National Center for Emerging and Zoonotic Infectious Diseases Division of Vector-Borne Diseases Updated August 5, 2016 Overview of Tick Borne Viral Diseases Christopher J. Gregory, MD, MPH Chief, Arboviral Diseases Branch Division of Vector-borne Diseases National Center for Emerging and Zoonotic Infectious Diseases U.S. Centers for Disease Control and Prevention
Transcript
National Center for Emerging and Zoonotic Infectious DiseasesDivision of Vector-Borne Diseases
Updated August 5, 2016
Overview of Tick Borne Viral Diseases
Christopher J. Gregory, MD, MPHChief, Arboviral Diseases Branch
Division of Vector-borne DiseasesNational Center for Emerging and Zoonotic Infectious Diseases
U.S. Centers for Disease Control and Prevention
LEARNING OBJECTIVES
Learn about ticks and tick-borne viral diseases including:
– Tick entomology
– Virology and transmission
– Epidemiology
– Clinical features
– Diagnosis
– Treatment and prevention
OUTLINE• Ticks 101• Key tick-borne diseases, their distributions and
vectors • Current disease burden, trends and drivers• Tick borne viruses• Tick-borne disease prevention
Ticks 101
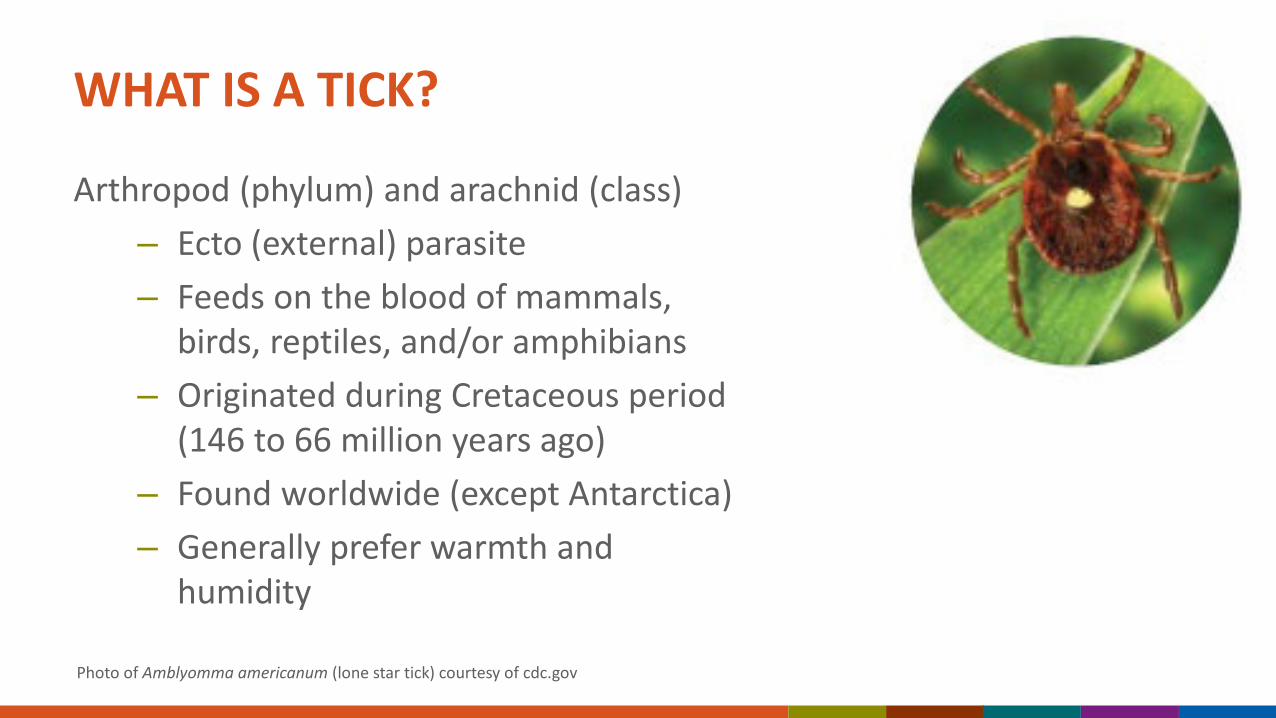
WHAT IS A TICK?
Arthropod (phylum) and arachnid (class)– Ecto (external) parasite – Feeds on the blood of mammals,
birds, reptiles, and/or amphibians– Originated during Cretaceous period
(146 to 66 million years ago)– Found worldwide (except Antarctica)– Generally prefer warmth and
humidity
Photo of Amblyomma americanum (lone star tick) courtesy of cdc.gov
HARD TICKSFamily Ixodidae
– Hard dorsal plate or scutum– Mouth parts visible from above– “Quests” for a host in tall vegetation– Can stay attached and feed for days– Amblyomma spp.– Dermacentor spp. – Ixodes spp.– Rhipicephalus spp.
