Toxicology for Industrial and Regulatory Scientists P th l i T i l St di Pathology in T oxicology Studies Tom Steinbach, D.V.M., DACVP, DABT Experimental Pathology Laboratories, Inc. April 28, 2015
Transcript
Toxicology for Industrial and Regulatory Scientists
P th l i T i l St di
gy g y
Pathology in Toxicology Studies
Tom Steinbach, D.V.M., DACVP, DABTExperimental Pathology Laboratories, Inc.
April 28, 2015
Pathology in Toxicology Studies
P t ti O tli• Study Design and Pathology Protocol
Presentation Outline
• Necropsy Responsibilities• Initial histopathologic evaluation• Informal pathology evaluation• Peer review• Pathology Working Groups (PWG)• Pathology Working Groups (PWG)• Data Interpretation Cases
Slide 2
Toxicologic Pathology
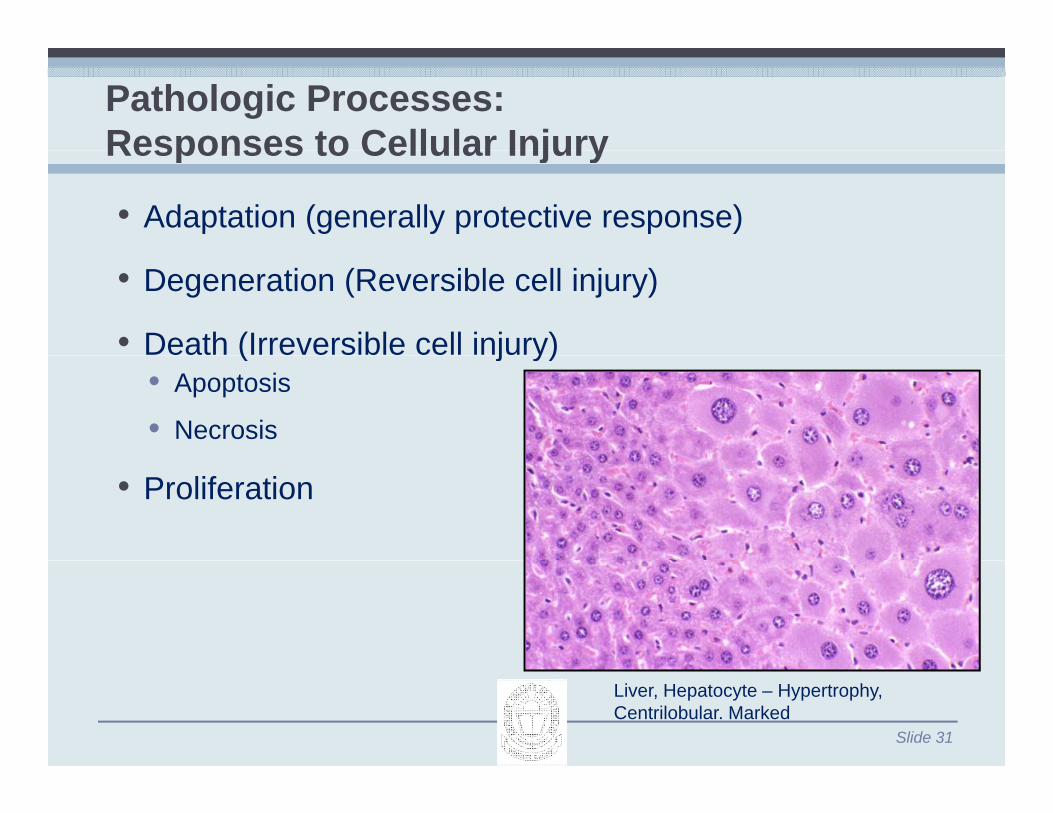
• Goal is to produce a ptabulation of treatment-related tissue changes (both gross and microscopic) andgross and microscopic) and a discussion of the significance of these ffindings.
• Pathology is an imprecise science.
Slide 3
Challenges in Toxicologic Pathology
• Normal variation between species, strains, sexes and individual animals
• Incidental findings
• Spontaneous diseasep
• Tissue artifacts
• AutolysisAutolysis
Slide 4
Study Design
• Pathologist should be involved during the study design and pathology protocol developmentdesign and pathology protocol development.
• Selection of fixatives
• Necropsy procedures
Ti ll t d• Tissues collected
• Special diagnostic techniques (PCR, special stains, in situ hybridization, electron microscopy)
Slide 5
Necropsy
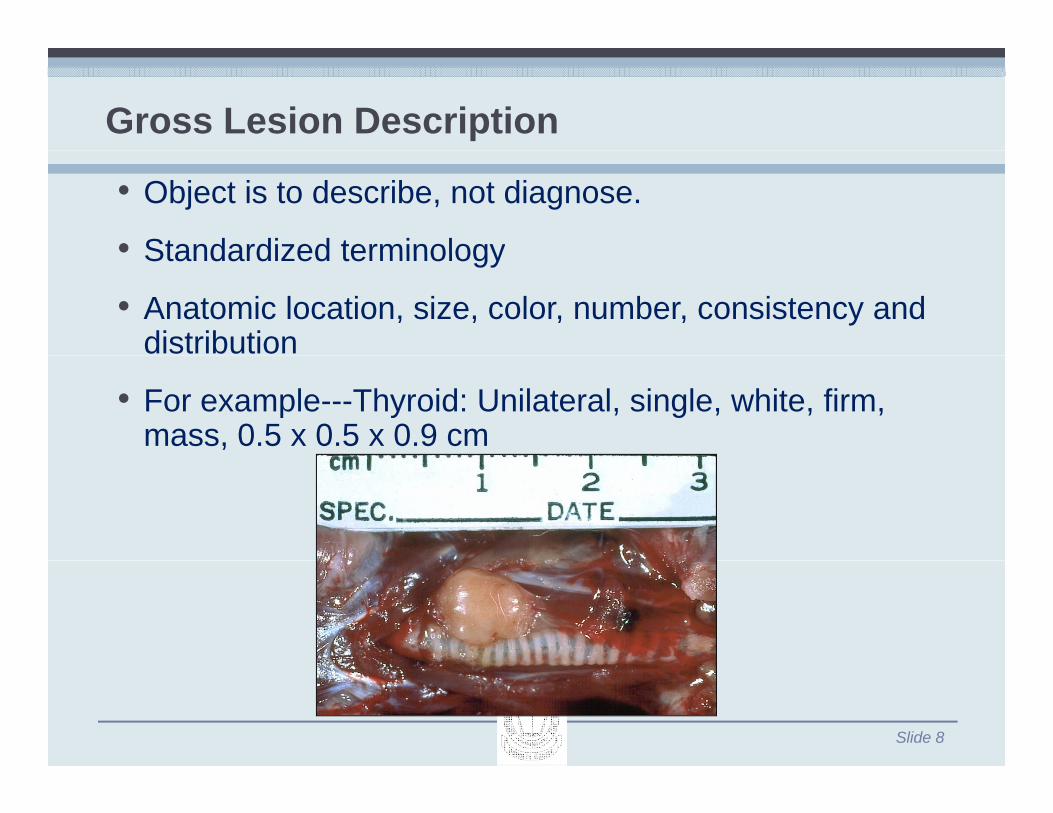
• Collection of all protocol required tissues• Recognition description and collection of all gross• Recognition, description and collection of all gross
lesions—serves as a basis for tissue trimming• Trained and experienced technicians with pathologist
i htoversight• Only one chance to do it right; once tissues are
discarded, potentially valuable information is lost., p y
Slide 6
Necropsy
• Evaluation and tissue handling must be the same for every animal.
