1 AN ABSTRACT OF THE DISSERTATION OF Erica G. Srinivasan for the degree of Doctor of Philosophy in Human Development and Family Studies presented on June 12, 2009. Title: Bereavement Experiences Following a Death Under Oregon’s Death With Dignity Act. Abstract approved: Patricia B. Moran Oregon residents with a terminal illness have had the option to use aid-in-dying under the Oregon Death with Dignity Act (DWDA) since 1997. The DWDA allows terminally ill Oregonians to make a request for lethal dosages of medication, prescribed by physicians for the purpose of self-administering to end one’s life. Many studies have been published on patient motivations for seeking hastened death, experiences of physicians, nurses, and hospice workers with persons who have died using aid-in-dying, and attitudes of the general public, medically ill persons, and healthcare professionals toward aid-in-dying, yet virtually no research has explored the experience of family members who have had a relative seek or use aid-in-dying. This qualitative study explored the bereavement experiences of persons who had a family member die using aid-in-dying during the past three years. Twenty-two participants were interviewed about their bereavement experiences using a structured interview. Interviews were recorded, transcribed, and analyzed using Grounded Theory methods. Themes that emerged from the data revealed that aid-in-dying allows for the
Transcript
1
AN ABSTRACT OF THE DISSERTATION OF
Erica G. Srinivasan for the degree of Doctor of Philosophy in Human Development and
Family Studies presented on June 12, 2009.
Title: Bereavement Experiences Following a Death Under Oregon’s Death With Dignity
Act.
Abstract approved:
Patricia B. Moran
Oregon residents with a terminal illness have had the option to use aid-in-dying
under the Oregon Death with Dignity Act (DWDA) since 1997. The DWDA allows
terminally ill Oregonians to make a request for lethal dosages of medication, prescribed
by physicians for the purpose of self-administering to end one’s life. Many studies have
been published on patient motivations for seeking hastened death, experiences of
physicians, nurses, and hospice workers with persons who have died using aid-in-dying,
and attitudes of the general public, medically ill persons, and healthcare professionals
toward aid-in-dying, yet virtually no research has explored the experience of family
members who have had a relative seek or use aid-in-dying.
This qualitative study explored the bereavement experiences of persons who had a
family member die using aid-in-dying during the past three years. Twenty-two
participants were interviewed about their bereavement experiences using a structured
interview. Interviews were recorded, transcribed, and analyzed using Grounded Theory
methods. Themes that emerged from the data revealed that aid-in-dying allows for the
2
opportunity to say goodbye to one’s loved one, and to plan and prepare for the death.
Grief was eased by knowing that aid-in-dying was the loved one’s choice, that the mode
of death was legal, and that love ones avoided prolonged suffering. Personal and family
agreement with loved ones decision to use aid-in-dying also eased grief. Conflict arose
from mixed feelings or disagreement with loved ones decision to use aid-in-dying. Grief
reconciliation from conflict included expressing feelings to others, religious support for
aid-in-dying, thoughts that the loved one’s death was imminent, thoughts that using aid-
in-dying was what the loved one wanted, and thoughts that the timing was appropriate
because had loved one’s health further declined they may have risked being able to meet
the law’s requirement to self-administer the prescription and would not have been able to
Bereavement Experiences Following a Death Under Oregon’s Death With Dignity Act
by Erica G. Srinivasan
A DISSERTATION
submitted to
Oregon State University
In partial fulfillment of the requirements for the
degree of
Doctor of Philosophy
Presented June 12, 2009 Commencement June 2010
5
Doctor of Philosophy dissertation of Erica G. Srinivasan presented on June 12, 2009
APPROVED:
Major Professor, representing Human Development and Family Studies Chair of the Department of Human Development and Family Sciences Dean of the Graduate School
I understand that my dissertation will become part of the permanent collection of Oregon State University libraries. My signature below authorizes release of my dissertation to any reader upon request.
Erica G. Srinivasan, Author
6
ACKNOWLEDGEMENTS
I would like to thank my committee members, Dr. Patricia Moran, Dr. Karen
Hooker, Dr. Rick Levenson, Dr. Larry Roper, and Dr. Sam Vuchinich, for their help,
support, and guidance. I am especially grateful for the help of my major professor,
Patricia Moran, who is always very gracious with her time, has offered me much
guidance and encouragement, and is a wonderful mentor.
Special thanks to George Eighmey and Yvonne Shaw of Compassion and Choices
of Oregon for the time and effort they devoted to this project. They were instrumental in
recruiting participants for this study. I am also grateful to all of the participants for
sharing their experiences with me so openly.
Many thanks to Bethany Chamberlin, who was such a wonderful support
throughout this process and was helpful in countless ways. I would also like to thank my
husband, David, and my family for always being so supportive and encouraging.
7
TABLE OF CONTENTS
Page
Chapter1: Introduction…………………………………. 2
Chapter 2: Literature Review………………………….. 4
Theory……………………………………………… 4
Attachment Theories…………………………… 4
Phase Models of Grief…………………………. 5
Task Theories…………………………………… 7
Grief Theories Related to Stress and Coping…… 8
Postmodern Model of Grief: Meaning…………... 9
Disenfranchised Grief …………………………… 10
Oregon Death With Dignity Act: History…………… 14 And Requirements
Demographics of persons who have died under Oregon’s Death with Dignity Act………………… 16 Arguments For and Against Aid-in-Dying……….. 19 Bereavement from Suicide…………………………… 23
Difference in Bereavement From Suicide Versus Bereavement From Other Types of Death…………………………. 26
Attitudes Towards Suicide …………………………. 31
Differences in Bereavement from an Anticipated Death Versus a Sudden Death……………………………… 32
8
TABLE OF CONTENTS (Continued)
Page Bereavement from Assisted Suicide…………………………… 35 Euthanasia and Bereavement in the Netherlands……………… 39 Chapter Three: Methods………………………………………… 42 Sample………………………………………………………… 42 Participant Recruitment and Informed Consent……………… 47 Data Collection………………………………………………. 48 Data Analysis………………………………………………… 49
Chapter Four: Results…………………………………………… 52 Theme 1: Common Grief Reactions and Grief Reconciliation… 52 Theme 2: Grief from Aid-in-Dying……………………………. 55 Theme 3: Saying Goodbye……………………………………. 58 Theme 4: Timing of Death……………………………………. 62 Theme 5: Agreement with Loved One’s Decision to Use Aid-in-Dying…………………………………………………… 64 Theme 6: Family Member Agreement with Decision and Impact on Grief………………………………………………… 69 Theme 7: The Impact of Aid-in-Dying Being Legal…………… 71 Theme 8: Experience of Death………………...……………….. 74 Theme 9: Anticipating Death…………………………………… 75 Theme 10: Death with Dignity Act Process……………………. 76 Theme 11: Expressing Grief…………………………………… 79 Theme 12: Grief Reconciliation from Aid-in-Dying…………… 80
9
TABLE OF CONTENTS (Continued) Page
Theme 13: Minimal Uncertain Feelings Over How to Act Or Behave Following a Death from Aid-in-Dying…………….. 81
Chapter Five: Discussion…………………………………………… 84 Common Grief Reactions, Grief Reconciliation, and Grief Theories………………………………………………….. 84 Grief from Aid-in-Dying Versus Sudden Death………………. 86 Grief from Aid-in-Dying Versus Suicide……………………… 87 Anticipatory Grief………………………………………………. 90 Grief from Aid-in-Dying Versus Grief from Anticipated Illness…………………………………………………………… 91 Grief Reactions and Grief Reconciliation After a Death from Aid-in-Dying……………………………… 91 Limitations……………………………………………………... 93 Benefits and Future Studies……………………………………. 96 References …………………………………………………….. 99
Appendices ……………………………………………………. 109
Appendix A: Informational Letter About the Study from Compassion and Choice of Oregon………………………… 109 Appendix B: Invitation Letter to Participate in Study…..….. 110
Appendix C: Informed Consent Document ………………… 111
Appendix D: Interview Protocol…………………………….. 114
10
LIST OF TABLES
Table Page
1 Characteristics and End-of-Life Care of 401 Death with Dignity Act Patients Who Died After Ingesting A Lethal Dose of Medication, By Year, Oregon, 1998 – 2008……………………………. 17 2 Participant Characteristics………………………………….. 43
3 Deceased Family Member Characteristics.……………………… 45
Bereavement experiences following a death under the Death with Dignity Act
Dissertation
Erica G. Srinivasan
Oregon State University
2
Chapter One
Introduction
Oregon residents with a terminal illness have had the option to request aid-in-
dying (formerly referred to in Oregon as physician assisted death or physician assisted
suicide) under the Oregon Death with Dignity Act (DWDA) since 1997. The DWDA
defines aid-in-dying as the “voluntary ending of life through self-administration of lethal
medications that have been prescribed by a physician for the purpose of dying” (Oregon
Department of Human Services, 2006, p. 7). This law has been met with much public
interest, controversy and legal challenges which has created a demand for research on
aid-in-dying and the DWDA. Many studies have been published on patient motivations
for seeking hastened death, experiences of physicians, nurses, and hospice workers with
persons who have died using aid-in-dying, and attitudes of the general public, medically
ill persons, and healthcare professionals toward aid-in-dying, yet virtually no research has
explored the experience of family members who have had a relative seek or use aid-in-
dying.
Because the Oregon Death with Dignity act is a law, there is an ethical duty to
investigate how those involved will be affected. There is good reason to believe that an
increasing number of families will experience the death of a loved one from aid-in-dying.
Aid-in-dying is also legal in Washington and Montana, although the law in Montana is
being challenged in the Supreme Court (O’Reilly, 2009). Arizona, California, and
Wisconsin have made legislative efforts to pass a law similar to Oregon’s Death with
Dignity Act (Compassion and Choices, 2008). Results from a U.S. Gallup survey among
3
475 adults who were asked “When a person has a disease that cannot be cured, do
you think doctors should be allowed by law to end the patient's life by some painless
means if the patient and his family request it?" indicate 72% support for aid-in-dying
(Carroll, 2007, p.1). Understanding the experience of grieving a death from aid-in-dying
has potential to assist persons who are considering this option and their families. For
example, being able to forewarn family members of feelings common to this experience
may help them to feel less isolated and better understood.
The purpose of this study is to explore the bereavement experience of persons
who have had a family member use aid-in-dying under the Oregon Death with Dignity
Act. This research topic is significant for several reasons. Few studies have been
published on grief following a death from aid-in-dying and in all of these studies the
exploration of grief was minimal. Many studies have been published on the
characteristics of grief from a suicide and the characteristics of grief from a terminal
illness so it is possible to compare their similarities and differences. The degree to which
grief from aid-in dying has characteristics that are similar to suicide or terminal illness is
unknown.
Few qualitative studies have been conducted on aid-in-dying. Qualitative research
could reveal new understandings and complexities of aid-in-dying that empirical studies
are unable to uncover. Additionally, this study will make a contribution to literature on
grief and bereavement.
4
Chapter 2
Literature Review
Theory
Bereavement is defined as “the state or condition caused by loss through death”
(Cavanaugh & Blanchard-Fields, 2006, p. 487). Grief is viewed as the feelings and
reactions that are experienced after a loss; it is the response to bereavement. There is no
fixed definition or agreement of grief responses experienced and the time course of grief,
however it is generally accepted that grief reactions can have physical, emotional,
cognitive, behavioral, psychological and spiritual components (Dent, 2005) and that is a
multi-dimensional, individualized process (Hooymen & Kramer, 2006; Kalischuk &
Hayes, 2004). Earlier grief theorists tended to view grieving as a linear process that
involved passing through stages or phases (Averill, 1968; Kalischuk & Hayes, 2004;
Kübler-Ross, 1969; Martocchio, 1985; Parkes, 1970) and often emphasized breaking
bonds with the deceased, while contemporary theorists acknowledge grieving as a
dynamic process, explore different contextual variables of grief such as stress, meaning,
and social factors, and emphasize the importance of continuing bonds with the deceased
as part of the grief process.
Attachment theories
Freud (1957) has been attributed with developing the first influential theory of
grief. He introduced the concept of griefwork, which is work following a death that
involves accepting the reality of the loss and detaching from the original attachment to
the person who died. This process involves dealing with feelings and memories
5
associated with the deceased person and dealing with the need to want to stay attached to
the deceased person. According to Freud, those who can accept the loss and let go of
attachment can return to a normal, functioning life, while those who are unable to accept
the loss will continue to experience difficulties with reintegrating back to their lives
Bonnano and Kaltmen’s (1999) four-component model also acknowledges the
role of stress and coping. Their model is unique in that it allows for understanding of
individual differences of grieving (Friedman & Silver, 2007). The four components are 1)
The context of loss, which address factors such as the type and timing of death, age and
gender of the bereaved person, and cultural and social factors 2) subjective meanings
associated with the loss, 3) changes in the representation of the relationship with the
deceased person which involves redefining the relationship and maintaining a connection
with the deceased and 4) coping and emotional regulation as it relates to the stress
associated with loss. In this framework, it is believed that recovery from the loss is more
9
likely when negative emotions associated with grief are minimized and positive emotions
are enhanced. As with other grief theories, expressing grief is an important part of the
process (Bonnano & Kaltman, 1999; Friedman & Silver, 2007).
Postmodern model of grief: meaning
In contrast to models of grief that focus on detaching from the deceased and
passing through phases and completing tasks, postmodernists view finding meaning as
central to the grief process. Giles and Neimeyer (2006) describe in their emerging model
of meaning reconstruction in bereavement a process that includes making sense of the
loss, finding benefits from the loss while still dealing with sorrow and pain, and identity
change, which can involve personal growth, continuing bonds with the deceased, and
new views of the world. This perspective incorporates some of the ideas from earlier
theories, however the main focus is on meaning as it relates to the grief process
The above mentioned theories all provide a framework for understanding how
grief is expressed, conceptualized, how different factors affect grief, and what tasks are
involved with coping and adjusting to life. Theorists such as Giles and Neimeyer and
Stroebe and Schut provide additional insight about the role that meaning and stress play
respectively in resolving grief. All of the theories have in common that loss from a death
creates a disruption in one’s current state of equilibrium which leads to experiencing a
range of emotions, and that resolving grief involves a process that takes time (Hooyman
& Kramer, 2006). Death from a legal physician assisted suicide is a “new” type of death.
Therefore the grieving process and which theory precisely applies is unknown. It is
possible that a new theory may need to be developed to adequately address grief
following a legal physician assisted suicide, but it is likely that aspects of the discussed
10
theories will be helpful in informing this study. One aspect of the grief process that many
theories fail to fully incorporate/address is the social aspect of grief and how social
factors affect the grief process. Doka’s (1989) emerging theory of disenfranchised grief
provides a sociological perspective on grief and shows how social factors can affect grief.
Physician assisted suicide is a topic that has received much social attention and social
critique. For this reason it is important to explore disenfranchised grief.
Disenfranchised Grief
Society has standards or rules for how people are expected to behave and feel after
a death and how one is expected to express grief (Doka, 2002). According to Doka,
societal norms for grief “govern what losses one grieves, how one grieves them, who can
legitimately grieve the loss, and how and to whom others respond with sympathy and
support (Doka, 2002, p.6). Disenfranchised grief refers to the type of grief experienced
following a loss that “is not or cannot be openly acknowledged, publicly mourned, or
socially sanctioned” (Doka, 1989, p. 4). According to Doka, when grief is
disenfranchised or “hidden” emotions associated with normal grief can be intensified,
complicating grief, and subsequently the healing process can be prolonged. Clinicians
and researchers have found that social support and open communication, or being able to
directly talk about grief with others, is a factor related to better bereavement outcomes
and resolving grief (Doka, 2005; Powers & Wampold, 2008). This implies that normal
grief reactions are complicated when grief is disenfranchised because social support and
open communication, which facilitate mourning, are diminished. Disenfranchised grief
both inhibits a person from fully expressing their feelings related to the loss and can limit
social support if others are not aware of the loss. For example, in the case of aid-in-dying,
11
survivors may not feel like they can tell others about the circumstances of the death due
to the controversies over aid-in-dying and as a result might not receive support or fully
express their grief.
Doka describes five categories of losses that can be disenfranchised. The first
category of loss is “The Relationship is not Recognized” (p. 10). Relationships that are
not publicly recognized or socially accepted can fall into this category, such as
homosexual relationships, or relationships of unmarried people who are living together.
The second category of loss is “The Loss is Not Acknowledged” (p.11). This category
includes losses which society may not acknowledge as being significant. Doka gives loss
through abortion as an example and explains that in this case the loss might not be
acknowledged because others might not know that an abortion occurred, or might not
acknowledge the loss because they do not approve of abortion, or that those who approve
of the act might “minimize the sense of loss” (p.11). A loss from physician-assisted
suicide could fit into this category for the same reasons given in the abortion example.
“The Griever is Excluded” (p.13) is the third category of loss and refers to situations
where the bereaved person is viewed as not being capable of grief and as a result does not
receive social recognition of their loss or their need to grieve. Doka gives the example of
persons with developmental disabilities and the young and very old as types of people
who are socially excluded from grief. The fourth category is “Circumstances of Death”
(p. 14). The nature of the death might make the bereaved person feel constrained in
asking for support or the nature of death could make other hesitant to give support.
Deaths such as a suicide or AIDS-related death are some examples where the bereaved
report feeling a sense of stigma and receiving limited support. Doka also illustrated
12
disenfranchised grief based on circumstances of loss involving an assisted suicide. A man
named John who had attended a workshop given by Doka wrote him a letter afterwards
describing the disenfranchised grief he experienced when participating in an assisted
suicide. John’s mother had terminal breast cancer and wanted to hasten her death by
using a lethal use of morphine. It is unclear how the morphine was administered, but
clear in the letter that the family was all in agreement and did help with assisting in their
mother’s death. This assisted death happened in Minnesota, where assisted suicide is not
legal. John described his disenfranchised grief:
Our extended family came to know and affirm how mom died. We had to let most everyone else believe that it was just an extraordinary coincidence that everyone was at her side. There’s enormous dissonance when you feel that you have mislead friends about the truth-when you don’t think you did anything wrong-when there is no shame or guilt. The “normal grief” of losing a parent was further aggravated by a sense that there are some in society that would disapprove of her decision or feel it was improper or even criminal for us to assist…(p. 16) As illustrated in John’s example it is possible that disenfranchised grief as related to
circumstances of loss could be experienced by those who had a family member die under
the DWDA because these survivors may not feel they can openly acknowledge their grief
due to the public controversy over the Oregon Death with Dignity Act and assisted death
and to stigma that suicide survivors report experiencing (Dunn & Morrish-Vidners, 1998;
Fielden, 2003).
A research study conducted on disenfranchised grief and family members of death
row inmates also further supports Doka’s theory (Jones & Beck, 2006 – 2007).
