18
Paul Clarke, RN BSN Rapid Resuscitation Action Plan: How One Unit Tries To Beat The Odds

Paul Clarke, RN BSN
Rapid Resuscitation Action Plan:How One Unit Tries To Beat The Odds
Disclosure Statement
I do not have any relevant financial relationships with any commercial interests to disclose.
Objectives
Discuss Goals for Rapid Resuscitation Action Plans
Review Inclusion Criteria
Current Methodology
Preliminary Outcomes
Problem
Current Pediatric CVICU Code Outcomes Nursing Turnover Jr. Physicians

Solution
Unit Specific Code Review Committee
Examined Past Codes
RAP, ASAP

Goals
To prevent code events in the CVICU at Children’s of Alabama by identifying patients at high risk for cardiac or respiratory arrest
To reduce severity of remaining code events by identifying best choice interventions based on most likely route of deterioration
Goals
Improve efficiency of code events by pre-identifying healthcare provider roles to speed time to first interventions
Decreased code events and reduction in severity will improve patient outcomes

Inclusion Criteria
Single Ventricle physiology pre or post Stage I palliation
Neonates with restrictive atrial septum (d-TGA or single ventricle)
Neonates POD 0 and POD 1
Open Sternum
Inclusion Criteria
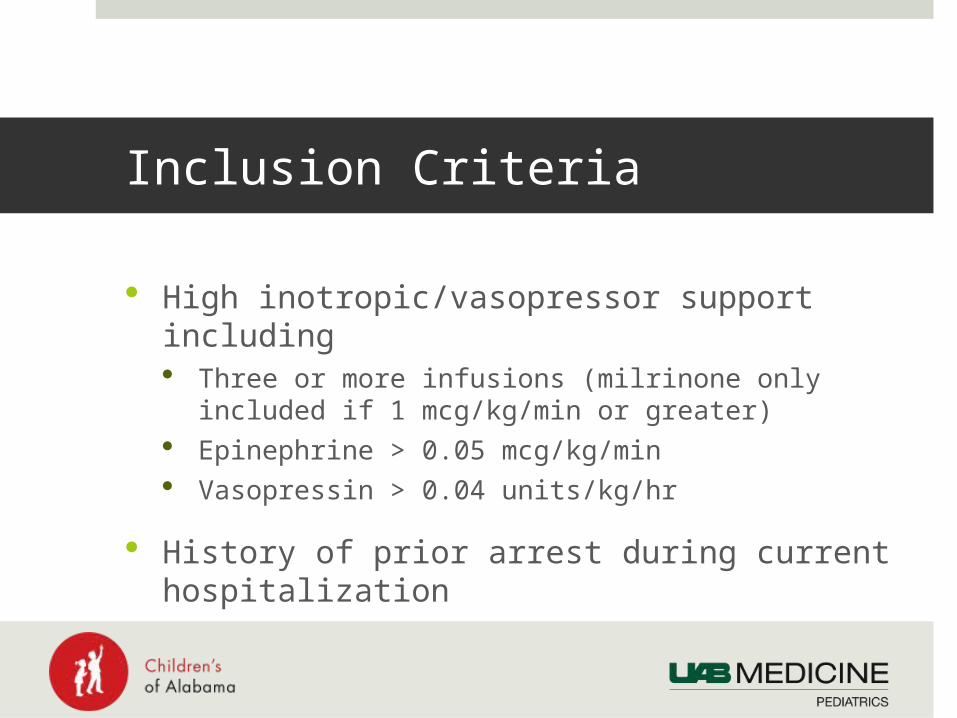
High inotropic/vasopressor support including Three or more infusions (milrinone only included if 1
mcg/kg/min or greater) Epinephrine > 0.05 mcg/kg/min Vasopressin > 0.04 units/kg/hr
History of prior arrest during current hospitalization
Inclusion Criteria
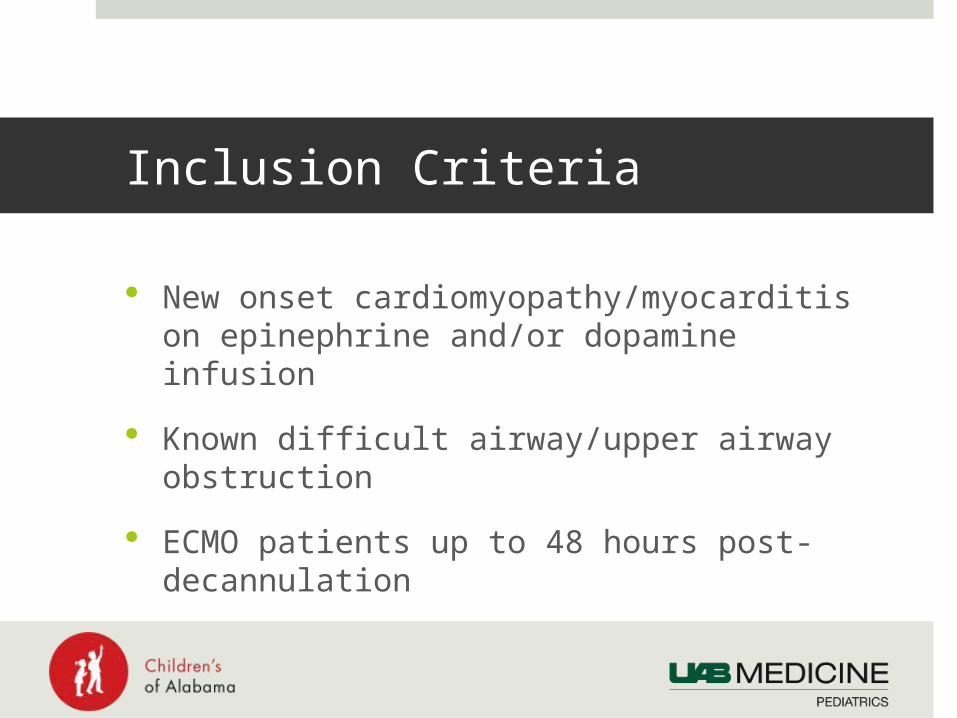
New onset cardiomyopathy/myocarditis on epinephrine and/or dopamine infusion
Known difficult airway/upper airway obstruction
ECMO patients up to 48 hours post-decannulation
Inclusion Criteria
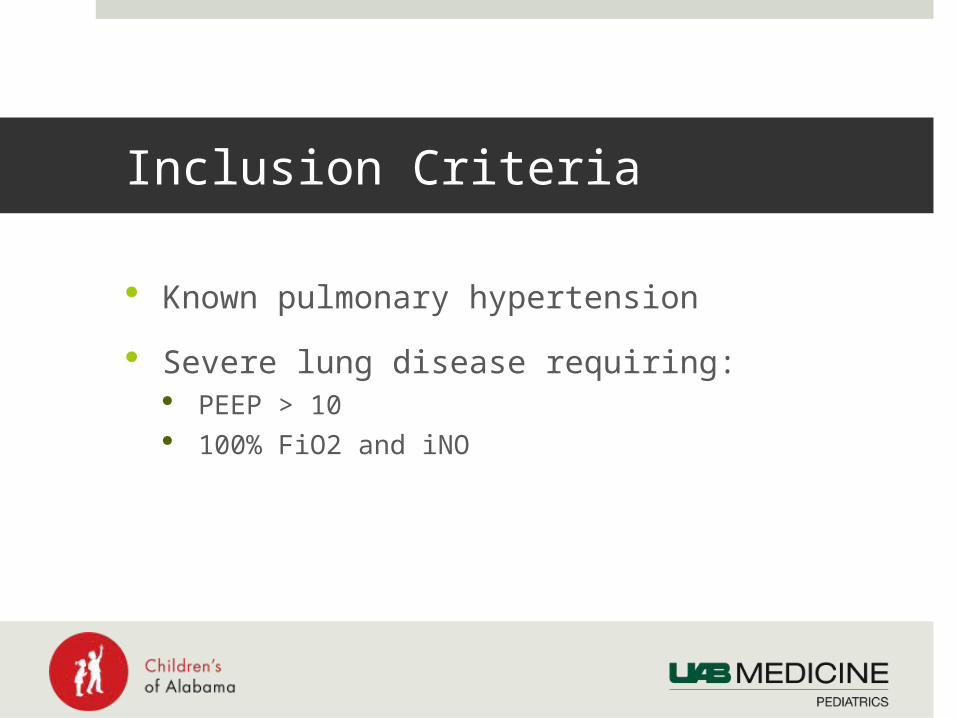
Known pulmonary hypertension
Severe lung disease requiring: PEEP > 10 100% FiO2 and iNO

