Palbociclib (PD 0332991): targetingthe cell cycle machinery in breastcancerAndrea Rocca†, Alberto Farolfi, Sara Bravaccini, Alessio Schirone &Dino Amadori†Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS,
Department of Medical Oncology, Meldola, Italy
Introduction: The cyclin D-cyclin-dependent kinases 4 and 6 (CDK4/6)-retino-
blastoma (Rb) pathway, governing the cell cycle restriction point, is frequently
altered in breast cancer and is a potentially relevant target for anticancer
therapy. Palbociclib (PD 0332991), a potent and selective inhibitor of
CDK4 and CDK6, inhibits proliferation of several Rb-positive cancer cell lines
and xenograft models.
Areas covered: The basic features and abnormalities of the cell cycle in
breast cancer are described, along with their involvement in estrogen
signaling and endocrine resistance. The pharmacological features of palboci-
clib, its activity in preclinical models of breast cancer and the potential
determinants of response are then illustrated, and its clinical development
in breast cancer described. A literature search on the topic was conducted
through PubMed and the proceedings of the main cancer congresses of recent
years.
Expert opinion: The combination of palbociclib with endocrine agents is a
very promising treatment and Phase III clinical trials are ongoing to confirm
its efficacy. Further, potentially useful combinations are those with drugs
targeting mitogenic signaling pathways, such as HER2- and PI3K-inhibitors.
Combination with chemotherapy seems more problematic, as antagonism
has been reported in preclinical models. The identification of predictive
factors, already explored in preclinical studies, must be further refined and
validated in clinical trials.
Keywords: breast cancer, cell cycle, cyclin-dependent kinase inhibitors, endocrine resistance,
palbociclib
Expert Opin. Pharmacother. (2014) 15(3):407-420
1. Introduction
Breast cancer is the most frequent cancer among women, both in developed anddeveloping regions, with an estimated 1.38 million new cancer cases diagnosed in2008 (23% of all cancers) [1]. About 200 women per 100,000 are diagnosed withbreast cancer every year in the USA, two-thirds of whom have estrogen receptor(ER)-positive tumors. ER-positive cancers are expected to increase in the nearterm (2009 through 2016), whereas ER-negative tumors show a more encouragingtrend, with a steady decrease of nearly 2% per year [2].
Treatment of metastatic breast cancer is palliative in nature, and advances in ourknowledge of the biology of this disease are fundamental to the identification of newtargets and the development of new active treatments.
Sustained cell proliferation is a hallmark of cancer [3], and cell cycle control isaltered in virtually all cancer cells, often as a result of abnormal oncogene productsor deletion or inactivation of tumor suppressor genes. Many anticancer agents aim
at disrupting the cell proliferation process, often ultimatelytriggering apoptosis. Improved knowledge of the cell cyclemachinery has led to identifying different families of kinaseswith specific important roles in the cell cycle [4,5], which arepotential targets for cancer therapy [6-8]. Among these, thecyclin-dependent kinases (CDKs) have a prominent role.This review summarizes the basic features of the cell cycle
and its abnormalities in breast cancer, describes their involve-ment in estrogen signaling and endocrine resistance and illus-trates the preclinical and clinical activity of palbociclib (PD0332991) (Box 1), a potent and selective inhibitor of CDKs4 and 6.
1.1 Cell cycle machinery and controlA broad molecular apparatus executes the cell cycle, and itsregulation is likewise complex [4,5,9,10]. The mammalian cellcycle is composed of four phases: a first preparatory G1 (gap1) phase, the S phase during which DNA synthesis takesplace, a second gap G2 phase and the mitotic M phase, fol-lowed by cytokinesis and the formation of two daughter cells.Although newborn cells re-enter the cell cycle, at some pointduring late G1 phase (called restriction or R point) [11], thecell cycle regulatory machinery must make a decision on theultimate fate of the cell: continue cycling, or exit active prolif-eration and enter a quiescent (G0) state [12]. The progressionof the cell cycle during G1 phase is the result of a balancebetween growth factors and growth inhibitors present in theextracellular environment, and this balance will ultimatelyaffect the decision of the cell cycle regulatory machinery, aprevalence of growth factors portending active cycling and aprevalence of growth inhibitors inducing entry into G0. TheG1 phase is therefore the most critical site of cell cycle control:if the cell passes the restriction point, then the rest of the cyclewill proceed automatically until cell division, independently
of growth- and inhibitory-factors, unless major damage occursto the dividing cell [12].