Qualitative interviews with 26 family members of death row inmates revealed that stigma
associated with having a family member on death row kept participants from telling
others about their loss. Participants who did tell others about their loss reported that
13
people responded with negative comments, which resulted in disenfranchised grief.
Mothers of death row inmates reported withholding information regarding the death from
young children, aging parents, or children with developmental disabilities. This relates to
Doka’s third category. (The griever is excluded” (p. 14)), however in the cases presented
in the study, children, older adults and people with developmental disabilities were
viewed as capable of grief, but were excluded from details of the loss as it was believed
that the grief would be too much too handle.
The last type of disenfranchised grief concerns the way people grieve. “Certain
cultural modes of expressing grief, such as stoicism or wailing, may fall beyond the
grieving rules of a given society and thus be disenfranchising” (p. 14).
While many factors can contribute to grief, the emerging theory of
disenfranchised grief is helpful for understanding the experience of grief among aid-in-
dying survivors. Although not all factors involved with bereavement are addressed by
this theory, it serves as a guide to develop interview questions and to explore the
bereavement experience. Other discussed grief theories will also be considered when
developing interview questions. As previously stated, no single theory can be utilized for
this study, but concepts from all of the theories are helpful in understanding the
bereavement experience.
Review of Literature
The Literature Review will begin with a description of the history and
requirements of the DWDA, demographics of those who have used the DWDA, and
arguments for and against aid-in-dying. These topics are important background to this
14
study because grief experiences occur within a societal context that is strongly
opinionated about aid-in-dying.
A death from aid-in-dying could be conceptualized as a type of death that is both
a suicide and an anticipated death from a terminal illness, as those who died under the
DWDA voluntarily ended their own life and were required to have a terminal diagnosis.
Thus I will review studies on 1) bereavement from a suicide, 2) how grief from a suicide
differs from grief from a terminal illness and other types of death, 3) social attitudes
towards suicide 4) how grief from an anticipated death differs from grief from a sudden
death, and 5) grief after a loss from aid-in-dying. The final section of the literature review
discusses studies on euthanasia and physician assisted suicide conducted in the
Netherlands where these practices have been accepted and practiced for many years.
Oregon Death with Dignity Act: History and Requirements
The Oregon Death with Dignity Act was first passed in 1994, with 51% in support
of DWDA. No one utilized the Act, however, because a legal injunction was
immediately imposed by opponents of the Act. In 1997 Oregonians were asked to vote on
repealing the Death with Dignity Act. The measure to repeal failed, with 60% in support
of the DWDA (Patel, 2004). After the failed effort to repeal the measure, the injunction
was immediately lifted and people began utilizing the Act. The DWDA was challenged
again in November of 2001 when Attorney General John Ashcroft issued the “Ashcroft
Directive” which stated that the Department of Justice had reversed its former decision,
that prescribing controlled substances under the DWDA did not violate the Controlled
Substance Act. A four-month restraining order was issued against the Ashcroft Directive
and, in April 2002, the U.S District Court issued a permanent injunction, blocking the
15
Ashcroft Directive and retaining the Oregon Death with Dignity Act. In 2004 Ashcroft
filed an appeal to the U.S. Supreme Court to allow authorization from the Federal
Controlled Substance Act to the Department of Justice to override states’ rights in
determining the legitimate use of medications. In 2006 the U.S Supreme court ruled
against Ashcroft’s appeal and Oregon’s Death with Dignity Act remains in effect today
(Compassion and Choices, 2008).
Requirements
In order to request a prescription for lethal medications one must be a) 18 years of
age or older, b) a legal resident of Oregon, c) defined as capable of making and
communicating healthcare decisions, d) diagnosed with a terminal illness with a life
expectancy of 6 months or less (Oregon Department of Human Services, 2006).
Extensive guidelines exist for receiving the prescription for the lethal medication.
The guidelines below are from Oregon’s Department of Human Services (2006) report on
the DWDA:
• “The patient must make two oral requests to their physician, separated by at least 15 days” (p.1).
• “The patient must provide a written request to his or her physician, signed
in the presence of two witnesses” (p.1). • “The prescribing physician and a consulting physician must confirm the
diagnosis and prognosis” (p.1). • “The prescribing physician and a consulting physician must determine
whether the patient is capable” (p.1).
• “If either physician believes the patient’s judgment is impaired by a psychiatric or psychological disorder, the patient must be referred for a psychological examination” (p.1).
• “The prescribing physician must inform the patient of feasible alternatives
to DWDA, including comfort care, hospice care, and pain control” (p.2)
16
• “The prescribing physician must request, but may not require, the patient
to notify their next-of-kin of the prescription request” (p.2).
Additionally, the act requires that physicians must report all prescriptions for
lethal medication to the Oregon Health Division, and pharmacists must be informed of
the prescribed medication’s intended use. The Act also requires that the Oregon Health
Division monitor and collect information on aid-in-dying use in Oregon.
Demographics of persons who have died under the DWDA.
Reports on the DWDA indicate that 401 persons died under the DWDA between
1998-2008 (Oregon Department of Human Services, 2008). Slightly more men than
women have been DWDA patients (53.1%). The majority of DWDA patients have been
older adults, with 28.4% between the ages of 65-74, and 27.9% between the ages of 75-
84. The majority of DWDA patients were Caucasian (97.5%,) married (46.1%), highly
educated, with a baccalaureate degree or higher (43.9%), and held residence in western
Oregon counties (42.4%) or the Portland metro area (42.1%). The underlying illness that
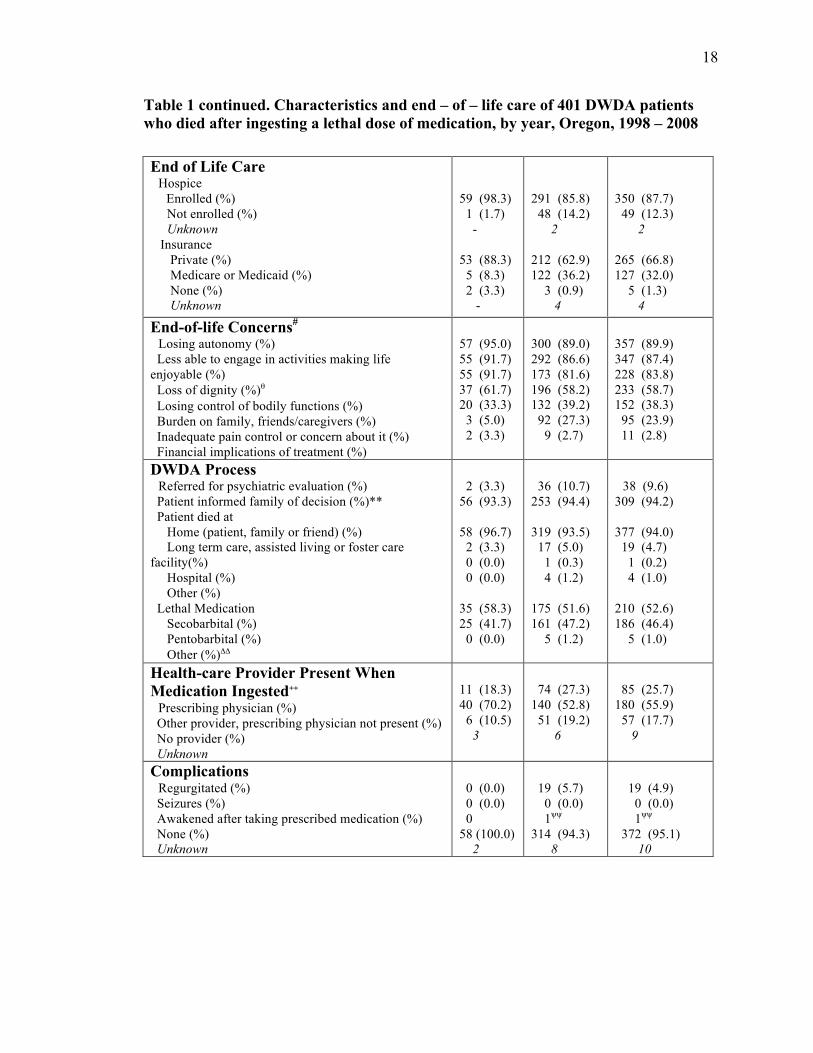
most DWDA patients had was cancer (81.8%). See table 1 for a more detailed summary
of the demographics of persons who have died under the DWDA between 1998-2008,
and for isolated percentages of the demographics of person who died under the DWDA
in 2008 (Oregon Department of Human Services, 2008).
17
Table 1. Characteristics and end – of – life care of 401 DWDA patients who died after ingesting a lethal dose of medication, by year, Oregon, 1998 – 2008 Characteristics 2008
(N = 60) 1998-2007 (N = 341)
Total (N = 401)
Sex Male (%) Female (%)
N (%)* 30 (50.0) 30 (50.0)
N (%)* 183 (53.7) 158 (46.3)
N (%)* 213 (53.1) 158 (46.9)
Age 18-34 (%) 35-44 (%) 45-54 (%) 55-64 (%) 65-74 (%) 75-84 (%) 85+ (%) Median years (range)
Table 1 continued. Characteristics and end – of – life care of 401 DWDA patients who died after ingesting a lethal dose of medication, by year, Oregon, 1998 – 2008
End of Life Care Hospice Enrolled (%) Not enrolled (%) Unknown Insurance Private (%) Medicare or Medicaid (%) None (%) Unknown
End-of-life Concerns# Losing autonomy (%) Less able to engage in activities making life enjoyable (%) Loss of dignity (%)θ Losing control of bodily functions (%) Burden on family, friends/caregivers (%) Inadequate pain control or concern about it (%) Financial implications of treatment (%)
DWDA Process Referred for psychiatric evaluation (%) Patient informed family of decision (%)** Patient died at Home (patient, family or friend) (%) Long term care, assisted living or foster care facility(%) Hospital (%) Other (%) Lethal Medication Secobarbital (%) Pentobarbital (%) Other (%)ΔΔ
Health-care Provider Present When Medication Ingested++ Prescribing physician (%) Other provider, prescribing physician not present (%) No provider (%) Unknown
Table 1 continued. Characteristics and end – of – life care of 401 DWDA patients who died after ingesting a lethal dose of medication, by year, Oregon, 1998 – 2008 Emergency Medical Services Called for intervention after lethal medication ingested (%) Calls for other reasons (%)## Not called after lethal medication ingested (%) Unknown
Timing of DWDA Event Duration (weeks) of patient-physician relationship Median Range Unknown Duration (days) between prescription written and death Median Range Minutes between ingestion and unconsciousness Median Range Unknown Minutes between ingestion and death Median Range (minutes-hours) Unknown
* Unknowns are excluded when calculating percentages. ∆ Clackamas, Multnomah, and Washington counties. Ω As only form of health insurance coverage. ψ Includes alcoholic hepatic failure, corticobasal degeneration, diabetes mellitus with renal complications, hepatitis C, organ-limited amyloidosis, scleroderma, Shy-Drager syndrome, multiple sclerosis, and meningioma. ## Calls included three to pronounce death and one to help a patient who had fallen off a sofa.# Affirmative answers only ("Don't know" included in negative answers). Available for 17 patients in 2001. ℮ First asked in 2003. ++ The data shown are for 2001-2008 since information about the presence of a health care provider/volunteer, in the absence of the prescribing physician, was first collected in 2001. ψψ In 2005, one patient regained consciousness 65 hours after ingesting the medications, subsequently dying from their illness 14 days after awakening. The complication is recorded here but the patient is not otherwise included in the total number of DWDA deaths. ** First recorded beginning in 2001. Since then, 12 patients (3.7%) have chosen not to inform their families and 7 patients (2.1%) have had no family to inform. ∆∆ Other includes combinations of secobarbital, pentobarbital, and/or morphine.
Arguments for and against aid-in-dying
The arguments for and against aid-in-dying revolve around autonomy, religion,
pain/suffering, professional integrity, and societal consequences. Supporters of aid-in-
dying use the argument that autonomy is central to American law, thus patients should be
allowed to exert free choice and make their own decision regarding their death (Ersek,
20
2004; Rosenfeld, 2004; Scherer & Simon, 1999). Arguments against the autonomy
principle have a religious or philosophical basis. Western religious arguments assert that
it is immoral for humans to take their own lives and the decision to end life should be left
to God (Campbell, 2000; Ersek, 2004). Eastern philosophies argue that engaging in aid-
in-dying would defy the sacredness of life (Campbell, 2000).
Supporters of aid-in-dying argue that it is a compassionate means to end pain and
suffering for terminally ill patients. They further point out that not all pain can be
completely controlled, that patients may have difficulty communicating the intensity of
pain, and that pain medication could put a person in an unconscious or non-functioning
state, which, supporters argue, is almost equivalent to being dead (Scherer & Simon,
1999). Another argument in support of aid-in-dying is the view that “when the burdens of
life outweigh the benefits because of uncontrollable pain, severe psychological suffering,
loss of dignity, or loss of quality of life as judged by the patient, and when the
circumstances are not remediable, the dying person should be able to ask for and receive
help in assisted suicide” (American Psychological Association, 2001, p.1). In response to
these beliefs, opponents argue that allowing patients to choose aid-in-dying as an end to
suffering is equivalent to abandoning patients, as medical treatments and palliative care
can relieve pain (Ersek, 2004; Rosenfeld, 2004; Scherer & Simon, 1999). They also point
out that requests for aid-in-dying could indicate that there is a need to improve palliative
and hospice care, pain management, and psychological and social support (American
Psychological Association, 2001). Reports from those who used the DWDA between
1998-2008 show that 23.9% listed inadequate pain control or concern about it as an end
of life concern, while the highest listed end of life concerns were losing autonomy
21
(89.9%), less able to engage in activities making life enjoyable (87.4%) and loss of
dignity (83.8%) (Oregon Department of Health, 2008). Supporters of aid-in-dying might
interpret these percentages as indicative of pain and suffering, while opponents might
interpret percentages as not meeting the needs of those with a terminal illness.
Arguments for aid-in-dying regarding professional integrity are related to the
issue of pain. The professional integrity principle in support of aid-in-dying claims that
not allowing a doctor to prescribe means to end suffering destroys trust between the
doctor and patient. Opponents of this principle argue that aid-in-dying violates the
Hippocratic oath that many doctors swear allegiance to, which prohibits aid-in-dying
(Ersek, 2004; Rosenfeld, 2004). In response to this argument, supporters of aid-in-dying
point out that in aid-in-dying, the doctor is not ending the patient’s life, but that the
patient is the one who takes the medicine to end his or her life (American Psychological
Association, 2001). Another argument against aid-in-dying related to professional
integrity is that misdiagnoses and mis-prognoses do occur and new treatments are found,
and if this is the case, a death from aid-in-dying may have occurred unnecessarily
(American Psychological Association, 2001).
The argument most commonly cited against aid-in-dying in the literature regards
societal consequences and is referred to as the “slippery slope”. The slippery slope
argument is that there is risk of expanding the criteria of who is eligible for aid-in-dying.
For example, opponents fear that the criteria may be extended to people with a
psychiatric disorder, or a non-terminal illness, as has happened in a few cases in the
Netherlands, where both aid-in-dying and euthanasia are legal. These cases in the
Netherlands have been challenged. The criteria for who is eligible for aid-in-dying in the
22
Netherlands is unclear as their act does not specifically limit the option of aid-in-dying to
persons with a terminal illness, but states that aid-in-dying or active euthanasia is an
option for those who perceive their suffering as unbearable (Rosenfeld, 2004). Opponents
also fear that the option of aid-in-dying might encourage a cultural view that the dying
process should be hastened for all persons and that end of life decisions and care could be
influenced as a result. Additionally, opponents feel there is risk of vulnerable groups
choosing aid-in-dying to avoid being a burden to families, or to avoid financial burdens
(Ersek, 2004). Reports from the ODDA from 1998-2008 do show that 39.2% of those
who used the act listed “Burden on family, friends/caregivers” as one of their end-of-life
concerns and 2.7% listed “financial implications of treatment as one of their end-of-life
concerns (Oregon Department of Health, 2007). It is important to note that these are not
necessarily the reasons that people choose to request or use aid-in-dying (although it is
possible it could have been) but that it was one of their concerns. Those advocating for
aid-in-dying challenge the slippery slope argument with the position that with
legalization of aid-in-dying comes safeguards that can protect against risk to vulnerable
groups, such as the requirement in Oregon’s DWDA that limits the option of aid-in-dying
to only the terminally ill (Ersek, 2004). They also point out that end of life options such
as withholding or withdrawing treatment are legally supported with safeguards
(American Psychological Association, 2001).
Bereavement from suicide
Studies on suicide indicate that guilt, anger, fear, depression, self-blame, and
shame, and role uncertainty are common emotions associated with grief post-suicide
(Dunn & Morrish-Vidners, 1988; Fielden, 2003; Range & Calhoun, 1990; Van Dongen,
23
1993) and that suicide survivors may also experience complicated grief (Mitchell et al,
2004). Suicide survivors may also experience a lack of support and feel or perceive
stigma from others (Dunn & Morrish-Vidners, 1998; Fielden, 2003).
Using interviews with 24 people from the San Francisco Bay Area (7 males and
17 females) who were survivors of suicide for five years or less, Dunn and Morrish-
Vidners (1988) analyzed accounts of responses to the suicide, perceptions of others’
response to the suicide, and experiences of personal changes following the suicide. The
sample consisted of 7 spousal survivors, seven parent survivors, 2 child survivors, and 8
sibling survivors. Participants’ initial responses described feeling shock, disbelief, fear,
anger, helplessness, guilt and shame. They also described feeling rejected and abandoned
by their loved one. Participants described needing emotional and moral support, but
receiving a lack of support. Support was provided primarily from a few close friends.
Conflict tended to arise in families over blaming each other for the suicide. Friends and
acquaintances who were either unable or unwilling to discuss the suicide either distanced
themselves or cut off relationships with survivors. Survivors reported that they felt anger
towards the person who died. Survivors also reported feeling anger when others who
they told about the suicide responded with inappropriate behavior, such as blaming the
survivor, having a revolted expression, or being completely silent. The authors speculated
that the responses of others may have been in response to the behavior of the survivor, as
some participants described difficulty with expressing their grief and socially
withdrawing as they anticipated awkwardness or stigma from others. When participants
were asked if they felt stigmatized by others, most responded that they did not, however
over 80% of the participants reflected experiencing stigma when describing feelings such
24
as being embarrassed, or ashamed in reference to talking about how others acted and their
own bereavement. In terms of changes within self, participants described having lower
self-esteem and self-confidence, more depression, and less trust in others. Positive
changes included being more sensitive to others problems, reconnecting with religion and
family and shifting focus to their own mental health.
