PREECLAMPSIA - Overview and Update - Professor Shaun Brennecke Director Department of Maternal Fetal Medicine Royal Women’s Hospital Parkville, Victoria, Australia The past, the present, the future: challenges & opportunities for Maternal & Child Health Nurses and Midwives Annual Conference 18 August 2018
Transcript
PREECLAMPSIA - Overview and Update -
Professor Shaun Brennecke Director
Department of Maternal Fetal Medicine Royal Women’s Hospital
Parkville, Victoria, Australia
The past, the present, the future: challenges & opportunities for
Maternal & Child Health Nurses and Midwives
Annual Conference 18 August 2018
PREECLAMPSIA
OVERVIEW
PREECLAMPSIA
DEFINITION
PREGNANCY INDUCED…..
• Hypertension
• Proteinuria
• Generalised oedema
• Multisystem dysfunctions
The Hypertensive Disorders of Pregnancy: Classification, Diagnosis and Management
International Society for the Study of Hypertension in Pregnancy
Proposed Recommendations for International Practice
Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy F, Saito S, Hall D, Warren C, Adoyi G, Ishaku S. on behalf of the International Society for the Study of Hypertension in Pregnancy (ISSHP).
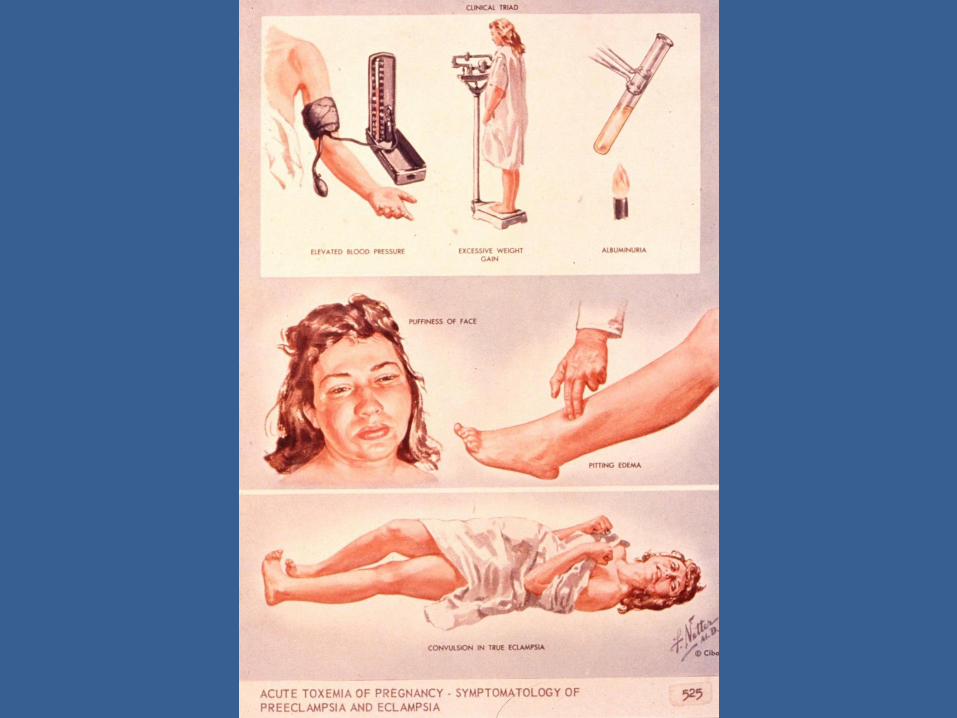
CLINICAL FEATURES OF PREECLAMPSIA
• First pregnancy
• New onset hypertension
• New onset proteinuria
• Generalised oedema
• Unpredictable progression to ECLAMPSIA
• Widespread maternal organ failure
• Feto-placental compromise
PREECLAMPSIA
FEATURES
• Unique to human pregnancy
• Usually latter half of pregnancy
• Disease of first pregnancy
• Resolves following delivery
Preeclampsia is the most common serious medical disease of human pregnancy with an incidence of 1-5% in most parts of the world
PREECLAMPSIA
SIGNIFICANCE
WORLDWIDE …..
