18
Paediatric Asthma 26 th November 2014 Julie Westwood Asthma Nurse Specialist RHSC 0131 536 0773
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | victor-griffith |
| View: | 216 times |
| Download: | 1 times |

Paediatric Asthma
26th November 2014Julie Westwood
Asthma Nurse SpecialistRHSC
0131 536 0773

Topics to explore
• Normal childhood• Diagnosing asthma in children• Considering the probability• Treatment
Normal Childhood
Some facts
<2 years of age– Average of 12 URTIs (colds) per year– Cough can last for up to 14 days with
each cold (i.e. up to 24 weeks cough/yr)
<6 years of age– 50% of children will have had at least
one episode of wheeze (c10% have asthma) I.e. almost normal to wheeze

Asthma in children
• SIGN/BTS Guideline October 2014 (online) 141
• Diagnosis by probability (introduced 2008)
• Adolescent section• Supersedes 101
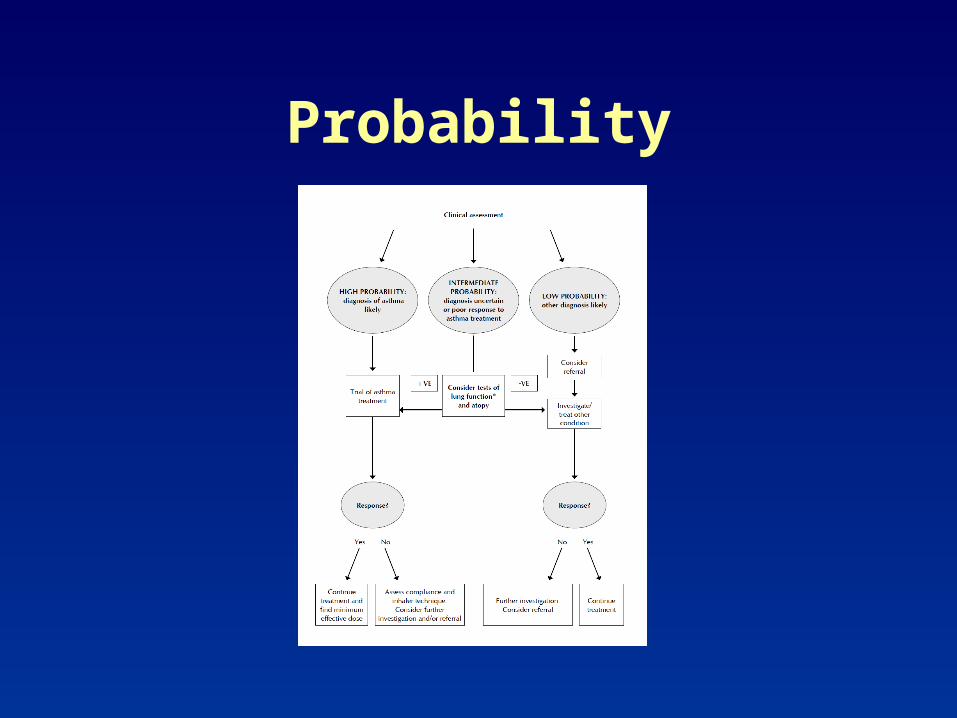
Probability

Asthma in children - high probability
• > 1 of: wheeze, cough, difficulty breathing, chest tightness esp if:– Frequent and recurrent– Worse at night / early morning– In response to triggers– Occur apart from colds
• Personal history of atopic disorders• Family history of atopic disorder/asthma • Widespread wheeze heard on auscultation• History of improvement in symptoms or lung
function in response to adequate treatment

Asthma in children - low probability
• Symptom with URTI only – with no interval symptoms
• Isolated cough in the absence of wheeze or difficulty breathing
• History of moist cough• Prominent dizziness, light headedness or
peripheral tingling• Repeatedly normal physical examination of chest
when symptomatic• Normal PEF/Spirometry when symptomatic• No response to trial of asthma therapy• Clinical features pointing to alternative diagnosis

Asthma in children - intermediate probability
• In between the two!• Try reversibility – using PEFR• Trial of treatment• Ensuring appropriate devices and
explanation of medication use• Consider other testing but ? not
appropriate in primary care (exercise testing, allergy testing)

