Overview of Periodontics for Overview of Periodontics for the General Practitioner the General Practitioner - - Initial Therapy Initial Therapy Nashville Area Dental Continuing Education Nashville Area Dental Continuing Education September 22, 2008 September 22, 2008 Phillip D. Woods, DDS, MPH Phillip D. Woods, DDS, MPH Commander, USPHS Commander, USPHS BOP National Periodontal Consultant BOP National Periodontal Consultant Diplomate, American Academy of Periodontology Diplomate, American Academy of Periodontology Chief Dentist, MCC San Diego Chief Dentist, MCC San Diego
Transcript
Overview of Periodontics for Overview of Periodontics for the General Practitioner the General Practitioner
-- Initial TherapyInitial Therapy
Nashville Area Dental Continuing EducationNashville Area Dental Continuing EducationSeptember 22, 2008September 22, 2008
Phillip D. Woods, DDS, MPHPhillip D. Woods, DDS, MPHCommander, USPHSCommander, USPHS
BOP National Periodontal ConsultantBOP National Periodontal ConsultantDiplomate, American Academy of PeriodontologyDiplomate, American Academy of Periodontology
Chief Dentist, MCC San DiegoChief Dentist, MCC San Diego
Reference TextReference Text
Manual of Clinical Periodontics , 2Manual of Clinical Periodontics , 2ndnd Edition Edition by Francis Serio and Charles Hawleyby Francis Serio and Charles HawleyCopyright (c) LexiCopyright (c) Lexi--Comp, Inc. 1978Comp, Inc. 1978--2008 All Rights 2008 All Rights Reserved.Reserved.
Great narratives, clinical photographs, and online accessGreat narratives, clinical photographs, and online access
Many of the slides from this presentation are found in this Many of the slides from this presentation are found in this source!source!
Overview of Presentation #2Overview of Presentation #2
1.1. Questions from Presentation #1Questions from Presentation #12.2. Initial Periodontal TherapyInitial Periodontal Therapy
1.1. Scaling/Root Planing/ultrasonics vs. hand Scaling/Root Planing/ultrasonics vs. hand instrumentsinstruments
3.3. Occlusal FactorsOcclusal Factors4.4. Recall MaintenanceRecall Maintenance5.5. Systemic Disease and Periodontal TherapySystemic Disease and Periodontal Therapy6.6. MedicoMedico--legal Considerations legal Considerations
Preferred Sequence of Preferred Sequence of Periodontal Therapy Periodontal Therapy
•• Procedures not classified as surgicalProcedures not classified as surgical proceduresprocedures..Control of biofilm and etiology of diseaseControl of biofilm and etiology of diseaseScaling and root planing to disrupt and remove biofilm Scaling and root planing to disrupt and remove biofilm and calculus. Although this is a nonsurgical procedure, and calculus. Although this is a nonsurgical procedure, the gingival attachment to the tooth and underlying bone the gingival attachment to the tooth and underlying bone may be invaded.may be invaded.Local antimicrobial delivery Local antimicrobial delivery −− systemic and local systemic and local antibioticsantibioticsOcclusal therapyOcclusal therapyElimination of local plaqueElimination of local plaque--retentive factorsretentive factorsControl of systemic factors (smoking, diabetes, stress) Control of systemic factors (smoking, diabetes, stress) where possiblewhere possible
Pathway to periodontal diseasePathway to periodontal disease
Presence of BacteriaPresence of BacteriaActinobacillus actinomycetemcomitansActinobacillus actinomycetemcomitansPorphyromonas gingivalisPorphyromonas gingivalisBacteroides forsythusBacteroides forsythus
Endotoxin: LipopolysaccharideEndotoxin: LipopolysaccharideReleased from gram (Released from gram (--) bacteria) bacteriaInitiates host responseInitiates host responseActs with host factors>bone resorptionActs with host factors>bone resorption
Periodontal TherapyPeriodontal Therapy
Treatment goalsTreatment goalsResolve inflammationResolve inflammationArrest disease progressionArrest disease progressionMaintain estheticsMaintain estheticsRegenerate lost periodontiumRegenerate lost periodontiumCreate an environment that deters recurrent diseaseCreate an environment that deters recurrent diseaseMaintain periodontal healthMaintain periodontal health
