43
Robert N. Cuyler, Ph.D., Senior Associate, OPEN MINDS The 2014 OPEN MINDS Planning & Innovation Institute June 3, 2014 | 11:15am – 12:30pm

Robert N. Cuyler, Ph.D., Senior Associate, OPEN MINDS
The 2014 OPEN MINDS Planning & Innovation Institute
June 3, 2014 | 11:15am – 12:30pm

I. Overview Of The Current Telehealth Market
II. Telehealth In An Integrated Environment
III. Telehealth Case Studies • Sherrie Williams, LCSW, Executive Director,
Georgia Partnership For Telehealth
• Bob Franko, Vice President, Marketing & National Training Coordinator, Cherokee Health Systems, Inc.
• Jonathan Evans, President & Chief Executive Officer, Safe Harbor Behavioral Health
IV. Questions & Discussion

Overview Of The Current Telehealth Market
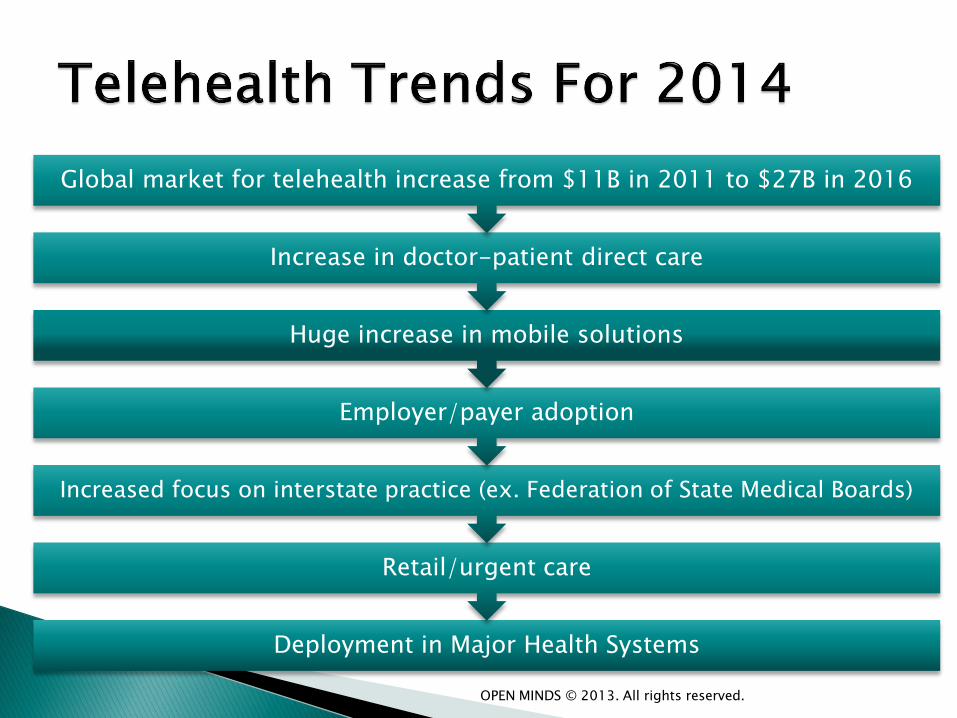
Deployment in Major Health Systems
Retail/urgent care
Increased focus on interstate practice (ex. Federation of State Medical Boards)
Employer/payer adoption
Huge increase in mobile solutions
Increase in doctor-patient direct care
Global market for telehealth increase from $11B in 2011 to $27B in 2016
OPEN MINDS © 2013. All rights reserved.

