41
Part 3: Patient Counseling and Education – Overdose Prevention and Naloxone Use New Mexico Pharmacists Association & Project ECHO 2014
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | primrose-shepherd |
| View: | 213 times |
| Download: | 1 times |
Part 3: Patient Counseling and Education – Overdose Prevention and Naloxone Use
New Mexico Pharmacists Association &Project ECHO
2014
Learning Objectives • To reinforce communication skills for patient
counseling and education• To understand the principles of harm reduction• To learn key overdose prevention messages
for patient education• To learn to teach patients to use Naloxone

“Extensive research has shown that no matter how knowledgeable a clinician might be, if he or she is not able to open good communication with the patient, he or she may be of no help.”
Impact of Communication in Healthcare, Institute for Healthcare Communication, July 2011.

How do you define communication
?

Communication is…
• The transmission of information between individuals or groups by any means.
• A 2-way process – sending and receiving. If a message that is sent is not received, communication has not taken place.
Author: Romith Wikimedia Commons

Why are communication skills important in providing patient
education?

Research indicates strong positive relationships between a healthcare provider’s communication skills and a client’s capacity to:
• follow through with medical recommendations • self-manage a chronic medical condition• adopt preventive health behaviors
All of the client actions identified above are relevant to overdose prevention.
Impact of Communication in Healthcare, Institute for Healthcare Communication, July 2011.

Strategies to improve patient education
• Use simple language → avoid use of medical terms and acronyms
• Focus on 2-3 key messages and use brief explanations
• Use Teach-Back → verify patient’s understanding by asking him/her to repeat back or demonstrate information (e.g., demonstrate naloxone use)
• Solicit questions → “what questions do you have?” vs. “do you have any questions?”
• Provide patient-friendly handouts → low-literacy level, pictures, “how-to” instructions, etc.

In addition to a current knowledge of pharmacotherapy,pharmacists need to have the knowledge and skills to provide effective and accurate patient education and counseling.
Effective, open-ended questioning and active listeningare essential skills for obtaining information from andsharing information with patients.
A patient may learn best by hearing spoken instructions; by seeing a diagram, picture, or model; or by directly handling medications and administration devices.
ASHP Guidelines on Pharmacist-Conducted Patient Education and Counseling http://www.ashp.org/DocLibrary/BestPractices/OrgGdlPtEduc.aspx

What does the term Harm Reduction
mean to you?

Harm Reduction is……a health education and treatment strategy aimed at reducing the negative consequences of many human behaviors without eliminating the behavior.
Common examples of harm reduction include wearing seat belts to reduce injury or death from motor vehicle accidents and using condoms to decrease the risk of sexually transmitted infections.

Harm Reduction for opioid users includes…
…any interventions, strategies or policies designed to reduce the negative consequences of drug use without requiring drug use cessation.
Harm reduction is a way of working with patients to improve their health even if they are not ready, willing or able to stop using drugs.
Syringe exchange and providing naloxone to opioid users to prevent overdose are great examples of harm reduction.

A key reason to talk about harm reduction at this training…
• Some of your clients will have a history of current or previous substance abuse.
• Relapse is often part of recovery - knowing this helps you to help your clients. • Relapse ≠ failure.• Clients with a history of opioid abuse who
relapse are at high risk of overdose. • Providing naloxone is a harm reduction
strategy that can save a life!

Can you think of some Overdose
prevention messages for patients?
Case 1: Ms. J• Ms. J was in a serious car accident and recently
was released from the hospital after 5 days • She had a concussion, several fractured ribs, and
a dislocated shoulder, plus numerous bruises• She comes to your pharmacy with a prescription
for Oxycodone 30 mg q4hrs PRN and cyclobenzaprine 10mg TID PRN for pain and muscle spasms
• What are some questions you might ask Ms. J?• What are some overdose prevention and safety
messages you might provide to Ms. J?• Would you offer her naloxone?

