an anabolic effect leading to increased osteoblast number and in-creases in bone formation. This contrasts with continuous exposure to PTH, whichleads to increased bone resorption and a net decrease in trabecular bone volume.
Currently teriparatide (recombinant human PTH [1-34]) is the only formulation ofPTH available for the management of osteoporosis. It is anticipated, however, that thefull-length recombinant molecule (hPTH 1-84) will also soon be available. In a phase IIItrial in 1637 postmenopausal women, treatment with teriparatide was shown to reducethe risk of vertebral fractures by 65% and non-vertebral fractures overall by 53%.51 Thestudy was not powered to detect treatment effects at individual skeletal sites and, there-fore, there is no data on hip fracture reduction. In Europe teriparatide has recently beenapproved for a treatment duration of 18 months in postmenopausal women, whereas inthe US treatment is licensed for 24 months and it is also available for use in men.
Calcitonin
Calcitonin is an endogenous peptide of 32 amino acids that possesses anti-osteoclasticactivity. It interacts with the osteoclast via specific receptors resulting in a flattening ofthe cell brush border and an alteration of its cytoplasm. Calcitonin is also thought tointerfere with the differentiation of pre-osteoclasts thereby reducing the lifespan andnumber of mature osteoclasts. In clinical practice, four calcitonins (human, pig, salmon,eel) have been used in studies of osteoporosis. Parenteral administration of calcitoninis given either by intramuscular injection, suppository or nasal spray.
Data for an effect of calcitonin on fracture risk is limited and comes mainly fromthe Prevent Recurrence Of Osteoporotic Fractures (PROOF) study.52 This was a
Table 3. Effect of lifestyle interventions on key outcomes in osteoporosis.
Lifestyle interventions Aim of intervention
Function and structure Activity and participation
Tissue damage Symptom
BMD Fracture
Diet e calcium Iaþ IIIþ IE IE
Weight e maintenance of a
normal body mass index
IIIþ IIIþ IE IE
Exercise e weight bearing Iaþ IIIþ IE IE
Avoiding smoking IIIþ IIIþ IE IE
Avoiding alcohol abuse IVþ IVþ IE IE
Ia e IV, grading of evidence.
Nature of effect: þ, positive; 0, evidence of no effect; �, negative effect; #, inconsistent findings;
IE, inadequate evidence.
118 R. Keen
5 year prospective double blind, randomised, placebo-controlled study of 1255 post-menopausal women with osteoporosis. Data from that study demonstrated a reductionof vertebral fractures by 30% in individuals taking 200 IU of intranasal salmon calcitonin.There was, however, no effect on peripheral fractures. The study has subsequentlybeen criticised for the following reasons: 60% of subjects in the study were lost to fol-low-up, doses of 100 IU and 400 IU had no effect on vertebral fracture risk and therewas no consistent effect on BMD and biochemical markers of bone turnover.
Although rarely used as a first-line treatment to prevent fractures, calcitonin hasbeen shown to have analgesic properties which make it suitable for use in thosewith pain secondary to vertebral collapse, particularly in the acute state. The physio-logical mechanisms underlying this action are poorly understood.
TARGETS FOR INTERVENTION
Targets that are most important in the prevention or management of osteoporosis andlow trauma fractures are to:
� Maximise bone mass� Maximise peak bone mass� Reduce age-related bone loss
Table 4. Effect of therapeutic interventions on outcomes in postmenopausal osteoporosis.
Nature of effect: þ, positive; #, inconsistent findings.a Evidence only applies to very elderly women living in sheltered accommodation, not the whole
elderly population.b Post-hoc analysis.
Osteoporosis: prevention and management 119
� Prevent falls� Avoid other risk factors for osteoporosis and fracture� Reduce pain� Reduce disability
These can be further grouped into the following categories:
Symptoms: PainTissue damage: BMD, fractureActivity and participation: Quality of life measurements (disease-specific orgeneric).
Table 3 summarises the level of evidence for lifestyle interventions on the targetoutcomes. Table 4 summarises the evidence for therapeutic interventions.