Fielden (2003) found similar experiences from her research with 6 suicide
survivors (5 parents, and 1 sister) who had been bereaved between 2-9 years. In-depth
interviews revealed that survivors experienced feelings of shock, disbelief, emptiness,
fear and guilt. Participants also described experiencing blame and stigma from some
family members and others in the community. They felt embarrassment and difficulty
when trying to explain the nature of the death to others, which resulted in avoidance of
people. Although participants described avoiding others, they also felt that others avoided
them either because they did not know what to say, or because others could not accept the
nature of the death.
In a quantitative study, Mitchell, K., Prigerson, H., and Mortimer-Stephens, M
(2004) assessed 60 persons within one month of a family member committing suicide for
complicated grief using the Inventory of complicated grief. Complicated grief is a newly
proposed disorder, not yet included in the DSM-IV. The criteria include being bereaved
by death, preoccupation with the person who died (such as searching for that person),
efforts to avoid memories of the deceased, feelings of hopelessness, shock,
meaninglessness, extreme anger or irritability, feelings that part of oneself is missing or
died, difficulty imagining living a life without the deceased and accepting the death,
harmful behaviors, and a “shattered worldview”(Jacobs et al, 2000, p. 189; Mitchell et
25
al., 2004). Results indicated that children (80%), spouses (77.8%), parents (66.7%),
siblings (57.1%), in-laws, (27.8%) and friends or co-workers (14.3) all experienced
complicated grief.
In order to assess concerns related to bereavement, needs for assistance and
attempts to seek support following a suicide, Provini & Everett (2000) examined self-
reports completed by next-of-kin (adult relatives) to someone who had committed
suicide. Participants reported having bereavement concerns related to difficulties in the
family, such as difficulties with maintaining routines and roles and providing emotional
support for one another (65%), co morbid stressors, such as poor physical health,
financial difficulties, or not being able to participate in traditional funeral services at
church due to the mode of death (62%), grief reactions such as depression, anxiety, anger
and guilt, and having difficulties following daily routines (54%), and unresolved
bereavement, including difficulties in expressing grief and discussing the circumstances
of the death (38%). In terms of needs for assistance, participants indicated that they had
needs for professional help such as therapy (81%), needs for help with issues related to
bereavement such as resolving grief and telling others about the nature of the death
(43%), and needs for more emotional support from family members (38%). While 72%
of participants desired formal assistance from professionals, and 16% desired informal
help from friends and family, only 47% received formal help, while 41% received
informal help. The barriers mentioned to seeking help included disagreements in the
family over if assistance was needed, language difficulties, and lack of time, finances, or
transportation.
26
Van Dongen (1993) interviewed 35 survivors of suicide on their social
relationships and perceived social support 3-9 months after the suicide occurred.
Participants consisted of 10 men and 25 women between the ages of 25-68 years. The
majority of participants were bereaved parents (17), and the remaining participants were
bereaved siblings (8), bereaved adult children (5), and bereaved spouses (5). Initially,
survivors openly discussed the suicide with family members, but after some time
survivors stopped expressing concerns to family members because they perceived that
family members were emotionally exhausted and they did not want to add to their
emotional pain. Participants reported receiving strong social support, yet also described
friends and relatives as seeming uncertain in how to behave towards survivors. Although
few participants felt stigmatized, most experienced anger and frustration over others not
understanding their grief and not wanting to listen. Survivors also experienced feelings of
uncertainty over their role as a suicide survivor in terms of whom they could talk to, how
they should act, and whether they could be honest about their feelings.
Differences in bereavement from suicide versus bereavement from other types of death
Quantitative studies that compare bereavement from suicide to other types of
death have produced mixed results in terms of grief differences. The majority of studies
indicate some overlap in the grief process, while also uncovering grief reactions that are
unique to suicide. The main differences in the experience of suicide survivors compared
to other bereaved groups, found in both quantitative and qualitative studies, were having
feelings of embarrassment, rejection, abandonment, being punished, self-blame, guilt,
shame, being treated differently by others, and receiving less community support (Barrett
27
& Scott, 1990; Harwood et al., 2002; Houck, 2007; Range & Calhoun 1990; Seguin et al.,
1995; Silverman et al., 1995).
Barrett and Scott (1990) compared suicide survivors with survivors of accidents,
unanticipated natural deaths, and expected natural deaths (terminal illnesses). Twelve
men and 45 women between the ages of 24-48 were interviewed 2-4 years after the death
of a spouse. Participants completed the Grief Experience Questionnaire, a measure
designed to compare bereavement in suicide vs. non-suicide and The Purpose-in-Life
Test, a measure designed to assess survivors quality of Reinvolvement. Results indicated
that, in addition to experiencing normal grief reactions, suicide survivors and those who
experienced a death from non-natural causes also experienced stigma, shame, and
abandonment, and feelings that the death was preventable. Suicide survivors and those
who had experienced any type of sudden death also reported feeling blamed for the death,
taking responsibility for the death, and searching for a meaning. Suicide survivors
uniquely reported feeling rejected, feeling embarrassed over mode of death, lying about
the mode of death, wondering about their spouse’s motivation for not living longer, and
feeling as if their deceased spouse was trying to get even with them by committing
suicide. Overall, suicide survivors experienced more grief reactions than other survivors,
but the course and quality of recovery from grief were not different than other groups.
De Groot et al. (2006) examined self-reports of psychiatric and general health of
150 relatives of 74 people who had committed suicide and 70 relatives of 39 people who
had natural deaths after three months of being bereaved. This study was conducted in the
Netherlands. The authors found that the self-reported psychiatric and general health of
those who had a relative die from suicide was worse than those who had a relative die
28
from a natural death. Those who had been bereaved from a suicide scored higher on
scales of loneliness, depression and complicated grief. Participants were also asked to
report if they felt an unmet need for professional help. Those bereaved from a suicide
scored higher on feeling a need for professional help even after adjusting for
“expectedness of death, sociodemographic differences, and relatives’/spouses’
neurotocism” (p.418).
Harwood et al. (2002) examined grief experiences of 85 friends and family
members ranging in age from 23-85 years of persons who were 60 years of age or older
when they committed suicide. Grief reactions were compared with a control group of 46
persons who were bereaved by the natural death of an older adult. Relationships to the
deceased were as followed: 38 children, 17 friends, 16 spouses, 9 siblings, and 5 other
relatives. The researchers administered the Grief Experience Questionnaire and the
Montgomery and Asberg Depression Rating scale. They found that depression scores
were similar in both groups and that suicide survivors scored higher on scales measuring
stigmatization, shame, sense of rejection, and unique grief reactions (unique grief
reactions was not defined).
Houck (2007) compared grief reactions in cancer (n=50), HIV/aids (n=50), and
suicide (n=50) bereavement among family members who had been bereaved for 3
months-5 years. The sample consisted of 105 women and 45 men ranging in age from 19-
79 years. The relationship to the deceased was as follows: children (24%), spouses
(21%), siblings (15.4%), parents (13.6%), close friends (10.5%), and life-partners (7.4%).
Participant grief was measured using the Grief Experience Questionnaire. In contrast to
other studies, results indicated that those in the suicide group and the cancer group scored
29
similarly on the measure of stigmatization and those in the HIV/AIDS groups
experienced higher levels of stigma. Those in the suicide group scored higher than the
other two groups on unique reactions to suicide and their average on the questionnaire
was higher than the other two groups, which may indicative of experiencing more intense
grief.
Range and Calhoun (1990) interviewed 57 college students (15 men and 42
women), ranging in age from 18-36 years, who had had a friend or relative die by suicide
(n=11), accident (n= 17), homicide (n=3), natural anticipated death (n=13), or natural
unanticipated death (n=13) within the past year. The students were interviewed about
their reactions and how others treated them. Results indicated that suicide survivors and
survivors of accidental deaths felt pressure from others to explain the cause of death.
Suicide survivors were unique compared to other groups in that they perceived less social
supports, and reported being treated differently by others. Another difference in those
bereaved from suicide compared to other groups was that almost half of the suicide
survivors lied about the cause of death.
In order to study differences between suicide and other types of death in terms of
long term bereavement, Range and Niss (1990) examined results from questionnaires on
social support, impact of death, recovery from grief, and current mood that they had
administered to college students who had been bereaved for more than 2 years from
either a suicide, homicide, accidental death, natural anticipated death, or natural
unanticipated death. Participants were matched on age, gender, and length of
bereavement. No differences were found between the groups, which indicated that over
30
time, the experience of bereavement from a suicide is similar to the experience of
bereavement from other types of death.
Silverman et al. (1994) surveyed 55 college students (42 women, 30 men) who
were bereaved within five years from a suicide (n=9), homicide (n=9), natural anticipated
death (n=12), and natural unanticipated death (n=12), and accident (n=16) on their
perception of social support, and grief and distress reactions. Bereavement from suicide
was associated with more intense grief reactions compared to the other groups. In
contrast to other studies, Silverman et al found that all groups were similar on measures
of social support and distress reactions.
Jordan et al (2001) conducted an assessment of literature on suicide in order to
assess if suicide bereavement is different than other types of bereavement. He concluded
that suicide bereavement is different in terms of certain aspects of grief (such as more
feelings of guilt, blame, and abandonment, and more questions concerning meaning-
making), social processes that influence grief (such as feelings of stigma, tendency of
survivors to withdraw, negative responses from others), and the impact on family (such
as more difficulties in the functioning of the family).
Bailley et al (1999) surveyed 350 university students who were survivors of
suicide (n=34), accidental death (n=57), unanticipated natural death (n=102, or
anticipated natural (n=157) death using the grief experience questionnaire, impact of
event scale, and Texas revised inventory of grief. Participants also responded to a
questionnaire that contained questions related to grief. The authors found that suicide
survivors scored higher than other groups on experiencing feelings of rejection,
responsibility, unique grief reactions, and total grief reactions and also had increased
31
levels of shame and perceived stigmatization. Additionally they found that factors such as
whether the death was natural or not considered natural, or expected or unexpected had
less influence than the mode of death.
Attitudes towards suicide
In their comparison study of thoughts about social reactions to suicidal death,
accidental death, and death from natural causes, Calhoun et al’s (1984) provides support
for the perceived feelings of stigmatization and negative social responses to those
bereaved from a suicide. They interviewed 23 females and 12 males from an
undergraduate population at mid-sized university in the southeastern region of the United
States who knew someone who was bereaved by suicide about that person’s bereavement
experience and compared their responses to responses of those who knew someone who
was bereaved by an accident and bereaved by natural causes about those bereavement
experiences. Participants reported higher discomfort levels with suicide survivors than
survivors from an accidental death or death by natural causes when rating interactions
with expressing sympathy to and talking to survivors at a funeral.
Attitudes about the social acceptability of suicide differ based on reasons for
committing suicide. Deluty (1989) presented in a questionnaire to 455 college students
one of seven fictional scenarios in which a man had decided to kill himself, followed by
questions about the situation and the man’s decision. In five of the scenarios, the man had
chronic severe depression. These scenarios differed in terms of the description of
depression. In the sixth scenario the man had chronic, severe pain, and in the seventh
scenario the man had a terminal illness. Results indicated that suicide was viewed as
more acceptable when it occurred in response to a terminal illness.
32
These studies show that while there is an overlap between the characteristics of
grief after a suicide and grief following other forms of death, there are also unique
characteristics of grief following a suicide. Overall, grief following a suicide is
particularly difficult. One study indicated that there is greater public acceptance when
the suicide is in response to a terminal illness.
Differences in bereavement from an anticipated death vs. sudden death
Family members who had a relative die under the DWDA may or may not have
known prior to death that their loved one was using physician assistance to die, as the
DWDA does not require those seeking or using assistance to inform others. Overall, 3.7%
of those who have used the DWDA have not told family members (Oregon Department
of Human Services, 2006). Family members who did have knowledge of their loved
one’s decision to use physician assistance to die may have different grief experiences
from those who experienced the death as sudden. It is important to understand the grief
reactions from both an anticipated death and a sudden death as bereaved family members
may have experienced either type of death.
One body of research indicates that a forewarned or anticipated death allows
families to deal with unfinished business, say good-byes, and prepare for the upcoming
loss which results in easing the intensity of grief after the death occurs (Rando, 1984;
Zisook, 2000). In contrast, research on anticipatory grief has also been found to have
negative outcomes for bereavement. Still other studies have presented mixed findings, or
reported no relationship between anticipatory grief and bereavement outcomes (Reynolds
and Botha, 2006). One reason for the differences in findings might be due to the
conceptualization of anticipated death. Many researchers have the incorrect assumption
33
that those who are anticipating a death have fully accepted the terminal diagnosis and are
preparing for their loved one’s death (Reynolds & Botha, 2006). Another reason for
differences is inconsistency in operational definitions of anticipatory grief. One approach
to studying outcomes of bereavement based on anticipatory grief is to examine the
duration of the deceased person’s illness. Many studies have used this approach, however
they all use different durations of illness to define anticipatory grief. Other studies look at
different aspects of anticipatory grief, and thus have different definitions of anticipatory
grief, which produces misleading results. Methodological issues are another reason for
contradictions in findings. For example, some studies use open-ended questionnaires,
while others use an Anticipatory Grief inventory, or interviews. Other methodological
issues concern the questionable validity of instruments intending to measure anticipatory
grief and the failure to control for factors in the dying process related to anticipating
death (such as caregiver stress) (Botha, 2006; Carr &Utz, 2002). It is important to keep
these critiques in mind when reviewing studies of anticipatory death.
Most studies on sudden deaths describe grief reactions from different types of
sudden death, and were described in the section of the literature review on bereavement
from suicide versus other types of death. The purpose of those studies was to differentiate
between different types of sudden death rather than describe the grief experience
following a sudden death. Some studies have specifically explored grief following a
sudden traumatic death, but again, in these studies aspects of grief related solely to the
suddenness of death were not explored. Thomson (1990a) found that grief reactions
following a sudden death or suicide include “irritability, sleep disturbance, anxiety, startle
Residence Portland Metropolitan Counties (%) Willamette Valley (%) Central (%) Central Coast (%) Columbia Gorge (%) Southern Oregon (%) Not Disclosed (%)
Relationship to deceased Spouse/partner: husband (%) Spouse/partner: wife (%) Daughter (%) Sister-in-law (%) Son (%)
6 (27.3) 10 (45.5) 3 (13.6) 2 (9.1) 1 (4.5)
Time since bereaved 6 month-1 year (%) 1-2 years (%) 2-3 years (%)
9 (40.9) 4 (18.2) 9 (40.9)
44
Table 3 describes the characteristics of participants’ loved ones who died using
aid-in-dying. Participants’ loved ones consisted of 9 females and 13 males, varying in age
from 42-91, with the majority between the ages of 61-70. Twenty-one of the deceased
family members were Caucasian, and one person had a mixed racial background. Similar
to participants, religious backgrounds varied, with the majority belonging to no defined
organized religion (40.9%). Participants’ loved ones were largely from the Portland, or
greater Portland area (63.2%), with others from Central Oregon, Central Coastal Oregon,
Southern Oregon, Columbia Gorge, and the Willamette Valley. Education levels ranged
from having a high school degree to having completed some graduate work or holding
graduate degrees. The majority had a Bachelor’s degree (40.9%). Relationships to the
bereaved participants included spouse/partner (husband or wife), mother, father, sister-in-
law, and brother-in-law, with 10 in the category of spouse/husband. Underlying illness
included cancer of various kinds (N=18), Amyotrophic lateral sclerosis, and Multiple
Systems Atrophy.
45
Table 3. Deceased Family Member Characteristics (N=22) Characteristic N(%) Age 42-50 (%) 51-60 (%) 61-70 (%) 71-80 (%) 81-91 (%)
N(%) 1 (4.5) 3 (13.6) 8 (36.4) 6 (27.3) 4 (18.2)
Sex Female (%) Male (%)
9 (40.9) 13 (59.1)
Race Caucasian (%) Mixed (%)
21 (95.5) 1 (4.5)
Education High school Some college (%) Baccalaureate (%) Some graduate school or higher (%) Unknown (%)
5 (22.7) 3 (13.6) 9 (40.9) 4 (18.2) 1 (4.5)
Residence Portland Metropolitan Counties (%) Willamette Valley (%) Central (%) Central Coast (%) Columbia Gorge (%) Southern Oregon (%) Not Disclosed (%)
Underlying illness Pancreatic cancer Amyotrophic lateral sclerosis Breast cancer Lung cancer Prostate cancer Lymphoma Colon cancer Esophagus cancer Multiple systems atrophy Stomach and Liver melanoma
The sample of deceased family members in this study were relatively similar to
the overall population of persons who died using the DWDA during the past three years.
Reports from the Oregon Department of Human Services (2006, 2007, 2008) indicate that
the median age of those who used the DWDA in 2006 was 74, the median age in 2007
was 65, and the median age in 2008 was age 72. The median age of participants deceased
family members in this study was 69.5 years, with ages ranging between 42-91 years.
Between 2006-2008, approximately 84 % of those who used the DWDA had cancer. In
this study, 82% had cancer. In 2006, 41% of the people who died from DWDA had a
baccalaureate degree, while in 2007, 69% had some college, and in 2008, 60% had a
baccalaureate degree or higher. In this study, approximately 59% had a baccalaureate
degree or higher. Reports indicate that in 2007, 55% of those who died using the DWDA
resided in Portland metropolitan areas, and in 2008, 48.3% resided in Portland
Metropolitan areas. In this study, 63.6% resided in Portland metropolitan areas. In 2008,
98% of people who used the DWDA were Caucasian. In this study, 95.5% of the sample
was Caucasian.
47
Participant Recruitment and Informed Consent
The majority of people who have used aid-in-dying in Oregon have had the help
and support of Compassion and Choice of Oregon, an aid-in-dying advocacy
organization. Compassion and Choices has contact information for their past clients
(people who have used the Death with Dignity law) and their past clients’ immediate
family members. Compassion and Choices mailed recruitment letters for this study to all
family members over the age of 18 of persons who had died using aid-in-dying during the
past 3 years. Family member was defined as unmarried or married partners, in-laws,
relatives through marriage or unmarried partnership, and close friends. The mailing
consisted of 2 letters. One letter was from Compassion and Choices. This letter informed
potential participants about the study (See appendix A). The second letter was from the
researcher and gave more details about the study and asked interested potential
participants to contact the researcher either through phone or email if they wished to
participate (See appendix B). The initial mailing was sent in early January of 2009 to 97
participants. Four of the mailings were returned without a forwarding address. A second
follow up mailing was sent February 18, 2009 to 80 participants. Compassion and
Choices was provided with a list of addresses of those who were not to receive the 2nd
mailing. The follow-up mailing consisted again of 2 letters, one from Compassion and
Choices reminding potential participants about the study, and 1 from the researcher with
further details about the study and the researcher’s contact information for potential
participants to ask inquiries and/or schedule a time for an interview.
