84
PAIN IN ELDERLY Cho Mar Lwin, Chit Soe 18.10.13 Pain-Elderly 1
| Date post: | 16-Jul-2015 |
| Category: |
Healthcare |
| Upload: | myanmarrheumatology |
| View: | 196 times |
| Download: | 4 times |
PAIN IN ELDERLY
Cho Mar Lwin, Chit Soe
18.10.13 Pain-Elderly 1

Pain in the Elderly
• Definition of Pain—An individual’s
unpleasant sensory or emotional
experience
– Acute pain is abrupt usually abrupt in onset
and may escalate
– Chronic pain is pain that is persistent or
recurrent
18.10.13 Pain-Elderly 2

18.10.13 Pain-Elderly 3

Age related changes:
Reduction in number and function of peripheral nociceptive neurons.
Sensory threshold for thermal and vibratory stimuli increase with age.
Pain receptors: 50% decrease in Pacini's corpuscles,10%-30% decrease in Meissner's/Merkle's disks
Diminished endogenous analgesic response (endorphins)
in the older patients.
Geriatric medicine: An evidence based approach 4th edition 2003
18.10.13 Pain-Elderly 4
Age related changes:
Peripheral nerves :
Myelinated nerves
Decreased density
Increase abnormal/degenerating fibers
Slower conduction velocity
Unmyelinated nerves
Decreased number of large fibers (1.2-1.6 mm
No change in small fibers (0.4 mm)
Substance P content decreased
18.10.13 Pain-Elderly 5

Age related changes:
Central nervous system
Loss in dorsal horn neurons
Altered endogenous inhibition, hyperalgesia
Loss of neurons in cortex, midbrain, brainstem
18% loss in thalamus
Altered cerebral evoked responses
Decreased catacholamines, acetylcholine,
GABA, serotonin
Endogenous opioids: mixed changes
Neuropeptides: no change
18.10.13 Pain-Elderly 6

Prevalence of pain in Elderly
1 in 5 elderly have pain
• 18% above 65 are taking pain medications regularly
• One-fifth of adults 65 years and older said they had experienced pain in the past month that persisted for more than 24 hours.
• Almost three-fifths of adults 65 and older with pain said it had lasted for one year or more.
• Women report severely painful joints more often than men (10 percent versus 7 percent).
CDC′s National Center for Health Statistics 2006,
18.10.13 Pain-Elderly 7

Pain in the Elderly
• The most common reason for unrelieved
pain in the U.S. is failure of staff to
routinely assess for pain
• Therefore, JCAHO has incorporated
assessment of pain into its practice
standards
• “The fifth vital sign”
18.10.13 Pain-Elderly 8

Return to top.
In 2000 42% of population >65 and over reported long lasting
disability
18.10.13 Pain-Elderly 9

Pain in the ElderlySources of pain in the nursing home
Source: Stein et al, Clinics in Geriatric
Medicine: 1996Condition causing pain Frequency (%)
Low back pain 40
Arthritis 37
Previous fractures 14
Neuropathies 11
Leg cramps 9
Claudication 8
Headache 6
Generalized pain 3
Neoplasm: 318.10.13 Pain-Elderly 10

Pain in the Elderly
• Degenerative joint
disease
• Gastrointestinal causes
• Fibromyalgia
• Peripheral vascular
disease
• Rheumatoid arthritis
• Post-stroke syndromes
• Low back disorders
• Improper positioning
Conditions Associated with the Development of
Pain in the Elderly
18.10.13 Pain-Elderly 11

Pain in the Elderly
• Crystal-induced
arthropathies
• Renal conditions
• Gastrointestinal
disorders
• Osteoporosis
• Immobility, contracture
• Neuropathies
• Pressure ulcers
• Headaches
• Amputations
• Oral or dental Pathology
Conditions Associated with the Development of
Pain in the Elderly
18.10.13 Pain-Elderly 12

