34
Ovarian tumor Wei Jiang, M.D., Ph.D. Attending of Ob & Gyn Ob & Gyn Hospital, Fudan University 419 Fangxie Road, Shanghai [email protected] -----From textbook to application
| Date post: | 02-Jan-2016 |
| Category: |
Documents |
| Upload: | hu-stevens |
| View: | 62 times |
| Download: | 0 times |

Ovarian tumor
Wei Jiang, M.D., Ph.D.
Attending of Ob & GynOb & Gyn Hospital, Fudan University419 Fangxie Road, [email protected]
-----From textbook to application

Overview
Key points
Case discussion

What is the difference between cancer and tumor?
What do you think?

What is Cancer?
• Simplest definitionFrom the American Cancer Society
“ cancer is a group of diseases characterized by uncontrolled growth and spread of abnormal cells. If the spread is not controlled, it can result in death.”
• Tumor– Two types:
• Benign (non-cancerous) – not cancer!– Does not spread; it can eventually become malignant in
some cases.
• Malignant (cancerous) – this is cancer!– Has the potential to spread to other parts of body

5
Role of Cell Division in Cancer
Top = normal cell division
Bottom = unregulated cell division and tumor formation
Malignant
If tumor invades surrounding tissue
(cancerous)
Metastatic
If individual cells break away and start a new
tumor elsewhere(cancerous)
BenignIf tumor has no effect on
surrounding tissue (non-cancerous)
Image from the National Cancer Institute



Primary ovarian tumors
• Epithelial: serous; mucinous; endometroid- Benign- Borderline- Malignant
• Germ cell tumors
• Sex cord (gonadal stromal) tumors

Epithelial


EOC


Germ cell tumors



Sex cord tumors


Complications
Torsion 10%Torsion 10%
Rupture 1%Rupture 1%
InfectionInfection
MalignancyMalignancy


Case discussion
Case 1 A 23-year-old female presented to our hospital in April 2013 with m
onths history of increasing facial and truncal hair, acne. The patient had been amenorrheic for 2 years prior to the onset of her virilizing symptoms. In the recent one year, she was treated as Polycystic Ovary Syndrome (PCOS) in the local hospital, but the signs and symptoms were deteriorated
Physical examination revealed a 56kg, normotensive female with obvious facial hair and atrophy of the breasts. Excessive hair was present on her lower abdomen and thighs. Pelvic examination was notable for an enlarged clitoris and a 5cm right adnexal mass. Abdominal ultrasound identified a 64×52×51mm, solid, left ovarian tumor. Doppler evaluation of intratumoral blood vessels confirmed a low resistance to flow. No ascites or other abnormalities were present. A CT scan of the pelvis confirmed the ultrasound findings and detected no adrenal gland enlargement or tumor. Laboratory analysis revealed normal values of folicle stimulating hormone (FSH), luteinising hormone (LH), serum prolactin (PRL) and cortisol. Total serum testosterone was 3.68ng/ml (normal 0.15-0.51ng/ml),