Interviews were scheduled in the order that the potential participants contacted the
researcher. Most interviews took place in the participant’s home. Two interviews took
48
place in a public place chosen by the participant, and 1 interview took place at the
researcher’s home. Before the interview, participants were given informed consent
documents, approved by Oregon State University’s institutional review board, to review
and sign (see appendix C). The informed consent document described the purpose, risk
and benefits, and interview procedures of the study. The document contained statements
informing participants of their rights to refuse to answer any question or to withdraw
from the study. Participants’ were asked to initial their consent for the interview to be
audio-recorded and were asked to sign and date the informed consent. Participants were
also provided with a list of bereavement counselors and bereavement support groups in
the event that they wished to speak with a professional. In order to protect confidentiality,
participants were assigned an identification number that was written on their informed
consent document. This identification number was used in the audio-recording to specify
which interview was taking place. Participants were never identified by name.
Pseudonyms were assigned and are used in the results section to identify quotations from
participants.
Data Collection
A structured interview was used to ask participants about their bereavement
experience (see appendix D). Interview questions were designed to address aspects of
grief theories and processes identified from previous research, and to explore
participants’ bereavement experience from aid-in-dying. All interviews were tape-
recorded and transcribed. The researcher began the interview by reminding participants
that they could refuse to answer any question, take a break if needed, or withdraw from
the study at any point.
49
Demographic information was collected from the participant, followed by
questions about their bereavement experience. Interview questions pertained to 1) the
background of their loved one, including demographic characteristics, thoughts about
being sick and dying, and motivation for using aid-in-dying 2) participants involvement
with caregiving, and participants’ coping process during the illness. 3) details of their
loved ones death a 4) grief reactions, reconciliation, and previous grieving experiences 5)
personal feelings and family members feelings of their loved ones’ decision to use aid-in-
dying, and 6) reactions and support from others. (See appendix D for the full interview.)
All interviews were transcribed in order to be in the appropriate form for analysis.
Data analysis
Data were analyzed using grounded theory, a method that emphasizes letting
ideas, themes and theories emerge from data during analysis. The grounded theory
analysis involved identifying categories and themes through a coding process that
consisted of open coding, axial coding, and selective coding. In the open coding stage,
transcribed interviews were read repeatedly and emerging categories and themes were
written in the margin. Examples of primary codes included grief reactions, conflict in
agreement, and support for loved one’s decision. Many themes were derived from the
specific questions that were asked. For example, one interview question was “How did
your agreement with your loved one’s decision to use aid-in-dying affect your grief?”
The themes which emerged from this question directly related to how one’s agreement
with their loved one’s decision to use aid-in-dying affected their grief. Other themes
emerged spontaneously from the data and were not directly reflective of the specific
interview questions. For example, although participants were not asked a specific
50
question about anticipating the death, many still spoke about this. Axial coding followed
after coding reached a saturation point with no new themes emerging. During the axial
coding process, “categories are refined, developed and related or interconnected” (Gibbs,
2007, p. 50). Categories identified during open coding were reviewed to gain a deeper
understanding of how they related to one another. Identified themes were further
categorized into sub-groups. For example, codes relating to grief were further refined into
subgroups such as immediate grief responses, grief reactions, and grief reconciliation.
Notes were written about the emerging themes and sub-categories and a coding hierarchy
was used to organize codes in order to understand the general categories and the more
specific themes that related. Coding hierarchies are used to keep the data tidy, and is a
helpful step before beginning selective coding (Gibbs, 2007). Coding hierarchies provide
a visual picture of the data, which follows a tree structure. The main branch is the
category, and smaller branches that stem from the main branch are themes. For example,
in this study, one main branch was grief reconciliation, with sub-theme branches of
common grief reconciliation and grief reconciliation from aid-in-dying.
The selective coding process is often described as telling a story that joins together
the different elements of the study (Gibbs, 2007, Baskersville & Pries-Heje, 1999). This
last step of the coding process involved identifying coded themes that were central to the
study, (Back et al., 2002; Gibbs, 2007). The visual image that the coding hierarchy
provided and notes that had been taken were used to identify the themes that were the
most connected to the different patterns that emerged from the data. Selective coding was
followed by constant comparison analysis.
Constant Comparison analysis entails reviewing how central themes relate to
51
existing theory and research and seeing what new theory or themes may have emerged.
An important aspect of this analysis is that it “differentiates a rigorous grounded theory
analysis from inductive guesswork” (Gasson, 2004, p.84). Consistent with grounded
theory, themes that have emerged from the data will guide the process. Newly derived
themes were read multiple times and compared to existing literature to find connections
to the existing literature and to identify new themes distinctive to this study.
52
Chapter 4
Results
Theme 1: Common Grief Reactions and Grief Reconciliation Participants all described grief reactions that are commonly experienced
following any death such as sadness, disbelief, numbness, anger, and anxiety. Grief
reactions also included experiencing a general sense of loss, a loss of sense of self, or
identity in relation to that person (i.e. losing the identity of being a wife if the husband
had died), and feeling tired and overwhelmed. Participants also described feeling a sense
of relief that their loved one was no longer suffering, or dealing with the illness.
Well that feeling of his spirit going out the window was really great b/c it absolutely was a very positive thing and then knowing he wasn’t in pain and knowing that I actually felt that whatever his essence was went on and then since then with the smell of the roses, uh, I feel like the essence is still sort of around me or has been and perhaps we’ll meet again. I think the next day I was really depleted, the next day, cause it’s like you’re in this really heightened sense of existence and then there’s this letdown, you know, afterwards, even though yes there’s relief I could sleep, I could not have to, you know, be worrying every second. But it was definitely…a vacuum in my life, you know, of, of caring about someone and trying to help them and, um, so one way, you know, I could sleep, but I wouldn’t, I could try to start taking care of myself, but I also was very, um, I felt that it, definitely after he died, the few weeks after he died, I felt more and more anxious or anxiety of, like, you know it’s like they say people will work really hard through an emergency and the, the emergency is over they get sick, you know, and I felt really rundown. [Eden] Relief. First thing relief and then my god, he’s gone. All our hopes and aspirations, we had plans, are gone. Me, I’m gone. What, I don’t have a life. I’m going to have to, you know, he was my life. But it was, it was relief and a great deal of sadness of course. [Laura] Participants also described ways of reconciling grief that are commonly
experienced following a death. Common grief reconciliation included expressing grief
through crying or talking with loved ones, accepting the loss, giving oneself permission
to take time to grieve, reading books about grief or spirituality, journaling about grief,
53
recalling memories of their loved one, honoring their loved one in a celebration of life
ceremony, attending grief counseling or bereavement support groups, receiving support
from family and friends, socializing, making plans, and regaining a new sense of identity
without their loved one.
…you go through everything, um…feels good to cry, so a lot of times I just cry, feels good to go through photos and memories. We spent a long time making a big video for the funeral and the memorial and that was, I think, a good, helpful thing to do for, you know, very beneficial for our state of mind, just to relive a lot of moments and keep the memories alive. [Deidre] I started going to a grief counselor and she’s got some ideas about, ideas for journal writing, like you’re supposed to write a letter to the person who died expressing your thoughts and feelings about the following issues, a special memory I have about you, what I miss the most about you and our relationship, what I wish I’d said or hadn’t said, what I’d like to ask you, what I wish we had or hadn’t done, what I have the hardest time dealing with, ways you continue to live on with me, special ways I have of keeping my memories of you alive. Chose one of several ideas that have significance for you, start at the top of the list and walk your way down. These topics may help to serve you to come up with your own ideas specific to the situation and relationship. I’ve been looking at that thinking I need to, I should write, I like to write, so I should sit down and just write, but it seems like when I look at them I just think about them I haven’t put them down on paper yet, but. And then they have this other one for saying goodbye in a dialogue and I assume that it’s for not necessarily dead but when someone for whatever reasons, says explore possible feelings alone to an empty chair, photographs, to a partner who simply listens, received, the person involved appropriate. I do that also, like where he sat, talk to a chair or I talk to a picture. [Betty] Theme 2: Grief from aid-in-dying
Participants were asked to compare their grief from their loved one’s death from
aid-in-dying to their grief from other deaths they had experienced. Eight participants
emphasized that their emotional closeness to their loved one impacted their grief more so
than the mode of death itself. Eight participants compared their experience from aid-in-
dying to their experience from a sudden death. Nine participants compared their
experience from aid-in-dying to their experience from an anticipated natural death, and
five participants made distinctions between death using aid-in-dying and death by
54
suicide. Three participants had not experienced other deaths in their adult life or of close
family members. Several participants overlapped within the different categories.
Subtheme: Emotional closeness of relationship Eight participants emphasized that emotional closeness to their loved one affected
their grief, rather than the mode of death.
But the intensity of the grief is like 99% the relationship, you know. If you see what I mean, 1% would be the cause of death, and within that 1%, cancer is more horrid than a lot of the ways, even heart, you know, there’s something merciful of dying of a heart attack, although I guess it can be very painful. But, but it’s, the grief does not arise from the cause of death. It’s the relationship. Just, she’s supposed to be here. [Roger] Well, you know, I guess that having one’s husband die is a different story than having one’s parents die or having even one’s ex-husband who you haven’t lived with for a lot of years. Having your husband die or somebody you are actually interacting with on a, you know, on a pretty much 24/7 kind of thing is a lot more grief involved than any of the other deaths than I’ve discussed. So it’s the relationship that dies as well as the person that is the grief and so it’s different, but it doesn’t have anything to do with the method of death, it’s just the relationship. [Ingrid] I think the emotional loss of my spouse so far overlays the nature of the death. The cause of the death, it’s not a relevant discussion. It’s not a relevant part of the death. Does that make sense? [Paul] Subtheme: Grief from aid-in-dying easier to deal with than grief from a sudden death
Eight participants felt that grief from aid-in-dying was easier to deal with than
grief from a sudden death. Reasons included that the death from aid-in-dying was less of
a shock (n=7), was easier to make sense of (n=3), and allowed for opportunity to prepare
for the death, to begin grieving before the actual death, and to say goodbye (n=3).
Multiple ideas are expressed within the quotations.
If I had a different reaction it had to do with suddenness of death rather than slow debilitating illness. Like I said, with my son it was like someone hit me on the back with a baseball bat. It kept coming back, didn’t go away. For 6 months a physical kind of shock, but with M having gone through the cancer and stuff with her sister, that sort of thing, there was all sorts of preparation. Not a surprise. My experience of grief had more to do with quickness and suddenness of this doesn’t make any sense, it shouldn’t happen,
55
and it was a different physical kind of thing. [Ned] I think mainly just knowing it was going to happen and preparing in a sense, and starting the grief before the death actually happened. I think you start grieving before and that almost eases the grief when death does come. Compared to a tragic or sudden death that you’re not expecting, then, you know, once you get over to the shock of a sudden, tragic accident or death, the grief can be pretty strong, you just, it’s just hard to accept and it seems to last a little longer too in my experience, but, I don’t know, this was almost like watching, say, a grandparent kind of fade away. You’re just kind of getting ready or setting yourself, setting the tone in a sense of this is going to happen and you start dealing with it before it happens. [Deidre] I don’t even know if they are the similar. I mean there’s grief there, but it’s, with B, since he’d been sick for awhile, it was kind of expected. I was able to deal with it and we’d always say this is better than getting hit by a bus, which would be one of those sudden deaths, because everything would be so unprepared and, I mean I’m, everything, we were able to set things up and be prepared for, so there’s the difference. You know mom, it was just such a shock to your system. I think B and I were luckier, cause we got time to discuss the future, you know, and what he thought about dying, and so I think that was easier- I don’t know if it’s easier, I think it’s better though than having something happen, cause most of the time you don’t talk about this stuff. You just don’t. So. So I think it was, our way was better. [Olivia] Subtheme: grief from aid-in-dying easier to deal with compared to anticipated death from an illness (non aid-in-dying) Nine participants reflected on their experiences with grief from anticipated deaths
from an illness and how it compared to their experience with aid-in-dying. Participants
described feeling that their grief from aid-in-dying was easier to handle because aid-in-
dying made it possible for their loved one to avoid prolonged suffering (n=6), and gave
loved ones a sense of control with the dying process (n=4). Participants also pointed out
differences in grief related to preparing for the moment of death (n=2) when using aid-in-
dying.
Six participants stated feeling that their grief was eased by knowing their loved
one would be avoiding suffering and by not having to watch their loved one go through
prolonged suffering. It should be noted that one of these participants was not comparing
his own experience with an anticipated natural death, but was speculating about grief
56
differences based on his experience with a death from aid-in-dying and comparing it to
the grief he watched a friend go through when dealing with an anticipated death from a
terminal illness. The following quotation is from someone who had compared his
experience of caregiving for friends who died from a terminal illness to his experience of
his loved who died using aid-in-dying.
It was, to have that lingering impression of the last few minutes, it was not pleasant. To see N go out and you know, a few seconds after making people laugh changes the whole complexion of the way you feel about it. You still of course feel this great void in your life that you were so used to having, and, but the way it made it, it took the edge of it that way. [Ron] Three participants emphasized that knowing that their loved had the option of
having some control over their death eased grief. The following quotation illustrates ideas
related to avoiding prolonged suffering, having control and being present at the moment
of death.
It’s easier to understand, or to accept when you’re right there and you know somebody’s made this choice to go and that you’re, I mean it’s, the closure is so much, it’s so different than when you have that prolonged suffering, and you know, process, um. I mean it’s, to me it’s a much more intimate sort of experience, because you’re just right there, versus most other you know experiences you’re not there at the time when someone dies, or you’re, you know, you have some contact and you’re in and out, but it’s much more intimate personal sort of experience. But I still think, you know, the fact that somebody has the opportunity to have control when they basically had no control is probably the most important thing, for the family, for the individual. [Catherine] One of the three participants who emphasized control described how grief is eased
by knowing that the loved one is not in the situation of dying under hospital or hospice
care, with less control over their own dying process.
It was more organized. In most such cases where it’s like a close friend, or a relative, there’s this hospital experience which is full of unknowns, an all pervading sense that control has somehow been lost, that you’re just in the hands of others, not only their well-meaning care, but their ethical systems, whatever they may be. And, with this situation, I think it makes it possible for you to retain control of what happens to you, and the circumstances and the environment up to a degree. It wouldn’t necessarily be true in a
57
hospital. It wouldn’t necessarily be true in a hospice situation because whenever there are other people involved, family members or not, you have to respect the ethics under which they function, and particularly if they’re being paid for their work. And those can strip away from you, and the ability to have certainty, and I’ve been over that with other people. I don’t think anyone else that I know became quite as obsessed with it as I had been. If you want to keep control of this situation in your own hands, this may be the only way to do it. [Al] Two participants pointed out that while a death from a terminal illness without
use of aid-in-dying and a death from a terminal illness using aid-in-dying are both
anticipated, aid-in-dying allows more preparation for the time of death and the
opportunity to be present for the death, if desired.
Well the only thing that I’m going to say is that when you know in advance that you’re going to die or somebody’s going to die, you have an amount of preparation that is a very comforting kind of preparation, I mean, you know it’s going to happen, it’s not just suddenly, it doesn’t just suddenly happen, and the others we were anticipating the fact that they were going to die, but we had no idea when cause there wasn’t a when. This one you’ve got a very specific when, and so you can have people come in and so you can be surrounded by people who are very, you know, are very comforting to you. So I loved the idea that I could have the house full of people that , you know, were just there to talk to, to hug, to hold, to move furniture, to tell stories, to laugh with, to cry with, or whatever. It was, it was a better experience. [Ingrid] Subtheme: Aid-in-dying vs. suicide Five participants compared aid-in-dying and suicide. One participant compared
her experience with aid-in-dying to her experience with a death from a suicide, while the
4 other participants offered their opinions about the difference between aid-in-dying and
suicide. The participant who compared her experience with aid-in-dying to an experience
where a loved one had shot himself commented briefly, explaining that a death from aid-
in-dying is nothing like a death from suicide, that they are two different situations and
should not be considered similar. One of the four participants who discussed their
opinions of suicide emphasized that the people who commit suicide are usually secretive
about it, whereas the legal sanction of aid-in-dying created a chance for open dialogue.
58
One participant described how she felt the moment of death with a suicide is filled with
feelings of anger, despair, and vengeance, which was not the case with her experience of
her loved one’s death from aid-in-dying. One participant who described her loved one’s
cause of death as an overdose clarified that she felt that in this instance overdosing was
different than suicide because death was inevitable in the sense that there was no mental
or physical condition that could have been addressed with treatment to allow her loved
one to continue living.
Um, I think K, and I mean I know you asked what did K die of and I said he overdosed. But in my mind, I don’t like the word suicide in these circumstances because he’s, the card was dealt. He’s dying. He’s, he’s going to die. It’s not like other suicides where like oh if we do mental health therapy or whatever we can get you thru this, or cancer, let’s do some treatments and maybe we can get over this. K, he was dying, and the Compassion and Choices people used the word hastening, we’ll attend K’s hastening, versus his suicide. Softer word, you know, it’s all the same, I guess, but I like that word because K, he was dying, that was, he didn’t have a choice to live or die, and chose suicide. He was dying, period. And he just kind of chose the way, and the time. So, but still, he overdosed, so… [Jane] Two of the participants who compared aid-in-dying to suicide explained that they
considered aid-in-dying to be a way of hastening death rather than taking one’s life.
Several other participants also used the word “hastening” in their interviews to describe
aid-in-dying.
Theme 3: Saying Goodbye Participants were asked if they felt they were able to say goodbye to their loved
one. All of the deaths were anticipated, which allowed for time to say goodbye (although
some had a shorter time between the diagnosis and the death than others). Although all
participants were able to say goodbye during their loved one’s illness, 8 participants
spoke directly about the moment of saying goodbye at their loved one’s death.
Subtheme: Chance to say goodbye
59
All participants felt that they were able to say goodbye to their loved one.
Participants explained that knowing that their loved one was going to die allowed for a
chance to address unfinished business and provided an opportunity for them and other
friends and family members to say goodbye.
Oh yeah. So, so, you know that last week several times I said, if some of the major issues that we’d had, and she once asked me do you want to talk about that and I said only if you do, I don’t feel the need to. (Participant’s loved one):No, I think I’m okay. And then I’d ask her a couple of days later, and it’s like do you feel any need to talk about this, No. And then some thing we did talk about. Some regrets, some apologies, so. So I think that’s the gift of planning your own death. You have the time to say goodbye and to apologize and forgive. [Maureen] Oh yeah, yes, yeah. That was a good thing about this. Say goodbye at a time and to see him saying goodbye to people. And then I got to say goodbye to his people that meant a lot to him who he hadn’t talked to and still have people calling to talk. [Sarah] Sub-theme: Goodbye at time of death While most of the participants were present at the time of death to say goodbye, 3
participants spoke directly to how having a specific moment to say goodbye was
meaningful to them.