Pain in the Elderly: Myths
• To acknowledge pain is a sign of personal
weakness
• Chronic pain is an inevitable part of aging
• Pain is a punishment for past actions
• Chronic pain means death is near
• Chronic pain always indicates the presence of a
serious disease
• Acknowledging pain will mean undergoing
intrusive and possible painful tests.
18.10.13 Pain-Elderly 13

Pain in the Elderly
Consequences of untreated pain:
• Depression
• Suffering
• Sleep disturbance
• Behavioral disturbance
• Anorexia, weight loss
• Deconditioning, increased falls
18.10.13 Pain-Elderly 14

18.10.13 Pain-Elderly 15

18.10.13 Pain-Elderly 16

Treatment
Age-Related Physiologic Changes
Decreased renal function
Decreased volume of distribution because
of decreased lean body weight
Decreased liver mass and hepatic blood
flow
Decreased activity of some drug-
metabolizing enzymes
Decreased serum protein concentrations 18.10.13 Pain-Elderly 17

18.10.13 Pain-Elderly 18

Treatment
Nonopioid Analgesics for Older Adults
Acetaminophen:
1)Treatment of choice for Osteoarthritis
2)Exhibits an analgesic ceiling beyond which
higher doses do not provide greater pain
relief.
3) Maximum dose 4 gm/day
18.10.13 Pain-Elderly 19
Treatment
Nonselective NSAIDs
Inhibit prostaglandin synthesis
Appropriate for short term use
All have ceiling effect
Risk of gastrointestinal bleed, renal
impairment, platelet dysfunction
Selective COX-2 inhibitors (celecoxib is
only one currently available in U.S.)
Reduced gastrointestinal side-effects and 18.10.13 Pain-Elderly 20
18.10.13 Pain-Elderly 21

Treatment with Opioids
Stimulates mu opioid receptor.
Used for moderate to severe pain.
Used for both nociceptive and neuropathic
pain.
Opioid drugs have no ceiling to their
analgesic effects and have been shown to
relieve all types of pain.
Elderly people, compared to younger
people, may be more sensitive to the
analgesic properties.
18.10.13 Pain-Elderly 22

Opioids
Morphine
Hepatic metabolism and renally excreted; not dialyzable.
Oral bioavailability 30-40%,
M6G is active metabolite with analgesic activity,
M3G is another metabolite causes neurotoxicity,
Morphine is available in oral (liquid and pill), topical, sublingual, parenteral, intrathecal, epidural and rectal routes.
High doses can lead to myoclonus and hyperalgesia.
18.10.13 Pain-Elderly 23

Opioids
Oxycodone
Only available in oral form
More potent than morphine
Available as single agent and in combination with NSAIDs and acetamenophen
Available in long-tacting, slow release form – OxyContin)
Methandone
Blocks NMDA receptors, inexpensive, lacks active metabolite
Used for neuropathic pain
Variable(long) half-life, high tissue distribution,
Converting from any opioid to methadone takes several days
18.10.13 Pain-Elderly 24

Opioids
Hydrocodone (Vicodin, Lortab, Norco, others)
Only available in combination with acetamenophen or NSAID
Hydromorphone (Dilaudid)
5 times more potent than morphine
Not available in long acting preparation
Propoxyphene (darvocet)
very weak analgesic effect, can cause ataxia and neurotoxicity, twofold higher risk of hip fractures.
18.10.13 Pain-Elderly 25

Non-opioid medications for pain Tricyclic antidepressants ( amytriptyline, desipramine) for
neuropathic pain, depression, sleep disturbance. Not used often due to side-effects.
Duloxetine (Cymbalta ) is newer antidepressant FDA approved for neuropathic pain.
Anticonvulsants ( gabapentin, pregabalin, carbamazepine)
for neuropathic pain. Carbamazepine can be used for trigeminal neuralgia, may cause pancytopenia.
Muscle relaxants : for muscle spasm, monitor for sedation
Local anesthetics (lidocaine patch, topical voltaren gel, capsaicin). Capsaicin depletes substance P, may take weeks to reach full effect, adverse effects include burning and erythema. Lidocain patch FDA approved for post herpetic neuralgia.
Placebos: unethical
18.10.13 Pain-Elderly 26

