Hong Kong J. Dermatol. Venereol. (2019) 27, 31-35 Case Report Papillon-Lefevre syndrome: a rare case report and review of literature D Vupperla, P Elaprolu, FT Taj Papillon-Lefevre syndrome (PLS) is a rare genetically inherited autosomal recessive disorder. A 34- year-old woman presented with complaints of diffuse hyperkeratosis with scaling over both palms and soles with sclerodactyly of all fingers, increased sweating, loss of teeth with periodontitis and recurrent skin infections. History of first-degree consanguinity among the patients was present. Loss of teeth can be prevented by prompt administration of oral retinoids during the eruption of permanent teeth. Despite meticulous attention, many patients are still identified with PLS. Therefore, clinicians should be aware of this entity to avoid delay in diagnosis. 34 Keywords: Keywords: Keywords: Keywords: Keywords: Cathepsin C, hyperkeratosis, Palmoplantar keratoderma, Periodontitis, Pyoderma C Divya Skin Clinic, c/o V Divya Skin Clinic, c/o V Divya Skin Clinic, c/o V Divya Skin Clinic, c/o V Divya Skin Clinic, c/o Vasan Eye Care, 1st Floor asan Eye Care, 1st Floor asan Eye Care, 1st Floor asan Eye Care, 1st Floor asan Eye Care, 1st Floor, Beside Dr Nagabhushanam Hospital, 11-5-8,9,10 Beside Dr Nagabhushanam Hospital, 11-5-8,9,10 Beside Dr Nagabhushanam Hospital, 11-5-8,9,10 Beside Dr Nagabhushanam Hospital, 11-5-8,9,10 Beside Dr Nagabhushanam Hospital, 11-5-8,9,10 Wyra R Wyra R Wyra R Wyra R Wyra Road, Khamam 507003, India oad, Khamam 507003, India oad, Khamam 507003, India oad, Khamam 507003, India oad, Khamam 507003, India D Vupperla, MD Sri Muthukumaran Medical College Hospital and Sri Muthukumaran Medical College Hospital and Sri Muthukumaran Medical College Hospital and Sri Muthukumaran Medical College Hospital and Sri Muthukumaran Medical College Hospital and Research Institute, Chikk esearch Institute, Chikk esearch Institute, Chikk esearch Institute, Chikk esearch Institute, Chikkarayapuram, Chennai arayapuram, Chennai arayapuram, Chennai arayapuram, Chennai arayapuram, Chennai 600069, India 600069, India 600069, India 600069, India 600069, India P Elaprolu, MD Department of Dermatology Department of Dermatology Department of Dermatology Department of Dermatology