Dr Richard Harding Department of Palliative Care, Policy and Rehabilitation King’s College London, England Richard A. Powell, Fatia Kiyange, Dr Julia Downing, Dr Faith Mwangi-Powell African Palliative Care Association Uganda January 2007 PAIN RELIEVING DRUGS IN 12 AFRICAN PEPFAR COUNTRIES: Mapping current providers, identifying current challenges, and enabling expansion of pain control provision in the management of HIV/AIDS
Transcript
Dr Richard HardingDepartment of Palliative Care, Policy and RehabilitationKing’s College London, England
Richard A. Powell, Fatia Kiyange, Dr Julia Downing, Dr Faith Mwangi-PowellAfrican Palliative Care AssociationUganda
January 2007
PAIN RELIEVINGDRUGS IN 12AFRICAN PEPFARCOUNTRIES:Mapping current providers, identifying current challenges, and enablingexpansion of pain control provision in the management of HIV/AIDS
We are grateful to Presidents Emergency Plan forAIDS Relief for funding this study, to the members of the US Office of the Global Co-ordinator andMembers of the USG Palliative Care TechnicalWorking Group who gave useful input andcomments on protocol drafts, and to all the sitesand INCB competent authorities that participated.
Background 7Defining palliative care 7The holistic nature of palliative care 7Palliative care in Sub-Saharan Africa 7Opioid availability 8Barriers to opioid availability 9
Study aim 10Study objectives 10Study design 10
Methods 10Procedure 10Recruitment and data collection 10Survey items 11Data processing and analysis 11
Results 11Palliative care sites 11
Site sample characteristics 11Disease groupings served and antiretroviral therapy provision 13Number of adult and child patients seen 14Clinical staff on service 15Pain and symptom control prescribing and dispensing 16Government, country and policy context 18Opioid training, expanding access and current challenges 22Current challenges: purchasing, producing, dispensing and prescribing 26
INCB competent authority data 29Respondents 29Current opioid supply and regulatory system 29Comparison to site responses 31
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 1
TABLE OF CONTENTS
Discussion 32Definitions and components of palliative care 32Antiretroviral therapy 32Patient population 32Staff skills 32Analgesia and symptom controlling drug availability 33The service perspective on opioid access: factors hampering provision, expanding access and facingchallenges 33
The INCB and Provider data: common goals and disparate perspectives 35Advocacy for greater access 35Drug availability: INCB and site views 35Limitations 35Conclusion 36Recommendations 36
Department of Palliative Care, Policy and Rehabilitation, King’s College London 40
African Palliative Care Association 41
References 42
Appendix 1 APCA's Tool for the Classification of Palliative Care Activities 43
Figure 1 The WHO Pain Ladder 8
Figure 2 Challenges and responses: data integration 34
Table 1 Country of respondents 11
Table 2 Category of care site and components of service delivered 12
Table 3 Sites of care 13
Table 4 Disease groupings and antiretroviral therapy 14
Table 5 Number of patients seen per year 14
Table 6 Clinical staff mix and opioid-prescribing staff 15
Table 7 Analgesics prescribed, dispensed and supply continuity 16
Table 8 Opioid sources 17
Table 9 Symptom control drugs prescribed, dispensed and supply continuity 17
Table 10 Opioids, essential drug lists and legal requirements 19
Table 11 Opportunities and challenges: expanding opioid provision 23
Table 12 Current issues in opioid provision 27
Table 13 INCB views: current opioid supply and regulation 30
Table 14 Comparison of INCB and provider data: opioid availability 31
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 2
TABLE OF CONTENTS
Rationale
1) Pain is a significant and distressing problemexperienced by people living with HIV/AIDS. In order to adhere to the World HealthOrganisation’s (WHO) pain ladder, it is essentialthat HIV care providers can access opioidanalgesia for their patients. Although palliativecare is defined by its multidimensional focus onphysical, emotional and spiritual pain, the lackof access to opioids in Sub-Saharan Africa hasbeen identified as a major challenge. This studyaimed to identify current opioid prescribingservices and regulatory bodies within 12PEPFAR countries, and to describe barriers to,and potential for, expansion in the number ofopioid providers, for people with HIV/AIDS.
Methods
2) A cross sectional survey questionnaire wasdistributed to palliative care sites in 12countries, and a telephone interview conductedwith International Narcotics Control Board(INCB) competent authorities in each. The datawere analyzed and integrated to identifypotential strategies for opioid expansion.
Main findings Site configuration and activity
3) The majority of the sample (56.4%) were‘integrated’ Non-Governmental Organisations(NGOs) offering a range of HIV services,including a component of palliative care. These services focused on general counseling,family/community education, food parcels/grants/income generation, HIV prevention andtesting. The palliative-only services (35.5%, e.g.hospices) stressed bereavement counseling,family support, spiritual care, professionaleducation and advocacy.
4) All sites concurred with the WHO definition ofpalliative care, with no deviations or adaptations.
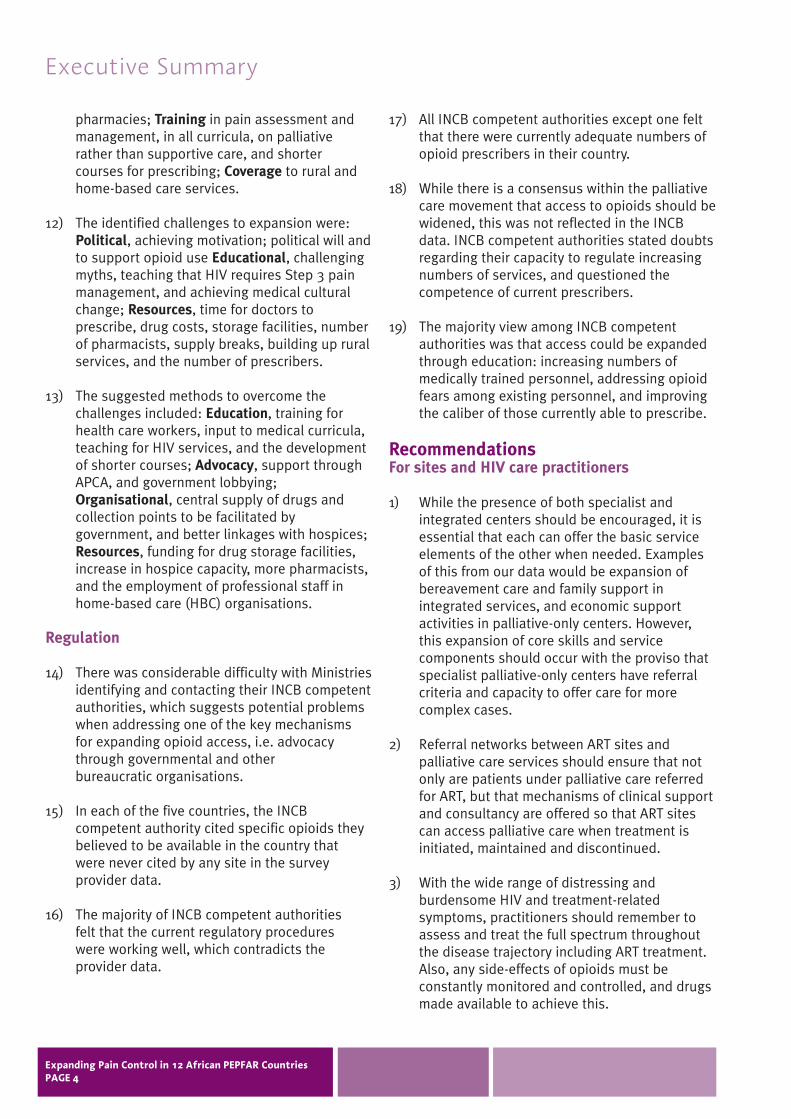
5) Although palliative care should be offeredalongside antiretroviral therapy (ART), only 11sites (17.7%) were ART providers, and 5 (8.1%)had no local access at all, the remaining 40(64.5%) having nearby provider access for their patients.
6) Palliative-only services cared for significantlyfewer patients per year than did the integratedNGOs and were significantly more likely toprescribe opioids to both adult and childpatients while under their care.
7) Comparing palliative-only to integratedservices, there was no significant difference inthe number of clinical staff, nor in theproportion of staff able to prescribe opioids.However, the palliative-only services had asignificantly higher proportion of clinical stafftrained in palliative care.
Opioids
8) 36 sites (58.1%) were currently dispensingopioids. Less than constant supply of analgesiawas reported by sites at all three levels of theWHO Pain Ladder. Seven sites reported lessthan constant supply of Step 1 analgesics.
9) 18 sites did not report access to an agent forthe management of neuropathic pain, acommon symptom of HIV disease and an ARTside-effect. Again, there were breakages in thesupply of antiemetics (11 sites), anxiolytics (7sites) and neuropathic pain treatments (7 sites).
10) The common factors hampering opioidprovision were: Supply (e.g. central stores notstocking adequately, overly tight control,unreliable stocks, few dispensers); Legislation(e.g. regulations, lack of national policy onopioid use, bureaucratic processes); Education(e.g. existing clinicians do not know how toassess and treat pain, fear of addiction, poorpatient compliance, palliative care stresses itsspecialty to the point of exclusion, doctors lackinterest in dying patients); Practical (e.g. costs,storage requirements, not enough prescribers,unqualified staff in home-based care, poorinfrastructure to follow discharged patientshome, lack of sugar for making up syrup, andshort shelf-life of morphine).
11) Responses suggesting mechanisms to assistmore providers to access opioids: Advocacy atgovernmental and public levels on the need foropioids, and on lifting restrictive legislation;Collaboration with prescribing doctors, acrossprimary and secondary care, with hospital
Executive Summary
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 3
pharmacies; Training in pain assessment andmanagement, in all curricula, on palliativerather than supportive care, and shortercourses for prescribing; Coverage to rural andhome-based care services.
12) The identified challenges to expansion were:Political, achieving motivation; political will andto support opioid use Educational, challengingmyths, teaching that HIV requires Step 3 painmanagement, and achieving medical culturalchange; Resources, time for doctors toprescribe, drug costs, storage facilities, numberof pharmacists, supply breaks, building up ruralservices, and the number of prescribers.
13) The suggested methods to overcome thechallenges included: Education, training forhealth care workers, input to medical curricula,teaching for HIV services, and the developmentof shorter courses; Advocacy, support throughAPCA, and government lobbying;Organisational, central supply of drugs andcollection points to be facilitated bygovernment, and better linkages with hospices;Resources, funding for drug storage facilities,increase in hospice capacity, more pharmacists,and the employment of professional staff inhome-based care (HBC) organisations.
Regulation
14) There was considerable difficulty with Ministriesidentifying and contacting their INCB competentauthorities, which suggests potential problemswhen addressing one of the key mechanisms for expanding opioid access, i.e. advocacythrough governmental and other bureaucratic organisations.
15) In each of the five countries, the INCBcompetent authority cited specific opioids theybelieved to be available in the country that were never cited by any site in the surveyprovider data.
16) The majority of INCB competent authorities felt that the current regulatory procedures were working well, which contradicts theprovider data.
17) All INCB competent authorities except one feltthat there were currently adequate numbers ofopioid prescribers in their country.
18) While there is a consensus within the palliativecare movement that access to opioids should bewidened, this was not reflected in the INCBdata. INCB competent authorities stated doubtsregarding their capacity to regulate increasingnumbers of services, and questioned thecompetence of current prescribers.
19) The majority view among INCB competentauthorities was that access could be expandedthrough education: increasing numbers ofmedically trained personnel, addressing opioidfears among existing personnel, and improvingthe caliber of those currently able to prescribe.
Recommendations For sites and HIV care practitioners
1) While the presence of both specialist andintegrated centers should be encouraged, it isessential that each can offer the basic serviceelements of the other when needed. Examplesof this from our data would be expansion ofbereavement care and family support inintegrated services, and economic supportactivities in palliative-only centers. However,this expansion of core skills and servicecomponents should occur with the proviso thatspecialist palliative-only centers have referralcriteria and capacity to offer care for morecomplex cases.
2) Referral networks between ART sites andpalliative care services should ensure that notonly are patients under palliative care referredfor ART, but that mechanisms of clinical supportand consultancy are offered so that ART sitescan access palliative care when treatment isinitiated, maintained and discontinued.
3) With the wide range of distressing andburdensome HIV and treatment-relatedsymptoms, practitioners should remember toassess and treat the full spectrum throughoutthe disease trajectory including ART treatment.Also, any side-effects of opioids must beconstantly monitored and controlled, and drugsmade available to achieve this.
Executive Summary
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 4
4) Where opioid access is poor, networks shouldbe established with current hospice andgovernmental providers to establish routes for dispensing.
5) Rural and HBC services should consider theirpotential routes to palliative care drugs whenarranging palliative care training for their staff,as spiritual and emotional pain cannot beoptimally managed without the control ofphysical pain.
For educators
6) All services, whether palliative-only, integratedNGO or government facilities, must ensure thatall clinical staff are trained in palliative care to abasic agreed level. This would assist staff toassess palliative care needs, to provide generalpalliative care, and be aware of when to makeappropriate referrals for specialist input.
7) Training and education providers should formcollaborative teaching activities with currentclinicians. Those in practice require ongoingprofessional education to improve the paincontrol of those living with HIV, and to meet theneeds of the dying.
8) Training and education providers should formcollaborative teaching activities with futureclinicians. The inclusion of palliative care inmedical school curricula should be a goal for all countries.
9) Education must take a long-term view of theprocess of teaching, and mechanisms put inplace to ensure follow-up to support theapplication of skills learned.
10) Shorter palliative care courses that focus on prescribing should be considered for current clinicians.
11) Educators need to redouble efforts to addressthe public fears of opioids. A potential means toachieve this may be through the existingsignificant global networks for HIV advocacygroups such as ICW and GNP. Currently theissues of palliative care and opioid use are notcampaigning issues by advocacy groups ofpeople living with HIV/AIDS.
12) There may be educational opportunities to work with INCB competent authorities todemonstrate the successes of opioid use andthe current limitations that could be addressed.Such consultation may also offer INCBcompetent authorities an opportunity to sharetheir concerns. Interactive education andsharing of viewpoints may offer better potentialfor feasible and acceptable strategies for opioid expansion.
For funders
13) Funders must take account of the high burdenof pain and symptoms that affect quality of life and allocate resources to ensure that these manageable problems are adequatelycontrolled.
