27
PCRRT PRESCRIPTIONS PCRRT PRESCRIPTIONS in ARF in ARF Patrick D. Brophy MD Patrick D. Brophy MD University of Michigan University of Michigan Pediatric Nephrology Pediatric Nephrology
PCRRT PRESCRIPTIONSPCRRT PRESCRIPTIONSin ARFin ARF
Patrick D. Brophy MD Patrick D. Brophy MD University of Michigan University of Michigan Pediatric NephrologyPediatric Nephrology
ObjectivesObjectives
Define ARFDefine ARF
Prescriptions: Based on What?Prescriptions: Based on What?– Case FormatCase Format– ModalityModality– BFRBFR– UF rateUF rate– Dialysate/FRF ratesDialysate/FRF rates– Other issues – anticoagulation, accessOther issues – anticoagulation, access

Acute Renal failureAcute Renal failure
Definition: A life threatening abrupt Definition: A life threatening abrupt cessation/reduction of urinary output to less than cessation/reduction of urinary output to less than 300ml/m300ml/m2 2 caused by prolonged renal ischemia in caused by prolonged renal ischemia in most cases (may occasionally present as high most cases (may occasionally present as high output renal failure- high urinary output with output renal failure- high urinary output with increasing BUN and Creatinine)increasing BUN and Creatinine)
Can lead to severe hypertension (fluid overload) Can lead to severe hypertension (fluid overload) metabolic abnormalities (acidosis, hyperkalemia) metabolic abnormalities (acidosis, hyperkalemia) requiring emergent therapyrequiring emergent therapy

ARF-- EtiologyARF-- Etiology
Developing CountriesDeveloping Countries– Hemolytic-Uremic Hemolytic-Uremic
Syndrome (31%)Syndrome (31%)– Glomerulonephritis Glomerulonephritis
(23%)(23%)– Post-Op Post-Op
Sepsis/Prerenal Sepsis/Prerenal ischemiaischemia
Chan et.al. PIR, Chan et.al. PIR, 23:200223:2002
Industrialized Industrialized CountriesCountries– Intrinsic Renal Disease Intrinsic Renal Disease
(44%)(44%)– Post-Op Septic Shock Post-Op Septic Shock
(34%)(34%)– Organ/Bone Marrow Organ/Bone Marrow
Transplant (13%)Transplant (13%)

ARF—Treatment OptionsARF—Treatment Options
Conservative- fluid management and Conservative- fluid management and nutritionnutrition
Renal Replacement Options:Renal Replacement Options:– Hemodialysis- Hemodynamic InstabilityHemodialysis- Hemodynamic Instability– Peritoneal Dialysis- efficiencyPeritoneal Dialysis- efficiency– CVVH(D)/(DF)- Hemodynamically less volatile CVVH(D)/(DF)- Hemodynamically less volatile
than HD, Can provide optimal fluid and than HD, Can provide optimal fluid and nutritional management & Clearancenutritional management & Clearance
Classic CaseClassic Case– 10kg infant (75 cm) BSA=0.45m10kg infant (75 cm) BSA=0.45m22, high vent , high vent
settings-lungs wet, ? sepsissettings-lungs wet, ? sepsis– up 2 kg from dry weight, no urine for 12 hrup 2 kg from dry weight, no urine for 12 hr– HR 160, BP 80/40 on pressors, pH 7.2HR 160, BP 80/40 on pressors, pH 7.2– Creatinine= 1.0 mg/dl BUN 40, lactate 4.0, Creatinine= 1.0 mg/dl BUN 40, lactate 4.0,
iCa=1.0, K=5.8 iCa=1.0, K=5.8
PEDIATRIC PRESCRIPTION PEDIATRIC PRESCRIPTION for CRRTfor CRRT
This patient clearly is in need of This patient clearly is in need of Hemofiltration Hemofiltration ISSUES: Determining the prescriptionISSUES: Determining the prescription– CAVH(D)/(DF) vs CVVH(D)/(DF)CAVH(D)/(DF) vs CVVH(D)/(DF)– Blood Flow RateBlood Flow Rate– Ultrafiltrate (dialysate/FRF rate)Ultrafiltrate (dialysate/FRF rate)– Access & MachineryAccess & Machinery– Fluids for dialysate/Filter ReplacementFluids for dialysate/Filter Replacement– AnticoagulationAnticoagulation
ApproachApproach
CAVH(D) vs CVVH(D)CAVH(D) vs CVVH(D)
CAVH(D)CAVH(D)– Initial form of therapy, Dependent on BP of Initial form of therapy, Dependent on BP of
patient (difficult to control UF), Technologically patient (difficult to control UF), Technologically easier (require 2 catheters)easier (require 2 catheters)
CVVH(D)CVVH(D)– Newer machines, 1 catheter, improved solute Newer machines, 1 catheter, improved solute
clearance, increased extracorporeal volume, clearance, increased extracorporeal volume, standard of carestandard of care
Werner et al.,1994, Critical Care Medicine, Werner et al.,1994, Critical Care Medicine, 22, 320-32522, 320-325
Goals: Evaluation of CVVH using 4 week Goals: Evaluation of CVVH using 4 week old lambs (pediatric size ~ 12.2 kg)old lambs (pediatric size ~ 12.2 kg)
Compared 3 systems postdilution, Compared 3 systems postdilution, predilution and hemofiltration (post-filter predilution and hemofiltration (post-filter replacement) with counter-current dialysis replacement) with counter-current dialysis (standardized UF, BFR and hemofilter)(standardized UF, BFR and hemofilter)