Non-opioid treatment
Massage reduces pain, including release of
muscle tension, improved circulation,
increased joint mobility, and decreased
anxiety
TENS unit: Can be considered for diabetic
neuropathy but not for chronic low back
pain
18.10.13 Pain-Elderly 27

Non-drug treatment
Education: basic knowledge about pain (diagnosis, treatment, complications, and prognosis), other available treatment options, and information about over-the-counter medications and self-help strategies.
Exercise: tailored for individual patient needs and lifestyle; moderate-intensity exercise, 30 min or more 3-4 times a week and continued indefinitely.
Physical modalities (heat, cold, and massage)
Cold for acute injuries in first 48 hours, to decrease bleeding or hematoma formation, edema, and chronic back pain. Heat works well for relief of muscle aches and abdominal cramping.
18.10.13 Pain-Elderly 28

Non-drug treatment
Physical or occupational therapy; should be
conducted by a trained therapist
Chiropractic: Effective for acute back pain.
Potential spinal cord or nerve root
impingement should be ruled out before any
spinal manipulation
Acupuncture: Performed by qualified
acupuncturist. Effects may be short lived
and require repetitive treatments18.10.13 Pain-Elderly 29

Non-drug treatments
Relaxation: repetitive focus on sound, sensation, muscle
tension, inattention towards intrusive thoughts. Requires
individual acceptance and substantial training.
Meditation: Guided or self-directed technique for calming the
mind, allows thoughts, emotions and sensations to travel
through conscious awareness without judgment.
Progressive muscle relaxation: Individual tensing and relaxing
of certain muscle groups.
Hypnosis: effective analgesic, state of inner absorption and
focused attention. Reduces pain by distraction, altered pain
perception, increased pain threshold.Norelli L J et.al., : Behavioral approaches to pain management in the elderly, 24(2), Clinics in Geriatric Medicine, 2008.
18.10.13 Pain-Elderly 30

Consequences of untreated pain
Impaired function: Pain can lead to decreased activity and ambulation leading to de-conditioning, gait disturbances and injuries from falls.
Sleep deprivation: decrease pain thresholds, limit the amount of daytime energy, increased risk of depression and mood disturbances.
Increases financial and care giving burdens placed on families and friends by increased utilization of health care services.
Diminished quality of life by isolating individuals from important social stimulation, amplifying the functional and emotional losses already experienced from undertreated pain.
Jakobsson, U. et.al., Old people in pain: A comparative study. Journal of Pain and Symptom Management, 26, 625-636,2003.Weiner, D.K., et.al., Pain in nursing home residents; management strategies. Drugs and Aging, 18(1), 13-19,2001.
18.10.13 Pain-Elderly 31

Epidemiology of LBP
Among Older Adults

LBP in Older Adults
• Little research has been done in the area of
LBP among the older population (>65yrs).
• Reasons for lack of research interest in
older adults with LBP?
– Younger, working population
– Less serious than other conditions/diseases
– Societal attitudes
18.10.13 Pain-Elderly 33

Epidemiology
• Prevalence of LBP is uncertain in 65yo+
– 6.8% to 49%
• Factors influencing prevalence reports
– cognitive impairment, decreased pain
perception, co-morbidities, resignation to
perceived effects of aging, depression
18.10.13 Pain-Elderly 34

What do we know so far?
• Back Pain is associated with impaired function
(ADL’s and mobility)– SOF (women)
– Iowa 65+ Rural Health Study
– WHAS (women)
– Framingham
– Health ABC
*primarily measure self-reported function
• Very little research done in the areas of underlying
mechanisms or interventions in this age group
18.10.13 Pain-Elderly 35

1.67
1.77
1.87
1.97
2.07
2.17
2.27
Year 1 Year 4
No/Mild Back Pain Mod/Extreme Back Pain
Back Pain and Function
Hicks et al, J Gerontol Med Sci, Nov 200518.10.13 Pain-Elderly 36

• Population-based survey study
• 522 men (32%) and women
• Aged 60 and above
• Independently living resident in one of four CCRCs
in MD and Northern VA
Retirement Community Back Pain Study
18.10.13 Pain-Elderly 37

