Overcoming Overcoming Addictions: Addictions: Skills Training for Skills Training for People with Schizophrenia People with Schizophrenia Thad A. Eckman, Ph.D. Thad A. Eckman, Ph.D. Program Director, Dual Diagnosis Program Director, Dual Diagnosis Treatment Program, West Los Treatment Program, West Los Angeles VA Medical Center Angeles VA Medical Center and and Associate Professor of Psychiatry Associate Professor of Psychiatry and Biobehavioral Sciences, UCLA and Biobehavioral Sciences, UCLA School of Medicine School of Medicine
Transcript
Overcoming Overcoming Addictions: Addictions: Skills Training for Skills Training for People with SchizophreniaPeople with Schizophrenia
Thad A. Eckman, Ph.D.Thad A. Eckman, Ph.D.Program Director, Dual Diagnosis Program Director, Dual Diagnosis Treatment Program, West Los Angeles Treatment Program, West Los Angeles VA Medical CenterVA Medical Center
andand
Associate Professor of Psychiatry and Associate Professor of Psychiatry and Biobehavioral Sciences, UCLA School of Biobehavioral Sciences, UCLA School of MedicineMedicine
Schizophrenia and Schizophrenia and AddictionAddiction Common comorbidityCommon comorbidity Creates special problems for:Creates special problems for:
– patientspatients– cliniciansclinicians– health care systemshealth care systems– social service agenciessocial service agencies
Special ProblemsSpecial Problems
Diagnostic uncertaintyDiagnostic uncertainty Poorly integrated treatmentPoorly integrated treatment High drop-out (and drop-in) rateHigh drop-out (and drop-in) rate Disability income facilitates drug Disability income facilitates drug
useuse Encumbered by serious Encumbered by serious
learning deficitslearning deficits
Comprehensive Dual Diagnosis Comprehensive Dual Diagnosis Treatment ProgramTreatment Program
Single clinical team treats both disorders in a Single clinical team treats both disorders in a single settingsingle setting
Acute inpatient care, day treatment and Acute inpatient care, day treatment and outpatient clinicoutpatient clinic
Incentive Program (modified token economy)Incentive Program (modified token economy) Assertive case managementAssertive case management Twice weekly urine testsTwice weekly urine tests Representative payees for money Representative payees for money
managementmanagement Skills trainingSkills training
BehavioralBehavioral Skills Training Skills Training ModulesModules
Symptom ManagementSymptom Management Medication ManagementMedication Management Successful LivingSuccessful Living Recreation for LeisureRecreation for Leisure Basic Conversation SkillsBasic Conversation Skills Social Problem SolvingSocial Problem Solving Friendship and IntimacyFriendship and Intimacy Workplace FundamentalsWorkplace Fundamentals Substance Abuse ManagementSubstance Abuse Management
Tried standard cognitive-behavioral Tried standard cognitive-behavioral drug relapse prevention strategies drug relapse prevention strategies with groups of schizophrenic patients.with groups of schizophrenic patients.
Selected those most readily accepted Selected those most readily accepted and understood.and understood.
Adapted these using a skills training Adapted these using a skills training methods originally developed to methods originally developed to teach social and independent living teach social and independent living skills to schizophrenics. skills to schizophrenics.