Werner et al.,1994, Critical Care Werner et al.,1994, Critical Care Medicine, 22, 320-325Medicine, 22, 320-325
Werner et al.,1994, Critical Care Medicine, Werner et al.,1994, Critical Care Medicine, 22, 320-32522, 320-325
ConclusionsConclusions– 1) CVVH(D) feasible in this size group1) CVVH(D) feasible in this size group– 2) Stable blood flow rates from 5-10 ml/kg/min2) Stable blood flow rates from 5-10 ml/kg/min– 3) BFR in this range with UF rates of 1ml/kg/ 3) BFR in this range with UF rates of 1ml/kg/
min can produce urea clearance of 1 min can produce urea clearance of 1 ml/kg/min (without causing to large a negative ml/kg/min (without causing to large a negative intrafilter pressure)intrafilter pressure)
– 4) dialysis didn’t increase urea clearance 4) dialysis didn’t increase urea clearance (animals not uremic though)(animals not uremic though)

Bunchman et al 1995, AJKD, 25,17-21Bunchman et al 1995, AJKD, 25,17-21
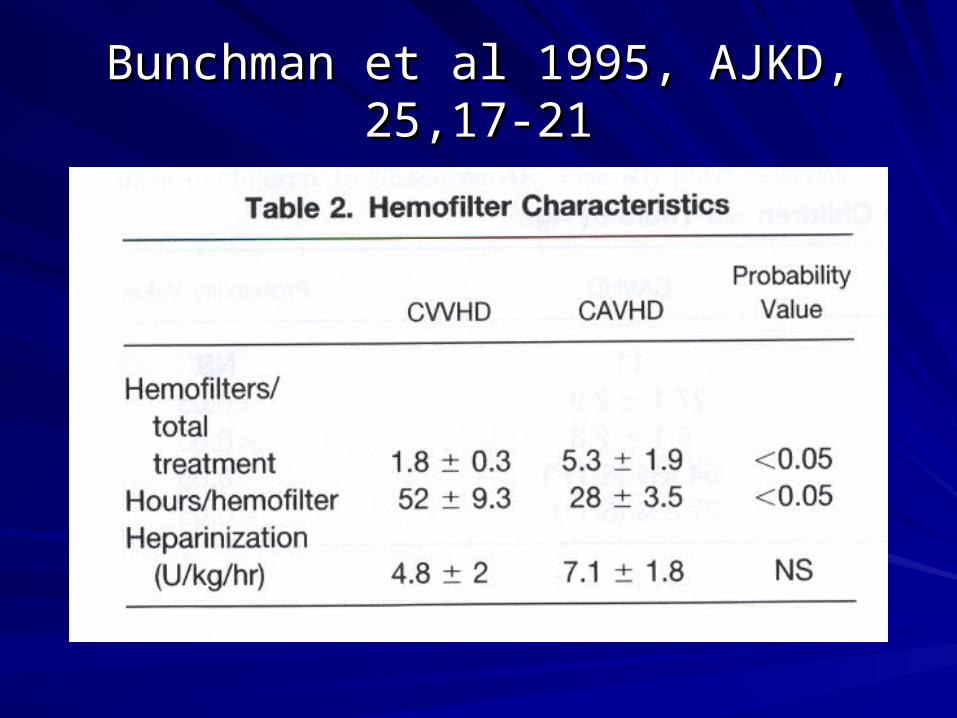
Bunchman et al 1995, AJKD, 25,17-21Bunchman et al 1995, AJKD, 25,17-21
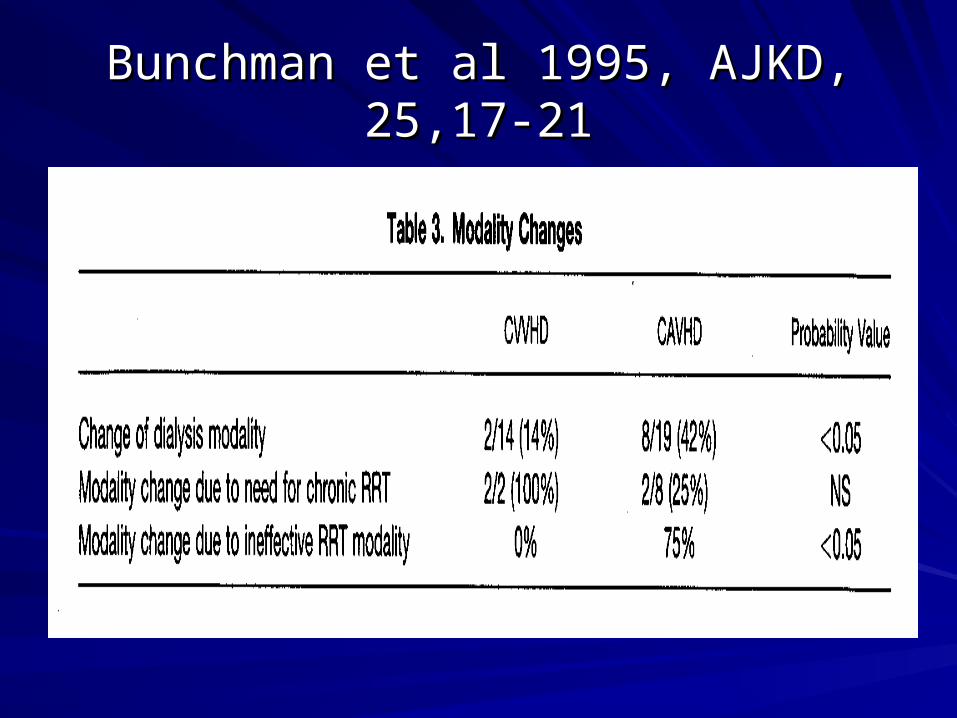
Bunchman et al 1995, AJKD, 25,17-21Bunchman et al 1995, AJKD, 25,17-21