H dli tif t ( hi• Handling artifact (crushing, squeezing, tearing) must be minimized.
• Autolysis begins immediately; dissection should start within 5should start within 5 minutes of death.
• Careful handling of tissue is essentialCareful handling of tissue is essential• Must ensure accurate identification of tissues• Must ensure tissue accountability at all stepsMust ensure tissue accountability at all steps• Recuts from fixed tissue and/or paraffin blocks should be
made to guarantee tissue accountability and slide quality
• Quality control steps should ensure that:Quality control steps should ensure that:• All required tissues and gross lesions are
present• All blocks and slides are properly labeled• Section and stain quality is adequate
Slide 12
Tissue TrimmingGeneral MethodsGeneral Methods
• Initial step in the processing of tissuesg• All tissues should be trimmed for embedding in a
standard manner• Tissues must be consistently sampled from similar
anatomic sites for all animals
Slide 13
Sample Variation – Affect on Study Results
Cystic Degeneration
Slide 14
Incidence of Cystic Degeneration in the Liver was Four Times Greater in Study 1 when compared to Study 2
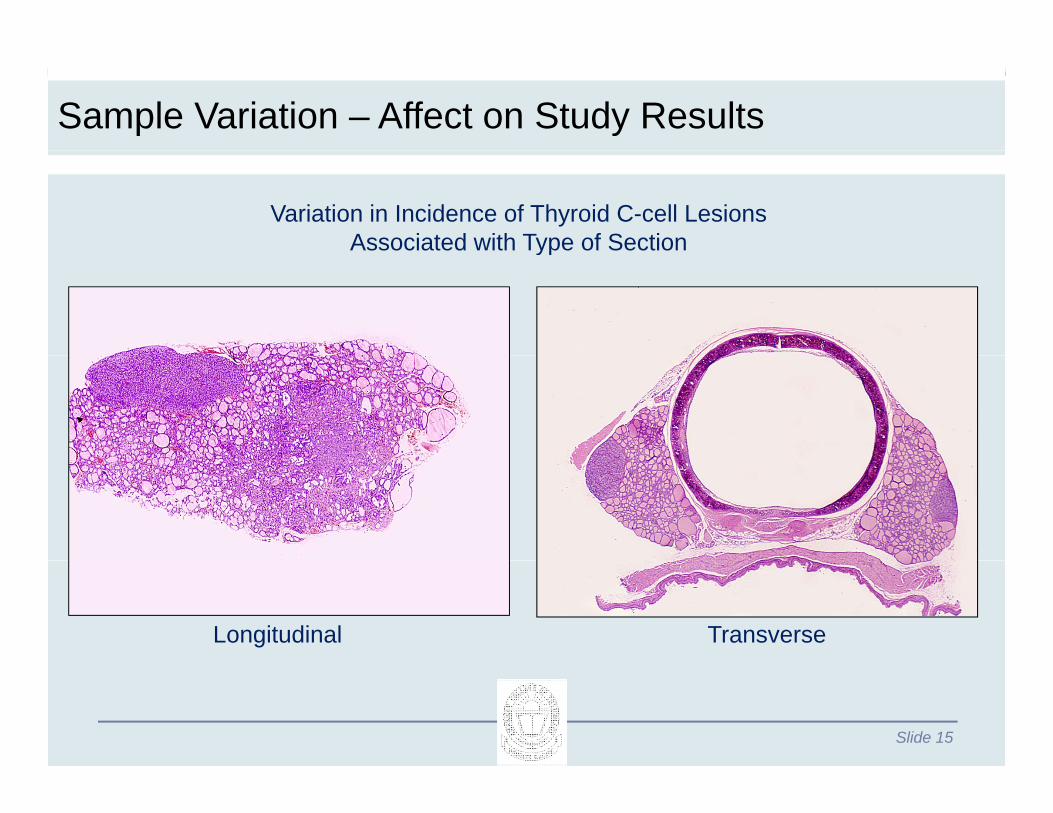
Sample Variation – Affect on Study Results
Variation in Incidence of Thyroid C-cell Lesions Associated with Type of Sectionyp
Longitudinal Transverse
Slide 15
Initial Histopathology Evaluation
• Performed with full knowledge of all data available, including treatment
• Screening test designed to detect potential treatment-Screening test designed to detect potential treatmentrelated lesions
• Responsibility of pathologist to synthesize and t l t i l i i t i f l di titranslate visual images into meaningful diagnostic terms which can be tabulated
• Requires training and experience q g p
Slide 16
Microscopic Evaluation
• Requires an experienced q pcomparative toxicologic pathologist
• Knowledge of species, strain, and sex differences of animal model usedanimal model used
Slide 17
Toxicologic Pathologist
• Role is to recognize and translate visual a d a s a e suaimages into standardized diagnosticdiagnostic terminology that can be tabulated.
