Partnership for Reviving Routine Immunisation in Northern Nigeria, Maternal Newborn and Child Health Initiative (PRRINN-MNCH) Annual Review 2011: Narrative Report Fiona Duby August 2012 Final
Transcript
Partnership for Reviving Routine
Immunisation in Northern Nigeria,
Maternal Newborn and Child Health
Initiative (PRRINN-MNCH)
Annual Review 2011: Narrative Report
Fiona Duby
August 2012 Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 1 304298/ Final
Acknowledgements
The review would not have been possible without the plethora of excellent documentation which, in the absence of field visits, provided the basis for this review. Sincere thanks go to PRRINN-MNCH for their hard work in preparing for this review and providing the documentation including the presentations.
The review team could not travel to the states because of the political unrest but the state teams made the long and difficult journeys to Abuja to make their presentations and share their experiences. Sincere thanks to all those on the teams.
Thanks to Chris Collins, an observer from NPHCDA, and Jennifer Armitage from PATHS2 for their very useful technical contributions.
Thanks to Edward Idenu for all the preparatory work and logistic support for this mission and special thanks to Susan Elden, DFID Health Adviser for the northern states for arranging this mission.
It has been a challenge, if not an impossible task to capture the vast range of activities and accomplishments, and to do justice to the programme in this brief review in such a very short time. While the programme documentation provides significant and fascinating detail, there is no substitute for seeing the work on the ground. As a result, there are likely to be many omissions and some factual errors for which sincere apologies are made.
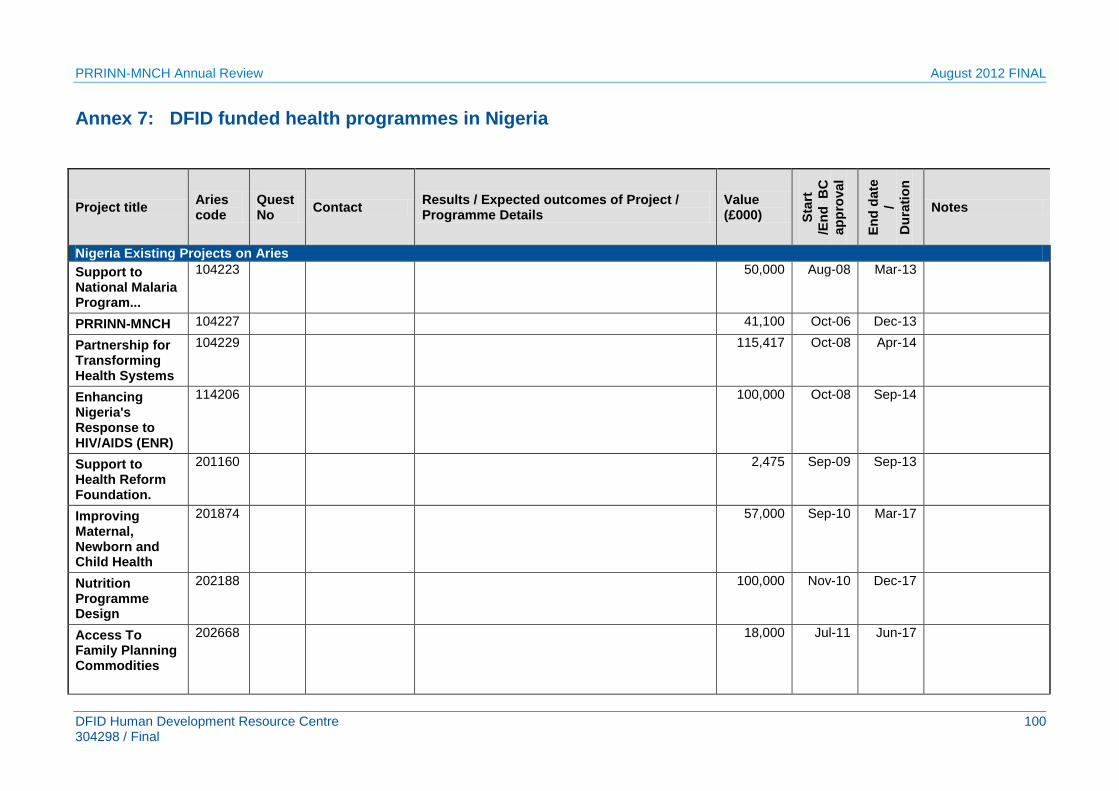
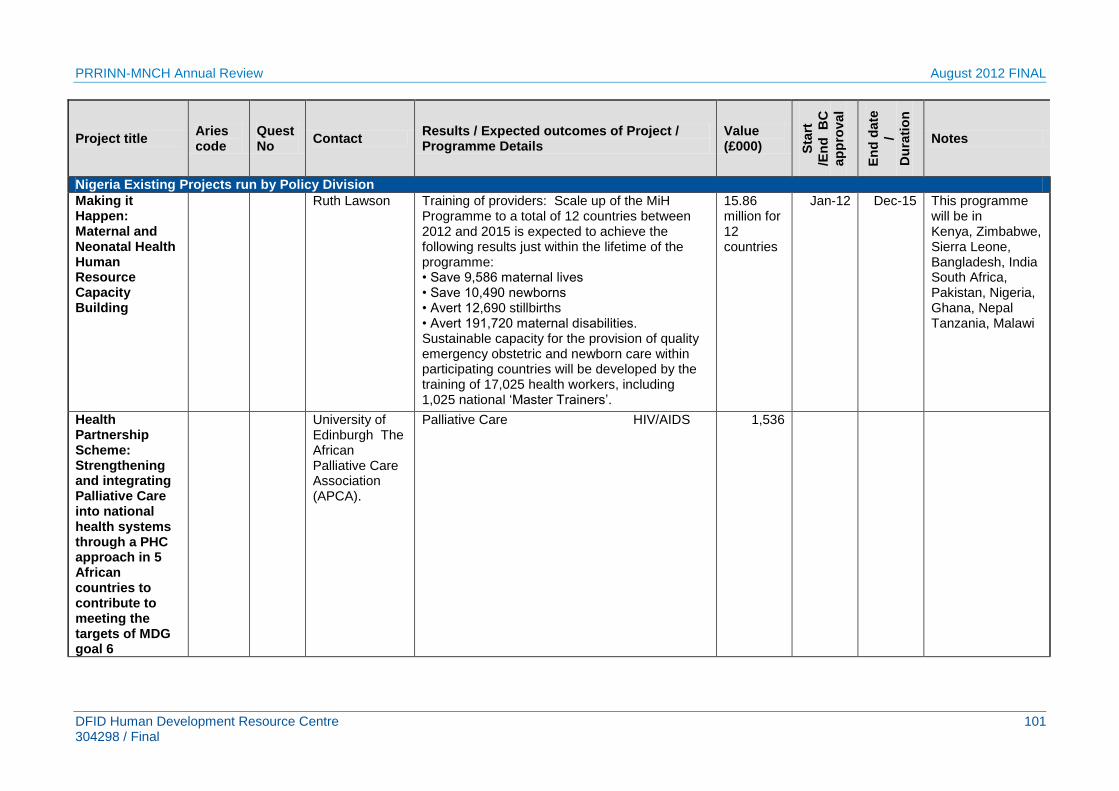
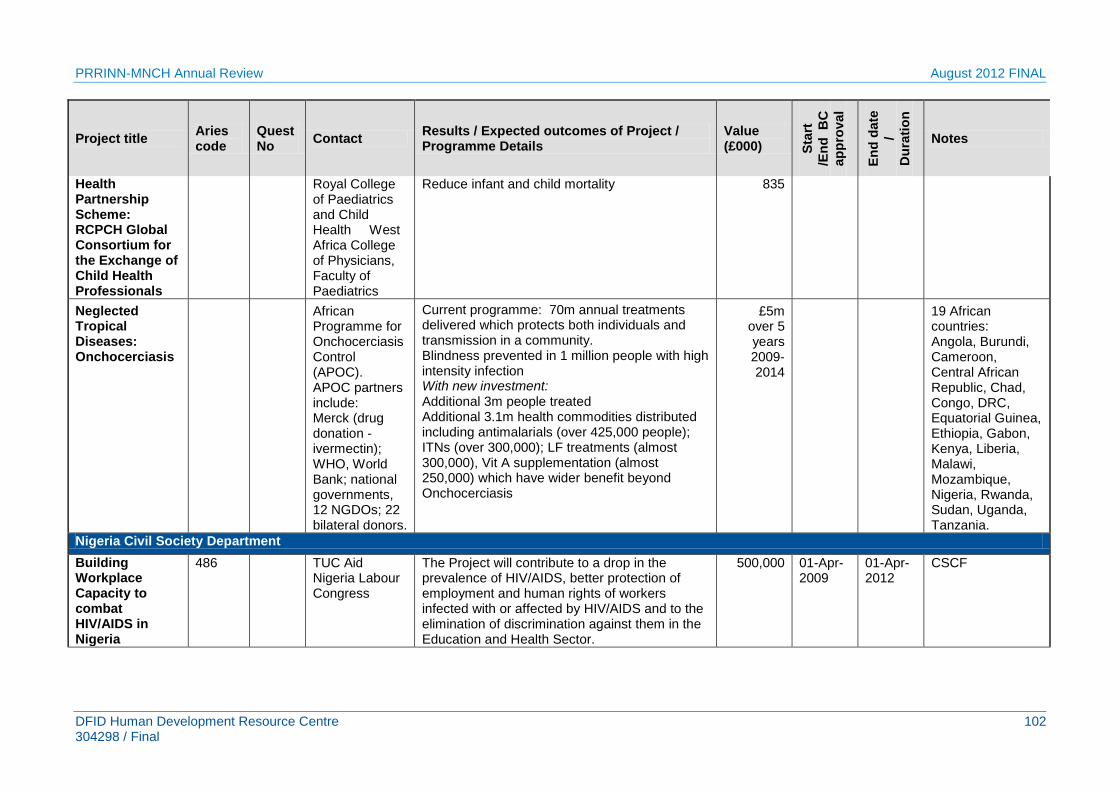
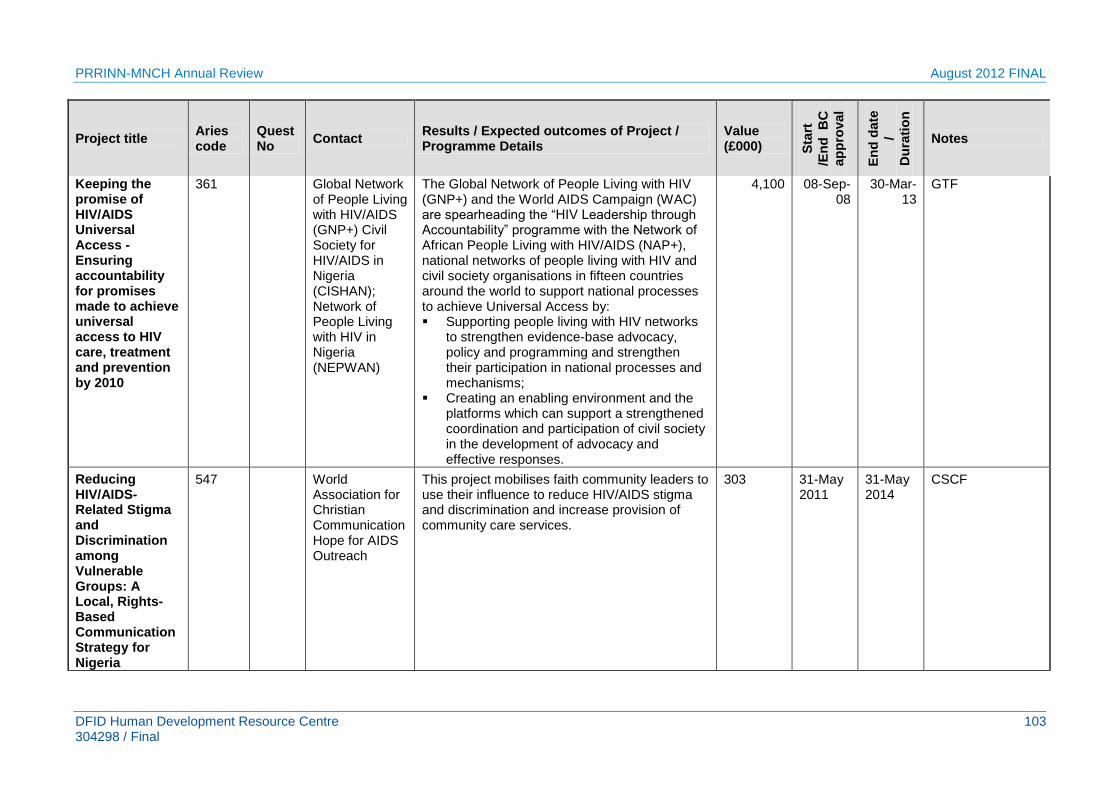
This report is accompanied by a document addressing Value for Money (VFM) of PRRINN-MNCH (Susan Elden) and another listing all the health and development programmes in the four focal states for reference.
Fiona Duby
Figure 1 Map of Nigeria showing PRRINN-MNCH states
PRINN-MNCH combined programme
Zamfara Katsina Yobe
PRRINN programme
Jigawa
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 2 304298/ Final
Acronyms and abbreviations
AFP Acute Flaccid Paralysis ANC Antenatal Care BCC Behaviour Change Communication BEOC Basic Emergency Obstetric Care CBOs Community Based Organizations CDC Centre for Disease Control CEOC Comprehensive Emergency Obstetric Care CHEW Community Health Extension Worker CHPS Community Health Planning and Services (in Ghana) CS Caesarean Section CSO Civil Society Organization DFID Department for International Development DHIS District Health Information System DRF Drug Revolving Fund ED Executive Director EDP Essential Drugs Programme EMC Emergency Maternal Care EOC Emergency Obstetric Care ES Executive Secretary ETS Emergency Transport Scheme FANC Focussed Antenatal Care FHD Family Health Department FMoH Federal Ministry of Health GAVI Global Alliance Vaccine Initiative GHSB Gunduma Health System Board HDSS Health Demographic Surveillance System (or Site) HDCC Health Data Consultative Committee HMH Honourable Minister of Health HMIS Health Management Information System HPO Health Promotion Officer HRCC Human Resource Coordinating Committee HRH Human Resources for Health HRIS Human Resource Information System HSR Health Sector Reform HSRP Health Sector Reform Programme ICC Inter Agency Coordinating Committee IPCC Inter-personal Communication and Counselling IPD Immunisation Plus Days IMCI Integrated Management of Childhood Illnesses LEC Local Engagement Consultant LEO Local Engagement Officer LID Local Immunisation Day LiST Lives Saved Tool LG/LGA Local Government/Local Government Area (or Authority) LGC Local Government Chairmen LLGA Learning LGA LOA Letter of Agreement LSS Life Saving Skills M & E Monitoring and Evaluation MDGs Millennium Development Goals
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 3 304298/ Final
MDR Maternal Death Review/Audit MLM Mid-level manager MLSS Modified Life Saving Skills MoH Ministry of Health MNCH Maternal Neonatal and Child Health MOU Memorandum of Understanding MSP Minimum Service Package MSS Midwives’ Service Scheme MTSS Medium Term Sector Strategy NAS Nigeria Academy of Science NASS NGO
National Assembly Non-Governmental Organization
NHIS National Health Insurance Scheme NICS National Immunisation Coverage Survey NIA National Immunisation Advisor NPHCDA National Primary Health Care Development Agency NPI National Program on Immunisation NVI OR
New Vaccine Initiative Operations Research
OP Operational Plan (for the Heath Sector) OPV Oral Polio Vaccine OPR Output to Purpose Review (DFID Annual Review) PATHS Partnership for Transforming Health Systems PEI Polio Eradication Initiative PHC Primary Health Care PHCUOR Primary Health Care Under One Roof PMS Programme monitoring system (or site) PPP Public private partnership PPRHAA Peer Participatory Rapid Health Appraisal RI Routine Immunisation SBA Skilled birth attendant SDP State Development Plan SSHDP State Strategic Health Development Plan SHDP Strategic Health Development Plan SHF Secondary Health Facility SIACC State Inter-Agency Coordinating Committee SLP State Lead Programme SMoH State Ministry of Health SM Safe Motherhood SON & M School of Nursing and Midwifery SOP State Operational Plan SDSS Sustainable Drug Supply System SSP State Strategic Plan (for the Health Sector) STL State team leader THE Total Health Expenditure TOR Terms of reference TOT Training of trainers TT Tetanus Toxoid UNICEF United Nations Children’s Fund WB World Bank WHO World Health Organisation WPV Wild Polio Virus
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 4 304298/ Final
1 Context ............................................................................................................ 15 1.1 Maternal, newborn and child health in northern Nigeria ............................. 15
1.1.1 Maternal health .................................................................................. 15 1.1.2 Newborn and child health ................................................................... 16
1.2 Governance and systems reform .............................................................. 17
2 Background to PRRINN-MNCH programme ................................................. 19
3 Methodology ................................................................................................... 20 3.1 The evaluation team .................................................................................. 20
4.2.1 Likely contribution to state and national performance and influence on policy and practice ........................................................................................... 22 4.2.2 Headlines for each state..................................................................... 23
4.3 Output assessments ................................................................................. 24 4.3.1 Output 1: Strengthened State and LGA governance ......................... 24 4.3.2 Output 2: Improved human resource policies and practices .............. 29 4.3.3 Output 3: Improved delivery of RI and MNCH services ...................... 32 4.3.4 Output 4: Operational Research ......................................................... 37 4.3.5 Output 5: Improved Information generation and use ........................... 39 4.3.6 Output 6: Increased demand for RI and MNCH services .................... 41 4.3.7 Output 7: Improved capacity of Federal Ministry level ........................ 44
5 Risk analysis and mitigation ......................................................................... 47 5.1 Key challenges .......................................................................................... 47 5.2 Other challenges ....................................................................................... 47
6 Key strengths and challenges of partnership with Government ............... 49
7 Partnerships and synergy with other related programmes ......................... 50 7.1 Programme partners ................................................................................. 50 7.2 DFID-funded state partners ....................................................................... 51
7.2.1 Governance programmes ................................................................... 51 7.2.2 Health programmes ............................................................................ 51
7.3 Other health partners ................................................................................ 53
8 Overall conclusions, lessons and implications for the future .................... 54
Annex 9: Terms of Reference ........................................................................... 110
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 5 304298/ Final
Tables
Table 1: PRRINN-MNCH project scoring by output ................................................. 14 Table 2: Profile of PRRINN-MNCH focal states compared with national profile ....... 19 Table 3: Annual Review team members .................................................................. 20 Table 4: Progress against expected results ............................................................. 22 Table 5: Performance against Output 1 indicators ................................................... 25 Table 6: Performance against Output 2 indicators ................................................... 30 Table 7: Performance against Output 3 indicators ................................................... 32 Table 8: Progress against Output 4 indicators ......................................................... 37 Table 9: Progress against Output 5 targets ............................................................. 39 Table 10: Progress against logframe targets ........................................................... 41 Table 11: Progress on Maternal health M&E indicators from mid-term evaluation ... 42 Table 12: Progress against Output 7 targets ........................................................... 45
Figures
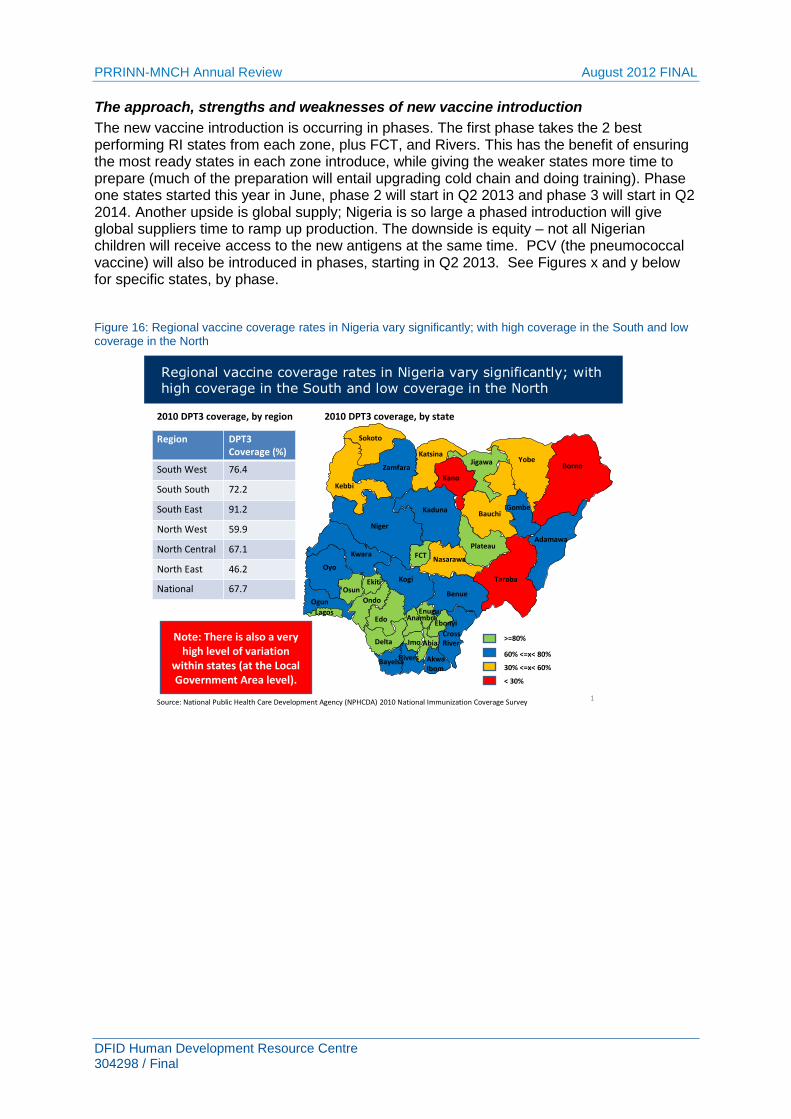
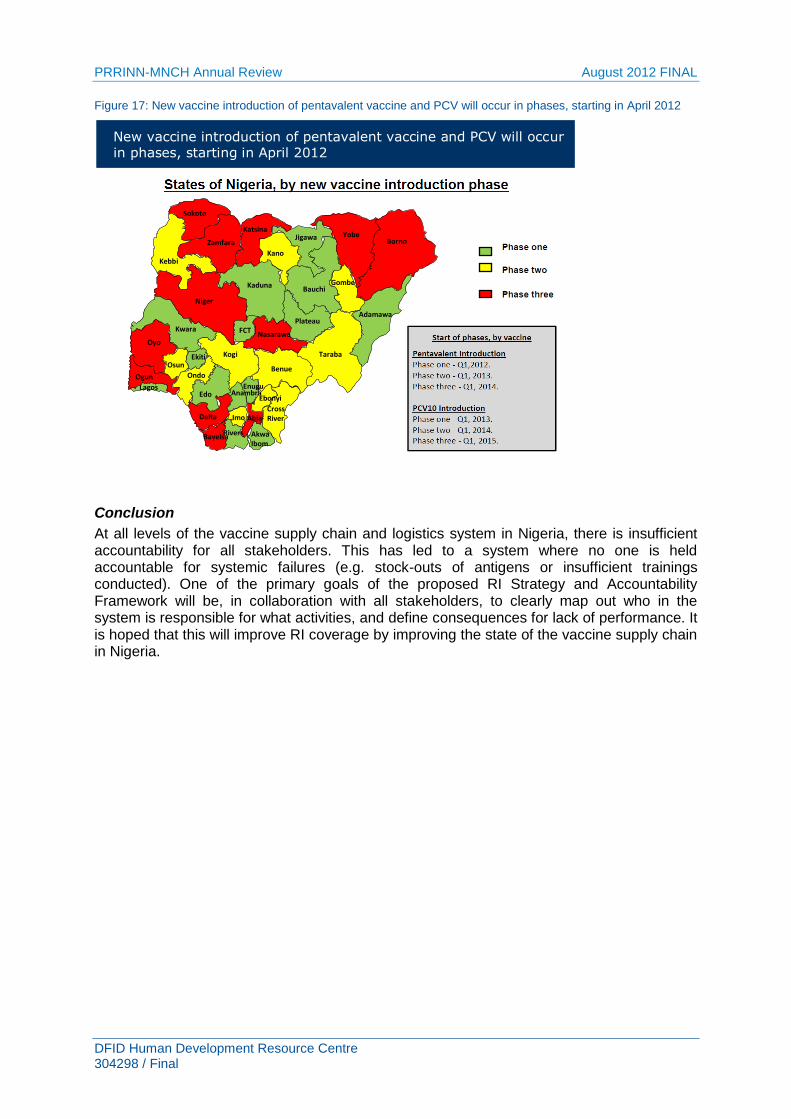
Figure 1 Map of Nigeria showing PRRINN-MNCH states .......................................... 1 Figure 2: Actual and projected Maternal Mortality Rate ........................................... 15 Figure 3: % Contraceptive prevalence in 4 states and nationally ............................ 15 Figure 4: Causes of under 5 mortality in the 4 PRRINN-MNCH states.................... 16 Figure 5: Causes of neonatal mortality in Nigeria .................................................. 16 Figure 6: Children fully immunised by history or card ............................................. 17 Figure 7: Government spending on health .............................................................. 18 Figure 8: Infant mortality rate across states ............................................................. 21 Figure 9: % births attended by skilled attendants ................................................... 21 Figure 10: Trends in budget allocated to health in Jigawa ....................................... 26 Figure 11: Immunisation coverage .......................................................................... 33 Figure 12: Barriers to uptake of immunisation services reported by state personnel34 Figure 14: Contraceptive use in PRRINN-MNCH states by age .............................. 36 Figure 15: Knowledge of at least 4 of the danger signs by gender ........................... 42 Figure 16: Regional vaccine coverage rates in Nigeria vary significantly; with high coverage in the South and low coverage in the North .............................................. 95 Figure 17: New vaccine introduction of pentavalent vaccine and PCV will occur in phases, starting in April 2012 .................................................................................. 96
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 6 304298/ Final
Executive summary
Background
The Partnership for Reviving Routine Immunisation in Northern Nigeria (PRRINN) and the Northern States Maternal, Newborn and Child Health Initiative (MNCH) is a six-year programme working across four states in Northern Nigeria. It is jointly funded by DFID and the Government of Norway. The programme began in 2006 as a DFID-funded health system project with a focus on routine immunisation (£19m).
In September 2008, the same consortium with some additional partners (Liverpool Associates in Tropical Health, Mailman School of Public Health, Columbia University and Ahmadu Bello University) was awarded an additional contract to extend the PRRINN programme to a MNCH programme to three of the four states (Katsina, Yobe and Zamfara).1 The funding for this extension was from the State Department of the Norwegian Government who provided an additional £24m to target maternal, neonatal, and child health (MNCH) components. This is now run as a joint programme (PRRINN-MNCH) with UKAID as the co-ordinating development partner. The Partnership for Transforming Health Systems (PATHS2) programme leads on MNCH activities in Jigawa.
In October 2010, DFID provided a funding extension of £19m for both PRRINN and MNCH, until 2013, with revised results that double coverage of maternal and newborn care interventions. Funding for PRRINN-MNCH now totals £61 million.
In January 2012 the programme was awarded a further £4 million by DFID in connection with the DFID Girl Hub Initiative, a partnership between DFID and the Nike Foundation, to add a focus on young women into ongoing programme activities. This is expected to improve health equity by increasing married young women‟s access to essential maternal and newborn health services (ANC, birth spacing, skilled birth attendance, and post-natal care) and to advise on reproductive health and nutrition.
2011 Annual Review
The annual review team consisted of one external consultant, a health adviser, state representative, and delegate from Government of Norway and one observer from NPHCDA, with additional input from an expert on value for money (VFM). This „light touch‟ review was conducted over a four day period with a de-brief to the PRRINN-MNCH team on the fifth day. It was intended that the team would spend three of these days visiting Zamfara and Katsina states however this was not possible owing to the uncertain security situation. Instead, the PRRINN-MNCH state teams from Jigawa, Katsina, Zamfara and Yobe all made presentations in Abuja. The team also had meetings with a number of key stakeholders in Abuja. The review therefore had to rely fully on the information provided by PRRINN-MNCH and from key informant interviews. The team was therefore very grateful for both the quality and range of presentations and reports generated by the programme.
Summary of key findings and recommendations
General
Working in northern states poses significant challenges and more so during the past year with civil disturbances. These notwithstanding, the PRRINN-MNCH 2011 mid-term household survey results suggest that the state governments, with support of PRRINN-MNCH have brought about substantial improvements in maternal and infant health: infant mortality in the intervention communities reduced from 90 to 55.6 per 1,000 live births.
1 PATHS2 covers MNCH programming in Jigawa State
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 7 304298/ Final
The programme has achieved positive results against most outcome indicators. Of the 7 outcome indicators, 5 have already been surpassed, one, CPR, is likely to be achieved and polio might decline to near zero cases, if exogenous factors do not impede progress. There has been a 270% increase or an additional 24,748 women per annum attending antenatal care (ANC) and a 271% increase or an additional 13,998 women being delivered by skilled birth attendants (SBAs) each year in targeted facilities in the CEOC first clusters from a baseline of 11.2% to 23.4%. In addition, the proportion of fully immunised of children has risen by 314% (an additional 222,141 children) each year. All this has been achieved in an environment in which there is still emphasis on polio eradication and numerous problems associated with vaccines, including inefficient distribution and stock-out, non-availability of documents for vaccine management, poor record keeping, insufficient cold chain capacity and lack of maintenance and repair. Various interventions initiated by the programme have been adopted at federal level for national roll-out. These include among others, the Maternal Death Audit, and various technical tools adapted by NPHCDA. Achievements at output level have also been impressive. The following provides some of the highlights and recommendations under each output.
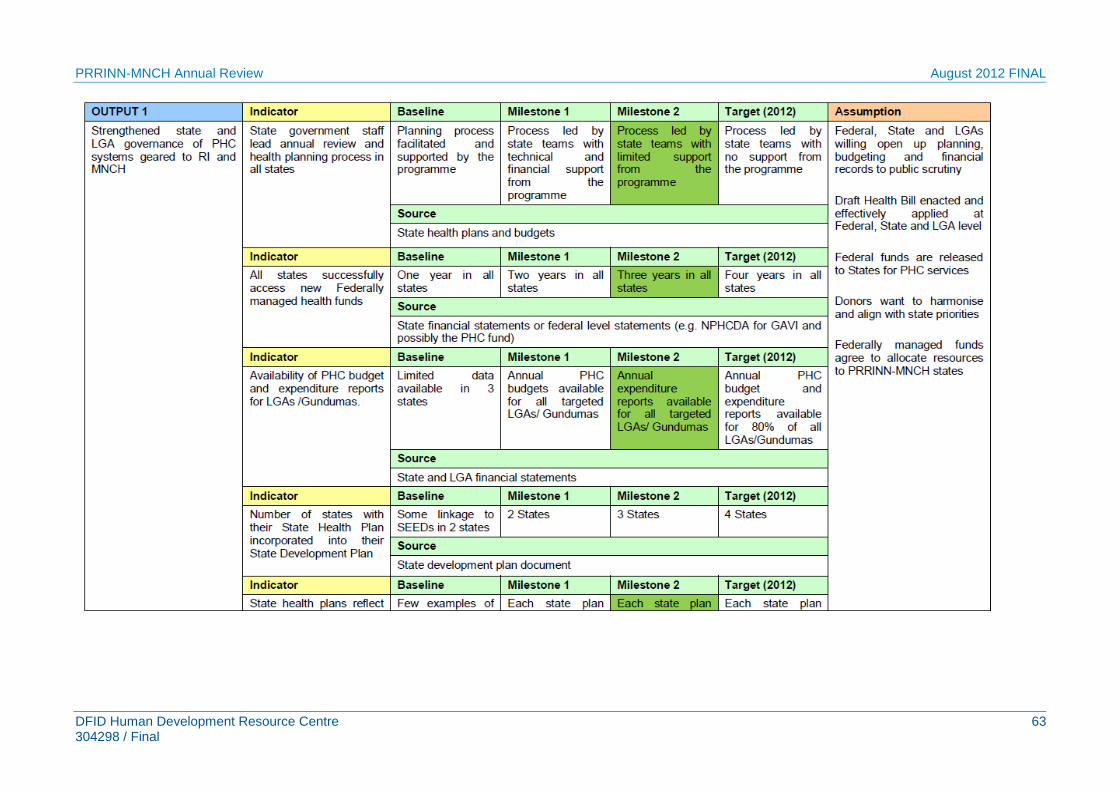
Output 1: Strengthened State and LGA governance of PHC systems geared to RI and MNCH
The PRRINN programme approach has focused on improving the PHC delivery system as a way to increase immunisation coverage. This systems approach has been carried over into the combined PRRINN-MNCH programme. This first output focuses on the policy and strategy framework within which the health system functions and deals with policy and planning; partner co-ordination; advocacy and institutional change; and Public Finance Management (PFM).
Of the seven indicators, five have been achieved and two partially achieved. PHCUOR has gained state-level recognition and is being implemented in state-specific ways in one form or another in each of the 4 states – a major improvement from the previous fragmented institutional arrangements. Jigawa appears to be most advanced (with 12% budget allocation and 80% of resources used for Human Resources); Zamfara and Yobe commencing and Katsina beginning the process. It will be important that Zamfara advance their agenda of the Basket Fund and build on this achievement. Other highlights include: developing the Minimum Service Package; building blocks for a service investment plan; strengthening public financial management systems; and creating an Eminent Persons Group.
Recommendations for Output 1:
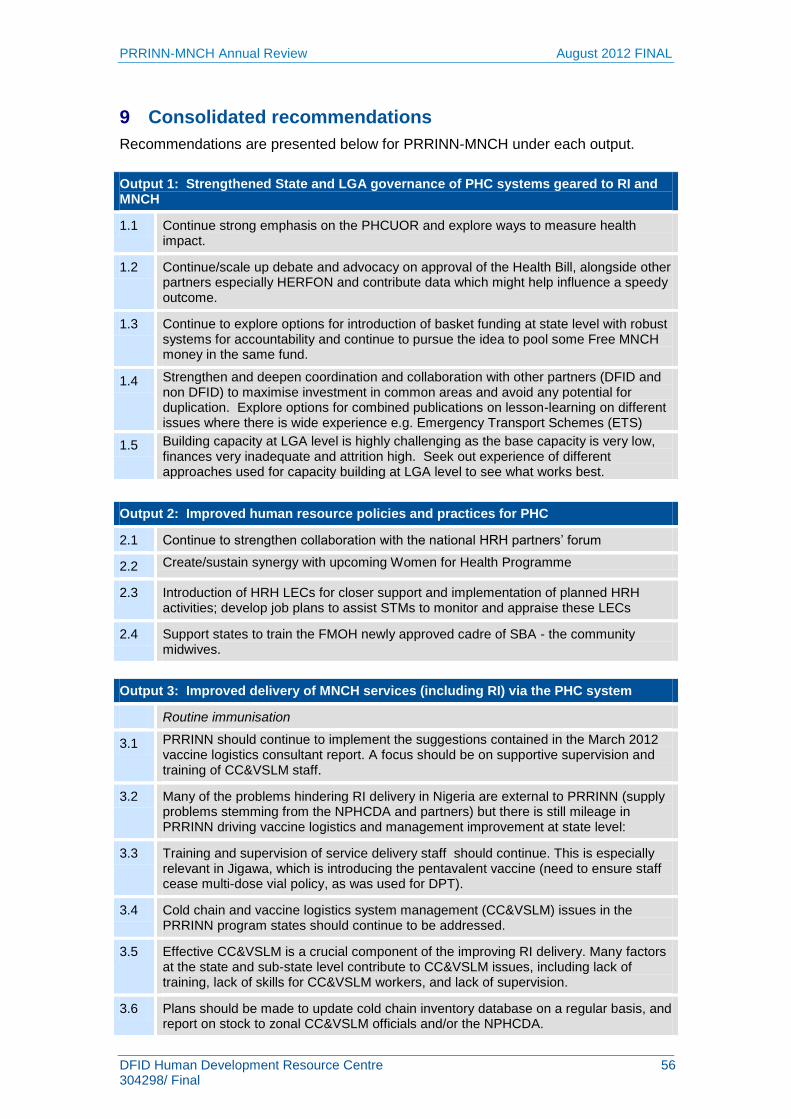
1.1 Continue strong emphasis on the PHCUOR and explore ways to measure the health impact.
1.2 Continue/scale up debate and advocacy on approval of the Health Bill, alongside other partners especially HERFON and contribute data which might help influence a speedy outcome.