Photo of Ixodes scapularis (blacklegged tick / deer tick) courtesy of cdc.gov
SOFT TICKSFamily Argasidae
– No hard dorsal plate or scutum– Mouth parts underneath body and not
visible from above– Lives near burrows, nests, rustic cabins – Sneaks up and attaches at night– Does not stay attached or feed for long– Less likely to bite humans– Ornithodoros spp.
Photo of Ornithodoros spp. soft tick courtesy of cdc.gov
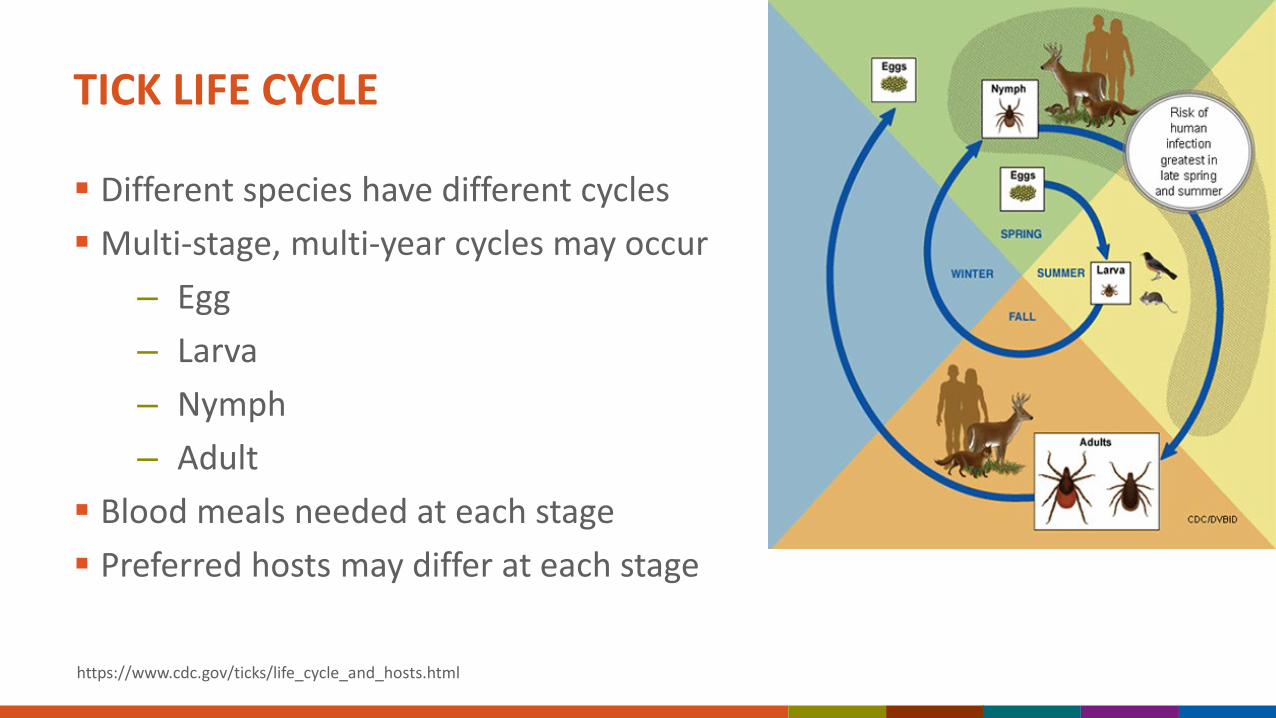
TICK LIFE CYCLE
Different species have different cycles Multi-stage, multi-year cycles may occur
– Egg– Larva– Nymph– Adult
Blood meals needed at each stage Preferred hosts may differ at each stage
TICK QUESTING Ticks cannot fly or jump Many hard ticks “quest” to find a host
– Perch at end of vegetation– Outstretch front legs– Wait for host to walk by
Questing site chosen based on CO2, other odors, shadows, vibrations, etc. Larvae quest lower for smaller hosts Nymphs/adults quest higher for bigger hosts
Photos of hard ticks questing courtesy of Griffin Dill at the University of Mainehttps://extension.umaine.edu/ipm/tickid/tick-biology/
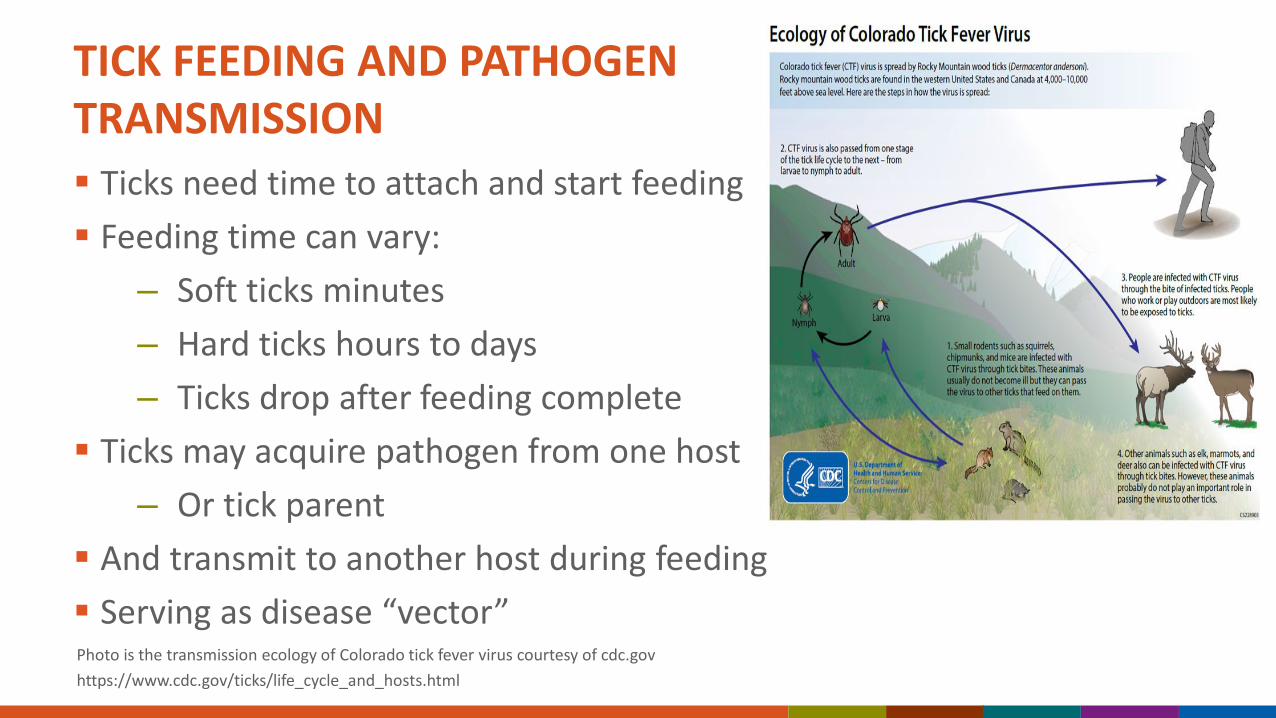
TICK FEEDING AND PATHOGEN TRANSMISSION Ticks need time to attach and start feeding Feeding time can vary:
– Soft ticks minutes– Hard ticks hours to days – Ticks drop after feeding complete
Ticks may acquire pathogen from one host– Or tick parent
And transmit to another host during feeding Serving as disease “vector” Photo is the transmission ecology of Colorado tick fever virus courtesy of cdc.govhttps://www.cdc.gov/ticks/life_cycle_and_hosts.html
Key tick-borne diseases, their distributions and vectors
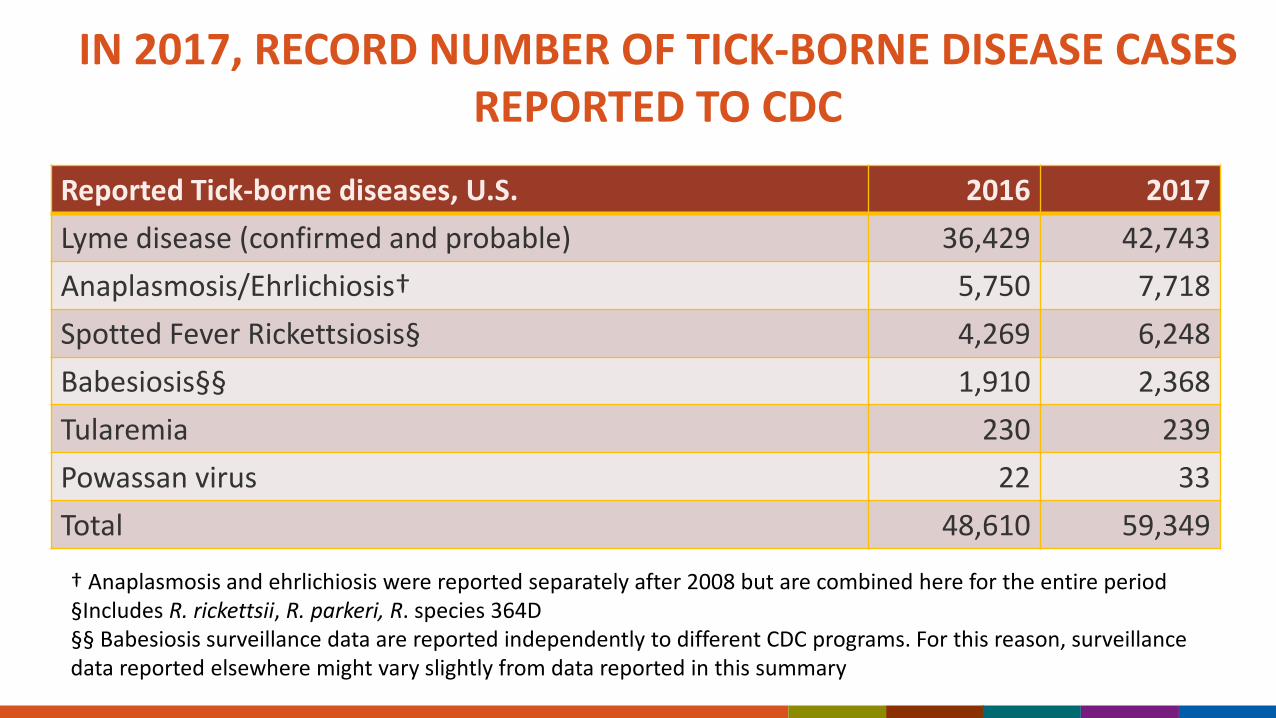
NATIONALLY NOTIFIABLE TICK-BORNE DISEASES IN THE U.S.