Clinical thinking What is the most likely diagnosis?
What should be your next steps?
How would you confirm the diagnosis?
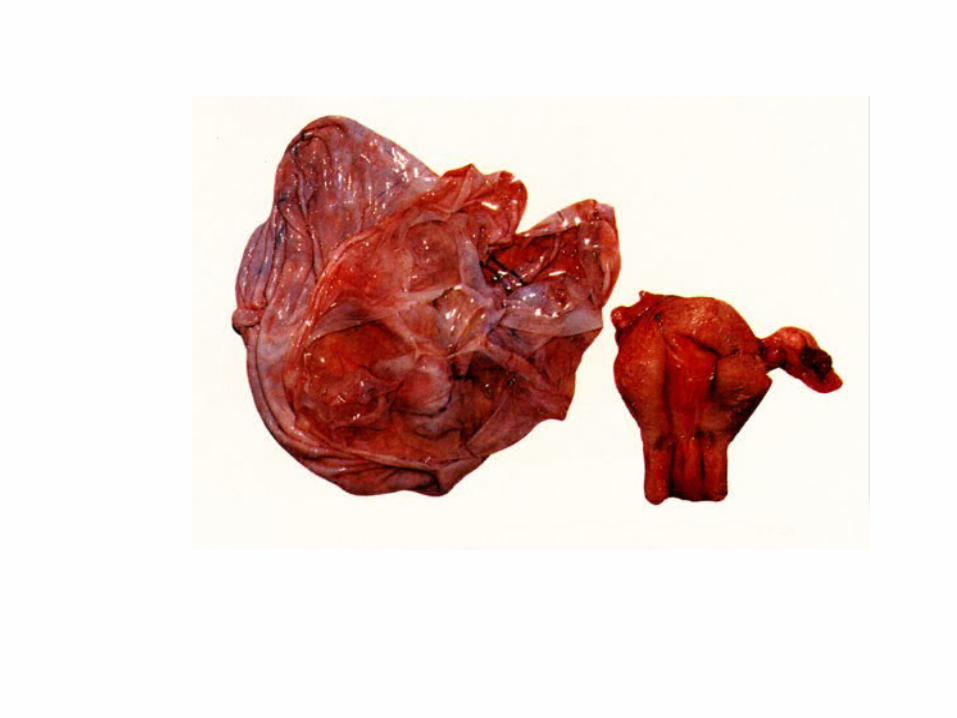
Laparoscopic examination
• Identified a 6×5×5cm, enlarged right ovary.
• Oophorocystectomy

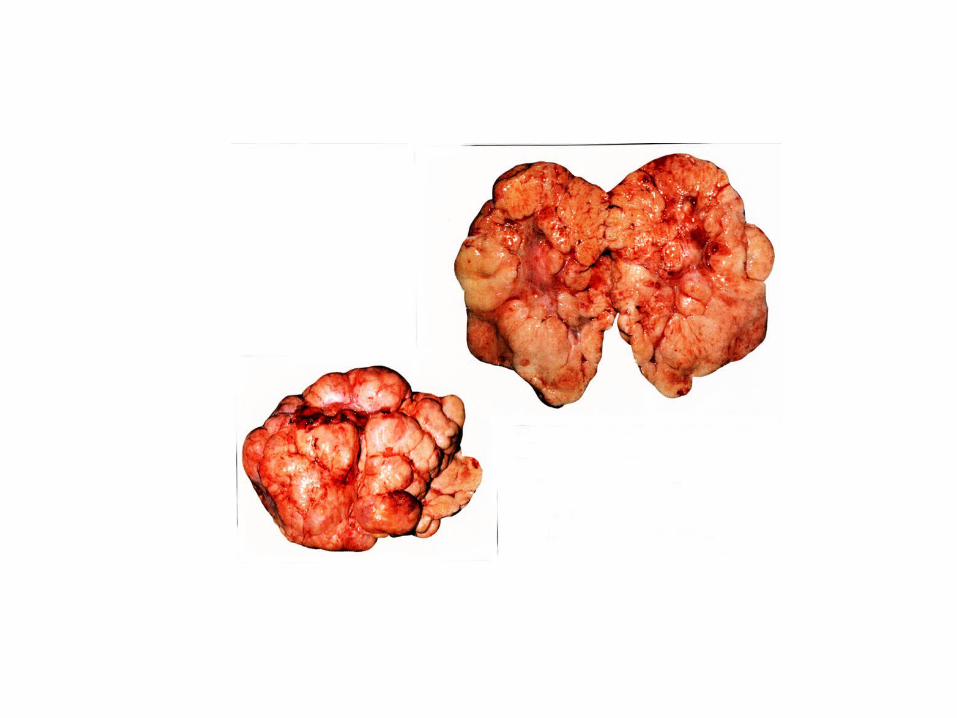
After operation………
• Pathological diagnosis: ovarian steroid cell tumor
• T: 1.02
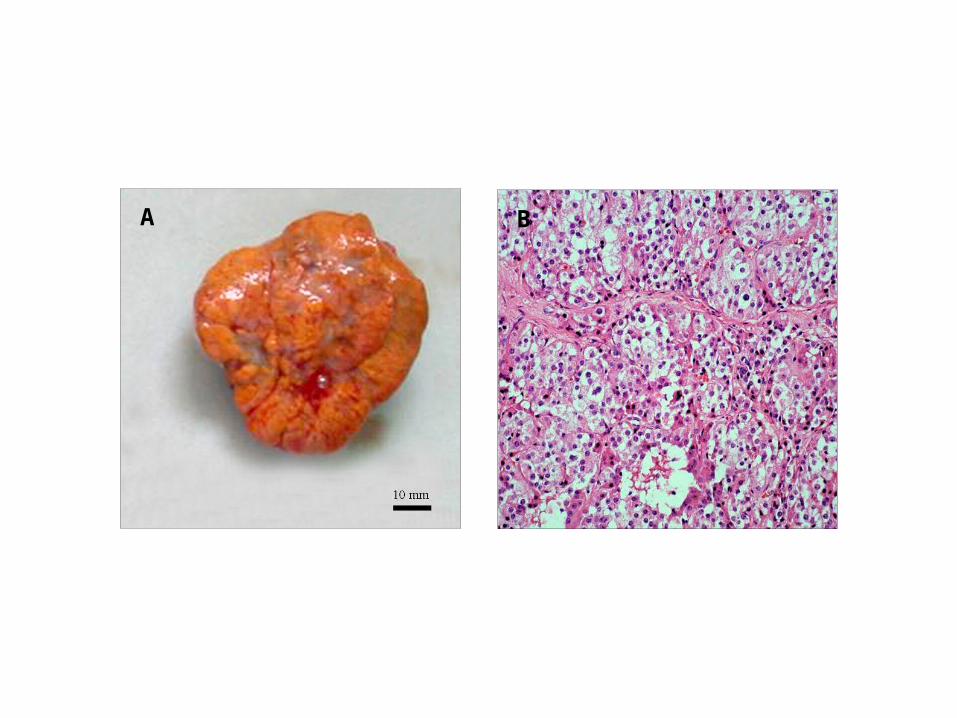
A B

