3
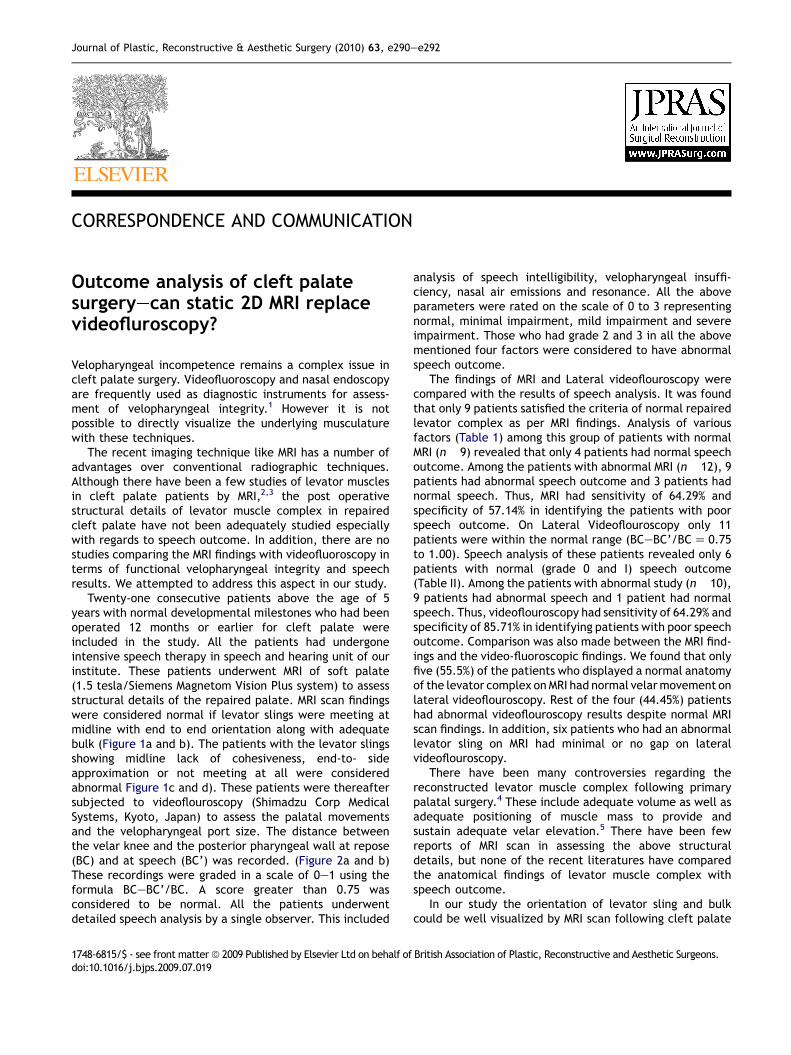
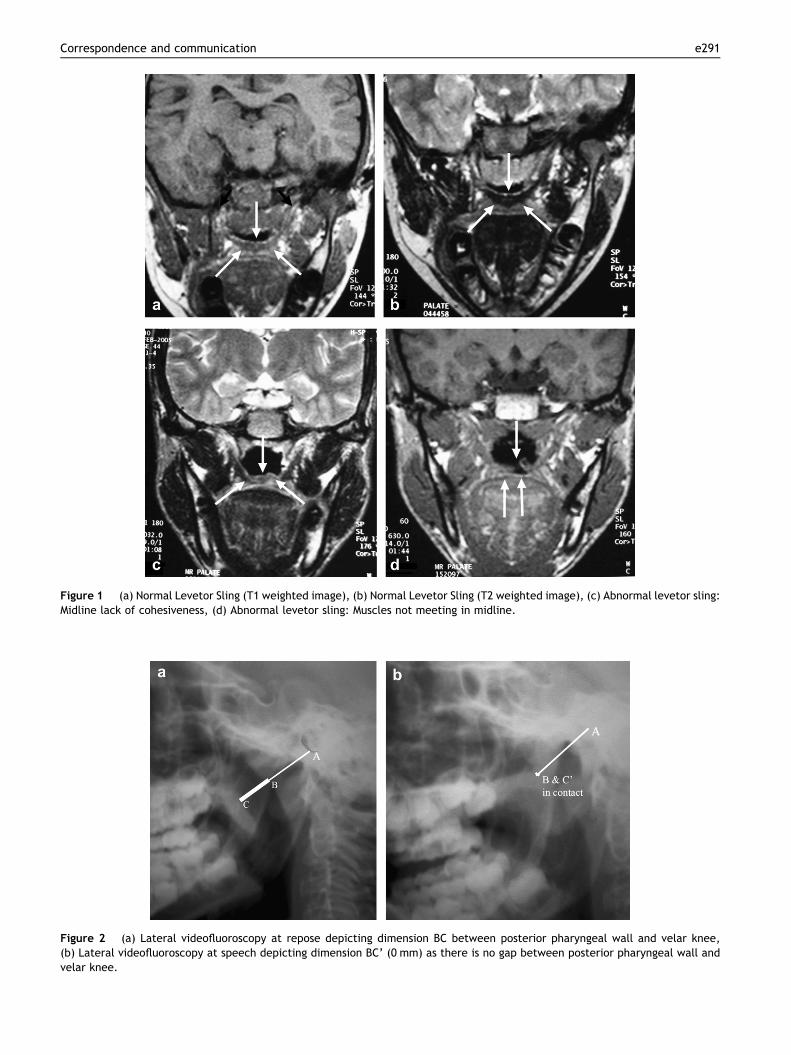
CORRESPONDENCE AND COMMUNICATION Outcome analysis of cleft palate surgeryecan static 2D MRI replace videofluroscopy? Velopharyngeal incompetence remains a complex issue in cleft palate surgery. Videofluoroscopy and nasal endoscopy are frequently used as diagnostic instruments for assess- ment of velopharyngeal integrity. 1 However it is not possible to directly visualize the underlying musculature with these techniques. The recent imaging technique like MRI has a number of advantages over conventional radiographic techniques. Although there have been a few studies of levator muscles in cleft palate patients by MRI, 2,3 the post operative structural details of levator muscle complex in repaired cleft palate have not been adequately studied especially with regards to speech outcome. In addition, there are no studies comparing the MRI findings with videofluoroscopy in terms of functional velopharyngeal integrity and speech results. We attempted to address this aspect in our study. Twenty-one consecutive patients above the age of 5 years with normal developmental milestones who had been operated 12 months or earlier for cleft palate were included in the study. All the patients had undergone intensive speech therapy in speech and hearing unit of our institute. These patients underwent MRI of soft palate (1.5 tesla/Siemens Magnetom Vision Plus system) to assess structural details of the repaired palate. MRI scan findings were considered normal if levator slings were meeting at midline with end to end orientation along with adequate bulk (Figure 1a and b). The patients with the levator slings showing midline lack of cohesiveness, end-to- side approximation or not meeting at all were considered abnormal Figure 1c and d). These patients were thereafter subjected to videoflouroscopy (Shimadzu Corp Medical Systems, Kyoto, Japan) to assess the palatal movements and the velopharyngeal port size. The distance between the velar knee and the posterior pharyngeal wall at repose (BC) and at speech (BC’) was recorded. (Figure 2a and b) These recordings were graded in a scale of 0e1 using the formula BCeBC’/BC. A score greater than 0.75 was considered to be normal. All the patients underwent detailed speech analysis by a single observer. This included analysis of speech intelligibility, velopharyngeal insuffi- ciency, nasal air emissions and resonance. All the above parameters were rated on the scale of 0 to 3 representing