37
Treatment of VTE in cancer patients XXth IST, London 2013 Paolo Prandoni, MD, PhD University of Padua (Italy) Anatomic theatre, Padua University

Treatment of VTE in cancer patients
XXth IST, London 2013
Paolo Prandoni, MD, PhD University of Padua (Italy)
Anatomic theatre, Padua University

VTE and cancer: diagnostic aspects ● Patients with active cancer should be promptly investigated
whenever clinical symptoms and signs suggestive of VTE arise
● Clinical signs and symptoms of PE are often mimiked by those of the underlying malignancy
● D-dimer is less likely to be useful than in cancer-free patients
● DVT of the lower extremities is less likely to be present in patients with PE (Sorensen HT. et al. Circulation. 2011;124:1435-1441; Schwartz T, et al. Ann Vasc Surg. 2012;26:973-976.)

● Areas of (relative) certainty (Asco Guidelines, JCO 2013; International Clinical Practice Guidelines, JTH 2013)
● Areas of uncertainty (Guidance from the SSC of the ISTH, June 2013)
● Potential role of new drugs ● Management of incidental PE
VTE and cancer: diagnostic aspects

Treatment of CAT: areas of (relative) certainty
● Cancer patients are less likely than patients without cancer to require
thrombolytic therapy (potential for bleeding, unlikelihood of long-term
complications in severely ill patients).
● The treatment of SVT should not differ from that of non-cancer
patients.
● The treatment of (catheter-induced) upper limb DVT should not differ
from that of DVT of the lower extremities.
● Low-molecular-weight heparins represent the drugs of choice for the
initial and long-term treatment of upper or lower limbs DVT,
pulmonary thromboembolism and visceral thrombosis.
Asco Guidelines, JCO 2013; International Clinical Practice Guidelines, JTH 2013

Cumulative proportion of recurrent thromboembolism during VKA treatment
20
2 4 6 8 10 12
cancer
%
Months
Risk ratio=3.2; P<0.001
18
10
5
no cancer
Prandoni P, et al. Blood. 2002;100:3484-3488.

5
10
15
20
2 4 6 8 10 12
cancer no cancer
%
Months
HR=2.1; p=0.019
Cumulative proportion of major bleeding during VKA treatment
Prandoni P, et al. Blood. 2002;100:3484-3488.

Monreal M, Falgà C, Valdès M, Suarez C, Gabriel F, Tolosa C, Montes J,
for the RIETE registry
Fatal pulmonary embolism and fatal bleeding in cancer patients with venous thromboembolism*
J Thomb Haemost. 2006;4:1950-1956.
* during the first three months of conventional anticoagulation

Multivariate analysis on the risk of fatal PE (14 391 patients, of whom 2945 with cancer)
Variables OR (95% CI) P-value
Symptomatic PE 13.9 (6.3 – 30.0) < 0.001
Metastatic cancer 2.9 (1.8 – 4.8) < 0.001
Recent major bleeding 2.8 (1.2 – 6.3) 0.013
Renal insufficiency 2.6 (1.6 – 4.3) < 0.001
Immobility > 4 days 1.9 (1.1 – 3.2) 0.014

Multivariate analysis on the risk of fatal bleeding (14 391 patients, of whom 2945 with cancer)
Variables OR (95% CI) P-value
Immobility > 4 days 4.1 (1.4 – 7.1) < 0.001
Metastatic cancer 3.1 (1.8 – 4.8) 0.006
Recent major bleeding 3.0 (1.0 – 9.1) 0.058
Renal insufficiency 2.8 (1.3 – 5.8) 0.008
Body weight < 60 Kg 2.5 (1.1 – 5.3) 0.021

Treatment of CAT
• All major consensus guidelines recommend
monotherapy with LMWH as the preferred treatment
for CAT
• Recommendations are based on results of 3 open
label, randomized controlled trials
- CATHANOX: enoxaparin vs warfarin
- CLOT: dalteparin vs warfarin or acenocoumarol
- LITE: tinzaparin vs warfarin

Recurrent VTE Major bleeding
Dalteparin (N=336)OAT (N=336)
(%)
8.8%
17.4%
5.6%
3.6%
CLOT 2003
5
10
15
20
HR=0.48; P=0.0017
Lee AY, et al. N Engl J Med. 2003;349:146-153.
Implications for the detection of occult cancer
• The strong advantage of LMWH over VKA adds to the still
unresolved issue on the need for cancer detection in patients
with otherwise unexplained VTE.
• Indeed, the detection of cancer gives indication for
prolonging the initial LMWH treatment or shifting from VKA –
whenever initiated – to LMWH therapy
• In addition, the use of LMWHs in subgroups of patients with
cancer may ultimately prolong survival