30
35
40
45
50
55
60
65
70
PCS MCS
No pain LBP only LBP + leg pain
PCS and MCS Subscale Scores
by LBP status
Good Health
Poor Health
Norm
P<.0001 P<.0001
18.10.13 Pain-Elderly 38
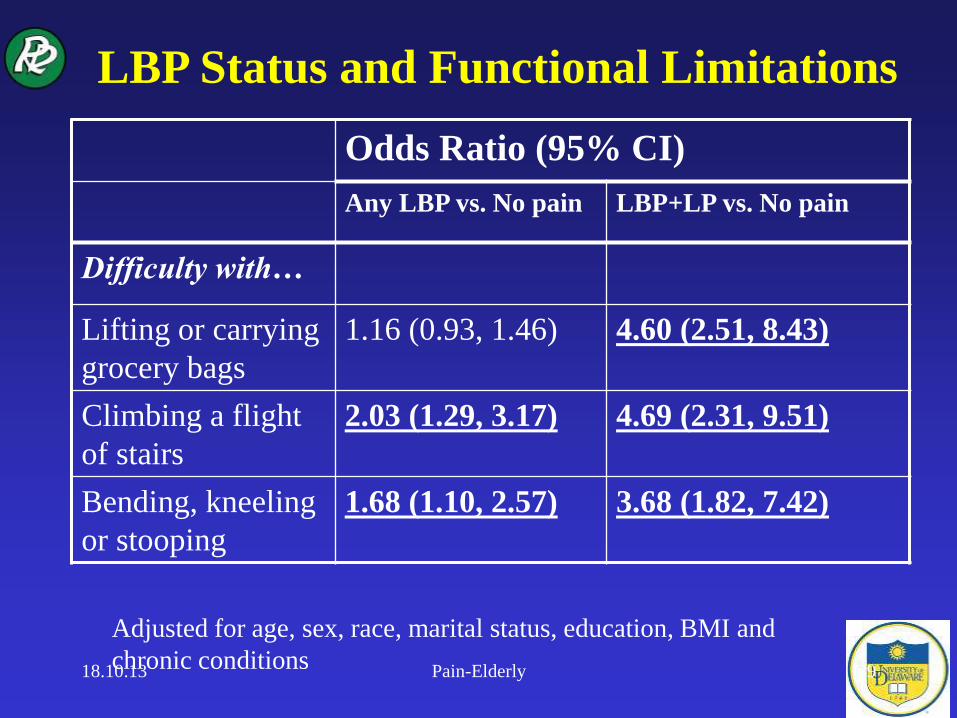
LBP Status and Functional Limitations
Odds Ratio (95% CI)
Any LBP vs. No pain LBP+LP vs. No pain
Difficulty with…
Lifting or carrying
grocery bags
1.16 (0.93, 1.46) 4.60 (2.51, 8.43)
Climbing a flight
of stairs
2.03 (1.29, 3.17) 4.69 (2.31, 9.51)
Bending, kneeling
or stooping
1.68 (1.10, 2.57) 3.68 (1.82, 7.42)
Adjusted for age, sex, race, marital status, education, BMI and
chronic conditions18.10.13 Pain-Elderly 39

LBP Status and Functional Limitations
Odds Ratio (95% CI)
Any LBP vs. No pain LBP+LP vs. No pain
Difficulty with…
Walking several
blocks
1.18 (0.95, 1.46) 3.97 (2.19, 7.20)
Walking one block 1.00 (0.80, 1.25) 3.79 (2.05, 6.99)
Bathing and
dressing
1.08 (0.83, 1.39) 3.53 (1.54, 8.09)
Adjusted for age, sex, race, marital status, education, BMI and
chronic conditions18.10.13 Pain-Elderly 40

