Patient, Parent, and Staff Attitudes toward Allowing AdolescentPsychiatric Inpatients to Smoke
STUART L. KAPLAN, M.D., JOAN BUSNER, PH.D., EILEEN ROGERS, M.S.W.,AND EVELYN WASSERMANN, M.D.
Abstract. A smoking attitude survey was developed and administered to adolescent patients, parents, andstaff members at a psychiatric hospital for adolescents 6 months before and 6 months after the institution of apatient smoking ban. Attitudes before the ban were significantly more favorable toward allowing patient smokingthan attitudes after the ban; smokers were significantly more in favor of allowing patient smoking than nonsmokers ;and patients were significantly more in favor of allowing patient smoking than parents, who were significantlymore in favor of allowing patient smoking than staff (overall ps < 0.0001; post-hoc ps < 0.05). The findingssupport the feasibility of implementing smoking bans in adolescent inpatient facilities. J . Am . Acad. Child Adolesc.Psychiatry, 1990, 29, 6:925-928. Key Words: adolescent psychiatric inpatients, smoking, parent, staff attitudes.
In recent years, there has been a trend to ban smokingin general hospitals (Kelly and Cohen, 1979; Riffer, 1982;Andrews, 1983) as well as in other public places. Banningsmoking in psychiatric hospitals has come about more slowly(Campbell, 1976; Catford and Nutbeam , 1983). There aremany possible reasons for the reluctance to ban psychiatricpatients from smoking. There may be concern over negativeconsequences to psychiatric patients' emotional state thatmight arise from imposing nicotine withdrawal, such asincreased irritability, inability to concentrate, confusion,and anxiety (Hatsukami et al., 1984; Hughes and Hatsukami, 1986). In psychiatric hospitals, there may be practicalconcerns over enforcement issues, and there may be concernover patients' rights.
When the patients are children or adolescents, there maybe additional issues complicating the decision of whetherto ban smoking. Both parents and staff may have a strongersense of responsibility for supervising and controlling aspects of daily life of adolescent psychiatric inpatients compared to adult psychiatric inpatients . Some staff and administrators believe there is an ethical conflict in allowingadolescents in a hospital to engage in a behavior that isinjurious to their health. Parents ' wish that adolescents notsmoke may conflict with the wish of adolescents to smoke.
Several recent studies have measured patient and staffattitudes and compliance before and after the institution of
Accepted June 28, 1990.Dr. Kaplan is Executive Director, Rockland Children's Psychiatric
Center, New York State Office ofMental Health , and Associate ClinicalProfessor of Psychiatry, Columbia University College of Physiciansand Surgeons . Dr. Busner is Staff Psychologist , Rockland Children'sPsychiatric Center, New York State Office of Mental Health, andInstructor in Clinical Psychology in Psychiatry , Columbia UniversityCollege of Physicians and Surgeons. Mrs . Rogers is Social WorkSupervisor, and Dr . Wassermann is Staff Psychiatrist, both at Rockland Children's Psychiatric Center , New York State Office of MentalHealth.
Reprint requests to Dr. Kaplan, Rockland Children's PsychiatricCenter, Convent Rd. , Orangeburg , NY 10962.
smoking bans in adult psychiatric settings. These studieshave been remarkably consistent in their findings: in adultpsychiatric settings, smoking bans at several months followup are met with relatively little patient or staff resistance ordifficulty, despite patient and staffbefore the ban predictionsto the contrary (Resnick and Bosworth, 1989; Resnick etal., 1989; Smith and Grant , 1989).
The authors know of no examination of smoking bans inadolescent psychiatric facilities. The furor over allowing ornot allowing smoking for patients at the authors' own institution, an 80-bed public psychiatric hospital for childrenand adolescents , led the authors to develop and then administer to patients, parents, and staff a questionnaire thatassessed attitudes toward allowing patient smoking in thehospital. Six months after administering the questionnaire,the institutional policy was changed, from one that hadgranted limited smoking privileges to adolescents with parental permission, to one that completely banned smokingby patients inside or outside the building. The questionnairewas readministered 6 months after this change in policy inan effort to measure acceptance of the policy. To the authors' knowledge, this is the first study of patient, parent ,and staff attitudes toward allowing or not allowing smokingfor adolescent psychiatric inpatients .