Bunchman et al 1995, AJKD, 25,17-21Bunchman et al 1995, AJKD, 25,17-21

Zobel et al,1991 in Contiuous Hemofiltration. Zobel et al,1991 in Contiuous Hemofiltration. Contrib Nephrol. V93 pp257-260Contrib Nephrol. V93 pp257-260
Dialysate/ Ultrafiltration RatesDialysate/ Ultrafiltration Rates
No Study has identified effective, safe UF No Study has identified effective, safe UF or dialysate flow rates in Children.or dialysate flow rates in Children.
For HEMODIALYSIS– NET UF rate of For HEMODIALYSIS– NET UF rate of 0.2ml/kg/min is tolerated (Donckerwolke –0.2ml/kg/min is tolerated (Donckerwolke –Ped Neph 8:103-106,1994)-This Ped Neph 8:103-106,1994)-This extrapolates out to 1 ml/kg/ hr (NET UF) extrapolates out to 1 ml/kg/ hr (NET UF) over 48 hr of continuous hemofiltration. over 48 hr of continuous hemofiltration.
Dialysate/ Ultrafiltration RatesDialysate/ Ultrafiltration Rates
The UF rate/plasma flow rate [=BFRx(1-HCT)] The UF rate/plasma flow rate [=BFRx(1-HCT)] ratio should < 0.35-0.4 in order to avoid filter ratio should < 0.35-0.4 in order to avoid filter clotting (Golper AJKD 6: 373-386,1985)clotting (Golper AJKD 6: 373-386,1985)
Dialysate flow rates ranging from 10-20 Dialysate flow rates ranging from 10-20 ml/min/mml/min/m22 (~2000ml/1.72m (~2000ml/1.72m22/hr) are usually /hr) are usually adequate (experiential but consistent with adult adequate (experiential but consistent with adult data) data)
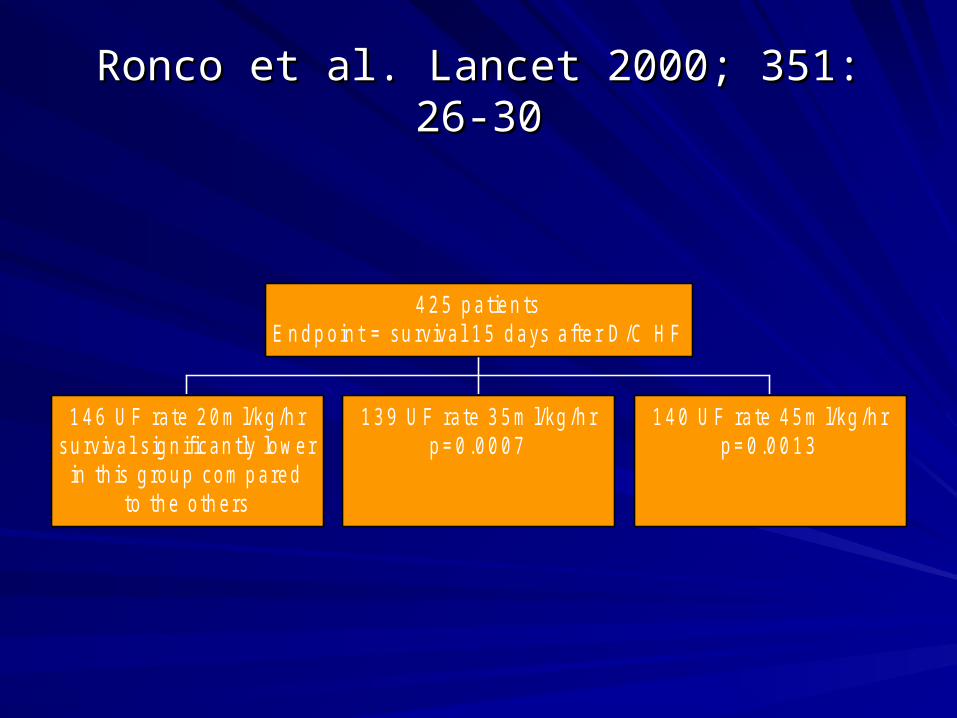
Ronco et al. Lancet 2000; 351: 26-30Ronco et al. Lancet 2000; 351: 26-30
1 4 6 U F ra te 2 0 m l/kg /h rsu rviva l s ig n ifican tly low er
in th is g rou p com p aredto th e o th ers
1 3 9 U F ra te 3 5 m l/kg /h rp = 0 .0 0 0 7
1 4 0 U F ra te 4 5 m l/kg /h rp = 0 .0 0 1 3
4 2 5 p a tien tsE n d p o in t = su rviva l 1 5 d ays a fte r D /C H F

Ronco et al. Lancet 2000; 351: 26-30Ronco et al. Lancet 2000; 351: 26-30
Conclusions:Conclusions:– Minimum UF rates should reach at least 35 Minimum UF rates should reach at least 35
ml/kg/hrml/kg/hr– Survivors in all their groups had lower BUNs Survivors in all their groups had lower BUNs
than non-survivors prior to commencement of than non-survivors prior to commencement of hemofiltrationhemofiltration
Access & MachineryAccess & Machinery
Machinery:Machinery:– PRISMA, DIAPACT, BAXTER, EDWARDS, PRISMA, DIAPACT, BAXTER, EDWARDS,
FRESENIUSFRESENIUS
Access:Access:– If poor blood flow- no point in continuing!If poor blood flow- no point in continuing!– Generally want to keep Venous pressure no > Generally want to keep Venous pressure no >
200 mm Hg200 mm Hg– IJ placement preferable (triple lumen ideal!)IJ placement preferable (triple lumen ideal!)– Size based on Patient’s sizeSize based on Patient’s size
Bicarbonate Vs Lactate FluidBicarbonate Vs Lactate Fluid
Commercial vs Custom Solutions For FRF Commercial vs Custom Solutions For FRF or Dialysateor Dialysate– Generally Bicarbonate based solutions Generally Bicarbonate based solutions
preferable (no definitive study to support this- preferable (no definitive study to support this- but easier to interpret lactic acidosis)but easier to interpret lactic acidosis)
– FDA approved: ie. Normocarb (D –only)FDA approved: ie. Normocarb (D –only)– Cost effectiveness: pharmacy/nursing costsCost effectiveness: pharmacy/nursing costs

AnticoagulationAnticoagulation
HeparinHeparin
CitrateCitrate
NoneNone– No good head to head studies comparing No good head to head studies comparing
Heparin vs. Citrate in PediatricsHeparin vs. Citrate in Pediatrics– Center specific and Comfort levelCenter specific and Comfort level
Other ConsiderationsOther Considerations
Nutrition:Nutrition:– CRRT allows optimization of nutritional CRRT allows optimization of nutritional
supplementation (esp in high catabolic states- supplementation (esp in high catabolic states- such as ARF)- but it also contributes to a such as ARF)- but it also contributes to a negative nitrogen balancenegative nitrogen balance
– Aim for anabolic state- 1.5 g/kg/day protein is Aim for anabolic state- 1.5 g/kg/day protein is inadequate – 2-3 g/kg/day better, with 20-30% inadequate – 2-3 g/kg/day better, with 20-30% increase in caloric intake over resting energy increase in caloric intake over resting energy expenditureexpenditure
– Maxvold et.al. Crit Care Med 28:2000Maxvold et.al. Crit Care Med 28:2000

Recommendations for Pediatric Recommendations for Pediatric PrescriptionPrescription
CVVH/CVVHD/CVVHDF—D useful when limited by CVVH/CVVHD/CVVHDF—D useful when limited by membrane UF capacitymembrane UF capacityPre/Post FRF or Dialysate Pre/Post FRF or Dialysate Combined UF+dialysate flow rates 10-20 ml/min/m2 Combined UF+dialysate flow rates 10-20 ml/min/m2 (~2000ml/1.72m2/hr) {INCREASE WITH TOXINS) (~2000ml/1.72m2/hr) {INCREASE WITH TOXINS) – At 0.45m2 = 540ml/hr (exceeds adult recommendations)At 0.45m2 = 540ml/hr (exceeds adult recommendations)
Net UF rate 1 ml/kg/hrNet UF rate 1 ml/kg/hrBFR (4-10 ml/kg/min)-Huge blood flow circulations in BFR (4-10 ml/kg/min)-Huge blood flow circulations in small infantssmall infants
Recommendations ContinuedRecommendations Continued
Access-Dual lumen 8 Fr (triple Lumen if Access-Dual lumen 8 Fr (triple Lumen if available)available)
Bicarbonate based Dialysate or FRFBicarbonate based Dialysate or FRF
Anticoagulation- based on patient Anticoagulation- based on patient circumstance and center experiencecircumstance and center experience
Maximize Nutrition (good communication Maximize Nutrition (good communication among caregivers imperative)among caregivers imperative)
ACKNOWLEDGEMENTSACKNOWLEDGEMENTS– MELISSA GREGORYMELISSA GREGORY– ANDREE GARDNERANDREE GARDNER– JOHN GARDNERJOHN GARDNER– THERESA MOTTESTHERESA MOTTES– TIM KUDELKATIM KUDELKA– LAURA DORSEY & BETSY ADAMSLAURA DORSEY & BETSY ADAMS
![[ ] ARF slides.ppt](https://static.documents.pub/doc/80x56/55ca7deabb61eb604e8b456c/-arf-slidesppt.jpg)
















