57
Pay-for-performance.. Can it deliver? Dale W. Bratzler, DO, MPH QIOSC Medical Director
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | jeffry-goodman |
| View: | 218 times |
| Download: | 0 times |

Pay-for-performance..
Can it deliver?
Dale W. Bratzler, DO, MPH
QIOSC Medical Director

What’s driving policy on health
care?

US Healthcare SpendingProblem #1 - Cost!
• $1.9 trillion• 16% of the gross domestic product• $6,280 for each man, woman, and
child
• Medicare and Medicaid - $600 billion in 2006

US Healthcare Spending
• Five percent of the population accounts for almost half of total healthcare expenses
• The 15 most expensive health conditions account for 44 percent of total healthcare care expenses
• Patients with multiple chronic conditions cost up to seven times as much as patients with only one chronic condition
Stanton MW, Rutherford MK. The high concentration of U.S. health care expenditures. Rockville (MD): Agency for Healthcare Research and Quality; 2005. Research in Action Issue 19. AHRQ Pub. No. 06-0060.

Spending is Unevenly Distributed
22
49
64
80
97
3
0
20
40
60
80
100
Top 1% Top 5% Top 10% Top 20% Top 50% Bottom 50%
Pe
rce
nt
of
tota
l ex
pe
nd
itu
res

Spending is Unevenly Distributed
Percent of Population
Expenses per person
$
Top 1% > 35,543
Top 5% > 11,487
Top 10% > 6,444
Top 20% > 3,219
Top 50% 664
Bottom 50% < 664Conwell LJ, Cohen JW. Statistical Brief #73. March 2005. Agency for Healthcare Research and Quality, Rockville, MD.

Spending is Unevenly DistributedAge Distribution of the Top 5%
5
9 10
15
18
29
14
0
10
20
30
40
18 andunder
19-34 35-44 45-54 55-64 65-79 80 andover
Age in years
Pe
rce
nt
of
tota
l ex
pe
nd
itu
res

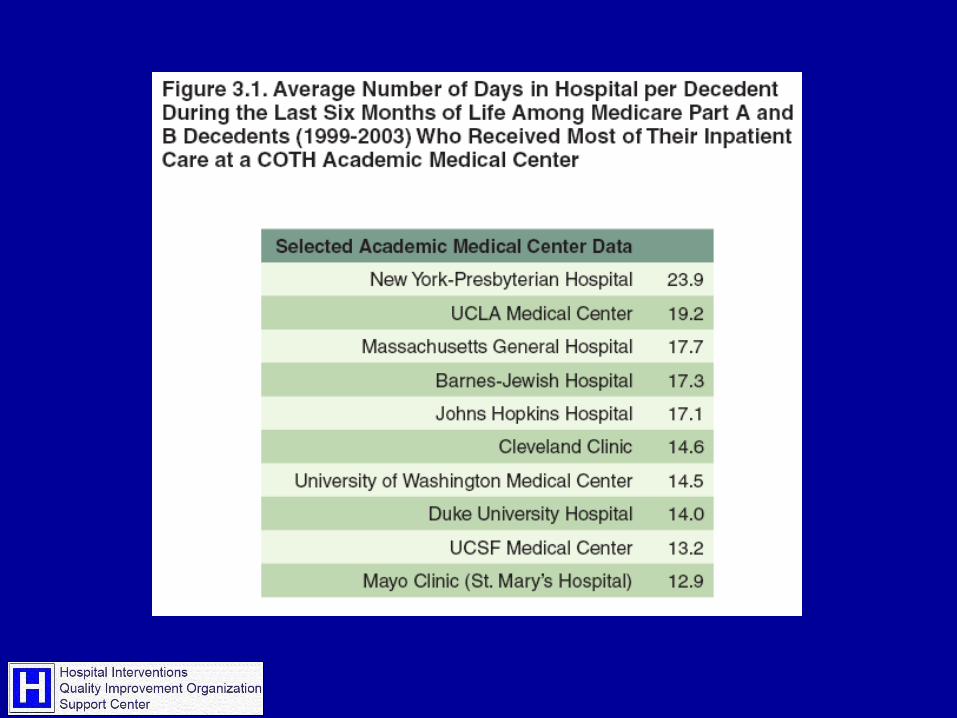
Problem #2 = Variation
Dartmouth Atlas of Healthcare