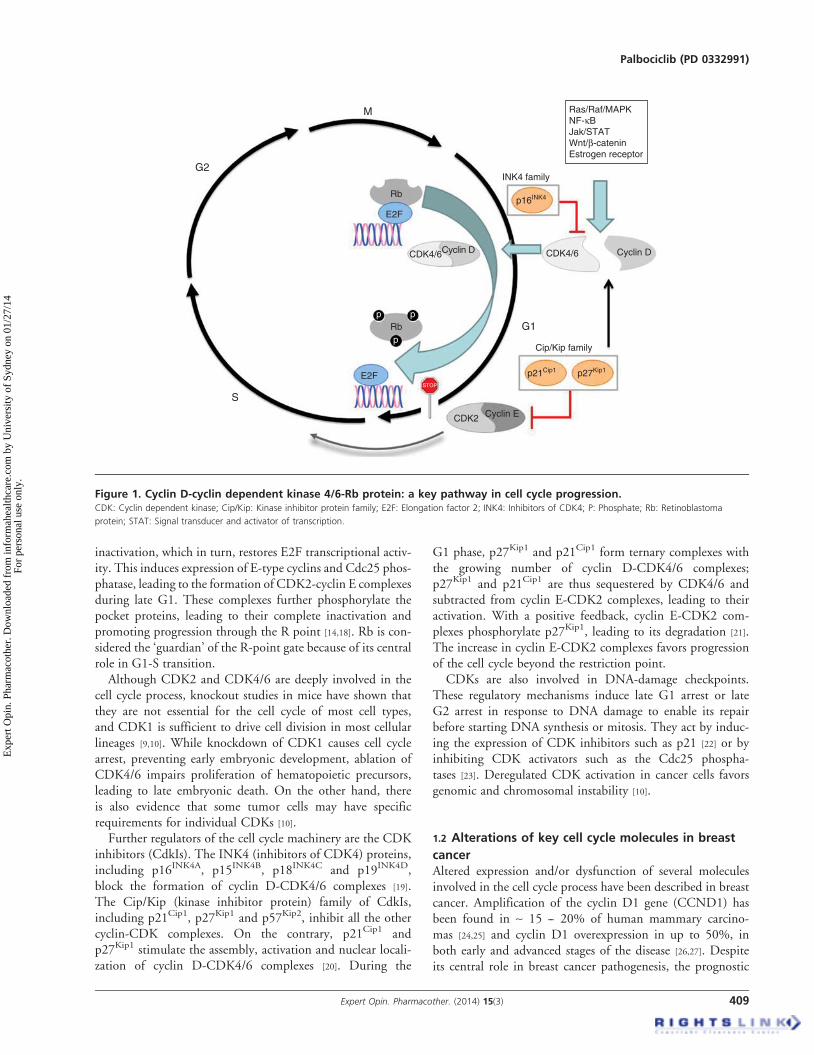
Major players in cell cycle regulation are a family of serine/threonine kinases, called cyclin-dependent kinases or CDKs,which act in conjunction with their regulatory subunits calledcyclins. In human cells, at least 13 CDKs have been described(only some of which are involved in the cell cycle) that inter-act with at least 25 cyclins, each CDK binding only one or afew types of cyclins [9,10]. As their name indicates, most cyclinsare synthesized in a cyclic way, only at specific times duringcell cycle, while CDK levels are more stable. As the kinaseactivity of CDKs is present only when they bind their cyclinpartner, the levels of the different types of cyclins affect theCDK-cyclin complexes that are active during specific phasesof the cell cycle. During G1 phase, mitogenic growth factors,acting through different signaling cascades (such as the Ras/Raf/MAPK pathway, NF-kB pathway, Jak/STAT pathway,hedgehog pathway, Wnt/b-catenin pathway, steroid hor-mones), induce the expression of D-type cyclins (D1,D2 and D3) that preferentially bind and activate two closelyrelated CDKs: CDK4 and CDK6, often referred to collec-tively as CDK4/6 due to their similar function [13].CDK4/6-cyclin D complexes sustain progression of cell cyclethrough the G1 phase and, in late G1, induce cyclin E synthe-sis and the formation of CDK2-cyclin E complexes, whichcontribute to progression through the R point and entryinto S phase (Figure 1) [14]. CDK4/6-cyclin D complexes aretherefore important mediators of cell cycle regulatory deci-sions, which make them potentially strategic targets for anti-cancer treatment. After crossing the R point, sequentialactivation of the other cyclins governs the cell throughoutthe entire cell cycle: E-type cyclins, binding CDK2, controlentry into S phase; A-type cyclins bind CDK2 for S-phaseprogression and subsequently CDK1 during G2; finallyB-type cyclins, binding CDK1, govern entry into mitosis.
The CDK4/6-cyclin D complexes carry out their functionon cell cycle by phosphorylating and thus inactivating theso-called pocket proteins: Rb (the product of the Rb --retinoblastoma -- tumor suppressor gene) and its relatedproteins p107 (RBL1) and p130 (RBL2). Rb and its cousinproteins, when present in an unphosphorylated state at thebeginning of G1, bind to transcription factors, primarily ofthe E2F family, inhibiting their transcriptional activity. E2Ftranscription factors are bound to the promoters of their targetgenes whose products mediate S-phase entry and mitosis [15,16];these include factors involved in subsequent cell cycle progres-sion, such as cyclin E, cyclin A and the CDK activator mem-bers of the Cdc25 phosphatase family [17]; factors involved inDNA replication, such as DNA polymerase a, proliferatingcell nuclear antigen (PCNA) and minichromosome mainte-nance 7 (MCM7); factors involved in DNA damage repair,such as Rad51; and factors involved in mitosis, such as cyclinB1 and CDK1. The CDK4/6-cyclin D complexes produceprogressive phosphorylation of the pocket proteins at serineand threonine residues during G1, leading to their gradual
Box 1. Drug summary.
Drug name Palbociclib (PD 0332991)Phase IIIIndication First-line advanced breast cancerPharmacologydescription
inactivation, which in turn, restores E2F transcriptional activ-ity. This induces expression of E-type cyclins and Cdc25 phos-phatase, leading to the formation of CDK2-cyclin E complexesduring late G1. These complexes further phosphorylate thepocket proteins, leading to their complete inactivation andpromoting progression through the R point [14,18]. Rb is con-sidered the ‘guardian’ of the R-point gate because of its centralrole in G1-S transition.
Although CDK2 and CDK4/6 are deeply involved in thecell cycle process, knockout studies in mice have shown thatthey are not essential for the cell cycle of most cell types,and CDK1 is sufficient to drive cell division in most cellularlineages [9,10]. While knockdown of CDK1 causes cell cyclearrest, preventing early embryonic development, ablation ofCDK4/6 impairs proliferation of hematopoietic precursors,leading to late embryonic death. On the other hand, thereis also evidence that some tumor cells may have specificrequirements for individual CDKs [10].
