72
PATHOLOGY OF THE KIDNEY Dody Novrial Department of Pathology, JSU
| Date post: | 21-Jul-2016 |
| Category: |
Documents |
| Upload: | conan-armstrong |
| View: | 27 times |
| Download: | 3 times |
PATHOLOGY OF THE KIDNEY
Dody NovrialDepartment of Pathology, JSU
Renal Diseases
Renal diseases are divided into 4 categories based on basic anatomic compartment principally affected : Glomeruli Tubules Interstitium Blood vessels
Clinical Manifestation Renal diseases clinically manifest
themselves within reasonably well-defined syndromes :
Stages of renal diseases progression :1. Diminished renal reserve (approximately
50% of normal GFR)2. Renal insufficiency (20%-50% of normal
GFR)3. Renal failure (<20% of normal GFR)4. End-stage renal disease (<5% of normal
GFR
Congenital Anomalies
1. Renal agenesis2. Hypoplasia3. Ectopic kidneys4. Horseshoe kidney
Most arise from developmental defects rather than inherited genes
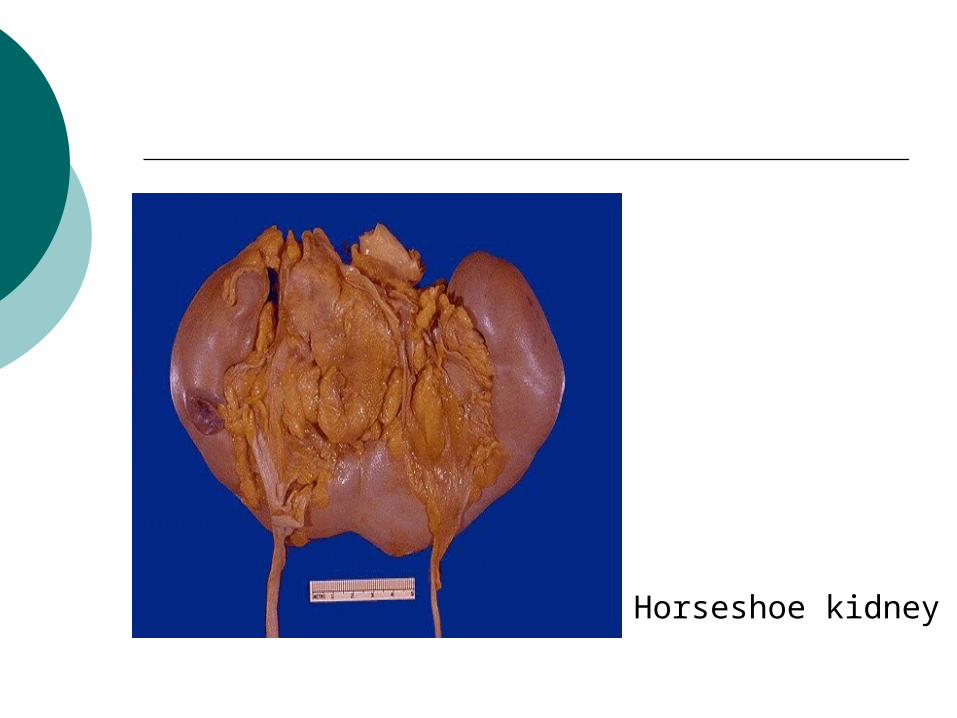
Horseshoe kidney
Cystic Diseases of the Kidney
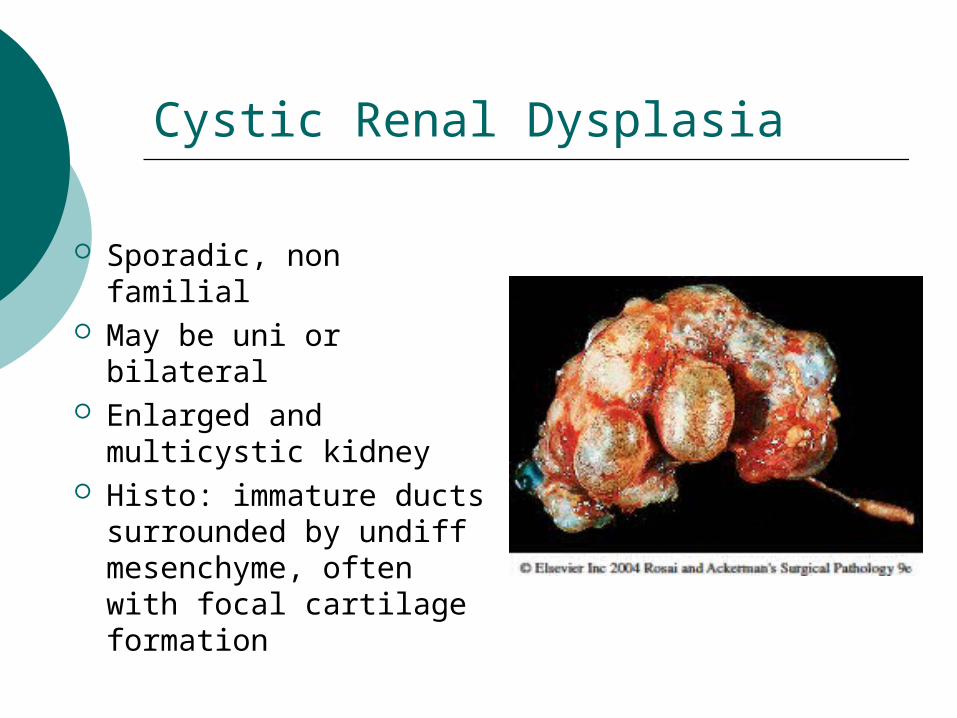
Cystic Renal Dysplasia
Sporadic, non familial May be uni or bilateral Enlarged and
multicystic kidney Histo: immature ducts
surrounded by undiff mesenchyme, often with focal cartilage formation
Polycystic Kidney DiseaseAutosomal dominant (adult) Caused by mutation of PKD1 or PKD2 genes Always bilateral Can present from early childhood to as late
as 80 years of age Enlarged kidney composed of cysts up to 3-4
cm in diameter Associated with liver cysts, cerebral berry
aneurysms, mitral valve prolaps Clinically : hypertension, chronic renal failure,
hematuria
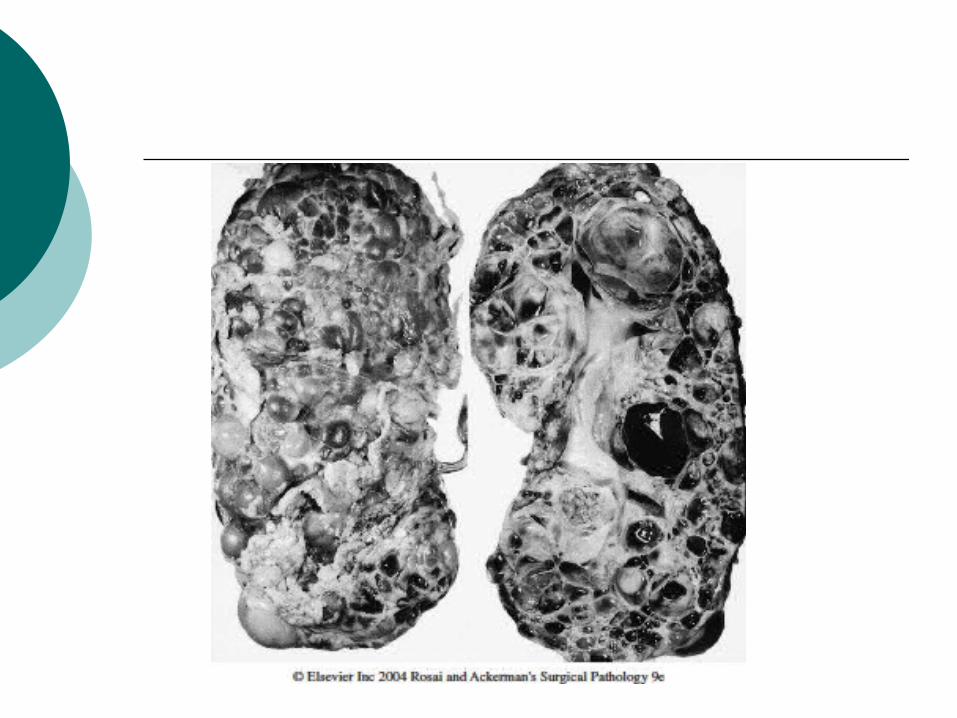
Polycystic Kidney Disease
Autosomal recessive (childhood) Rarely Infants often succumb rapidly to
renal failure Kidneys are enlarged by multiple,
cylindrically dilated collecting ducts Associated with liver cysts and
congenital hepatic fibrosis