LBP Status and Functional Limitations
Odds Ratio (95% CI)
Any LBP vs. No pain LBP+LP vs. No pain
Fallen in past year 1.10 (0.90, 1.34) 2.05 (1.11, 3.78)
Assistive device
for walking
1.02 (0.82, 1.27) 2.81 (1.45, 5.46)
Fair/poor self-
rated health
1.09 (0.87, 1.38) 2.64 (1.34, 5.31)
Social interference
due to physical
problems
1.08 (0.80, 1.46) 8.94 (2.73, 29.26)
Adjusted for age, sex, race, marital status, education, BMI and
chronic conditions18.10.13 Pain-Elderly 41

• Less than half (45.2%) with LBP sought care
– LBP only: 30% sought care
– LBP + leg pain: 65% sought care
• All sought care with a physician, but no other
healthcare practitioners (i.e. PT, DC, CMT)
• Only 37.7% took prescription meds for LBP
Care-seeking and LBP
18.10.13 Pain-Elderly 42

• Two mainstays in conservative management of LBP
are active rehabilitation and medication use
– Interestingly, no one received PT services and <40% were
prescribed medicine
• Why do so few older adults seek care?
• The combination of high prevalence and low care-
seeking suggests that clinicians who see older adults
should routinely:
– Ask targeted questions about LBP and leg pain
– Make appropriate referrals prn to prevent decline
Summary
18.10.13 Pain-Elderly 43

Epidemiology
• Depression and Back Pain in the Elderly– Depressive symptoms are common in older adults
– Depressive symptoms and LBP are strongly associated in
cross-sectional studies
– Chronic pain can increase risk for depressive symptoms
– Depressive symptoms are a strong, independent risk factor
for onset of disabling back pain 1 year later (Reid, 2003)
– Disabling LBP increases odds of depressive symptoms 2
years later (Meyer, 2007)
– Relationship may be bi-directional
18.10.13 Pain-Elderly 44

Classification and Staging
of Older Patients with LBP

First-Level Classification
Physical Therapy Only Consultation Referral
Stage 1
Stage 2
Stage 3
Inflammatory Process
(Medical)
Psychological
Medical
Psychological
Surgical
18.10.13 Pain-Elderly 46

First-Level Classification
Serious Pathology
• Sleep disturbances
• Bowel/Bladder Dysfunction
• Unexplained Weight Loss
• Recent Episodes of Fever Related to LBP
• Trauma
18.10.13 Pain-Elderly 47

First-Level Classification
Serious Pathology
• Abdominal Aortic Aneurysm (AAA)
– Ballooning of the aorta
• Risk factors- HTN and atherosclerosis
• Most often seen in older, Caucasian men
• Medical emergency when rupture occurs
18.10.13 Pain-Elderly 48

18.10.13 Pain-Elderly 49

First-Level Classification
Abdominal Aortic Aneurysm (AAA)
– Symptoms
• Back pain—severe, sudden, persistent
• Pulsating sensation in abdomen
• Pain in abdomen
• Nausea and vomiting
• Light-headedness and fainting with upright posture
– Signs
• Bruit on auscultation “Whooshing sound”
• Pulsatile mass sensitive to palpation around umbilicus
• Rapid Pulse18.10.13 Pain-Elderly 50

Second-Level Classification
18.10.13 Pain-Elderly 51
Third-Level Classification
• Immobilization
• Mobilization
– Sacroiliac
Mobilization
– Lumbar
Mobilization
• Specific Exercise
– Extension Syndrome
– Flexion Syndrome*
– Lateral Shift
(able to centralize)
• Traction
18.10.13 Pain-Elderly 52

Differential Diagnosis:
LBP vs. Hip Pain

LBP vs. Hip Pain
• Source = Lumbar spine
– Provocation and amelioration of symptoms
with spinal movement
• Source = Hip
– Hip Osteoarthritis (OA)
– Hip fracture
– Trochanteric bursitis
Ben-Galim et al. Hip-spine syndrome: the effect of total hip replacement surgery
on low back pain in severe osteoarthritis of the hip. Spine 200718.10.13 Pain-Elderly 54
Hip OA(Altman et al, 1991)
Presence of all 5 findings
• Hip Pain
• Hip IR > 15 degrees
• Pain with Hip IR
• Morning Stiffness
< 60 minutes
• >50 years of age
Presence of all 3 findings
• Hip Pain
• Hip IR < 15 degrees
• Hip Flexion < 115
degrees
Undiagnosed hip OA is one of the leading causes of failed
back surgery syndrome18.10.13 Pain-Elderly 55

Management of the Patient
in Stage I

Stabilization/Immobilization
Category
Do we need to address the core
muscles to reduce pain and improve
function in older adults with LBP?