Responding to overdose:
New Mexico ranks #2 in the nation in opioid overdose deaths. All clients using opioids (prescription pain medication, methadone, heroin or buprenorphine) should be taught about:
1. safe use of opioids (e.g., not mixing with alcohol or benzodiazepines)
2. risk factors for overdose3. recognizing signs of overdose4. what to do in case of overdose:
a) calling 911b) recovery positionc) rescue breathingd) using naloxone

1. Safe Use of Opioids• Take only the prescribed dose• Avoid unsafe combinations of drugs:
• Opioids + alcohol• Opioids + benzodiazepines• Opioids + alcohol + benzodiazepines• Alcohol + benzodiazepines
Mixing drugs is the main cause of overdose in New Mexico.
Alcohol can also be very dangerous when used with many OTC drugs. Educate clients about the dangers of mixing alcohol with other drugs or medications.
Author: Super Raptor1 Wikimedia Commons

2. Risk factors for overdose - in addition to mixing prescription opioids with other drugs or alcohol, other risk factors for overdose include:
• Increased opioid tolerance → patients increasing dosages on their own without medical oversight
• Decreased opioid tolerance for patients with a history of opioid abuse, including:• Relapse after completion of opioid detox, inpatient
or intensive outpatient program• Recent release from incarceration• Any other period of either chosen or enforced
sobriety• Overdosing when alone increases risk of fatal
overdose
3. Recognizing signs of overdose
• unconscious or unresponsive (no response to shouting or shaking)
• pale or blue lips, face and fingertips (from lack of oxygen)
• skin feels cold to the touch• slow, shallow or raspy breathing or no breathing• gurgling or snore-like sounds when a person
appears to be sleeping, especially if they have blue or purple-tinged lips or face
• pinpoint pupils

OVERDOSE: WHAT TO DO

In case of overdose:• try to wake the person by calling their name,
shaking them, or causing pain by rubbing your knuckles over their sternum (breastbone) → if this works, get them up and walking around → call 911
• if no response, check their breathing by listening for breath sounds and seeing if their chest rises
• if no breath → call 911 and begin rescue breathing
• prepare Naloxone if you have it
Calling 911
• Overdose is a medical emergency and patients should be strongly encouraged to call 911, but….many patients with a history of substance abuse have had negative interactions with either first responders and/or emergency departments and are wary of calling 911.
• Patients with a history of substance abuse may also be on probation or parole and be afraid of a violation if they call 911 and police respond.
• On the next page are some tips to pass on to patients about calling 911.

Tips for calling 911• Stay calm and tell the 911 operator that someone is not
breathing. If multiple people are at the scene, keep the noise down. Lots of yelling in background will definitely send the police!
• Give good directions so EMS can find you → address, intersecting streets, etc. Send someone out to the street to wait for EMS if possible.
• If applicable, remove any drugs or drug paraphernalia before EMS arrives. Place the person in the recovery position while you do this.
• When EMS arrives, give them as much information as possible. Tell them that you gave Narcan (if you did) and how much.

NM’s Good Samaritan 911 Law• In 2007, NM passed the 1st Good Samaritan 911 law
in the nation.• It allows someone to call 911 or take someone to the
hospital for a drug overdose without being charged for possession.
• The law covers both the caller and person who OD’d.• The law does NOT protect someone if:
• they are on probation, parole, or have arrest warrants• there is evidence of drug dealing → scales, baggies,
drugs or money in plain sight• there is evidence of other crimes, including weapons’
possession or DUI
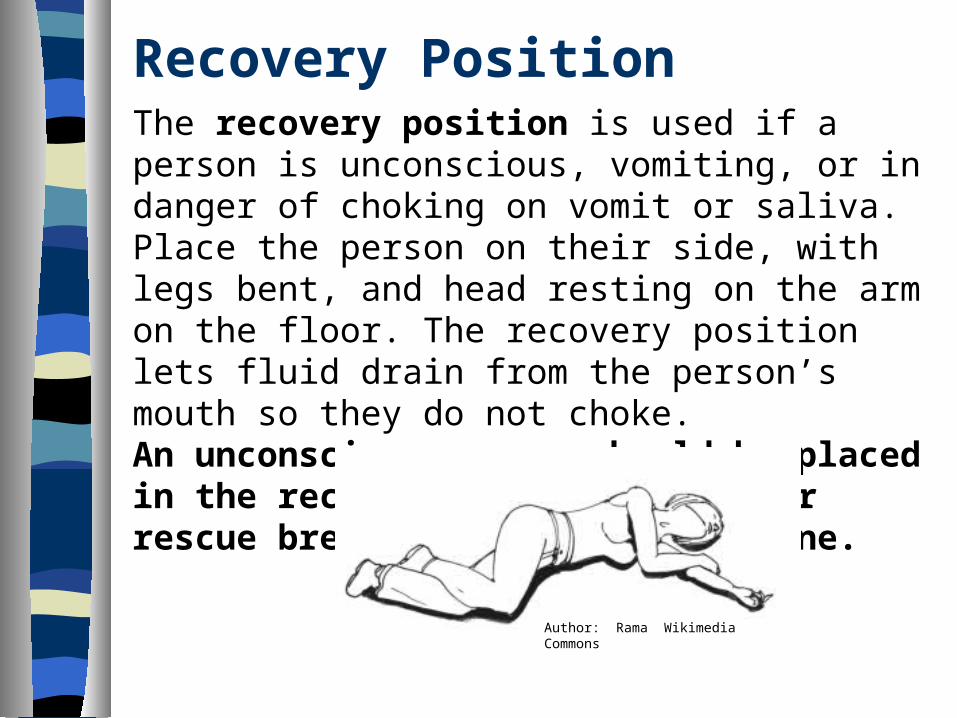
Recovery PositionThe recovery position is used if a person is unconscious, vomiting, or in danger of choking on vomit or saliva. Place the person on their side, with legs bent, and head resting on the arm on the floor. The recovery position lets fluid drain from the person’s mouth so they do not choke.An unconscious person should be placed in the recovery position whenever rescue breathing is not being done.
Author: Rama Wikimedia Commons

