Janet K. Johnson, Ph.D.Director, Clinical Research
Supernus Pharmaceuticals, Inc.
ASENT Pipeline Projects Session
March 5, 2010
Development of OXC XRDevelopment of OXC XR
• Supernus Pharmaceuticals, Inc– Small pharmaceutical company with
proprietary drug delivery methodology– Experience with CNS products (ADHD,
epilepsy) as Shire Labs
• OXC as candidate for XR development– Effective doses 600 – 2400mg/d– Increase response rate with increase in dose– Highest doses associated with significant AEs
OXC v Placebo, Barcs Study% Seizure Free% Seizure Free
Med
ian
% s
eizu
re re
ducti
on
0.6%3% 10%
22%
26%*
40%*
50%*
8%
N=173
N=169
N=178
N=174~
Epilepsia, 41(12):1597, 2000* p=0.0001 compared to placebo
~ includes 47 pts at 1800 mg; 73% of patients on 2400mg dropped from the study or decreased to 1800mg
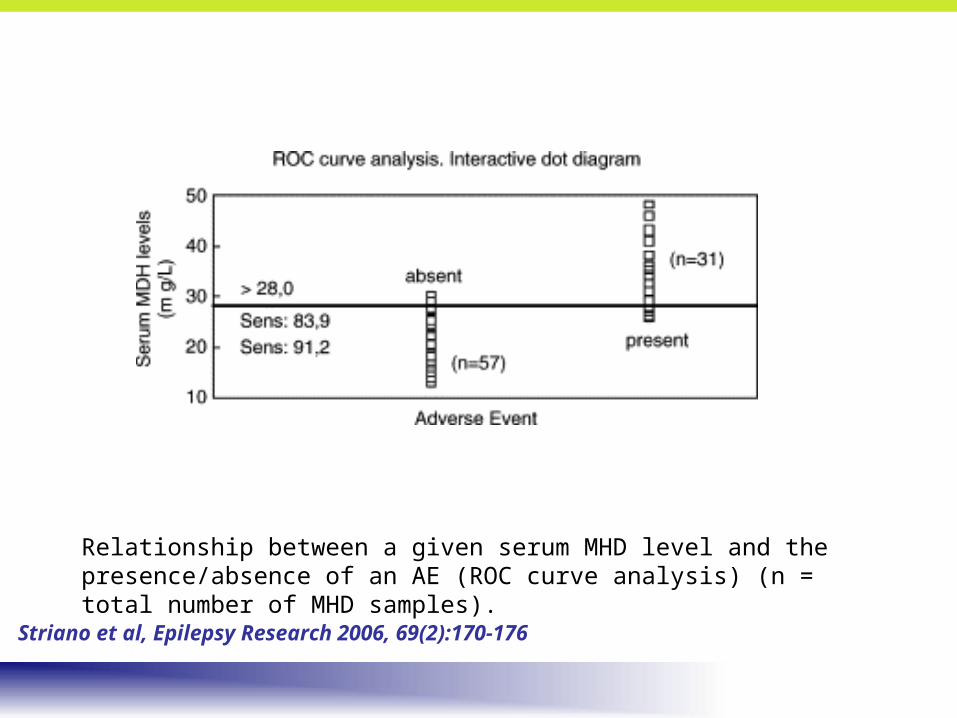
Relationship between a given serum MHD level and the presence/absence of an AE (ROC curve analysis) (n = total number of MHD samples).
Striano et al, Epilepsy Research 2006, 69(2):170-176
Incentives for Development of OXC XRIncentives for Development of OXC XR
• Current Formulation– BID dosing– Association of AEs with peak levels
• Possible Advantages of XR Formulation– QD dosing – may increase compliance– Lower peak – may increase tolerablity
Drug + Polymer Core
Receding Solid Interface
