Systematic review Communication in the operating theatre S.-M. Weldon 1 , T. Korkiakangas 1 , J. Bezemer 2 and R. Kneebone 1 1 Department of Surgery and Cancer, Imperial College London, and 2 Department of Culture, Communication and Media, Institute of Education, University of London, London, UK Correspondence to: Ms S.-M. Weldon, Division of Surgery, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, QEQM, St Mary’s Hospital, 10th Floor, South Wharf Road, London W2 1NY, UK (e-mail: [email protected]) Background: Communication is extremely important to ensure safe and effective clinical practice. A systematic literature review of observational studies addressing communication in the operating theatre was conducted. The focus was on observational studies alone in order to gain an understanding of actual communication practices, rather than what was reported through recollections and interviews. Methods: A systematic review of the literature for accessible published and grey literature was performed in July 2012. The following information was extracted: year, country, objectives, methods, study design, sample size, healthcare professional focus and main findings. Quality appraisal was conducted using the Critical Appraisal Skills Programme. A meta-ethnographic approach was used to categorize further the main findings under key concepts. Results: Some 1174 citations were retrieved through an electronic database search, reference lists and known literature. Of these, 26 were included for review after application of full-text inclusion and exclusion criteria. The overall quality of the studies was rated as average to good, with 77 per cent of the methodological quality assessment criteria being met. Six key concepts were identified: signs of effective communication, signs of communication problems, effects on teamwork, conditions for communication, effects on patient safety and understanding collaborative work. Conclusion: Communication was shown to affect operating theatre practices in all of the studies reviewed. Further detailed observational research is needed to gain a better understanding of how to improve the working environment and patient safety in theatre. Paper accepted 13 September 2013 Published online in Wiley Online Library (www.bjs.co.uk). DOI: 10.1002/bjs.9332 Introduction It is estimated that 234 million surgical procedures are performed globally each year 1 . In developed countries, where 73·6 per cent of procedures occur, 3 – 16 per cent end in morbidity, and of these 0·4–0·8 per cent are fatal 1 . The majority of surgical errors that contribute to morbidity and mortality can be attributed to communication breakdown 2,3 . The World Health Organization 4 states: ‘Problems associated with surgical safety in developed countries account for half of the avoidable adverse events that result in death or disability. The economic benefits of improving patient safety are compelling. Studies show that additional hospitalization, litigation costs, infections acquired in hospitals, lost income, disability and medical expenses have cost some countries between US$ 6 billion and US$ 29 billion a year’. Interprofessional communication plays an essential role in information transfer during operations and has relevance to patient safety 5–8 . The professionals working on operations include surgeons, anaesthetists, operating department practitioners and nurses, as well as surgical trainees, medical and nurse students. Increasingly, team members represent diverse backgrounds and have different levels of experience and expertise with regard to working in the operating theatre. Although a surgical operation depends on the technical skills of the operating surgeon, the operation itself is a social situation where many tasks are accomplished through communication between team members. Some health research has examined team communication between medical professionals through self-report methods such as interviews 9,10 and documentation 11 . Where direct observation has been used to describe the patterns of communication 12,13 , the communication has generally not been transcribed and analysed in any great detail. The aim of the present paper is to review systematically the studies that have addressed communication in the operating theatre. The objectives were: to identify current knowledge with regard to communication between healthcare professionals in an operating theatre; to assess 2013 British Journal of Surgery Society Ltd British Journal of Surgery 2013; 100: 1677–1688 Published by John Wiley & Sons Ltd
Transcript
Systematic review
Communication in the operating theatreS.-M. Weldon1, T. Korkiakangas1, J. Bezemer2 and R. Kneebone1
1Department of Surgery and Cancer, Imperial College London, and 2Department of Culture, Communication and Media, Institute of Education,University of London, London, UKCorrespondence to: Ms S.-M. Weldon, Division of Surgery, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, QEQM,St Mary’s Hospital, 10th Floor, South Wharf Road, London W2 1NY, UK (e-mail: [email protected])
Background: Communication is extremely important to ensure safe and effective clinical practice. Asystematic literature review of observational studies addressing communication in the operating theatrewas conducted. The focus was on observational studies alone in order to gain an understanding of actualcommunication practices, rather than what was reported through recollections and interviews.Methods: A systematic review of the literature for accessible published and grey literature was performedin July 2012. The following information was extracted: year, country, objectives, methods, study design,sample size, healthcare professional focus and main findings. Quality appraisal was conducted using theCritical Appraisal Skills Programme. A meta-ethnographic approach was used to categorize further themain findings under key concepts.Results: Some 1174 citations were retrieved through an electronic database search, reference lists andknown literature. Of these, 26 were included for review after application of full-text inclusion andexclusion criteria. The overall quality of the studies was rated as average to good, with 77 per cent of themethodological quality assessment criteria being met. Six key concepts were identified: signs of effectivecommunication, signs of communication problems, effects on teamwork, conditions for communication,effects on patient safety and understanding collaborative work.Conclusion: Communication was shown to affect operating theatre practices in all of the studiesreviewed. Further detailed observational research is needed to gain a better understanding of how toimprove the working environment and patient safety in theatre.Paper accepted 13 September 2013Published online in Wiley Online Library (www.bjs.co.uk). DOI: 10.1002/bjs.9332
Introduction
It is estimated that 234 million surgical procedures areperformed globally each year1. In developed countries,where 73·6 per cent of procedures occur, 3–16 per cent endin morbidity, and of these 0·4–0·8 per cent are fatal1. Themajority of surgical errors that contribute to morbidityand mortality can be attributed to communicationbreakdown2,3. The World Health Organization4 states:‘Problems associated with surgical safety in developedcountries account for half of the avoidable adverse eventsthat result in death or disability. The economic benefitsof improving patient safety are compelling. Studies showthat additional hospitalization, litigation costs, infectionsacquired in hospitals, lost income, disability and medicalexpenses have cost some countries between US$ 6 billionand US$ 29 billion a year’.