1.3 Continue to explore options for introduction of basket funding at state level with robust systems for accountability and continue to pursue the idea to pool some Free MNCH money in the same fund.
1.4 Support the state to develop a detailed map of programmes, using appropriate software, down to LGA (and district levels if possible). This will need to be
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 8 304298/ Final
updated and LGAs empowered to track current and incoming resources, all of which need to be reflected in plans and budgets.
1.5 Continue to build the collaboration with SAVI and SPARC. Strengthen and deepen coordination and collaboration with other partners (DFID and non DFID) to maximise investment in common areas and avoid any potential for duplication. Explore options for combined publications on lesson-learning on different issues where there is wide experience e.g. Emergency Transport Schemes (ETS).
1.6 Building capacity at LGA level is highly challenging as the base capacity is very low, finances very inadequate and attrition high. Seek out experience of different approaches used for capacity building at LGA level to see what works best.
For DFID:
1.7 Maintain and improve the frequency and quality of monthly partner coordination meetings.
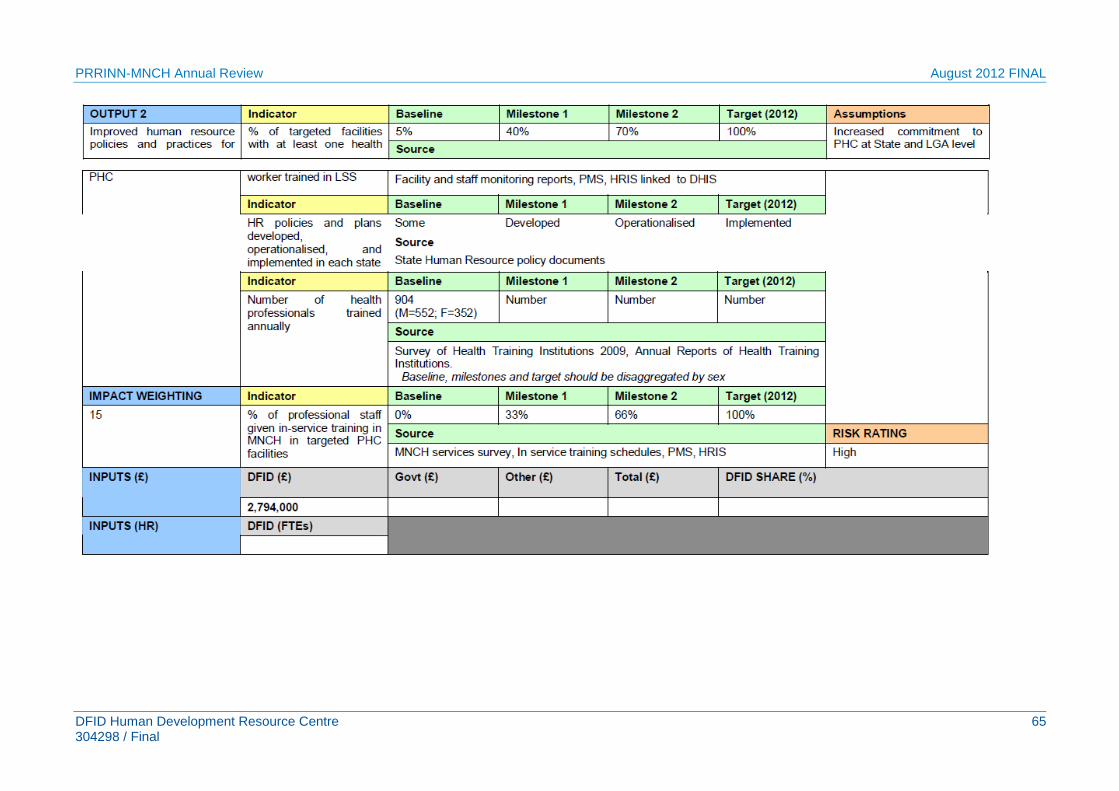
Output 2: Improved human resource policies and practices for PHC
Output 2 focuses on human resource management which is so vital for effective health service delivery. This is as much dependent on production factors, information systems, distribution, staff mix, recruitment and retention as it is on the political factors influencing human resources. Strengthening HR management is a major thrust of the PRRINN-MNCH programme as this is seen as one of the key bottlenecks to improving the PHC services in Nigeria.
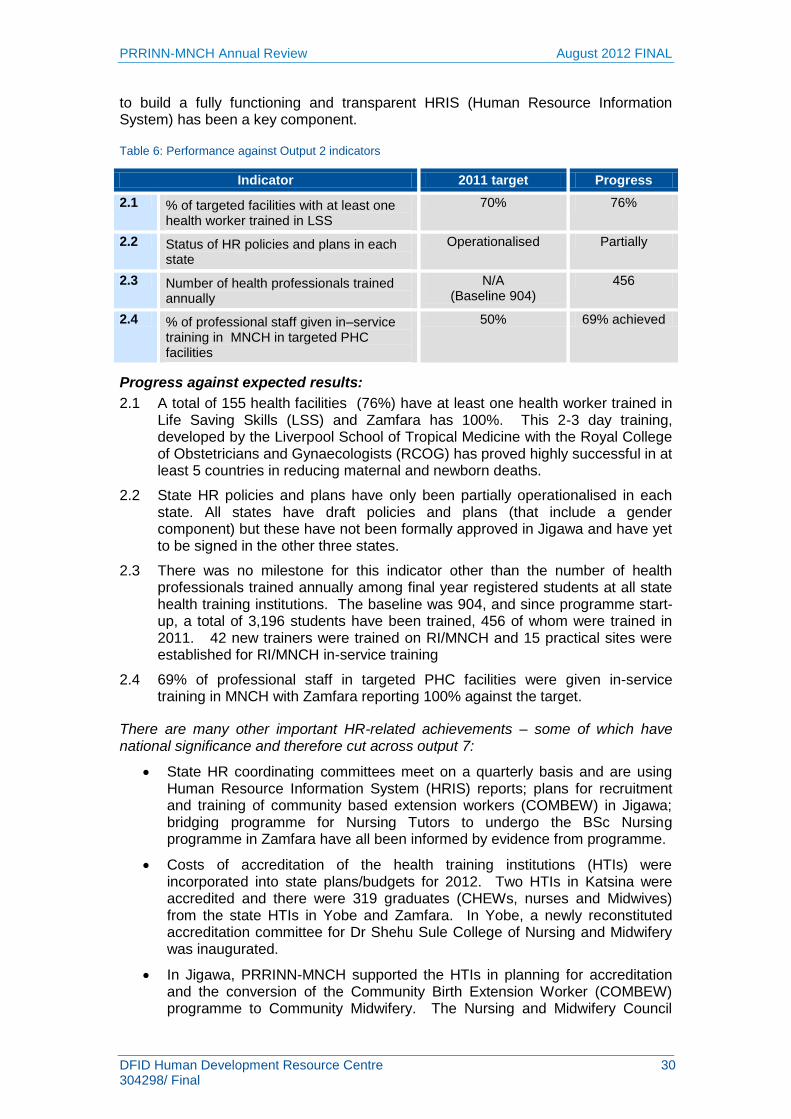
Increasing the numbers and distribution of female health workers in northern Nigeria is a priority. Focus has been on accreditation of schools and training institutions and, improving the throughput rate of training institutions. Helping to build a fully functioning and transparent HRIS (Human Resource Information System) has been a key component. Of the four indicators, one was achieved, and the three others not fully achieved.
Recommendations for Output 2
2.1 Continue and strengthen collaboration with the national HRH partners‟ forum
2.2 Introduction of HRH LECs for closer support and implementation of planned HRH activities; develop job plans to assist STMs to monitor and appraise these LECs
2.3 Support states to train the FMOH newly approved cadre of SBA - the community midwives.
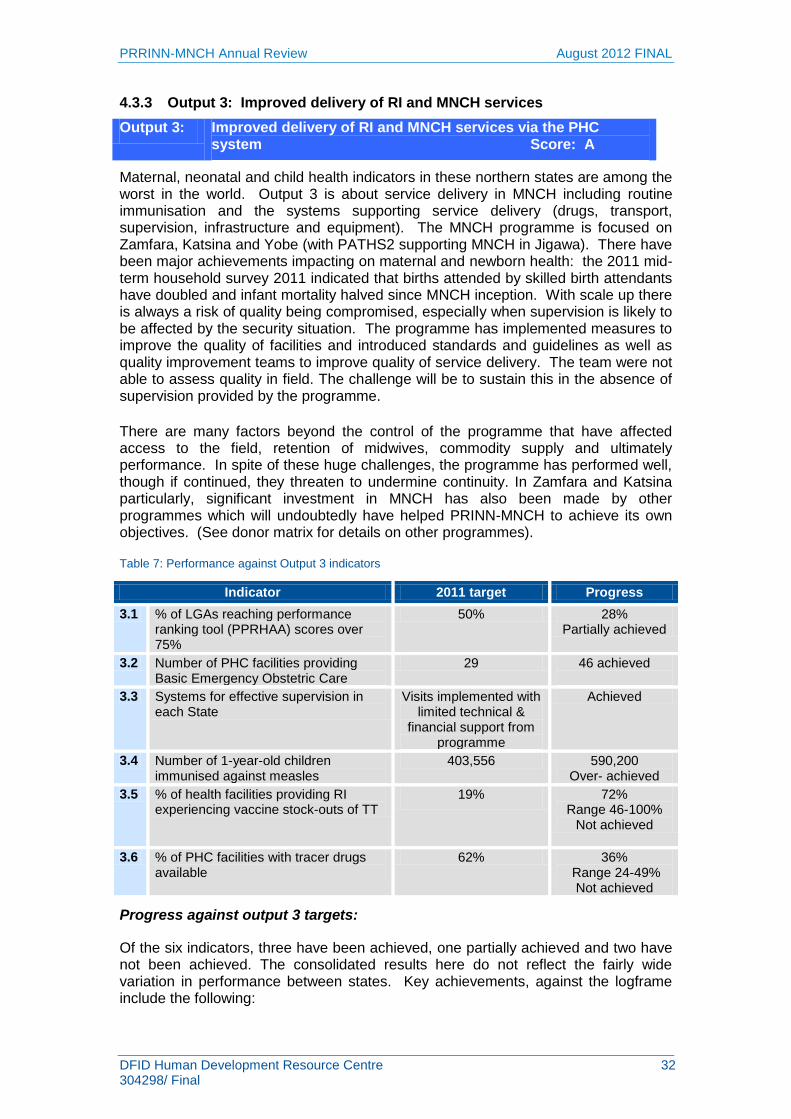
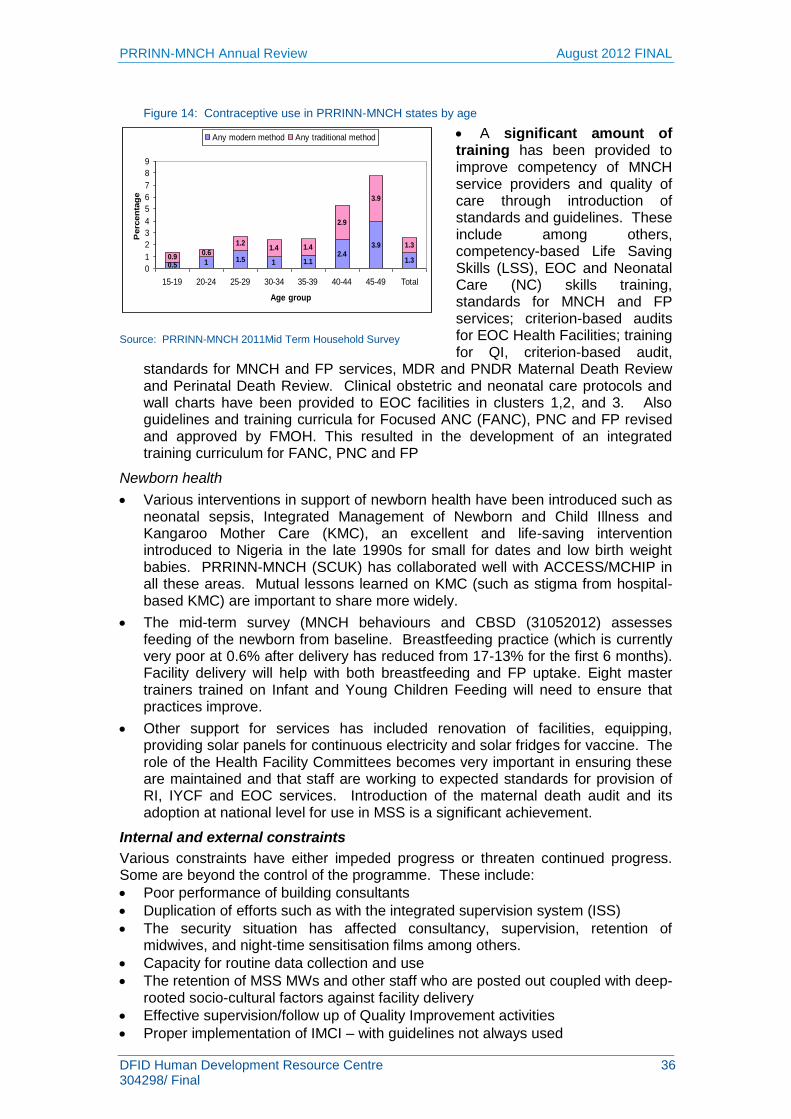
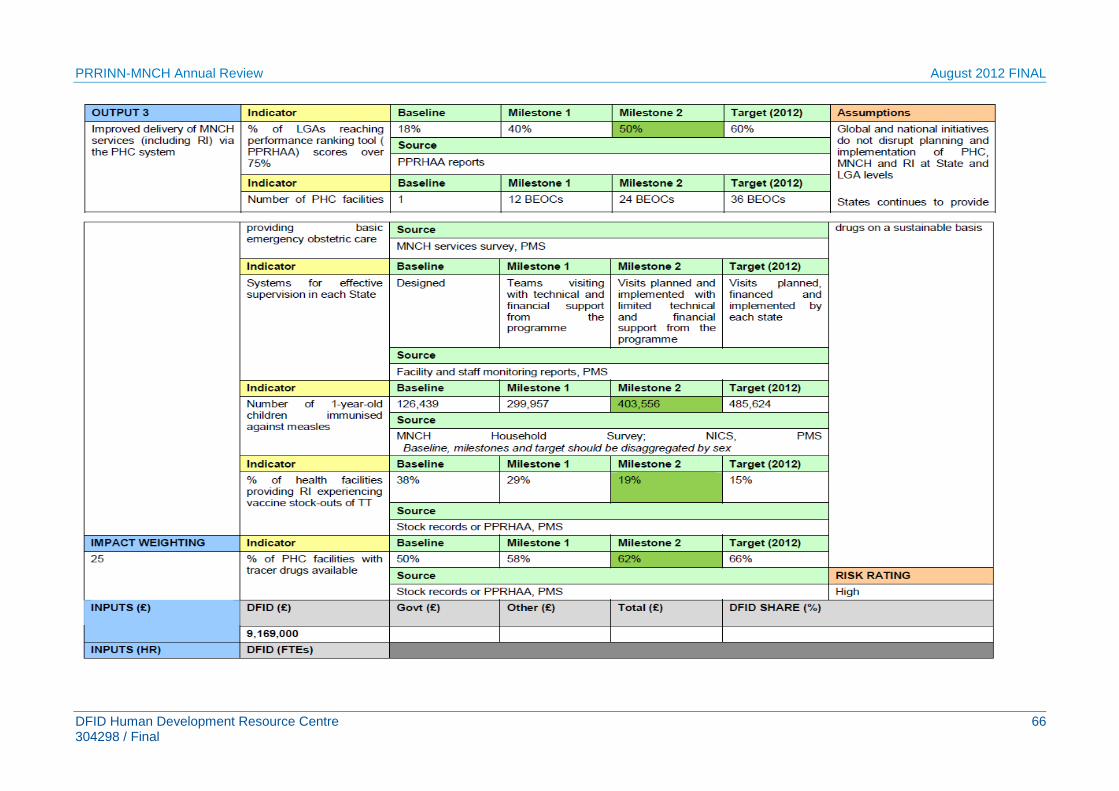
Output 3: Improved delivery of RI and MNCH services via the PHC system
Maternal, neonatal and child indicators in these northern states are among the worst in the world. Output 3 is about service delivery in MNCH and routine immunisation and the systems supporting service delivery (drugs, transport, supervision, infrastructure and equipment). There have been major achievements impacting on maternal and newborn health: the 2011 mid-term household survey 2011 indicated that births attended by skilled birth attendants have doubled and infant mortality halved since MNCH inception. Of the six indicators, three met their targets, one partially and two under achieved.
There are many factors beyond the control of the programme that have affected access to the field, retention of midwives, commodity supply and ultimately performance. In spite of these huge challenges, the programme has performed well.
Recommendations for Output 3
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 9 304298/ Final
Routine immunisation
3.1 The study PRRINN commissioned in March is a great first step. A focus should be on supportive supervision and training of CC&VSLM staff.
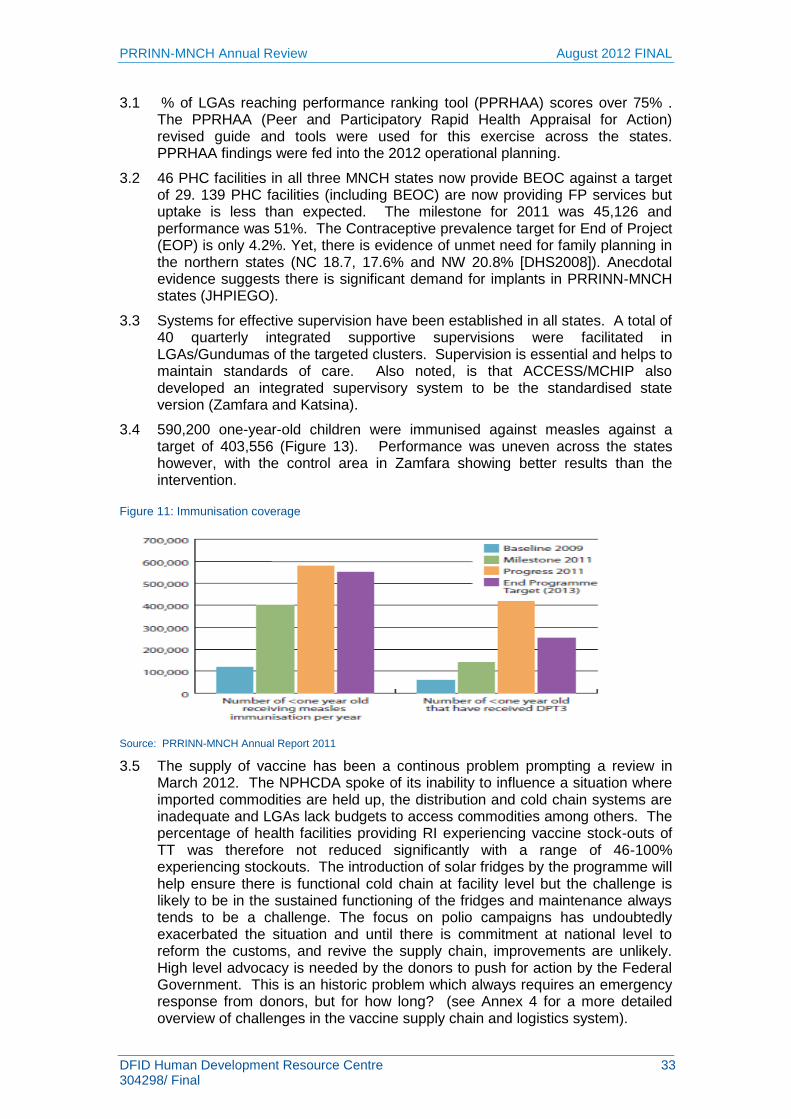
3.2 Many of the problems hindering RI delivery in Nigeria are external to PRRINN (supply problems stemming from the NPHCDA and partners) but there is still mileage in PRRINN driving vaccine logistics and management improvement at state level.
Training and supervision of service delivery staff should continue. This is especially relevant in Jigawa, which is introducing the pentavalent vaccine.
Cold chain and vaccine logistics system management (CC&VSLM) issues in the PRRINN program states should continue to be addressed.
Effective CC&VSLM is a crucial component of the improving RI delivery. Many factors at the state and sub-state level contribute to CC&VSLM issues, including lack of training, lack of skills for CC&VSLM workers, and lack of supervision.
Plans should be made to update cold chain inventory database on a regular basis, and report on stock to zonal CC&VSLM officials and/or the NPHCDA.
Ongoing strengthening of planned preventive maintenance for cold chain equipment should continue.
PRRINN should advocate that any new cold chain equipment procured at the state level be certified vaccination equipment, and that equipment is allocated to LGAs/sites based on need/population base.
3.3 Waste disposal is an area which requires additional attention and assessment. Training should continue, as should construction of burn and bury sites and distribution of injection safety boxes. Supervisory visits to sites should ensure injection waste is safely disposed and disposal sites appropriately maintained.
3.4 Continue to support programme states to draw on GAVI funds (e.g. ISS funds). Work with states to facilitate receipt of funds from the NPHCDA.
Maternal health
3.5 The mid-term review and other studies provide important qualitative evidence to inform service delivery to be „mother friendly‟ and meet women‟s specific needs. This might include maternity waiting homes to reduce the second delay and provide opportunities for appropriate antenatal and postnatal support.
3.6 Ensure support and supervision of newly qualified midwives (including MSS) and those having received classroom-based LSS training.
3.7 The 2011 MTR recommendations on FP still stand and action points recommended from the 2011 household survey are appropriate but too general and not new.2 The evidence on FP and spacing) in reducing maternal, perinatal and child mortality is overwhelming.3 Postpartum care is critical and FP should be integral.
3.8 Compare experience with other programmes on a range of issues where challenges have arisen such as Emergency Transport schemes and compensation, Family Planning.
3.9 There are many different LSS tools being used. PRRINN-MNCH should continue to contribute to the (PATHS2-supported) LSS harmonising project led by the FMOH and first attended by LSTM.
2 PRRINN-MNCH FACT SHEET: Women‟s awareness and use of FP : Findings from the 2011 Midterm Household
Survey. 3 Contraception and health. John Cleland et al. Lancet. Family Planning series. July 2010.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 10 304298/ Final
3.10 There were delays in procurement and therefore supply of equipment and essential medicines through the Crown Agent‟s contract. The situation is now improving with better quantification and communication among others. Since the states will not, in the long term be procuring through the Crown Agents, it is vitally important that state capacity for transparent and effective procurement is built without delay.
3.11 There is evidence that removing fees for facility delivery increases use of facilities but also that out-of-pocket expenses are still required. It will be useful to track these trends through OR.
Newborn health
3.12 The problem of vaccine procurement and distribution is larger than PRRINN-MNCH can tackle. It is recommended that donor agencies use their combined influence to exert pressure at national level on the Minister of Health. PRRINN-MNCH‟s role will be to provide updated data to use for advocacy.
3.13 Reinforcing IMCI and growth monitoring at PHC facility level is important alongside routine immunisation. Adherence to treatment protocols needs consistent monitoring.
Procurement and distribution is larger than PRRINN-MNCH can tackle.
3.14 It is recommended that donor agencies use their combined influence to exert pressure at national level on the Minister of Health. PRRINN-MNCH‟s role will be to provide updated data to use for advocacy.
Public Private Partnerships
3.15 SFH reports that they have 60 distributors throughout the country who could easily transport commodities. PRRINN-MNCH might explore ways with other programmes and partners to assist with distribution of essential commodities.
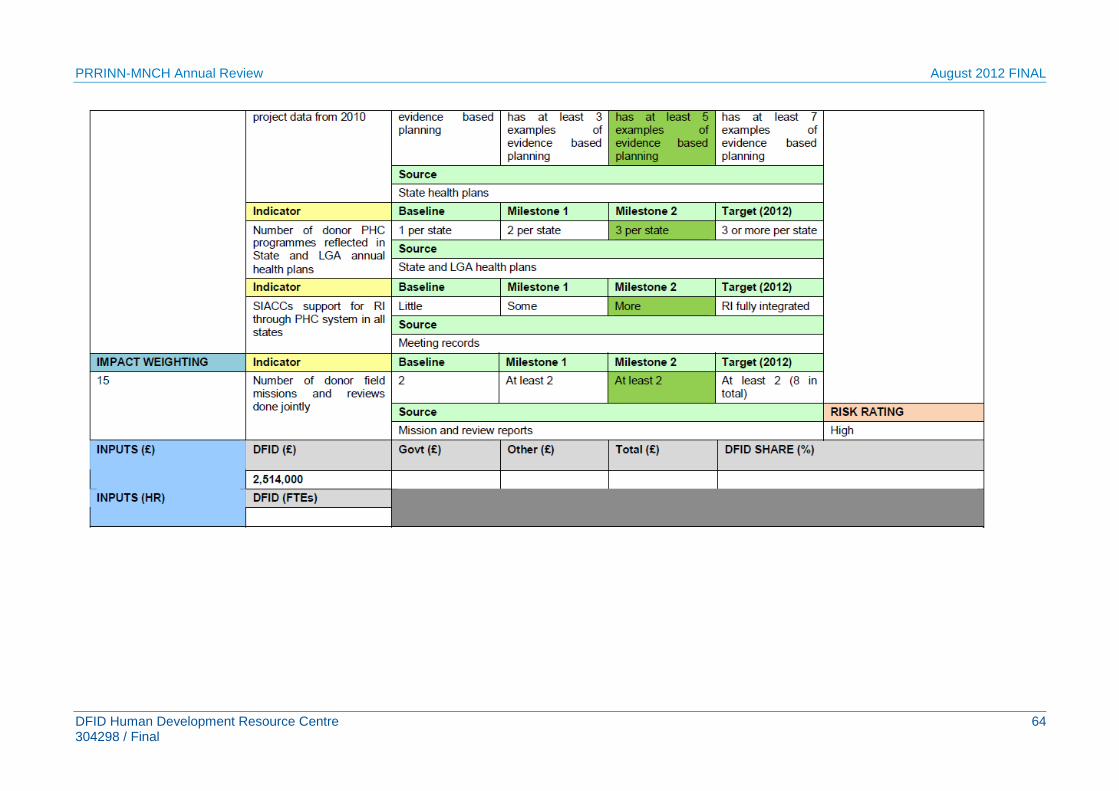
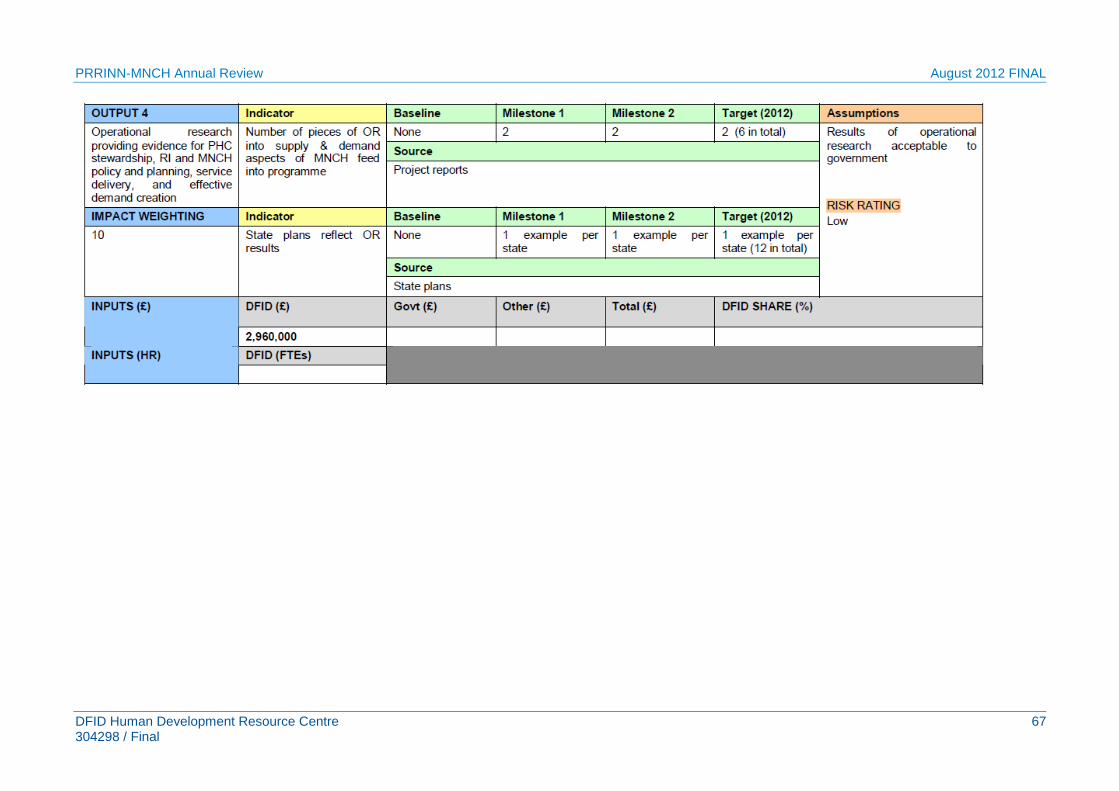
Output 4: Operational research providing evidence for PHC stewardship, RI and MNCH policy and planning, service delivery, and effective demand creation
A study in Nigeria revealed that some of the major challenges in informing policy and practice with evidence from health systems research are capacity constraints at individual and organisational levels, communication gaps and poor networking between policy makers and researchers, and the non-involvement of healthcare recipients in identifying and planning care delivery needs.
Output 4 cuts across all others. There is emphasis on strengthening OR capacity and on the use and dissemination of the results. The core activities of the health systems research component of the PRRINN MNCH project are to build a sustainable operations research capacity, conduct research (including performance based financing), and develop an Health Demographic Surveillance Site (HDSS) that meets international data quality standards.
Recommendations for Output 4
4.1 Summary reports would be useful of the various studies being conducted across areas such as: Performance Based Financing (PBF), Emergency Transport Support (ETS) and Community Based Service Delivery (CBSD). Lessons learnt and OR findings could be disseminated with the World Bank Health Results Innovations Trust Fund (on PBF) and the international forum generally.
4.2 To ensure smooth handover to the University of Sokoto it is important to share learning on how analysis and research is undertaken and written up.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 11 304298/ Final
4.3 The Annual Report 2011 reported on data coming out of the mid-term household survey. Analysis of this data is especially important when anomalies in the data exist that might require further explanation.
4.4 A further recommendation on the HDSS site is to continue to seek membership of the INDEPTH network. This network can provide a good way to connect with other HDSS sites and share learning and best practice which can support the development of the Zamfara site.
4.5 Developing a narrative on OR across the life of the PRRINN-MNCH programme would be an appropriate end document for the OR component. This way the findings and lessons learnt across all the research conducted will enable detailed evidence based approaches to the design and implementation of future programmes.
4.6 It would be useful to know how PRRINN-MNCH‟s experience compares with that of ACCESS/MCHIP in the same states in areas including Kangaroo Mother Care where similar challenges have been highlighted.
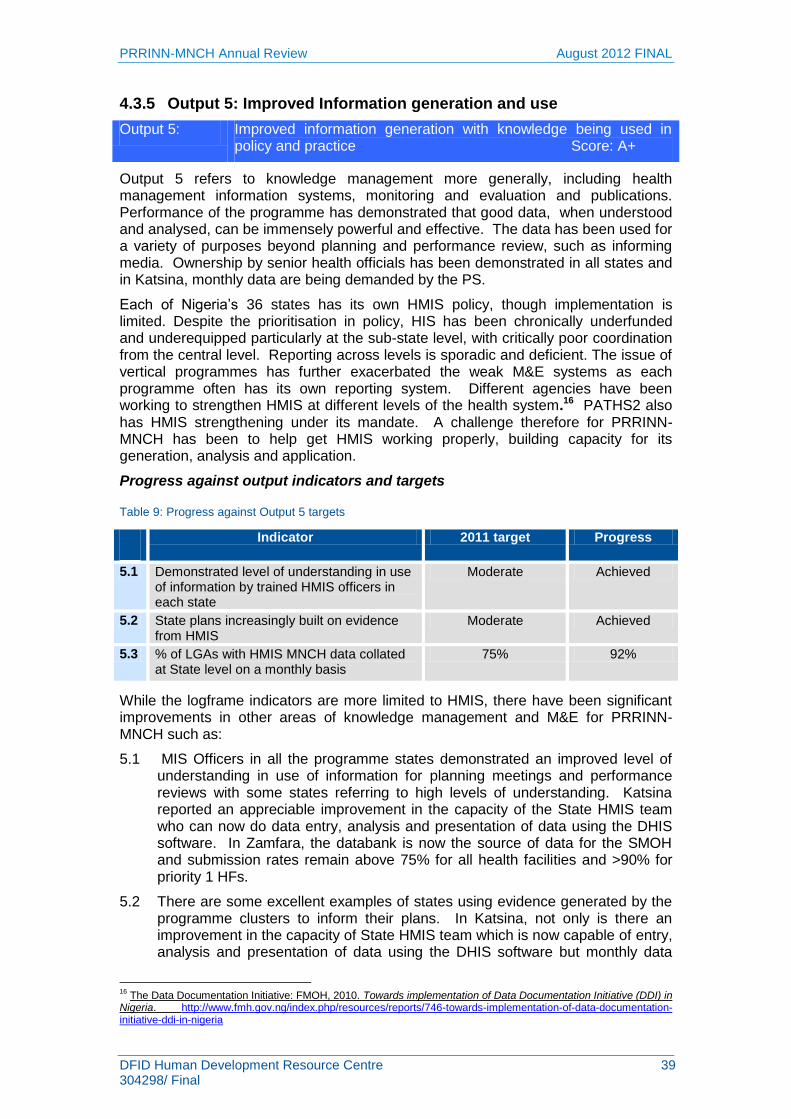
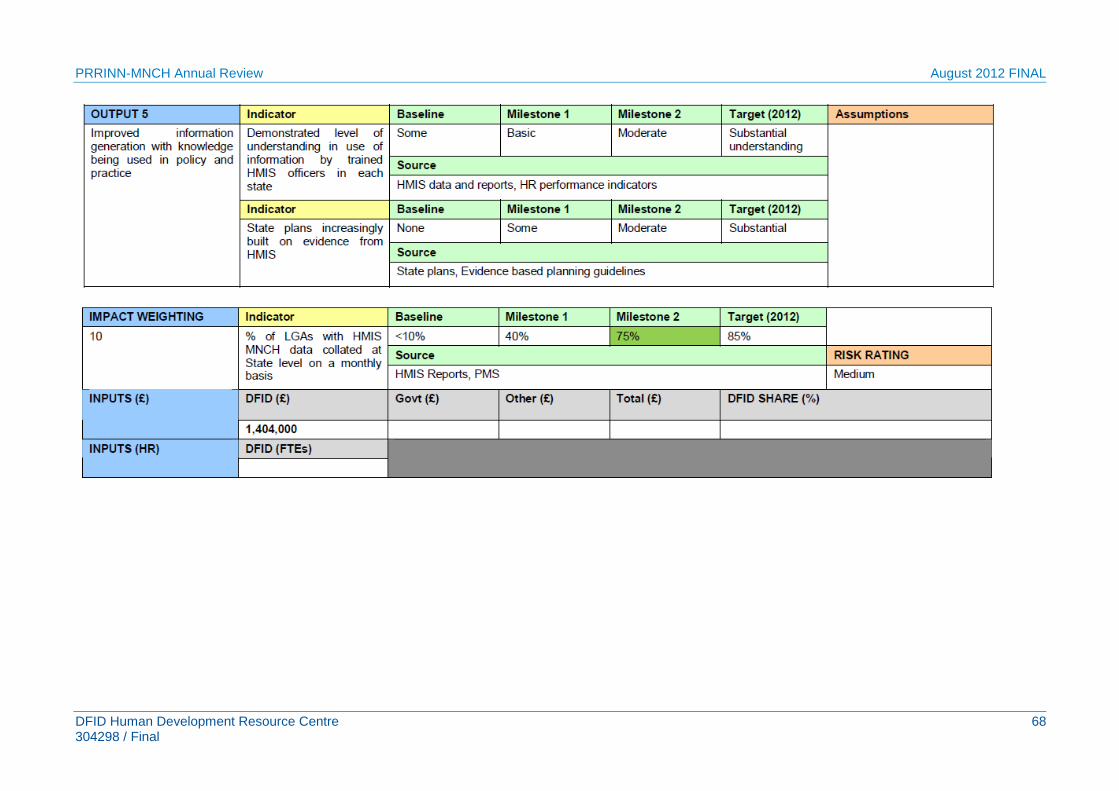
Output 5: Improved information generation with knowledge being used in policy and practice
Output 5 has demonstrated that good data, when understood and analysed, can be immensely powerful and effective. The study tour organised by PRRINN-MNCH to South Africa clearly had an impact. The data has been used for a variety of purposes beyond planning and performance review, such as informing media. Ownership by senior health officials has been demonstrated in all states and in Katsina, monthly data are being demanded by the PS. This output goes beyond HMIS – into knowledge management more generally with international publications and M&E.
