32
Overview of HMO HEDIS 2006 Results 11:00 a.m.–11:30 a.m. March 28, 2007
| Date post: | 13-Dec-2015 |
| Category: |
Documents |
| Upload: | donna-phelps |
| View: | 217 times |
| Download: | 3 times |

Overview of HMO HEDIS 2006 Results
11:00 a.m.–11:30 a.m.
March 28, 2007
Florida Medicaid HEDIS 2006 Results
Presented by:
Peggy Ketterer, RN, BSN, CHCA
Presentation Overview
I. Welcome
II. Key Measure Results
III. Upcoming Changes in HEDIS 2007
IV. Questions and Comments
HEDIS is a registered trademark of the National Committee
for Quality Improvement (NCQA)

Dimensions of Care
• Pediatric Care
• Women’s Care
• Living with Illness

AnalyticsComparative
– Florida 2006 weighted average compared to the national 2005 Medicaid 50th percentile
Distribution
– Range of MHP reported rates
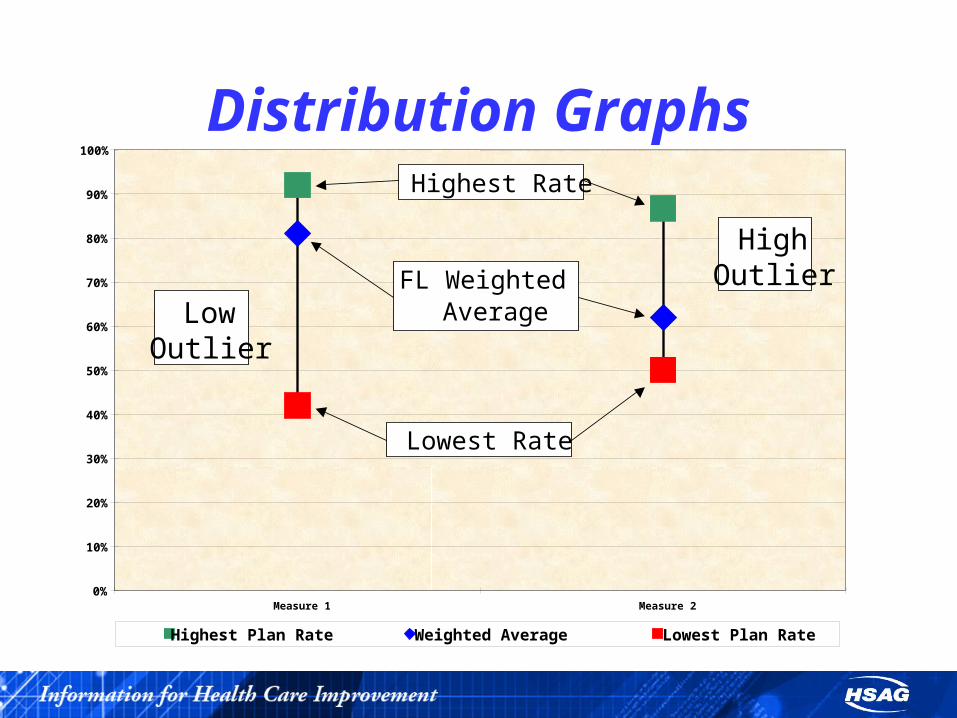
Distribution Graphs
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Measure 1 Measure 2
Highest Plan Rate Weighted Average Lowest Plan Rate
Highest Rate
Lowest Rate
FL Weighted Average
HighOutlier
LowOutlier
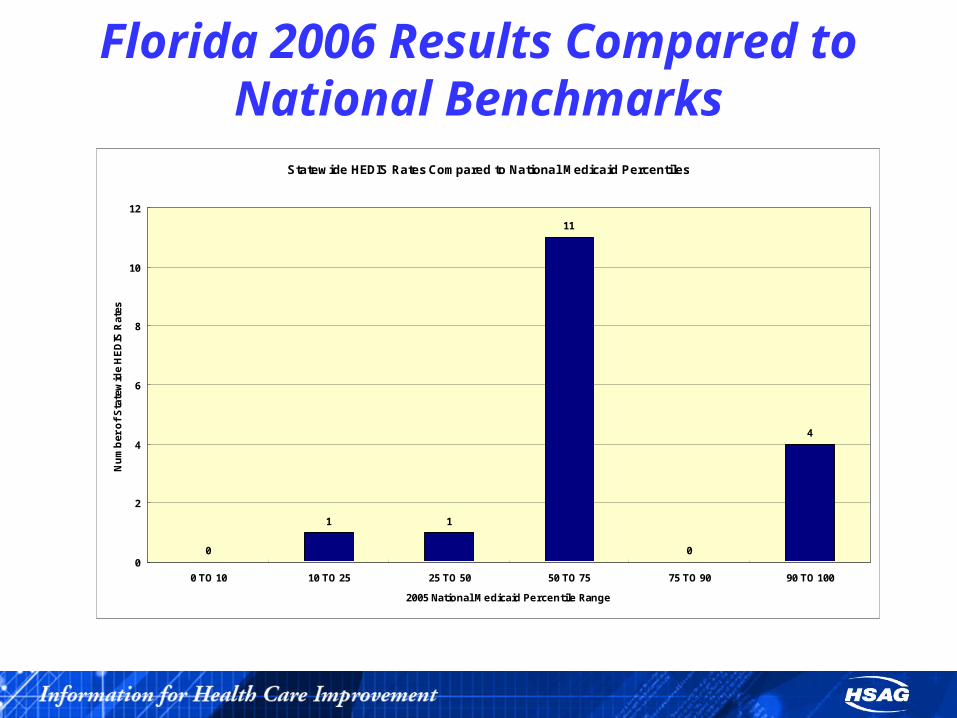
Florida 2006 Results Compared to National Benchmarks
Statewide HEDIS Rates Compared to National Medicaid Percentiles
0
1 1
11
0
4
0
2
4
6
8
10
12
0 TO 10 10 TO 25 25 TO 50 50 TO 75 75 TO 90 90 TO 100
2005 National Medicaid Percentile Range
Nu
mb
er o
f S
tate
wid
e H
ED
IS R
ates