Interprofessional communication plays an essentialrole in information transfer during operations and hasrelevance to patient safety5–8. The professionals workingon operations include surgeons, anaesthetists, operating
department practitioners and nurses, as well as surgicaltrainees, medical and nurse students. Increasingly, teammembers represent diverse backgrounds and have differentlevels of experience and expertise with regard to workingin the operating theatre. Although a surgical operationdepends on the technical skills of the operating surgeon,the operation itself is a social situation where manytasks are accomplished through communication betweenteam members. Some health research has examinedteam communication between medical professionalsthrough self-report methods such as interviews9,10 anddocumentation11. Where direct observation has beenused to describe the patterns of communication12,13, thecommunication has generally not been transcribed andanalysed in any great detail.
The aim of the present paper is to review systematicallythe studies that have addressed communication in theoperating theatre. The objectives were: to identifycurrent knowledge with regard to communication betweenhealthcare professionals in an operating theatre; to assess
2013 British Journal of Surgery Society Ltd British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
1678 S.-M. Weldon, T. Korkiakangas, J. Bezemer and R. Kneebone
observational studies and explore the analytical methodsused for this approach; to map the key communicationbarriers that have been identified and how these may affectthe safety of a procedure; and to identify gaps in knowledgeand understanding.
Methods
A systematic review of the literature was performedfor accessible published and grey literature. Qualityappraisal was conducted using the Critical Appraisal SkillsProgramme14 as a guide.
Data sources
The following databases were searched in July 2012 usingkeywords and subject/medical subject heading (MeSH)terms: MEDLINE, Embase, PsycINFO (American Psy-chological Association, Washington, DC, USA), ProQuest,Web of Knowledge, International Bibliography of theSocial Sciences (IBSS) and Eldis. Grey literature wassearched using Eldis, including conference proceedingsand governmental publications. A hand reference searchof the available literature was performed, as well as theauthors’ own knowledge of the available literature and useof personal contacts. This was achieved by sending a listof the retrieved references to surgeons and nurses withthe request to check whether any relevant literature wasmissing.
Study selection
All citations from database searches were exported toEndNote version X5 (Thomson Reuters, New York,USA)15. Duplicates were removed. Two authors scannedall article titles and abstracts using an initial screeninginclusion flow chart. The first screening inclusion wasdeveloped in order to select only studies that addressed theoperating theatre environment, excluding other clinicalenvironments such as hospital wards and clinics. Second,the selected studies had to address communication betweenhealthcare professionals, thus excluding studies thatfocused on interactions between clinicians and patients,for example. Third, the selected studies had to reportobservational data, thus excluding studies based on self-reporting, documentation or interviews only. All languageswere included and translations sought where necessaryby either contacting the author directly or seekinga translator.
A second set of eligibility criteria was then used toscreen the full texts of the articles in more detail. Inclusion
criteria were: assesses communication between healthcareprofessionals within the operating theatre; reports obser-vational research (with qualitative or quantitative analysis).Exclusion criteria were: addresses communication betweenpatient and healthcare professionals; communication issuesthat arose but were not the focus of the study; surveys,documentation, interviews and focus group studies; stud-ies focusing on communication on wards and other clinicalsites separate from the operating theatre; studies of surgicalsimulation and education.
Each author’s final set of included articles wasthen compared and discrepancies were resolved throughdiscussion and clarification.
Data extraction
A data extraction form was created and piloted to ensure asystematic and fair retrieval of relevant information fromthe included studies. The form took into account thestudy year, country of origin, objectives, methods, studydesign, sample size, healthcare professional focus and mainfindings.
Two authors extracted data using the specified format.A consensus on discrepancies was reached throughdiscussion. Authors of the studies were contacted forfurther information, if not present in the paper.
Quality assessment
The Critical Appraisal Skills Programme14 was used toassess the quality of the studies. Two authors assessedeach study against the criteria, including rigour, methods,credibility and relevance. Discrepancies in the authors’assessments were discussed and mitigated. Owing to thesubjectivity of assessing qualitative studies, the tool shouldbe regarded only as indicative. Assessments were madeusing the information provided in the published paperonly. Assessment criteria for qualitative studies were notincluded in quantitative study appraisals and this wasreflected in the scoring.
Data synthesis
A meta-ethnography approach16 was used to synthesize thestudy data. This approach was chosen as it is designed togenerate new theories and explain the outcomes of a rangeof different methodological approaches. It is particularlyuseful when there is an emphasis on qualitative studies asit uses induction and interpretation.
Noblit and Hare16 provide a stepped approach tosynthesizing study outcomes. These include: deciding what
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
Communication in the operating theatre 1679
is relevant to the initial interest; reading the studies;determining how the studies are related; translating thestudies into one another; synthesizing translations; andexpressing the synthesis. From reading the includedstudies, key concepts were identified and second-orderinterpretations were taken directly from the studiesthemselves and associated with the relevant concept.By combining all of the interpretations under each keyconcept, third-order interpretations were turned into aform of hypothesis.
As a result of variation between the quantitative resultsobtained (some did counts of communication failureswhereas others measured time under different conditions),no synthesis or meta-analysis of the quantitative data couldbe performed, and therefore a descriptive table and shortnarrative of the results are presented.