Recommendations for Output 5
5.1 It is rightly stated in PRRINN documentation, that the government must own the programme and the products because it is hoped that the government will use the documents (especially guidelines and protocols) beyond the life of the programme. It is therefore most important that the documentation shows the government logos to reflect this ownership. Donor logos should not be prominent.
5.2 PRRINN-MNCH produces excellent reports on the clusters. Does the state produce equally detailed reports, drawing on its new expertise and good HMIS for the whole state? This would be an excellent advocacy tool for governors among others.
5.3 There is need for close collaboration with Evidence for Action (E4A) – the DFID funded regional programme and the Centre for Research in Reproductive Health National data system on Maternal Death Audit to avoid duplication of efforts.
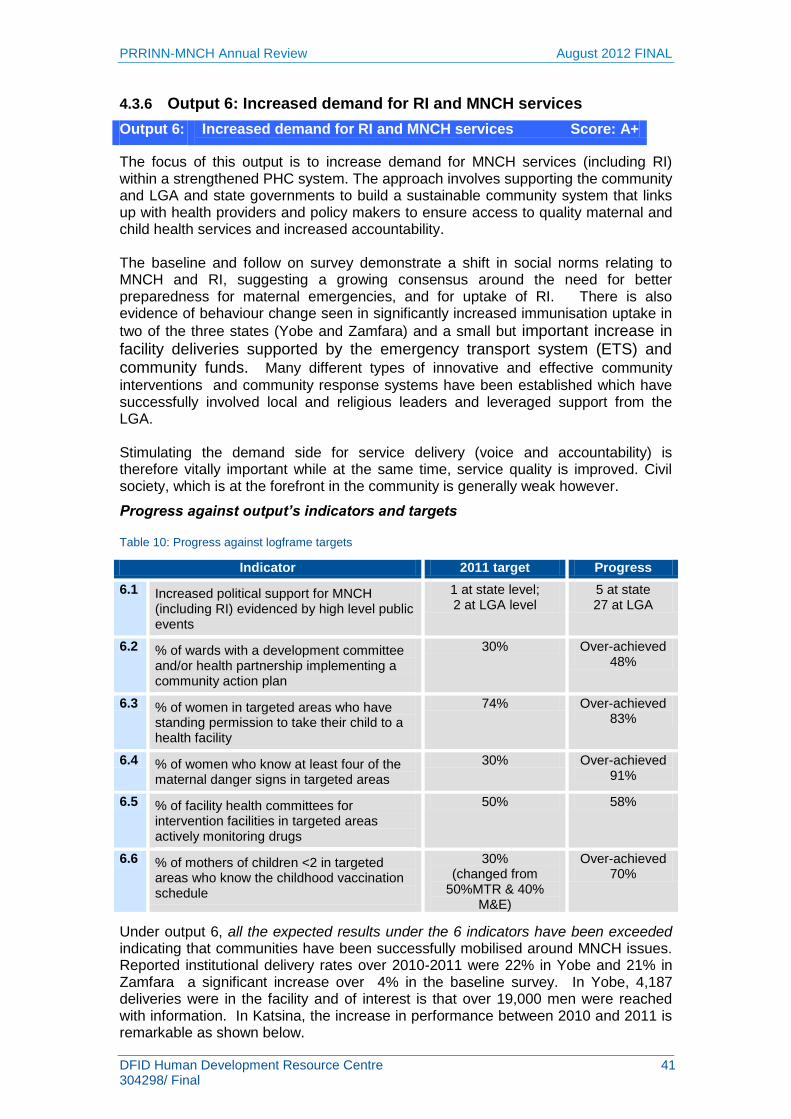
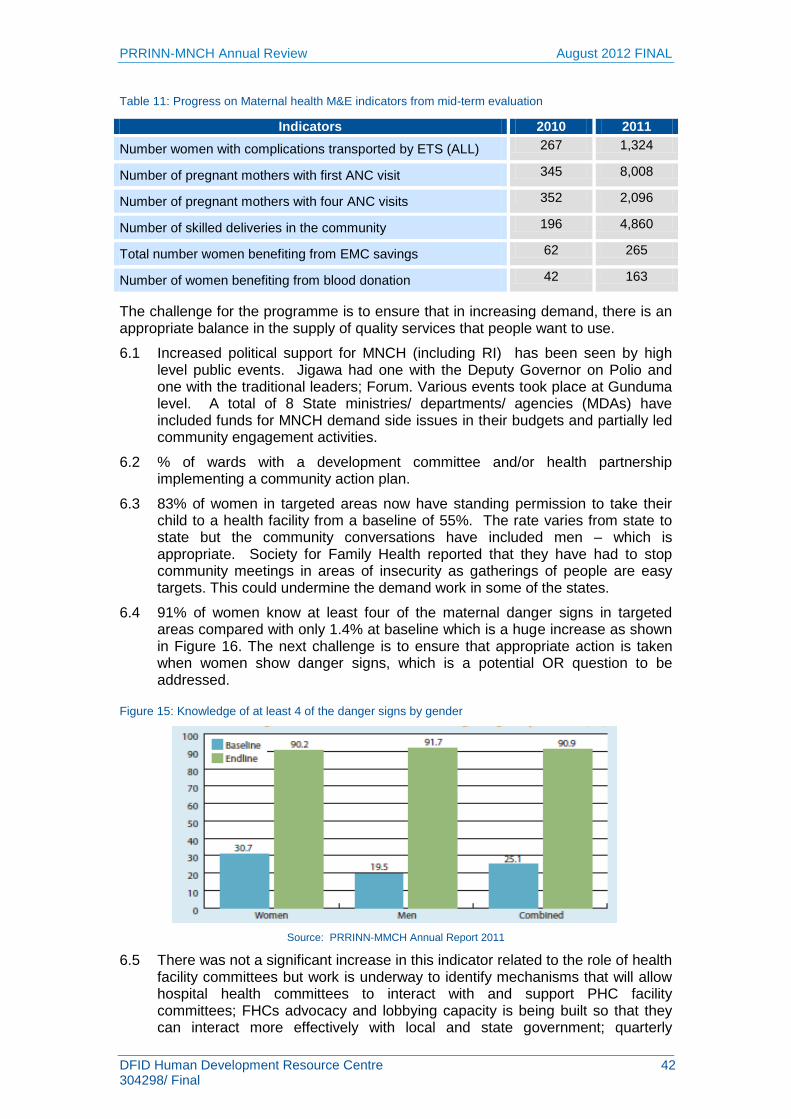
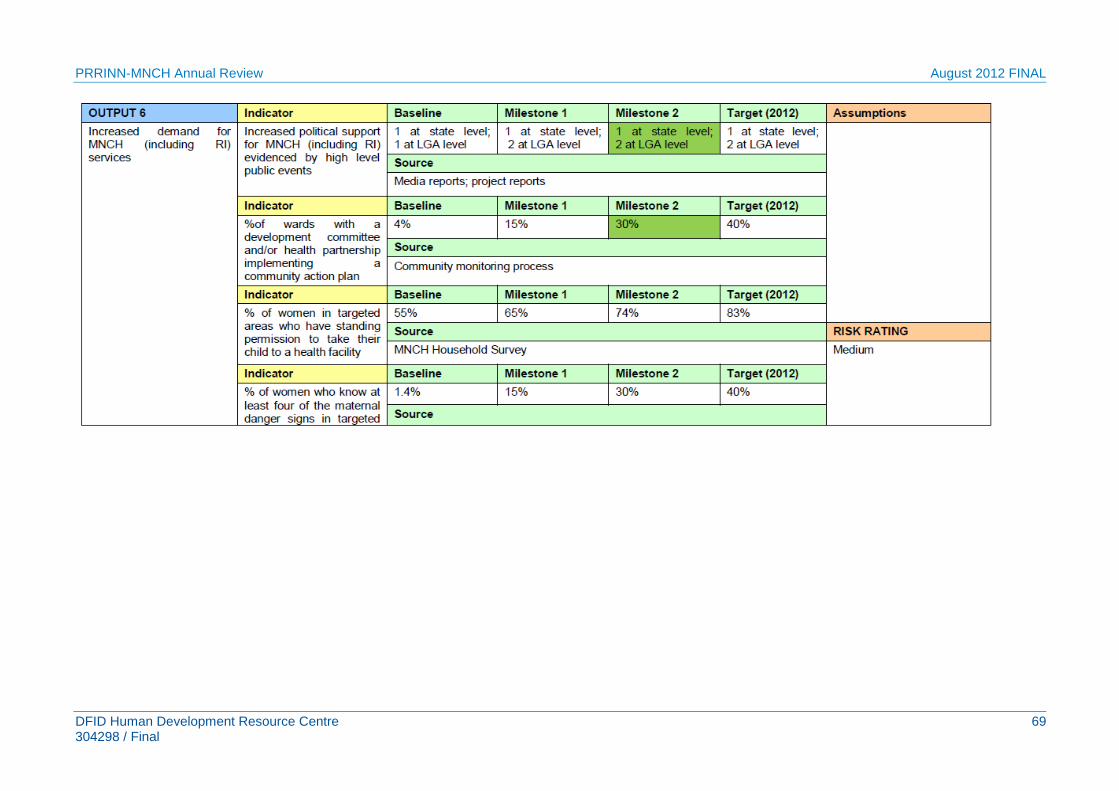
Output 6: Increased demand for RI and MNCH services
The focus of this output is to increase demand for MNCH services (including RI) within a strengthened PHC system. The approach involves supporting the community and LGA and state governments to build a sustainable community system that links up with health providers and policy makers to ensure access to quality maternal and child health services and increased accountability. The baseline and follow on survey demonstrate a shift in social norms relating to MNCH and RI, suggesting a growing consensus around the need for better preparedness for maternal emergencies, and for uptake of RI. There is also evidence of behaviour change seen in significantly increased immunisation uptake in two of the three states (Yobe
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 12 304298/ Final
and Zamfara) and a small but important increase in facility deliveries supported by the emergency transport system (ETS) and community funds.
Recommendations for Output 6
Routine immunisation
6.1 Continue to leverage demand data from HMIS, and evidence from PRRINN experience in field, to work with communities to generate demand for RI and MNCH services.
6.2 Continue work on vaccine supply (see Output 7) and health worker training (see Output 3), as a reliable supply of vaccines and respectful health workers are crucial components to sustain demand for services.
6.3 Sustainability for community engagement work will be crucial. PRRINN should continue to work on establishing/implementing strategies to ensure community engagement work is sustainable and continues to address key barriers to uptake e.g. date of vaccination, religious objections etc.
6.4 Develop recording system to compile database of community members trained in, and currently conducting, RI and MNCH CE activities.
6.5 In Jigawa state, incorporate pentavalent and PCV vaccines into RI CE materials (with a goal of eventually incorporating new vaccines into all programme state materials).
6.6 Continue targeted CE activities to most at risk populations (e.g. younger women, marginalised women).
6.7 Continue to engage with LGA political and technical leadership to ensure funding for community engagement (CE) for RI and MNCH.
MNCH
6.8 An important message for both women and men is that women who do not appear to be in danger can develop danger signs during labour and those with danger signs earlier in pregnancy are often not at risk. For the latter the „second delay‟ can be fatal.
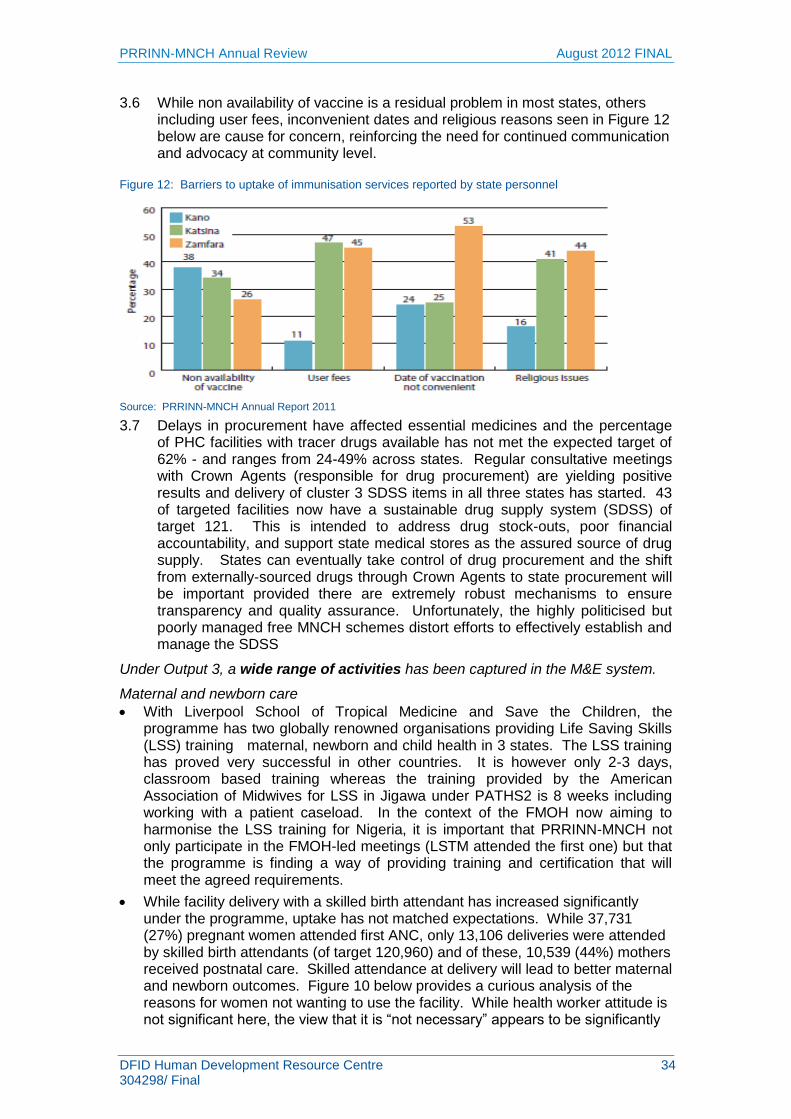
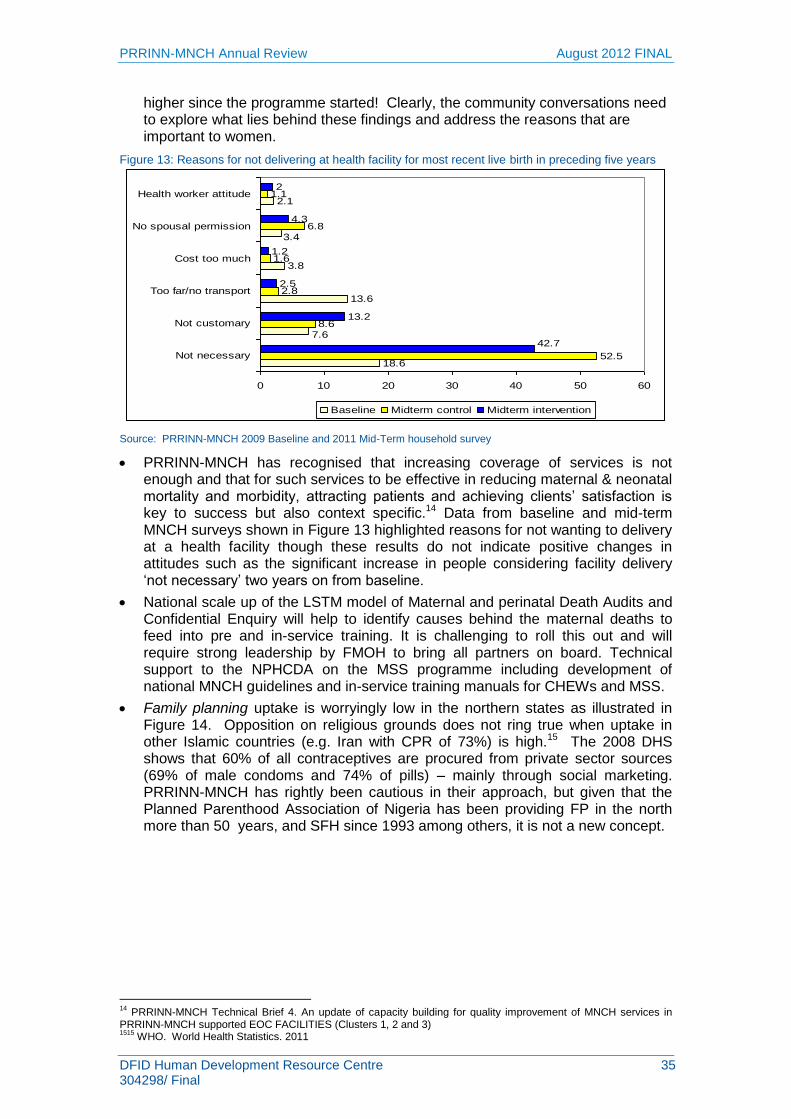
6.9 The Mid-term survey showed that the view that it is “not necessary” to go to a health facility appears to be significantly higher since the programme started. The community conversations need to explore what lies behind these findings and address the reasons that are important to women.
6.10 Various organisations and projects have used an ETS for transferring women in labour and arguably have different experiences which could be compared and shared as a way of finding best solutions to tackle some of the emerging challenges arising such as demand for payment etc. If one organisation has a different kind of arrangement with the union, this could undermine that of PRRINN-MNCH.
6.11 Also discussed under output 3, there still appears to be a degree of caution around FP which has been provided in northern states for more than 50 years (e.g. Planned Parenthood Federation of Nigeria) .4 The programme can draw on the experience of such organisations in strengthening FP. Study tours for Imams helped to reduce stigma and misconceptions around immunisation, so perhaps the same can be tried for family planning.
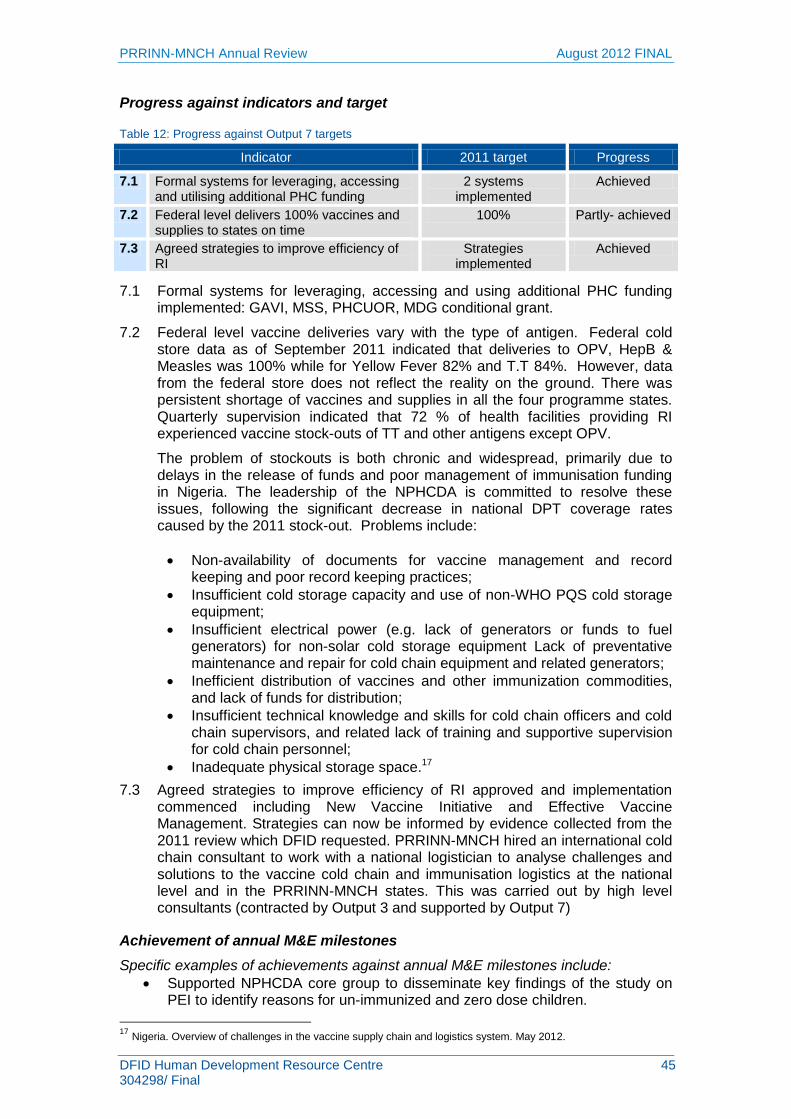
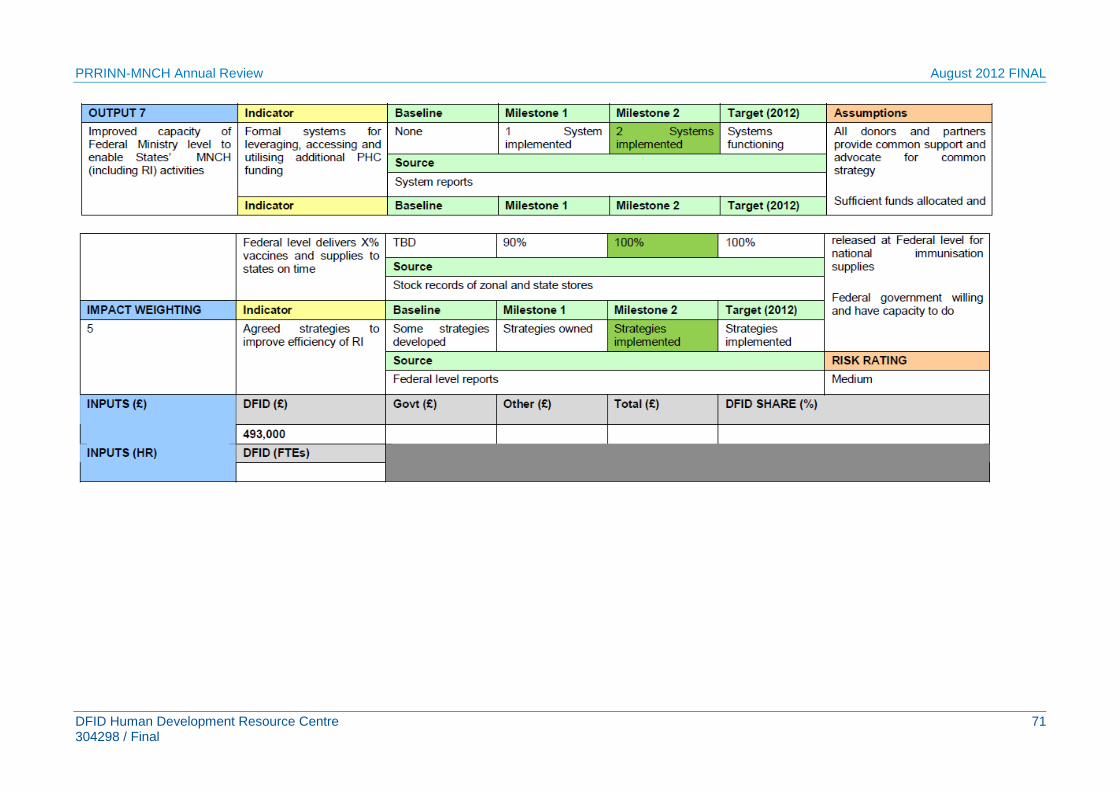
Output 7: Improved capacity of Federal Ministry level to enable States’ routine immunisation activities
The federal-level office in Abuja participates in a number of key groups and committees and works to strengthen relations with government MDAs (e.g. FMOH,
4 Planned Parenthood Federation of Nigeria since the 1950s, and since 1993 by Society for Family Health
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 13 304298/ Final
NPHCDA, MDG, NHIS, MSS) and other development partners/programmes. The federal-level office provides the link between programme implementation at state level, policy makers and leaders at federal level. The NPHCDA is a key partner and has collaborated on the work of „Bringing PHC under one roof‟; the Midwifery Service Scheme (MSS), the system for Integrated Supportive Supervision (ISS), and the Maternal Death Review (MDR), among others. The programme has also built links with the National Health Insurance Scheme, the Federal Ministry of Health and the MDG office. PRRINN has succeeded in getting various interventions/approaches (e.g. Maternal Death Review, PHCUOR) adopted by FMOH for national roll-out.
Recommendations for Output 7
The recommendation to continue working closely with the NPHCDA still holds:
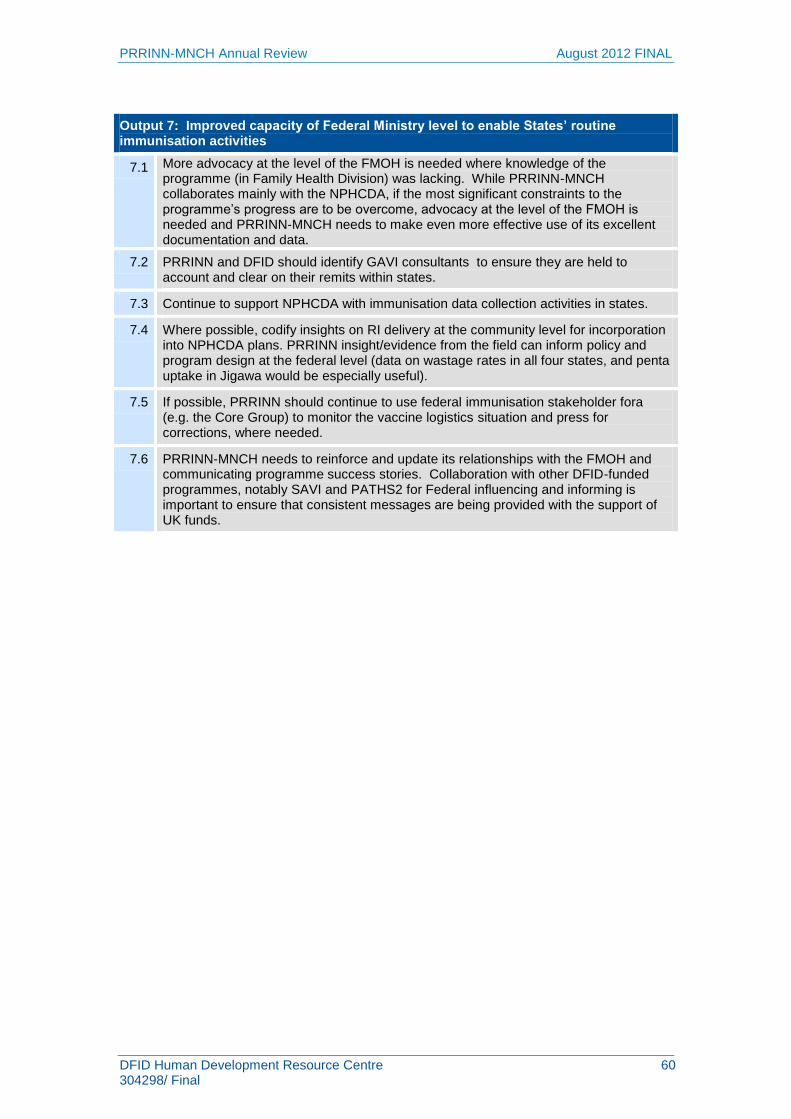
7.1 The 2011 MTR recommended that programme evidence is used for advocacy– and more can be done in this area especially at the level of the FMOH where knowledge of the programme (in Family Health Division) was lacking. While PRRINN-MNCH collaborates mainly with the NPHCDA, if the most significant constraints to the programme‟s progress are to be overcome, advocacy at the level of the FMOH is needed and PRRINN-MNCH needs to make even more effective use of its excellent documentation and data.
7.2 PRRINN and DFID should identify GAVI consultants to ensure they are held to account and clear on their remits within states. Continue to support NPHCDA with immunisation data collection activities in states.
7.3 Where possible, codify insights on RI delivery at the community level for incorporation into NPHCDA plans. PRRINN insight/evidence from the field can inform policy and program design at the federal level (data on wastage rates in all four states, and penta uptake in Jigawa would be especially useful).Cvc
7.4 Issues with logistics and supply chain for immunisation commodities (antigens and injection materials) at the federal level are a major risk for the PRRINN programme. If possible, PRRINN should continue to use federal immunisation stakeholder fora (e.g. the Core Group) to monitor the vaccine logistics situation and press for corrections, where needed.
7.5 PRINN-MNCH needs to reinforce and update its relationships with the FMOH and communicating programme success stories. Collaboration with other DFID-funded programmes, notably SAVI and PATHS2 for Federal influencing and informing is important to ensure that consistent messages are being provided with the support of UK funds.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 14 304298/ Final
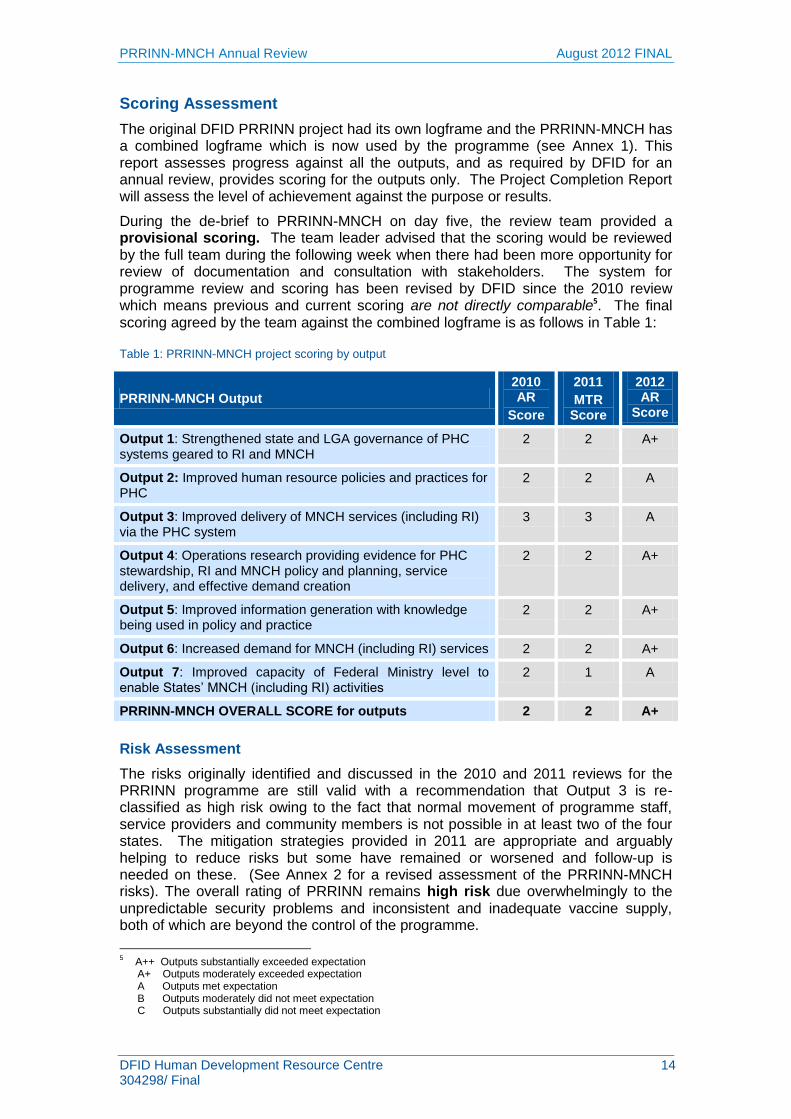
Scoring Assessment
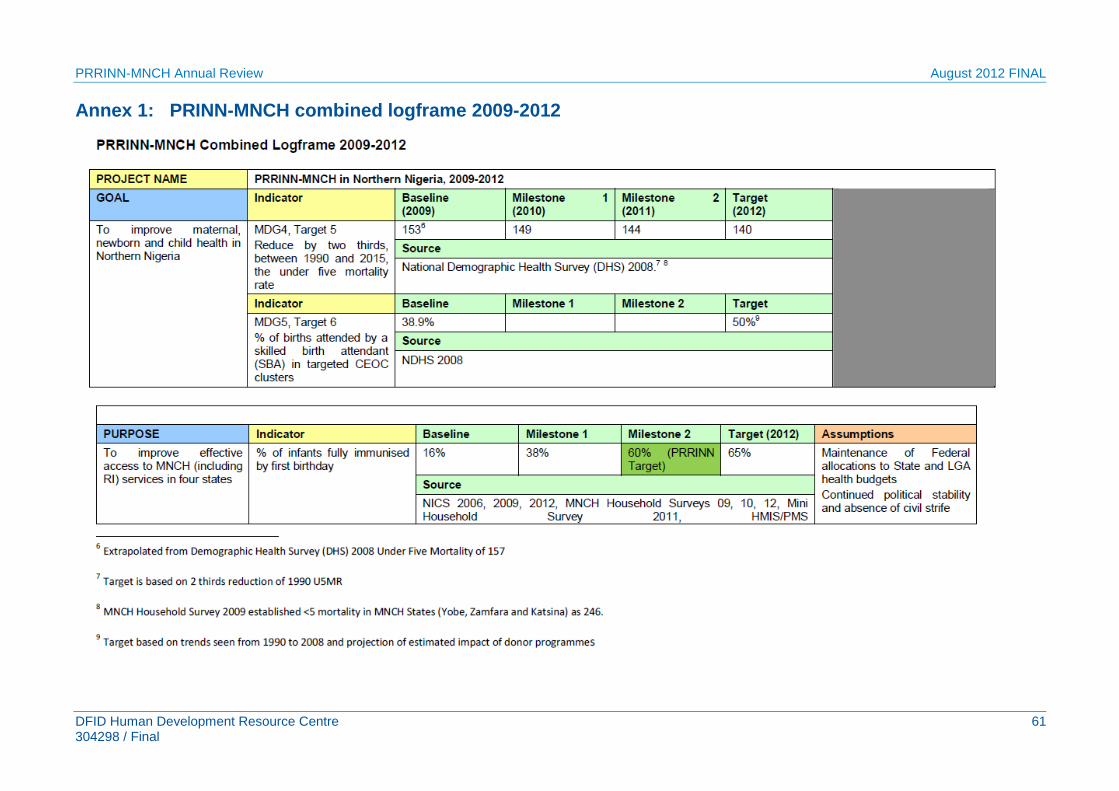
The original DFID PRRINN project had its own logframe and the PRRINN-MNCH has a combined logframe which is now used by the programme (see Annex 1). This report assesses progress against all the outputs, and as required by DFID for an annual review, provides scoring for the outputs only. The Project Completion Report will assess the level of achievement against the purpose or results.