Kirkaldy-Willis Model of LBP
DysfunctionDegenerative changes begin
InstabilityAbnormal movement due to degenerative changes
StabilizationSevere degenerative changesDevelopment of osteophytesMotion limitations18.10.13 Pain-Elderly 58

Spinal Stabilizing System
The spinal stabilizing system consists of
three inter-related subsystems:
Neuromuscular
Control
Passive
Subsystem
Active
Subsystem
18.10.13 Pain-Elderly 59

Active Subsystem:
Aging Factors• Decreased muscle strength and mass associated
with aging (Sarcopenia)
– May be due to a decrease in number of muscle fibers,
size of individual fibers or both
• Type II (fast-twitch) fiber atrophy associated
with aging
– Results in slower muscle contractile properties
– Can be reversed with training
• Decreased muscle attenuation (increased
intramuscular fat infiltration) is associated with
aging muscle 18.10.13 Pain-Elderly 60

• Longitudinal cohort study
• 3075 black (42%) and white, men (48%) and women
• Aged 70-79 years between 4/97 – 6/98
• Community-resident in Memphis or Pittsburgh
• Well-functioning- no reported difficulty walking ¼ mile, up 10 steps,
or performing basic ADL
- no need for a walking aid or proxy respondent
• Present analysis—Pittsburgh site only•1527 black (44%) and white, men (48%) and women
•CT scans of paraspinous muscles only done in Pittsburgh
Health, Aging and Body Composition Study
18.10.13 Pain-Elderly 61

14
16
18
20
22
24
Baseline
No LBP Mild LBP Mod LBP Severe/Extreme LBP
Back Pain & Trunk Muscle Composition
Hicks et al, J Gerontol Med Sci, Jul 2005
p-value for trend <.0001
18.10.13 Pain-Elderly 62

1.67
1.77
1.87
1.97
2.07
2.17
2.27
Year 1 Year 4
No/Mild Back Pain Mod/Extreme Back Pain
Back Pain and Function
Hicks et al, J Gerontol Med Sci, Nov 200518.10.13 Pain-Elderly 63

Variable Parameter
Estimate
Standard
Error
Partial
R2
Intercept 2.585 .590
Trunk Muscle Attenuation .006* .002 .123
Thigh Muscle Attenuation -.002 .003 .024
Back Pain Severity -.088* .029 .003
Covariates .369
Model R2=.519† Dependent Variable=Health ABC PPB
18.10.13 Pain-Elderly 64

Muscle attenuation, HU, at Year 1Hea
lth
AB
C P
hysi
cal
Per
form
ance
Bat
tery
Yea
r 4
No/Mild Back Pain
Mod/Extreme Back Pain
18.10.13 Pain-Elderly 65

Variable Parameter
Estimate
Standard
Error
Partial
R2
No/Mild Back Pain
Intercept 2.500 .667
Trunk Muscle Attenuation .005* .002 .087
Thigh Muscle Attenuation -.001 .003 .025
Covariates .372
Model R2=.484‡ Dependent Variable=Health ABC PPB
Moderate/Extreme Back Pain
Intercept 2.312 1.240
Trunk Muscle Attenuation .006† .004 .178
Thigh Muscle Attenuation -.002 .006 .023
Covariates .336
Model R2=.537‡ Dependent Variable=Health ABC PPB18.10.13 Pain-Elderly 66

Point
Estimate 95% CI
Trunk Muscle Attenuation
1st Quartile (Lowest Quality) 4.50 (1.55, 13.03)
2nd Quartile 3.10 (1.29, 7.46)
3rd Quartile 1.61 (.73, 3.58)
4th Quartile (Best Quality) 1.00 ------
Trunk Muscle Attenuation & Falls in
Elders with Significant LBP
Model was adjusted for age, sex, race, BMI, disease status, thigh muscle
composition, benzodiazepine use and year 1 functional performance score.
Hicks et al, Unpublished preliminary data18.10.13 Pain-Elderly 67