Wennberg/Fisher et al.
• Evidence-sensitive care• The easiest one to attack
• Patient preference-sensitive care• We are beginning to (finally) scratch the
surface• Supply-sensitive care
• Nobody has any idea what to do about this, short of legislative mandates and/or rationing


Elyria has three times the rate of angioplasties of Cleveland, 30 miles away

www.dartmouthatlas.com

Care of Patients with Chronic Illness
New Study Shows Need for a Major Overhaul of How United StatesManages Chronic Illness
“Almost One-Third of Medicare Spending for Chronically Ill Unnecessary. Improving Care Could
Also Lower Costs”

Care of Patients with Chronic Illness
"Variation is the result of an unmanaged supply of resources, limited evidence about what kind of care really contributes to the health and longevity of the chronically ill, and falsely optimistic assumptions about the benefits of more aggressive treatment of people who are severely ill with medical conditions that must be managed but can't be cured."


Problem #3 - Performance
Patients’ care often deficient, study says. Proper treatment given half the time. On average, doctors provide appropriate health care only half thetime, a landmark study of adults in 12 U.S. metropolitan areas suggests.Medical Care Often Not Optimal Failure to Treat Patients Fully Spans Range of What Is Expected of Physicians and Nurses
Study: U.S.Doctors are not following the guidelines for ordinary illnesses
.
The American healthcare system,often touted as a cutting-edge leader in the world, suddenlyfinds itself mired in serious questions about the ability of itshospitals and doctors to deliverquality care to millions.
Medical errors corrodequality of healthcare system
RAND Study: Quality of Health Care Often Not
Optimal

In summary, we found that the quality of hospital care in the United States varies
widely across different indicators of quality and that individual hospitals vary in their performance according to indicators and
conditions.
N Engl J Med 2005;353:265-274.

Quality from the Patient’s Perspective
Hospital Quality Measures, Qtr. 4, 2005
60.2
83.2
57.6
39.7
58.6
0
20
40
60
80
100
HF AMI SCIP Inf Pneumonia 23 Measures
Pe
rce
nt
The “Appropriate Care Measure” reflects the percentage of hospital patients that receive all indicated care (all-or-none).

Unsustainable cost growth(questionable returns in healthy lifespan)
+ Huge variation in services delivered
(no relationship to outcomes)
+
Data demonstrating significant gaps in delivery of ideal care
=
Need to Pay Differently

Calls for Medicare to Provide Payment for Quality
• IOM report 2002, 2006• Health Affairs article, former
HCFA administrators, 2003• MedPAC report 2004• Private sector efforts
• Bridges to Excellence• Leapfrog Group
Presentation Outline
• Pay-for-performance… does it work to improve quality?
• Payment incentive models
• The potential for unintended consequences
Does Pay-for-performance improve quality?
• Strategies for accelerating quality improvement:• Public reporting• Pay-for-performance
Despite limited evidence demonstrating benefit, P4R and P4P are being widely advocated

Hospital Public Reporting
434
1407
1952
4043 4192
August, 2003 February,2004
May, 2004 October, 2004 March, 2005
Number of Reporting Hospitals
0.4% payment incentive

Hospital Public Reporting
• Currently have a very limited set of measures• Focus predominantly on processes of
care• Few outcomes measures because of
risk-adjustment challenges

Hospital Public Reporting
• Hospital Quality Alliance• 10 measures recently expanded to 21 (AMI,
HF, Pneumonia, SIP)
• New York State CABG mortality• Wisconsin “Quality Counts”
• Generally, quality seems to improve• Mechanism??
• Little data that reporting drives much patient decision making at this point
• Hospital market share largely unaffected

Pay-for-PerformanceMuch to be learned
• While there are lots of demonstrations, there is little evaluative data at this time

Ann Intern Med. 2006;145:265-272.

Does P4P improve the quality of health care?
• Seventeen studies with control groups• 13 focused on process of care measures
• 5 of 6 studies of physician-level financial incentives linked to improved quality
• 7 of 9 studies of provider group-level incentives found partial or positive effects on quality
• 4 studies suggested unintended consequences of payment incentives
Petersen LA, et al. Ann Intern Med. 2006;145:265-272.

HQID Hospital Participation
• Voluntary• Eligibility: Hospitals in Premier Perspective
system as of March 31, 2003 • 278 hospitals started• Demonstration Project: Pilot test of concept
• Can economic incentives effectively improve quality of care?