14) Patients should have local access toantiretroviral therapy at all services that offerpalliation whatever disease stage the servicefocuses on. Referral and co-management care pathways should be in place to ensure that even if palliative care and therapy are not available at the same site, they are co-ordinated to ensure that they can beintegrated across services.
15) Currently, palliative-only services see fewerpatients. While not all people living with anincurable life-limiting disease should requirespecialist palliative care, and not all people atthe end of life should or could access hospicecare, resources are required to increase thecapacity of these institutions to enhance theireducative, advocacy and specialist role forcomplex case management.
16) Funding for clinically trained staff is essential inHBC HIV sites, as opioids cannot be utilizedwithout staff able to prescribe.
17) Funders should consider the structuralrequirements of sites, e.g. the essential currentproblems of adequate opioid storage facilitiesand pharmacy facilities, in addition to staff andtraining costs.
18) Funders should consider those analgesicsbeyond opioids, i.e. neuropathic pain agents,which are essential for pain that often cannotbe controlled with opioids.
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 5
For policy makers and regulators
19) The current opioid (and non-opioid) drug supplysystems experience a number of blockages anduncertainty in supply. Any expansion willrequire identification of the strongest routes,and to strengthen these further, beforeexpanded drug supply can be achieved.
20) The emphasis on expanding opioid supply isbeing pursued to enhance adherence to theWHO pain ladder. It is clear from the data thatthis requires attention at all steps of the ladder,including in some cases provision of Step 1pain-relieving drugs.
21) Policies to expand opioid access must carefullybalance the need for expansion with the threatof additional pressure on unreliable currentpurchase, production and dispensing.Expansion should not be at the cost of reliability to existing providers.
22) Any strategy for expansion must take account of the concerns of INCB competent authoritieswith respect to regulation. Advocacy andlobbying must convince this essentialstakeholder group of the feasibility ofexpansion programs, as current INCBskepticism may prove a significant barrier.INCB’s need adequate resources to monitor and support existing and new opioid providers.
23) The synergies of strengthening supply systems for opioids can also enhance othersymptom-controlling drugs, such as antiemeticsand anxiolytics, which are also essential for this population.
24) Any strategic approach to opioid expansionmust use a multi-pronged approach takingaccount of: supply (e.g. ordering and stocking, consistency of availability), legislation(e.g. regulations on storage and prescribing),education (i.e. ensuring that opioids are usedappropriately) and practical site-specificsupport (e.g. adequate numbers of trained and able-to-prescribe staff, funds and storagefacilities). Failure to address each of these areasis unlikely to achieve sustainable success.
25) Each country should undertake a wide-rangingconsultation process to appraise its currentlegislation and identify the potential to pilot and test safe, feasible and practical legislationfor the prescribing and dispensing of opioids.
26) Policy change, across the legislative andregulatory settings, can only be achievedthrough co-ordinated advocacy that takesaccount of governmental disinterest andprofessionals’ fears of opioid use.
27) Current funding goals to increase the numbersof patients accessing palliative care should takeaccount of the current limitations on opioid useand supply, and address the likely pressure onexisting infrastructure.
28) In order to address the current weaknesses insupply, and build capacity for expansion,greater emphasis and capacity needs to beplaced on training and employing pharmacists.
For researchers
29) In the light of different models of care andnumbers of trained staff and patients seenaccording to service model, multidimensionaloutcome evaluations are required, includingmeasurement of pain and symptom control.
30) Evaluative studies should compare botheconomic costing and levels of analgesiaavailable, taking account of comparativebaseline patient need across models.
31) Referral criteria and care networks should beexamined to understand the movementbetween sites as patients move up and downthe pain ladder.
32) All strategies and programs to expand opioiduse should be evaluated at the site/countrylevel to ensure that lessons can bereplicated/adapted for use in other sites.
33) Longitudinal evaluation of education forinitiatives in opioid use should be conducted to measure practice outcomes.
Executive Summary
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 6
Defining palliative care
The World Health Organisation (WHO) describes the goal of palliative care as aiming to improve:
‘the quality of life of patients and families who face life-threatening illness, by providing pain and symptom relief, spiritual and psychosocialsupport from diagnosis to the end of life andbereavement’. (1)
The holistic nature of palliative care
As demonstrated above by the WHO definition,palliative care is concerned with pain in all itsmanifestations among patients and families affectedby life-limiting incurable disease. This embracesphysical, emotional and spiritual pain (13). Palliativecare can only be said to be present if this ‘total care’package is evident in whatever format is feasible and appropriate in the local setting. Pain controlwithout good psychosocial care may be termedanesthesiology; psychosocial care without adequatepain control is supportive care. This study focusedon the physical pain control tasks of palliative careas this component has been identified as a particularchallenge in the African context. However, werecognize that there is equally important research tobe undertaken into the provision of control ofemotional and spiritual pain, and family support aswell as distressing symptoms other than pain, and in training initiatives.
Why do we need PC as we roll out access toantiretrovirals?
Although palliative care is based on a multi-disciplinary family-based approach to care andsupport, the defining feature of palliative care thatdistinguishes it from supportive care is the elementof pain and symptom control. Given that pain isexperienced throughout the HIV disease trajectoryfrom the point of diagnosis (2), and that severe painis experienced by approximately 80% of those withadvanced HIV disease at the end of life (3), palliativecare has been advocated by the WHO as:
‘an essential component of a comprehensive HIVcare package because of the variety of symptomsthey can experience – such as pain, diarrhea, cough,shortness of breath, nausea, weakness, fatigue,fever, and confusion. Palliative care is an important
means of relieving symptoms that result in unduesuffering and frequent visits to the hospital or clinic.Lack of palliative care results in untreated symptomsthat hamper an individual’s ability to continue his orher activities of daily life. At the community level,lack of palliative care places an unnecessary burdenon hospital or clinic resources.’ (4)
A recent systematic review of patient outcomes inHIV palliative care found significant improvements in pain and symptom control, anxiety and patientinsight (6).
Palliative care in Sub-Saharan Africa
To achieve adequate patient care, the WHOrecommends a three-part strategy for developing acancer pain relief program (7). This strategy can betransferred to other life-limiting illnesses, includingpain management for HIV/AIDS. The three step-strategy states:
(a) Government policy – the national governmenthealth and regulatory authorities shouldestablish and support a policy that makes painrelief a high priority in the health care system;
(b) Education/training – the public, policymakers,and regulators should be informed that pain can be relieved, and health care professionalsshould be trained to manage pain using thethree-step ladder; and
(c) Drug availability – analgesics, including opioidssuch as morphine, should be made available.
Current provision of palliative care in Africa is patchyand is often thought to be provided from centers ofexcellence rather than integrated into the health care system. Home-based care (HBC) (the primemodality of African HIV care provision) has beencriticized for the often inadequate pain controlclinical skills and use of appropriate pain-controllingdrugs (5). A current challenge to improve patientoutcomes is to disseminate lessons learned by thosewho have pioneered palliative care and to balanceexpansion of coverage with quality (8).
Providers of end-of-life care have identified paincontrol availability as a primary challenge (9). The need for adequate pain control will increase asantiretroviral therapy is rolled out across the region,
Background
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 7
because side effects can be highly prevalent andburdensome (10) and need to be managed toenhance adherence, while the emergence of otherlife-limiting co-morbidities require palliative therapyas the chronic disease phase increases in length (11) (12).
The growth of awareness of the need to expandpalliative care in Sub-Saharan Africa, and increasingavailability of funds available, have been majordevelopments in patient care in recent years.Increasing numbers of HIV care providers aredemanding to acquire palliative care skills, and themeans to support this growth need to be identified.
Opioid availability
Opioids are essential for the management of severepain, and can effectively control the vast majority ofpain presented. It is not possible to control the rangepain intensity in the clinical care setting withoutaccess to the Pain Ladder, i.e. drugs fromparacetamol to codeine to morphine. The WHOExpert Drug Committee on essential drugs hasdesignated morphine, codeine and other opioids as essential drugs, defined as those that satisfy thehealth care needs of majority of the population, that should therefore be available at all times inadequate amounts and in appropriate dosages. Oral opioid analgesics such as codeine, fentanyl,hydromorphone, morphine, and oxycodone areconsidered to be the cornerstone of good painmanagement. Drugs from these classes of analgesicmust be made available for medical use if acomprehensive palliative care program is to succeed. According to the WHO pain ladder, opioids must beavailable to manage pain in patients whose pain has not been adequately controlled by the use ofnon-opioids, weak opioids and the addition ofadjuvants (see Figure 1). In addition, it is requiredthat opioids are delivered:
‘by the ladder’, i.e. according to Figure 1
‘by the clock’, i.e. titrated for consumption atregular intervals to avoid the unnecessary anddistressing experience of breakthrough pain
‘by the mouth’, i.e. oral morphine for simple selfadministration in the home setting, and absorbedto avoid peaks in the analgesia levels.
These drugs have, however, proved extremelydifficult to obtain in many African countries.Although in theory many countries permitimportation and distribution of the drugs, it can beimpossible in practice to obtain the necessaryauthority from regulating bodies to prescribe thesedrugs. Indeed, the International Narcotics ControlBoard (INCB, the global authority which monitors thecontrol and supply of narcotics) found that one ofthe biggest obstacles to the use of opioids was thefear among health professionals of legal action thatmight be taken against them if they prescribed these drugs.
There is little or no use of morphine in nearly half ofthe countries in the world. Almost all morphine isconsumed in developed countries. Indeed, in manyparts of Africa, there is limited availability of evensimple pain-relieving drugs. Opioids in countries likeKenya, Malawi and Zambia are only accessible orimported within very tight regulatory frameworks.Since access to appropriate medication for pain
Background
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 8
Pain 3
STEP ONENonopioid with or without adjuvant
STEP TWOWeak opioid with or
without nonopioid,adjuvant
STEP THREEStrong opioid with or
without nonopioid,adjuvant
Pain persisting or increasing 3
Pain persisting or increasing 3
Freedom from cancer pain 5
relief and opportunistic infections is central topalliative care, identifying the means to increase thenumbers of HIV care providers who can offeradequate pain relieving drugs, and have thenecessary palliative care skills, is a key stage inscaling-up palliative care in the region.
Barriers to opioid availability
International health and drug regulatory authorities have recognized that opioid analgesicsare not sufficiently available for the treatment ofpain in many places throughout the world. The INCB has asked all countries to take thenecessary steps to assure that opioids are available for pain management.
A number of economic and historic factors contribute to the current lack of oral opioidavailability. Many countries do not have theresources and health care infrastructure to produce and distribute medicines. Traditionally, the treatment of pain has not been as high a priority as the treatment of disease. Injectablemorphine has long been recognized as a potentanalgesic, but the broader realization that oralmorphine is also very effective is more recent.Although the international narcotics control treatyhas recognized for many years that opioids areindispensable in the management of pain, somecountries have drug legislation that prohibits orrestricts the availability and medical use of opioids.In addition, misunderstanding and fear of addictionimpede the rational use of opioids in pain reliefthroughout the world.
The global barriers to opioid availability can besummarized as:
Stringent and outdated laws and regulations forimportation of opioids.
Bureaucracy involved in obtaining authority fromregulating bodies to prescribe drugs.
Fear of addiction to opioids among healthprofessionals.
Poor or no health infrastructures.
Cultural attitudes that make pain relief less of a priority.
Ignorance of the availability and potency of oralmorphine, although the potency of injectablemorphine is known.
Inadequate numbers of properly trained staff toasses and treat pain.
Inadequate resource allocation of medications.
Low funder priority for pain and symptom control.
Lack of training in paediatric palliative care, and lack of availability of drug formulations for children.
Symptoms other than pain
People living with HIV disease experience a range of symptoms beyond pain, and these can be verydistressing and may appear to clinicians to beuntreatable. These symptoms can appear early in the disease trajectory, and may also be a result oftreatment. Symptoms can include diarrhea,rash/itching, anxiety and depression, sexualdysfunction, and fatigue 1-5 6. Therefore, it isessential that clinicians are able to assess and treatthe full range of symptoms, which includes havingaccess to symptom controlling drugs.
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 9
This study aimed to identify current opioidprescribing services and regulatory bodies within 12African PEPFAR (Presidents Emergency Plan for AIDSRelief ) countries, and to examine the barriers to, andappraise the potential for, expansion in the numberof opioid providers, for people with HIV/AIDSaccording to the WHO pain ladder.
Study objectives
The three study objectives were:
1. To identify the policy and practice context, and the necessary steps for providers toincorporate step 3 analgesics prescribing in 12 PEPFAR countries.
2. To identify current challenges, practice andopioid supply issues, and practical steps forexpanding the number of palliative careproviders in the 12 PEPFAR countries.
3. To describe the country context of opioidprescribing, the current opportunities andblockages in opioid prescribing, and identifysteps that services in the 12 countries can taketo integrate palliative pain control into theirexisting HIV care services.
Study design
The study utilized a cross-sectional surveymethodology, collecting data from palliative care providers and INCB competent authorities,integrating and comparing findings at the country and continent levels.
Procedure
The study population was defined as servicescurrently in operation defined by the AfricanPalliative Care Association (APCA) as a palliative care service. A clear definitional framework wasutilized (see Appendix 1), with any service thatoperated at Levels 2, 3 or 4 included. Therefore,according to the APCA classification, the minimumservice package that met the inclusion criteria wasuse of health care professionals as well ascommunity health workers, and delivery of clinicaland supportive opportunistic infection management,and at least Step 1 analgesics.
Recruitment and data collection
A comprehensive list of potential palliative careservice providers was compiled from:
The APCA contact list.
The International Observatory, University of Lancaster.
USG representatives and their partners.
The Hospice Africa Uganda Distance LearningDiploma and other contacts.
University of Cape Town MSc in Palliative Care.
Mildmay Uganda contacts from their training courses.
Further contacts proposed by the project’sSteering Group members.
All services identified as meeting the study inclusion criteria were contacted initially by email.The questionnaire was formatted electronically andattached to the mailing. Contact details wereidentified for services without electronic contactdetails and these were telephoned. Hard copies wereprinted and posted to those without access to emailfacilities, and hard copies delivered by hand to thoseservices that were visited by the APCA team duringthe period of data collection.
The INCB competent authorities were identifiedthrough each country’s Department of Health andcontacted by telephone to ask for participation.
Study Aim Methods
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 10
Where telephone appointments were refused, thesurvey was sent electronically for self-completion.
