1 1 Neuromuscular disorders: Respiratory assessment and ventilatory management. In patients with Amiotrophic Lateral Sclerosis Joan Escarrabill MD Master Plan of Respiratory Diseases (PDMAR) Institut d’Estudis de la Salut Barcelona [email protected]Stressa, April 4th 2009
Transcript
11
Neuromuscular disorders: Respiratory assessment and ventilatory management.
In patients with Amiotrophic Lateral Sclerosis
Joan Escarrabill MDMaster Plan of Respiratory Diseases (PDMAR)
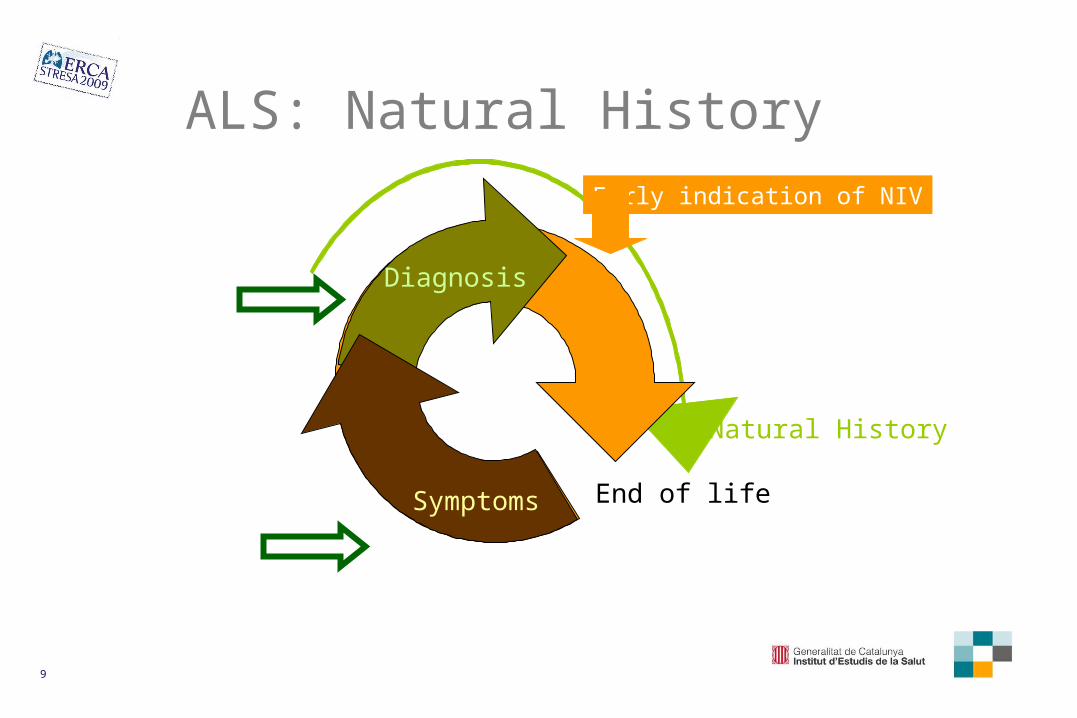
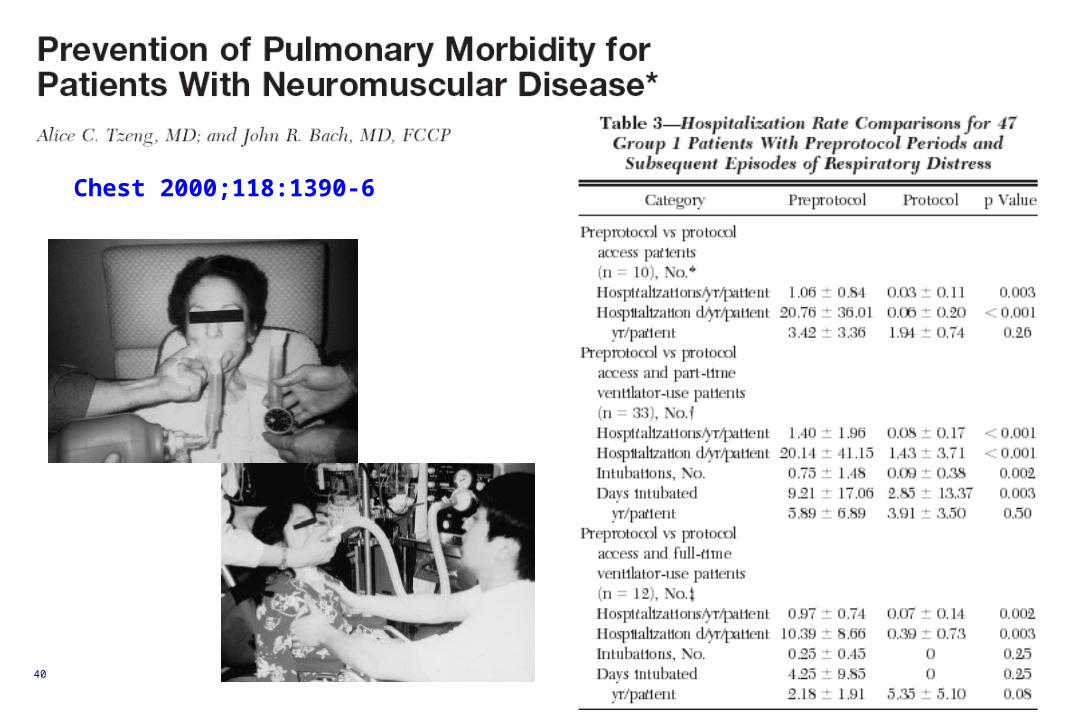
Early systematic respiratory evaluation is necessary to improve
the results of HMV in ALS