† Anaplasmosis and ehrlichiosis were reported separately after 2008 but are combined here for the entire period§Includes R. rickettsii, R. parkeri, R. species 364D§§ Babesiosis surveillance data are reported independently to different CDC programs. For this reason, surveillance data reported elsewhere might vary slightly from data reported in this summary
• All reportable conditions are subject to under-reporting.• Magnitude of under-reporting less for diseases that:
– Are rare or unusual– Require hospitalization– Have a definitive diagnostic test
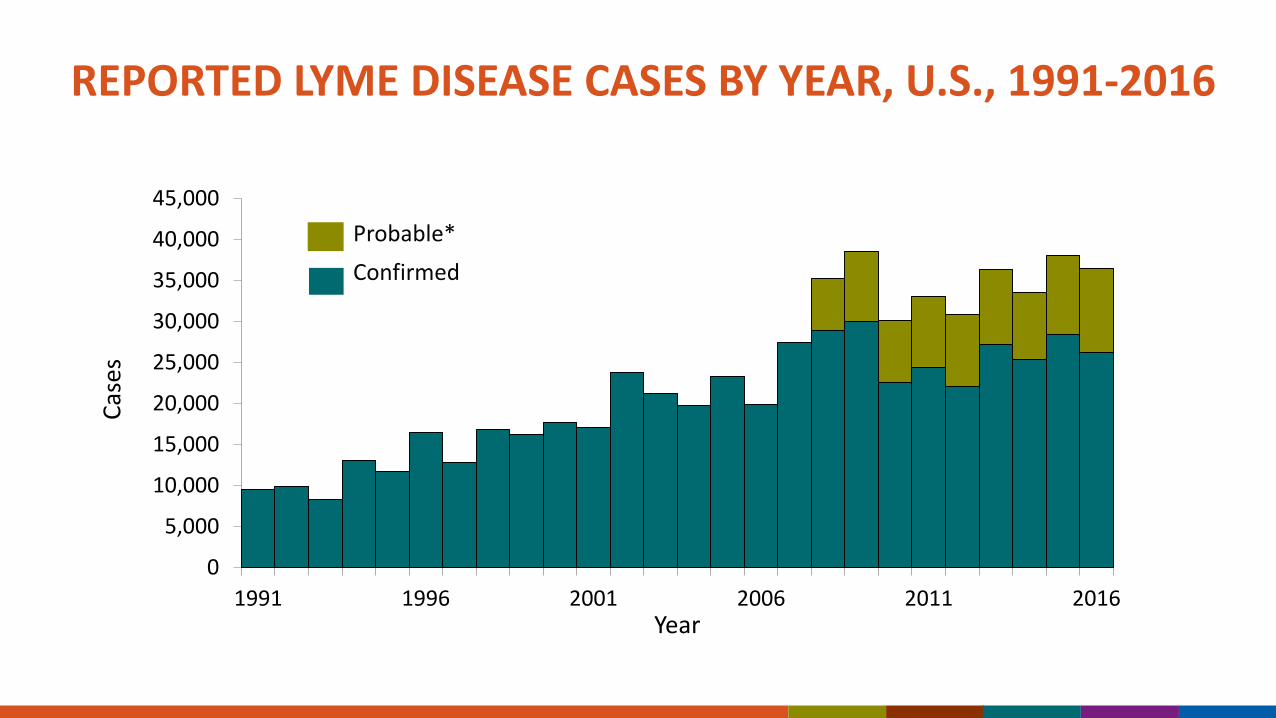
• Principal reasons for under-reporting of Lyme disease:– Busy health care providers don’t fill out the report form.– Health departments do not have time to follow up on missing
information.
ROCKY MOUNTAIN SPOTTED FEVER
Rickettsiae released into bite site within a few hours after attachment
Incubation period following tick bite: 3-12 days (4-8 days in most patients)
Inverse correlation between incubation period and illness severity
Treatment of choice - doxycycline
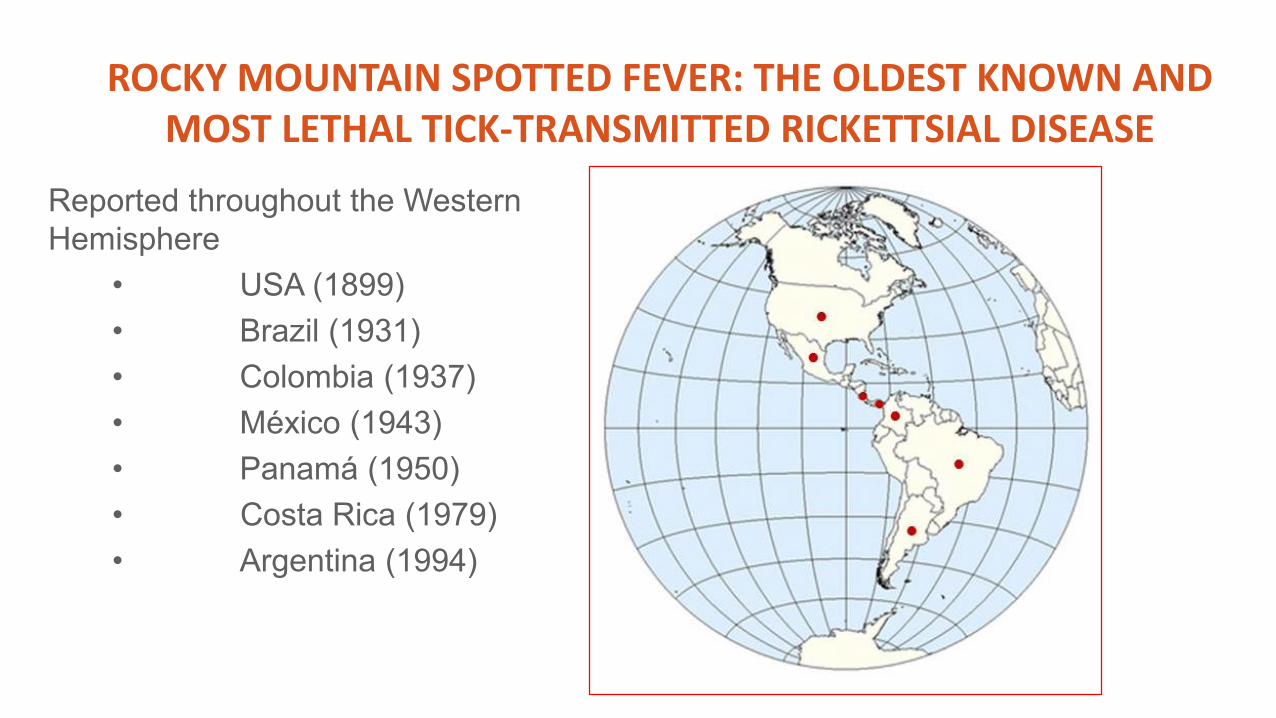
Reported throughout the Western Hemisphere
• USA (1899)• Brazil (1931) • Colombia (1937) • México (1943)• Panamá (1950)• Costa Rica (1979)• Argentina (1994)
ROCKY MOUNTAIN SPOTTED FEVER: THE OLDEST KNOWN AND MOST LETHAL TICK-TRANSMITTED RICKETTSIAL DISEASE
PATHOGENIC ANAPLASMATACAE OF HUMANS IN U.S, 2018
• Ehrlichia chaffeensis (1987)
• Anaplasma phagocytophilum (1994)
• Ehrlichia ewingii (1999)
• Ehrlichia muris euclairensis (2011)
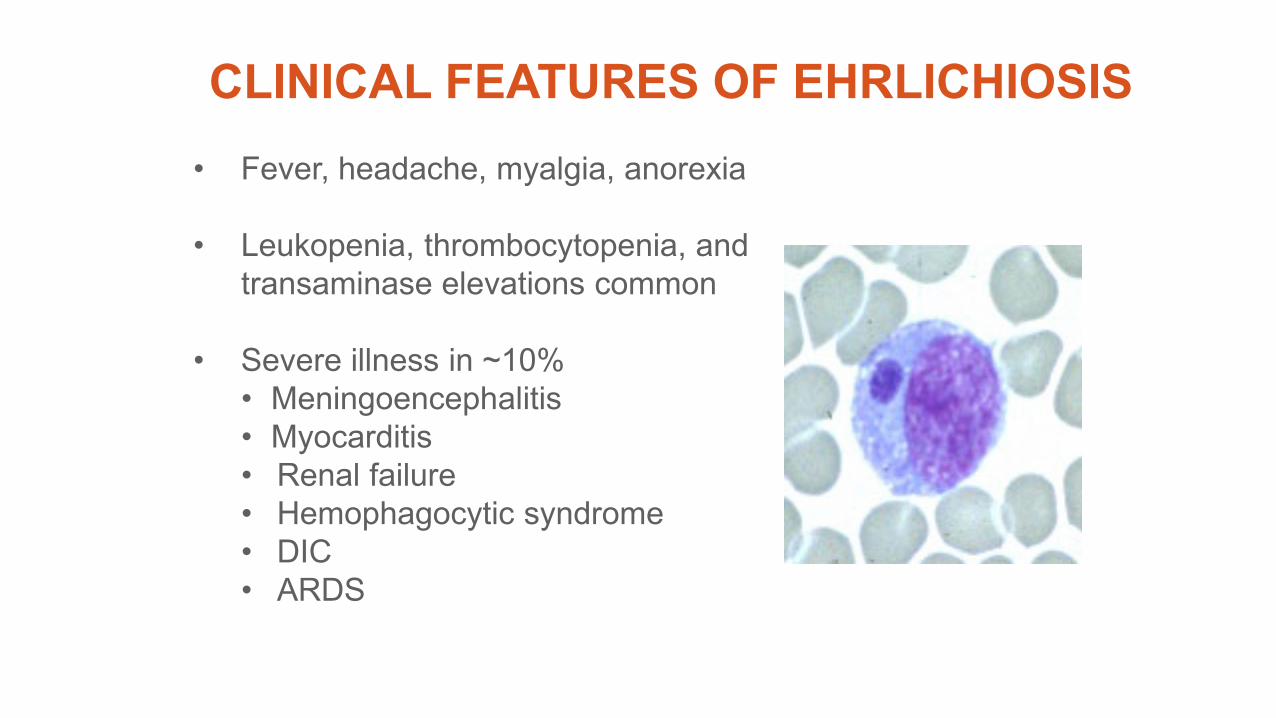
CLINICAL FEATURES OF EHRLICHIOSIS• Fever, headache, myalgia, anorexia
• Leukopenia, thrombocytopenia, and transaminase elevations common
• Severe illness in ~10%• Meningoencephalitis• Myocarditis• Renal failure• Hemophagocytic syndrome• DIC• ARDS
• Case fatality rate <1%, deaths occur predominantly in persons >70 years-of-age
• Multiple instances of transfusion-associated anaplasmosis reported
Disease trends and drivers
DISCOVERY OF TICK-BORNE PATHOGENS AS CAUSES OF HUMAN DISEASE BY YEAR, 1960–2016
• Year represents when tickborne pathogen was recognized as cause of human disease.• Adapted from: Paddock CD, Lane RS, Staples JE, Labruna MB. 2016. In: Mack A, Editor. Global health impacts of vector-borne diseases:
workshop summary. National Academies Press. p. 221-257.