Results
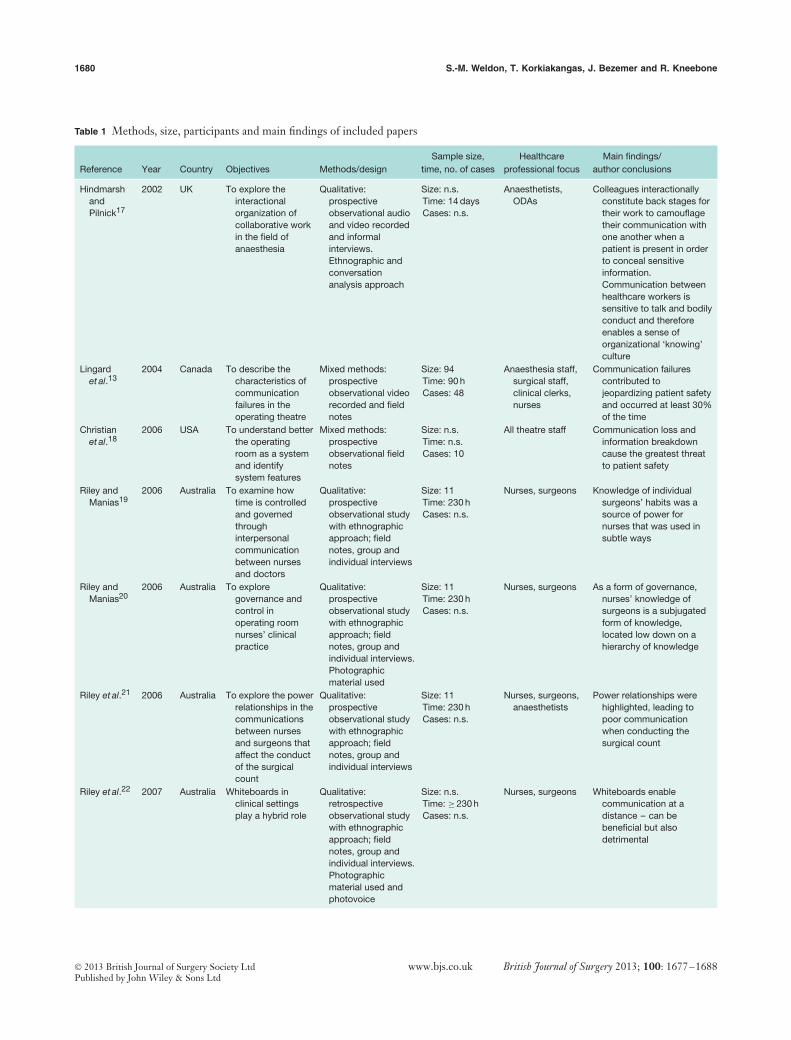
A total of 1174 citations were retrieved, 1165 citationsfrom the electronic search and nine from the referencelist hand-search. After removal of duplicates and papersthat did not meet the initial inclusion criteria, 36 articlesremained (Fig. 1). Application of the second screeningcriteria resulted in the inclusion of 26 studies and theexclusion of ten. Based on the information provided, the26 studies13,17–41 included a minimum of 584 researchparticipants, 1094 cases and 2200 observational hours(Table 1). Of the 26 studies, 19 were qualitative, two werequantitative and five mixed. Twenty were prospectiveobservational studies; of these, ten used audio/videorecordings, seven interview methods, six field notes,two photographs, one questionnaire and one assessmenttool. Most studies used a mix of approaches. A varietyof theatre staff healthcare professionals were observedacross studies, with nurses and surgeons dominating.All of the studies were undertaken in high-incomecountries, with the majority being from the UK,followed by Australia and the USA. Fourteen of theincluded studies had been published in a health-relatedjournal13,18–22,25,27–31,33,34, and five were in surgicaljournals18,25,29,30,34. Of the ten excluded studies42–51, mostwere excluded on the basis of focus on educationalinformation transfer or organizational structure rather thancommunication and interactions between individuals. Onewas excluded because it focused on overlapping job roles tocut costs42.
Quality appraisal results
Overall the quality of the studies was judged to beaverage to good, with 77 per cent of the methodological
Potentially relevant abstracts from databases, reference lists and known studies, identified and screened for
retrieval n = 1174
Articles retrieved for more detailed evaluation
n = 36
Abstracts excluded n = 1129 Duplicate n = 279 Did not meet all of the first inclusion criteria n = 850
Potentially appropriate articles to be included in meta-analysis and
meta-ethnography n = 26
Articles included in meta-ethnography n = 25
Articles that could be included in meta-analysis
n = 5
Articles with usable information, by outcome
n = 26
Articles excluded (did not meet second inclusion criteria) n = 10
Articles excluded from meta-ethnography (lack of depth) n = 1 Articles excluded from meta-analysis (no quantitative results) n = 21
Fig. 1 PRISMA diagram of articles selected for review
quality assessments being met (Fig. 2). A large proportionof studies did not meet the quality appraisal criteriawith regard to addressing the researcher/participantrelationship, declaring any commercial funding and ethicalconsiderations. This would have ensured there was nocommercial or participant/observer bias and that theresearch had been carried out ethically. This aspect needsto be addressed more often in observational studies. Onlythree studies17,18,41 met all of the quality appraisal criteria.
Meta-synthesis
Six key themes were identified throughout the resultssections of the included papers: signs of effectivecommunication; signs of communication problems; effectson teamwork; conditions for communication; effect onpatient safety; and understanding collaborative work(Table 2).
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
1680 S.-M. Weldon, T. Korkiakangas, J. Bezemer and R. Kneebone
Table 1 Methods, size, participants and main findings of included papers
Reference Year Country Objectives Methods/designSample size,
time, no. of casesHealthcare
professional focusMain findings/
author conclusions
HindmarshandPilnick17
2002 UK To explore theinteractionalorganization ofcollaborative workin the field ofanaesthesia
Qualitative:prospectiveobservational audioand video recordedand informalinterviews.Ethnographic andconversationanalysis approach
Size: n.s.Time: 14 daysCases: n.s.