normal, minimal impairment, mild impairment and severe impairment. Those who had grade 2 and 3 in all the above mentioned four factors were considered to have abnormal speech outcome. The findings of MRI and Lateral videoflouroscopy were compared with the results of speech analysis. It was found that only 9 patients satisfied the criteria of normal repaired levator complex as per MRI findings. Analysis of various factors (Table 1) among this group of patients with normal MRI (n 9) revealed that only 4 patients had normal speech outcome. Among the patients with abnormal MRI (n 12), 9 patients had abnormal speech outcome and 3 patients had normal speech. Thus, MRI had sensitivity of 64.29% and specificity of 57.14% in identifying the patients with poor speech outcome. On Lateral Videoflouroscopy only 11 patients were within the normal range (BCeBC’/BC Z 0.75 to 1.00). Speech analysis of these patients revealed only 6 patients with normal (grade 0 and I) speech outcome (Table II). Among the patients with abnormal study (n 10), 9 patients had abnormal speech and 1 patient had normal speech. Thus, videoflouroscopy had sensitivity of 64.29% and specificity of 85.71% in identifying patients with poor speech outcome. Comparison was also made between the MRI find- ings and the video-fluoroscopic findings. We found that only five (55.5%) of the patients who displayed a normal anatomy of the levator complex on MRI had normal velar movement on lateral videoflouroscopy. Rest of the four (44.45%) patients had abnormal videoflouroscopy results despite normal MRI scan findings. In addition, six patients who had an abnormal levator sling on MRI had minimal or no gap on lateral videoflouroscopy. There have been many controversies regarding the reconstructed levator muscle complex following primary palatal surgery. 4 These include adequate volume as well as adequate positioning of muscle mass to provide and sustain adequate velar elevation. 5 There have been few reports of MRI scan in assessing the above structural details, but none of the recent literatures have compared the anatomical findings of levator muscle complex with speech outcome. In our study the orientation of levator sling and bulk could be well visualized by MRI scan following cleft palate 1748-6815/$ - see front matter ª 2009 Published by Elsevier Ltd on behalf of British Association of Plastic, Reconstructive and Aesthetic Surgeons. doi:10.1016/j.bjps.2009.07.019 Journal of Plastic, Reconstructive & Aesthetic Surgery (2010) 63, e290ee292