Page 1
Pacemaker Pacemaker Follow-upFollow-up
Alpay Çeliker MD.
Hacettepe University
Department of Pediatric Cardiology
3rd International Summer School on CardiacArrhythmias, 9-12 September, Eskişehir
Page 3
OrganizationOrganization
Regular follow-up schedule Pacemaker record files X-ray ECG Telemetry units
Page 4
Pacemaker Follow-up:Pacemaker Follow-up:ObjectivesObjectives
Adjust the pacing system
Maximize the benefits of pacing therapy
Predict impending pacemaker system failure before the patient is at risk
Ascertain the nature of malfunction
Look for accompanying complications
Page 5
PATIENT
TELEMETRY ECG&TELE
PHYSICAL EXAM
• THRESHOLDS• INTRINSIC AMPLITUDES• PACEMAKER DEPENDENCY• PACING RATIO• HISTOGRAMS
• PACING EFFICACY• LEAD PROBLEMS
HOLTER, EXERCISE TEST
• EXERCISE PERFORMANCE• MAXIMUM HEART RATE• DETECT CAPTURE AND SENSING PROBLEMS
ECHO
Page 6
Pacemaker Follow-upPacemaker Follow-up
Patient evaluationPatient evaluation History Physical examination Chest x-ray Echocardiography
Pacing system evaluationPacing system evaluation Surface ECG Telemetric control of pacemaker Holter monitoring Treadmill testing
Page 7
HistoryHistory Palpitations
Rapid ventricular rate, PMT, intrinsic tachycardia
Weakness, fatigue, malaise, dyspnea Pacemaker syndrome, capture failure, inappropriate
programming, cardiac or pulmonary disease
Hiccups Syncope, presyncope
Pacemaker syndrome, capture problem, inhibition due to oversensing
Cough, chest pain
Page 8
Radiologic EvaluationRadiologic Evaluation
Page 9
Pacemaker Interrogation Administrative data verificationAdministrative data verification
Name, implant date Programmed data controlProgrammed data control Examine the pacing&sensing parametersExamine the pacing&sensing parameters
Capture threshold Voltage measurements Battery&lead measurements
Overview the memorized dataOverview the memorized data
Page 11
Capture ThresholdsCapture Thresholds
Automatic or manual measurements
Voltage or pulse width thresholds
Pacing rate > spontan rate during test
Test during coughing and deep respiration to detect malfunction
Page 12
Absence of PM Stimuli or Absence of PM Stimuli or CaptureCapture
Intrinsic rate > pacing rate Hysteresis Very tiny bipolar stimuli Lead problems
Fracture, loose connection
Pulse generator problems EOL, failure
Electromagnetic interference Oversensing
Page 13
Atrial NoncaptureAtrial Noncapture
Page 14
Ventricular NoncaptureVentricular Noncapture
Page 15
Sensing ThresholdsSensing Thresholds
Automatic or manual measurements
Print-out of intracardiac electrocardiogram
Needs for spontaneous atrial or ventricular rhythm