Anaesthetists,ODAs
Colleagues interactionallyconstitute back stages fortheir work to camouflagetheir communication withone another when apatient is present in orderto conceal sensitiveinformation.Communication betweenhealthcare workers issensitive to talk and bodilyconduct and thereforeenables a sense oforganizational ‘knowing’culture
Lingardet al.13
2004 Canada To describe thecharacteristics ofcommunicationfailures in theoperating theatre
Mixed methods:prospectiveobservational videorecorded and fieldnotes
Communication failurescontributed tojeopardizing patient safetyand occurred at least 30%of the time
Christianet al.18
2006 USA To understand betterthe operatingroom as a systemand identifysystem features
Mixed methods:prospectiveobservational fieldnotes
Size: n.s.Time: n.s.Cases: 10
All theatre staff Communication loss andinformation breakdowncause the greatest threatto patient safety
Riley andManias19
2006 Australia To examine howtime is controlledand governedthroughinterpersonalcommunicationbetween nursesand doctors
Qualitative:prospectiveobservational studywith ethnographicapproach; fieldnotes, group andindividual interviews
Size: 11Time: 230 hCases: n.s.
Nurses, surgeons Knowledge of individualsurgeons’ habits was asource of power fornurses that was used insubtle ways
Riley andManias20
2006 Australia To exploregovernance andcontrol inoperating roomnurses’ clinicalpractice
Qualitative:prospectiveobservational studywith ethnographicapproach; fieldnotes, group andindividual interviews.Photographicmaterial used
Size: 11Time: 230 hCases: n.s.
Nurses, surgeons As a form of governance,nurses’ knowledge ofsurgeons is a subjugatedform of knowledge,located low down on ahierarchy of knowledge
Riley et al.21 2006 Australia To explore the powerrelationships in thecommunicationsbetween nursesand surgeons thataffect the conductof the surgicalcount
Qualitative:prospectiveobservational studywith ethnographicapproach; fieldnotes, group andindividual interviews
Size: 11Time: 230 hCases: n.s.
Nurses, surgeons,anaesthetists
Power relationships werehighlighted, leading topoor communicationwhen conducting thesurgical count
Riley et al.22 2007 Australia Whiteboards inclinical settingsplay a hybrid role
Qualitative:retrospectiveobservational studywith ethnographicapproach; fieldnotes, group andindividual interviews.Photographicmaterial used andphotovoice
Size: n.s.Time: ≥ 230 hCases: n.s.
Nurses, surgeons Whiteboards enablecommunication at adistance – can bebeneficial but alsodetrimental
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
Communication in the operating theatre 1681
Table 1 Continued
Reference Year Country Objectives Methods/designSample size,
Anaesthetists and nursesobtained the lowestscores on communication.In addition to low scoreson communication,surgeons’ teamworkbehaviours appeared todeteriorate as theprocedures were finished
Finn26 2008 UK To explore operatingtheatre teamworkdiscourse
Qualitative:retrospectiveobservational studywith ethnographicapproach; fieldnotes and interviews
The privileged position ofanaesthetists andsurgeons over nurses andODPs is legitimated andmaintained
Gardeziet al.27
2009 Canada To explore whetherthe use of astructuredchecklist for apreoperativebriefing was aneffective way tosupportcommunication inthe operatingtheatre
Qualitative:retrospectiveobservationalethnographic studyusing field notes
Size: 201Time: n.s.Cases: ≥ 700
Surgeons, nurses,anaesthetists
There are multiple andcomplex ways thatconstrain, and silentcommunication isproduced within theoperating theatre; beingaware of them may helphealth professionals tointerpret the multiplemodalities and strategiesof communication at play,in particular with regard tosilence
Riley andManias28
2009 Australia To provide anin-depthunderstandingabout gatekeepingpractices bynurses to highlightpowerrelationships
Qualitative:prospectiveobservationalethnographic studyusing single andgroup interviews,photographs anddiaries
Size: ≥ 11Time: 230 hCases: n.s.
Nurses, surgeons,anaesthetists
Gatekeeping acts caninfluence and shapeclinical practice and, moreimportantly, can impacton patient care
Zheng andSwanstrom29
2009 USA To examine teamcooperationamong surgeonsin a surgical teambuilt up withdifferent timelengths
Quantitative:prospectiveobservational study;video recorded
Size: 27Time: n.s.Cases: 59
Surgeons, assistantsurgeons, nurses,anaesthetists
Working in a team allowssurgeons to developsophisticated cognition toanticipate an upcomingtask and provideassistance without verbalcommunication
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
1682 S.-M. Weldon, T. Korkiakangas, J. Bezemer and R. Kneebone
Table 1 Continued
Reference Year Country Objectives Methods/designSample size,
time, no. of casesHealthcare
professional focusMain findings/
author conclusions
Zhenget al.30
2009 USA To record surgicalrelated activitiesperformed by thescrub nurse withdifferent levels ofexperience
Quantitative:prospectiveobservational study;video recorded
Size: 27Time: n.s.Cases: 28
Nurses Experienced nurses developsophisticated cognition,with anticipatorymovement and eye gazebeing two valuablebehavioural markers forassessing teamperformance
Bahl et al.31 2010 UK To define thenon-technicalsocial skills ofoperative vaginaldelivery tofacilitate transferof skills fromobstetrician totraineeobstetrician
Qualitative:prospectiveobservational study;interview and videorecorded
Size: 18Time: n.s.Cases: 30
Midwives,obstetricians
Explicitly defined skillstaxonomy could aidtrainees’ understanding ofthe non-technical skills tobe considered whenconducting an operativedelivery
Collin et al.32 2010 Finland To examine surgicaloperations asparticipatorypractices from theperspective ofinterprofessionallearning andpractice
Qualitative:prospectiveethnographicinterview and fieldnotes observationalstudy; videorecorded
Size: 23Time: n.s.Cases: n.s.
Nurses, surgeons,physicians
Interprofessional teamworkcan be implemented bycollegial support,transgressing professionalroles and sustaining aninclusive atmosphere
Finn et al.33 2010 UK To examine howteamworkphenomenonplays out inpractice
Teamwork discourse can beinstrumentally co-opted inthe reproduction of thevery occupationaldivisions it is designed toameliorate, or simplyignored when comparedwith other forms ofcollective identity
Mooreet al.34
2010 Australia The role of bodyorientation as atool forcommunication inthe operatingtheatre
Explicit coordinationprocesses were relied onin order to deal withnon-routine events duringteamwork
n.s., Not specified; ODA, operating department assistant; ODP, operating department practitioner.