Further regulators of the cell cycle machinery are the CDKinhibitors (CdkIs). The INK4 (inhibitors of CDK4) proteins,including p16INK4A, p15INK4B, p18INK4C and p19INK4D,block the formation of cyclin D-CDK4/6 complexes [19].The Cip/Kip (kinase inhibitor protein) family of CdkIs,including p21Cip1, p27Kip1 and p57Kip2, inhibit all the othercyclin-CDK complexes. On the contrary, p21Cip1 andp27Kip1 stimulate the assembly, activation and nuclear locali-zation of cyclin D-CDK4/6 complexes [20]. During the
G1 phase, p27Kip1 and p21Cip1 form ternary complexes withthe growing number of cyclin D-CDK4/6 complexes;p27Kip1 and p21Cip1 are thus sequestered by CDK4/6 andsubtracted from cyclin E-CDK2 complexes, leading to theiractivation. With a positive feedback, cyclin E-CDK2 com-plexes phosphorylate p27Kip1, leading to its degradation [21].The increase in cyclin E-CDK2 complexes favors progressionof the cell cycle beyond the restriction point.
CDKs are also involved in DNA-damage checkpoints.These regulatory mechanisms induce late G1 arrest or lateG2 arrest in response to DNA damage to enable its repairbefore starting DNA synthesis or mitosis. They act by induc-ing the expression of CDK inhibitors such as p21 [22] or byinhibiting CDK activators such as the Cdc25 phospha-tases [23]. Deregulated CDK activation in cancer cells favorsgenomic and chromosomal instability [10].
1.2 Alterations of key cell cycle molecules in breast
cancerAltered expression and/or dysfunction of several moleculesinvolved in the cell cycle process have been described in breastcancer. Amplification of the cyclin D1 gene (CCND1) hasbeen found in ~ 15 -- 20% of human mammary carcino-mas [24,25] and cyclin D1 overexpression in up to 50%, inboth early and advanced stages of the disease [26,27]. Despiteits central role in breast cancer pathogenesis, the prognostic
significance of cyclin D1 overexpression is less clear [28].Cyclin D1-null mice have been shown to be resistant to breastcancers induced by the neu and ras oncogenes, while remain-ing sensitive to other oncogenic pathways, such as thosedriven by c-myc or Wnt-1 [29]. This has been attributed tothe fact that the neu-ras pathway is closely connected to thecell-cycle machinery by cyclin D1, and suggests potentialactivity of anti-cyclin D1-CDK4/6 agents in these tumors [29].The critical role of cyclin D1 in breast cancer has been
shown to be related to its ability to activate CDK4, and thecontinued presence of CDK4-associated kinase activity seemsnecessary to maintain breast tumorigenesis [30]. Amplificationof CDK4 gene is reported in about 15% of breast cancers,resulting in CDK4 protein overexpression, and is associatedwith high Ki-67 labeling index [31].Several breast cancer cell lines show homozygous deletion
of p16INK4A or p15INK4B, or low expression of these CDKinhibitors, while others have high expression levels associatedwith deletion or inactivation of Rb [32]. P21Cip1 expressionis frequently reduced as a consequence of TP53 mutation [32]
or MYC overexpression [33], and p27Kip1 expression is reducedas a result of HER2 amplification [34].Rb gene deletion or mutation is found in 20 -- 30% of breast
cancers, but Rb inactivation due to cyclin D1 overexpressionor p16INK4A inactivation is present in the majority of breastcancers [35]. While immunohistochemical studies of Rb expres-sion have yielded contrasting results, an Rb-loss gene signaturecan identify tumors with dysregulated Rb [35]. Maximal dereg-ulation of Rb target gene expression is observed in ER-negativebreast cancer, where it is devoid of relevant prognostic effectbut is associated with a better response to chemotherapy.Immunohistochemically detected Rb loss confirms this associ-ation in triple-negative breast cancer [36]. In ER-positive breastcancer Rb deregulation is rarer but confers poor prognosis [35].
1.3 Cell cycle, estrogen activity and endocrine
resistanceEstrogens stimulate cellular proliferation in the female repro-ductive tract and mammary gland, and play an important rolein breast cancer carcinogenesis [37] and breast cancer progres-sion. In normal breast epithelium [38], as well as inMCF-7 breast cancer cell lines [39], 17-b-estradiol binds tonuclear estrogen receptor alpha (ER-a), a ligand-dependenttranscription factor, inducing the expression of several genesincluding CCND1, coding for cyclin D1, and therefore, acti-vating CDK4/6 with subsequent Rb inactivation. Estradiol-bound ER-a can also bind other transcription factors, suchas members of the activation protein 1 (AP1), specificityprotein 1 (SP1) and NF-kB, to induce transcription of differ-ent sets of genes [40]. In addition, estradiol inhibitsthe expression of the p21Cip1 and p27Kip1 CDK inhibitorsand induces the expression of the CDK-activating phospha-tase Cdc25A [41], independently of D cyclin-CDK4function, both mechanisms contributing to sustain cell
proliferation. Furthermore, cyclin D1 has been shown tointeract directly with ER-a, activating its transcriptional func-tion independently of CDKs and estrogens [42].
Inhibiting ER-a inMCF-7 breast cancer cells using selectiveER modulators (SERMs) such as tamoxifen leads to cell cyclearrest in G1 and apoptosis as a result of reduced expressionof cyclin D and B, increased expression of p53 and p21Cip1
and loss of the prosurvival protein Bcl-2 [43]. The selectiveER downregulator (SERD) fulvestrant shows similar activitybut also induces accumulation of p130-E2F4 complexescharacteristic of quiescence and G0 arrest [44].
Aberrant expression of several molecules involved in cellcycle regulation and in estrogen and tamoxifen action mayinduce endocrine resistance. Overexpression of MYC sup-presses p21Cip1expression, favoring the formation of cyclinE1-CDK2 complexes and tamoxifen resistance [33]. CyclinD1 overexpression favors formation of cyclin D1-CDK4/6complexes, which sequester p21Cip1 and p27Kip1, allowingactivation of cyclin E1-CDK2 complexes and inducing tamox-ifen resistance, as shown in breast cancer cell lines [45] and inpatients with breast cancer [46-48]. Cyclin E1 overexpressionhas also been implicated in endocrine resistance [49]. Rb inacti-vation has resulted in tamoxifen and fulvestrant resistance inxenograft breast cancer models [50], and gene expression profil-ing studies on human breast cancer specimens have shown anassociation between Rb-dysfunction signatures and luminalB breast cancer subtype [51] or increased recurrence risk follow-ing tamoxifen therapy [50]. Reduced expression of p27 [34]
and cytoplasmic localization of p21Cip1 [52] have also beenassociated with endocrine resistance.