Least complex
technology needs
of any medical
specialty
Just two talking
heads, no need to
‘lay hands’
Robust empirical
base
Readily adopted by
consumers
Practitioners are
clustered in urban
settings
Huge needs in
limited-access
settings
Interstate Practice
limited by
practitioner
license
OPEN MINDS © 2013. All rights reserved.
“The best evidence for telemedicine, especially live interactive
office/hospital-based telemedicine is in the psychiatry and neurology
specialties”
“Verbal interaction is the key assessment component”
ARHQ Research Review - Locatis & Ackerman, NIMH, 2013
• Telemental health services are unquestionably effective in most regards, although more analysis is needed.
• Effective for diagnosis and assessment, across many populations (adult, child, geriatric, and ethnic)
• For disorders in many settings (emergency, home health)
• Are comparable to in-person care, and complement other services in primary care.
Hilty et al 2013 Meta Analysis
• Standards of care defined by states, vary widely
• Restrictions on interstate practice of medicine
• Federation of State Medical Boards attempting to improve portability
• Patchwork reimbursement policies
• Interoperability of Health Records
• Incentives for Providers
• Shift from grant to sustainable and business-viable remains work in progress
• Reimbursement climate improving but fragmented
• Lack of exposure/training in clinical education
• Best fit when provides system leverage
• No business model has emerged as winner yet

Telehealth In An Integrated Environment
• 14% of population receive treatment for BH, but account for 30% of healthcare spending
• Fragmentation of care increases spending and worsens outcomes
• Costs for treating co-morbid conditions two-to-three times higher than ‘uncomplicated’ physical heath problems
• Effective integration could save $26-48 Billion annually ◦ Milliman Report: Economic Impact of Integrated
Medical-Behavioral Healthcare, April, 2014
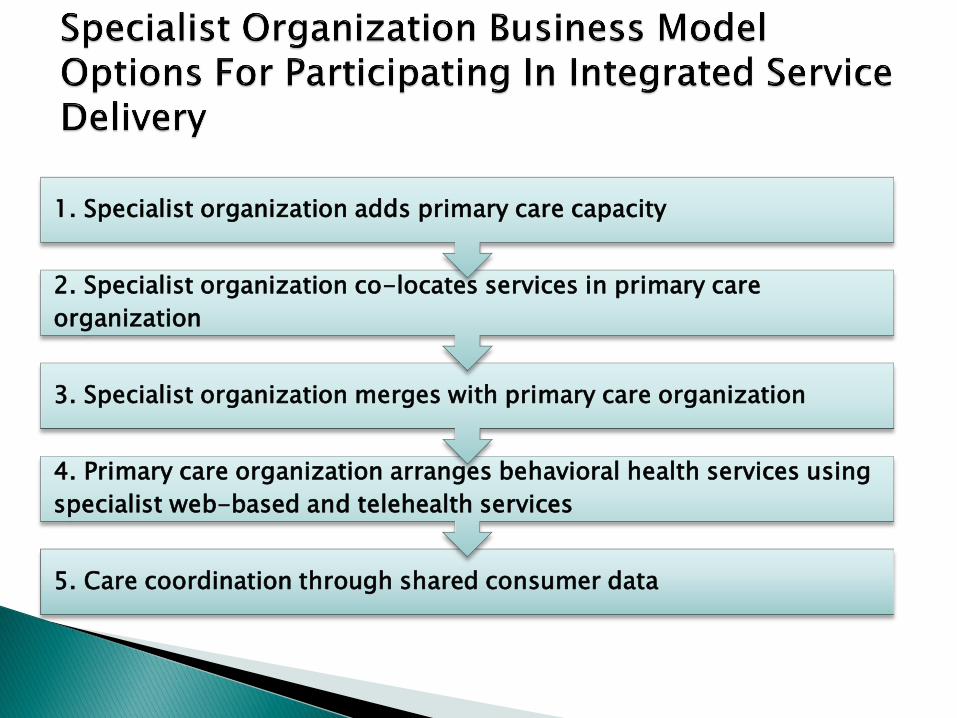
5. Care coordination through shared consumer data
4. Primary care organization arranges behavioral health services using
specialist web-based and telehealth services
3. Specialist organization merges with primary care organization
2. Specialist organization co-locates services in primary care
organization
1. Specialist organization adds primary care capacity
• Behavioral health services have historically been “siloed”
• Limited models for collaboration
• Problems in maintaining rapid access of behavioral health specialists in physically co-located settings
• Problems in providing access to care in smaller and/or de-centralized primary care settings
• Provider shortage and lack of access outside of urban areas
• Demographics of psychiatrists (aging, limited emergency access, boutique/quality of life choices)