During the de-brief to PRRINN-MNCH on day five, the review team provided a provisional scoring. The team leader advised that the scoring would be reviewed by the full team during the following week when there had been more opportunity for review of documentation and consultation with stakeholders. The system for programme review and scoring has been revised by DFID since the 2010 review which means previous and current scoring are not directly comparable5. The final scoring agreed by the team against the combined logframe is as follows in Table 1:
Table 1: PRRINN-MNCH project scoring by output
PRRINN-MNCH Output
2010 AR
Score
2011
MTR Score
2012 AR
Score
Output 1: Strengthened state and LGA governance of PHC systems geared to RI and MNCH
2 2 A+
Output 2: Improved human resource policies and practices for PHC
2 2 A
Output 3: Improved delivery of MNCH services (including RI) via the PHC system
3 3 A
Output 4: Operations research providing evidence for PHC stewardship, RI and MNCH policy and planning, service delivery, and effective demand creation
2 2 A+
Output 5: Improved information generation with knowledge being used in policy and practice
Output 7: Improved capacity of Federal Ministry level to enable States‟ MNCH (including RI) activities
2 1 A
PRRINN-MNCH OVERALL SCORE for outputs 2 2 A+
Risk Assessment
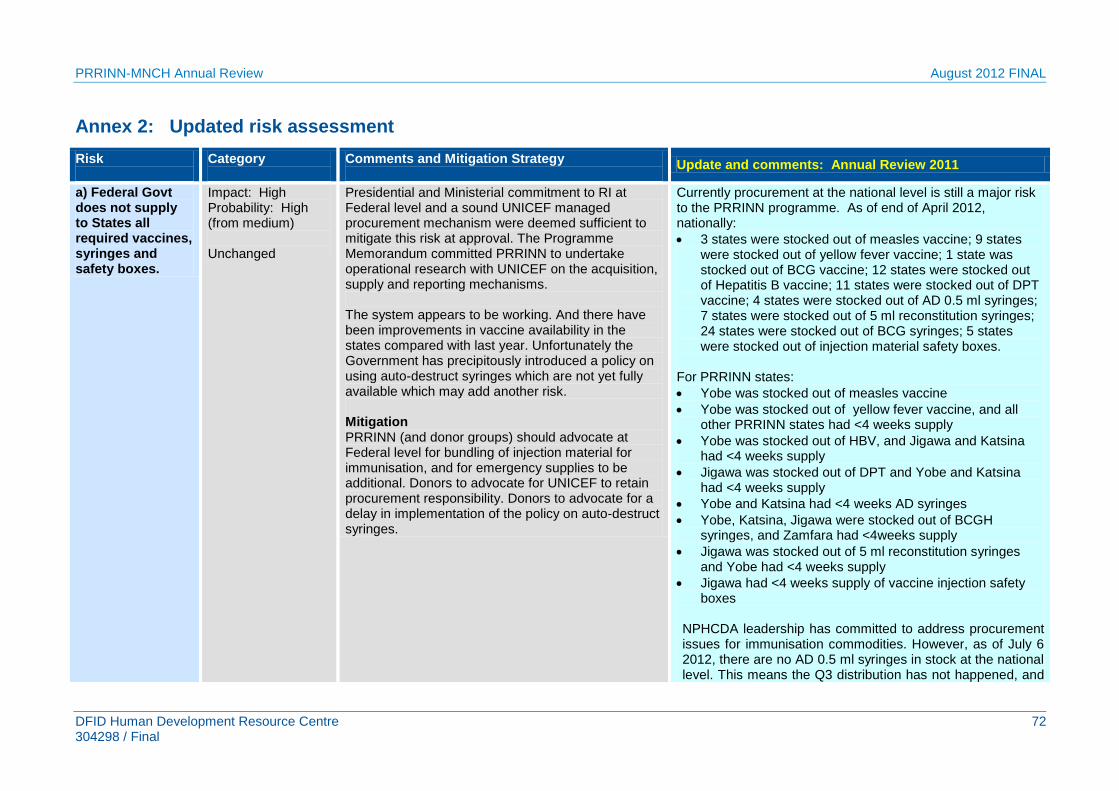
The risks originally identified and discussed in the 2010 and 2011 reviews for the PRRINN programme are still valid with a recommendation that Output 3 is re-classified as high risk owing to the fact that normal movement of programme staff, service providers and community members is not possible in at least two of the four states. The mitigation strategies provided in 2011 are appropriate and arguably helping to reduce risks but some have remained or worsened and follow-up is needed on these. (See Annex 2 for a revised assessment of the PRRINN-MNCH risks). The overall rating of PRRINN remains high risk due overwhelmingly to the unpredictable security problems and inconsistent and inadequate vaccine supply, both of which are beyond the control of the programme.
5 A++ Outputs substantially exceeded expectation
A+ Outputs moderately exceeded expectation A Outputs met expectation B Outputs moderately did not meet expectation C Outputs substantially did not meet expectation
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 15 304298/ Final
1 Context
1.1 Maternal, newborn and child health in northern Nigeria
1.1.1 Maternal health
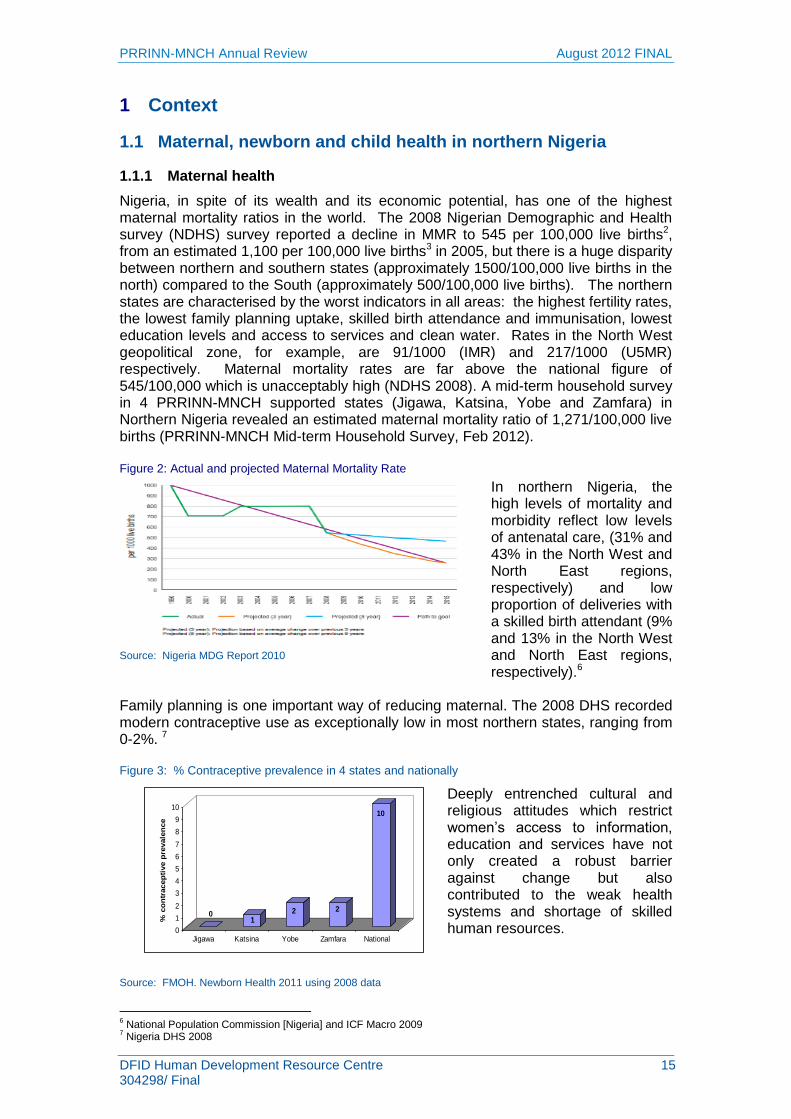
Nigeria, in spite of its wealth and its economic potential, has one of the highest maternal mortality ratios in the world. The 2008 Nigerian Demographic and Health survey (NDHS) survey reported a decline in MMR to 545 per 100,000 live births2, from an estimated 1,100 per 100,000 live births3 in 2005, but there is a huge disparity between northern and southern states (approximately 1500/100,000 live births in the north) compared to the South (approximately 500/100,000 live births). The northern states are characterised by the worst indicators in all areas: the highest fertility rates, the lowest family planning uptake, skilled birth attendance and immunisation, lowest education levels and access to services and clean water. Rates in the North West geopolitical zone, for example, are 91/1000 (IMR) and 217/1000 (U5MR) respectively. Maternal mortality rates are far above the national figure of 545/100,000 which is unacceptably high (NDHS 2008). A mid-term household survey in 4 PRRINN-MNCH supported states (Jigawa, Katsina, Yobe and Zamfara) in Northern Nigeria revealed an estimated maternal mortality ratio of 1,271/100,000 live births (PRRINN-MNCH Mid-term Household Survey, Feb 2012).
In northern Nigeria, the high levels of mortality and morbidity reflect low levels of antenatal care, (31% and 43% in the North West and North East regions, respectively) and low proportion of deliveries with a skilled birth attendant (9% and 13% in the North West and North East regions, respectively).6
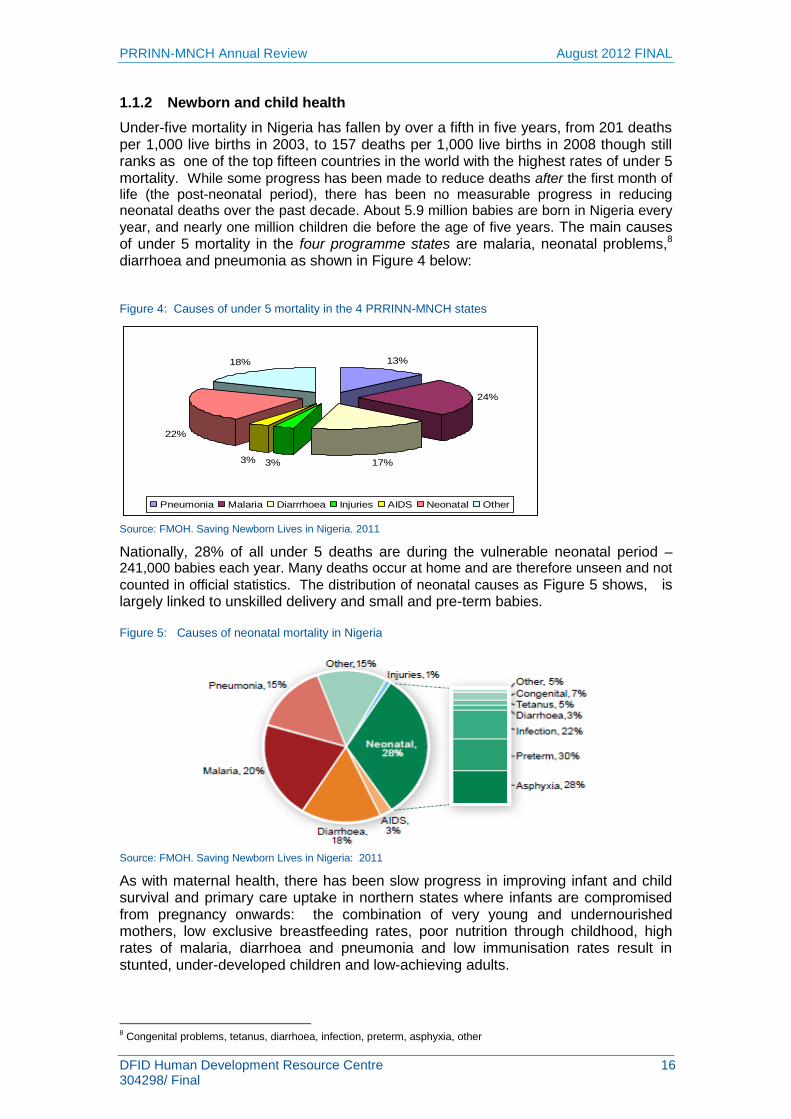
Family planning is one important way of reducing maternal. The 2008 DHS recorded modern contraceptive use as exceptionally low in most northern states, ranging from 0-2%. 7
Figure 3: % Contraceptive prevalence in 4 states and nationally
Deeply entrenched cultural and religious attitudes which restrict women‟s access to information, education and services have not only created a robust barrier against change but also contributed to the weak health systems and shortage of skilled human resources.
6 National Population Commission [Nigeria] and ICF Macro 2009
7 Nigeria DHS 2008
Figure 2: Actual and projected Maternal Mortality Rate
Source: Nigeria MDG Report 2010
Source: FMOH. Newborn Health 2011 using 2008 data
01
2 2
10
0
1
2
3
4
5
6
7
8
9
10
% c
on
tracep
tive p
revale
nce
Jigawa Katsina Yobe Zamfara National
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 16 304298/ Final
1.1.2 Newborn and child health
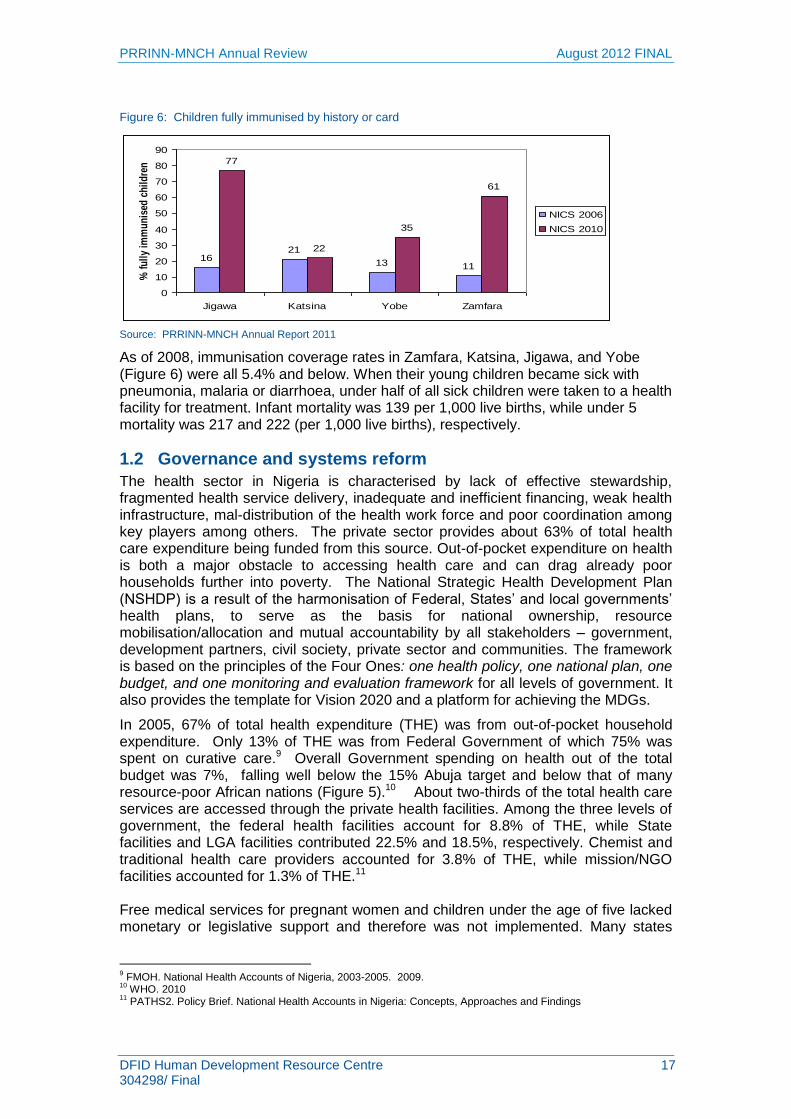
Under-five mortality in Nigeria has fallen by over a fifth in five years, from 201 deaths per 1,000 live births in 2003, to 157 deaths per 1,000 live births in 2008 though still ranks as one of the top fifteen countries in the world with the highest rates of under 5 mortality. While some progress has been made to reduce deaths after the first month of life (the post-neonatal period), there has been no measurable progress in reducing neonatal deaths over the past decade. About 5.9 million babies are born in Nigeria every
year, and nearly one million children die before the age of five years. The main causes of under 5 mortality in the four programme states are malaria, neonatal problems,8 diarrhoea and pneumonia as shown in Figure 4 below:
Figure 4: Causes of under 5 mortality in the 4 PRRINN-MNCH states
Source: FMOH. Saving Newborn Lives in Nigeria. 2011
Nationally, 28% of all under 5 deaths are during the vulnerable neonatal period – 241,000 babies each year. Many deaths occur at home and are therefore unseen and not
counted in official statistics. The distribution of neonatal causes as Figure 5 shows, is largely linked to unskilled delivery and small and pre-term babies.
Figure 5: Causes of neonatal mortality in Nigeria
Source: FMOH. Saving Newborn Lives in Nigeria: 2011
As with maternal health, there has been slow progress in improving infant and child survival and primary care uptake in northern states where infants are compromised from pregnancy onwards: the combination of very young and undernourished mothers, low exclusive breastfeeding rates, poor nutrition through childhood, high rates of malaria, diarrhoea and pneumonia and low immunisation rates result in stunted, under-developed children and low-achieving adults.
8 Congenital problems, tetanus, diarrhoea, infection, preterm, asphyxia, other
13%
24%
17%3%3%
22%
18%
Pneumonia Malaria Diarrrhoea Injuries AIDS Neonatal Other
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 17 304298/ Final
Figure 6: Children fully immunised by history or card
Source: PRRINN-MNCH Annual Report 2011
As of 2008, immunisation coverage rates in Zamfara, Katsina, Jigawa, and Yobe (Figure 6) were all 5.4% and below. When their young children became sick with pneumonia, malaria or diarrhoea, under half of all sick children were taken to a health facility for treatment. Infant mortality was 139 per 1,000 live births, while under 5 mortality was 217 and 222 (per 1,000 live births), respectively.
1.2 Governance and systems reform The health sector in Nigeria is characterised by lack of effective stewardship, fragmented health service delivery, inadequate and inefficient financing, weak health infrastructure, mal-distribution of the health work force and poor coordination among key players among others. The private sector provides about 63% of total health care expenditure being funded from this source. Out-of-pocket expenditure on health is both a major obstacle to accessing health care and can drag already poor households further into poverty. The National Strategic Health Development Plan (NSHDP) is a result of the harmonisation of Federal, States‟ and local governments‟ health plans, to serve as the basis for national ownership, resource mobilisation/allocation and mutual accountability by all stakeholders – government, development partners, civil society, private sector and communities. The framework is based on the principles of the Four Ones: one health policy, one national plan, one budget, and one monitoring and evaluation framework for all levels of government. It also provides the template for Vision 2020 and a platform for achieving the MDGs.
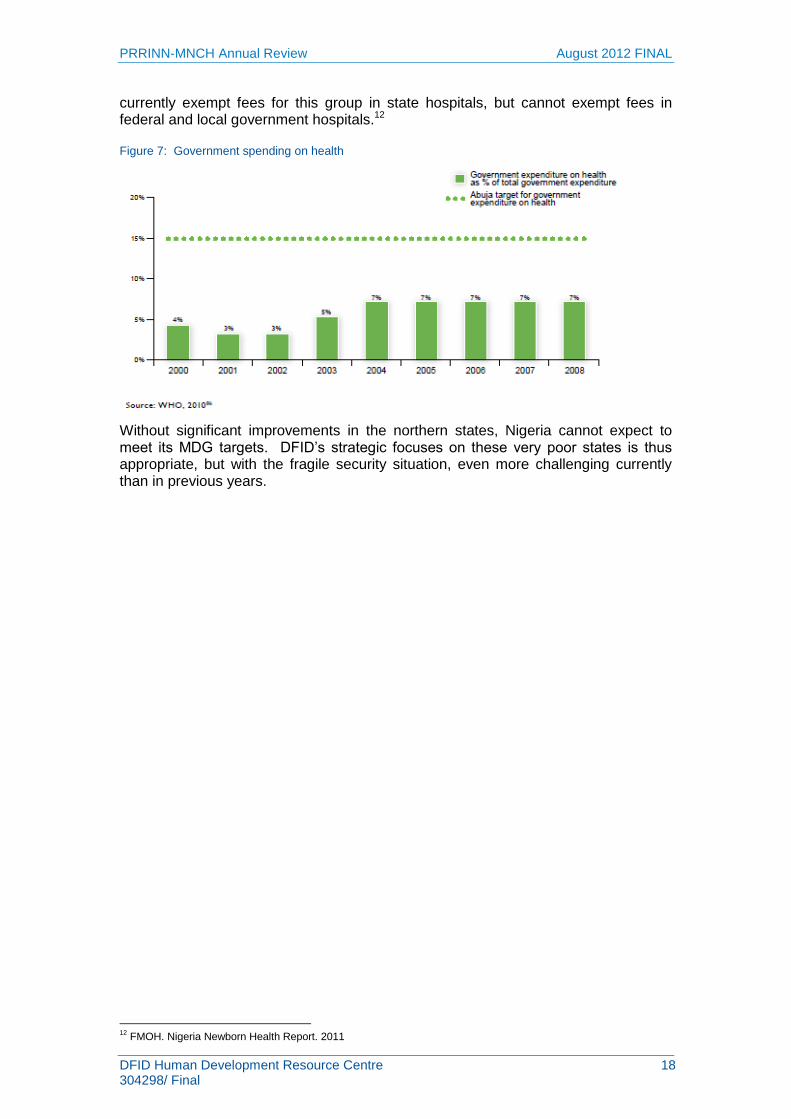
In 2005, 67% of total health expenditure (THE) was from out-of-pocket household expenditure. Only 13% of THE was from Federal Government of which 75% was spent on curative care.9 Overall Government spending on health out of the total budget was 7%, falling well below the 15% Abuja target and below that of many resource-poor African nations (Figure 5).10 About two-thirds of the total health care services are accessed through the private health facilities. Among the three levels of government, the federal health facilities account for 8.8% of THE, while State facilities and LGA facilities contributed 22.5% and 18.5%, respectively. Chemist and traditional health care providers accounted for 3.8% of THE, while mission/NGO facilities accounted for 1.3% of THE.11 Free medical services for pregnant women and children under the age of five lacked monetary or legislative support and therefore was not implemented. Many states
9 FMOH. National Health Accounts of Nigeria, 2003-2005. 2009.
10 WHO. 2010
11 PATHS2. Policy Brief. National Health Accounts in Nigeria: Concepts, Approaches and Findings
1621
13 11
77
22
35
61
0
10
20
30
40
50
60
70
80
90
Jigawa Katsina Yobe Zamfara
% f
ull
y im
mu
nis
ed c
hil
dre
n
NICS 2006
NICS 2010
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 18 304298/ Final
currently exempt fees for this group in state hospitals, but cannot exempt fees in federal and local government hospitals.12
Figure 7: Government spending on health
Without significant improvements in the northern states, Nigeria cannot expect to meet its MDG targets. DFID‟s strategic focuses on these very poor states is thus appropriate, but with the fragile security situation, even more challenging currently than in previous years.
12
FMOH. Nigeria Newborn Health Report. 2011
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 19 304298/ Final
2 Background to PRRINN-MNCH programme
PRINN-MNCH combines two projects from two funding sources which have been merged into one programme. The „Programme to Revitalise Routine Immunisation in Northern Nigeria‟ (PRRINN) project was a DFID-funded programme begun in 2006, as a health system strengthening programme, particularly focused on routine immunisation. In September 2008, the contract to implement the Maternal, Newborn and Child Health (MNCH) programme (funded by the Government of Norway) was awarded to the same consortia managing the PRRINN programme and the two programmes are now fully merged administratively and programmatically. (The one exception to this is that the PRRINN project must still report to DFID using its original five outputs in order to account separately for the DFID funding.) The combined logframe which was used for this review can be found in Annex 1.
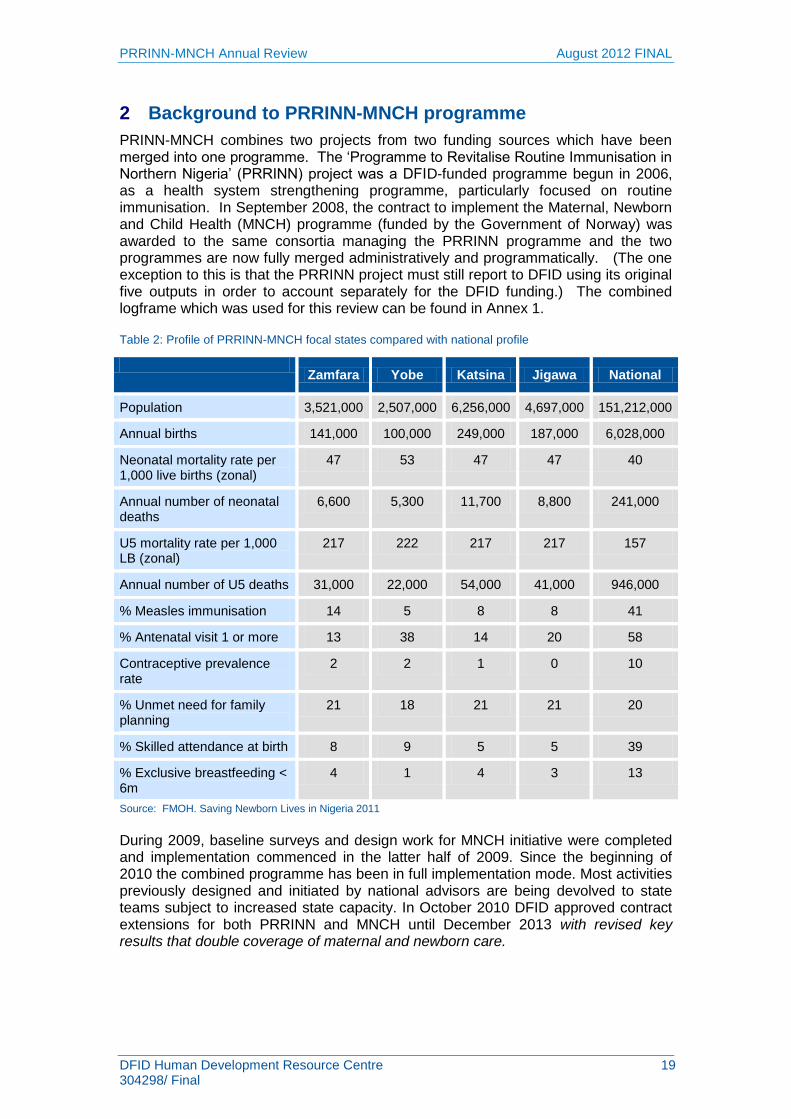
Table 2: Profile of PRRINN-MNCH focal states compared with national profile
Zamfara Yobe Katsina Jigawa National
Population 3,521,000 2,507,000 6,256,000 4,697,000 151,212,000
Neonatal mortality rate per 1,000 live births (zonal)
47 53 47 47 40
Annual number of neonatal deaths
6,600 5,300 11,700 8,800 241,000
U5 mortality rate per 1,000 LB (zonal)
217 222 217 217 157
Annual number of U5 deaths 31,000 22,000 54,000 41,000 946,000
% Measles immunisation 14 5 8 8 41
% Antenatal visit 1 or more 13 38 14 20 58
Contraceptive prevalence rate
2 2 1 0 10
% Unmet need for family planning
21 18 21 21 20
% Skilled attendance at birth 8 9 5 5 39
% Exclusive breastfeeding < 6m
4 1 4 3 13
Source: FMOH. Saving Newborn Lives in Nigeria 2011
During 2009, baseline surveys and design work for MNCH initiative were completed and implementation commenced in the latter half of 2009. Since the beginning of 2010 the combined programme has been in full implementation mode. Most activities previously designed and initiated by national advisors are being devolved to state teams subject to increased state capacity. In October 2010 DFID approved contract extensions for both PRRINN and MNCH until December 2013 with revised key results that double coverage of maternal and newborn care.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 20 304298/ Final
3 Methodology
The four day review, intended to be „light touch‟, was scheduled to have the first day with presentations from Yobe and Jigawa, followed by three days visiting the field in Zamfara and Katsina, and a de-brief by the team to PRRINN-MNCH on the fifth day. Owing to the very uncertain security situation, it was agreed to cancel the field visits so the appraisal cannot draw from personal observation as intended.
The review was thus re-scheduled so that the team met with key stakeholders in Abuja and the Zamfara and Katsina teams travelled to Abuja to give presentations. The review thus relied on information generated by the PRINN-MNCH programme including the presentations themselves and the very substantial number and range of programme documents as well as those sourced from other related programmes (e.g. the USAID-funded MCHIP and PATHS2). In addition, team members were able to meet with key stakeholders in Abuja and the team leader spent a further four days in Abuja meeting related stakeholders and preparing the reports.
3.1 The evaluation team
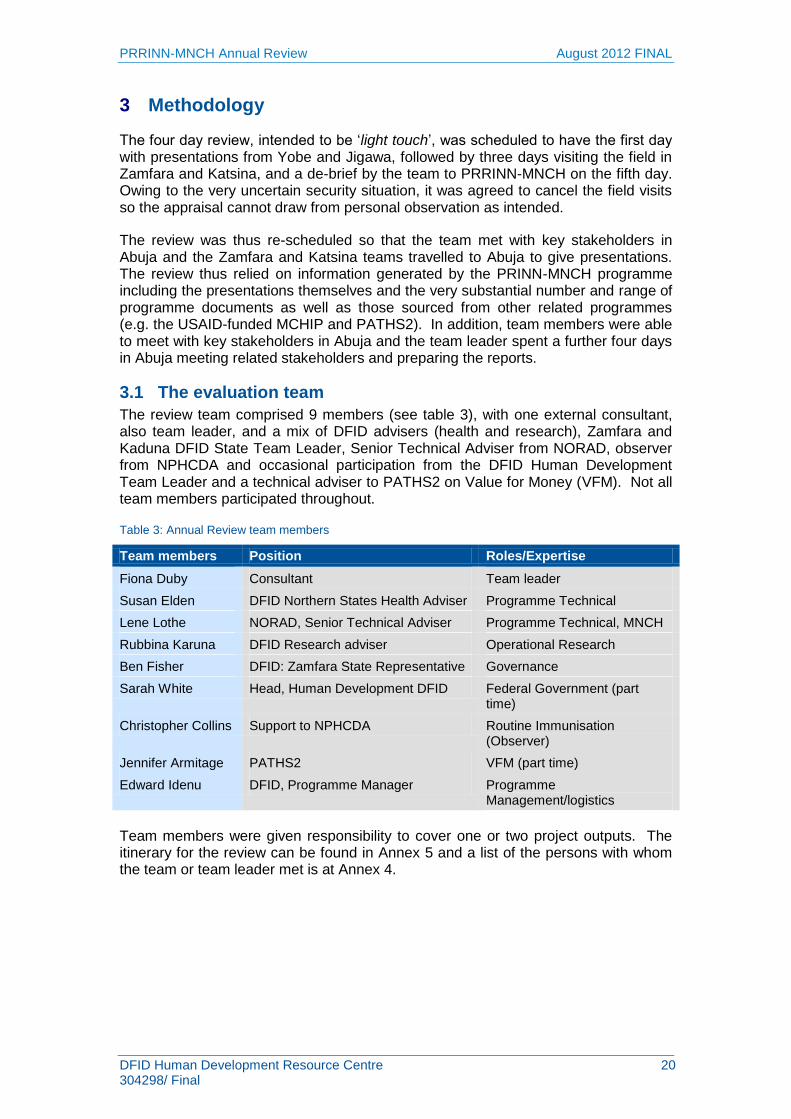
The review team comprised 9 members (see table 3), with one external consultant, also team leader, and a mix of DFID advisers (health and research), Zamfara and Kaduna DFID State Team Leader, Senior Technical Adviser from NORAD, observer from NPHCDA and occasional participation from the DFID Human Development Team Leader and a technical adviser to PATHS2 on Value for Money (VFM). Not all team members participated throughout.
Table 3: Annual Review team members
Team members Position Roles/Expertise
Fiona Duby Consultant Team leader
Susan Elden DFID Northern States Health Adviser Programme Technical
Rubbina Karuna DFID Research adviser Operational Research
Ben Fisher DFID: Zamfara State Representative Governance
Sarah White Head, Human Development DFID Federal Government (part time)
Christopher Collins Support to NPHCDA Routine Immunisation (Observer)
Jennifer Armitage PATHS2 VFM (part time)
Edward Idenu DFID, Programme Manager Programme Management/logistics
Team members were given responsibility to cover one or two project outputs. The itinerary for the review can be found in Annex 5 and a list of the persons with whom the team or team leader met is at Annex 4.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 21 304298/ Final
4 Programme assessment
4.1 General progress
“One of the biggest assets to the PRRINN programme is the technical expertise, the
dedication, the local knowledge and experience of its staff. This team knows what needs to be done and “how” it should be done. An example is their knowledge of traditional rules, the political environment. They have established trust within LGA and state officials in order to see where their budget is going and the areas of allocation. State directors in health, planning and budget areas can state how they are better informed and able to make decisions and influence within the Ministry. PRRINN uses a responsible and sensitive approach on areas such as female health workers, family planning and women getting standing permission to attend facilities”. (DFID Adviser)
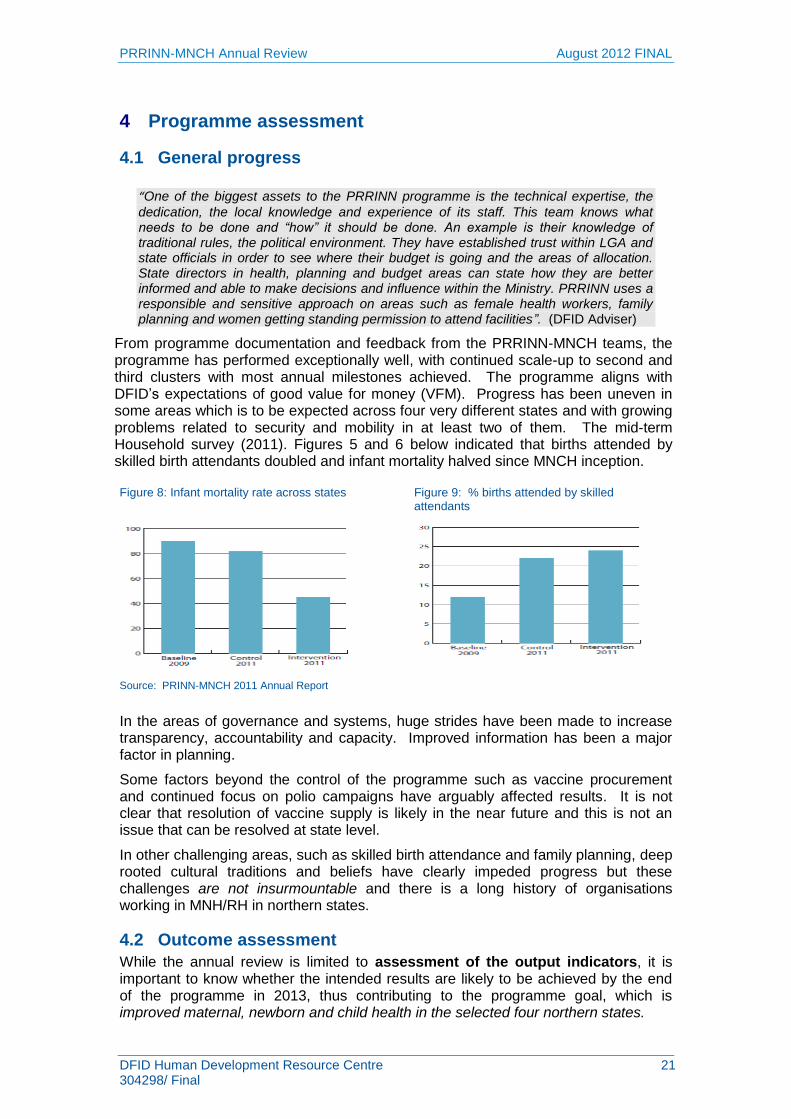
From programme documentation and feedback from the PRRINN-MNCH teams, the programme has performed exceptionally well, with continued scale-up to second and third clusters with most annual milestones achieved. The programme aligns with DFID‟s expectations of good value for money (VFM). Progress has been uneven in some areas which is to be expected across four very different states and with growing problems related to security and mobility in at least two of them. The mid-term Household survey (2011). Figures 5 and 6 below indicated that births attended by skilled birth attendants doubled and infant mortality halved since MNCH inception.
Figure 8: Infant mortality rate across states Figure 9: % births attended by skilled attendants
Source: PRINN-MNCH 2011 Annual Report
In the areas of governance and systems, huge strides have been made to increase transparency, accountability and capacity. Improved information has been a major factor in planning.
Some factors beyond the control of the programme such as vaccine procurement and continued focus on polio campaigns have arguably affected results. It is not clear that resolution of vaccine supply is likely in the near future and this is not an issue that can be resolved at state level.
In other challenging areas, such as skilled birth attendance and family planning, deep rooted cultural traditions and beliefs have clearly impeded progress but these challenges are not insurmountable and there is a long history of organisations working in MNH/RH in northern states.