Other mechanisms of endocrine resistance, not primarilyinvolving alterations of molecules of the cell cycle machinery,may still implicate cyclin D-CDK4/6 activity as a mediatorof cellular proliferation [40,53] and therefore as a potential ther-apeutic target. Ligand-independent activation of ER-a mayoccur as a result of activation of receptor tyrosine kinases thatinduce phosphorylation of ER-a or its coregulators. Bidirec-tional cross-talk between ER-a and members of the epidermalgrowth factor receptor family, such as EGFR and HER2 [54,55],or the insulin-like growth factor receptor (IGFR) [56], havebeen extensively associated with the development of endocrineresistance. The same occurs with alterations of components oftheir downstream signaling pathways, such as MAPK/ERKand PI3K/Akt [57]. Estrogens also bind to G-protein coupledreceptor GPR30, located on the cell membrane, which medi-ates nongenomic effects, assembling with c-Src and otherproteins and activating Akt or ERK and their downstreamcascades (Figure 2) [58].
Several other mechanisms of endocrine resistance have beendescribed, including increased activity of transcription factorssuch as AP1 and NF-kB, alterations in ER-a coregulators,increased expression of survival molecules such as Bcl2, anddecreased expression of death factors such as BAK, BIKor caspases, aberrant miRNA expression and epigeneticalterations [40,53].
Resistance to aromatase inhibitors is not as well understoodat the molecular level, may differ, in part, from resistance toSERMs or SERDs and seems to involve the activation of cel-lular stress response and apoptosis [59]. In long-term estrogen-deprived breast cancer cell lines exhibiting hyperactivation ofthe PI3K pathway, the unbound ER has been shown to playa role in hormone-independent growth of these cells by acti-vating E2F transcriptional activity [60], a process mediatedby CDK4.
Given the plethora of mechanisms underlying endocrineresistance, the position of CDK4/6 downstream of multiplegrowth factors pathways and the preserved high CDK4/6activity and CDK4/6 tumor addiction in many cases [61], tar-geting CDK4/6 appears a promising strategy to overcomeendocrine resistance [62]. It has been shown that, in differentMCF7-derived models of spontaneous and acquired endo-crine-resistance, treatment with fulvestrant, although effec-tively downregulating ER-a, does not reduce the expressionof cyclin D and as a result does not lead to Rb dephosphory-lation and activation and to cell cycle arrest [51]. Treatment ofthese cell lines with the CDK4/6 inhibitor palbociclib hasresulted in effective Rb dephosphorylation and profoundinhibition of cell cycle progression, across all of the models
employed. In contrast to the quiescent state induced by fulves-trant in sensitive cells, palbociclib has been shown to inducecellular senescence, an irreversible cell-cycle arrest, indicatedby large, flat cellular morphology and b-galactosidaseexpression [51].
2. Palbociclib preclinical studies
As first-generation pan-CDK inhibitors showed modest clini-cal activity as single agents and considerable toxicity, subse-quent efforts have led to the development of more potentand selective small molecule CDK inhibitors [63,64].
2.1 Preclinical pharmacologyPalbociclib is an orally active, potent and highly selectiveinhibitor of CDK4 and CDK6, with IC50 values for CDK4/cyclinD1, CDK4/cyclinD3 and CDK6/cyclinD2 of 11, 9and 15 nmol/l, respectively, and low or absent activity againsta panel of 36 additional protein kinases, including CDK2,CDK1 and several tyrosine kinases and serine-threonine kin-ases. It is a pyridopyrimidine derivative, inhibiting CDK4/6by binding to the ATP site [65]. As Rb phosphorylation byCDK4 and CDK6 occurs specifically on serine residues
Ser780 and Ser795, the phosphorylation status of these sitesserves as a specific biomarker of CDK4/6 inhibition by palbo-ciclib. In cell cultures, reduction of Rb phosphorylationbegins 4 h after exposure, reaches a maximum at 16 h and iscompletely reversible after removal of the drug. Palbociclibis a potent inhibitor of cell proliferation, preventing progres-sion of the cell cycle from G1 into the S phase in Rb-positivecells of different tumor types, but showing no activity againstRb-negative tumor cells in vitro or in vivo [65]. This fact,combined with the exclusive G1 arrest even at very high con-centrations, is consistent with selective CDK4/6 inhibition asits only mechanism of action [65].In mouse xenograft models, palbociclib showed significant
antitumor activity in several tumor types, including breastcancer xenografts. In mice bearing MDA-MB-435 breast car-cinoma, antitumor activity was present only at doses yieldingcomplete suppression of Rb Ser780 phosphorylation through-out the entire treatment period, whereas resumption ofSer780 phosphorylation during the intervals between doseswas associated with treatment failure, indicating that totaltarget inhibition must be maintained between doses toachieve tumor regression. Substantial differences in dose(up to eightfold) were necessary to produce comparable effi-cacy in xenograft models with different sensitivity to thedrug [65]. Although palbociclib has a cytostatic effect ontumor cell cultures in vitro and does not induce apopto-sis [65,66], it has led to tumor regression in vivo, includingsome durable complete remissions. This could be attributedto the presence of a fraction of cells spontaneously dyingwithin tumors, or to the need for CDK4/6 as a survivalfactor by some tumors [65].