Rickettsia 364D
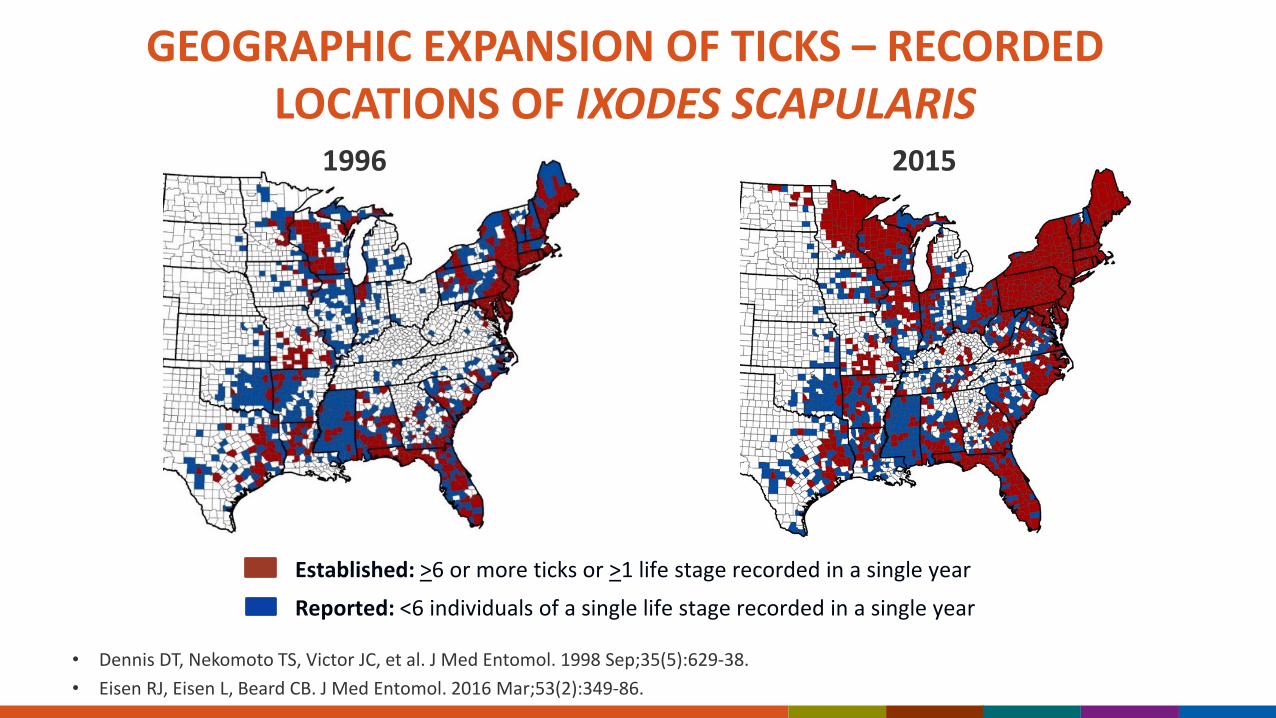
GEOGRAPHIC EXPANSION OF TICKS – RECORDED LOCATIONS OF IXODES SCAPULARIS
Established: >6 or more ticks or >1 life stage recorded in a single year
Reported: <6 individuals of a single life stage recorded in a single year
1996 2015
• Dennis DT, Nekomoto TS, Victor JC, et al. J Med Entomol. 1998 Sep;35(5):629-38.• Eisen RJ, Eisen L, Beard CB. J Med Entomol. 2016 Mar;53(2):349-86.
TICK-BORNE DISEASE EMERGENCE – RE-EMERGENCE IN THE U.S.
• Reforestation• Overabundant deer • Expansion of suburbia into wooded
areas• Abundant habitat around homes
for Lyme reservoir hosts • Increased numbers of ticks• Increased exposure opportunities
in people • Changing climate
Source: Bald hills: New England before the trees returned. From Thoreau's Country.American Scientist Onlinehttp://www.amercanscientist.org
Source: K. Stafford, CT Agricultural Experiment Station
CLIMATE, WEATHER, AND TICK-BORNE DISEASES Warmer annual temperatures will result in a generally
northward expansion in tick distribution. Warmer temperatures increase reproductive capacity of ticks,
leading to larger populations of ticks. Higher moisture levels allow tick survival in warmer
environments. With milder winters and earlier springs, tick vectors will likely
show earlier seasonal activity. Larger tick populations, longer seasonal activity and
expanding range of ticks will likely increase risk of human exposure to infected tick. Brownstein, J. S., T. R. Holford, and D. Fish. 2003. Environ Health Persp 111: 1152-1157 Eisen, L., R. J. Eisen, and R. S. Lane. 2002. Med Vet Entomol 16: 235-244 Yuval, B., and A. Spielman. 1990. J Med Entomol 27: 196-201 Moore, S. M., R. J. Eisen, A. Monaghan, and P. Mead. 2014. Am J Trop Med Hyg 90: 486-496Beard, C.B., Eisen, R.J., Barker, C.M. et al. 2016. The Impacts of Climate Change on Human Health in the United States: A ScientificAssessment. U.S. Global Change Research Program, Washington, DC, 129–156. http://dx.doi.org/10.7930/J0765C7V
HAEMOPHYSALIS LONGICORNIS (ASIAN LONGHORNED TICK)
• Discovered in New Jersey in 2017, and now reported from 10 states – Arkansas, Connecticut, Kentucky, Maryland, North Carolina, New
Jersey, New York, Pennsylvania, Virginia, and West Virginia– Documented in 49 counties
• Reported from 15 animal species and from humans• Pathogens found in these ticks elsewhere that are in the U.S., include
Borrelia, Anaplasma, Ehrlichia, Rickettsia, Babesia, and Theileria. • Additional concerns about potential transmission of viral pathogens
in the U.S., including Heartland and Powassan viruses • Potential for broad U.S. distribution
Sources:Beard CB, et al. Multistate Infestation with the Exotic Disease–Vector Tick Haemaphysalis longicornis —United States, August 2017–September 2018. MMWR Morb Mortal Wkly Rep. Vol. 67 , 2018.
National Haemaphysalis longicornis (Asian longhorned tick) Situation Report. November 13, 2018. USDA
Tick-borne viruses
POWASSAN VIRUS: VIROLOGY AND TRANSMISSION Single-stranded RNA flavivirus in Flaviviridae
– Tick-borne encephalitis (TBE) virus serogroup Two viral lineages:
– POW 1: Identified in Powassan, Ontario, in 1958– POW 2 (deer tick virus): Identified in northern Colorado in 1952– Clinically and serologically indistinguishable (only molecularly)
Reservoirs include small and medium-size mammals Transmission cycle:
– POWV 1: Ixodes cookei and woodchucks; Ixodes marxi and squirrels– POWV 2: Ixodes scapularis and white-footed mice
Photos of Ixodes cookei (woodchuck tick) courtesy of cdc.gov https://www.cdc.gov/powassan/index.html
POWASSAN VIRUS : EPIDEMIOLOGY
POW virus circulates throughout northern U.S., Canada, and eastern Russia Most POW virus disease cases reported from
Northeast and Great Lakes states– Surveillance bias?