Process
Multidisciplinary “RAP” team
RAP rounds twice daily, once per shift
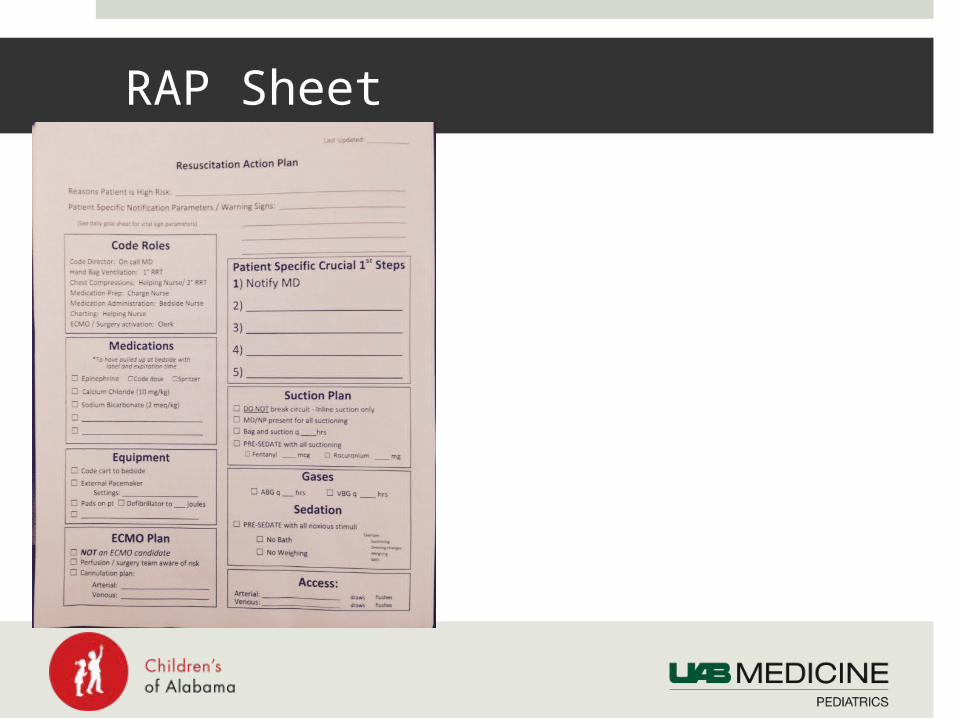
RAP Sheet
Process
RAP sheet to include Reason(s) patient is high risk Warning signs and notification parameters for RN/RT Potential prevention measures for arrest Necessary equipment and medication to have
readily available at bedside Patient specific first steps in event of arrest
Process
RAP sheet reviewed and updated each round
Bedside Nurse responsible for keeping needed medications in locked bedside cart

Process
RAP sheet reviewed for all nursing handoffs
Code Roles preassigned to minimize role duplication and extraneous personnel

Interventions Beyond RAP
Three Person Suction
Pre-sedate with noxious stimuli/Minimal Stimuli
Prostaglandin Checks
20/10’s Rule

Current Progress
Initiated August 2014
Better multidisciplinary awareness and communication
MD, NP, RT and RN acceptance

