Rescue BreathingRescue breathing means breathing for a person unable to breathe on his own. If someone is not breathing or only breathing a few times per minute, rescue breathing must be started immediately.
OPIOID OVERDOSE↓
BREATHING SLOWS ↓ ↓ RESCUE BREATHING NO INTERVENTION AND/OR NALOXONE ↓
↓ BREATHING STOPS LIFE! ↓
DEATH

Steps in Rescue Breathing
1. Place the person on their back with head tilted back and chin lifted (1 hand on forehead and 1 under their chin).2. Pinch their nose shut and breathe into their mouth 2 times (normal breaths).3. Check to make sure their chest is rising. If not, lift chin a little higher and be sure nose is pinched shut.4. Give 1 slow breath every 5 seconds (count: 1-1,000, 2-1,000, 3-1,000, 4-1,00. Take a breath after 4-1,000 and give another breath on 5-1,000).
Picture used by permissionHarm Reduction Coalition

Steps in Rescue Breathing(continued)
5. Continue for 12 breaths (1 minute) and recheck breathing.6. If still no breathing, give Naloxone. If the person wakes up, get them up and moving.7. If still no response, give another dose of Naloxone and continue rescue breathing until the person responds or until EMS arrives.
Picture used by permissionHarm Reduction Coalition

Naloxone: a little assembly required• Pull off the long yellow top of
syringe.• Open the white spray top and screw
it slowly onto the top of the syringe.• Pop-off the red or purple cap on the
medicine vial and the yellow cap on the base of the syringe and gently screw the glass vial into the plastic syringe until you feel slight resistance (about 3 turns).
• Naloxone will start to spray out of the syringe - STOP!

Using Naloxone• Place the spray top in one nostril of the overdosing person. • Push quickly on the glass vial and squirt half of the
liquid up the person’s nose (pushing slowly will prevent the liquid from misting correctly).
• Place the spray top in the other nostril and squirt what’s left in the vial up the person’s nose.
• If no response, use a 2nd box of naloxone. • Continue to do rescue breathing until the person
responds or EMS arrives.
NOTE: more than 1 dose of naloxone is often needed for multi-drug overdoses, especially those combining opioids with alcohol and/or benzodiazepines.

Example: explaining OD and Narcan use to a patient - 1
• Opioids go to receptors in your brain that control pain (or “that make you feel good” for clients who abuse opioids).
• In addition to pain control, opioids make you sleepy and slow your breathing and heart rate (even prescribed doses).
• When you take more than your body can handle, your breathing gets slower and slower over time.
• You might actually stop breathing = overdose.
Picture from NIDA websitePrescription Drugs: Abuse and Addiction
Explaining OD and Narcan use to a patient - 2• Narcan goes to the same receptors
in the brain where the opioid is attached.
• The receptors like Narcan better than the opioid, so the Narcan pushes the opioid off the receptor, which allows you to start breathing again.
• Usually 1 dose of Narcan is enough to get someone breathing again, but you might need to use more if they were mixing opioids with alcohol or other drugs.