Most cases occur May–November Male predominance Increasing reported cases over time
– True increase or better surveillance?
Map is reported POWV disease cases (based on residence) from 2008–2017; graph is number of reported cases in U.S. per year; both courtesy of cdc.govKrow-Lucal ER, Lindsey NP, Fischer M, Hills SL. Powassan Virus Disease in the United States, 2006-2016. Vector Borne Zoonotic Dis. 2018;18(6):286-290.
POWASSAN: CLINICAL FEATURES Most infected are asymptomatic
– Exact asymptomatic rate unknown Incubation period 1–4 weeks Initial flu-like illness with headache May progress to meningitis and/or encephalitis
– CSF pleocytosis (L or N) with normal glucose– May have widespread lesions and cerebral edema– 10% mortality; 50% long-term neurologic sequelae
MRI Brain FLAIR sequences showing cerebellar, midbrain, and medial temporal lesions in POWV disease courtesy of Drs. Jennifer Lyons and Amanda PiquetPiantadosi A, Rubin DB, McQuillen DP, et al. Emerging Cases of Powassan Virus Encephalitis in New England. Clin Infect Dis. 2016;62(6):707-713.https://www.cdc.gov/powassan/index.html
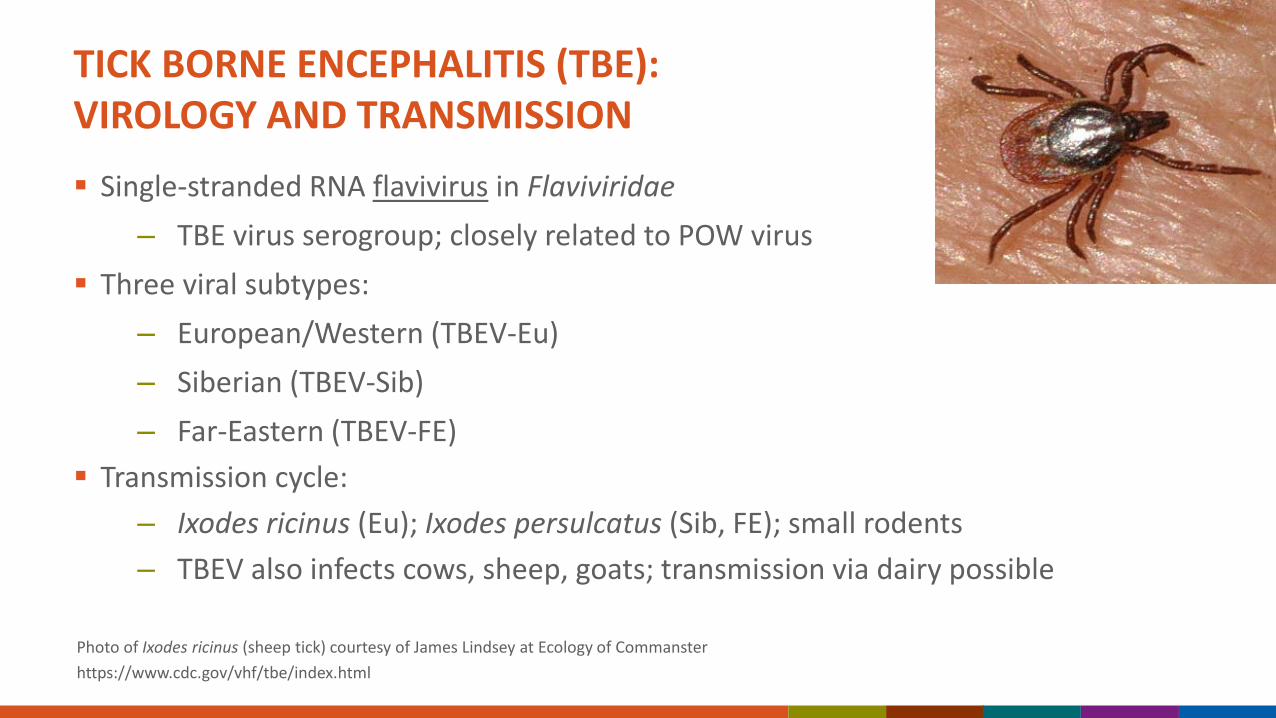
TICK BORNE ENCEPHALITIS (TBE): VIROLOGY AND TRANSMISSION
Single-stranded RNA flavivirus in Flaviviridae– TBE virus serogroup; closely related to POW virus
Three viral subtypes:– European/Western (TBEV-Eu)– Siberian (TBEV-Sib)– Far-Eastern (TBEV-FE)
Transmission cycle:– Ixodes ricinus (Eu); Ixodes persulcatus (Sib, FE); small rodents– TBEV also infects cows, sheep, goats; transmission via dairy possible
Photo of Ixodes ricinus (sheep tick) courtesy of James Lindsey at Ecology of Commansterhttps://www.cdc.gov/vhf/tbe/index.html
TBE: EPIDEMIOLOGY
TBE virus circulates from central Europe across Russia to northeastern Asia 5,000–13,000 TBE virus disease cases reported
annually– Russia with most reported cases
Most cases occur April–November Spending time in forested areas (e.g., camping,
hiking, hunting) highest risk Ingesting unpasteurized dairy also risk
Map is TBEV risk area; photo is of unpasteurized milk; both courtesy of cdc.govhttps://wwwnc.cdc.gov/travel/yellowbook/2018/infectious-diseases-related-to-travel/tickborne-encephalitis
TBE: CLINICAL FEATURES
Approximately 2/3 infected are asymptomatic Incubation period 1–2 weeks (shorter for ingestion) Biphasic disease possible
– First phase: Non-specific flu-like illness, 2/3 recover– Second phase: 1/3 may progress to meningitis, encephalitis, or
myelitis after period of remission TBEV-European disease generally milder (2% mortality) TBEV-Far Eastern disease more severe (20-40% mortality) Inactivated TBEV vaccine available in Europe
MRI Brain FLAIR sequence showing basal ganglia lesions in TBEV disease courtesy of J Zajkowska and cdc.govZajkowska J, Moniuszko A, et al. Chorea and Tick-Borne Encephalitis, Poland. Emerg Infect Dis. 2013;19(9):1544-1545.https://wwwnc.cdc.gov/travel/yellowbook/2018/infectious-diseases-related-to-travel/tickborne-encephalitis
COLORADO TICK FEVER (CTF): VIROLOGY AND TRANSMISSION
Double-stranded RNA coltivirus in Reoviridae Transmission cycle:
chipmunks) Rare transmission through blood transfusion or laboratory
exposures Intracellular infection of red blood cells
– Antibody formation may be delayed
Photo of Dermacentor andersoni (Rocky Mountain wood tick) and red blood cells courtesy of cdc.govPastula DM, Tyler KL. Coltiviruses and Seadornaviruses. In: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 9th Edition.
CTF: EPIDEMIOLOGY
CTF virus circulates in the higher-elevations of western United States Campers, hikers, ranchers, forestry workers most at
risk Most cases occur March–September Male predominance Not nationally notifiable (only certain states)
– Likely under-reported – 83 reported cases from 2002–2012
Map is reported CTF virus disease cases by county of residence (dark blue) from 2002–2012 and range of D. andersoni (light blue) courtesy of cdc.govhttps://www.cdc.gov/coloradotickfever/index.html
CTF: CLINICAL FEATURES
Unclear asymptomatic rate Incubation period 1–14 days (usually within 3–4 days) Fever, fatigue, myalgias, headache common Rash, leukopenia, thrombocytopenia may occur Biphasic “saddleback” fever in approximately 50% Meningitis or encephalitis can occur (with lymphocytic pleocytosis) Death is very rare Residual fatigue can last for weeks to months Should not donate blood for 6 months after illness
Photo is electron microscopy of Colorado tick fever virus courtesy of cdc.govPastula DM, Tyler KL. Coltiviruses and Seadornaviruses. In: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 9th Edition.
