Oxalate and Sucralose Absorption inIdiopathic Calcium Oxalate Stone FormersJohn Knight, Juquan Jiang, Kyle D. Wood, Ross P. Holmes, and Dean G. Assimos
OBJECTIVES To better understand intestinal oxalate transport by correlating oxalate and sucralose absorptionin idiopathic calcium oxalate stone formers. Oxalate has been hypothesized to undergo absorp-tion in the large and small intestine by both paracellular and transepithelial transport. Sucraloseis a chlorinated sugar that is absorbed by paracellular mechanisms.
METHODS Idiopathic calcium oxalate stone formers were recruited to provide urine specimens on both aself-selected diet and after a meal containing 90 mg of 13C2-oxalate and 5 g of sucralose, and astool sample for determination of Oxalobacter formigenes colonization. The 24-hour urine col-lections were fractionated into the first 6 hours and the subsequent 18 hours. Sucralose andoxalate excretion were measured during these periods and used to estimate absorption.
ESULTS Thirty-eight subjects were evaluated. The majority of both the 13C2-oxalate and sucraloseabsorption occurred within the 0-6-hour collection. The 13C2-oxalate and sucralose absorptionswere significantly correlated at the 0-6 hour, the 6-24 hour, and the total 24-hour time periods(P �.04). All 5 oxalate hyperabsorbers(�15% absorption) also absorbed significantly moresucralose during the 0-6 hour and whole 24-hour time points (P �.04). Oxalobacter formigenescolonization did not significantly alter oxalate absorption.
CONCLUSIONS The results suggest that most oxalate is absorbed in the proximal portion of the gastrointestinaltract and that paracellular transport is involved. Augmented paracellular transport, as evidencedby increased sucralose absorption, may also influence oxalate absorption. UROLOGY 78:
In typical Western diets, �100-300 mg of oxalate isconsumed daily and 5-10% is absorbed in the intes-tine and excreted in the urine.1,2 The amount ab-
sorbed has been reported to be higher in stone formersthan non-stone formers and to increase significantly aftercertain types of bariatric surgery or with the developmentof intestinal disease.3,4 This oxalate contributes to theormation of calcium oxalate kidney stones because evenmall increases in urinary excretion are associated withn increased stone risk.5
Oxalate is thought to be absorbed in the intestine byboth paracellular and transepithelial transport.6 It hasbeen hypothesized that paracellular transport is moreprominent in the small intestine than the large intestinebecause junctional resistance is lower and luminal ox-alate content is higher.6 Transepithelial transport is reg-lated by the SLC26 family of anion transporters, andnock-out mouse models have demonstrated the influ-nce of 3 such transporters in these processes: SLC26A6
Funding Support: This work was supported by NIH grant DK62284.From the Department of Urology, Wake Forest University Medical Center, Winston-
Salem, NC; and Department of Microbiology and Biotechnology, Northeast Agricul-tural University, Harbin, China
Reprint requests: Dean Assimos, M.D., Department of Urology, WFUBMC,Medical Center Boulevard, Winston-Salem, NC 27157. E-mail: dassimos@wfubmc.
edu.
Submitted: February 4, 2011, accepted (with revisions): April 4, 2011
Oxalate loading studies in humans have demonstratedthat a significant amount of oxalate is absorbed in thefirst 2-6 hours after its administration,4,10 suggesting thata significant amount of oxalate is absorbed in the smallintestine. The slow decline in urinary oxalate excretionon an oxalate-free diet shows that absorption from thelarge intestine is also significant.1
Sucralose, a chlorinated sugar used as an artificialsweetener, is not transported across the gut epitheliumbut moves via paracellular pathways. It is not metabolizedby bacteria in the colon and after absorption it is excretedunchanged in the urine. These properties have allowed itto be used to estimate whole-gut permeability and as anindex of intestinal paracellular transport.11 We haveompared both oxalate and sucralose absorption in cal-ium oxalate stone formers in an effort to better under-tand mechanisms of intestinal oxalate transport in thisohort.