2.2 Sensitivity and resistance to palbociclibRb-negative breast cancer cell lines are resistant to palbocicliband are characterized, apart from loss of Rb, by an upregula-tion of p16INK4A and no appreciable cyclin D1 protein expres-sion. It appears therefore that they do not respond topalbociclib simply because they lack the palbociclib target,that is, active cyclin D-CDK4/6, because CDK4/6 is alreadyinhibited by the overexpression of p16INK4A
[67].Sensitivity to palbociclib was assessed in a panel of 44
human breast cancer cell lines, representative of the differentbreast cancer subtypes, to identify predictors of response [66].ER-positive cell lines with luminal features were the mostsensitive, and three-quarters of the genes highly expressedin sensitive lines were luminal markers, whereas none werebasal markers. Of 16 HER2-amplified cell lines, 10 were sen-sitive, and these generally had luminal (ER-positive) features.Cell lines with basal features were the most resistant. Highlevels of cyclin D1 and Rb, and low levels of p16 were pre-dictors of sensitivity to palbociclib. Although the drug hadno effect on total Rb levels, Rb phosphorylation decreasedafter drug exposure in sensitive cells. Resistant cells usuallyhad low baseline levels of Rb, and in the few resistant lineswith detectable levels of Rb, its phosphorylation did not
decrease after drug exposure. Therefore, the presence of Rbappears to predict response to palbociclib in luminal, ER-positive breast cancer cell lines but not in basal cell lines. Ithas been speculated that failure of palbociclib to dephos-phorylate Rb could be due to CDK4/6 mutations, to agreater dependence on CDK1/2-cyclin E interactions or toa loss of negative regulators of CDKs, but these hypothesesremain to be confirmed in breast cancer [66]. However, resis-tance to palbociclib due to p27 downregulation and CDK2reactivation has been demonstrated in models of acute mye-logenous leukemia [68]. Resistance to palbociclib in breastcancer cell lines with basal features appears frequently relatedto a lack of Rb, and loss of Rb has been described in basal-likebreast cancer [69] and can result in epithelial-mesenchymaltransition [70].
Further investigation of the mechanisms of response andresistance to palbociclib was conducted on a panel of breastcancer cell lines using Rb knockdown experiments [67]. Rb sta-tus appeared to play a prominent role in acute response to pal-bociclib, but compensatory mechanisms controlling E2Factivity would also seem to influence response, especiallylong-term. Although Rb knockdown resulted in a modestincrease in baseline proliferation, palbociclib still exerted a par-tial cytostatic effect (albeit much lower than in Rb-proficientcells), suggesting that Rb protein is not essential for responseto palbociclib. On the other hand, E2F overexpression bytransduction yielded complete resistance to palbociclib, inde-pendently of Rb status. This suggests that E2F transcriptionalcontrol may be partly independent of Rb protein and poten-tially mediated by p107 protein, and that palbociclib mightcause partial repression of E2F-target genes by activatingp107. Nonetheless, while Rb-proficient cells may become tem-porarily resistant to palbociclib after prolonged exposure, theyusually remain sensitive to deferred second rounds of treat-ment. Loss of Rb function normally marks the evolution totrue, long-term resistance. Cell populations retrieved afterlong-term exposure to palbociclib often show elevated p107protein expression as well as increased CDK2 protein and/orloss of p21Cip1 and p27Kip1. In this context, loss of Rb functionleads to increased transcription of the E2F-target genes cyclinA and E, which activate CDK2 and drive cell cycle indepen-dently of CDK4/6 in some tumor cells [67]. On the contrary,Rb function is necessary for the induction of senescence bypalbociclib, wherein tumor cells permanently exit the cellcycle [67].
CDK4 inhibition has also been reported to induce apoptosisin colon cancer cell models by causing degradation of theNF-kB suppressor protein IkB, with subsequent translocationof RelA (principal component of NF-kB) from the cytoplasmto the nucleoplasm and the nucleolus, and repression of NF-kB-driven transcription of anti-apoptotic genes [71]. It has alsobeen shown that inhibition of CDK4 sensitizes pancreatic can-cer cells to TRAIL-induced apoptosis via downregulation ofsurvivin [72]. The role of these processes in breast cancer remainsto be assessed.
2.3 Combination of palbociclib with other targeted
agentsCombinations of palbociclib with trastuzumab or withtamoxifen were tested in HER2-amplified cell lines and inER-positive cell lines, respectively [66]. Both combinationswere synergistic, with a mean combination index < 1 acrossclinically relevant concentrations of the drugs. Furthermore,tamoxifen-resistant MCF7 cell lines were sensitive to palboci-clib monotherapy, and palbociclib partially restored sensitiv-ity to tamoxifen in resistant lines [66]. This is consistent withother observations of the potentially enhanced endocrinesensitivity of CDK inhibition [73].
A sequential combination of palbociclib with a PI3K inhib-itor (GS-1101, inhibiting PI3K-d, whose expression isrestricted to cells of the hematopoietic lineage) yielded arobust apoptotic response in lymphoma cell lines [74]; studiesare also warranted in combination with other PI3K inhibitorsin breast cancer.
2.4 Combination of palbociclib with
chemotherapeutic agentsAlthough the synergism between palbociclib and endocrineagents such as tamoxifen or anti-HER2 drugs such as trastu-zumab is well documented in preclinical models, the associa-tion of palbociclib with chemotherapeutic agents is moreproblematic. Indeed, most chemotherapeutic agents act spe-cifically on proliferating cells, and their combination with acytostatic agent may be ineffective. In genetically engineeredmouse models of a HER2-positive, Rb-competent breast can-cer (MMTV-c-neu), palbociclib showed antitumor activity asa single agent, but the combination of palbociclib with carbo-platin or with doxorubicin proved less active than single-agentcarboplatin or doxorubicin [75]. This antagonism was not seenin engineered models of a basal-like, Rb-incompetent breastcancer, where palbociclib showed no antitumor effect as a sin-gle agent and did not reduce the activity of carboplatin whengiven in combination. The same authors demonstrated theability of palbociclib to protect an immortalized human fibro-blast cell line from the toxicity of a variety of DNA-damagingagents, such as carboplatin, doxorubicin, etoposide and camp-tothecin, or from the antimitotic agent paclitaxel, and toprotect the bone marrow from carboplatin-induced myelo-suppression in mice, highlighting the potential use of palboci-clib as a chemoprotectant of normal tissues to overcome thedose-limiting toxicity of many chemotherapeutic agents.