Survival in patients without bulbar involvement
Protocol
Pre-Protocol
13
Muscle strength vs Vital capacity
M. Estenne, 1991
14
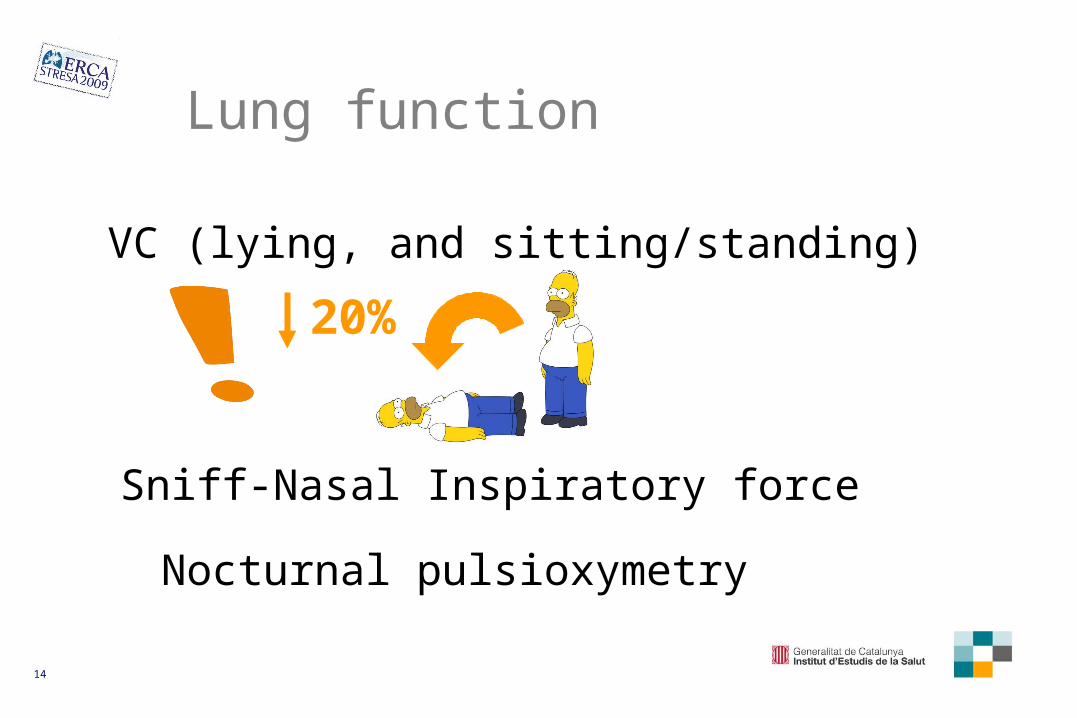
Lung function
VC (lying, and sitting/standing)
20%
Sniff-Nasal Inspiratory force
Nocturnal pulsioxymetry
15
Eur Respir J 2008; 31: 93–98
Many patients with neuromuscular disease find the PImax manoeuvre difficult to perform
-70 cmH2O in males or ,-60 cmH2O in females is unlikely to be associated with inspiratory muscle weakness
Sniff-Nasal Inspiratory force (SNIP)
16
Am J Respir Crit Care Med 2005;171:269–274
Kaplan-Meier survival curves based on the SNIF categories
17
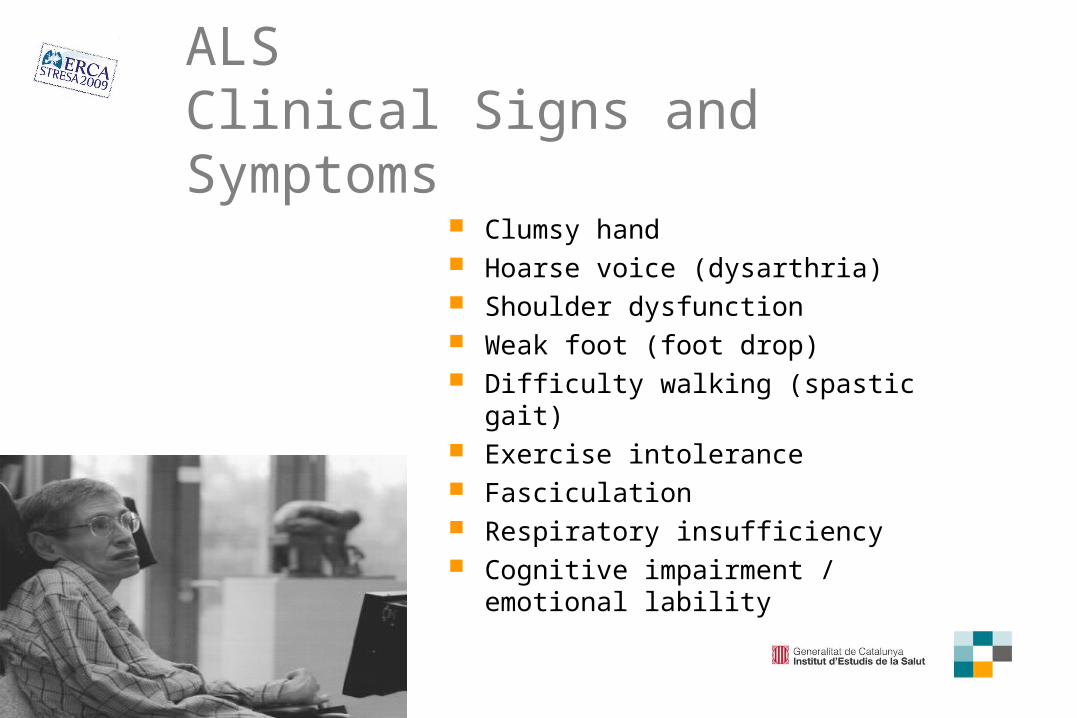
Lung & bulbar function:Signs and symptoms
Weight loss > 10%
Dysarthria
Dysphagia
Syalorrhea
Aspiration
Intolerance to supine position
Ineffective coughLung function
Bulbar function
18
ALS: 3 key words
Precocious Team
Package
19
Effective team It has a range of individuals who contribute in different
ways. Clear goals. Everyone understands the tasks they have to do. Coordinator There is a supportive, informal atmosphere. Comfortable with disagreement. A lot of discussion (Group members listen to each other) Feel free to criticise Learns from experience.
www.kent.ac.uk/careers/sk/teamwork.htm
20
The team produces more than the individual contributions of members.