1st Decile
Hospital
Hospital
Year One Year Two Year Three
Top Performance Threshold
Payment Adjustment Threshold
2nd Decile
3rd Decile
4th Decile
5th Decile
6th Decile
7th Decile
8th Decile
9th Decile
10th Decile
1st Decile
2nd Decile
3rd Decile
4th Decile
5th Decile
6th Decile
7th Decile
8th Decile
9th Decile
10th Decile
1st Decile
2nd Decile
3rd Decile
4th Decile
5th Decile
6th Decile
7th Decile
8th Decile
9th Decile
10th Decile
Condition XCondition X
Condition X

Results show significant improvement
Composite Quality Score: Quarterly Median Improvement by Focus AreaCMS/Premier Hospital Quality Initiative Demonstration Project Participants
October 1, 2003 - December 31, 2004Preliminary Results
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
AMI CABG Pneumonia Heart Falure Hip and Knee
Clinical Focus Area
Co
mp
os
ite
Qu
alit
y S
co
re
Q4-03 Q1-04 Q2-04 Q3-04 Q4-04

CMS/Premier HQI ProjectReduction in Variation
AMI Composite Quallity Score Distribution
Time Periods:4Q03 - 2Q04
2Q041Q044Q03
Co
mp
osi
te Q
ua
lity
Sco
re
120
100
80
60
• Positive trend in both upper and lower scores of range
• Reduction in variance (narrowing of range)
• Median moving upward

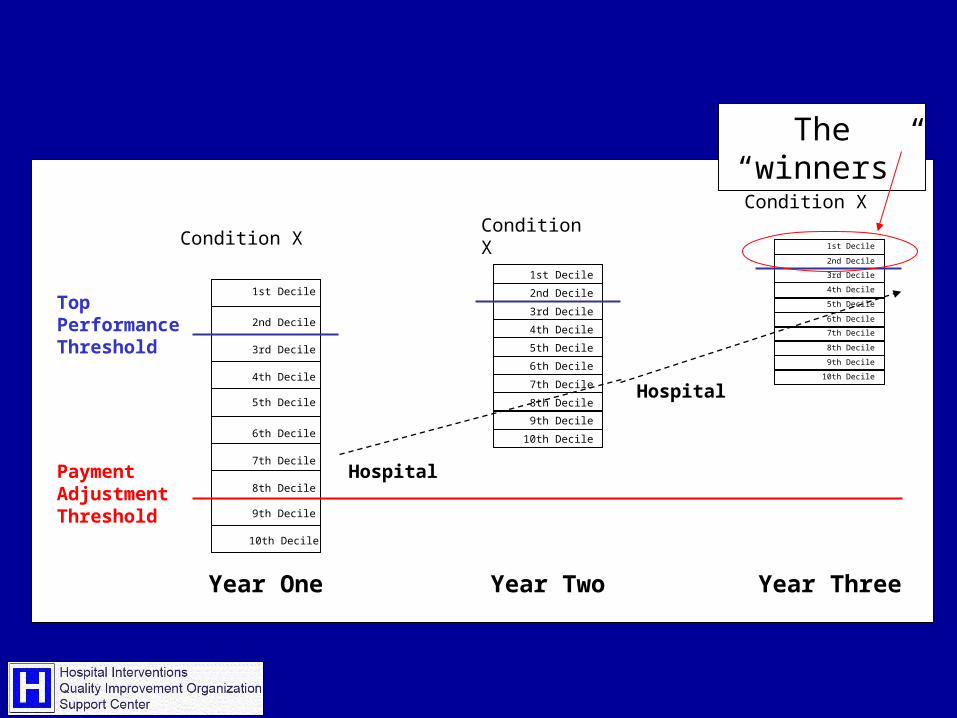
Does P4P reward improvement?
Those that improved the most, received the lowest bonus payments. Those at high levels of performance to start with reaped most of the rewards.
Rosenthal MB, et al. JAMA. 2005;294:1788-1793.
1st Decile
Hospital
Hospital
Year One Year Two Year Three
Top Performance Threshold
Payment Adjustment Threshold
2nd Decile
3rd Decile
4th Decile
5th Decile
6th Decile
7th Decile
8th Decile
9th Decile
10th Decile
1st Decile
2nd Decile
3rd Decile
4th Decile
5th Decile
6th Decile
7th Decile
8th Decile
9th Decile
10th Decile
1st Decile
2nd Decile
3rd Decile
4th Decile
5th Decile
6th Decile
7th Decile
8th Decile
9th Decile
10th Decile
Condition XCondition X
Condition X
The “winners”

