Topical review Pain modulation profile and pain therapy: Between pro- and antinociception David Yarnitsky a,b,⇑ , Michal Granot c , Yelena Granovsky a,b a Department of Neurology, Rambam Medical Center, Haifa, Israel b Clinical Neurophysiology Lab, Technion Faculty of Medicine, Haifa, Israel c Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa, Israel 1. Introduction A large body of knowledge has been generated on human pain modulation when pain-free and when experiencing pain on the basis of, among other tools, psychophysical dynamic stimulation protocols, which utilize a spatial and/or temporal array of stimuli in order to evoke an experimental process of pain modulation. Protocols designed to evoke inhibition or facilitation of pain are be- lieved to better depict the clinical pain experience than the classi- cal static parameters, such as pain thresholds. A commonly used protocol for pain inhibition is based on the diffuse noxious inhibi- tory control (DNIC) effect, typically using 2 remote painful stimuli, whose interaction generates, in most cases, pain inhibition [12] (for review, see Pud et al. [21]). The term conditioned pain modula- tion (CPM) was coined for the psychophysical protocols that explore DNIC in humans [28]. The protocols for pain facilitation use temporal summation (TS), where pain reports are obtained along a series of identical stimuli [19]. The common response is an increase in pain ratings along the series representing the phys- iological phenomenon of windup. Evaluation of response to these arrays of experimental pain can be a useful clinical tool; it can predict future pain [27] and predict the efficacy of analgesics [29]. Although the current data do not allow practical implementa- tion, the following hypothesis may carry the translation of pain modulation into practice. 2. Hypothesis Lab-based pain modulation, for which the term pain modulation profile (PMP) is suggested, ranges between inhibitory and facilita- tory ends. We propose that on the basis of CPM and/or TS responses, which indicates the inhibitory/facilitatory balance, individuals can be positioned on a clinical spectrum between pron- ociception and antinociception. Thus, an individual expressing low-efficiency CPM and/or enhanced TS positioned on the pronociceptive side of the spectrum would express a higher pain phenotype, resulting, for example, in higher risk of pain acquisi- tion. In turn, an individual expressing efficient CPM and/or nonen- hanced TS located on the antinociceptive side would express a lower clinical pain phenotype (Fig. 1). 3. Evidence Convincing evidence associates pain-lab-based altered pain modulation and clinical pain morbidity, mostly describing a pron- ociceptive pain modulation in pain patients compared to controls. For CPM, less efficient inhibitory pain modulation was reported for several pain syndromes, including fibromyalgia [7,10], irritable bowel syndrome [2], migraine [22], tension headache [18], tempo- romandibular disorder [14], osteoarthritis and muscle pain [8], and whiplash [3] (see also review in [13]). For TS, enhanced pain facil- itation has been documented in fibromyalgia [20], osteoarthritis [1], migraine [25], and temporomandibular disorder [23]. Several articles have also reported co-occurrence of both enhanced TS and less efficient CPM in pain patients, such as osteoarthritis [1], cluster headache [17], and chronic postmastectomy pain [4]. Thus, a pronociceptive profile seems to be associated with pain morbid- ity. It is noted that in most of the above articles, assessment of pain modulation was performed in unaffected body areas, thus repre- senting the generalized pain modulation rather than the modula- tion of data transmitted from a specific painful region. Notably, pronociceptive profile was reported in widespread pain disorders such as fibromyalgia. The above-mentioned cross-sectional studies do not reveal whether the interrelations between the modulation profile and the presence of the various pain syndromes are causative, and if so, which is primary to the other. It could be, on the one hand, that a preexisting facilitatory modulation state leads to the establish- ment of the pronociceptive profile and the acquisition of the idiopathic pain syndromes; on the other hand, it could be that Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article. 0304-3959/$36.00 Ó 2013 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.pain.2013.11.005 ⇑ Corresponding author at: Department of Neurology, Rambam Health Care Campus, Haifa, Israel. Tel.: +972 48542605; fax: +972 48542755. E-mail addresses: [email protected], [email protected](D. Yarnitsky). PAIN Ò 155 (2014) 663–665 www.elsevier.com/locate/pain
Transcript
PAIN�
155 (2014) 663–665
w w w . e l s e v i e r . c o m / l o c a t e / p a i n
Topical review
Pain modulation profile and pain therapy: Betweenpro- and antinociception
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
0304-3959/$36.00 � 2013 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.pain.2013.11.005
⇑ Corresponding author at: Department of Neurology, Rambam Health CareCampus, Haifa, Israel. Tel.: +972 48542605; fax: +972 48542755.