4.2 Outcome assessment
While the annual review is limited to assessment of the output indicators, it is important to know whether the intended results are likely to be achieved by the end of the programme in 2013, thus contributing to the programme goal, which is improved maternal, newborn and child health in the selected four northern states.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 22 304298/ Final
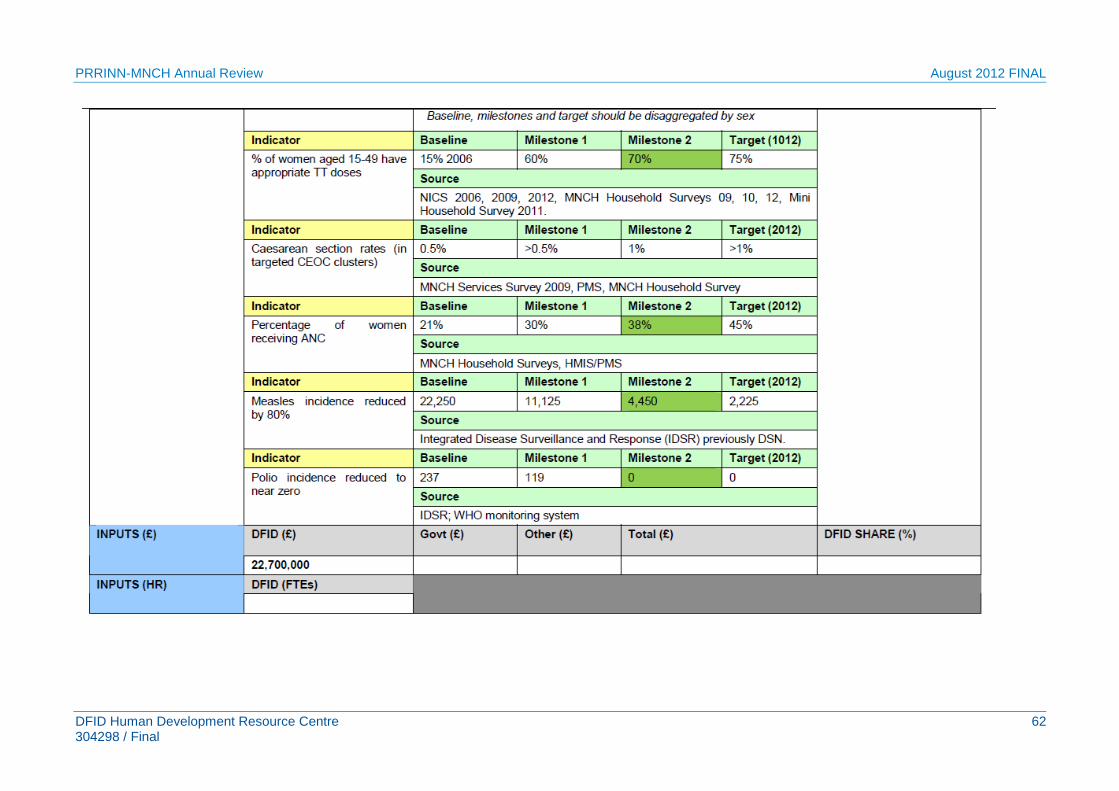
Using data from within the programme and from federal surveys, the following results in comparison with the baseline data illustrate the effectiveness of the programme. The programme can already measure positive results against outcome indicators as shown in Table 4 below. Of 7 outcome indicators, 5 have already been surpassed, one (CPR) is likely to be achieved and polio might decline to near zero cases, if exogenous factors do not impede progress. Table 4: Progress against expected results
Outcome/result indicator Target Status
1 32% increase in infants fully immunised by their first birthday
314% increase children fully immunised
Over-achieved
2 50% of pregnant women with appropriate tetanus toxoid doses
431% increase in pregnant women appropriately immunised
Over-achieved
3 4.18% of women ages 15-49 with access to modern family planning services
# PHC facilities providing contraceptives is 139 over 2011 target of 50. # users (23,231) in 2011 falls short of target (45,126)
Likely to be achieved
4 1.25% of facility births in targeted clusters delivered by caesarean section
271% increase or an additional 13,998 women being delivered by skilled birth attendants
Over-achieved
5 50% of women making 4 antenatal visits
270% increase women attending antenatal care first visits
Over-achieved
6 80% reduction in measles incidence
Measles cases are declining significantly from baseline of 22,250
Over-achieved.
Total incidence 3,734 in 2011. (Jigawa target 6,020 and incidence 2,113 in 2011; Yobe 142 (target 1,112); Katsina 169 against 2011 target of 1,113)
7 Incidence of polio reduced to near zero
At 62 polio cases in 2011
increased from 9 cases in 2010
14 cases in 4 programme states Jan-June 2012. Could be achieved but not in control of the programme.
4.2.1 Likely contribution to state and national performance and influence on policy and practice
PRRINN has contributed positively to immunisation performance in the four focal states, though some more than others. However, the state performance relies on a functional national system and systemic problems in vaccine supply, including transparency and accountability, are undermining performance at state level. If PRRINN is to influence this situation, it needs to engage more strongly at the national level. However, with a goal in mind to improve maternal, newborn and child health and thus reduce maternal, newborn and child mortality and morbidity, there is every likelihood that with improvements in skilled delivery and increased uptake of family planning,
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 23 304298/ Final
the programme will have a positive impact on maternal, newborn and child health and achievement of MDGs 4 and 5.
4.2.2 Headlines for each state
Jigawa
State Comprehensive Development Framework (CDF) has been used to develop the Medium Term Sector Strategy (MTSS) for 2011-2013, and the 2012 Operational Plan is linked to the Health Sector Development Plan (HSDP) and MTSS 2012.
The state allocated 12% of the state budget to health, representing a 30% increase in actual funding and getting closer to the Abuja declaration of 15%.
Jigawa is one of the states that qualified for the first phase pentavalent introduction.
The Emir of Dutse permitted female health workers to ride motorbikes to improve access for home visiting.
Government has approved and implemented the federally legislated enhanced salary for health care workers
Katsina
High-level political support to the programme and the health sector was obtained as a result of sustained advocacy and networking with political and traditional leaders.
Concept of PHCUOR has received high-level political commitment but not yet received budget allocation. and memo has been drafted for approval by the Governor.
Embargo on health workers‟ employment lifted. 40 MSS Midwives employed by the HMB. The MSS Midwife allowance budget was included in 2012 plan and payment backdated from January 2012.
Advocacy on accreditation of health training institutes led to recruitment of 18 tutors and approval of 100 million naira based on the costed accreditation plan
SDSS policy was approved and the system set up in three clusters.
Yobe
State PHC Board is operational and has developed its costed plan for 2012.
Government is undertaking a staff verification exercise to reduce fraud within the system by identifying ghost workers.
The Donor partner coordination forum has been re-established
Zamfara
Nursing and Midwifery Council approved the community midwifery training programme in Zamfara State, as the state has met the key conditions of the council.
Results of the 2011 health Sector Performance review 2011 were presented to Commissioners of Health, Local Government, Finance and Budget. This Exercise in transparency means that fewer government officials undertook medical treatment overseas.
Basket Fund remains reliable and transparent source for monitoring and supervision of routine immunisation, PEI and PHC services.
State Government signs MOU with UDU Sokoto on HDSS.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 24 304298/ Final
4.3 Output assessments
4.3.1 Output 1: Strengthened State and LGA governance
Output 1: Strengthened State and LGA governance of PHC systems
geared to RI and MNCH Score: A+
The PRRINN programme approach has focused on improving the PHC delivery system as a way to increase immunisation coverage. This systems approach has been carried over into the combined PRRINN-MNCH programme. This first output focuses on the policy and strategy framework within which the health system functions and deals with policy and planning: partner co-ordination; advocacy and institutional change; and Public Finance Management (PFM).
Highlights under this output include bringing Primary Health Care under one roof (PHCUOR) – a major improvement from the previously fragmented institutional arrangements; developing the Minimum Service Package; building blocks for a service investment plan; strengthening public financial management systems; creating an Eminent Persons Group; and leveraging increased resources. Growing collaboration at state level with SAVI and SPARC has provided opportunities for increased and sustained support in the area of governance.
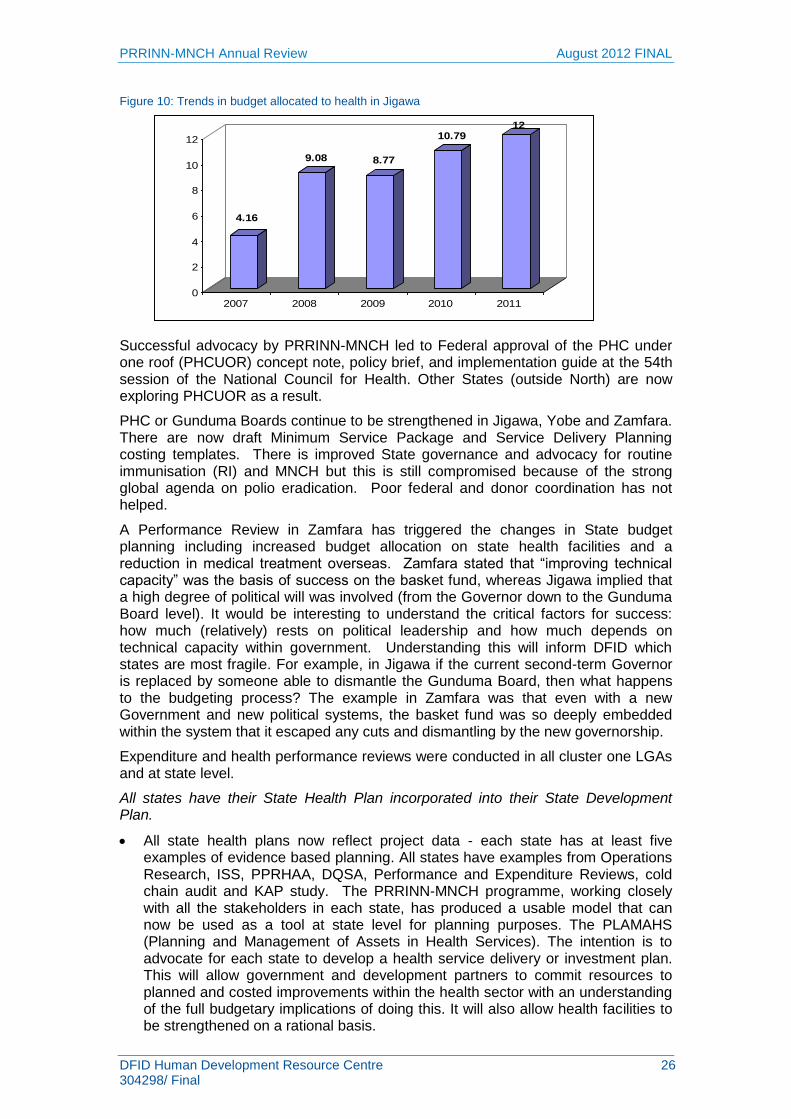
As with other outputs, states have progressed at different rates and in different ways, but each state has success stories. Jigawa is often (rightly) cited as a strong performer – one example being its 12% allocation to the health budget (Figure 7) – a success also reflected in PATHS2 reports owing to their concurrent engagement in strengthening institutional functions at state and Gunduma levels. Attribution in this case must be accorded to both programmes but it also remains to be seen how much of this budget is
disbursed and spent – which can be addressed in subsequent evaluations. It is too early to say whether governance reform will pay off in terms of “real results” of improved PFM, improved budget allocation and release. The first step is to educate state partners and improve their technical capacity and accountability. For example, Yobe is starting to implement reform but because improvements are seen in health, it does not mean that there is an appetite for wider reform.
Primary Healthcare Under One Roof
One single management body
Enabling legislation and regulations
Decentralised authority, responsibility and accountability
One management, one plan, and one M&E system
Integrated supportive supervisory system
Integration of all PHC services under one authority
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 25 304298/ Final
Progress against Output 1 indicators and targets
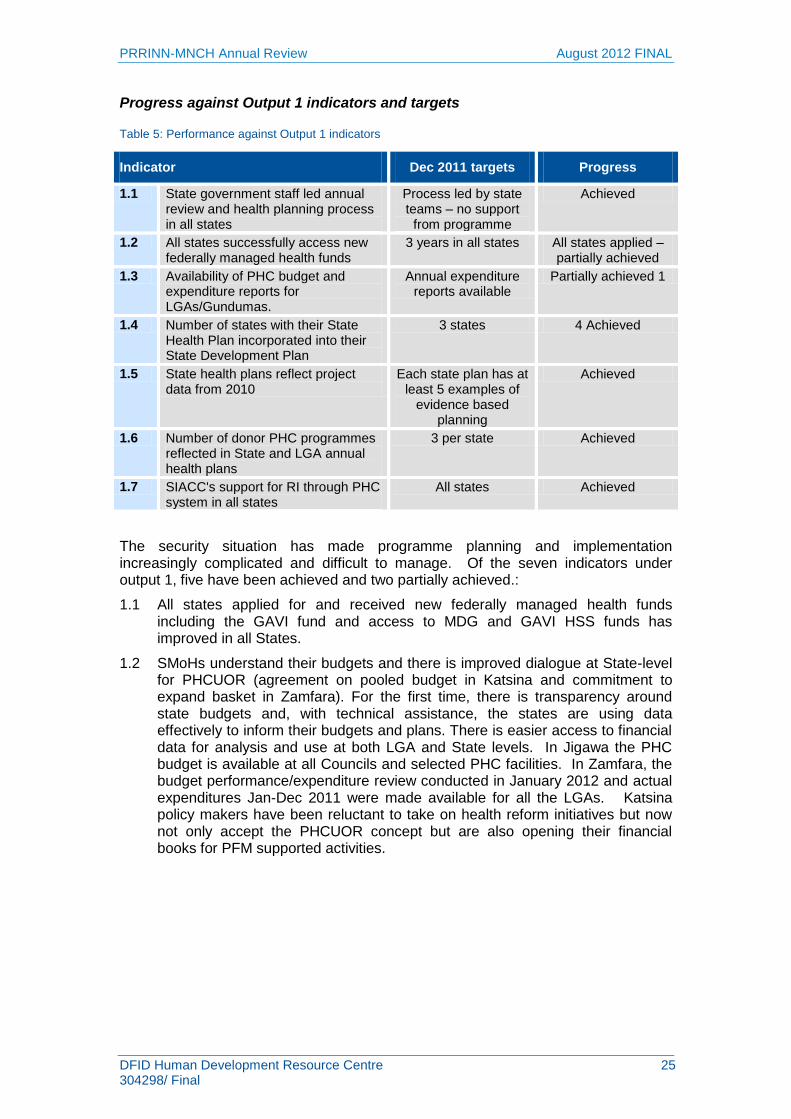
Table 5: Performance against Output 1 indicators
Indicator Dec 2011 targets Progress
1.1 State government staff led annual review and health planning process in all states
Process led by state teams – no support
from programme
Achieved
1.2 All states successfully access new federally managed health funds
3 years in all states All states applied – partially achieved
1.3 Availability of PHC budget and expenditure reports for LGAs/Gundumas.
Annual expenditure reports available
Partially achieved 1
1.4 Number of states with their State Health Plan incorporated into their State Development Plan
3 states 4 Achieved
1.5 State health plans reflect project data from 2010
Each state plan has at least 5 examples of
evidence based planning
Achieved
1.6 Number of donor PHC programmes reflected in State and LGA annual health plans
3 per state Achieved
1.7 SIACC's support for RI through PHC system in all states
All states Achieved
The security situation has made programme planning and implementation increasingly complicated and difficult to manage. Of the seven indicators under output 1, five have been achieved and two partially achieved.:
1.1 All states applied for and received new federally managed health funds including the GAVI fund and access to MDG and GAVI HSS funds has improved in all States.
1.2 SMoHs understand their budgets and there is improved dialogue at State-level for PHCUOR (agreement on pooled budget in Katsina and commitment to expand basket in Zamfara). For the first time, there is transparency around state budgets and, with technical assistance, the states are using data effectively to inform their budgets and plans. There is easier access to financial data for analysis and use at both LGA and State levels. In Jigawa the PHC budget is available at all Councils and selected PHC facilities. In Zamfara, the budget performance/expenditure review conducted in January 2012 and actual expenditures Jan-Dec 2011 were made available for all the LGAs. Katsina policy makers have been reluctant to take on health reform initiatives but now not only accept the PHCUOR concept but are also opening their financial books for PFM supported activities.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 26 304298/ Final
Figure 10: Trends in budget allocated to health in Jigawa
Successful advocacy by PRRINN-MNCH led to Federal approval of the PHC under one roof (PHCUOR) concept note, policy brief, and implementation guide at the 54th session of the National Council for Health. Other States (outside North) are now exploring PHCUOR as a result.
PHC or Gunduma Boards continue to be strengthened in Jigawa, Yobe and Zamfara. There are now draft Minimum Service Package and Service Delivery Planning costing templates. There is improved State governance and advocacy for routine immunisation (RI) and MNCH but this is still compromised because of the strong global agenda on polio eradication. Poor federal and donor coordination has not helped.
A Performance Review in Zamfara has triggered the changes in State budget planning including increased budget allocation on state health facilities and a reduction in medical treatment overseas. Zamfara stated that “improving technical capacity” was the basis of success on the basket fund, whereas Jigawa implied that a high degree of political will was involved (from the Governor down to the Gunduma Board level). It would be interesting to understand the critical factors for success: how much (relatively) rests on political leadership and how much depends on technical capacity within government. Understanding this will inform DFID which states are most fragile. For example, in Jigawa if the current second-term Governor is replaced by someone able to dismantle the Gunduma Board, then what happens to the budgeting process? The example in Zamfara was that even with a new Government and new political systems, the basket fund was so deeply embedded within the system that it escaped any cuts and dismantling by the new governorship.
Expenditure and health performance reviews were conducted in all cluster one LGAs and at state level.
All states have their State Health Plan incorporated into their State Development Plan.
All state health plans now reflect project data - each state has at least five examples of evidence based planning. All states have examples from Operations Research, ISS, PPRHAA, DQSA, Performance and Expenditure Reviews, cold chain audit and KAP study. The PRRINN-MNCH programme, working closely with all the stakeholders in each state, has produced a usable model that can now be used as a tool at state level for planning purposes. The PLAMAHS (Planning and Management of Assets in Health Services). The intention is to advocate for each state to develop a health service delivery or investment plan. This will allow government and development partners to commit resources to planned and costed improvements within the health sector with an understanding of the full budgetary implications of doing this. It will also allow health facilities to be strengthened on a rational basis.
4.16
9.08 8.77
10.7912
0
2
4
6
8
10
12
2007 2008 2009 2010 2011
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 27 304298/ Final
All states have at least 3 PHC programmes reflected in State and LGA annual health plans
All states have at least 3 donor PHC programmes reflected in State and LGA
annual health plans (Milestone – 3 per state). Other donor programmes include
UNICEF, WHO, SUNMaP, PATHS2, SCUK, TSHIP, MAPS.
The State inter-agency coordinating committees (SIACCs) now established in all states have helped in coordination of programmes and are generally considered effective but not yet sufficiently effective to influence the Federal ICC or to ensure that programmes are sufficiently harmonised. Some state officials complained of overlapping programmes which is supported in the literature.
In Jigawa, the quarterly meeting focused on the PEI emergency plan and addressing key RI challenges and in Zamfara State Task Force on PHC and immunisation has been championing the release of funds to the "Basket Fund" which is used in funding RI amongst other activities. (The WHO health mapping tool will help states to avoid geographical duplication of programmes such as was seen in Zamfara and Katsina with PRINN-MNCH and MCHIP).
There has been more coordination between other DFID-funded programmes. Successful collaboration with SPARC and SAVI led to a Political Economy analysis for Zamfara. Katsina and Yobe States are exploring common areas for collaboration to impact positively on health. There is some overlap of roles between PRINN-MNCH and PATHS2 in Jigawa which was pointed out by the government state representatives. PRRINN and PATHS2 outputs are similar, with their focus on strengthening governance, health systems, services and capacity and improving voice and accountability, In Jigawa, where it is PATHS2 taking responsibility for MNCH training and services, a very different model (supported by the American Midwives‟ Association) is being used. This provides an interesting opportunity to compare effectiveness of different approaches. While each programme needs to demonstrate results and attribution, anecdotal evidence suggestions that relationships between the two programmes could be much stronger and more collaborative, drawing on each other‟s relative strengths. But it is also DFID‟s role to ensure value for money – so any unnecessary duplication should be avoided from the outset.
Other findings
Governance Each state is at a different stage in strengthening governance. There is strong variation across states and even within states (at LGA level). Two areas which may be worth exploring in the future are to understand and gather evidence on the following:
Understanding the health impact of PHCUOR is important. A well-conducted evaluation may help to understand the factors (causal and non-causal) and the associations from good governance. For example, despite having the same baseline demographics of other states, Jigawa has some of the highest rates of routine immunisation, high rates of health worker retention, low incidence of polio, harmonised health/Watson. Where this has a measurable health impact (immunisation rates, infant mortality etc.) it is important to understand how much is related to financing, governance, and how much is simply chance and whether this model can be replicated in other states.
Public Financial Management:
Progress has been made with the provision of key guidelines and templates for expenditure tracking, budget development guidelines and expenditure review manuals. Jigawa and Zamfara have developed medium term expenditure
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 28 304298/ Final
frameworks; access to financial data from both the States Health Sector and LGA / PHC levels have significantly improved. The health sector budget proportion to the state budget size has also shown an upward trend for almost all the programme states.
Strong partnerships have been established with religious leaders and institutions in the promotion of MNCH services across states
Concept and implementation guide approved by National Council for Health – disseminated at national level
Pooled funds for PHC incorporated into SPHCMB legislation in 3 states
Basket funds in Zamfara extended beyond RI to PHC services and demand side work ; advocacy continues for free MNCH services from the basket fund
States have continued to strengthen the capacity of Planning and Budget team members on PFM for budget tracking, reporting and evidence based budgeting.
SPARC sees Yobe as having good potential. Their budget performance is good (realistic allocation, release). YoSERA (with EUSHRIP). Government is committed to state development plans. Yobe is starting to implement reform. Just because improvements are seen in health, does not mean that there is an appetite for wider reform.
Basket Fund in Zamfara – a model
“It is an innovative pooled funding mechanism that provides guaranteed funds to finance crucial recurrent PHC activities, through a transparent disbursement and efficient utilization mechanism.”16 The fund began in September 2009 and was created to address three interlinked issues at LGA level: • Poor service delivery e.g. coverage of routine immunisation services was very low in
the state; • Inadequate release of resources or poor utilization of released funds; and • Challenges with coordinating different sources of funding for PHC and RI(from m
government, WHO, UNICEF, PRRINN‐ MNCH, EU PRIME, etc) Activities supported include routine immunisation, supplemental immunisation, maternal health, supervision, routine data collection, community mobilisation, allowances for the midwives service scheme and currently exploring funding the free MNCH services. Funding is from LGAs (70%), state government (20%) and partners (10%) plus the partners provide technical support. The state has an account as does each LGA with adequate checks and balances re signing powers. Funds are released directly to the PHC finance officers who submit retirement statements every month signed by the LGA chairman. Subsequent funds are only disbursed upon retirement of previous funds collected.
Constraints affecting programme implementation
Security threats have moved from simple post election political violence to attacks that are of terrorist in nature with suspected international dimensions. The nature and complexity of the issues makes predictions on when the security situation virtually impossible. As a result programme planning and implementation is likely to become increasingly complicated. The PRRINN-MNCH programme has taken measures to mitigate risk while ensuring that the programme activities continue and that the service to, and improvements in, mother and child health in northern Nigeria are maintained. Nevertheless, the fragility of the situation cannot be under-estimated. The PRRINN-MNCH teams are congratulated on their dedication to the programme and to the issues which keeps them at their work under such difficult, tense and sometimes dangerous circumstances.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 29 304298/ Final
MOUs and change matrix – weak technical capacity among stakeholders and the unstable polity have slowed down progress to: i) establish monitoring framework for the MOU in Yobe and Zamfara States; ii) establish the similar monitoring arrangement for the change matrix agreement in Yobe, Katsina and Zamfara State. Scheduling a meeting with stakeholders has been the major stumbling block toward the development of the monitoring framework.
Across all 4 states:
There is weak leadership, governance and low institutional capacity at LGA level – which will have implications for future sustainability. Lack of realistic fiscal projections and timely, full release of funds at LGA level indicates both poor capacity and budget performance.
Zamfara & Yobe
The change in government in Zamfara has stalled the establishment of a Primary Healthcare Board and therefore slowed down the implementation of the PHCUOR law. Non release of GAVI funds by NPHCDA to Zamfara has created problems for the RI programme.
Other SLPs (SAVI and SPARC) are in the process of setting up, so support and synergies have not reached full potential yet
Jigawa:
State scale op of CBSD strategy needs to be revised based on affordable staffing model
Katsina:
The signing of the MOU between DFID and Katsina state government has been delayed and may be attributable to the current security challenges that limit movement of international staff. Stakeholder engagement with the health sector has not helped address major policy issues; disconnect between high level political commitment and results. Comparing the state allocation to health on a per capita basis, Katsina demonstrated the worst performance out of the four states.
4.3.2 Output 2: Improved human resource policies and practices
Output 2: Improved human resource policies and practices for PHC Score: A
Nigeria used to have one of the largest pools of human resources for health (HRH) in Africa: in 2006 there were approximately 39,210 doctors and 124,629 nurses registered (ratio of 30 doctors/100,000 pop and 100 nurses/100,000pop). As with other components of the health system, HRH varies tremendously across the country
with the north and rural areas bearing the brunt of staff shortages.13
Output 2 focuses on human resource management which is so vital for effective health service delivery. This is as much dependent on production factors, information systems, distribution, staff mix, recruitment and retention as it is on the political factors influencing human resources. Strengthening HR management is a major thrust of the PRRINN-MNCH programme as this is seen as one of the key bottlenecks to improving the PHC services in Nigeria.
Increasing the numbers and distribution of female health workers in northern Nigeria is a priority. Focus has been on accreditation of schools and training institutions, improving the throughput rate of training institutions, exploring retention strategies and the strengthening of the NPHCDA‟s MSS (Midwives Service Scheme). Helping
13
USAID and FMOH, 2009. Nigeria Health System Assessment. USAID. http://www.healthsystems2020.org/content/resource/detail/2326/.
DFID Human Development Resource Centre 30 304298/ Final
to build a fully functioning and transparent HRIS (Human Resource Information System) has been a key component.
Table 6: Performance against Output 2 indicators
Indicator 2011 target Progress
2.1 % of targeted facilities with at least one health worker trained in LSS
70% 76%
2.2 Status of HR policies and plans in each state
Operationalised Partially
2.3 Number of health professionals trained annually
N/A (Baseline 904)
456
2.4 % of professional staff given in–service training in MNCH in targeted PHC facilities
50% 69% achieved
Progress against expected results:
2.1 A total of 155 health facilities (76%) have at least one health worker trained in Life Saving Skills (LSS) and Zamfara has 100%. This 2-3 day training, developed by the Liverpool School of Tropical Medicine with the Royal College of Obstetricians and Gynaecologists (RCOG) has proved highly successful in at least 5 countries in reducing maternal and newborn deaths.
2.2 State HR policies and plans have only been partially operationalised in each state. All states have draft policies and plans (that include a gender component) but these have not been formally approved in Jigawa and have yet to be signed in the other three states.
2.3 There was no milestone for this indicator other than the number of health professionals trained annually among final year registered students at all state health training institutions. The baseline was 904, and since programme start-up, a total of 3,196 students have been trained, 456 of whom were trained in 2011. 42 new trainers were trained on RI/MNCH and 15 practical sites were established for RI/MNCH in-service training
2.4 69% of professional staff in targeted PHC facilities were given in-service training in MNCH with Zamfara reporting 100% against the target.
There are many other important HR-related achievements – some of which have national significance and therefore cut across output 7:
State HR coordinating committees meet on a quarterly basis and are using Human Resource Information System (HRIS) reports; plans for recruitment and training of community based extension workers (COMBEW) in Jigawa; bridging programme for Nursing Tutors to undergo the BSc Nursing programme in Zamfara have all been informed by evidence from programme.
Costs of accreditation of the health training institutions (HTIs) were incorporated into state plans/budgets for 2012. Two HTIs in Katsina were accredited and there were 319 graduates (CHEWs, nurses and Midwives) from the state HTIs in Yobe and Zamfara. In Yobe, a newly reconstituted accreditation committee for Dr Shehu Sule College of Nursing and Midwifery was inaugurated.
In Jigawa, PRRINN-MNCH supported the HTIs in planning for accreditation and the conversion of the Community Birth Extension Worker (COMBEW) programme to Community Midwifery. The Nursing and Midwifery Council
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 31 304298/ Final
approved community midwifery training in Zamfara State. PRRINN-MNCH was a key facilitator of the approval process.
PRRINN-MNCH supported the recruitment and training of HRH Local engagement consultants (LECs) from all programme States and development of job plans.
Only 15 EOC facilities have at least 3 health workers trained in FP and 106 PHC facilities of a target of 80 have at least 1 health worker trained in FP. This expertise must now be matched with demand for services – otherwise the trainees will become de-skilled.
State capacity to carry out step down training in Infant and Young Child Feeding (IYCF) was developed. A total of 24 trainers (8 per state) have been prepared for the 3 target states.
The 54th session of the National Council on Health has approved the establishment of HRH Divisions in all health Ministries Departments and Agencies (MDAs) as a national policy. (0utput 7)
The programme is concerned about the retention of midwives on the Midwives Service Scheme (MSS) and has initiated national policy dialogue around retention packages to sustain the scheme. (Relevant to 0utput 7)
A costing analysis was produced based on the HR Audit staffing norms for the development of MSP and Free MNCH costing template.
The capacity of the HR units in all states was improved through additional training of staff on HRIS, management tool kits, and Training Information Management System (TIMS).
Development of costed accreditation plans (through a participatory process with relevant stakeholders) for the 11 training institutions (schools of nursing and midwifery plus schools of health technology) of the 4 states including Jigawa.
Key internal and external constraints
Working in four of the most challenging states in Nigeria poses a number of problems and risks to the programme. These include the following:
Recent salary increases for health workers on limited state budgets already skewed towards personnel costs
High attrition levels and „ghost workers‟ have compounded the problem of collecting accurate HR data.
State HRH coordinating committees unable to influence national workforce policy issues
Strikes by labour unions, the petrol price hike and rising insecurity in many of the States, has slowed progress on planned activities including technical support to states to conduct in-service/step down training: e.g., CBLSS and FANC, PNC and FP.
Budget release to implement plans for accreditation requires persistent advocacy and follow up from state government (the Governor).
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 32 304298/ Final
4.3.3 Output 3: Improved delivery of RI and MNCH services
Output 3: Improved delivery of RI and MNCH services via the PHC system Score: A
Maternal, neonatal and child health indicators in these northern states are among the worst in the world. Output 3 is about service delivery in MNCH including routine immunisation and the systems supporting service delivery (drugs, transport, supervision, infrastructure and equipment). The MNCH programme is focused on Zamfara, Katsina and Yobe (with PATHS2 supporting MNCH in Jigawa). There have been major achievements impacting on maternal and newborn health: the 2011 mid-term household survey 2011 indicated that births attended by skilled birth attendants have doubled and infant mortality halved since MNCH inception. With scale up there is always a risk of quality being compromised, especially when supervision is likely to be affected by the security situation. The programme has implemented measures to improve the quality of facilities and introduced standards and guidelines as well as quality improvement teams to improve quality of service delivery. The team were not able to assess quality in field. The challenge will be to sustain this in the absence of supervision provided by the programme.
There are many factors beyond the control of the programme that have affected access to the field, retention of midwives, commodity supply and ultimately performance. In spite of these huge challenges, the programme has performed well, though if continued, they threaten to undermine continuity. In Zamfara and Katsina particularly, significant investment in MNCH has also been made by other programmes which will undoubtedly have helped PRINN-MNCH to achieve its own objectives. (See donor matrix for details on other programmes).
Table 7: Performance against Output 3 indicators
Indicator 2011 target Progress
3.1 % of LGAs reaching performance ranking tool (PPRHAA) scores over 75%
50% 28% Partially achieved
3.2 Number of PHC facilities providing Basic Emergency Obstetric Care
29 46 achieved
3.3 Systems for effective supervision in each State
Visits implemented with limited technical &
financial support from programme
Achieved
3.4 Number of 1-year-old children immunised against measles
403,556 590,200 Over- achieved
3.5 % of health facilities providing RI experiencing vaccine stock-outs of TT
19% 72% Range 46-100%
Not achieved
3.6 % of PHC facilities with tracer drugs available
62% 36% Range 24-49%
Not achieved
Progress against output 3 targets:
Of the six indicators, three have been achieved, one partially achieved and two have not been achieved. The consolidated results here do not reflect the fairly wide variation in performance between states. Key achievements, against the logframe include the following:
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 33 304298/ Final
3.1 % of LGAs reaching performance ranking tool (PPRHAA) scores over 75% . The PPRHAA (Peer and Participatory Rapid Health Appraisal for Action) revised guide and tools were used for this exercise across the states. PPRHAA findings were fed into the 2012 operational planning.
3.2 46 PHC facilities in all three MNCH states now provide BEOC against a target of 29. 139 PHC facilities (including BEOC) are now providing FP services but uptake is less than expected. The milestone for 2011 was 45,126 and performance was 51%. The Contraceptive prevalence target for End of Project (EOP) is only 4.2%. Yet, there is evidence of unmet need for family planning in the northern states (NC 18.7, 17.6% and NW 20.8% [DHS2008]). Anecdotal evidence suggests there is significant demand for implants in PRRINN-MNCH states (JHPIEGO).
3.3 Systems for effective supervision have been established in all states. A total of 40 quarterly integrated supportive supervisions were facilitated in LGAs/Gundumas of the targeted clusters. Supervision is essential and helps to maintain standards of care. Also noted, is that ACCESS/MCHIP also developed an integrated supervisory system to be the standardised state version (Zamfara and Katsina).
3.4 590,200 one-year-old children were immunised against measles against a target of 403,556 (Figure 13). Performance was uneven across the states however, with the control area in Zamfara showing better results than the intervention.
Figure 11: Immunisation coverage
Source: PRRINN-MNCH Annual Report 2011
3.5 The supply of vaccine has been a continous problem prompting a review in March 2012. The NPHCDA spoke of its inability to influence a situation where imported commodities are held up, the distribution and cold chain systems are inadequate and LGAs lack budgets to access commodities among others. The percentage of health facilities providing RI experiencing vaccine stock-outs of TT was therefore not reduced significantly with a range of 46-100% experiencing stockouts. The introduction of solar fridges by the programme will help ensure there is functional cold chain at facility level but the challenge is likely to be in the sustained functioning of the fridges and maintenance always tends to be a challenge. The focus on polio campaigns has undoubtedly exacerbated the situation and until there is commitment at national level to reform the customs, and revive the supply chain, improvements are unlikely. High level advocacy is needed by the donors to push for action by the Federal Government. This is an historic problem which always requires an emergency response from donors, but for how long? (see Annex 4 for a more detailed overview of challenges in the vaccine supply chain and logistics system).
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 34 304298/ Final
3.6 While non availability of vaccine is a residual problem in most states, others including user fees, inconvenient dates and religious reasons seen in Figure 12 below are cause for concern, reinforcing the need for continued communication and advocacy at community level.
Figure 12: Barriers to uptake of immunisation services reported by state personnel
Source: PRRINN-MNCH Annual Report 2011
3.7 Delays in procurement have affected essential medicines and the percentage of PHC facilities with tracer drugs available has not met the expected target of 62% - and ranges from 24-49% across states. Regular consultative meetings with Crown Agents (responsible for drug procurement) are yielding positive results and delivery of cluster 3 SDSS items in all three states has started. 43 of targeted facilities now have a sustainable drug supply system (SDSS) of target 121. This is intended to address drug stock-outs, poor financial accountability, and support state medical stores as the assured source of drug supply. States can eventually take control of drug procurement and the shift from externally-sourced drugs through Crown Agents to state procurement will be important provided there are extremely robust mechanisms to ensure transparency and quality assurance. Unfortunately, the highly politicised but poorly managed free MNCH schemes distort efforts to effectively establish and manage the SDSS
Under Output 3, a wide range of activities has been captured in the M&E system.
Maternal and newborn care
With Liverpool School of Tropical Medicine and Save the Children, the programme has two globally renowned organisations providing Life Saving Skills (LSS) training maternal, newborn and child health in 3 states. The LSS training has proved very successful in other countries. It is however only 2-3 days, classroom based training whereas the training provided by the American Association of Midwives for LSS in Jigawa under PATHS2 is 8 weeks including working with a patient caseload. In the context of the FMOH now aiming to harmonise the LSS training for Nigeria, it is important that PRRINN-MNCH not only participate in the FMOH-led meetings (LSTM attended the first one) but that the programme is finding a way of providing training and certification that will meet the agreed requirements.
While facility delivery with a skilled birth attendant has increased significantly under the programme, uptake has not matched expectations. While 37,731 (27%) pregnant women attended first ANC, only 13,106 deliveries were attended by skilled birth attendants (of target 120,960) and of these, 10,539 (44%) mothers received postnatal care. Skilled attendance at delivery will lead to better maternal and newborn outcomes. Figure 10 below provides a curious analysis of the reasons for women not wanting to use the facility. While health worker attitude is not significant here, the view that it is “not necessary” appears to be significantly
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 35 304298/ Final
higher since the programme started! Clearly, the community conversations need to explore what lies behind these findings and address the reasons that are important to women.
Figure 13: Reasons for not delivering at health facility for most recent live birth in preceding five years
Source: PRRINN-MNCH 2009 Baseline and 2011 Mid-Term household survey
PRRINN-MNCH has recognised that increasing coverage of services is not enough and that for such services to be effective in reducing maternal & neonatal mortality and morbidity, attracting patients and achieving clients‟ satisfaction is key to success but also context specific.14 Data from baseline and mid-term MNCH surveys shown in Figure 13 highlighted reasons for not wanting to delivery at a health facility though these results do not indicate positive changes in attitudes such as the significant increase in people considering facility delivery „not necessary‟ two years on from baseline.