Department of Dermatology, V , V , V , V , Venereology and enereology and enereology and enereology and enereology and Leprosy, Jawaharlal Nehru Medical College, KLE Leprosy, Jawaharlal Nehru Medical College, KLE Leprosy, Jawaharlal Nehru Medical College, KLE Leprosy, Jawaharlal Nehru Medical College, KLE Leprosy, Jawaharlal Nehru Medical College, KLE University University University University University, Belgaum, Karnatak , Belgaum, Karnatak , Belgaum, Karnatak , Belgaum, Karnatak , Belgaum, Karnataka, India a, India a, India a, India a, India FT Taj, MD Correspondence to: Dr. D Vupperla Divya Skin Clinic, c/o Vasan Eye Care, 1st Floor, Beside Dr Nagabhushanam Hospital, 11-5-8,9,10 Wyra Road, Khamam 507003, India Introduction Introduction Introduction Introduction Introduction Papillon-Lefevre syndrome (PLS) is a rare autosomal recessive disorder characterised by periodontopathy, palmoplantar hyperkeratosis and severe early onset loss of deciduous and permanent dentition. 1 It presents between the ages of one to five years and patients become edentulous by their early teens. 2 The prevalence rate ranges from 1-4 cases per million individuals. Both men and women are affected equally without any racial or gender preponderance. 3 Multiple aetiological factors are implicated in the development of PLS. However, three main factors-
Transcript
Hong Kong J. Dermatol. Venereol. (2019) 27, 31-35
Case Report
Papillon-Lefevre syndrome: a rare case report and reviewof literature
D Vupperla, P Elaprolu, FT Taj
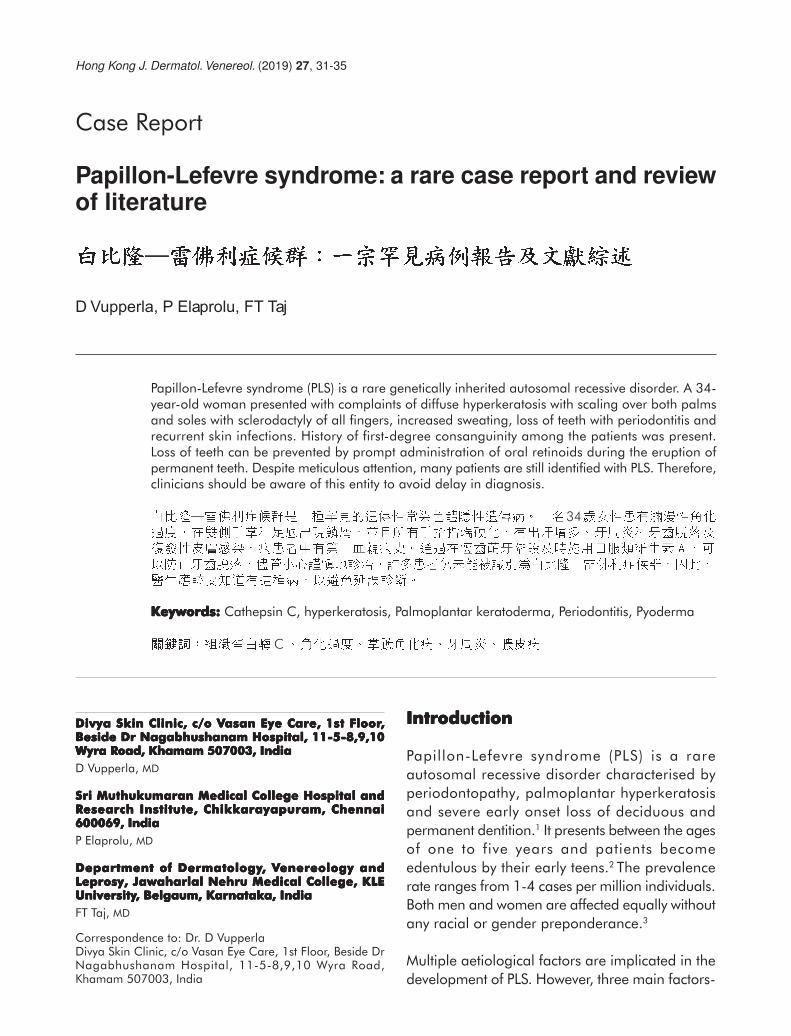
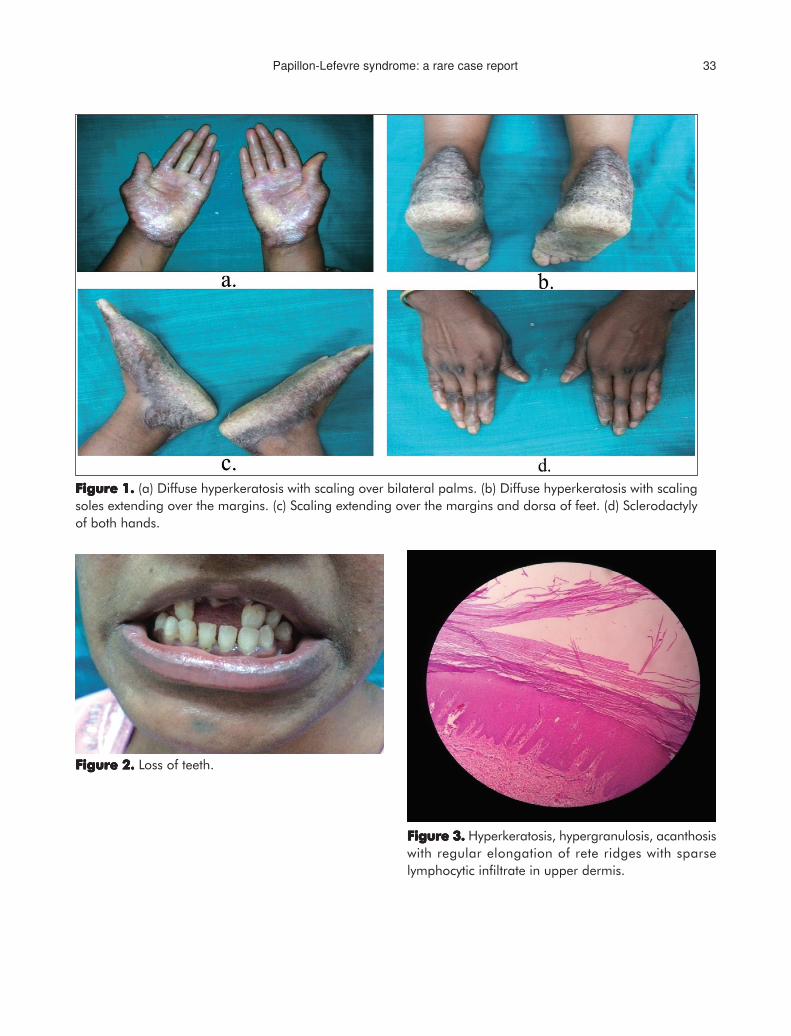
Papillon-Lefevre syndrome (PLS) is a rare genetically inherited autosomal recessive disorder. A 34-year-old woman presented with complaints of diffuse hyperkeratosis with scaling over both palmsand soles with sclerodactyly of all fingers, increased sweating, loss of teeth with periodontitis andrecurrent skin infections. History of first-degree consanguinity among the patients was present.Loss of teeth can be prevented by prompt administration of oral retinoids during the eruption ofpermanent teeth. Despite meticulous attention, many patients are still identified with PLS. Therefore,clinicians should be aware of this entity to avoid delay in diagnosis.