Signs of effective communication
Several of the studies reported an underlying ‘knowing’between established staff members within the operatingtheatre17. This form of knowing is described as theteam member’s ability to interpret what is happening,or about to happen, with very little information beingprovided. It was recognized in most studies that thisarea was often overlooked owing to the difficulties inmeasuring such instances34. Where studies did try toidentify and interpret this form of communication, non-verbal communication was identified as the dominantfactor. For instance, anticipatory movements enablethe scrub nurse to interpret the next movements ofthe surgeon and pass the requested instruments in atimely manner. Non-technical skills such as anticipatorymovements, eye gaze and bodily orientations wererecognized as being more developed within establishedteams29–31.
This synthesis recognized the need for studies to lookat non-verbal communication and pinpoint which ofthese resources are most dominant and reliable in thecontribution to effective communication.
Signs of communication problems
The synthesized studies addressed not only what con-tributed to communication failures but also what enhancedcommunication within the operating theatre environment.Communication failures were identified in many of thestudies, from power relationships between healthcareprofessionals to the use of second-hand communicationtools, such as whiteboards22,24,27,31. Communicationproblems were attributed to a mixture of role identities(lack of clarity with regard to role), power relationshipsand conflicting ideas of appropriateness in communication.Communication appeared to be more effective whennon-technical skills such as meaning, negotiating andreasoning were used18,35.
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
1684 S.-M. Weldon, T. Korkiakangas, J. Bezemer and R. Kneebone
0
Clear statement of aims and objectives?
Is a qualitative methodology appropriate?
Appropriate research design?
Appropriate recruitment strategy?
Appropriate data collection methods?
Researcher/participant relationship considered?
Considered ethical issues?
Rigorous data analysis?
Clear statement of findings?
Value of research?
Was the study free of commercial funding?
Yes Unclear No
10 20 30 40 50
% of studies
60 70 80 90 100
Fig. 2 Critical Appraisal Skills Programme quality appraisal of included studies
Thus the studies recognized the importance ofmeasuring communication successes and failures, and theimportance of adjusting the environment and personalconduct to recognize them.
Effects on teamwork
Teamwork occurred in many different ways and was rec-ognized as often failing within operating theatres25. It wasidentified that teamwork is often hindered or complicatedby other forms of collective identity, such as role identities,thus jeopardizing an inclusive atmosphere28,33. Teamworkcoordination was seen as paramount in order for it to beeffective39,41. Interprofessional communication is a prereq-uisite of teamwork; without (effective) communication theteam cannot function.
Hierarchical structures and separate healthcare profes-sional identities can prohibit successful teamwork. Furtherresearch should explore how these forms of organizationalstructure have been dealt with in similar organizations,such as the military and aviation.
Conditions for communication
Power relationships within the operating theatreswere recognized as an important factor underlyingcommunication21,27,35. These forms of power include thenurses’ control over surgeons19, and the privileged posi-tions of surgeons and anaesthetists over the rest of theteam26. It was recognized that on occasions these formsof power contributed to team members feeling unable tospeak up when necessary, thus leading to unsafe prac-tice and reduced team effort26. One example where thishappened in particular was with regard to the surgicalcount. One of a nurse’s responsibilities is to ensure noth-ing is left inside a patient; however, if an environment iscreated where nurses do not feel they can ask the sur-geon to stop what they are doing during a count, unsafepractice ensues21. Safe atmospheres, in which people feelthey have the right and duty to speak up regardless ofjob role, were identified as a prominent aspect in needof change20.
This interpretation challenges the hierarchical environ-ment that exists in theatres, and highlights the need forchange in communication between professions.
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
Communication in the operating theatre 1685
Table 2 Meta-ethnography concepts and interpretations
Signs of effective communication Established teams allow more non-verbalcommunication29; anticipatory movement and eyegaze increase with experience30; non-technicalskills31; intentions identified by particularmovements or bodily orientations34; organizational‘knowing’ culture17
Teams that are well established communicate onan increased level, using less verbalcommunication and more anticipatorymovements such as eye gaze and positioning
Signs of communication problems Communication loss, information breakdown18; poorcommunication27; communication throughwhiteboards22; case-irrelevant communication,small talk24; silence27; non-technical skills31;meaning to be negotiated in situ35; practice ispermeated with ordinary forms of reasoning andaction37
Communication failure, loss and breakdowns canbe exemplified by irrelevant talk, silences,power relationships and second-handcommunication methods. By understanding theoperating theatre’s culture of reasoning andaction through understanding verbal andnon-verbal communication, practitioners canfine-tune their communication skills to suit theenvironment
Effects on teamwork Surgeons’ teamwork deteriorates near end ofprocedure, and nurses and anaesthetists score lowfor teamwork25; need to sustain an inclusiveatmosphere32; teamwork can be ignored whencompared with other forms of collective identity33;in order for teamwork-distributed activities to bemanaged, the coordination of people, technologiesand objects is required39; explicit coordinationprocesses were relied on in order to deal withnon-routine events during teamwork41
Communication within teamwork needs to bemaintained to ensure successful proceduresand patient safety. Teamwork is recognized asoften unsatisfactory within operating theatresand deteriorates as time goes on. Banishingseparate professional identities andencouraging inclusive atmospheres canimprove teamwork. This can be achievedthrough coordination and training
Conditions for communication Nurses’ power over surgeons19; powerrelationships21; hierarchy of knowledge20;surgeons’ and anaesthetists’ privileged positionsover nurses and ODPs26; silence27; open,participatory power structures needed35
Power relationships are prominent within theoperating theatre. Power relationships are seenacross all disciplines of the operating theatreand generally relate to a hierarchy ofknowledge. Power relationships cause fear andsilences, which can in turn relate to unsafepractice. In relation to a changing society,structures need to be challenged
Effects on patient safety Communication failure a threat to safety13; poorlyconducted surgical counts owing to powerrelationships21; gatekeeping practices impact onpatient care28; understanding non-technical skillscould potentially prevent morbidity and improvepatient experience31
Communication failures through powerrelationships, gatekeeping practices andhierarchy issues all impact on patient safety.Learning to understand the non-technical skillsof the operating theatre has the potential toimprove patient safety
Understanding collaborative work Seemingly simple tasks23; anticipatory movementand eye gaze30; non-technical skills31; intentionsidentified by particular movements or bodilyorientations34; social interactions betweensurgeons and nurses are analytically inseparablefrom the technical demands of their work36;procedure both determines and is determined byits object38; in multiactivity, talk and other actionscan project parallel sequential constraints that canbe responded to simultaneously or successively40
Non-technical skills between healthcareprofessionals in the operating theatre areinseparable from the technical demands of thetask and therefore the need to understandthese interactions is just as important. Byobserving not just talk but other bodily actionsand behaviours, a more complete picture ofoperating theatre culture can be created
ODP, operating department practitioner.
