65
Patient safety Dr. Mohamed Mosaad Hasan MD, CPHQ, MPH, CPPS, GBSS
| Date post: | 15-Jul-2015 |
| Category: |
Healthcare |
| Upload: | mohamed-mosaad-hasan |
| View: | 54 times |
| Download: | 1 times |
Patient safety
Dr. Mohamed Mosaad Hasan
MD, CPHQ, MPH, CPPS, GBSS
Patient Safety Definition
• “ The reduction and mitigation of unsafe acts within the health-care system, as well as through the use of best practices shown to lead to optimal patient outcomes.”
• Essentially, patient safety is about constantly working to avoid, manage and treat unsafe acts within the health care system.
Definitions
Patient safety practice is a type of process or
structure whose application reduces the probability of
adverse events resulting from exposure to healthcare
system.
Mistake-proofing is the use of process or design
features to prevent errors or the negative impact of
errors.

Evolving Issues
Taxonomy – how we categorize and group different
patient safety events.
Nomenclature – using a common and universally
accepted language
Patient Safety

Patient Safety Terms
Adverse Event
Medical Error
Sentinel event
Near Miss
Retrospective Analysis
Prospective Analysis
Identifying risks and processes before they happen
Bad outcome from care
Major and enduring loss of function
An examination of past events
Deficient process of care
Could have resulted in loss, injury or illness, but did not
Patient Safety: Challenges and
Concerns
Difficulty recognizing errors
Lack of information systems to identify errors
Relationship of trust with providers
Shortages of clinical professionals
Concern about liability
Limited capacity on how to use quality
improvement tools such as PDSA
Culture of patient safety is lacking
Some Reasons Why Errors Occur
System Factors
Complexity of healthcare processes
Complexity of health care work environments
Lack of consistent administration practices
Deferred maintenance
Clumsy technology
Human Factors
Limited knowledge
Poor application of knowledge
Fatigue
Sub-optimal teamwork
Attention distraction
Inadequate training
Reliance on memory
Poor handwriting
Not Who caused the accident but
What caused the accident?
“ We cannot change the human condition, but
we can change the conditions under which
human works.” (Reason 2000)
Adoption of this paradigm by leaders is the
beginning for culture change.

Trigger
s
DEFENSES
Accident
Regulatory
Narrowness
Incomplete
Procedure
s
Mixed
Messages
Production
Pressures
Responsibility
Shifting
Inadequate
Training
Attention
Distraction
s
Deferred
Maintenanc
eClumsy
Technology LATENT
FAILURES
Goal Conflicts
and Double
Binds
The
World
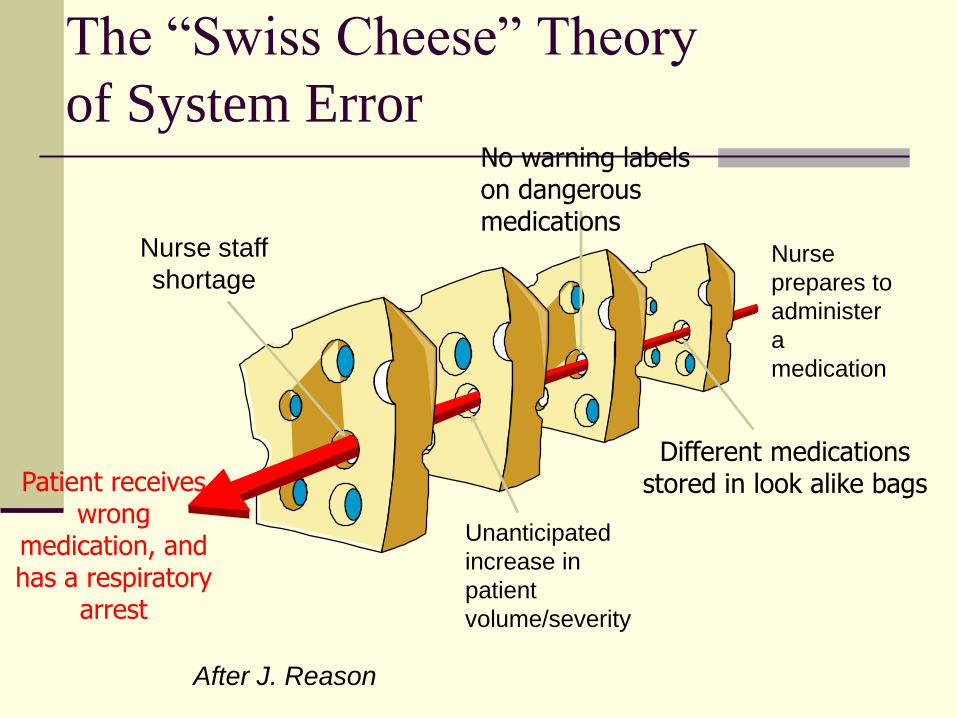
The “Swiss Cheese” Theory
of System Error
After J. Reason
Patient receives wrong
medication, and has a respiratory
arrest
Different medications stored in look alike bags
Nurse staff
shortage
No warning labels on dangerous medications
Nurse
prepares to
administer
a
medication
Unanticipated
increase in
patient
volume/severity
Patient Safety
Active Failures
highly visible errors with immediate consequences
Latent Failures
may be hidden for years and generally rooted in
organizational culture
takes the right set of circumstances for the error to
become visible or known