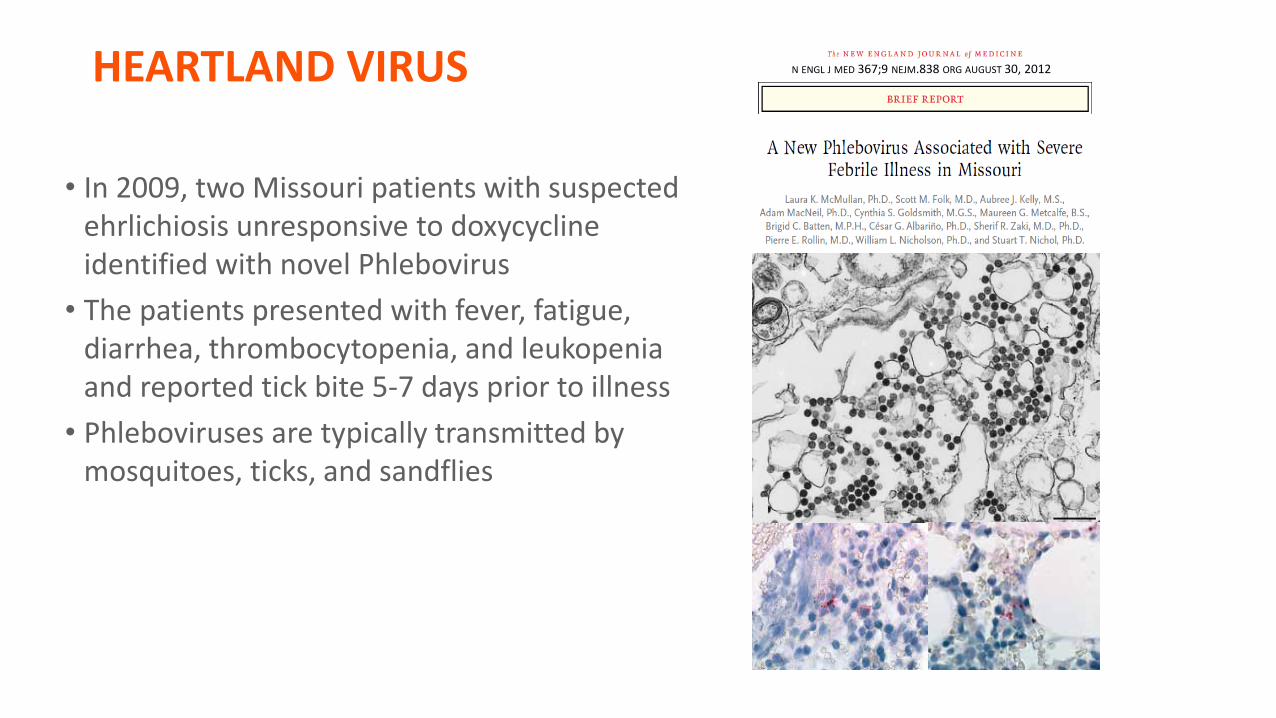
HEARTLAND VIRUS
• In 2009, two Missouri patients with suspected ehrlichiosis unresponsive to doxycycline identified with novel Phlebovirus
• The patients presented with fever, fatigue, diarrhea, thrombocytopenia, and leukopenia and reported tick bite 5-7 days prior to illness
• Phleboviruses are typically transmitted by mosquitoes, ticks, and sandflies
N ENGL J MED 367;9 NEJM.838 ORG AUGUST 30, 2012
Am J Trop Med Hyg. 2013 Sep;89(3):445-52.
HEARTLAND VIRUS (HRT): VIROLOGY AND TRANSMISSION
Single-stranded RNA phlebovirus in Phenuiviridae– Related to Severe Fever and Thrombocytopenia
Syndrome virus in Asia Transmission cycle:
– Amblyomma americanum (lone star tick)– Other tick species possible– Deer or raccoons may be amplifying hosts
Photo of Heartland virus and Amblyomma americanum (lone star tick); Map of lone star tick range; all courtesy of cdc.govhttps://www.cdc.gov/heartland-virus/index.html
HRT: EPIDEMIOLOGY
HRT virus is thought to circulate in the Midwest and southern U.S.
Over 40 HRT virus disease cases have been reported so far
Most cases occur May–September
Most cases reported recent tick exposure
May have male predominance
Map is of states with reported HRT virus disease cases courtesy of cdc.govhttps://www.cdc.gov/heartland-virus/index.html Pastula DM, Turabelidze G, Yates KF, et al. Heartland Virus Disease — United States, 2012–2013. MMWR 2014;63:270-71.
HRT: CLINICAL FEATURES
Photo is of HRT virus infecting bone marrow using immunohistochemistry courtesy of cdc.gov https://www.cdc.gov/heartland-virus/index.html Pastula DM, Turabelidze G, Yates KF, et al. Heartland Virus Disease — United States, 2012–2013. MMWR 2014;63:270-71.Carlson AL, Pastula DM, et al. Heartland virus and HLH in immunocompromised patient, Missouri, USA. Emerg Infect Dis. 2018 May;24(5):893–897.
Full clinical spectrum not currently known
Fever, anorexia, fatigue common
Leukopenia and thrombocytopenia common
Rash seems less common than with ehrlichiosis
CNS invasion potentially possible, but uncommon
Most cases hospitalized
Deaths have occurred (elderly, immunocompromised)
BOURBON VIRUS (BRB): VIROLOGY AND TRANSMISSION
Single-stranded RNA thogotovirus in Orthomyxoviridae
Novel thogotovirus identified in HRTV study– Severely ill patient who died in 2014– Serum contained cytopathic virus– No genetic match; closest Dhori virus
Thought to be transmitted by Amblyomma americanum(lone star tick)