A mother dies every 8 minutes
from
complications of preeclampsia
PREECLAMPSIA
CURRENT AUSTRALIAN FIGURES
Mild Preeclampsia 5-10%
Severe Preeclampsia 1-2%
Maternal Mortality 15%
Perinatal Mortality 10%
Labour Inductions 20%
Caesarean Sections 15%
Preterm Deliveries 5-10%
Maternal Bed Costs $50 million pa
Neonatal Bed Costs $10 million pa
SIGNIFICANCE
PREECLAMPSIA
PROBLEMS FOR THE MOTHER
High blood pressure … If severe → weakens blood vessels → stroke
→ weakens the heart → heart failure
“Leaky” kidneys → protein in urine
“Leaky” blood vessels → swelling of face and limbs
Fits/convulsions/ “epilepsy”
“Thinning” of blood → uncontrolled bleeding
Liver failure → jaundice
“Wet” lungs
THE HELLP
SYNDROME
Haemolysis
Elevated Liver Enzymes
Low Platelet Count
PREECLAMPSIA PROBLEMS FOR THE BABY
Impaired functioning of placenta (afterbirth), so…. - baby’s supply of nutrients in womb decreased - baby’s supply of oxygen in womb decreased
- baby’s growth in womb slowed - baby’s survival in womb jeopardised
Possible need therefore for early delivery, so… -problems of prematurity…
MATERNAL CIRCULATING PLGF IS ABNORMALLY LOW IN PREECLAMPSIA
Levine RJ et al (2004) NEJM 350(7): 672-683
Maynard SE et al. J Clin Invest (2003)
MATERNAL CIRCULATING sFlt-1 IS ABNORMALLY HIGH IN PREECLAMPSIA
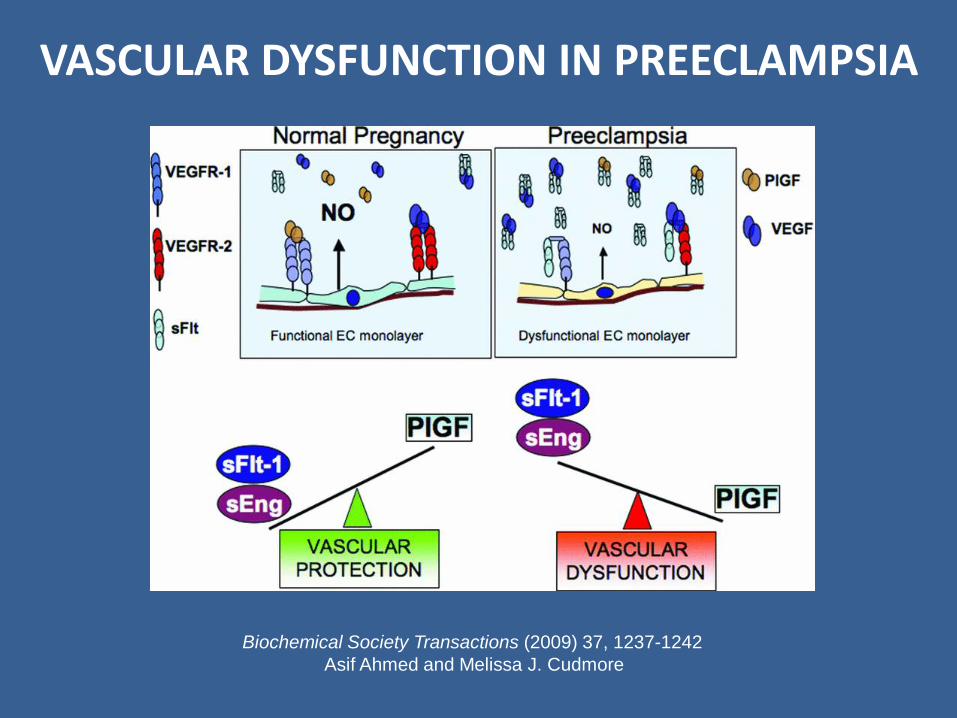
VASCULAR DYSFUNCTION IN PREECLAMPSIA
Biochemical Society Transactions (2009) 37, 1237-1242
Asif Ahmed and Melissa J. Cudmore
Schoofs K et al. J Perinat Med (2014)
sFlt-1/PlGF RATIO AND PREGNANCY OUTCOME
sFlt-1/PlGF RATIO
A Test of Placental Dysfunction
CAN WE USE THIS TEST TO
PREDICT PREECLAMPSIA?