Scaling and Root PlaningScaling and Root PlaningScaling and root planing is the cornerstone of almost Scaling and root planing is the cornerstone of almost all initial therapy treatment plans for periodontitis. all initial therapy treatment plans for periodontitis. It may be the only mechanical therapy required for the It may be the only mechanical therapy required for the management of mild (1management of mild (1--2 mm clinical attachment loss, 2 mm clinical attachment loss, pockets to 6 mm in depth) chronic periodontitis. pockets to 6 mm in depth) chronic periodontitis. While scaling and root planing procedures are utilized While scaling and root planing procedures are utilized routinely, they remain among the most technically routinely, they remain among the most technically demanding procedures performed in periodontics. demanding procedures performed in periodontics. When performed with optimal access and skill, scaling When performed with optimal access and skill, scaling and root planing will produce a decrease in gingival and root planing will produce a decrease in gingival inflammation, a reduction in periodontal probing inflammation, a reduction in periodontal probing depths, and a gain in periodontal attachment. depths, and a gain in periodontal attachment.
DefinitionsDefinitions
ScalingScaling-- Mechanical removal of plaque, calculus and Mechanical removal of plaque, calculus and stains from crown and root surfacesstains from crown and root surfacesRoot planingRoot planing-- more definitivemore definitive…….time consuming .time consuming scaling type procedure designed to remove cementum scaling type procedure designed to remove cementum and or dentinand or dentin
What Is Endotoxin and Where Does It What Is Endotoxin and Where Does It Come From?Come From?
Endotoxin is the lipopolysaccharide component Endotoxin is the lipopolysaccharide component of the outer membrane of Gramof the outer membrane of Gram--negative cell negative cell walls. walls. Endotoxin will produce a severe local Endotoxin will produce a severe local inflammatory reaction when injected inflammatory reaction when injected experimentally in tissue experimentally in tissue
deposits are firmly deposits are firmly attached to and interattached to and inter--lock with dentin and lock with dentin and root surface root surface Irregularities.Irregularities.
What instruments to use whereWhat instruments to use where
SUGGESTED SCALING AND ROOT PLANING INSTRUMENTS AND APPLICATIONS
Application Instrument
Supragingival calculus removal Scalers − Jacquette 34/35, Taylor
Universal scaling and root planing Columbia 4R/4L or 13/14, McCall's 17S/18S
Interproximal surfaces of anterior teeth Gracey 1/2, 3/4
Interproximal surfaces of posterior teeth Gracey 11/12 (mesial), Gracey 13/14 or 15/16 (distal)
Scaling and Root PlaningScaling and Root Planing
Initial TherapyInitial Therapy
Patient with Patient with plaqueplaque--induced induced gingivitis.gingivitis.
Initial TherapyInitial Therapy
Three weeks Three weeks following following compliance compliance with with excellent excellent patient patient hygienehygiene
Initial TherapyInitial Therapy
Gingival Gingival inflammation inflammation is a is a combination combination of acute and of acute and chronic chronic changes.changes.
Initial TherapyInitial Therapy
Root planing Root planing with curettes with curettes has largely has largely resolved the resolved the inflammationinflammation
Initial TherapyInitial Therapy
Subgingival Subgingival calculus deposits calculus deposits and related and related inflammation.inflammation.
Initial TherapyInitial Therapy
Four weeks Four weeks after after initial therapyinitial therapy
Initial TherapyInitial Therapy
Pocket reduction Pocket reduction following scaling following scaling and root planingand root planing
Initial TherapyInitial Therapy
Gross Gross amounts of amounts of plaque and plaque and calculus.calculus.
Initial TherapyInitial Therapy
RadiographsRadiographsconfirm confirm
hopelesshopelessprognosis of prognosis of
toothtooth
Initial TherapyInitial Therapy
Removal Removal of hopeless of hopeless
teethteeth
Initial TherapyInitial Therapy
Deep pockets Deep pockets seen on the seen on the distal of upper distal of upper left first molar.left first molar.