Effects on patient safety
Most studies suggested that patient safety is partlycontingent on communication13,28,31. Seemingly simpletasks such as the surgical count can become compromisedif the task is not communicated effectively21. Patient safetyshould be at the forefront of any procedure, and even thesimple and mundane practices should be taken seriously ifthey compromise this.
Understanding collaborative work
Although it is important to gather information aboutthe outcomes of work in the operating theatre forpatients and staff, the studies reviewed also recognizedthe need to understand in detail the processes, includingthe complex communication patterns, that lead to thoseoutcomes. In almost all of the studies, it was recognizedthat communication skills play just as important a
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
1686 S.-M. Weldon, T. Korkiakangas, J. Bezemer and R. Kneebone
Table 3 Basic description of quantified study measurements andoutcomes
Metric Outcome
Communication failure Occurred at least 30% of the time13
Verbal exchanges Anaesthetists and nurses obtainedlowest scores on communication25
Anticipatory movements(surgeons)
More anticipatory movements wereperformed in dedicated teams thanin developing teams; however, thishad no significant effect onprocedure duration29
Anticipatory movements(nurses)
Experienced nurses spent less timewatching the procedures butperformed more anticipatorymovements30
Case-irrelevantcommunication
Small-talk accounted for more thanhalf of case-irrelevantcommunication24
role with regard to a clinical task as do technicalskills30,34,36,41. However, although this is recognized, itis often overlooked, and technical skills are the focusof improvement or training needs30. Intentions andmisunderstandings can be understood best when lookingat collaborative work through an observational lens23.Seemingly mundane actions such as eye gaze, anticipatorymovements and gestures can often be overlooked30,although they can give better insight into how cliniciansactually organize and accomplish collaborative work in theoperating theatre40.
Quantified narrative
Table 3 provides a description of the quantitative resultsobtained from the observational studies. The resultsare few, and use different measures; therefore a meta-analysis could not be performed. Although they indicatethe frequency of communication issues within theoperating theatre, they provide limited detail of theactual contexts in which these practices occur, and howthey might be changed. However, they do highlight thatcommunication failures can have important implicationsfor effective and safe surgical outcomes. Case-irrelevantcommunication was also seen as dominant within the typesof communication; this can have particular implications forcommunication during surgical operations.
Discussion
Communication plays a crucially important and complexrole in the operating theatre. It is shaped by organizationalculture, and non-verbal resources are just as relevantfor effective communication. The tacit knowledge/skills
underlying the use of non-verbal communication could beexamined by observing practitioners at work. Once madeexplicit, they can inform important debates about waysto improve clinical practice and feed into training andeducation.
Considering the volume of communication failuresreported, communication ought to be investigated andrecognized as an important area for training andprofessional development. Addressing communicationbetween healthcare professionals complements growingattention to doctor–patient communication, for instance inthe undergraduate medical curriculum. Without effectivecommunication to create inclusive environments, andcoordinate the multiplicity of tasks involved in surgery,teamwork cannot be successful.
The themes that have emerged from the synthesizedstudies could determine further research by testing thefollowing hypothesis: by understanding the operating the-atre’s culture of reasoning and action through understand-ing verbal and non-verbal cues, practitioners can fine-tunetheir communication skills to suit the environment andcolleagues’ conduct within it; discouraging separate pro-fessional identities and encouraging inclusive atmospherescan improve teamwork. This can be achieved throughcoordination and training. Communication impacts onpatient safety, which can be improved by developing inter-professional communication skills; non-technical skills areinseparable from the technical skills demanded by the taskand therefore the need to understand these interactions isjust as important. By observing, not just talk, but otherbodily actions and behaviours, a more complete picture ofoperating theatre culture is created. Power relationshipsaffect communication in the operating theatre; power rela-tionships can prevent junior staff from speaking up, in turnrelating to unsafe practice.
In spite of growing acknowledgement of its implicationsfor patient safety, communication in the operating theatreis under-researched: only 26 studies were found thataddressed communication through observation of workpractices in the operating theatre. These studies, althoughall observational, differed in approach and methods, makingit difficult to draw comparisons and conclusions. Videoanalysis of observed communication could be used toidentify what communication behaviours are likely tobe effective or ineffective, as video enables a repeatedaccess to the occurring practices and captures in detailthe range of ways in which professionals communicate.Those details cannot be recorded in note-taking on-the-spot and are rarely articulated by healthcare professionals ininterviews. Many of the generated interpretations resonatewith non-observational studies, such as that of a study
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
Communication in the operating theatre 1687
by Belyansky and colleagues52: ‘Our findings indicatethat resident attending intraoperative communicationcan prevent adverse patient events. Trainees often feelimpaired in voicing their concerns to their attendings.Strategies that improve resident attending communicationintraoperatively are needed as they are likely to enhancepatient safety’.