Reminder emails and telephone calls were made tonon-responders periodically throughout the datacollection period, which ran for a period of 8 monthsfrom August 2005-March 2006.
Survey items
For the provider survey, the items addressed theiroperational definition of palliative care, servicecomponents and activity, ARV use, health careprofessional staffing, analgesia and symptom control prescribing and dispensing, the nationallegislative framework for opioid use, and challengesto opioid provision.
INCB competent authorities questions investigatedopioid availability, essential drug lists, legislativerestrictions, and current challenges.
Data processing and analysis
Data were entered into SPSS V.12® for cleaning,checking and analysis. To ensure the anonymity andconfidentiality of responding services, the codeddata was subjected to restricted access; completedquestionnaires were stored in a secure location.
The inputted data were subjected to profilingdescriptive statistics, and inferential statistics, inparticular, the Chi-square (x2) test for categoricaldata, and the t-test and the ANOVA for continuousdata to determine statistically significant differences.Where open-ended questions had been asked, post-hoc coding frames were developed to presentdata thematically.
Palliative care sites
Site sample characteristics Sixty-two sites participated, a response rate of 61%,with responses broken down by country as follows:
The sites categorized themselves as either 1) a palliative care-only service (e.g. Hospice), 2) a non-governmental organisation (NGO) offering anumber of services including palliative care (i.e.integrated care), 3) or as a Governmental service(e.g. Hospital or clinic). In addition, they were askedto list the main service components that theyprovide, which are presented in Table 2 overleafaccording to category of service. In addition,participants described their sites of care (Table 3).
Responding sites were required to categorisethemselves as 1 of the following:
1) A palliative care-only service – These servicescan be characterized as providing solelyspecialist palliative care. The most commonexample of this is the Hospice (which mayprovide home, daycare and inpatient care),although there are other specialist palliativecare teams, for example those based inhospitals offering consultancy.
2) An NGO offering a number of services includingpalliative care – These services can becharacterized as providing a range of HIV careservices of which one is palliative care althoughthis is usually integrated throughout the
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 11
services offered. Therefore, the service is likelyto offer care from the point of diagnosis.
3) A governmental service – These services can becharacterized as primary or secondary and formpart of the state facility network.
Table 2 Components of care described by sites
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 12
Category of site:
Number of services in category
Service components (no. of times mentioned)
Palliative care only (e.g. Hospice)
n=22 (35.5%)
Bereavement counseling 11
Counseling 5
Family/communityeducation 5
Family planning 0
Family support 4
Food parcels & grants 6
HIV testing 1
Hospice mentoring 1
Income generation 1
Nutrition support 0
Orphan care 9
Pain & symptom control 4
Palliative care advocacy 5
Primary prevention 1
Professional Education & Training 10
Psychosocial support 3
Rehabilitation 1
Resource centre 1
Respite 1
Social work 2
Spiritual care 4
Terminal care 3
Non-Governmental careprovider offering morethan palliative care
n=35 (56.4%)
Bereavement counseling 6
Counseling 14
Family/communityeducation 10
Family planning 1
Family support 1
Food parcels & grants 10
HIV testing 9
Hospice mentoring 0
Income generation 6
Nutrition support 5
Orphan care 15
Pain & symptom control 2
Palliative care advocacy 1
Primary prevention 6
Professional Education & Training 6
Psychosocial support 4
Rehabilitation 1
Resource centre 0
Respite 2
Social work 4
Spiritual care 3
Terminal care 1
Government servicefacility (e.g. Govt.hospital/clinic)
n=5 (8.1%)
Bereavement counseling 0
Counseling 2
Family/communityeducation 0
Family planning 0
Family support 0
Food parcels & grants 0
HIV testing 0
Hospice mentoring 0
Income generation 0
Nutrition support 0
Orphan care 0
Pain & symptom control 3
Palliative care advocacy 0
Primary prevention 0
Professional Education & Training 1
Psychosocial support 1
Rehabilitation 0
Resource centre 0
Respite 0
Social work 0
Spiritual care 1
Terminal care 0
All sites reported that they concurred with the WHO definition of palliative care, with none offering a deviation or adaptation. The data in Table 2 demonstrate different foci between theservice models:
Palliative care-only services (e.g. hospices) moreoften sited a focus on bereavement counseling,family support, spiritual care, professionaleducation and advocacy.
Integrated NGOs more often described their focuson general counseling, family/communityeducation, food parcels/grants/incomegeneration, HIV prevention and testing.
Government hospital services described servicecomponents of pain and symptom control inaddition to screening, medical, and surgical input. However, there were only five services inthis category.
Table 3 Sites of care
While the palliative-only services and integratedNGO’s were broadly similar in the sites of careprovided, the government facilities appeared to beless likely to provide home care, although the smallnumbers prevent statistical testing.
Disease groupings served and antiretroviraltherapy provision
There were observed differences in the proportionsof each category of site with respect to the diseasegroup served and provision of ART (Table 4). The majority of each service type provided care forboth HIV and cancer, and none provided care forcancer patients alone. A similar proportion ofpalliative-only and integrated services were unableto provide ART, either in-house or from other local agencies.
Excluding government facilities due to the lownumber of cells, a chi-square was not significantwhen testing for a difference in the availability ofART between palliative-only and NGO integratedservices. However, it is notable that only 11 serviceswere ART providers, and 5 had no local access at all.It is a strength that the majority (40) sites had localaccess, but it is unclear from the remit of this studywhether ART sites request palliative care support forthose initiating and maintaining therapy.
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 13
Sites of careInpatient care Home careDay careHospital consultancyOutpatient care
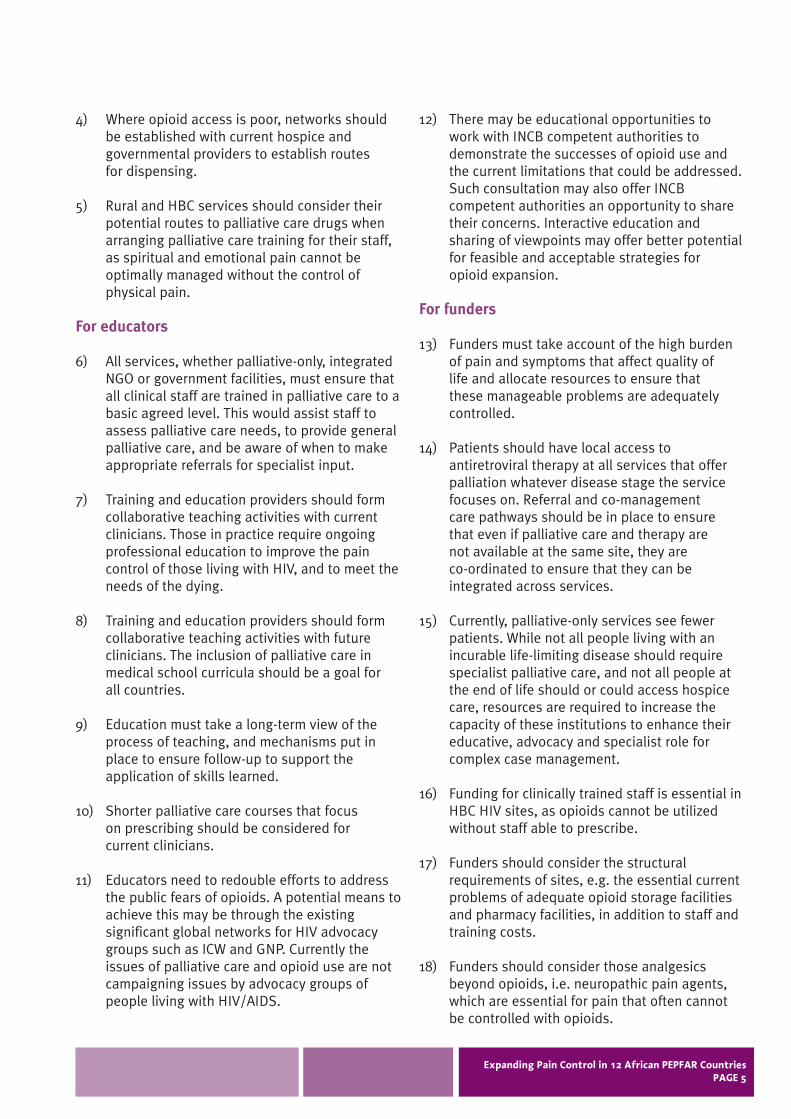
Table 5 below demonstrates that palliative care-only services provide care for a statistically smaller numberof patients per year than either integrated NGOs or governmental facilities, and that both their adult andchild patients are statistically significantly more likely to be prescribed opioids at any point under care.
Clinical staff on service
The clinical staff mix for each service category isdescribed in Table 6. To statistically compare thestaff mix, the governmental services were excludeddue to the low number of sites (i.e. N=5).
Interestingly, although the palliative-only servicessaw fewer patients (Table 5), they did not havesignificantly fewer clinical staff (no tests forcomparison of means were significant for each of the staff levels). This reflects the nature of multi-dimensional and holistic specialist care, which hasbeen shown to offer greater time per patient andfamily and is reflected in the data in Table 2, whichshows a greater focus on bereavement counseling,family support, spiritual care and education.
When the proportion of each grade of clinical staff able to prescribe opioids was compared(excluding Government facilities), there was nosignificant difference between palliative-only andintegrated services.
When the proportion of each grade of clinical stafftrained in palliative care was compared, it was foundthat palliative-only services had a significantlygreater proportion of trained nurses (68% v 45%,t=2.147 p=0.037) compared to integrated services.Therefore, comparing palliative-only to integratedservices, staff numbers and prescribing ability do notdiffer, although the proportion of nurses trained inpalliative care is higher, fewer patients are seen, andthey are more likely to be prescribed opioids in thepalliative-only services.
Table 6 Clinical staff mix and opioid-prescribing staff
A= Mean number of staff (range)B= Mean number able to prescribeC= Mean number trained in palliative care
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 15
Clinical staff:
Palliative care only(e.g. Hospice)
NGO offering morethan palliative care
Government facility(e.g. hospital/clinic)
Nurse
A B C
8.25 1.65 5.83(1-33)(0-17) (0-33)
11.53 0.45 3.53(1-110)(0-4) (0-38)
7.0 0.60 1.0(4-10) (0-2) (0-2)
Medical Officer
A B C
1.64 2.23 1.46(0-8) (0-11) (0-11)
1.33 1.30 0.70(0-13)(0-13) (0-13)
3.75 3.75 1.67(2-5) (2-5) (0-3)
Doctor
A B C
1.47 1.44 1.19(0-5) (0-5) (0-5)
0.94 0.61 0.33(0-6) (0-2) (0-2)
3.33 3.33 0.33(0-5) (0-5) (0-1)
Clinical Officer
A B C
0.73 0.44 0.50(0-3) (0-2) (0-2)
0.85 0.33 0.33(0-4) (0-4) (0-3)
1.0 1.0 0.67(0-2) (0-2) (0-1)
Pain and symptom control prescribing and dispensing
Thirty-six sites (58.1%) were currently dispensingopioids, and they were dispensed in the followingformulations: liquid (oral) n=29 (46.8%), tabletsn=20 (32.3%), injectable n=17 (27.4%). 1
The specific drugs prescribed for each step of theWHO ladder are described in Table 7. The number oftimes each drug was mentioned is listed after eachdrug name.
Of the Step 1 analgesics listed, 156/180 responsesindicated that they were dispensed onsite. Forty-twoservices indicated that Step 1 analgesics wereavailable 100 % of the time, the remaining 7 rangedfrom only 10-95 % (9 missing).
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 16
1 This question had a multiple answerformat, hence the responses do not add upto 100 percent.
Of the Step 2 analgesics, 52/73 drugs cited weredispensed onsite. Twenty-one services indicated that Step 2 analgesics were available 100 % of thetime, the remaining 7 ranged from only 10-75 % (15 missing).
Of the Step 3 analgesics, 45/69 drugs weredispensed onsite. Twenty-eight services indicatedthat Step 3 analgesics were available 100% of thetime, the remaining 7 ranged from only 5-90 % (8 missing).
Therefore, although the majority had access onsiteto Step 1 analgesics, fewer had access to Step 2 and3 analgesics. However, those that listed Step 2 alsowere likely to have Step 3.
For those who dispensed opioids, they wereobtained from the following sources:
Table 8 Opioid sources
Opioid Sources
Joint Central Medical Stores 9Government hospital 8Private pharmacy 7Pharmaceutical supplier 5Hospice 1Locally from pharmacy in powder form 1Manufacturers 1Cancer Institute 1Patients buy from outside hospital 1Import from UK 1Missing 1
TOTAL 36
The most common sources of opioid supply weregovernmental, i.e. via Joint/Central medical storesand government hospitals, with private pharmaciesthe next most common source.
The prescribed symptom control drugs are describedin Table 9.
Table 9 Symptom control drugs prescribed,dispensed and supply continuity
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 17
Of the antiemetics listed, 81/109 responses indicatedthat they were dispensed onsite. Seventy responsesindicated that the drug was available to bedispensed 100 % of the time, the remaining 32ranged from only 20-90 % (7 missing).
Of the agents listed for the management ofneuropathic pain, 68/90 of the cited drugs weredispensed onsite. Sixty-three responses indicatedthat neuropathic pain agents were available to bedispensed 100 % of the time, the remaining 20ranged from only 5-95 % (7 missing).
Of the anxiolytics listed, 51/71 drugs cited weredispensed onsite. Forty-one responses indicated thatanxioloytics were available 100 % of the time, theremaining 16 ranged from only 1-95 % (14 missing).