Cystic Diseases of Renal Medulla
Medullary Sponge Kidney Multiple cystic dilatations in the
collecting ducts of the medulla Usually presenting in adults It can predispose to renal calculi
Cystic Diseases of Renal Medulla
Nephronophthisis-Medullary Cystic Disease Complex
Progressive renal disorder Onset in childhood Small medullary cyst in corticomedullary
area associated with cortical tubular atrophy and interstitial fibrosis
Variants : Sporadic (20%), Familial juvenile nephronophthisis (50%), Renal- retinal dysplasia (15%), adult-onset medullary cystic disease (15%)
Cystic Diseases of Renal Medulla
Acquired (Dialysis-Associated) Cystic Disease
End Stage kidney patients with prolonged renal dialysis
Multiple cortical and medullary cysts Often lined by atypical, hyperplastic
epithelium Can undergo malignant
transformation – renal cell ca
Cystic Diseases of Renal Medulla
Simple Cysts Multiple or single cyst 1-5 cm, but can measured up to 10
cm Commonly postmortem findings
without clinical significance Composed of single layer of
cuboidal or flattened cuboidal epithelium
GLOMERULAR DISEASES
Primary Glomerulopathies
Acute diffuse proliferative GN- post streptococcal- non post streptococcal
Rapidly progressive GN Membranous glomerulopathy Minimal change disease Focal segmental glomerulosclerosis Membranoproliferative GN IgA nephropathy Chronic GN
Systemic Diseases with Glomerular Involvement
Systemic lupus erythematosus Diabetes Mellitus Amyloidosis Goodpasture syndrome Microscopic polyarteritis/polyangiitis Wegener granulomatosis Henoch-Schonlein purpura Bacterial endocarditis
Hereditary Disorders
Alport syndrome Thin basement membrane disease Fabry disease
Pathogenesis of Glomerular Injury
Immune mechanism >>> Non immune factors can initiate GN
or cause its progression
Immune Mechanism of Glomerular Injury