• Evaluation of significance of findingsfindings
• Determination of possible
Slide 18
possible pathogenesis
Importance of Experimental Control GroupControl Group
• Establish baseline
• Determine incidence and nature of non-test article related changes in the population
• Necessary for detection of s btle changessubtle changes• Increases or decreases in cell
size• Changes in intracellular• Changes in intracellular
components• Numbers and populations of cells
within tissues
Slide 19
• Mitotic activity
Pathology Evaluation of Toxicology Studies
• Pathologist should know:• Compound name or class of compoundCompound name or class of compound• Results of previous toxicity studies• Clinical pathology data• Relevant clinical signs• Relevant clinical signs• Organ weights
• This increases the sensitivity ofThis increases the sensitivity of detection of treatment related effects.
Slide 20
Microscopic Evaluation
• Most common method of slide l tievaluation:
• Control males evaluated first• High dose males
Mid d l• Mid-dose males• Low-dose males• Females (In same order)
• This will vary for different study types and between pathologists.pathologists.
• Generally findings are entered into a computer system for
Slide 21
tabulation.
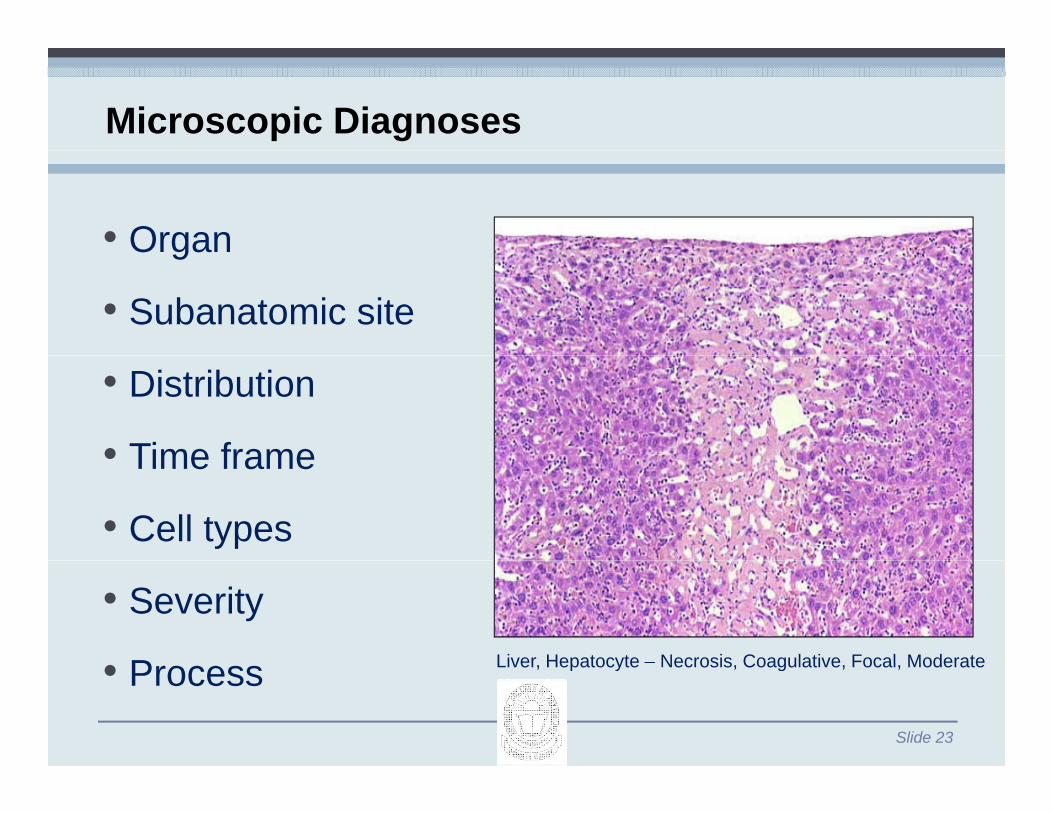
Microscopic Diagnoses
• Standardized terminology
• Consistent, so they can be tabulated• NTP Atlas of Nonneoplastic Lesions in Rats and Mice
• (htt // t i h ih / l/i d ht )• (http://ntp.niehs.nih.gov/nnl/index.htm)
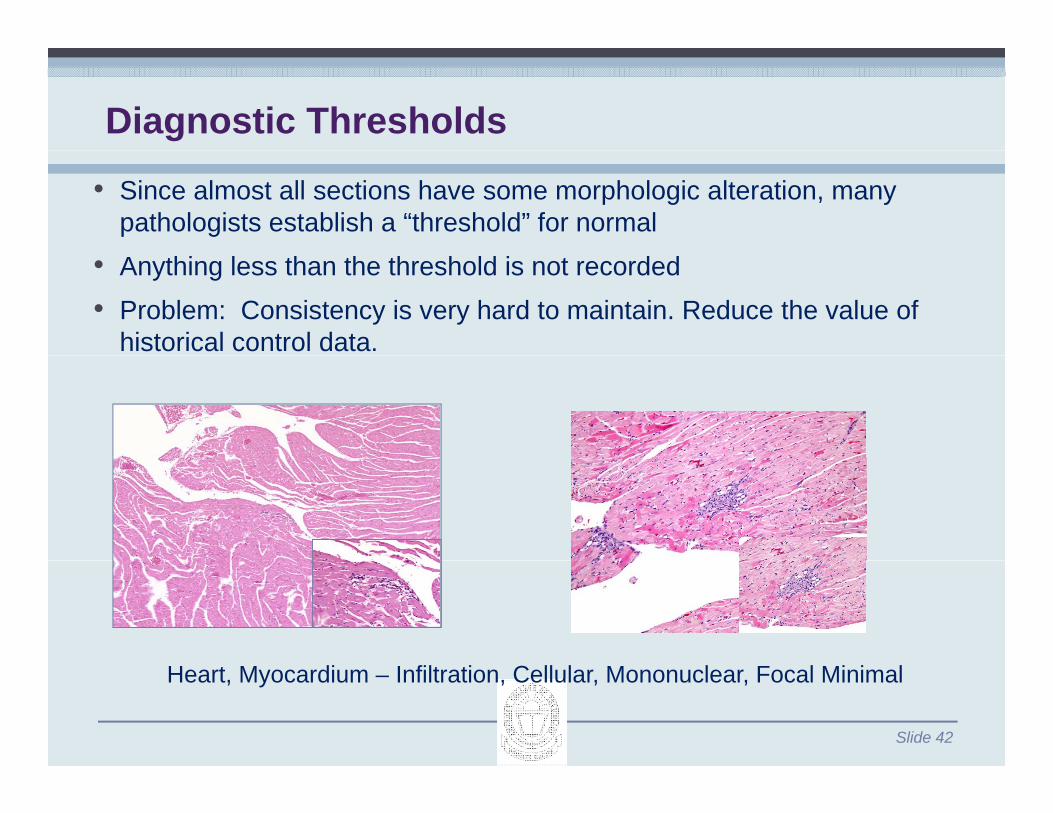
Pathologic Processes: InflammationInflammation• Reaction of vascularized living tissue to a local injury
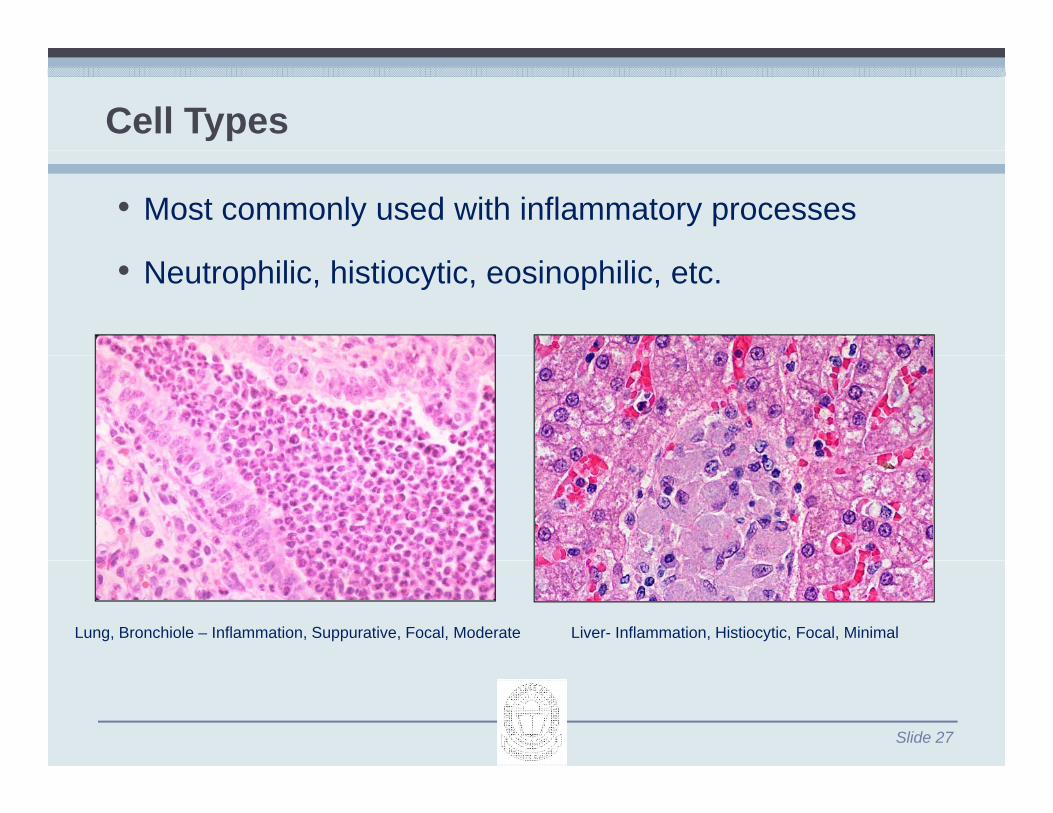
• Cell types vary with time course and inciting stimulus• Cell types vary with time course and inciting stimulus• Neutrophils: Acute inflammation• Eosinophils: Parasites; certain hypersensitivity reactions• Multinucleated macrophages (granulomatous
• Used for variations in tissue morphology, tissue artifacts and spontaneous background findingsartifacts and spontaneous background findings.
• Reduce number of diagnoses so treatment-related effects are easier to detecteffects are easier to detect.
• Insufficient or inconsistent recording of background changes may reduce the value of historical controlchanges may reduce the value of historical control data.
Slide 43
Skin - Haarscheibe Lung – Inadequate Inflation
Reporting Pathology Data
• Generally accepted nomenclaturey p• Consistent diagnostic criteria throughout report• Same terminology in summary & individual animal tables• All observations must be reported• Easy-to-follow style• Clear interpretation of findings• Unambiguous conclusion
Slide 44
Pathology Raw Data
• Pathology Raw Data “Defined as the signed and dated finalDefined as the signed and dated final report of the diagnostic pathologist” (Lepore, PD, 1996, Tox Path, Vol. 24, No 1)No. 1)
• Pathology Specimens which must be retained in archive.
P ffi bl k t ti lid• Paraffin blocks, wet tissues, slides• Final report can be reconstructed by
verification of pathology findings • Pathologist's interim notes are not raw
data because they do not contribute to study reconstruction.