The PROGNOSIS Study
Key Points
Sample size n=1050
A single sFlt/PlGF ratio cut-off value of 38 is appropriate
for gestational ages 24-37 weeks
A low sFlt-1/PlGF ratio (≤ 38) rules out preeclampsia within one week (NPV of 99.3%)
and within four weeks (NPV of 94.3%)
A high sFlt-1/PlGF ratio (> 38) predicts preeclampsia within four weeks (PPV of 36.7%)
The PROGNOSIS Study
sFlt-1/PlGF
Prediction Diagnosis
Progression of
Preeclampsia
PERT
The new PreEclampsia Ratio Test
Currently in use at the RWH
CAN WE
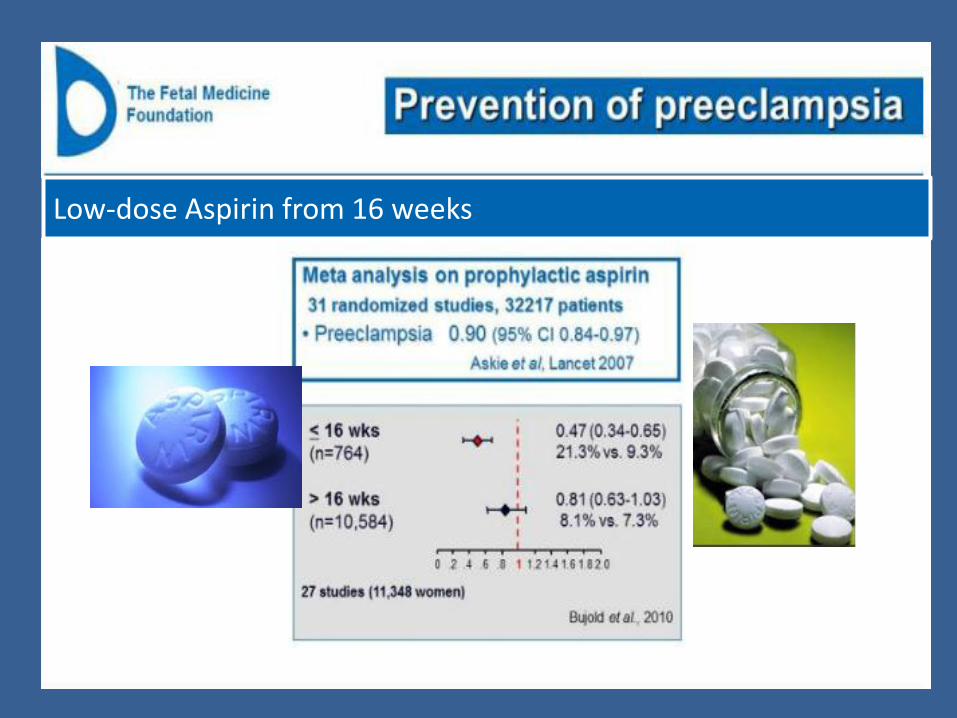
PREVENT PREECLAMPSIA?
Low-dose Aspirin from 16 weeks
Combined Multi-Marker Screening and Randomised Patient Treatment with Aspirin for Evidence-Based Preeclampsia Prevention
IS THERE A BETTER ANTENATAL CARE SYSTEM
FOR PREDICITNG
AND PREVENTING
PREECLAMPSIA?
DECREASING PREECLAMPSIA MORTALITY
Historical Perspective
Dr John Ballantyne 1861-1923
Edinburgh Perinatologist Apostle of Antenatal Care
DECREASING PREECLAMPSIA MORTALITY
Historical Perspective
PREECLAMPSIA
Historically, the primary medical justification
for antenatal care
Cause 1935 1950 1950 as a percentage of 1935
Toxaemia 7.8 2.6 33.3
Maternal mortality rates per 10,000 births. Source: A. Macfarlane and M. Mugford, Birth Counts: Statistics of Pregnancy and Childbirth (London, 1984), ii. 276-7.
DECLINE IN PREECLAMPSIA MATERNAL MORTALITY ENGLAND AND WALES
1935-1950
DR at 5% FPR
History MAP uA-PI PAPP-A PlGF Reference
33 X Yu (2005)
Akolekar (2011)
38 X Poon (2009)
47 X X Akolekar (2011)
54 X X Akolekar (2011)
60 X X X Foidart (2010)
78 X X X Foidart (2010)
78 X X X X X Akolekar (2011)
84 X X X X Poon (2010)
89 X X X X Poon (2010)
93 X X X X X Poon (2009)
FIRST TRIMESTER MULTIPARAMETRIC MODEL DETECTION RATES FOR EARLY-ONSET PE
History: body mass index, family history of PE, previous PE, ethnicity, smoking; MAP: mean arterial blood pressure; uA-PI: uterine artery pulsatility index
Biochemical markers: PAPP-A, PlGF
Costa FS, (2011) Rev Bras Gincol Obstet 33(11) 367-375
Nicolaides KH, Prenat Diag (2011): 31: 3-6
Pyramid of prenatal care: past (left) and future (right)
A MODEL FOR A NEW PYRAMID OF PRENATAL CARE BASED ON THE 11 TO 13 WEEKS’ ASSESSMENT
CAN WE IMPROVE ON LOW DOSE ASPIRIN
FOR PREVENTING
PREECLAMPSIA?
The ESPRESSO Trial
Can esomeprazole (Nexium)
reduce the risk of preeclampsia?
A Multicentre Trial
Principal Investigator - Prof Jon Hyett
Involving Maternity Hospital in NSW, Victoria and SA

























































![Sensitivity in Experimental Preeclampsia · pregnancy [17]. During preeclampsia, the increased Ang-II sensitivity may even develop before the clinical manifestation of the disease](https://static.documents.pub/doc/80x56/60bf031e1077c9480d759388/sensitivity-in-experimental-pregnancy-17-during-preeclampsia-the-increased-ang-ii.jpg)