21
Patient care team
Wagner. BMJ 2000;320:569-72.
R. Casas & P Romeu (1897)
22
Aiken L. NEJM 2003;348:164-6
Holistic vision
Better care related to coordination
Increasing role of non-physcian health professionals.
23
Mitsumoto H & Rabkin JG. JAMA. 2007;298:207-216
Care in multidisciplinary clinics is
associated with enhanced quality
of life by alleviating symptoms
and may extend survival
24
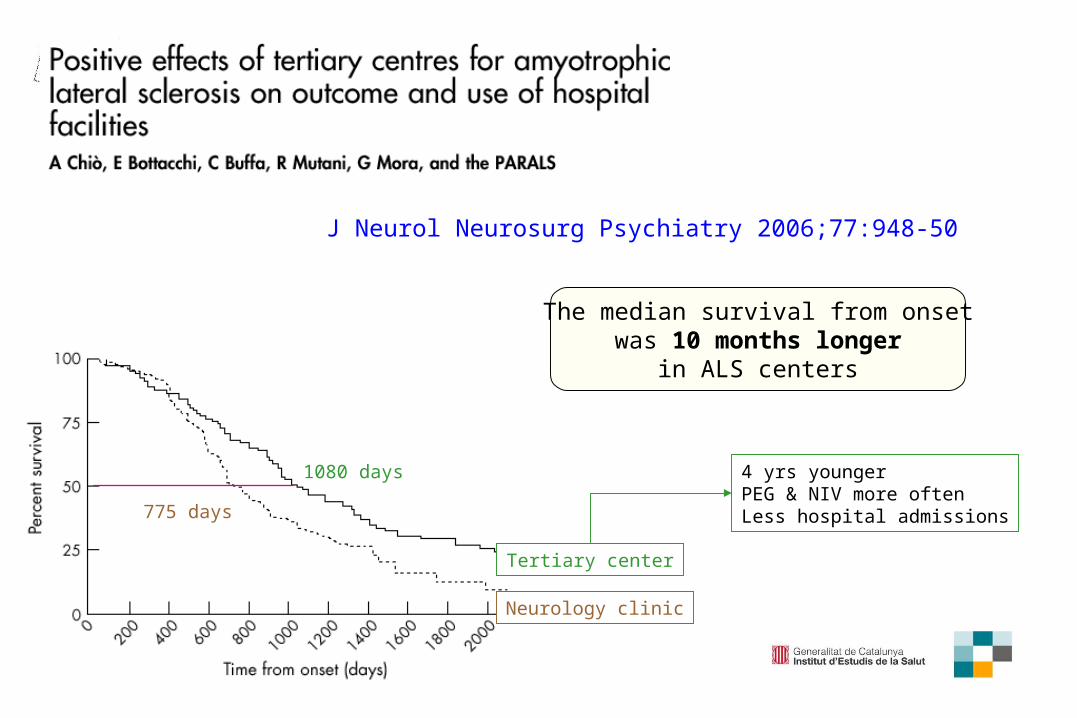
J Neurol Neurosurg Psychiatry 2006;77:948-50
Tertiary center
Neurology clinic
1080 days
775 days
The median survival from onsetwas 10 months longer
in ALS centers
4 yrs youngerPEG & NIV more oftenLess hospital admissions
25
www.has-sante.fr/
2003 17 Reference centers
CoodinationWorking groupsLocal organization
26
59%
41%
Ile de France Non ILD
Evalutaion of ALS reference centers
27
Survival of Irish ALS patients
One year mortality wasdecreased by 29.7%
Prognosis of bulbar onset patients was extended by 9.6 months
28
ALS patients who received their care at a multidisciplinary clinic had a better prognosis
Recruitment bias
ALS clinic treated a group of fitter ALS patients
General neurologistssaw all ALS patients
Living further from ALS clinicMore disabledIncreased ageBulbar onsetShorter duration of illness
Hutchinson M. J Neurol Neurosurg Psychiatry 2004;75:1208-12
29
Effect of referral bias
Sorenson EJ et al. Neurology 2007;68:600-602
132 subjectsTertiary center3 years.