MATERIAL AND METHODS
This study was approved by the Institutional Review Board ofWake Forest University School of Medicine. Fifty-nine subjectswere recruited from April 2007 to July 2010, with 38 subjectscompleting the study. Inclusion criteria required subjects to be
competent adults, 18-64 years of age, with a history of calcium
oxalate kidney stones, defined by at least one stone analysisdemonstrating �50% calcium oxalate. Exclusionary criteriaincluded a body mass index (BMI) �35 and a history of anyhepatic, renal, bowel, or endocrine disease (ie, pregnancy, pri-mary hyperparathyroidism, renal tubular acidosis, enteric hy-peroxaluria, primary hyperoxaluria, cystinuria, chronic kidneydisease) or any other condition that could influence the absorp-tion, transport, or urinary excretion of ions. The subjects didnot consume vitamins or supplements during the day of thestudy.
The subjects initially collected two 24-hour urine specimenswhile consuming self-selected diets and they provided a stoolsample to determine colonization with Oxalobacter formigenes(OxF) using an established culture test.12 After an overnightast, they drank 500 mL of distilled water and voided at 8:00 AM
(initial void). They then consumed a sausage biscuit, orangejuice, and 90 mg of 13C2-oxalate (Cambridge Isotopes Labora-ories, Andover, MA) and 5 g of sucralose (McNeil nutritionalsLC, Ft. Washington, PA) dissolved in 100 mL of distilledater. They then consumed self-selected diets except for lim-
ting dairy products and high oxalate–containing foods forunch and dinner. Urine was collected for 24 hours after thenitial void but fractionated into the first 6 hours and theubsequent 18 hours.
Creatinine was measured on a Beckman C5E Analyzer (Brea,A). Total oxalate was measured using a kit provided byrinity Biotech (St. Louis, MO). Reagent-free ion chromatog-
aphy coupled with negative ion electrospray mass spectrometryRFIC-MS) (Dionex Corp., Sunnyvale, CA) was used to mea-ure 13C2-oxalate. A Thermo-Finnigan MSQTM ELMO single
quadrupole mass spectrometer specifically designed for the anal-ysis of low-molecular-weight ions was used for mass determina-tions. The ion chromatography (IC) portion of the IC/MSconsisted of an ED50 conductivity detector, a GS50 gradientump, an AS50 refrigerated autosampler, an EG50 potassiumydroxide gradient generator, and an AS50 thermal compart-ent containing an AS11-HC, 2 � 150 mm, anion exchange
column at a controlled temperature of 30°C and an ASRS 3002-mm suppressor. A gradient of potassium hydroxide from0.5-80 mM over 60 minutes at a flow rate of 0.4 mL min�1 wassed to separate anions in samples. The relative abundance ofpecific anions was determined by selected-ion monitoringSIM) at the following mass/charge ratios: oxalate (SIM89) and
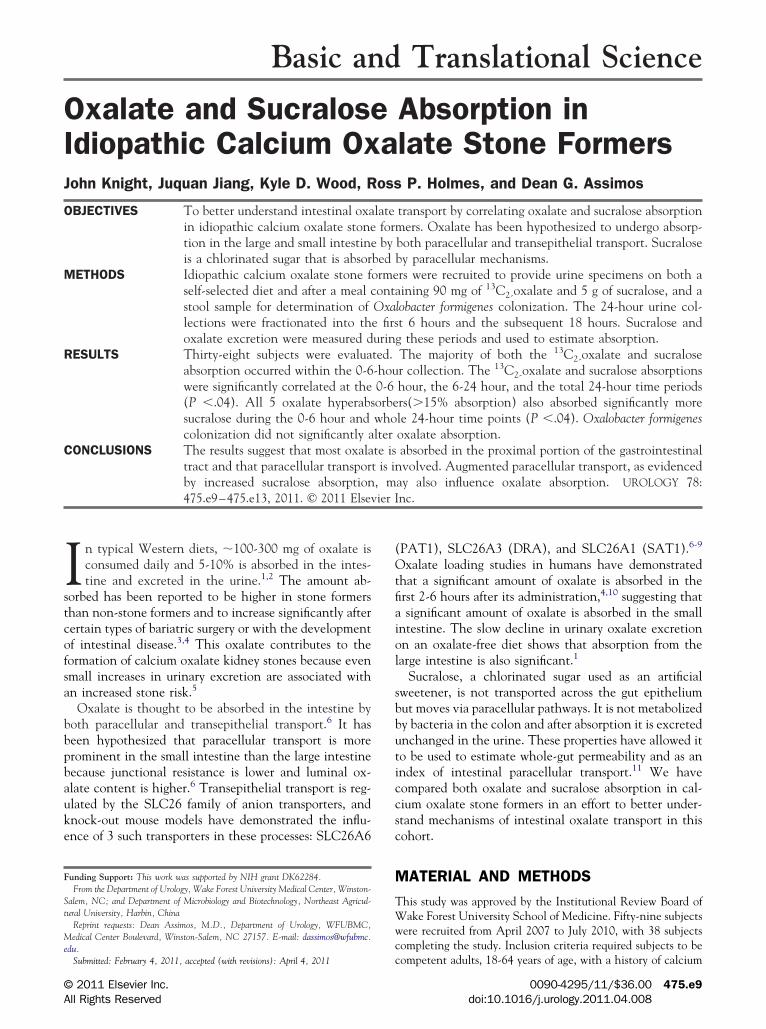
Figure 1. Distribution of 13C2 oxalate (A) and sucral
13C2-oxalate (SIM91). The enrichment of 13C2-oxalate in sam- o
475.e10
ples was determined from curves prepared using known amountsof 13C2-oxalate producing 0-40% enrichment.