The Anatomy of Errors in Healthcare
Blunt End of the System
Sharp end
of the
System
Organizational Factors -
culture, policies,
procedures, regulations
Environmental Factors -
equipment, staffing,
resources, constraints
Human Factors - clinical
competency, communication
skills, problem solving skills
Culture of Safety
Indicate the extent to which you agree with following statements. Scoring: strongly disagree, neutral, agree, strongly agree.
A. Senior management provides a climate that promotes patient safety
B. If people find out that I made a mistake, I will be disciplined.
C. My supervisor/manager says a good word when he/she sees a job done according to established patient safety procedures
D. Discussion around major events focuses mainly on systems-related issues, rather than focusing on the individual(s) most responsible for the event.
Important issues facing healthcare
organizations.
Establishing culture of patient safety and just
culture.
Identifying organizational champions.
Deploying patient safety strategies.
Adoption of safety-related technologies.
Just culture
Balancing safety and accountability.
The single greatest impediment to error
prevention in the medical industry “that we
punish people for the medical mistakes”.
Just culture
3 basics:
1. It doesn’t reduce the personal accountability and
discipline. It emphasizes the learning from the errors
and near misses to reduce errors in the future.
2. The greatest error not to report a mistake. Thereby
prevent learning.
3. All in the organization to serve as safety advocates.
Both providers and consumers will feel safe and
supported when they report medical errors, near
misses and voice concerns about patient safety.
It has zero tolerance for reckless behavior.
Behaviors
Human error – inadvertent action: doing other than what should
have been done.
Manage through change in processes, procedures and training.
At risk behavior: behavioral choice that increase risk where risk
is not recognized or is believed to be justified.
Manage through increase awareness, and providing incentives
for healthy behaviors and disincentives for risky behaviors.
Reckless behavior: consciously disregard substantial and
unjustifiable risk.
Manage through Remedial and punitive action.
Red rules
cannot be broken
few in number
easy to remember
associated only with processes that can cause
serious harm to employees, customers, or the
product line.
must be followed exactly as specified except in rare
or urgent situations.
Every worker, regardless of rank or experience in the
company, is expected to stop the work or production
line if the red rule is violated.

Learning Organization
A learning healthcare system “is designed to
generate and apply the best evidence for the
collaborative healthcare choices of each
patient and provider; to drive the process of
discovery as a natural outgrowth of patient
care; and to ensure innovation, Quality,
Safety, and value in healthcare”IOM Roundtable on EBM
Patient Safety
Highly Reliable Organizations
Risk auditing: monitoring of activities to identify both expected and unexpected risks
Appropriate reward systems that encourage safety-related behavior
System quality standards
Acknowledgment of risk to learn from error
Flexible management model to promote teamwork and communication

Responsibilities of Governing
body to enhance patient safety
Setting aims
Getting data
Establishing and monitoring system-level
measures.
Change the environment, policies and
cultures.
Learning.
Establish executive accountability.

More Definitions
Never events: As defined by the National Quality
Forum, these are preventable events considered so
harmful that they should never occur. Also called
serious reportable events (SREs), they include
most medication errors as well as instances of
performing surgery on the wrong body part or the
wrong patient.
Complications of care: Healthcare-associated
complications, including infections that patients
develop while in the hospital, are thought to be
largely preventable.
Patient Safety
Communication and Teamwork Challenges
Healthcare is traditionally hierarchical
Personal communication styles of staff
Lack of common language – led to development of
SBAR
Addressed with other patient safety initiatives
Simulation training
Rapid Response Teams (RRT)
Walkroundstm
Patients participating on committees/RCAs
Patient Safety
Miscommunication: Breakdowns in
communication can result in the wrong
treatment, a lack of treatment, or incorrect
self-care by the patient. Miscommunication
can be the result of faulty systems (poor
methods of reporting critical test results, for
example); lack of attention to the health
literacy of patients; or a lack of cultural
competency on the part of the healthcare
team.

Disclosure
Implement a formal (transparent) policy
and process of disclosure of adverse
events to patients/families, including
support mechanisms for patients, family,
and care/service providers
Patient Safety: Disclosure
Reasons to Disclose
Right thing to do
Patients expect it
Professional responsibility
Earn trust/possibly forgiveness of patient
Supports patient safety initiatives
Required by The Joint Commission for
unanticipated outcomes

Patient Safety: Disclosure
Personnel Barriers to Disclosure
Fear of legal liability
Fear of loss of credibility and reputation
Fear of loss of licensure
Fear of punishment by organization or loss of job
Feelings of vulnerability
Difficulty in accepting role in error

Patient Safety: Disclosure
System Barriers to Disclosure
We’ve always done it this way
Hierarchical structure of medicine
Profession demands perfection
Struggle with accepting even most well trained and
competent can make mistakes
Conflict of Interest
Patient Safety: Disclosure
Michael Woods 4R’s
Recognition
Regret
Responsibility
Remedy

Patient Safety
Human Factors
Simplification
Standardization
Use of constraints and forcing functions
Reduce reliance on memory and vigilance
Use of protocols and checklists
Avoid or reduce fatigue
Heighten awareness of error prevention through
communication and training
Patient Safety
Mistake Proofing
Knowledge in the Head
Knowledge in the Environment

Patient Safety
Technology to Improve Patient Safety
CPOE
Barcoding
Robotics
Electronic medical records

International Patient Safety Goals
International Patient Safety Goals
Goal 1 Identify Patients Correctly
Goal 2 Improve Effective Communication
Goal 3 Improve the Safety of High-AlertMedications
Goal 4 Ensure Correct-Site, Correct-Procedure, Correct-Patient Surgery
Goal 5 Reduce the Risk of Health Care-Associated Infections
Goal 6 Reduce the Risk of Patient HarmResulting from Falls
Goal 1: Identify Patients Correctly
Rationale:
Wrong-patient errors occur in virtually all
aspects of diagnosis & treatment.
The intent for this goal is two-fold:
First, to reliably identify the individual as the
person for whom the service or treatment is
intended;
Second, to match the service or treatment to
that individual.
Requirement
Use at least two patient identifiers whenever
collecting laboratory samples or
administrating medications or blood products.
Acceptable identifiers may be the individual’s
name, an assigned identification number,
telephone number, photograph or other
person-specific identifier. (e.g. birth date)

Requirement
Prior to the start of any invasive procedure,
conduct a final verification process, (such as
a “time out”) to confirm the correct patient,
procedure and communication techniques.
Problems associated with surgical safety in
developed countries account for half of the
avoidable adverse events that result in death
or disability

Goal 2: Improve Effective
Communication
Rationale:
Ineffective communication is the most
frequent cited category of root causes of
sentinel events. Effective communication,
which is timely, accurate, complete,
unambiguous, and understood by the
recipient, reduces error and results in
improved patient/client/resident safety.