Government, country and policy context
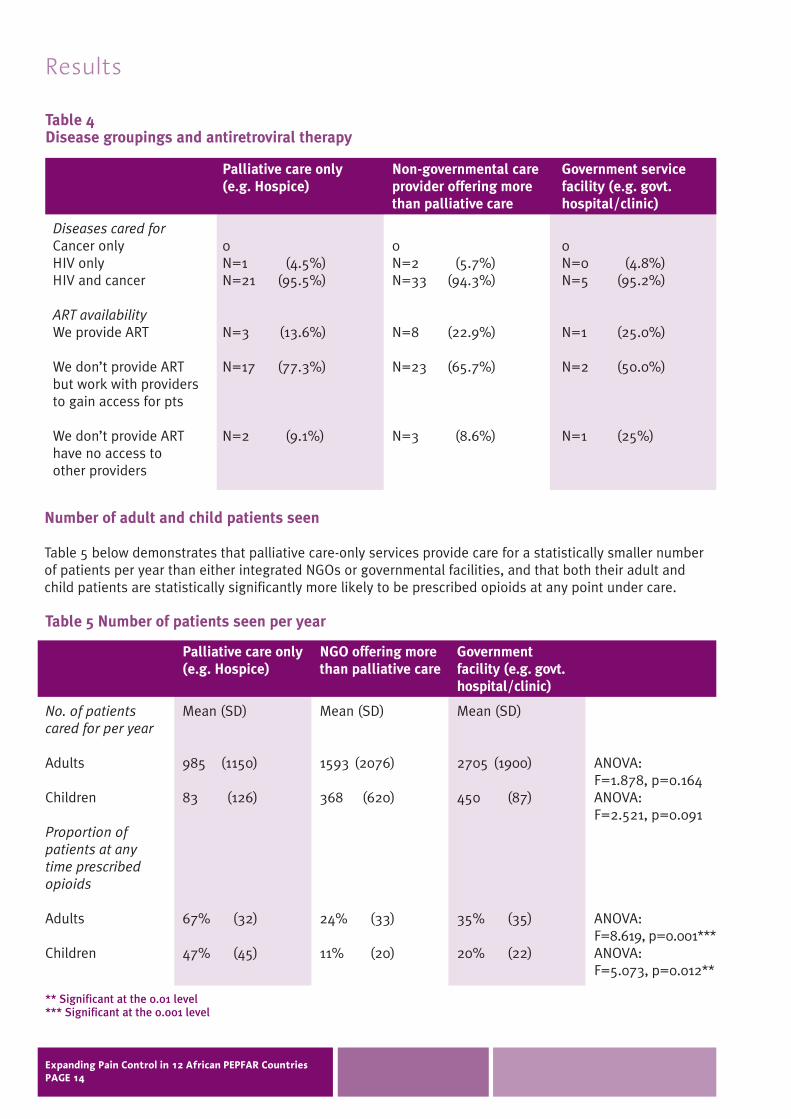
Each respondent identified whether opioids were ontheir essential drugs list. Also they were asked todescribe the legal requirements for obtaining,producing, storing and prescribing opioids, and themain factors hampering opioid provision within theircountry (see Table 10).
The data shows that, although some countries suchas Uganda have made advances in opioid provisionin comparison to others, there is a remarkablesimilarity in the identified factors hampering opioidprovision. They can be summarized as:
SupplyE.g. stores do not stock, overly tight control,unreliable stocks, and few dispensers.
LegislationE.g. regulations requiring 7-days only forprescribing, lack of national policy on opioid use,and bureaucratic processes.
EducationE.g. existing clinicians do not know how to assessand treat pain, fear of addiction, poor patientcompliance, palliative care stresses specialty tothe point of exclusion, and doctors are lessinterested in dying patients.
PracticalCosts, storage requirements, not enoughprescribers, inadequate staff in HBC, poorinfrastructure to follow patients home, lack ofsugar for making up syrup, and short shelf-life of morphine.
There was concordance between sites with regard towhether opioids were on the country essential drugslist, with the notable exception of Zambia.
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 18
Table 10 Opioids, essential drug lists and legal requirements
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 19
Bot
swan
a
Cote
d’Iv
oire
Ethi
opia
Keny
a
Moz
ambi
que
Nam
ibia
Opi
oids
on
esse
ntia
ldr
ugs
list
?
Yes
No
1 (1
00%
)0
1 (1
00%
)0
1 (1
00%
)0
06
(100
%)
1 (1
00%
)0
1 (1
00%
)0
Lega
l re
quir
emen
ts
Opi
oids
sup
plie
d by
Cen
tral
M
edic
al S
tore
s
Supp
ly, s
tock
and
dis
pens
ing
tight
ly c
ontr
olle
dO
nly
doct
ors
can
pres
crib
e, w
ith
spec
ific
pres
crip
tion
form
s an
d fo
r 7
days
No
idea
bec
ause
alt
houg
h it
is o
nes
sent
ial d
rugs
list
it is
not
ava
ilabl
ein
the
cou
ntry
A li
cens
e is
req
uire
d fo
r ha
ndlin
gdr
ugs
Onl
y ho
spic
es c
an p
urch
ase,
sto
rean
d di
spen
seM
ust
have
a s
tron
g ro
omO
rder
ed b
y do
ctor
, adm
inis
tere
d by
a r
egis
tere
d nu
rse,
che
cked
by
seco
nd n
urse
, rec
orde
d in
boo
k,lo
cked
in c
upbo
ard
Onl
y do
ctor
s ca
n pr
escr
ibe
Onl
y do
ctor
s ca
n pr
escr
ibe;
onl
yav
aila
ble
thro
ugh
hosp
ital
s
Mai
n fa
ctor
s ha
mpe
ring
op
ioid
pro
visi
on
Lack
of p
rofe
ssio
nal k
now
ledg
e of
pai
nre
lief f
or H
IV p
atie
nts
Lack
of t
rain
ing
Cent
ral M
edic
al S
tore
s do
n’t p
rovi
deor
al m
orph
ine
Logi
stic
al s
uppl
y pr
oble
ms
Lack
of p
olit
ical
will
Doc
tors
fear
of o
pioi
ds
Lack
of a
vaila
bilit
y co
untr
y-w
ide
Lack
of k
now
ledg
e of
opi
oids
Lack
of n
atio
nal p
olic
yN
on-a
vaila
bilit
y in
mos
t se
ttin
gsN
ot r
ecog
nize
d as
a n
eed
Few
dis
pens
ers
Cost
sD
octo
rs fe
ar a
ddic
tion
Scar
city
of s
uppl
yLa
ck o
f sup
ervi
sory
sta
ffLo
ng &
tir
ing
bure
aucr
atic
pro
cess
esLa
ck o
f tra
inin
g La
ck o
f sto
rage
faci
litie
s
Fear
of m
isus
eO
ver
cent
raliz
ed c
ontr
ol
Lack
of t
rain
ed m
edic
al s
taff
Pu
blic
mis
unde
rsta
ndin
g
Ora
l mor
phin
e on
esse
ntia
l dru
gs li
st?
Yes
No
1 (1
00%
)0
1 (1
00%
)0
1 (1
00%
)0
06
(100
%)
1 (1
00%
)0
01
(100
%)
Table 10 Opioids, essential drug lists and legal requirements – continued
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 20
Nig
eria
Rw
anda
Sout
h A
fric
a
Tanz
ania
Opi
oids
on
esse
ntia
ldr
ugs
list
?
Yes
No
2(66
.7%
)1(
33.3
%)
01(
100%
)
24(8
8.9%
)D
K 3(
11.1
%)
1 (2
5%)
3 (7
5%)
Lega
l re
quir
emen
ts
Curr
ent
gove
rnm
ent
emba
rgo
on u
se
Non
e ye
t
Nee
d a
disp
ensi
ng li
cens
eSt
rong
opi
oids
on
nam
ed p
atie
ntba
sis
only
from
lice
nsed
pha
rmac
ist
Onl
y do
ctor
s ca
n pr
escr
ibe
Cons
tant
eva
luat
ion
of e
ffec
tD
aily
cou
nt o
f loc
ked
stor
esN
o N
GO
/CB
O a
llow
ed t
o st
ore,
hosp
ital
dis
pens
esPr
escr
ipti
on n
ot r
epea
tabl
e O
btai
n fr
om a
reg
iste
red
phar
mac
y St
ore
behi
nd 2
lock
s2
nurs
es w
itne
ss d
ispe
nsin
gSt
reng
th fr
eque
ncy
and
rout
e st
ated
in w
ords
and
figu
res
Lack
of n
atio
nal a
vaila
bilit
y D
iffic
ulti
es in
mee
ting
gov
ernm
ent
requ
irem
ents
Mai
n fa
ctor
s ha
mpe
ring
op
ioid
pro
visi
on
Lack
of s
taff
and
faci
litie
sLa
ck o
f sup
ply
Legi
slat
ion
Fear
of a
ddic
tion
Lack
of t
rain
ing
prog
ram
s
Palli
ativ
e Ca
re N
atio
nal A
ssoc
iatio
n is
new
ly fo
rmed
N
o na
tiona
l pol
icy
Lack
of p
rogr
ams
Pres
crib
ing
rest
rictio
nsAv
aila
bilit
yCo
stCu
ltura
l acc
epta
nce
of p
ain
Dis
tanc
e fr
om s
uppl
iers
Hea
lth c
are
staf
f lac
k co
nfid
ence
Igno
ranc
e of
pai
n in
HIV
Poor
clin
ical
trai
ning
Lack
ing
full
time
pres
crib
erM
orph
ine
myt
hsSu
stai
nabi
lity
of s
uppl
y La
ck o
f pol
itica
l sup
port
La
ck o
f doc
tor p
rese
nce
in H
BC
Stor
age
diffi
culti
es
Lack
of k
now
ledg
e of
pai
n la
dder
Resp
irato
ry d
epre
ssio
n fe
ars
Poor
pai
n as
sess
men
t wor
kPo
or p
atie
nt c
ompl
ianc
eH
IV c
ompl
icat
ions
(e.g
. vom
iting
)
Lack
of k
now
ledg
e an
d sk
ills
Lack
of p
lace
s fo
r mak
ing
up
pow
dere
d m
orph
ine
Acce
ssFe
ars
Lack
of s
uppl
iers
/dis
pens
ers
Lack
of b
urea
ucra
tic s
uppo
rtPa
in a
sses
smen
t ski
ll pr
oble
ms
Lack
of c
linic
al w
ill a
nd s
uppo
rt
Lack
of e
duca
tion
oppo
rtun
ities
Lack
of k
now
ledg
e of
effe
ctiv
enes
s
Ora
l mor
phin
e on
esse
ntia
l dru
gs li
st?
Yes
No
01
(100
%)
01
(100
%)
25(9
2.6%
)D
K 1(
3.7%
)
1 D
K3
(75%
)
Table 10 Opioids, essential drug lists and legal requirements – continued
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 21
Uga
nda
Zam
bia
Opi
oids
on
esse
ntia
ldr
ugs
list
?
Yes
No
8(10
0%)
0
3(37
.5%
)1(
12.5
%)
DK
4(50
%)
Lega
l re
quir
emen
ts
Regi
ster
ed p
harm
acy
adhe
ring
to
Clas
s A
pol
icy
inc
pres
crib
ing,
phar
mac
y &
war
d ro
unds
, sto
rage
Regi
ster
wit
h N
atio
nal D
rugs
Aut
hori
ty
Mus
t ha
ve le
tter
by
med
ical
supe
rint
ende
nt/p
harm
acis
t to
col
lect
wit
h w
ritt
en a
utho
rity
B
e pa
rty
to in
tern
al c
onve
ntio
n B
e re
gist
ered
wit
h m
edic
al c
ounc
il to
pre
scri
beD
uplic
ate
pres
crip
tion
wit
hpa
tien
t/ca
rer
sign
atur
eD
oubl
e lo
cked
cup
boar
dKe
ep r
ecor
d of
sto
ckN
eed
licen
se t
o pr
oduc
e m
orph
ine
solu
tion
Nur
ses
can
not
pres
crib
eO
nly
hosp
ital
s ca
n st
ock
Gov
ernm
ent
med
ical
sto
res
mus
tdi
stri
bute
thr
ough
the
mai
n ho
spit
al p
harm
acy
Pres
crib
e on
ly b
y do
ctor
sU
nder
Dan
gero
us D
rugs
Act
Mai
n fa
ctor
s ha
mpe
ring
op
ioid
pro
visi
on
Nur
ses
not b
eing
abl
e to
pre
scrib
eLa
ck o
f pha
rmac
ists
D
octo
rs: u
nwill
ing,
lazy
, lac
k of
inte
rest
in d
ying
pat
ient
s Ch
roni
c la
ck o
f edu
catio
n St
aff d
o no
t wan
t to
expl
ain
and
writ
epr
oper
pre
scrip
tions
In
adeq
uate
ly tr
aine
d st
aff
Myt
hs/f
ears
Illite
racy
Poor
infr
astr
uctu
re to
follo
w
patie
nts
hom
ePo
or s
ide-
effe
ct m
onito
ring
syst
ems
Cultu
ral b
elie
fsM
orph
ine
roll-
out n
eeds
to re
ach
mor
e di
stric
ts
Nee
d m
ore
prov
ider
s of
trai
ning
U
nrel
iabl
e su
pply
(dis
trib
utio
n,st
ocki
ng, s
helf
life)
Pa
lliat
ive
care
spe
cial
ists
ove
r-em
phas
ise
the
spec
ialis
t nat
ure
and
excl
ude
othe
rs
Mor
phin
e ha
s sh
ort s
helf-
life
Gov
ernm
ent r
egul
atio
nsPo
or a
cces
sFu
nds
Legi
slat
ion/
rest
rictiv
e po
licy
Doc
tors
will
not
pre
scrib
e to
thos
e in
nee
dPr
ofes
sion
als
fear
add
ictio
nLa
ck o
f pha
rmac
ists
M
yths
Lack
of q
ualif
ied
pers
onne
lPo
or k
now
ledg
e of
opi
oid
use
in H
IVLa
ck o
f num
bers
of p
resc
riber
s La
ck o
f sug
ar fo
r mix
ing
oral
mor
phin
ePo
or p
ain
asse
ssm
ent s
kills
In
adeq
uate
dos
ing
and
not b
y th
e cl
ock
Ora
l mor
phin
e on
esse
ntia
l dru
gs li
st?