Pediatric Care

Pediatric Care
Statewide performance results ranged from below average to above average.
Pediatric Care•Statewide results for the Well-Child Visits in the Third, Fourth, Fifth, and Sixth Years of Life and Adolescent Well-Care Visits measures were average when compared nationally.
•Well-Child Visits in the First 15 Months of Life—Zero Visits and Well-Child Visits in the First 15 Months of Life—Six or More Visits, had performance results below the LPL.
•A wide range of reported rates was observed for the Well-Child Visits in the First 15 Months of Life—Six or More Visits measure.
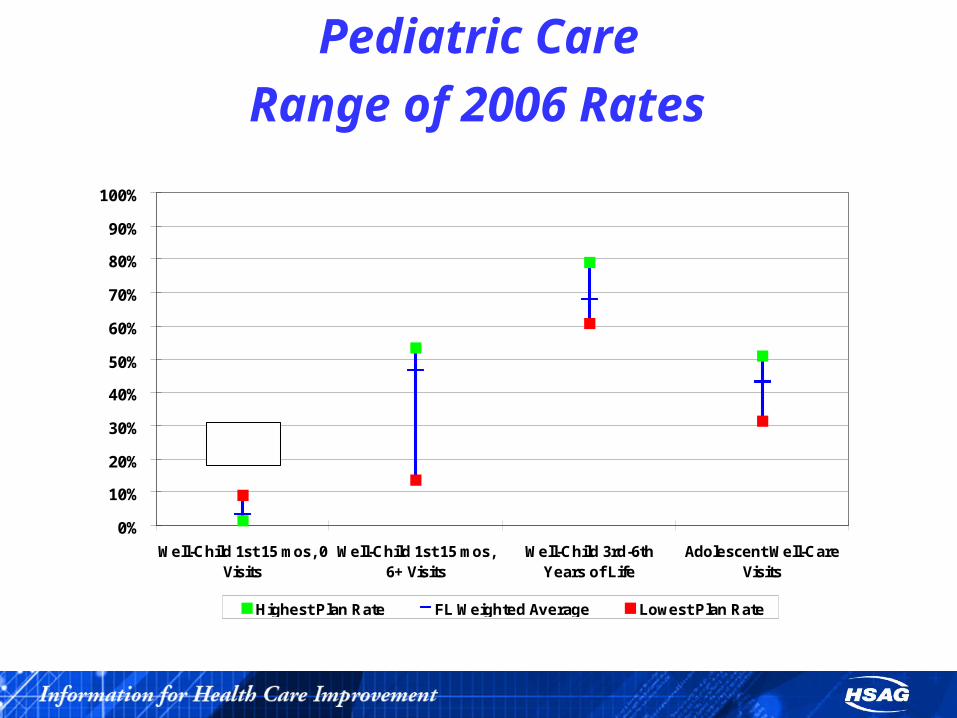
Pediatric Care
Range of 2006 Rates
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Well-Child 1st 15 mos, 0Visits
Well-Child 1st 15 mos,6+ Visits
Well-Child 3rd-6thYears of Life
Adolescent Well-CareVisits
Highest Plan Rate FL Weighted Average Lowest Plan Rate
ReverseMeasure

Pediatric CareImprovement efforts to consider for well-child measures:
•Barriers to improvement could be identified and evaluated in terms of greatest impact. A good barrier analysis can assist in targeting interventions that would bring about the most effective results.
•HMOs may want to focus on tracking and monitoring missing medical records during medical record pursuit.
•Provider and member reminders and education have been shown to have positive affects on health plan performance.

Pediatric Care•The HMOs may want to evaluate noncompliant cases (children in the eligible population who did not meet numerator compliance) and try to determine the reasons why they were noncompliant.
•The HMOs should also consider evaluating cases that are defined as missed opportunities.
Women’s Care

Women’s Care
Overall performance for the Women’s Care dimension was below average to average.