Requirement
Simply repeating back the order or test result
is not sufficient. Whenever possible, the
receiver of the order or test result enter it into
a computer, then read it back, and receive
confirmation from the individual who gave the
order or test result.

Requirement
“Critical test results” are defined by the
individual health care organization and will
typically include “stat” test, “panic value”
reports, and other diagnostic test results that
require urgent response.
Requirement
o Requirement: Standardize a list of
abbreviations, acronyms, symbols, and dose
designations that are not be used throughout
the organization.

Requirement
Implement a standardized approach to “hand
off” communications, including an
opportunity to ask and respond to questions.

Requirement
Measure, assess, and if appropriate, take action
to improve the timeliness of reporting, and
the timeliness of receipt by the responsible
licensed caregiver, of critical tests and critical
results and values.
Requirement
Reconcile Medications: Accurately and
completely reconcile medications across the
continuum of care.
Reconcile Medications
o Requirement: A complete list of the patient’smedications is communicated to the next provider ofservice when a patient is referred or transferred toanother setting, service, practitioner or level of carewithin or outside the organization. The complete listof medications is also provided to the patient ondischarge from the facility
Communication in Patient Care
Is not:
- Yelling
- Accusatory (angry)
- Being respectful of authority
Is:
- Focused on patient
- Nothing your perceptions
- Persistently raising concerns, intended tomove toward desired action
SBAR
A structured communication technique
designed to convey a great deal of
information in an organized & brief manner.
This is important as we all have different
styles of communicating, varying by
profession, culture, and gender.
SBAR
Situation
A concise statement of the problem
What is going on now
Background
Pertinent and brief information related to the situation
What has happened
Assessment
Analysis and considerations of options
What you found/think is going on
Recommendation
Request/recommend action
What you want done
SBA
R

Example SBAR briefing
55 YO Man with HTN, admitted for GI Bleed –
received 2 units, last hematocrite 31
VS: BP 90/50, Pulse 120
Looking pale, sweaty
Feels confused and weak, some problem with
heavy chest

Example SBAR briefing
Situation: Dr. Jones, I have a 55 Y/O Man who looks
pale, sweaty and is complaining of chest pressure.
• Background: He has a history of HTN, admitted for GI
Bleed received 2 units, last crit two hours ago was 31
vital signs are: BP 90/50, Pulse 120
• Assessment: I think he’s got an active bleed and we
can’t rule out an MI but we don’t have a troponin or a
recent H&H.
• Recommendation: I’d like to get an EKG and labs and
I need for you to evaluate him in right away.
Goal 3: Improve the Safety of High-
Alert Medications
Implementation Expectation
Remove concentrated electrolytes (including,
but not limited to, potassium chloride,
potassium phosphate, Nacl~0.9%) from
patient care units.
Standardize & limit the number of drug
concentrations available in the organization.

Requirement
o Identify and, at a minimum, annually review alist of look-alike/sound-alike drugs used bythe organization, and
take action to prevent errors involving theinterchange of these drugs.