David Yarnitsky a,b,⇑, Michal Granot c, Yelena Granovsky a,b
a Department of Neurology, Rambam Medical Center, Haifa, Israelb Clinical Neurophysiology Lab, Technion Faculty of Medicine, Haifa, Israelc Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa, Israel
1. Introduction ociception and antinociception. Thus, an individual expressing
A large body of knowledge has been generated on human painmodulation when pain-free and when experiencing pain on thebasis of, among other tools, psychophysical dynamic stimulationprotocols, which utilize a spatial and/or temporal array of stimuliin order to evoke an experimental process of pain modulation.Protocols designed to evoke inhibition or facilitation of pain are be-lieved to better depict the clinical pain experience than the classi-cal static parameters, such as pain thresholds. A commonly usedprotocol for pain inhibition is based on the diffuse noxious inhibi-tory control (DNIC) effect, typically using 2 remote painful stimuli,whose interaction generates, in most cases, pain inhibition [12](for review, see Pud et al. [21]). The term conditioned pain modula-tion (CPM) was coined for the psychophysical protocols thatexplore DNIC in humans [28]. The protocols for pain facilitationuse temporal summation (TS), where pain reports are obtainedalong a series of identical stimuli [19]. The common response isan increase in pain ratings along the series representing the phys-iological phenomenon of windup. Evaluation of response to thesearrays of experimental pain can be a useful clinical tool; it canpredict future pain [27] and predict the efficacy of analgesics[29]. Although the current data do not allow practical implementa-tion, the following hypothesis may carry the translation of painmodulation into practice.
2. Hypothesis
Lab-based pain modulation, for which the term pain modulationprofile (PMP) is suggested, ranges between inhibitory and facilita-tory ends. We propose that on the basis of CPM and/or TSresponses, which indicates the inhibitory/facilitatory balance,individuals can be positioned on a clinical spectrum between pron-
low-efficiency CPM and/or enhanced TS positioned on thepronociceptive side of the spectrum would express a higher painphenotype, resulting, for example, in higher risk of pain acquisi-tion. In turn, an individual expressing efficient CPM and/or nonen-hanced TS located on the antinociceptive side would express alower clinical pain phenotype (Fig. 1).
3. Evidence
Convincing evidence associates pain-lab-based altered painmodulation and clinical pain morbidity, mostly describing a pron-ociceptive pain modulation in pain patients compared to controls.For CPM, less efficient inhibitory pain modulation was reported forseveral pain syndromes, including fibromyalgia [7,10], irritablebowel syndrome [2], migraine [22], tension headache [18], tempo-romandibular disorder [14], osteoarthritis and muscle pain [8], andwhiplash [3] (see also review in [13]). For TS, enhanced pain facil-itation has been documented in fibromyalgia [20], osteoarthritis[1], migraine [25], and temporomandibular disorder [23]. Severalarticles have also reported co-occurrence of both enhanced TSand less efficient CPM in pain patients, such as osteoarthritis [1],cluster headache [17], and chronic postmastectomy pain [4]. Thus,a pronociceptive profile seems to be associated with pain morbid-ity. It is noted that in most of the above articles, assessment of painmodulation was performed in unaffected body areas, thus repre-senting the generalized pain modulation rather than the modula-tion of data transmitted from a specific painful region. Notably,pronociceptive profile was reported in widespread pain disorderssuch as fibromyalgia.
The above-mentioned cross-sectional studies do not revealwhether the interrelations between the modulation profile andthe presence of the various pain syndromes are causative, and ifso, which is primary to the other. It could be, on the one hand, thata preexisting facilitatory modulation state leads to the establish-ment of the pronociceptive profile and the acquisition of theidiopathic pain syndromes; on the other hand, it could be that
Fig. 1. Proposed pain modulation profile and pain phenotypes.