We had spent enough time together and then we all, that day, we all said goodbye to him before he drank the drug…. That was the nice thing about everybody being here we did, we all got a chance to tell him goodbye, and that’s one of the plusses I think about, if you can say a plus about someone taking their life in that way, but I think in making that choice and taking the time, you do have time to say the goodbyes, and so I think that’s one of the positives. [Elizabeth] Absolutely. And that’s the great gift of Death with Dignity. There’s a moment. I’m assuming that she’s lucid, that whoever you’re dealing with is lucid, she was reasonably lucid. Yeah, we had months and weeks and certainly even a moment to say goodbye, yeah. I treasure that. [Ted] In one interview, the participant had felt the goodbye to her husband right before
his death was filled with some tension (not related to aid-in-dying, but private details)
and felt that the final, more loving goodbye followed in a spiritual message from her
60
loved one after dying. Three other participants also reported having a continued goodbye
with their loved one through spiritual messages from their loved one after death.
Three participants reflected on not saying goodbye at the time of death. In all
cases participants felt that they had said goodbye prior to the death during talks with each
other and from the way they lived their lives. One participant reflected on wishing to be
able to recall a more formal goodbye. The second participant described how she felt
lucky that she was able to say goodbye to her loved one throughout the illness and a few
weeks before the death. This participant recalled that when saying goodbye at the
moment of death her loved one stopped her and reassured her that they had already said
everything they had wanted to say to each other beforehand.
I started to try to tell him, you know, goodbye, and some of my feelings, and um, he didn’t want to talk about that b/c he didn’t want to just break down. He wanted to hold it together. And we’d been able to say those things to each other before, so that was good, um, I think he said you know, it’s okay, we’ve already said all the things we want to say. [Natalie] These two participants stated that they did not have conflict over the goodbye and
felt very lucky to have said goodbye during their loved ones illness. The participant in the
quotation above who did not say a formal goodbye at the time of death spoke to saying
goodbye during her loved one’s illness.
Oh yeah, yeah, yeah I was. Um…yeah, we, we were able to have some really good talks, which were amazing because of [D’s] stoicism, cause he’s not usually someone who talks about his emotions, but we had about 3 or 4 really good talks about a year and a half leading up to his passing away, um, and just about a couple of weeks before he passed away we’d taken a walk down by the river…He couldn’t walk very far but we walked like 20, you know, 25 feet and looked at the ducks and, you know, that kind of thing, and hung out at this bridge and said, you know, just how much we…loved each other and appreciated how good of a relationship we have now and how much we appreciate the time we’ve gotten to spend together, and yeah, so, um, we got to say that pre ..close before hand, And then, you know, when I started to say those things again to him right
61
before he passed away he said it’s okay, we’ve already gotten to say everything we wanted to say. [Natalie] Another participant indicated regret at not expressing more appreciation for his
loved one, not saying a formal goodbye at the time of death, and wished he had put more
energy into the goodbye. He, too, was grateful for being able to say goodbye during the
illness but described not saying a formal goodbye at the time of death as something he
would always regret. Below is his response to the question “Did you feel you were able
to say goodbye to your loved one?”
Well, no. ..But then I don’t think you ever could. I don’t know. I think about that…Um…I think from the spiritual and emotional growth I’ve had since I’ve lost A, perhaps I could have done a better job of it, now. Um, it’s, it’s impossible to evaluate that now. I could’ve done a better job of it, I’m just not certain. But I think I could probably say no, not adequately. And that probably will always be a regret. [Paul] Paul continued to further clarify his regret at not saying a formal goodbye. I think my regret would be better expressed as not thanking her for just a wonderful life. And I guess that could be under the same category of saying goodbye, but it’s an entirely different expression, emotion. But on the other hand, we always lived our lives in gratitude for each other, so, it was implicitly there. Yeah, you know, I think that question of saying goodbye is really quite a good academic question. But…if I would have had to do it today I would have put some more energy into expressing my appreciation of her. Yeah. I think that would be a better way of putting it in my mind right now. A little disclaimer. [Paul] One participant reported that at the time of death her loved one was telling a joke
and smiling and abruptly turned his head and went into a coma, in which he remained for
an unusually long duration of 25 hours before dying. Although his sudden transition to a
coma was jarring, she felt that his prolonged death turned out to be a blessing because it
gave her more of a chance to say goodbye.
62
Theme 4: Timing of Death In response to the question “How did it feel to you for your loved one to use aid-
in-dying at the stage of illness s/he was in?”, 20 participants expressed that they felt
strongly that the timing was appropriate, often expressing multiple reasons for why they
agreed with the timing. One participant felt that the timing was just at the point of being
appropriate and 2 participants expressed that they felt their loved one could have used
aid-in-dying sooner.
Subtheme: Appropriate timing The majority of participants (n=20) felt very strongly that the timing of their
loved one using aid-in-dying was appropriate for the stage of illness they were in. Nine
participants indicated that the timing felt appropriate to them because their loved one was
in a lot of pain and/or discomfort.
It was, it was good. I mean it’s…It was the time. I knew that he was in such pain the day before and, and this, there was no way I would have wanted him to go on like that. He couldn’t have stood it. It would’ve been horrible, it would’ve been horrible. [Betty] Yeah, the timing of death was the best time I think. It was really getting bad, so it was, I think it was the right time. Of course I wanted him a little longer, but you know, it was seeing him suffer was very, very hard on me to watch him. [Alice] Eight participants explained that the timing of their loved one’s death felt
appropriate because it was clear that their loved one’s health was not going to improve
and that the end was soon approaching.
Yes, Yes, yeah. He was at the end. There was no question. He was not going to rebound from where he was at. [Olivia] Oh yeah. Was probably was, got it about as close as she could physically, because she still has to drink it, and she was really getting pretty, pretty, you know, pancreas, squeezed, it was pressing so rapidly, a few more days, maybe a week, but what point? And it drops off. She was ready. I don’t have, I don’t have any, I don’t have any disagreement about the timing at all. She was absolutely ready. [Ted]
63
The DWD act requires that the person using aid-in-dying law ingest the
prescription intended for death on their own, without the assistance of others. Ten
participants noted that the timing of their loved one’s death felt appropriate because they
felt their loved one would quickly be at the point of losing the ability to take the medicine
on their own (losing the ability to swallow, to keep food and liquids down, to be
cognitively aware, and to have the strength).
I know it was a tough decision, cause I think like anybody she probably wanted to stay and get as much time to live as she could. When she realized that and, you know, if she waited any longer it might, she might start to lose it, her ability to make her own decisions, and so she was consciously aware enough that process happening to her and she said I better do it no. And so I, I think I sense that we were close to that point anyway and when she said it’s now, we both felt it was the right time. [Ron] I think it was good that he did it when he did because I think he wouldn’t have been able to swallow, maybe even a week or two later, he probably couldn’t have taken the prescription, so I think the timing was, you know, it was better that he did it. [Jane] Sub-theme: Hesitation with timing
One person agreed with some hesitation that her loved one was just at the point in
the illness where it felt acceptable to her for her loved one to use aid-in-dying. (*in this
case the participant disagreed with the decision to use aid-in-dying, but assented to it).
It was just okay at that point. Yeah. Just at the point that I could agree with it. If he had, if his health were the same as it had been a week or two before, um, there was some reasons not to do it then. [Sarah] Subtheme: Aid-in-dying could have been used sooner Two participants said they would have understood if their loved one would have
wanted to use aid-in-dying sooner to avoid pain.
My only regret was that he couldn’t have taken the medication…not the pain medication, but the final medication, uh three days early and avoided those last horrible days of horrible, horrible pain. (*This participant’s loved one did not have the option to use aid-in-dying earlier because he was still in the process of requesting to use the law). [Deidre]
64
Theme 5: Agreement with Love one’s Decision to Use Aid-in-dying Nineteen participants initially agreed completely with their loved one’s decision
to use aid-in-dying. Twelve of the 19 participants who agreed with their loved one’s
decision felt that their agreement affected their grief in a positive way. Four of the 19
participants who initially agreed with their loved one’s decision expressed having
conflicted feelings about their agreement when reflecting upon their agreement after their
loved one had died. Two of the 19 participants who agreed with their loved one’s
decision felt that their agreement had no impact on grief. One participant felt her
agreement with her loved one’s decision impacted her anticipatory grief. Three
participants agreed with their loved one’s decision with some conflict at the time of
agreement.
Subtheme: Positive impact on grief Nineteen participants agreed with their loved one’s decision to use aid-in-dying.
Twelve of these participants felt their agreement impacted their grief in a positive way.
Four participants felt that the fact of being in agreement with their loved one’s decision
eased grief.
I think it eased it a lot. Cause we’re all in the same boat. We’re all in the same track. We’re all in the same mind. It was almost like one person’s decision. You can’t get better than that I don’t think. [Ted] Three participants indicated that their agreement meant that their loved one would
not have to have prolonged suffering and this alleviated their grief
I think it helped alleviate my grief. Very much so. It would have been very, very difficult for me to witness her death. I don’t know how much longer she would’ve lived. It might have been a long as a month from that time and that would’ve been a very difficult month for me, so I think it actually did help me a lot. [Ron] Interviewer: can you explain a little more in what way it helped ease your grief?
65
Because rather than see her become helpless, see her actually wither to, you know, cause she would’ve starved to death, unless she had some organ failure that took her out more swiftly, but more than likely she would’ve starved to death and to watch that process for any greater length of time than I did, down to the bitter end would have been very agonizing and gruesome for me. So. And the fact that she was able to smile in the last minutes. [Ron] Two participants spoke about how agreement with the decision made it possible
to plan and prepare for the death and to begin grieving with the loved one before death
Well I think you just totally prepare yourself in a different way when you know that it’s going to happen and that you’re, I mean, that way you can really talk about it prior to, you can, you know, both feel like you’re in a place where you’re, you’re okay, you know, where you’re at piece with each other’s decisions, where you are at, and I think it’s, you know, it’s a good thing. For both people, when they both believe in that. [Catherine] Two participants discussed how being firm in their own agreement and not
doubting their support for aid-in-dying affected their grief.
Probably in a positive way. I didn’t have to struggle with it. I didn’t have to wrestle in my mind if this was really a right thing to do or not. [Deidre] One participant emphasized that agreement made it possible to have a plan in
place and knowing what was going to happen eased grief.
I think the preparation made it easier. [Al] Interviewer: Could you explain a little more about that? You…I would’ve been much more distressed, you know, had I been you know, called to my mother’s bedside in the hospital, um, with people hovering about saying things like, well this is what we think the situation is, what do you think we should do? This was a situation that had been discussed, argued about, agreed upon, and put into action, so it was easier to follow the steps even though in some cases the steps were not terribly clear, you knew what the goal was. [Al] Subtheme: Impact on anticipatory grieving One participant felt her agreement had an impact on her anticipatory grieving: The aid-in-dying impacted my grief. It got it over sooner. Having him die sooner. That’s the only thing I could say. The anticipatory grief would have gone on longer, that’s certainly for sure. [Linda]
66
Subtheme: Grief from conflict over agreement with loved one’s decision to use aid-in-dying Four of the 19 participants who initially fully agreed with their loved one’s
decision to use aid-in-dying felt some conflict over their agreement when reflecting on it
after their loved one had died. Three participants had indicated having initial conflict over
their loved one’s decision to use aid-in-dying. One of these participants felt her conflict
in agreement had an impact on her grief, while the other two felt conflict in agreement
had little or not impact on grief. A total of 5 people felt that conflict in their agreement
with their loved one’s decision impacted their grief.
The reasons for conflict varied. In all cases participants expressed that they
ultimately still agreed with their decision to support their loved one, but there were some
mixed feelings relating to helping a loved take their life (n=1), wondering if the decision
was right in general (2), feeling conflict because the loved one’s mid was healthy, and
feeling an undercurrent of conflict related to religion (1).
One participant indicated wavering feelings over his agreement with his loved
one’s decision, noting that while his agreement was helpful in ending his loved one’s
suffering, it also made him feel sad that she was gone and that his agreement played a
part in it:
Well made you feel good that she got done what she wanted done, and made you feel bad cause you killed her, or that she’s gone. It wouldn’t make any difference who killed her, I guess, or who helped her do this. But you know there’s not rational thinking when you, emotions do that…[Roger] Two people indicated having mixed feelings over their agreement with their loved
one’s decision. They were able to resolve these feelings as indicated in the quotations.
I guess I have mixed feelings about that. I have mixed feelings about the fact that I did what I had to do, and one part of me says, you know, was it really right? The other part of me said but it was what he wanted. So, I guess that’s my only way I can really explain
67
that. I don’t know for sure. I…most of the time I feel that what we did, and it was a family, I mean, the whole family was aware of this and was involved in it. It was, uh, they were all there, all of us wish that the reason to make the decision hadn’t been there, but that that was what he wanted and that we had to do what he wanted. And I think, uh…it gave him some dignity at the end that he hadn’t had for quite awhile, so in that respect I knew it was right, but still it made it hard. [Elizabeth] That’s what, what I said was helpful with the hospice grief group that I went to when we talked a lot about that death is not, that death is not optional, you know, the timing of death, the place of death, and a lot of other things are optional, but death is not optional, so when there would be questions in my mind, you know, I wonder how much longer he would’ve lived on his own, I wonder if that was the best thing, but he was so uncomfortable, he was so miserable. The other thing was there was no way to oppose him anyway (laughs). He was going to do what he was going to do. So I certainly did not want to have my final days any more conflictual than it was. [Ingrid] One participant expressed some conflict in her agreement because her loved one’s
condition was such that his mind and sense of humor remained very sharp and healthy.
This participant explained that her loved one looked different than other people she had
seen who had terminal illness. She felt that it was the right decision because her loved
one was physically suffering and was going to soon lose the ability to swallow on his
own, but it was difficult to make sense of since he didn’t look as “terrible” as they way
someone she had known with terminal lung cancer looked before their death.
One participant expressed some conflict related to her religion. She supported her
loved one’s choice, but wavered in her thoughts about her support as a spiritual person,
feeling it was acceptable while still feeling some conflict.
Yes it did impact it in terms of, I wasn’t quite sure. I know what I felt in my heart and what I believed and what I felt, and I feel like, well, yeah, so I was feeling that, but there was still a little bit of turmoil that, oh maybe being a Presbyterian, being a Christian, you shouldn’t supporting K, which I knew that wasn’t true, I mean, that’s not how, that’s not how our church believes. Love and support them, and that’s what I was doing. So it kind of reinforced my feeling you’re loving and supporting him, so, whatever L’s thought are with God, that’s between K and God, don’t get in the middle of that, and that’s kind of how I was feeling, so, it did, um, there was kind of an undercurrent of conflict there for a little bit, but I just though, no, this is okay, and it was okay. [Jane]
68
Subtheme: Agreement with loved one’s decision to use aid-in-dying had little or no impact on grief Four participants agreed with their loved one’s decision and felt their agreement
had no impact on their grief. Two people expressed conflict in their agreement with their
loved one’s decision but felt that this did not impact their grief.
One participant did express having conflict when describing her agreement with
her loved one’s decision, feeling as if she assented to his decision, but when describing
grief from the decision, explained that other than subtle impact, their was no affect on
grief from missing him.:
I assented to it. And, oh gosh, I, I wish he hadn’t. But I assented to it. And it was, went better than I had feared. Yeah…I would have wished that he could have lived until he found that he couldn’t eat and then given up eating and drinking instead, which is more of a, something you can do openly. But, um…cause it was kind of a , it was kind of like a back alley abortion. It wasn’t that much different from that kind of a feeling. Yeah. But I, yeah, but I’d have to say that I went along with it. I helped him, to get, to get the paperwork done and the medications here, making the calls and stuff. [Sarah] In response to the question of how assenting to his decision affected her grief, she
responded:
It must have, but it’s subtle. I don’t really feel that that’s made that much of a difference in the missing of him and stuff. [Sarah] One participant described that she intellectually agreed with her loved one’s
decision but emotionally and some conflict.
Sure…you know, intellectually. I mean emotionally of course you don’t want somebody to die sooner than they have to. So, no. I mean, emotionally no, no. no. But, you know, that’s why I voted for the law. Because I believe in it. [Emma] She continued to explain that her conflict in agreement had no impact on her grief
because she had resolved it before her loved one died.
I don’t think so. No. I think, you know, I’ve, as it worked out. She was failing, very fast. And I, you know, I, professionally I could see that. So I knew that, you know, she, she was going to even lose the choice soon. And so I think I had resolved emotionally, you
69
know, whether she should do it or not. I mean I, of course, you know, there’s always that hope that they, you know, another day, another day. But I knew that she didn’t have much time. So. [Emma] Theme 6: Family Member Agreement with Decision and Impact on Grief The immediate family members of 18 participants were in agreement with their
loved one’s decision to use aid-in-dying. In 9 of these cases, there were some extended
family members and friends who were not told about the use of aid-in-dying. Participants
self-selected who they told either because it was the request of their loved one, because
they had family members who they thought would disapprove and they wanted to avoid
conflict, or because they felt it wasn’t anyone’s business. Three participants had family
members who disagreed with their loved one’s decision to use aid-in-dying, but despite
their disagreement, were ultimately supportive of the choice and not vocal about their
disapproval. One participant had family members who voiced their disagreement about
their loved one’s choice to use aid-in-dying.
Subtheme: Family member agreement eases grief Ten participants felt that their family member’s agreement with their loved one’s
decision to use aid-in-dying eased their grief.
Ten participants felt that being on the same page and having the support of being
in agreement helped with the grieving process.
Very, you know, just knowing that they were there for me before , during and after. That it would’ve been hard if we’d have anybody that was against it. Yeah. [Jennifer] I just think it made it easier. I mean I think if someone had really disagreed I would’ve been so surprised that that probably would’ve made me feel guilty, but it shouldn’t have made me feel guilty, but it probably would’ve had that power because everybody was so not surprised because I think it takes a strong individual to do that and they knew he was. So yes, it made it easier. I mean I think that everybody agreeing with it made it easier for everyone. [Olivia]
70
One participant felt that both the support from having immediate family members
agree and having the support of her church helped with the grieving process because she
could talk about it her loved one’s decision to use aid-in-dying.