National scale up of the LSTM model of Maternal and perinatal Death Audits and Confidential Enquiry will help to identify causes behind the maternal deaths to feed into pre and in-service training. It is challenging to roll this out and will require strong leadership by FMOH to bring all partners on board. Technical support to the NPHCDA on the MSS programme including development of national MNCH guidelines and in-service training manuals for CHEWs and MSS.
Family planning uptake is worryingly low in the northern states as illustrated in Figure 14. Opposition on religious grounds does not ring true when uptake in other Islamic countries (e.g. Iran with CPR of 73%) is high.15 The 2008 DHS shows that 60% of all contraceptives are procured from private sector sources (69% of male condoms and 74% of pills) – mainly through social marketing. PRRINN-MNCH has rightly been cautious in their approach, but given that the Planned Parenthood Association of Nigeria has been providing FP in the north more than 50 years, and SFH since 1993 among others, it is not a new concept.
14
PRRINN-MNCH Technical Brief 4. An update of capacity building for quality improvement of MNCH services in PRRINN-MNCH supported EOC FACILITIES (Clusters 1, 2 and 3) 1515
WHO. World Health Statistics. 2011
18.6
13.6
3.8
2.1
52.5
8.6
2.8
1.6
6.8
1.1
13.2
2.5
1.2
4.3
2
7.6
3.4
42.7
0 10 20 30 40 50 60
Not necessary
Not customary
Too far/no transport
Cost too much
No spousal permission
Health worker attitude
Baseline Midterm control Midterm intervention
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 36 304298/ Final
Figure 14: Contraceptive use in PRRINN-MNCH states by age
A significant amount of training has been provided to improve competency of MNCH service providers and quality of care through introduction of standards and guidelines. These include among others, competency-based Life Saving Skills (LSS), EOC and Neonatal Care (NC) skills training, standards for MNCH and FP services; criterion-based audits for EOC Health Facilities; training for QI, criterion-based audit,
standards for MNCH and FP services, MDR and PNDR Maternal Death Review and Perinatal Death Review. Clinical obstetric and neonatal care protocols and wall charts have been provided to EOC facilities in clusters 1,2, and 3. Also guidelines and training curricula for Focused ANC (FANC), PNC and FP revised and approved by FMOH. This resulted in the development of an integrated training curriculum for FANC, PNC and FP
Newborn health
Various interventions in support of newborn health have been introduced such as neonatal sepsis, Integrated Management of Newborn and Child Illness and Kangaroo Mother Care (KMC), an excellent and life-saving intervention introduced to Nigeria in the late 1990s for small for dates and low birth weight babies. PRRINN-MNCH (SCUK) has collaborated well with ACCESS/MCHIP in all these areas. Mutual lessons learned on KMC (such as stigma from hospital-based KMC) are important to share more widely.
The mid-term survey (MNCH behaviours and CBSD (31052012) assesses feeding of the newborn from baseline. Breastfeeding practice (which is currently very poor at 0.6% after delivery has reduced from 17-13% for the first 6 months). Facility delivery will help with both breastfeeding and FP uptake. Eight master trainers trained on Infant and Young Children Feeding will need to ensure that practices improve.
Other support for services has included renovation of facilities, equipping, providing solar panels for continuous electricity and solar fridges for vaccine. The role of the Health Facility Committees becomes very important in ensuring these are maintained and that staff are working to expected standards for provision of RI, IYCF and EOC services. Introduction of the maternal death audit and its adoption at national level for use in MSS is a significant achievement.
Internal and external constraints
Various constraints have either impeded progress or threaten continued progress. Some are beyond the control of the programme. These include:
Poor performance of building consultants
Duplication of efforts such as with the integrated supervision system (ISS)
The security situation has affected consultancy, supervision, retention of midwives, and night-time sensitisation films among others.
Capacity for routine data collection and use
The retention of MSS MWs and other staff who are posted out coupled with deep-rooted socio-cultural factors against facility delivery
Effective supervision/follow up of Quality Improvement activities
Proper implementation of IMCI – with guidelines not always used
Source: PRRINN-MNCH 2011Mid Term Household Survey
0.5 1 1.5 1 1.12.4
3.9
1.30.90.6
1.21.4 1.4
2.9
3.9
1.3
0
1
2
3
4
5
6
7
8
9
15-19 20-24 25-29 30-34 35-39 40-44 45-49 Total
Age group
Perc
en
tag
eAny modern method Any traditional method
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 37 304298/ Final
Delays in procurement of medicines and other supplies by Crown Agents (oxytocin, anti-helminthics, blood bags etc.). This appears to be resolved but it is important that Crown Agents has knows what budget they are working to avoid back and forth on quantification and procurement, which has caused delays.
4.3.4 Output 4: Operational Research
Output 4: Operational research providing evidence for PHC stewardship, RI and MNCH policy and planning, service delivery, and effective demand creation Score: A+
A study in Nigeria revealed that some of the major challenges in informing policy and practice with evidence from health systems research are capacity constraints at individual and organisational levels, communication gaps and poor networking between policy makers and researchers, and the non-involvement of healthcare recipients in identifying and planning care delivery needs.
Output 4 cuts across all others. There is emphasis on strengthening OR capacity and on the use and dissemination of the results. The core activities of the health systems research component of the PRRINN MNCH project are to build a sustainable operations research capacity, conduct research (including performance based financing), and develop an Health Demographic Surveillance Site (HDSS) that meets international data quality standards.
Table 8: Progress against Output 4 indicators
Indicator 2011 target Progress
4.1 Number of OR outputs into supply & demand aspects of MNCH feed into programme
4 8 Achieved
4.2 State plans reflect OR results 1 example per state
Achieved
The results from 2011 demonstrate that the milestones against the two indicators for output 4 have been met: The number of OR outputs into supply & demand aspects of MNCH feed into programme was double the target.
4.1 In terms of OR into supply and demand aspects of MNCH, examples include the expansion of outreach services into 3 LGAs in Jigawa state agreeing to buy and supply motorbikes to female CHEWS. There has been a delay in the CHEWS using this approach waiting for appropriate training.
These examples demonstrate the ability of OR to develop new approaches to delivery of services and feed this back into the programme and this can be seen in all four states. The number of OR outputs into supply & demand aspects of MNCH feed into programme was double the target
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 38 304298/ Final
4.2 Plans in all states reflect OR results as follows:
In Jigawa, community based service delivery is incorporated in the state 2012 plan. Jigawa state will also introduce ETS and CE activities into CBSD pilot communities.
In Katsina, the SPHCDA is implementing a bi-annual monitoring and supervision of the mobile ambulance scheme (MAS) and the SMOH has a budget line for OR.
In Yobe, a supplementary budget for recruitment of skilled birth attendants was based on data from outreach pilots.
In Zamfara, the formation of women groups and TICK sheet pilot for immunisation is included in 2012 plans
Other achievements under this output include:
The on-going development of the HDSS site is highly commendable and demonstrates strong leadership from the OR team to ensure that this site will not be lost once the programme draws to a close. The HDSS site has real potential to generate useful data that can be used for further analysis and research.
The establishment of the ORACs in each state strengthens health research governance and a growing understanding of the importance and usefulness of research. As with the HDSS site there is a legacy for the ORAC beyond the life of the programme and now the ORACs are in place to have oversight of any research that is undertaken in their state.
Operational research results, dissemination and impact
The ETS studies that have been conducted under the MacArthur programme are using different models across the different states. However it was clear that implementing one such study in Katsina where some financial incentive was given to drivers has raised some issues about disrupting the existing ETS process which already existed, but on a voluntary basis. This demonstrates the need to look at how such studies are designed and implemented within these communities and this issue should be reflected in the write up of the study.
Other OR studies in each of the states have included:
Katsina is exploring the effect of providing existing community volunteers, who are expected to facilitate referrals for emergency obstetric care, with mobile phone recharge cards and solar battery chargers on the rates of ETS referral from the communities to the facilities.
Zamfara is exploring the effect of providing financial incentives to health workers (Nahuche Health Centre) and ETS drivers on the outcomes of emergency maternal care services.
Yobe is piloting the provision of outreach MNCH services by female Community Health Extension Workers (CHEWs) to five hard-to-reach communities in Kelluri District of Geidam Local Government Area (LGA). Yobe is also piloting a demand side PBF scheme that will reward uptake of specific maternal and child health services.
The study in Jigawa is a trial of a strategy to bring health services close to the doorsteps of communities by deploying female CHEWs to live and provide a pre-determined package of maternal and child health services in these remote communities.
A national dissemination meeting was held in Kano. Each state was represented by a number of stakeholders, the state team managers, and the OR coordinators. Participation also included representatives of collaborating institutions (ABU, UDUS, and Bayero University). Implementation research studies presented were the CBSD, Integrated Outreach services, the TICK study, and evaluation of the mobile PHC services.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 39 304298/ Final
4.3.5 Output 5: Improved Information generation and use
Output 5: Improved information generation with knowledge being used in policy and practice Score: A+
Output 5 refers to knowledge management more generally, including health management information systems, monitoring and evaluation and publications. Performance of the programme has demonstrated that good data, when understood and analysed, can be immensely powerful and effective. The data has been used for a variety of purposes beyond planning and performance review, such as informing media. Ownership by senior health officials has been demonstrated in all states and in Katsina, monthly data are being demanded by the PS.
Each of Nigeria‟s 36 states has its own HMIS policy, though implementation is limited. Despite the prioritisation in policy, HIS has been chronically underfunded and underequipped particularly at the sub-state level, with critically poor coordination from the central level. Reporting across levels is sporadic and deficient. The issue of vertical programmes has further exacerbated the weak M&E systems as each programme often has its own reporting system. Different agencies have been working to strengthen HMIS at different levels of the health system.16 PATHS2 also has HMIS strengthening under its mandate. A challenge therefore for PRRINN-MNCH has been to help get HMIS working properly, building capacity for its generation, analysis and application.
Progress against output indicators and targets
Table 9: Progress against Output 5 targets
Indicator 2011 target Progress
5.1 Demonstrated level of understanding in use of information by trained HMIS officers in each state
Moderate Achieved
5.2 State plans increasingly built on evidence from HMIS
Moderate Achieved
5.3 % of LGAs with HMIS MNCH data collated at State level on a monthly basis
75% 92%
While the logframe indicators are more limited to HMIS, there have been significant improvements in other areas of knowledge management and M&E for PRRINN-MNCH such as:
5.1 MIS Officers in all the programme states demonstrated an improved level of understanding in use of information for planning meetings and performance reviews with some states referring to high levels of understanding. Katsina reported an appreciable improvement in the capacity of the State HMIS team who can now do data entry, analysis and presentation of data using the DHIS software. In Zamfara, the databank is now the source of data for the SMOH and submission rates remain above 75% for all health facilities and >90% for priority 1 HFs.
5.2 There are some excellent examples of states using evidence generated by the programme clusters to inform their plans. In Katsina, not only is there an improvement in the capacity of State HMIS team which is now capable of entry, analysis and presentation of data using the DHIS software but monthly data
16
The Data Documentation Initiative: FMOH, 2010. Towards implementation of Data Documentation Initiative (DDI) in Nigeria. http://www.fmh.gov.ng/index.php/resources/reports/746-towards-implementation-of-data-documentation-initiative-ddi-in-nigeria
DFID Human Development Resource Centre 40 304298/ Final
being demanded by the PS. There is monthly supervision from the DPRS and regular HMIS meetings. In Jigawa, State 2012 MTSS and operational plan significantly reflects data from HMIS and there are numerous improvements in data quality, frequency. Yobe showed some very impressive results with 100% of LGAs collating HMIS data on a monthly basis with 91% timely submission of data.
5.3 92% of LGAs in the programme states collated HMIS MNCH data at state level on a monthly basis (milestone - 75%). Yobe and Zamfara reported 100% while Jigawa and Katsina reported 75% and 65% respectively.
Other achievements include:
At Federal level, the programme supported the NPHCDA to conduct the first quarter external data quality audit. A total of 12 states were included in the audit
The website is fully functional and is being updated quarterly. A total of 31 technical and policy briefs as well as case studies across the 7 outputs were produced.
A video documentary of programme interventions in Yobe State was produced and discussion Guide on Community Engagement developed
In the absence of vital registration, getting accurate maternal mortality estimates is notoriously difficult, especially when the majority of births are at home. Using the sisterhood method to estimate MMR in the four states interviewing, 3,080 women were interviewed which provided valuable estimates. While not providing estimate for survey year, the data showed that the lifetime risk (LTR) of maternal death was 9% (or about 1 in 11) and the estimated MMR was 1,271 deaths per 100,000 live births (95% CI = 1,152 to 1,445) which is significantly higher than official estimates.
Abstracts on maternal mortality estimates in northern Nigeria and RI communication in Jigawa accepted by international journals.
Concept notes on Governance/PHCUOR, operational system strengthening and community engagement developed for panel discussions at WHO conference in Beijing.
Papers for panel discussion at Beijing conference submitted for review and abstracts on measuring maternal mortality in the programme states and on RI communication have been accepted for publication in international journals.
The PRRINN-MNCH website is fully functional and is being regularly updated and edited. A total of 31 technical and policy briefs as well as case studies across the 7 outputs were produced.
The programme M&E system is very detailed, providing feedback on all aspects of the programme. The midterm MNCH household survey took place in 2011. A baseline MNCH household survey was conducted in 2009 and the 2011 survey tracks progress on baseline or pre-intervention levels.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 41 304298/ Final
4.3.6 Output 6: Increased demand for RI and MNCH services
Output 6: Increased demand for RI and MNCH services Score: A+
The focus of this output is to increase demand for MNCH services (including RI) within a strengthened PHC system. The approach involves supporting the community and LGA and state governments to build a sustainable community system that links up with health providers and policy makers to ensure access to quality maternal and child health services and increased accountability. The baseline and follow on survey demonstrate a shift in social norms relating to MNCH and RI, suggesting a growing consensus around the need for better preparedness for maternal emergencies, and for uptake of RI. There is also evidence of behaviour change seen in significantly increased immunisation uptake in
two of the three states (Yobe and Zamfara) and a small but important increase in facility deliveries supported by the emergency transport system (ETS) and community funds. Many different types of innovative and effective community
interventions and community response systems have been established which have successfully involved local and religious leaders and leveraged support from the LGA. Stimulating the demand side for service delivery (voice and accountability) is therefore vitally important while at the same time, service quality is improved. Civil society, which is at the forefront in the community is generally weak however.
Progress against output’s indicators and targets
Table 10: Progress against logframe targets
Indicator 2011 target Progress
6.1 Increased political support for MNCH (including RI) evidenced by high level public events
1 at state level; 2 at LGA level
5 at state 27 at LGA
6.2 % of wards with a development committee and/or health partnership implementing a community action plan
30% Over-achieved 48%
6.3 % of women in targeted areas who have standing permission to take their child to a health facility
74% Over-achieved 83%
6.4 % of women who know at least four of the maternal danger signs in targeted areas
30% Over-achieved 91%
6.5 % of facility health committees for intervention facilities in targeted areas actively monitoring drugs
50% 58%
6.6 % of mothers of children <2 in targeted areas who know the childhood vaccination schedule
30% (changed from
50%MTR & 40% M&E)
Over-achieved 70%
Under output 6, all the expected results under the 6 indicators have been exceeded indicating that communities have been successfully mobilised around MNCH issues. Reported institutional delivery rates over 2010-2011 were 22% in Yobe and 21% in Zamfara a significant increase over 4% in the baseline survey. In Yobe, 4,187 deliveries were in the facility and of interest is that over 19,000 men were reached with information. In Katsina, the increase in performance between 2010 and 2011 is remarkable as shown below.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 42 304298/ Final
Table 11: Progress on Maternal health M&E indicators from mid-term evaluation
The challenge for the programme is to ensure that in increasing demand, there is an appropriate balance in the supply of quality services that people want to use.
6.1 Increased political support for MNCH (including RI) has been seen by high level public events. Jigawa had one with the Deputy Governor on Polio and one with the traditional leaders; Forum. Various events took place at Gunduma level. A total of 8 State ministries/ departments/ agencies (MDAs) have included funds for MNCH demand side issues in their budgets and partially led community engagement activities.
6.2 % of wards with a development committee and/or health partnership implementing a community action plan.
6.3 83% of women in targeted areas now have standing permission to take their child to a health facility from a baseline of 55%. The rate varies from state to state but the community conversations have included men – which is appropriate. Society for Family Health reported that they have had to stop community meetings in areas of insecurity as gatherings of people are easy targets. This could undermine the demand work in some of the states.
6.4 91% of women know at least four of the maternal danger signs in targeted areas compared with only 1.4% at baseline which is a huge increase as shown in Figure 16. The next challenge is to ensure that appropriate action is taken when women show danger signs, which is a potential OR question to be addressed.
Figure 15: Knowledge of at least 4 of the danger signs by gender
Source: PRRINN-MMCH Annual Report 2011
6.5 There was not a significant increase in this indicator related to the role of health facility committees but work is underway to identify mechanisms that will allow hospital health committees to interact with and support PHC facility committees; FHCs advocacy and lobbying capacity is being built so that they can interact more effectively with local and state government; quarterly
Indicators 2010 2011
Number women with complications transported by ETS (ALL) 267 1,324
Number of pregnant mothers with first ANC visit 345 8,008
Number of pregnant mothers with four ANC visits 352 2,096
Number of skilled deliveries in the community 196 4,860
Total number women benefiting from EMC savings 62 265
Number of women benefiting from blood donation 42 163
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 43 304298/ Final
meetings between FHCs and LGAs have been introduced, providing for the first time a systematic mechanism through which the committees can challenge service delivery and policy failures; and plans are underway to organise the committees into an alliance of LGA FHCs.
6.6 There was a 4-fold increase (from an average of 15% to more than 60%) in knowledge of the immunisation schedule across the three states. Uptake also increased. Across the three states 60% of respondents stated that their child had received four immunisation doses, compared to the baseline figure of 21%. At baseline, 68% of children were reported as never immunised. This had fallen to 31% at end line.
There are many activities under this output – some of these are discussed below:
Getting women in labour to health facilities saves lives. At the time of the baseline KAP survey, many women who had suffered a complication used public transport to get to a health facility. By the time of the end line survey, there had been a significant increase in the use of the community emergency transport system (from 20% to 78%). 3,334 women, equivalent to 94% of reported maternal complications, were supported by community emergency transport schemes in 2010 and 2011. The KAP end line survey showed that 75% of respondents knew of someone in the community who had benefited from the services of an ETS driver.
KAP end-line community engagement survey in the first cluster indicated very positive results in terms of increased knowledge, changes in social norms and behaviour change. Community savings schemes have been created for emergency maternal care in the three MNCH states.
“PRRINN uses a responsible and sensitive approach on areas such as female health workers, family planning and women getting standing permission to attend facilities. This permeates every level of the organisation. The logistics officer has a level of professionalism, the State Team Leaders are well connected and well respected by their state technocrats and political officials (particularly recognised in Yobe State). (DFID Adviser)
Hospitals do not have functional blood banks and the situation where blood donors pay to give their blood is of great concern as there has been significant investment nationally in the blood transfusion service and the National Blood Policy calls for free donation of blood. Nigeria‟s leadership as seen below, has voiced commitment to safe blood. Lack of implementation is an advocacy issue since without this, CEOC is problematic. During 2010 and 2011, a total of 654 women were supported by blood donor groups under the programme – this is an achievement. Advocacy is nevertheless strongly recommended.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 44 304298/ Final
“Goodluck Ebele Jonathan, is fully committed to NBTS and the Former President, Commander in-Chief of the Armed Forces GCFR, Chief Olusegun Obasanjo, at the opening of the Abuja Demonstration Centre of the National Blood Transfusion Service on May 12th 2005. Certainly, an act to emulate. Let us follow such life-saving acts.” NBTS August 2012
To add a focus on young women into ongoing programme activities PRRINN-MNCH programme was awarded additional funding by DFID in partnership with the Nike Foundation (the DFID Girls Hub Initiative). With this it is aimed to create 2000 young women support groups. This initiative has the potential to highlight the problems resulting from child marriage, lack of girls‟ education and access to information and services among others. It is badly needed in northern Nigeria and the approach has been successful in other countries e.g. Ethiopia where similar problems exist.
The 2011 MTR recommended that programme evidence is used for advocacy– and more can be done in this area especially at the level of the FMOH where knowledge of the programme (in Family Health Division) was lacking. While PRRINN-MNCH collaborates mainly with the NPHCDA, if the most significant constraints to the programme‟s progress are to be overcome, advocacy at the level of the FMOH is needed and PRRINN-MNCH needs to make even more effective use of its excellent documentation and data.
4.3.7 Output 7: Improved capacity of Federal Ministry level
Output 7: Improved capacity of Federal Ministry level to enable States’ routine immunisation activities Score: A
The federal-level office in Abuja participates in a number of key groups/committees and works to strengthen relations with government MDAs (e.g. FMOH, NPHCDA, MDG, NHIS, MSS) and other development partners/programmes. A key feature of PRRINN-MNCH‟s approach has been the interlinking between what happens at federal level, in terms of policy and supporting implementation, and activities at state and LGA levels.
The NPHCDA is a key partner and has collaborated on the work of „Bringing PHC under one roof‟, the Midwives Service Scheme (MSS), the system for Integrated Supportive Supervision (ISS), and the Maternal Death Review (MDR), among others. The programme has also built links with the National Health Insurance Scheme, the Federal Ministry of Health and the MDG office. PRRINN has succeeded in getting various interventions/approaches (e.g. Maternal Death Review, PHCUOR)adopted by FMOH for national roll-out.
The 2011 MTR recommended that programme evidence is used for advocacy. While PRRINN-MNCH collaborates mainly with the NPHCDA more could be done in advocacy at the level of the FMOH where knowledge of the programme (in Family Health Division) was found lacking.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 45 304298/ Final
Progress against indicators and target
Table 12: Progress against Output 7 targets
Indicator 2011 target Progress
7.1 Formal systems for leveraging, accessing and utilising additional PHC funding
2 systems implemented
Achieved
7.2 Federal level delivers 100% vaccines and supplies to states on time
100% Partly- achieved
7.3 Agreed strategies to improve efficiency of RI
Strategies implemented
Achieved
7.1 Formal systems for leveraging, accessing and using additional PHC funding implemented: GAVI, MSS, PHCUOR, MDG conditional grant.
7.2 Federal level vaccine deliveries vary with the type of antigen. Federal cold store data as of September 2011 indicated that deliveries to OPV, HepB & Measles was 100% while for Yellow Fever 82% and T.T 84%. However, data from the federal store does not reflect the reality on the ground. There was persistent shortage of vaccines and supplies in all the four programme states. Quarterly supervision indicated that 72 % of health facilities providing RI experienced vaccine stock-outs of TT and other antigens except OPV.
The problem of stockouts is both chronic and widespread, primarily due to delays in the release of funds and poor management of immunisation funding in Nigeria. The leadership of the NPHCDA is committed to resolve these issues, following the significant decrease in national DPT coverage rates caused by the 2011 stock-out. Problems include:
Non-availability of documents for vaccine management and record keeping and poor record keeping practices;
Insufficient cold storage capacity and use of non-WHO PQS cold storage equipment;
Insufficient electrical power (e.g. lack of generators or funds to fuel generators) for non-solar cold storage equipment Lack of preventative maintenance and repair for cold chain equipment and related generators;
Inefficient distribution of vaccines and other immunization commodities, and lack of funds for distribution;
Insufficient technical knowledge and skills for cold chain officers and cold chain supervisors, and related lack of training and supportive supervision for cold chain personnel;
Inadequate physical storage space.17
7.3 Agreed strategies to improve efficiency of RI approved and implementation commenced including New Vaccine Initiative and Effective Vaccine Management. Strategies can now be informed by evidence collected from the 2011 review which DFID requested. PRRINN-MNCH hired an international cold chain consultant to work with a national logistician to analyse challenges and solutions to the vaccine cold chain and immunisation logistics at the national level and in the PRRINN-MNCH states. This was carried out by high level consultants (contracted by Output 3 and supported by Output 7)
Achievement of annual M&E milestones
Specific examples of achievements against annual M&E milestones include:
Supported NPHCDA core group to disseminate key findings of the study on PEI to identify reasons for un-immunized and zero dose children.
17
Nigeria. Overview of challenges in the vaccine supply chain and logistics system. May 2012.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 46 304298/ Final
SPHCDA established in 15 states and processes for establishment in additional 5 states on-going
Proposal for the New Vaccine Initiative (NVI) developed and approved by GAVI. Programme supported review of the existing RI tools in line with NVI
GAVI fund guarantee through UNICEF against vaccines stock-outs while Presidential Economic Team approved for 1st line charge to the Federal Budget for Immunisation funds from 2012
Emergency action plan on intensifying the polio eradication effort developed for the period of May – December 2011.
NPHCDA supported to conduct external data quality audit in selected 12 states
Support for federal level child survival and maternal health actions
At federal level, the PRRINN-MNCH federal-level office has played a key role in linking central policy with implementation at sub-national levels as shown in the following examples:
Helping states to access GAVI funds, by supporting the State Ministries of Health to effectively retire and access ongoing funding tranches from GAVI. Subsequently at federal level where PRRINN-MNCH assisted the GAVI office in NPHCDA to review the processes and tools for accessing and retiring the funds and participated in developing a set of master trainers who now train across all states in Nigeria.
„Bringing PHC under one roof‟ by working closely with NPHCDA at federal level to develop the core concepts and implementation guidelines which were subsequently adopted by the NPHCDA Board and presented by them to the National Council for Health (NCH) in May 2011, where they were endorsed as federal-level policy.
The Midwives Service Scheme (MSS) is an ongoing initiative to address the shortage of skilled birth attendants (SBAs) particularly in Northern Nigeria. At federal level activities have included development of M&E tools for the initiative and fieldwork with NPHCDA reviewing the effectiveness and impact of the MSS.
Work on the costed minimum service package (MSP) HAS continued to gain momentum. The MSP modelling work was finished in 2011 and after piloting it in the PRRINN-MNCH states, this model will be revised in early 2012.
To overcome constraints to support for the immunisation programme, advocacy at the level of the FMOH (Family Health Division, Permanent Secretary) is needed and PRRINN-MNCH could make even more effective use of its excellent documentation and data.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 47 304298/ Final
5 Risk analysis and mitigation
A detailed and updated risk assessment from the previous review is found at Annex 4.
5.1 Key challenges
Most of the challenges have already been highlighted in different sections of this report. Over-arching challenges include the following:
Political insecurity is a real threat to the programme – affecting movement of staff, supplies and access to services. It will also be difficult to arrange group/community meetings which could potentially be a terrorist target. The programme has no control over this situation except to have policy and measures in place to prevent and cope with any problems.
Regular and adequate supply of vaccines – cannot be resolved at state level. High-level advocacy is needed by the donors. However, even if vaccine availability is improved, the distribution to LGA level remains problematic. Options for using private sector delivery channels can be explored.
There is still global pressure on Nigeria to eradicate polio. This is important, but consumes vast human and financial resources and consistently takes the focus away from routine immunisation.
Balancing supply and demand of services - this will be an on-going need. If demand is generated and people‟s expectations are not met, because of lack of commodities, lack of staff or similar, they will be harder to convince in future.
Overcoming cultural barriers to demand for facility delivery and family planning: in northern Nigeria there are extremely deep-rooted cultural factors which determine where a woman should deliver and how. This varies from area to area, but finding out what factors are important and trying to address them in the facilities is critically important. Also important is changing the mindset of clinicians who appear reluctant to accept that traditional practices such as squatting for delivery is in fact better and easier for the woman and is supported by evidence.
Chaotic drug supply system at all levels challenges the provision of quality SDSS commodities beyond the seed stock supply. The programme has resolved many of the problems related to medicine supply but measures need to be in place to ensure continuity of supply through state systems. Building procurement capacity is vitally important. For contraceptives – supply is centralised and erratic. Good quantification helps and backup arrangements through the private sector e.g. Society for Family Health.
5.2 Other challenges
The recent increase in state personnel expenditure as a result of the new national minimum wage has an impact on recurrent & capital budgets
Delays in release of funds by states has slowed down implementation of some activities
Slowing down of planned facility upgrades for quality MNCH services due to security constraints
Flood of donor resources to NPHCDA (but with not well defined agenda) crowding out program strategic but minimally resourced support
Steep decline in retention of MSS MWs in Yobe and Katsina and to a lesser extent in Zamfara as a result of security concerns
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 48 304298/ Final
The slow progress by the new government in Zamfara to implement the PHCUOR law passed by its predecessor
Accreditation of health training institutions is not a top priority for state governments and therefore receiving minimal funding
HRH is strongly influenced by politics
Collaboration with MANY programmes is time-consuming. Opportunity costs and potential synergies have to be carefully managed.
Layered decision-making and changes in leadership leads to inconsistencies in focus and implementation of policies.
Weak PFM causes delay in state and LGA budget approval and release.
Limited capacity of state agencies to effectively coordinate and lead community engagement activities.
Internal challenges
Resource constraints limit ability to pursue opportunities at National level
Staff and consultants restricted movement due to security situation
High workload on staff limits available time to closely follow up and provide monitoring support
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 49 304298/ Final
6 Key strengths and challenges of partnership with Government
The assessment team had little opportunity to interact with government partners and to understand their perspective on PRRINN-MNCH. From programme documentation, PRINN-MNCH has done a vast amount to strengthen the capacity of state ministries and of the NPHCDA in a variety of ways – already discussed. There are strong and encouraging statements such as the one below that reflect the government partners‟ appreciation of the support PRRINN-MNCH has provided over the years.
For a programme that focuses on the public sector, sustainability is very difficult to achieve especially at LGA/Gunduma level where financial and human resources are in short supply and very inconsistent.
The greater the ownership by government, and the more the government does on its own, the stronger the chance of sustaining capacity, commitment and
functionality of systems. While the team was not in a position to judge the level of ownership by government, there are signs that efforts to strengthen relationships and government ownership might be increased:
When the team visited the Federal Ministry of Health, the programme was not known by the Director of the Family Health Division or her colleagues. While this team is relatively new, it suggests that PRRINN-MNCH might be somewhat slow off the mark in building these important and strategic relationships.
None of the Ministry of Health websites in the four states mentions PRRINN-MNCH. This could be a good sign, in terms of having a discrete approach, but it might be expected that PRRINN-MNCH is seen as a partner to the MOH.
PRINN-MNCH exists to support and strengthen the work of government. This is not fully reflected in the literature which is PRRINN-MNCH „branded‟, and in the case of the excellent Annual report, carrying logos of the donors and implementing partners but no logo of the government or, a foreword by the state Ministers or Commissioners.
There is a risk that the PRRINN-MNCH branded literature will be side-lined when another new programme takes its place (as has happened to a large extent with other similar programmes). Where possible, documents should reflect the partnership and in the case of any state reports, guidelines, manuals etc., these should be fully government branded with PRRINN-MNCH support discretely reflected.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 50 304298/ Final
7 Partnerships and synergy with other related programmes
PRRINN-MNCH is a programme based on partnerships. The key partnership is that of PRRINN-MNCH with the government of Nigeria partners at different levels and this has been discussed. Another key partnership is that of DFID with its Norwegian co-financiers. As „like-minded‟ donor organisations, with DFID having oversight at country level and NORAD contributing to the reviews, this partnership appears to work well.
There are many other partnerships, and this section will discuss some of these:
a) Programme partners; b) DFID-funded state partners; and c) other health partners. In the absence of any other available partner mapping, a 2010 (UN-generated) map is provided separately to this document for reference.
7.1 Programme partners
The three key implementing partners are Health Partners International (HPI), GRID Consultants and Save the Children UK. Liverpool School of Tropical Medicine (LSTM)/Liverpool Associates for Tropical Health (LATH) is a technical partner, providing Life Saving Skills Training.
HPI (UK-based) and GRID (Lagos based) were among the implementing partners of PATHS1, so have long experience in Nigeria and have used their prior experience on PATHS1 and other programmes to good effect, building on earlier work. Save the Children UK is based in Abuja, and provides the inputs on newborn health. SCUK also collaborates with other programmes so can use this wider perspective to good advantage. LSTM‟s training model is well known to DFID, and Nigeria is one of the participating countries of the latest multi-country „Making it Happen‟ LSS programme funded by DFID African Regional programme.
Crown Agents has been contracted for the procurement and has been based in Nigeria for many years providing procurement expertise to many DFID-funded programmes.
Both PRRINN-MNCH and Crown Agents (interviewed during this mission) report significant improvements, with procurement now on schedule and on cost targets. Crown Agents explained some of these delays which include:
CA reported that when responding to quantification from the programme, they would then make specifications. When these were costed, (with import duty) and this reported back to PRRINN-MNCH, were well above the budget. (Import duty was subsequently waivered reducing the cost from £600K to £250K. However, there appeared to be some back and forth as the quantifications and specs were revised and had to be approved by state ministries. All this led to significant delays.
Local suppliers do not carry stock and have to import. At least one supplier reneged on his contract.
Clearly lessons were learned, and it would appear that while unfortunate for the programme, CA had some valid reasons for the delays. In addition, CA reported that they had no knowledge of the programme budget (or with other programmes) and this meant that they had no idea of the spending parameters. This is now being resolved in DFID.
It is also clear from discussion with Society for Family Health, that it is important to over-estimate the waiver to allow for unexpected items. (They have not experienced problems in procurement and import and indeed have adequate allowance to import on behalf of others when urgently requested e.g. bednets for SUNMAP).
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 51 304298/ Final
7.2 DFID-funded state partners
7.2.1 Governance programmes
The PRRINN-MNCH programme has been aware for several years of the need to increase the resources available for strengthening the governance component. As such, discussions with DFID led to the request for involvement of the SPARC and SAVI programmes in the three states they were currently not operational in: Katsina, Yobe and Zamfara.
SPARC and SAVI have been engaged in the three states since middle 2011 and have established offices and employed staff and conducted baseline assessments. The assessments have been shared with the PRRINN-MNCH programme and a joint planning process is envisaged for early 2012. PRRINN-MNCH participated in the recruitment of SAVI‟s key staff for the three states.
The work between SPARC and PRRINN is largely working well and complements the macro (wider state governance) and specific improvement within the sector for a specific purpose. There is good synergy between what SPARC and PRRINN want to achieve. SPARC can therefore help with experience, expertise, knowledge management, and lesson learning for the sector.
SPARC sees their role of working alongside PRRINN-MNCH, particularly on MTSS on the health sector, to use health as the entry point into government reform, and to build greater awareness on the importance of reform. SPARC has used its tools, public sector management and diagnostic tools.
7.2.2 Health programmes
Details of all current health-related programmes funded by DFID in Nigeria are found at Annex 7.
Key health partners funded by DFID are PATHS2 and Evidence for Action (E4A) as follows:
PATHS2 Jigawa: PATHS2 covers the MNCH activities in Jigawa and interventions in a number of other areas which appear to overlap with PRRIN.. These areas of work include the strengthening of:
State-level Coordination Mechanisms (SIACC)
Planning and linkages with National level Health Management Information System
Human Resource for Health (HRH), Health Financing and Public Private Partnership Management of Sustainable Pro-poor Drugs Supply System and Supply Chain management.
Capacity of service providers (Public & Private)
Referral system
Safe Motherhood Initiative (SMI)
Implementation of Demand-Side IMNCH Services
Polio Eradication Initiative (PEI) and Supplementary Immunisation
Knowledge Management (KM)
Voice and Accountability (V&A)
Health Communications and Behaviour Change Communications (BCC)
PATHS2 support for MNCH in Jigawa takes a somewhat different approach to that of PRRINN-MNCH in the three other states. The Advanced Life Saving Skills (ALSS) training of trainers is provided by the American College of Nurses and Midwives and adapted the Federal Ministry of Health national curriculum to include focused
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 52 304298/ Final
antenatal care (FANC). In Jigawa, PATHS2 has also provided integrated supportive supervision of Community Health Extension Workers (CHEWs) in Advanced Life Saving Skills (ALSS) and cascading the trainings to additional CHEWs in the communities.
Having two DFID-funded programmes working in the same state such as this poses various challenges in terms of ensuring harmonisation, consistency and clarity with state and local government. The efforts of FMOH to harmonise training etc. in life saving skills therefore provides a useful forum provided all organisations are in agreement on the models with some regional adaptation where needed.