Page 16
UndersensingUndersensing
Page 17
UndersensingUndersensing Low amplitude EGM due to poor lead
position Lead dislodgement Lead malfunction Metabolic or toxic causes Development of new bundle branch
block Myocardial infarciton near the electrode
tip
Page 18
OversensingOversensing
Page 19
Causes of OversensingCauses of Oversensing VentricularVentricular
T wave Crosstalk Myopotentials False signals
AtrialAtrial Far-field R wave Myopotentials False signals
Page 20
Change in Pacing RateChange in Pacing Rate
Battery depletion Runaway pacemaker Component failure Oversensing External effects on battery Phantom or wrong programming
Page 21
Signs of Lead FractureSigns of Lead Fracture
No stimuli Stimuli without capture Oversensing of false signals Permanent or intermittant high lead
impedance Maneuvers X-ray
Page 24
Testing of Specific Testing of Specific FunctionsFunctions
Check for crosstalk
Evaluate the VA interval
Examine rate adaptive parameters
Hysteresis, sleep rate
Automatic mode switching
Histogram settings
Page 25
Rate Adaptive Pacemaker Rate Adaptive Pacemaker
Page 26
Rate HistogramRate Histogram
Assess rate response settings
Assess high rate events
Evaluate percent pacing versus sensing
Determine if a change in disease state condition
has occurred
Page 27
Atrial Pace/sense HistogramAtrial Pace/sense Histogram
Page 28
Physical ExaminationPhysical Examination
Pacing System
Pocket Vascular System Leads
•Infection•Erosion•Migration•Twiddler’s syndrome•Muscle stimulation•Chronic pain
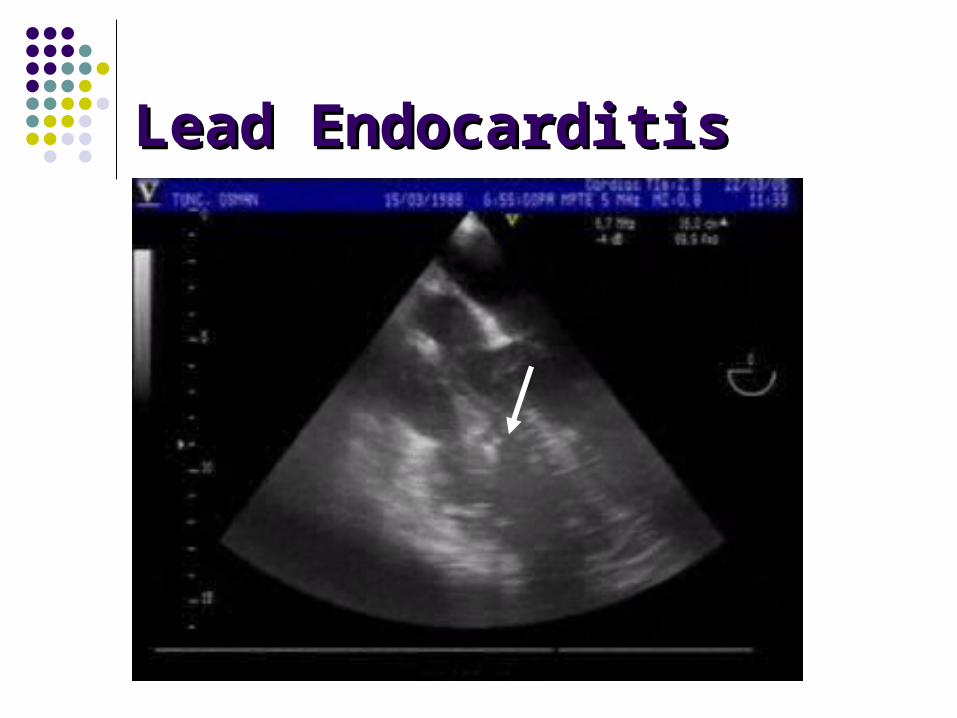
•Venous thrombosis•Intracardiac thrombus•Lead Endocarditis•Tricuspid valve entanglement•TR
•Displacement•Perforation•Diaphragmatic pacing
Page 29
Lead EndocarditisLead Endocarditis
Page 30
Venous ObstructionVenous Obstruction
<obstruction
Page 32
Pacemaker SyndromePacemaker Syndrome
Dizziness
Presyncope
Chest tightness
Shortness of breath
Neck pulsations
Apprehension/malaise
Fatigue
Page 35
Conclusions IConclusions I Long rhythm strips with markers and IEGM’s
may needed for correct diagnosis 12 lead paced ECG is very valuable Know the timing cycles Do not attribute patient symptoms to age,sex
or underlying heart disease Do not leave the pacemaker at factory
settings, since every patient has different necessities.
Page 36
Conclusions IIConclusions II
Make every effort to prolong battery life The other purpose of pacing is optimization of
quality of life Optimal AV delay can not be predicted Test the retrograde VA conduction Keep the records carefully Be obsessive in pacemaker dependent
patient