664 D. Yarnitsky et al. / PAIN�
155 (2014) 663–665
the presence of the pain syndrome consumed the antinociceptivecapacity and led to a pronociceptive profile. We explored theserelationships in a prospective study, where prethoracotomy pain-free patients were examined for their pain modulation and werefollowed up for acquisition of chronic pain after surgery [27].CPM efficiency was found to predict chronic postthoracotomypain; patients with less efficient CPM had a higher risk ofdeveloping chronic pain, and vice versa. This reasonablyestablishes causative relations suggesting pronociceptive PMP asa pathogenetic factor for future clinical pain. Similar results werelater found by Landau et al. [9] and Wilder-Smith et al. [26] forcesarean section and abdominal surgery, respectively.
A second key question pertains to the intraindividual plasticityof the PMP. Two studies on osteoarthritis patients indicated thatPMP is plastic; Kosek and Ordberg [8] found that less efficientCPM obtained in patients with painful hip osteoarthritis improvedafter total hip replacement surgery in parallel with pain alleviation.Similar results have been reported by Graven-Nielsen et al. [6] forknee osteoarthritis. Yarnitsky et al. [29] and Niesters et al. [16]showed that pharmacological alleviation of polyneuropathy painimproved CPM in proportion to the extent of pain alleviation. Inline with this, parallel reduction of pain and TS response was re-ported for patients with complex regional pain syndrome aftersympathetic blockade [15]. Thus, PMP seems to change in conjunc-tion with changes in clinical pain.
A third and pertinent issue, one that provides the main motiva-tion for the use of PMP, is its relevance for pain treatment. By beinginvolved in pain pathogenesis, it is likely that PMP also plays a rolein its alleviation. Targeting a dysfunctional mechanism of painmodulation by a drug capable of rectifying that dysfunction willachieve the best pain alleviation. This way, patients with less effi-cient CPM should benefit more from serotonin norepinephrinereuptake inhibitors that augment descending inhibition by spinalmonoamine reuptake inhibition than patients whose CPM is al-ready efficient. Similarly, those with enhanced TS should benefitmore from gabapentinoids or NMDA blockers such as ketamine,which inhibit neuronal sensitization, than those whose baselinesummation was not enhanced.
We examined CPM and TS in painful diabetic neuropathypatients and found that CPM predicts the efficacy of duloxetine,an SNRI; patients with less efficient CPM experienced highly effica-cious pain reduction, while those with efficient CPM did not gainbenefits from the drug [29]. Further, in the first group, an improve-ment in CPM efficiency was found along with pain reduction,whereas no change in CPM was found in the second group.Similarly, Lavand’homme and Roelants [11] used ketamine for
post-cesarean section pain; they found that the more pronocicep-tive patients, those with enhanced TS, gained from ketamine,which attenuates neuronal sensitization, while those withnonenhanced TS did not benefit from the drug. It thus seems thatidentifying the dysfunctional modulation state can be the key tothe choice of drug for pain alleviation. This is a step forwardtoward individualized pain medicine.
4. Discussion
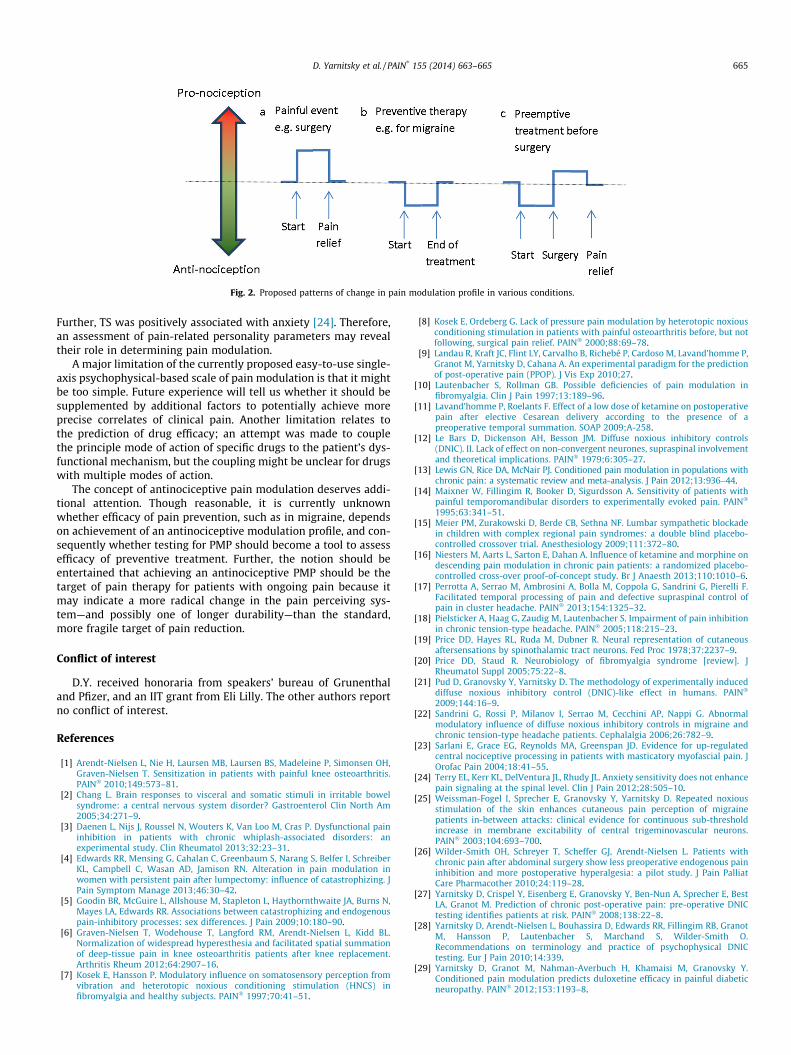
On the basis of the described evidence, and in conjunction withour hypothesis, we suggest the following scenario for the clinicalrelevance of pain modulation. (i) A pain-free individual expressesa certain PMP, be it eu-, pro-, or antinociceptive. Higherexpressions of clinical pain and higher chances of acquiring paincharacterize pronociceptive individuals, and vice versa. (ii) Whenexperiencing a substantial nociceptive event, modulation is shifted,and an altered pain modulation of pronociception develops. (iii)Use of pain-modulating drugs, as is routinely done for neuropathicpain and often for other sorts of pain, may rectify the dysfunctionalparameter or parameters of PMP; thus, an individual-basedcoupling of drug and modulation dysfunction can be established.(iv) Preventive treatment (eg, migraine prevention or preoperativepreemptive analgesia) shifts the profile toward antinociceptivityand lowers the pain phenotype (Fig. 2).
A few practical points need to be further clarified to ease clinicalapplication of PMP: clinical experimental data should be strength-ened; better test-to-test reliability of these psychophysical proto-cols should be obtained by improving them; and further studiesshould use various test modalities (ie, thermal, electrical, mechan-ical) and types of stimuli (ie, phasic, tonic, repetitive) because re-sults seem to depend on these factors. Further, the scientificbasis of the relevant pain modulation paradigms, mainly CPM,could be widened, clarifying the relations with other top-downpain-regulating mechanisms, including cognitive and emotionalfactors such as stress and anxiety. In addition, the interrelationsbetween the facilitatory and inhibitory factors and the relativeweight of each in construction of the PMP need furtherclarification.
Pain modulation is, of course, not a single player on the stage ofclinical pain, which is affected by the causative diseases in additionto many genetic and environmentally influenced psychological andcognitive factors. The alleviation of pain and rectifying of the pron-ociceptive profile is also influenced by pharmacogenetic factorsand drug interactions. For example, the association between CPMand pain was found to be mediated by pain catastrophizing [5].
Fig. 2. Proposed patterns of change in pain modulation profile in various conditions.
D. Yarnitsky et al. / PAIN�
155 (2014) 663–665 665
Further, TS was positively associated with anxiety [24]. Therefore,an assessment of pain-related personality parameters may revealtheir role in determining pain modulation.
A major limitation of the currently proposed easy-to-use single-axis psychophysical-based scale of pain modulation is that it mightbe too simple. Future experience will tell us whether it should besupplemented by additional factors to potentially achieve moreprecise correlates of clinical pain. Another limitation relates tothe prediction of drug efficacy; an attempt was made to couplethe principle mode of action of specific drugs to the patient’s dys-functional mechanism, but the coupling might be unclear for drugswith multiple modes of action.
The concept of antinociceptive pain modulation deserves addi-tional attention. Though reasonable, it is currently unknownwhether efficacy of pain prevention, such as in migraine, dependson achievement of an antinociceptive modulation profile, and con-sequently whether testing for PMP should become a tool to assessefficacy of preventive treatment. Further, the notion should beentertained that achieving an antinociceptive PMP should be thetarget of pain therapy for patients with ongoing pain because itmay indicate a more radical change in the pain perceiving sys-tem—and possibly one of longer durability—than the standard,more fragile target of pain reduction.
Conflict of interest
D.Y. received honoraria from speakers’ bureau of Grunenthaland Pfizer, and an IIT grant from Eli Lilly. The other authors reportno conflict of interest.
References
[1] Arendt-Nielsen L, Nie H, Laursen MB, Laursen BS, Madeleine P, Simonsen OH,Graven-Nielsen T. Sensitization in patients with painful knee osteoarthritis.PAIN� 2010;149:573–81.
[2] Chang L. Brain responses to visceral and somatic stimuli in irritable bowelsyndrome: a central nervous system disorder? Gastroenterol Clin North Am2005;34:271–9.
[3] Daenen L, Nijs J, Roussel N, Wouters K, Van Loo M, Cras P. Dysfunctional paininhibition in patients with chronic whiplash-associated disorders: anexperimental study. Clin Rheumatol 2013;32:23–31.
[4] Edwards RR, Mensing G, Cahalan C, Greenbaum S, Narang S, Belfer I, SchreiberKL, Campbell C, Wasan AD, Jamison RN. Alteration in pain modulation inwomen with persistent pain after lumpectomy: influence of catastrophizing. JPain Symptom Manage 2013;46:30–42.
[5] Goodin BR, McGuire L, Allshouse M, Stapleton L, Haythornthwaite JA, Burns N,Mayes LA, Edwards RR. Associations between catastrophizing and endogenouspain-inhibitory processes: sex differences. J Pain 2009;10:180–90.
[6] Graven-Nielsen T, Wodehouse T, Langford RM, Arendt-Nielsen L, Kidd BL.Normalization of widespread hyperesthesia and facilitated spatial summationof deep-tissue pain in knee osteoarthritis patients after knee replacement.Arthritis Rheum 2012;64:2907–16.
[7] Kosek E, Hansson P. Modulatory influence on somatosensory perception fromvibration and heterotopic noxious conditioning stimulation (HNCS) infibromyalgia and healthy subjects. PAIN� 1997;70:41–51.
[8] Kosek E, Ordeberg G. Lack of pressure pain modulation by heterotopic noxiousconditioning stimulation in patients with painful osteoarthritis before, but notfollowing, surgical pain relief. PAIN� 2000;88:69–78.
[9] Landau R, Kraft JC, Flint LY, Carvalho B, Richebé P, Cardoso M, Lavand’homme P,Granot M, Yarnitsky D, Cahana A. An experimental paradigm for the predictionof post-operative pain (PPOP). J Vis Exp 2010;27.
[10] Lautenbacher S, Rollman GB. Possible deficiencies of pain modulation infibromyalgia. Clin J Pain 1997;13:189–96.
[11] Lavand’homme P, Roelants F. Effect of a low dose of ketamine on postoperativepain after elective Cesarean delivery according to the presence of apreoperative temporal summation. SOAP 2009;A-258.
[12] Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls(DNIC). II. Lack of effect on non-convergent neurones, supraspinal involvementand theoretical implications. PAIN� 1979;6:305–27.