Communication in the operating theatre is not onlyunder-researched, it also receives disproportionately littleattention in the academic surgical community; of the 26studies reviewed, only five were published in a surgicaljournal, with only one of these being qualitative. Thus,the small body of research does not currently reach one ofits key audiences through one of their major informationchannels. A particular focus should be placed on the types ofmethod adopted for this kind of research in order to allowbetter synthesis of results and therefore stronger inferences,which could lead to the development of education andtraining in this undervalued area of surgical performance.By understanding this subject in greater detail, furtherresearch and training based on data-grounded evidence-based research could be developed that would improveboth the working environment and patient safety.
Acknowledgements
This review was funded by the Economic and SocialResearch Council (grant reference: RES-062-23-3219) aspart of an ongoing research project on communication inthe operating theatre.Disclosure: The authors declare no conflict of interest.
References
1 Weiser TG, Regenbogen SE, Thompson KD, Haynes AB,Lipsitz SR, Berry WR et al. An estimation of the globalvolume of surgery: a modelling strategy based on availabledata. Lancet 2008; 372: 139–144.
2 Makary MA, Mukherjee A, Sexton JB, Syin D, Goodrich E,Hartmann E et al. Operating room briefings and wrong-sitesurgery. J Am Coll Surg 2007; 204: 236–243.
3 Lingard L, Regehr G, Espin S, Whyte S. A theory-basedinstrument to evaluate team communication in the operatingroom: balancing measurement authenticity and reliability.Qual Saf Health Care 2006; 15: 422–426.
4 World Health Organization. 10 Facts on Patient Safety; 2012.http://www.who.int/features/factfiles/patient_safety/en/index.html [accessed 5 September 2012].
5 Adams JG, Bohan JS. System contributions to error. AcadEmerg Med 2000; 7: 1189–1193.
6 Donchin Y, Gopher D, Olin M, Badihi Y, Biesky M, SprungCL et al. A look into the nature and causes of human errorsin the intensive care unit. Crit Care Med 1995; 23: 294–300.
7 Schaefer HG, Helmreich RL. The importance of humanfactors in the operating room. Anesthesiology 1994; 80: 479.
8 Wilson RM, Runciman WB, Gibberd RW, Harrison BT,Newby L, Hamilton JD. The Quality in Australian HealthCare Study. Med J Aust 1995; 163: 458–471.
9 Spafford MM, Lingard L, Schryer CF, Hrynchak PK.Tensions in the field: teaching standards of practice inoptometry case presentations. Optom Vis Sci 2004; 81:800–806.
10 Knifed E, Goyal A, Bernstein M. Moral angst for surgicalresidents: a qualitative study. Am J Surg 2010; 199:571–576.
11 Greenberg CC, Regenbogen SE, Studdert DM, Lipsitz SR,Rogers SO, Zinner MJ et al. Patterns of communicationbreakdowns resulting in injury to surgical patients. J Am CollSurg 2007; 204: 533–540.
12 Lingard L, Reznick R, Espin S, Regehr G, DeVito I. Teamcommunications in the operating room: talk patterns, sitesof tension, and implications for novices. Acad Med 2002; 77:232–237.
13 Lingard L, Espin S, Whyte S, Regehr G, Baker GR,Reznick R et al. Communication failures in the operatingroom: an observational classification of recurrent types andeffects. Qual Saf Health Care 2004; 13: 330–334.
14 Critical Appraisals Skills Programme. Qualitative Research:Appraisal Tool. 10 Questions to Help You Make Sense ofQualitative Research. Public Health Resource Unit: Oxford,2006.
15 Thomson Reuters. EndNote X5; 2011.http://endnote.com/ [accessed 21 September 2013]
17 Hindmarsh J, Pilnick A. The tacit order of teamwork:collaboration and embodied conduct in anesthesia. TheSociological Quarterly 2002; 43: 139–164.
18 Christian CK, Gustafson ML, Roth EM, Sheridan TB,Gandhi TK, Dwyer K et al. A prospective study of patientsafety in the operating room. Surgery 2006; 139: 159–173.
19 Riley R, Manias E. Governing time in operating rooms. JClin Nurs 2006; 15: 546–553.
20 Riley RG, Manias E. Governance in operating roomnursing: nurses’ knowledge of individual surgeons. Soc SciMed 2006; 62: 1541–1551.
21 Riley R, Manias E, Polglase A. Governing the surgical countthrough communication interactions: implications forpatient safety. Qual Saf Health Care 2006; 15: 369–374.
22 Riley R, Forsyth R, Manias E, Iedema R. Whiteboards:mediating professional tensions in clinical practice. CommunMed 2007; 4: 165–175.
23 Sanchez Svensson M, Heath C, Luff P. Instrumental action:the timely exchange of implements during surgicaloperations. In ECSCW 2007: Proceedings of the 10th EuropeanConference on Computer-Supported Cooperative Work, Limerick,Ireland, 24–28 September 2007, Bannon LJ, Wagner I,
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd
1688 S.-M. Weldon, T. Korkiakangas, J. Bezemer and R. Kneebone
Gutwin C, Harper THR, Schmidt K (eds). Springer:London, 2007; 41–60.
24 Sevdalis N, Healey AN, Vincent CA. Distractingcommunications in the operating theatre. J Eval Clin Pract2007; 13: 390–394.
25 Undre S, Sevdalis N, Healey AN, Darzi A, Vincent CA.Observational teamwork assessment for surgery (OTAS):refinement and application in urological surgery. World JSurg 2007; 31: 1373–1381.
26 Finn R. The language of teamwork: reproducingprofessional divisions in the operating theatre. HumanRelations 2008; 61: 103–130.
27 Gardezi F, Lingard L, Espin S, Whyte S, Orser B, BakerGR. Silence, power and communication in the operatingroom. J Adv Nurs 2009; 65: 1390–1399.