Photo is plaque reduction neutralization antibody testing of the index patient for HRTV and phylogenetic analysis of viral polymerase courtesy of cdc.govKosoy OI, Lambert AJ, et al. Discovery of a novel thogotovirus associated with a febrile illness and death in the U.S. Emerg Infect Dis. 2015 May; 21(5). Savage HM, Burkhalter KL, et al. Bourbon Virus in Field-Collected Ticks, Missouri, USA. Emerg Infect Dis. 2017;23(12):2017-2022.
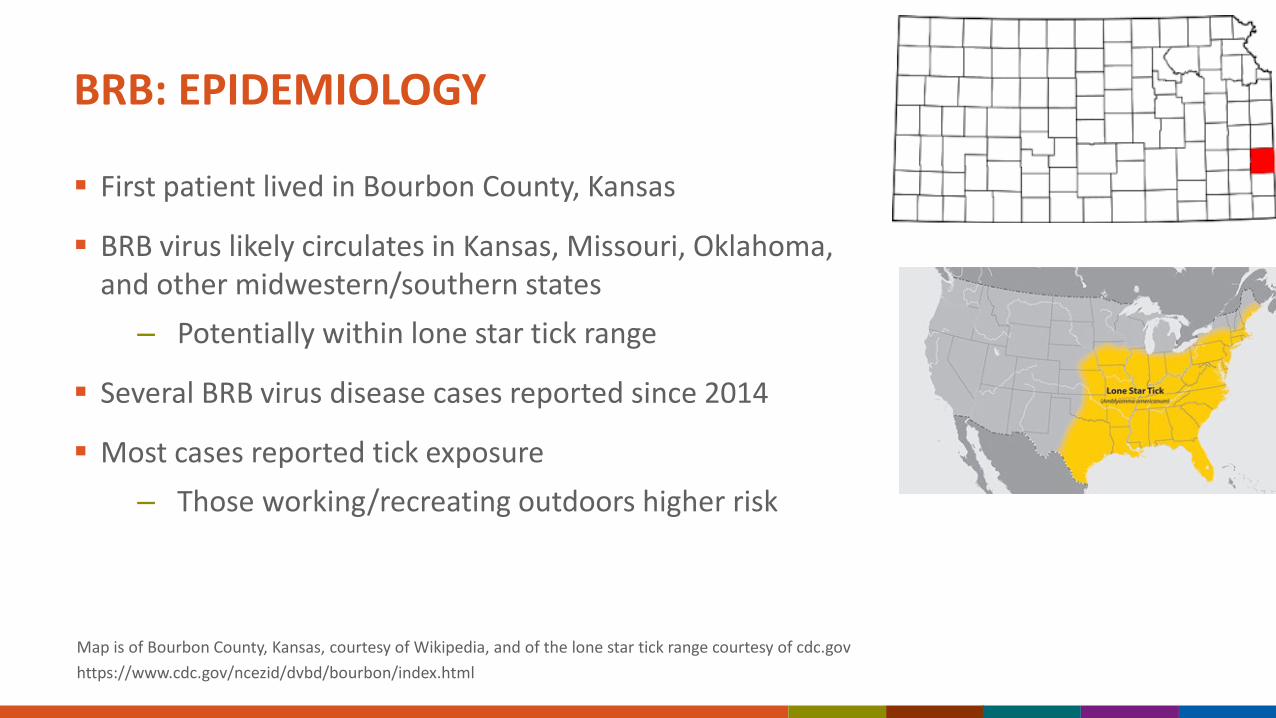
BRB: EPIDEMIOLOGY
First patient lived in Bourbon County, Kansas
BRB virus likely circulates in Kansas, Missouri, Oklahoma, and other midwestern/southern states
– Potentially within lone star tick range
Several BRB virus disease cases reported since 2014
Most cases reported tick exposure– Those working/recreating outdoors higher risk
Map is of Bourbon County, Kansas, courtesy of Wikipedia, and of the lone star tick range courtesy of cdc.govhttps://www.cdc.gov/ncezid/dvbd/bourbon/index.html
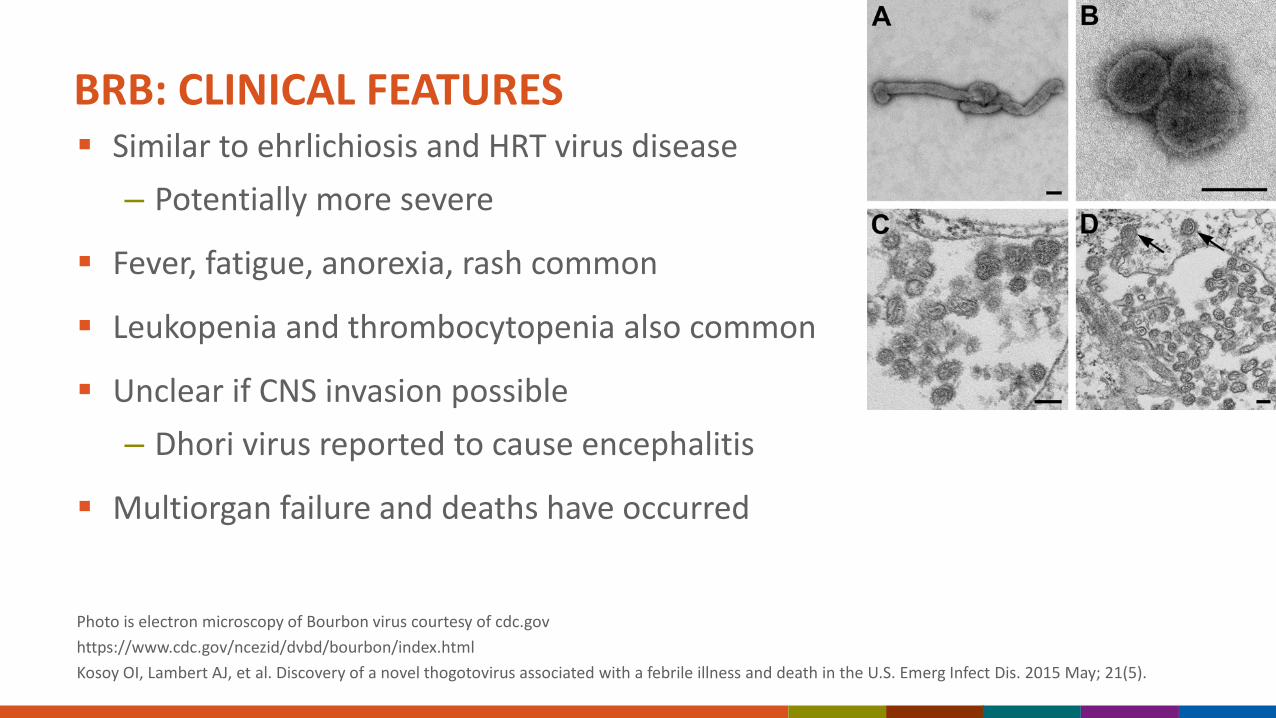
BRB: CLINICAL FEATURES
Photo is electron microscopy of Bourbon virus courtesy of cdc.govhttps://www.cdc.gov/ncezid/dvbd/bourbon/index.htmlKosoy OI, Lambert AJ, et al. Discovery of a novel thogotovirus associated with a febrile illness and death in the U.S. Emerg Infect Dis. 2015 May; 21(5).
Similar to ehrlichiosis and HRT virus disease– Potentially more severe
Fever, fatigue, anorexia, rash common
Leukopenia and thrombocytopenia also common
Unclear if CNS invasion possible– Dhori virus reported to cause encephalitis
Multiorgan failure and deaths have occurred
New Apparent Tick-borne Virus Identified in China
NEJM 2019, 2019: 380:2116-25
Tick-borne viral disease diagnosis and treatment
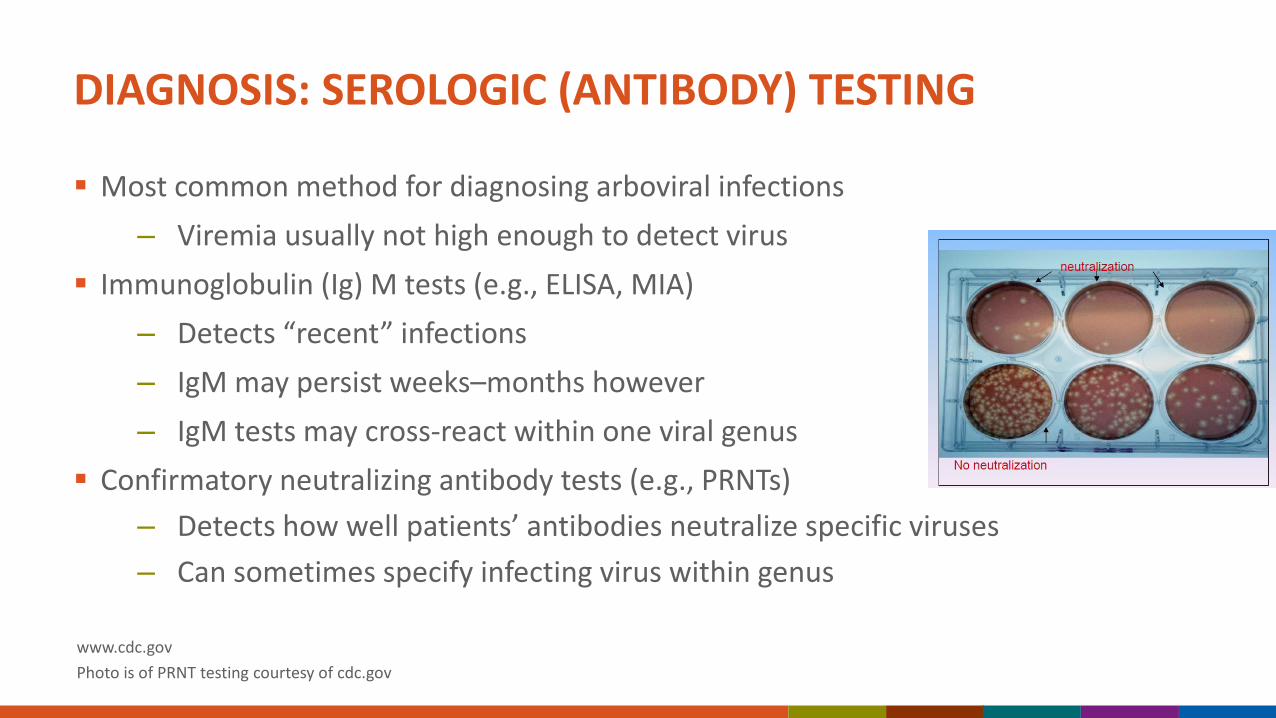
DIAGNOSIS: SEROLOGIC (ANTIBODY) TESTING
Most common method for diagnosing arboviral infections– Viremia usually not high enough to detect virus
Immunoglobulin (Ig) M tests (e.g., ELISA, MIA)– Detects “recent” infections– IgM may persist weeks–months however– IgM tests may cross-react within one viral genus
Confirmatory neutralizing antibody tests (e.g., PRNTs)– Detects how well patients’ antibodies neutralize specific viruses– Can sometimes specify infecting virus within genus
www.cdc.gov Photo is of PRNT testing courtesy of cdc.gov
DIAGNOSIS: MOLECULAR AND OTHER METHODS
Molecular / nucleic acid tests (e.g., RT-PCR)– Useful in immunocompromised, high viremia, or intracellular viruses– Particularly useful with CTF, HRT, and maybe BRB viruses
Other methods:– Immunohistochemistry (IHC) to identify virus in tissues– Viral culture if viremia high enough or in tissue
Call state or local health department for help!– Can facilitate testing at state laboratory or CDC– Can facilitate reporting to ArboNET (national arboviral surveillance)
www.cdc.govPhoto is ArboNET logo courtesy of cdc.gov