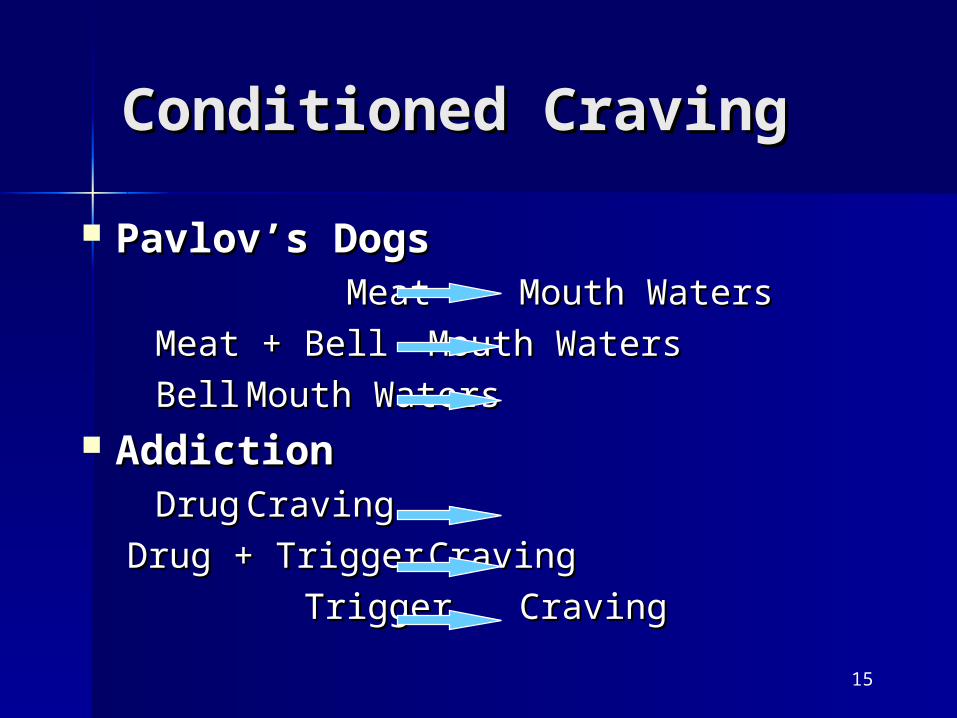
Lessons from Lessons from DevelopmentDevelopment ““Talk doesn’t cook rice.” Severely Talk doesn’t cook rice.” Severely
mentally ill individuals suffermentally ill individuals suffer– Significant deficits in verbal learning Significant deficits in verbal learning
ability ability – Conceptual disorganizationConceptual disorganization– Deficits in executive functionDeficits in executive function
Focus on SkillsFocus on Skills One size fits mostOne size fits most Keep it simpleKeep it simple
Module ThemeModule Theme
How to say no to drugsHow to say no to drugs
and yes to healthy pleasures.and yes to healthy pleasures.
How to Avoid Drugs:How to Avoid Drugs:7 Recommendations7 Recommendations
Seek healthy pleasuresSeek healthy pleasures Do things that are fun and healthy.Do things that are fun and healthy.
Avoid high risk situationsAvoid high risk situationsDon’t get into situations where you can’t say Don’t get into situations where you can’t say no.no.
Escape high risk situationsEscape high risk situationsIf someone offers drugs, say no.If someone offers drugs, say no.
Control damage from a slipControl damage from a slipIf you slip, quit early.If you slip, quit early.
Violation EffectViolation Effect High Risk High Risk
SituationsSituations
Warning Signs Warning Signs U-turnsU-turns Healthy HabitsHealthy Habits Healthy PleasuresHealthy Pleasures Support PersonsSupport Persons Pros and Cons of Pros and Cons of
drugsdrugs Money Money
managementmanagement
Nine Specific SkillsNine Specific SkillsHow to:How to: Quit before a slip becomes a relapseQuit before a slip becomes a relapse Report a slipReport a slip Refuse drugs from an aggressive dealerRefuse drugs from an aggressive dealer Refuse drugs from a friendRefuse drugs from a friend Enlist a support personEnlist a support person Get an appointment with a busy personGet an appointment with a busy person Discuss symptoms and side-effects with a Discuss symptoms and side-effects with a
psychiatristpsychiatrist Negotiate with a payeeNegotiate with a payee Get someone to join you in a healthy Get someone to join you in a healthy
pleasurepleasure
Refusing Drugs Offered by a Refusing Drugs Offered by a FriendFriend
1.1.Make eye contact. Use a firm, sincere voice Make eye contact. Use a firm, sincere voice tone. Say you're not interested.tone. Say you're not interested.
2. Use the broken record technique. Repeat 2. Use the broken record technique. Repeat yourself.yourself.
3. Level with the person. Tell them that drugs 3. Level with the person. Tell them that drugs were causing you problems and it's better for were causing you problems and it's better for you to leave them alone.you to leave them alone.
4. Suggest an alternative. Request to do 4. Suggest an alternative. Request to do something other than use drugs.something other than use drugs.
5. Tell the other person how you feel about being 5. Tell the other person how you feel about being pressured.pressured.
6. Leave the situation. Tell the person that you 6. Leave the situation. Tell the person that you are serious about not using.are serious about not using.