Evidence for Action (E4A: E4A is funded from the Africa Regional Division in London and is a five year programme which aims to improve maternal and newborn survival in six sub-Saharan countries by focusing on using better evidence and improved advocacy and accountability E4A will target most of its efforts in Kano and Jigawa with strategic input at the federal level to focus on:
Strengthening and expanding maternal death reviews in tertiary facilities;
Assessing the potential to set up a confidential enquiry system;
Improving maternal mortality estimates through census and forums and Engaging with partners in national level MNH advocacy campaigns to improve MNH resource allocation and expenditure
It is important that the work to build capacity for knowledge management, and now maternal death audit and confidential enquiry under PRRINN-MNCH is incorporated into E4A‟s own work to avoid overlap. This need for collaboration with E4A has been recognised by PRRINN-MNCH and continued DFID coordination of partners is vitally important.
There is evidence of overlap in Jigawa with PATHS2 and in Katsina and Zamfara with the USAID-funded MCHIP (ended March 2012). By way of example, the latter developed national MNCH performance standards (199 for hospitals and 173 for PHCs), Integrated Supervision tools and HMIS systems among others. It is not clear to what extent, efforts were made to avoid unnecessary duplication, and opportunity cost and confusion for partners. Hence the strong need for government stewardship.18
Making it Happen: Maternal and Neonatal Health Human Resource Capacity Building:
This programme, in its second phase, is funded by Policy Division in 12 countries including Nigeria. It is providing the same training as already provided by Liverpool for PRRINN-MNCH. Sustainable capacity for the provision of quality emergency obstetric and newborn care within participating countries will be developed by the training of 17,025 health workers, including 1,025 national „Master Trainers‟. The PRINN-MNCH focal states can provide a useful model for the additional states to be funded under Making it Happen with additional resources from this programme to reinforce and provide continuity to activities in PRINNN-MNCH programme states when PRRINN-MNCH ends in December 2013.
18
Access to clinical and community maternal, neonatal and women‟s health (ACCESS)/Maternal and child health integrated progam (MCHIP. Evaluation. USAID. March 2012. www.mchip.net/.../MCHIP%20%20Final%20Evaluation%20Report-4...
DFID Human Development Resource Centre 53 304298/ Final
7.3 Other health partners
Because of its poor indicators, northern Nigeria has been a focus for a range of other MNCH programmes. Some of these (e.g. MCHIP [ended March 2010] and Society for Family Health) have been referred to in the narrative. In its work to strengthen the capacity of state and LGA ministries to coordinate and harmonise programmes, a starting point is to have detailed mapping of who is working where and doing what to avoid unnecessary overlap and maximise resources and expertise. The state participants attending the presentations stated the need to do this and that attribution of results cuts across various organisations and programmes. (Details of all health programmes as in November 2010 in the four focal states are found in an accompanying document.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 54 304298/ Final
8 Overall conclusions, lessons and implications for the future
The team‟s overall assessment of the programme was that it had made outstanding achievements in a very difficult environment. Exogenous factors such as delayed and inadequate supply of commodities, shortage of midwives and inadequate budgets have undermined immunisation rates and coverage of skilled birth attendance among others. Without these issues resolved, some of the end of programme targets at outcome level (mainly related to immunisation) may not be achieved. It should also be noted that the overall scoring does not reflect the significant variation in performance against targets between states.
As the programme runs into its final year, it will need to consolidate the very considerable gains made and focus on issues that can be resolved at state level:
Phasing down PRINN-MNCH support to a mentorship role should be carefully planned and implemented. Exit strategies or programme transfers with focus on sustainability should be carefully designed. This is increasingly important given the unpredictable security situation which has now meant that expatriate staff have re-located and are unlikely to be able to travel to states as before. The same will be true for external consultants.
The goal of the programme is to improve maternal, newborn and child health in northern Nigeria. If immunisation continues to be disrupted because of the supply problems, the programme can still have impact on maternal, newborn and child health by increased emphasis on the other MNCH interventions (already discussed under Option 3). The programme needs to maintain a degree of flexibility to adjust to an uncertain operating environment and incorporate any changes that might be needed to the work plans especially in the most affected states (currently Yobe and Katsina).
While there are many successes from community initiatives to increase demand and facilitate women‟s access to services, such as community conversations and engagement of traditional and religious leaders, these have not yet translated into increased skilled birth attendance (SBA) at facility level and family planning uptake. There is clearly deep-rooted resistance to facility delivery which can arguably be overcome if the manner in which the services are provided, address critical cultural priorities. Experience of other organisations suggests that PRRINN-MNCH has been overly cautious in its approach to family planning. The Planned Parenthood Federation of Nigeria has been providing FP services since the late 1950s; SFH has worked in northern Nigeria since 1993. SFH and JHPIEGO reports significant unmet need but also indicated that their organisations had adopted a careful approach initially. These organisations and others are a strong resource for PRRINN-MNCH.
The programme is highly valued by government both at national and sub-national levels, such as could be seen from limited discussion and reports. PRRINN-MNCH staff rightly argue that it takes years to shift attitudes and behaviour in the northern context. As to be expected, the hope on the part of programme partners, is for an extended programme under the same management, to ensure continuity. This is of particular importance at the LGA level which continues to be the weakest link in the chain, because of poor governance, low human capacity and major funding shortfalls among others. To get LGAs to function as they need to, if sustainable change is to occur, will require prolonged and holistic support.
The impression is that government „owns‟ the programme at state level where this is most relevant. The governance lessons already referred to under Output 2 in Zamfara and Jigawa are interesting and understanding the critical factors for success: how much (relatively) rests on political leadership and how much depends
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 55 304298/ Final
on technical capacity within government. At LGA level, it is more difficult to assess. At Federal level, with new people in place, there was no evidence from discussion that they knew the programme, which suggests a need for more public relations and dissemination of PRRINN-MNCH publications. Furthermore, it is advised that PRRINN-MNCH changes the look of its publications to better reflect the partnership with Government i.e. use of government logos and forewords etc.
Lessons learnt
The operations research outputs, policy briefs and technical updates reflect many lessons learned from the programme. Some examples of things that worked well in Katsina:
Engagement with different stakeholders outside health and reaching the top to get the message to governor and SSG helped resolved MSS, SDSS and some HR issues
Increasing the number and use of State-based facilitators for MNCH/RI/CE trainings minimise reliance on external expertise and will ensure sustainability and ownership
Use of the programme‟s training site for trainings instead of hotels proved cost effective and convenient
…… and those that didn’t work:
Strengthening the financial management system without commensurate policy level strengthening
Implementing MSP in the current framework of health system governance
Implementing staffing norms in the context of lack of available SBAs
Expecting the government to fast-track implementing accreditation recommendations under competing priorities without adequate support from the programme
Where results are exceeding expectation what does this tell us?
It is difficult to predict results accurately in four different environments and with very uncertain external factors. Arguably some of the targets are set too low – and this includes family planning.
The security situation is an unknown variable and could go either way or remain the same so its impact on results is unpredictable. If it remains the same, there is every reason to believe that the programme will continue to operate with national staff, supported at a distance by the few expatriate staff and international consultants, though attrition is inevitable (both among staff and non-indigene health workers), and distribution of supplies will be problematic. Increased used of internet to communicate data and reports is increasingly important.
Contractural changes
No contractual changes are suggested.
Changes recommended to the logframe
At this point in the programme, it is not considered necessary to make any changes to the logframe except for the wording of Output 7, which is confusing. It currently reads:
„Improved capacity of Federal Ministry level to enable States‟ routine immunisation activities‟
It is recommended that the output is changed to read:
„Improved capacity of federal institutions to enable States‟ routine immunisation activities‟
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 56 304298/ Final
9 Consolidated recommendations
Recommendations are presented below for PRRINN-MNCH under each output.
Output 1: Strengthened State and LGA governance of PHC systems geared to RI and MNCH
1.1 Continue strong emphasis on the PHCUOR and explore ways to measure health impact.
1.2 Continue/scale up debate and advocacy on approval of the Health Bill, alongside other partners especially HERFON and contribute data which might help influence a speedy outcome.
1.3 Continue to explore options for introduction of basket funding at state level with robust systems for accountability and continue to pursue the idea to pool some Free MNCH money in the same fund.
1.4 Strengthen and deepen coordination and collaboration with other partners (DFID and non DFID) to maximise investment in common areas and avoid any potential for duplication. Explore options for combined publications on lesson-learning on different issues where there is wide experience e.g. Emergency Transport Schemes (ETS)
1.5 Building capacity at LGA level is highly challenging as the base capacity is very low, finances very inadequate and attrition high. Seek out experience of different approaches used for capacity building at LGA level to see what works best.
Output 2: Improved human resource policies and practices for PHC
2.1 Continue to strengthen collaboration with the national HRH partners‟ forum
2.2 Create/sustain synergy with upcoming Women for Health Programme
2.3 Introduction of HRH LECs for closer support and implementation of planned HRH activities; develop job plans to assist STMs to monitor and appraise these LECs
2.4 Support states to train the FMOH newly approved cadre of SBA - the community midwives.
Output 3: Improved delivery of MNCH services (including RI) via the PHC system
Routine immunisation
3.1 PRRINN should continue to implement the suggestions contained in the March 2012 vaccine logistics consultant report. A focus should be on supportive supervision and training of CC&VSLM staff.
3.2 Many of the problems hindering RI delivery in Nigeria are external to PRRINN (supply problems stemming from the NPHCDA and partners) but there is still mileage in PRRINN driving vaccine logistics and management improvement at state level:
3.3 Training and supervision of service delivery staff should continue. This is especially relevant in Jigawa, which is introducing the pentavalent vaccine (need to ensure staff cease multi-dose vial policy, as was used for DPT).
3.4 Cold chain and vaccine logistics system management (CC&VSLM) issues in the PRRINN program states should continue to be addressed.
3.5 Effective CC&VSLM is a crucial component of the improving RI delivery. Many factors at the state and sub-state level contribute to CC&VSLM issues, including lack of training, lack of skills for CC&VSLM workers, and lack of supervision.
3.6 Plans should be made to update cold chain inventory database on a regular basis, and report on stock to zonal CC&VSLM officials and/or the NPHCDA.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 57 304298/ Final
Output 3: Improved delivery of MNCH services (including RI) via the PHC system
3.7 Ongoing strengthening of planned preventive maintenance for cold chain equipment should continue.
3.8 PRRINN should advocate that any new cold chain equipment procured at the state level be certified vaccination equipment
3.9 Waste disposal is an area which requires additional attention and assessment. Training should continue
3.10 Continue to support programme states to draw on GAVI funds (e.g. ISS funds). Work with states facilitate the states receiving these funds from the NPHCDA.
Maternal health
3.11 Ensure support and supervision of newly qualified midwives (including MSS) and those having received classroom-based LSS training.
3.12 The 2011 MTR recommendations on FP still stand and action points recommended from the 2011 household survey are appropriate but too general and not new.
19 The
evidence on FP and spacing) in reducing maternal
3.13 Compare experience with other programmes on a range of issues where challenges have arisen such as Emergency Transport schemes and compensation
3.14 There are many different LSS tools being used. PRRINN-MNCH should continue to contribute to the (PATHS2-supported) LSS harmonising project led by the FMOH and first attended by LSTM.
3.15 There were delays in procurement and therefore supply of equipment and essential medicines through the Crown Agent‟s contract. The situation is now improving with better quantification and communication among others. Since the states will not, in the long term be procuring through the Crown Agents, it is vitally important that state capacity for transparent and effective procurement is built without delay.
3.16 There is evidence that removing fees for facility delivery increases use of facilities but also that out-of-pocket expenses are still required. It will be useful to track these trends through OR.
Newborn health
3.17 Reinforcing IMCI and growth monitoring at PHC facility level is important alongside routine immunisation. Adherence to treatment protocols needs consistent monitoring.
Public Private Partnerships
3.18 SFH reports that they have 60 distributors throughout the country that could easily transport commodities. PRRINN-MNCH might explore ways with other programmes and partners to assist with distribution of essential commodities.
Output 4: Operations research providing evidence for PHC stewardship, RI and MNCH policy and planning, service delivery, and effective demand creation
4.1 It would be useful to see summary reports for each area (Performance Based Financing (PBF), Emergency Transport Support (ETS) and Community Based Service Delivery (CBSD). These summaries could usefully draw out lessons learnt from the studies, comparing the different models and which ones worked best and why.
4.2 Close collaboration with the University of Sokoto such as a joint paper with the HDSS research centre on the next set of data as part of the hand over process will help
19
PRRINN-MNCH FACT SHEET: Women‟s awareness and use of FP : Findings from the 2011 Midterm Household Survey.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 58 304298/ Final
establish this type of work for the university to conduct in the future.
4.3 The Annual Report 2011 reported on data coming out of the mid-term household survey. It would be useful to have some more commentary when presenting the analysis of this data within the report. This is especially important when anomalies in the data exist that might require further explanation.
4.4 A further recommendation on the HDSS site is to continue to seek membership of the INDEPTH network. This network can provide a good way to connect with other HDSS sites and share learning and best practice which can support the development of the Zamfara site.
4.5 It would be useful to explore establishing a research component to this programme. This could be qualitative in nature - understanding perceptions and barriers before, during and after the groups are implemented.
4.6 The OR team is encouraged to share their findings on PBF from the PRRINN-MNCH programme with the World Bank to encourage lesson learning and debate. This would also be a good opportunity to push dissemination of OR findings into the international forum.
4.7 Developing a narrative on OR across the life of the PRRINN-MNCH programme would be a useful end document for the OR component. This way the findings and lessons learnt across all the research conducted will enable detailed evidence based approaches to the design and implementation of future programmes.
4.8 It would be useful to know how PRRINN-MNCH‟s experience compares with that of ACCESS/MCHIP in the same states in various areas including Kangaroo Mother Care where similar challenges have been highlighted.
Output 5:
Improved information generation with knowledge being used in policy and practice
5.1 It is rightly stated in PRRINN documentation, that the government must own the programme and the products because it is hoped that the government will use the documents (especially guidelines and protocols) beyond the life of the programme. It is therefore most important that the documentation shows the government logos to reflect this ownership. Donor logos should not be prominent.
5.2 PRRINN-MNCH produces excellent reports on the clusters. Does the state produce equally detailed reports?
5.3 There is need for close collaboration with Evidence for Action (E4A) – the DFID funded regional programme and the Centre for Research in Reproductive Health National data system on Maternal Death Audit to avoid any duplication of efforts.
Output 6: Increased demand for RI and MNCH services
Routine immunisation
6.1 Continue to leverage demand data from HMIS, and evidence from PRRINN experience in field, to work with communities to generate demand for RI and MNCH services.
6.2 Continue work on vaccine supply (see Output 7) and health worker training (see Output 3), as a reliable supply of vaccines and respectful health workers are crucial components to sustain demand for services.
6.3 PRRINN should continue to work on establishing/implementing strategies to ensure community engagement work is sustainable and continues to address key barriers to uptake e.g. date of vaccination, religious objections etc.
6.4 In Jigawa state, incorporate pentavalent and PCV vaccines into RI CE materials (with a goal of eventually incorporating new vaccines into all program state materials).
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 59 304298/ Final
6.6 Continue targeted CE activities to most at risk populations (e.g. younger women, marginalised women).
6.7 Continue to engage with LGA political and technical leadership to ensure funding for community engagement (CE) for RI and MNCH.
MNCH
6.10 Various organisations and projects have used an ETS for transferring women in labour and arguably have different experiences which could be compared and shared as a way of finding best solutions to tackle some of the emerging challenges arising such as demand for payment etc. If one organisation has a different kind of arrangement with the union, this could undermine that of PRRINN-MNCH.
6.11 Also discussed under output 3, there still appears to be a degree of caution around FP which has been provided in northern states for more than 50 years (e.g. Planned Parenthood Federation of Nigeria) .
20 The programme can draw on the experience of
such organisations in strengthening FP. Study tours for Imams helped to reduce stigma and misconceptions around immunisation, so perhaps the same can be tried for family planning.
20
Planned Parenthood Federation of Nigeria since the 1950s, and since 1993 by Society for Family Health
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 60 304298/ Final
Output 7: Improved capacity of Federal Ministry level to enable States’ routine immunisation activities
7.1 More advocacy at the level of the FMOH is needed where knowledge of the programme (in Family Health Division) was lacking. While PRRINN-MNCH collaborates mainly with the NPHCDA, if the most significant constraints to the programme‟s progress are to be overcome, advocacy at the level of the FMOH is needed and PRRINN-MNCH needs to make even more effective use of its excellent documentation and data.
7.2 PRRINN and DFID should identify GAVI consultants to ensure they are held to account and clear on their remits within states.
7.3 Continue to support NPHCDA with immunisation data collection activities in states.
7.4 Where possible, codify insights on RI delivery at the community level for incorporation into NPHCDA plans. PRRINN insight/evidence from the field can inform policy and program design at the federal level (data on wastage rates in all four states, and penta uptake in Jigawa would be especially useful).
7.5 If possible, PRRINN should continue to use federal immunisation stakeholder fora (e.g. the Core Group) to monitor the vaccine logistics situation and press for corrections, where needed.
7.6 PRRINN-MNCH needs to reinforce and update its relationships with the FMOH and communicating programme success stories. Collaboration with other DFID-funded programmes, notably SAVI and PATHS2 for Federal influencing and informing is important to ensure that consistent messages are being provided with the support of UK funds.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 61 304298 / Final
Annex 1: PRINN-MNCH combined logframe 2009-2012
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 62 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 63 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 64 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 65 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 66 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 67 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 68 304298 / Final
x
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 69 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 70 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 71 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 72 304298 / Final
Annex 2: Updated risk assessment
Risk
Category
Comments and Mitigation Strategy
Update and comments: Annual Review 2011
a) Federal Govt does not supply to States all required vaccines, syringes and safety boxes.
Impact: High Probability: High (from medium) Unchanged
Presidential and Ministerial commitment to RI at Federal level and a sound UNICEF managed procurement mechanism were deemed sufficient to mitigate this risk at approval. The Programme Memorandum committed PRRINN to undertake operational research with UNICEF on the acquisition, supply and reporting mechanisms. The system appears to be working. And there have been improvements in vaccine availability in the states compared with last year. Unfortunately the Government has precipitously introduced a policy on using auto-destruct syringes which are not yet fully available which may add another risk. Mitigation PRRINN (and donor groups) should advocate at Federal level for bundling of injection material for immunisation, and for emergency supplies to be additional. Donors to advocate for UNICEF to retain procurement responsibility. Donors to advocate for a delay in implementation of the policy on auto-destruct syringes.
Currently procurement at the national level is still a major risk to the PRRINN programme. As of end of April 2012, nationally:
3 states were stocked out of measles vaccine; 9 states were stocked out of yellow fever vaccine; 1 state was stocked out of BCG vaccine; 12 states were stocked out of Hepatitis B vaccine; 11 states were stocked out of DPT vaccine; 4 states were stocked out of AD 0.5 ml syringes; 7 states were stocked out of 5 ml reconstitution syringes; 24 states were stocked out of BCG syringes; 5 states were stocked out of injection material safety boxes.
For PRRINN states:
Yobe was stocked out of measles vaccine
Yobe was stocked out of yellow fever vaccine, and all other PRRINN states had <4 weeks supply
Yobe was stocked out of HBV, and Jigawa and Katsina had <4 weeks supply
Jigawa was stocked out of DPT and Yobe and Katsina had <4 weeks supply
Yobe and Katsina had <4 weeks AD syringes
Yobe, Katsina, Jigawa were stocked out of BCGH syringes, and Zamfara had <4weeks supply
Jigawa was stocked out of 5 ml reconstitution syringes and Yobe had <4 weeks supply
Jigawa had <4 weeks supply of vaccine injection safety boxes
NPHCDA leadership has committed to address procurement issues for immunisation commodities. However, as of July 6 2012, there are no AD 0.5 ml syringes in stock at the national level. This means the Q3 distribution has not happened, and
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 73 304298 / Final
Risk
Category
Comments and Mitigation Strategy
Update and comments: Annual Review 2011
states are at risk of stocking-out Bundling of injection material is crucial. Currently, the government procures syringes domestically, and does not bundle them with vaccines. This is a major risk for immunisation.
Ensuring UNICEF retains procurement responsibility is also important, though donors need to ensure NPHCDA pays for commodities. UNICEF doesn‟t do anything if NPHCDA doesn‟t transfer funds for cost estimates for commodities.
b) PHC services do not get delivered.
Impact: High, Probability: High Unchanged
Uptake of RI constrained by the absence or poor quality of services available from PHC facilities. There has been little improvement since last year although some evidence of progress e.g. the use of mobile clinics in Katsina, and some increase in resources being put to PHC by the States and LGAs Mitigation: The UK Norway MNCH programme will provide additional support to strengthen PHC.
Uptake of RI is also constrained by absence of properly trained health workers
c) Negative impact of PEI and measles campaigns
Impact: High Probability: High Unchanged
The distorting effect of IPDs in the Nigerian immunisation system is acknowledged by all stakeholders (including WHO and UNICEF) to be preventing improvement of RI and wider PHC reform. IPDs absorb excessive resources and create a monetisation of incentives for patients and Government/donor IPD staff. This has meant little pressure for change. The Federally initiated Task Force established to look at ways of transiting to a more sustainable RI programme delivered through the PHC system has not delivered.
Training and supportive supervision of health care workers will be an important aspect here. Also, accountability is needed in the system to ensure funds for these activities are properly used. What is the result of the review? How has this guided resource allocation to ensure there are adequate funds for RI? Has this targeting of polio eradication been achieved?
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 74 304298 / Final
Risk
Category
Comments and Mitigation Strategy
Update and comments: Annual Review 2011
Mitigation: The issue cannot be tackled by PRRINN alone: there are high level political and international dimensions. DFID HQ and DFIDN will continue to work with PRRINN, PATHS2 and donors to gather strong evidence on the strengths, impact and opportunity cost of IPDs. A review is being carried out now in order to guide a new strategy for polio eradication. PRRINN/MNCH Yobe will simultaneously work with WHO and the SMoH to develop a proposal for focusing IPD activities in Polio hotspots only, whilst strengthening PHC and RI in other LGAs.
d) Incorrect storage and use of vaccines
Impact: High Probability: Low Unchanged
There have been improvements in the storage and use of vaccines. Cold chain has improved at State level although there is more work to be done at LGA level. Training has been given to all cold chain managers in the States. A solar fridge engineer was trained by PRRINN and went to install solar fridges purchased by the State. There has been more money put into transport of vaccines by some LGAs.
Mitigation: PRRINN will continue to focus on rehabilitation of solar fridges and maintenance at LGA level.
Need ongoing training and supervision at state and especially at LGA level because of rotation of staff out of cold chain. Cold chain is still a major problem, as highlighted by the PRRINN logistics review conducted by Kashem Prasad. Need to ensure that WHO PQS cold storage equipment is purchased by states that plan to buy their own equipment (e.g. Katsina). Also, for generators for LGA cold stores, need to ensure money is available to purchase petrol.
e) Communities and households do not take up RI
Impact: High Probability: Medium Unchanged
There are a range of demand side factors affecting communities‟ ability and willingness to utilise services, including culture, mistrust, lack of knowledge and information, cost, etc. Work this year has shown a significant increase in uptake of first vaccinations in pilot communities.
Mitigation: PRRINN will work with MNCH and other partners to scale up proved strategies and will continue to collect evidence of what works.
PRRINN needs to ensure funds for social mobilisation are used properly by state and LGA officials.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 75 304298 / Final
Risk
Category
Comments and Mitigation Strategy
Update and comments: Annual Review 2011
f) Lack of State and LGA commitment to RI and subsequent inadequate or mismanaged financial allocations.
Impact: High, Probability: Medium Unchanged
There has been small-scale but significant increases in commitments by both States and LGAs to RI and PHC. Mitigation: PRRINN will continue to work with Ministries of Budget and Planning as well as line Ministries to increase budgetary allocations. DFID will continue advocacy at a higher level.
The Governors‟ forum would be a good place for this advocacy.
g) Failure to develop and sustain effective data management systems
Impact: Medium, Probability: Medium Unchanged
Lack of data is a key issue in analysing and monitoring the programme although it is still possible to revive routine immunisation without it. HMIS data remains of dubious quality in all States. Collection is inconsistent, in part due to poor management at the facility level and the low priority SMoHs appear to give data. SMoHs and SMoLGs do not appear to appreciate the value of good data or know how it can be utilised for both planning and impact monitoring Mitigation: Development of sound, shared data is a priority within PRRINN/MNCH‟s workplan. PRRINN/MNCH will work with other donors to establish more effective HMIS systems that provide district level data that can be used by all stakeholders. The programme will support capacity building within State Governments for analysis and planning.
Standardised data tools not yet distributed within states or reprinted. Lack of staff training on data collection remain issues of concern. Both training and supervision are still needed.
h) Lack of PRRINN linkages to central strategic planning and resource allocation initiatives (SEEDS, PMF etc).
Impact: Medium Probability: Medium Probability: changed to low
Inclusion of PHC reform and RI in SEEDS 2 is critical to securing political commitment, budget allocations and effective M&E. Links are not effectively made at present, except in Jigawa & Zamfara where they could be deepened.
Collaboration on reform at a strategic level with SAVI and SPARC has been strengthened in three states and in Jigawa. Close collaboration with PATHS1 on governance essential. CSOs at the local level could be encouraged to press for more accountability with the health system in their respective
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 76 304298 / Final
Risk
Category
Comments and Mitigation Strategy
Update and comments: Annual Review 2011
Mitigation: PRRINN/MNCH will continue its broader engagement, as it has done in Zamfara. However there will be other networks, including civil society and private sector that should be investigated. PRRINN needs to cast its net widely.
areas (e.g. mothers groups demanding more training be done for health workers)
i) Gunduma system in Jigawa fails. PHCDA system in Yobe fails.
Impact: Medium, Probability: Medium Unchanged
The Gunduma system in Jigawa and the proposed PHCDA in Yobe have enormous potential to secure adequate funding, effective delivery and effective supervision at health facilities. However they will be contested by stakeholders whose power and influence will be eroded under the new system. These systems are likely to be compromised if insufficient staff members are available at facility level to make the systems work.
Mitigation PRRINN/MNCH and PATHS2 (in Jigawa) will work with other donors to support the implementation of Gunduma and PHCDA, and to help Jigawa and Yobe State Governments measure and communicate the positive impact of these systems.
k) Ineffective Federal MoH
Impact: Medium Probability: Medium Unchanged
Relationships and lines of responsibility across the Federal MoH and parastatals (e.g. NPHCDA) have been unclear. The lack of a substantive Minister of Health and a new task force on polio exacerbated this. However there is a new Minister and a new head of the National Primary Health Care Agency who are working well together and bring new possibilities. Mitigation PRRINN, PATHS 2 and DFID, will continue to work to support the new leaders in order address these structural and organisational issues. The new Health Bill will help when passed.
Experience thus far suggests that neither the new Minister of Health nor the new ED of the NPHCDA are reform activists. There is still a risk that these leaders will focus disproportionately on polio eradication. Donors still rely on the State Minister for Health (ex ED/NPHCDA) to get things done but it is risky to rely on individuals who work within large (unreformed) public sector institutions. After 7 years, the Health Bill is still not passed though some (useful) amendments may be incorporated before it becomes law. Further collaboration with SPARC and SAVI, HERFON (and others) needed with like-minded NGOs and DFID-funded programmes including Evidence for Action
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 77 304298 / Final
Risk
Category
Comments and Mitigation Strategy
Update and comments: Annual Review 2011
(E4A) which has global advocacy expertise. This is needed to address the critical issues of vaccine and commodity shortage and to hold the GoN to account on their commitments to family planning at the July 2012 London Summit. .
l) Political and civil instability
Impact: High Probability: High Changed
Remains a risk outside of PRRINN‟s control. Mitigation includes building capacity to sustain workplans without close PRRINN presence or oversight.
This situation still holds true but is worse than previously affecting in particular, Yobe and Zamfara. The probability has been changed from low to high. The insecurity has already affected access by (expatriate) staff to states and the field and is likely to affect community work (especially for meetings) and distribution of medicines. While many MSS midwives left during the worst of the riots, some have returned but they cannot be expected to stay when there are threats.
Increasingly important for PRRINN-MNCH to phase down external support enabling nationals to support the programme at state and LGA level and give extra effort to building capacity – „hands off‟.
m) Insufficient or inadequately trained staff at PHC facilities New risk (2011)
Impact: High Probability: Medium Unchanged
PHC are often inadequately staffed, or staffed by health workers with insufficient training to safely perform the range of functions that facilities should provide. There are particular shortages of trained midwives and unrealistic qualifications are demanded for entry into health training institutions. An embargo on health personnel recruitment in Yobe further complicates the issue . Mitigation PRRINN/MNCH is undertaking HR Audits and will support the development of practical HR policies and strategies. This will include recommendations on training and HR development requirements.
Staffing continues to be a challenge and attrition of MSS midwives created gaps though some are coming back. Incentives have helped retention but created a drain on budgets. PRRINN-MNCH supported HR audits have revealed ghost workers and new IT systems will help ministries with HR. Also, cold chain and logistics vaccine infrastructure also inadequately staffed.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 78 304298 / Final
Risk
Category
Comments and Mitigation Strategy
Update and comments: Annual Review 2011
n) Ineffective donor coordination New risk (2011)
Impact: Medium Probability: Medium Unchanged
Donor coordination structures, especially in Yobe where there is no SIACC, remain sub-optimal. The inability of donors to present a united front to Government lessons traction and influence. WHO and donors involved in IPDs continue to give insufficient priority to coordination. Mitigation PRRINN/MNCH will continue to prioritise this and seek to secure effective partner coordination and engagement. In Yobe, working with other donors, the programme will advocate with the new Governor for an SIACC, with a broad (i.e. not just IPD) remit. DFID will work at Federal levels to ensure central directives don‟t undermine coordination at State level.
National Planning Commission (NPC) not using mandate for coordination. Is health donor mapping kept updated and who does this? SIACCs at state level now functional but yet to see how effective and leading to harmonisation. Evidence of duplication in various areas. PRRINN-MNCH can help states with mapping. PRRINN-MNCH can also do more to collaborate. Nigeria, including PRRINN states would benefit from a national roadmap on immunisation, laying out responsibilities of each partner.
o) Lack of Government ownership of PRRINN-MNCH programme and capacity to sustain systems after December 2013 New risk (2012)
Impact: High Probability: Medium
Mitigation (2012) As PRRINN-MNCH phases down, and hands over tasks still performed by PRRINN-MNCH staff ownership and capacity will increase. All future publications should reflect the partnership with GoN.
PRRINN-MNCH has worked hard to expand the programme coverage. As with all similar programmes, there is more motivation (on GoN‟s part) to do the job when there are incentives (and funding) from the programme. Much of the literature is PRRINN-MNCH „branded‟. GoN at national and sub-national levels need to fully „own‟ and manage the programme interventions and new tools and systems, and these need to carry the GoN „brand‟.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 79 304298 / Final
Annex 3: Follow up on midterm review recommendations
PRRINN-MNCH presented follow up to the MTR recommendations in their presentations. The following are found in the 2011 Annual Report: Output 1
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 80 304298 / Final
Output 2
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 81 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 82 304298 / Final
Output 3
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 83 304298 / Final
Output 3/continued
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 84 304298 / Final
Output 3/continued
Output 4
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 85 304298 / Final
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 86 304298 / Final
Output 5
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 87 304298 / Final
Output 6
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 88 304298 / Final
Output 6 continued
Output 7
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 89 304298 / Final
Annex 4: Challenges in the vaccine supply chain
Overview of challenges in the vaccine supply chain and logistics system Nigeria faces a number of chronic systemic challenges with logistics and supply chain management of immunisation commodities (vaccines, injection materials, paper data collection files). These persistent challenges contribute to the low level of routine immunisation coverage in country and, until resolved, will prevent Nigeria from attaining desired levels of immunisation coverage. Specific logistics and supply chain management challenges facing the immunisation system in Nigeria include:
1. Stock-outs of vaccines and injection materials.
2. Non-availability of documents for vaccine management and record keeping, and poor
record keeping practices.
3. Insufficient cold storage capacity and use of non-WHO PQS cold storage equipment.
4. Insufficient electrical power (e.g. lack of generators or funds to fuel generators) for
non-solar cold storage equipment.
5. Lack of preventative maintenance and repair for cold chain equipment and related
generators.
6. Inefficient distribution of vaccines and other immunisation commodities, and lack of
funds for distribution.
7. Insufficient technical knowledge and skills for cold chain officers and cold chain
supervisors, and related lack of training and supportive supervision for cold chain
personnel.
8. Inadequate physical storage space for vaccines.
Plans to address the majority of these challenges exist, but they are often either not implemented or not implemented effectively. Additionally, financial and human resources deployed in this system are often misallocated. This suggests that the majority of the above challenges stem from insufficient accountability in the immunisation space in Nigeria, at all levels, rather than a requirement to develop new strategies or secure additional resources. To improve immunisation coverage, persons responsible for immunisation commodity supply chain and logistics need to be held accountable, in a transparent manner, for appropriately deploying resources and implementing strategies. Below, more information is provided about each of the problems listed above. Also provided are some suggestions on how increasing accountability will help address these challenges.
1. Stock-outs of vaccines and injection materials
In 2011, Nigeria stocked out of several vaccines used for routine immunisation of infants, including DPT and BCG vaccines. These stock-outs were caused by several factors, including the diversion of funds intended for RI vaccines to support campaign vaccines and funding delays caused by the 2011 election. In 2012, stock-outs persist in the system. In April 2012, the most recent time for which data are available, stock-outs remained a major issue. According to data from the NPHCDA, in April 2012:
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 90 304298 / Final
One state was stocked out of BCG vaccine.
Three states were stocked out of measles vaccine.
Nine states were stocked out of yellow fever vaccine.
Twelve states were stocked out of Hepatitis B vaccine.
Eleven states were stocked out of DPT vaccine.
Four states were stocked out of AD 0.5 ml syringes.
Seven states were stocked out of 5 ml reconstitution syringes.
Twenty-four states were stocked out of BCG syringes.
Five states were stocked out of injection material safety boxes.
As stated above, these stock outs are primarily due to delays in the release of funds and poor management of immunisation funding in Nigeria. The leadership of the NPHCDA has committed to resolve these issues, following the significant decrease in national DPT coverage rates caused by the 2011 stock-out. To support the NPHCDA to better manage vaccine financing, the NPHCDA Finance and Accounts Department leadership is developing a tool to track payments for immunisation commodities. It is expected that this tool, coupled with the NPHCDA leadership‟s emphasis on timely payment for vaccines, will help address stock-outs of vaccines in Nigeria. The tool will promote accountability and transparency in the system by showing all stakeholders in the immunisation commodity space who is accountable for what action (e.g. releasing a payment for an order or developing a cost estimate), and also clearly showing what payments are due to whom and when. Ideally, this will ensure payments for vaccines and other commodities are made on time, and thus reduce stock-outs. The proposed RI Strategy and Accountability Framework will further promote accountability with regards to immunisation financing and procurement by clearly listing what stakeholders have what responsibilities for financing and procurement, and by developing a series of “carrots and sticks” to hold these stakeholders accountable for delivering against these responsibilities.
Non-availability of documents for vaccine management and record keeping and poor record keeping practices
A DFID funded March 2012 review of the vaccine cold chain in northern Nigeria found that standardised documents for record keeping (e.g. temperature, requisition, stock, wastage) were lacking at different levels of the immunisation supply chain. This review also found that vaccine logistics staff (e.g. state and LGA cold chain officers and other vaccine logistics staff) had insufficient knowledge and/or willingness to comply with proper record keeping practices. Supervisors did not have sufficient knowledge and/or ability to ensure that their sub-ordinates were correctly maintaining vaccine management records. Similarly, the 2011 Effective Vaccine Management (EVM) report, which surveyed a collection of state and LGA cold stores and health facilities, found that 65% of the health facilities visited did not have a formal recording system for supplies (no standardised requisition/issue/receipt vouchers). Sites are either not receiving these record tools, or are receiving them but are not properly using them. The NPHCDA does, with the assistance of WHO and UNICEF, produce and distribute standardised vaccine management tools. And, following the introduction of pentavalent vaccine in Q2 2012, a new updated set of these tools was produced and is being distributed to pentavalent phase one introduction states. The fact that sites are not using these tools suggests that greater emphasis needs to be placed on ensuring correct tool distribution,
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 91 304298 / Final
training vaccines logistics workers in use of the tools, and supportive supervision to ensure the tools are used correctly. All tools should be provided in sufficient quantities to all LGAs and states. And states and LGAs should be held accountable for distributing the relevant tools to health facilities and, if needed, for printing more tools. Increasing accountability in the system will ensure that resources deployed to support training and supervision for data collection will be properly utilized. Additionally, increased accountability in the system has the potential to hold all parties accountable for maintaining records, as directed by existing protocols.