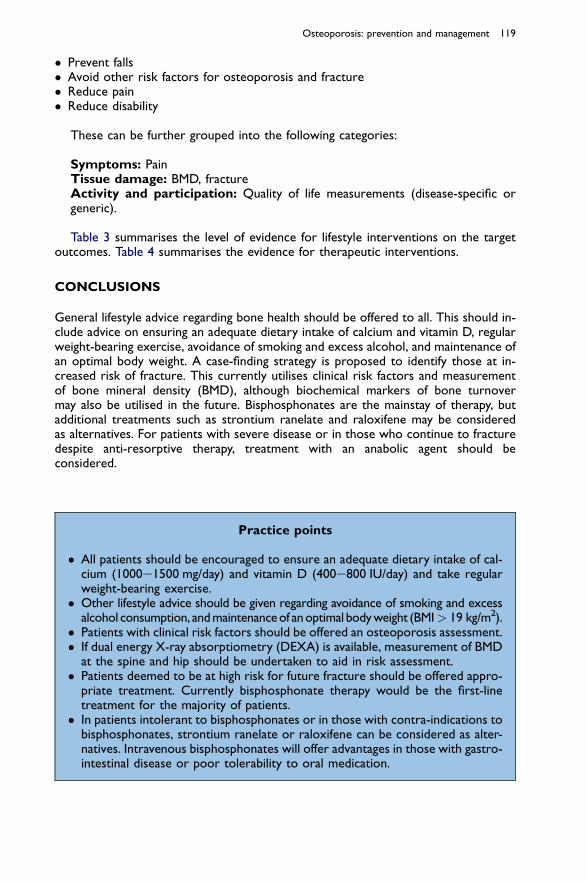
CONCLUSIONS
General lifestyle advice regarding bone health should be offered to all. This should in-clude advice on ensuring an adequate dietary intake of calcium and vitamin D, regularweight-bearing exercise, avoidance of smoking and excess alcohol, and maintenance ofan optimal body weight. A case-finding strategy is proposed to identify those at in-creased risk of fracture. This currently utilises clinical risk factors and measurementof bone mineral density (BMD), although biochemical markers of bone turnovermay also be utilised in the future. Bisphosphonates are the mainstay of therapy, butadditional treatments such as strontium ranelate and raloxifene may be consideredas alternatives. For patients with severe disease or in those who continue to fracturedespite anti-resorptive therapy, treatment with an anabolic agent should beconsidered.
Practice points
� All patients should be encouraged to ensure an adequate dietary intake of cal-cium (1000e1500 mg/day) and vitamin D (400e800 IU/day) and take regularweight-bearing exercise.� Other lifestyle advice should be given regarding avoidance of smoking and excess
alcohol consumption, andmaintenance of anoptimal body weight (BMI> 19 kg/m2).� Patients with clinical risk factors should be offered an osteoporosis assessment.� If dual energy X-ray absorptiometry (DEXA) is available, measurement of BMD
at the spine and hip should be undertaken to aid in risk assessment.� Patients deemed to be at high risk for future fracture should be offered appro-
priate treatment. Currently bisphosphonate therapy would be the first-linetreatment for the majority of patients.� In patients intolerant to bisphosphonates or in those with contra-indications to
bisphosphonates, strontium ranelate or raloxifene can be considered as alter-natives. Intravenous bisphosphonates will offer advantages in those with gastro-intestinal disease or poor tolerability to oral medication.
120 R. Keen
REFERENCES
1. World Health Organization Study Group. Assessment of fracture risk and its application to screening for
postmenopausal osteoporosis. WHO Technical Report Series No. 843. Geneva: World Health Organiza-
tion, 1994.
2. Kanis JA, Johnell O, De Laet C et al. A meta-analysis of previous fracture and subsequent fracture risk.
Bone 2004; 29: 517e522.
*3. Sambrook P & Cooper C. Osteoporosis. Lancet 2006; 367: 2010e2018.
4. Roy DK, O’Neill TW, Finn JD et al. Determinants of incident vertebral fracture in men and women: results
from the European Prospective Osteoporosis Study (EPOS). Osteoporosis International 2003; 14(1): 19e26.
5. O’Neill TW, Cooper C, Finn JD et al. Incidence of distal forearm fracture in British men and women.
Osteoporosis International 2001; 12: 555e558.
6. van Staa TP, Dennison EM, Leufkens HG & Cooper C. Epidemiology of fractures in England and Wales.
Bone 2001; 29(6): 517e522.
7. Sexson SB & Lehner JT. Factors affecting hip fracture mortality. Journal of Orthopaedic Trauma 1987; 1(4):
298e305.