Antibody mediated immune injuryIn situ immune complex depositionFixed intrinsic tissue Ag : - anti GBM nephritis- Heymann antigen- Mesangial antigenPlanted Ag :- Exogenous (infectious agent, drug)- Endogenous (DNA, nuclear prot, Ig, immune complex)
Immune Mechanism of Glomerular Injury
Circulating immune complex deposition- Endogenous (DNA, tumour Ag)- Exogenous (Infectious products)Cytotoxic Antibodies
Cell-mediated immune injury Activation of alternative
complement pathway
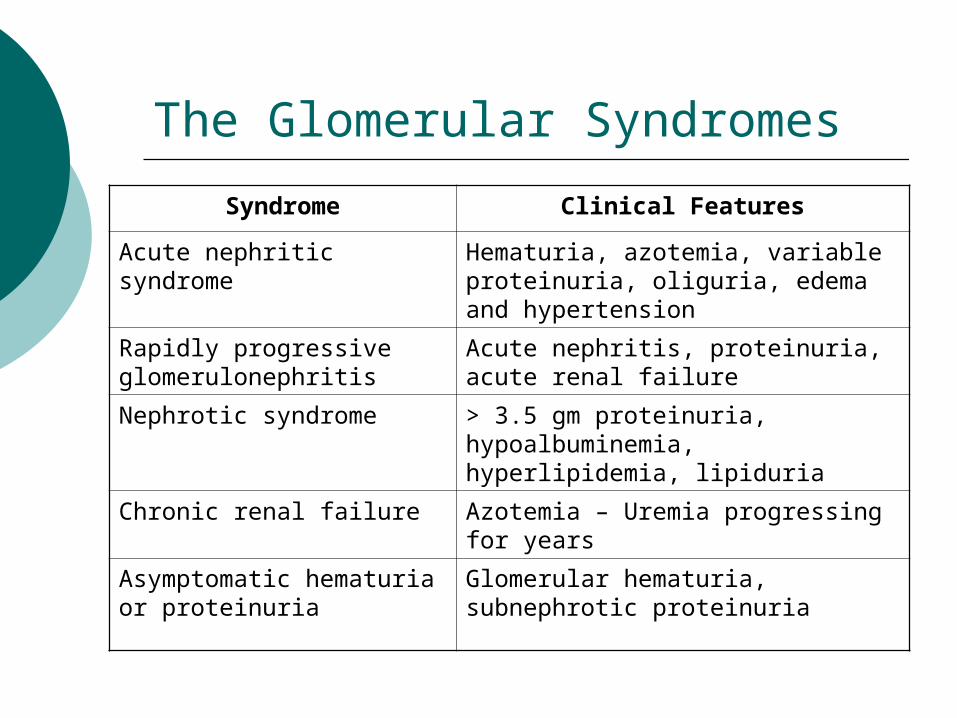
The Glomerular Syndromes
Syndrome Clinical FeaturesAcute nephritic syndrome Hematuria, azotemia, variable
proteinuria, oliguria, edema and hypertension
Rapidly progressive glomerulonephritis
Acute nephritis, proteinuria, acute renal failure
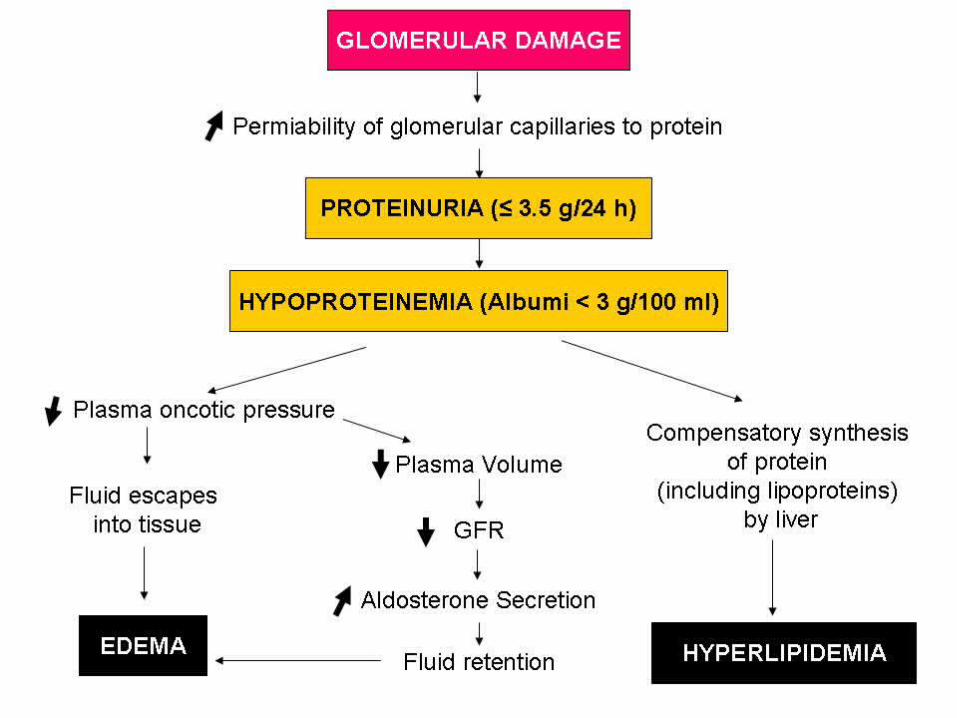
Nephrotic syndrome > 3.5 gm proteinuria, hypoalbuminemia, hyperlipidemia, lipiduria
Chronic renal failure Azotemia – Uremia progressing for years
Asymptomatic hematuria or proteinuria
Glomerular hematuria, subnephrotic proteinuria
Histologic Alteration
Hypercellularity- Cellular proliferation of mesangial
and endothelial cells- Leukocytic infiltration- Formation of crescents
Basement membrane thickening Hyalinization and sklerosis
Acute Glomerulonephritis
Poststreptococcal GN Etiology : α-β hemolytic streptococci types
12,4,1 Immune complex mediated Clinically :
- Malaise, fever, nausea, oliguria, hematuria after recovery from sore throat- Elevation of ASO
Morphology :- enlarged and hypercellular glomeruli
Acute Glomerulonephritis
Nonstreptococcal GN Etiology : other bacterial, viral or
parasitic infections Immune complex mediated Granular immunofluorescent and
subepithelial humps are present
Rapidly Progressive (Cressentic) GN
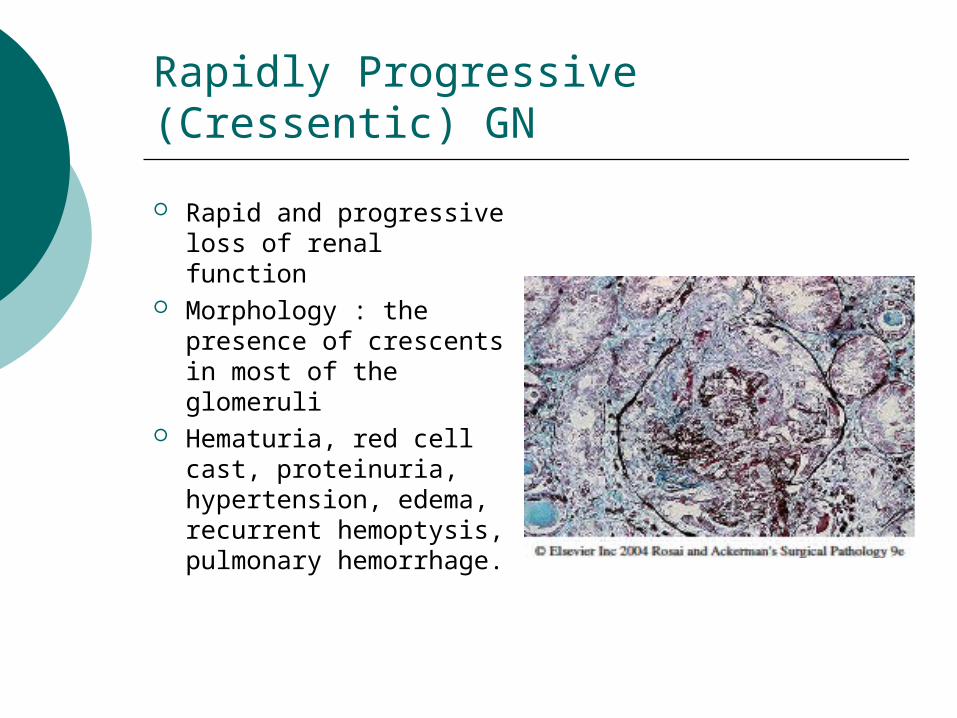
Rapid and progressive loss of renal function
Morphology : the presence of crescents in most of the glomeruli
Hematuria, red cell cast, proteinuria, hypertension, edema, recurrent hemoptysis, pulmonary hemorrhage.