Further experiments in Rb-proficient, triple-negative breastcancer cell lines and xenograft mice models showed that,although the combination of palbociclib with doxorubicinyielded an additive cytostatic effect, palbociclib antagonizeddoxorubicin-mediated cytotoxicity, greatly reducing theinduction of apoptosis [76]. As a result, palbociclib maintainedviability of Rb-proficient cells treated with doxorubicin,resulting in a recurrent population of cells after doxorubicinexposure. Again, these effects were not seen in Rb-deficient,
triple-negative breast cancer models. Anthracyclines induceDNA damage, and palbociclib can shift DNA repair fromhomologous recombination to non-homologous end joining,a more error-prone mechanism that could contribute totumor progression [77]. Pretreatment or co-treatment oftriple-negative breast cancer cell lines with palbociclib alsoshowed antagonism to paclitaxel, a microtubule-stabilizingagent that acts by promoting mitotic catastrophe [77]. In con-trast, a short exposure to palbociclib to synchronize cells priorto paclitaxel treatment resulted in increased cytotoxicity.
2.5 Further potentially useful or deleterious effectsPalbociclib has been shown to reverse epithelial dysplasia asso-ciated with abnormal activation of the cyclin D-CDK4/6-Rbpathway, highlighting a potential role of this molecule as achemopreventive agent [78].
Other studies raise some potential concerns about CDK4/6inhibition in specific experimental models. Palbociclib hasbeen shown to induce epithelial-mesenchymal transition andenhance invasiveness in pancreatic cancer cell lines by activatingSmad-dependent TGF-b signaling. Senescent fibroblast overex-pressing CDK inhibitors also promote tumor growth via theparacrine production of high-energy mitochondrial fuels, suchas L-lactate [79].
3. Palbociclib clinical development
A Phase I dose escalation study of palbociclib was conductedwith two different schedules: daily treatment for 2 weeksfollowed by 1 week off treatment (schedule 2/1) [80] and dailytreatment for 3 weeks followed by 1 week off (schedule3/1) [81]. Eligible patients had Rb-positive (assessed by immu-nohistochemistry) solid tumors or non-Hodgkin’s lymphomarefractory to standard therapy or for which no standardtherapy was available.
For the first schedule, a total of 33 patients were enrolled.The dose escalation sequence progressed from 100 to150 mg/day, and then to 225 mg/day, the maximum admin-istered dose at which two dose-limiting toxicities (DLTs)occurred: one case of grade 4 neutropenia and thrombocyto-penia and another of grade 3 neutropenia, resulting in a delayin the initiation of cycle 2. The dose was then reduced to200 mg/day, and this dose level was expanded to a total of20 patients and selected as the MTD. Four DLTs occurredat this dose level, all consisting in grade 3 neutropenia, withor without grade 3 thrombocytopenia, delaying the initiationof the subsequent cycle. Non-hematological toxicity wasgenerally mild, with only five grade 3 adverse events (AEs)reported overall and no treatment-related grade 4 toxicity.The most common non-hematological AEs included fatigue,nausea, diarrhea and constipation, with some patients alsoexperiencing vomiting. Of 31 patients assessable for response,1 patient with testicular cancer had a partial response and anadditional 9 (29%) with different types of tumors had stable
disease, which in 3 cases lasted beyond 10 cycles oftreatment [80].Forty-one patients were enrolled for the second schedule,
with a sequential dose escalation ranging from 25 to150 mg/day [81]. Again, the major AEs were related to myelo-suppression. Overall, 5 patients experienced DLTs, allconsisting of neutropenia, grade 4 in 2 cases and grade 3 in3 cases, the latter resulting in a delay in the subsequent cycle.Non-hematological toxicity was generally mild and, like theschedule 2/1, included, fatigue, nausea, vomiting andconstipation. No clinically significant effects on cardiac repo-larization were reported (with either schedule). The recom-mended Phase II dose was 125 mg/day. Among 37 patientsevaluable for response, disease stabilization for at least twocycles was achieved in 13 cases (35%) and maintained for atleast 10 cycles in 6 patients, including one with breast cancerand high levels of Rb-positive cells. There were no partialresponses according to RECIST criteria.Pharmacokinetic parameters for palbociclib with the two
schedules are reported in Table 1 [80,81]. The main parametersshowed low-to-moderate inter-patient variability, with a gen-erally dose-dependent increase in exposure (assessment basedon maximum observed plasma concentration [Cmax] and thearea under the plasma concentration-time curve from 0 to10 h [AUC0-10]) over the dose range studied. At steady state,palbociclib was absorbed with a median Tmax (time to firstoccurrence of Cmax) of ~ 4 -- 5.5 h. The mean drug apparentvolume of distribution (Vz/F) was significantly greater thantotal body water, suggesting an extensive penetration intoperipheral tissues and substantial tissue binding. Palbociclibwas eliminated slowly, with a mean terminal half-life (t1/2)of ~ 26 h and a mean apparent clearance of 80 -- 90 l/h. Renalexcretion was a minor route of elimination with a mean of1.8% of unchanged palbociclib found in urine.A pharmacodynamic model correlating the AUC with
nadir values of absolute neutrophil count (ANC) and plateletcount showed a non-linear relationship, with increasing drugexposure resulting in a saturable decrease from baseline forboth ANC and platelets [80,81].Based on the results from the Phase I study, the schedule
3/1 at a dose of 125 mg/day was selected for further clinicaldevelopment. Preliminary results of a Phase II, single-armstudy of palbociclib (schedule 3/1) in patients with advancedbreast cancer expressing the Rb protein have only beenreported in abstract form and were updated at the2013 ASCO Annual Meeting [82]. Of the 37 patients enrolled,30 had hormone receptor-positive tumors (HER2-positive intwo cases) and showed 2 (7%) partial responses and 17 (57%)disease stabilizations lasting longer than 6 months in 3 cases(10%); 11 patients (36%) had disease progression. Triple-negative tumors were seen in 6 patients, and 5 of themshowed disease progression at first assessment, whereas only1 had disease stabilization, lasting longer than 6 months.Median progression-free survival (PFS) was 3.8 months inhormone receptor-positive patients (95% CI 2.3 -- 7.7) and
1.9 months in triple-negative patients (95% CI 0.9 -- ¥). Tox-icities were consistent with previous studies, with grade3/4 AEs limited to neutropenia and thrombocytopenia. Thistrial confirms results from preclinical studies, showing betteractivity of palbociclib in hormone-receptor-positive andHER2-positive tumors compared with triple-negative ones.