Hydrated Polymer Layer
Solubilized Drug Release Path
Solutrol
Drug + Polymer Core
Receding Solid Interface
Solubilized Drug Release Path
Solutrol
0
20
40
60
80
100
0 2 4 6 8 10 12
Time (hr)
Dru
g D
isso
lve
d (
%)
pH 1.2 pH 6.8
Solutrol vs pH Dependent Dissolution
0
20
40
60
80
100
0 2 4 6 8 10 12
Time (hr)
Dru
g D
isso
lve
d (
%)
Control pH 1.2 Control pH 6.8
OXC solubility
15 mg/mL at pH 1.0 0.22 mg/mL at pH 7.0
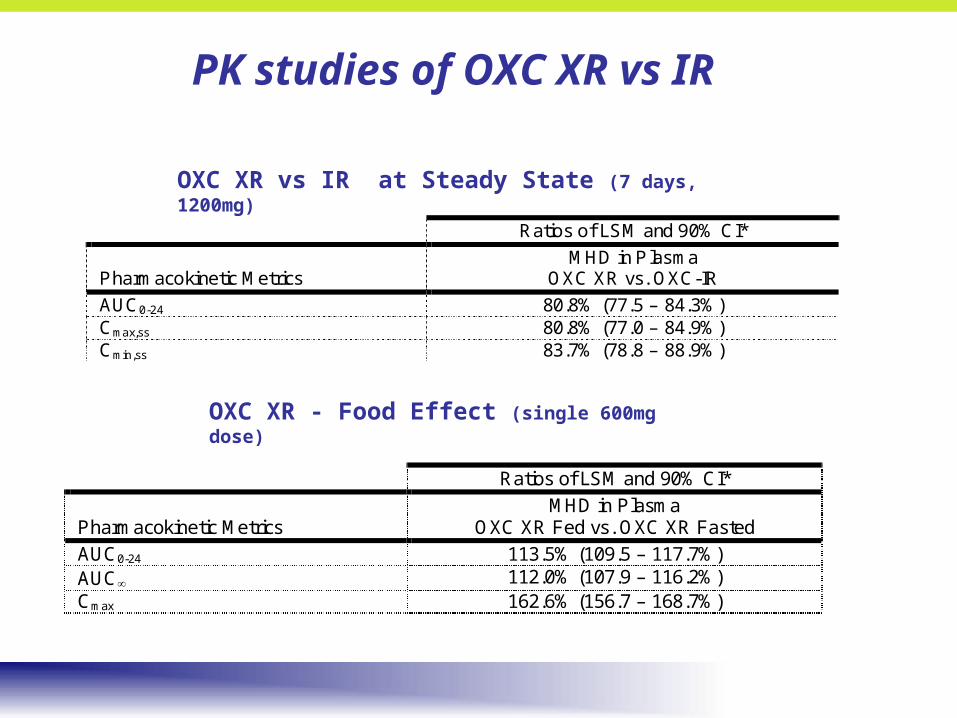
OXC XR vs IR at Steady State Healthy Normal Volunteers, 7 days, 1200mg, crossover
– Option for 1 year open-label follow-on study– 1Efficacy = % change seizures/28d, OXC XR vs Placebo
– 2Efficacy = % seizure-free, other efficacy, safety, QOL
804P301 Study Design
6
1800
1200
2400 mg/d
1200 mg/d
Placebo
1800
1200
600 600
MaintenanceTitration ConversionScreening
BASELINE TREATMENT
VISIT
WEEK
1 2 33
1-8 to -1 2 3 4 5 9 13 17 18 19
44 55 66 7
3 weeks12 weeks8 weeks 4 weeks
SEIZURE DIARY
Seizure Identification Form PK Sampling
Development of XR, CR for Epilepsy
• Supernus status– Development of OXC XR for partial epilepsy
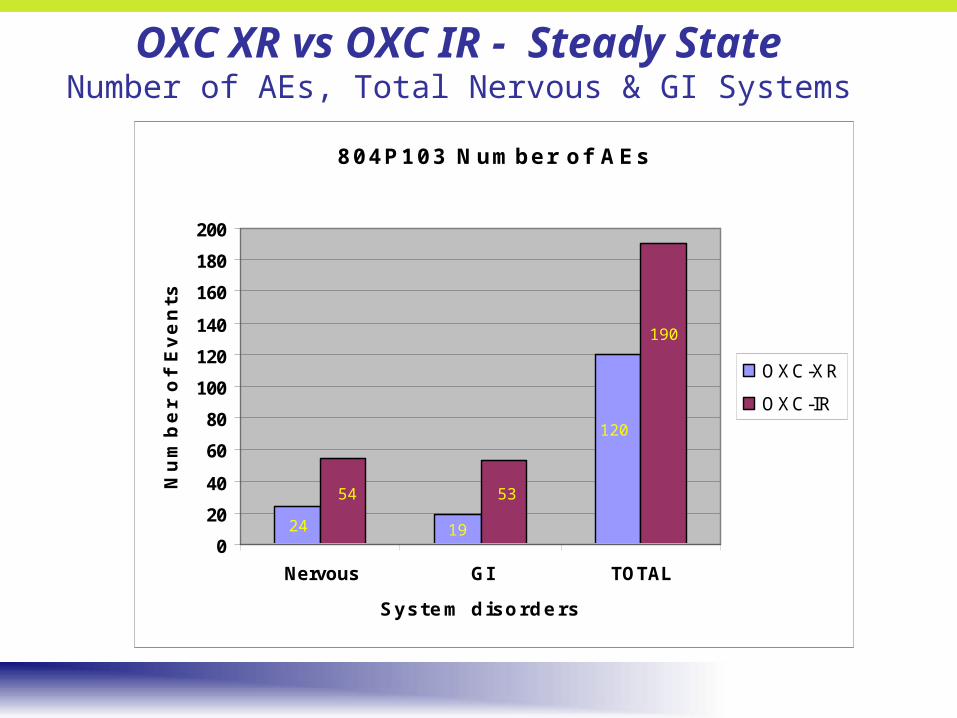
• QD formulation, 80% AUC, Cmax vs OXC IR• Lower incidence of AEs in PK study of HNV at 1200mg• Possible greater utility of high dose (2400mg)• Ongoing Phase 3 placebo-controlled study in adults• Ongoing PK study in pediatrics