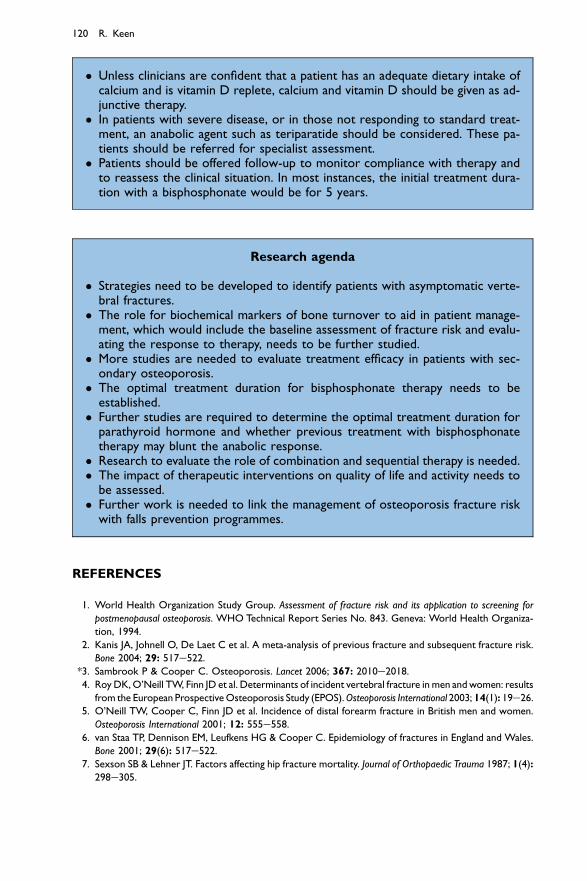
� Unless clinicians are confident that a patient has an adequate dietary intake ofcalcium and is vitamin D replete, calcium and vitamin D should be given as ad-junctive therapy.� In patients with severe disease, or in those not responding to standard treat-
ment, an anabolic agent such as teriparatide should be considered. These pa-tients should be referred for specialist assessment.� Patients should be offered follow-up to monitor compliance with therapy and
to reassess the clinical situation. In most instances, the initial treatment dura-tion with a bisphosphonate would be for 5 years.
Research agenda
� Strategies need to be developed to identify patients with asymptomatic verte-bral fractures.� The role for biochemical markers of bone turnover to aid in patient manage-
ment, which would include the baseline assessment of fracture risk and evalu-ating the response to therapy, needs to be further studied.� More studies are needed to evaluate treatment efficacy in patients with sec-
ondary osteoporosis.� The optimal treatment duration for bisphosphonate therapy needs to be
established.� Further studies are required to determine the optimal treatment duration for
parathyroid hormone and whether previous treatment with bisphosphonatetherapy may blunt the anabolic response.� Research to evaluate the role of combination and sequential therapy is needed.� The impact of therapeutic interventions on quality of life and activity needs to
be assessed.� Further work is needed to link the management of osteoporosis fracture risk
with falls prevention programmes.
Osteoporosis: prevention and management 121
8. Bonar SK, Tinetti ME, Speechley M & Cooney LM. Factors associated with short-versus longterm
skilled nursing facility placement among community-living hip fracture patients. Journal of the American
Geriatrics Society 1990; 38(10): 1139e1144.
9. Pluijm SM, Tromp AM, Smit JH et al. Consequences of vertebral deformities in older men and women.
Journal of Bone and Mineral Research 2000; 15(8): 1564e1572.
10. Oleksik A, Lips P, Dawson A et al. Health-related quality of life in postmenopausal women with low BMD
with or without prevalent vertebral fractures. Journal of Bone and Mineral Research 2000; 15(7): 1384e1392.
11. Cummings SR & Melton LJ. Epidemiology and outcomes of osteoporotic fracture. Lancet 2002; 359:
1761e1767.
12. European Commission. Report on Osteoporosis in the European Community: Action for Prevention. Luxem-
bourg: European Commission, 1998.
13. Ray NF, Chan JK, Thamer M & Melton III LJ. Medical expenditures for the treatment of osteoporotic
fractures in the United States in 1995: report from the National Osteoporosis Foundation. Journal of
Bone and Mineral Research 1997; 12(1): 24e35.
*14. Marshall D, Johnell O & Wedel H. Meta-analysis of how well measures of bone mineral density predict
occurrence of osteoporotic fractures. British Medical Journal 1996; 312: 1254e1259.