Explaining OD and Narcan use to a patient - 3 • Narcan only lasts for about 1 hour
and most opioids last much longer than that in your body.
• When Narcan wears off, the opioid still in your body will go back to receptors in your brain and you could overdose again.
• I strongly recommend that 911 be called for any overdose, but if not, someone MUST remain with the person for at least 2 hours.
• What questions do you have for me?
Notes on Narcan• Narcan: Clients who are familiar with naloxone will
most likely know it as Narcan. • How long it lasts: Narcan will only be effective for
45-60 minutes. Because most opioids last longer, when the Narcan wears off, the person can OD again from the drug still in their system. The person needs to be observed for several hours to ensure their safety.
• Withdrawal: Although the doses suggested here usually will not cause severe withdrawal symptoms, they are possible, and may include sweating, nausea/vomiting, shaking, and agitation.
More Notes on Narcan• Storage: Narcan needs to be stored away from
extreme heat or cold and kept away from direct sunlight.
• Color: Narcan should be clear in color. Ask clients to return for a refill if it appears cloudy.
• Expiration Date: Tell clients to check expiration date on the box of Narcan on a regular basis (maybe once a month) and ask them to return for a refill if it is expired.

Miscellaneous notes for prescribers• Ensure that patients know that naloxone only works
on opioids, BUT that it will work on combination drug overdoses which include opioids (e.g., mixing opioids with benzodiazepines or alcohol).
• Make sure patients know what opioids are! (e.g., “opioids include morphine, codeine, oxycodone, Percocet, Darvon, Vicodin, hydrocodone and most other prescription pain medications, as well as methadone, buprenorphine, and heroin.”)
• Suggestion: tape an atomizer bag to each box of naloxone. That way both pieces are together if needed in an emergency.

Case Studies Which of the following patients might be offered
naloxone? Why or why not? What questions might you ask these patients?1. Mr. K is an Iraq war veteran on long-term opioids for
pain related to combat injuries.2. Ms. T is filling a suboxone prescription for 16mg QD X
30 days. 3. John is a 20-year old college student filling a
prescription for Vicodin #30 after dental surgery.4. Mrs. S is 62-years old and has a history of chronic
migraines and anxiety disorder. She has been using oral opioids for many years and now has a new prescription for a long-acting Fentanyl patch.

“Act as if what you do makes a difference. It does.”
― William James, American philosopher and psychologist (1842-1910)

Questions?????

Resources• Substance Dependence, Abuse and Treatment Need, Chapter 5,
National Survey on Drug Use and Health, SAMHSA, 2008-2009. http://www.samhsa.gov/data/2k9State/Ch5.htm#fig5.20
• Harmful Interactions: Mixing Alcohol with Medicines, National Institute on Alcohol and Alcoholism, NIH Publication No. 03-5329, Revised 2007 http://pubs.niaaa.nih.gov/publications/Medicine/Harmful_Interactions.pdf
• Good communication helps to build a therapeutic relationship, Nursing Times.net, June 2009 http://www.nursingtimes.net/nursing-practice/clinical-zones/educators/good-communication-helps-to-build-a-therapeutic-relationship/5003004.article
• Impact of Communication in Healthcare, Institute for Healthcare Communication, July 2011. http://healthcarecomm.org/about-us/impact-of-communication-in-healthcare/

Resources• Alston, C., Paget, L., Halvorson, G., Novelli, B., Guest, J., McCabe, Pl,
Hoffman, K., Koepke, C., Simon, M., Sutton, S., Okun, S., Wicks, P., Underm, T., Rohrbach, V., and Kohorn, V. Communicating with Patients on Healthcare Evidence, Institute of Medicine, September 2012. http://www.iom.edu/Global/Perspectives/2012/~/media/Files/Perspectives-Files/2012/Discussion-Papers/VSRT-Evidence.pdf
• ASHP Guidelines on Pharmacist-Conducted Patient Education and Counseling http://www.ashp.org/DocLibrary/BestPractices/OrgGdlPtEduc.aspx
• Harm Reduction Coalition, Opioid Overdose Basics http://harmreduction.org/issues/overdose-prevention/overview/overdose-basics/
• Prescribe to Prevent website http://prescribetoprevent.org/

