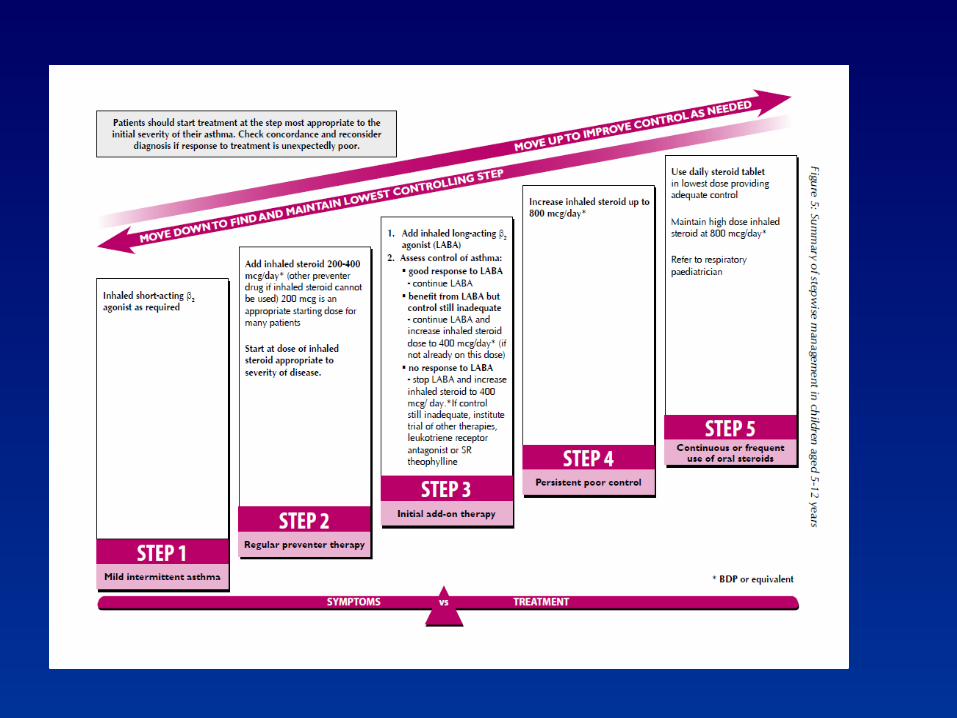
Asthma treatment in children

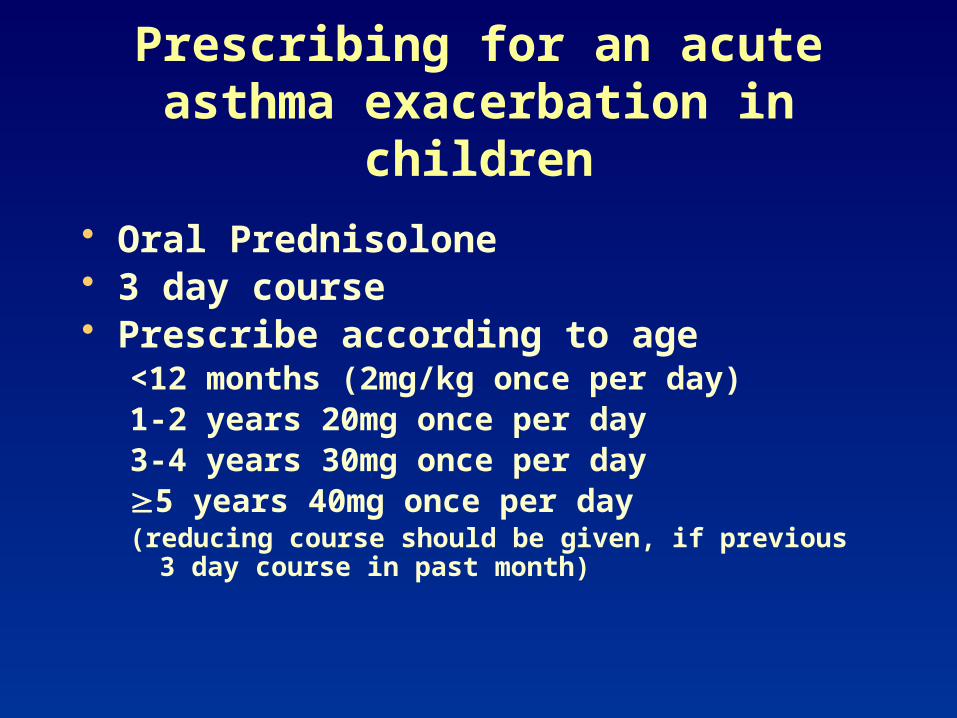
Prescribing for an acute asthma exacerbation in children
• Oral Prednisolone• 3 day course• Prescribe according to age
<12 months (2mg/kg once per day)1-2 years 20mg once per day3-4 years 30mg once per day5 years 40mg once per day(reducing course should be given, if previous 3 day course
in past month)

Prescribing for an acute asthma exacerbation in children in any
age group
Increased Bronchodilator: Salbutamol - remember the
4’s4 puffs4 times a day4 days
Acute attack10 puffs Salbutamol through
Spacer – no more than 2 multi doses within 24hrs without review

Please consider….
• Oral Prednisolone for Preschool Children with Acute Virus-Induced Wheezing
• Jayachandran Panickar, M.D., M.R.C.P.C.H., Monica Lakhanpaul, M.D., F.R.C.P.C.H., Paul C. Lambert, Ph.D.,
• Priti Kenia, M.B., B.S., M.R.C.P.C.H., Terence Stephenson,
D.M., F.R.C.P.C.H., Alan Smyth, M.D., F.R.C.P.C.H., and Jonathan Grigg, M.D., F.R.C.P.C.H.
• n engl j med 360;4 nejm.org January 22, 2009

• Viral wheeze is common• Conventional ‘asthma’ treatments
may not be effective• Caution – repeated oral steroid
prescribing without perceived day 1 response
• Limited effect from inhaled steroids• Is Montelukast a good alternative?

ACUTE PRE-SCHOOL WHEEZE– Montelukast may shorten duration of
symptoms around colds and respiratory viruses
– Some suggestion of acute reduction in trouble breathing in association with infections
Bacharier J Allergy Clin Immunol 2008

Ref Help


