Rapidly Progressive (Cressentic) GNType I RPGN (Anti-GBM antibody) Idiopathic Goodpasture syndrome
Type II RPGN (Immune complex) Idiopathic Post infectious SLE Henoch-Schonlein purpura (IgA)
Type III RPGN (Pauci-Immune) ANCA associated Idiopathic Wegener granulomatosis Microscopic polyarteritis/polyangiitis
Nephrotic Syndrome
Primary glomerular lesions :- Minimal change disease- Membranous glomerulopathy- Focal segmental glomerulosclerosis
Systemic causes :- DM- SLE- Amyloidosis
Membranous glomerulopathy
The most common cause of NS Immune complex mediated Associated with drugs (penicilamine,
captopril, NSAID), malignant tumor, SLE, infection, other autoimmune disorders
Morphology :- diffuse thickening of glomerular capillary
wall without cells proliferation- accumulation of electron dense- Ig containing deposits along the subepithelial side of the basement membran
Minimal Change (Lipoid Nephrosis)
The most frequent cause of NS in children
Associated with immunologic disorders
Normal glomeruli by light microscopy
Diffuse effacement of foot processes of epithelial cells in glomeruli (by electron microscopy
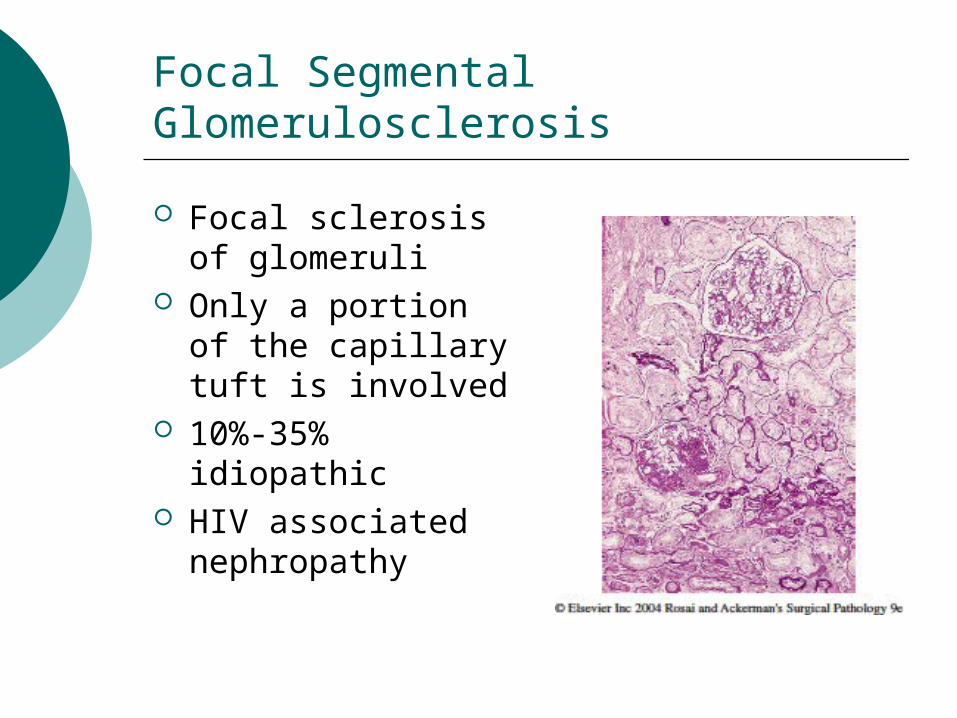
Focal Segmental Glomerulosclerosis
Focal sclerosis of glomeruli
Only a portion of the capillary tuft is involved
10%-35% idiopathic
HIV associated nephropathy
Membranoproliferative GN Characterized histologically by
- alterations in the basement membrane- proliferation of glomerular cells- leucocyte infiltration
Primary MPGN- Type I and Type II- Evidence of immune complexes- Evidence of activation of both classical and alternative complement pathway