• Telemedicine can be a distribution system for all professionals
• Deliver multi-disciplinary team to all locations
• Can individualize care regardless of location (ex. PTSD, family therapy, eating disorder)

• Can be organized as internal network for larger systems or contracted network for smaller systems
• Dependent on shift away from fee-for-service
• Dependent on risk-based payment systems
• Dependent on system architects to recognize and prioritize innovating behavioral health delivery
• Must be strategically driven by system leadership
• Potential to physically co-locate in central or hub setting and reach other ‘spoke’ sites via telehealth
• Advantage of strong IT resources and integrated system EMR
• System can select, manage, and set priorities of behavioral health providers
• Compensation systems more readily designed for practitioner productivity, quality control, shared savings

• Multi-hospital Health System
• Internal or Contracted Behavioral Heath Network
• Primary Care & Clinic Network
• Single EMR & Integrated Telehealth Network
• May be hub to Rural Hospital ‘Spokes’
• Will open opportunities for inter-organizational work
• RFP to provider groups/networks to provide behavioral health integration
• Fee structure may range from fee-for-service, contracted rates, capitation, or shared savings
• Opportunity for behavioral heath networks to develop solution/services and offer services to multiple ACO organizations
• Technology platform more complicated as ‘between-organization’ system without centrally-controlled IT, purchasing, technical support
• But … allows smaller organizations to participate in behavioral health integration without co-location
• Single or Small System Hospital without Behavioral Health Department
• Reach extends to owned/affiliated Primary Care, FQHC, or Rural Heath Clinic
• Reach may extend to long-term care
• Size & resources will not support internal behavioral health providers
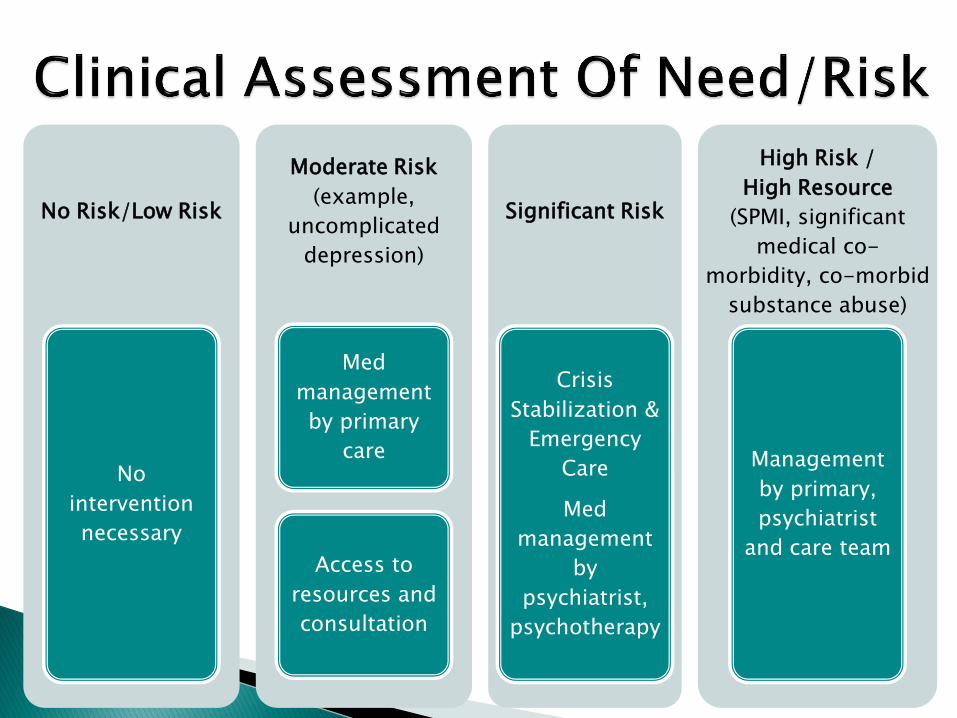
No Risk/Low Risk
No
intervention
necessary
Moderate Risk
(example,
uncomplicated
depression)
Med
management
by primary
care
Access to
resources and
consultation
Significant Risk
Crisis
Stabilization &
Emergency
Care
Med
management
by
psychiatrist,
psychotherapy
High Risk /
High Resource
(SPMI, significant
medical co-
morbidity, co-morbid
substance abuse)
Management
by primary,
psychiatrist
and care team
• Opened 120,000 sq. ft. Virtual Care Center
• To support 75 telemedicine offerings
• Range: 24/7 Nurse Call Center
• Home Monitoring
• Tele-ICU
• Projects 3 million visits over 5 years
• System has 300,000 lives in revenue-sharing reimbursement models
• Primary Care locations will offer behavioral health services via co-location & telehealth consultation
• Focus: Team-based management of behavioral health problems in primary care
• Goals: ◦ Improve outcomes for chronic and co-morbid
conditions ◦ Reduce physician burnout via team approach ◦ Lower cost of care by reducing ED visits &
hospitalization
• Massive paradigm shift underway in health care
• Telemedicine has been ‘about to happen’
• Expect tipping point for telemedicine as risk-based payment begins to escalate
• Only practical way to supply right practitioner at right time at right location
• Technology is ready for prime time
• Technology integration not yet ready (interoperability of EMRs is key)
• Lack of exposure and training for practitioners
• Telemedicine training and certification will be essential
• Systems and payers will favor knowledgeable providers and BH systems
Telehealth Case Studies
• Sherrie Williams, LCSW, Executive Director, Georgia Partnership For Telehealth
• Bob Franko, Vice President, Marketing & National Training Coordinator, Cherokee Health Systems, Inc.
• Jonathan Evans, President & Chief Executive Officer, Safe Harbor Behavioral Health