Survival
p = 0.007
referral population
local
population
29 months 18 months
30
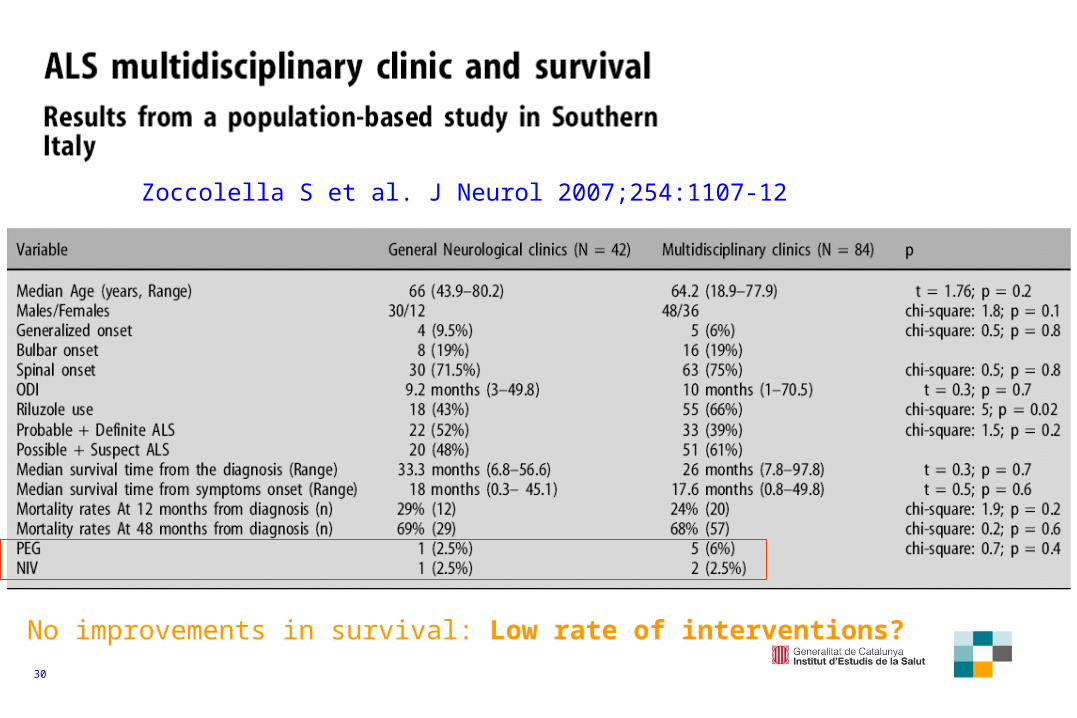
Zoccolella S et al. J Neurol 2007;254:1107-12
No improvements in survival: Low rate of interventions?