Given the important role of both estrogens and CDKs inthe genesis and progression of breast cancer, the preclinicalresults showing preferential activity of palbociclib in luminaltumors, and the synergism between palbociclib and tamoxifendemonstrated in vitro, clinical trials were planned to test thecombination of palbociclib with letrozole. In a Phase IBstudy [83], 12 post-menopausal patients with ER-positive,HER2-negative advanced breast cancer pretreated with che-motherapy (67%) or endocrine therapy (50%) received palbo-ciclib 125 mg/day (schedule 3/1) and letrozole 2.5 mg/daycontinuously. The median duration of treatment was6 months (range 2 -- 13). Treatment was well tolerated, withthree DLTs (grade 4 neutropenia in two cases and dose inter-ruption in one) and leuko-neutropenia and fatigue as themost common side-effects. The pharmacokinetic evaluationsuggested that there was no interaction between palbocicliband letrozole. Out of 9 patients with measurable disease,3 experienced a partial response and 9 showed stable disease.
A randomized Phase II study was then conducted in post-menopausal patients with ER-positive, HER2-negativeadvanced breast cancer who were randomized to receive letro-zole 2.5 mg/day alone or in combination with palbociclib125 mg/day (schedule 3/1) as first-line therapy for advanceddisease (TRIO-18 trial). The trial consisted of two parts: inthe first part, patient selection was based only on ER andHER2 status, whereas in the second part, CCND1 amplifica-tion and/or p16 loss, assessed by fluorescence in situ hybrid-ization, was required for eligibility. Patients were stratifiedby disease site and disease-free interval. Part 1, enrolling66 patients, showed a significant improvement in PFS withthe combination of palbociclib plus letrozole compared withletrozole alone (HR = 0.35; 95% CI, 0.17 -- 0.72;p = 0.006) [84,85]. Objective response rates (27 vs 23%) andclinical benefit (partial responses plus stable disease‡ 24 weeks) rates (59 vs 44%) were also improved in patientstreated with the combination [84]. The most commontreatment-related adverse events in the combination armwere neutropenia, leukopenia and fatigue. In an exploratoryanalysis, CCND1 and p16 status did not add a further predic-tive value over ER expression alone. Thus, after a further99 patients had been randomized in part 2, results from thesecond interim analysis were presented at the 2012 San Anto-nio Breast Cancer Symposium, combining parts 1 and 2 ofthe study, for a total of 165 patients, 84 randomized in thecombination arm and 81 in the letrozole-alone arm. Baselinecharacteristics were well balanced between the two arms.A PFS of 26.1 months was observed for patients receivingpalbociclib plus letrozole, compared with 7.5 months forthose treated with letrozole alone (HR = 0.37; 95% CI,
0.21 -- 0.63; p < 0.001). The objective response rate was 34%in the combination arm and 26% in the letrozole-alone arm,while clinical benefit rates were 70 and 44%, respectively. Thetoxicity profile for the combination was favorable, the mostcommon AEs being uncomplicated neutropenia, leukopenia,anemia and fatigue [85].
On the basis of these extremely promising results, enroll-ment is ongoing in a randomized, multicenter, double-blind,first-line Phase III study of palbociclib plus letrozole com-pared with letrozole/placebo in postmenopausal women withER-positive, HER2-negative advanced breast cancer whohave not received any prior systemic anticancer treatmentfor advanced disease [86].
Other Phase II or III studies are planned or ongoing withpalbociclib in combination with endocrine agents in patientswith hormone receptor (HR)-positive, HER2-negative disease:in combination with fulvestrant after endocrine failure in met-astatic breast cancer (NCT01942135); in combination withstandard endocrine treatment in patients with residual diseaseafter neoadjuvant chemotherapy and surgery for primarybreast cancer (PENELOPE-B, NCT01864746); and in com-bination with anastrozole as neoadjuvant therapy in patientswith stage II or III ER-positive, HER2-negative breast cancer(without PI3K hotspot mutations) (NCT01723774).A Phase I study is ongoing to establish the MTD and the rec-ommended Phase II dose of a combination of palbocicliband paclitaxel (NCT01320592).
4. Conclusions
Deregulation of cell cycle control is a prominent feature of can-cer, and the cyclin D-CDK4/6-Rb pathway, governing the cellcycle restriction point, is often altered in breast cancer, contrib-uting to tumor progression and to the development of endo-crine resistance. Palbociclib, a small molecule and highlyselective, reversible inhibitor of CDK4 and CDK6, inhibitsprogression of the cell cycle from G1 into the S phase in Rb-proficient cells, exerting cytostatic activity on different tumortypes in vitro and in vivo. It is not active on Rb-negative,p16INK4A overexpressing tumor cells.
Palbociclib has shown considerable activity in luminal, ER-positive breast cancer cell lines and xenograft models, includ-ing some luminal HER2-positive lines, and little or no activ-ity in breast cancer models with basal features. Combinationsof palbociclib with trastuzumab or tamoxifen have provensynergistic in HER2-amplified and in ER-positive cell lines,respectively.
Based on these preclinical findings, palbociclib was testedin a randomized Phase II study in combination with letrozole,versus letrozole alone, as first-line therapy in patients withadvanced ER-positive, HER2-negative breast cancer, leadingto a substantial improvement in PFS. Palbociclib alone hasalso shown some activity in patients with ER-positive breastcancer expressing Rb protein.