Initial TherapyInitial Therapy
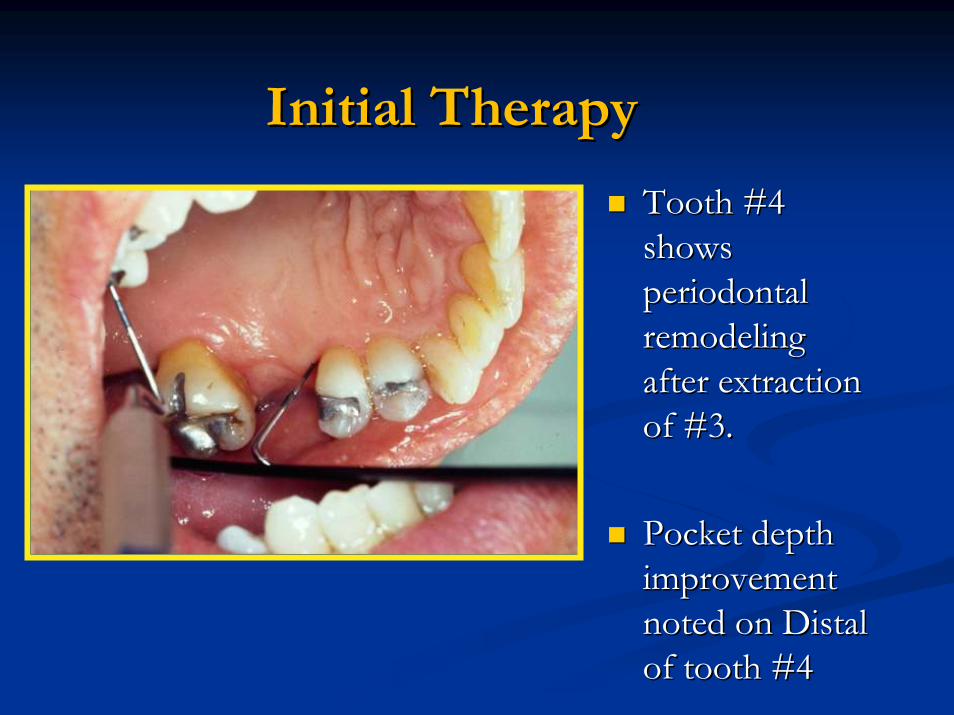
Tooth #4 Tooth #4 shows shows periodontal periodontal remodeling remodeling after extraction after extraction of #3.of #3.
Pocket depth Pocket depth improvement improvement noted on Distal noted on Distal of tooth #4of tooth #4
Initial TherapyInitial Therapy
Caries Caries removal removal and root and root canal canal therapytherapy
Challenges to Hand InstrumentationChallenges to Hand Instrumentation
Teeth with root Teeth with root concavities and concavities and grooves tend not grooves tend not do as well as flat do as well as flat surfaces post SRP surfaces post SRP with hand with hand instruments.instruments.