[13] Lewis GN, Rice DA, McNair PJ. Conditioned pain modulation in populations withchronic pain: a systematic review and meta-analysis. J Pain 2012;13:936–44.
[14] Maixner W, Fillingim R, Booker D, Sigurdsson A. Sensitivity of patients withpainful temporomandibular disorders to experimentally evoked pain. PAIN�
in children with complex regional pain syndromes: a double blind placebo-controlled crossover trial. Anesthesiology 2009;111:372–80.
[16] Niesters M, Aarts L, Sarton E, Dahan A. Influence of ketamine and morphine ondescending pain modulation in chronic pain patients: a randomized placebo-controlled cross-over proof-of-concept study. Br J Anaesth 2013;110:1010–6.
[17] Perrotta A, Serrao M, Ambrosini A, Bolla M, Coppola G, Sandrini G, Pierelli F.Facilitated temporal processing of pain and defective supraspinal control ofpain in cluster headache. PAIN� 2013;154:1325–32.
[18] Pielsticker A, Haag G, Zaudig M, Lautenbacher S. Impairment of pain inhibitionin chronic tension-type headache. PAIN� 2005;118:215–23.
[19] Price DD, Hayes RL, Ruda M, Dubner R. Neural representation of cutaneousaftersensations by spinothalamic tract neurons. Fed Proc 1978;37:2237–9.
[20] Price DD, Staud R. Neurobiology of fibromyalgia syndrome [review]. JRheumatol Suppl 2005;75:22–8.
[21] Pud D, Granovsky Y, Yarnitsky D. The methodology of experimentally induceddiffuse noxious inhibitory control (DNIC)-like effect in humans. PAIN�
2009;144:16–9.[22] Sandrini G, Rossi P, Milanov I, Serrao M, Cecchini AP, Nappi G. Abnormal
modulatory influence of diffuse noxious inhibitory controls in migraine andchronic tension-type headache patients. Cephalalgia 2006;26:782–9.
[23] Sarlani E, Grace EG, Reynolds MA, Greenspan JD. Evidence for up-regulatedcentral nociceptive processing in patients with masticatory myofascial pain. JOrofac Pain 2004;18:41–55.
[24] Terry EL, Kerr KL, DelVentura JL, Rhudy JL. Anxiety sensitivity does not enhancepain signaling at the spinal level. Clin J Pain 2012;28:505–10.
[25] Weissman-Fogel I, Sprecher E, Granovsky Y, Yarnitsky D. Repeated noxiousstimulation of the skin enhances cutaneous pain perception of migrainepatients in-between attacks: clinical evidence for continuous sub-thresholdincrease in membrane excitability of central trigeminovascular neurons.PAIN� 2003;104:693–700.
[26] Wilder-Smith OH, Schreyer T, Scheffer GJ, Arendt-Nielsen L. Patients withchronic pain after abdominal surgery show less preoperative endogenous paininhibition and more postoperative hyperalgesia: a pilot study. J Pain PalliatCare Pharmacother 2010;24:119–28.
[27] Yarnitsky D, Crispel Y, Eisenberg E, Granovsky Y, Ben-Nun A, Sprecher E, BestLA, Granot M. Prediction of chronic post-operative pain: pre-operative DNICtesting identifies patients at risk. PAIN� 2008;138:22–8.
[28] Yarnitsky D, Arendt-Nielsen L, Bouhassira D, Edwards RR, Fillingim RB, GranotM, Hansson P, Lautenbacher S, Marchand S, Wilder-Smith O.Recommendations on terminology and practice of psychophysical DNICtesting. Eur J Pain 2010;14:339.
[29] Yarnitsky D, Granot M, Nahman-Averbuch H, Khamaisi M, Granovsky Y.Conditioned pain modulation predicts duloxetine efficacy in painful diabeticneuropathy. PAIN� 2012;153:1193–8.
















![[McConnell Therapy Versus Coumans Bandage for Patellofemoral Pain] [Dutch]](https://static.documents.pub/doc/80x56/55cf99b0550346d0339eabdd/mcconnell-therapy-versus-coumans-bandage-for-patellofemoral-pain-dutch.jpg)