Method
Subjects
At Time 1 (before the smoking ban), subjects were 3813- to 17-year-old patients , 16 parents of patients, and 96staff members of an 80-bed public psychiatric hospital forchildren and adolescents. At Time 2 (after the smoking ban;1 year later), subjects were 23 13- to 17-year-old patients,22 parents, and 83 staff members. The only selection criterion imposed on patients, other than willingness to participate , was that the patient not be overtly psychotic at thetime of questionnaire administration . No selection criteriawere imposed on parents. The only selection criterion imposed on staff was that staff be of disciplines that had directclinical interaction with the patients. Administrative, secretarial, maintenance, kitchen, and other staff with no reg-
925
KAPLAN ET AL .
ular patient contact were not asked to participate. Becauseof the short length of stay at the facility, none of the TimeI patients or parents were present at Time 2. Sixty percentof the Time 2 staff had completed the survey at Time 1.
Instruments
To assess attitudes toward allowing or not allowing patient smoking, patient , parent, and staff versions of a selfreport questionnaire were developed . The questionnaire(available from the authors) consisted of background information concerning smoking history and current smokingstatus of the respondent, 27 attitudinal items regarding bothethics of allowing or not allowing adolescent impatientsmoking (e.g., "hospitals should not promote an unhealthyactivity" and "not allowing smoking adds stress to an already stressful situation "), and the feasibility of allowingor not allowing adolescent inpatient smoking (e.g . , "if patients are allowed to smoke they will not participate in othermore beneficial program activities" and "if patients are notallowed to smoke they will spend a lot of time trying to getand smoke cigarettes") . The attitudinal items were rated on5-point, strongly agree to strongly disagree scales and wereworded such that the items that supported and opposedsmoking alternated.
Procedure
Subjects were told the surveys were designed to learnabout patients', parents', and staff's feelings about allowingsmoking for the adolescent patients at the hospital. Patientswere group administered the questionnaire on their livingunits; staff were group administered the questionnaires attheir individual departmental meetings; and parents wereindividually administered the questionnaires as they cameto the hospital for appointments or to visit their children.At Time 2, because only a small number of parents regularlycame to the hospital, parents who did not regularly visittheir children were sent the questionnaires, along with aself-addressed envelope . Approximately one third of thepatients came from long-term residential institutions and hadlimited parental contact. Employees not present at departmental meetings and night employees were left questionnaires in a central sign-in location. Participation was voluntary.
Response rates at Time 1 were 100% for patients on thethree adolescent units included in the study (N = 47), 100%for parents who came to the hospital (N = 17), and 64%for staff (N = 107). One patient was grossly psychotic andwas not asked to participate in the survey. At Time 2, onepatient on one of the three units that had been surveyed atTime 1 announced during the group-administered study description that he wasn't going to participate in anything thathe didn't have to participate in; upon hearing this, the otherpatients in the group promptly refused to participate as well,and no one on the unit was administered the questionnaires .The Time 2 patient response rate for the other two unitswas 100% (N = 26). Parent response rates at Time 2 were100% for parents who came to the hospital (N = 8), and31% for parents contacted by mail (N = 13); the staffresponse rate was 52% (N = 84). Nine Time 1 and three
926
Time 2 patient questionnaires and 11 Time 1 and one Time2 staff questionnaires were omitted from the data analysesbecause of incomplete responses. Subject numbers reportedin Subjects and Results sections of this paper reflect subjectnumbers after these omissions . No parent questionnaireswere omitted.
Results
Internal Consistency of the Smoking Attitude Survey
Cronbach's alpha of the 27 attitudinal items, collapsedacross respondent group and time, was 0.92. This highdegree of internal consistency allowed for combining theitems to obtain a single score that reflected general attitudetoward allowing patient smoking.
Respondent Smoking Status
At Time 1, 66% of patient respondents, 25% of staffrespondents, and 38% of parent respondents reported themselves to be smokers. At Time 2, 72% of patient respondents, 16% of staff respondents, and 32% of parent respondents reported themselves to be smokers (individual time Xgroup X2's NS). Thus, any differences in attitudes foundacross the two times cannot be attributed to differences insmoking rates across the two times.