Slide 45
o s udy eco s uc o
“Blinded” or “Coded”Slide Examination
Slide 46
“Blinded” or “Coded”Slide Examination
• Not recommended for screening studies• Substantial increases in time and cost• Decreased sensitivity for subtle changes• Increased potential for identification error because ofIncreased potential for identification error because of
coding and decoding process; requires more QA oversight
• Best reserved for situations requiring a determination about whether a very specific lesion is present or not
Slide 47
Comparison of Coded PathologyApproachesApproaches
Female Mice (Non-Glandular Stomach)
G C t l L D Hi h DGroup Control Low Dose High Dose
Study Pathologist (SP) – Examined in open manner with knowledge of treatment
Reviewing Pathologist (RP) – Examined in coded manner without knowledge of treatment
Pathology Working Group (PWG) – First reviewed control slides then examined all control and treated animals in a coded manner without knowledge of treatment
Slide 48
treated animals in a coded manner without knowledge of treatment
Forestomach – Epithelial Hyperplasia
SP – Normal SP – Hyperplasia, minimalSP NormalRP – NormalPWG - Normal
•Performed by a second pathologist• Involves a subset of tissues from initial evaluation• Involves a subset of tissues from initial evaluation
• Routine peer reviews • A i t i t i l d di• Assure consistency in terminology and grading• Increase confidence in the study data• Ensure data meets requirements of regulatory
Subchronic or Chronic Rodent Toxicity StudiesTechnical ApproachTechnical Approach
• Review of all tissues from two (20%) control and six (60%) high-dose male and female animals selected randomly from the highest dose with at least 60% survival.
• Review of selected tissues from all animals that die on test to• Review of selected tissues from all animals that die on test to verify the probable cause of death.
• Review of potential target organs from all animals in all groups for specific toxicologic endpoints to verify the probable “no observed effect level.”
• Resolution of all differences of opinion with the study• Resolution of all differences of opinion with the study pathologist.
Slide 60
Subchronic or Chronic Dog/Non-Human Primate Toxicity Studies
Technical ApproachR i f ll ti f t l t (25%) t l d t
Primate Toxicity Studies
• Review of all tissues from at least one (25%) control and at least three (75%) high-dose male and female animals selected randomly from the highest dose with 100% survival.y g
• Other aspects similar
Slide 61
Rodent Carcinogenicity Studies
Technical ApproachR i f ll ti f fi (10%) t l d fi (10%)• Review of all tissues from five (10%) control and five (10%) high-dose male and female animals selected randomly.
• Review of all reported proliferative lesions.Review of all reported proliferative lesions.• Review of potential target organs from all animals in all groups
for specific toxicologic endpoints to verify the probable “no b d ff t l l ”observed effect level.”
• Resolution of all differences of opinion with the study pathologist.pathologist.
• Draft histopathology report including narrative summary, p gy p g y,summary incidence tables and individual animal histopathology tablesAll h li d i i d i i lid• All hematoxylin and eosin stained microscopic slides
• Summary of Clinical Pathology Data (hematology, serum chemistry and urinalysis)chemistry and urinalysis)
• Summary of actual and relative body and organ weight data• Information concerning previous studies conducted with the• Information concerning previous studies conducted with the
compound• Information concerning the expected pharmacologic activity
Slide 63
of the test article
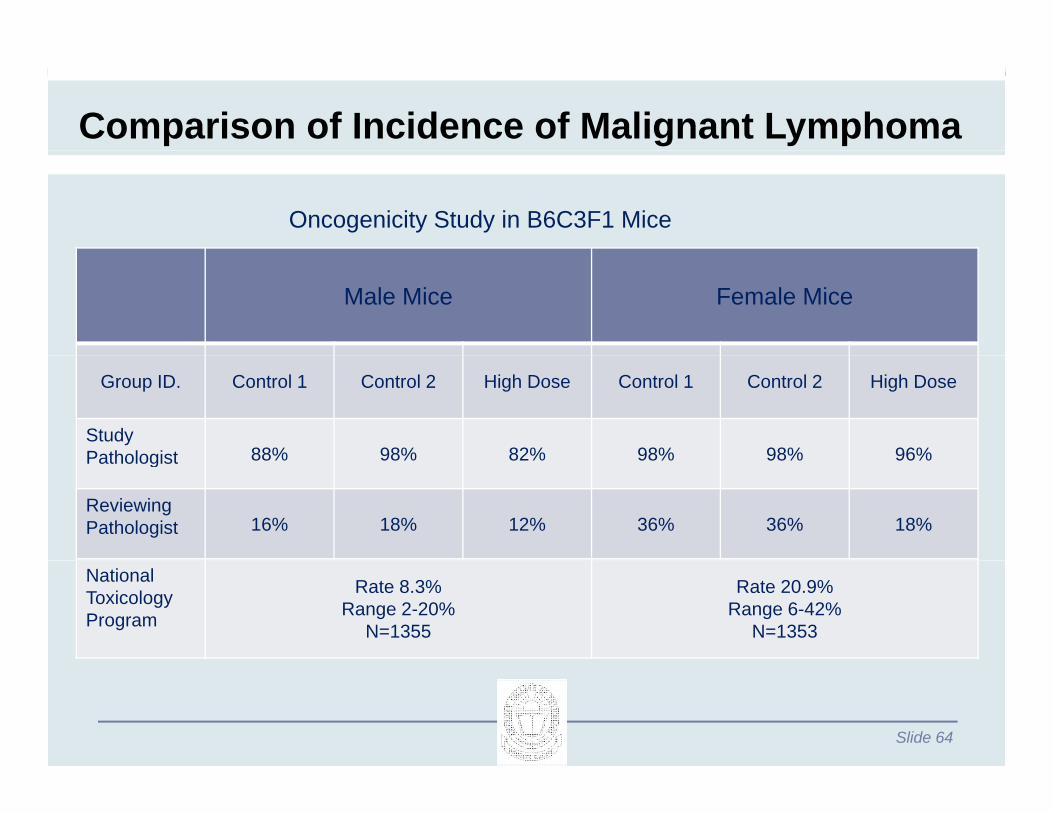
Comparison of Incidence of Malignant Lymphoma
Oncogenicity Study in B6C3F1 Mice
Male Mice Female Mice
Group ID. Control 1 Control 2 High Dose Control 1 Control 2 High Dose
• Panel of expert pathologists assembled to review a specific question concerning study resultsquestion concerning study results
• Members selected from academia, private consultants, government, and industry
• PWG participants selected based on their experience in toxicologic pathology and expertise with the target organ
Slide 66
What is the purpose of a Pathology Working Group (PWG)?g p ( )
• Independent assessment to address specific questions concerning the study resultsquestions concerning the study results
• The PWG does not review the entire study• Review limited to specific findings or toxicologic• Review limited to specific findings or toxicologic
end points• Pathology peer review and data audits are used toPathology peer review and data audits are used to
provide a detailed review
Slide 67
Is a PWG review of study data required by regulatory agencies?by regulatory agencies?