Yes
No
7(87
.5%
)m
issi
ng n
=1
2(25
%)
4(50
%)
DK
2(25
%)
Opioid training, expanding access and current challenges
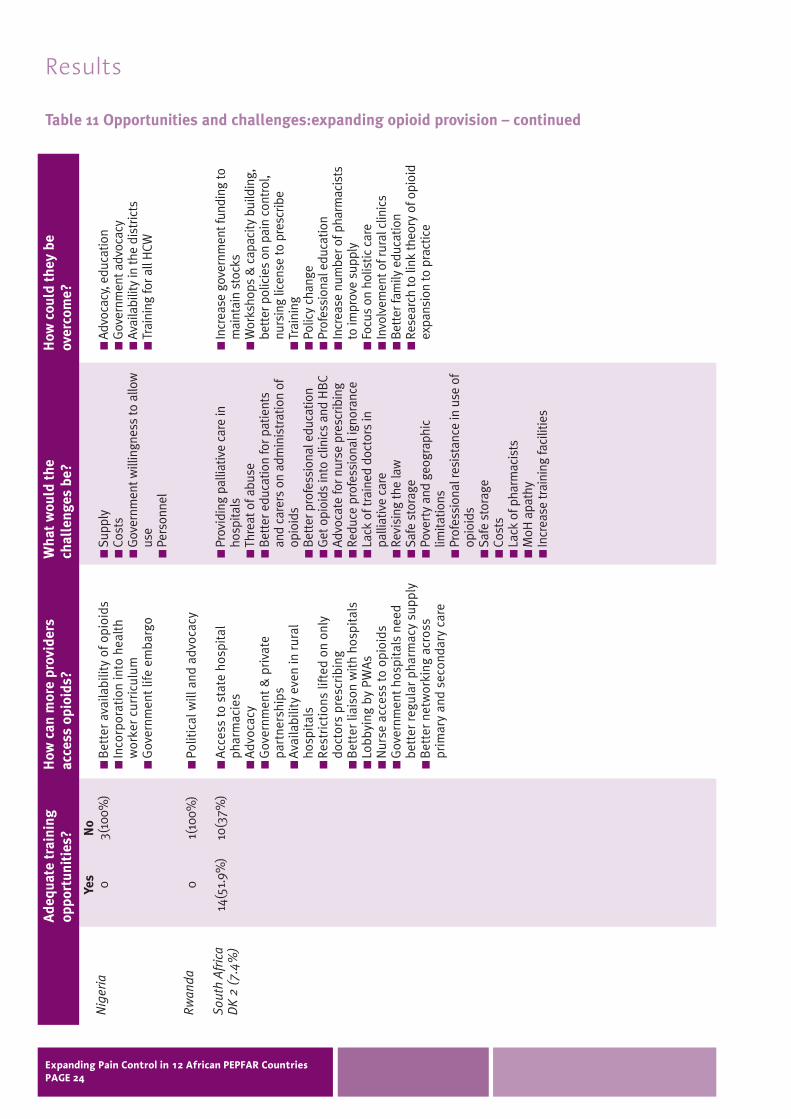
Respondents indicated whether they felt there wereadequate opportunities for staff training in the useof opioids, what mechanisms they recommend forexpanding access to a greater number of HIV careproviders, and what challenges they envisage inachieving this (see Table 11).
Again, despite there being some disparity in theprogress being made between individual countrieswithin the region, there were notable similaritieswith respect to their views.
In terms of assisting more providers in accessingopioids, the suggestions were:
Advocacy: at government and public levels on the need for opioids, and on lifting restrictive legislation.
Collaboration: with prescribing doctors, across primary and secondary care, and withhospital pharmacies.
Training: in pain assessment and management, in all curricula, on palliative rather than supportive care, and a shorter course for prescribing.
Coverage: to rural and HBC services.
With respect to potential challenges to expansion,the difficulties were:
Political: achieving sufficient motivation.
Educational: challenging myths, teaching that HIVrequires Step 3 pain management, and achievingmedical cultural change.
Resources: time for doctors to prescribe, drugcosts, storage facilities, number of pharmacists,supply breaks, building up rural services, and thenumber of prescribers.
The suggested methods to overcome the challengeswere as follows:
Education: training for HCW, input in to curricula,teaching for HIV services, and developing shorter courses.
Advocacy: support through APCA, andgovernment lobbying.
Organisational: central supply of drugs andcollection points facilitated by government, and better linkages with hospices.
Resources: fund storage, increase hospicecapacity, more pharmacists, and employprofessional staff in HBC organisations.
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 22
Table 11 Opportunities and challenges:expanding opioid provision
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 23
Bot
swan
a
Cote
d’Iv
oire
Ethi
opia
Keny
a
Moz
ambi
que
Nam
ibia
Ade
quat
e tr
aini
ngop
port
unit
ies?
Yes
No
01(
100%
)
01(
100%
)
1(10
0%)
0
DK
1(16
.7%
)5(
83.3
%)
1(10
0%)
0
01(
100%
)
How
can
mor
e pr
ovid
ers
acce
ss o
pioi
ds?
Wor
k w
ith
MoH
to
rais
eaw
aren
ess
and
advo
cate
for
mor
phin
e us
e, p
ublic
edu
cati
on
Adv
ocat
e fo
r us
e of
opi
oids
,in
crea
se c
ount
ry-w
ide
avai
labi
lity
Chan
ge p
resc
ribi
ng r
ules
Clos
er w
orki
ng w
ith
Ethi
opia
ndo
ctor
s
Ord
er in
opi
oids
from
cur
rent
stoc
kist
sG
over
nmen
t ch
ange
res
tric
tive
rule
sPu
rcha
se p
riva
tely
Bet
ter
trai
ning
in p
ain
asse
ssm
ent
and
man
agem
ent/
disp
ensi
ngCo
llabo
rati
on w
ith
hosp
ices
MoH
sup
port
The
indi
vidu
al is
the
onl
y w
ayto
adv
ocat
e su
cces
sful
ly a
ndch
ange
pol
icy
Nee
d do
ctor
and
nur
se t
rain
ing
to a
sses
s an
d pr
escr
ibe,
bet
ter
supe
rvis
ion
of v
olun
teer
s
Wha
t w
ould
the
ch
alle
nges
be?
Mot
ivat
ing
the
MoH
and
plan
ners
of h
ealth
car
e pr
ovis
ion
Fear
of o
pioi
d ab
use
For d
octo
rs to
com
ply
in w
orki
ngw
ith H
IV c
are
prov
ider
s. D
octo
rsdo
not
see
m to
hav
e th
e tim
e to
wor
k w
ith p
rovi
ders
and
this
stop
s pa
tient
s ge
ttin
g ef
fect
ive
pain
relie
f
Cost
Gov
ernm
ent a
ccep
tanc
e of
mor
phin
e us
e fo
r HIV
and
licen
se m
orph
ine
Inad
equa
te s
uppl
y an
d la
ck o
fpr
escr
ibin
g pe
rson
nel
Lack
of p
harm
acis
ts to
reco
nstit
ute,
and
lack
of s
tora
gefa
cilit
ies
Lack
of p
harm
acy
stoc
ksG
over
nmen
t pol
icy
Nee
d to
str
engt
hen
advo
cacy
orga
nisa
tions
Min
istr
y un
ders
tand
ing
Gov
ernm
ent p
olic
ies
How
cou
ld t
hey
be
over
com
e?
Trai
n H
CW w
ith h
elp
from
APC
A,tr
ain
mor
e nu
rses
and
doc
tors
,ed
ucat
e th
e pu
blic
on
palli
ativ
eca
re in
can
cer a
nd H
IV
Incr
ease
adv
ocac
y
Bet
ter e
duca
tion
for d
octo
rs
Cent
raliz
e pu
rcha
sed
and
colle
ctio
n po
ints
and
cos
tre
duct
ion.
Gov
ernm
ent s
houl
dfa
cilit
ate
this
pro
cess
Bet
ter s
uppl
y, tr
aini
ng, i
ncre
ase
hosp
ice
capa
city
Gov
ernm
ent l
egis
latio
n ch
ange
Advo
cacy
with
MoH
/Gov
ernm
ent
Trai
ning
for s
taff
on p
resc
ribin
g&
dis
pens
ing,
and
redu
ce to
ugh
impo
rtat
ion
rule
sB
ette
r use
of a
vaila
ble
phar
mac
ists
, mor
e st
orag
ecu
pboa
rds
Advo
cacy
is th
e on
ly w
ay
Educ
atio
n &
lobb
ying
Table 11 Opportunities and challenges:expanding opioid provision – continued
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 24
Nig
eria
Rw
anda
Sout
h A
fric
aD
K 2
(7.
4%)
Ade
quat
e tr
aini
ngop
port
unit
ies?
Yes
No
03(
100%
)
01(
100%
)
14(5
1.9%
)10
(37%
)
How
can
mor
e pr
ovid
ers
acce
ss o
pioi
ds?
Bet
ter
avai
labi
lity
of o
pioi
dsIn
corp
orat
ion
into
hea
lth
wor
ker
curr
icul
umG
over
nmen
t lif
e em
barg
o
Polit
ical
will
and
adv
ocac
y
Acc
ess
to s
tate
hos
pita
lph
arm
acie
sA
dvoc
acy
Gov
ernm
ent
& p
riva
tepa
rtne
rshi
psA
vaila
bilit
y ev
en in
rur
alho
spit
als
Rest
rict
ions
lift
ed o
n on
lydo
ctor
s pr
escr
ibin
gB
ette
r lia
ison
wit
h ho
spit
als
Lobb
ying
by
PWA
sN
urse
acc
ess
to o
pioi
dsG
over
nmen
t ho
spit
als
need
bett
er r
egul
ar p
harm
acy
supp
lyB
ette
r ne
twor
king
acr
oss
prim
ary
and
seco
ndar
y ca
re
Wha
t w
ould
the
ch
alle
nges
be?
Supp
lyCo
sts
Gov
ernm
ent w
illin
gnes
s to
allo
wus
ePe
rson
nel
Prov
idin
g pa
lliat
ive
care
inho
spita
lsTh
reat
of a
buse
Bet
ter e
duca
tion
for p
atie
nts
and
care
rs o
n ad
min
istr
atio
n of
opio
ids
Bet
ter p
rofe
ssio
nal e
duca
tion
Get
opi
oids
into
clin
ics
and
HB
CAd
voca
te fo
r nur
se p
resc
ribin
gRe
duce
pro
fess
iona
l ign
oran
ceLa
ck o
f tra
ined
doc
tors
inpa
lliat
ive
care
Revi
sing
the
law
Safe
sto
rage
Pove
rty
and
geog
raph
iclim
itatio
nsPr
ofes
sion
al re
sist
ance
in u
se o
fop
ioid
sSa
fe s
tora
geCo
sts
Lack
of p
harm
acis
tsM
oH a
path
yIn
crea
se tr
aini
ng fa
cilit
ies
How
cou
ld t
hey
be
over
com
e?
Advo
cacy
, edu
catio
nG
over
nmen
t adv
ocac
yAv
aila
bilit
y in
the
dist
ricts
Trai
ning
for a
ll H
CW
Incr
ease
gov
ernm
ent f
undi
ng to
mai
ntai
n st
ocks
Wor
ksho
ps &
cap
acity
bui
ldin
g,be
tter
pol
icie
s on
pai
n co
ntro
l,nu
rsin
g lic
ense
to p
resc
ribe
Trai
ning
Polic
y ch
ange
Prof
essi
onal
edu
catio
nIn
crea
se n
umbe
r of p
harm
acis
tsto
impr
ove
supp
lyFo
cus
on h
olis
tic c
are
Invo
lvem
ent o
f rur
al c
linic
sB
ette
r fam
ily e
duca
tion
Rese
arch
to li
nk th
eory
of o
pioi
dex
pans
ion
to p
ract
ice
Table 11 Opportunities and challenges:expanding opioid provision – continued
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 25
Tanz
ania
Uga
nda
Zam
bia
Ade
quat
e tr
aini
ngop
port
unit
ies?
Yes
No
4(10
0%)
5(62
.5%
2(25
%)
2(25
%)
8(75
%)
How
can
mor
e pr
ovid
ers
acce
ss o
pioi
ds?
Get
ting
tra
inin
g in
pal
liati
vera
ther
tha
n su
ppor
tive
car
eTr
ain
in o
pioi
d us
e be
yond
canc
erRe
duce
gov
ernm
ent
rest
rict
ions
Impr
ove
netw
ork
betw
een
trai
ned
pres
crib
ers
and
HIV
care
org
anis
atio
nsG
raft
ing
palli
ativ
e ca
re o
nto
exis
ting
ser
vice
s, e
spec
ially
pain
and
sym
ptom
con
trol
Rela
x pr
escr
ibin
g re
quir
emen
tsw
itho
ut c
ompr
omis
ing
cont
rol
Non
-spe
cial
ists
sho
uld
begi
ven
a sh
orte
r co
urse
to
enab
le t
hem
to
pres
crib
eR
N o
r CO
to
atte
nd p
resc
ribi
ngco
urse
at
HA
U r
athe
r th
an o
nly
doct
ors
Liai
se w
ith
hosp
ices
Empl
oy p
erso
nnel
who
can
pres
crib
eTr
ain
HB
Cs a
nd M
oH a
ppro
veop
ioid
use
Adv
ocat
e to
Gov
ernm
ent
Trai
n cl
inic
al o
ffic
ers
and
nurs
es t
o pr
escr
ibe
as t
hey
are
clos
er t
o th
e co
mm
unit
yPo
licy
chan
geO
btai
n op
ioid
s th
roug
h pr
ivat
eim
port
er o
r th
roug
h U
nive
rsit
yte
achi
ng h
ospi
tal
Opi
oid
clin
ics
in h
ospi
tals
Wha
t w
ould
the
ch
alle
nges
be?
Fear
s of
pre
scrib
ing
and
usin
g op
ioid
sCo
sts
Hum
an re
sour
ces
MoH
/Med
ical
Sch
ools
mus
tin
clud
e in
cur
ricul
umG
over
nmen
t bur
eauc
racy
Redu
ctio
n of
rest
rictio
ns
Fina
nce/
cost
sRe
cord
kee
ping
Fear
of o
pioi
dsB
urea
ucra
cy in
bei
ng a
pro
vide
rH
avin
g en
ough
med
ical
sta
ffN
ot a
ll di
stric
ts tr
aine
d an
dse
nsiti
zed
Doc
tor r
eluc
tanc
e to
pres
crib
e/pr
escr
ibe
inco
rrec
tlyN
ot e
noug
h pr
escr
iber
sB
ette
r org
anis
atio
nal
man
agem
ent
Fear
of a
buse
Chan
ge le
gisl
atio
nTr
ain
in p
resc
ribin
g an
d pa
inm
anag
emen
tPo
or a
vaila
bilit
y of
mor
phin
epo
wde
rFu
ndin
gD
octo
rs a
re re
sist
ant t
o ch
ange
Trai
ning
cos
tsH
BC
serv
ices
som
etim
es la
ckhe
alth
car
e st
aff
Gov
ernm
ent p
ersu
asio
n
How
cou
ld t
hey
be
over
com
e?