The fact that his children especially were okay with it and supportive and many times and a lot of talk about it made grieving much easier. The fact that my pastor came here and was willing to, um…still interact with me and a couple of other people who at the church, you know, that made, that made, it made it easier for me so I didn’t feel so alone. As I would if I were having to keep a secret. So I am keeping a secret but it’s not, it’s not qualitatively different from not sharing personal information with somebody that I wouldn’t share, doesn’t deserve to have personal information. So yes, it really did help. It helped to be able to talk about it. [Sarah] Sub-theme: Family member agreement didn’t affect grief
Among the 18 participants whose immediate family members agreed with their
loved one’s decision, 9 felt that the agreement had no impact on their grief. In all cases,
participants felt that had there been conflict, their grief may have been negatively
impacted. Six participants had extended family members who did not know about the
decision to use aid-in-dying. This did not have an impact on their grief. Three participants
had family members who disagreed with their loved one’s decision to use aid-in-dying
but were not vocal about it. Two of these 3 participants felt that there was no impact on
their grief because they were not close to those family members. (The third participant
felt a positive impact on grief that her family members were supportive despite their
disapproval. This was included in the previous section on family agreement easing grief.)
There was one participant whose extended family members openly expressed
disapproval. This participant explained that there was no impact on her grief because
neither she nor her loved one were close to these family members.
71
Theme 7: The Impact of Aid-in-dying Being Legal Participants were asked to discuss how the fact that aid-in-dying is legal in
Oregon impacted their experience. Eighteen participants emphasized the importance of
having aid-in-dying as an option, 7 participants discussed their feelings that having a law
for aid-in-dying made it possible for their loved one to avoid unnecessary pain, 3
participants expressed being glad that there were safeguards for the law and with that a
group (Compassion and Choices) to assist with information, 2 participants focused on
being able to use aid-in-dying in good conscience and 2 participants felt that their loved
one may have committed or considered suicide if aid-in-dying had not been a legal
option.
Subtheme: Legal option to die provides sense of control Eighteen participants highlighted that it was a relief for their loved one to know
that aid-in-dying was an option. Knowing that aid-in-dying was an option provided loved
ones with a sense of control over death and final months of life. Participants were
comforted in knowing their loved ones had this sense of control.
…There was still a lot of pain of course, but he knew he could end it anytime and it just gave him a point where he felt like he was managing his life, instead of the disease, where the disease was managing it till that time, whereas he was in charge, and it really made those last few months bearable for him I think. [Alice] Interviewer: And so, how did that affect your experience? It made those last months for me a lot better too. He stopped being so angry and so resentful and he stopped babbling it to the point where he was just obsessed with trying to stop, because I think he was terrified of what was going to happen too, and it was almost a release for both of use, you know, it made it a lot easier, and we did take pleasure in that time together, even though it was agony in some way, you know, we’d been together for a lot of year, but we’d both worked a lot, you know, and we took this time to really, really, really get to know everything about each other and I think we felt more in love during that part, you know, cause it gave us that opportunity, it didn’t matter, we could just be free to say whatever, and live those months out as best we could, and there was a
72
lot of joy that we did experience and w/out that law I don’t think that’ would’ve happened. He would’ve fought it tooth and nail to the end. [Alice] You know, I hope people die naturally, but if they can’t, they should have the power, some power when they’re ill, cause there isn’t much that you, that you do have. You’re, you know, physically and medically you’re pretty, at that point alive, and to have that power to say I’m going to die on the day I’m going to, I think it’s a wonderful right for any human to have, but certainly not for everyone. [Doris] I think it was a gift. That he could make that choice. And I know a lot of people just get the stuff and don’t ever do it and I’m all for that too, cause it gives you, it puts you in a position of choice. Position of a little bit of power, over, you know, and I think that, like I said, it was a very positive thing for us. Describing him, nobody would be surprised that knew him that that’s what he choose to do, so, so I think Washington now too, isn’t it? [Olivia] It was huge. Um, knowing that that was an option for him was hugely comforting to my dad and therefore me. And…the kind of passing it enabled for him was…given the circumstances the best possible kind of passing. Um, and that…made a huge difference to him and to us…um, in terms of…being more at peace with what was happening and having it be a more peaceful event. [Natalie] You know, and I think within OR, even though, I mean there were restrictions to being able to use that act, you know, at the end, but I still think it’s, you know, if you know something’s coming and you don’t want to have to go through the pain and suffering of it all, or the, that you do have an option and you chose not to do chemo because it’s no, I’d rather feel at least reasonably good, instead of going through all the stuff you go through with chemo. [Catherine] Subtheme: Aid in dying law makes it possible to avoid prolonged suffering
Seven participants felt that the fact that aid-in-dying was legal made it possible
for their loved one to avoid prolonged suffering.
It really helped to avoid quite a lot of unnecessary pain, both physical and emotional as he would’ve been…um, anxious and fighting death, but anxious about wanting it to come and take him and not knowing when that would happen and being in pain and not being able to, to end it, just keeping the ability to end his pain. Um, words can’t describe how…compassionate that is, really, and how comforting to him and to us, so, it helped enormously with, um, with what’s a very difficult situation. It helped make it better. It really did. [Natalie] Oh it avoided whatever prolonged misery might have been. I think it worked absolutely perfect for us. She clearly was failing. I frankly don’t think she would’ve made another month. [Sam]
73
Subtheme: Safeguards within the law While many participants expressed throughout the interview their comfort with
the fact that there is a process to follow at the time of death, 3 participants spoke directly
about their appreciation for safeguards and having a process to follow when reflecting on
aid-in-dying being legal in Oregon.
I think, I think it should be a person’s choice if they are terminally ill. And with all the safeguards that they have, cause we had to go be checked again by another doctor to see if he had depression or anything else. I think with all the safeguards they have I believe in it. [Linda] So yeah, the fact that it was legal and that there was a group available to help, which came out of the practical, the, at least, I don’t know if it’s written in the law, but certainly the group that advocated for it has turned into a helper group, and certainly they were helpful. I don’t know if that’s a question further down, but. And I was glad it was legal. To be able to go to a pharmacy instead of hoarding, you know. [Maureen] Subtheme: If aid-in-dying had not been legal, suicide may have been considered Three participants felt that their loved one may have considered suicide if aid-in-
dying had not been legal and were glad that their loved one didn’t have to consider
suicide.
It freed him from considering killing himself the way G killed herself, which he was willing to consider, and I was terrified that he would do that. Not really terrified, because he couldn’t have managed it by himself, but, it just, oh god. And it made it possible to go through a process that had been worked out. [Sarah] …if we wouldn’t have had that, I don’t know if K might have tried to take some of the other pills that he had started collecting, which T and I looked at and we thought, this is just going to make you go to sleep for awhile, I don’t think it’s really, it wouldn’t have killed him, or he would’ve, you know, maybe been in a coma and thrown up and aspirated and had pneumonia and been in the hospital for his last, you know, it could’ve been a lot worse, or…I don’t know if he, you know, he, not taking anything at all and just let the disease take its course, it would’ve been a longer, not so much physically painful, but more painful way to die, just the suffering I think. [Jane]
74
Subtheme: Use of aid-in-dying in good conscience Two people emphasized that their loved one would have had conflicted feelings
using aid-in-dying had it not been legal.
It meant so much to be able to do this in good conscience. I think, you know, this is going on all over the country. I’m quite certain…but that would’ve been an extra strain on her I think if she thought she was doing it illegally. I think she may have had some, some moral hurdles to get over, but, yeah. If it was against the law I don’t know what we would’ve done. [Roger] Theme 8: Experience of Death When reflecting on their loved one’s death, twenty participants emphasized being
appreciative that their loved one’s dying process was peaceful. It was not clear if this had
a great impact on grief, but was mentioned in terms of a positive impact on the overall
experience. Participants indicated strong support for this method of dying.
It was short. It was so calm, and, and the information that we were given was so calming that it was, for all of us. It was a blessed, holy time. Yeah. And they felt that too, they said that as well. Very peaceful. [Sarah] Well that was probably the most peaceful part of it, after he drank the drug, I don’t think it was even 5 minutes till he was like in a coma or something, and it was very, very peaceful, and it was like between 15 ad 20 minutes you could see the color go out of him and you knew he was gone. [Elizabeth] Subtheme: Complications in dying Three participants described complications in their loved one’s dying process, but
they did not indicate that this affected their grieving process.
One participant described how his loved one convulsed when taking the
prescription, which was surprising for him, but after that initial difficulty she died within
15 minutes. He still described the death as a good death.
One participant’s loved one vomited part of the medication, but died quickly. This
participant described the death as a very positive experience.
75
One participant described how her husband was telling a joke and smiling and
abruptly went into a coma 15 minutes after ingesting the prescription. She initially
experienced his transition into a coma as sudden:
And that was my husband. He was so much just like him that it was like someone shot him right in front of me. He was gone. [Linda] The death ended up taking an unusual amount of time (25 hours) which the
participant described as a blessing because it gave her a longer chance to say goodbye
and a chance to see him in a “dying and debilitating” state, which helped for making
sense of the death as opposed to if he had died immediately while talking with his family.
She also stated that it helped her make sense of his death to see him in the coma because
his disease was such (ALS) that he was still very alert in his mind, and although he was
suffering physically, it wasn’t always so clear to her that he was terminally ill when she
thought about other terminally ill people she had seen who were not as cognitively aware
or alert. Despite this difficulty in the dying process, the participant was still a strong
supporter of death from aid-in-dying and was very glad her loved one had the option.
Theme 9: Anticipating Death Participants discussed having anticipatory grief and having specific anxieties from
knowing the specific date when the death was planned.
Subtheme: Anticipatory grief Eleven people mentioned that they had anticipatory grief. Participants described
grieving beginning at the time of their loved one’s diagnosis. Eight participants felt that
anticipatory grieving eased their grief post-death, while 3 participants did not indicate if
anticipatory grieving had an affect on their grief post-death.
I think the really hard, hard grieving loss isn’t like it was when he first died, but I also tell people we started grieving the day we found out, you know, that was a year and a half long process. And
76
so his death was more closure for him, and you know, the ending of his pain that he was going through then, you know, something that you’re just not expecting and it happens. I think that makes a big difference. [Catherine] Subtheme: Anxiety from anticipating the day of death Six participants described having noticeable feelings the day before the death and
leading up to the moment of death from knowing when it was going to happen. People
described feeling anxious, surreal, or weird when anticipating the death. These 6
participants pointed out that this did not take away from their overall positive experience.
…when we were all sitting around, like the hour before he died, I kind of felt like, I wonder if this was like when people are on death row and you know that when you’re going to die, this is very odd, cause I know oh its like 45 minutes, K’s going to be dead. [Jane] …The hardest part in the whole thing was going to bed the night before. Hmm, my wife’s going to die tomorrow. That was just, that was, that was really the hardest part. [Sam] One of the 6 participants, although comforted that her loved one had the option of
DWD and had a positive experience, described initial anxiety both from knowing that her
loved one could choose to use the medicine at any time and from having him change his
mind over the timing of using the medicine.
Um, but, I guess what I’m trying to say is that, um, you know there’s, there’s… emotions changing related to his health and the illness, and having the DWD act option adds a layer to that of emotions. On the one hand, um, it was really, really comforting to have that option. And on the other hand, and this wasn’t true for D, but for me, it was harder sometimes too because, for instance, when he would say I’ve decided it’s time, um, and then we would talk about it some more and then you know, usually take a few days or a week for him to change his mind, um, it was a little bit of an emotional rollercoaster because several times he would say okay it’s time and then, and then he would decide it wasn’t time. [Natalie] Theme 10: Death with Dignity Act Process
Participants expressed support for Compassion and Choices and hospice, but also
expressed having difficulties with initiating the DWDA and feeling stigma from others.
77
Subtheme: Grateful for support with dying process Participants described how they were grateful for the help that hospice provided
with end of life care (n=9) and for the support from Compassion and Choices with
navigating the law and providing volunteers to explain the dying process from aid-in-
dying (n=11).
…They [hospice] were very supportive of him and helping him, you know, keeping him as comfortable as could be and getting him medications and just being here, and they, they even said, why are you bathing him? We can do that. You know, they just took a lot of load off the family in general, which was nice. [Jane] I think Compassion and Choices is wonderful. They were so helpful, um, and I think it’s really important that there be some kind of organization for that. It’s like K [C&C volunteer] knew and I remember her a couple of times going thru it with M. I think she had three visits with M before the, before the final one, and just being able to know step by step, you’re going to take this drug and it’s going to do that and take it with this drug and it’s going to do that, and then within, what is it, half hour, they do the premeds, I think a half hour, and then you’re going to take this and it’s going to taste really awful, it will be really bitter, but you just drink it down and then this is going to happen and this is going, it’s just, what a comfort. [Maureen] Subtheme: Difficulties with seeking DWD Nine participants described having difficulty obtaining signatures from doctors to
approve the DWD process. Reasons included facility religious policies against the DWD
act or discomfort with approving the use of aid in dying. Three participants experienced
what they felt was unkind treatment or words from doctors after requesting information
on the DWD act. They did not say whether or not this affected their grief, but they did
express feeling bothered that their loved one was treated poorly.
I think what he said, was, because it was a Catholic hospital he can’t write the prescription, but he understood why people would do it. The other doctor, who also was Catholic, he was at ___, told A point blank, he says, the only people who, uh, participate in DWD are, um, atheists and um…another word for egoists, you know, self-absorbed people. [Ted]
78
One of these 3 participants also related a distressing experience where a doctor
had agreed to sign the necessary papers to receive the aid-in-dying prescription and then
changed his mind without informing the family and avoided their calls. This caused a
delay in the process for obtaining the prescription. The law requires that the person using
the prescription ingest the medicine on their own, and her loved one was unsure of how
quickly his health and physical ability to ingest the medicine would decline. He feared
losing the opportunity to use the law from this delay.
Subtheme: Stigma from others Four participants described feeling stigma associated with aid-in-dying, with
some expressing stigma from multiple sources.
One participant felt that pharmacists felt a stigma from providing a prescription
intended to end one’s life. This participant also felt stigma from federal government
policies which limit the amount of the aid-in-dying prescription that can be made or
manufactured.
One participant explained how in a small community there is a lot of fear among
the doctors to support aid-in-dying. They disagree with it philosophically and even
though it is legal, there is fear of lawsuits. This participant described aid-in-dying as
being similar to abortion in the way that it’s legal but there is stigma that accompanies it.
This participant also reported feeling she received a disapproving look from a doctor
when at church.
Another participant described feeling nervous when going to the pharmacy to pick
up the prescription from feeling that aid-in-dying is taboo. She also made a reference to
the stigma associated with abortion. The participant was relieved when the pharmacist
treated her kindly:
79
And part of me is watching this and it’s just surreal. And part of me knows this is exactly the right thing to do and there’s a little part of me always sits, the culture , and that was true when we went to get the prescription, when we went to the drugstore that evening I felt like I was, like walking into an abortion clinic, you know, that taboo, I wonder what will happen at the counter, and there were a lot, this was evening, and there were a lot of people around the counter and what would be said and why we were there and if whoever gave us the prescription would, would say something about, “oh? 3 months worth of secanol? “ You fantasize what’s going to happen. And so this young , tall, nice pharmacist came and said I was able to get insurance to pay for one moth of your prescription. Made no other comment. And I said I really appreciate your drugstore, um, cooperating with this. And he said, and I won’t name the drugstore b/c we try to keep that confidential, “we feel the people of OR deserve an option” and it just washed over me and I felt so comforted….[Jennifer] This participant also experienced stigma from a funeral home worker. The funeral
home worker was aware that aid-in-dying had been used and incorrectly insisted that the
death certificate would need to read “suicide,” even though pre-arrangement had been
made for the death certificate not to list cause of death as suicide as legally aid-in-dying
is not considered to be suicide. The participant felt like the funeral home worker blamed
and chided her.
One person received a negative reaction from a neighbor. This participant relayed
feeling very angry when neighbors questioned her young daughter about how their loved
one died and told her that her loved one was committing a sin. Her daughter was upset
and felt verbally attacked.
Theme 11: Expressing Grief Seventeen participants said that they self-select who they tell that their loved one
used aid-in-dying. Reasons for being selective about who to tell included honoring their
loved one’s wishes to not tell others, wanting to avoid conflict with friends or family
members who might disapprove, and being unsure of what others think about the law and
not wanting to make others uncomfortable. For some participants, their loved one’s use
of aid-in-dying is not a secret, but it is not something they bring up. If it comes up in
80
conversation they do talk about it. While people self-selected who they told, everyone
had support from family members and friends who did know. In most cases, people
needed to express their grief from their loss rather than any troubled feelings over aid-in-
dying.
Well most of the people that I’ve discussed it with knew that that was what he wanted. Other people I’ve not told, just that he died. I don’t really feel that it’s any of their business, and I’m not always sure, I mean it’s, it’s such a private thing. I’m not always sure how people feel. I have some people that I know I would not ever tell because of their religious beliefs…People that I think would understand and, I have talked to them about it, and most of them because they saw him go down so bad and knew how bad he was, most of them understand, and whether it’s their personal belief that that’s what they would want to do, uh, I think most of them understand. [Elizabeth] Four participants who had some conflict related to aid-in-dying reported that they
needed to find someone to talk with about their feelings. Two of these 4 participants
expressed their conflict to their pastor. One participant spoke about her conflict to a
bereavement counselor and the last participant had others she could talk to. One of the
four participants said that during the illness process she did not have anyone to speak to
about her conflicted thoughts about aid-in-dying because her loved one initially wanted to
keep the decision private. This participant felt a relief when her loved one did inform
others of his decision before dying and she was able to discuss her thoughts. She felt able
to express her grief to others after her loved one died as well. These participants
experiences are further described in the next theme, grief reconciliation from aid-in-
dying.
Theme 12: Grief Reconciliation from Aid-in-dying As previously discussed, grief was eased by being able to say goodbye, knowing
that aid-in-dying was the loved one’s choice, knowing it was legal, personal and family
81
agreement with the loved one’s decision, and support from others. There were 5
participants who expressed some additional conflict in their grieving process.
Two participants wondered if it was the right decision. Their grief was reconciled
by knowing that it was what their loved one wanted. One of these participants also
reconciled grief by attending a grief support group where it was discussed that death from
a terminal illness is inevitable.
…I’ve gone to a grief group and some of the things in the grief group that I learned or that was very helpful is you’re with other people who have lost loved ones, and part of the thing is, especially when you have something like somebody deciding to go with aid-in-dying DWD is well, maybe I shouldn’t, maybe I should’ve stopped him, maybe I should’ve not supported him in this at all. Maybe I should’ve just stopped him and not been, not been in agreement with it all, and the thing that we kept talking about in the group is that death is not optional. When you get into the terminal phases, it’s not optional. You can, it can be with some aid in being in control, or it can be helping out on your own. It can be in a hospital or in the homes, It can be, you know, but there’s a lot of variables that can happen around death, but death itself is not optional. We die…[Ingrid] Two participants spoke with their pastor about their conflict and felt their grief
was eased after having the support of the pastor.