Reporting Symptoms and Side Reporting Symptoms and Side EffectsEffects
1.1.Greet your doctor politely. Make eye contact Greet your doctor politely. Make eye contact and use a pleasant tone of voice.and use a pleasant tone of voice.
2.2.Describe the symptom or side effect specifically.Describe the symptom or side effect specifically.
3.3.Say how long you’ve had the symptom or side Say how long you’ve had the symptom or side effect.effect.
4.4.Describe the severity or your problem by Describe the severity or your problem by explaining how it interferes with your daily explaining how it interferes with your daily activities.activities.
5.5.Ask directly for your doctor’s help.Ask directly for your doctor’s help.
6.6.Repeat the doctor’s instructions.Repeat the doctor’s instructions.
7.7.Ask how long it will take to get relief.Ask how long it will take to get relief.
8.8.Thank the doctor for assistanceThank the doctor for assistance..
Three Types of Group Three Types of Group SessionsSessions Basic trainingBasic training
– engagement in treatmentengagement in treatment– terms and conceptsterms and concepts
Skills trainingSkills training– how to avoid drugshow to avoid drugs– how to approach healthy pleasureshow to approach healthy pleasures
PracticePractice– how to apply skills to real-life how to apply skills to real-life
situationssituations
Basics
Practice
Timing of SessionsTiming of Sessions
Skills Training
•Basic Training -- 3 per week x 3 weeks (9 total)
•Skills Training -- 3 per week x 9 weeks (27 total)
•Practice Groups -- twice weekly throughout
Learning ActivitiesLearning Activities
IntroductionIntroduction Video question and answerVideo question and answer Role playRole play Resource managementResource management Outcome problemsOutcome problems In vivo exercisesIn vivo exercises HomeworkHomework
Rationale for Learning Rationale for Learning ActivitiesActivities
People who have severe mental People who have severe mental disorders have trouble with:disorders have trouble with:– attention attention – planningplanning– impulse controlimpulse control
Learning activities work by:Learning activities work by:– repeating material in different waysrepeating material in different ways– participants practice skills in various participants practice skills in various
environmentsenvironments– offering increased opportunities to offering increased opportunities to
– reminders of negative reminders of negative consequencesconsequences
– advantages of not usingadvantages of not using– reminders of coping strategiesreminders of coping strategies– phone numbers of support peoplephone numbers of support people
Recognize critical conceptsRecognize critical concepts– damage control, high risk situations, damage control, high risk situations,
warning signs, u-turns, healthy warning signs, u-turns, healthy habits and healthy pleasureshabits and healthy pleasures
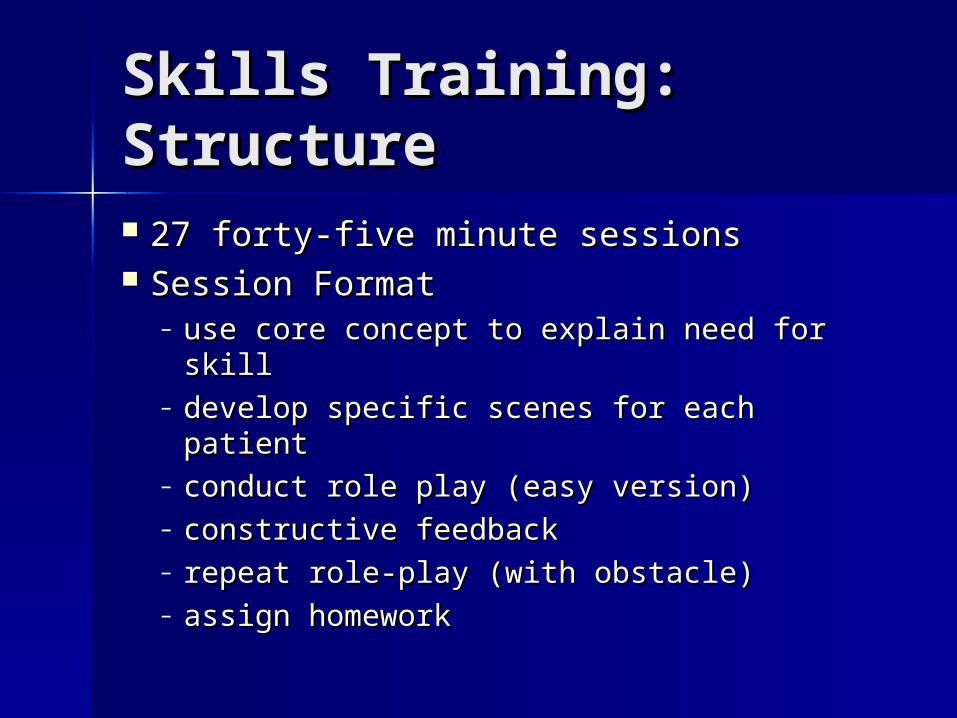
Skills Training: Skills Training: RationaleRationale Talk doesn’t cook rice -- Chinese Talk doesn’t cook rice -- Chinese
proverbproverb Each patient learns all skillsEach patient learns all skills Skills tailored to each patientSkills tailored to each patient
– use core concept to explain need for skilluse core concept to explain need for skill– develop specific scenes for each patientdevelop specific scenes for each patient– conduct role play (easy version)conduct role play (easy version)– constructive feedbackconstructive feedback– repeat role-play (with obstacle)repeat role-play (with obstacle)– assign homeworkassign homework
Practice: RationalePractice: Rationale
Real life => high relevanceReal life => high relevance Real time => high dramaReal time => high drama Attention grabbing => better Attention grabbing => better
learninglearning
Practice: StructurePractice: Structure
All stages of treatmentAll stages of treatment Series of questions Series of questions
– about prior weekabout prior week– about next weekabout next week
High-risk situations (recent or High-risk situations (recent or anticipatedanticipated))
Practice: Structure Practice: Structure (cont.)(cont.) Choose one or two situationsChoose one or two situations Illustrate how to manage the riskIllustrate how to manage the risk Much group participation and role Much group participation and role
playplay Homework assignmentsHomework assignments
Schedule of GroupsSchedule of Groups
Basic TrainingBasic Training– 3 times weekly until all eight 3 times weekly until all eight
sessions attended and test passedsessions attended and test passed Skills TrainingSkills Training
– 3 times weekly for 27 sessions total3 times weekly for 27 sessions total Practice SessionsPractice Sessions
– twice weekly, throughout the twice weekly, throughout the modulemodule
Nine Specific SkillsNine Specific SkillsHow to:How to: Quit before a slip becomes a relapseQuit before a slip becomes a relapse Report a slipReport a slip Refuse drugs from an aggressive dealerRefuse drugs from an aggressive dealer Refuse drugs from a friendRefuse drugs from a friend Enlist a support personEnlist a support person Get an appointment with a busy personGet an appointment with a busy person Discuss symptoms and side-effects with a Discuss symptoms and side-effects with a
psychiatristpsychiatrist Negotiate with a payeeNegotiate with a payee Get someone to join you in a healthy Get someone to join you in a healthy
pleasurepleasure
How to Do Skills How to Do Skills TrainingTraining Each of the nine skills has:Each of the nine skills has:
– Overview of the sessionOverview of the session– Detailed step-by-step instructionsDetailed step-by-step instructions– Sample therapist scriptSample therapist script– Video segment that models the skillVideo segment that models the skill
How to do Skills How to do Skills Training Training Introduce the goal of the moduleIntroduce the goal of the module
– Say Say NoNo to drugs and to drugs and YesYes to healthy to healthy pleasurepleasure
Introduce the session goalIntroduce the session goal– E.g., To learn how to refuse drugs offered E.g., To learn how to refuse drugs offered
by a dealerby a dealer Check for assimilationCheck for assimilation
– Make sure participants can repeat the Make sure participants can repeat the goalsgoals
Identify benefits of achieving the goalIdentify benefits of achieving the goal
How to do Skills How to do Skills TrainingTraining Review module terms and concepts Review module terms and concepts
related to the skill to be learnedrelated to the skill to be learned– What is a What is a high risk situationhigh risk situation??
Any situation that make it really hard not Any situation that make it really hard not to use.to use.
– What do I mean by What do I mean by Damage ControlDamage Control To reduce the harm; to get out as soon as To reduce the harm; to get out as soon as
possible.possible.
How to do Skills How to do Skills TrainingTraining
Develop the skill stepsDevelop the skill steps– Brainstorm with group membersBrainstorm with group members– Write suggestions on blank flip chartWrite suggestions on blank flip chart– Shape responsesShape responses– After group has developed their list, After group has developed their list,
show them prepared flip chartshow them prepared flip chart– Reinforce their ability to generate Reinforce their ability to generate
skill stepsskill steps
How to do Skills How to do Skills TrainingTraining Video illustrationVideo illustration
– Introduce videoIntroduce video– Critique model’s performanceCritique model’s performance– Elicit suggestions for improvementElicit suggestions for improvement
How to do Skills How to do Skills TrainingTraining Set up role-play scenarioSet up role-play scenario
– Select group memberSelect group member– Set up role-playSet up role-play– Think of real situation; set the Think of real situation; set the
scene; elicit specific detailsscene; elicit specific details Who, where, what was participant Who, where, what was participant
thinking and feelingthinking and feeling– Review rolesReview roles– Review steps on flip-chartReview steps on flip-chart
Model SkillsModel Skills
Showing Showing works better than works better than tellingtelling Before you model a sequence, tell Before you model a sequence, tell
patients what they will be patients what they will be expected to do and what to watch expected to do and what to watch for (refer to flip-chart)for (refer to flip-chart)
If possible, have a patient who If possible, have a patient who already possesses the requisite already possesses the requisite skill demonstrateskill demonstrate
Conduct Role-playsConduct Role-plays
Behavioral rehearsal is keyBehavioral rehearsal is key Brief scenes enacted by patientsBrief scenes enacted by patients Very active - get out of your seatsVery active - get out of your seats Instruct and guideInstruct and guide
– prompt specific behaviorsprompt specific behaviors– model responsesmodel responses– provide corrective feedbackprovide corrective feedback
Cue Responses /Shape Cue Responses /Shape BehaviorBehavior Prompt participant during Prompt participant during
exerciseexercise– Stay nearStay near– Whisper what to say in his earWhisper what to say in his ear– Cue him with gesturesCue him with gestures
missing from repertoiremissing from repertoire Excesses: behaviors that are Excesses: behaviors that are
overbearing, intrusive, overbearing, intrusive, flamboyant or aggressive flamboyant or aggressive
How to do Skills How to do Skills TrainingTraining Review Role-playReview Role-play
– Ask role-player what was most effectiveAsk role-player what was most effective– Elicit positive feedback from group Elicit positive feedback from group
membersmembers– Ask co-trainer for feedbackAsk co-trainer for feedback– Summarize effective behaviors, elicit Summarize effective behaviors, elicit
group applausegroup applause– Provide Corrective FeedbackProvide Corrective Feedback– Repeat role-play Repeat role-play
Give Feedback:Give Feedback:Positive and SpecificPositive and Specific Always praise efforts as soon as a Always praise efforts as soon as a
scene ends. scene ends. (Even if a scene was grossly (Even if a scene was grossly deficient)deficient)
State remarks in specific behavioral State remarks in specific behavioral terms:terms:– ““That was terrific. You looked him right That was terrific. You looked him right
in the eye and firmed up your voice in the eye and firmed up your voice when you told him you didn’t want any when you told him you didn’t want any drugs” (as opposed to “That was good”).drugs” (as opposed to “That was good”).
Feedback TipsFeedback Tips
Point out elements that were “effective”Point out elements that were “effective”(avoid value judgments like “good” or “correct”)(avoid value judgments like “good” or “correct”)
Invite participants to comment on role-playInvite participants to comment on role-play(guide remarks to emphasize positive qualities)(guide remarks to emphasize positive qualities)
Avoid criticism of patient’s effortsAvoid criticism of patient’s efforts Suggest improvements in behavioral terms-Suggest improvements in behavioral terms-
– ““Next time, I want you to avert your gaze…”Next time, I want you to avert your gaze…”
How to do Skills How to do Skills TrainingTraining
Challenge scenariosChallenge scenarios– Introduce an obstacleIntroduce an obstacle– Elicit suggestions about how to Elicit suggestions about how to
overcome the obstacleovercome the obstacle– Conduct challenge role-playConduct challenge role-play– Elicit feedback Elicit feedback
How to Conduct How to Conduct Practice SessionsPractice Sessions
Welcome group members, Welcome group members, reinforce attendancereinforce attendance
Introduce new membersIntroduce new members Review goals of SAMM and Review goals of SAMM and
Practice SessionsPractice Sessions Review previously assigned Review previously assigned
homeworkhomework
How to Conduct Practice How to Conduct Practice SessionsSessions
Ask 4 questionsAsk 4 questions– Has anyone encountered a High Risk Has anyone encountered a High Risk
Situation since our last meeting?Situation since our last meeting?– Does anyone anticipate encountering a Does anyone anticipate encountering a
High Risk Situation during the coming High Risk Situation during the coming week?week?
– Has anyone begun a new Healthy Habit?Has anyone begun a new Healthy Habit?– Has anyone begun a new Healthy Pleasure?Has anyone begun a new Healthy Pleasure?
Identify a “theme” related to any of the Identify a “theme” related to any of the 9 skills taught in skills training9 skills taught in skills training
How to Conduct How to Conduct Practice SessionsPractice Sessions
Create a role-play that comes Create a role-play that comes closest to theme identifiedclosest to theme identified
Rehearse role-play with as many Rehearse role-play with as many participants as time will permitparticipants as time will permit
Assign homework where Assign homework where appropriateappropriate
Remind members of next meeting Remind members of next meeting timetime
Teaching TipsTeaching Tips Prepare classroom in advancePrepare classroom in advance Gather needed materialsGather needed materials Close door. Start and end on Close door. Start and end on
timetime Take attendanceTake attendance Use incentivesUse incentives Demonstrate courtesyDemonstrate courtesy Project a positive attitudeProject a positive attitude Model interpersonal skillsModel interpersonal skills
Organize the settingOrganize the setting
Large room Large room Gather relevant propsGather relevant props Position chairs in semi-circlePosition chairs in semi-circle Create space for role-play Create space for role-play
exercisesexercises Use 2 flip charts:Use 2 flip charts:
– one blank for brainstorming steps one blank for brainstorming steps with participantswith participants
– one prepared with concepts and one prepared with concepts and role-play steps role-play steps
Overcome Resistance to Overcome Resistance to Role-playingRole-playing
Liveliness and spontaneity are keyLiveliness and spontaneity are key Project acceptance, tolerance, and optimismProject acceptance, tolerance, and optimism Display warmth and enthusiasm toward Display warmth and enthusiasm toward
reluctant patientsreluctant patients Begin with most enthusiastic patients Begin with most enthusiastic patients Call on reluctant patients to provide feedbackCall on reluctant patients to provide feedback Then ask them to demonstrate what they Then ask them to demonstrate what they
meanmean Allow reluctant patients to take secondary Allow reluctant patients to take secondary
role or remain in their seatsrole or remain in their seats
Pilot TestPilot Test
PurposePurpose MethodMethod
Pilot Test: PurposePilot Test: Purpose
Is it practical?Is it practical? Will patients attend?Will patients attend? Can therapists follow the manual?Can therapists follow the manual? Do patients find the material Do patients find the material
relevant?relevant? Do patients learn the concepts and Do patients learn the concepts and
skills?skills? Do they tend to improve?Do they tend to improve?
SubjectsSubjects
Recruited on admission to DDTPRecruited on admission to DDTP Any chronic psychotic disorderAny chronic psychotic disorder Any current drug abuse or Any current drug abuse or
dependencedependence Unlikely to tolerate or benefit Unlikely to tolerate or benefit
from standard substance abuse from standard substance abuse treatment programs.treatment programs.
MeasuresMeasures
Initial diagnostic assessment (SCID)Initial diagnostic assessment (SCID) Pretreatment, post-treatment and Pretreatment, post-treatment and
Subjects learned and remembered Subjects learned and remembered a wide range of drug relapse a wide range of drug relapse prevention concepts and skills. prevention concepts and skills.
Skills were retained at 3-month Skills were retained at 3-month follow-up.follow-up.
Clinically and statistically Clinically and statistically significant reduction in drug and significant reduction in drug and alcohol use 3 months after alcohol use 3 months after completion of training.completion of training.