Smoking Attitudes by Group, Time, and Smoking Status
A 2 (smoking status: smoker , nonsmoker) by 2 (time:before smoking ban, after smoking ban) by 3 (group: patient,parent, staff) analysis of variance (ANOVA) was performedon the average attitude scores. This was done to assesswhether attitude toward allowing patient smoking was related to own smoking status, whether the survey was conducted before or after the smoking ban, and whether therespondent was a patient, a parent , or a staff member.
All three main effects were significant. One main effectwas that smokers were more in favor of allowing patientsmoking than nonsmokers, F(I,266) = 92.62 p < 0.001.Another main effect was that attitudes before the ban weresignificantly more favorable toward allowing patient smoking than attitudes after the ban, F(1 ,266) = 13.69, P <0.0001. The third main effect was that patients were significantly more in favor of allowing patient smoking thanparents, who were significantly more in favor of allowingpatient smoking than staff, F(2,266) = 83.37, P < 0.0001,Student Newman Keuls post hoes ps < 0.05. Also, theinteraction of smoking status and whether the respondentwas a patient, a parent, or a staff member was significant,F(2,266) = 5.84, P < 0.003. The pattern ofthe interactionwas such that the difference between patient smokers andpatient nonsmokers , in terms of attitude toward allowingsmoking, was relatively greater than the difference betweensmokers and nonsmokers in the other two groups (staff andparents) . Finally, the three-way interaction of smoking status, time, and whether the respondent was a patient, a parent, or a staff member was significant, F(2,266) = 3.18,p < 0.04. The pattern of the interaction was such that thedecrease from before the ban to after the ban in patientsmoking endorsement seen in all of the groups was relatively
l .Am.Acad. Child Adolesc .Psychiatry ,29:6, November1990
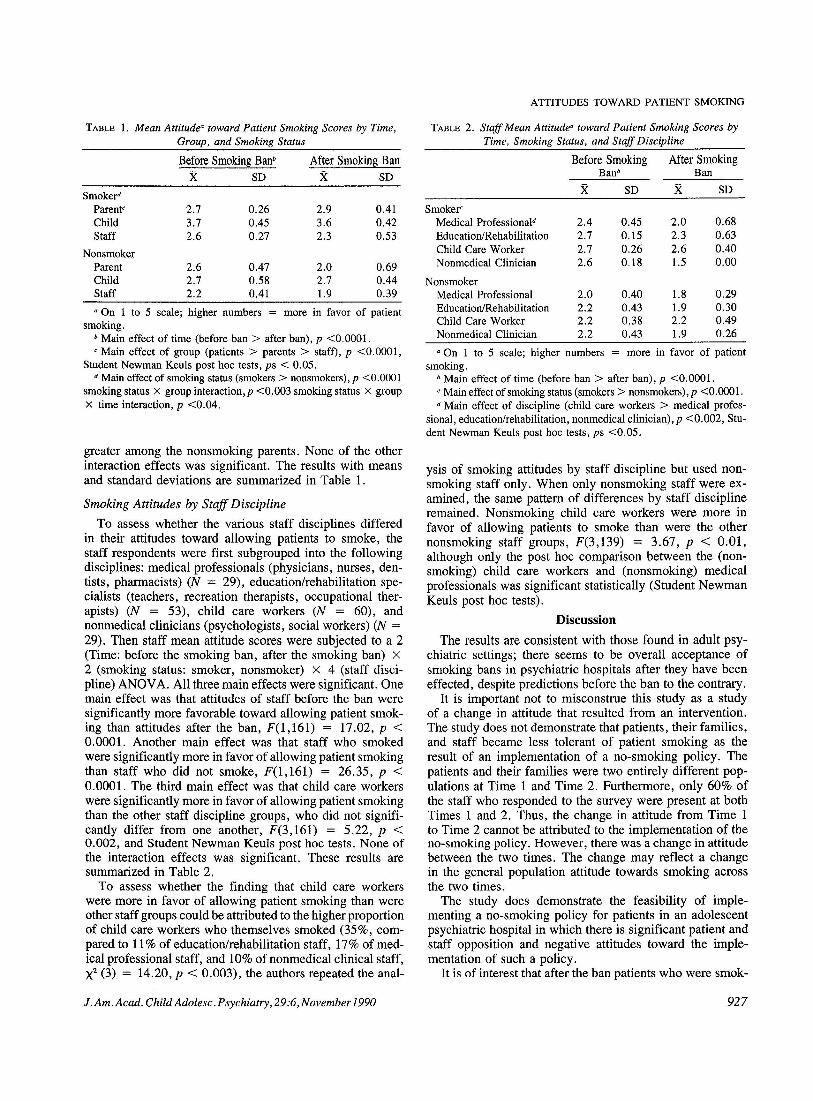
TABLE 1. Mean Attitude: toward Patient Smoking Scores by Time,Group, and Smoking Status
a On 1 to 5 scale; higher numbers = more in favor of patientsmoking.