Secondary MPGN- Chronic immune complex disorders- α1-antitrypsin deficiency- Malignant diseases- Hereditary deficiencies of complement regulatory proteins
Ig A Nephropathy (Berger Disease) Ig A deposits in mesangial regions Frequent cause of recurrent
gross/microscopic hematuria
Alport Syndrome Nephritis – chronic renal failure Nerve deafness Various eye disorders (lens dislocation,
posterior cataracts, corneal dystrophy)
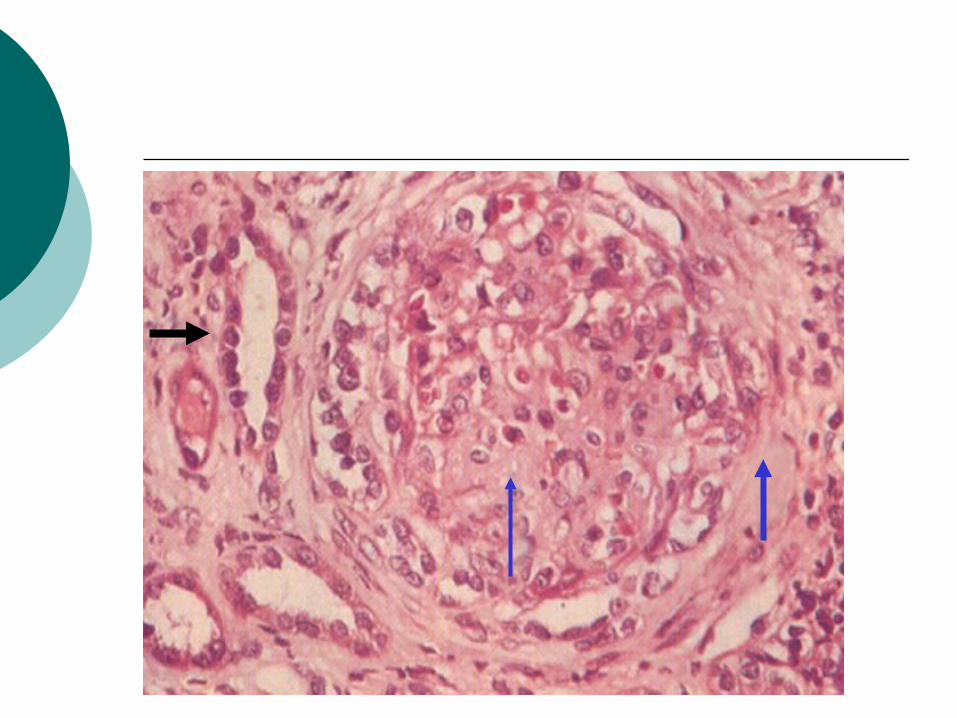
Chronic Glomerulonephritis
End stage glomerular disease Some cases arise mysteriously Thin cortex Hyaline obliteration of glomeruli Arterial and arteriolar sclerosis Atrophy of associated tubules Dialysis change Uremic complication
Diseases Affecting Tubules and Interstitium
Group of processes
Ischemic or toxic tubular injury leading to acute tubular necrosis (ATN) and acute renal failure
Inflammatory reaction (tubulointerstitial nephritis)
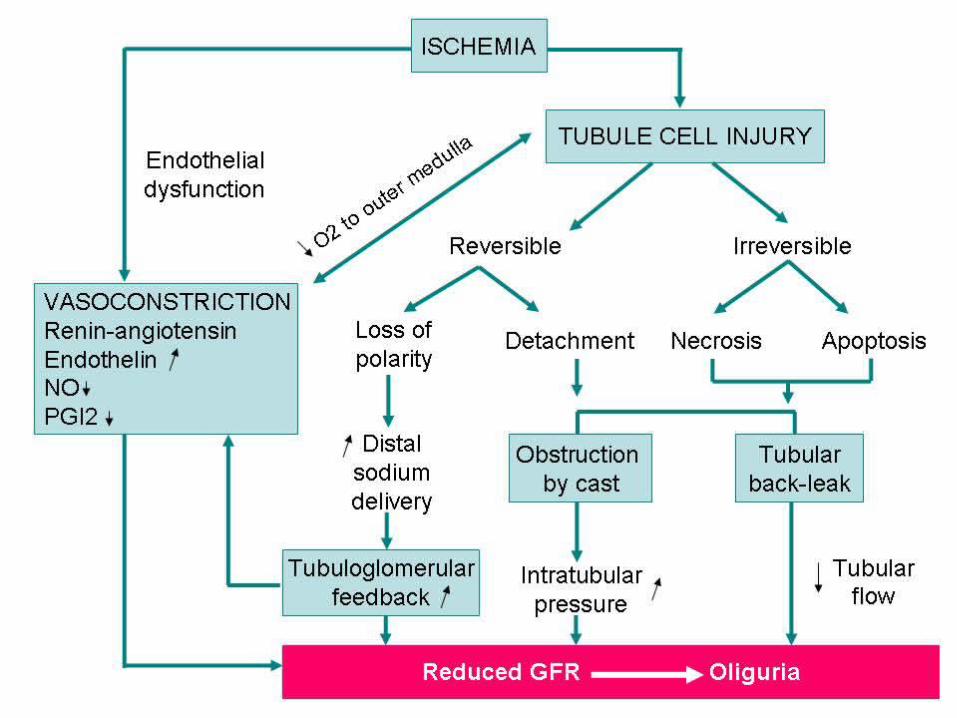
Acute Tubular Necrosis
Destruction of tubular epithelial cells
Diminution or loss of renal function Causes :
- Ischemia- Direct toxic injury to the tubules- Acute tubulointerstitial nephritis- DIC- Urinary obstruction
Tubulointerstitial Nephritis Involve predominantly the tubules and
interstitium Acute TIN
Interstitial edema Leukocytic infiltration of the interstitium and
tubules Focal tubular necrosis
Chronic TIN Infiltration of predominantly MN Prominent interstitial fibrosis Widespread tubular atrophy
Tubulointerstitial Nephritis