Insufficient cold storage capacity and use of non-WHO PQS cold storage equipment
The cold chain in Nigeria has storage capacity challenges. These challenges are particularly acute at the health facility level. Additionally, the use of non-WHO PQS cold storage equipment is common across the system. According to an assessment of the cold chain conducted in 17 states in Q3 2011, 44% of the 1,572 sites surveyed did not have capacity to accommodate the PCV10 vaccine in WHO PQS cold storage equipment, in addition to the vaccines used in the current routine immunisation schedule. Following potential repairs of 80% of non-functional cold storage equipment, 20% of sites would still have insufficient capacity for PCV10. There is also a significant amount of non-PQS cold storage equipment in the immunisation system. While the Nigeria National Immunisation Policy requires PQS equipment to be purchased and used for vaccine storage, these guidelines are not regularly enforced. According to a March 2012 study, 24% (2,562 pieces) of cold chain in Nigeria was non-PQS equipment. The majority of this equipment was door-open type domestic refrigerators, which have variable temperatures and poor insulating capacity following power outages (common in Nigeria). Use of non-PQS equipment is particularly common at the lower levels of the supply chain, where this equipment is often purchased on the local market. This use of non-WHO PQS represents a risk to vaccine security, as it increases the risk vaccines will undergo heat exposure. Significant funding has been committed to Nigeria to procure additional cold storage equipment address these gaps in storage capacity. Much of this funding has been committed to UNICEF, to procure cold storage equipment for Nigeria. However, measures will need to be put in place to ensure that appropriate equipment is purchased and this equipment is effectively and efficiently distributed across Nigeria. One good first step is ensuring that UNICEF be the organization to procure cold chain equipment in Nigeria using GAVI funds. This is because UNICEF will procure WHO PQS equipment, while governments may not (in past years, the Federal Ministry of Health has procured a number of non-PQS refrigerators for the NPHCDA). In addition to this, appropriate supervision and accountability is needed in Nigeria to ensure the correct type of cold storage equipment is purchased, in accordance with the national guidelines. States do procure their own vaccine cold chain equipment (e.g. Katsina state currently plans to purchase several hundred cold storage refrigerators). Ideally, a system should be put in place to ensure that when this equipment is purchased, it is done so in a transparent manner and the selected equipment is of the acceptable WHO PQS standard. Additionally, health decision makers should be held accountable for distributing purchased equipment in an effective manner.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 92 304298 / Final
Insufficient electrical power (e.g. lack of generators or funds to fuel generators) for non-solar cold storage equipment
In Nigeria, access to reliable electrical power and functional generators to power electrical (i.e. non solar) cold storage equipment are major issues. According to the Q3 2011 cold chain assessment, in the 17 states surveyed over 80% of sites that required electricity for cold chain storage (i.e. that use electrical, rather than solar, refrigerators) had access to less than eight hours of electrical power from the grid per day. Additionally, 45% of sites that used electrical equipment did not have a generator and many sites with generators do not have funds to purchase generator fuel or misallocate funds intended for generator fuel. Similar findings were reported in the 2011 EVM study, which found that 48% of LGA stores do not have generators. Additionally, according to the EVM, 50% of the available generators at the LGA level are inadequate and/or not in good working condition. Finally, anecdotal evidence reported by senior NPHCDA immunisation personnel suggests that some funds, sent to some LGA stores that have generators and meant to purchase fuel and fund preventative maintenance for those generators, is misallocated. A robust system of transparency, accountability, and supervision is required to ensure that funds allocated for generator fuel and maintenance and repair are used for their intended purpose. State and LGA decision-makers must be held accountable to budget for activities required for sufficient electricity at their sites, to carry these activities out, and to properly utilize the funds intended for these activities. This system of accountability will also be needed to ensure that those vaccine storage sites that do not adopt solar powered equipment will be provided appropriate generators.
Lack of preventative maintenance and repair for cold chain equipment and related generators
Preventative maintenance is not routinely carried out for cold chain equipment and related generators. Additionally, a large number of cold chain equipment units are non-functional and are not repaired in a timely manner. According to the 2011 EVM study, only 68% of refrigerators and freezers in sites surveyed were operational at the time of assessment. Similarly, the Q3 2011 cold chain assessment assessed almost 2,800 refrigerators at the state, LGA, and health facility levels in 17 states. Of these, only 59% (1,635) were functional. Compounding the problem, much non-functional cold chain equipment is not repaired in a timely manner, largely due to lack of training and misallocation of resources needed for repairs. According to the Q3 2011 cold chain assessment, 71% of non-functional cold chain equipment (993 units) had been non-functional for six months or longer. 62% of equipment (876 units) was reported to have been non-functional for greater than 12 months. This suggests that repairs are not regularly conducted when they are needed. One of the major contributing factors to the lack of maintenance for cold chain equipment and generators is the current lack of a national maintenance and repair guideline for Nigeria. Because of the lack of a national guideline, repairs are conducted in an ad hoc manner, or not at all. To address this issue, Nigeria should produce national cold chain equipment repair and maintenance guidelines, and these guidelines should include a set of standard operating procedures for facilities to use with respect to cold chain equipment and generator repair and maintenance. Additionally, the guidelines should include provisions to ensure repairs and maintenance activities are appropriately documented and supervised. Also, as stated in the
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 93 304298 / Final
previous section, cold chain personnel should be held accountable for correctly utilizing funds for repairs and for ensuring that repairs are conducted in a timely manner.
Inefficient distribution of vaccines and other immunisation commodities, and lack of funds for distribution
Vaccines should be distributed regularly based on need of sites. However, currently in Nigeria vaccines are distributed according to availability of the vaccine, rather than the need of sites. State and LGA stores will push what they have in stock down the chain, not what is needed by the lower levels. This contributes to vaccine stock-outs, and is a sign that rational data driven vaccine distribution plans are either not made or not implemented. Transporting vaccines from site to site is also an issue. According to the 2011 EVM study, 81% of the facilities do not provide reliable and sufficient transport to locations where vaccines and consumables are utilized. According to the 2011 Q3 cold chain assessment, in the 17 states assessed 67% of surveyed sites have no transportation equipment. And for sites with transport equipment, only 58% of this equipment is functional. To address these issues, vaccine logistics personnel need to be held accountable for developing vaccine distribution plans and for correctly implementing these plans. Also, decision-makers need to be held accountable for allocating funds for distribution and transport, and for appropriately maintaining transportation equipment. Consequences for non-performance in these areas should be developed. If needed, the NPHCDA and partners should provide states with technical assistance to develop and distribute proper vaccine distribution plans.
Insufficient technical knowledge and skills for cold chain officers and cold chain supervisors, and related lack of training and supportive supervision for cold chain personnel
A March 2012 assessment of the technical skills of state and LGA cold chain officers found these personnel had a low level of technical knowledge pertaining to cold chain and vaccine handling and logistics. Specifically, the study found that personnel demonstrated an inadequate knowledge of core vaccine handling and logistics practices such as:
Ice pack conditioning.
Vaccine volume and storage space calculation.
Record keeping (including cold chain temperature data collection) and use of
existing record keeping templates.
Vaccine requisition and buffer stock calculation.
The 2011 EVM found similar issues. For example, according to the EVM study, 68% of surveyed LGA level cold stores did not conduct regular physical inventory of stocks and less than 50% of LGA cold stores assessed had forecast their annual needs for vaccine and consumables using nationally approved methods. This suggests that these sites either had personnel who were not trained to do these activities, or were insufficiently supervised to ensure they carried the activities out. Training is also an issue for vaccine supply chain management. State Immunisation Officers (SIOs) have not been able to provide CHAI much detailed information about trainings at the state level. Observations suggest that there does not appear to be systematic trainings for vaccine logistics scheduled or extensive training plans in place (though the WHO is currently working with CHAI to plan a vaccine logistics training for H2 2012). Many SIOs have indicated they rely on the support from WHO and UNICEF to conduct trainings, and do not conduct significant domestically funded training activities. Currently, ongoing training of EPI staff and health workers on vaccine logistics, when it does occur, occurs primarily on an ad hoc basis. There are also reports from personnel in the
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 94 304298 / Final
system that the funding they receive is not sufficient to conduct trainings frequently. One SIO also mentioned to CHAI the challenges of regularly needing to re-train staff, due to the high turnover of staff and the transfer of staff to other posts and LGAs. Supportive supervision is also weak at the LGA and HF levels. One SIO reported that, in their state, the LGA officers do not visit the HFs in their respective wards at all. Another SIO stated that supervision should be occurring once per month, but other activities have been prioritized and capacity is strained. A lack of funding dedicated to supportive supervision was cited as a major barrier. Hands-on training for relevant vaccine supply chain workers (with a focus on cold chain and vaccine handling) is required. Also required is regular supportive supervision. Together, these will be crucial activities to increase performance of vaccine logistics and cold chain staff. Key to achieving these regular training and supervision will be holding state and LGA vaccine program officials accountable for budgeting and utilizing funds for these activities, with a focus on creating an effective structure of supervisors and trainers at the state, LGA, and health facility level.
Inadequate physical storage space
Many of the physical sites used to store vaccines and other commodities are not adequately maintained. This presents a significant risk to the safe storage of vaccines. Some specific examples of poor physical storage include:
To date in 2012, two state cold stores (in Kebbi and Ogun States) have burned down
due to either poor electrical wiring or inadequate security and arson (reasons for fires
not yet determined).
The March 2012 review of the cold chain found there is an inadequate storage space
at the national vaccine store. Similarly, the 2011 EVM study found that “the national
vaccine store has no adequate capacity of cold, dry and transport capacity sufficient
to accommodate all vaccines and supplies needed for the programme.”
According to the 2011 EVM, the quality of the vaccine store buildings does not meet
the minimum requirements in 46% of assessed LGA cold stores.
National, State and LGA officials need to be held accountable for providing adequate cold and dry storage facilities for vaccines and other immunisation commodities, and funding repairs to sites as needed. Consequences for under-performance in this area need to be indentified and implemented.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 95 304298 / Final
The approach, strengths and weaknesses of new vaccine introduction
The new vaccine introduction is occurring in phases. The first phase takes the 2 best performing RI states from each zone, plus FCT, and Rivers. This has the benefit of ensuring the most ready states in each zone introduce, while giving the weaker states more time to prepare (much of the preparation will entail upgrading cold chain and doing training). Phase one states started this year in June, phase 2 will start in Q2 2013 and phase 3 will start in Q2 2014. Another upside is global supply; Nigeria is so large a phased introduction will give global suppliers time to ramp up production. The downside is equity – not all Nigerian children will receive access to the new antigens at the same time. PCV (the pneumococcal vaccine) will also be introduced in phases, starting in Q2 2013. See Figures x and y below for specific states, by phase.
Figure 16: Regional vaccine coverage rates in Nigeria vary significantly; with high coverage in the South and low coverage in the North
AgendaRegional vaccine coverage rates in Nigeria vary significantly; with high coverage in the South and low coverage in the North
1
Region DPT3 Coverage (%)
South West 76.4
South South 72.2
South East 91.2
North West 59.9
North Central 67.1
North East 46.2
National 67.7
Source: National Public Health Care Development Agency (NPHCDA) 2010 National Immunization Coverage Survey
2010 DPT3 coverage, by region 2010 DPT3 coverage, by state
Note: There is also a very high level of variation
within states (at the Local Government Area level).
Sokoto
Kebbi
Zamfara
Katsina
Kano
Jigawa YobeBorno
BauchiGombe
Adamawa
Taraba
Plateau
Kaduna
Nasarawa
Benue
Niger
Kwara
Oyo
Ogun
Lagos
FCT
Kogi
Edo
Osun
Ondo
Cross RiverDelta
Bayelsa
Ekiti
EnuguAnambra
Ebonyi
Rivers Akwa Ibom
Imo Abia>=80%
60% <=x< 80%
< 30%
30% <=x< 60%
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 96 304298 / Final
Figure 17: New vaccine introduction of pentavalent vaccine and PCV will occur in phases, starting in April 2012
Conclusion
At all levels of the vaccine supply chain and logistics system in Nigeria, there is insufficient accountability for all stakeholders. This has led to a system where no one is held accountable for systemic failures (e.g. stock-outs of antigens or insufficient trainings conducted). One of the primary goals of the proposed RI Strategy and Accountability Framework will be, in collaboration with all stakeholders, to clearly map out who in the system is responsible for what activities, and define consequences for lack of performance. It is hoped that this will improve RI coverage by improving the state of the vaccine supply chain in Nigeria.
Sokoto
Kebbi
Zamfara
Katsina
Kano
Jigawa YobeBorno
BauchiGombe
Adamawa
Taraba
Plateau
Kaduna
Nasarawa
Benue
Niger
Kwara
Oyo
Ogun
Lagos
FCT
Kogi
Edo
Osun
Ondo
Cross RiverDelta
Bayelsa
Ekiti
EnuguAnambra
Ebonyi
Rivers Akwa Ibom
Imo Abia
New vaccine introduction of pentavalent vaccine and PCV will occur in phases, starting in April 2012
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 97 304298 / Final
Annex 5: People met
Name Designation Organisation
Hadjara Shibkau STL SPARC
Dr Garba Idris NPM PRRINN MNCH
Dr Rodion Kraus DNPM PRRINN MNCH
Dr Solomon Mangeste HIMA PRRINN MNCH
Dr Eric Amuah HAS PRRINN MNCH
Dr Fatimah Adamu SDA PRRINN MNCH
Dr Ahmad Abdulwahab STM ZF PRRINN MNCH
Yussuff M.J Onipe N.L PRRINN MNCH
Dr Godwin Afenyadu ORM PRRINN MNCH
Dr Henry Doctor ORA PRRINN MNCH
Dr Anthony Aboda MNCHA PRRINN MNCH
Salma A. Mijinyawa POD ZF PRRINN MNCH
Yusuf Yusufari STM, YB PRRINN MNCH
Dr Emmanuel Sokpo Consultant PRRINN MNCH
Dr Ben Anyene NIA PRRINN MNCH
Yussuff M.J onipe NL PRRINN MNCH
Alhaji Yusuf Musa DPHC SMoH
Hamza Salihu Director, MBEP
Kabiru Mohammed Permsec MBEP
Halilu Hassan DPHC MLG
Dr Lawal Umar Permsec SMoH
Yussuff M.J Onipe N.L PRRINN MNCH
Dr Usman Matazu STM, KT PRRINN MNCH
Hafsat Baba Musa POD, KT PRRINN MNCH
Zulai Sule Ingawa Director Ministry of Women Affairs
Rukayya Manga SSPO PRRINN MNCH
Saude Tasiu POS PRRINN MNCH
Halima Ben CA PRRINN MNCH
Nura Haruna CO PRRINN MNCH
Zainab Moukarim POD PRRINN MNCH
Ahmad Said STM PRRINN MNCH
Usman Tahir DG Gunduma Health System Board
Adamu Garin Gabas Perm Secretary Min Planning & Economic Planning
Sani Mohammed Chiromari Special Adviser His Excellency on Health
Lawan Kawu Ibrahim DG SPHCMB
Bulama Umar Suleiman Director PRS, SMoH
Hauwa L Goni Director PHC SPHCMB
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 98 304298 / Final
Usman Abdullahi Director Medical Services, HMB,
Dr Ben Anyene STL Abuja PRINN-MNCH
Richard Montgomery Head of Office DFID
Dr. Mustapha Mahmud Head of Immunisation NPHCDA
Pharm. Musa Dangana Head Immunisation Logistician
NPHCDA
Ms. Musonda Kasonde Supply and Logistics Specialist
UNICEF
Sajil Liaqat Health Adviser DFID
Dr Abimbola Williams Newborn and Child Health Adviser
Save the Children UK
Dr Bene Aneyene PRRINN MNCH
John Igboke Fin/Admin Manager HERFON
Dr Nkenu Ene Programme Mgr HERFON
Layi Erinosho Executive Sec HERFON
Ishaya Bajama Advocacy/Media SAVI
Kevin Gager National TL SAVI
Dr Steve Fraser Dty TL SAVI
Adam Suleiman M&E SAVI
Richard Boustred Country Adviser Marie Stopes Nigeria
Prof Emmanuel Otolorin Country Director JHPIEGO
Dr Bridget Okoeguale Head FHD FMOH (and other directors)
Jiru Bako Tech Manager Crown Agents
Dr Mark Abani Country Director Crown Agents
Mike Thaw Relationship Mgr Crown Agents
Kemi Williams Country Director Girl Hub Nigeria
Bright Ekwemeradu Executive Director Society for Family Health
Mike Egboh Chief of Party PATHS2
Benson Obonyo Director Technical PATHS2
Hadjara Shibkau STL SPARC
Dr Garba Idris NPM PRRINN MNCH
Dr Rodion Kraus DNPM PRRINN MNCH
Dr Solomon Mengiste HIMA PRRINN MNCH
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 99 304298 / Final
Annex 6: PRRINN-MNCH Annual review schedule
Date Time Meeting Responsible Venue
Monday 18.06.12
9:00 – 10:00 Introductory meeting: DFID setting the scene of the review.
Dr Idris + Susan + Fiona
DFID/ Immaculate Hotel
10:00 – 1:00 Yobe State Presentation Yobe STL Immaculate Hotel
1:00 – 2:00 Lunch Hotel
2:00 - 5: 00 Jigawa State Presentation Jigawa STL Immaculate Hotel
Tuesday 19.06.12
2:00 Ann Bartholomew Susan, Ben DFID
04:00 Dr Sokpo/Fatima Fiona, Lene Hotel
7:30 Dinner with Sarah White Fiona, Susan, Rubbina, Chris
DFID Human Development Resource Centre 100 304298 / Final
Annex 7: DFID funded health programmes in Nigeria
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Nigeria Existing Projects on Aries
Support to National Malaria Program...
104223 50,000 Aug-08 Mar-13
PRRINN-MNCH 104227 41,100 Oct-06 Dec-13
Partnership for Transforming Health Systems
104229 115,417 Oct-08 Apr-14
Enhancing Nigeria's Response to HIV/AIDS (ENR)
114206 100,000 Oct-08 Sep-14
Support to Health Reform Foundation.
201160 2,475 Sep-09 Sep-13
Improving Maternal, Newborn and Child Health
201874 57,000 Sep-10 Mar-17
Nutrition Programme Design
202188 100,000 Nov-10 Dec-17
Access To Family Planning Commodities
202668 18,000 Jul-11 Jun-17
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 101 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Nigeria Existing Projects run by Policy Division
Making it Happen: Maternal and Neonatal Health Human Resource Capacity Building
Ruth Lawson Training of providers: Scale up of the MiH Programme to a total of 12 countries between 2012 and 2015 is expected to achieve the following results just within the lifetime of the programme: • Save 9,586 maternal lives • Save 10,490 newborns • Avert 12,690 stillbirths • Avert 191,720 maternal disabilities. Sustainable capacity for the provision of quality emergency obstetric and newborn care within participating countries will be developed by the training of 17,025 health workers, including 1,025 national „Master Trainers‟.
15.86 million for 12 countries
Jan-12 Dec-15 This programme will be in Kenya, Zimbabwe, Sierra Leone, Bangladesh, India South Africa, Pakistan, Nigeria, Ghana, Nepal Tanzania, Malawi
Health Partnership Scheme: Strengthening and integrating Palliative Care into national health systems through a PHC approach in 5 African countries to contribute to meeting the targets of MDG goal 6
University of Edinburgh The African Palliative Care Association (APCA).
Palliative Care HIV/AIDS 1,536
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 102 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Health Partnership Scheme: RCPCH Global Consortium for the Exchange of Child Health Professionals
Royal College of Paediatrics and Child Health West Africa College of Physicians, Faculty of Paediatrics
Reduce infant and child mortality 835
Neglected Tropical Diseases: Onchocerciasis
African Programme for Onchocerciasis Control (APOC). APOC partners include: Merck (drug donation - ivermectin); WHO, World Bank; national governments, 12 NGDOs; 22 bilateral donors.
Current programme: 70m annual treatments delivered which protects both individuals and transmission in a community. Blindness prevented in 1 million people with high intensity infection With new investment: Additional 3m people treated Additional 3.1m health commodities distributed including antimalarials (over 425,000 people); ITNs (over 300,000); LF treatments (almost 300,000), Vit A supplementation (almost 250,000) which have wider benefit beyond Onchocerciasis
Building Workplace Capacity to combat HIV/AIDS in Nigeria
486
TUC Aid Nigeria Labour Congress
The Project will contribute to a drop in the prevalence of HIV/AIDS, better protection of employment and human rights of workers infected with or affected by HIV/AIDS and to the elimination of discrimination against them in the Education and Health Sector.
500,000 01-Apr-2009
01-Apr-2012
CSCF
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 103 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Keeping the promise of HIV/AIDS Universal Access - Ensuring accountability for promises made to achieve universal access to HIV care, treatment and prevention by 2010
361
Global Network of People Living with HIV/AIDS (GNP+) Civil Society for HIV/AIDS in Nigeria (CISHAN); Network of People Living with HIV in Nigeria (NEPWAN)
The Global Network of People Living with HIV (GNP+) and the World AIDS Campaign (WAC) are spearheading the “HIV Leadership through Accountability” programme with the Network of African People Living with HIV/AIDS (NAP+), national networks of people living with HIV and civil society organisations in fifteen countries around the world to support national processes to achieve Universal Access by: Supporting people living with HIV networks
to strengthen evidence-base advocacy, policy and programming and strengthen their participation in national processes and mechanisms;
Creating an enabling environment and the platforms which can support a strengthened coordination and participation of civil society in the development of advocacy and effective responses.
4,100 08-Sep-08
30-Mar-13
GTF
Reducing HIV/AIDS-Related Stigma and Discrimination among Vulnerable Groups: A Local, Rights-Based Communication Strategy for Nigeria
547 World Association for Christian Communication Hope for AIDS Outreach
This project mobilises faith community leaders to use their influence to reduce HIV/AIDS stigma and discrimination and increase provision of community care services.
303 31-May 2011
31-May 2014
CSCF
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 104 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Developing Southern Civil Society advocacy in Water and Sanitation in Sub-Saharan Africa, South Asia, and Central America
10 Water Aid Dadur Bol Development Association (DBOLDA); National Network on Water and Sanitation (NEWSAN); Women in Nigeria(WIN)
The WaterAid GTF programme aims to increase the capacity and resources of civil society “policy communities” in 16 target countries (across Africa, Asia and central America) to participate in effective evidence-based dialogue with decision-makers in the water and sanitation arena and add to the pressure to secure pro-poor service delivery. The programme also assists in increasing and improving the allocation of resources for the water and sanitation sector. A series of activities will enable civil society actors to develop local understanding of budgeting processes and increase their advocacy for improved sector financing. A focus on promoting the inclusion of marginalised groups in gathering evidence, advocacy and decision-making will also contribute to ensuring that the poorest benefit from changes in the sector. To increase the impact of the strengthened voice of civil society, the programme also ensures support for governments and service providers to respond appropriately to civil society and engage effectively in dialogue with local actors.
5,000 27-Aug-08
30-Sep-13
GTF
Raising Her Voice: Promoting Poor Women’s Participation in Governance
158
Oxfam Great Britain Women‟s Rights Advancement and Protection Alternative (WRAPA),
Oxfam's Raising Her Voice programme promotes the rights and capacity of poor women to engage effectively in governance at all levels through increased voice and influence and more effective institutional accountability. The overall objective of the programme is to ensure that public policy, decision-making and expenditure reflect the interests of poor and marginalised
5,000 18-Aug-08
17-Aug-13
GTF
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 105 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Garki Abuja, Nigeria
women, especially those excluded from political, social and economic life. It will achieve this by supporting women‟s leadership and addressing attitudes and beliefs about the role of women in public decision-making using strategies such as media and communications work to disseminate learning and best practice, networking, lobbying and advocacy, working with public institutions and decision-making forums and empowering and building capacity of civil society organisations. The programme consists of a pan-African element in 8 countries, 9 country components in South/East Asia, Central/South America and Eastern Europe/CIS, and a global component on learning and cross-fertilisation between projects.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 106 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Nigeria Africa Regional Programmes
Prevention of Maternal Death from Unwanted Pregnancy (PMDUP)
201518 Jane Miller PMDUP will help achieve MDG 5 by increasing family planning use and reducing maternal mortality in 14 participating country 9 of which are in Africa. In selected countries, PMDUP will support legal, regulatory and policy reform. Results will be calculated from models which link programme service delivery volumes to outcomes. As with any model, these results will be estimates. Expected results are as follows: 18,300 maternal deaths averted in the prog period and beyond; 2.8 million unsafe abortions averted; 2.8 million unintended pregnancies prevented. Evidence of institutionalized and sustainable commitment at the national level to ensure access to safe abortion and family planning The programme aims to provide over 2.9 million women with access to comprehensive abortion care, and 13.3 million women with family planning products/services over the programme period.
39,270 for 9 African
Countries
Sep-10 Jun-16 PMDUP is managed by consortium led by MSI with close partnership with IPAS.
It operates in 9 Africa Countries: DRC Ethiopia Ghana Malawi Nigeria Sierra Leone South Sudan Zambia Zimbabwe
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 107 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Evidence for Action to Reduce Maternal and Neonatal Mortality in Africa (E4A)
201512 Tony Daly In six countries (Sierra Leone, Ghana, Nigeria, Tanzania, Malawi, Ethiopia) the project will Put neglected EVIDENCE to work by the use of powerful communication – especially through reviewing and acting on the experience of every single maternal and newborn death.
Raise the profile of maternal health such that each and every maternal death is unacceptable through country and regional ADVOCACY campaigns
Secure ACCOUNTABILITY mechanisms for maternal and newborn health backed by sound data as part of the COIA activities in 6 countries –including transparency mechanisms for all stakeholders that include civil society groups and the creation of an easily accessible website featuring key information on maternal and newborn mortality.
Th3ese three core activities will be based on robust alignment and harmonisation activities ensuring that national and regional activities such as CARMMA, the Maputo Plan of Action and country maternal health roadmaps are strengthened by E4A
19,154 for 6
countries
Sep-10 Jun-16 The E4A consortium is led by Options Consultancy Services Ltd and includes the London School for Hygiene and Tropical Medicine, Advocacy International and the African networks of the White Ribbon Alliance
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 108 304298 / Final
Project title Aries code
Quest No
Contact Results / Expected outcomes of Project / Programme Details
Value (£000) S
tart
/En
d B
C
ap
pro
val
En
d d
ate
/
Du
rati
on
Notes
Nigeria Health Research
COMDIS – Health Services and communicable diseases
University of Leeds
RPC
RESYST: Resilient and Responsive Health Systems
London School of Hygiene & Tropical Medicine, UK
RPC
Artemisinin Resistance Malaria Research programme
University of Ilorin Teaching Hospital Ilorin, Nigeria: University of Oxford Centre for Tropical Medicine
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 109 304298 / Final
PRINN-MNCH Progress Reports, Quarterly reports, Case studies, Technical Briefs, KAP studies
PRINN-MNCH QI Manual. 2012-07-12
GoN. MDG 2010 Report
Nigeria Demographic Health Survey. 2008
USAID. Access to clinical and community matenral, neonatal and women‟s health (ACCESS)/Maternal and Child Health integrated program (MCHIP). March 2012.
FMOH. Maternal Mortality Situation and determinants in Nigeria. Adesegun Fatusi. March 2004
FMOH. SCUK. JHPIEGO. Saving Newborn lives in Nigeria. 2011.
PATHS1 technical briefs, fact sheets.
DFID. The Independent Monitoring and Evaluation Project for the State Level Programmes (IMEP). Mid Term Review PATHS 2. August 1, 2011
Population Council. AHIP. The Experience of Married Adolescents in Northern Nigeria. Annabel Erulkar. Mairo Bello. 2007.
Contraception and health. John Cleland et al. Lancet Family Planning series. July 2012.
WHO. Maternity Waiting Homes: A review of experiences. WHO. RHT/MSM. 96-21
The role of a maternity waiting area (MWA) in reducing maternal mortality and stillbirths in high-risk women in rural Ethiopia. J Kelly et al. RCOG 2010 BJOG An International Journal of Obstetrics and Gynaecology July 2010.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 110 304298 / Final
Annex 9: Terms of Reference
Annual Review of the Partnership for Reviving Routine Immunisation in Northern
Nigeria - Maternal Newborn and Child Health Initiative; PRRINN – MNCH June 18th – 29th June 2012
1. Objective
The aim is to undertake an Annual Review of DFID‟s Partnership for Reviving Routine Immunisation in Northern Nigeria; Maternal Newborn and Child Health Initiative (PRRINN-MNCH) following the Mid Term Review of February 2011.
Specific outputs are: i. Assess progress against the log frame purpose, outputs and OVIs. ii. Assess progress from MTR 2011 recommendations. iii. Identify new opportunities or risks. iv. Complete DFID Annual Review template for PRRINN-MNCH v. Produce draft and final report to include findings, conclusions and recommendations
and expected outcomes and results till the programme completion date. vi. Examine VFM aspects including monitoring of resource spend in health against
allocation.
2. The Recipient
DFID Nigeria. 3. Scope of Work
The Review Team will consider issues that include, but are not limited to, the following:
Quantitative and qualitative progress and achievements against programme purpose and outputs following the MTR.
Follow-up on recommendations in the MTR.
Risk analysis and mitigation;
Identify key strengths and weaknesses of partnership with Government of Nigeria.
Examine donor harmonisation within programme and other RI, MNCH and Primary Healthcare related programmes.
Conduct a value for money review of PRINN/MNCH, by assessing o Whether outcomes at the end of the project worth the costs. To what degree? o Identify changes which could increase the cost effectiveness of the programme (by
increasing the results or reducing costs) o Examine the economy, efficiency and effectiveness of PRINN/MNCH across the
results chain
Results and scale up – balanced with ability to leverage on Nigeria‟s own resources.
Examine operational research results, dissemination and impact.
Specify any considered contractual changes needed; Identify particular successes or challenges and identify lessons learnt.
Consistency with state and federal strategy
Likely contribution to state and national performance in the areas of immunisation and MNH and how the programme has influenced policy and practice.
Synergy with other related DFID supported programmes, notably PATHS2 and Evidence for Action.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 111 304298 / Final
4. Method PRRINN-MNCH will provide necessary and related information and documentation prior to the review by soft copy. The VFM review requires unit cost by output (where possible) and appropriate sub output.
The Review Team will do preparatory reading in advance of the review.
The review will take place predominantly in Northern Nigeria. There will be meetings in Abuja and Kano, where the programme has its national office. The team might visit some implementing states. States to be confirmed. Activities will include:
Read and analyse background information on: Nigerian Federal and State policies and strategies particularly for MNCH and routine immunisation; the current status of MNCH in Nigeria; PRRINN-MNCH documentation including programme memoranda and reports;
Hold discussions with Federal and State Government officials and other national and international partners active in immunisation e.g. Gates, USAID, WHO, UNICEF.
Review the status of immunisation, MNCH and primary health care services in the field in at least one health facility.
Examine the approach, strengths and weaknesses of new vaccine introduction.
Review one MNCH cluster to assess quality and MNCH continuum of care.
The value for money review should compare the costs against the inputs, outputs and outcomes. The review should be for both performance to date and for the expected performance for the remaining lifetime of the project. The review should examine o Economy (cost of inputs) that are under the control of the project o Efficiency (maximising the outputs for the given inputs) o Effectiveness (maximising the achievement of desired outcomes or benefits in both
quantitative and qualitative terms) o The consultants should strengthen the VFM review by comparing the programme‟s
economy, efficiency and effectiveness against appropriate benchmarks where this is feasible.
5. Reporting
The Team Leader will be responsible for writing the combined report with specified inputs from some other team members, and for completing the internal DFID annual reviews template for PRRINN MNCH.
A draft narrative report of the Annual Review with key findings and recommendations will be forwarded to DFID 2 weeks after the end of the mission. Comments will be provided by DFID and final report should be submitted by 6th August, 2012.
The standard DFID Annual Review will be completed for PRRINN by the same schedule as the main report.
6. Timeframe
Essential background reading for the review will be supplied to team members by end of April and this reading should be undertaken before the start of the main review mission on 18th June. Weekly productive days for the purpose of this consultancy will be Monday – Friday. This will bring productive days in Nigeria to 10 days and 4 days in the UK, subsistence will be negotiated for days in the week end. The team leader will provide inputs to the preparation of the review in May 2012. The review mission will be undertaken from 18th – 29th June 2012 with finalisation of the reports by: first Draft 16th July, DFID comments by 27th July and final draft report by 6th August 2012.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 112 304298 / Final
7. DFID Coordination
The overall coordinator will be Mick McGill, Programme Manager with Susan Elden DFID Health Adviser providing professional and technical advice. 8. Review Team
The Review Team will comprise of representation from:
DFID
Independent consultants
Government of Norway
State representatives of Health (SMOH, Gunduma SPHCDA etc)
The Review Team will be split into two if state visits are involved. Logistics and planning support will be provided by DFID Kano office manager with support by HD team in Abuja, and by PRRINN-MNCH offices in Kano, Abuja and the States.
9. Background More background information is available in the recommended documents. Key issues are highlighted below. MNCH in Nigeria Nigeria is not on target to reach MDGs 4 and 5. Maternal, newborn and child health mortalities in northern Nigeria are amongst the highest in the world. While the national under-five mortality is 157 per 1000 live births in the 2008 DHS the figures for the North West and North East zones are 217 and 222 respectively. Immunisation coverage in Nigeria has fallen since the 1990s to become one of the lowest in the world. The 2008 DHS suggests full immunisation coverage in the 4 PRRINN States to be between 0 and 5%, with measles coverage between 8 and 25%. In 2007, the „Reaching Every Ward‟ strategy was developed for immunisation. An Integrated Maternal, Newborn and Child Health strategy and a Midwifery Service Scheme are being rolled out PRRINN- MNCH DFID-funded PRRINN was originally a 5-year programme supporting the strengthening of routine immunisation and was extended by a year as a result of the findings of the OPR of 2009. The programme is now due to end on 31st December 2013 coinciding with the MNCH completion date. The programme‟s outputs include capacity building of governmental partners, increasing community demand for immunisation, and harmonisation of donors‟ inputs in order to revitalise routine immunisation. It has been operational in four states (Jigawa, Katsina, Yobe and Zamfara) in Northern Nigeria since early 2007. In 2008 the Norwegian-funded MNCH programme was added, designed to augment and strengthen PRRINN by deepening the governance components of PRRINN, strengthen the broader PHC system with focus on maternal and child health and creating a larger operational research component. DFID is managing the programme on behalf of Norway through a delegated cooperation arrangement. The consortium managing PRRINN won the tender for this new component, which started in September 2008, and the two components are now being implemented in an integrated way with a combined logframe, monitoring and evaluation framework and combined workplan. However, annual reporting requirements are still separate. The narrative report of the annual review of the combined logframe and workplan is required for the Norwegians. DFID requires a separate assessment of progress against the purpose and outputs of the PRRINN logframe, with the information being derived from the combined review.
PRRINN-MNCH Annual Review August 2012 FINAL
DFID Human Development Resource Centre 113 304298 / Final
The combined annual review of PRRINN and Inception Review of MNCH in February 2010 showed that: PRRINN was making good progress against most outputs at state level especially Output 4 on the demand side for immunisation. On the other hand it was too soon for Output 3 on strengthening primary healthcare systems to demonstrate progress. 10. Relevant Documentation
The following documents will be available to the review team prior to the start of the field work and should be read before commencement of the field work.
1. PRRINN programme memorandum (2007) 2. MNCH programme memorandum (2008) 3. PRRINN-MNCH combined logframe 4. PRRINN MNCH MYR report 2011 5. ToRs “Safe Spaces” for adolescent girls 6. Maternal Health Review of Nigeria 7. Key Paths 1 and 2 documents
The DFID Human Development Resource Centre (HDRC) provides technical assistance and information to the British Government‟s Department for International Development (DFID) and its partners in support of pro-poor programmes in education and health including nutrition and AIDS. The HDRC services are provided by three organisations: HLSP, Cambridge Education
(both part of Mott MacDonald Group) and the Institute of Development Studies.
This document is issued for the party which commissioned it and for specific purposes connected with the captioned project only. It should not be relied upon by any other party or
used for any other purpose.
We accept no responsibility for the consequences of this document being relied upon by any other party, or being used for any other purpose, or containing any error or omission which is
due to an error or omission in data supplied to us by other parties.