Divya Skin Clinic, c/o VDivya Skin Clinic, c/o VDivya Skin Clinic, c/o VDivya Skin Clinic, c/o VDivya Skin Clinic, c/o Vasan Eye Care, 1st Floorasan Eye Care, 1st Floorasan Eye Care, 1st Floorasan Eye Care, 1st Floorasan Eye Care, 1st Floor,,,,,Beside Dr Nagabhushanam Hospital, 11-5-8,9,10Beside Dr Nagabhushanam Hospital, 11-5-8,9,10Beside Dr Nagabhushanam Hospital, 11-5-8,9,10Beside Dr Nagabhushanam Hospital, 11-5-8,9,10Beside Dr Nagabhushanam Hospital, 11-5-8,9,10Wyra RWyra RWyra RWyra RWyra Road, Khamam 507003, Indiaoad, Khamam 507003, Indiaoad, Khamam 507003, Indiaoad, Khamam 507003, Indiaoad, Khamam 507003, India
D Vupperla, MD
Sri Muthukumaran Medical College Hospital andSri Muthukumaran Medical College Hospital andSri Muthukumaran Medical College Hospital andSri Muthukumaran Medical College Hospital andSri Muthukumaran Medical College Hospital andRRRRResearch Institute, Chikkesearch Institute, Chikkesearch Institute, Chikkesearch Institute, Chikkesearch Institute, Chikkarayapuram, Chennaiarayapuram, Chennaiarayapuram, Chennaiarayapuram, Chennaiarayapuram, Chennai600069, India600069, India600069, India600069, India600069, India
P Elaprolu, MD
Department of DermatologyDepartment of DermatologyDepartment of DermatologyDepartment of DermatologyDepartment of Dermatology, V, V, V, V, Venereology andenereology andenereology andenereology andenereology andLeprosy, Jawaharlal Nehru Medical College, KLELeprosy, Jawaharlal Nehru Medical College, KLELeprosy, Jawaharlal Nehru Medical College, KLELeprosy, Jawaharlal Nehru Medical College, KLELeprosy, Jawaharlal Nehru Medical College, KLEUniversityUniversityUniversityUniversityUniversity, Belgaum, Karnatak, Belgaum, Karnatak, Belgaum, Karnatak, Belgaum, Karnatak, Belgaum, Karnataka, Indiaa, Indiaa, Indiaa, Indiaa, India
FT Taj, MD
Correspondence to: Dr. D VupperlaDivya Skin Clinic, c/o Vasan Eye Care, 1st Floor, Beside DrNagabhushanam Hospital, 11-5-8,9,10 Wyra Road,Khamam 507003, India
1. Reddy KV, Maloth KN, Anusha NV, Thummala VS,Thakur M. Papillon-Lefèvre syndrome: A case series withreview of literature. J Oral Med, Oral Surg, Oral PatholOral Radiol 2016;2:248-51.
2. Hart TC, Shapira L. Papillon-Lefèvre syndrome.Periodontol 2000 1994;6:88-100.
3. Pavankumar K. Papillon-Lefèvre syndrome: A casereport. Saudi Dent J 2010;22:95-8.
4. Kaur B. Papillon lefevre syndrome: A case report withreview. Dentistry 2013;3:156.
5. Ramadan ARM, Bashir AH. Papillon-Lefèvre syndrome-a case report and a multidisciplinary approach in thetreatment of 18 years old Sudanese female. Am JDermatol Venereol 2017;6:11-5.