Causes of TIN : Infection Toxins Metabolic diseases Physical factors Neoplasms Immunologic reactions Vascular diseases Idiopathic
Pyelonephritis and UTI
Renal disorder affecting the tubules, interstitium and renal pelvis
Acute : UTI Chronic : UTI, vesicoureteral reflux,
obstruction E. Colli, Proteus, Klebsiella, etc Hematogenous or ascending
infection
Acute Pyelonephritis Acute suppurative inflammation of the
kidney caused Morphology :
Patchy interstitial suppurative inflammation Intratubular aggregates of neutrophils Tubular necrosis
Complication Papillary necrosis Pyonephrosis Perinephric abcess Pyelonephritic scar
Chronic Pyelonephritis
Chronic tubulointerstitial inflammation and renal scarring associated with pathologic involvement of the calyces and pelvis
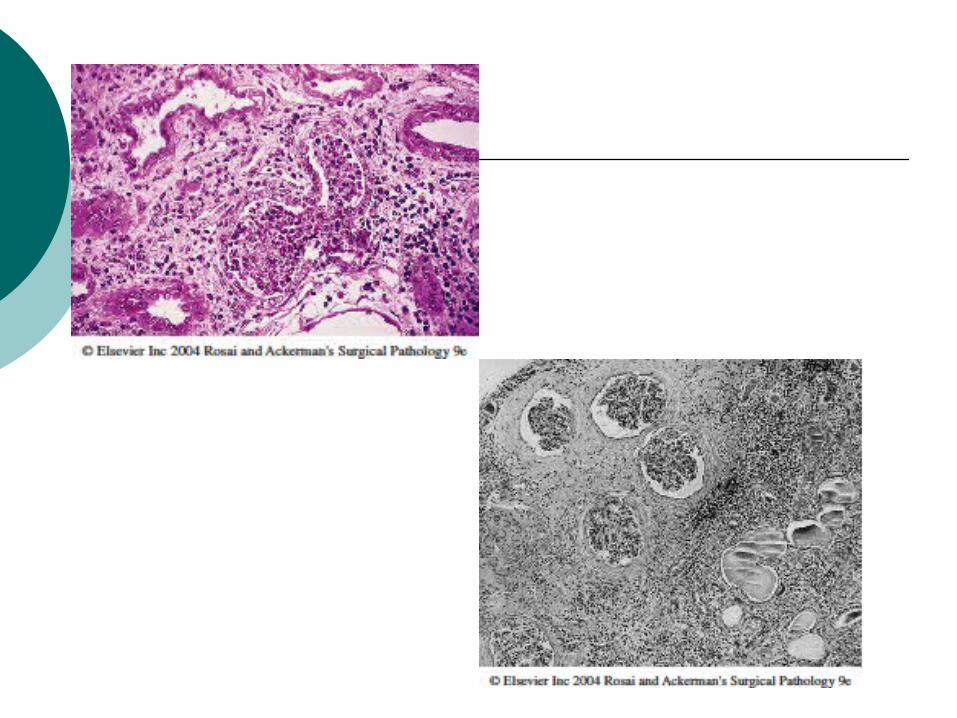
Morphology Gross : irregularly scarred, asymmetric if
bilateral Atrophy and or hypertrophy or dilatation of
tubules Coloid casts (thyroidization) Chronic interstitial inflammation Fibrosis in the cortex or medulla
Diseases of Blood Vessels
Benign Nephrosclerosis
Renal pathology associated with sclerosis of renal arterioles and small arteries
Morphology Medial and intimal thickening Hyaline deposition in arterioles (hyaline
arteriosclerosis)
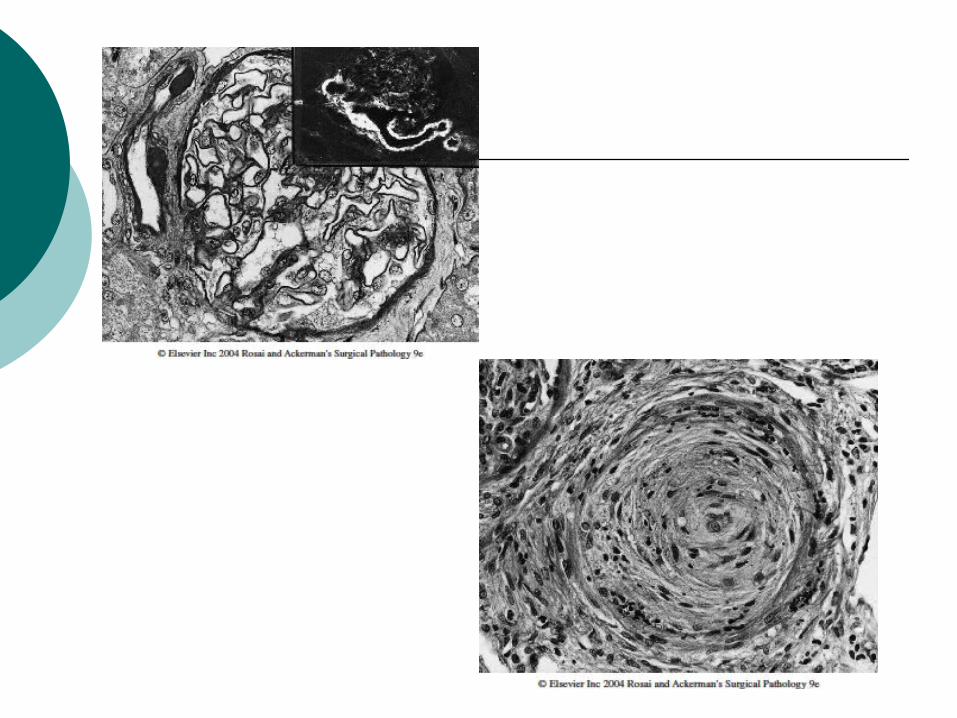
Malignant Hypertension and Accelerated Nephrosclerosis
Associated with the malignant or accelerated phase of hypertension
Relatively uncommon Pathogenesis is unclear Morphology
Gross : “flea-bitten” appearance Fibrinoid necrosis of arterioles Interlobular arteries/arteriole ntimal