Case 2• A 39-year-old, female, gravida 1, para 1, was admitted to a local hospital, co
mplaining of fatigue, anorexia, and abdominal swelling. Her medical history included nothing special. Physical examination revealed a palpable mass in the lower abdomen. A thoracoabdominal computed tomography (CT) scan showed marked pleural effusion and a heterogeneous mass, large ascites with many nodosity images in the pelvic wall.
• She was transferred to our hospital for further treatment. The patient’s serum CA 125 level was 1230.9U/mL, while CEA, AFP, CA 199, and CA 153 levels were within the normal range. Abdominal ultrasonography showed a heterogeneous, multiloculated mass, with a moderate amount of ascites, and subsequent transvaginal ultrasonography revealed a large complex pelvic mass, 16cm largest dimension, of probable adnexal origin. The uterus was normal in size. Abdominal paracentesis yielded 2 liters of yellow serous fluid consistent with an exudative process. Microscopy and cytology revealed only reactive mesothelial cells without malignant cells.
Clinical thinking – What is the most likely diagnosis?– What should be your next steps?– How would you confirm the diagnosis?

Chemotherapy?
Laparoscopy?Exploratory laparotomy?
Exploratory laparotomy
• Two rounds of TP– Ascites fall down– CA125: 820
• Operation– Ascites: clear, yellow– The uterus and left ovary was normal– Right ovary: A 20×18×15cm complex, multicystic mass, without
evidence of external excrescences

After operation…….
• CA125: 235
• Pathological diagnosis: Struma ovarii
Case 3
From ER:
A 32-year-old female presented with a sudden lower right abdominal pain

