Urinary sucralose excretion was measured using high-perfor-mance anion-exchange chromatography with pulsed ampero-metric detection as described (www.dionex.com; Dionex appli-cation update 151). A CarboPac PA20 column, 3 � 150 mm,with 100 mM sodium hydroxide/60 mM sodium acetate as theeluent at a flow rate of 0.5 mL/min, was used to measuresucralose in urine samples. With this method, the limit ofdetection, defined as the mean blank signal plus 3 � standarddeviation, and the limit of quantitation, defined as the meanblank signal plus 10� SD, were 0.07 �M and 0.16 �M, respec-ively. With each batch analysis, a urine control was run andhe mean and SD sucralose level was136.8 � 2.5 �M, giving an
interassay variability of 1.9%.Experimental results were analyzed by Student’s t-test and
correlation coefficients were determined by linear regressionusing GraphPad software (San Diego, CA). P values �.05were considered statistically significant. Data are expressedas mean � SD.
RESULTSThirty-eight subjects (10 females, 28 male) completedthis study. The mean age was 49 � 13 years. The meanurinary oxalate excretion measured in the 2 collectionson self-selected diets was 33.6 � 9.3 mg and 10/38 (26%)
ad hyperoxaluria, defined as a mean excretion �40 mg.ix (15.8%) of the subjects were colonized with OxF.he mean 24-hour urinary oxalate excretion of the OxF-ositive cohort on self-selected diets was lower (29.4 �.0 mg) than those not colonized (34.4 � 9.6 mg), butas not statistically different (P � .24).The mean 24-hour 13C2-oxalate absorption was 8.7 �
.9% for the whole group and the distribution is shown inigure 1A. Five subjects (13.2%) hyperabsorbed oxalateith a value �15%, which was previously used to defineyperabsorption in Voss et al.4 None of the hyperabsorb-rs were colonized with OxF. Furthermore, absorptionas not statistically different in OxF-colonized (5.2 �.2%) and noncolonized (9.3 � 6.2%) subjects (P �13). Consistent with other studies, the bulk of the 13C2-
(B) absorption in 38 calcium oxalate stone-formers.
xalate absorption—67%—occurred in the first 6 hours
after the load was administered (Fig. 2A).4 This mayepresent predominant absorption in the small intestine.