• Generally not required for data submitted to• Generally not required for data submitted to regulatory agencies
• EPA Pesticide Regulation (PR) Notice 94-5 is the• EPA Pesticide Regulation (PR) Notice 94-5 is the only regulatory requirement for a PWG review
• May be required on a study-by-study basis• May be required on a study-by-study basis depending on the issues to be resolved by other regulatory agenciesg y g
Slide 68
When should a PWG review be considered?
• Studies with final reports• Studies with final reports• Pivotal studies with controversial end points• Address questions that are of concern by• Address questions that are of concern by
regulatory agencies• Comparison of results of multiple studies that mayComparison of results of multiple studies that may
have been conducted and evaluated by different laboratories and/or pathologists
Slide 69
What is the role of the Peer Review Pathologist?Pathologist?
• E al ate the st d pathologist’s findings for• Evaluate the study pathologist’s findings for consistency and accuracy
• Identify all lesions that are relevant to the issue being• Identify all lesions that are relevant to the issue being addressed including “borderline lesions” that may otherwise not be reviewed by the PWGotherwise not be reviewed by the PWG
Slide 70
What is the role of the PWG Chairperson?p
• Thoroughly understand the issue in question• Review all relevant data and study results• Organization of the PWG review• Select and prepare materials to be reviewed by the
PWGR d PWG fi di• Record PWG consensus findings
• Author a detailed pathology report which includes the PWG findings and conclusionsthe PWG findings and conclusions
Slide 71
How are slides selected for examination by the PWG?PWG?
• Slides are selected for the PWG review that are t dd th i i tinecessary to address the issue in question
• All slides with the diagnoses to be reviewed that were recorded by either the study or peer reviewwere recorded by either the study or peer review pathologist
• For example: all liver tumors in all animalsFor example: all liver tumors in all animals• In some instances, all target organs are examined
by the PWG y
Slide 72
Examples of Issues Resolved by PWG Review:
• Incidence of neoplasms occurring in a target organ tissue in oncogenicity studies
• Comparison of proliferative liver lesions in multiple studies conducted with several PCB compounds
• Comparison of heart lesions in rats given the same test• Comparison of heart lesions in rats given the same test article in two different labs and evaluated by two different pathologists
• Vascular and subcutaneous tumors induced with• Vascular and subcutaneous tumors induced with PPARs
• Mode of action of brain tumors induced by acrylonitrile• Human relevance of liver or lung tumors in mice• Separating formalin artifacts in testes from potential
testicular toxicity
Slide 73
testicular toxicity
How is the PWG review performed?
• PWG examines coded slides without knowledge of t t t i ditreatment group or previous diagnoses
• Each panel member records the diagnoses on orksheets pro ided b the chairmanworksheets provided by the chairman
• Each member of the panel voices their opinion (vote) concerning each diagnosis(vote) concerning each diagnosis
Slide 74
PWG Worksheet
PATHOLOGY WORKING GROUP DIAGNOSESCHEMICAL NAME: XXXXXXX STUDY IDENTIFICATION: XXXXX
I i t h th i id i f i i• In instances where there is wide variance of opinions concerning a diagnosis, the panel discusses the lesion and a second vote may be necessary
• A PWG consensus diagnosis is determined for each slide examined by majority voteexamined by majority vote• There is an odd number of Supreme Court judges for a reason!
Th fi l di i f th PWG i d d b• The final consensus diagnosis of the PWG is recorded by the PWG chairperson
Slide 76
How is the PWG review performed?
• After the chairperson records the final PWG diagnoses theAfter the chairperson records the final PWG diagnoses, the results are decoded and tabulated for evaluation
• No changes in diagnoses are allowed after the final PWG diagnoses have been decoded
• The PWG panel evaluates the results and provides concl sionsconclusions
• PWG Chairman serves as the author of the PWG report, which is reviewed and edited by the PWG participants priorwhich is reviewed and edited by the PWG participants prior to finalization
Slide 77
Slide 78
Slide 79
Slide 80
Data Interpretation Cases
Slide 81
Case 1 – Male B6C3F1 mice
0 ppm
10 ppm
100 ppm
1000 ppmpp pp pp pp
Liver – hepatocellular adenoma 23 18 18 17
Liver – hepatocellular carcinoma 10 11 16 21**
Li er adenoma orLiver – adenoma or carcinoma 30 24 31 30
50 animals examined per group; **p<0.01p g p; pQuestion: Is there evidence of a carcinogenic effect due to this compound?Points for discussion:•Should HCAd and HCCas be combined? Is it necessary?•Is there a shift (progression) to malignancy? If so does that constitute a carcinogenic
Slide 82
Is there a shift (progression) to malignancy? If so, does that constitute a carcinogenic effect?•Does it matter if increased liver tumors are only in mice (not rats)?