New techniquesNew techniques
Changing from Hand Scaling and Root Changing from Hand Scaling and Root Planing to Powered Ultrasonic DebridementPlaning to Powered Ultrasonic Debridement
Use powered Ultrasonic scalers for about Use powered Ultrasonic scalers for about 90% of the cleaning90% of the cleaning
Ultrasonic TechnologyUltrasonic Technology
1943: originally designed for cavity preparation1943: originally designed for cavity preparation1957: shift to tooth scaling use1957: shift to tooth scaling use
UltrasonicsUltrasonics
Correct use: gross calculus & stainCorrect use: gross calculus & stainBetter time efficiency; less operator fatigueBetter time efficiency; less operator fatigueHand planing followHand planing follow--up is not always necessaryup is not always necessary
Better access into furcations Better access into furcations (Oda 1989)(Oda 1989)No difference 16 months No difference 16 months post treatment with hand post treatment with hand vs. ultrasonics (Schrorer vs. ultrasonics (Schrorer 1991)1991)Superior to hand Superior to hand instruments (Takacs 1993)instruments (Takacs 1993)
Complete kill of motile rods after 60 seconds Complete kill of motile rods after 60 seconds (Thilo, 1987)(Thilo, 1987)Sonics and ultrasonics reduced microflora by Sonics and ultrasonics reduced microflora by 88% (Baehni 1992)88% (Baehni 1992)As effective as hand instruments (Oosterwaal As effective as hand instruments (Oosterwaal 1987, Breninger 1987)1987, Breninger 1987)
CavitronCavitron
Not as portableNot as portableElliptical motionElliptical motionStandard and Standard and slimline tipsslimline tips
Automatically maintains the scaler’s power and frequency settings as it comes in contact with the tooth
Cavitron setCavitron set--upup
The handpiece must be filled with water before The handpiece must be filled with water before the instrument is insertedthe instrument is inserted
Patient ComfortPatient Comfort
Small, probe like tips: Small, probe like tips: patients comfortable patients comfortable without anesthesia without anesthesia (Kawanami 1988)(Kawanami 1988)Temperature sensitivity can Temperature sensitivity can be controlled by reducing be controlled by reducing water flow (Chapple 1992)water flow (Chapple 1992)
Power SettingsPower Settings
high power for initial high power for initial debridement if heavy calculusdebridement if heavy calculusLow power for fine Low power for fine debridementdebridementThin tips may wear out Thin tips may wear out prematurely if used for prematurely if used for heavier calculus and stainheavier calculus and stain
AdaptationAdaptation
The point of the The point of the tip should not be tip should not be adapted at a 90adapted at a 90ººangleangleLight pressure Light pressure should be usedshould be usedOnly the last 1Only the last 1--2 2 mm of the tip mm of the tip does any workdoes any work
AdaptationAdaptation
Curettes: specific cutting edgeCurettes: specific cutting edgeUltrasonic and sonic tips can be activated with Ultrasonic and sonic tips can be activated with any side in contact with the toothany side in contact with the toothThe length of the tip is held parallel to the The length of the tip is held parallel to the tooth surfacetooth surfaceThe point of the tip should not be adapted at a The point of the tip should not be adapted at a 9090ºº angleangleThe tip can build up heat rather quickly if held The tip can build up heat rather quickly if held against soft tissue such as the lip or cheek.against soft tissue such as the lip or cheek.
Ultrasonic TechniqueUltrasonic Technique
Brush away calculus with sweeping cross strokesBrush away calculus with sweeping cross strokesLargest metal mass possible at the lowest power Largest metal mass possible at the lowest power possible for efficiency and comfortpossible for efficiency and comfort
Ultrasonic TechniqueUltrasonic Technique
Ultrasonic TechniqueUltrasonic Technique
Current OptionsCurrent Options
MicroMicro--ultrasonic (thinline) tipsultrasonic (thinline) tipsLonger, thinnerLonger, thinnerDesigned for fine debridementDesigned for fine debridement
Ultrasonics with AntimicrobialsUltrasonics with Antimicrobials
0.12% chlorhexidine + ultrasonic0.12% chlorhexidine + ultrasonicSignificant reduction in probing depth vs. Significant reduction in probing depth vs. scaling and irrigation with waterscaling and irrigation with water
Reynolds 1992Reynolds 1992
Curettes vs. UltrasonicsCurettes vs. Ultrasonics
Distance from base of pocketDistance from base of pocketCurette: 1.25 mmCurette: 1.25 mmPP--10 Cavitron: 1.13 mm10 Cavitron: 1.13 mmMicroultrasonic: 0.78 mmMicroultrasonic: 0.78 mm
Dragoo 1992Dragoo 1992
Curettes vs. UltrasonicsCurettes vs. Ultrasonics
““Similar improvement occurred after use of hand and Similar improvement occurred after use of hand and ultrasonic instruments. This agrees with results by ultrasonic instruments. This agrees with results by Torfason et al. (1979), Badersten et al. (1981), Torfason et al. (1979), Badersten et al. (1981), Oosterwaal et al. (1987) and Boretti et al. (1995), and Oosterwaal et al. (1987) and Boretti et al. (1995), and suggests that debridement of the contaminated root suggests that debridement of the contaminated root surfaces in deep pockets can be equally accomplished surfaces in deep pockets can be equally accomplished by ultrasonic and hand instruments.by ultrasonic and hand instruments.”” Badersten (1984) and Badersten (1984) and Badersten et al (1984, 1985, 1987)Badersten et al (1984, 1985, 1987)
Curettes vs. UltrasonicsCurettes vs. Ultrasonics
Ultrasonics can:Ultrasonics can:Achieve equal or better clinical resultsAchieve equal or better clinical resultsBe more efficientBe more efficientBe more comfortable for patientsBe more comfortable for patientsProvide better access for furcationsProvide better access for furcationsPreserve more tooth structurePreserve more tooth structureRemove smear layerRemove smear layer
Curettes vs. UltrasonicsCurettes vs. Ultrasonics
No difference in pocket depths between hand and ultrasonic instrumentation
Patients with heart valve defects must be Patients with heart valve defects must be premedicated with antibiotics prior to premedicated with antibiotics prior to periodontal probing, ultrasonic or hand periodontal probing, ultrasonic or hand instrumentationinstrumentation
SummarySummary
Endotoxin causes inflammation, and can be Endotoxin causes inflammation, and can be removedremovedTooth structure and gum tissue should not be Tooth structure and gum tissue should not be traumatizedtraumatizedUse antimicrobials whenever possibleUse antimicrobials whenever possiblePowered instruments, not hand instruments, Powered instruments, not hand instruments, should be used for most of the cleaningshould be used for most of the cleaning
Periodontal MaintenancePeriodontal Maintenance
Also known as . . .Also known as . . .Supportive Periodontal TherapySupportive Periodontal TherapyPeriodontal RecallPeriodontal RecallMaintenance TherapyMaintenance TherapyPhase III TherapyPhase III Therapy
Periodontal MaintenancePeriodontal MaintenanceHow Important Is Maintenance in How Important Is Maintenance in Periodontal Therapy?Periodontal Therapy?
A Key component of periodontal therapy!A Key component of periodontal therapy!70% fewer lost teeth were observed comparing untreated 70% fewer lost teeth were observed comparing untreated patients to those who received treatment and followed patients to those who received treatment and followed through with regular maintenance.through with regular maintenance.
50% improvement in tooth retention comparing treated 50% improvement in tooth retention comparing treated patients without maintenance to treated patients who were patients without maintenance to treated patients who were both treated and well maintained.both treated and well maintained.
Periodontal MaintenancePeriodontal Maintenance
Components of the Recall VisitComponents of the Recall VisitUpdate and review the medical/dental historyUpdate and review the medical/dental historyExtraoral and intraoral soft tissue examsExtraoral and intraoral soft tissue examsDental examinationDental examinationPerio evaluationPerio evaluationRadiographic reviewRadiographic reviewRemoval of plaque and SRP where indicatedRemoval of plaque and SRP where indicatedSelective polishing/Topical FluorideSelective polishing/Topical FluorideFinal OHI and dispensing of personal hygiene Final OHI and dispensing of personal hygiene implementsimplements
What determines the Interval?What determines the Interval?
Several FactorsSeveral FactorsInitial level of diseaseInitial level of diseaseAggressiveness of attachment lossAggressiveness of attachment lossPatientPatient’’s response to therapys response to therapyPatientPatient’’s ability to perform effective plaque controls ability to perform effective plaque controlPostPost--treatment stability of inflammation and treatment stability of inflammation and attachment levelsattachment levels
Periodontal MaintenancePeriodontal MaintenanceWhat Type of Biological Modulation May What Type of Biological Modulation May Be Used to Control Recurrent Periodontal Be Used to Control Recurrent Periodontal Disease in the Maintenance Patient?Disease in the Maintenance Patient?
In situations where the attachment loss is localized, In situations where the attachment loss is localized, local delivery of antibiotics or antimicrobial agents local delivery of antibiotics or antimicrobial agents such as doxycycline (Atridoxsuch as doxycycline (Atridox™™), minocycline ), minocycline (Arestin(Arestin™™), or chlorhexidine (PerioChip), or chlorhexidine (PerioChip®®) may be ) may be effective in maintaining attachment levels.effective in maintaining attachment levels.
Host ModulationHost Modulation
Subantimicrobial dose of doxycycline (SDD) has Subantimicrobial dose of doxycycline (SDD) has been advocated to help prevent attachment loss been advocated to help prevent attachment loss (PerioStat(PerioStat®®). ).
SDD stabilizes the activity of collagenase and other SDD stabilizes the activity of collagenase and other matrix metalloproteinases and, therefore, slows matrix metalloproteinases and, therefore, slows down the destructive inflammatory process.down the destructive inflammatory process.
Initial clinical studies to receive U.S. Food and Drug Initial clinical studies to receive U.S. Food and Drug Administration approval were of 9 months duration. Administration approval were of 9 months duration. There is minimal evidence of the effect of PerioStatThere is minimal evidence of the effect of PerioStat®®over longer time periods. over longer time periods.
Recall Visit ComplianceRecall Visit Compliance
How Compliant Is the Average How Compliant Is the Average Periodontal Patient?Periodontal Patient?
One study suggests that only about 16% of One study suggests that only about 16% of patients receiving periodontal therapy comply patients receiving periodontal therapy comply with recommended maintenance intervals.with recommended maintenance intervals.
Recall Visit ComplianceRecall Visit Compliance
Steps to improve patient compliance:Steps to improve patient compliance:Simplify behavioral change.Simplify behavioral change.Accommodate the patient.Accommodate the patient.Remind patients of appointments.Remind patients of appointments.Keep compliance records.Keep compliance records.Inform the patient about the necessity for and Inform the patient about the necessity for and consistency of keeping maintenance appointments.consistency of keeping maintenance appointments.Provide positive reinforcement.Provide positive reinforcement.Ensure the dentist's involvementEnsure the dentist's involvement
What are some of the reasons dentists are What are some of the reasons dentists are sued by patients related to periodontal sued by patients related to periodontal care?care?
Here are a few examples of real cases. . . Here are a few examples of real cases. . .
failure to use bacteriological monitoring of failure to use bacteriological monitoring of dental unit water lines and evacuation systems to dental unit water lines and evacuation systems to verify that chemical disinfectants have verify that chemical disinfectants have eliminated waterline biofilm buildup;eliminated waterline biofilm buildup;performing periodontal screening examinations performing periodontal screening examinations instead of comprehensive periodontal instead of comprehensive periodontal examinations before performing fullexaminations before performing full--mouth mouth restorative procedures;restorative procedures;
performing prescription periodontal surgery for bridge performing prescription periodontal surgery for bridge abutment teeth while ignoring periodontitis elsewhere, abutment teeth while ignoring periodontitis elsewhere, including adjacent or opposing teeth;including adjacent or opposing teeth;evaluating periodontal disease control by pocket evaluating periodontal disease control by pocket measurements alone and not considering bleeding on measurements alone and not considering bleeding on probing as a component of periodontal disease probing as a component of periodontal disease diagnosis;diagnosis;diagnosing pulpal disease, but failing to consider diagnosing pulpal disease, but failing to consider
periodontalperiodontal--endodontic lesions or that successful endodontic lesions or that successful endodontics may not salvage a tooth compromised with endodontics may not salvage a tooth compromised with severe periodontitis;severe periodontitis;
Impact of Systemic Disease Impact of Systemic Disease on Perio Diseaseson Perio Diseases
Diabetes MellitusDiabetes Mellitus
SmokingSmoking
HIV DiseaseHIV Disease
Heart DiseaseHeart Disease
Impact of Systemic Disease Impact of Systemic Disease
Diabetes Mellitus Diabetes Mellitus Clear associations exist between severity of Clear associations exist between severity of periodontal diseases and glycemic control.periodontal diseases and glycemic control.Controlled diabetics may receive perio treatment Controlled diabetics may receive perio treatment without restrictions.without restrictions.Uncontrolled diabetics, poorly controlled diabetics, Uncontrolled diabetics, poorly controlled diabetics, or diabetics whose control is unknown should only or diabetics whose control is unknown should only receive emergency periodontal therapy, and that receive emergency periodontal therapy, and that treatment should be performed with intraprocedural treatment should be performed with intraprocedural and/or postoperative antibiotic coverageand/or postoperative antibiotic coverage
Impact of Systemic DiseasesImpact of Systemic Diseases
SmokingSmokingLength of time an individual has been smoking and Length of time an individual has been smoking and the frequency of smoking contribute to severity of the frequency of smoking contribute to severity of periodontal disease. periodontal disease. Greater accumulation of plaque and calculus Greater accumulation of plaque and calculus Less probing depth reduction following both SRP Less probing depth reduction following both SRP and surgical periodontal therapy in smokers vs. and surgical periodontal therapy in smokers vs. nonsmokers nonsmokers Higher implant failure rates. Higher implant failure rates.
Impact of Systemic DiseasesImpact of Systemic Diseases
HIV DiseaseHIV DiseaseEarly studies described increased severity of periodontal Early studies described increased severity of periodontal diseases. diseases.
Recently, reports of no increases in the prevalence or Recently, reports of no increases in the prevalence or extent of periodontal diseases among HIVextent of periodontal diseases among HIV--positive positive individualsindividuals
Impact of Systemic Disease Impact of Systemic Disease
PregnancyPregnancyProgesterone and estrogen levels increase to levels Progesterone and estrogen levels increase to levels that are several orders of magnitude greater than that are several orders of magnitude greater than those seen during a normal menstrual cycle. those seen during a normal menstrual cycle. Varying degrees of a reversible Varying degrees of a reversible ““pregnancy pregnancy gingivitisgingivitis”” are common during pregnancy.are common during pregnancy.
Oral Contraceptives (BCP)Oral Contraceptives (BCP)May see cyclic changes of pregnancyMay see cyclic changes of pregnancy--like changes.like changes.
Antibiotics in PeriodonticsAntibiotics in Periodontics
What is AntiWhat is Anti--infective Periodontal therapy?infective Periodontal therapy?It is the use of local and systemic agents to It is the use of local and systemic agents to control the bacterial etiology of the inflammatory control the bacterial etiology of the inflammatory periodontal diseases. periodontal diseases.
These agents include both locally and systemically These agents include both locally and systemically delivered antibiotics and chemotherapeutic delivered antibiotics and chemotherapeutic agents.agents.
Antibiotics in PeriodonticsAntibiotics in PeriodonticsWhen are antibiotics indicated in periodontics?When are antibiotics indicated in periodontics?
Periodontal abscess Periodontal abscess Aggressive periodontitisAggressive periodontitisChronic periodontitis with severe gingival inflammation or as anChronic periodontitis with severe gingival inflammation or as anadjunct to SRP adjunct to SRP Refractory forms of the periodontal diseasesRefractory forms of the periodontal diseasesProphylaxis for SBEProphylaxis for SBEWhen surgery is contraindicated or not desired and When surgery is contraindicated or not desired and inflammation persists after thorough root instrumentationinflammation persists after thorough root instrumentationAs a host modulation technique As a host modulation technique −− subantimicrobial dose to subantimicrobial dose to stabilize collagenase stabilize collagenase
Antibiotics in PeriodonticsAntibiotics in Periodontics
What are some common ones to use?What are some common ones to use?Amoxicillin (with or without clavulanic acid Amoxicillin (with or without clavulanic acid AugmentinAugmentin®®))MetronidazoleMetronidazoleCiprofloxacinCiprofloxacinClindamycinClindamycinDoxycyclineDoxycyclineAzithromycinAzithromycin
The use of subantimicrobial dose of The use of subantimicrobial dose of doxycycline (SDD) has been shown to reduce doxycycline (SDD) has been shown to reduce the rate and amount of attachment loss the rate and amount of attachment loss associated with advancing periodontal disease. associated with advancing periodontal disease. SDD is currently used as a 20 mg dose of SDD is currently used as a 20 mg dose of doxycycline twice a day, available commercially doxycycline twice a day, available commercially under the name PerioStatunder the name PerioStat®®. . LongLong--term studies have been for 9term studies have been for 9--month month durations. durations.
Indications for Locally Delivered Indications for Locally Delivered Antibiotic and Antimicrobial TxAntibiotic and Antimicrobial Tx
Local site(s) with signs of inflammation that Local site(s) with signs of inflammation that have not responded to conventional mechanical have not responded to conventional mechanical therapytherapyLocal site that has recurrent signs of Local site that has recurrent signs of inflammation at a maintenance visitinflammation at a maintenance visitBuying time for a soBuying time for a so--called hopeless tooth called hopeless tooth before extractionbefore extractionResolving marginal inflammation when oral Resolving marginal inflammation when oral hygiene has reached maximum effectivenesshygiene has reached maximum effectiveness
What therapeutic Mouth rinses are available to What therapeutic Mouth rinses are available to
Reduce Plaque and Help Control Gingival Inflammation?Reduce Plaque and Help Control Gingival Inflammation?
Currently, only mouth rinses containing 0.12% Currently, only mouth rinses containing 0.12% chlorhexidine gluconate (Peridex) or the chlorhexidine gluconate (Peridex) or the ““essential oilsessential oils””(phenolic compounds (phenolic compounds −− thymol, menthol, eucalyptol, thymol, menthol, eucalyptol, methyl salicylate) are able to reduce plaque and gingivitis. methyl salicylate) are able to reduce plaque and gingivitis.
These mouth rinses are available to consumers through a These mouth rinses are available to consumers through a variety of manufacturers and distributors, and must be used variety of manufacturers and distributors, and must be used appropriately, usually a 30appropriately, usually a 30--second rinse twice daily to be second rinse twice daily to be effectiveeffective
Occlusal TherapyOcclusal Therapy
What is Occlusal Traumatism?What is Occlusal Traumatism?Signs and Symptoms of Occlusal TraumatismSigns and Symptoms of Occlusal Traumatism
Fractures, occlusal wear or inflammation of Fractures, occlusal wear or inflammation of supporting structures (bone and pdl) supporting structures (bone and pdl)
Other signs and symptomsOther signs and symptomsPain, Pain, Mobility and fremitusMobility and fremitusRadiographic widening of the pdl space.Radiographic widening of the pdl space.
Primary Occlusal TraumaPrimary Occlusal Trauma
Excessive forces Excessive forces along a healthy along a healthy periodontiumperiodontiumCrown root ratio Crown root ratio is 1:2 and center is 1:2 and center of rotation is in of rotation is in the coronal 1/3 the coronal 1/3 of the root.of the root.
CAPT Nick Makrides, Chief Dentist, BOPCAPT Nick Makrides, Chief Dentist, BOPCAPT Tim Ricks, IHS Nashville Area DirectorCAPT Tim Ricks, IHS Nashville Area DirectorCAPT Bill Stenberg, CG PeriodontistCAPT Bill Stenberg, CG PeriodontistDr. Debra Lacy, Clinical Director, MCC San DiegoDr. Debra Lacy, Clinical Director, MCC San Diego
Reference TextReference Text
Manual of Clinical Manual of Clinical PeriodonticsPeriodontics , 2, 2ndnd Edition Edition by Francis by Francis SerioSerio and Charles Hawleyand Charles HawleyCopyright (c) Copyright (c) LexiLexi--Comp, Inc. 1978Comp, Inc. 1978--2008 All Rights 2008 All Rights Reserved.Reserved.
Great narratives, clinical photographs, and online accessGreat narratives, clinical photographs, and online access
Many of the slides from this presentation are found in this Many of the slides from this presentation are found in this source!source!