The mean 24-hour sucralose absorption in the entireroup was 3.2 � 1.2% and its distribution in the cohort
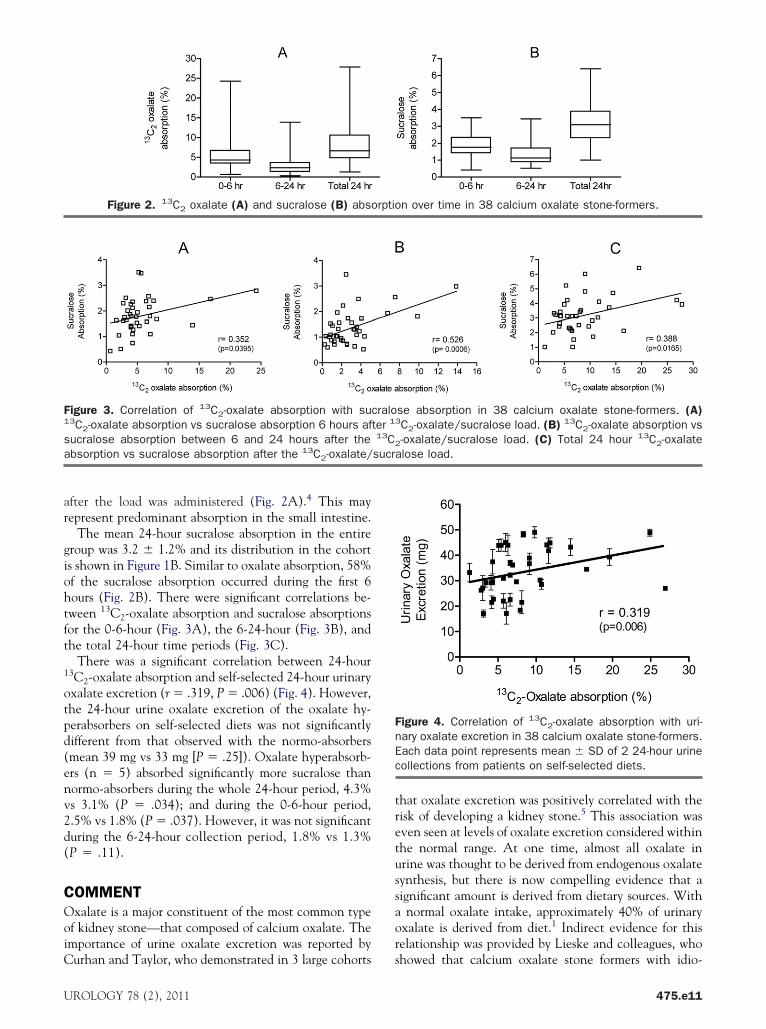
is shown in Figure 1B. Similar to oxalate absorption, 58%of the sucralose absorption occurred during the first 6hours (Fig. 2B). There were significant correlations be-tween 13C2-oxalate absorption and sucralose absorptionsor the 0-6-hour (Fig. 3A), the 6-24-hour (Fig. 3B), andhe total 24-hour time periods (Fig. 3C).
There was a significant correlation between 24-hour13C2-oxalate absorption and self-selected 24-hour urinaryoxalate excretion (r � .319, P � .006) (Fig. 4). However,the 24-hour urine oxalate excretion of the oxalate hy-perabsorbers on self-selected diets was not significantlydifferent from that observed with the normo-absorbers(mean 39 mg vs 33 mg [P � .25]). Oxalate hyperabsorb-ers (n � 5) absorbed significantly more sucralose thannormo-absorbers during the whole 24-hour period, 4.3%vs 3.1% (P � .034); and during the 0-6-hour period,2.5% vs 1.8% (P � .037). However, it was not significantduring the 6-24-hour collection period, 1.8% vs 1.3%(P � .11).
COMMENTOxalate is a major constituent of the most common typeof kidney stone—that composed of calcium oxalate. Theimportance of urine oxalate excretion was reported by
Figure 3. Correlation of 13C2-oxalate absorption with su13C2-oxalate absorption vs sucralose absorption 6 hours afucralose absorption between 6 and 24 hours after thebsorption vs sucralose absorption after the 13C2-oxalate/
Figure 2. 13C2 oxalate (A) and sucralose (B) abs
Curhan and Taylor, who demonstrated in 3 large cohorts s
UROLOGY 78 (2), 2011
that oxalate excretion was positively correlated with therisk of developing a kidney stone.5 This association wasven seen at levels of oxalate excretion considered withinhe normal range. At one time, almost all oxalate inrine was thought to be derived from endogenous oxalateynthesis, but there is now compelling evidence that aignificant amount is derived from dietary sources. With
normal oxalate intake, approximately 40% of urinaryxalate is derived from diet.1 Indirect evidence for thiselationship was provided by Lieske and colleagues, who
se absorption in 38 calcium oxalate stone-formers. (A)3C2-oxalate/sucralose load. (B) 13C2-oxalate absorption vs-oxalate/sucralose load. (C) Total 24 hour 13C2-oxalate
alose load.