Duration of anticoagulation
• General expert/guidelines consensus: – minimum of 3 – 6 months – continue as long as cancer is active or chemotherapy is ongoing – discontinue if risk of serious bleeding is high or patient preference
• Consider risk factors for recurrence and bleeding
• Frequently evaluate patients and tailor therapy according to risk, benefits, preference

Thromb Haemost 2013


Treatment of CAT: areas of uncertainty
● Management of recurrent cancer-associated thrombosis
despite anticoagulation
● Management of cancer-associated thrombosis in patients
with thrombocytopenia
● Management of cancer-associated thrombosis in patients
who are bleeding
Guidance from the SSC of the ISTH, June 2013
Management of recurrent CAT despite anticoagulation
● Cancer patients with symptomatic recurrent VTE despite therapeutic
anticoagulation with VKA should be switched to therapeutic weight-
adjusted doses of LMWH [A]
● Cancer patients with symptomatic recurrent VTE despite
anticoagulation with LMWH should continue with LMWH at a higher
dose, starting at an increase of approximately 25% of the current
dose or increasing it back up to the therapeutic weight-adjusted
dose if receiving non-therapeutic dosing [B]
Guidance from the SSC of the ISTH, June 2013: A=recommendation; B=suggestion

Management of CAT in patients with thrombocytopenia (1)
● Full therapeutic doses of anticoagulation
without platelet transfusion should be given
in patients with CAT and platelet count ≥ 50
X 109/L [A]
Guidance from the SSC of the ISTH, June 2013: A=recommendation; B=suggestion

Management of CAT in patients with thrombocytopenia (2)
Acute CAT and platelet count < 50 X 109/L
● Full therapeutic doses of anticoagulation with platelet transfusion
should be given to maintain a platelet count ≥ 50 X 109/L [A]
● If platelet transfusion is not possible or contraindicated, the insertion
of a retrievable filter is suggested, as well as its removal when platelet
count recovers and anticoagulation can resume [B]
Guidance from the SSC of the ISTH, June 2013: A=recommendation; B=suggestion

Management of CAT in patients with thrombocytopenia (3)
Sub-acute or chronic CAT and platelet count <50 X 109/L
● In patients with platelet count of 25 to 50 X 109/L subtherapeutic
or prophylactic doses of LMWH should be used [B]
● In patients with platelet count < 25 X 109/L anticoagulation
should be discontinued [B]
Guidance from the SSC of the ISTH, June 2013: A=recommendation; B=suggestion

Management of CAT in patients who are bleeding (1) The panelists recommend:
● Careful and thorough assessment of each bleeding episode,
including identification of the source, its severity or impact, and
reversibility [A]
● Usual supportive care with transfusion and surgical intervention to
correct the bleeding source, whenever indicated and possible [A]
● Withholding anticoagulation in patients having a major or life-
threatening bleeding episode [A]
Guidance from the SSC of the ISTH, June 2013: A=recommendation; B=suggestion

Management of CAT in patients who are bleeding (2)
● The panel members suggest IVC filter insertion in patients with
acute CAT or sub-acute CAT who are having a major or life-
threatening bleeding episode [B]
● They recommend against IVC filter insertion in patients with chronic
CAT [A]
● They recommend initiating or resuming anticoagulation and
removing retrievable IVC filter (if inserted) once the bleeding
resolves [A]
Guidance from the SSC of the ISTH, June 2013: A=recommendation; B=suggestion


● Paucity of clinical trial data
● No comparison against long‐term LMWH
● Liver and renal dysfunction is common in cancer
● Lack of experience on management for procedures and
thrombocytopenia
● Drug interactions may be clinically important
● Lack of measurement (therapeutic range) and antidote
Limitations of NOAs for treatment of CAT


Management of incidental PE in cancer patients

Incidental VTE
Frequent finding in oncology patients (2 to 6%) Clinical significance uncertain, but most are being treated
Khorana AA, et al. Cancer. 2007;110:2339-2346. Browne AM, et al. J Thorac Oncol. 2010;5:798-803. Douma RA, et al. Thromb Res. 2010;125:e306-309.