One participant had some professional conflict about her loved one using aid-in-
dying. This participant supported the law by voting for it and supported her loved one’s
decision, but felt conflict as a nurse. She was not present at the time of death as she felt it
professionally clashed and reconciled grief by realizing that her loved one was soon
going to lose the ability to swallow and use the law.
Theme 13: Minimal Uncertain Feelings Over How to Act or Behave Following a Death from Aid-in-dying Sixteen participants expressed no uncertainty as to how to behave or feel as a
survivor from a death from aid in dying. Several participants even emphasized their
support for the law and discussed how they think it is important to tell others about their
82
positive experience. A few of the participants mentioned that their support for the law is
the reason why they volunteered to be in this study.
Six participants expressed some uncertainty, with some expressing multiple
concerns. Three participants expressed uncertainty in talking about aid-in-dying with
unfamiliar people because it is difficult to know what others’ personal beliefs or opinions
are about the subject and how they might react. Although these participants were willing
to talk about their experience with others, they’re not interested in having to debate
whether or not aid-in-dying should be legal.
I guess I’m a bit careful when I talk to people about it, cause I know that there are all these different belief systems and just as I don’t want to have them try to convince me or debate me, I’m not able to debate with them, I’m there to share if they’re interested, curious and so when I meet new people and the issue would happen to come up, I always preface it with I’m not sure how you feel about this, this was an option that really fit for us, but I know it doesn’t fit for…[Jennifer] One participant mentioned that while she was comfortable participating in this
study, she did not feel ready to talk publicly about her experience.
One participant described feeling uncomfortable and uncertain as to how to
explain to the home health aide and hospice nurse that they didn’t need to return the next
day because her loved one would be using aid-in-dying. This participant felt that it may
have been unethical not to let the nurse and aide know beforehand that her loved one was
using aid-in-dying because their nursing duties, which they counted on for income, would
suddenly end without notice. She was hesitant to inform the aide about her loved one’s
decision because she feared that the aide might have disapproved due to her religious
beliefs. The aide had been very caring toward her loved one and she also worried that her
loved one’s decision might hurt the aide’s feelings. This participant also expressed
uncertainty about whether or not she should tell others about her loved one’s use of aid-
83
in-dying. She was very grateful to have been present at her loved one’s death and for the
moments she shared with him at the time of and directly after his death. However, she
only felt able to express this to those whom she didn’t mind knowing that he used DWD.
She worried that people might ask how it was possible that she was able to be present at
her loved one’s death and say goodbye.
One participant relayed a situation that happened early in her grieving process
where she wanted to talk about her experience and defend aid-in-dying when someone
was critical of it but felt unable to. The situation occurred at a church social event where
the movie Inside the Sea, in which the main character, a quadriplegic, campaigns to use
euthanasia to end his life was being shown. In the discussion that followed afterwards,
someone spoke about euthanasia being the “easy way out.” This participant wanted to
respond and share her experience and views that it takes courage to use aid-in-dying, but
she felt unable to speak up since it was early in her grieving process. She explained that
she would be able to talk about it now after having some years to grieve and heal from
her loss. This participant also described feeling uncertain when going to pick up the
prescription for aid-in-dying about how the pharmacist and others present might react,
and feeling discomfort when a funeral home worker treated her unkindly after hearing
that her loved one used aid-in-dying.
One participant discussed feeling hesitant to talk about topics related to death and
dying, such as aid in dying, because death is a taboo subject.
One participant noted feeling uncertainty about the procedure for using the Death
with Dignity Act, mentioning details such as feeling unsure as to which pharmacies
would supply the prescription, and what the shelf-life of the prescription was.
84
Chapter 5
Discussion
This is the first study, known to the author, that focuses on bereavement
experiences of persons who had a family member die using Oregon’s aid-in-dying law,
the Death with Dignity Act. Other studies about family members’ experiences with aid-
in-dying have focused on the loved one’s motivation to use aid-in-dying (Pearlman et al.,
2005; Ganzini et al., 2008), views of aid-in-dying (Ganzini et al., 2006), and caregiving
experiences (Starks et al., 2006).
This is also one of only a few qualitative studies on aid-in-dying. Most studies on
aid-in-dying have been quantitative, focusing on topics such as motivations to use aid-in-
dying (Ganzini et al., 2009), and healthcare workers experiences with the Death with
Dignity Act (Ganzini et al., 2002; Ganzini et al., 2000). The qualitative research design of
the current study allowed participants to share in-depth, detailed information from their
perspective, providing a unique look at grief and bereavement from aid-in-dying. The
following sections discuss the results of the analysis, limitations of the study, and
recommendations for future studies.
Common Grief Reaction, Grief Reconciliation, and Grief Theories
Results of this exploratory study indicate that there is a broad overlap between
grief reactions and grief reconciliation following a death using aid in dying and general
grief reactions and grief reconciliation experienced following any type of death. Some
common grief reactions included feeling sad, angry, numb, and feeling a sense of loss
and disbelief. Common grief reconciliation included recalling memories of the loved one,
journaling about feelings associated with the loss, honoring the loved one with a
85
celebration of life ceremony, receiving support from others, engaging in social and/or
work or volunteer activities, gaining a new sense of identity, and adjusting to life without
the deceased. The grief reactions and ways of reconciling grief are consistent with task
and phase models of grieving which emphasize accepting the loss, experiencing grief
reactions, and adjusting to life without the person who died (Sander, 1999; Worden,
2002;).
Kenneth Doka’s theory of disenfranchised grief suggests that if the circumstances
of death, in this case aid-in-dying, are not socially sanctioned and grief cannot be openly
acknowledged or expressed, then the grief becomes disenfranchised, or hidden,
intensifying and complicating grief reactions and making grief reconciliation more
difficult. Although results from this study indicate that participants do express feeling
social stigma and are not open in telling everyone about the mode of death, all have a
large support system of people with whom they can openly grieve. Only one participant
expressed some distress over whether or not she should tell others about her loved one’s
use of aid-in-dying, and noted that while she is very grateful that she was able to be with
her loved one at the time of his death, she feels that she can only share this with people
who she is comfortable telling that her loved one used the DWDA. While she did not say
that this affected her grief and did say that she had people with whom she could grieve, it
did seem to be troubling and she possibly could be experiencing some level of
disenfranchised grief. It is not clear though. Others did not seem to be affected by their
decision to self-select who they told. They explained matter-of-factly that they decided
not to tell certain others for what they considered to be practical reasons. While there is
controversy over aid-in-dying and it is not universally socially accepted, only one
86
participant in this study potentially experienced disenfranchised grief. Several
participants did indicate that they felt social stigma, mainly from those in the medical
field. While this clearly bothered participants, it did not seem to have an impact on their
ability to express their grief.
One participant who had conflict over her loved one’s decision to use aid-in- was
unable to discuss this conflict with others for some time because her loved one had not
wanted to share his decision with others. After her loved one changed his mind and
informed others of his decision, the participant expressed feeling like a weight was lifted
when she could talk about his decision and no longer had to keep it a secret. After she
was able to discuss her loved one’s decision with others, her grief following the death
focused on dealing with her feelings from the loss of her loved one rather than the mode
of death. This supports the idea in Doka’s theory that if grief cannot be expressed, then it
intensifies, although this occurred before the participant’s loved one’s death.
Grief from Aid-in-Dying vs. Sudden Death
Those who pursue and decide to use aid-in-dying are encouraged but not required
to notify their next of kin about their decision to use the law, (Oregon Department of
Human Services, 2008; Miller et al., 2006) so it is possible that family members could
experience a loved one’s death from aid-in-dying as sudden if they were not aware of
either their loved one’s decision, or the chosen date to use aid-in-dying. In this study,
however, all participants were aware of their loved one’s decision to use aid-in-dying and
had the option of being present at the death, thus experiencing the death as anticipated.
Similar to studies comparing grief from anticipated deaths and grief from sudden
deaths, participants in this study emphasized that grief from a death from aid-in-dying
87
was easier to deal with than grief from a sudden death because aid-in-dying, like
anticipated deaths, allowed for the opportunity to say goodbye, address any issues with
their loved one, and prepare for the upcoming loss (Rando, 1984; Zisok, 2000).
Participants also described that their grief from aid in dying was less intense, less
shocking compared to grief from a sudden death, and that the death was easier to make
sense of. These findings are similar to other studies on anticipated versus sudden deaths
(Deranieri et al., 2002; Rodger et al., 2007).
Grieving from Aid-in-Dying vs. suicide
Participants did not compare their grief from aid in dying to grief from a suicide,
but several made comparisons of suicide and aid-in-dying. One person stated that they
were two completely different situations. One person highlighted differences in feelings
at the time of death, noting that suicide is filled with anger, despair, and vengeance. One
person explained that suicide is generally done in secrecy and the fact that aid-in-dying is
legal allows for an opportunity for openness. One participant explained that although she
considered the cause of her loved one’s death to be an overdose, she didn’t consider her
loved one’s death to be a suicide her because he was terminally ill and there was no cure
for his condition. She clarified that aid-in-dying was similar to a hastening, although she
still considered the process to also be overdosing. It is implicit that the openness that
comes with the legal sanctions of aid-in-dying allow for this participant to differentiate
her loved one’s dying process as different from suicide. There could be an instance where
persons with a terminal illness take their own lives by overdosing in secrecy and this
grieving process might look very different than a grieving process from aid-in-dying.
There could also be instances where persons with a terminal illness take their life in
88
secrecy and in a violent manner, which would affect grief differently than grief from a
death using the DWDA that is not done in secrecy. Another possible situation is that a
person could use aid-in-dying in secrecy, which would also affect grieving in a very
different way than knowing the specific date and time the loved one planned to use aid-
in-dying. Several other participants also used the word hastening in their interviews as
well to describe aid-in-dying. Participants’ opinions on the differences between aid-in-
dying and suicide and their use of the word hastening to describe aid-in-dying also
indicate that aspects of their grief would be processed differently than they would from a
suicide.
Bereavement studies on suicide indicate that the bereaved feel guilt and shame,
and a sense of rejection from their loved one (Dunn & Morrish-Vidners, 1988). Studies
on grief following a spouse’s suicide show that the bereaved wondered about their
spouse’s motivation for ending their life, felt embarrassed by and lied about the mode of
death. Data from this study did not find that loved ones had these reactions during
bereavement. Participants did not report feeling guilt, shame, embarrassment, or a sense
of rejection. Many participants described feeling proud of their loved one for choosing to
use aid-in-dying, referring to the their loved ones as brave and courageous. The loved
ones’ motivation to end their life, or hasten their death, was clear to the participants, and
almost all participants agreed without hesitation with their loved one’s decision to use
aid-in-dying. Participants did not lie about the mode of death if asked if their loved one
used aid-in-dying, but oftentimes this information was withheld either out of respect for
their loved one’s wishes to not tell others, to avoid potential conflict from those who
89
might disapprove, from feeling unsure about others’ feelings about aid-in-dying and not
wanting to put them on the spot, or because it did not come up in conversation.
Most participants considered the cause of death to be their loved one’s terminal
diagnosis. In these instances, aid-in-dying wasn’t brought up because it was a secret, but
because it wasn’t considered a cause of death. Studies on bereavement from suicide also
show that the bereaved report receiving less community support and negative reactions
from others (Barrett & Scott, 1990; Harwood et al., 2002; Houck, 2007; Range &
Calhoun 1990; Seguin et al., 1995; Silverman et al., 1995), which was not the case with
participants in this study who all reported receiving adequate support and mostly positive
reactions. Again, participants self-selected who they told about the use of aid-in-dying,
but participants reported that those who did know were supportive. Negative reactions
from others were minimal. One person reported receiving a negative reaction from a
neighbor, one person received a negative reaction from a funeral worker, and one person
is unsure, but feels that she may have received a disapproving look from someone who
knew that her loved one used aid-in-dying.
While most participants in this study indicated that others reacted supportively, 6
participants reported feeling that there is a stigma in the medical community. Similarly,
some studies on bereavement from a suicide have found that people report feeling
stigmatized from others (but not specifically the medical field) (Harwood, 2002; Range
and Calhoun, 1991).
Another overlap with grief reactions from a suicide is feeling uncertainty about
who can be told about the mode of death due to not knowing how others will react.
Studies on suicide and bereavement also report that the bereaved feel uncertain about
90
how to act or behave (Van Dogen, 1993; Fielden, 2003). Participants in this study did not
feel uncertain about how to act, but 4 participants did express uncertainty about telling
others about the mode of death due to being unsure of how others felt about the law. One
participant was in a situation where someone was publicly criticizing aid-in-dying. The
participant wanted to speak up about her loved one’s decision and defend the DWDA, but
felt uncertain at the time because it was early in the grieving process. She explained that
now that it has been years since her loved one died, her grief is less intense, and she is
able to speak up about her beliefs and her loved one’s mode of death.
Anticipatory Grief
Studies on the impact of anticipatory grief on the experience of bereavement after
a death have produced mixed results. Some studies have found that when a death is
anticipated, grieving starts before the person has died, and as a result grief after the death
is less intense (Rando, 1984; Zisook, 2000). Some studies have reported that anticipatory
grief has negative outcomes for bereavement while other studies show that anticipatory
grief has either mixed results on bereavement or no impact on bereavement (Reynolds &
Botha, 2006). Results from this study were consistent with studies that showed that
anticipatory grief eased grief following the death. In this study participants also
mentioned having anticipatory grief, but did not indicate if it affected their grief post-
death.
Another result with this study related to grieving beforehand is that some
participants had anxiety over knowing the specific day and time that their loved one was
going to die. This did not seem to affect grief after the death but was part of the feelings
or grief involved with anticipating the death.
91
Grief from Aid-in-Dying vs. Grief from Anticipated Illness
Grief from aid in dying and grief from an anticipated illness were similar in the
sense that the death was not experienced as sudden. However, those who compared their
grieving experience from aid-in-dying to their grieving experience from an anticipated
illness felt that their grief was eased from knowing that their loved one had a sense of
control over the dying process, and that they were able to avoid prolonged suffering.
Grief was also eased from the opportunity that aid-in-dying provided to plan for the
actual death in terms of rituals and who was going to present, and to say goodbye at the
moment of death.
Grief and Grief Reconciliation After a Death from Aid-in-dying
For many participants in this study, grief arose from the loss itself rather than
from the particular mode of death. This finding was consistent with results from
Thomasina et al’s (1998) study of grief following death by euthanasia. Thomasina et al’s
study is not directly comparable since euthanasia is different than aid-in-dying, but the
results can be compared on the basis that both are modes of hastening a death .
In this study, grief from aid in dying was eased by being able to say goodbye,
knowing that aid-in-dying was the loved one’s choice, knowing it was legal, having
personal and family agreement with the loved one’s choice and receiving support from
others. These were consistent with Starks et al’s (2007) findings that the legal status and
agreement with and support for the loved one’s decision affects grief. This study
additionally shows that conflict in grief arose from wondering if it was the right decision,
not agreeing with loved one’s decision to use aid-in-dying (as in Starks et al’s study),
religious conflict, and professional conflict arising from working in healthcare and
92
feeling aid-in-dying is contradictory to professional goals. In these cases, grief
reconciliation included thoughts that it was what the loved one wanted, thoughts that the
loved one was close to death and would soon lose ability to ingest the prescription for
aid-in-dying, a requirement for DWD, support from hospice bereavement groups that
discussed how death is inevitable but timing and mode can be optional, and talks with
and approval from church religious leaders.
Starks et al’s study on family caregiving with hastened deaths showed that the
legal status of aid-in-dying affects grief. Consistent with Starks et al’s findings, results
from this study show that participants were grateful for the legal support and option and
glad that their loved one’s wish to use aid-in-dying was met. Additionally, results from
this study indicate that participants appreciated the sense of control that aid-in-dying
provided for their loved one, and that the law made it possible for their loved one to avoid
prolonged suffering, and to avoid considering suicide. Participants were also glad that
there were safeguards in the law with a process to follow and that the legal status made it
possible for their loved ones to seek a hastened death in good conscience.
Starks et al found that disagreement with a loved one’s decision to use aid-in-
dying complicates grief. Results were the same in this study.
This study also looked at the impact of family agreement with their loved one’s
decision to use aid-in-dying. Participants stated that had there been conflict within the
immediate family over their loved one’s decision, this would have complicated the
grieving process. However no major family conflict was reported among any participants.
There were some participants whose family members did not know about their loved
one’s decision to use aid-in-dying and one participant who had family members who
93
disapproved of her loved one’s decision but were still supportive. This participant’s grief
was eased by her family members’ support despite their conflicted feelings about the law.
Two participants had extended family members who disapproved, but this did not have
an impact on grief because the disapproving family members were not emotionally close
with the participants or loved one.
Limitations
While the qualitative methodology used in this study has the benefit of allowing
participants to express their in-depth perspectives about grief, and to give insight into the
complexities of grief from aid-in-dying, there are also limitations of this study. There
were 22 subjects who were self-selected and therefore the results are not generalizable to
the greater population of those who had a family member who died with the use of aid-in-
dying. The study should be repeated with a larger sample size to gain more data and
possibly different perspectives on grief from aid-in-dying. Although qualitative methods
allow participants to explain phenomena in their own words and analysis involves coding
data until a saturation point, qualitative methods also allow the potential for bias in
results since participants’ words are interpreted by the researcher.
It is possible that some people who received the invitation to participate in the
study chose not to do so because they are either uncomfortable with the topic, or are
currently experiencing distressed grief. It is also possible that those who did participate
had reconciled their grief to a certain extent, so any conflicts in grief may not have been
brought up. Several participants mentioned that the reason they participated in this study
was because they had had a good experience and hoped that sharing their good
experience would bring further support for the law. They understood that the focus of the
94
study was grief and not support for or opposition to the law, but were earnest in wanting
to share their good experience in hopes that the results might encourage others to support
the law. They also wanted to share their experience in order to help others who might
have loved ones considering the option to understand the dying and grieving process
from aid-in-dying. Although it seemed that participants were very honest about their
grieving process and the conflicts that they did experience, it is possible that participants
painted an easier picture of their grief, or are in denial about possible difficulties in grief
from aid-in-dying due to their desire to maintain continued public support for the law.
Several participants expressed their appreciation for the support offered by
Compassion and Choices for navigating the law and helping their loved one through their
dying process. Although Compassion and Choices mailed recruitment letters to all family
members who had been bereaved in the past three years and did not influence participants
to participate, it is possible that some participants may have felt an obligation to be
positive about their experience because of the help Compassion and Choices provided.