Figure 4. Correlation of 13C2-oxalate absorption with uri-ary oxalate excretion in 38 calcium oxalate stone-formers.ach data point represents mean � SD of 2 24-hour urineollections from patients on self-selected diets.
n over time in 38 calcium oxalate stone-formers.
craloter 1
13C2
howed that calcium oxalate stone formers with idio-
475.e11
5bcusom
wc
eo
oga2sros6trj
fr
ItmtS
ava
pathic hyperoxaluria reduced oxalate excretion by 36%when consuming a low-oxalate diet.13
We observed a mean oxalate absorption of 8.7% �.9% in our study, which is within the range reportedy other groups using 13C-oxalate loading. Hesse andolleagues reported that the mean oxalate absorptionsing this approach in 70 recurrent calcium oxalatetone-formers was 9.2 � 5.1%.3 In a subsequent studyf 120 such subjects, they reported a somewhat higherean absorption of 10.2 � 5.2%.4 We detected a
subgroup of stone-formers who hyperabsorbed oxalateas defined by an absorption of �15% as suggested byVoss et al.4 Five subjects (13.2%) met this criterion,within the range previously reported by others. Hesseet al reported that 6/70 (8.6%) calcium oxalate stone-formers hyperabsorbed in one study and 19/120(15.8%) hyperabsorbed in a later study.3,4 In keeping
ith the study by Voss et al, we observed a significantorrelation between 13C2-oxalate absorption and uri-
nary oxalate excretion.Gastrointestinal transport is dependent on a number of
factors, including gender, food composition, medications,and method used to measure transit time.14 However, itis generally accepted that small intestinal transport oc-curs within 6 hours of a meal, with colonic transportrequiring significantly more time. In our study, mostoxalate (67%) was absorbed in the first 6 hours after the13C-oxalate load. This suggests that a significant amountof the oxalate is absorbed proximal to the colon based onknown gastrointestinal transport times.15 Similarly, Vosst al reported in 8 healthy adult subjects that 85% of thexalate absorption occurred within the first 6 hours.4
Chai reported that 83% of the oxalate was absorbed in agroup of 14 normal subjects and calcium oxalate stone-formers during this same interval.16
Our results demonstrate significant correlations be-tween sucralose and oxalate absorption for the whole24-hour period and the 2 segmented collections. Su-cralose is an artificial sweetener formed by the chlori-nation of sucrose and is resistant to degradation bybacteria in the colon. There is limited gut absorptionand therefore what is transported is attributed to para-cellular uptake. This property forms the basis of the useof its absorption as an index of whole-gut permeabil-ity.11 The mean 3.2% 24-hour sucralose absorption in
ur study is consistent with that published by otherroups in adults without bowel disease. Farhadi andssociates in 2 studies reported values of 2.32% and.49%.17,18 Because of the significant absorption ofucralose in both the 0-6 and 6-24-hour periods, ouresults suggest that paracellular transport of oxalateccurs throughout the gastrointestinal tract. The ab-orption of most oxalate and sucralose during the firsthours is consistent with this absorption occurring in
he small bowel. A higher paracellular transport in thisegion of the bowel is expected because of its low
unctional resistance.19
475.e12
Colonization with OxF has been demonstrated to re-duce the risk of recurrent calcium oxalate stone forma-tion by 70%.20 None of the oxalate hyperabsorbers werecolonized with OxF. A statistically significant relation-ship between colonization and oxalate hyperabsorptionwas not observed, but no conclusions can be reachedbecause of the small number colonized. Further studiesare required to determine the impact of OxF colonizationon oxalate hyperabsorption. The hyperabsorbers did havea significantly higher 24-hour percentage of sucraloseabsorption than the normo-absorbers. When the resultswere analyzed according to the collection period, a sig-nificant difference was observed only in the 0-6-hourperiod. This suggests that paracellular oxalate transportin the small intestine may contribute to oxalate hypera-bsorption.
The apparent role of paracellular transport in oxalateabsorption highlights the need for a better understandingof junctional permeability and function. Junctional com-plexes have a complex ultrastructure and may be com-prised of such proteins as cadherin, catenin, occluding,and claudin.21 Their permeability may not only be af-ected by these proteins, but also by the intestinal envi-onment.
Transepithelial transport of oxalate is also important.nsight into this process has been provided by the study ofhe SLC26 family of anion transporters. Knock-outouse models have demonstrated the influence of 3 such
ransporters, SLC26A6 (PAT1), SLC26A3 (DRA),LC26A1 (SAT1) on intestinal oxalate transport.6-9
Further investigations are required to better define boththe transepithelial and paracellular transport of this an-ion. Better understanding of the mechanisms involvedmay lead to future therapeutic interventions.
We recognize that our study has certain limitations.Subjects were not placed on controlled diets, which mayhave contributed to variability. A comparison with anormal age-matched population was not undertaken andit is possible that the responses might be different in thiscohort. In addition, other measures of gut permeability,which could define regional gut differences, were notused.22 This study assessed the absorption of soluble ox-late and we recognize that this form of oxalate in foodaries and thus could influence the dynamics of thebsorption of food-derived oxalate.