● In patients who are incidentally found to have asymptomatic PE, we suggest the same initial and long-term anticoagulation as for comparable patients with symptomatic PE (Grade 2B)
Recommendations on treatment of incidental VTE

ISSPE: accuracy of diagnosis
1. We do not know the accuracy of detecting PE on CT-scans that
were not specifically ordered to diagnose PE
2. Higher risk of false positive diagnosis compared to patients with
suspected PE
3. In a series of 70 patients diagnosed with subsegmental PE, this
diagnosis was confirmed in only 51% by a reviewing radiologist
(Pena E, et al. J Thromb Haemost. 2012;10:496-498.)
4. PE may not be acute but chronic

Withholding anticoagulation can be safe in ISSPE patients
1. A total of 65 cases of untreated
subsegmental PE have been reported
2. None of these patients developed
recurrent VTE
Donato AA, et al. Thromb Res. 2010;126:e266-270.

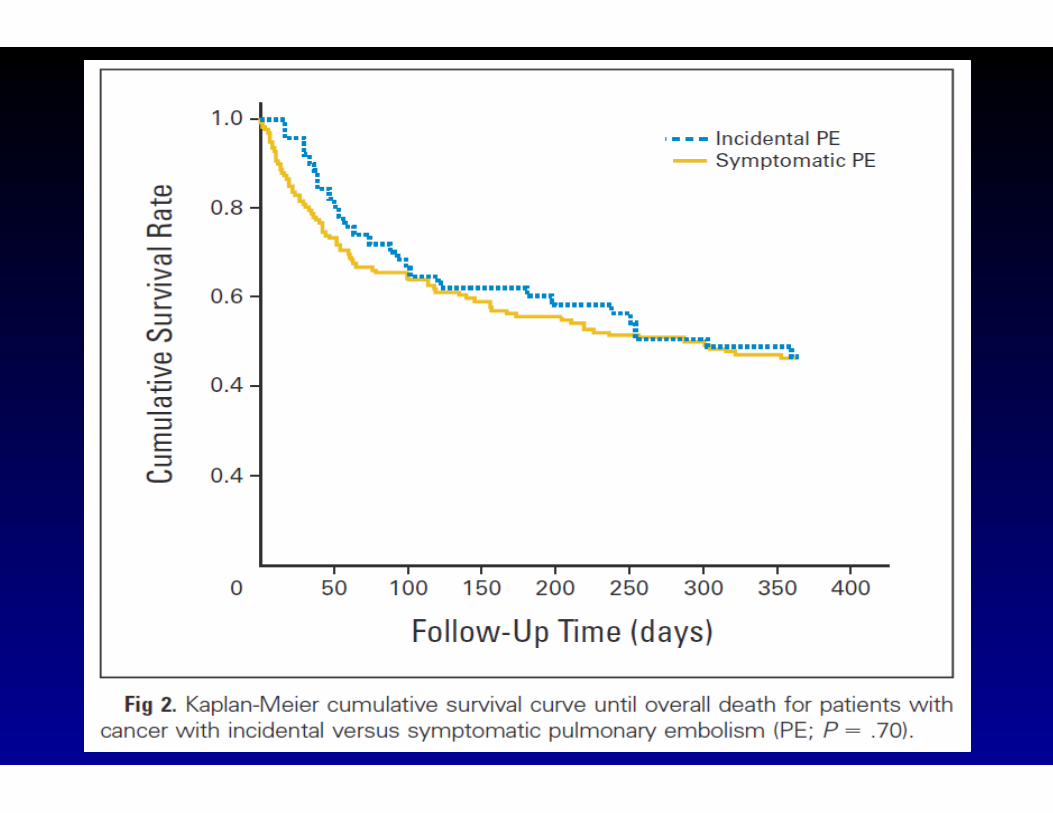
ISSPE: uncertainty of outcome
There is uncertainty on the outcome of patients with
incidental PE who receive anticoagulant
Cohort study of 51 patients with incidental PE: 5 (9.8%)
patients developed major bleeding of which 2 cases were
fatal
den Exter PL, et al. J Clin Oncol. 2011;29:2405-2409.

Instead of instant initiation of therapy consider:
1. Clinical evaluation:
- are symptoms of PE present?
- is there evidence of DVT?
- what is the bleeding risk with anticoagulation?
2. Evaluation of imaging studies:
- review CT critically, is the diagnosis accurate?
- is there the involvement of at least one segmental vessel?
- compare with recent CT-scans, are the findings new?

Treatment of CAT: main conclusions
1. LMWH is the “best” agent available for initial and long-term treatment
2. Duration of treatment is dependent on status of patients, treatment, other risk
factors and patients preference
3. LMWH dose adjustment is effective in treating recurrent thrombosis and in
patients with bleeding or thrombocytopenia. IVC filters should be discouraged
4. Novel anticoagulants should be investigated more carefully before routine usage
in cancer patients
5. Incidentally detected sub-segmental PE is unlikely to require full-dose
anticoagulation

