Advo
cacy
and
ext
erna
las
sist
ance
Sens
itize
pol
icy
mak
ers
Med
ical
sch
ools
sca
le-u
ptr
aini
ngTr
aini
ng fo
r HIV
car
e pr
ovid
ers
on p
allia
tive
care
Gov
ernm
ent r
ecog
nitio
n of
palli
ativ
e ca
re tr
aini
ng c
ours
es
Dev
elop
sho
rter
trai
ning
cou
rses
Har
mon
ize
exis
ting
trai
ning
toin
corp
orat
e m
orph
ine
Educ
atio
nAd
voca
cyCu
rren
t cen
ters
take
resp
onsi
bilit
y fo
r rol
ling
out i
nto
dist
ricts
Link
ages
with
hos
pice
sEx
pand
bas
e of
pre
scrib
ers
i.e.
non-
doct
ors
Inst
itutio
ns g
iven
sto
rage
faci
litie
sSe
nsiti
ze p
olic
e an
d go
vern
men
tU
nder
stan
d th
e tr
aini
ng n
eeds
Advo
cacy
to G
over
nmen
tPo
licy
chan
geSo
urci
ng fu
ndin
g fo
r opi
oids
Trai
n no
n-pr
ofes
sion
al s
taff
Enco
urag
e H
BC
serv
ices
to h
ave
prof
essi
onal
sta
ffIn
crea
se o
pioi
d su
pply
Wea
k op
ioid
s sh
ould
be
avai
labl
e to
clin
ical
offic
ers/
nurs
es w
ho a
re tr
aine
din
opi
oid
pres
crib
ing
with
out
need
for a
n on
-site
pha
rmac
ist
Current challenges: purchasing, producing,dispensing and prescribing
Finally, respondents described current challenges in the purchasing, production, dispensing andprescribing or opioids (see Table 12).
The Purchasing issues can be summarized as:
Overwhelming cost due to new taxes; expensive and scarce single source of supply;lack of funds; unreliable supply; distances; too many restrictions.
The Producing issues can be summarized as:
None produced due to government embargo; hard to produce and source enough due toexpanding patient base; lack of pharmacists;limits on sugar supply to make up syrup.
The Dispensing issues can be summarized as:
Restrictions to hospitals and hospices mean patients do not get access; massive delays between scripts and dispensing; lack of pharmacists.
The Prescribing issues can be summarized as:
Being the sole prescriber; heavy restrictions;professionals do not know how to prescribe; lack of education; refusal to prescribe forchildren; lack of rural staff; gross underuse due to fears and myths.
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 26
Table 12 Current issues in opioid provision
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 27
Bot
swan
a
Cote
d/V
oire
Ethi
opia
Keny
a
Moz
ambi
que
Nam
ibia
Nig
eria
Rw
anda
Non
e1(
100%
)
1(10
0%)
1(10
0%)
2/6(
33%
)
1(10
0%)
– 1/3(
33%
)
–
Issu
es
Cost
has
alm
ost
doub
led
due
to n
ew t
ax la
ws
on d
rugs
Dru
g co
mpa
nies
do n
ot s
tock
enou
gh o
pioi
ds
–
Can
only
be
purc
hase
d at
Nat
iona
l D
rug
Stor
eSc
arce
and
expe
nsiv
e
–
Non
e0(
0%)
1(10
0%)
1(10
0%)
1/6(
16.7
%)
1(10
0%)
– 1/3(
33%
)
–
Issu
esN
one
is p
rodu
ced
in B
otsw
ana
Har
d to
sou
rce
enou
gh t
o pr
ovid
efo
r ex
pand
ing
pati
ent
base
due
to G
over
nmen
tre
stri
ctio
ns o
nim
port
N
ot a
ll co
mpa
nies
can
prod
uce
Not
sur
e if
they
have
the
cond
itio
ns t
opr
oduc
e
–
Not
pro
duce
d in
coun
try
Onl
y pr
oduc
edce
ntra
lly
–
Pur
chas
ing
Non
e1(
100%
)
0(0%
)
1(10
0%)
3/6(
50%
)
1(10
0%)
– 2/3(
66.7
%)
–
Issu
es
Mos
tly
disp
ense
din
hos
pita
ls a
ndho
spic
es s
o m
any
pati
ents
do
not
get
acce
ss
–
Onl
y do
ctor
s ca
npr
escr
ibe
–
Dis
pens
ing
Prod
ucin
g
Non
e1
(100
%)
0 (0
%)
N/A
3/6
(50%
)
1 (1
00%
)
– 3/3
(100
%)
–
Issu
es
Onl
y do
ctor
s ca
npr
escr
ibe
and
for
7 da
ys a
t a
tim
e
Rest
rict
ions
on
pres
crib
ing
Mos
tpr
ofes
sion
als
dono
t kn
ow h
ow t
opr
escr
ibe
Pres
crib
ing
Table 12 Current issues in opioid provision – continued
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 28
Sout
h A
fric
a
Tanz
ania
Uga
nda
Zam
bia
Non
e12
/27
(44.
4%)
4(10
0%)
6(75
%)
3/8(
37.5
%)
Issu
esCa
nnot
pur
chas
ew
itho
utpr
escr
ipti
on
Not
eno
ugh
fund
ing
topu
rcha
seB
lack
pat
ient
sca
nnot
sou
rce
mor
phin
e ou
tsid
eth
e pr
ivat
esy
stem
Esse
ntia
l dru
gsno
t al
way
sav
aila
ble
at p
ublic
heal
th fa
cilit
ies
Lack
of d
octo
rsD
ista
nce
todi
spen
sers
Dru
gs r
un o
ut o
fst
ock
Cost
Des
pite
us
requ
esti
ngqu
arte
rly
inad
vanc
e, M
edic
alSt
ores
do
not
orde
r in
tim
e
Too
man
yre
stri
ctio
ns
Non
e12
/27
(44.
4%)
2(50
%)
4(50
%)
2/8(
25%
)
Issu
esFe
w q
ualif
ied
phar
mac
ists
Lack
of d
octo
rs t
opr
escr
ibe
New
reg
ulat
ions
are
limit
ing
spre
ad o
f opi
oids
acro
ss t
heco
untr
y La
ck o
fpr
escr
iber
s in
rura
l are
as
Cost
No
loca
lpr
oduc
tion
-
Relia
nce
on s
ugar
to m
ake
pow
der
into
syr
upLi
mit
edph
arm
aceu
tica
lin
dust
ry
Pur
chas
ing
Non
e9/
27(3
3.3%
)
2(50
%)
8(10
0%)
3/8(
37.5
%)
Issu
esN
eed
disp
ensi
nglic
ense
N
eed
corr
ect
scri
pts
from
doct
orCa
n ta
ke 3
-wee
kde
lay
betw
een
scri
pt w
riti
ng a
ndm
orph
ine
deliv
ery
from
dis
pens
ary
NG
O s
tatu
sde
bars
from
disp
ensi
ngN
o di
spen
sing
from
pre
mis
es
Too
few
phar
mac
ists
Staf
f ina
dequ
atel
ytr
aine
d in
pai
nas
sess
men
t an
dm
anag
emen
t
Rest
rict
ions
to
hosp
ital
s on
ly
Onl
y av
aila
ble
inm
ajor
hos
pita
lsSt
orag
ere
stri
ctio
ns li
mit
acce
ss
Dis
pens
ing
Prod
ucin
g
Non
e13
/27
(48.
1%)
2(50
%)
7/8(
87.5
%)
2/8(
25%
)
Issu
esTa
kes
too
long
to
get
mor
phin
e,es
peci
ally
in r
ural
area
s D
octo
rs n
eed
educ
atio
n in
mor
phin
e us
e D
octo
rs r
efus
e to
pres
crib
em
orph
ine
for
child
ren
Pati
ent/
fam
ilyfe
ar o
f add
icti
on
No
licen
seRu
ral a
reas
do
not
have
doc
tor
avai
labl
e to
wri
tesc
ript
sN
urse
s ne
ed t
o be
able
to
pres
crib
e
Too
few
pres
crib
ers
Onl
y do
ctor
s, a
ndno
t al
l doc
tors
,kn
ow h
ow t
opr
escr
ibe
I am
the
onl
ype
rson
abl
e to
pres
crib
e!
Gro
ssly
unde
ruse
d du
e to
fear
s of
add
icti
onCa
n no
t pr
escr
ibe
outs
ide
hosp
ital
s
Pres
crib
ing
INCB competent authorities data Respondents
Despite significant efforts over a period of eightmonths, five interviews were achieved. This was due, in large part, to considerable confusion withinMinistries as to whom the appropriate person wasand a lack of accurate contact details for theidentified individual.
The interviews that were achieved were:
Ethiopia
Kenya
Namibia
Tanzania
Uganda
Current opioid supply and regulatory system
All five stated that opioids were currently on theirrespective country’s essential drugs list andavailable in country for pain relief.
In Table 13, it is notable that the majority of INCBcompetent authorities were satisfied with thefunctioning of the current regulatory system,contrary to provider data. INCB competentauthorities also felt (with the exception of Uganda)that there were currently adequate numbers ofopioid providers. An important finding from theseinterviews is that INCB competent authorities feelthat they may not be able to offer adequateregulation and monitoring for increased numbers ofproviders, and that they question the skills of thosealready prescribing opioids.
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 29
Table 13 INCB competent authorities views: current opioid supply and regulation
Results
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 30
Keny
a
Ethi
opia
Tanz
ania
Uga
nda
Nam
ibia
Due
to
the
puni
tive
natu
re o
f the
199
4A
ct, m
ost
prov
ider
sha
ve s
hied
aw
ay fr
omse
lling
opi
oids
.
The
fear
s ar
ound
pres
crib
ing
may
be
due
to t
he r
egul
atio
n.Th
ere
is a
lack
of
awar
enes
s of
appr
opri
ate
opio
idus
e am
ong
thos
e ab
leto
pre
scri
be.
Prof
essi
onal
fear
of
tran
scri
bing
.
Stri
ngen
t la
ws
onim
port
atio
n.D
ispe
nsin
gph
arm
acie
s an
dhe
alth
car
e fa
cilit
ies
fear
sto
ckin
g op
ioid
sdu
e to
tou
ghre
quir
emen
ts. T
oo fe
wpr
escr
iber
s.
Ava
ilabi
lity
of d
octo
rsto
pre
scri
be a
ndph
arm
acis
ts t
odi
spen
se.
App
ly fo
r a
licen
sefr
om t
he P
harm
acy
&Po
ison
s B
oard
and
empl
oy le
gally
reco
gniz
ed s
taff
.
Regi
ster
wit
h D
ACA
,an
d ei
ther
use
dru
gson
the
ess
enti
al d
rug
list
OR
wor
k w
ith
exis
ting
gov
ernm
ent
faci
litie
s w
ho h
ave
acce
ss.
App
ly fo
r pe
rmit
fr
om T
FDA
.
Gra
nt a
utho
riza
tion
from
MoH
,or
gani
sati
on is
surv
eyed
for
suit
abili
ty.
Nee
d a
doct
or t
opr
escr
ibe
and
aph
arm
acis
t to
disp
ense
and
reg
iste
rw
ith
Gov
ernm
ent.
Wha
t ar
e th
ebl
ocka
ges
and
prob
lem
s?
How
wou
ld a
sit
ebe
com
e a
prov
ider
Yes
Yes
Yes
Too
few
Yes
BU
Tno
ten
ough
to
real
lyco
pe w
ith
HB
C
Yes
Yes
Yes
No
No
Are
the
re
enou
ghpr
ovid
ers?
Doe
s th
ere
gula
tory
sy
stem
w
ork
wel
l?
Non
e, p
harm
acy
&Po
ison
s B
oard
Insp
ecto
rate
ope
rate
sef
ficie
ntly
.
The
polic
y an
dre
gula
tory
envi
ronm
ents
are
enab
ling,
the
prob
lem
aris
es fr
om p
eopl
e no
tpr
escr
ibin
g dr
ugs
beca
use
they
lack
know
ledg
e an
d do
not
stim
ulat
e de
man
d.
The
curr
ent s
yste
mw
orks
wel
l but
do
need
to im
prov
ein
spec
tion,
and
tora
ise
awar
enes
sam
ong
prov
ider
s.
Too
few
per
sonn
el to
cond
uct s
urve
ys a
ndm
onito
ring
for t
hew
hole
cou
ntry
.
Lack
of s
taff
tore
gula
te! T
he p
owde
rit
is m
ade
from
is a
Sche
dule
7 d
rug,
als
one
ed c
ompo
undi
ngeq
uipm
ent e
tc. S
helf
life
is o
nly
1 m
onth
.
We
need
to im
prov
eth
e qu
ality
of
pres
crib
ing
pers
onne
lth
roug
h tr
aini
ng n
otin
crea
se th
e nu
mbe
rs.
Bet
ter t
rain
ing
ofth
ose
able
topr
escr
ibe,
revi
ew
the
regu
lato
ryen
viro
nmen
t, re
view
curr
icul
a, im
prov
ees
timat
ion
syst
em.
Incr
ease
med
ical
stud
ent i
ntak
e, a
ndm
otiv
ate
pres
crib
ers
to b
e ac
tive
in a
llar
eas.
Inte
grat
e tr
aini
ng s
oan
y qu
alify
ing
clin
ical
staf
f are
con
fiden
t to
pres
crib
e.
If nu
rses
wer
e to
pres
crib
e w
e’d
need
to
cha
nge
curr
ent
legi
slat
ion,
exp
and
trai
ning
, and
impr
ove
mon
itorin
g.
Dif
ficu
ltie
s &
chal
leng
es t
ore
gula
tory
sy
stem
Syst
ems
&re
sour
ces
need
ed
to in
crea
se n
o.
of p
rovi
ders
Comparison to site responses
The data from INCB competent authorities and thedata from care sites were integrated and comparedto appraise the congruity of their perspectives onopioid availability.
It is noteworthy in Table 14 that although theEthiopian INCB competent authority reported thatopioids were available in the country, the respondentsaid that while they were on the essential drugs list,they were unavailable anywhere. In every countrywithout exception, INCB competent authorities citedspecific opioids that they believed to be available in-country that were never cited by any servicewithin that country.
• Noted by INCB comp auth as present in country ✓ Mentioned by at least one service in country ✗ Not mentioned by any service
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 31
Table 14 Comparison of INCB competent authorities and provider data: opioid availability
Definitions and components of palliative care
Palliative care is delivered in an increasingly diverserange of settings, with the potential for generalistpalliative care to be rolled-out more easily than thespecialist care which offers expert management ofcomplex cases. Our data offer two important andfundamental opportunities for opioid expansion forpeople living with HIV in Sub Saharan Africa.
Firstly, all the respondents reported that they definepalliative care in exactly the same way as the WHO2002 definition. As a common thread throughout thedata is the need for education and collaboration toincrease opioid access, the united acceptance of theWHO definition will make the roll-out, monitoringand provision of opioids to common objectiveseasier to achieve. As the PEPFAR legislation hasbeen designed to operationalize this definition, inparticular the WHO pain ladder, then scale-upstrategies can more easily embrace the range ofservices with the knowledge that a commondefinition is shared.
Second, the range of services offered by the 3categories of provider demonstrate clear differencesin focus, with palliative-only services stressingbereavement counseling, family support, spiritualcare, professional education and advocacy, whilemore integrated NGOs offer general counseling,family/community education, food parcels/grants/income generation, HIV prevention andtesting. This probably reflects the needs of thepatient population referred to these types ofprovider, suggesting that the palliative-only serviceprovides a more end-of–life focus (i.e. hospice) whilethe integrated service cares for a wider disease-spectrum population. However, it is not possible forpalliative-only services to care for all dying patients,and integrated services should be able to offeradvanced disease care (including opioids) for thosewho need it, and further research is required to mapreferral criteria for the management of complexcases which may require a more specialist palliativecare setting.
Antiretroviral therapy
Of the sample, six had no local access to ART fortheir patients, although all were PEPFAR countries.ART is an essential complement of palliative care,
even for those with late-stage infection and aninadequate response to therapy (14). While it is notnecessary for all sites to provide ART, it should beavailable for co-management between providers.Also, all sites should have access to the full range ofpain and symptom-controlling drugs and trainedstaff to provide skills in managing the side effects oftherapy and immune reconstitution events amongART-referred patients, as the majority of respondentsdid not provide ART for their patients but workedwith ART sites to gain access.
Patient population
The data show that the palliative-only services seesignificantly fewer patients, and that they are morelikely to be prescribed opioids while on service. This is unsurprising as specialist palliative careusually offers more detailed assessments, offerslonger contact per consultation, and if more patientsare prescribed opioids then closer monitoring isrequired. Also, as these patients are likely to benearer to the end of life, their needs can be expectedto be greater, as are those of the family. Therefore, it is essential to recognize that the smaller number of patients, while not reflected in smaller staffnumbers, is likely to be a function of the type of care provided and patient need, a view supported by the data describing service components and the proportion of patients prescribed opioids.However, the possibility that the data might suggestunder-use of opioids in integrated services cannot be discounted, particularly as these staff aresignificantly less likely to be palliative-trained.
Staff skills
While the number of staff did not differ in line withthe site patient population size, the proportion ofpalliative-trained staff was significantly lower for the integrated NGOs. While it is expected that anintegrated service has more components of care and so fewer palliative-specific staff, it is importantthat all staff can recognize palliative need and canprovide generalist palliative care during their patientinteraction, and refer appropriately, and so werecommend that all staff in an integrated servicehave at least some basic training. The number ofstaff able to prescribe did not differ betweenservices, which suggests that there are adequatenumbers of staff on service in integrated serviceswho could prescribe if they received adequatetraining in the assessment and management of pain.
Discussion
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 32
Analgesia and symptom controlling drugavailability
Firstly, looking at Step 1 analgesics, it is concerningthat even among these participating a significantnumber had problems in accessing Step 1analgesics. These are the least complex in terms of legislative bureaucracy and control, and sochallenges here suggest an inability to even begin to use the WHO ladder with certainty of continuity.Also, a small number of services were unable todispense Step 1 analgesics, and while it is notnecessary for all services to dispense Steps 2 and 3 (e.g. South African hospices tend not to dispenseopioids), the prevalence of pain and lack of policyrestraints suggest that any site should be able toprovide Step 1 analgesia.
Looking at Step 2 and 3 analgesics, both weredispensed by fewer sites and supply was anincreasing issue. Less than half the sites werecurrently prescribing opioids of any strength, andthose that did were mainly relying on Joint MedicalStores and Government Hospital pharmacies. Clearly,while reliance is on these sources, any strategy toincrease the number of providers must take accountof how best to assist these centers in offeringcontinuing supply. The data identified a number ofalternative methods, such as direct importation fromthe UK, and these centers should be investigatedmore closely in the search for reliable mechanisms of supply.
Neuropathic pain is a common, distressing andchallenging presentation among people with HIVdisease, and can be a result of the underlyingdisease or a side-effect of antiretroviral therapy. The most effective drugs, such as Gabapentin, areexpensive, and this is reflected in the low number of services that cited its use. Antiemetics andanxiolytics are also essential drugs in themanagement of patients with HIV disease, andfurther problems were identified with these both inavailability and supply continuity. Although opioidsoften have an anxiolytic effect, they should alwaysbe available for patients with advanced disease.Nausea and vomiting are common side effects ofboth opioid and ART use, and so antiemetics shouldalways be available. The data demonstrate somesystemic problems that suggest that opioid supplyissues are not solely related to this class of drugsbut are compounded by the legislative framework,
and that less controlled drugs such as antiemeticsexperience similar problems. Therefore, whilelobbying for opioid availability is a clear andessential task, there are issues beyond this thatspeak to drug supplies across the formularyspectrum.
The service perspective on opioidaccess: factors hampering provision,expanding access and facing challenges
The sample represents diverse countries in terms ofprogress towards opioid availability for a true publichealth approach to palliative care provision, from the well-recognized Ugandan experience, thegovernmental/hospice links across South Africa, to the challenges of Ethiopia. However, it is notablethat despite these significant differences, the dataoffers common themes to guide a strategic approachto opioid scale-up. To aid identification of feasibleand appropriate strategies for opioid expansion, the data have been integrated from Tables 10-12demonstrating the commonalities across themes and countries (See Figure 2).
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 33
Figure 2 Challenges and responses: data integration
Factors hampering roll out & challenges
PoliticalStore supplies are unreliable Lack of political willMotivating MoH Lack of national policyBureaucracy
ClinicalProfessionals lack knowledge on HIV pain,assessment, management Professionals fear opioidsLack of professional trainingLack of clinician interest in the dying Public opioid fear
Site-specificLack of storage facilitiesRural distance from suppliers Specialist palliative care excludes otherorganisations
ResourcesLack of prescribers and pharmacistsCostsLack of facilities to follow patients home
Suggested responses & solutions to challenges
PoliticalAdvocacy to MoH to raise awareness Public educationChange prescribing rules PWA lobbyingGovernment take responsibility for centralpurchase & distributionLicense nurses to prescribe Legislative change
ClinicalFocus on training palliative not supportive careFocus on training in opioid use in HIV not just cancerGraft onto existing providers Provide a shorter prescribing course for non-specialists Better HBC training
Site-specificCloser collaboration with doctors Improve clinical training Better clinical supervisionAccess to state pharmaciesRoll-out to rural areasImprove primary / secondary integration Improve networking with existing prescribersIncrease hospice capacityBetter pharmacy links More storage cupboards
ResourcesIdentify sources of opioid fundingMore pharmacists Evaluation of opioid expansion
Discussion
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 34
The INCB competent authorities and provider data:common goals and disparate perspectives It is very illuminating to compare the data from theprovider sample to the INCB sample. Although thiscould only be conducted for 5/12 countries, thecontrast in the data suggests some conflicting viewson the current provision of opioids.
Advocacy for greater access
A first point is that despite the need to lobby throughgovernment and achieve policy, legislative andbureaucratic change, it was extremely difficult forAPCA (the principal advocacy body in Africa) to evenidentify and then make contact with INCB competentauthorities in the majority of countries.
Second, among INCB competent authorities, themajority felt that a) the current bureaucratic processworks well and, b) that there are adequate numbersof providers currently.
Third, it is important to recognize that any expansion in opioid availability carries implicationsfor the regulatory bodies (i.e. the Ministry and INCB competent authorities), and these resourcerestrictions were noted by the respondents. There was a far from clear view that expansion was possible, with fears expressed that the currentcadre of prescribing professionals should be furthertrained and improved before more prescribers are trained. Indeed, the regulatory and legislativeframeworks were described by INCB competentauthorities as ‘enabling’, with many commentsfocusing on the weaknesses of existing prescribing staff.
However, despite these concerns, it should be noted that there were important areas of congruencebetween care sites and INCB competent authorities.These were: recognition that legislation has caused a reluctance to prescribe opioids; the need to reviewmedical training curricula; and a need for an increasein medical school intake.
Drug availability: INCB competentauthorities and site views
The availability of drugs, both opioids and othersymptom-controlling drugs, was a constant themethroughout the data. However, the integration ofdata from care sites and INCB competent authorities
highlights a disparity in the understanding of theavailability of specific drugs. Table 14 demonstratesthat in every country, the INCB competent authoritynamed a drug that was not listed by any service inthat country. It may be that the low number ofrespondents in some countries led to an under-reporting of some drugs at sites, but these siteswere identified by APCA as the most prominent andaccessible palliative care providers, and if they donot have access then this suggests under-supply.
Limitations
There are several limitations to our findings. Firstly,the lists of potential contacts may have excluded anumber of providers, but was composed of everyservice known to the funders, research centre andAPCA, and so we believe it was an inclusive andexhaustive recruitment procedure.
Secondly, significant difficulties were experienced in the data collection phases, mainly logisticalchallenges (including failing power, telecommuni-cations, lost emails and unobtainable contacts) thatmay have reduced the response rate. The significantchallenges of undertaking primary research in Africa,which are well recognized (15), were compounded byour aim of collecting data in 12 countries.
Thirdly, the sample was weighted towards SouthAfrica, and although it would be useful to comparethe findings according to country, there are currentlyinsufficient operational services to allow this. The low number of palliative care providers andpatchy coverage disallow the potential to generalizefrom a random sample, and therefore we attemptedto contact all services according to the APCAClassification (Appendix 1).
Fourthly, the focus is solely on opioids. As a definingfeature of palliative care that separates it from those services unable to control pain this is useful.However, opioids alone do not constitute a palliativecare service. It is not possible to deliver a fullinvestigation of palliative care in this study, andother data sources are available. The focus will becentral to delivering the stated outputs. A furtherexclusion is education, an important activity thatcannot be given full consideration. It is howeverincluded as a variable.
The INCB competent authorities and provider data: common goalsand disparate perspectives
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 35
Fifth, the inclusivity and thoroughness of the contact list was central to sampling and thegeneralisability of the data. We designed the list ofpotential participants in collaboration with countryrepresentatives to ensure that all relevant people are involved. We acknowledge that in South Africaopioids are “essential drugs” and as such are usuallyavailable in public health care facilities. The scope of this small-scale exercise did not allow all suchfacilities to be included and focuses instead on theperspective of palliative care services that may or may not have access to opioids.
Conclusion
A key finding from this study has been that whilethere are common issues raised by services andINCB competent authorities, it is clear that these key stakeholders have concerns regarding thepotential roll-out of opioids. A number of verypractical suggestions have been made, all of whichmust be taken into account in any strategic plan toenhance pain relief, as strategies that target changein the domains of education, resources, bureaucracy,legislation and provider sites cannot achieve thegoal in isolation.
The data suggest similar numbers of clinical staffingand different domains of care between integratedand palliative-only services, while the latter offerscare to fewer patients with a greater likelihood ofopioid use and staff who are trained in palliativecare. Each may have its merits, and further attentionshould be paid to networks of referral to ensureaccess appropriate to patient need, as well as thedevelopment and use of multi-dimensional outcome evaluations to appraise the resourceimplication costings in the light of varying outcomes.The question of education has not been addressed inthis study, and was a constant theme in discussionof solutions to opioid use. The educative role of‘specialist’ centers should not be underestimated,and evaluative studies should take account of theeducation activities and outcomes of these services.
Finally, previous work reviewing evidence andoutcomes for palliative care in Africa has identifiedthe need to balance quality and coverage. This study shows that opioid expansion needs tobalance supply and skills: there are currently notenough staff to prescribe and supply is unreliable,and any efforts to expand supply should ensure that it does not weaken current systems.
Recommendations For practitioners
1) While the presence of both specialist andintegrated centers should be encouraged, it is essential that each can offer the basicservice elements of the other when needed.Examples of this from our data are expansion of bereavement care and family support inintegrated services, and economic supportactivities in palliative-only centers. However,this expansion of core skills and servicecomponents should occur with the proviso that specialist palliative-only centers havereferral criteria and capacity to offer care formore complex cases.
2) Referral networks between ART sites andpalliative care services should ensure that notonly are patients under palliative care referredfor ART, but that mechanisms of clinical supportand consultancy are offered so that ART sitescan access palliative care as treatment isinitiated and continued.
3) With the wide range of distressing andburdensome HIV and treatment-relatedsymptoms, practitioners should remember toassess and treat the full spectrum throughoutthe disease trajectory including ART treatment.Also, any side-effects of opioids must beconstantly monitored and controlled, and drugsmade available to achieve this.
4) Where opioid access is poor, networks should be established with current hospice and governmental providers to establish routesfor dispensing.
5) Rural and HBC services should consider theirpotential routes to palliative care drugs whenarranging palliative care training for their staff,as the management of spiritual and emotionalpain cannot be achieved without themanagement of physical pain.
For educators
6) All services, whether palliative-only, integratedNGO or government facilities, must ensure thatall clinical staff are trained in palliative care to a basic agreed level. This would assist staff toassess palliative care needs, to provide general
The INCB competent authorities and provider data: common goalsand disparate perspectives
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 36
palliative care, and be aware of when to makeappropriate referrals for specialist input.
7) Training and education providers should formcollaborative teaching activities with currentclinicians. Those in practice require ongoingprofessional education to improve the paincontrol needs of those living with HIV, and tomeet the needs of the dying.
8) Training and education providers should formcollaborative teaching activities with futureclinicians. The inclusion of palliative care inmedical school curricula should be a goal for all countries.
9) Education must take a long-term view of theprocess of teaching, and mechanisms put inplace to ensure follow-up to support theapplication of skills learned.
10) Shorter palliative care courses that focus on prescribing should be considered for current clinicians.
11) Educators need to redouble efforts to addressthe public fears of opioids. A potential means to achieve this may be through the existingsignificant global networks for HIV advocacygroups. Currently the issues of palliative careand opioid use are not championed by peopleliving with HIV/AIDS.