b Main effect of time (before ban> after ban), p <0.0001.c Main effect of smoking status (smokers> nonsmokers), p <0.0001.d Main effect of discipline (child care workers> medical profes-
sional, education/rehabilitation, nonmedical clinician), p <0.002, Student Newman Keuls post hoc tests, ps <0.05.
greater among the nonsmoking parents. None of the otherinteraction effects was significant. The results with meansand standard deviations are summarized in Table 1.
Smoking Attitudes by Staff Discipline
To assess whether the various staff disciplines differedin their attitudes toward allowing patients to smoke, thestaff respondents were first subgrouped into the followingdisciplines: medical professionals (physicians, nurses, dentists, pharmacists) (N = 29), education/rehabilitation specialists (teachers, recreation therapists, occupational therapists) (N = 53), child care workers (N = 60), andnonmedical clinicians (psychologists, social workers) (N =29). Then staff mean attitude scores were subjected to a 2(Time: before the smoking ban, after the smoking ban) X2 (smoking status: smoker, nonsmoker) X 4 (staff discipline) ANOVA. All three main effects were significant. Onemain effect was that attitudes of staff before the ban weresignificantly more favorable toward allowing patient smoking than attitudes after the ban, F(1,16l) = 17.02, P <0.0001. Another main effect was that staff who smokedwere significantly more in favor of allowing patient smokingthan staff who did not smoke, F(l,161) = 26.35, p <0.0001. The third main effect was that child care workerswere significantly more in favor of allowing patient smokingthan the other staff discipline groups, who did not significantly differ from one another, F(3,16l) = 5.22, p <0.002, and Student Newman Keuls post hoc tests. None ofthe interaction effects was significant. These results aresummarized in Table 2.
To assess whether the finding that child care workerswere more in favor of allowing patient smoking than wereother staff groups could be attributed to the higher proportionof child care workers who themselves smoked (35%, compared to 11% of education/rehabilitation staff, 17% of medical professional staff, and 10% of nonmedical clinical staff,X2 (3) = 14.20, P < 0.003), the authors repeated the anal-
ysis of smoking attitudes by staff discipline but used nonsmoking staff only. When only nonsmoking staff were examined, the same pattern of differences by staff disciplineremained. Nonsmoking child care workers were more infavor of allowing patients to smoke than were the othernonsmoking staff groups, F(3,139) = 3.67, P < 0.01,although only the post hoc comparison between the (nonsmoking) child care workers and (nonsmoking) medicalprofessionals was significant statistically (Student NewmanKeuls post hoc tests).
Discussion
The results are consistent with those found in adult psychiatric settings; there seems to be overall acceptance ofsmoking bans in psychiatric hospitals after they have beeneffected, despite predictions before the ban to the contrary.
It is important not to misconstrue this study as a studyof a change in attitude that resulted from an intervention.The study does not demonstrate that patients, their families,and staff became less tolerant of patient smoking as theresult of an implementation of a no-smoking policy. Thepatients and their families were two entirely different populations at Time 1 and Time 2. Furthermore, only 60% ofthe staff who responded to the survey were present at bothTimes 1 and 2. Thus, the change in attitude from Time 1to Time 2 cannot be attributed to the implementation of theno-smoking policy. However, there was a change in attitudebetween the two times. The change may reflect a changein the general population attitude towards smoking acrossthe two times.
The study does demonstrate the feasibility of implementing a no-smoking policy for patients in an adolescentpsychiatric hospital in which there is significant patient andstaff opposition and negative attitudes toward the implementation of such a policy.