thickening (onion-skinning)
Renal Artery Stenosis
Occlusion by an atheromatous plaque (70%)
Fibromuscular dysplasia Intimal Medial Adventitial
Thrombotic Microangiopathies
Thrombosis in capillaries Clinically :
Microangiopathic hemolytic anemia Thrombocytopenia Renal failure
Categories : Classic childhood hemolytic-uremic syndrome
(HUS) Adult HUS Familial HUS Idiopathic TromboticTrombocytophenic Purpura
(TTP)
Types of Hypertension Related Renal Diseases
Primary or essential hypertension Secondary hypertension
Acute GN Chronic renal disease Renal artery stenosis Renal vasculitis Renin-producing tumors
Obstructive Uropathy and Urolithiasis
Obstructive Uropathy Increases susceptibility to infection and stone
formation Leads to permanent renal
atrophy/hydronephrosi/obstructive uropathy Causes
Congenital anomalies Urinary canaliculi BPH Tumors Inflammation Sloughed papillae or blood clots Normal pregnancy Uterine prolaps and cystocele Functional disorders
Urolithiasis
Various types of renal stones Calcium oxalate and phosphate (70%) Magnesium ammonium phosphate
(struvite) (15-20%) Uric acid (5-10%) Cystine Others or Unknown
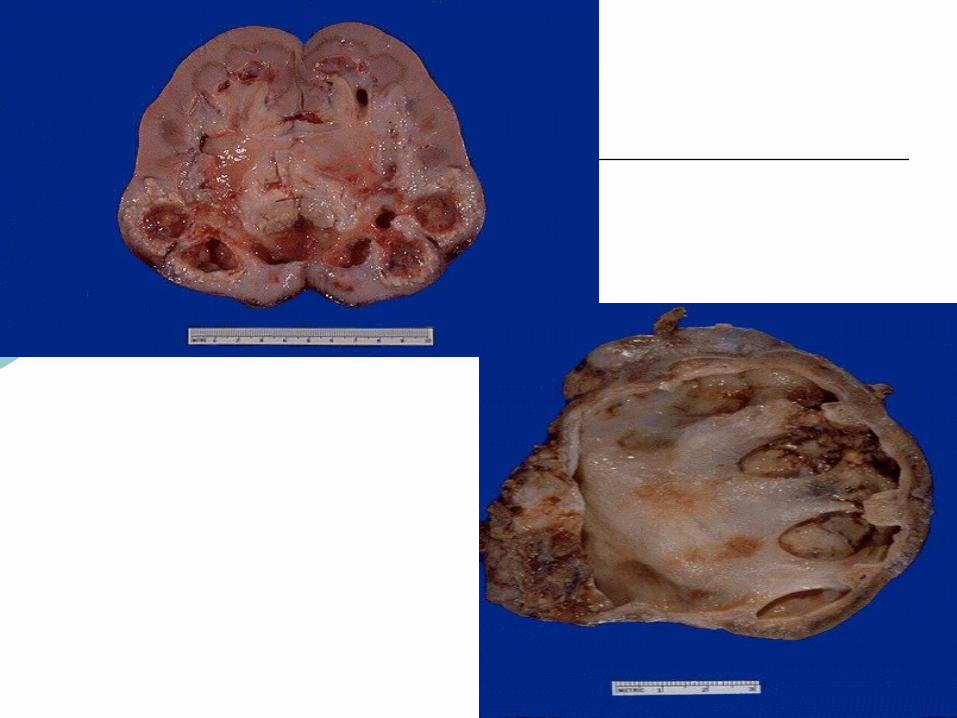
Urolithiasis
Morphology Unilateral in about 80% of patients Usually in renal calyces, pelvis and
bladder Progressive accretion of salts
Staghorn stones
Tumors of the Kidney
Benign Tumors
Rarely cause clinical problems except oncocytoma
Consist of : Renal papillary adenoma Renal fibroma Angiomyolipoma Oncocytoma
Malignant Tumor
Most common type Renal Cell Carcinoma Wilms tumor Urothelial Ca of renal pelvis