28 Riley R, Manias E. Gatekeeping practices of nurses inoperating rooms. Soc Sci Med 2009; 69: 215–222.
29 Zheng B, Swanstrom LL. Video analysis of anticipatorymovements performed by surgeons during laparoscopicprocedures. Surg Endosc 2009; 23: 1494–1498.
30 Zheng B, Taylor MD, Swanstrom LL. An observationalstudy of surgery-related activities between nurses andsurgeons during laparoscopic surgery. Am J Surg 2009; 197:497–502.
31 Bahl R, Murphy DJ, Strachan B. Non-technical skills forobstetricians conducting forceps and vacuum deliveries:qualitative analysis by interviews and video recordings. Eur JObstet Gynecol Reprod Biol 2010; 150: 147–151.
32 Collin K, Paloniemi S, Mecklin J-P. Promotinginter-professional teamwork and learning – the case of asurgical operating theatre. Journal of Education and Work2010; 23: 43–63.
33 Finn R, Learmonth M, Reedy P. Some unintended effects ofteamwork in healthcare. Soc Sci Med 2010; 70:1148–1154.
34 Moore A, Butt D, Ellis-Clarke J, Cartmill J. Linguisticanalysis of verbal and non-verbal communication in theoperating room. ANZ J Surg 2010; 80: 925–929.
35 Bezemer J, Cope A, Kress G, Kneebone R. ‘Do you haveanother Johan?’ Negotiating meaning in the operatingtheatre. Applied Linguistics Review 2011; 2: 313–334.
36 Bezemer J, Murtagh G, Cope A, Kress G, Kneebone R.‘Scissors, please’: the practical accomplishment of surgicalwork in the operating theater. Symbolic Interaction 2011; 34:398–414.
37 Koschmann T, Zemel A. ‘So that’s the ureter.’ The informallogic of discovering work. Ethnographic Studies 2011; 12:31–46.
38 Koschmann T, LeBaron C, Goodwin C, Feltovich P. ‘Canyou see the cystic artery yet?’ A simple matter of trust.Journal of Pragmatics 2011; 43: 521–541.
39 Mondada L. [Coordinating actions in the operating theatre.The creation of a common space of vision, action and
participation in the interaction.] Etnografia e RicercaQualitativa 2011; 4: 9–38.
40 Mondada L. Operating together through videoconference:members’ procedures for accomplishing a common space ofaction. In Orders of Ordinary Action: REspecting SociologicalKnowledge, Hester A, Francis D (eds). Ashgate: Aldershot,2011; 51–67.
41 Schraagen JM. Dealing with unforeseen complexity in theOR: the role of heedful interrelating in medical teams.Theoretical Issues in Ergonomics Science 2011; 12: 256–272.
42 Koschmann T, LeBaron C, Goodwin C, Zemel A,Dunnington G. Formulating the Triangle of Doom: LeGeste dans son Contexte. 2nd Conference of the InternationalSociety for Gesture Studies (ISGS), Lyons, 2004.
43 Timmons S, Tanner J. A disputed occupational boundary:operating theatre nurses and operating departmentpractitioners. Sociol Health Illn 2004; 26: 645–666.
44 Hazlehurst B, McMullen CK, Gorman PN. Distributedcognition in the heart room: how situation awareness arisesfrom coordinated communications during cardiac surgery. JBiomed Inform 2007; 40: 539–551.
45 Hindmarsh J, Pilnick A. Knowing bodies at work:embodiment and ephemeral teamwork in anaesthesia.Organization Studies 2007; 28: 1395–1416.
46 ElBardissi AW, Wiegmann DA, Henrickson S, Wadhera R,Sundt TM III. Identifying methods to improve heartsurgery: an operative approach and strategy forimplementation on an organizational level. Eur JCardiothorac Surg 2008; 34: 1027–1033.
47 Manser T, Howard SK, Gaba DM. Adaptive coordination incardiac anaesthesia: a study of situational changes incoordination patterns using a new observation system.Ergonomics 2008; 51: 1153–1178.
48 Zheng B, Martinec DV, Cassera MA, Swanstrom LL. Aquantitative study of disruption in the operating roomduring laparoscopic antireflux surgery. Surg Endosc 2008; 22:2171–2177.
49 Undre S, Sevdalis N, McDermott J, Giddie J, Dinner L,Smith G. Interruptions, teamwork, and safety in theoperating room: a prospective quantitative study inurological surgery. Eur Urol Suppl 2011; 10: 60.
50 Zemel A, Koschmann T, LeBaron C. Pursuing a response:prodding recognition and expertise within a surgical team.In Embodied Interaction: Language and Body in the MaterialWorld, Streeck J, Goodwin C, LeBaron C (eds). CambridgeUniversity Press: Cambridge, 2011; 227–242.
51 Svensson MS, Luff P, Heath C. Embedding instruction inpractice: contingency and collaboration during surgicaltraining. Sociol Health Illn 2009; 31: 889–906.
52 Belyansky I, Martin TR, Prabhu AS, Tsirline VB, HowleyLD, Phillips R et al. Poor resident-attending intraoperativecommunication may compromise patient safety. J Surg Res2011; 171: 386–394.
2013 British Journal of Surgery Society Ltd www.bjs.co.uk British Journal of Surgery 2013; 100: 1677–1688Published by John Wiley & Sons Ltd




















![viewsyndrome*[ot] OR motor development disorder*[ot] OR Stereotypic Movement Disorder*[ot] OR Body Rocking[ot] OR Body-Focused Repetitive Behavio*[ot] OR Head Banging[ot] OR trichotillomania[ot] OR Tic Disorder*[ot] OR ...](https://static.documents.pub/doc/80x56/5b0593dc7f8b9ad1768b921d/viewsyndromeot-or-motor-development-disorderot-or-stereotypic-movement-disorderot.jpg)