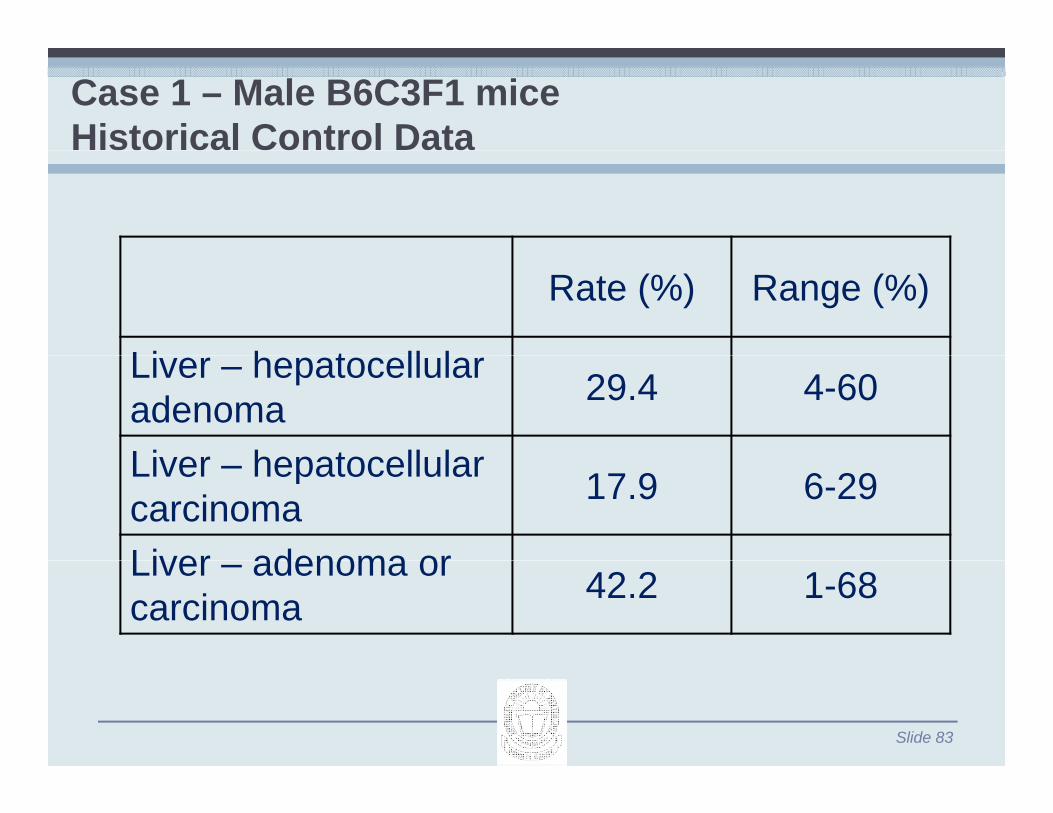
Case 1 – Male B6C3F1 miceHistorical Control Data
Rate (%) Range (%)
Li h t ll lLiver – hepatocellular adenoma 29.4 4-60
50 animals examined per groupMammary gland carcinoma – significant only by trend testAd d i bi d i id 7 9 9 15* h * 0 05 d th
Questions:Is there any compound induced carcinogenic effect?
Adenoma and carcinoma combined, incidence = 7, 9, 9, 15* where *p<0.05, and the trend test is positive
Slide 85
Is there any compound induced carcinogenic effect?Can you combine any of the above lesions? If so, which ones?
Case 4 – Mammary gland carcinomas in female Sprague-Dawley ratsp g y
0 ppm 10 ppm 100 ppm 1000 ppmpp pp pp ppm
Incidence (percentage)
Mammary gland 5 6 5 7Mammary gland –carcinoma
5(10%)
6(12%)
5(10%)
7(14%)
Survival (%) 60 61 55 25
50 animals examined per group
Question:QIs there any chemically-induced effect on mammary gland carcinomas?
Slide 86
STP Best Practices Paperswww toxpath orgwww.toxpath.orgData Interpretation⁄Management
• Recommendations for the Evaluation of Pathology Data in Nonclinical Safety Biomarker Qualification Studies
• Best Practices for Use of Historical Control Data of Proliferative Rodent Lesions• Points to Consider on the Statistical Analysis of Rodent Cancer Bioassay Data
When Incorporating Historical Control DataWhen Incorporating Historical Control Data• Examples of Historical Data Presentation• Stand Alone HCD Reference List
• Evaluation of Organ Weights for Rodent and Non-Rodent Toxicity Studies: A ReviewEvaluation of Organ Weights for Rodent and Non Rodent Toxicity Studies: A Review of Regulatory Guidelines and a Survey of Current Practices
• Pathology Image Data: Compliance with 21 CFR Parts 58 and 11
• Pathology Position on Histopathology Data Collection and Audit TrailPathology Position on Histopathology Data Collection and Audit Trail
• Assessment of Hyperplastic Lesions in Rodent Carcinogenicity Studies
• Recommendations on Classification of Rodent Neoplasms for Peto Analysis
Slide 87
STP Best Practices Paperswww toxpath orgwww.toxpath.org
Study Design
• Best Practices for Veterinary Toxicologic Clinical Pathology, with Emphasis on the Pharmaceutical and Biotechnology IndustriesPharmaceutical and Biotechnology Industries(DOI: 10.1111/vcp.12059)
• Society of Toxicologic Pathology Position Paper on Best Practices on Recovery Studies: The Role of the Anatomic Pathologist
• Interpreting Stress Responses during Routine Toxicity Studies: A Review of the Biology, Impact, and Assessment
• Use of Animal Models of Human Disease for Nonclinical Safety Assessment of Novel Ph ti lPharmaceuticals
• Scientific and Regulatory Policy Committee (SRPC) Paper: Validation of Digital Pathology Systems in the Regulated Nonclinical Environment
• Organ Weight Recommendations for Toxicology Studies• Organ Weight Recommendations for Toxicology Studies
• Best Practices Guideline: Toxicologic Histopathology
• Recommended Tissue List for Histopathologic Examination in Repeat-Dose Toxicity and Carcinogenicity Studies
Slide 88
Carcinogenicity Studies
• Diet as a Variable in Rodent Toxicology and Carcinogenicity Studies
STP Best Practices Paperswww toxpath orgwww.toxpath.org
Study Reports⁄Peer Review
• Pathology Peer Review Recommendations—2010
• Best Practices for Reporting Pathology Interpretations within GLP Toxicology Studies
• Documentation of Pathology Peer ReviewDocumentation of Pathology Peer Review
• Peer Review in Toxicologic Pathology: Some Recommendations
Slide 89
STP Best Practices Paperswww toxpath orgwww.toxpath.org
System⁄Organ Specific
• STP Position Paper: Recommended Practices for Sampling and Processing the Nervous System (B i S i l C d N d E ) d i N li i l G l T i it St di(Brain, Spinal Cord, Nerve, and Eye) during Nonclinical General Toxicity Studies
• Scientific and Regulatory Policy Committee (SRPC) Paper: Assessment of Circulating Hormones in Nonclinical Toxicity Studies III. Female Reproductive Hormones
• Society of Toxicologic Pathology Position Paper: Review Series: Assessment of Circulating y g gy p gHormones in Nonclinical Toxicity Studies: General Concepts and Considerations