*15. Kanis J, Borgsrom F, De Lart C et al. Assessment of fracture risk. Osteoporosis International 2005; 16:
581e589.
16. Gregory L, Lowe C, Bates C et al. National Diet and Nutrition Survey: Young People aged 4 to 18 Years.
Volume 1: Report of the Diet and Nutrition Survey. London: The Stationery Office, 1998.
17. Finch S, Doyle W, Lowe C et al. National Diet and Nutrition Survey: People aged 65 Years or Over. Volume 1:
Report of the Diet and Nutrition Survey. London: The Stationery Office, 1998.
18. New SA, Robins SP, Campbell MK et al. Dietary influences on bone mass and bone metabolism: further
evidence of a positive link between fruit and vegetable consumption and bone health. American Journal of
Clinical Nutrition 2000; 71: 142e151.
19. Tucker KL, Hannan MT, Chen H et al. Potassium, magnesium, and fruit and vegetable intake are asso-
ciated with greater bone mineral density in elderly men and women. American Journal of Clinical Nutrition
1999; 69: 727e736.
20. Booth SL, Tucker KL, Chen H et al. Dietary vitamin K intakes are associated with hip fracture but not
with bone mineral density in elderly men and women. American Journal of Clinical Nutrition 2000; 71:
2504e2512.
21. Harris SS & Dawson-Hughes B. Caffeine and bone loss in healthy menopausal women. American Journal
of Clinical Nutrition 1994; 60: 573e578.
22. Law MR & Hackshaw AK. A meta-analysis of cigarette smoking, bone mineral density and risk of hip
fracture: recognition of a major effect. British Medical Journal 1997; 315: 841e846.
23. Feder G, Cryer C, Donovan S et al. Guidelines for the prevention of falls in people over 65. British Med-
ical Journal 2000; 321: 1007e1011.
24. Van Schoor NM, Deville WL, Bouter LM et al. Acceptance and compliance with external hip protec-
tors: a systemic review of the literature. Osteoporosis International 2002; 13: 917e924.
25. Sawka AM, Boulos P, Beattie K et al. Do hip protectors decrease the risk of hip fracture in institutional
and community-dwelling elderly? A systematic review and meta-analysis of randomized controlled tri-
als. Osteoporosis International 2005; 16: 1461e1474.
26. Dawson-Hughes B, Dallal GE, Krall EA et al. A controlled trial of the effect of calcium supplementation
on bone density in postmenopausal women. The New England Journal of Medicine 1990; 323: 878e883.
27. Reid IA, Ames RW, Evans MC et al. Effect of calcium supplementation on bone loss in postmenopausal
women. The New England Journal of Medicine 1993; 328: 460e464.
*28. Chapuy MC, Arlot ME, Delmas PD & Meunier PJ. Effect of calcium and cholecalciferol treatment for
three years on hip fracture in elderly women. British Medical Journal 1994; 308: 1081e1082.
*29. Grant AM, Avenell A, Campbell MK et al. Oral vitamin D3 and calcium for secondary prevention of
low-trauma fractures in elderly people (Randomised Evaluation of Calcium Or vitamin D, RECORD):
a randomised placebo-controlled trial. Lancet 2005; 365: 1621e1628.
30. Jackson RD, LaCroix AZ, Gass M et al. Calcium plus vitamin D supplementation and the risk of frac-
tures. The New England Journal of Medicine 2006; 354: 669e683.
31. Albright F, Smith PH & Richardson AM. Postmenopausal osteoporosis. Journal of the American Medical
Association 1941; 116: 2465e2474.
122 R. Keen
32. Torgerson DJ & Bell-Seyer SE. Hormone replacement therapy and prevention of vertebral fractures:
a meta-analysis of randomized trials. BMC Musculoskeletal Disorders 2001; 2: 7.
33. Torgerson DJ & Bell-Seyer SE. Hormone replacement therapy and prevention of nonvertebral fractures:
a meta-analysis of randomized trials. Journal of the American Medical Association 2001; 285: 2891e2897.
34. Rossouw JE, Anderson GL, Prentice RL et al. Risks and benefits of estrogen plus progestin in healthy
postmenopausal women: principal results from the Women’s Health Initiative randomized controlled
trial. Journal of the American Medical Association 2002; 288: 321e333.