TREATMENT
No specific anti-viral treatments available– Experimental arboviral treatments with IVIG, ribavirin, corticosteroids– None proven to work
Supportive care is mainstay of treatment
May need rehydration and/or hospitalization in severe cases
Seizures and/or cerebral edema may need to be managed in severe encephalitis cases
Photo of tick repellent application courtesy of cdc.govhttps://www.cdc.gov/ticks/avoid/index.html
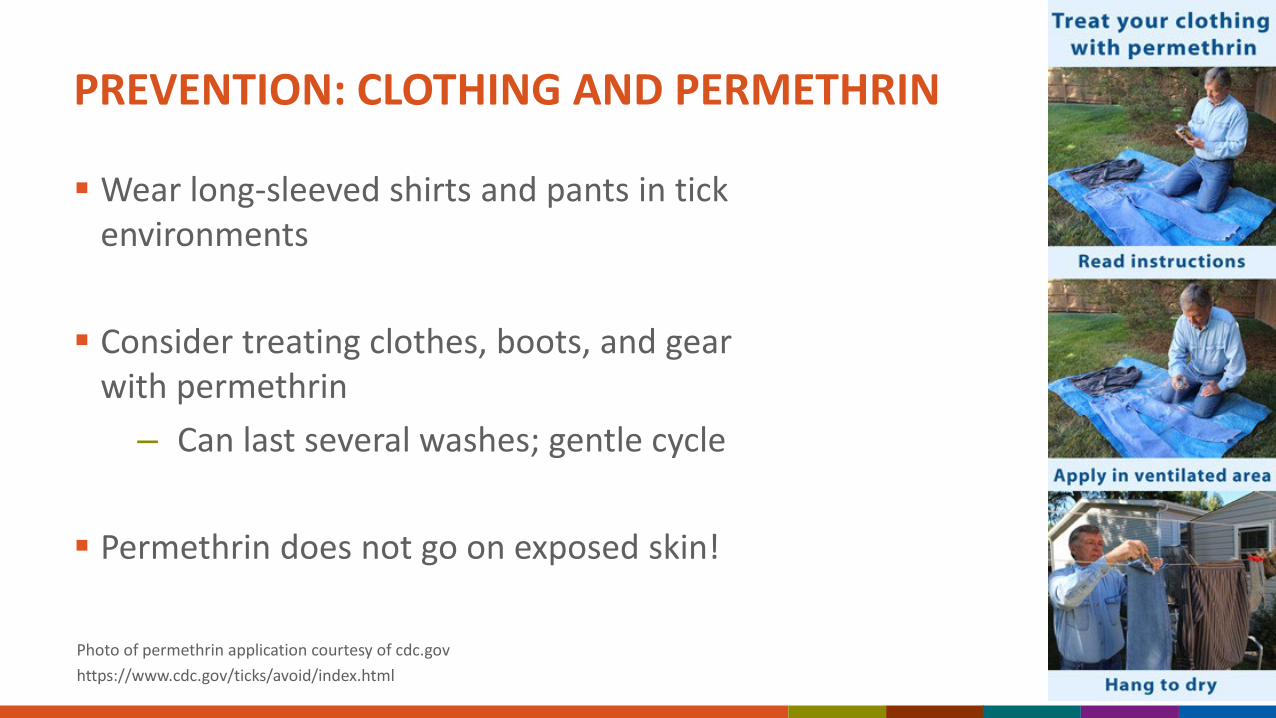
PREVENTION: CLOTHING AND PERMETHRIN
Wear long-sleeved shirts and pants in tick environments
Consider treating clothes, boots, and gear with permethrin
– Can last several washes; gentle cycle
Permethrin does not go on exposed skin!
Photo of permethrin application courtesy of cdc.govhttps://www.cdc.gov/ticks/avoid/index.html
PREVENTION: TICK CHECKS AND REMOVAL
Remove clothes and shower after being outdoors– Showering removes unattached ticks– Tumble-drying clothes with heat kills ticks
Check for and remove attached ticks:– Grab tick close to skin with tweezers– Pull straight out– Avoid burning, Vaseline, nail polish, etc.– Just remove the tick as soon as possible
Check pets too!
Photos are of sites to check for attached ticks and proper tick removal courtesy of cdc.govhttps://www.cdc.gov/ticks/avoid/index.html
NEVER USE ON ATTACHED TICKS!
REMOVE ATTACHED TICKS AS QUICKLY AS POSSIBLE
• Transmission of Rickettsia spp. can occur in < 3 hours after attachment
• Use tweezers or fine-tipped forceps
• Grab close to the mouth parts
• Pull straight up, do not twist or jerk
• Wash area
• Watch for sore or pimple at bite site, or onset of fever for following 10-14 days
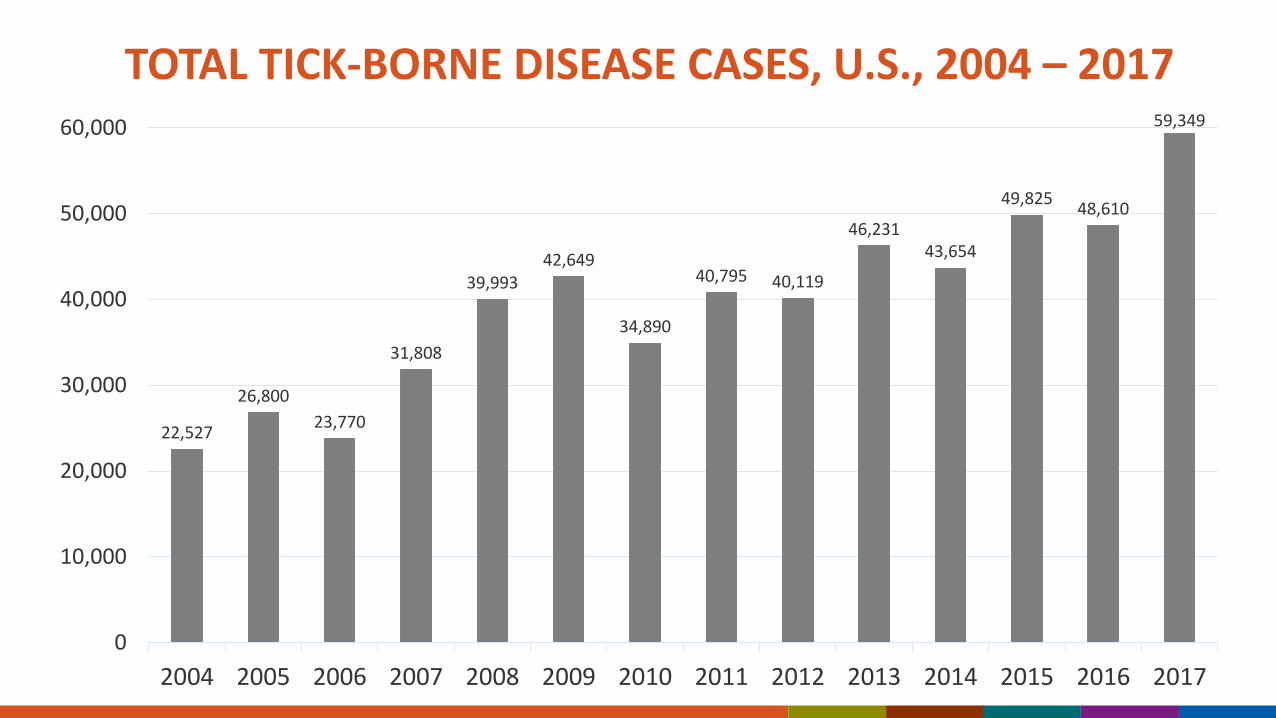
• Tick-borne diseases are an important public health concern in U.S.• Tick-borne diseases are increasing in incidence, distribution, and in
the numbers of new disease agents in U.S. • The drivers for tick-borne disease emergence related to increasing
exposure to infected ticks, result of increasing deer populations and other changes in natural or built environments
• In the absence of vaccines to any tick-borne disease in U.S., primary prevention focuses on reducing exposure to ticks and quickly removing any ticks on people or their clothing
SUMMARY AND CONCLUSIONS
“Potlucks at the CDC must be a hoot.”“Great. Now can you do this with all the other high carb foods I should avoid forever?”“Proof that government does indeed ruin everything.”
“Sorry we ticked some of you off! Don't let a tick bite ruin your summer. Protect yourself: http://bit.ly/2K2XAfF” .
CDC TWEET—MAY 4, 2018
ACKNOWLEDGEMENTS Dan Pastula Marc Fischer Carolyn Gould Chris Paddock Ben Beard