Although palbociclib appears to be a very promising agentin breast cancer, preliminary results must now be confirmedin Phase III trials, which are ongoing. Further clinical studiesare currently exploring its activity or efficacy in other diseasesettings and in combination with other agents. Translationaland basic research is focusing mainly on the detection of pre-dictive biomarkers that could identify patients who are likelyto benefit from this agent.
5. Expert opinion
The cyclin D-CDK4/6-Rb pathway represents a master regula-tor of cell cycle and is downstream of multiple mitogenic cas-cades, representing a relevant target for anticancer therapy.Preclinical evaluation shows that palbociclib, a reversibleinhibitor of CDK4 and CDK6, is active in breast cancer mod-els, especially those with luminal features, including someHER2-positive tumors. Synergistic results have also beenreported for palbociclib when used in combination withtamoxifen and trastuzumab, while a potential antagonism hasbeen noted with several chemotherapeutic agents.
Preliminary results from clinical trials confirm the preferen-tial activity of the drug in ER-positive tumors [82] and itspotential synergism with letrozole [85].
An important characteristic that should be taken intoaccount for the clinical development of palbociclib is itspure cytostatic action exerted in most tumor models, that is,
Table 1. Pharmacokinetic parameters for palbociclib by schedule after multiple doses.
Cmax (ng/ml), mean (%CV) 174 (17) 86 (34)Tmax (h), median (range) 4 (2 -- 7) 4 (1 -- 10)AUC(0 -- 10) (ng·h/ml), mean (%CV) 1395 (23) 724 (38)Vz/F (l) 3241 2793t1/2 (h), mean 26.7 26CL/F (l/h), mean 88.5 80.6Rac, median 2.4 2.2
Reported values for Cmax, Tmax and AUC were measured at day 8 of the first cycle; Vz/F, t1/2, CL/F and Rac were estimated following repeated daily dosing to
steady-state for both schedules.
CL/F: Apparent clearance; CV: Coefficient of variation; Rac: Drug accumulation ratio; Vz/F: Apparent volume of distribution during the terminal phase.
no induction of apoptosis, but a capacity to induce cellularsenescence. This may explain the low objective response ratesand higher rates of disease stabilization obtained when palbo-ciclib has been used as a single agent in clinical trials [82,87].Although tumor remissions have been observed in preclinicalstudies, the use of palbociclib alone may be more appropriateas ‘maintenance’ therapy, whereas treatment in combinationwith other agents may be needed to obtain maximal, rapidtumor shrinkage.Preclinical studies clearly point at Rb-proficiency, cyclin
D1 overexpression or gene amplification and loss or reducedexpression of p16 as predictors of response. Nonetheless, anexploratory analysis from the TRIO-18 trial showed that nei-ther CCND1 amplification nor p16 loss added any furtherpredictive value over ER expression alone [85]. There couldbe several reasons for this discrepancy. CCND1 amplificationis only responsible for a minority of cases of cyclin D1 over-expression. In some tumor models, the activation of cyclinE-CDK2 complexes may compensate for the lack or inactiva-tion of cyclin D-CDK4/6 complexes, abolishing the predic-tive value of cyclin D. Palbociclib has also been reported toexert some activity in experimental models after Rb knock-down, possibly due to compensation of Rb protein functionby p107 protein, which may be activated by palbociclib [66].Thus, prediction of response to palbociclib needs to be furtherinvestigated as a constellation of molecules is involved. An Rbgene expression signature could perhaps be more informative,albeit also more complicated, than the assessment of singlemolecules.The combination of palbociclib with endocrine agents
appears to be a highly promising area of application. Theimpressive results from the TRIO-18 trial are awaiting confir-mation in the ongoing Phase III trial [86]. However, the trialdoes not include an arm of letrozole followed by palbociclibor an arm in which palbociclib is added to letrozole only atthe moment of progression. The need for combined treatmentmay differ in tumors with intrinsic endocrine resistance com-pared to those that develop acquired resistance. A randomizedtrial testing the addition of lapatinib to letrozole showed, inthe subgroup of HER2-negative tumors, a trend towards pro-longed PFS only in patients who relapsed < 6 months after
tamoxifen discontinuation, but no effect in those who pro-gressed after ‡ 6 months or who had not received prior adju-vant tamoxifen [88]. Other drugs have also produced a benefitwhen combined with endocrine agents with the intent ofovercoming or preventing endocrine resistance: trastuzumabadded to anastrozole in patients with HER2/hormonereceptor-copositive tumors [89]; everolimus combined withexemestane in patients with HER2-negative breast cancerwho had disease recurrence or progression while receiving anon-steroidal aromatase inhibitor [90]; the histone deacetylaseinhibitor entinostat added to exemestane in the same diseasesetting [91]. The usefulness of the sequential administrationof these combinations and the best sequence remain to beascertained. However, confirmation of an important advan-tage in the metastatic setting could lead to their developmentin the adjuvant setting.
Combinations of palbociclib and other targeted therapiessuch as anti-HER2 agents, PI3K inhibitors or mTOR inhibi-tors could represent potentially important areas of research.The association of palbociclib with chemotherapy, however,appears more problematic because of the potential antago-nism. An ongoing Phase I trial of palbociclib in associationwith paclitaxel could provide an important insight into thepotential of such associations. Experiments carried out ontumor cell synchronization also indicate the possible useful-ness of cyclic palbociclib in combination with metronomicchemotherapies [78].
Although palbociclib has been shown to offer protectionfrom chemotherapy-induced myelosuppression, it would benecessary to accurately identify CDK4/6-independent tumorsin which palbociclib would not antagonize the activity of che-motherapy before implementing this strategy in clinical prac-tice. The ability of palbociclib to reverse epithelial dysplasiaalso highlights a possible chemopreventive role in selectedwomen at high risk for breast cancer.
Declaration of interest
The authors state no conflict of interest and have received nopayment in preparation of this manuscript.