CONCLUSIONSOur study suggests that most soluble oxalate is absorbedin the proximal portion of the gastrointestinal tract andthat paracellular transport plays a role in its uptake. Inaddition, augmented paracellular transport, as evidencedby increased sucralose absorption, may influence oxalatehyperabsorption. This result requires further investigationto determine whether an inherent or acquired increase in
gut permeability plays a role in oxalate hyperabsorption.
UROLOGY 78 (2), 2011
1
1
1
1
1
1
1
1
1
1
2
2
2
References1. Holmes RP, Goodman HO, Assimos DG. Contribution of dietary
oxalate to urinary oxalate excretion. Kidney Int. 2001;59:270.2. Holmes RP, Kennedy M. Estimation of the oxalate content of foods
and daily oxalate intake. Kid Intl. 2000;57:1662.3. Hesse A, Schneeberger W, Engfeld S, et al. Intestinal hyperabsorp-
tion of oxalate in calcium oxalate stone formers: application of anew test With [13C2] oxalate. J Am Soc Nephrol. 1999;10:S229-S333.
4. Voss S, Hesse A, Zimmermann DJ, et al. Intestinal oxalate absorp-tion is higher in idiopathic calcium oxalate stone formers than inhealthy controls: measurements with the [(13)C2] oxalate absorp-tion test. J Urol. 2006;175:1711.
5. Curhan GC, Taylor EN. 24-h uric acid excretion and the risk ofkidney stones. Kidney Int. 2008;73:489.
6. Hatch M, Freel RW. The roles and mechanisms of intestinal oxalatetransport in oxalate homeostasis. Semin Nephrol. 2008;28:143.
7. Dawson PA, Russell CS, Lee S, et al. Urolithiasis and hepatotox-icity are linked to the anion transporter SatI in mice. J Clin Invest.2010;120(3):706.
8. Freel RW, Hatch M, Green M, Soleimani M. Ileal oxalateabsorption and urinary oxalate excretion are enhanced inSlc26a6 null mice. Am J Physiol Gastrointest Liver Physiol. 2006;290:G719.
1. Meddings JB, Gibbons I. Discrimination of site-specific alterations in
gastrointestinal permeability in the rat. Gastroenterology. 1998;114:83.
UROLOGY 78 (2), 2011
2. Hatch M, Cornelius J, Allison M, et al. Oxalobacter sp. reducesurinary oxalate excretion by promoting enteric oxalate secretion.Kidney Int. 2006;69:691.
3. Lieske JC, Tremaine WJ, De Simone C, et al. Diet, but not oralprobiotics, effectively reduces urinary oxalate excretion andcalcium oxalate supersaturation. Kidney Int. 2010;78:1178.
4. Degen LP, Phillips SF. Variability of gastrointestinal transit inhealthy women and men. Gut. 1996;39:299.
5. Bjarnason I, MacPherson A, Hollander D. Intestinal permeability:an overview. Gastroenterology. 1995;108:1566.
6. Chai W, Liebman M. Assessment of oxalate absorption from al-monds and black beans with and without the use of an extrinsiclabel. J Urol. 2004;172:953.
7. Farhadi A, Gundlapalli S, Shaikh M, et al. Susceptibility to gutleakiness: a possible mechanism for endotoxaemia in non-alcoholicsteatohepatitis. Liver Int. 2008;28:1026.
8. Farhadi A, Keshavarzian A, Holmes EW, et al. Gas chromato-graphic method for detection of urinary sucralose: application tothe assessment of intestinal permeability. J Chromatogr B AnalTechnol Biomed Life Sci. 2003;784:145.
9. Hatch M, Freel RW. Intestinal transport of an obdurate anion:oxalate. Urol Res. 2005;33:1.
0. Kaufman DW, Kelly JP, Curhan GC, et al. Oxalobacter formigenesmay reduce the risk of calcium oxalate kidney stones. J Am SocNephrol. 2008;19:1197.
1. Turner JR. Intestinal mucosal barrier function in health and dis-ease. Nat Rev Immunol. 2009;9:799.
2. Anderson AD, Jain PK, Fleming S, et al. Evaluation of a triplesugar test of colonic permeability in humans. Acta Physiol Scand.