31
Home care organized through reference centers has many limitations
Complex organization, Distance, Response to emergencies
In most cases the reference center coordinates care but it can not assume direct care
32
Bias in the care of patients
Accessibility
Low rate of interventions
Distance
Referral Bias
33
ALS: Multidisciplinary Approach to Care
Neurologist Clinical/research nurse Dietician Speech/swallowing therapist Family/caregivers Psychologists General Practitioner Community nurse
Respiratory therapist Occupational therapist Social worker GI physician Support organizations Homehealth/hospice Pulmonologist Volunteer Helpers
Adapted from Leigh PN. J Neurol Neurosurg Psychiatry 2003;74(Suppl IV):iv32–iv47
34
Conclusions:
3 key words
Precocious Team
Package
35
ALS: Management
weakness fatigue nutrition dysphagia feeding tube dysarthria communication
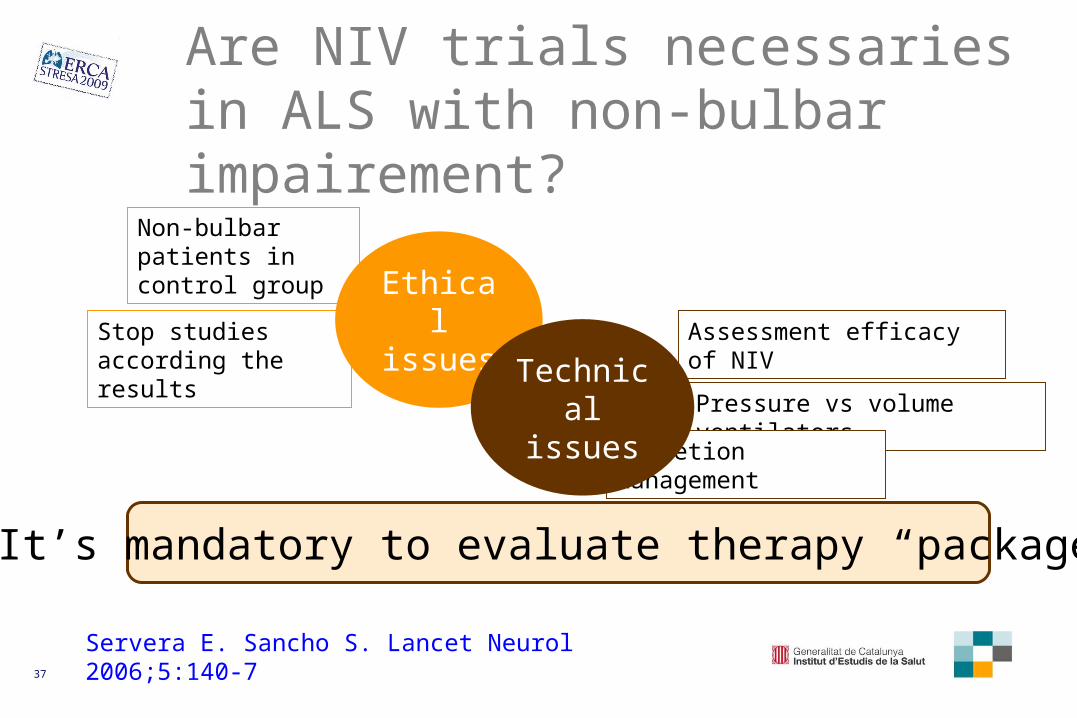
Are NIV trials necessaries in ALS with non-bulbar impairement?
Servera E. Sancho S. Lancet Neurol 2006;5:140-7
Non-bulbar patients in control group
Stop studies according the results
Assessment efficacy of NIV
Pressure vs volume ventilators
Secretion management
It’s mandatory to evaluate therapy “package”
Ethical issues
Technical issues
38
“Therapy package” in ALS
Mobility Swallowing &
Speaking
Coping with changes
Breathingchanges
Symptoms
Caregiver
Adapted from www.alsa.org/
39
Coping with changes = Accessibility to the team Symptoms control Non invasive ventilation (tracheo?) Mechanical assisted cough Daily living activities aids Communication devices Percutaneous endoscopic gastrostomy Caregiver support End-of-life issues
“Therapy package” in ALS
40
Chest 2000;118:1390-6
41
Chest 2002;122:92-98
NIV Mechanical assisted cough Oximetry as feedback
Delay the need for tracheotomy
42
Chest 2004;125:1400-5
PCFMIC > 4 L/sMI-E not generate greater PCF than manually assisted coughing
PCFMIC < 2.7 L/s Dynamic collapse of the upper airway during the exsufflation
43
Lung function
Sancho J. Chest 2004;125:1400-5
44
Caregivers’ perception of the impact of ALS on the patients, The duration of ALS, The coping strategies employed, Satisfaction with the support services available
The QoL of caregivers is a complex interaction between: