Mr. S, 50 yo, was admitted to the hospital with productive cough, dyspnea, short of brethness, icteric and pruritus since 1 month ago. He was treated with cathegory 1 TB medicine, but there was no good response. The doctor asked the pharmacist about the most possible drug which could be resistant to this patient and about the best theraphy. R/ inj SNMC R/ HP Pro 1 x 1 tab R/ GG 3 x 1 tab R/ codein 1 x 1 tab R/ omeprazole S O A P Productive cough Dyspnea Short of breathness TB PARU • Pengobatan batuk produktif : GG • Pengobatan TB untuk sementara dihentikan sampai fungsi hati normal dan dilanjutkan dengan pengobatan TBC second line
Transcript
Mr. S, 50 yo, was admitted to the hospital with productive cough, dyspnea, short of brethness, icteric and pruritus since 1 month ago. He was treated with cathegory 1 TB medicine, but there was no good response. The doctor asked the pharmacist about the most possible drug which could be resistant to this patient and about the best theraphy. R/ inj SNMC
R/ HP Pro 1 x 1 tab
R/ GG 3 x 1 tab
R/ codein 1 x 1 tab
R/ omeprazole
S O A P
Productive cough
Dyspnea
Short of breathness
TB PARU• Pengobatan batuk produktif :
GG
• Pengobatan TB untuk sementara dihentikan sampai fungsi hati normal dan dilanjutkan dengan pengobatan TBC second line
Icteric
Pruritus
Increase of total bilirubin
ALT 650,
AST 498
Gangguan hepar• Inj SNMC 2 ampul (@20
ml)/hari selama 2 minggu, dilanjutkan 80 mg 2x/minggu selama 24 minggu
• HP pro 1 x 1 tab
• Domperidone untuk mengatasi gejala mual muntah karena gangguan hati
TB Paru adalah infeksi Mycobacterium tuberculosis yang menyerang paru-paru
PATOFISIOLOGY
ETIOLOGI
TBC Mycobacterium tuberculosis yang sebagian besar (80%) menyerang paru-paru.
Penyebaran kuman melalui percikan dahak (droplet) di udara oleh penderita TB.
GANGGUAN HEPAR Penggunaan obat-obat TB seperti PZA, Inh Tanpa ada hepatoprotektor
FAKTOR RESIKO
TBC Umur
Status sosial dan ekonomi
Keadaan tempat tinggal
Prilaku / kebiasaan:merokok
Daya tahan tubuh
Status gizi
Penyakit lain
GANGGUAN HEPAR
Umur
Kebiasaan hidup: miras
Penggunaan obat dengan efek samping pada hepar
PENATALAKSANAAN TERAPI TBC
Kategori 1 : 2HRZE/4H3R3
Tablet Isoniazid @ 300 mg
Kaplet Rifampisin @ 450 mg
Tablet Pirazinamid @ 500 mg
Tablet Etambutol @ 250 mg
Obat ini diberikan untuk:
Penderita baru TB Paru BTA Positif Penderita baru TB Paru BTA negatif Röntgen Positif yang “sakit berat
Penderita TB Ekstra Paru berat
Kategori 2 : 2HRZES/HRZE/5H3R3E3
Tablet Isoniazid @ 300 mg
Kaplet Rifampisin @ 450 mg
Tablet Pirazinamid @ 500 mg
Tablet Etambutol @ 250 mg
Tablet Etambutol @ 500 mg
Vial Streptomisin @ 1,5 gr
Obat ini diberikan untuk penderita TB paru BTA(+) yang sebelumnya pernah diobati, yaitu:
Penderita kambuh (relaps) Penderita gagal (failure)
Penderita dengan pengobatan setelah lalai (after default).
Kategori 3 : 2 HRZ/4H3R3
Tablet Isoniazid @300 mg
Kaplet Rifampisin @ 450 mg
Tablet Pirazinamid @ 500 mg
Obat ini diberikan untuk:
Penderita baru BTA negatif dan röntgen positif sakit ringan Penderita TB ekstra paru ringan
PENATALAKSANAAN TERAPI
TB Dengan gangguan hati kronik
2 RHES/6RH atau 2HES/10HE atau 9RE
Regimen pengobatan TB RESISTEN (WHO):
6Z-Km-Mfx-Eto-Trd/ 18 Z-Mfx-Eto-Trd Z = pirazinamid
Mr. S, 50 yo, was admitted to the hospital eith productive cough, dyspnea, short of brethness, icteric and pruritus since 1 month ago. He was treated with cathegory 1 TB medicine, but there was no good response. The doctor asked the pharmacist about the most possible drug which could be resistant to this patient and about the best theraphy.
R/ inj SNMC
R/ HP Pro 1 x 1 tab
R/ GG 3 x 1 tab
R/ codein 1 x 1 tab
R/ omeprazole
PH : TB since 5 weeks ago DH : 1 cathegory of TB medicine
Rekomendasi pengobatan TB selanjutnya yaitu second line :
• PAS 500 mg 1x sehari• Levofloxacin 250 mg 1 x sehari
• Etionamid 125 mg 1x sehari
• Amicacyin 1000 mg 1 x sehari
• (selama 6 bulan)
Gangguan hepar karena efek samping obat TB• Inj SNMC 2 ampul (@20 ml)/hari selama 2
minggu, dilanjutkan 80 mg 2x/minggu selama 24 minggu
• HP pro 1 x 1 tab
• Omeprazole 20 mg sekali sehari untuk mengatasi gejala mual muntah karena gangguan hati
ASSESMENT
DRP Ada Solusi
Ada indikasi tidak ada obat - -
Ada obat tdk ada indikasi - -
Pemilihan obat tdk tepatCodein (narkotik)
Utk px dyspnea & SOB, gang hati tidak tepat
Batuk berdahak diberi GG
Overdose - -
Underdose - -
Muncul ESO Codein menimbulkan depresi pernapasan
Tidak dianjurkan
Interaksi obat - -
Pasien gagal menerima obat - -
Monitoring Keberhasilan Terapi
obat P. Monitoring Rentang Normal End Point Frekuensi Monitoring
Inj SNMC 80 mg/hari selama 2 minggu
HP Pro
ALT AST, bilirubin
ALT = 11-41 u/L
AST = 10-41 U/L
Bilirubin total = 0,2-1,3 mg/dL
Perbaikan fungsi hati. Nilai tes lab hati menjadi normal
Sebulan sekali
GG Frekuensi batuk , RR
RR = 20-24 Batuk berkurang, tidak Dyspnea &SOB
Sehari sekali
OmeprazoleMual muntah
Stress ulcer- Tidak mual muntah Sehari sekali
MONITORING ESO
obat P. Monitoring Rentang Normal Frekuensi Monitoring
Inj SNMC 80 mg/hari selama 2 minggu
HP Pro
- - -
GG Mual, mengantuk - Sehari sekali
Omeprazole Diare, sakit kepala, konstipasi, dll
- Sehari sekali
Kasus 7
A 50 yo male patient admit to the Emergency Departement with chest pain, especially during high activity, headache and dyspnea. He was diagnosed with AMI with acute STEMI. BW 95 kg, height 165 cm
R/ Streptokinase inj, dose confirm pharmacist
R/ Aspirin 1x 80 mg
R/ isosorbid mononitrat 3x1tab
R/ carvedilol
Problem klinik
• Pasien didiagnosis menderita AMI dengan STEMI akut
FARMAKOTERAPI
• Tujuannya adalah:
1. Mengatasi kondisi gawat darurat
2. Membatasi luasnya infark
3. Mempertahankan fungsi jantung
4. Meningkatkan kualitas hidup pasien (quality of life)
5. Mencegah serangan AMI kedua
Unstable
Angina Non occlusive
thrombus
Non specific
ECG
Normal cardiac
Enzymes
NSTEMI
Occluding thrombus
sufficient to cause
tissue damage & mild
myocardial necrosis
ST depression +/-
T wave inversion on
ECG
Elevated cardiac
enzymes
STEMI
Complete thrombus
occlusion
ST elevations on
ECG or new LBBB
Elevated cardiac
enzymes
More severe
symptoms
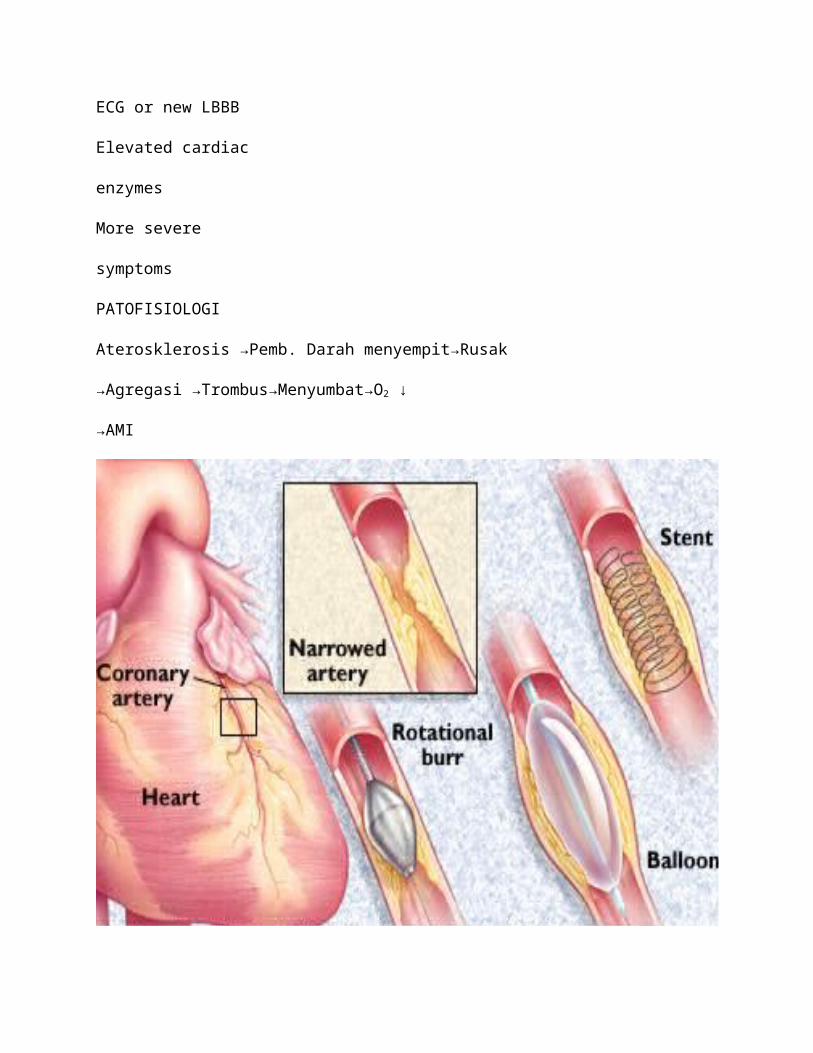
PATOFISIOLOGI
Aterosklerosis →Pemb. Darah menyempit→Rusak
→Agregasi →Trombus→Menyumbat→O2 ↓
→AMI
ETIOLOGI
• Terlepasnya plak aterosklorosis dari arteri koroner dan menyumbat aliran darah ke miokardium
• Suplai oksigen ke miocard berkurang
• Curah jantung yang meningkat
• Kebutuhan oksigen miocard meningkat
RISK FACTORS
Uncontrollable
• Jenis kelamin• Hereditas
• Umur
Controllable• Tekanan darah tinggi• Kolesterol darah tinggi• Merokok• Aktivitas fisik• Obesitas• Diabetes• Stress
Penatalaksanaan di IGD1) Pasang infus intravena: dekstrosa 5% atau NaCl 0,9%.2) Pantau tanda vital: setiap ½ jam sampai stabil, kemudian tiap 4 jam atau sesuai dengan kebutuhan (frekuensi jantung)3) Aktifitas istirahat di tempat tidur dengan kursi commode di samping tempat tidur dan mobilisasi sesuai toleransi setelah 12 jam.4) Diet: puasa sampai bebas nyeri, kemudian diet cair. Selanjutnya diet jantungCon’t Penatalaksanaan di IGD5). Medika mentosa :• Oksigen nasal• Mengatasi rasa nyeri: Morfin 2,5 mg (2-4 mg) iv, atau Petidin 25-50 mg iv, atau Tramadol 25-50 mg iv. Nitrat sublingual/patch, intravena jika nyeri berulang dan berkepanjangan.6) Terapi reperfusi (trombolitik) streptokinase 7) Antitrombotik :• Aspirin (160-325 mg hisap atau telan) atau heparin8) Mengatasi rasa takut dan cemas: diazepam 3 x 2-5 mg oral9) Obat pelunak tinja: laktulosa (laksadin) 2 x 15 ml.10) Terapi tambahan: Penyekat beta, atau Penghambat ACE atau antagonis kalsiumPATIENT ASSESMENT
S : chest pain during high activity, headache, dyspneaO : BW 95kg, heigh 165 cm, Lab chol 450 mg/dL, TG 250 mg/dL, LDL 100 mg/dL, TD 130/80A : AMI with acute STEMIP : analgetic narkotika, trombolitica agent, vasodilator, resustasi cairan, O2
• P: AMI with acute STEMI• I : Isosorbid mononitrat
• C: Isosorbid dinitrat
• O : oncet, effectiveness
• Jurnal: Comparison of the time to onset of action on myocardial ischaemia following intravenous administration of isosorbide dinitrate and 5-isosorbide mononitrate in Chinese patients.
• DOC: digunakan ISDN
Quick Management Guide in Emergency Medicine, 2010
JURNAL ISDN
EBM Beta Bloker
• P: acute myocard infaction• I : atenolol
• C: carvedilol
• O : vasodilatasi
• Jurnal: A Comparison of the Two β-Blockers Carvedilol and Atenolol on Left Ventricular Ejection Fraction and Clinical Endpoints after Myocardial Infarction
• DOC: atenolol (tidak ada perbedaan bermakna antara carvedilol dan atenolol namun pada carvedilol ada kejadian kardiovaskuler serius)
Ventricular Ejection Fraction and Clinical Endpoints after Myocardial Infarction
Background: β-Blockers have been found to reduce mortality and morbidity in postmyocardial infarction patients. However, it is not fully understood whether all β-blockers have similar favourable cardiovascular effects. The aim of this study was to compare the effects of carvedilol and atenolol on global and regional left ventricular ejection fraction (LVEF) and on predefined cardiovascular endpoints.
JURNAL Beta Bloker
Methods: In a single-centre, randomized, open, endpoint-blinded, parallel group study, 232 patients with acute myocardial infarction were randomized to treatment with carvedilol or atenolol. LVEF was measured by gated blood pool scintigraphy during the first week and after 12 months. The treatment was given orally within 24 h. The mean dose was 36.2 and 72.1 mg in the carvedilol and atenolol groups, respectively.
Results: No significant difference was found between the two study groups in the mean global and regional LVEF. There tended to be fewer first serious cardiovascular events in the carvedilol compared with the atenolol group (RR = 0.83, 95% CI 0.56–1.23, p = 0.39). Cold hands and feet were observed less frequently in the carvedilol group (20 vs. 33%, p = 0.025).
Conclusion: In patients following an acute myocardial infarction, no difference in either global or regional LVEF was observed between baseline and 12 months when treatment with carvedilol was compared with atenolol.
EBM Antihiperlipidemia
• P:• I :
• C:
• O :
• Jurnal:
• DOC:
JURNAL Antihiperlipidemia
Plan
Untuk SERANGAN:
R/NaCl 0,9% infus
R/Streptokinase inj 1,5 jt IU/1 jam
R/Aspirin 165 mg
R/Morfin 2,5 mg iv
R/ atenolol 50 mg/hari
Con’t Plan
Untuk PEMELIHARAAN:
R/ISDN 10 mg 2x1
R/Aspirin 80 mg
R/ laksadin 2 x 15 ml
R/ atenolol 50 mg/hari
R/simvastatin 20-50 mg/hari
Monitoring
Keberhasilan terapi, meliputi:
- Monitoring trombus pasien End point = kesadaran pasien pulih- EKG End point = gelombang ST (mendekati normal)
- Kadar kolesterol normal End point = 200 mg/dL
- Kadar TG normal End point = 150 mg/dL
- Penggunaan vasodilator End point = tekanan darah
Monitoring
Efek samping, meliputi:
- ES carvedilol: sakit kepala, bradikardi
Konseling
• Hentikan faktor resiko.• Minum obat secara teratur.
• Bila ada masalah dalam penggunaan obat hubungi apoteker anda