Many participants were sorting out their feelings as they responded to questions,
often changing their response as they reflected upon their feelings. For example, in
response to the question “Did your agreement with your loved one’s decision to use aid-
in-dying affect your grief?”, several participants initially said no, and then paused and
reflected and then explained that agreement made it easier. One person felt that her
conflicted agreement impacted her grief but was initially unable to pinpoint exactly why
and how her grief was impacted. She eventually was able to identify the source of
conflict and impact on grief after talking through her feelings. Because of these
ambiguities, it is possible that participants expressed one opinion during the study, but
95
later when reflecting on their own after the interview may have changed their mind.
Several participants indicated this was the first time they had thought about some of the
questions. They may have responded differently had they had more time to reflect upon a
question. Participants were reflecting back on their grieving experiences and may not
recall their feelings correctly. One participant even questioned how self aware he was
when responding to questions, indicating that what he expressed about his grieving
process may have been different that how it actually was.
Participants were not provided with a definition of grief. Depending on how
participants conceived of grief, they may or may not have expressed all grief feelings or
the full extent of how their grief was impacted. For example, one participant had conflict
with her loved one’s decision to use aid-in-dying, but when asked if it impacted her grief
responded that there was probably a subtle impact on her grief but not in terms of missing
her loved one. Her response indicated that part of her definition of grieving included
missing her loved, but it was unclear what else grief meant to her. A follow up question
asking for more information about the subtle impact may have provided more insight.
This participant mentioned throughout the interview that she had felt stress related to not
being sure who she could tell about her loved one’s decision to use aid-in-dying based on
how they might react, however, when asked if she could express her grief to others, she
replied yes, with a disclaimer that she may be fooling herself. It is unclear if the stressful
feelings related to not being able to express to others that her loved one had used aid-in-
dying did not impact grief, if feelings were recalled incorrectly, or if her answer may
have been different had a definition of grief been provided. It is possible that some
participants may have left out descriptions of their grief because their own personal
96
definition of grief did not include certain feelings or actions. Responses about grief may
have been different had a common definition of grief been provided.
Benefits and Future Studies
Despite limitations, this study does contribute to information on the grieving
process following a death from aid-in-dying and may be helpful for those who are
grieving a death from aid-in-dying. The results from this study can be used to improve
services for those bereaved from aid-in-dying. Bereavement counselors should be aware
of the unique conflicts that are specific to those grieving from a death from aid-in-dying,
such as conflict in agreement due to religion or personal beliefs, thoughts related to the
timing and whether or not the decision in general was the right one. Counselors should
also be aware of social stigma and uncertainties about expressing the loved one’s use of
aid-in-dying.
Future studies should replicate this study with a larger sample size. Future studies
should also use mixed methods, which could provide more insight into the grieving
process. Another area for future studies involves analyzing the impact of demographic
differences on grief, taking into account factors such as age, gender, religion, type of
disease, and length of bereavement. Personality of the person who died and personality of
the bereaved are other areas for future research.
In the current study, interviews were conducted with only one family member.
Future studies could interview multiple family members to gain an understanding of how
the use of aid-in-dying affects a family system.
Participants in this study were all aware of their loved one’s decision to use aid-in-
dying, and all were present for their loved one’s death, although a few were not in the
97
same room at the time of death. The law states that “the prescribing physician must
request, but may not require, the patient to notify his or her next-of-kin of the prescription
request” (Oregon Department of Human Services, 2008, p.2). It is possible that a loved
one could use aid-in-dying in secrecy, which could complicate grief. Future studies
should seek to include participants with a broader range of experience with the law and
compare grief from an unexpected death from aid-in-dying to grief from a sudden death,
grief from a suicide, and grief from an anticipated death from a terminal illness. One
participant may have experienced disenfranchised grief, but it was not clear as she
relayed that not being able to openly acknowledge the mode of death did not impact her
grief. The relationship between disenfranchised grief and aid-in-dying is another potential
area for research.
Aid-in-dying is also legal in Washington and Montana, although the law in
Montana is being challenged in the Supreme Court. Assisted suicide is legal in the
Netherlands and euthanasia is legal in both the Netherlands and Belgium. While
euthanasia has not been made legal in Switzerland, their law does protect those who
perform and use euthanasia. Future studies could compare Oregon, Washington, and
Montana, or the U.S. and the Netherlands, Belgium, and Switzerland, and examine how
the level of acceptability, the length of time since the law was passed, and other factors
affect grief.
In conclusion, this is an understudied area of grief that should continue to be
examined. Two states have an aid-in-dying law and there is a movement to continue
making aid-in-dying legal across the United States. There is a need to continue
98
researching topics explored in this study so that we can better understand and support
families whose loved one chooses aid-in-dying.
99
References
American Psychological Association (n.d). Assisted suicide. Retrieved April 22, 2007
from http://www.apa.org/pi/eol/arguments.html
Averill, 1968. (2003 – 2004). Grief: Its nature and significance. Psychological Bulletin,
70(6), 721 – 748.
Bailey, S., Kral, M., Dunham, K. (1999). Survivors of suicide do grieve differently:
Empirical support for a common sense proposition. Suicide and Life-Threatening
Ball, J. (1976 -1977). Widow’s grief: The impact of age and mode of death. Omega,
Journal of Death and Dying, 7(4), 307 – 331.
Barrett, T., & Scott, T. Suicide bereavement and recovery patterns compared with
nonsuicide bereavement patterns. Suicide and Life-Threatening Behavior, 20(1),
1 – 15.
Baskerville, R., & Pries-Heje, J. (1999). Grounded action research: A method for
understanding IT practice. Accounting, Management and Information Technology,
9, 1 – 23.
Beder, J. (1998). Bereavement after a physician-assisted suicide: A speculation based on
theory. Suicide and life-threatening Behavior, 28(3), 302 – 308.
Beder, J. (2004). Voices of bereavement: A casebook for grief counselors. United States:
Taylor & Francis Books, Inc.
Berg, B. (2001). Qualitative research methods for the social sciences. Masachusetts:
Allyn & Bacon.
Blank, R., & Merrick, J. (2005). End-of-life decision making. Cambridge, Massachusetts:
MIT Press.
100
Bonanno, G., & Kaltman, S. (1999). Toward an integrative perspective on bereavement.
Psychological Bulletin,, 125(6), 760 – 776.
Bowlby, J. (I980a). Attachment and loss, Vol. 3: Loss, sadness and depression. New
York: Basic Books.
Bowlby, J., & Parkes, C. M. (1970). Separation and loss within the family. In E. J.
Anthony & C. Koupernik (Eds.), The child in his family: International Yearbook of
Child Psychiatry and Allied Professions (pp. 197-216), New York: Wiley.
Calhoun, L., & Allen, B. (1991). Social reactions to the survivor of a suicide in the
family: A review of the literature. Omega, 23(2), 95-107.
Calhoun, L., Selby, J., & Abernathy, C. (1984). Suicidal death: Social reactions to
bereaved survivors. The Journal of Psychology, 116, 255 – 261.
Campbell, C. (2000). Euthanasia and religion. The Unesco Courier, 37-39.
Carr, D., & Utz., R. (2001). Late-life widowhood in the United States: New directions in
research and theory. Ageing international, 27(1), 65 – 88.
Carroll, J. (2007). Public divided over moral acceptability of doctor-assisted suicide.
Asking to die: Inside the Dutch debate about euthanasia. Dordrecht, The
Netherlands: Kluwer Academic Publishers.
Van Der Wal, J. (1989 – 1990). The aftermath of suicide: A review of empirical
evidence. Omega, Journal of Death and Dying, 20(2), 149 – 171.
Van Dongen, C. (1993). Social context of postsuicide bereavement. Death Studies, 17,
125-141.
Views on doctor assisted suicide follow religious lines (2002). Retrieved February 14,
108
2008 from http://www.gallup.com/poll/6754/Views-DoctorAssisted-Suicide-
Follow-Religious-Lines.aspx.
Worden, W. (2002). Grief counseling and grief therapy: A handbook for the mental
health professional (3rd edition). New York: Springer publishing company, Inc.
Zisook, S. (2000). Understanding and managing bereavement in palliative care. In H.M.
Chochinov, & B. William (Eds.), Handbook of Psychiatry in Palliative Medicine.
(pp. 321 – 324). New York: Oxford university press, Inc.
109
Appendix A
Dear , Compassion and Choices of Oregon has been approached by Erica Srinivasan, a PhD graduate student at Oregon State University, and Dr. Patricia Moran, a professor at Oregon State University, regarding a research project Erica is conducting for her dissertation about the bereavement experience under the Death With Dignity Act. You might be interested in participating in this study. The attached letter from Erica describes the study. Participation in the study is entirely voluntary. Refusal to participate will not affect your relationship with us. All results are confidential, for research purposes, and neither placed in your record nor released to our staff. We have not released any information about you to these researchers. Compassion and Choices of Oregon is independent of this study and is not conducting this study. We support Erica’s efforts to better understand the experience of bereavement of those who have had a loved one die under Oregon’s Death With Dignity Act.
If you would like to participate in this study, please contact Erica directly either by email : [email protected], or by phone: xxx-xxx-xxxx (Portland area code). Please contact us if you have any questions or concerns about the study. Sincerely, George Eighmey Executive Director Compassion and Choices of Oregon xxx-xxx-xxxx
110
Appendix B
Dear , My name is Erica Srinivasan. I am a PhD student in the department of Human Development and Family Sciences at Oregon State University. For my dissertation research I am conducting a study entitled “Bereavement experiences following a death under the Death with Dignity Act.” I am inviting you to participate in this academic study. I am interested in your participation because you have had a loved one use aid-in-dying. Results from this study will have the potential to help others who have had a loved one use aid-in-dying under the Death With Dignity Act.
Many studies have been published on various aspects of aid-in-dying, such as opinions of medical professionals, characteristics of persons who use aid-in-dying, and healthcare workers experiences with aid-in-dying, but virtually nothing is known about bereavement. The best way to explore this topic is to directly ask people, such as you, about their experiences. Those who choose to participate in this study are in a unique position to inform and help others who find themselves in similar circumstances.
Participation in this study will include a 1-3 hour interview about your loved one and the feelings you experienced after your loved one’s death. I would be happy to come to your home, or wherever you feel comfortable to conduct the interview I have had experience working with families through hospice and have a lot of compassion for anyone who has lost a loved one. I am very interested in hearing about your experience. If you are interested in participating in this study, please contact me either by email: [email protected], or by phone at xxx-xxx-xxxx (Portland area code). Thank you for your time. Sincerely, Erica G. Srinivasan
111
APPENDIX C
INFORMED CONSENT DOCUMENT
Project Title: Bereavement experiences following a death under the Death with Dignity Act Principal Investigator: Patricia Moran, PhD, Human Development and Family Sciences Co-Investigator: Erica G. Srinivasan, PhD candidate, Human Development and Family Sciences WHAT IS THE PURPOSE OF THIS STUDY?
You are being invited to take part in a research study designed to explore the bereavement experience following a death from aid-in-dying under the Death with Dignity Act. The results are intended to help add to our understanding of the grief process associated with a death from aid-in-dying.
WHAT IS THE PURPOSE OF THIS FORM?
This consent form gives you the information you will need to help you decide whether or not you wish to participate in the study or not. Please read the form carefully. You may ask any questions about the research, the possible risks and benefits, your rights as a volunteer participant, and anything else that is not clear to you. When all of your questions have been answered, you can decide whether or not you want to participate in this study.
WHY AM I BEING INVITED TO TAKE PART IN THIS STUDY?
You are being invited to take part in this study because you are over the age of 18 and have had a family member or close friend die under the Oregon Death with Dignity Act within the past three years.
WHAT WILL HAPPEN DURING THIS STUDY AND HOW LONG WILL IT TAKE?
If you decided to participate in this study you will be interviewed for approximately 1-3 hours about your bereavement experiences. Questions will be asked that pertain to your relationship to your loved one, your feelings and family members feelings about your loved one’s decision to use aid-in-dying, feelings about your loss and grief, and questions related to reactions and support you received from others. The interview will take place shortly, here at this current location.
WHAT ARE THE RISKS OF THIS STUDY?
It is possible that you could feel upset after talking about your grief over a loved one’s death. We hope that sharing your grief will be a positive and cathartic experience. We will provide you with a list of community resources you can access in the unlikely possibility that this interview raises issues you wish to continue talking to a professional about.
112
WHAT ARE THE BENEFITS OF THIS STUDY? We do not know if you will benefit from this study. However, we hope that you will find participating in this study to be a positive experience. We also hope that other people will benefit from the knowledge about the grief process following a death from aid-in-dying that will be gained in this study. We will send you a brief written summary of the results.
WILL I BE PAID FOR PARTICIPATING?
You will not be paid for being in this study.
WHO WILL SEE THE INFORMATION I GIVE?
The information you provide during this research study will be kept confidential, as is required by law. To help protect your confidentiality, no identifying information will be on the tape recording. All respondents will be given an id number that will be the only way you are identified. Data and informed consent forms will be kept in separate locked filing boxes in the student researcher’s home office until data collection is complete. Only the student researcher will have access to this locked filing box. After data collection is complete, informed consent forms and all data will be kept in separate locked filing boxes in the primary investigator’s office at Oregon State University. Only the student researcher and primary investigator will have access to this locked box. If the results of this study are published, your identity will not be made public. AUDIO RECORDING By initialing in the space provided, you verify that you have been told that an audio recording will be generated during the course of this study and give your consent for an audio recording to be generated. Recordings are being made so that the student researcher and primary investigator can transcribe and code your responses. As mentioned earlier, you will be identified only by an assigned ID number. The data will be destroyed after five years. It is your choice to be audio-recorded. If you do not want to be audio-recorded, an alternate recording method of handwritten notes will be taken. ___________ Participants initials By initialing in the space provided, you verify that you have been told that the alternate method of hand-written notes will be taken during the interview in place of an audio recording and give your consent for hand-written notes to be taken. __________ Participant’s initials DO I HAVE A CHOICE TO BE IN THE STUDY?
If you decide to take part in the study, it should be because you really want to volunteer. You will not lose any benefits or rights with Compassion and Choices of Oregon you would normally have if you choose not to volunteer. You can stop at any time during the study and still keep the benefits and rights you had before volunteering.
113
You will not be treated differently by Compassion and Choices of Oregon nor the student researcher or primary investigator if you decide to stop taking part in the study. You are free to skip any questions that you would prefer not to answer, but we would appreciate receiving as complete information as possible. If you choose to withdraw from this project before it ends, we may keep information collected about you and this information may be included in study reports.
WHAT IF I HAVE QUESTIONS?
If you have any questions about this research project, please contact Erica Srinivasan, the graduate student investigator at [email protected] or 971-227-2877, or Dr. Patricia Moran, the principal investigator at [email protected] or 541-737-1074. If you have questions about your rights as a participant, please contact the Oregon State University Institutional Review Board (IRB) Human Protections Administrator, at (541) 737-4933 or by email at [email protected].
Your signature indicates that this research study has been explained to you, that your questions have been answered, and that you agree to take part in this study. You will receive a copy of this form. Participant's Name (printed): __________________________________________________________ __________________________________________ _______________________________ (Signature of Participant) (Date)
114
Appendix D
Bereavement experiences following a death under the Death with Dignity Act Interview Protocol
As you know, this study is about your bereavement experiences from the loss of your loved one who died using Oregon’s aid-in-dying law, the Death with Dignity Act. I’m going to be asking you different questions about your loved one and your feelings associated with your loss. If at any time you need a break, or need to stop, or if there are any questions you don’t want to answer, please let me know. Before we begin, I’d like to get some general demographic information from you. If you’re comfortable, could you tell me your age? Your race? Your education level? Your occupation? Your religion? And is this the town you live in? Thank you. We will proceed to the interview now. I would like to begin by hearing about your loved one. 1. Could you tell me a little bit about your loved one? Prompts: What were his/her interests? How old was he/she? What was his/her race? What was his/her education level? What was his/her occupation? What was his/her religion? Where did he/she live?
A) What was your relationship to _______?
B) What illness did _______ have?
C) When was ______diagnosed with this illness?
D) What types of treatments did _______ seek?
E) How did ______feel about being sick? About dying? Please explain. 2. Next I’d like to ask you about your involvement with caregiving or spending time with______. Could you tell me about the time you spent with ______? Prompts: Did you take care of ______? How often would you see each other? How did you spend time together?
A) What kind of practical and/or emotional issues came up for you during ______’s illness? Please explain.
115
B) Did your ability to cope with what was happening change as the illness progressed? If yes, how and why did it change? If no, why do you think it didn’t change? 3. The next set of questions deal with your feelings about the loss. Were you present for the death or did you hear about it? A) if you were present, could you describe the death? If you weren’t present, could you describe what you were told about the death?
B) What were your immediate feelings about the death? C) Are you still dealing with the same feelings now as you did when _____ first
died?
D) Did you experience any other grief reactions other than the ones you’ve mentioned?
E) Did you feel you were able to say goodbye to ________?
Prompt: Was there anything you were unable to express to _______before he/she died? F) How did the fact that aid-in-dying is legal in Oregon impact your experience of
_____’s death?
G) What deaths of other loved ones or friends have you have experienced? H) How was your experience of grief from aid-in-dying similar to your grief from
these other deaths you have experienced? How was it different? 4. Now I’d like to ask you questions related to _______’s decision to use aid-in-dying. First, how did _______ arrive at the decision to use aid-in-dying?
A) To your knowledge, did _______ consider alternatives to aid-in-dying?
Prompt: Did Compassion and Choices of Oregon refer _______ to hospice?
B) Did you agree with _______’s decision to use aid-in-dying? Please explain.
C) Do you think your agreement or disagreement affected your grief? Please explain.
D) Did your other family members agree with _______’s decision to use aid-in- dying? Please explain.
116
E) How did your family members’ agreement or disagreement affect your grief? Please explain.
F) How did it feel to you for _______ to use aid-in-dying at the stage of illness
he/she was in? Please explain.
Prompt: How did you feel about the timing of the death?
5. And last, I’d like to ask you about other people’s reactions to the death. How did other people react to the death? Prompts: Were there people who reacted in a supportive way to the news of the death and of aid-in- dying? Were there people who reacted in a negative way?
A) When you think privately about _______’s death, what do you think of as the cause of death? Is this different than what you say to people who ask you how he/she died? Please explain.
B) Did you feel you could express your grief to others? Please explain.
Prompts: Who did you grieve with? Could you express your grief to family members? To friends?
C) Did you use grief/bereavement services offered through hospice? If you used any grief/bereavement services, did it help? Please explain.
D) Did you receive support from others and did you feel the support you received
was adequate? Please explain.
E) Did you feel any uncertainty about how you should behave or feel as a survivor of a death from aid-in-dying? Please explain.
That is the end of the interview. Is there anything else you would like to add? Thank you so much for your time and for sharing your experiences. I very much appreciate it and I believe that your responses will help other people who may find themselves in a similar circumstance in the future.