+
TeleMental Health
Lessons Learned From the
Frontline of Care
+ Georgia Partnership For Telehealth
GPT Headquarters is located in Waycross, Ga.
Extended offices in Atlanta and Prattville, AL
Field-Based TM Liaisons
Support for Credentialing and Scheduling
All Specialists & Allied Healthcare Providers are required to complete the modified application that is accepted by The Joint Commission.
Dedicated toll free scheduling line.
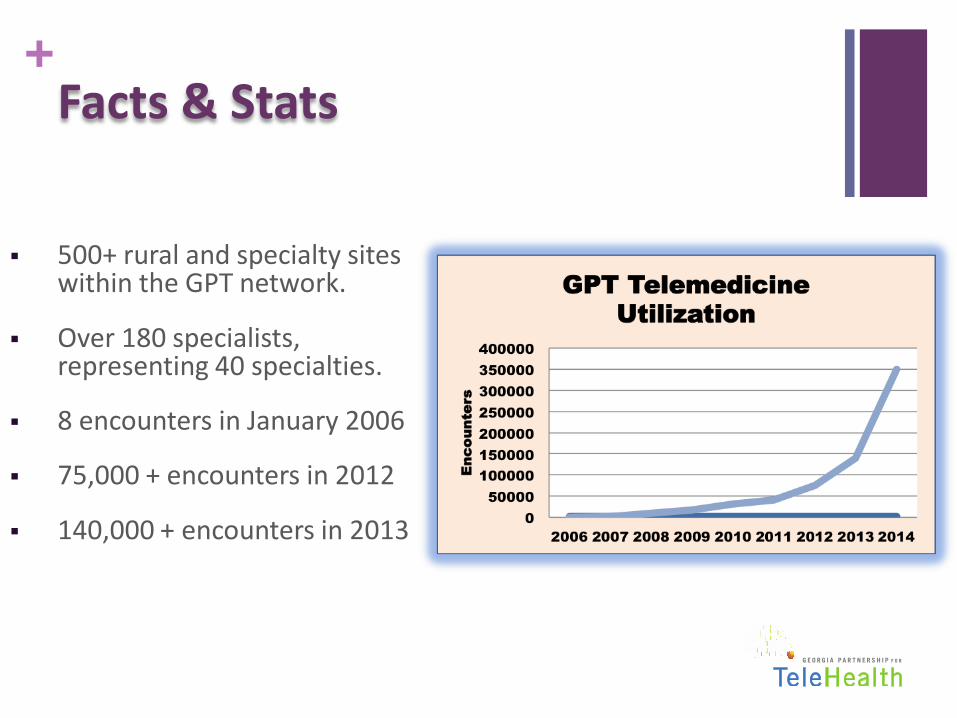
+ Facts & Stats
500+ rural and specialty sites within the GPT network.
Over 180 specialists, representing 40 specialties.
8 encounters in January 2006
75,000 + encounters in 2012
140,000 + encounters in 2013

+
“Open Access” Network Model
Creates a web of access points
Any Presentation Site can connect to any other site
Specialty
Center
Specialty
Center
Specialty
Center
Presentation
Site
Presentation
Site
Presentation
Site Presentation
Site

+
+ What We Know
In GA, severe deficit of mental health care providers
376 HPSAs
National mental health HPSA = 3900
Need at least 2600 more psychiatrists to fill gap
Since GPT was developed, Mental Health has ranked as the
top 3 requested services:
C&A Psychiatry
Adult Psychiatry
Geriatric Psychiatry
+ Lessons Learned
Commitment from providers and presentation sites
Providers must understand that telemedicine patients are
treated just like traditional face-to-face patients
Quality of connectivity has to be reliable and crisp
Large screens are better than smaller monitors
Sound has to be good
Contract vs. billing

+ Environments For Care
Corrections
Schools
Community Health Centers
Public Health Departments
SNFs
Hospitals
Private practices
+ PRESENTER
Sherrie Williams, LCSW
Georgia Partnership For Telehealth
Executive Director
Utilization of Telepsychiatry in an Integrated Model of Care
Jonathan Evans
President & CEO
InnovaTel Telepsychiatry. LLC
Telepsychiatry Implementation
• Safe Harbor Behavioral Health pioneered telepsychiatry regionally in 2007, with a SAMSHA Grant.
• 2010 telepsychiatry expansion to a full time employed psychiatrist.
• 2012, providing 20 hours weekly to rural clinic in PA .
• 2013,expansion in multi-state clinics.
Compass Grant
• Compass team consists of nurse care managers,
psychiatrist, PCP and internists. • 2013, Compass Grant with St. Vincent’s Medical Center
to provide telepsych consultation service to 35 physicians in the primary care network.
• Weekly consultation meetings scheduled for case review and consultation.
• Screenings PHQ9 depression rating scales completed on patients during normal outpatient visits.
• A compass nurse care manager calls patients to determine stressors and barriers to care/recovery.

Compass Grant
• The team meets weekly via conference call to review all patients in the program. The telepsychiatrist will make treatment recommendations
• Starting an SSRI, consider switching meds due to blood pressure concerns, recommending therapy.
• Average LOS in the program is 6 months.

Compass Program Results (Unpublished)
• Many patients evaluated by psychiatrist in a timely manner vs. typical months waiting time.
• Multiple issues addressed at once via consultation with nurse care manager linking patient to community resources.
• Consultation model allows many cases for review in an hour.


www.openminds.com [email protected]
717-334-1329 | 877-350-6463 163 York Street, Gettysburg , Pennsylvania 17325
The market intelligence to navigate. The management expertise to succeed.

