• Proliferative and Nonproliferative Lesions of the Rat and Mouse Male Reproductive System
• Assessment of Circulating Hormones in Regulatory Toxicity Studies II. Male Reproductive HormonesHormones
• Best Practice Guideline for Routine Pathology Evaluation of the Immune System
• Ovarian Follicular Counting in the Assessment of Rodent Reproductive Toxicity
• G id li f th E l ti f T ti l T i it• Guidelines for the Evaluation of Testicular Toxicity
• STP Position Paper: A ‘Best Practices’ Approach to Neuropathologic Assessment in Developmental Neurotoxicity Testing—for Today
• (ASVCP) Selection and Interpretation of Clinical Pathology Indicators of Hepatic Injury in
Slide 90
( ) p gy p j yPreclinical Studies
• - See more at: http://www.toxpath.org/positions.asp#sthash.J9sB8C5P.dpuf
SSNDC Guideswww toxpath orgwww.toxpath.org
Standardized System of Nomenclature and Diagnostic Criteria (SSNDC) Guides
• Adrenal Proliferative Rat
• Bladder Proliferative Rat
• Bone Joint Tooth Nonproliferative Rat
• Bone Joint Tooth Proliferative Rat
• Cardiovascular Nonproliferative Rat• Cardiovascular Nonproliferative Rat
• Cardiovascular Proliferative Rat
• CNS Neoplasia Rat
• Endocrine Nonproliferative Rat
• Endocrine Pancreas Proliferative Rat
• Exocrine Pancreas Proliferative Rat
• Eye Proliferative Rat
• Female Reproductive Proliferative Rat
• GI Nonproliferative Rat
• GI Proliferative Rat
• Hematopoietic Nonproliferative Rat
Slide 91
• Hematopoietic Nonproliferative Rat
• Hemolymphatic Proliferative Rat
SSNDC Guideswww toxpath orgwww.toxpath.org
Standardized System of Nomenclature and Diagnostic Criteria (SSNDC) Guides
• Kidney Bladder Nonproliferative Rat
• Kidney Bladder Proliferative Rat• Kidney Bladder Proliferative Rat
• Liver Proliferative Rat
• Male Sex Glands Proliferative Rat
• Mammary Proliferative Rat
• Nervous Nonproliferative Rat
• Pituitary Proliferative Rat
• Respiratory Nonproliferative Rat
• Respiratory Proliferative Rat
• Skin Proliferative Rat
• Soft Tissue Muscle Nonproliferative Rat
S ft Ti M l P lif ti R t• Soft Tissue Muscle Proliferative Rat
• Stomach Proliferative Rat
• Testes Proliferative Rat
• Thyroid Parathyroid Proliferative Rat
Slide 92
y y
• A joint STP/ILSI effort on the mouse is available for purchase.International Classification of Rodent Tumours. The Mouse (Hardcover) by Ulrich Mohr (Editor)
Journals
• American Journal of Pathology• American Journal of Pathology
• Comparative Medicine (Laboratory Animal Science)
• Journal of Veterinary Diagnostic Investigation
• Laboratory Investigation
• Toxicologic Pathology
• Veterinary Pathology• Veterinary Pathology
Slide 93
Textbooks
• Bennett, Abee and Henrickson - Nonhuman Primates in Biomedical Research: Diseases
• Boorman, Eustis, Elwell, Montgomery and MacKenzie - Pathology of the Fischer RatBoorman, Eustis, Elwell, Montgomery and MacKenzie Pathology of the Fischer Rat
• Fox, Anderson, Loew and Quimby - Laboratory Animal Medicine, 2nd Ed
• Fox - Biology and Diseases of the Ferret, 2nd Ed
F B th ld D i N Q i b d S ith Th M i Bi di l• Fox, Barthold, Davisson, Newcomer, Quimby and Smith - The Mouse in Biomedical Research, 2nd Ed
• Jones, Hunt and King – Veterinary Pathology, 6th Ed
• Maronpot Boorman and Gaul Pathology of the Mouse• Maronpot, Boorman and Gaul - Pathology of the Mouse
• Percy and Barthold - Pathology of Laboratory Rodents and Rabbits, 3rd Ed
• Ward, Mahler, Maronpot and Sundberg - Pathology of Genetically Engineered Mice
• Greaves – Histopathology of Preclinical Toxicity Studies
• Lesions of Genetically Engineered Micey g• A Digitized Atlas of Rodent Kidney Lesions• A Digitized Atlas of Mouse Liver Lesions (Version 2 and 3)• A Digitized Atlas of Rat Liver Lesions (Version 1)• Respiratory Collection Protocol of the Laboratory Dogp y y g• Heart Trimming Protocol of the Laboratory Rat• Heart Collection Protocol of the Laboratory Dog and Monkey• Ocular Collection Protocol of the Laboratory Rabbit, Dog and Monkey• RNA Collection• A Monograph on Histomorphologic Evaluation of the Lymphoid Organs, Toxicologic Pathology,