Requirement
Label all medications, medication containers
(for example, syringes, medicine cups,
basins) or other solutions on and off the
sterile field.
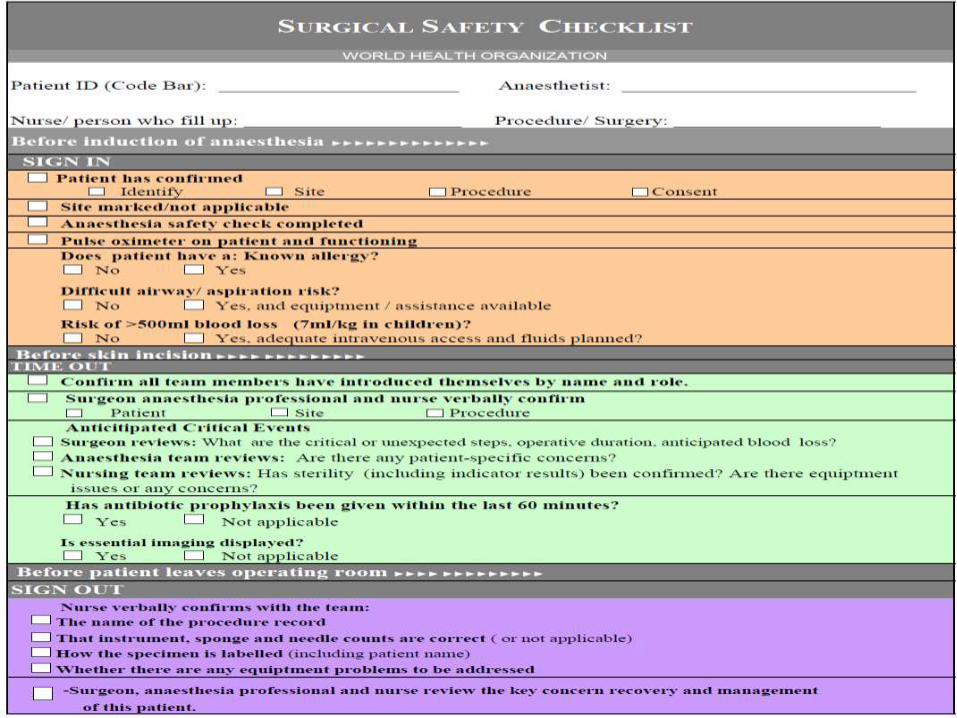
Goal 4: Ensure Correct-Site, Correct-
Procedure, Correct-Patient Surgery
Rationale
Wrong-site, wrong-patient, wrong-procedure
surgery can be prevented if appropriate
processes are in place.
The intent is to establish and implement
processes to always identify the correct site,
correct person and correct procedure.
Implementation Expectation
The requirement is for a “preoperative
verification process”. The checklist is an
example of one approach-the most common
one.
The intent of the requirement is to ensure that
all of the relevant documents are available
prior to the start of the procedure & that they
have been reviewed & consistent with each
other & with staffs’ understanding of the
intended site, patient, & procedure.
Goal 5: Reduce the Risk of Health
Care-Associated Infections
Rationale
At any given time, 1.4 million people worldwide suffer
from infections acquired in hospitals.
The risk of health care-associated infection in some
developing countries is as much as 20 times higher
than in developed countries.
Compliance with the CDC hand hygiene guidelines
will reduce the transmission of infectious agents by
staff to patients/clients/residents thereby decreasing
the incidence of healthcare associated infections.
Goal 6: Reduce the Risk of Patient
Harm Resulting from Falls
Rationale
Falls account for a significant portion ofinjuries in hospitalized patients, long-termcare residents, and home care recipients. Inthe context of the population it serves, theservices it provides, and its environment ofcare, the organization should assess, itspatient risk for falls and take action to reducethe risk of falling and to reduce the risk ofinjury, if a fall occur.
Implementation Expectation
As appropriate to the population served, the
services provided, and the environment of
care, a fall reduction program may include
risk assessment and periodic re-assessment
of individual patients or of the environment of
care.
Implementation Expectation
The program should include risk reduction
strategies involving patients/families in
education and environment of care redesign.
The program should also include
development and implementation of transfer
protocols (e.g., bed-to-chair), when relevant.

Question
The most important procedure to prevent
hospital acquired infection is :
1 . Using gloves
2 . Hand washing
3 . Wearing protective gowns
4 . All of the above
5 . None of the above
Question
For inpatient identification all of the
following Can be used except for :
1 . Patient room number
2 . Patient medical ID
3 . Patient full name
4 . Patient national ID
5 . None of the above


