• Addressing trunk muscle composition/ core
muscle integrity may be an important, yet
overlooked, approach to manage symptoms,
maintain functional mobility and potentially
reduce balance impairments and falls in older
adults with a history of significant back pain
Conclusions
18.10.13 Pain-Elderly 68

Mobilization Sub-Group:
Aging Factors
• Facet joint degeneration (OA) is associated with the
aging spine
• Dessication of the disc occurs with time
• Changes in the disc height also affect amount of
loading on the facet joints and can lead to
approximation of spinous processes
• Which position is more likely to irritate facet joints--
flexion or extension?
• What types of manipulation techniques to avoid?18.10.13 Pain-Elderly 69

Mobilization Sub-Group:
Aging Factors• Consider use of muscle energy techniques
• Must consider entire patient history before undertaking
manipulation or mobilization
• Any factors that would suggest manipulation/
mobilization as unsafe or questionable
– osteoporosis, infection, fracture, spondylolysis/listhesis, CA,
prolonged steroid use, severe degenerative changes
– If any doubt, find another way to achieve the goal of
increasing mobility
18.10.13 Pain-Elderly 70

Specific Exercise:
Key Examination Findings
• Extension Principle
– symptoms centralize with lumbar extension
– symptoms peripheralize with lumbar flexion
• Treatment
– Extension exercises
– Avoid flexion activities (bracing)
• Not typically seen in older adult
18.10.13 Pain-Elderly 71

Specific Exercise:
Key Examination Findings
• Flexion Syndrome
– symptoms centralize with lumbar flexion
– symptoms peripheralize with lumbar extension
• Treatment
– Flexion exercises
– Avoid extension activities (bracing)
• *Typically seen in older adult
18.10.13 Pain-Elderly 72

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
• LSS = narrowing of the spinal canal, nerve
root canal, and/or intervertebral foramina
• Usually acquired due to degenerative
changes
– facet joint arthrosis, ligamentum flavum
thickening, posterior bulging of discs,
spondylolisthesis
• Leg pain reported in 90% of cases
• Neurologic changes in 50% of cases18.10.13 Pain-Elderly 73

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
• Extension results in narrowing of the
dimensions of the central and lateral spinal
canals
• Axial loading also narrows the canals
18.10.13 Pain-Elderly 74

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
• Key Exam Findings
– Age > 65 (+LR=2.5)
– No pain when seated (+LR=6.6)
– Symptoms improved when seated (+LR=3.1)
– Improved walking tolerance with spinal flexion
(+LR=6.4)
18.10.13 Pain-Elderly 75
Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
Differential Diagnosis: Neurogenic vs.
Vascular Claudication
• Both conditions may present as cramping
pain, tightness and fatigue in LE’s during
walking and relieved by sitting
• Vascular claudication is typically secondary
to PAD
18.10.13 Pain-Elderly 76

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
Differential Diagnosis: Neurogenic vs.
Vascular Claudication
• Bicycle Test (Dyck & Doyle, 1977)
– Neurogenic -- Pt would pedal further with
flexed spine than with extended spine
– Vascular --Pt would pedal equal distances
regardless of position of the spine
– Results were not sufficiently sensitive for this
test (Dong and Porter, 1989)18.10.13 Pain-Elderly 77

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
Differential Diagnosis: Neurogenic vs. Vascular Claudication
• Ankle Brachial Index
– Supine
– Typical systolic measurement from arm
– Systolic measurement from leg
• Cuff around ankle
• Dorsalis Pedis or Posterior Tibial Arteries
– <.90 indicates Peripheral Arterial Disease
18.10.13 Pain-Elderly 78

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
Two-Staged Treadmill Test
• Pt walks on level surface (10 min or
fatigue) followed by incline surface (10 min
or fatique) with a 10 min rest break in
between
– Earlier onset of symptoms on level vs. incline
(+LR=4.1 for neurogenic claudication)
– Longer recovery time after level vs. incline
(+LR=2.6 for neurogenic claudication)18.10.13 Pain-Elderly 79

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
• Surgical intervention is common
– Fusion and Decompression Procedures
• Surgical rates are on the rise for LSS
• In 1994, nearly $1billion spent on LSS surgery
• 23% re-operation rate
• Increased complication rates when surgical
interventions used on older adults
• Non-surgical treatment has not been well-
explored yet.18.10.13 Pain-Elderly 80

Lumbar Spinal Stenosis (LSS):
Flexion Syndrome Sub-Group
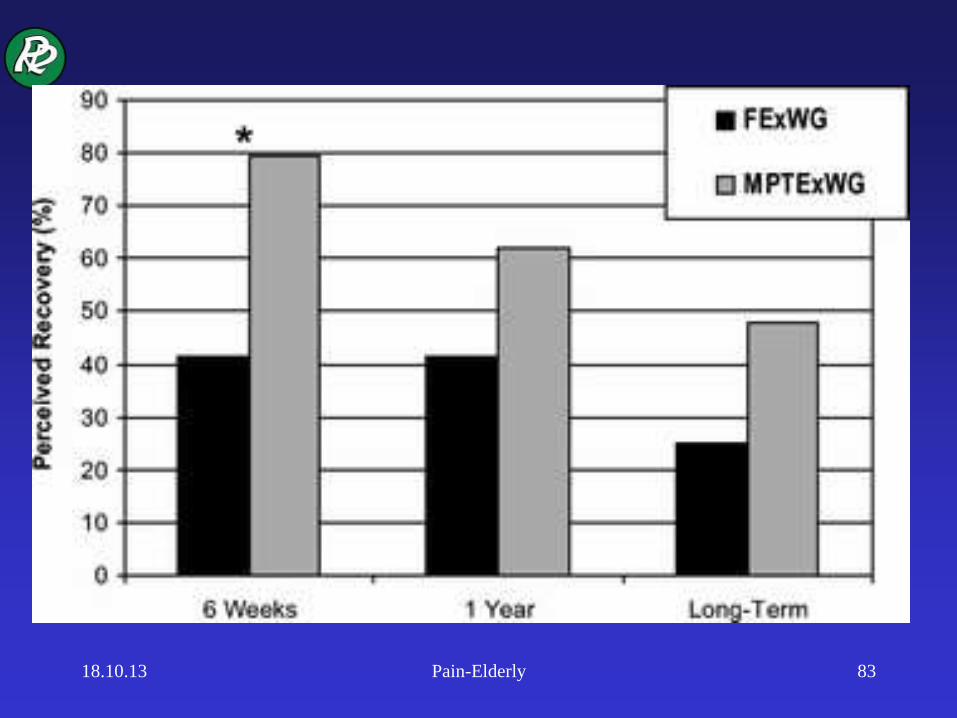
• Comparison between 2 PT treatments for LSS (Whitman et al, Spine, 2006)
– Randomized to:
• Flexion, Sub-therapeutic ultrasound and Level walking
on treadmill
or
• Manual Therapy, Exercise and Body-Weight Supported
walking on treadmill
18.10.13 Pain-Elderly 81

BWS Treadmill Ambulation
• De-weighted ambulation on a treadmill is also an option. (Fritz et al., Phys Ther, 1997)
• Shown to reduce compressive forces on the body. (Flynn et al., Phys Ther, 1997)
• Progression is made by decreasing the traction force.
18.10.13 Pain-Elderly 82
18.10.13 Pain-Elderly 83

18.10.13 Pain-Elderly 84


![2017 WSES and SICG guidelines on acute calcolous ... · and epigastric pain has been reported in studies focused on the elderly patients [16–18]. Atypical pain or no pain at all](https://static.documents.pub/doc/80x56/6096156f9d1c3d3b33774577/2017-wses-and-sicg-guidelines-on-acute-calcolous-and-epigastric-pain-has-been.jpg)