Women’s Care
•None of the HMOs had a rate above the HPL for this dimension of care.
•Five of the nine HMOs that reported a rate for the Breast Cancer Screening measure performed below the LPL.
•One HMO performed below the LPL in all three Chlamydia Screening in Women measures.

Women’s Care
For Breast Cancer Screening, rates may have been hampered in 2006 because the hybrid method was retired for this specific measure. HMOs that may have relied on medical record review for the Breast Cancer Screening measure in the past likely observed a reduction in their performance.
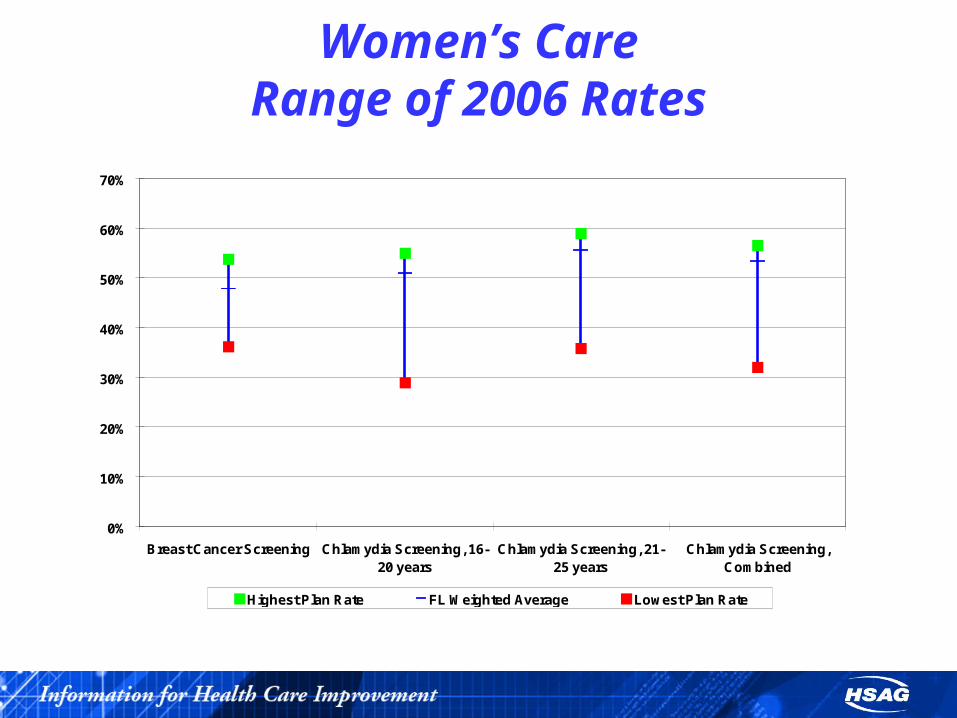
Women’s CareRange of 2006 Rates
0%
10%
20%
30%
40%
50%
60%
70%
Breast Cancer Screening Chlamydia Screening, 16-20 years
Chlamydia Screening, 21-25 years
Chlamydia Screening,Combined
Highest Plan Rate FL Weighted Average Lowest Plan Rate
Women’s Care
Improvement efforts to consider for breast cancer screening measure:
•Conduct a barrier analysis survey to identify why women are not getting the needed screenings.
•Mobile mammography/extended hours.

Women’s Care
Improvement efforts to consider for the Chlamydia Screening in Women measure:
•Analyze physician and lab coding practices.

Women’s Care
•Missed opportunities could be examined to identify barriers to improvement and target specific interventions.
Living with Illness

Living with Illness
The overall statewide results in the Living With Illness dimension were above average when compared with national Medicaid percentiles; however, caution should be exercised when interpreting or extrapolating results due to significant changes to the HEDIS specifications for the asthma measure.
Living with Illness
• Significant changes were made in the 2006 measure specifications.
• Nationwide and in Florida, these changes resulted in lower eligible populations and higher rates.

Living with Illness
Overall, the HMOs should still implement quality improvement initiatives to increase rates. To realize improvement in the asthma measures:•Strong, focused case management programs are essential. •The use of an internal registry that contains current, member-level data, such as claims/encounters and lab tests with results that are shared with the managing physicians, are very effective.

Living with IllnessRange of 2006 Rates, cont’d
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Asthma, 5-9 Years Asthma, 10-17 Years Asthma, 18-56 Years Asthma, CombinedRate
Highest Plan Rate FL Weighted Average Lowest Plan Rate

Changes to HEDIS 2007
Changes to Existing Measures
•Breast Cancer Screening – lowered age criteria to 40 years old, reporting in two age cohorts.

Changes to Existing Measures
•Chlamydia Screening in Women – Minor coding changes were made to the denominator identification algorithms and numerator identification codes

Changes to Existing Measures
•Use of Appropriate Medications for People with Asthma – Minor coding changes were made to the denominator identification algorithms

Changes to Existing Measures
•No changes were made to any of the well-child measures. For HEDIS 2008, NCQA is considering retiring the hybrid method.

Questions?

