Renal Cell Carcinoma
1-3% of all visceral cancer 85% of renal ca in adults Age : older individual (60-70) M:F = 3:1 Arise from tubular epithelium Risk factors
Tobacco Obesity Hypertension Estrogen therapy Exposure to asbestos, petroleum products,
heavy metal
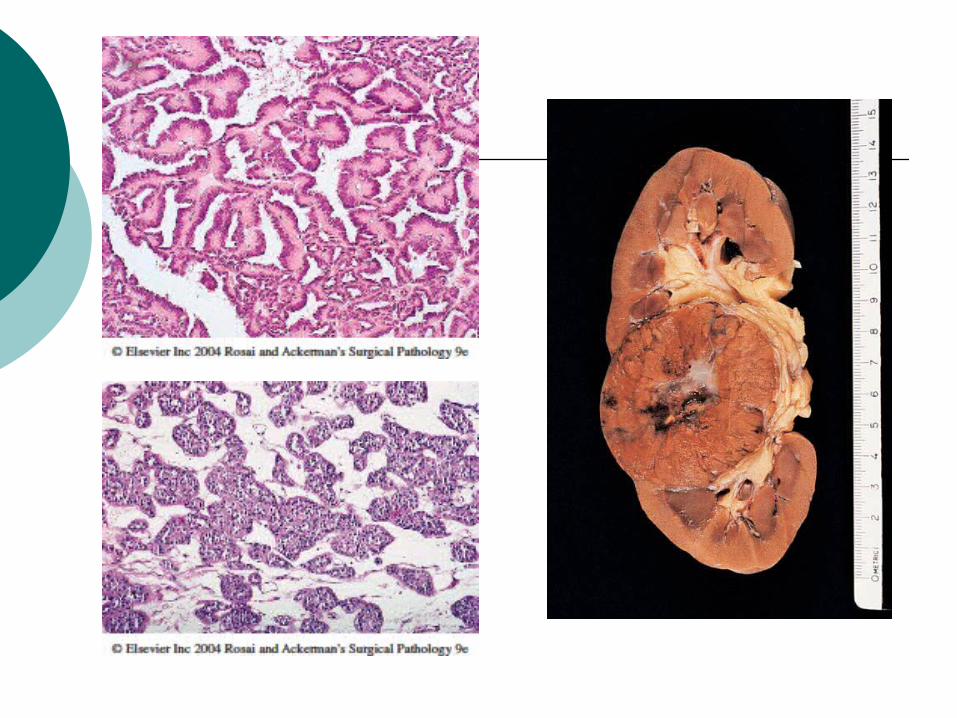
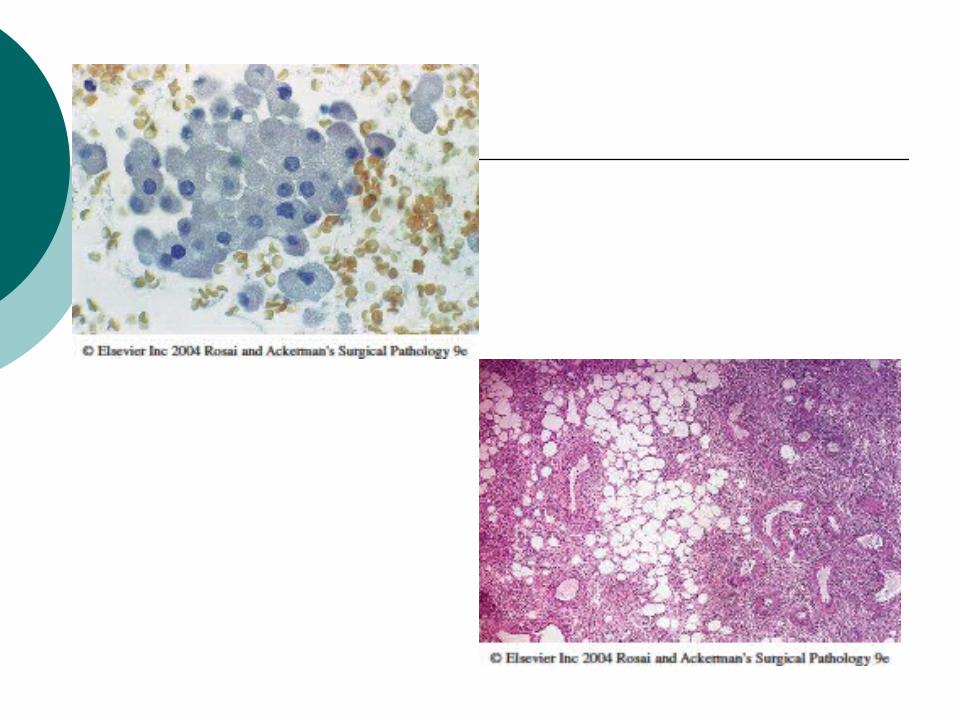
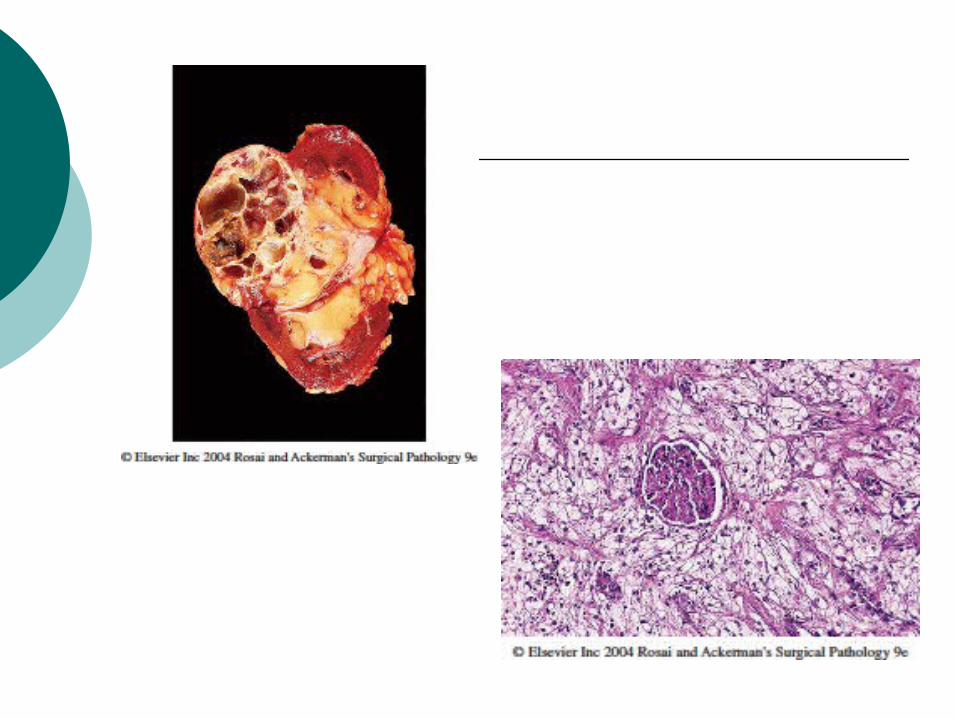
Renal Cell Carcinoma
The major types of tumor : Clear cell ca Papillary ca Chromophobe renal ca Collecting duct (Bellini duct) ca
Urothelial Ca of Renal Pelvis
5% - 10 % of primary renal tumors Originate from urothelium of renal
pelvis Almost never palpable clincally Histo : exact counterpart of those
found in the urinary bladder
Wilms Tumor
The most common primary renal tumor of childhood
5-10% bilateral Associated with WAGR Syndrome
Aniridia Genital anomalies Mental retardation
Wilms Tumor
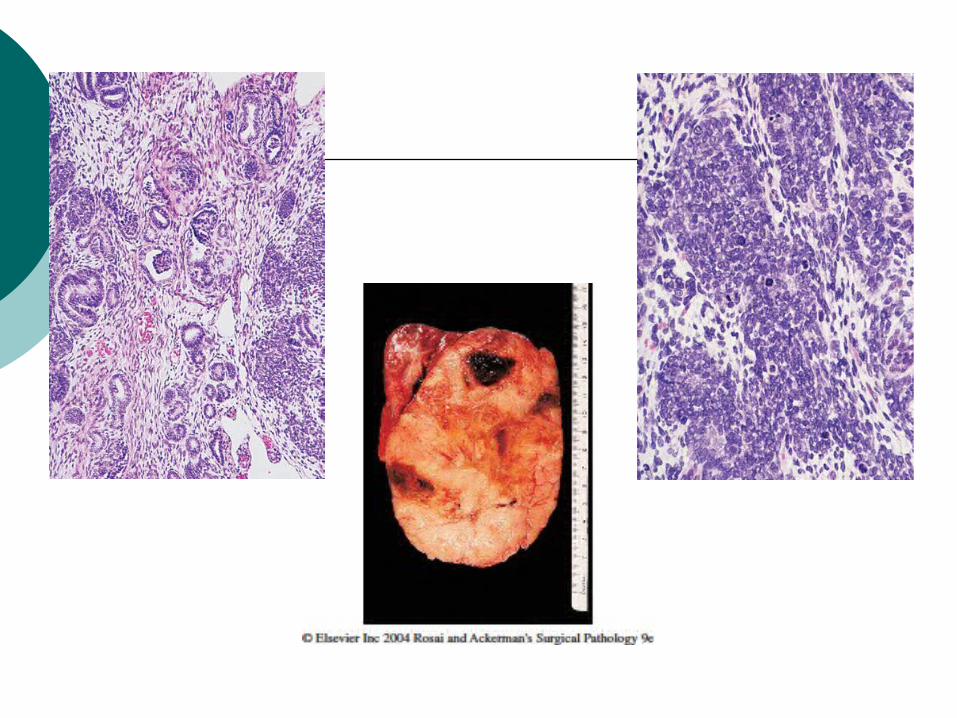
Morphology Gross : large, solitary, well
circumscribed mass. On cut section, the tumor is soft, homogenous, tan to gray with occasional foci of hemorraghe, cyst form, necrosis
Histo : The classic triphasic combination of blastemal, stromal and epithelial cell types.
Referrences
Robbins and Cotran. Pathologic basis of disease. 7th ed. Elsevier. 2005.
Rosai and Ackerman’s. Surgical pathology.9Th ed. Mosby. 2004.
Rubin's Pathology : Clinicopathologic Foundations of Medicine, 5th Edition. Lippincott Williams & Wilkins.2008.
www.pathconsult.com www.webpath.com www.pathblog.net
THANK YOU

