It is of interest that after the ban patients who were smok-
927
KAPLAN ET AL.
ers continued to strongly endorse allowing patient smoking .This raises the possible civil rights issue of denying thesepatients a freedom they would most likely exercise werethey not psychiatric inpatients. The issue is complicated inthat it is at present unknown whether adolescent patientsbenefit from an enforced smoking ban with regard to smoking reduction or cessation beyond hospital discharge . However, according to Feister (1990), adolescents in residentialtreatment facilities that allowed free access to cigarettesincreased their smoking rates substantially during their stay.Thus , allowing smoking for adolescent psychiatric patientsmay expose them to a risk over and beyond that to whichthey would be exposed were they not psychiatric inpatients.
Despite the fact that 67% of the adolescent patient respondents reported themselves to be smokers, and the factthat after the ban patients expressed the wish to be allowedto smoke, the patients in this study seem to have acceptedthe ban good-naturedly. Incidents surrounding obtaining orillicitly smoking cigarettes are few, and requests for nicotinegum or reports in the chart of patient complaints of nicotinewithdrawal are low.
As this survey demonstrated, child care staff had significantly more lenient attitudes than other staff groups towardallowing patient smoking both before and after the ban waseffected. The child care workers in this study are of lowersocioeconomic status (SES) than the other disciplines surveyed, and lower SES has been frequently reported to beassociated with greater prevalence rates of smoking (Fraumen, 1983; Sterling , 1983). However , the greater leniencyof child care workers toward patient smoking should not besimply attributed to their lower SES. The finding held evenwhen nonsmoking staff were examined , suggesting that itis more than simply increased smoking prevalence that mediates the effect. A possible explanation is that child careworkers may have been responding to concerns regardingtheir responsibility for enforcing the ban. Enforcing the banand dealing on a day to day basis with patients' complaintsor requests to smoke is almost exclusively in the purviewof this staff group. The burden for the direct responsibilityof enforcing the ban may, in part , account for the morelenient patient smoking attitude of the child care staff.
928
From an administrative perspective, surveying the staffmay have increased staff support for an administrative dictum that had been met with strenuous objections from thechild care staff. Although the authors have no data on thismatter , the simple act of having initially expressed interestin the views of the staff, via the administration of the smoking attitudes survey , may have increased later support ofthe ban.
The results of this study provide encouragement to thepsychiatric administrator faced with implementing a nosmoking policy for patients in an inpatient psychiatric settingfor adolescents.
ReferencesAndrews, J. L. (1983), Reducing smoking in the hospital : an effective
model program. Chest, 84:206--209.Campbell, D. (1976), Smoking policies in hospitals. Dimens. Health
Serv., 53:20-23.Catford, J. C. & Nutbeam, D. (1983), Smoking in hospitals . Lancet,
9:94-96.Fiester, S. J . (1990) , Adolescents smoking and psychopathology. Pre
sented at the 1990 Annual Meeting of the American PsychiatricAssociation, New York.
Fraumen, T . F. (1983) , The face of cancer in the United States. Hosp.Pract ., 18:81-96.
Hatsukami, D. K., Hughes, J. R., Pickens , R. W. &Svikis , D. (1984),Tobacco withdrawal symptoms: an experimental analysis. Psychopharmacology, 84:231-236 .
Hughes, J. R. & Hatsukami, D. (1986) , Signs and symptoms of tobacco withdrawal. Arch. Gen. Psychiatry. 43:289-294 .
Kelly, N. R. & Cohen, F. L. (1979), Smoking policies in U. S.hospitals: current status. Prevo Med ., 8:557-561.
Resnick, M. P. & Bosworth, E. E. (1989), A smoke-free psychiatricunit. Hosp. Comm. Psychiatry, 40:525-527.
-- Gordon, R. & Bosworth, E. E. (1989), Evolution of smokingpolicies in Oregon psychiatric facilities. Hosp. Community Psychiatry, 40:527-529 .
Rifferv J. (1982), Hospitals challenged to restrict smoking . Hospitals,16:20-24.
Smith, W. R. & Grant, B. L. (1989) , Effects of a smoking ban on ageneral hospital psychiatric service . Hosp . Community Psychiatry,40:497-502.
Sterling, T. (1983), Perceived versus actual risks: the problem ofmultiple confounding. In: The Analysis ofActual vs. Perceived Risks,eds. V. T . Covello , W. G. Flamm, J. V. Rodricks & R. G. Tardiff.New York: Plenum Press .
l.Am.Acad. Child Adolesc. Psychiatry,29:6, No vember 1990