Cost savings?
• To date, there is little evidence that pay-for-performance programs save money• Many target measures that address
underutilization of care and services• Most do not provide incentives for
efficiency

Little coordination
• At this time, there has been little coordination between payers• Multiple different models and
measures even within the same clinical setting

Payment Incentives

Financial Rewards/Incentives
• Bonus Payments
• Awards for Improvement Projects
• Fee Schedules Based on Performance
• “At-Risk” Contracting
• Cost Differentials for Consumers
P4P Issues
• What to Reward• Relative quality• Absolute threshold• Improvement
• How to Finance Incentives• Across-the-board reduction to create pool• Offsetting penalties• Offsetting savings• New dollars: ? Source

P4P Issues
• Who to reward?• Individual practitioners• Groups of practitioners• Communities (?!)

Challenges and Pitfalls to P4P
The potential for unintended consequences….

Challenges to Incentives for Quality Performance
• Selection of measures/off label use of measures
• Dynamic measurement environment• Measures maintenance• Hospital Burden • Time lags• Validation/Scoring methodology• Need for proof of effectiveness• Unintended consequences


Issues in the Selection of Quality Measures
• Outcome measures (i.e. mortality) require risk adjustment
• Disease-specific measures don’t necessarily reflect overall quality
• Volume may or not be a proxy for quality
• Statistical issues with low volume programs
• Hospital performance versus medical staff performance

Unintended Consequences
• Direct harm
• Indirect harm

Pneumonia as an example…Direct Harm
• Antibiotics within 4 hours of hospital arrival• Process linked to improved patient
outcomes, however• Some patients who are ultimately diagnosed
with pneumonia do not have an obvious diagnosis at the time of arrival
• Potential for inappropriate antibiotic administration to those who don’t have pneumonia to achieve high performance rates on the measure
Unintended ConsequencesDirect Harm
• Giving a beta blocker to a patient with contraindications
• Use of VTE prophylaxis in patients with bleeding risks
• Clinical issues of uncertainty that are exacerbated by incentives created by pay-for-performance

Unintended ConsequencesIndirect Harm
• Caregivers shift attention to those conditions that are subject to payment incentives• e.g., triage pneumonia patients in preference to
abdominal pain patients• Focus on glucose control in a diabetic while
ignoring control of hyperlipidemia• Reallocating resources to excel on measures with
payment incentives• Risk avoidance – turn away high risk patients• Performance in one area does not necessarily
predict performance in another
“playing to the test”

What do we know about P4P?
• Currently resource intensive (data collection, validation, etc)
• A number of issues to be resolved with regard to incentive structure
• Programs are proliferating• The evidence on effectiveness is mixed• Expansion is inevitable• Need to build evaluation into P4P
programs prospectively

What do we know about P4P?
• Hospitals• Dislike relative thresholds (prefer absolute
thresholds)• ? Support for payment based on
improvement• Don’t currently include hospital outpatient
services• How to calculate ROI• Don’t track unintended consequences• Don’t currently align with physician
incentives

Current CMS P4P Demonstrations
• Premier HQID
• Physician Group Practice Demonstration• Medicare Care Management Performance
Demonstration• Medicare Health Care Quality Demonstration• Chronic Care Improvement Program• ESRD Disease Management Demonstration• Disease Management Demonstration for Severely
Chronically Ill Medicare Beneficiaries• Disease Management Demonstration for Chronically
Ill Dual Eligible Beneficiaries • Care Management For High Cost Beneficiaries

PVRP
• On October 28, 2005, CMS announced the Physician Voluntary Reporting Program (PVRP) to begin on January 3, 2006. The primary purpose of the PVRP is to provide a means for physicians to report clinical data using the claim process. This clinical and other claims data can be used to calculate quality measures. Physicians who participate will receive confidential feedback, if requested, on their reporting and performance rates.
The future
• More transparency• More partnerships and coalitions• More measures
• Efficiency measures• Efficiency across providers – Current
demonstration projects• Mortality measures
• More P4P


