12) There may be educational opportunities to work with INCB competent authorities todemonstrate the successes of opioid use and the current limitations that could beaddressed. Such consultation may also offerINCB competent authorities an opportunity toshare their concerns. Interactive education and sharing of viewpoints may offer betterpotential for feasible and acceptable strategiesfor opioid expansion.
For funders
13) Funders must take account of the high burdenof pain and symptoms that affect quality of life and allocate resources to ensure that these manageable problems are adequatelycontrolled.
14) Patients should have local access toantiretroviral therapy at all services that offerpalliation whatever disease stage the servicefocuses on. Referral and co-management carepathways should be in place to ensure thateven if palliative care and therapy are notavailable at the same site, they are co-ordinated to ensure that they can beintegrated across services.
15) Currently, palliative-only services see fewerpatients. While not all people living with anincurable life-limiting disease should requirespecialist palliative care, and not all people atthe end of life should or could access hospicecare, resources are required to increase thecapacity of these institutions to enhance theireducative, advocacy and specialist role forcomplex case management.
16) Funding for clinically trained staff is essential inHBC HIV sites, as opioids cannot be utilizedwithout staff able to prescribe.
17) Funders should consider the structuralrequirements of sites, e.g. the essential currentproblems of adequate opioid storage facilitiesand pharmacy facilities, in addition to staff andtraining costs.
18) Funders should consider those analgesicsbeyond opioids, i.e. neuropathic pain agents,which are costly, but essential for pain thatcannot be controlled with opioids.
For policy makers
19) The current opioid (and non-opioid) drug supplysystems experience a number of blockages anduncertainty in supply. Any expansion willrequire identification of the strongest routes,and to strengthen these further, beforeexpanded drug supply can be achieved.
20) While there is emphasis on expanding opioidsupply, this is being pursued to enhanceadherence to the WHO pain ladder. It is clearfrom the data that this requires attention to allsteps of the ladder, including in some casesprovision of Step 1 pain-relieving drugs.
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 37
21) Policies to expand opioid access must carefully balance the need for expansion with the threat of additional pressure onunreliable current purchase, production anddispensing. Expansion should not be at the cost of reliability.
22) Any strategy for expansion must take account of the concerns of INCB competent authoritieswith respect to regulation. Advocacy andlobbying must convince this essentialstakeholder group of the feasibility ofexpansion programs, as current INCBskepticism may prove a significant barrier.
23) The synergies of strengthening supply systems for opioids can also enhance othersymptom-controlling drugs, such as antiemeticsand anxiolytics, which are also essential for this population.
24) Any strategic approach to opioid expansionmust use a multi-pronged approach takingaccount of: supply (e.g. ordering and stocking,constistency of availability), legislation (e.g. regulations on storage and prescribing),education (i.e. ensuring that opioids are usedappropriately) and practical site-specificsupport (e.g. adequate numbers of trained and able-to-prescribe staff, funds and storagefacilities). Failure to address each of these areasis unlikely to achieve sustainable success.
25) Each country should undertake a wide-rangingconsultation process to appraise its currentlegislation and identify the potential to pilot and test safe, feasible and practical legislationfor the prescribing and dispensing of opioids.
26) Policy change, across the legislative andregulatory settings, can only be achievedthrough co-ordinated advocacy that takesaccount of governmental disinterest andprofessionals’ fears of opioid use.
27) Current funding goals to increase the numbersof patients accessing palliative care should takeaccount of the current limitations on opioid useand supply, and address the likely pressure onexisting infrastructure.
28) In order to address the current weaknesses insupply, and build capacity for expansion,greater emphasis and capacity needs to beplaced on training and employing pharmacists.
For researchers
29) In the light of different models of care andnumbers of trained staff and patients seenaccording to service model, multidimensionaloutcome evaluations are required, includingmeasurement of pain and symptoms.
30) Evaluative studies should compare botheconomic costing and levels of analgesiaavailable, taking account of comparativebaseline patient need across models.
31) Referral criteria and care networks should beexamined to understand the movementbetween sites as patients move up and downthe pain ladder.
32) All strategies and programs to expand opioiduse should be evaluated to ensure that lessonscan be replicated/adapted for use in other sites.
33) Longitudinal evaluation of education should beconducted to measure practice outcomes.
The INCB competent authorities and provider data: common goalsand disparate perspectives
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 38
We are grateful to Presidents Emergency Plan forAIDS Relief for funding this study, to the members of the US Office of the Global Co-ordinator andMembers of the USG Palliative Care TechnicalWorking Group who gave useful input and commentson protocol drafts, and to all the sites and INCBcompetent authorities that participated.
The participating sites were:
AFXBAIDS Care Training and Support (ACTS) InitiativeAssociacao Nacional dos Enfermeiros deMocambique (ANEMO)Bamalete Lutheran HospitalBreede River HospiceCamdeboo HospiceCatholic AIDS ActionCatholic Diocese of Ndola, Integrated AIDSProgramChatsworth Regional HospiceChipata DioceseCHU de COcodyCoast HospiceCotlands Western CapeCradock Hospice (Good Samaritan Home)Eldoret HospiceEstcourt HospiceFederal Medical Centre, Abeokuta, Hospice andPalliative Care ServicesGolden Gateway HospiceGood Shepherd HospiceGrahamstown HospiceHighway HospiceHoly Cross AIDS HospiceHospice Africa UgandaHospice East RandHospice RustenburgHospice ViljoenskroonHowick HospiceJOY Hospice (Deliverance Church MedicalServices)Kara-Ranchod HospiceKara Counseling and Training TrustKhanya Hospice AssociationKisumu Hospice and Palliative CareKitovu Mobile AIDS Home Care and OrphansProgramKNYSNA HospiceLadybrand HospiceLittle Hospice HoimaMeru Hospice
Mildmay InternationalMMM Counseling and Social Service CentreMobile Hospice MbararaMoretele Sunrise HospiceMother of Mercy Hospice TrustMuheza Hospice CareNairobi HospiceNyeri HospiceOcean Road Cancer InstitutePalliative Care InitiativePASADAPretoria Sungardens HospiceRadio and Oncology Centre, Ahmadu BelloUniversity Teaching HospitalRays of Hope Hospice JinjaSelian Lutheran Hospital HospiceSouth Coast HospiceSt Joseph's Care and Support TrustSt Nicholas Children's HospiceStellenbosch HospiceSWAA-RwandaTapologo HospiceTikondane Home-Based Care FoundationTygerberg Hospice
Acknowledgements
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 39
Our mission is to produce cutting edge innovativeresearch to improve care for patients and familiesaffected by progressive life limiting disease, anddiscover more humane and effective care andtreatment. We have special expertise in those groupswho have been neglected or who have problems wecontinue to struggle to alleviate.
The Department is multi-professional, comprising 2 clinical Professors, 2 Clinical Senior Lecturers, 3 Lecturers, 2 Senior Research Fellows and around20 multi-professional research, education andsupport staff and consultants in the three mainhospitals to which our Medical School is partnered,Guy’s and St Thomas’ NHS Trust, and King’s CollegeHospital. We also have collaborations and sharedappointments with many palliative care teams,hospices and related services in the UK and overseasand with colleagues in Schools throughout King'sCollege London, including Medicine, BiomedicalSciences, Dentistry, Nursing and Midwifery, Law andEthics, the Institute of Psychiatry and theHumanities.
Our portfolio of work in palliative care research inSub-Saharan Africa, and our history of research intocare for people with non-malignant diseasesincluding HIV/AIDS, has resulted in a number ofteaching and research projects in the region,including the generation and appraisal of originalresearch.
Department of Palliative Care, Policy and Rehabilitation, King’s College London
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 40
The mission of the African Palliative Care Association(APCA) is to promote and support affordable andculturally appropriate palliative care throughoutAfrica. APCA was provisionally established inNovember 2002, and formally established in Arusha,Tanzania, in June 2004. Its aim is to contribute to theAfrican response to the HIV/AIDS epidemic byscaling-up palliative care provision across Africathrough a culturally appropriate public healthapproach that strives to balance quality withcoverage. Its broad objectives are to:
Promote the availability of palliative care for all inneed, including orphans and vulnerable children.
Encourage governments across Africa to supportaffordable and appropriate palliative care which isto be incorporated into the whole spectrum ofhealth care services.
Promote the availability of palliative care drugsfor all in need.
Encourage the establishment of national palliativecare associations in all African countries.
Promote palliative care training programmessuitable for African countries.
Develop and promote quality standards inpalliative care training and service provision for different levels of health professionals andcare providers.
To achieve these objectives, APCA employs a fourfoldapproach in their work that includes:
1. Working in collaboration with thoseorganisations and individuals championingpalliative care service provision in Africa toensure governments and other internationaldonors accept palliative care as a vitalcomponent in the care of people with life-limiting illnesses (including HIV/AIDS) andincorporate budget lines for dedicated fundingthat will be used to build palliative care capacityacross the region.
2. Providing technical assistance to non-governmental organisations and Faith-basedorganisations working on HIV/AIDS to helpthem integrate palliative care into existing work
programmes, thereby ensuring palliative care isrecognized as part of the spectrum of responsesfor effective HIV/AIDS management.
3. Supporting identified champions of palliativecare (both individual and organisational) inpositions that can influence national policy so that:
Palliative care is included in the curricula for allmedical and nurse training, thereby increasing the existing skills base so that palliative careprovision in the region can be sustained;
Palliative care is incorporated into the nationalhealth plans of African governments;
Appropriate drugs for the alleviation of pain andto combat opportunistic infections are madeavailable.
4. Developing a mentorship programme for neworganisations with ongoing technical support to ensure initiatives are sustainable.
As implied above, APCA does not provide directclinical care to people living with life-limitingillnesses. Rather, it plays a facilitative role, workingcollaboratively with existing and potential providersof palliative care services to help expand the scale ofservice provision by training existing and potentialservice providers, providing support for effectiveadvocacy work and offering a mentorship program tosupport emerging initiatives; and to improve thequality of care provision by the introduction of aquality assurance and standards of care program.
(2) Mathews WM, Chrisopher MD, McCutchan JA,Asch S, Turner BJ, Giffird AL, et al. Nationalestimates of HIV-related symptom prevalencefrom the HIV Cost and Services UtilizationStudy. Medical Care 2000;38(7):750-62.
(3) Solano JP, Gomes B, Higginson IJ. A comparisonof symptom prevalence in far advanced cancer,AIDS, heart disease, chronic obstructivepulmonary disease (COPD) and renal disease.Journal of Pain and Symptom Management2006, 31 (1):58-69.
(4) WHO. Palliative Care. [cited 5 A.D. Mar22];Available from: URL:http://www.who.int/hiv/topics/palliative/PalliativeCare/en/
(5) Crowe S. Home truths. Nursing Times2001;97(39):26-7.
(6) Harding R, Easterbrook PE, Karus D, Raveis VH,Higginson IJ, Marconi K. Does palliative careimprove outcomes for patients with HIV/AIDS?A systematic review of the evidence. Sexually Transmitted Infections 2005, 81: 5-14.
(7) WHO. Cancer pain relief and palliative care. pdf1990 [cited 5 A.D. Mar 23];Available from: URL:http://www.wpro.who.int/pdf/pub/84/125.pdf
(8) Harding R, Higginson IJ. Palliative Care in Sub-Saharan Africa: an appraisal of reportedactivities, evidence and opportunities. Lancet 2005, 365:1971-1977.
(9) Harding R, Stewart K, Marconi K, O'Neill JF,Higginson IJ. Current HIV/AIDS end-of-life carein sub-Saharan Africa: a survey of models,services, challenges and priorities. BioMed Central Public Health 2003;3(33).
(10) Harding R, Molloy T, Easterbrook PE, Frame K,Higginson IJ. Is antiretroviral therapy associatedwith symptom prevalence and burden?International Journal of STD & AIDS. 2006;17: 400-405.
(11) Easterbrook P, Meadway J. The changingepidemiology of HIV infection: new challengesfor HIV palliative care. Journal of the RoyalSociety of Medicine 2003;94:442-8.
(12) Selwyn P. Why should we care about palliativecare for AIDS in the era of antiretroviraltherapy? Sexually Transmitted Infections2005;(81):2-3.
(13) Saunders CM. Foreword. In: Doyle D, Hanks G,Cherny N, Calman K, editors. Oxford Textbook ofPalliative Medicine. 3rd ed. Oxford: OxfordUniversity Press; 2004. p. xvii-xx.
(14) Gandhi T, Wei W, Amin K, Kazanjian P. Effect ofmaintaining highly active antiretroviral therapyon AIDS events among patients with late-stageHIV infection and inadequate response totherapy. Clinical Infectious Diseases2006;42:878-84.
(15) Volmink J, Dare L. Addressing inequalities inresearch capacity in Africa. British MedicalJournal 2005;331:705-6.
References
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 42
APCA's Tool for the Classification of Palliative Care Activities
Appendix 1
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 43
Level 1Not palliative care
Level 2
Level 3
Level 4Centre of Excellence
1. Relies mainly on community health workers (CHW)/volunteers2. Includes basic administrative structures3. Provides supportive care4. Does not provide basic OI and/or pain assessment and management services
1. Relies on CHW/volunteers and part-time qualified health professionals2. Includes basic administrative structure and procedures (e.g. job descriptions)3. Provides support and basic clinical services for OI, WHO level 1 pain assessment
and management
1. Relies on CHW/volunteers and full-time qualified health professionals2. Includes managerial and administrative structure and procedures
(management, technical and support staff3. Relies on multidisciplinary team approach for service delivery4. Uses protocols for support and clinical services for OI and pain assessment
and management5. Provides support and clinical services for OI and at least WHO level 2 pain
assessment and management6. Manages a basic referral network for provision of essential palliative
care components
1. All the above2. Manages a proactive referral network3. Provide support and clinical services for OI and WHO level 3? pain assessment
and management4. Provide technical assistance and training to partner organisations5. Recognised palliative care champion
OrganisationalCapacity Level
Qualifying Criteria for Organisational Capacity Level
Notes
Expanding Pain Control in 12 African PEPFAR CountriesPAGE 44
African Palliative Care AssociationPO Box 72518Plot 850 Dr Gibbons RoadKampalaUgandaTel +256 414 266251Fax +256 414 266217Email: [email protected] www.apca.co.ug
NGO Registration Number 4231
Design by Strudel Communicationswww.strudelcommunications.co.uk