35. Jackson RD, Wactawski-Wende J, LaCroix AZ et al. Effects of conjugated equine estrogen on risk of
fractures and BMD in postmenopausal women with hysterectomy: results from the Women’s Health
Initiative randomized trial. Journal of Bone and Mineral Research 2006; 21: 817e828.
36. Ettinger B, Black DM, Mitlak BH et al. Reduction of vertebral fracture risk in postmenopausal women
with osteoporosis treated with raloxifene: results from a 3 year randomized clinical trial. Journal of the
American Medical Association 1999; 282: 637e645.
37. Siris E, Harris ST, Eastell R et al. Skeletal effects of raloxifene after 8 years: results from the continuing
outcomes relevant to Evista (CORE) Study. Journal of Bone and Mineral Research 2005; 20: 1514e1524.
38. Storm T, Thamsborg G, Steiniche Tet al. Effect of intermittent cyclical etidronate therapy on bone mass
and fracture rate in women with postmenopausal osteoporosis. The New England Journal of Medicine
1990; 322: 1265e1271.
39. Harris ST, Watts NB, Jackson RD et al. Four-year study of intermittent cyclic etidronate treatment of
postmenopausal osteoporosis: three years of blinded therapy followed by one year of open therapy.
American Journal of Medicine 1993; 95: 557e567.
40. Cranney A, Guyatt G, Krolicki N et al. A meta-analysis of etidronate for the treatment of postmeno-
pausal osteoporosis. Osteoporosis International 2001; 12: 140e151.
*41. Black DM, Thompson DE, Bauer DC et al. Fracture risk reduction with aledronate in women with os-
teoporosis: the fracture intervention trial. The Journal of Clinical Endocrinology and Metabolism 2000; 85:
4118e4124.
42. Harris ST, Watts NB, Genat HK et al. Effects of risedronate treatment on vertebral and nonvertebral
fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Journal of the
American Medical Association 1999; 282: 1344e1352.
*43. McClung MR, Geusens P, Miller PD et al. Effect of risedronate on the risk of hip fracture in elderly
women. The New England Journal of Medicine 2001; 344: 333e340.
44. Chesnut 3rd CH, Skag A, Christiansen C et al. Effects of oral ibandronate administered daily or inter-
mittently on fracture risk in postmenopausal osteoporosis. Journal of Bone and Mineral Research 2004;
19: 1241e1249.
45. Bone HG, Hosking D, Devogelaer JP et al. Ten years’ experience with alendronate for osteoporosis in
postmenopausal women. The New England Journal of Medicine 2004; 350: 1189e1199.
46. Reid IR, Wattie DJ, Evans MC et al. Continuous therapy with pamidronate, a potent bisphosphonate, in
postmenopausal osteoporosis. The Journal of Clinical Endrocrinology and Metabolism 1994; 79: 1595e1599.
47. Reid IR, Brown JP, Burckhardt P et al. Intravenous zoledronic acid in postmenopausal women with low
bone mineral density. The New England Journal of Medicine 2002; 346: 653e661.
*48. National Institute for Clinical Excellence. Bisphosphonates (alendronate, etidronate, risedronate), selective
oestrogen receptor modulators (raloxifene) and parathyroid hormone (teriparatide) for the secondary prevention
of osteoporotic fragility fractures in postmenopausal women. Health Technology Appraisal 87. London:
NICE, 2005. Available at: http://www.nice.org.uk/TA087guidance.
49. Meunier PJ, Roux C, Seeman E et al. The effects of strontium ranelate on the risk of vertebral fracture in
women with postmenopausal osteoporosis. The New England Journal of Medicine 2004; 350: 459e468.
*50. Reginster JY, Seeman E, De Vernejoul MC et al. Strontium ranelate reduces the risk of nonvertebral
fractures in postmenopausal women with osteoporosis: Treatment of Peripheral Osteoporosis (TRO-
POS) study. The Journal of Clinical Endocrinology and Metabolism 2005; 90: 2816e2822.
*51. Neer RM, Arnaud CD, Zanchetta JR et al. Effect of parathyroid hormone (1-34) on fractures and bone
mineral density in postmenopausal women with osteoporosis. The New England Journal of Medicine
2001; 344: 1434e1441.
52. Chesnut 3rd CH, Silvermann S, Andriano K et al. A randomised trial of nasal spray salmon calcitonin in
postmenopausal osteoporosis: the prevent recurrence of osteoporotic fracture study. American Journal